This is a modern-English version of Shell-shock and other neuropsychiatric problems : Presented in five hundred and eighty-nine case histories from the war literature, 1914-1918, originally written by Southard, Elmer Ernest.
It has been thoroughly updated, including changes to sentence structure, words, spelling,
and grammar—to ensure clarity for contemporary readers, while preserving the original spirit and nuance. If
you click on a paragraph, you will see the original text that we modified, and you can toggle between the two versions.
Scroll to the bottom of this page and you will find a free ePUB download link for this book.
E-text prepared by Brian Coe
and the Online Distributed Proofreading Team
(http://www.pgdp.net)
from page images generously made available by
Internet Archive
(https://archive.org)
| Note: | Images of the original pages are available through Internet Archive. See https://archive.org/details/shellshockother00sout |
THE
CASE HISTORY SERIES
The Case History Series
CASE HISTORIES IN MEDICINE
BY
Richard C. Cabot, M.D.
CASE HISTORIES IN MEDICINE
BY
Richard C. Cabot, M.D.
Third edition, revised and enlarged
Third edition, updated and expanded
DISEASES OF CHILDREN
BY
John Lovett Morse, M.D.
DISEASES OF CHILDREN
BY
John Lovett Morse, M.D.
Third edition, revised and enlarged
Third edition, updated and expanded
Presented in two hundred Case Histories
Presented in two hundred case histories
ONE HUNDRED SURGICAL PROBLEMS
BY
James G. Mumford, M.D.
ONE HUNDRED SURGICAL PROBLEMS
BY
James G. Mumford, M.D.
Second Printing
Second Edition
CASE HISTORIES IN NEUROLOGY
BY
E. W. Taylor, M.D.
CASE HISTORIES IN NEUROLOGY
BY
E.W. Taylor, M.D.
Second Printing
Second Edition
CASE HISTORIES IN OBSTETRICS
BY
Robert L. DeNormandie, M.D.
CASE HISTORIES IN OBSTETRICS
BY
Robert L. DeNormandie, M.D.
Second Edition
Second Edition
DISEASES OF WOMEN
BY
Charles M. Green, M.D.
DISEASES OF WOMEN
BY
Charles M. Green, M.D.
Second Edition
Second Edition
Presented in one hundred and seventy-three Case Histories
Presented in one hundred seventy-three case histories
NEUROSYPHILIS
MODERN SYSTEMATIC DIAGNOSIS AND TREATMENT
Presented in one hundred and thirty-seven Case Histories
BY
E. E. Southard, M.D., Sc.D.
AND
H. C. Solomon, M.D.
NEUROSYPHILIS
MODERN SYSTEMATIC DIAGNOSIS AND TREATMENT
Presented in one hundred and thirty-seven Case Histories
BY
E. E. Southard, M.D., Sc.D.
AND
H.C. Solomon, M.D.
Being Monograph Number Two of the Psychopathic Department of the Boston State Hospital, Massachusetts. (Monograph Number One was A Point Scale for Measuring Mental Ability by Robert M. Yerkes, James W. Bridges and Rose S. Hardwick. Published by Warwick and York. Baltimore 1915.)
Being Monograph Number Two of the Psychopathic Department of the Boston State Hospital, Massachusetts. (Monograph Number One was A Point Scale for Measuring Mental Ability by Robert M. Yerkes, James W. Bridges, and Rose S. Hardwick. Published by Warwick and York. Baltimore 1915.)
SHELL SHOCK and other NEUROPSYCHIATRIC PROBLEMS
Printed in five hundred and eighty-nine Case Histories
BY
E. E. Southard, M.D., Sc.D.
SHELL SHOCK and other NEUROPSYCHIATRIC ISSUES
Printed in 589 Case Histories
BY
E.E. Southard, M.D., Sc.D.
Being Monograph Number Three of the Psychopathic Department of the Boston State Hospital, Massachusetts
Being Monograph Number Three of the Psychopathic Department of the Boston State Hospital, Massachusetts
HORSLEY, 1857-1916
Horsley, 1857-1916
DEJERINE, 1849-1917
DEJERINE, 1849–1917
VAN GEHUCHTEN, 1861-1914
VAN GEHUCHTEN, 1861-1914
IN MEMORIAM
IN MEMORY
SHELL-SHOCK
AND MORE
NEUROPSYCHIATRY PROBLEMS
PRESENTED IN FIVE HUNDRED AND EIGHTY-NINE
CASE HISTORIES
PRESENTED IN 589
CASE STUDIES
FROM THE
WAR LITERATURE, 1914-1918
FROM THE
WORLD WAR I LITERATURE
BY
E. E. SOUTHARD, M.D., Sc.D.
BY
E. E. SOUTHARD, M.D., Sc.D.
Director (1917-1918), U. S. Army Neuropsychiatric Training School (Boston Unit); Late
Major, Chemical Warfare Service, U. S. Army; Bullard Professor of Neuropathology,
Harvard Medical School; Director, Massachusetts State Psychiatric
Institute (of the Massachusetts Commission on Mental Diseases);
Late President, American Medico-Psychological Association
Director (1917-1918), U.S. Army Neuropsychiatric Training School (Boston Unit); Former Major, Chemical Warfare Service, U.S. Army; Bullard Professor of Neuropathology, Harvard Medical School; Director, Massachusetts State Psychiatric Institute (of the Massachusetts Commission on Mental Diseases); Former President, American Medico-Psychological Association
WITH A BIBLIOGRAPHY BY
NORMAN FENTON, S.B., A.M.
WITH A BIBLIOGRAPHY BY
NORMAN FENTON, S.B., A.M.
Sergeant Medical Corps, U. S. Army (Assistant in Psychology to the Medical Director,
Base Hospital 117 A. E. F.); late interne in Psychology, Psychopathic Department,
Boston State Hospital; Assistant in Reconstruction, National Committee for
Mental Hygiene
Sergeant, Medical Corps, U.S. Army (Assistant in Psychology to the Medical Director,
Base Hospital 117 A.E.F.); recently an intern in Psychology, Psychopathic Department,
Boston State Hospital; Assistant in Reconstruction, National Committee for
Mental Hygiene
AND AN INTRODUCTION BY
CHARLES K. MILLS, M.D., L.L.D.
AND AN INTRODUCTION BY
CHARLES K. MILLS, M.D., L.L.D.
Emeritus Professor of Neurology, University of Pennsylvania
Emeritus Professor of Neurology, University of Pennsylvania
BY VOTE OF THE TRUSTEES OF THE BOSTON STATE HOSPITAL
MONOGRAPH NUMBER THREE
OF THE
PSYCHOPATHIC DEPARTMENT
BY VOTE OF THE TRUSTEES OF THE BOSTON STATE HOSPITAL
MONOGRAPH #3
OF THE
PSYCHOPATHIC DEPARTMENT
BOSTON
W. M. LEONARD, Publisher
1919
BOSTON
W. M. LEONARD, Publisher
1919
COPYRIGHT, 1919, BY
W. M. LEONARD
COPYRIGHT, 1919, BY
W. M. LEONARD
To
THE NATIONAL COMMITTEE FOR
MENTAL HYGIENE
AND
ITS WORK IN
WAR AND PEACE
To
THE NATIONAL COMMITTEE FOR
MENTAL HYGIENE
AND
ITS WORK IN
WAR AND PEACE
PREFACE
This compilation was begun in the preparedness atmosphere of the U. S. Army Neuropsychiatric Training School at Boston, 1917-18. This particular school had to adapt itself to the clinical material of the Psychopathic Hospital. Although war cases early began to drift into the wards (even including some overseas material), it was thought well to supplement the ordinary “acute, curable, and incipient” mental cases of the hospital wards and out-patient service with representative cases from the literature.
This collection started in the readiness environment of the U.S. Army Neuropsychiatric Training School in Boston, 1917-18. This school needed to adjust to the clinical cases from the Psychopathic Hospital. Although war-related cases began to come into the wards early on (including some from overseas), it was deemed valuable to enhance the typical “acute, curable, and incipient” mental cases in the hospital wards and outpatient services with representative cases from the literature.
As time wore on, this “preparedness” ideal gave place to the ideal of a collection of cases to serve as a source-book for reconstructionists dealing with neuroses and psychoses. Shortage of medical staff and delays incidental to the influenza epidemic held the book back still further, and, as meantime Brown and Williams had served the immediate need with their Neuropsychiatry and the War, it was determined to make the compilation the beginning of a case-history book on the neuropsychiatry of the war, following in part the traditions of various case-books in law and medicine.
As time went on, the ideal of “preparedness” shifted to the idea of creating a collection of cases to serve as a resource for reconstructionists tackling neuroses and psychoses. A lack of medical staff and delays caused by the influenza epidemic postponed the book even more. Meanwhile, since Brown and Williams had already addressed the immediate need with their Neuropsychiatry and the War, it was decided to turn the compilation into the start of a case-history book on the neuropsychiatry of the war, partly following the traditions of various case-books in law and medicine.
With the conclusion of the armistice, there is by no means an end of these problems. Peace-practice in neuropsychiatry is bound to undergo great changes and improvements, if only from the influx into the peace-community of many more trained neuropsychiatrists than were ever before available. This is particularly true in the American community by reason of the many good men specially trained in camp and hospital neuropsychiatry, both at home and in the A. E. F., through the enlightened policy of our army in establishing special divisions of the Surgeon-General’s Office dealing separately with those problems.
With the end of the armistice, these issues are far from resolved. The practice of neuropsychiatry in peace will definitely see significant changes and improvements, especially with the arrival of many more trained neuropsychiatrists than we've had before. This is especially true in the American community due to the many skilled individuals specifically trained in camp and hospital neuropsychiatry, both domestically and in the A.E.F., thanks to the forward-thinking approach of our army in creating special divisions within the Surgeon-General’s Office that focus on these issues.
Though a book primarily for physicians, some of its material has interest for line-officers, who may see how much “criming” is matter for medical experts, by running through the boxed headings (especially of Sections A and B) and[ii] reading the simulation cases. As Chavigny remarks, “shooting madmen neither restrains crime nor sets a good example.”
Though this book is mainly for doctors, some of its content might interest line-officers, who can see how much of the “criming” falls under the expertise of medical professionals by going through the boxed headings (especially in Sections A and B) and[ii] reading the simulation cases. As Chavigny points out, “shooting madmen neither stops crime nor sets a good example.”
But parts of the book look ahead to Reconstruction. Surely occupation-workers, vocationalists, war risk insurance experts, and in fact all reconstructionists, medical and lay, must find much to their advantage in the data of Section D (Treatment and Results). Had time permitted, the whole old story of “Railway Spine”—Shell-shock’s congener—might have been covered in a series of cases from last century’s literature, together with others illustrating the effects of suggestion and psychotherapy; but this must be a post-bellum task.
But parts of the book look ahead to Reconstruction. Surely, those working in occupations, vocational fields, war risk insurance experts, and all reconstructionists, both medical and non-medical, will find a lot of valuable information in the data of Section D (Treatment and Results). If there had been more time, we could have explored the entire history of “Railway Spine”— a condition similar to Shell-shock— with a series of cases from last century’s writings, along with others showing the effects of suggestion and psychotherapy; but that will have to be a task for after the war.
The compiler, who has personally dictated (and as a rule redictated and twice condensed) all the cases from the originals (or in a few instances, e.g., Russian, from translations), hopes he has not added anything new to the accounts. The cases are drawn from the literature of the belligerents, 1914-1917, English, French, Italian, Russian, and—so far as available here—German and Austrian.
The compiler, who has personally dictated (and usually redictated and condensed twice) all the cases from the original sources (or in a few instances, e.g., from translations in Russian), hopes he hasn't added anything new to the accounts. The cases are taken from the literature of the warring countries, 1914-1917, including English, French, Italian, Russian, and—as much as is available here—German and Austrian.
I would call the collection not so much a posey of other men’s flowers as a handful of their seeds. For I have constantly not so much transcribed men’s general conclusions as borrowed their specific fine-print and footnotes. The lure of the 100 per cent has been very strong in many authors; but the test of fine-print, viz., of the actual case-protocols, saves us from premature conclusions, and the plan of the book allows us to confront actualities with actualities. One gets the impression of a dignified debate from the way in which case-histories automatically confront each other, say in Section C (Diagnosis).
I’d describe the collection not so much as a bouquet of other people's flowers but rather a handful of their seeds. I haven't so much transcribed people's broad conclusions as borrowed their detailed fine print and footnotes. Many authors have been very tempted by the idea of a perfect 100 percent; however, the test of the fine print, specifically the actual case protocols, protects us from hasty conclusions, and the structure of the book lets us compare realities with realities. You get the sense of a respectful debate from the way the case histories naturally confront each other, as seen in Section C (Diagnosis).
Obligations to the books of Babinski and Froment, Eder, Hurst, Mott (Lettsomian Lectures), Roussy and Lhermitte, Elliot Smith and Pear, and others are obvious. Yealland’s book came too late for sampling its miracles, though cases of his in the periodical literature had already been incorporated in my selection.
Obligations to the works of Babinski and Froment, Eder, Hurst, Mott (Lettsomian Lectures), Roussy and Lhermitte, Elliot Smith and Pear, and others are clear. Yealland’s book arrived too late for me to sample its wonders, although his cases had already been included in my selection from the periodical literature.
Some of the cases in Section A, I, had already been abstracted in Neurosyphilis: Modern Systematic Diagnosis and Treatment (Southard and Solomon, 1917).[iii]
Some of the cases in Section A, I have already been summarized in Neurosyphilis: Modern Systematic Diagnosis and Treatment (Southard and Solomon, 1917).[iii]
What we actually have made is a case-history book in the newly combined fields now collectively termed neuropsychiatry. The more general the good general practitioner of medicine, the more of a neuropsychiatrist! And this is no pious wish or counsel of perfection. Neuropsychiatry, mental hygiene, psychotherapy and somatotherapy—all these will flourish intra-bellum and post-bellum, in days of destruction and in days of reconstruction. And who amongst us, medical or lay, will not have to deal in reconstruction days with cases like some here compiled? A minor blessing of the war will be the incorporation of mental hygiene in general medical practice and in auxiliary fields of applied sociology, e.g., medico-social work.
What we’ve actually created is a case-history book in the newly merged fields now called neuropsychiatry. The better the general practitioner of medicine, the more of a neuropsychiatrist they become! And this isn't just an idealistic wish or a call for perfection. Neuropsychiatry, mental hygiene, psychotherapy, and somatotherapy—all of these will thrive during and after war, in times of destruction and in times of rebuilding. And who among us, whether in medicine or not, won’t have to handle cases like some compiled here during the rebuilding phase? A minor benefit of the war will be the inclusion of mental hygiene in general medical practice and in related fields of applied sociology, e.g., medico-social work.
Subsidies aiding publication are due to the National Committee for Mental Hygiene; the Permanent Charity Foundation (Boston Safe Deposit and Trust Company); Mrs. Zoe D. Underhill of New York; Mr. H. T. White of New York; and Dr. W. N. Bullard of Boston—to all of these the various military recipients of the book will be under obligations, as well as others who would otherwise have had to pay the great majoration de prix due to war times.
Subsidies for publication come from the National Committee for Mental Hygiene; the Permanent Charity Foundation (Boston Safe Deposit and Trust Company); Mrs. Zoe D. Underhill of New York; Mr. H. T. White of New York; and Dr. W. N. Bullard of Boston. The military recipients of the book are grateful to all of these contributors, as well as to others, who helped avoid the significant price increase due to wartime conditions.
Of those great dead contributors to neurology laid (in the Epicrisis) at the feet of the neo-Attila, perhaps only Sir Victor was in a narrow sense the Kaiser’s victim: still, but for the war, they might all remain to us.
Of those great deceased contributors to neurology laid (in the Epicrisis) at the feet of the new Attila, perhaps only Sir Victor was, in a strict sense, the Kaiser’s victim: still, if it weren't for the war, they might all still be with us.
By the way, just as I found John Milton had said things that fitted neurosyphilis, so also Dante is observed in the chosen mottoes to have had inklings even of Shell-shock. To the Inferno it was natural to turn for fitting mottoes (Carlyle’s renderings mainly used). The pages might have been strewn with them. A glint of too great optimism might seem to shine—in the pre-Epicrisis motto—from the lance of Achilles with its “sad yet healing gift;” but out of Shell-shock Man may get to know his own mind a little better, how under stress and strain the mind lags, blocks, twists, shrinks, and even splits, but on the whole is afterwards made good again.
By the way, just as I discovered that John Milton had insights related to neurosyphilis, Dante can also be seen in the selected quotes to have hinted at what we now know as shell shock. It made sense to refer to the Inferno for appropriate quotes (mainly using Carlyle’s translations). The pages could have been filled with them. There might be a hint of excessive optimism in the pre-Epicrisis quote, with Achilles's lance and its "sad yet healing gift," but from experiencing shell shock, a person can start to understand their own mind a bit better. They may realize how, under pressure and strain, the mind can lag, block, twist, shrink, and even split, but overall, it tends to recover in the end.
E. E. Southard.
E. E. Southard.
Washington,
November, 1918.
Washington,
November 1918.
INTRODUCTION
The duties of an introducer, whether of a platform speaker to an audience, or of a writer to his anticipated readers, are not always clearly defined. It has been sometimes said that the critic or reviewer may meet with better success if he has not acquainted himself too thoroughly with the contents of the book about which he writes, as in that case he will have a larger opportunity to indulge his imagination, but a critique thus produced may have the disadvantage of possible shortcoming or unfairness. In the case of this volume, however, I have felt it worth while to acquaint myself with its contents, no light task when one is confronted with a thousand pages.
The role of an introducer, whether it's getting a speaker ready for an audience or a writer for their future readers, isn't always clearly defined. Some say that a critic or reviewer might do better if they haven’t read too deeply into the book they're discussing, as that allows more room for imagination. However, this type of critique might end up lacking depth or fairness. In the case of this volume, though, I found it worthwhile to familiarize myself with its content, which is no small feat when faced with a thousand pages.
The great war just closing has done much to enlighten us as to the causes, nature, outcome, and treatment of injuries and diseases to which its victims have been subjected. The object of this book is to present both the data and the principles involved in certain neuropsychiatry problems of the war. These are presented in a wealth of detail through an extraordinary series of case records (589 in all) drawn from current medical literature, during the first three years of the conflict. Case reporting is here seen at its best, and the experiences recorded are largely allowed to speak for themselves, although comments are not wanting and are often illuminating.
The recent war has significantly increased our understanding of the causes, nature, consequences, and treatment of the injuries and illnesses experienced by its victims. The purpose of this book is to present both the data and the principles involved in certain neuropsychiatry issues related to the war. These are detailed through an extensive collection of case records (589 in total) taken from current medical literature during the first three years of the conflict. The case reporting here is exemplary, and the experiences documented largely allow themselves to be understood, though there are also insightful comments throughout.
Many criticisms have been heard on the use of the term Shell-shock as applied to some of the most important psychiatric and neurological problems of the recent war; but that the designation has meaning will be evident if Dr. Southard’s book is not simply skimmed over by the reader, but is studied in its entirety. The symptoms of a very large number, if not the majority, of the cases recorded, had for their initiating influence the psychic[vi] and physical horrors of life among exploding shells. As the author and those from whom he has received his clinical supply not infrequently point out, in many cases it would appear that purely psychic influences have played the chief rôle, but in others physical injuries have not been lacking. Much more than this is true: in many instances the soil was prepared by previous defect, disease, or injury, or to use one of Dr. Southard’s favorite expressions, “weak spots” were present before martial causes became operative.
Many criticisms have been made about using the term Shell-shock for some of the major psychiatric and neurological issues from the recent war; however, the term's significance becomes clear if the reader not only skims through Dr. Southard’s book but studies it thoroughly. The symptoms of a very large number, if not the majority, of cases documented were initiated by the psychological and physical horrors of living among exploding shells. As the author and those who provided him with clinical insights often highlight, it appears that in many cases, purely psychological factors took center stage, but in others, physical injuries were also present. Even more important, in many instances, the groundwork for these issues was laid by previous vulnerabilities, illnesses, or injuries, or as Dr. Southard likes to say, "weak spots" existed before the war-related causes became active.
While the contributions to the medical and surgical history of the war have been somewhat numerous in current medical journals and in monographs, few comprehensive volumes have appeared. The reasons for this are not far to seek. The conflict has been of such magnitude, and the demands on the bodily and mental activity of the medical profession have been so intense and continuous, that time and opportunity for the careful and complete recording of experiences have not been often available; but works are beginning to appear in the languages of all the belligerent countries and these will increase in number and value during the next lustrum and decade, although it may be that some of the most important contributions will come after a decade or more is past. The great work before me is one that will leave its lasting impress, not only upon military but on civil medicine, for the lessons to be drawn from its pages are in large part as applicable to the one as to the other.
While there have been quite a few contributions to the medical and surgical history of the war in current medical journals and monographs, there are still not many comprehensive books available. The reasons for this are obvious. The scale of the conflict has been enormous, and the demands on the physical and mental efforts of the medical profession have been so intense and ongoing that there hasn’t often been time or opportunity to carefully and thoroughly record experiences. However, works are starting to emerge in the languages of all the countries involved in the war, and these will become more numerous and valuable over the next five years and decade. It’s possible that some of the most significant contributions will come only after a decade or more has passed. The significant work ahead of me will have a lasting impact not only on military medicine but also on civilian medicine, as the lessons learned from its pages are largely applicable to both.
Looking backward to our Civil War, one is strongly impressed with the fact that the present volume, one of the earliest works of its kind to appear in book form, deals largely with psychiatry and functional nervous diseases, whereas during and after the American conflict the most important contributions to neurology related to organic disease, especially as illustrated by the work of Weir Mitchell and his collaborators on injuries of nerves. This is the more interesting when it is remembered that Mitchell not very long after the close of the Civil War became the most prominent exponent of functional neurology, from the diagnostic[vii] and therapeutic sides. To him the profession the world over has been indebted for the development of new views as to the nature of neurasthenia and hysteria and new methods for combating these disorders. In this fact is to be found matter for thought. Those who handled best the neuropsychiatric problems of the present war were in large part qualified not merely by a knowledge of psychology and psychiatry, but far more by a thorough training in organic neurology. The problems of psychiatry can be grasped fully only by those who have a fundamental knowledge of the anatomy, physiology, and diseases of the nervous system.
Looking back at our Civil War, it’s striking to note that this volume, one of the earliest works of its kind in book form, focuses mainly on psychiatry and functional nervous diseases. In contrast, during and after the American conflict, the key contributions to neurology were related to organic diseases, particularly seen in the work of Weir Mitchell and his team on nerve injuries. This is even more interesting considering that Mitchell, shortly after the Civil War ended, became the leading advocate for functional neurology from both diagnostic and therapeutic perspectives. The profession around the world owes him for advancing new views on neurasthenia and hysteria, as well as for developing new methods to treat these disorders. This is something worth contemplating. Those who effectively addressed the neuropsychiatric challenges of the current war were largely qualified not just by their knowledge of psychology and psychiatry, but even more by their solid training in organic neurology. The issues of psychiatry can only be fully understood by those with a fundamental grasp of the anatomy, physiology, and diseases of the nervous system.
Dr. Southard, preëminently a neuropathologist, is well grounded in organic neurology, and shows at every turn his capabilities for considering the neuroses, psychoses, and insanities from the standpoint of the neurologist. Moreover, he clearly shows training and insight into the problems of non-neurological internal medicine.
Dr. Southard, a leading neuropathologist, has a solid foundation in organic neurology and consistently demonstrates his ability to analyze neuroses, psychoses, and insanities from a neurologist's perspective. Additionally, he clearly exhibits training and understanding of issues in non-neurological internal medicine.
The ideal method of training a student for neuropsychiatric work—if one had the opportunity of directing his course from the time of his entry into medicine—would be to see to it, after a good grounding in the fundamental sciences like anatomy, physiology, and chemistry, that medicine and surgery in their broadest phases first received school and hospital attention; that the fields of neurology, pure and applied, were then fully explored; and that psychology and psychiatry received late but thorough consideration. When after America’s entrance into the world war the writer assisted in preparing medical reserve officers for neuropsychiatric service, those men did best both during their postgraduate work and in base hospitals and in the field, who had built from the bottom after the manner indicated.
The best way to train a student for neuropsychiatric work—if you could guide their education from when they start studying medicine—would be to ensure that, after a solid foundation in basic sciences like anatomy, physiology, and chemistry, they first focus on the broad aspects of medicine and surgery during their school and hospital training; then thoroughly explore both pure and applied neurology; and finally, give psychology and psychiatry comprehensive attention, even if it's later on. After the U.S. entered World War I, when I helped prepare medical reserve officers for neuropsychiatric service, those who thrived both in their advanced training and in base hospitals and the field were those who followed this foundational approach.
At the outset of Dr. Southard’s book, for more than two hundred and fifty pages, the author considers under ten subdivisions the acquired diseases and constitutional defects which may predispose the soldier to functional and reflex nervous disease.[viii] Neurosyphilis, on which Dr. Southard and Dr. Solomon have already given us a valuable treatise, the pharmacopsychoses, especially alcoholism, and the somatopsychoses covering fevers like typhoid and paratyphoid, are considered in numerous carefully chosen case reports. The reader needs only to look closely into the case records of the first quarter of the volume to get a knowledge of the affections chiefly predisposing the soldier or civilian to functional and reflex nervous diseases. To those familiar with the medical history of the war it is well known that one of the reasons for the efficiency of the American Expeditionary Force resided in the fact that the preliminary examinations of the recruits received the fullest attention not only from the points of view of acquired and inherited disease, but also from those of special psychiatric and even psychological deficiencies. Our country, however, had for its guidance the experience of nations which were fighting for three years before we entered the arena and in addition had a large surplus of material from which to cull out the weaklings.
At the start of Dr. Southard’s book, over two hundred and fifty pages long, the author explores under ten categories the acquired diseases and inherent weaknesses that might make soldiers more susceptible to functional and reflex nervous disorders.[viii] Neurosyphilis, which Dr. Southard and Dr. Solomon have already addressed in a valuable treatise, pharmacopsychoses, particularly alcoholism, and somatopsychoses covering fevers like typhoid and paratyphoid, are discussed in numerous carefully selected case reports. To grasp the conditions primarily making soldiers or civilians prone to functional and reflex nervous diseases, readers only need to closely examine the case records in the first part of the volume. Those familiar with the medical history of the war know that a significant factor in the efficiency of the American Expeditionary Force was the thorough attention given to the preliminary exams of recruits, not just concerning acquired and inherited diseases, but also special psychiatric and even psychological issues. However, our country benefited from the experiences of nations that had been fighting for three years before we entered the conflict and also had a large pool of candidates to weed out the weaker individuals.
Among the predispositional affections considered—besides syphilis, alcohol, and other drug habits, and the somatopsychoses—are the feeble-mindednesses or hypophrenoses, the epilepsies, the psychoses due to focal brain lesions, the presenile and senile disorders, the schizophrenoses including dementia præcox and allied affections, the cyclothymoses like manic depressive insanity, the psychoneuroses, and the psychopathoses. The last two subjects indicated, considered in special chapters, seem to some extent to be receptacles for affections which cannot well be otherwise placed,—hallucinoses, hysteria, neurasthenia, and psychasthenia,—and under the psychopathoses, pathological lying, Bolshevism, delinquencies of various sorts, homosexuality, suicide and self-mutilation, nosophobia, and even claustrophobia with its exemplar who preferred exposure to shell-fire to remaining in a tunnel.
Among the predispositional conditions considered—besides syphilis, alcohol, and other drug habits, and somatic-psychological disorders—are cognitive impairments or mild intellectual disabilities, epilepsy, psychoses caused by specific brain injuries, age-related disorders, schizophrenia including early-onset dementia and related conditions, mood disorders like manic-depressive illness, psychoneuroses, and psychopathologies. The last two mentioned, discussed in special chapters, seem to be catch-all categories for conditions that don't fit elsewhere—such as hallucinations, hysteria, neurasthenia, and psychasthenia—and under psychopathology, include compulsive lying, Bolshevism, various types of delinquency, homosexuality, suicide and self-harm, fear of illness, and even claustrophobia exemplified by someone who preferred to face gunfire rather than stay in a tunnel.
Under the encephalopsychoses are found interesting illustrations of focal lesions and the general effects of infection and[ix] toxemia. Cases of brain abscess, of spinal focal lesions, and meningeal hemorrhage are in evidence, aphasias, monoplegias, Jacksonian spasm, and thalamic disease receiving consideration.
Under encephalopsychoses, there are interesting examples of localized damage and the overall effects of infection and[ix]toxemia. Cases of brain abscesses, spinal focal lesions, and bleeding in the membranes surrounding the brain are noted, along with conditions like aphasia, monoplegia, Jacksonian spasms, and thalamic disorders being taken into account.
All neurologists know the difficulties in diagnosticating epilepsy in the absence of opportunities to see attacks and to receive the carefully analyzed statement of the observers of the patient. All this and much more is well brought out in the chapter on the epileptoses. Many epileptics found their way into the armies either through the carelessness of examiners or by suppression of the facts on the part of those who desired to serve.
All neurologists understand the challenges in diagnosing epilepsy without the chance to witness seizures and receive detailed accounts from those observing the patient. This, and much more, is clearly presented in the chapter on the epileptoses. Many people with epilepsy ended up in the military either due to the negligence of examiners or by hiding the truth from those who wanted to serve.
The fact that an imbecile can shoot straight and face fire comes out in one or two places, but this does not seem to prove that a good rifleman is necessarily an all-round good soldier.
The fact that a fool can shoot accurately and handle fire comes up in a few instances, but this doesn't seem to prove that a skilled marksman is automatically a well-rounded soldier.
A book like Dr. Southard’s could be made of much use in teaching students, especially postgraduates, by having them, when a particular subject like epilepsy or schizophrenia, for instance, is under discussion, use as collateral reading the case reports of this work.
A book like Dr. Southard’s could be really helpful in teaching students, especially grad students, by having them use the case reports from this work as supplementary reading when topics like epilepsy or schizophrenia are being discussed.
Dr. Southard’s book will prove useful to many workers—to the medical officer whose duty it is to examine recruits for the service or to pass upon and treat them while in service; almost equally to the medical officer in time of peace; to authors of textbooks and treatises and to contributors to neurological and psychiatric journals; to lecturers and clinical demonstrators; to the examiner for the juvenile courts; and to members of the psychopathic, psychiatric, and neurological staffs of our hospitals.
Dr. Southard’s book will be helpful to many professionals—including the medical officer responsible for examining recruits or providing treatment during service; it’s just as valuable to the medical officer in peacetime, to authors of textbooks and research papers, and to contributors to neurology and psychiatry journals; to lecturers and clinical demonstrators; to examiners for juvenile courts; and to members of the psychopathic, psychiatric, and neurological teams in our hospitals.
One is not called upon in an introduction to review at length the contents of the volume, but it may prove of value to the reader to dip here and there into the pages of the work to which his attention is being invited.
One doesn't need to provide a detailed review of the book in an introduction, but it might be helpful for the reader to browse through different sections of the work being recommended.
It will be remembered that fifty years ago and much later, down to the time of Babinski’s active propaganda in favor of the theories of suggestion, counter-suggestion, and persuasion in hysteria, various affections of a vasomotor and thermic type[x] were included in the list of hysterical phenomena. These and some other phenomena sometimes classed as hysterical, Babinski and those who accord with him now find it necessary to sweep entirely from the domain of hysteria, which being produced by suggestion and cured by counter-suggestion or persuasion cannot include symptoms which are beyond the control of the will and intellect of the patient.
It’s important to note that fifty years ago and even later, up until Babinski’s active promotion of suggestion, counter-suggestion, and persuasion theories in hysteria, various symptoms related to blood flow and temperature regulation[x] were considered part of hysterical phenomena. Babinski and his supporters now find it necessary to completely remove these and some other symptoms previously classified as hysterical from the hysteria category, as these conditions arise from suggestion and can be treated by counter-suggestion or persuasion, which means they cannot include symptoms that the patient cannot control with their will or intellect.
According to the new or rather revived pronouncement, these must be due either to definite organic lesion, or to a disorder of reflex origin, connoting the occurrence of changes in the nervous centers as long ago taught by Vulpian and Charcot. In the records of cases and in the discussions thereon this differentiation receives much consideration.
According to the new or rather revived statement, these must be due either to a specific organic issue or to a reflex disorder, indicating that changes are happening in the nervous centers, as long ago explained by Vulpian and Charcot. In the case records and the discussions around them, this distinction gets a lot of attention.
It is held that the paralysis in the reflex cases is more limited, more persistent, and assumes special forms not observable in hysteria. The attitudes in hysterical palsies conform more to the natural positions of the limbs than do those observed in reflex paralysis. Probably the presence of marked amyotrophies in the reflex nervous disorders is the most convincing factor in separating these from pithiatic affections. These atrophies correspond to the arthritic muscular atrophies of Vulpian, Charcot, Gowers, and others, and cannot for a moment be regarded as caused by suggestion or as removable by counter-suggestion or persuasion. They are influenced, discounting the effect of time and natural recuperation, only by methods of treatment designed to improve the peripheral and central nutrition of the patient. Pithiatic atrophies are slight and probably always to be accounted for by disuse or the association of some peripheral neural disorder with the hysteria. Affections of the sudatory and pilatory systems are more definitely pronounced in reflex cases than in those of a strictly hysterical character.
It is believed that the paralysis in reflex cases is more limited, more persistent, and takes on specific forms that aren't seen in hysteria. The postures in hysterical paralysis align more with the natural positions of the limbs compared to those in reflex paralysis. Likely, the notable muscle wasting in reflex nerve disorders is the most convincing factor in distinguishing these from pithiatic conditions. This muscle wasting corresponds to the arthritic muscle atrophies described by Vulpian, Charcot, Gowers, and others, and cannot be considered as caused by suggestion or something that can be fixed through counter-suggestion or persuasion. They are influenced, aside from the effects of time and natural healing, solely by treatment methods aimed at improving the patient’s peripheral and central nutrition. Pithiatic atrophies are mild and are likely always due to disuse or the association of some peripheral nerve disorder with the hysteria. Issues with sweating and hair growth are more pronounced in reflex cases than in purely hysterical ones.
Some of the facts brought forward by Babinski and Froment to demonstrate the differentiation of reflex paralyses from pithiatic disorders of motion are challenged in the records of this volume by others, as for instance, by Dejerine, Roussy, Marie,[xi] and Guillain. Babinski tells us that in pithiatism, properly so designated, the tendon reflexes are not affected. He believes that even in pronounced anesthesia of the lower extremities the plantar reflexes can always be elicited and are not abnormal in exhibition. Dejerine, however, produces cases to illustrate the fact that in marked hysterical anesthesia of the feet plantar responses cannot be produced. I have personally studied cases which lend some strength to either contention. In some of these I was not able to conclude that either the use of the will or the presence of contractions in extension was sufficient to exclude the normal responses.
Some of the facts presented by Babinski and Froment to show the difference between reflex paralysis and pithiatic movement disorders are questioned in this volume by others, such as Dejerine, Roussy, Marie,[xi] and Guillain. Babinski states that in true pithiatism, the tendon reflexes are not affected. He believes that even with significant anesthesia in the lower limbs, the plantar reflexes can always be triggered and appear normal. However, Dejerine provides cases that illustrate that in severe hysterical anesthesia of the feet, plantar responses cannot be elicited. I have personally studied cases that support both arguments. In some of these, I couldn't determine that either the use of will or the presence of extension contractions was enough to rule out normal responses.
Differences in muscle tonicity, in mechanical irritability of the muscles, and the presence or absence of fibrotendinous contractions are indications of a separation between the reflex and purely functional cases, as apparently demonstrated in some of the case records. True trophic disorders of the skin, hair, and bones observed in the reflex cases are also said to have no place in the illustrations of pithiatism.
Differences in muscle tone, how easily the muscles respond to stimuli, and whether there are fibrotendinous contractions are signs of a distinction between reflexive and purely functional cases, as shown in some case records. Genuine trophic disorders of the skin, hair, and bones seen in the reflex cases are also said to be absent in the examples of pithiatism.
The delver into the case histories of this volume will find numerous instructive combinations of hystero-reflex and organo-hysterical associations which are not to be enumerated in an introduction. The great importance of what all recognize as pathognomonic signs of organic disease—Babinski extensor toe response, persistent foot clonus, reactions of degeneration, marked atrophy, lost tendon jerks, etc.—is, of course, continuously in evidence. Extraordinary associations of hysterical, organic, and reflex disorders with other affections due to direct involvement of bone, muscle, and vessels and with the secondary effects of cicatrization and immobilization are brought out on many pages. In quitting this branch of our subject it might be remarked that considerable changes must be made in our textbook descriptions of nervous diseases in the light of the contributions to the neurology of the present war.
The person looking into the case histories in this volume will find many informative combinations of hystero-reflex and organo-hysterical associations that can't just be listed in an introduction. The significant importance of what everyone recognizes as distinctive signs of organic disease—such as the Babinski extensor toe response, persistent foot clonus, degeneration reactions, noticeable atrophy, lost tendon jerks, and so on—is always evident. Unusual links between hysterical, organic, and reflex disorders with other conditions caused by direct involvement of bones, muscles, and blood vessels, as well as the secondary effects of scarring and immobilization, are highlighted on many pages. As we move away from this area of our discussion, it should be noted that we need to make significant changes to our textbook descriptions of nervous diseases in light of the contributions to neurology from the current war.
One is reminded in the details of some of the cases of the discussions some decades since on the subject of spinal traumatisms;[xii] of the work of Erichsen which resulted in giving his name and that of “railway spine” to many of the cases now commonly spoken of as traumatic hysteria and traumatic neurasthenia; of the rejoinders of Page and his views regarding spinal traumatisms; and of Oppenheim’s development of the symptom complex of what he prefers to term the traumatic neurosis. One who has taken part in much court work cannot but read these case records with interest, for the neurology of the war as presented in this volume and in numerous monographs which are now appearing, throws much light upon many often mooted medicolegal problems. I recall how many able and honest neurological observers have changed their points of view since the early days of Erichsen’s “railway spine,” a pathological suggestion which is said to have cost the corporations of England an almost fabulous sum during a score of years. I recall also that a certain Court of Appeals in one of our states even felt itself called upon to promulgate an opinion intended to exorcise entirely the plea for damages for alleged injuries if it could be shown that these were due to fright. The data of this book do not put weapons entirely into the hands of the attorney and the expert for either the plaintiff or the defendant.
One is reminded in the details of some of the cases of the discussions from a few decades ago about spinal injuries; [xii] of Erichsen's work, which led to his name and the term “railway spine” being associated with many cases now commonly referred to as traumatic hysteria and traumatic neurasthenia; of Page's responses and his views on spinal injuries; and of Oppenheim’s development of the symptom complex he prefers to call traumatic neurosis. Anyone who has participated in much court work cannot help but read these case records with interest, as the neurology of the war presented in this volume and in numerous monographs now being published sheds light on many frequently debated legal and medical issues. I remember how many skilled and honest neurological observers have changed their perspectives since the early days of Erichsen’s “railway spine,” a pathological concept that is said to have cost the corporations of England an almost unbelievable amount over the years. I also recall that a certain Court of Appeals in one of our states even felt compelled to issue an opinion aimed at completely dismissing claims for damages for alleged injuries if it could be shown that these were caused by fear. The data in this book do not fully empower the attorney and the expert for either the plaintiff or the defendant.
Some of the French writers on the neurology of the war, as illustrated in the records collected by Dr. Southard, have brought to our attention distinctions which they draw between états commotionnels and états émotionnels—happy terms, and yet not sufficient in their invention or in the explanations which accompany them, fully to satisfy the requirements of the facts presented. These writers seem to think of the commotional states as denoting some real disease or condition of the brain, and yet one which is really curable and reversible. They explicitly tell us, however, that these commotions fall short of being lésionnel. After all, is this not somewhat obscure? Is it not something of a return to the period of “railway spine” when one of the comparisons sometimes made was that the injury suffered by the nervous tissues produced in them a state[xiii] comparable to that of a magnet which had been subjected to a severe blow? At any rate, in commotion thus discussed the nervous structures are supposed to sustain some real injury of a physiochemical character, whereas in the emotional states the neurones are, as Southard puts it, affected somewhat after the manner of normal emotional functioning, except perhaps that they are called upon to deliver an excessive stream of impulses. The latter would be classed among the psychopathic, the former among the physiopathic affections, and yet the distinction between the two is not always quite clear.
Some French writers studying the neurology of war, as shown in the records gathered by Dr. Southard, have pointed out differences between états commotionnels and états émotionnels—terms that are helpful, but their definitions and explanations don't fully capture the facts at hand. These writers seem to view commotional states as indicating some real disease or condition of the brain, yet one that is truly treatable and reversible. They specifically mention that these commotions do not reach the level of lésionnel. Isn't that a bit vague? Doesn't it harken back to the time of “railway spine,” when one of the comparisons sometimes made was that the injury to the nervous tissues created a condition similar to that of a magnet that had been struck hard? In any case, the commotion being discussed is thought to result in some actual injury of a physiochemical nature, while in the emotional states, the neurones, as Southard explains, are affected somewhat like normal emotional functioning, except perhaps that they are required to produce an excessive flow of impulses. The former would be categorized under psychopathic conditions, while the latter falls into physiopathic issues, yet the line between the two isn't always very clear.
In not a few instances of Shell-shock—although these are not numerous, so far as records have been obtained—actual structural lesions have been recorded even in cases in which no direct external injury of a material kind was experienced as a result of the explosion of shells. In others the evidences of external injury were relatively unimportant. Various lesions, in some cases recognizable even by the naked eye, were present. Mott, for example, found not only minute hemorrhages, but in one instance a bulbar extravasation of moderate massiveness, the patient not showing external signs of injury. Cases are also recorded of hematomyelia; others with edematous or necrotic areas in the cord; and still others with lesions of the ependyma or even with splitting of the spinal canal, reminding one of the classical experiments of Duret on cerebral and cerebrospinal traumatisms.
In several cases of Shell Shock—though these are not common based on the records available—actual physical damage has been noted, even when there was no direct external injury from shell explosions. In some instances, the signs of external injury were relatively minor. Various injuries, some visible even to the naked eye, were observed. For example, Mott found not only tiny hemorrhages but also, in one case, a significant bulbar hemorrhage, although the patient showed no external signs of injury. There are also reports of hematomyelia, as well as cases with swollen or dead areas in the spinal cord, and others with damage to the ependyma or even splitting of the spinal canal, reminiscent of Duret's classic experiments on brain and spinal cord injuries.
It has been argued that too much stress should not be laid on a few cases of this sort—but are they as few as they seem to be? The fact is that necropsical opportunities are not often afforded. May not such scattered lesions often be present without resulting in death or even in long continued disturbance? There is no essential reason why minute hemorrhages into the brain and spinal cord, and especially into their membranes, may not undergo rapid absorption or even remain unchanged for some time without dire results.
It has been argued that we shouldn’t focus too much on a few cases like this—but are they really as few as they appear? The truth is that we don’t often get the chance to conduct autopsies. Could these scattered injuries be present without leading to death or even causing long-term issues? There’s no fundamental reason why tiny hemorrhages in the brain and spinal cord, especially in their membranes, can’t be quickly absorbed or even stay the same for a while without severe consequences.
One of the reported cases in which lung splitting occurred from[xiv] severe concussion without external injury is not without interest in this connection, reminding one, as the commentator says, of those cases of severe concussion in which the interior of a building is injured while the exterior escapes. In the same connection also the cited experiments of Mairet and Durante on rabbits are not without instructiveness. As a result of explosives set off close to these animals, pulmonary apoplexy, spinal cord and root hemorrhages, and extravasations, perivascular and ependymal, and into the cortical and bulbar gray were found. Russca obtained direct and contrecoup brain lesions, etc., in a similar way.
One of the reported cases where a lung split occurred due to severe concussion without any external injury is quite interesting. It brings to mind, as the commentator mentions, those instances of severe concussion where the inside of a building is damaged while the outside remains unharmed. In the same vein, the experiments conducted by Mairet and Durante on rabbits are also quite enlightening. After explosives were detonated near these animals, they observed pulmonary hemorrhaging, spinal cord and nerve root bleeding, as well as bleeding and fluid accumulation around blood vessels and in the brain's gray matter. Russca also found direct and contrecoup brain injuries in a similar manner.
Here and there throughout the book will be found references to symptoms and syndromes which will have a particular interest for the reader—soldier’s heart, trench foot, congealed hand, tics, tremors, convulsions, sensory areas variously mapped, and forms of local tetanus, the last being distinctly to be differentiated from pithiatic contractures and those due to organic lesions of the nervous system. Cases of an affection described by Souques as camptocormia, from Greek words meaning to bend the trunk, were shown to the Neurological Society of Paris in 1914 and later, the main features of this affection being pronounced incurvation forward of the trunk from the dorsolumbar region, with extreme abduction and outward rotation of the lower limbs, pain in the back, and difficult and tremulous walking. In some of these cases, organic lesions of the trunkal tissues were present, but in addition psychic elements played a not unimportant part, and the cases were restored to health by a combination of physical measures with psychotherapy, enforced by electrical applications.
Here and there throughout the book, you'll find references to symptoms and syndromes that will particularly interest the reader—soldier’s heart, trench foot, congealed hand, tics, tremors, convulsions, variously mapped sensory areas, and forms of local tetanus, the last of which should be clearly distinguished from pithiatic contractures and those resulting from organic lesions of the nervous system. Cases of a condition described by Souques as camptocormia, derived from Greek words meaning to bend the trunk, were presented to the Neurological Society of Paris in 1914. The main features of this condition involve a pronounced forward bending of the trunk from the dorsolumbar region, with extreme abduction and outward rotation of the lower limbs, back pain, and difficult, shaky walking. In some of these cases, organic lesions of the trunk tissue were present, but psychological factors also played a significant role, and patients were restored to health through a combination of physical treatments and psychotherapy, supported by electrical applications.
The part of this book given over to the discussion of treatment will doubtless to some prove the most interesting section. The presentation of the subject of therapeutics is in some degree a discussion also of diagnosis and prognosis; and so it happens in various parts of the volume that the particular subject under consideration is more or less a reaffirmation or anticipation of remarks under other headings.
The section of this book dedicated to the discussion of treatment will certainly be the most interesting part for some readers. The way therapeutics is discussed also involves elements of diagnosis and prognosis; as a result, throughout the book, the topic being addressed often reaffirms or anticipates points made in other sections.
Similar results are brought about by various therapeutic procedures. Nonne, Myers, and a few others bring hypnosis into the foreground, although non-hypnotic suggestion plays a larger rôle by far.
Similar results come from different therapeutic methods. Nonne, Myers, and a few others highlight hypnosis, although non-hypnotic suggestion plays a much larger role.
Miracle cures are wrought through many pages. Mutism, deafness and blindness, palsies, contractures, and tics disappear at times as if by magic under various forms of suggestion. Ether or chloroform narcosis drives out the malady at the moment when it reveals its true nature. Verbal suggestion has many adjuvants and collaborators—electricity, sometimes severely administered, lumbar puncture, injections of stovaine into the cerebrospinal fluid, injections of saline solution, colored lights, vibrations, active mechanotherapy, hydrotherapy, hot air baths and blasts, massage, etc. Painful and punitive measures have their place—one is inclined to think a less valuable place than is given them by some of the recorders. In some instances the element of suggestion, while doubtless present, is overshadowed by the material methods employed. Persuasion and actual physical improvement are in these cases highly important. Reëducation is not infrequently in evidence. The patient in one way or another is taught how to do things which he had lost the way of doing.
Miracle cures are created through many pages. Conditions like mutism, deafness, blindness, palsies, contractures, and tics sometimes vanish as if by magic under different forms of suggestion. Ether or chloroform anesthesia can eliminate the illness at the moment it shows its true nature. Verbal suggestion has many helpers—electricity, sometimes given in strong doses, lumbar puncture, stovaine injections into the cerebrospinal fluid, saline solution injections, colored lights, vibrations, active mechanotherapy, hydrotherapy, hot air baths and blasts, massage, and more. Painful and punitive measures have their place—though one might argue a less significant role than some reports suggest. In certain cases, while the element of suggestion is likely present, it is overshadowed by the physical methods used. Persuasion and actual physical improvement are very important in these instances. Re-education is often evident. The patient is taught, in one way or another, how to do things they had forgotten how to do.
It is interesting to American neurologists to note how frequently in the reports, especially of French observers, the “Weir Mitchell treatment” was the method employed, including isolation, the faradic current, massage, and Swedish movements, hydrotherapy, dietetic measures, reëducative processes, and powerful suggestion variously exhibited, especially through the mastery of the physician over the patient. It is rather striking that few records of Freudian psychoanalytic therapy are presented.
It’s interesting for American neurologists to see how often the “Weir Mitchell treatment” was used in reports, especially by French observers. This included isolation, the faradic current, massage, Swedish movements, hydrotherapy, dietary measures, re-educative processes, and strong suggestion, particularly through the physician's control over the patient. It's quite noticeable that there are few records of Freudian psychoanalytic therapy.
When all is said, however, counter-suggestion and persuasion, in whatever guise made use of, were not always sufficient and this not only in the clearly organic cases, but in those which are ranked under the head of reflex nervous disorders. In these the long-continued use of physical agencies was found necessary to[xvi] supplement the purely psychic procedures, these facts sometimes giving rise in the Paris Society of Neurology and elsewhere to animated discussion as to the real nature of the cases. The pithiatic features of the case at times disappear, but leave behind much to be explained and more to be accomplished. The cures wrought are not always permanent and in some cases post-bellum experiences may be required to prove the real value of the measures advocated. The reader must study well the detailed records in order to arrive at just conclusions; nevertheless, the tremendous efficacy of suggestion and persuasion stands out in many of the recitals.
When everything is considered, though, counter-suggestion and persuasion, in whatever form they are used, weren’t always enough. This was true not only in clear organic cases but also in those classified as reflex nervous disorders. In these instances, long-term use of physical methods was necessary to supplement purely psychological approaches. These facts sometimes sparked lively debates within the Paris Society of Neurology and other places regarding the true nature of these cases. The pithiatic features may sometimes fade, but they leave behind much to clarify and more to achieve. The cures achieved are not always lasting, and in some cases, post-war experiences may be needed to properly assess the actual effectiveness of the recommended treatments. Readers must carefully examine the detailed records to draw accurate conclusions; nevertheless, the significant power of suggestion and persuasion is evident in many of the accounts.
Perhaps the author may permit the introducer a little liberty of comment. His non-English interpellations, especially Latin and French, may be regarded by some as overdone or perhaps pedantic, but are rather piquant, giving zest to the text. Diagnosis per exclusionem in ordine is sonorous and has a scholarly flavor, but does not prevent the reader who lives beyond the faubourgs of Boston from understanding that the author is speaking of an ancient and well-tried method of differential diagnosis. Passim may be more impressive or thought-fixing than its English translation, but this to the reader will simply prove a matter of individual opinion. Psychopathia martialis is not only mouth-filling like Senegambia or Mesopotamia, but really has a claim to appreciation through its evident applicability. It is agreeable to note that the book seems nowhere to indicate that psychopathia sexualis and psychopathia martialis are convertible terms.
Maybe the author will allow the introducer a bit of freedom to comment. His non-English references, especially in Latin and French, might seem excessive or even pretentious to some, but they add a nice touch and bring excitement to the text. Diagnosis per exclusionem in ordine sounds scholarly and has a nice ring to it, but it doesn’t stop readers outside of Boston from recognizing that the author is talking about an old and well-known method of differential diagnosis. Passim might be more impressive or memorable than its English equivalent, but that will really just depend on individual opinions. Psychopathia martialis is not only a mouthful like Senegambia or Mesopotamia, but it also deserves appreciation for its clear relevance. It’s nice to see that the book doesn’t suggest that psychopathia sexualis and psychopathia martialis are interchangeable terms.
The bibliography of the volume challenges admiration because of its magnitude and thoroughness and is largely to be credited, as the author indicates, to the energy and efficiency of Sergeant Norman Fenton, who did the work in connection with the Neuropsychiatric Training School at Boston, resorting first-hand to the Boston Medical Library and the Library of the New York Academy of Medicine. After Sergeant Fenton joined the American Expeditionary Force, Dr. Southard greatly increased the value of the bibliography by his personal efforts.
The bibliography of the volume commands respect due to its size and depth and is primarily thanks to the hard work and efficiency of Sergeant Norman Fenton, who contributed while associated with the Neuropsychiatric Training School in Boston, making direct use of the Boston Medical Library and the New York Academy of Medicine Library. After Sergeant Fenton became part of the American Expeditionary Force, Dr. Southard significantly enhanced the bibliography through his personal contributions.
This bibliography covers not only the 589 case histories of the book, but it goes beyond this, especially in the presentation of references for 1917, 1918, and even 1919. Owing to the time when our country entered the war, American references are, in the main, of later date than the case histories. They will be found none the less of value to the student of neuropsychiatric problems.
This bibliography includes not just the 589 case histories from the book, but it also expands on this, particularly with the references from 1917, 1918, and even 1919. Because of when our country entered the war, most American references are dated later than the case histories. Nevertheless, they will still be valuable to anyone studying neuropsychiatric issues.
The references in the bibliography number in all more than two thousand, distributed so far as nationalities are concerned about as given below, although some mistakes may have crept into this enumeration for various reasons, like the publication of the same articles in the journals of different countries. The list of references includes French, 895; British (English and Colonial), 396; Italian, 77; Russian, 100; American, 253; Spanish, 5; Dutch, 5; Scandinavian, 5; and Austrian and German, 476. It will be seen, therefore, that the bibliography covers in number nearly four times the collected case studies, most of these records being from reports made during the first three years of the war. The author has wisely made an effort to bring the bibliographic work up to and partially including 1919.
The references in the bibliography total over two thousand, categorized by nationality as follows, although there may be some errors in this count for various reasons, such as the same articles being published in different countries' journals. The list of references includes: French, 895; British (English and Colonial), 396; Italian, 77; Russian, 100; American, 253; Spanish, 5; Dutch, 5; Scandinavian, 5; and Austrian and German, 476. Therefore, it's clear that the bibliography is nearly four times the number of collected case studies, with most of these records coming from reports made during the first three years of the war. The author has sensibly worked to update the bibliographic work to include information up to and partially including 1919.
The manner in which the French neurologists and alienists continued their work during the strenuous days of the terrible conflict is worthy of all praise. The labors of the Society of Neurology of Paris never flagged, its contributions in current medical journals having become familiar to neurologists who have followed closely the trend of medical events during the war. Cases and subjects were also frequently presented and discussed at the neurological centers connected with the French and allied armies in France.
The way French neurologists and psychiatrists carried on their work during the challenging days of the awful conflict deserves high praise. The Society of Neurology of Paris never slowed down; its contributions in medical journals became well-known to neurologists who kept a close eye on medical developments during the war. Cases and topics were often presented and discussed at the neurological centers associated with the French and allied armies in France.
It may be almost invidious to specify names, the work done by many was of so much interest and value. Dejerine in the early days of the war, before his untimely sickness and death, contributed his part. Marie from the beginning to the end of the conflict continued to make the neurological world his debtor. The name of Babinski stands out in striking relief. Other[xviii] names frequently appearing among the French contributors are those of Froment, Clovis Vincent, Roussy and Lhermitte, Léri, Guillain, Souques, Laignel-Lavastine, Courbon, Grasset, Claude, Barre, Benisty, Foix, Chavigny, Charpentier, Meige, Thomas, and Sollier.
It might seem unfair to mention specific names since the work done by many was so significant and valuable. Dejerine, in the early days of the war, before his untimely illness and death, played his part. Marie contributed significantly from the beginning to the end of the conflict, leaving the neurological community in his debt. The name Babinski stands out prominently. Other[xviii] names that frequently appear among the French contributors include Froment, Clovis Vincent, Roussy, Lhermitte, Léri, Guillain, Souques, Laignel-Lavastine, Courbon, Grasset, Claude, Barre, Benisty, Foix, Chavigny, Charpentier, Meige, Thomas, and Sollier.
For a work of this character not only as complete a bibliography as possible, but a thorough index is absolutely necessary, and this has been supplied. The author has not made the index too full, but with enough cross-references to enable those in all lines of medical work interested to cull out the cases and comments which most concern them.
For a work like this, a complete bibliography and a thorough index are essential, and this has been provided. The author hasn't made the index overly detailed, but there are enough cross-references to help those in all areas of medical work find the cases and comments that matter most to them.
My prologue finished, I step aside for the play and the player, with the recommendation to the reader that he give close heed to the performance—to the recital of the cases, the comments thereon, and the general discussion of subjects—knowing that such attention will be fully rewarded, for in this wonderful collection of Dr. Southard is to be seen an epitome of war neurology not elsewhere to be found.
With my introduction complete, I now step back for the play and the performer, encouraging the reader to pay close attention to the performance—following the cases presented, the commentary on them, and the overall discussion of the topics—understanding that such focus will be richly rewarded. In this remarkable collection by Dr. Southard, you will find a summary of war neurology that can't be found anywhere else.
Charles K. Mills.
Charles K. Mills.
Philadelphia, May, 1919.
Philadelphia, May 1919.
TABLE OF CONTENTS
| SECTION A. PSYCHOSES INCIDENTAL IN THE WAR | |||
| I. The Syphilis Society (Syphilopsychoses) | |||
| Case | Page | ||
| 1. | Desertion of an officer | Briand, 1915 | 8 |
| 2. | Visions of a naval officer | Carlill, Fildes, Baker, 1917 | 9 |
| 3. | Aggravation of neurosyphilis by war | Weygandt, 1915 | 10 |
| 4. | Same | Hurst, 1917 | 10 |
| 5. | Same | Beaton, 1915 | 10 |
| 6. | Same | Boucherot, 1915 | 11 |
| 7. | Same | Todd, 1917 | 12 |
| 8. | Same | Farrar, 1917 | 13 |
| 9. | Same | Marie, Chatelin, Patrikios, 1917 | 14 |
| 10. | Root-sciatica | Long, 1916 | 15 |
| 11. | Disciplinary | Kastan, 1916 | 17 |
| 12. | Same | Kastan, 1916 | 18 |
| 13. | Same? | Kastan, 1916 | 19 |
| 14. | Hysterical chorea versus neurosyphilis | de Massary, du Sonich, 1917 | 20 |
| 15. | Traumatic general paresis | Hurst, 1917 | 22 |
| 16. | Head trauma; shell-shock; mania; W. R. positive | Babonneix, David, 1917 | 23 |
| 17. | Head trauma in a syphilitic | Babonneix, David, 1917 | 24 |
| 18. | Shell wound: general paresis | Boucherot, 1915 | 25 |
| 19. | “Shell-shock” ocular palsy: syphilitic | Schuster, 1915 | 26 |
| 20. | Shell-shock: general paresis | Donath, 1915 | 27 |
| 21. | Shell-shock: tabes | Logre, 1917 | 28 |
| 22. | Same | Duco, Blum, 1917 | 28 |
| 23. | Pseudotabes (Shell-shock) | Pitres, Marchand, 1916 | 29 |
| 24. | Shell-shock neurosyphilis | Hurst, 1917 | 30 |
| 25. | Shell-shock neurosyphilis | Hurst, 1917 | 31 |
| 26. | Pseudoparesis (Shell-shock) | Pitres, Marchand, 1916 | 32 |
| 27. | War strain and Shell-shock in a syphilitic | Karplus, 1915 | 34 |
| 28. | Shell-shock recurrence of syphilitic hemiplegia | Mairet, Piéron, 1915 | 36 |
| 29. | Shell-shock (functional!) amaurosis in a neurosyphilitic | Laignel-Lavastine, Courbon, 1916 | 37 |
| 30. | Shell-shock (functional) phenomena in a neurosyphilitic | Babonneix, David, 1917 | 39 |
| [xx]31. | Vestibular symptoms in a neurosyphilitic | Guillain, Barré, 1916 | 40 |
| 32. | Syphilophobic suicidal attempts | Colin, Lautier, 1917 | 41 |
| 33. | Simulated chancre | Pick, 1916 | 42 |
| 34. | Exaggeration | Buscaino, Coppola, 1916 | 43 |
| II. The Weak-minded Group (Hypophrenoses) | |||
| 35. | A feeble-minded person fit for service | Pruvost, 1915 | 44 |
| 36. | An imbecile superbrave | Pruvost, 1915 | 45 |
| 37. | An imbecile fit for barracks work | Pruvost, 1915 | 45 |
| 38. | A feeble-minded inventor | Laignel-Lavastine, Ballet, 1917 | 47 |
| 39. | A feeble-minded simulator | Pruvost, 1915 | 49 |
| 40. | Enlistment for amelioration of character | Briand, 1915 | 49 |
| 41. | An imbecile fit for service at the front | Pruvost, 1915 | 50 |
| 42. | An imbecile with sudden initiative | Lautier, 1915 | 51 |
| 43. | Emotional fugue in subnormal subject | Briand, 1915 | 52 |
| 44. | Regimental surgeon versus alienist re feeble-mindedness | Kastan, 1916 | 53 |
| 45. | An imbecile rifleman | Kastan, 1916 | 55 |
| 46. | An imbecile hypomaniacal | Haury, 1915 | 57 |
| 47. | Feeble-minded desire to remain at the front | Kastan, 1916 | 58 |
| 48. | An imbecile sent back by Germans | Lautier, 1915 | 60 |
| 49. | Unfit for service: feeble-mindedness? | Kastan, 1916 | 61 |
| 50. | Oniric delirium in a feeble-minded subject | Soukhanoff, 1915 | 62 |
| 51. | Shell-shock and burial: situation not rationalized | Duprat, 1917 | 63 |
| 52. | Shell-shock in weak-minded subject; fear, fugues | Pactet, Bonhomme, 1917 | 64 |
| III. The Epilepsy Group (Epileptoses) | |||
| 53. | Epilepsy: neurosyphilis | Hewat, 1917 | 65 |
| 54. | Epilepsy brought out by syphilis | Bonhoeffer, 1915 | 66 |
| 55. | Syphilis in a psychopathic subject | Bonhoeffer, 1915 | 67 |
| 56. | Epileptic imbecile court-martialed | Lautier, 1916 | 68 |
| 57. | Psychogenic seizures in feeble-minded subject | Bonhoeffer, 1915 | 69 |
| 58. | Drunken epileptic: responsibility? | Juquelier, 1917 | 71 |
| 59. | Epilepsy: disciplinary case | Pellacani, 1917 | 74 |
| 60. | Same | Pellacani, 1917 | 76 |
| 61. | Desertion: epileptic fugue | Verger, 1916 | 78 |
| 62. | Specialist in escapes | Logre, 1917 | 80 |
| 63. | Epilepsy and other factors: disciplinary case | Consiglio, 1917 | 82 |
| 64. | Strange conduct and amnesia in epileptic | Hurst, 1917 | 83 |
| 65. | Epilepsy after antityphoid inoculation | Bonhoeffer, 1915 | 84 |
| 66. | Shell-shock: Jacksonian seizures—decompression | Leriche, 1915 | 86 |
| 67. | Blow on head: hysterical convulsions—cure by neglect | Clarke, 1916 | 87 |
| 68. | Epilepsy with superposed hysteria | Bonhoeffer, 1915 | 88 |
| 69. | Musculocutaneous neuritis: Brown-Séquard’s epilepsy | Mairet, Piéron, 1916 | 89 |
| [xxi]70. | Bullet wound: reactive epilepsy? | Bonhoeffer, 1915 | 92 |
| 71. | Epilepsia tarda | Bonhoeffer, 1915 | 93 |
| 72. | Convulsions by auto-suggestion | Hurst, 1916 | 95 |
| 73. | Epilepsy, emotional | Westphal, Hübner, 1915 | 97 |
| 74. | Hysterical convulsions | Laignel-Lavastine, Fay, 1917 | 98 |
| 75. | Desertion: fugue, probably not epileptic | Barat, 1914 | 100 |
| 76. | Epileptic episode | Bonhoeffer, 1915 | 102 |
| 77. | Narcoleptic seizures | Friedmann, 1915 | 103 |
| 78. | Sham fits | Hurst, 1917 | 106 |
| 79. | Epileptoid attacks controllable by will | Russel, 1917 | 106 |
| 80. | Epileptic taint brought out at last by shell-shock | Hurst, 1917 | 107 |
| 81. | Shell-shock epilepsia larvata | Juquelier, Quellien, 1917 | 108 |
| 82. | To illustrate a theory of Shell-shock as epileptic | Ballard, 1915 | 110 |
| 83. | Same | Ballard, 1917 | 110 |
| 84. | Same | Ballard, 1917 | 111 |
| 85. | Epileptic equivalents | Mott, 1916 | 112 |
| IV. The Substance Abuse Group (Pharmacopsychoses) | |||
| 86. | Pathological intoxication | Boucherot, 1915 | 113 |
| 87. | Same | Loewy, 1915 | 116 |
| 88. | Desertion in alcoholism: fugue | Logre, 1916 | 117 |
| 89. | Alcoholic amnesia experimentally reproduced | Kastan, 1915 | 118 |
| 90. | Desertion and drunkenness | Kastan, 1915 | 119 |
| 91. | Desertion by alcoholic dement | Kastan, 1915 | 121 |
| 92. | Desertion by alcoholic with other factors | Kastan, 1915 | 124 |
| 93. | Alcoholism: disciplinary case | Kastan, 1915 | 126 |
| 94. | Atrocity, alcoholism | Kastan, 1915 | 127 |
| 95. | Atrocity, alcoholic | Kastan, 1915 | 128 |
| 96. | Alcoholism and amnesia: disciplinary case | Kastan, 1915 | 129 |
| 97. | Post-traumatic intolerance of alcohol | Kastan, 1915 | 130 |
| 98. | Adventure with Parisian stranger | Briand, Haury, 1915 | 131 |
| 99. | Morphinism: tetanus | Briand, 1914 | 131 |
| 100. | Morphinism: medicolegal question | Briand, 1914 | 132 |
| 101. | Two morphinists | Briand, 1914 | 132 |
| 102. | |||
| V. The Focal Brain Lesion Team (Encephalopsychoses) | |||
| 103. | Aphasia and left hemiplegia: local and contrecoup lesions | L’Hermitte, 1916 | 133 |
| 104. | Gunshot head wound and alcohol: amnesia | Kastan, 1916 | 135 |
| 105. | Bullet in brain: cortical blindness and hallucinations | Lereboullet, Mouzon, 1917 | 136 |
| 106. | Content of existent psychosis changed by head trauma | Laignel-Lavastine, Courbon, 1917 | 139 |
| [xxii]107. | Meningococcus meningitis; apparent recovery: dementing psychosis | Maixandeau, 1915 | 141 |
| 108. | Meningococcus meningitis | Eschbach and Lacaze, 1915 | 143 |
| 109. | Shell-shock: meningitic syndrome | Pitres and Marchand, 1916 | 145 |
| 110. | Brain abscess in a syphilitic: matutinal loss of knee-jerks | Dumolard, Rebierre, Quellien, 1915 | 147 |
| 111. | Spinal cord lesion: early recovery | Mendelssohn, 1916 | 149 |
| 112. | Shell explosion and meningeal hemorrhage: pneumococcus meningitis | Guillain, Barré, 1917 | 150 |
| 113. | Ante bellum cortex lesion: shrapnel wound determines athetosis | Batten, 1916 | 151 |
| 114. | Hysterical versus thalamic hemianesthesia | Léri, 1916 | 152 |
| 115. | Shell-shock: multiple sclerosis syndrome | Pitres, Marchand, 1916 | 154 |
| 116. | Mine explosion: hysterical and organic symptoms | Smyly, 1917 | 156 |
| 117. | Same | Smyly, 1917 | 156 |
| VI. The Symptomatic Squad (Somatopsychoses) | |||
| 118. | Rabies: neuropsychiatric phenomena | Grenier de Cardenal, Legrand, Benoit, 1917 | 162 |
| 119. | Tetanus, psychotic | Lumière, Astier, 1917 | 164 |
| 120. | Tetanus fruste versus hysteria | Claude, L’Hermitte, 1915 | 165 |
| 121. | British officer’s letter concerning local tetanus | Turrell, 1917 | 166 |
| 122. | Dysentery: psychosis | Loewy, 1915 | 168 |
| 123. | Typhoid fever: hysteria | Sterz, 1914 | 169 |
| 124. | Dementia praecox versus posttyphoid encephalitis | Nordmann, 1916 | 170 |
| 125. | Paratyphoid fever: psychosis outlasting fever | Merklen, 1915 | 171 |
| 126. | Paratyphoid fever: psychopathic taint brought out | Merklen, 1915 | 172 |
| 127. | Diphtheria: post diphtheritic symptoms | Marchand, 1916 | 173 |
| 128. | Diphtheria: hysterical paraparesis | Marchand, 1915 | 174 |
| 129. | Malaria: amnesia | De Brun, 1917 | 175 |
| 130. | Malaria: Korsakow’s syndrome | Carlill, 1917 | 176 |
| 131. | Malaria: ventral horn symptoms | Blin, 1916 | 178 |
| 132. | Trench foot; acroparesthesia | Cottet, 1917 | 180 |
| 133. | Bullet injury of spine; bronchopneumonia: état criblé of spinal cord | Roussy, 1916 | 181 |
| 134. | Shell-shock (shell not seen); sensory and motor symptoms: decubitus; recovery | Heitz, 1915 | 183 |
| 135. | Shell-shock; later typhoid fever: neuritis (ante bellum hysteria) | Roussy, 1915 | 185 |
| 136. | Bullet wound of pleura: hemiplegia and ulnar syndrome | Phocas, Gutmann, 1915 | 186 |
| 137. | Tachypnoea, hysterical | Gaillard, 1915 | 188 |
| 138. | Soldiers’ heart | Parkinson, 1916 | 190 |
| 139. | Soldiers’ heart? | Parkinson, 1916 | 191 |
| 140. | War strain and shell wound: diabetes mellitus | Karplus, 1915 | 192 |
| 141. | Dercum’s disease | Hollande, Marchand, 1917 | 193 |
| [xxiii]142. | Hyperthyroidism | Tombleson, 1917 | 195 |
| 143. | Hyperthyroidism?, neurasthenia | Dejerine, Gascuel, 1914 | 196 |
| 144. | Hyperthyroidism | Rothacker, 1916 | 197 |
| 145. | Graves’ disease, forme fruste | Babonneix, Célos, 1917 | 198 |
| 146. | Shell-shock hysteria: surgical complications | Oppenheim, 1915 | 199 |
| VII. The Young and Old Group (Geriopsychoses)—No cases. | |||
| VIII. The Dementia Praecox Team (Schizophrenoses) | |||
| 147. | Hatred of Prussia: diagnosis, dementia praecox | Bonhoeffer, 1916 | 200 |
| 148. | Dementia praecox: arrest as spy | Kastan, 1915 | 201 |
| 149. | Fugue, catatonic | Boucherot, 1915 | 203 |
| 150. | Desertion: schizophrenic? | Consiglio, 1916 | 204 |
| 151. | Schizophrenia; alcoholism: disciplinary case | Kastan, 1915 | 206 |
| 152. | Schizophrenia aggravated by service | de la Motte, 1915 | 208 |
| 153. | Shot himself in hand: delusions | Rouge, 1915 | 209 |
| 154. | Dementia praecox volunteer | Haury, 1915 | 210 |
| 155. | Hysteria versus catatonia | Bonhoeffer, 1916 | 211 |
| 156. | “Hysteria” actually dementia praecox | Hoven, 1915 | 213 |
| 157. | Hallucinatory and delusional contents influenced by war experiences | Gerver, 1915 | 214 |
| 158. | Iron cross winner, hebephrenic | Bonhoeffer, 1915 | 215 |
| 159. | Occipital trauma; visual hallucinations | Claude, L’Hermitte, 1915 | 217 |
| 160. | Shell-shock: Dementia praecox | Weygandt, 1915 | 219 |
| 161. | Same | Dupuoy, 1915 | 220 |
| 162. | Shell-shock; fatigue; fugue; delusions | Rouge, 1915 | 221 |
| IX. The Bipolar Support Group (Cyclothymoses) | |||
| 163. | A maniacal volunteer | Boucherot, 1915 | 222 |
| 164. | Fugue, melancholic | Logre, 1917 | 223 |
| 165. | Apples in No-man’s-land | Weygandt, 1914 | 224 |
| 166. | Trench life: depression; hallucinations; arteriosclerosis; age, 38 | Gerver, 1915 | 225 |
| 167. | War stress: manic depressive psychosis | Dumesnil, 1915 | 226 |
| 168. | Predisposition; war stress: melancholia | Dumesnil, 1915 | 227 |
| 169. | Depression; low blood pressure; pituitrin | Green, 1916 | 228 |
| X. The Psychoneurotic Club (Psychoneuroses) | |||
| 170. | Three phases in a psychopath | Laignel-Lavastine, Courbon, 1917 | 229 |
| 171. | Fugue, probably hysterical | Milian, 1915 | 232 |
| 172. | Hysterical Adventist | de la Motte, 1915 | 234 |
| 173. | Fugue, psychoneurotic | Logre, —— | 235 |
| 174. | Shell-shy; war bride pregnant: fugue with amnesia and mutism | Myers, 1916 | 236 |
| [xxiv]175. | A neurasthenic volunteer | E. Smith, 1916 | 237 |
| 176. | War stress: neurasthenia in subject without heredity or soil | Jolly, 1916 | 238 |
| 177. | Arterial hypotension in psychasthenia | Crouzon, 1915 | 239 |
| 178. | War stress: psychasthenia | Eder, 1916 | 240 |
| 179. | Ante bellum attacks: neurasthenia | Binswanger, 1915 | 241 |
| 180. | Antityphoid inoculation: neurasthenia | Consiglio, 1917 | 244 |
| 181. | Neurasthenia (one symptom: sympathy with the enemy) | Steiner, 1915 | 245 |
| XI. The Psychopath Group (Psychopathoses) | |||
| 182. | Claustrophobia: shells preferred to tunnel | Steiner, 1915 | 246 |
| 183. | Pathological liar | Henderson, 1917 | 247 |
| 184. | Psychopath almost Bolshevik | Hoven, 1917 | 249 |
| 185. | Hysterical mutism: persistent delusional psychosis | Dumesnil, 1915 | 250 |
| 186. | Psychopathic inferiority brought out by the war | Bennati, 1916 | 251 |
| 187. | Psychopathic episodes | Pellacani, 1917 | 252 |
| 188. | Maniacal and hysterical delinquent | Buscaino, Coppola, 1916 | 253 |
| 189. | Psychopathic delinquent | Buscaino, Coppola, 1916 | 254 |
| 190. | Psychopathic excitement | Buscaino, Coppola, 1916 | 255 |
| 191. | Desertion: dromomania | Consiglio, 1917 | 256 |
| 192. | Suppressed homosexuality | R. P. Smith, 1916 | 257 |
| 193. | Psychopathic: at first suicidal, then self-mutilative | MacCurdy, 1917 | 258 |
| 194. | Bombardment: psychasthenia | Laignel-Lavastine, Courbon, 1917 | 259 |
| 195. | Nosophobia | Colin, Lautier, 1917 | 261 |
| 196. | Psychopath: Attacks of disgust and terror | Lattes, Goria, 1915 | 262 |
| SECTION B. SHELL-SHOCK: NATURE AND CAUSES | |||
| 197. | Shell explosion: Autopsy—hemorrhages; vagoaccessorius chromatolysis | Mott, 1917 | 265 |
| 198. | Mine explosion: Autopsy—hemorrhages | Chavigny, 1916 | 270 |
| 199. | Mine explosion: Autopsy—hemorrhages | Roussy, Boisseau, 1916 | 271 |
| 200. | Shell fragment in back: Autopsy—softenings in spinal cord | Claude, L’Hermitte, 1915 | 272 |
| 201. | Shell explosion: Autopsy—lungs burst! | Sencert, 1915 | 274 |
| 202. | Shell explosion: Hemorrhage in spinal canal and bladder | Ravaut, 1915 | 276 |
| 203. | Shell explosion: Hemorrhage and pleocytosis of spinal fluid | Froment, 1915 | 277 |
| 204. | Shell explosion: Pleocytosis of spinal fluid | Guillain, 1915 | 279 |
| 205. | Shell explosion: Pleocytosis of spinal fluid as late as a month after explosion | Souques, Donnet, 1915 | 280 |
| 206. | Burial: Thecal hemorrhage | Leriche, 1915 | 282 |
| 207. | Shell explosion: Hypertensive spinal fluid | Leriche, 1915 | 283 |
| 208. | Bullet wound: Hematomyelia; partial recovery | Mendelssohn, 1916 | 284 |
| 209. | Shell explosion, subject prone: Hematomyelia | Babinski, 1915 | 286 |
| [xxv]210. | Struck by missile: Hysterical paraplegia? Herpes; segmentary symptoms | Elliot, 1914 | 288 |
| 211. | Mine explosion: Head bruises, labyrinth lesions, canities unilateral | Lebar, 1915 | 291 |
| 212. | Shrapnel wounds: Focal canities; hysterical symptoms | Arinstein, 1915 | 292 |
| 213. | Burial: Organic (?) hemiplegia | Marie, Lévy, 1917 | 293 |
| 214. | Shell explosion; no wound: Organic and functional symptoms | Claude, L’Hermitte, 1915 | 294 |
| 215. | Gassing: Organic symptoms | Neiding, 1917 | 296 |
| 216. | Gassing: Mutism, battle dreams | Wiltshire, 1916 | 297 |
| 217. | Shell explosion: Organic deafness; hysterical speech disorder | Binswanger, 1915 | 298 |
| 218. | Distant shell explosion not seen or heard: Tympanic rupture, cerebellar symptoms | Pitres, Marchand, 1916 | 300 |
| 219. | Mine explosion: Organic and functional symptoms | Smyly, 1917 | 302 |
| 220. | Shrapnel skull wound: Differential recovery from functional symptoms | Binswanger, 1917 | 303 |
| 221. | Shell explosion shrapnel wound: Battle memories, scar hyperesthetic | Bennati, 1916 | 305 |
| 222. | Shrapnel wounds, operation: Hysterical facial spasm | Batten, 1917 | 306 |
| 223. | Shell explosion: Tremors and emotional crises | Myers, 1916 | 307 |
| 224. | Shell explosion, comrades killed: Tremors, crises | Meige, 1916 | 308 |
| 225. | Under fire: Tremophobia: French artist’s description | Meige, 1916 | 310 |
| 226. | Shell explosion: German soldier’s account of Shell-shock symptoms | Gaupp, 1915 | 312 |
| 227. | A British soldier’s account of shell-shock | Batten, 1916 | 315 |
| 228. | Blown up by shell: Crural monoplegia; hysterical four days later | Léri, 1915 | 317 |
| 229. | Shell explosion nearby: Description of treatment to demonstrate hysterical nature of characteristic symptoms | Binswanger, 1915 | 318 |
| 230. | Leg wound: Pseudocoxalgic monoplegia and anesthesia | Roussy, L’Hermitte, 1917 | 323 |
| 231. | Leg contusion: Crural monoplegia, hysterical; later crutch paralysis, organic | Babinski, 1917 | 324 |
| 232. | War strain: Arthritis; crural monoplegia and anesthesia; hysterical “conversion hysteria” | MacCurdy, 1917 | 325 |
| 233. | Lance thrust in back; Crural monoplegia | Binswanger, 1915 | 326 |
| 234. | Shell explosion: After six days, crural monoplegia (“metatraumatic” suggesting persisting hypersensitive phase after shell-shock) | Schuster, 1916 | 329 |
| 235. | Wound of foot: Acrocontracture, seven months’ duration; psycho-electric cure at one sitting | Roussy, L’Hermitte, 1917 | 330 |
| 236. | Shell explosion: Trauma; emotion; hysterical paraplegia | Abrahams, 1915 | 332 |
| 237. | Shell explosion: Burial; paraplegia | Elliot, 1914 | 334 |
| 238. | Shell explosion: Paraplegia and sensory symptoms, organic? | Hurst, 1915 | 335 |
| [xxvi]239. | War strain and rheumatism; no emotional factors: Paraplegia, later brachial tremor | Binswanger, 1915 | 336 |
| 240. | Emotion in fever patient from watching barrage creep up: Paraplegia | Mann, 1915 | 338 |
| 241. | Incentives, domestic and medical, to paraplegia | Russel, 1917 | 338 |
| 242. | Bullet in back: Hysterical bent back; “camptocormia” | Souques, 1915 | 339 |
| 243. | Shell explosion: Camptocormia | Roussy, L’Hermitte, 1917 | 340 |
| 244. | Shell explosion; burial: camptocormia | Roussy, L’Hermitte, 1917 | 342 |
| 245. | Shell explosion; burial; Paraplegia, later camptocormia | Joltrain, 1917 | 344 |
| 246. | Bullet in thigh: Astasia-abasia. Wound of neck: Again astasia-abasia | Roussy, L’Hermitte, 1917 | 346 |
| 247. | Shell explosion: Wound of thorax; astasia-abasia | Roussy, L’Hermitte, 1917 | 346 |
| 248. | War strain and fall in trench without trauma: Dysbasia | Nonne, 1915 | 347 |
| 249. | Shell explosion: Partial burial; hysterical symptoms in parts buried | Arinstein, 1916 | 349 |
| 250. | Wound of hand: Acroparalysis | Roussy, L’Hermitte, 1917 | 350 |
| 251. | Wound of arm: Hysterical paralysis | Chartier, 1915 | 351 |
| 252. | Wound in brachial plexus region: Supinator longus contracture | Léri, Roger, 1915 | 353 |
| 253. | Contusion of muscle with “stupefactive” paralysis of biceps (supinator longus still functioning) | Tinel, 1917 | 355 |
| 254. | Wound of arm: Blockage of impulses to hand movements | Tubby, 1915 | 356 |
| 255. | Shell explosion: Bilateral symmetrical phenomena | Gerver, 1915 | 357 |
| 256. | Shell explosion: Paralytic symptoms on side exposed: Contralateral irritative symptoms | Oppenheim, 1915 | 359 |
| 257. | Shell explosion: Bilateral asymmetrical symptoms | Gerver, 1915 | 360 |
| 258. | Shell explosion: Sensory disorder on side exposed | Gerver, 1915 | 362 |
| 259. | Shell explosion: Hysterical deafness and other symptoms; relapse | Gaupp, 1915 | 363 |
| 260. | Shell explosion: Deafness | Marriage, 1917 | 365 |
| 261. | Mine explosion: Deafmutism; recovery on epistaxis and fever | Liébault, 1916 | 366 |
| 262. | Shell explosion: Deafmutism | Mott, 1916 | 367 |
| 263. | Shell explosion: Deafmutism and convulsions | Myers, 1916 | 368 |
| 264. | Gunfire: Aphonia | Blässig, 1915 | 370 |
| 265. | Shell-shock mutism: (a), observed, (b) dreamed of, (c), developed by victim of shell explosion | Mann, 1915 | 370 |
| 266. | Mortar explosion: Deafness | Lattes, Goria, 1917 | 371 |
| 267. | Shell-explosion: onomatopœic noises | Ballet, 1914 | 371 |
| 268. | Shell explosion: Gravel in eyes; eye and face symptoms | Ginestous, 1916 | 372 |
| 269. | Shell explosion; burial; blow on occiput; Blindness | Greenlees, 1916 | 373 |
| 270. | Shell-shock amblyopia: Composite data | Parsons, 1915 | 374 |
| 271. | Factors in shell-shock amblyopia: Excitement, blinding flashes, fear, disgust, fatigue | Pemberton, 1915 | 375 |
| [xxvii]272. | Shell explosion amblyopia | Myers, 1915 | 376 |
| 273. | Shell windage without explosion: Cranial nerve disorder | Pachantoni, 1917 | 378 |
| 274. | Initial case in Babinski’s series to show chloroform elective exaggeration of reflexes | Babinski, Froment, 1917 | 380 |
| 275. | Wound of ankle: Contracture, chloroform effect | Babinski, Froment, 1917 | 383 |
| 276. | “Reflex” disorder of right leg: Chloroform effect | Babinski, Froment, 1917 | 384 |
| 277. | Bullet in calf: Hysterical lameness cured—reflex disorder associated therewith not cured | Vincent, 1916 | 385 |
| 278. | Trauma of foot: Hysterical dysbasia and reflex disorders; differential disappearance of hysterical symptoms | Vincent, 1917 | 386 |
| 279. | Shell-shock and paraplegia: Vasomotor and secretory disorder twenty months later | Roussy, 1917 | 387 |
| 280. | Tetanus clinically cured: Phenomena reproduced under chloroform anesthesia | Monier-Vinard, 1917 | 388 |
| 281. | Example of a “reflex” disorder after shell explosion at great distance | Ferrand, 1917 | 390 |
| 282. | Shell fire: Shell-shock symptoms delayed | McWalter, 1916 | 391 |
| 283. | Shell-shock symptoms early and late | Smyly, 1917 | 392 |
| 284. | Wounds: Gassing; burial; collapse on home leave | Elliot Smith, 1916 | 393 |
| 285. | Late sympathetic nerve effect after bullet wound of neck | Tubby, 1915 | 394 |
| 286. | Hysterical crural monoplegia after fall from horse under fire (reminiscence of similar ante bellum accident) | Forsyth, 1915 | 395 |
| 287. | Shell explosion, cave-in: Right leg symptoms (ante bellum experiences) | Myers, 1916 | 396 |
| 288. | Shell explosion, wound of back: Paraparesis (subject always weak in legs) | Dejerine, 1915 | 397 |
| 289. | Wound near heart: Fear; paraparesis (subject always weak in legs) | Dejerine, 1915 | 399 |
| 290. | Wounds: Tic on walking and recovery except frontalis tic (emphasis of ante bellum habit) | Westphal, Hübner, 1915 | 401 |
| 291. | Fatigue and emotion: Hysterical hemiplegia (similar hemiplegia ante bellum) | Roussy, L’Hermitte, 1917 | 402 |
| 292. | War strain: Hemiplegia (similar hemiplegia ante bellum, subject’s father hemiplegic) | Duprés, Rist, 1914 | 403 |
| 293. | Shell explosion and burial: Deafmutism (speech difficulty ante bellum) | MacCurdy, 1917 | 405 |
| 294. | War strain: Shell-shock and psychotic symptoms determined to parts ante bellum | Zanger, 1915 | 406 |
| 295. | Mine explosion: Emotion; delirium (previous head trauma without unconsciousness) | Lattes, Goria, 1917 | 407 |
| 296. | Sniper stricken blind in shooting eye | Eder, 1916 | 408 |
| [xxviii]297. | Anticipation of warfare: Fall while mounting sentry; hysterical blindness | Forsyth, 1915 | 408 |
| 298. | Spasmodic neurosis from bareback riding (similar episode ante bellum) | Schuster, 1914 | 409 |
| 299. | Ante bellum spasm of hands | Hewat, 1917 | 409 |
| 300. | Quarrel: Hysterical chorea, reminiscent of former attack and itself reminiscent of organic chorea in subject’s mother | Dupuoy, 1915 | 411 |
| 301. | Hallucinations and delusions of ante bellum origin: Treatment by explanation | Rows, 1916 | 412 |
| 302. | Tremors and convulsive crises in a poor risk | Rogues de Fursac, 1915 | 413 |
| 303. | Emotionality and tachycardia in a martial misfit | Bennati, 1916 | 415 |
| 304. | Hereditary instability | Wolfsohn, 1918 | 416 |
| 305. | Genealogical tree of a shoemaker | Wolfsohn, 1918 | 417 |
| 306. | Traumatic hysteria without hereditary or acquired psychopathic tendency | Donath, 1915 | 418 |
| 307. | Mine explosion, burial: Neurosis in perfectly normal soldier | MacCurdy, 1917 | 419 |
| 308. | Shell explosion: Tremophobia | Meige, 1916 | 421 |
| 309. | Frozen in bog: Glossolabial hemispasm | Binswanger, 1915 | 424 |
| 310. | Bruise by horse: Invincible pain—subject cured by performing heroic feat | Loewy, 1915 | 426 |
| 311. | Kick by horse: Hysterical symptoms including monocular diplopia | Oppenheim, 1915 | 427 |
| 312. | Windage from non-exploding shell: Emotion; homonymous hemianopsia | Steiner, 1915 | 428 |
| 313. | Shell-shock psoriasis | Gaucher, Klein, 1916 | 429 |
| 314. | Croix de guerre and Shell-shock got simultaneously: Hallucinatory bell-ringing reminiscent of civilian work | Laignel-Lavastine, Courbon, 1916 | 430 |
| 315. | Waked by shell explosion: Nystagmiform tremor (occupational reminiscence in cinema worker) and tachycardia | Tinel, 1915 | 432 |
| 316. | Synesthesialgia: Foot pain on rubbing dry hands | Lortat-Jacob, Sézary, 1915 | 433 |
| 317. | Shell-shock and burial: Clonic spasms, later stupor | Gaupp, 1915 | 435 |
| 318. | War stress (liquid fire) and shell-shock: Puerilism | Charon, Halberstadt, 1916 | 437 |
| 319. | Bombed from aeroplane: Battle dreams; dizziness; fugue | Lattes, Goria, 1917 | 439 |
| 320. | Hyperthyroidism after box drops from aeroplane | Bennati, 1916 | 440 |
| 321. | Shell dropped without bursting: Stupor and delirium | Lattes, Goria, 1917 | 441 |
| 322. | Subject carrying explosives is jostled: Unconsciousness, deafmutism, later camptocormia | Lattes, Goria, 1917 | 443 |
| 323. | Grazed by sliding cannon: Stupor and amnesia | Lattes, Goria, 1917 | 444 |
| 324. | Shell explosions nearby: Emotion and insomnia | Wiltshire, 1916 | 445 |
| [xxix]325. | Shell explosion: symptoms after hearing artillery twelve days later | Wiltshire, 1916 | 446 |
| 326. | Exhaustion (heat?): Hyperthyroidism, hemiplegia | Oppenheim, 1915 | 447 |
| 327. | War strain and rheumatism: tremors | Binswanger, 1915 | 448 |
| 328. | Shell explosion; emotion: Fear and dreams | Mott, 1916 | 451 |
| 329. | Under fire; barbed wire work: tremors and sensory symptoms | Myers, 1916 | 452 |
| 330. | Shell explosion: Emotional crises; twice recurrent mutism | Mairet, Piéron, Bouzansky, 1915 | 453 |
| 331. | Shell explosion: Emotional crises (fright at a frog) | Claude, Dide, Lejonne, 1916 | 455 |
| 332. | War strain; wound; burials; shell-shock: neurosis with anxiety and dreams: Relapse | MacCurdy, 1917 | 457 |
| 333. | Bombed by airplane: Suicidal thoughts; oniric delirium; “moving picture in the head” | Hoven, 1917 | 460 |
| 334. | Shell explosion; emotion at death of best friend: Stupor and amnesia | Gaupp, 1915 | 462 |
| 335. | Emotional shock from shooting comrade: Horror, sweat, stammer, nightmare | Rows, 1916 | 463 |
| 336. | Emotion at death of comrade: Phobias | Bennati, 1916 | 464 |
| 337. | Shell explosion: Fright; delayed loss of consciousness | Wiltshire, 1916 | 465 |
| 338. | Shell explosion; burial work: amnesia; unpleasant ideas reflexly conditioned by shell whistling | Wiltshire, 1916 | 467 |
| 339. | Comrade’s death witnessed: Suicidal depression | Steiner, 1915 | 468 |
| 340. | Marching and battles: Neurasthenia? | Bonhoeffer, 1915 | 469 |
| 341. | English schoolmaster’s account of dreams | Mott, 1918 | 470 |
| 342. | War dreams shifting to sex dreams | Rows, 1916 | 472 |
| 343. | Shock at death of comrade: War and peace dreams | Rows, 1916 | 474 |
| 344. | War dreams including hunger and thirst | Mott, 1918 | 475 |
| 345. | Burial work: Olfactory dreams and vomiting | Wiltshire, 1916 | 476 |
| 346. | War dreams: Phobia conditioned on postoniric suggestion | Duprat, 1917 | 477 |
| 347. | Service in rear: War dreams not based on actual experiences | Gerver, 1915 | 478 |
| 348. | Hysterical astasia-abasia: Heterosuggestive “big belly” | Roussy, Boisseau, Cornil, 1917 | 479 |
| 349. | Collapse going over the top: Neurasthenia | Jolly, 1916 | 481 |
| 350. | Battles: Mania and confusion | Gerver, 1915 | 483 |
| 351. | Machine-gun battle: Mania and hallucinations | Gerver, 1915 | 484 |
| 352. | Attacks and counter-attacks: Incoherence and quick development of scenic war hallucinations | Gerver, 1915 | 485 |
| 353. | Hysterical stupor under shell fire after 2 days in the trenches | Gaupp, 1915 | 486 |
| 354. | Monosymptomatic amnesia | Mallet, 1917 | 488 |
| 355. | Aviator shot down: Mental symptoms, organic | MacCurdy, 1917 | 489 |
| 356. | Shell fire and corpse work: Daze with relapse; mutism | Mann, 1915 | 491 |
| [xxx]357. | Mine explosion: Confusion | Wiltshire, 1916 | 492 |
| 358. | Shell explosion: Alternation of personality | Gaupp, 1915 | 493 |
| 359. | “A Horse in the Unconscious” | Eder, 1916 | 497 |
| 360. | Shell explosion, gassing, fatigue: Anesthesia | Myers, 1916 | 498 |
| 361. | Shell explosion and burial: Somnambulism; dissolution of amnesia under hypnosis | Myers, 1915 | 499 |
| 362. | Shell explosion with injuries: Somnambulism | Donath, 1915 | 502 |
| 363. | Shock: Stupor as if dead | Régis, 1915 | 503 |
| 364. | Emotions over battle scenes: Twenty-four days’ somnambulism | Milian, 1915 | 504 |
| 365. | Putative loss of brother in battle: Somnambulism and mutism twenty-seven days | Milian, 1915 | 506 |
| 366. | Shell explosion: Trauma, windage: Somnambulism four days | Milian, 1915 | 508 |
| 367. | Burial, head trauma; gassing: Tremors, convulsions, confusion, fugue | Consiglio, 1916 | 509 |
| 368. | Shell explosion: Hysterical symptoms and tendency to fugue | Binswanger, 1915 | 510 |
| 369. | Burial: Dissociation of personality | Feiling, 1915 | 512 |
| 370. | Ear Complications and hysteria | Buscaino, Coppola, 1916 | 516 |
| SECTION C. SHELL-SHOCK DIAGNOSIS | |||
| 371. | Value of lumbar puncture | Souques, Donnet, 1915 | 524 |
| 372. | Meningeal and intraspinal hemorrhage: Lumbar puncture | Guillain, 1915 | 525 |
| 373. | Burial: Slight hyperalbuminosis | Ravaut, 1915 | 526 |
| 374. | Paraplegia, organic: Lumbar puncture | Joubert, 1915 | 527 |
| 375. | Gunshot of spine: Spinal concussion, quadriplegia, cerebellospasmodic disorder | Claude, L’Hermitte, 1917 | 528 |
| 376. | Trauma of spine: Anesthesia and contracture, homolateral, with trauma | Oppenheim, 1915 | 529 |
| 377. | Mine explosion combining hysterical and lesional effects | Dupouy, 1915 | 530 |
| 378. | Shell explosion: Hysterical and organic symptoms | Hurst, 1917 | 532 |
| 379. | Gunshot: Cauda equina symptoms, combined with functional paraplegia | Oppenheim, 1915 | 533 |
| 380. | Intraspinal lesion: Persistent anesthesia | Buzzard, 1916 | 534 |
| 381. | Functional shell-shock: Erroneous diagnosis | Buzzard, 1916 | 534 |
| 382. | Retention of urine after shell-shock | Guillain, Barré, 1917 | 535 |
| 383. | Same | Guillain, Barré, 1917 | 536 |
| 384. | Incontinence of urine after shell-shock and burial | Guillain, Barré, 1917 | 536 |
| 385. | Struck by missile: Crural monoplegia; plantar reflex absent | Paulian, 1915 | 537 |
| 386. | Shell explosion: Crural monoplegia; sciatica (neuritis?) | Souques, 1915 | 538 |
| 387. | Functional paraplegia and internal popliteal neuritis | Roussy, 1915 | 540 |
| [xxxi]388. | Bullet in hip: Local “stupor” of leg | Sebileau, 1914 | 542 |
| 389. | Localized catalepsy: Hysterotraumatic | Sollier, 1917 | 544 |
| 390. | Contracture: Hysterotraumatic | Sollier, 1917 | 545 |
| 391. | Crural monoplegia, tetanic: Recovery | Routier, 1915 | 546 |
| 392. | Spasms, contracture, crises—tetanic | Mériel, 1916 | 548 |
| 393. | Shell explosion, windage, flaccid paraplegia, not “spinal contusion” | Léri, 1915 | 550 |
| 394. | Scalp wound: Quadriparesis; paraplegia, cataleptic rigidity of anesthetic legs | Clarke, 1916 | 551 |
| 395. | Shell explosion: Spasmodic contractions of sartorii, persistent in sleep | Myers, 1916 | 553 |
| 396. | Shell explosion: Brown-Séquard’s syndrome, hematomyelic? | Ballet, 1915 | 555 |
| 397. | Question of structural injury of spinal cord | Smyly, 1917 | 557 |
| 398. | Dysbasia, psychogenic round an organic nucleus (cerebellar?) | Cassirer, 1916 | 557 |
| 399. | Shell explosion: Dysbasia, in part hysterical, in part organic? | Hurst, 1915 | 558 |
| 400. | Peculiar walking tic | Chavigny, 1917 | 559 |
| 401. | Mine explosion: Camptocormia. Hospital rounder twenty months—cure by electrotherapy, 1 hour | Marie, Meige, Béhagne, Souques, Megevand, 1917 | 561 |
| 402. | Astasia-abasia | Guillain, Barré, 1916 | 563 |
| 403. | Shell wounds: Abdominothoracic contracture, tetanic, four months after injury | Marie, 1916 | 564 |
| 404. | Shoulder dislocation: Hysterical paralysis of arm | Walther, 1914 | 566 |
| 405. | Gunshot: Paralysis of arm increasing in degree | Oppenheim, 1915 | 567 |
| 406. | Wound of wrist: Differential glove anesthesias | Römner, 1915 | 568 |
| 407. | Hysterical contracture combined with edema and vasomotor disorder | Ballet, 1915 | 569 |
| 408. | Hemiparesis with syringomyelic dissociation of sensations: Hematomyelia? | Ravaut, 1915 | 570 |
| 409. | Brachial monoplegia: Tetanic | Routier, 1915 | 571 |
| 410. | Paralysis of right leg: Hysterical? Organic? “Microörganic”? | Von Sarbo, 1915 | 572 |
| 411. | Shell explosion: Burial: Paralysis on third day | Léri, Froment, Mahar, 1915 | 573 |
| 412. | Shell explosion: Hemiplegia. Plantar areflexia | Dejerine, 1915 | 575 |
| 413. | Shell explosion: Tic versus spasm | Meige, 1916 | 577 |
| 414. | Shell explosion: Tremors, anæsthesias | Mott, 1916 | 580 |
| 415. | Hysteria, appendix to trauma | MacCurdy, 1917 | 582 |
| 416. | Peripheral nerve injury: Neurasthenic hyperalgesia | Weygandt, 1915 | 583 |
| 417. | Soldier lead worker: Peripheral neuritis | Shufflebotham, 1915 | 584 |
| 418. | “Peripheral neuritis” cured by faradism | Cargill, 1916 | 585 |
| 419. | Late tetanus | Bouquet, 1916 | 586 |
| [xxxii]420. | Spasmodic neurosis and neurasthenia | Oppenheim, 1915 | 588 |
| 421. | Hysterical and reflex (“physiopathic”) disorders | Babinski, 1916 | 590 |
| 422. | Bullet wound: Paralysis non-“organic,” non-hysterical, i.e. reflex | Babinski, Froment, 1917 | 592 |
| 423. | Asymmetry of reflexes under chloroform | Babinski, Froment, 1917 | 594 |
| 424. | Reflexes under chloroform | Babinski, Froment, 1915 | 595 |
| 425. | Same | Babinski, Froment, 1915 | 596 |
| 426. | Shrapnel wound: Monoplegia, hysterical and organic | Babinski, Froment, 1917 | 597 |
| 427. | Gunshot, later Erb’s palsy: “reflex”? | Oppenheim, 1915 | 598 |
| 428. | Paralysis hysterical? Organic? | Gougerot, Charpentier, 1916 | 600 |
| 429. | Same | Gougerot, Charpentier, 1916 | 602 |
| 430. | Same | Gougerot, Charpentier, 1916 | 604 |
| 431. | Reflex “paralysis” | Delherm, 1916 | 606 |
| 432. | |||
| 433. | Shell explosion: Functional blindness, monosymptomatic | Crouzon, 1915 | 609 |
| 434. | Retrobulbar neuritis (nitrophenol) | Sollier, Jousset, 1917 | 611 |
| 435. | Eye symptoms, hysterical | Westphal, 1915 | 613 |
| 436. | Sandbag on head: Eye symptoms: Lenses | Harwood, 1916 | 615 |
| 437. | Hemianopsia, organic or functional? | Steiner, 1915 | 616 |
| 438. | Hysterical pseudoptosis | Laignel-Lavastine, Ballet, 1916 | 617 |
| 439. | Shell explosion: Rombergism | Beck, 1915 | 620 |
| 440. | Case for otologists and neurologists | Roussy, Boisseau, 1917 | 622 |
| 441. | Jacksonian syndrome: Hysterical | Jeanselme, Huet, 1915 | 625 |
| 442. | Leg tic: Phobia against crabs | Duprat, 1917 | 627 |
| 443. | Convulsions reminiscent of fright | Duprat, 1917 | 628 |
| 444. | Fatigue, delusions, fugue | Mallet, 1917 | 629 |
| 445. | Obsessions and fugue | Mallet, 1917 | 631 |
| 446. | Aprosexia and birdlike movements | Chavigny, 1915 | 632 |
| 447. | Shell explosion: Unconsciousness (45 days): Mutism | Liébault, 1916 | 633 |
| 448. | Shell explosion: Recurrent amnesia | Mairet, Piéron, 1917 | 634 |
| 449. | Shell explosion: Comrade killed: Amnesia | Gaupp, 1915 | 635 |
| 450. | Shell explosion: Recurrent amnesia | Mairet, Piéron, 1915 | 636 |
| 451. | Soldiers’ heart, neurotic and organic | MacCurdy, 1917 | 639 |
| 452. | Soldiers’ heart, neurotic | MacCurdy, 1917 | 640 |
| 453. | Shell explosion: Hysteria: Malingering (?) | Myers, 1916 | 642 |
| 454. | Officer who could not kick | Mills, 1917 | 644 |
| 455. | “Simulation”: Diagnosis incorrect | Voss, 1916 | 645 |
| 456. | Wound: Hysterical edema? | Lebar, 1915 | 646 |
| 457. | Head trauma: simulation? Hysteria? Surgical? | Voss, 1916 | 648 |
| 458. | Disease and disorder to avoid service | Collie, 1916 | 649 |
| 459. | Yes-No test in anesthesia | Mills, 1917 | 651 |
| 460. | Guardhouse test | Roussy, 1915 | 651 |
| 461. | Light in a dark room | Briand, Kalt, 1917 | 652 |
| [xxxiii]462. | Mutism simulated | Sicard, 1915 | 654 |
| 463. | Deafmutism simulated | Myers, 1916 | 655 |
| 464. | Same: Explained by patient | Myers, 1916 | 657 |
| 465. | Deafmutism: Appearance of malingering | Gradenigo, 1917 | 658 |
| 466. | A lame rascal | Gilles, 1917 | 659 |
| 467. | Picric acid jaundice | Briand, Haury, 1916 | 660 |
| 468. | Swelling of hand and arm, 7 months | Léri, Roger, 1915 | 663 |
| 469. | Shell-shy German | Gaupp, 1915 | 664 |
| 470. | Germany sends back a simulator | Marie, 1915 | 664 |
| 471. | Simulation of Quincke’s disease | Lewitus, 1915 | 665 |
| 472. | “Pensionitis” | Collie, 1915 | 666 |
| SECTION D. SHELL-SHOCK TREATMENT AND RESULTS | |||
| 473. | Deafmutism: Spontaneous cure | Mott, 1916 | 672 |
| 474. | Two returns to the front | Gilles, 1916 | 675 |
| 475. | Vicissitudes in 15 months | Purser, 1917 | 676 |
| 476. | Deafmutism: Spontaneous cure | Jones, 1915 | 678 |
| 477. | Course of an oniric delirium | Buscaino, Coppola, 1916 | 679 |
| 478. | Same | Buscaino, Coppola, 1916 | 681 |
| 479. | Paraplegia: Cure by Iron Cross | Nonne, 1915 | 682 |
| 480. | Mutism cured by getting drunk | Proctor, 1915 | 682 |
| 481. | Mutism cured by working in vineyard | Anon, 1916 | 683 |
| 482. | Deafmutism: Spontaneous recovery of speech. Recovery of hearing by isolation | Zanger, 1915 | 684 |
| 483. | Excess of sympathy on furlough | Binswanger, 1915 | 685 |
| 484. | Hysterical seizures treated by hydrotherapy | Hirschfeld, 1915 | 688 |
| 485. | Low blood pressure treated by pituitrin | Green, 1917 | 690 |
| 486. | Manual contracture: Various treatments | Duvernay, 1915 | 691 |
| 487. | Massage and mechanotherapy | Sollier, 1916 | 692 |
| 488. | Mine explosion; headache: Lumbar puncture | Ravaut, 1915 | 693 |
| 489. | Hysterical clenched fist: Treatment by fatigue of flexors | Reeve, 1917 | 694 |
| 490. | Hysterical adduction of arm: Treatment by induced fatigue | Reeve, 1917 | 695 |
| 491. | Hysterical cross-legs: Treatment by induced fatigue | Reeve, 1917 | 696 |
| 492. | Hysterical torticollis: Treatment by induced fatigue | Reeve, 1917 | 697 |
| 493. | Claw foot (2 years): Cure by induced fatigue | Reeve, 1917 | 698 |
| 494. | Traumatic and post-traumatic effects: Surgical treatment | Binswanger, 1917 | 699 |
| 495. | Vomiting: Cure by restoration of self-confidence | McDowell, 1917 | 701 |
| 496. | Self-accusatory delusions: Treatment by “autognosis” | Brown, 1916 | 702 |
| 497. | Deafmutism in three men shell-shocked at one time | Roussy, 1915 | 703 |
| 498. | |||
| 499. | |||
| 500. | Vomiting; incontinence, abasia: Cure by persuasion | McDowell, 1916 | 705-706 |
| 501. | Hysterical convulsions cured by an explanation | Hurst, 1917 | 706 |
| [xxxiv]502. | Course of a case with crises of trembling | Roussy, 1915 | 706 |
| 503. | Two cases of lameness cured by persuasion | Russel, 1917 | 707 |
| 504. | |||
| 505. | Head trauma: Treatments by bandage, isolation, open air and to-and-fro transfers | Binswanger, 1915 | 708 |
| 506. | Rationalization of war memories | Rivers, 1918 | 712 |
| 507. | Same | Rivers, 1918 | 713 |
| 508. | Same | Rivers, 1918 | 714 |
| 509. | Same | Rivers, 1918 | 715 |
| 510. | Same, without redeeming feature as nucleus of rationalization | Rivers, 1918 | 716 |
| 511. | Paraplegia cured by removal of crutches | Veale, 1917 | 717 |
| 512. | Same | Veale, 1917 | 718 |
| 513. | Paraplegia: Chocolates versus isolation | Buzzard, 1916 | 719 |
| 514. | Blindness, mutism, deafness. Immediate spontaneous recovery from the first; gradual recovery from second; deafness cured by “small operation” | Hurst, 1917 | 720 |
| 515. | Deafness: Treatment by stimulating vestibular apparatus | O’Malley, 1916 | 721 |
| 516. | Mutism: Treatment by operative manipulation | Morestin, 1915 | 722 |
| 517. | Visual impairment: Treatment by suggestion, faradism injections | Mills, 1915 | 724 |
| 518. | Aphonia: Treatment by manipulation in larynx | O’Malley, 1916 | 725 |
| 519. | Same | Vlasto, 1917 | 727 |
| 520. | Mutism, amnesia: Treatment by faradism; climatic cure in dream | Smyly, 1917 | 728 |
| 521. | Blindness: Cure by injections in temple | Bruce, 1916 | 729 |
| 522. | Deafness cured by suggestion in writing | Buscaino, 1916 | 730 |
| 523. | Reproduction of Shell-shock story in hypnosis: Recovery | Myers, 1916 | 732 |
| 524. | Same | Myers, 1916 | 733 |
| 525. | Automatism, amnesia, deafmutism: Recovery by hypnosis | Myers, 1916 | 734 |
| 526. | Mutism: Recovery by hypnosis | Hurst, 1917 | 736 |
| 527. | Stammering: Cure by hypnosis | Hurst, 1917 | 737 |
| 528. | Mutism and amnesia: Cure by hypnosis | Myers, 1916 | 739 |
| 529. | Victoria Cross winner: Bayonet clutch contracture revealed by hypnosis | Eder, 1916 | 741 |
| 530. | Contracture: Hypnotic cure “indecently quick” | Nonne, 1915 | 742 |
| 531. | “Doll’s head” anesthesia: Mutism: Cure by hypnosis | Nonne, 1915 | 744 |
| 532. | Mine explosion: Tremors (also ante bellum tremors): Cure by hypnosis | Grünbaum, 1916 | 745 |
| 533. | Astasia-abasia: Cure by hypnosis | Nonne, 1915 | 747 |
| 534. | Crural monoplegia: Cure by hypnosis | Hurst, 1917 | 748 |
| 535. | Tremors and sensory disorders: Cure by hypnosis | Nonne, 1915 | 749 |
| 536. | Paraplegia of gradual development: Cure by repeated hypnosis | Nonne, 1915 | 751 |
| [xxxv]537. | Visual impairment and dysbasia: Cure by hypnosis | Ormond, 1915 | 752 |
| 538. | Blindness cured by hypnosis | Hurst, 1916 | 753 |
| 539. | Postoperative retention of urine: Relief by hypnosis | Podiapolsky, 1917 | 754 |
| 540. | Postoperative pains: Relief by hypnosis | Podiapolsky, 1917 | 755 |
| 541. | Stereotyped war dream and ante bellum headache: Cure by hypnosis | Riggall, 1917 | 756 |
| 542. | Amnesia and ante bellum headache: Cure by hypnosis | Burmiston, 1917 | 757 |
| 543. | Convulsions cured by hypnosis | Hurst, 1917 | 759 |
| 544. | Two attacks of mutism: Spontaneous recovery from one in 18 months, from the other by hypnosis | Eder, 1916 | 759 |
| 545. | Neurasthenic symptoms cured by repeated hypnosis | Tombleson, 1917 | 760 |
| 546. | Neurasthenic symptoms: Improvement under repeated hypnosis | Tombleson, 1917 | 761 |
| 547. | Convulsions “Jacksonian” and dysbasia: Cure by hypnosis | Tombleson, 1917 | 762 |
| 548. | Agoraphobia: Cure by hypnosis | Hurst, 1917 | 763 |
| 549. | Manual tremors: Treatment by forcing and isolation | Binswanger, 1915 | 764 |
| 550. | Mutism: Psychoelectric cure | Scholz, 1915 | 766 |
| 551. | Hemiplegia and deafmutism; (also convulsions by heterosuggestion): Improvement by faradism; full recovery by suggestion | Arinstein, 1915 | 767 |
| 552. | Deafmutism, cures, relapses and eventual cure by anesthesia | Dawson, 1916 | 768 |
| 553. | Deafness: Cure by suggestion on emerging from ether | Bruce, 1916 | 770 |
| 554. | Aphasia, hemiplegia, hemianesthesia, and (by medical suggestion) trismus: Cure by anesthesia and suggestion | Arinstein, 1915 | 771 |
| 555. | Triplegia, mutism, jumping-jack reactions: Cure by anesthesia, verbal suggestion, faradism | Arinstein, 1915 | 773 |
| 556. | Mutism and musical alexia: Cure by anesthesia | Proctor, 1915 | 775 |
| 557. | Deafmutism: Deafness cured by anesthesia | Gradenigo, 1917 | 776 |
| 558. | Interaction of two cases (deafmute and mute) under treatment | Smyly, 1917 | 777 |
| 559. | |||
| 560. | Dysbasia: Cure by stovaine anesthesia | Claude, 1917 | 778 |
| 561. | Same | Claude, 1917 | 779 |
| 562. | Deafmutism | Bellin, Vernet, 1917 | 780 |
| 563. | Monoplegia: Cure by electricity administered with a bored and authoritative look | Adrian, Yealland, 1917 | 782 |
| 564. | Monoplegia after sling: Technique of electrical suggestion and “rapid” reëducation | Adrian, Yealland, 1917 | 783 |
| 565. | Hysterical “sciatica”: Treatment by faradism and verbal suggestion | Harris, 1915 | 785 |
| 566. | Prognosis of intensive reëducation in reflex (physiopathic) disorder | Vincent, 1916 | 786 |
| [xxxvi]567. | Hysterical contracture (with physiopathic features) brutally conquered | Ferrand, 1917 | 788 |
| 568. | Paraparesis: Cure by exercises electrically provoked | Turrell, 1915 | 790 |
| 569. | Astasia-abasia: (“Lourdes-like” cure) | Voss, 1916 | 791 |
| 570. | Abasia: Rapid cure | Schultze, 1916 | 792 |
| 571. | Heterosuggestive brachial paresis: Electric suggestion and recovery in five days | Hewat, 1917 | 794 |
| 572. | Contracture of right index finger and thumb: Psychoelectric cure | Roussy, L’Hermitte, 1917 | 795 |
| 573. | Brachial monoplegic able to descend ladder with arms only | Claude, 1916 | 795 |
| 574. | Brachial monoparesis: Vicissitudes of treatment | Vincent, 1917 | 796 |
| 575. | Paresis and sensory disorder: Reëducation | Binswanger, 1915 | 798 |
| 576. | Seizures (of ante bellum origin), astasia-abasia, anesthesias: Reëducation | Binswanger, 1915 | 800 |
| 577. | Progress in case of paresis of foot and spasticity of hip | Binswanger, 1915 | 805 |
| 578. | Mutism (Reëducation) | Briand, Philippe, 1916 | 808 |
| 579. | Stammering: Isolation and reëducation | Binswanger, 1915 | 810 |
| 580. | Deafmutism: Phonetic reëducation | Liébault, 1916 | 814 |
| 581. | Aphonia: Pressure on sternum and respiratory gymnastics | Garel, 1916 | 816 |
| 582. | Stammering: Reëducation | MacMahon, 1917 | 817 |
| 583. | Speech disorder: Reëducation | MacMahon, 1917 | 818 |
| 584. | Camptocormia: Psycho-electric cure: lameness cured by reëducation | Roussy, L’Hermitte, 1917 | 819 |
| 585. | Deafmutism: Speech recovery by suggestion and reëducation: Hearing by reëducation | Liébault, 1916 | 822 |
| 586. | Mutism; stammering; Reëducation; hypnosis | MacCurdy, 1917 | 823 |
| 587. | Anesthesias: Spontaneous gradual recovery: “Paralysis” cured by reëducation | Binswanger, 1915 | 824 |
| 588. | Deafmutism; head movements, anesthesia: Cure by faradism, massage and reëducation | Arinstein, 1916 | 827 |
| 589. | Amnesia and paralysis: Reëducation | Batten, 1916 | 828 |
| SECTION E. EPICRISIS | |||
| PARAGRAPH | |||
| Terminology | 1-8 | ||
| Diagnostic Boundaries Issue | 9-39 | ||
| The Nature of Combat PTSD | 40-74 | ||
| Diagnosis Differentiation Issue | 75-99 | ||
| General Nature of PTSD | 89-102 | ||
| Treatment: General Notes | 103-114 | ||
A. PSYCHOSES INCIDENTAL IN THE WAR
The data from all the belligerent countries, collected in this book, go far to prove that, whatever at last you elect to term Shell-shock, you must pause to consider whether your putative case is not actually:
The data from all the warring countries, gathered in this book, strongly suggests that, no matter what you ultimately decide to call Shell-shock, you need to take a moment to think about whether your supposed case is actually:
A matter of spirochetes?
A spirochete issue?
The response of a subnormal soldier?
The response of an underperforming soldier?
An equivalent of epilepsy?
A type of epilepsy?
An alcoholic situation?
A drinking problem?
A result of neurones actually hors de combat?
A result of neurons actually out of action?
A state of bodily weakness (perhaps of faiblesse irritable)?
A state of physical weakness (maybe of irritable weakness)?
A bit of dementia praecox?
A touch of schizophrenia?
One of the ups and downs of the emotional (affective, cyclothymic) psychoses?
One of the highs and lows of emotional (affective, cyclothymic) psychoses?
An odd psychopathic reaction in which the response is abnormal not so much by reason of excessive stimulus as by reason of defective power of response?
An unusual psychopathic reaction where the response is strange not so much due to excessive stimulation but rather because of a weak ability to respond?
On a simpler basis, is not our Shell-shocker just a banal example of hysteria, neurasthenia, psychasthenia; and is not this psychoneurotic more peculiar in his capacity to be shocked than are the conditions that purvey the shocks?
On a simpler level, isn’t our Shell-shocker just a dull example of hysteria, neurasthenia, and psychasthenia? And isn’t this psychoneurotic person more unusual in their ability to be shocked than the situations that cause the shocks?
Put more concretely in the terms of available tests and criteria, open to the psychiatrist, does not every putative Shell-shock soldier deserve at some stage a blood test for syphilis? Should we not be reasonably sure we are not facing a man inadequate to start with, so far as mental tests avail? Should we not verify (even at considerable expense of time and money by so-called “social service” methods) the facts of epilepsy and epileptic taint? Of alcoholism? And so on? There can be no two answers to these questions.
Put more concretely in terms of available tests and criteria, which the psychiatrist can access, doesn’t every suspected Shell-shock soldier deserve a blood test for syphilis at some point? Shouldn’t we be reasonably sure that we’re not dealing with someone who has pre-existing issues, based on the mental tests available? Shouldn’t we confirm (even at significant time and cost through so-called “social service” methods) the facts about epilepsy and any related conditions? What about alcoholism? And so on? There can’t be any doubt about the answers to these questions.
Upon the following page is a practical grouping of mental diseases, devised in the first place, not for war psychoses, but for the initial sifting of psychopathic hospital cases. Now[2] the psychopathic hospital group of cases constitutes in peace practice the closest analogue of the mental cases met in active military practice, because the “incipient, acute, and curable”[1] cases, for which psychopathic hospitals are built and which flock to or are sent to the wards and outdoor departments of such hospitals, are precisely the cases that early come forward in active military practice. They are precisely the cases in which that pathological event—whatever it is—we know as Shell-shock may be expected to develop. It is precisely the “incipient, acute, and curable” instances of mental disease which we hope to exclude from our American army by cis-Atlantic winnowing-out at the hands of neuropsychiatric experts—the best preventive we hope both of Shell-shock and of other worse mental conditions, if such there be. Military mental practice plainly deals, not so much with frank and committable insanity, as with mental diseases of a medically milder but a militarily far more insidious nature.
On the next page is a practical classification of mental illnesses, created primarily not for wartime psychological issues but for the initial evaluation of psychiatric hospital cases. Now[2] the group of cases in psychiatric hospitals closely resembles the mental cases encountered in active military situations during peacetime, because the “incipient, acute, and curable”[1] cases that psychiatric hospitals are designed for—and that are either drawn to or sent to the wards and outdoor departments of these hospitals—are exactly the types of cases that emerge early in active military practice. They are precisely the cases in which that pathological phenomenon—whatever it is—we recognize as Shell-shock may be expected to arise. It is specifically the “incipient, acute, and curable” instances of mental illness that we aim to filter out of our American army through transatlantic assessments by neuropsychiatric experts—the best prevention we hope for both Shell-shock and potentially worse mental conditions, if they exist. Military mental health practice clearly focuses not just on overt and severe insanity, but on mental illnesses that are medically less severe yet militarily much more insidious.
A further inspection of this grouping of mental diseases shows not only that it contains many conditions not usually termed “insanity” (such as, e.g., feeblemindedness, epilepsy, alcoholism, sundry somatic diseases, psychoneuroses), but that these conditions are presented for practical purposes in a certain seemingly arbitrary order. Without attempting to justify this selection of scope (not too wide for modern psychiatry, most would readily acknowledge), I shall draw out a little further what I consider to be the virtues of the order selected. In the first place, all will concede, some order of consideration of collected data is a prime necessity to the tyro. Without an order of consideration the diagnostic tyro is but too apt to find in the best textbooks of psychiatry (even more easily the better the textbook) all he needs to prove that the case in hand is—almost anything he selects to make his case conform to! And how much more dangerous this debating-society method of diagnosis (by choice of a side and matching a textbook type) may become in the fluid and elastic conditions of psychopathic hospital practice, can readily be observed by one who contemplates the formes frustes and entity-sketches that the “incipient, acute, and curable” group of cases presents.
A closer look at this group of mental illnesses shows that it includes many conditions not usually called “insanity” (like, for example, intellectual disability, epilepsy, alcoholism, various physical illnesses, and psychoneuroses). It also presents these conditions in what seems to be a somewhat random order for practical reasons. Without trying to justify this selection of scope (most people would agree that it's not too broad for modern psychiatry), I want to highlight what I think are the benefits of the chosen order. First, everyone will agree that some level of organization when considering collected data is essential for beginners. Without this organization, diagnostic novices are too likely to find in the best psychiatry textbooks (more so with better textbooks) everything they need to argue that a particular case is—almost anything they want it to be! And how much more harmful this method of diagnosing through choice and matching textbook examples can be in the flexible and variable environment of psychopathic hospital practice can be easily noted by anyone who looks at the incomplete forms and entity sketches presented by the “incipient, acute, and curable” group of cases.
Chart 1
PRACTICAL GROUPING OF MENTAL DISEASES
The order adopted for these groups (which roughly correspond to botanical or zoological orders) is a pragmatic order for successive exclusion on the basis of available tests, criteria, or information: the actual diagnosis is a product of still further differentiation within the several groups.
The arrangement of these groups (which roughly align with botanical or zoological orders) is a practical method for progressively ruling out options based on the tests, criteria, or information available: the actual diagnosis results from additional differentiation within the various groups.
The case-histories of this book will show that
The case studies in this book will show that
(a) most shell-shock is in group X, Psychoneuroses,
(a) most shell-shock is in group X, Psychoneuroses,
(b) the diagnostic delimitation problem is chiefly against I. Syphilopsychoses, III. Epileptoses, VI. Somatopsychoses,
(b) the diagnostic boundary issue primarily involves I. Syphilopsychoses, III. Epileptoses, VI. Somatopsychoses,
(c) the finer differentiation problem is between X. Psychoneuroses and V. Encephalopsychoses. (See Epicrisis, propositions 9-12, 40-43, 72-73.)
(c) the finer differentiation problem is between X. Psychoneuroses and V. Encephalopsychoses. (See Epicrisis, propositions 9-12, 40-43, 72-73.)
| I. | Syphilitic Psychoses | SYPHILOPSYCHOSES |
| II. | Feeblemindedness | HYPOPHRENOSES |
| III. | Epilepsy | EPILEPTOSES |
| IV. | Alcoholic, Drug, and Poison Psychoses | PHARMACOPSYCHOSES |
| V. | Focal Brain Lesion Psychoses | ENCEPHALOPSYCHOSES |
| VI. | Symptomatic (Somatic) Psychoses | SOMATOPSYCHOSES |
| VII. | Presenile-Senile Psychoses | GERIOPSYCHOSES |
| VIII. | Dementia Praecox and Allied Psychoses | SCHIZOPHRENOSES |
| IX. | Manic-Depressive and Allied Psychoses | CYCLOTHYMOSES |
| X. | Psychoneuroses | PSYCHONEUROSES |
| XI. | Other Forms of Psychopathia | PSYCHOPATHOSES |
No conclusions are intended to be drawn in these introductory pages. Such conclusions as are risked are placed in the Epicrisis (see Section E). But so much can be said: If we are ever to surround the problem of Shell-shock (intra bellum or post bellum), we must approach it with no artificial and à priori limitations of its scope. We must not even agree beforehand that Shell-shock is nothing but psychoneurosis: that would be a deductive decision unworthy of modern science. In the collection of these cases, I have tried to place the topic upon the broadest clinical base. Samples of virtually every sort of mental disease and of several sorts of nervous disease have been laid down, some obviously not instances of Shell-shock, some mixed with clinical phenomena of Shell-shock, others hard to tell offhand from Shell-shock—the whole on the basis that we shall earliest learn what Shell-shock, the pathological event, is by studying what it is not. As the sequel may show, we are perhaps not entitled to regard Shell-shock, the pathological event, as always associated with shell-shock, the physical event. We shall, therefore, find in Section A (see tables on pages 6 and 7).
No conclusions are meant to be drawn in these introductory pages. Any conclusions that are suggested are included in the Epicrisis (see Section E). But here’s what we can say: If we’re ever going to tackle the issue of Shell-shock (whether during or after the war), we need to address it without any artificial or preconceived limits on its scope. We shouldn't even agree in advance that Shell-shock is just psychoneurosis; that would be a deductive conclusion unworthy of modern science. In gathering these cases, I’ve tried to base the topic on the widest clinical foundation. Samples of nearly every type of mental illness and several types of nervous disorders have been included, some clearly not examples of Shell-shock, some mixed with clinical signs of Shell-shock, and others that are difficult to distinguish from Shell-shock at first glance— all with the idea that we’ll better understand what Shell-shock, the pathological event, is by examining what it is not. As we’ll see later, we may not be justified in linking Shell-shock, the pathological event, to shell-shock, the physical event. Therefore, we’ll find information in Section A (see tables on pages 6 and 7).
(1) Cases without either physical shell-shock, or pathological Shell-shock—psychoses of various kinds incidental in the war (--+).
(1) Cases without physical shell shock or pathological shell shock—various types of psychoses that occur during the war (--+).
(2) Cases with physical shell-shock but without pathological Shell-shock—psychoses of various kinds seemingly liberated by, aggravated by, or accelerated by the physical factor of shell-shock (+-+).
(2) Cases with physical shell shock but without any mental disorders. Shell shock—various types of psychological conditions that appear to be triggered, worsened, or sped up by the physical impact of shell shock (+-+).
(3) Cases without physical shell-shock but with both symptoms of pathological Shell-shock as well as of other psychosis (-++).
(3) Cases without physical shell shock but with both symptoms of pathological shell shock and other psychosis (-++).
(4) Cases with physical shell-shock, with clinical phenomena of Shell-shock, as well as of other psychosis (+++).
(4) Cases with physical shell shock, showing clinical symptoms of shell shock, as well as other psychosis (+++).
(5) Cases without physical shell-shock but with symptoms of pathological Shell-shock (-+-).
(5) Cases without physical shell shock but with symptoms of psychological shell shock (-+-).
(6) Cases with physical shell-shock and pathological Shell-shock (++-).
(6) Cases with physical shell shock and pathological shell shock (++-).
The data of Section A will solidly prove that Shell-shock, however picturesque the term for laymen or in the argot of the clinic, is medically most intriguing. As we cannot get rid of the term (even by suppressing it in parentheses or by condemning it to the limbo of the so-called), we must make the best of it by calling Shell-shock just the ore in the clinical mine. To say the least, the term is harmless: it merely stimulates the lay hearer to questions. These questions he must ask of the expert. But every time that the expert suavely states that Shell-shock is nothing but psychoneurosis, that expert runs the risk of hurting some patient who may or not have a psychoneurosis but has been called psychoneurotic. All the while, of course, the suave expert is perfectly right—statistically. In fine, the man you have called a victim of Shell-shock is probably a victim of psychoneurosis, but only probably!
The data from Section A will convincingly show that Shell-shock, no matter how appealing the term might sound to the average person or in the jargon of the clinic, is actually quite medically fascinating. Since we can’t get rid of the term (even by burying it in parentheses or dismissing it as a so-called), we should accept it, treating Shell-shock as just the ore in the clinical mine. At the very least, the term is harmless: it simply encourages the layperson to ask questions. These questions need to be directed to the expert. However, whenever the expert calmly claims that Shell-shock is merely psychoneurosis, there’s a risk of upsetting someone who might or might not have psychoneurosis but has been labeled as such. Meanwhile, the confident expert is absolutely correct—statistically. Ultimately, the person you’ve called a victim of Shell-shock is probably a victim of psychoneurosis, but only probably!
Section A shows how he may—not probably, but possibly—be a victim of say ten other things. But it is not that he has an even chance of being one of these ten other things. As the reader watches the procession of cases in Section A, he will perceive that, amongst the ten major groups there studied, some have far greater diagnostic likelihood than others. Thus, syphilis, epilepsy, and somatic diseases will in the sequel prove more dangerous to our success as diagnosticians than, e. g., feeblemindedness or even perhaps alcoholism. But now let us look at these cases systematically, just as if we dealt with so many cases of Railway-spine or any other “incipient, acute, and curable” cases.
Section A shows how he might—not likely, but potentially—be a victim of, say, ten other conditions. However, it's not that he has an equal chance of being one of these ten conditions. As the reader goes through the cases in Section A, they'll notice that, among the ten major groups studied, some have a significantly higher likelihood of diagnosis than others. For example, syphilis, epilepsy, and somatic diseases will ultimately pose more challenges to our success as diagnosticians than, say, mental deficiency or possibly even alcoholism. Now, let’s examine these cases systematically, just as if we were looking at various cases of Railway spine or any other “incipient, acute, and curable” conditions.
Chart 2
PSYCHOPATHIA MARTIALIS
| ⎧‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾⎫ | |||
|---|---|---|---|
| ⎧‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾⎫ | |||
| SHELL-SHOCK (The Physical Factor) |
SHELL-SHOCK (ANXIETY SYMPTOMS) |
PSYCHOSIS (SYMPTOMS NOT RELATED TO NEUROSIS) |
|
| Missing | Missing | INCIDENTAL | |
| Present | Missing | LIBERATED, AGGRAVATED, ACCELERATED PSYCHOSES | |
| Missing | COMBINED NEUROSES AND PSYCHOSES [2](Formula -++) |
||
| Present | COMBINED NEUROSES AND PSYCHOSES (Formula +++) |
||
| Missing | NEUROSES (Shell shock) |
Missing | |
| Present | NEUROSES (Real Shell Shock) |
Unavailable | |
Chart 3
PSYCHOPATHIA MARTIALIS
FORMULAS
| Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ⎧‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾⎫ | |||
|---|---|---|---|
| ⎧‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾‾⎫ | |||
| S, N, P[3] = | SHELL-SHOCK (THE PHYSICAL__A_TAG_PLACEHOLDER_0__ FACTOR) IS HERE |
SHELL-SHOCK (NEUROTIC SYMPTOMS) PRESENT |
PSYCHOSIS (NON-NEUROTIC SYMPTOMS) IN EFFECT |
| P = | - | - | + |
| SP = | + | - | + |
| NP = | - | + | + |
| SNP = | + | + | + |
| N = | - | + | - |
| SN = | + | + | - |
[4] These plus-or-minus formulae are not intended to imply that the physical factor, where present (+), must have worked a physical effect upon the nervous system: the effects of the physical factor might be wholly emotional or otherwise psychic.
[4] These plus-or-minus formulas aren't meant to suggest that the physical factor, when present (+), necessarily impacted the nervous system physically: the effects of the physical factor could be entirely emotional or otherwise psychological.
I. SYPHILOPSYCHOSES (SYPHILITIC GROUP)
An officer of high rank deserts his command in a crisis: alienists’ report.
An officer of high rank abandons his post during a crisis: mental health professionals' report.
Case 1. (Briand, February, 1915.)
M. X. was an officer ranking high in the French army, having military duties of a critical nature and of great importance (social reasons forbid Briand’s giving informatory details). Suffice it to say that he was brought before court-martial for abandoning his post at the very moment when his presence was most urgently required. He turned tail, without taking the most elementary military precautions.
M. X. was a high-ranking officer in the French army, responsible for critical and important military duties (social reasons prevent Briand from providing specific details). It's enough to say that he was brought before a court-martial for leaving his post at the exact moment when his presence was needed most. He fled without taking even the most basic military precautions.
M. X. was passed up to alienists. He was not a case of Shell-shock unless of the anticipatory sort. He was somatically run-down and of lowered morale and now 65 years of age. The campaign had been fatiguing.
M. X. was referred to specialists. He didn’t have Shell-shock, unless it was the kind that comes from worrying about it. He was physically exhausted and had a low spirit, now at the age of 65. The campaign had taken a toll on him.
The alienists decided that the officer had not been responsible for his non-military acts. He had been, they found, in a state of mental confusion at the time of desertion, such that amnesia for his duties and heedlessness of consequences had allowed him to leave the front without looking behind him or securing substitution. This state of mental confusion had been preceded by overwork and several nights of insomnia.
The psychiatrists concluded that the officer wasn't accountable for his non-military actions. They determined he had been in a state of mental confusion at the time of his desertion, which caused him to forget his duties and be careless about the consequences, allowing him to leave the front without looking back or arranging for a replacement. This mental confusion had been brought on by excessive work and several nights of sleeplessness.
Moreover he was palpably arteriosclerotic. Blood pressure was high. The history was one of slight shocks and a mild hemiplegia. The confusion at the front was only the most recent of a series of transitory attacks of confusion. At the time of examination this high officer was actually in a state of mild dementia.
Moreover, he clearly had arteriosclerosis. His blood pressure was high. His medical history included minor strokes and mild paralysis on one side. The confusion he was experiencing was just the latest in a series of temporary bouts of confusion. At the time of the examination, this high-ranking officer was actually in a state of mild dementia.
M. X. was an old colonial man, malarial, and had been a victim of syphilis.
M. X. was an elderly colonial man, had malaria, and was a victim of syphilis.
A naval officer sees hundreds of submarines: General paresis.
A naval officer sees hundreds of submarines: General paresis.
Case 2. (Carlill, Fildes, and Baker, July, 1917.)
A naval officer, 36, during August, 1916, asserted that he could see hundreds of submarines. At one time he imagined that he was receiving trunk calls in the middle of the ocean. He was admitted to Haslar, and the Wassermann reaction of the serum was found strongly positive. The spinal fluid was not at this time examined. The officer recovered to some extent, was given no special treatment, and was sent on leave.
A naval officer, 36, claimed in August 1916 that he could see hundreds of submarines. At one point, he thought he was getting trunk calls in the middle of the ocean. He was admitted to Haslar, where the Wassermann reaction of his serum tested strongly positive. The spinal fluid wasn’t examined at that time. The officer recovered to some extent, wasn’t given any special treatment, and was sent on leave.
He came under observation again in October, 1916, having become very strange in his manner, on one occasion passing water into the coal box, and talked about impending electrocution. His ankle-jerks were found sluggish and there was a patch of blunting to pin pricks. The diagnosis of general paresis was made. The spinal fluid was afterward examined and found to be negative to the Wassermann reaction but contained 15 lymphocytes per cubic mm.
He was observed again in October 1916, having become quite odd in his behavior, even urinating in the coal box once, and he spoke about an upcoming execution by electric chair. His ankle reflexes were slow, and there was a patch of reduced sensitivity to pin pricks. They diagnosed him with general paresis. Later, his spinal fluid was examined and tested negative for the Wassermann reaction but had 15 lymphocytes per cubic mm.
Three full doses of Kharsivan freed him from delusions and left him apparently absolutely sane. It was recommended that he should be kept at Haslar to continue treatment. However, he had been certified insane and was therefore sent to Yarmouth, from which he was discharged in February, 1917, having been in good mental health throughout his stay there.
Three full doses of Kharsivan cleared his delusions and left him looking completely sane. It was suggested that he should stay at Haslar for further treatment. However, since he had been declared insane, he was sent to Yarmouth, where he was released in February 1917, having maintained good mental health throughout his time there.
Re syphilis and general paresis of military officers, as in Cases 1 and 2, Russo-Japanese experience was already at hand. Autokratow saw paretic Russian officers sent to the front in early but still obvious phases of disease. These paretics and various arteriosclerotics, Autokratow saw back in Russia in the course of a few months.
Re syphilis and general paresis of military officers, as in Cases 1 and 2, the Russo-Japanese experience was already available. Autokratow observed paretic Russian officers being sent to the front in the early but still recognizable stages of the disease. He saw these paretics and various arteriosclerotic individuals again in Russia over the course of a few months.
Re naval cases, see also Case 5 (Beaton). Beaton thinks that monotonous ship duty, alternating with critical stress of service, bears on morale and liberates mental disorder.
Re naval cases, see also Case 5 (Beaton). Beaton believes that the repetitive nature of ship duty, coupled with the intense pressure of service, affects morale and contributes to mental health issues.
Neurosyphilis may be aggravated or accelerated under war conditions.
Neurosyphilis can be worsened or speeded up during wartime.
Case 3. (Weygandt, May, 1915.)
A German, long alcoholic and thought to be weakminded, volunteered, but shortly had to be released from service. He began to be forgetful and obstinate, cried, and even appeared to be subject to hallucinations. The pupils were unequal and sluggish. The uvula hung to the right. The left knee-jerk was lively, right weak. Fine tremors of hands. Hypalgesia of backs of hands. Stumbling speech. Attention poor.
A German man, who had struggled with alcoholism for a long time and was seen as weak-minded, volunteered but had to be let go from service shortly after. He started becoming forgetful and stubborn, cried, and even seemed to experience hallucinations. His pupils were unequal and sluggish. His uvula was tilted to the right. The knee-jerk reflex on the left was active, while on the right it was weak. He had fine tremors in his hands, reduced sensitivity on the backs of his hands, slurred speech, and poor attention.
It appeared that he had been infected with syphilis in 1881 and in 1903 had had an ulcer of the left leg.
It seemed that he had contracted syphilis in 1881 and in 1903 had an ulcer on his left leg.
The military commission denied that his service had brought about the disease.
The military commission rejected the idea that his service had caused the disease.
Case 4. (Hurst, April, 1917.)
An English colonel thought himself perfectly fit when he went out with the original Expeditionary Force. He had had leg pains, regarded as due to rheumatism or neuritis. He was invalided home after exhaustion on the great retreat. He was now found to be suffering from a severe tabes. He improved greatly under rest and antisyphilitic treatment. He has now returned to duty.
An English colonel believed he was in great shape when he joined the original Expeditionary Force. He had experienced leg pain, which was thought to be caused by rheumatism or neuritis. He was sent home after becoming exhausted during the major retreat. Now, he was found to be suffering from severe tabes. He improved significantly with rest and antisyphilitic treatment. He has since returned to duty.
Case 5. (Beaton, May, 1915.)
An apparently healthy man, serving on an English battle-ship, severed a tendon in a finger. The injury was regarded as minor. The tendon was sutured and the wound healed. During the man’s convalescence he was accidentally discovered to have an Argyll-Robertson pupil and some excess reflexes. Neurosyphilis had probably antedated the accident. But from the moment of this trivial injury, the disease advanced rapidly.
A seemingly healthy man serving on an English battleship accidentally cut a tendon in his finger. The injury was considered minor. The tendon was stitched up, and the wound healed. During his recovery, it was unexpectedly found that he had an Argyll-Robertson pupil and some heightened reflexes. Neurosyphilis likely existed before the accident. However, from the time of this minor injury, the disease progressed quickly.
Overwork in service; several months exacting work well performed: General paresis.
Overwork in service; several months of demanding work well done: General paresis.
Case 6. (Boucherot, 1915.)
A lieutenant of Territorials, aged 41 (heredity good, anal fistula at 30, with ulceration of penis of an unknown nature at the same period). In 1907 when off service and married, his wife gave birth to a child; no miscarriages. Had been a good soldier in service before the war. The lieutenant was called to the colors August 2, 1914, and was detached for special duty, for the performance of which he was much praised by the commanding officers. The work, however, was too much for him and on April 1 he had to be evacuated to the hospital with a ticket saying “Nervous depression following overwork in service.” On April 14 he seemed well enough for a convalescent camp, but, apparently through red tape, was sent to a hospital at Orléans. On June 23 he had to be evacuated to the Fleury annex. His eyes were dull and features flaccid; his whole manner suggested fatigue. His pupils were myotic, tongue tremulous, speech slow and stumbling. Knee-jerks were exaggerated and gait difficult, the right leg dragging. Headaches. He could not perform the slightest intellectual work and was the victim of retrograde and anterograde amnesia. He was aware of the decline of his mental power and was fain to struggle against it, becoming restless and sad. The gaps in his memory grew deeper, he became more and more impulsive, even violent, and had spells of excitement. Dizziness and palpitation developed. Sometimes there were auditory and visual hallucinations of such intense character that he tried feebly to commit suicide with a penknife. He fell into semicoma, and then had a number of apoplectiform attacks. W. R. +
A 41-year-old Territorial lieutenant (good family background, had an anal fistula at 30, with an unexplained penile ulcer at that time). In 1907, while off duty and married, his wife gave birth to a child; no miscarriages. He had been a good soldier before the war. The lieutenant was called up on August 2, 1914, and was assigned special duties, which earned him a lot of praise from his commanding officers. However, the work was too demanding, and on April 1, he had to be evacuated to the hospital with a note that said “Nervous depression due to overwork in service.” By April 14, he seemed healthy enough for a convalescent camp but, apparently due to bureaucratic delays, was sent to a hospital in Orléans instead. On June 23, he had to be moved to the Fleury annex. His eyes looked dull, and his features were slack; his whole demeanor suggested exhaustion. His pupils were constricted, his tongue trembled, and his speech was slow and halting. He had exaggerated knee-jerk reflexes and had difficulty walking, with his right leg dragging. He experienced headaches and could not manage even the slightest intellectual task, suffering from retrograde and anterograde amnesia. He was aware of his declining mental ability and tried hard to fight against it, becoming restless and sad. The gaps in his memory deepened, and he became increasingly impulsive, even violent, experiencing fits of excitement. He developed dizziness and palpitations. At times, he had auditory and visual hallucinations so intense that he weakly attempted to take his own life with a penknife. He lapsed into semi-coma and then suffered several apoplexy-like attacks. W. R. +
Apparently the moral and physical situation of the lieutenant was absolutely normal when the campaign began and, as he fulfilled detail duties with absolute correctness for a number of months, Boucherot argues that here is an instance of general paresis declanché by overwork.
Apparently, the lieutenant's moral and physical condition was completely normal when the campaign started, and since he carried out his duties with total accuracy for several months, Boucherot suggests that this is a case of general paresis declanché by overwork.
Syphilis contracted before enlistment. Neurosyphilis aggravated by service.
Syphilis caught before joining the military. Neurosyphilis worsened by deployment.
Case 7. (Todd, personal communication, 1917.)
A laboring man, 42, who always strenuously denied syphilitic infection, proceeded to France eight months after enlistment. He had not been in France three weeks when he dropped unconscious. He regained consciousness, but remained stupid, dull in expression, and with memory impaired. His speech was also impaired. There was dizziness and a right-sided hemiplegia.
A 42-year-old worker, who firmly denied having syphilis, went to France eight months after joining the military. He had only been in France for three weeks when he collapsed. He came to but stayed dazed, had a blank expression, and his memory was affected. His speech was also off. He experienced dizziness and had weakness on the right side of his body.
He was confined to bed four months and was then “boarded” for discharge.
He was stuck in bed for four months and was then "released" for discharge.
Physically, his heart was slightly enlarged both right and left; sounds irregular; extra systoles; aortic systolic murmur transmitted to neck; blood pressure 140:40. Precordial pain, dyspnoea.
Physically, his heart was slightly enlarged on both the right and left sides; the sounds were irregular; there were extra heartbeats; an aortic systolic murmur was heard and transmitted to the neck; blood pressure was 140 over 40. He experienced chest pain and shortness of breath.
Neurologically, there was a partial spastic paralysis of the right thigh which could be abducted, could be flexed to 120°, and showed some power in the quadriceps. There was also a spastic paralysis of the right arm, but the shoulder girdle movements were not impaired. There was a slight weakness on the right side of the face. There was no anesthesia anywhere.
Neurologically, there was a partial spastic paralysis of the right thigh which could be abducted, could be flexed to 120°, and showed some strength in the quadriceps. There was also spastic paralysis of the right arm, but the shoulder girdle movements were not affected. There was slight weakness on the right side of the face. There was no loss of sensation anywhere.
The deep reflexes were increased on the right side, Babinski on right, flexor contractures of right hand, extensor contractures of right leg, abdominal and epigastric reflexes absent, pupils active, tongue protruded in straight line.
The deep reflexes were heightened on the right side, Babinski sign present on the right, flexor contractures in the right hand, extensor contractures in the right leg, abdominal and epigastric reflexes absent, pupils reactive, tongue sticking out straight.
Fluid: slight increase in protein. W. R. + + +
Fluid: slight increase in protein. W. R. + + +
The Board of Pension Commissioners ruled that the condition had been aggravated by service (not “on service”).
The Board of Pension Commissioners decided that the condition had been worsened by service (not “on service”).
Re general paresis, Fearnsides suggested at the Section of Neurology in the Royal Society of Medicine early in 1916, that in all cases of suspected Shell-shock the Wassermann reaction of the serum should be determined, and went on to say that cases of so-called Shell-shock with positive W. R. often improve rapidly with antisyphilitic remedies.
Re general paresis, Fearnsides suggested at the Section of Neurology in the Royal Society of Medicine early in 1916, that in all cases of suspected shell shock, the Wassermann reaction of the serum should be tested, and pointed out that cases of so-called shell shock with a positive W. R. often improve quickly with antisyphilitic treatments.
Duration of neurosyphilitic process important re compensation.
Duration of neurosyphilitic process is important for compensation.
Case 8. (Farrar, personal communication, 1917.)
A Canadian of 36 enlisted in 1915, served in England, and was returned to Canada in February, 1917, clearly suffering from some form of neurosyphilis (W. R. positive in serum and fluid, globulin, pleocytosis 108).
A 36-year-old Canadian joined the military in 1915, served in England, and returned to Canada in February 1917, clearly showing signs of some type of neurosyphilis (W. R. positive in serum and fluid, globulin, pleocytosis 108).
There is no record of any disability or symptom of nervous or mental disease at enlistment. The first symptoms were noted by the patient in May, 1916, six months or more after enlistment. The case was reviewed at a Canadian Special Hospital, October 11, 1916, by a board which reported:
There is no record of any disability or signs of nervous or mental illness at enlistment. The patient first noticed symptoms in May 1916, over six months after enlisting. The case was reviewed at a Canadian Special Hospital on October 11, 1916, by a board that reported:
“The condition could only come from syphilitic infection of three years’ standing” (a decision bearing on compensation); but the general diagnosis remained:
“The condition could only result from a syphilis infection that had been present for three years” (a decision related to compensation); but the overall diagnosis stayed the same:
“Cerebrospinal lues, aggravated by service.”
“Cerebrospinal lues, worsened by service.”
The picture which the medical board regarded as of at least three years’ standing was as follows:
The picture that the medical board considered to be at least three years old was as follows:
History of incontinence, shooting pains, attacks of syncope, general weakness, facial tremor, exaggerated knee-jerks, pupils react with small excursion. Speech and writing disorder, perception dull, lapses of attention, memory defect, defective insight into nature of disorder, emotional apathy.
History of incontinence, shooting pains, fainting spells, general weakness, facial tremors, exaggerated knee reflexes, pupils react with small movements. Speech and writing difficulties, dull perception, lapses in attention, memory issues, poor understanding of the disorder, emotional numbness.
1. Was the conclusion “aggravated by service” sound? On humanitarian grounds the victim is naturally conceded the benefit of the doubt. But it is questionable how scientifically sound the conclusion really was.
1. Was the conclusion “aggravated by service” reasonable? On humanitarian grounds, the victim is understandably given the benefit of the doubt. However, it's questionable how scientifically solid the conclusion actually was.
2. Could the condition come only from syphilitic infection of at least three years’ standing? Hardly any single symptom in this case need be of so long a standing; yet the combination of symptoms seems by very weight of numbers to justify the conclusion of the medical board.
2. Could the condition be the result of a syphilis infection that has lasted at least three years? It's unlikely that any single symptom in this case would require such a long duration; however, the combination of symptoms seems to strongly support the conclusion of the medical board.
Farrar’s case and thirteen others of “Neurosyphilis and the War” were included in a general work on Neurosyphilis (Case History Series, 1917, Southard and Solomon). For military syphilis in general, see Thibierge’s Syphilis dans l’Armée (also in translation).
Farrar’s case, along with thirteen others related to “Neurosyphilis and the War,” was featured in a comprehensive study on Neurosyphilis (Case History Series, 1917, Southard and Solomon). For a broader discussion on military syphilis, refer to Thibierge’s Syphilis dans l’Armée (also available in translation).
General paresis lighted up by the stress of military service without injury or disease?
General paresis sparked by the stress of military service without injury or illness?
Case 9. (Marie, Chatelin, Patrikios, January, 1917.)
In apparently good health a French soldier repaired to the colors, in August, 1914, being then 23 years old.
In seemingly good health, a French soldier enlisted in August 1914 at the age of 23.
Two years later, August, 1916, symptoms appeared: speech disorder with stammering, change of character (had become easily excitable), stumbling gait. He became more and more preoccupied with his own affairs, grew worse, and was sent to hospital in October, 1916.
Two years later, in August 1916, symptoms appeared: a speech disorder with stuttering, personality changes (he had become easily agitated), and a stumbling walk. He became increasingly absorbed in his own issues, his condition worsened, and he was admitted to the hospital in October 1916.
He was then foolish and overhappy, especially when interviewed. There was marked rapid tremor of face and tongue. Speech hesitant, monotonous, and stammering to the point of unintelligibility. His memory, at first preserved, became impaired so that half of a test phrase was forgotten. Simple addition was impossible and fantastic sums would be given instead of right answers. Handwriting tremulous, letters often missed, others irregular, unequal, and misshapen.
He was then foolish and overly happy, especially when being interviewed. There was a noticeable rapid shaking of his face and tongue. His speech was hesitant, flat, and stammering to the point of being hard to understand. His memory, which was initially intact, started to decline so that he forgot half of a test phrase. Simple addition became impossible, and he would provide absurd sums instead of correct answers. His handwriting was shaky, with letters often omitted, and others appearing irregular, uneven, and misshapen.
Excitable from onset, the patient now became at times suddenly violent, striking his wife without provocation. After visit at home, he would forget to return to hospital. Often he would leave hospital without permission (of course the more surprising in a disciplined soldier). No delusions.
Excitable from the start, the patient now sometimes became suddenly violent, hitting his wife without warning. After a visit home, he would forget to go back to the hospital. He often left the hospital without permission (which was especially surprising for a disciplined soldier). No delusions.
Serum and fluid W. R. positive; albumin; lymphocytosis.
Serum and fluid W. R. positive; albumin; lymphocytosis.
Neurological examination: Unequal pupils, slight right-side mydriasis, pupils stiff to light, weakly responsive in accommodation, reflexes lively, fingers tremulous on extension of arms.
Neurological exam: Uneven pupils, slight right-side dilation, pupils unresponsive to light, weakly reactive in accommodation, brisk reflexes, fingers shaking when arms are extended.
The patient had, December 5, 1916, an epileptiform attack with head rotation, limb-contractions and clonic movements. Should this soldier recover for disability obtained in service? Marie was inclined to think military service in part responsible for the development of the paresis. Laignel-Lavastine thought so also, but that the amount assigned should be 5%-10% of the maximum assignable.
The patient experienced an epileptic seizure on December 5, 1916, which included head turning, muscle contractions in the limbs, and shaking movements. Should this soldier receive compensation for the disability caused by his service? Marie believed that military service partially contributed to the development of the weakness. Laignel-Lavastine agreed but thought the compensation should be set at 5%-10% of the maximum possible amount.
SYPHILITIC ROOT-SCIATICA (lumbosacral radiculitis) in a fireworks man with a French artillery regiment.
SYPHILITIC ROOT-SCIATICA (lumbosacral radiculitis) in a fireworks technician with a French artillery regiment.
Case 10. (Long (Dejerine's clinic), February, 1916.)
No direct relation of this example of root-sciatica to the war is claimed nor was there a question of financial reparation.
No direct connection between this example of root-sciatica and the war is claimed, nor was there any discussion about financial compensation.
There was no prior injury. At the end of March, 1915, the workman was taken with acute pains in lumbar region and thighs, and with urgent but retarded micturition.
There was no previous injury. At the end of March 1915, the worker experienced sharp pain in the lower back and thighs, along with urgent but delayed urination.
Unfit for work, he remained, however, five months with the regiment, and was then retired for two months to a hospital behind the lines. He reached the Salpêtrière October 12, 1915, with “double sciatica, intractable.”
Unfit for work, he stayed with the regiment for five months but was then sent to a hospital behind the lines for two months. He arrived at the Salpêtrière on October 12, 1915, with "double sciatica, intractable."
There was no demonstrable paralysis but the legs seemed to have “melted away,” fondu, as the patient said. Pains were spontaneously felt in the lumbar plexus and sciatic nerve regions, not passing, however, beyond the thighs. These pains were more intense with movements of legs; but coughing did not intensify the pains. Neuralgic points could be demonstrated by the finger in lumbar and gluteal regions and above and below the iliac crests (corresponding with rami of first lumbar nerves). The inguinal region was involved and the painful zone reached the sciatic notch and the upper part of the posterior surface of the thigh.
There was no clear paralysis, but the legs seemed to have "melted away," fondu, as the patient described it. The patient felt spontaneous pain in the lumbar plexus and sciatic nerve areas, but this pain did not extend beyond the thighs. The pain became more intense with leg movement; however, coughing did not worsen the pain. Neuralgic points could be identified by touch in the lumbar and gluteal areas and above and below the iliac crests (related to the branches of the first lumbar nerves). The inguinal region was also affected, and the painful area extended to the sciatic notch and the upper part of the back of the thigh.
The sensory disorder had another distribution, objectively tested. The sacral and perineal regions were free. Anesthesia of inner surfaces of thighs, hypesthesia of the anterior surfaces of thighs and lower legs. The anesthesia grew more and more marked lower down and was maximal in the feet, which were practically insensible to all tests, including those for bone sensation. There was a longitudinal strip of skin of lower leg which retained sensation.
The sensory disorder showed a different pattern when tested objectively. The sacral and perineal areas were unaffected. There was a loss of feeling on the inner surfaces of the thighs and reduced sensitivity on the front surfaces of the thighs and lower legs. The lack of feeling increased as it moved downwards, reaching its peak in the feet, which were almost completely unresponsive to all tests, including those for bone sensation. There was a long strip of skin on the lower leg that still had sensation.
Position sense of toes, except great toes, was poor. There was a slight ataxia attributable to the sensory disorder—reflexes of upper extremities, abdominal, and cremasteric preserved, knee-jerks, Achilles and plantar reactions absent.
The sense of position in the toes, except for the big toes, was poor. There was some slight uncoordination due to the sensory issue—reflexes in the upper limbs, abdominal area, and cremasteric were intact, but the knee-jerk, Achilles, and plantar responses were absent.
The vesical sphincter shortly regained its function, though its disorder had been an initial symptom. Pupils normal.
The bladder sphincter quickly returned to normal function, even though its dysfunction had been an early symptom. Pupils are normal.
The “sciatica” here affects the lumbosacral plexus.
The "sciatica" here impacts the lumbosacral plexus.
As to the syphilitic nature of this affection, there had been at eighteen (22 years before) a colorless small induration of the penis, lasting about three weeks. There was now evident a small oval pigmented scar. The patient had married at 20 and had had three healthy children.
As for the syphilitic nature of this condition, there had been a small, colorless hardening on the penis at eighteen (22 years before), which lasted about three weeks. Now, there was a noticeable small oval pigmented scar. The patient had gotten married at 20 and had three healthy children.
The lumbar puncture fluid yielded pleocytosis (120 per cmm.). Mercurial treatment was instituted.
The lumbar puncture fluid showed pleocytosis (120 per cmm.). Mercurial treatment was started.
The treatment has not reduced the pains. Long thinks it was undertaken too long (six months) after onset. The warning for early diagnosis is manifest. There was somehow a delay under the medical conditions of the army.
The treatment hasn’t decreased the pain. Long believes it started too late (six months) after it began. The need for early diagnosis is clear. There was somehow a delay due to the medical conditions in the army.
Re syphilis in munition-workers Thibierge has much to say of French conditions. Throughout his work on syphilis in the army, he stresses the large number of venereal cases in men mobilized for munition-work. Medical inspections ought, according to Thibierge, imperatively to be made in the munition-works and upon all mobilized workmen, whether French or belonging to the Colonial contingents. These men are under military control in France, but they have more opportunities than the soldiers for contracting and disseminating syphilis. They are, in point of fact, very often infected and in a higher proportion than are the soldiers at the front. The munition-workers should also be obliged to report their infections to the physician, whether or no they are under treatment by military or by private physicians.
Re syphilis in munition workers, Thibierge has a lot to say about the situation in France. Throughout his research on syphilis in the army, he emphasizes the high number of venereal cases among men mobilized for munition work. Medical inspections should, according to Thibierge, be made mandatory in the munition factories and for all mobilized workers, whether they are French or from the Colonial contingents. These men are under military control in France, but they have more opportunities than soldiers to contract and spread syphilis. In fact, they are often infected at a higher rate than soldiers at the front. Munition workers should also be required to report their infections to a physician, regardless of whether they are being treated by military or private doctors.
Thibierge devotes a chapter to syphilis as a national danger. Not only do available statistics prove that there is more syphilis in the population since the outbreak of war, but the number of married women going to special hospitals for syphilis is abnormally high and entirely out of proportion to the number of married women resorting to these clinics in peace times. A certain number are contaminated by their husbands on leave. Thibierge calls attention to the fact of the extraordinary frequency of syphilis in young men (two or three, sixteen to eighteen years of age, at Saint-Louis Hospital at each consultation).
Thibierge dedicates a chapter to syphilis as a national threat. Statistics show that there has been an increase in syphilis cases since the war began, and the number of married women visiting special hospitals for syphilis is unusually high, especially compared to the number of married women using these clinics during peacetime. Many are infected by their husbands who are on leave. Thibierge highlights the alarming rate of syphilis among young men, noting that two or three boys aged sixteen to eighteen are seen at Saint-Louis Hospital during each consultation.
A disciplinary case: Syphilitic?
A disciplinary case: Got syphilis?
Case 11. (Kastan, January, 1916.)
Reports varied about a certain German soldier who came up for discipline. Inferiors thought he was harsh and tricky. A lieutenant declared that the man always wanted to have proper respect paid to him, and that he was unduly excited by trifles. The man had become latterly very nervous on account of battle strain and protracted shelling.
Reports varied about a certain German soldier who came up for discipline. His subordinates thought he was harsh and manipulative. A lieutenant stated that the man always demanded to be shown proper respect and that he got overly worked up about small things. Lately, the man had become very anxious due to the stress of battle and prolonged shelling.
July 28, 1915, the man, who had been drinking with comrades the night before, was excitedly talking to an officer concerning relief of a guard. The soldier stated, “As a sergeant on duty with a service record of 15 years, I think it is my affair.” The lieutenant replied, “So far as I am concerned, the matter is settled.” The sergeant yelled, “As far as I am concerned, it is settled also. By the way, my name is Mr. Vice Sergeant …,” and with that the sergeant wrote down the lieutenant’s words and refused to obey the lieutenant’s order to “Stop writing.” The lieutenant drew his sword and said, “Take your hands down.” The sergeant replied, “Surely I am permitted to write.” Lieutenant: “Subordination; don’t forget yourself, Vice Sergeant.…” The sergeant jeered, “You forgot yourself anyhow;” whereupon the lieutenant: “Well, such a thing never happened to me before.” The sergeant, jeeringly, “Nor to me either. If I were not in undress I should know what to do.” The lieutenant: “Vice Sergeant …, remain here. This matter will be settled at once.” The sergeant: “It is Mr. Vice Sergeant …,” whereupon he gave his notebook to a hornblower and said, “Write.” The lieutenant: “Stay.” The sergeant: “What, stay here. No, I’ll not stay,” and made off. The lieutenant called after him, “Put on your service dress and see the captain.” He made ready but said, “This half-idiot gives an order like that to a sergeant with 15 years’ record.”
On July 28, 1915, the man, who had been drinking with friends the night before, was excitedly talking to an officer about relieving a guard. The soldier said, “As a sergeant on duty with 15 years of service, I believe this concerns me.” The lieutenant replied, “As far as I'm concerned, that’s that.” The sergeant shouted, “As far as I’m concerned, it’s settled too. By the way, my name is Mr. Vice Sergeant …,” and with that, the sergeant wrote down the lieutenant’s words and ignored the lieutenant’s order to “Stop writing.” The lieutenant drew his sword and said, “Put your hands down.” The sergeant answered, “Surely I'm allowed to write.” The lieutenant replied, “Subordination; don’t forget yourself, Vice Sergeant.… ” The sergeant scoffed, “You forgot yourself anyway;” to which the lieutenant responded, “Well, I’ve never had this happen to me before.” The sergeant mockingly said, “Me neither. If I weren't in undress, I’d know what to do.” The lieutenant said, “Vice Sergeant …, stay here. This will be resolved immediately.” The sergeant retorted, “It’s Mr. Vice Sergeant …,” then handed his notebook to a hornblower and said, “Write.” The lieutenant commanded, “Stay.” The sergeant replied, “What, stay here? No, I won’t stay,” and walked away. The lieutenant called after him, “Put on your service dress and see the captain.” He prepared to comply but said, “This half-wit gives orders like that to a sergeant with 15 years of service.”
The examination showed that the man had a hypalgesia. He complained of violent headaches. He said that he had had syphilis 10 years before; there were no bodily stigmata.
The examination showed that the man had a reduced sensitivity to pain. He complained of severe headaches. He mentioned that he had syphilis 10 years earlier; there were no visible signs.
Regulations broken: General paresis.
Rules violated: General paresis.
Case 12. (Kastan, January, 1916.)
A German 1st-lieutenant, on active service before the war, had left the service because there was not enough for him to do in peace times. During his war service, he became drunk and had two soldiers bound to a doorpost, with coats unbuttoned and without their caps—a process quite verboten. While in Königsberg, he reported himself ill, and failed to go to a designated hospital. He was accordingly treated as a deserter. He ran up bills with landlady and servant girls, saying that he was going to receive money from his wife. Under hospital examination, he said he was only a Baden man with a lively temperament. He got angry at the phrase test feeding, refused food, got excited when asked to help in the care of other patients, and wrote a letter saying, “If it is the idea to make me nervous by removing the air from me, by prescribing rest in bed—a punishment only suitable for a boy who cannot keep himself neat—and such chicaneries, these philanthropic attempts are bound to fail on my robust peasant nerves. Of course I know that money considerations make the stay of every paying patient desirable, but I am really too good for that. [The expenses were being borne by the state.] I have openly stated what is being here done with me is foolery, and I stick to that phrase. The food, already poor enough, is no better, when the meat of a half-rotten cow comes twice to the table.” This patient was, according to Kastan, a victim of general paresis.
A German first lieutenant, who was on active duty before the war, left the military because there wasn't enough for him to do during peacetime. While serving in the war, he got drunk and had two soldiers tied to a doorpost, with their coats unbuttoned and without their caps—a totally forbidden act. When he was in Königsberg, he reported himself sick and didn’t go to the designated hospital, so he was treated as a deserter. He racked up bills with the landlady and servant girls, claiming he was going to receive money from his wife. During a hospital examination, he asserted that he was just a lively guy from Baden. He got upset at the term "test feeding," refused to eat, became agitated when asked to help care for other patients, and wrote a letter saying, “If the plan is to make me nervous by depriving me of air and prescribing bed rest—something only appropriate for a kid who can’t behave—and these nonsense tactics, then these well-meaning attempts are sure to fail against my strong peasant nerves. Of course, I know that financial reasons make it desirable for every paying patient to stay, but I’m really too good for that. [The state was covering the expenses.] I’ve said openly that what’s being done to me here is nonsense, and I stand by that statement. The food, which is already quite poor, doesn’t get any better when half-rotten cow meat is served twice at the table.” According to Kastan, this patient was a victim of general paresis.
Re general paresis and delinquency, Gilles de la Tourette long ago maintained that there was a medicolegal period in paresis. Lépine in his work on Troubles Mentales de la Guerre speaks of the unexpected frequency of general paresis in the army, and calls attention at the outset to the medicolegal period. The danger of overt delinquency is, in fact, greater under military than under civilian conditions on account of the closer surveillance of the soldier. Desertion and thievery are the main forms.
Re general paresis and delinquency, Gilles de la Tourette pointed out long ago that there is a medicolegal period in paresis. Lépine, in his work on Troubles Mentales de la Guerre, discusses the surprising prevalence of general paresis in the military and highlights the medicolegal period right from the start. The risk of overt delinquency is, indeed, higher in military settings than in civilian ones due to the tighter supervision of soldiers. The main forms of delinquency are desertion and theft.
Unfit for service: General paresis.
Unfit for service: General paresis.
Case 13. (Kastan, January, 1916.)
Kastan describes a non-commissioned officer, who came voluntarily into the clinic. It seems that he had absented himself (?) from the army in the suburbs of Königsberg, September 3, 1914. He was arrested October 7th. Once before he had been brought to Kastan’s clinic on the suspicion of general paresis, but had been dismissed as non-paretic. Brought in again in a condition of marked fear, he declared that he had to fall behind his company while he was on the march on account of a feeling of weakness. He had been taken to a hospital and then carried to the suburbs of Königsberg, examined, and found unfit for service.
Kastan talks about a non-commissioned officer who came to the clinic voluntarily. It appears he had gone absent without leave from the army in the suburbs of Königsberg on September 3, 1914. He was arrested on October 7th. Previously, he had been brought to Kastan’s clinic under suspicion of general paresis but was dismissed as not having it. This time, he was brought in displaying significant fear, saying he had to lag behind his company during a march due to feelings of weakness. He was taken to a hospital and then transferred to the suburbs of Königsberg, where he was examined and deemed unfit for service.
He had in his 20th year become infected with syphilis, and had recently become forgetful, subject to fears, and easily excitable. He had been very unhappily married with a woman who was hysterical and threatened to shoot and poison him. He lived in a condition of continual quarrels with her. The symptoms that he felt on the march were numbness of the legs and a rush of blood to the head. In the clinic, he was subject to much dreaming and raving about the war. There was excessive perspiration.
In his 20th year, he got infected with syphilis and had recently become forgetful, anxious, and easily excited. He had an extremely unhappy marriage with a woman who was hysterical and threatened to shoot and poison him. He was constantly fighting with her. While marching, he experienced numbness in his legs and a rush of blood to his head. In the clinic, he often dreamed and raved about the war. He was also sweating excessively.
1. As to the proper interpretation of this case, details are lacking as to the physical and laboratory side. In fact, it would appear that the suspicion of paresis at his first reception in a clinic was dismissed without resort to laboratory findings.
1. When it comes to the right interpretation of this case, there are missing details regarding the physical and lab aspects. In fact, it seems that the suspicion of paresis when he was first admitted to a clinic was disregarded without any laboratory tests.
There are no neurological symptoms in the case clearly suggestive of neurosyphilis, except perhaps the numbness of the legs. The remainder of the picture appears to be entirely psychic. Sensory and intellectual symptoms are missing unless we count the war dreams and mania as intellectual. It appears wiser to count these as emotional in the sense that they were roused by emotion-laden memories. The fear, perspiration, and feelings of head flush are perhaps to be best interpreted as satellites about an emotional nucleus.
There are no neurological symptoms in this case that clearly indicate neurosyphilis, except maybe the numbness in the legs. The rest of the situation seems to be purely psychological. Sensory and intellectual symptoms are absent unless we consider the war dreams and mania as intellectual. It seems more appropriate to classify these as emotional since they were triggered by emotionally charged memories. The fear, sweating, and hot flashes are probably best understood as related to an emotional core.
Hysterical chorea versus neurosyphilis.
Hysterical chorea vs. neurosyphilis.
Case 14. (De Massary and Du Sonich, April, 1917.)
There were various complications in the case of a lieutenant (nervous tic in childhood; travel 23 to 30), who was at Antwerp during the period of mobilization. He was taken there by the Germans; was a prisoner in their hands for 55 days; and succeeded under great strain in escaping.
There were several complications in the case of a lieutenant (nervous tic in childhood; travel 23 to 30), who was in Antwerp during the mobilization period. He was captured by the Germans and held as a prisoner for 55 days, managing to escape under extreme pressure.
He then entered his regiment, and, passing the examinations, was made an adjutant, and went to the front, March, 1915. He stayed ten months in the Verdun region, under heavy bombardment, and in June was bowled over and buried by a 210. He seemed to be fearless, getting no sensation from shell-bursts except a griping sensation in the bowels.
He then joined his regiment and, after passing the exams, became an adjutant and went to the front in March 1915. He spent ten months in the Verdun area, enduring heavy bombardment, and in June was knocked over and buried by a 210 shell. He appeared to be fearless, feeling nothing from the explosions except a gripping sensation in his stomach.
However, his character had altered in the direction of irritability; and by the end of January, 1916, he had to be evacuated for the first time from the front, for general weakness, with the diagnoses: neurasthenia, neuralgia, dyspeptic troubles, great general fatigue, marked depression. In fact, at Narbonne he was asked no questions for several days on account of his obvious depression. He was given ice-bags for violent headaches, complete rest in bed, cacodylate and sodium nucleinate. In two weeks he was up and about.
However, his character had shifted toward irritability; and by the end of January 1916, he had to be evacuated from the front for the first time due to general weakness, with diagnoses including neurasthenia, neuralgia, digestive issues, extreme fatigue, and significant depression. In fact, at Narbonne, no questions were asked of him for several days because of his clear depression. He was given ice packs for severe headaches, complete bed rest, cacodylate, and sodium nucleinate. In two weeks, he was up and moving around again.
At this time appeared choreiform movements, which reached their maximum in two or three days, whereupon he was sent, March 4, 1916, to the neurological centre at Montpellier. Here W. R. positive! Neosalvarsan on the second injection (0.45 and 0.60) yielded a strong reaction, with fever, delirium, vomiting, and then jaundice.
At this point, choreiform movements showed up, peaking in two or three days, after which he was sent to the neurological center in Montpellier on March 4, 1916. Here, W. R. tested positive! Neosalvarsan on the second injection (0.45 and 0.60) caused a strong reaction, including fever, delirium, vomiting, and later jaundice.
About a month later, he was given twenty more intravenous injections, whereupon the choreic movements now decreased, and July 15 he was given convalescence for three months. October 15 he went back to his dépôt cured; and October 20, on request, went to the front. He was potted and under machine-gun fire at times during the next three months, but the choreic movements did not reappear. January 1 he left the trenches as the division went into billets.[21] January 8, suddenly, without any emotional cause, he began to “dance” again. Accordingly, he was evacuated for the second time, January 10, 1917, with the diagnosis: choreic movements, especially on left; evacuate to special centre.
About a month later, he received twenty more intravenous injections, which led to a decrease in the choreic movements. On July 15, he was granted three months of convalescence. By October 15, he returned to his depot fully cured, and on October 20, at his request, he went back to the front. He encountered gunfire at times during the next three months, but the choreic movements did not return. On January 1, he left the trenches as the division moved into billets.[21] Then, on January 8, suddenly and without any emotional trigger, he started to “dance” again. As a result, he was evacuated for the second time on January 10, 1917, with the diagnosis: choreic movements, especially on the left; evacuate to a special center.
At Royallieu, a lumbar puncture showed a slight lymphocytosis. The headache improved. He was evacuated January 24, 1917, to Val-de-Grâce, with a diagnosis: Recurrent chorea; first attack followed commotio cerebri, nervous depression, inequality of pupils, various pains, contracted in the army. Another W. R. was positive. Twelve intramuscular injections of oxygen cyanide were given, besides baths. He was then sent to Issy-les-Moulineaux with a diagnosis of tic. He showed choreiform movements affecting the legs alone. When sitting, legs extended and flexed, the knees would abduct, then adduct; the thighs flexed. When standing, flexor movements were produced alternately on the left and the right, the knee being raised high, sometimes striking the patient’s hand. In walking, the thigh and lower leg flexion was always out of proportion to the required step. There was thus a sort of saltatory chorea limited to the legs. The reflexes so far as they could be tested were normal save that the left pupil was fixed to light and accommodation; the right pupil was sluggish to light but accommodated normally. Leucoplakia of the cheeks; nocturnal headaches; and pains resembling lightning pains in arms and legs. Lumbar puncture, March 26, showed blood-stained fluid, and the puncture was followed by headache, vomiting, and slow pulse. The fluid showed a slight lymphocytosis; W. R. negative.
At Royallieu, a lumbar puncture revealed a slight increase in lymphocytes. The headache got better. He was evacuated on January 24, 1917, to Val-de-Grâce, diagnosed with recurrent chorea; the first attack followed a concussion, along with nervous depression, uneven pupils, and various pains, all developed while in the army. Another W. R. was positive. He received twelve intramuscular injections of oxygen cyanide, along with baths. He was then sent to Issy-les-Moulineaux with a diagnosis of tic. He exhibited choreiform movements affecting only the legs. While sitting, his legs would extend and flex, and his knees would move outward and then inward; his thighs were flexed. When standing, alternating flexor movements would occur on the left and right legs, with one knee lifting high enough to sometimes hit his hand. In walking, the flexion of the thigh and lower leg was always disproportionate to the step required. This resulted in a sort of jumping chorea limited to the legs. The reflexes, as far as tested, were normal, except that the left pupil didn’t react to light or focus, while the right pupil was slow to light but focused normally. There was leukoplakia in the cheeks; nighttime headaches; and pain resembling sharp pains in the arms and legs. A lumbar puncture on March 26 showed blood-stained fluid, and the procedure led to headache, vomiting, and a slow pulse. The fluid indicated a slight increase in lymphocytes; W. R. was negative.
It is clear that a diagnosis limiting itself to the leg trouble would probably content itself with “hysterical chorea.” The lieutenant said that when he saw people “dance” he did have a tendency to imitate them; and when he was cured of that, he did not want to go to Lamalou because he would see the ataxic patients there and might fall back into his “dancing.” However, in view of the pupillary inequality, the lymphocytosis, the leucoplakia, the W. R., and the initial neurasthenia and depression found in the very first hospital in which he was examined, we probably should be entitled to consider that general paresis played a part in the chorea.
It’s obvious that a diagnosis focused solely on the leg issues would likely settle on “hysterical chorea.” The lieutenant mentioned that when he saw people “dancing,” he often felt the urge to copy them; and once he got past that, he didn’t want to go to Lamalou because he would see the ataxic patients there and might relapse into his “dancing.” However, considering the unequal pupils, lymphocytosis, leukoplakia, the W. R., and the initial neurasthenia and depression found at the very first hospital where he was examined, we should probably acknowledge that general paresis had a role in the chorea.
Shrapnel fragment driven through skull: General paresis.
Shrapnel fragment driven through skull: General paresis.
Case 15. (Hurst, April, 1917.)
A private, 31, was wounded December 7, 1916, by a shrapnel fragment which entered the skull above the left ear and lodged in the brain, an inch above and 2½ inches below the middle of the right orbital margin. At Netley, December 30, he proved to show a complete internal and external left sided ophthalmoplegia, with the exception of the external rectus. On the right side, there was a complete paralysis of the superior rectus and a partial paralysis of the inferior rectus and levator palpebrae superioris. There was a paresis of the left side of the face. The right plantar reflex was said to have been extensor at the clearing station, but at Netley it and the other reflexes proved to be normal, as were the optic. The patient was stuporous and had incontinence of urine and feces for two days. Shortly after admission, slurring of speech with a long latent period occurred. It was clear that the shrapnel fragment must have passed far above the crus, and it was not plain how isolated lesions of the third and seventh nerve nuclei could have been brought about without injury of the long tracts of the crus.
A private, 31, was injured on December 7, 1916, by a piece of shrapnel that penetrated the skull above the left ear and settled in the brain, one inch above and 2½ inches below the center of the right eye socket. At Netley, on December 30, he showed complete internal and external paralysis on the left side of his eye, except for the external rectus muscle. On the right side, there was total paralysis of the superior rectus muscle and partial paralysis of the inferior rectus and levator palpebrae superioris muscles. There was weakness on the left side of his face. The right plantar reflex was noted to be extensor at the clearing station, but at Netley, it and the other reflexes were normal, as were the optic reflexes. The patient was semi-conscious and experienced loss of control over urination and bowel movements for two days. Shortly after being admitted, he began to slur his speech, which had a long delay. It was evident that the shrapnel piece must have passed well above the crus, and it was unclear how isolated lesions of the third and seventh nerve nuclei could have occurred without damaging the long tracts of the crus.
The Wassermann reaction of the serum was negative, but that of the spinal fluid was positive. Iodide and mercury secured considerable improvement in the mental condition and some diminution in the paralysis. The patient is now extremely pleased with himself and has a speech suggestive of paresis.
The Wassermann test on the serum was negative, but the one on the spinal fluid was positive. Iodide and mercury greatly improved his mental state and reduced some of the paralysis. The patient is now very pleased with himself and speaks in a way that suggests paresis.
Head trauma: Shell-shock effects, over in a few months. Manic-depressive (?) attack more than two years later. X-ray evidence suggesting brain lesion. Serum Wassermann reaction positive.
Head trauma: Shell shock effects cleared up in a few months. Manic-depressive episode (?) occurred more than two years later. X-ray results indicate a brain lesion. Serum Wassermann test positive.
Case 16. (Babonneix and David, June, 1917.)
A bullet glancing from his gun barrel November 28, 1914, wounded a man in the head, whereupon he lost consciousness and was carried to a hospital and trephined. On coming to, he found that he could not hear and felt pains; but the latter disappeared in a few months. He was given sedentary employment and did his work properly until February, 1917, when he suddenly became sad, wept, slept poorly, stopped eating, had an absent air, and began to complain of his head. He passed whole days without moving, in a sort of stupor, which was then followed by a hypomaniacal agitation in which he walked furiously up and down in the room and threw objects about.
A bullet that grazed his gun barrel on November 28, 1914, wounded a man in the head, causing him to lose consciousness. He was taken to a hospital and underwent trepanation. When he regained consciousness, he discovered that he was deaf and experienced pain, which faded away over a few months. He was given a desk job and managed to do it well until February 1917, when he suddenly became depressed, cried, had trouble sleeping, stopped eating, appeared disengaged, and started complaining about his head. He would spend entire days inactive, in a sort of stupor, which was then followed by episodes of hypomanic agitation where he would pace wildly in the room and throw things around.
He was found subject to a generalized tremor and he was distinctly weaker on the right side. The tendon reflexes were excessive. The bony sensibility, as well as the pain and temperature sense, and the position and stereognostic senses were completely abolished on the right side. The scar lay on the left side. It was deep and very sensitive to pressure, so that if it was touched ever so slightly the patient began to weep. X-ray indicated loss of substance in the posterior part of the left parietal region. Remains of the projectile were found subcutaneously in the right supraorbital region. The W. R. of the serum was positive. There was no lymphocytosis in the spinal fluid.
He was found to have a general tremor and was noticeably weaker on his right side. The tendon reflexes were overactive. Sensation in the bones, as well as pain, temperature, position, and stereognostic senses, were completely lost on the right side. The scar was on the left side. It was deep and very sensitive to touch, causing the patient to cry if it was touched even lightly. X-rays showed a loss of tissue in the back part of the left parietal area. Fragments of the projectile were found under the skin in the right eyebrow area. The W. R. of the serum was positive. There was no increase in lymphocytes in the spinal fluid.
Interpretation of this case is manifestly difficult. Four possibilities exist: Syphilis, manic depressive psychosis, traumatic brain disease, and functional shock effects. More than two years had passed between the trauma and the change of character.
Interpretation of this case is clearly challenging. Four possibilities exist: syphilis, bipolar disorder, traumatic brain injury, and functional shock effects. More than two years passed between the trauma and the change in personality.
Skull trauma in a syphilitic.
Skull injury in a syphilitic.
Case 17. (Babonneix and David, June, 1917.)
A soldier, 31, sustained fracture of the occiput from shell-burst, and thereafter showed confusion and total loss of memory. Operation November 11 withdrew bony fragments and clots, whereupon the man returned practically to normal. He developed, however, a few seizures, in which he struggled, fell, and lost consciousness, afterward suffering from headache. The tendon reflexes were increased. The occipital cicatrix was a little depressed and slightly painful on pressure.
A 31-year-old soldier suffered a skull fracture from a shell explosion and later experienced confusion and complete memory loss. An operation on November 11 removed bone fragments and clots, after which he nearly returned to normal. However, he began to have a few seizures, during which he struggled, fell, and lost consciousness, followed by headaches. His tendon reflexes were heightened. The scar on the back of his head was slightly depressed and somewhat tender to the touch.
Lumbar puncture showed a very slight lymphocytosis (5 to 6 cells), practically negative globulin reaction, and a low albumin titer. There were no signs of syphilis in the eyes. The W. R. in the serum was strongly positive. Very possibly the traumatic phenomena in this case can be safely disengaged from the syphilitic phenomena.
Lumbar puncture revealed a very slight increase in lymphocytes (5 to 6 cells), a nearly negative globulin reaction, and a low albumin level. There were no signs of syphilis in the eyes. The W. R. in the serum was strongly positive. It's very likely that the traumatic effects in this case can be clearly separated from the syphilitic effects.
Re the mechanism by which trauma evokes or accelerates the course of neurosyphilis, it is probable that most neuropathologists believe that the commotio cerebri causes sundry chemical or physical effects in the nerve tissues such that spirochetes are moved into new and more dangerous places, or such that more appropriate food is supplied to the organisms, which then begin to multiply. Whether the organisms live in a kind of symbiosis in the tissues under ordinary circumstances in the pre-paretic period of the development of neurosyphilis, is unknown. Possibly fat embolism should be added to the list of possible causes of the hastening of the neurosyphilitic process. Fat embolism in the brain has been shown by various authors to be accompanied by minute hemorrhages, in the midst of which by proper stains the fat embolism can be made out.
Regarding the way trauma triggers or speeds up the progression of neurosyphilis, most neuropathologists likely think that commotio cerebri leads to various chemical or physical changes in the nerve tissues, allowing spirochetes to move to new and more dangerous locations, or providing a better food supply for the organisms, which then start to multiply. It's unclear whether these organisms coexist in a sort of symbiosis in the tissues during the normal pre-paretic phase of neurosyphilis development. It's possible that fat embolism should be added to the list of potential factors contributing to the acceleration of the neurosyphilitic process. Research has shown that fat embolism in the brain is often associated with tiny hemorrhages, amidst which, with the right stains, the fat embolism can be identified.
Shell-wound in battle: General paresis.
Shell-shocked in battle: General paresis.
Case 18. (Boucherot, 1915.)
A soldier in the Territorial Infantry, 42, a gardener who went to taverns, as he said, “like everybody else,” a widower with two children, a good worker though irascible, had had syphilis as a youth. He was called to the colors at the outbreak of the war and got on well despite tremendous strain. March 9, 1915, he was in a bayonet charge with his regiment and was bowled over by a shell of which a fragment wounded him above the knee and several fragments in the thorax. All these fragments were extracted at a temporary hospital, March 11. The man now became strange, refused to obey orders and did a number of peculiar things so that he was sent to Orléans temporary hospital whence he was evacuated to Fleury Asylum, March 19. He refused to give up his things because he was the master. He did not want to go to bed and wanted to keep on walking constantly. He was without sense of shame, satisfied with himself, grandiose as to his millions in bank and the thirty-six decorations he believed had been awarded him. He mistook the identity of the landscape and of the people about him.
A 42-year-old soldier in the Territorial Infantry, a gardener who visited pubs "like everyone else," a widower with two kids, a good worker but hot-tempered, had contracted syphilis in his youth. He was called up when the war broke out and managed well despite the massive pressure. On March 9, 1915, he participated in a bayonet charge with his regiment and was knocked down by a shell, with a fragment injuring him just above the knee and several others hitting his chest. All these fragments were removed at a temporary hospital on March 11. After that, he started acting strangely, refusing to follow orders and engaging in odd behavior, so he was sent to a temporary hospital in Orléans and then evacuated to Fleury Asylum on March 19. He resisted giving up his belongings because he believed he was in charge. He didn’t want to go to bed and insisted on walking around continuously. He lost all sense of shame, was self-satisfied, and thought he had millions in the bank along with thirty-six medals he believed he had received. He confused the identity of the landscape and the people around him.
Tongue tremulous; pupils unequal; knee-jerks exaggerated; dysarthria; gaps in memory. In May occurred a number of violent reactions.
Tongue shaking; uneven pupils; exaggerated knee-jerk reflexes; slurred speech; memory gaps. In May, several violent reactions happened.
In June, however, there was a remission; the ideas of grandeur disappeared first, then the tremors and reflex disorder and finally the speech disorder. There was a slight seizure at this point and the man said he had had another such just before he came to the army. July 20 he was invalided out much improved.
In June, however, there was a break; the feelings of grandeur went away first, followed by the tremors and reflex issues, and finally the speech problems. He had a slight seizure at this point and mentioned that he had experienced another one just before he joined the army. On July 20, he was discharged, feeling much better.
In this case of general paresis there is, besides the syphilis, also alcoholism to consider, so that it is not entirely plain that the exertions of campaign liberated the paresis.
In this case of general paresis, we also have to consider alcoholism in addition to syphilis, so it’s not completely clear that the stresses from the campaign caused the paresis.
Re wounds and paresis, see also Case 5 (Beaton), in which neurosyphilis advanced rapidly from the time of a trivial injury.
Re wounds and paralysis, see also Case 5 (Beaton), in which neurosyphilis progressed quickly after a minor injury.
Shell-explosion: Syphilitic ocular palsy.
Shell explosion: Syphilitic eye paralysis.
Case 19. (Schuster, November, 1915.)
Schuster notes briefly a curious result of the explosion of a shell, which caused the patient in question to lose consciousness. Shortly after the explosion, the patient came to his senses again, but a surprising paresis of the eye muscles had developed. This paresis looked precisely like a syphilitic paresis clinically.
Schuster briefly mentions an interesting outcome of the explosion of a shell, which caused the patient to lose consciousness. Soon after the explosion, the patient regained awareness, but an unexpected weakness in the eye muscles had emerged. This weakness resembled a syphilitic paralysis in terms of clinical presentation.
Examination of the blood serum yielded a strongly positive Wassermann reaction.
Testing the blood serum showed a highly positive Wassermann reaction.
According to Schuster, the explosion of the shell had brought about hemorrhage in vessels supplying the region of the eye muscle nerves or nuclei. The reason for the selection of these vessels for rupture due to shell explosion is, according to Schuster, that the vessels were probably already syphilitically diseased.
According to Schuster, the shell explosion caused bleeding in the vessels that supply the eye muscle nerves or nuclei. Schuster suggests that these vessels were likely already damaged by syphilis, which made them more susceptible to rupture from the explosion.
Re hemorrhages in the neighborhood of the oculomotor nuclei, the phenomena of polioencephalitis may be recalled. In that disease, the predisposition to hemorrhage is presumed to be alcoholic, as the cases of ophthalmoplegia of this group almost always appear in alcoholics. However, the first case of hemorrhagic superior polioencephalitis was a non-alcoholic one of Gayet (1875), in which the symptoms followed three days after a boiler explosion.
Re hemorrhages near the oculomotor nuclei, the symptoms of polioencephalitis may be noted. In that disease, the likelihood of hemorrhage is thought to be linked to alcohol use, as cases of ophthalmoplegia in this group almost always occur in people who consume alcohol. However, the first case of hemorrhagic superior polioencephalitis was a non-alcoholic one reported by Gayet (1875), where the symptoms appeared three days after a boiler explosion.
A tabetic lieutenant “shell-shocked” into paresis?
A tabetic lieutenant “shell-shocked” into paralysis?
Case 20. (Donath, July, 1915.)
An apparently competent German professor in an intermediate school, a lieutenant of infantry reserves, 33 years old, on the 17th August, 1914, was stunned for a while by the shock of a cannon-firing 25 feet away. Urination became difficult. Headaches and limb pains ensued, with paralysis of fingers, gastric troubles, forgetfulness, especially for names, insomnia, and general scattering of mental faculties.
A seemingly capable German professor at a middle school, a reservist lieutenant in the infantry, 33 years old, was momentarily taken aback by the blast of a cannon firing just 25 feet away on August 17, 1914. He struggled to urinate. He then experienced headaches and pain in his limbs, along with paralysis in his fingers, stomach issues, forgetfulness—especially regarding names—insomnia, and a general disorganization of his mental faculties.
Neurologically, the pupils were irregular, left larger than right; Argyll-Robertson reaction. Right knee-jerk livelier than left. Achilles reactions absent. Slow and dissociated pain reactions in feet, lower thighs and lower quarter of upper thighs, with hypalgesia or analgesia. Station good; gait steady. Mentally depressed, slow of thought. Speech poor and of indistinct construction (mild dementia). Calculation ability poor. No pleasure in work.
Neurologically, the pupils were uneven, with the left being larger than the right; Argyll-Robertson reaction present. The right knee-jerk was more responsive than the left. Achilles reflexes were absent. There were slow and inconsistent pain responses in the feet, lower thighs, and lower part of the upper thighs, with reduced sensitivity to pain or complete lack of it. Station was good; gait was steady. Mentally depressed and slow to think. Speech was poor and hard to understand (mild dementia). Calculation skills were lacking. No enjoyment in work.
Wassermann reaction of serum weakly positive.
Wassermann reaction of serum slightly positive.
It seems that for a year the patient had been subject to spells of anger. He was irritated by his wife who had been nervous since an earthquake.
It seems that for a year the patient had been experiencing bouts of anger. He was annoyed with his wife, who had been anxious since the earthquake.
On the occasion of the earthquake, 1911, the patient himself had had a spell of difficulty with urination. The spell had lasted two or three months. The patient had had a chancre in 1902, “cured” in four or five weeks with xeroform. In 1908, when about to marry, he had had six mercurial inunctions.
During the earthquake in 1911, the patient experienced a period of trouble urinating. This issue lasted for two to three months. He had a chancre in 1902 that was "cured" in four to five weeks with xeroform. In 1908, just before getting married, he underwent six treatments with mercury ointment.
Re tabes, Lépine shows that tabetics are numerous. They are numerous among officers and also in the auxiliary service, in which latter tabetics are maintained on desk duty. Perhaps they had been admitted to such work as unable to march or fight, on the basis of having had so-called[28] “rheumatism.”
Re tabes, Lépine shows that people with tabes are quite common. They are prevalent among officers and also in the auxiliary service, where those with tabes are assigned to desk jobs. They may have been allowed to do this work because they were unable to march or fight, supposedly due to something referred to as [28] “rheumatism.”
Shell-explosion may precipitate neurosyphilis in the form of tabes dorsalis.
Shell explosions may trigger neurosyphilis in the form of tabes dorsalis.
Case 21. (Logre, March, 1917.)
An artilleryman, 38, had a large calibre shell explode very near him and afterward could not hear the whistle of a shell without falling down in a generalized tremor, sweating profusely, urinating involuntarily, in a mental state approaching stupidity. Here was a case that might be regarded as one of morbid cowardice in a psychopath, following violent emotion.
An artilleryman, 38, had a large caliber shell explode very close to him, and afterward, he couldn't hear the whistle of a shell without collapsing in a complete tremor, sweating heavily, urinating involuntarily, and getting to a mental state that was almost like stupidity. This was a case that could be seen as morbid cowardice in a psychopath, following intense emotion.
The artilleryman proved to be a victim of tabes and of general paresis. The incontinence of urine under the influence of emotion was nothing but an effect of tabetic sphincter disorder. The crisis of cowardice proved nothing but an initial symptom of general paresis.
The artilleryman turned out to be suffering from tabes and general paresis. The loss of bladder control when he was emotional was just a result of tabetic sphincter dysfunction. His episode of cowardice was simply an early sign of general paresis.
Shell-explosion; burial: Tabes dorsalis incipiens.
Shell explosion; burial: Tabes dorsalis incipiens.
Case 22. (Duco and Blum, 1917.)
A French soldier was buried by effects of shell explosion September 8, 1914. He sustained no wound or fracture.
A French soldier was buried due to the effects of a shell explosion on September 8, 1914. He didn’t have any wounds or fractures.
Incontinence of urine developed. Anesthesia of penis and scrotum. Reflexes absent; pupils sluggish. Wassermann reactions suspicious.
Incontinence of urine occurred. There was numbness in the penis and scrotum. Reflexes were absent; pupils were sluggish. Wassermann reactions were questionable.
The diagnosis tabes dorsalis incipiens was made (hematomyelia of conus terminalis eliminated).
The diagnosis tabes dorsalis incipiens was confirmed (hematomyelia of the conus terminalis ruled out).
The patient was estimated to be “40% incapacitated,” according to the French “échelle de gravité” of conditions. A full pension would not be justified in the opinion of the French authors.
The patient was estimated to be “40% incapacitated,” according to the French “échelle de gravité” of conditions. A full pension would not be justified in the opinion of the French authors.
SHELL-SHOCK PSEUDOTABES (non-syphilitic, serum W. R. positive). Improvement.
SHELL-SHOCK PSEUDOTABES (non-syphilitic, serum W. R. positive). Improvement.
Case 23. (Pitres and Marchand, November, 1916.)
Innkeeper B., 36, a shell-shock and burial victim June 20, 1915, was looked on by a number of physicians as a case of genuine tabes.
Innkeeper B., 36, a victim of shell shock and burial on June 20, 1915, was regarded by several doctors as a case of true tabes.
Even eight months after the episode, he still showed (when observed by Pitres and Marchand, February 3, 1916) absence of knee-jerks and Achilles jerks, a slight swaying in the Romberg position, pupils sluggish to light, incoördination, delayed sensations. There was also a history of pains in the legs, compared by the patient to those of sciatica. These pains came in crises, the longest of which had lasted 30 hours.
Even eight months after the incident, he still showed (when observed by Pitres and Marchand on February 3, 1916) no knee-jerk or Achilles reflexes, a slight swaying in the Romberg position, sluggish pupils in response to light, lack of coordination, and delayed sensations. The patient also reported leg pain, which he compared to sciatica. These pains occurred in episodes, the longest of which lasted 30 hours.
It seems that this soldier’s troubles began the day after his shock with a feeling of swollen feet and of cotton wool under them. He stayed on service, however, walking with increasing difficulty.
It looks like this soldier’s problems started the day after he experienced a strange feeling of swollen feet and like he was walking on cotton. Nonetheless, he continued his service, moving with growing difficulty.
At the time of his evacuation, July 10, he could walk with great difficulty. “Strips of lead were between his legs.” He could hardly control movements in the dark, or descend stairs. Often his legs would bend under him. Vesical function sluggish.
At the time of his evacuation on July 10, he could walk with a lot of difficulty. “Strips of lead were between his legs.” He could barely control his movements in the dark or go down stairs. Often his legs would give out on him. Bladder function was slow.
After a few months the patient could walk better. In February, 1916, he walked thrusting his legs forward trembling, and dragging toes a little. He could not support himself on either leg. Jerkiness and incoördination in extension or flexion of leg on thigh.
After a few months, the patient could walk better. In February 1916, he walked by thrusting his legs forward while trembling and dragging his toes a bit. He couldn't support himself on either leg, displaying jerkiness and lack of coordination when extending or flexing his leg at the thigh.
The muscular weakness was decidedly against tabes or at all events a pure tabes. The incoördination proved to be due, not to loss of position sense (which was intact) but to unsteady muscular contractions. Deep sensibility was intact.
The muscle weakness clearly ruled out tabes, or at least a pure case of it. The lack of coordination was not due to a loss of position sense (which was normal) but to unsteady muscle contractions. Deep sensations were normal.
There were no mental symptoms. There was a slight hesitation in speech and doubling of syllables, but nothing demonstrable with test phrases.
There were no mental symptoms. There was a slight hesitation in speech and a doubling of syllables, but nothing that could be demonstrated with test phrases.
The serum W. R. was positive.
The serum W. R. tested positive.
Shell explosion; unconsciousness: Neurosyphilis.
Shell explosion; unconscious: Neurosyphilis.
Case 24. (Hurst, April, 1917.)
A private, 31, was in the retreat from Mons, was blown up by a shell and buried in May, 1915, went back to the front after two months leave, was knocked unconscious by a shell December, 1916. He came to himself two days later in the hospital, but remained confused and lethargic. In England, December 21, his legs were still weak and walking was unsteady. The right pupil reacted neither to light nor to accommodation and was irregular, eccentric, and dilated. The left pupil showed the Argyll-Robertson reaction. There was early primary optic atrophy. The right knee-jerk was slightly exaggerated. The vibration sense was reduced over sacrum and malleoli. At this time the man’s mental condition was practically normal.
A private, 31, was retreating from Mons when a shell exploded and buried him in May 1915. He returned to the front after two months of leave but was knocked unconscious by another shell in December 1916. He regained consciousness two days later in the hospital but felt confused and lethargic. In England, on December 21, his legs were still weak and his walking was unsteady. The right pupil didn’t react to light or focus and was irregular, off-center, and dilated. The left pupil had the Argyll-Robertson reaction. There was early primary optic atrophy. The right knee-jerk reflex was slightly exaggerated. Vibration sense was reduced over the sacrum and malleoli. At this time, the man’s mental condition was nearly normal.
The Wassermann reaction of the serum and spinal fluid proved positive. Improvement followed rest, iodide, mercury, and seven injections of salvarsan. By the middle of February he was able to walk well. The right pupil regained its power to react to accommodation, but remained inactive to light. Meanwhile, the left pupil had regained a slight power to react to light.
The Wassermann test on the serum and spinal fluid came back positive. After some rest, treatment with iodide and mercury, and seven injections of salvarsan, he started to improve. By mid-February, he could walk well. The right pupil regained its ability to react to changes in focus but still didn’t react to light. In contrast, the left pupil had regained a little ability to respond to light.
Re treatment of syphilis, both Thibierge and Lépine give warning of some bad results with arsenobenzol treatment, though Thibierge states that the number of serious accidents and especially of deaths has diminished more and more now that no arsenobenzol (drug No. 914) is given. Encephalitis is the gravest of the untoward results of injection, sometimes appearing in young and vigorous subjects. Hemorrhagic encephalitis appears to occur more frequently after the second injection than after the first, and according to Thibierge may be especially suspected in subjects who after the first injection present much fever, congestion of face, and cutaneous eruptions. Treatment in these cases should be suspended or given in moderate doses.
Re treatment of syphilis, both Thibierge and Lépine warn of some negative outcomes with arsenobenzol treatment, although Thibierge mentions that the number of serious incidents, particularly deaths, has increasingly declined now that no arsenobenzol (drug No. 914) is administered. Encephalitis is the most severe of the adverse effects from injection, sometimes occurring in young and healthy individuals. Hemorrhagic encephalitis seems to happen more often after the second injection than after the first, and according to Thibierge, it should be especially suspected in individuals who experience high fever, facial congestion, and skin eruptions after the first injection. In these cases, treatment should be paused or given in moderate doses.
Shell-explosion: Neurosyphilis. Fit for light duty.
Shell-explosion: Neurosyphilis. Able to perform light tasks.
Case 25. (Hurst, April, 1917.)
A corporal, 26, blown up by a shell December 7, 1916, was admitted to the hospital on the 13th, dazed and with symptoms of a left-sided hemiplegia of organic origin. The right pupil was larger than the left. There was a bruise of the scalp in the right parietal region. The man had had syphilis at 16. The Wassermann reaction of the serum was strongly positive. Rest, salvarsan, mercury, and iodides were given, and the general symptoms and hemiplegia gradually disappeared, until on December 12 there was only a moderate weakness of the left side, with knee-jerks in excess, abdominal reflexes absent, and the Babinski reaction.
A 26-year-old corporal, injured by a shell explosion on December 7, 1916, was admitted to the hospital on the 13th, confused and showing signs of a left-sided hemiplegia of organic origin. His right pupil was larger than the left. There was a bruise on the scalp in the right parietal region. The man had a history of syphilis at 16. The Wassermann test on his serum was strongly positive. He was treated with rest, salvarsan, mercury, and iodides, and over time, the general symptoms and hemiplegia gradually improved, until by December 12, he exhibited only moderate weakness on the left side, with hyperactive knee-jerks, absent abdominal reflexes, and a positive Babinski sign.
The Wassermann reaction was still strongly positive. Salvarsan, mercury, and iodide were continued. January 6, 1917, the plantar reflex had become flexor. The abdominal reflex returned. Babinski’s second sign (combined flexion of thigh and pelvis) was now the only evidence of organic disease. Further antisyphilitic treatment removed this sign also. February 28, the man was discharged fit for light duty, with unequal pupils and positive Wassermann reaction, and a complete amnesia for the four weeks following his blowing up in the trenches.
The Wassermann test was still very positive. Salvarsan, mercury, and iodide continued to be administered. On January 6, 1917, the plantar reflex had turned to a flexor response. The abdominal reflex returned. Babinski’s second sign (the combined flexion of the thigh and pelvis) was now the only sign of organic disease. Further antisyphilitic treatment eliminated this sign as well. On February 28, the man was discharged as fit for light duty, with unequal pupils and a positive Wassermann test, and he had complete amnesia for the four weeks after he was blown up in the trenches.
Re fitness for light duty, see remarks on Case 20 concerning desk duty for certain tabetics.
Re fitness for light duty, see comments on Case 20 regarding desk duty for certain tabetics.
Re the premature or unexpectedly early appearance of neurosyphilis under war conditions, the early claims of some authors have not been maintained. In the above instance, the infection was at 16 and the shell explosion occurred at 26, namely, at about the right interval for the development of neurosyphilitic signs. Gerver states that military service brings out the lesions of paresis earlier than they would otherwise come. Bonhoeffer has been unable to show that cerebrospinal syphilis is favored in its development by the exhaustion factor.
Re the premature or unexpectedly early appearance of neurosyphilis under wartime conditions, the initial claims of some authors have not held up. In this case, the infection was present at 16, and the shell explosion happened at 26, which is about the right time frame for the development of neurosyphilitic symptoms. Gerver notes that military service reveals the lesions of paresis sooner than they would typically appear. Bonhoeffer has not been able to demonstrate that the exhaustion factor promotes the development of cerebrospinal syphilis.
SHELL-SHOCK PSEUDOPARESIS (non-syphilitic). Recovery.
SHELL-SHOCK PSEUDOPARESIS (non-syphilitic). Recovery.
Case 26. (Pitres and Marchand, November, 1916.)
June 19, 1915, a shell exploded some distance from Lieutenant R. He remembers the gaseous smell, the bursting of several shells nearby and a sensation of being lifted into the air. When he recovered consciousness, he was in hospital at Paris-Plage, covered with bruises and scratches. They told him he had been delirious and had vomited and spat blood.
June 19, 1915, a shell went off some distance away from Lieutenant R. He recalls the smell of gas, the explosions of several shells nearby, and the feeling of being lifted into the air. When he came to, he was in a hospital in Paris-Plage, covered in bruises and scratches. They told him he had been delirious and had vomited and coughed up blood.
June 24, his wife came to see him, but this visit he could not remember. Nor could his wife at first recognize him, he was so thin. He roused a few moments and recognized his wife, but relapsed into torpor again. Speech was difficult and ideas confused.
June 24, his wife came to see him, but he couldn't remember the visit. Nor could his wife recognize him at first; he was so thin. He was briefly alert and recognized her, but then slipped back into a daze. Speaking was hard, and his thoughts were jumbled.
A few days later he was able to rise; but his mental status grew worse, especially as to speech and writing, the latter quite illegible. There was insomnia, or, if he slept, war dreams.
A few days later, he was able to get up; but his mental state got worse, especially concerning his speech and writing, which was now barely readable. He had insomnia, or if he did manage to sleep, he had nightmares about war.
August 7, he began a period of five months’ convalescence passed with his family, depressed, given to spells of weeping, confined to bed or couch, unable to “find words,” conscious of his state and troubled about it, speaking of nothing but the war, and afraid to go out for fear of ambuscade. There was at first a slight lameness of the right leg. Although he could walk, he felt pain in the knee on flexing the right leg on the thigh. He walked holding this leg in extension.
On August 7, he started a five-month recovery period spent with his family. He felt down, had bouts of crying, and was mostly stuck in bed or on the couch. He couldn’t find the words to express himself and was aware of his condition, which made him anxious. He only talked about the war and was scared to go outside because he feared an ambush. At first, there was a slight limp in his right leg. Even though he could walk, he felt pain in his knee when bending his right leg at the thigh. He walked with that leg extended.
On going back to the colors, he was immediately evacuated to the Centre Neurologique at Bordeaux, January 20, 1916.
On returning to the colors, he was quickly taken to the Centre Neurologique in Bordeaux, January 20, 1916.
Examination found a bored, impatient, irritated man, vexed that a man who was not sick should be sent up “comme fou.”
Examination found a bored, impatient, irritated man, frustrated that a healthy person should be sent up “comme fou.”
Omitting negative details, neurological examination showed slight lameness as above, body stiff and movements jerky, difficult, unsteady gait. The lieutenant could stand for some time on either leg. Tongue and face tremulous during speech. Limbs moderately tremulous, especially in the performance of test movements.
Omitting negative details, the neurological exam showed slight limping as mentioned, the body was stiff and movements were jerky, with a difficult, unsteady walk. The lieutenant could stand for a while on either leg. His tongue and face trembled during speech. His limbs were moderately shaky, especially when performing test movements.
Knee-jerks and Achilles jerks absent. Other reflexes, including pupillary, normal. Segmentary hypalgesia of right leg, especially about knee. Tremulous speech and writing. Patient would stop short in speaking for lack of words.
Knee-jerk and Achilles reflexes missing. Other reflexes, like the pupillary response, are normal. There's reduced sensitivity to pain in the right leg, particularly around the knee. The patient speaks and writes with trembling. They often pause mid-sentence because they can't find the words.
Malnutrition. Appetite good, but a bursting feeling after meals.
Malnutrition. Good appetite, but feels overly full after meals.
Skin dry, scaly on legs, fissured on fingers.
Skin dry, scaly on the legs, cracked on the fingers.
Serum W. R. negative. Fluid not examined.
Serum W. R. negative. Fluid not tested.
Mental examination. Conscious and complaining of his troubles, Lieutenant R. claimed persistently that he was not sick. Memory for recent events was in general poor. Errands easily forgotten. Lost in the street. Complaint of corpse odors round him. Everybody is looking at him and making fun of him. He was apt to insult bystanders. He was afraid of German spies. Things in shops angered him as they seemed to him to be of German manufacture.
Mental examination. Aware of his issues and voicing his concerns, Lieutenant R. repeatedly insisted that he wasn’t sick. His memory for recent events was generally weak. He often forgot errands. He got lost on the street. He complained of smelling corpse odors around him. He felt like everyone was watching and mocking him. He tended to insult people nearby. He was paranoid about German spies. He became angry at items in stores because they seemed to be German-made.
There were frequent periods of depression, with pallor and no spontaneous speech for some hours to a half-day. Headaches coming on and stopping suddenly.
There were frequent episodes of depression, characterized by a pale appearance and lack of spontaneous speech that could last for hours to half a day. Headaches would start and stop suddenly.
As to diagnosis, the first impression, say Pitres and Marchand, was that of general paresis. The progress of symptoms after the shock was consistent with this diagnosis. The mental state and the physical findings seemed consistent, although the pupils were normal. His partial insight into his symptoms was not inconsistent with the diagnosis. He had a characteristic self-confidence. There had been four stillbirths (two twins); two children are alive, 11 and 13. Typhoid fever at 30. Syphilis denied. No mental disease in the family.
Regarding the diagnosis, Pitres and Marchand's initial impression was that of general paresis. The way the symptoms progressed after the shock aligned with this diagnosis. The mental state and physical findings appeared to match up, even though the pupils were normal. His partial understanding of his symptoms did not contradict the diagnosis. He exhibited a typical level of self-confidence. There had been four stillbirths (two being twins); two children are currently alive, aged 11 and 13. He had typhoid fever at 30. He denied having syphilis. There was no history of mental illness in the family.
The patient had never done military duty, having been invalided for “right apex.” But he had volunteered and been accepted in September, 1914.
The patient had never served in the military because he had been discharged for “right apex.” However, he had volunteered and was accepted in September 1914.
How was Lieutenant R. cured? Apparently by rest in the Centre Neurologique. Pitres and Marchand do not speak of the subtle relation between mental state and the idea of non-return to military service. This motive might still work even if Lieutenant R. kept protesting sincerely that he wanted to go back into military service.
How did Lieutenant R. recover? It seems it was through resting at the Centre Neurologique. Pitres and Marchand don't mention the delicate connection between mental state and the thought of not returning to military service. This factor could still influence him, even if Lieutenant R. consistently claimed he truly wanted to return to military service.
War strain; shell explosion; unconsciousness. Sensory and motor disorders. Subject an old syphilitic.
War stress; bomb blast; loss of consciousness. Sensory and motor issues. Subject is an elderly syphilitic.
Case 27. (Karplus, February, 1915.)
A captain, 34, was under much stress and strain in the field and gave himself over to excesses of alcohol and tobacco. August 25, 1914, at the Krasnik battle he suddenly saw at his right a gleam of fire and was afterward able to remember very distinctly the words of a lieutenant standing near by, “The man is dead.” Three or four hours later he came to himself at a relief post, vomited and bled a good deal from nose and mouth. He heard later that he had been thrown on his back.
A 34-year-old captain was feeling a lot of stress on the battlefield and turned to drinking and smoking to cope. On August 25, 1914, during the battle of Krasnik, he suddenly noticed a flash of fire to his right and clearly recalled a lieutenant nearby saying, “The man is dead.” A few hours later, he regained consciousness at a first aid station, vomited, and bled quite a bit from his nose and mouth. He later learned that he had been knocked onto his back.
Manual tremors and general pains developed in the next few days. Two weeks after the accident a slight nystagmus on looking to the left appeared, but there was otherwise no disorder of head or extremities. He was able to sit up, supported by his arms, and he was able to contract his abdominal muscles normally. As for his legs, active movements were limited and weak. He could not lift his legs. The paralysis was more marked distally. He could walk with the support of two persons, but was unable to lift his feet from the ground. The right upper abdominal reflex was elicited, and both patellar reflexes were tolerably active. Cremasteric and plantar reflexes were absent. Neither of the Achilles jerks could be produced. There was hypesthesia and hypalgesia of the lower extremities, and of the back up to a horizontal line corresponding with the ninth dorsal segment; thermo-hyperesthesia and disorder of vibration sense in the lower legs. Both the motor and the sensory disorders were more marked on the right than the left. Insomnia and battle dreams.
Manual tremors and general pain developed over the next few days. Two weeks after the accident, a slight nystagmus appeared when looking to the left, but there were no other issues with his head or limbs. He could sit up, supported by his arms, and he could contract his abdominal muscles normally. However, his leg movements were limited and weak; he couldn’t lift his legs. The paralysis was more pronounced distally. He could walk with the help of two people but couldn't lift his feet off the ground. The right upper abdominal reflex was present, and both patellar reflexes were fairly active. The cremasteric and plantar reflexes were absent, and neither of the Achilles reflexes could be triggered. There was reduced sensitivity and pain in his lower extremities and back up to a horizontal line around the ninth dorsal segment, along with heightened sensitivity to temperature and problems with vibration sense in the lower legs. Both motor and sensory issues were more prominent on the right than the left. He also experienced insomnia and vivid war-related dreams.
The gait disorder and paresis gradually improved. There was no alimentary glycosuria and adrenalin produced no mydriasis. In the course of several weeks the patient gained seven kilograms, began to sleep well and showed gradual[35] improvement in his gait and in the execution of various movements with his feet. The abdominal reflexes were now both present, but there were no plantar reflexes and the Achilles were still both absent. The sensory disorder remained unchanged, so far as the skin was concerned, but the deep sensibility improved. Both legs from the knee down were somewhat cold.
The walking disorder and weakness slowly got better. There was no sugar in the urine after eating, and adrenaline didn't cause any pupil dilation. Over the course of several weeks, the patient gained seven kilograms, started sleeping well, and showed gradual[35] improvement in his walking and in performing various movements with his feet. The abdominal reflexes were now both present, but there were still no plantar reflexes, and the Achilles reflexes were absent. The sensory issues with the skin stayed the same, but deep sensation improved. Both legs from the knee down were a bit cold.
This man had had syphilis at twenty-two, had gone through an inunction cure, and repeated W. R.’s came through negative. He had suffered from vomiting spells and anxiety feelings for a number of years which had been diagnosed by physicians as cardiac neurosis. Yet for a year before going into the war he had felt absolutely well.
This man had syphilis at twenty-two, went through an ointment treatment, and had repeated tests that came back negative. He experienced vomiting spells and feelings of anxiety for several years, which doctors diagnosed as cardiac neurosis. However, for a year before he went to war, he felt completely healthy.
Shell-explosion: Amnesia; syphilitic hemiplegia. Recovery except for amnesia as to brief period and loss of occupational skill.
Shell explosion: Memory loss; paralysis on one side from syphilis. Recovery except for memory loss about the brief period and a decline in job skills.
Case 28. (Mairet and Piéron, July, 1915.)
A man of 40 underwent shell shock June 15, 1915, and had no remembrance of what happened up to July, 1915, when in hospital at Tunis he felt “born again.”
A 40-year-old man experienced shell shock on June 15, 1915, and couldn't remember anything that happened until July 1915, when he felt “born again” while in a hospital in Tunis.
Examined in January, 1916, it was found that he had a left hemiplegia (in fact, he had a syphilitic hemiplegia on that side, several years before, which had disappeared under antisyphilitic treatment). This hemiplegia passed, but he then had crises of depression due to his despair at not being able to know who he was and what he was doing. He could speak French and Spanish, and knew from the hospital ticket that he was born in Spain; but he had no idea what had happened to his relatives or what he was doing in France. He had, however, a very correct idea of what happened during six months after July, 1915.
Examined in January 1916, it was discovered that he had a left hemiplegia (in fact, he had experienced a syphilitic hemiplegia on that side several years earlier, which had disappeared with antisyphilitic treatment). This hemiplegia resolved, but he then experienced bouts of depression due to his despair over not knowing who he was or what he was doing. He could speak French and Spanish and knew from the hospital record that he was born in Spain; but he had no idea what had happened to his relatives or why he was in France. However, he had a clear understanding of what occurred during the six months after July 1915.
One morning in April, 1916, his old memories came back all of a sudden on waking. The gap was filled up to the moment of the shock. There was no gap left except for a period of about 25 days following the shock. He now found that he knew a little English but that he had lost his stenography as well as his professional skill at typewriting.
One morning in April 1916, his old memories suddenly came rushing back as he woke up. The missing pieces were filled in up to the moment of the shock. The only gap left was about 25 days after the shock. He realized that he knew a little English now, but he had lost his shorthand skills as well as his professional typing abilities.
Re French statistics for the occurrence of general paresis, Lautier found 27 cases in 426. Early in the war, Boucherot at Fleury received four cases of paresis among 107 cases; the majority of these, however, had not left the interior. Consiglio in Italy received two cases out of 270.
Re French statistics for the occurrence of general paresis, Lautier found 27 cases in 426. Early in the war, Boucherot at Fleury received four cases of paresis among 107 cases; most of these, however, had not left the interior. Consiglio in Italy received two cases out of 270.
Re hemiplegia in this case, it may be inquired whether the hemiplegia which developed after the shell explosion on the same side of the body on which the patient had a true syphilitic hemiplegia, was really syphilitic or not. Was it not, perhaps, in some sense psychogenic? A similar question may be raised concerning cases in which the locus minoris resistentiae becomes the site of symptoms. See Cases 409-414.
Re hemiplegia in this case, it's worth asking whether the hemiplegia that developed after the shell explosion on the same side of the body where the patient had true syphilitic hemiplegia was actually syphilitic or not. Could it have been, in some way, psychogenic? A similar question can be raised about cases in which the locus minoris resistentiae becomes the site of symptoms. See Cases 409-414.
Shell-shock: Hysterical blindness. Signs of cerebrospinal syphilis: Nevertheless, amaurosis functional.
Shell-shock: Hysterical blindness. Signs of cerebrospinal syphilis: Nevertheless, functional amaurosis.
Case 29. (Laignel-Lavastine and Courbon, March, 1916.)
A soldier of the class of 1906 underwent shell-shock August 13, 1914, regaining consciousness 20 days later, but blind. The light of the shellburst, he said, was the last thing he had seen.
A soldier from the class of 1906 experienced shell shock on August 13, 1914, and woke up 20 days later, but he was blind. He said that the flash from the shell explosion was the last thing he saw.
For sixteen months, he was transferred from hospital to hospital, looked on sometimes as blinded; sometimes as feigning. Finally, on the isolation service of Maison-Blanche, December 15, 1915, he received an ophthalmologist’s diagnosis namely, hysterical amaurosis. At this time there were found: stereotyped winking, with slight lachrymation, a slight left external strabismus, limitation in movement of all the extrinsic muscles of both eyes, especially to the right and in convergence and elevation; pupils slightly smaller than normal—and the general impression of a genuinely blinded or amblyopic subject. He seemed to be able to distinguish faint whitish spots, without contour or color, in objects brought to a distance of at least 40 cm.
For sixteen months, he was moved from one hospital to another, sometimes being viewed as genuinely blind and other times as pretending. Finally, on the isolation service at Maison-Blanche, on December 15, 1915, an ophthalmologist diagnosed him with hysterical amaurosis. At that time, the following symptoms were noted: repetitive winking with slight tearing, a mild left outward eye turn, limited movement in all the external muscles of both eyes—especially to the right and when trying to converge and elevate them; pupils slightly smaller than normal—and the overall impression of someone who was genuinely blind or had poor vision. He appeared to be able to make out faint whitish spots, lacking clear shape or color, in objects held at least 40 cm away.
He also complained of bad feelings inside his head on the left side, and he proved to have a left-sided hemianesthesia of hysterical nature. There were no other sensory disorders and no reflex disorders.
He also mentioned feeling uncomfortable on the left side of his head, and it turned out he had left-sided hemianesthesia of a hysterical nature. There were no other sensory issues or reflex problems.
The nasolabial fold on the left side was flattened out, and there was also on the same side a slight diminution in the lower abdominal skin reflexes, and no response to plantar stimulation. Examination of the mouth showed leucoplakia, and the history showed that the man’s fifth child was born before term and died at two months. Lumbar puncture yielded lymphocytosis (55 cells) and an excess of albumin. The fundus examination showed a slight papillary disorder, suggesting a retrobulbar affection of the optic nerves.
The nasolabial fold on the left side was flattened, and there was also a slight decrease in the lower abdominal skin reflexes on that side, with no response to plantar stimulation. Examining the mouth revealed leucoplakia, and the patient's history indicated that his fifth child was born prematurely and passed away at two months old. A lumbar puncture showed lymphocytosis (55 cells) and elevated albumin levels. The fundus examination indicated a slight papillary disorder, suggesting an issue with the optic nerves behind the eyes.
However, the preservation of the pupil reflexes seemed to indicate that nine-tenths, at least, of the amaurosis was[38] functional. After mercurial treatment the headache grew less and the man was able to see somewhat better with his right eye.
However, the preservation of the pupil reflexes seemed to indicate that at least nine-tenths of the amaurosis was[38] functional. After receiving mercurial treatment, the headache lessened and the man was able to see a bit better with his right eye.
Laignel-Lavastine and Courbon suggest that there was a dynamic disorder in this case, bearing the same relation to vision as mental confusion bears to the process of ideation. Analogous phenomena have been found in the sense of hearing, in such wise that the victims can, as it were, passively hear but do not listen.
Laignel-Lavastine and Courbon suggest that there was a dynamic disorder in this case, similar to how mental confusion relates to the process of thinking. Similar phenomena have been observed in the sense of hearing, where the victims can, in a way, hear passively but do not actually listen.
Re functional eye cases, see below, especially Cases 432-437.
For functional eye cases, see below, especially Cases 432-437.
Shell shock (functional) phenomena in a syphilitic.
Shell shock (functional) phenomena in a syphilitic.
Case 30. (Babonneix and David, June, 1917.)
A marine, 26, on land service March, 1916, was buried by the explosion of a large calibre shell which killed most of his comrades. He remained for a time in a sort of lethargy. Coming to, he found himself victim of a right hemiplegia and deafmutism, which phenomena vanished under electricity.
A 26-year-old marine, stationed on land in March 1916, was buried by the blast of a large-caliber shell that killed most of his fellow soldiers. He was in a kind of daze for a while. When he regained consciousness, he discovered he was suffering from right-sided paralysis and deaf-muteness, but those issues disappeared with electrical treatment.
In July, however, he had to be sent to a hospital on account of his sufferings, which received the diagnoses commotio cerebri, disorder of consciousness, disorientation, delirium, amnesia, over-emotionality. He was sent back to the front in December, 1916, but promptly reported sick, with headaches and insomnia.
In July, however, he had to be taken to a hospital due to his suffering, which was diagnosed as commotio cerebri, a disorder of consciousness, disorientation, delirium, amnesia, and heightened emotionality. He was sent back to the front in December 1916, but quickly reported being unwell, experiencing headaches and insomnia.
Examination showed nonorganic nervous disorders, consisting in a variable and patchy anesthesia of the legs, anesthesia of the conjunctiva and pharynx, and over-reaction, with sighing, during the course of the examination. The organic signs were: exaggeration of tendon reflexes, equilibration disorder, and incapacity to stand on one foot or execute a half turn or to stand still with eyes closed, and disorder of position sense. The lumbar puncture showed no cells, a slight globulin reaction, and an albumin titer within the normal. There was a leucoplakia and a positive W. R. The man was emaciated, febrile, and showed signs, with the X-ray, of bronchial lymph node disease. According to Babonneix and David, the normality of the fluid indicates that the phenomena here were Shell-shock phenomena, despite the indisputable syphilis of the blood serum.
Examination revealed non-organic nervous disorders, including variable and patchy numbness in the legs, numbness of the conjunctiva and pharynx, and overreactions, such as sighing, during the examination. The organic signs were: exaggerated tendon reflexes, problems with balance, inability to stand on one foot or turn halfway, and difficulty standing still with eyes closed, as well as issues with position sense. The lumbar puncture showed no cells, a slight globulin reaction, and an albumin level within the normal range. There was leukoplakia and a positive Wassermann reaction. The man was emaciated, had a fever, and X-rays indicated bronchial lymph node disease. According to Babonneix and David, the normality of the fluid suggests that these symptoms were due to shell shock, despite the clear presence of syphilis in the blood serum.
Re occurrence of functional phenomena in syphilitics, Freud’s remark may be recalled to the effect that a large proportion of his hysterics and other psychoneurotics are the offspring of syphilitics.
Re occurrence of functional phenomena in syphilitics, Freud’s observation can be remembered that many of his hysterics and other psychoneurotics come from syphilitics.
Consider in this connection also Case 28: an old syphilitic hemiplegia was followed by a probably psychogenic or hysterical hemiplegia on the same side.
Consider in this context also Case 28: an old syphilitic hemiplegia was followed by what was likely a psychogenic or hysterical hemiplegia on the same side.
Vestibular symptoms in a neurosyphilitic.
Vestibular symptoms in neurosyphilis.
Case 31. (Guillain-Barré Syndrome and Barré, April, 1916.)
A soldier, Colonial, 29, was twice in the 6th Army neurological centre. The first time, February, 1916, he was under observation for astasia-abasia, having been invalided twice for this disease,—once in 1915. This man had had syphilis at 21, and was then taken care of at Saint-Louis Hospital and at Cochin. A volunteer for the duration of war, September, 1914, he had intermittent disorders of station and walking, which caused his invaliding January, 1915. As the trouble stopped, he asked to go back to the front in September, but the same difficulty reappeared with fatigue, and he was sent to the army neurological centre. When standing, there was a ceaseless trembling of the whole body but especially of the legs, with tendency to propulsion. In walking also, there was a trepidant abasia, sometimes dizziness, and even a sudden fall. Standing on one foot he trembled and fell.
A soldier, 29 years old, was admitted twice to the 6th Army neurological center. The first time was in February 1916, where he was observed for astasia-abasia, having been discharged twice for this condition—once in 1915. This man had syphilis at 21, and received treatment at Saint-Louis Hospital and Cochin. He volunteered for the war in September 1914 and experienced intermittent issues with standing and walking, which led to his discharge in January 1915. When the problems subsided, he requested to return to the front in September, but the same difficulties returned with fatigue, resulting in him being sent back to the army neurological center. While standing, he had constant trembling all over, particularly in his legs, with a tendency to lean forward. In addition, he exhibited shaky walking, occasional dizziness, and even sudden falls. When trying to stand on one foot, he shook and fell.
Examined on his back, muscular strength was found intact in all limbs, and there was no trembling or incoördination or intention tremor in the performance of any movements, though there was a slight trembling of the raised fingers and hand. Reflexes were normal. The right pupil was dilated; the left pupil reacted sluggishly. There were lateral nystagmiform movements to the left. Caloric nystagmus appeared from the right ear in 15 seconds, from the left in 30. Rotatory nystagmus appeared in 35 seconds on both sides. Lumbar puncture yielded a fluid with a slight lymphocytosis; albumin, .3 grams; chloride, 7.30; sugar normal.
When examined lying on his back, all limbs showed normal muscular strength, with no trembling, lack of coordination, or intention tremor during movements, although there was slight shaking in the raised fingers and hand. Reflexes were normal. The right pupil was dilated, while the left pupil reacted slowly. There were side-to-side movements of the eyes to the left. Caloric nystagmus occurred from the right ear in 15 seconds and from the left in 30 seconds. Rotatory nystagmus appeared in 35 seconds on both sides. A lumbar puncture produced fluid with slight lymphocytosis; albumin was 0.3 grams; chloride was 7.30; and sugar levels were normal.
Rest in bed improved the astasia-abasia, and the man was sent back to his corps, February 20, 1916. He came back March 16, having had a dizzy spell, with suffocation feeling and a fall, whereupon the trepidant astasia-abasia had reappeared. There were none of the so-called defensive reflexes. The neuromuscular excitability of gastrocnemii was less on the right than on the left. A von Graefe sign was sometimes found; no diplopia save on looking far to right.
Resting in bed improved the astasia-abasia, and the man was sent back to his unit on February 20, 1916. He returned on March 16, having experienced a dizzy spell, a sensation of suffocation, and a fall, causing the astasia-abasia to come back. There were none of the so-called defensive reflexes. The neuromuscular excitability of the calves was lower on the right than on the left. A von Graefe sign was sometimes present; no double vision except when looking far to the right.
Lay reflections on syphilis: Suicidal attempts.
Lay reflections on syphilis: Suicidal attempts.
Case 32. (Colin and Lautier, July, 1917.)
A man was called to the auxiliaries at the outbreak of the war, and served as stretcher-bearer at the Marne. He then became an attendant at the Grand-Palais. Acquiring gonorrhoea, he was cared for but he grew depressed. The blood was examined and the W. R. found positive. The physician immediately made known the result without circumlocution, and knowing vaguely that the W. R. meant syphilis, the patient felt an irresistible impulse to suicide, and cut his throat. It seems that he had often before said that if he got syphilis he would kill himself. Recovering from his wound, he was invalided to Villejuif, Sept. 19, 1916, breathing through a cannula and responding to questions in writing. He had always been a nervous and emotional man, a farmer in Auvergne; he was married and the father of several children.
A man was called to the auxiliary forces when the war started and served as a stretcher-bearer at the Marne. He then became an attendant at the Grand-Palais. After contracting gonorrhea, he received treatment but fell into a depression. His blood was tested, and the test for syphilis came back positive. The doctor told him the results directly, and realizing that the positive result meant syphilis, the patient felt an overwhelming urge to end his life and cut his throat. He had often said before that if he got syphilis, he would commit suicide. After recovering from his injury, he was sent to Villejuif on September 19, 1916, breathing through a cannula and responding to questions in writing. He had always been a nervous and emotional man, a farmer from Auvergne; he was married and had several children.
Examination showed that the recurrent nerves had been cut and that the man must needs always breathe through the cannula. In point of fact, the W. R., only partially positive at the outset, did not indicate syphilis, and the gonorrhoea was now cured. But though the patient knew these facts, his hypochondria persisted, basing itself upon the suicidal wound. He said that his larynx had been stolen and he wondered why. He said that he had violent crises of suffocation, though there was, as a matter of fact, no difficulty with his breathing. Verdigris, he said, was forming on his cannula. Self-accusations about the suicide developed. On being transferred to his department asylum, he made a suicidal attempt on the trip.
Examination revealed that the recurring nerves had been severed, and the man would always need to breathe through the cannula. In reality, the W. R., which was only partially positive at first, did not indicate syphilis, and the gonorrhea was now cured. But even with this knowledge, the patient's hypochondria continued, rooted in the suicide attempt. He claimed that his larynx had been taken from him and wondered why. He stated that he experienced severe episodes of suffocation, even though he was actually not having any breathing issues. He mentioned that verdigris was forming on his cannula. He began to self-blame regarding the suicide. When he was moved to his department asylum, he attempted to commit suicide during the transfer.
Of course the gonorrhoea may have served as a partial factor in the genesis of the case, and his own mental attitude toward the contraction of syphilis may have been another factor.
Of course, gonorrhea might have played a role in the development of the case, and his own mindset about contracting syphilis could have been another factor.
The imitation of chancre.
The mimicry of chancre.
Case 33. (Choose, July, 1916.)
A married German farmer, 32, was in Prague hospital in 1908 during his period of military service and was then treated by inunction for a local chancre. He was given mercurial injections a year later for rash.
A 32-year-old married German farmer was in a hospital in Prague in 1908 during his military service and was treated with ointment for a local sore. A year later, he received mercury injections for a rash.
In 1912, he had signs of syphilis in the mouth.
In 1912, he showed signs of syphilis in his mouth.
He was sent home from service in 1913, with ulcers of hand.
He was sent home from service in 1913 due to hand ulcers.
At the beginning of the war he was found to have ulcers on the knee, legs, and mouth, and was sent home for six months.
At the start of the war, he was discovered to have ulcers on his knee, legs, and mouth, and was sent home for six months.
Again called up in 1915, the ulcers were still in evidence; he got inunctions in a military hospital four months.
Again called up in 1915, the ulcers were still noticeable; he received treatments in a military hospital for four months.
He was sent to his corps in July and had no relapse until July, 1916, when he was detailed for active service. Thereupon, ulcers began on the left hand and right leg. He reported sick, but was sent nevertheless to the front. In hospital he was found to have several scars about one inch across on each leg, on the dorsum of the left hand, at the right of the left index finger, and elsewhere. These scars were deeply pigmented. One of them was square! There were other recent ulcers that closely resembled tertiary ulcers. The most recent of these ulcers was angular, intensely red, and showed remains of a collapsed vesicle. There was a deep dark scab on the mucous membrane of the left cheek.
He was sent to his unit in July and didn't have any issues until July 1916, when he was assigned to active duty. Then, ulcers started appearing on his left hand and right leg. He reported being unwell, but still got sent to the front lines. In the hospital, they discovered several scars about an inch across on each leg, on the back of his left hand, to the right of his left index finger, and in other areas. These scars were heavily pigmented. One of them was square! There were also some recent ulcers that looked a lot like tertiary ulcers. The newest of these ulcers was angular, very red, and showed signs of a collapsed blister. There was a deep dark scab on the mucous membrane of his left cheek.
There is no doubt that these ulcers were produced by some caustic, the nature of which remains unknown. The patient had, however, been able to evade military obligation during peace time and for two years during war time.
There’s no doubt that these ulcers were caused by some kind of corrosive substance, the exact nature of which is still unknown. The patient, however, had managed to avoid military duty during peacetime and for two years during wartime.
Re simulation, according to Pick, some 5 to 7 per cent venereal diseases in the German army have been simulations. Gonorrhoea is simulated by soap, balanitis by cantharides, soft chancre by soap and mercuric or mercurous chloride mixed, hard chancre by a fluid or powder containing NaOH, Na2CO, and NaCl. Secondary syphilitic signs are imitated by cantharides or garlic, producing scrotal dermatitis. Tertiaries are imitated with caustics.
Re simulation, according to Pick, about 5 to 7 percent of venereal diseases in the German army have been simulated. Gonorrhea is faked using soap, balanitis with cantharides, soft chancre with a mix of soap and mercuric or mercurous chloride, and hard chancre with a fluid or powder containing NaOH, Na2CO, and NaCl. Secondary signs of syphilis are imitated with cantharides or garlic, which cause scrotal dermatitis. Tertiary symptoms are faked with caustics.
Ramón to Rosina: a soldier’s letter to his fiancée.
Ramón to Rosina: a soldier's letter to his girlfriend.
Case 34. (Buscaino and Coppola, January, 1916.)
“I am here to stay a month. Believe me, it is better here than in the army. There is a rule that we may eat as much as we can and everything is of the very best. The servants treat us like brothers. Do not think it is a nuisance to be inside four walls with a wee bit of a garden. No, indeed! But I have got to act the fool and from the very first day I began to play and act crazy with a kitten, so that if you had seen me you would say: “Ramón is really crazy.” Rosina, dear, to avoid paying taxes you have got to be a smuggler. And now that I am at the ball I have got to dance. I want to see if after all the suffering I cannot get something better. I am better off here than at the regiment. I sleep in a fine warm bed, and they have only cold straw; I have good food and drink and plenty of milk, and they have poor food and drink and so little.
“I’m here for a month. Trust me, it’s way better here than in the army. We can eat as much as we want, and the food is top-notch. The staff treats us like family. Don’t think it’s a hassle being cooped up with just a small garden. Not at all! But I have to act silly, and from day one, I started playing around with a kitten, so if you saw me, you’d think: “Ramón is really out of his mind.” Rosina, dear, to avoid paying taxes, you have to be a smuggler. And now that I’m at the ball, I have to dance. I want to see if after all the hardships, I can manage to get something better. I’m better off here than at the barracks. I sleep in a nice warm bed, while they have only cold straw; I have good food and drink and lots of milk, and they have poor meals and barely any.”
“I expect to go home in about three weeks. I would have been there before if some fool of a spy at our place had held his tongue and minded his own business. At the same time, Rosina, dear, remember what I told you at Leghorn: that they had some officers sent there to get information and instead of going home they asked somebody else and were told that I had never been sick and had never had neurasthenia. When this information was got from the officers I was called to the office and they read to me that all that I had said and done was not true. I kept on acting the fool, and as they were still doubtful they sent me here, where there is a professor who passes me every morning in the garden and says: “How are you?” I always say: “I am the same,” acting like a crazy man. Let me tell you, Rosina dear, not to say anything contrary to this in your letters because they open and read everything in order to find out everything that happens and everything that is said. Now what you must do is to ask me how I am feeling, and whether my headaches are gone, and whether I have them all the time as formerly, and any other trifle that will help me.”
“I expect to go home in about three weeks. I would have been there sooner if some idiot of a spy at our place had kept his mouth shut and minded his own business. At the same time, Rosina, dear, remember what I told you in Leghorn: they sent some officers there to gather information, and instead of going home, they asked someone else and were told that I had never been sick and never had neurasthenia. When the officers brought this information, I was called to the office, and they told me that everything I had said and done wasn’t true. I kept acting like a fool, and since they were still unsure, they sent me here, where there’s a professor who passes by me every morning in the garden and says, “How are you?” I always reply, “I’m the same,” acting like a crazy person. Let me tell you, Rosina dear, don’t say anything different in your letters because they open and read everything to find out what happens and what’s said. Now, what you need to do is ask me how I’m feeling and whether my headaches are gone, and whether I have them all the time like before, and any other little thing that will help me.”
Rosina’s fiancé had a strongly positive W. R. in the serum. It was negative in the fluid. He was returned to the front.
Rosina’s fiancé had a strongly positive W. R. in the serum. It was negative in the fluid. He was sent back to the front.
II. HYPOPHRENOSES
(THE FEEBLE-MINDED GROUP)
Moron of use at front (alienist’s report).
Moron of use at the front (alienist’s report).
Case 35. (Pruvost, 1915.)
Vigouroux reports concerning a tanner of 19 who could not read, write or calculate (3 plus 8 equals 14) and had been of the 1916 class in an infantry regiment at Brest, on the occasion of his asking to be sent to the front more speedily:
Vigouroux reports about a 19-year-old tanner who couldn't read, write, or do basic math (3 plus 8 equals 14) and had been part of the 1916 class in an infantry regiment in Brest when he requested to be sent to the front more quickly:
Mental weakness, with insufficient school and theoretical knowledge but with the ability to assimilate practical ideas, though not knowing how to read, write or calculate; seems to have earned his living in several lines.[45] “As a soldier, he does not know the insignia of the different ranks but understands how to obey a superior officer. Understands a gun and can tell a chargeur from a Le Bel gun. Moreover he seems to be perfectly stable, fixed in his wishes, persistently and intelligently wants to go to the front and kill Boches. He appears to be well disciplined and educable. Although feebleminded, he appears to us able to be useful at the front, though he should not be employed in any undertaking requiring initiative or foresight.”
Mental weakness, lacking sufficient school and theoretical knowledge but able to grasp practical ideas, even without knowing how to read, write, or do math; seems to have managed to earn a living in various jobs.[45] “As a soldier, he doesn’t know the insignia of different ranks but understands how to follow orders. He knows how to handle a gun and can distinguish a chargeur from a Le Bel gun. Additionally, he seems to be stable, set in his desires, and is determined and smart about wanting to go to the front and kill Germans. He appears to be well-disciplined and trainable. Although he has some cognitive limitations, he seems capable of being useful at the front, but he should not be put in any situation that requires initiative or foresight.”
An imbecile, superbrave.
A fool, super brave.
Case 36. (Pruvost, 1915.)
A loquacious, active fellow, 22, with very slight school knowledge and no idea of military ranks (treated his superiors like his comrades), was often punished in the barracks. He did not get on well with his instructors. His activities were never interrupted by any obstacles or by derision. He kept singing and talking enthusiastically during the mobilization. He was the butt of his section.
A talkative, energetic guy, 22, with very little education and no understanding of military ranks (he treated his superiors like his buddies), often got in trouble in the barracks. He didn’t get along well with his instructors. Nothing ever stopped him from being active or made him feel ashamed. He kept singing and chatting excitedly during the mobilization. He was the joke of his section.
At Dinant he did very well; though his section was losing a good many men he remained calm. He was careless of danger and remained at his post firing ceaselessly at the enemy and giving a magnificent example to the few comrades who remained with him. In fact, he remained so long in his shelter that he was surrounded and taken prisoner. He escaped, swam the Meuse and got back to his regiment.
At Dinant, he performed exceptionally well; even though his unit was losing a lot of men, he stayed composed. He was unbothered by danger and continued to fire non-stop at the enemy, setting a fantastic example for the few comrades who stayed with him. In fact, he stayed in his position for so long that he ended up surrounded and taken prisoner. He managed to escape, swam across the Meuse, and made it back to his regiment.
An imbecile of service in barracks work.
An idiot doing menial tasks in the barracks.
Case 37. (Pruvost, 1915.)
A farmer, 36 (father alcoholic, mother always sick, two brothers at the front; patient had typhoid at an unknown age; had gone to school at 13 but “learned nothing”; worked in fields with his brother who gave him some pennies on Sunday), was put into the auxiliary service by the Council at 20. Patient said he was not strong enough for this service. In 1914 the Council reconsidered the case and put him into a regiment of infantry. He could not be given military instruction or execute the most simple drilling manual. He said that 4 plus 2 equalled 7; 4 plus 3 equalled 5. He was of an excellent character, very docile and easily directed. He did all his comrades’ barracks work and was very proud because, as he said, “I do everything they tell me to do.” He was happy in working, everybody was good to him, but he had no comrades. He had no general knowledge and knew nothing about the war but that they were fighting the Boche.
A 36-year-old farmer (whose father was an alcoholic, mother was often sick, and two brothers were at the front; he had typhoid at an unknown age; he started school at 13 but “didn’t learn anything”; worked in the fields with his brother who gave him some change on Sundays) was assigned to auxiliary service by the Council at 20. He said he wasn't strong enough for this service. In 1914, the Council reviewed his case and placed him in an infantry regiment. He couldn’t receive military training or perform even the simplest drill commands. He insisted that 4 plus 2 was 7 and 4 plus 3 was 5. He had an excellent character, was very compliant, and could be easily directed. He did all the barracks chores for his comrades and felt very proud because, as he said, “I do everything they tell me to do.” He enjoyed working, everyone treated him well, but he had no friends. He lacked general knowledge and knew little about the war other than that they were fighting the Germans.
Re imbeciles, Colin, Lautier and Magnac found amongst 1000 soldiers entering Villejuif, 53 imbeciles. Twenty-four of them had been either exempt or retired at the outset of the war, when military surgeons had reviewed them and considered them fit for service. Several of the 29 others also had shown previous evidence of imbecility.
Re idiots, Colin, Lautier, and Magnac found among 1000 soldiers entering Villejuif, 53 idiots. Twenty-four of them had been exempt or retired at the start of the war when military doctors had evaluated them and deemed them fit for service. A few of the 29 others had also previously shown signs of idiocy.
Of course, French military surgeons may have felt that a number of these men would be of just such service in barracks and otherwise as Case 37 (Pruvost). But for one or two cases like Cases 37 and 41 of Pruvost, there are great numbers of other imbeciles who prove quite useless in the army. Two of the Villejuif cases had been volunteers: one volunteer declared that, if he had been intelligent, he never would have enlisted! Ten cases proved unable to use a gun; one turned his gun upon his mates. One regularly forgot the password. One (see Case 42 of Lautier) thought the war too long and tried to take command of the company in order to finish the war one way or the other. Three of the imbeciles had to be evacuated for desertion (unmotivated fugues); two of them cursed their officers. Some of the imbeciles had an emotional diarrhoea throughout their service.
Of course, French military surgeons might have thought that some of these men would be useful in the barracks and elsewhere as Case 37 (Pruvost). But aside from one or two examples like Cases 37 and 41 of Pruvost, there are a lot of other individuals who are completely useless in the army. Two of the Villejuif cases were volunteers: one volunteer stated that if he had been smart, he never would have enlisted! Ten cases were unable to use a gun; one even aimed his gun at his fellow soldiers. One continuously forgot the password. One (see Case 42 of Lautier) thought the war was dragging on too long and tried to take charge of the company to end the war one way or another. Three of the incompetent soldiers had to be sent home for desertion (unexplained absences); two of them cursed their officers. Some of the incompetent soldiers displayed emotional instability throughout their service.
Colin suggests that line officers and military surgeons ought to agree that these men are not fit for service, and that the civil authorities of the home towns should advise the review boards about known imbeciles and criminals. In point of fact, previous knowledge of imbecility could have been obtained quite readily in 27 of the 53 cases observed by Colin.
Colin suggests that line officers and military surgeons should agree that these men are unfit for service, and that the local authorities should inform the review boards about known idiots and criminals. In fact, prior knowledge of mental incapacity could have been easily obtained in 27 of the 53 cases studied by Colin.
A feeble-minded inventor.
An ineffective inventor.
Case 38. (Laignel-Lavastine and Ballet, 1917.)
A jockey of Nîmes, 31, entered the service May 15, 1917. He retired before the war. He was in the auxiliaries at the moment of mobilization. Nothing is known as to any pathological episodes in his past. He said he had been a poor scholar, had left the primary school at eleven hardly knowing how to write or spell, but he had a lively imagination and was a happy-go-lucky youth, playing many tricks on the trades people. He tried a variety of ideas in the industrial or commercial world with very varying success. He had a mechanical taste. The Colonial Exposition at Marseilles caused him to float a variety of projects, from that of having the visitors photographed on a camel to the sale of lemonade. He said he had been a jockey and then a trainer and had finally become a valet de jockey at Maisons Laffitte. He was a gambler and invented a “system.” He made various inventions in relation to horses. At the end of 1914 he had plans for a bomb thrower and placed his discovery at the service of the War Minister. He was not discouraged by the lack of success of the bomb thrower. He now made an aerial torpedo carrier. He had the idea of the tanks. However, he found the secret of his torpedo carrier printed in a magazine. There was a slight difference between the German apparatus and his own.
A 31-year-old jockey from Nîmes joined the service on May 15, 1917. He retired before the war began and was in the auxiliaries at the time of mobilization. There's no information about any health issues in his past. He mentioned he wasn't a great student, leaving primary school at eleven without really knowing how to write or spell, but he had a vivid imagination and was a carefree kid who played many pranks on local shopkeepers. He tried various ideas in the business world with mixed success. He had a knack for mechanics. The Colonial Exposition in Marseilles inspired him to come up with different projects, from taking photos of visitors on a camel to selling lemonade. He claimed to have been a jockey, then a trainer, and eventually a valet de jockey at Maisons Laffitte. He was a gambler and came up with a “system.” He made several inventions related to horses. By the end of 1914, he had plans for a bomb thrower and offered his invention to the War Minister. He wasn't discouraged by the bomb thrower's lack of success. He then created a design for an aerial torpedo carrier. He had the idea for tanks. However, he discovered that the details of his torpedo carrier had been published in a magazine, showing only a slight difference between the German model and his own.
From this time he began to be mistrustful, and now he jealously avoided entering into any details about his inventions and he did not let his officers see his plans. The Commandant offered to give a place in the safe to his documents, but he could not embrace the offer. He now invented a counter-torpedo machine. He went on leave to Paris, asked an audience of the Minister of Marine, who put him in relation to the Committee on Inventions, who put him off, desiring that he should forward all his plans. He emerged from one of his interviews so excited that there was a scandal on the public street and the police commissary evacuated him to Val-de-Grâce, but the patient says he does not remember[48] this incident. He came on service of Laignel-Lavastine May 15. He shortly wrote again to the Minister, who again referred him to the Committee on Inventions. He protested to the President of the Republic and wrote directly to the King of England, who referred him to the Military Administration. He is now occupied in creating a machine to destroy the first line trenches and continues to write to the Ministry. He has documents buried underground in a secret place. He still talks with great vivacity of his discoveries.
From this point on, he started to be suspicious and began carefully avoiding sharing any details about his inventions. He didn’t let his officers see his plans. The Commandant offered to store his documents in the safe, but he couldn’t accept the offer. He created a counter-torpedo machine. He took leave to Paris and requested a meeting with the Minister of Marine, who connected him with the Committee on Inventions, which asked him to submit all his plans. After one of his meetings, he came out so worked up that it caused a scene in the street, leading the police chief to escort him to Val-de-Grâce, but the patient claims he doesn’t remember this incident. He resumed service with Laignel-Lavastine on May 15. He soon wrote again to the Minister, who directed him back to the Committee on Inventions. He appealed to the President of the Republic and even wrote directly to the King of England, who sent him to the Military Administration. He is now focused on creating a machine to destroy the front line trenches and is still corresponding with the Ministry. He has documents hidden underground in a secret location. He continues to speak enthusiastically about his discoveries.
According to Laignel-Lavastine, we deal with a feeble-minded person who has for many years had a délire raisonnant of the inventing group.
According to Laignel-Lavastine, we're dealing with a mentally challenged person who has for many years had a délire raisonnant of the inventing group.
Re feeblemindedness in the British Army, Shuttleworth found 70 who had joined from special schools for the feeble-minded in London, and 100 from Birmingham in the year 1915. The institutional “children” were in general good at drilling and obeying. One of them, given to lying and stealing, got into constant trouble in Flanders.
Re feeblemindedness in the British Army, Shuttleworth found 70 who had joined from special schools for the feeble-minded in London, and 100 from Birmingham in the year 1915. The institutional “children” were generally good at drilling and following orders. One of them, who often lied and stole, kept getting into trouble in Flanders.
Sir George Savage stated that he had sometimes run the risk of allowing enlistment of men who had shown earlier in life a weakness for lying and pilfering, and remarked that such men might make good soldiers. A case like the above (38) would run counter to this view. On this matter, see below Case 183 (Henderson), one of pathological lying.
Sir George Savage said that he had sometimes taken the chance of enlisting men who had previously shown a tendency to lie and steal, and he noted that such men could become good soldiers. A case like the one above (38) would contradict this opinion. For more on this topic, see below Case 183 (Henderson), which discusses pathological lying.
An imbecile who walked lame.
A fool who walked limply.
Case 39. (Pruvost, 1915.)
A soldier, 20, eight days after being called to the colors, complained of pain in the knee and hip. He was observed for 18 days in hospital and then sent back to his company; but he continued to complain of the pains, and the regimental surgeon sent him to a neurological center where the joints were found to be normal and where no sensory, motor or reflex disorders were in evidence. The man continued to walk lame and insisted he could not get about without a cane. He also complained of his mouth and his belly and, though he was very ruddy, said he was á bout de forces.
A 20-year-old soldier, eight days after being called to duty, complained about pain in his knee and hip. He was monitored in the hospital for 18 days and then sent back to his unit; however, he continued to report the pains. The regimental doctor referred him to a neurological center, where his joints were found to be normal, and there were no signs of sensory, motor, or reflex issues. The soldier kept walking with a limp and insisted he couldn't move around without a cane. He also had complaints about his mouth and stomach and, despite looking quite healthy, said he was á bout de forces.
It was a question of simulation. The man, however, was a feebleminded person who could not read, write or calculate. He was invalided as such.
It was a matter of simulation. The man, however, was someone with intellectual disabilities who couldn’t read, write, or do math. He was deemed unfit because of this.
Enlistment to improve character.
Joining for character development.
Case 40. (Briand, February, 1915.)
A village boy had passed for simple ever since typhoid fever at 8. He had learned to read and write, but had always been impulsive and subject to fugues, running to see his grandmother, or off as a truant. It was decided that he, at 19, should enlist to improve his character. But one fine day, even before the war, he deserted. He said, in explanation, that he had lost his way, and he was being examined mentally when mobilization began.
A village boy had been seen as simple ever since he had typhoid fever at age 8. He learned to read and write, but he was always impulsive and prone to running away, either to visit his grandmother or to skip school. It was decided that at 19, he should enlist to help improve his character. But one day, even before the war started, he deserted. He explained that he had gotten lost, and he was being mentally evaluated when mobilization began.
He looked ape-like, with spread ears; had a low forehead, a head flattened behind, an asymmetrical face, prognathous jaws, an arched palate, and defective teeth. He talked freely of homosexual relations, and said he wandered off because it occurred to him to do so. He was determined to be unfit for service.
He looked kind of like an ape, with big ears; had a low forehead, a head that was flat at the back, an uneven face, jutting jaws, an arched palate, and bad teeth. He openly discussed homosexual relationships and mentioned that he left because he felt like doing it. He was set on being unfit for service.
An imbecile who may be sent to the front.
An idiot who might be sent to the front lines.
Case 41. (Pruvost, 1915.)
A Parisian sandwichman, 25, of unknown parentage and a state ward, placed out with a farmer at 12, escaping with a friend to Bordeaux at 14, thence leading a wild, improvident life at Lyons, Marseilles and Paris, sleeping in fields and hedges, earning 22 sous a day but in no case mixing with the police, was examined for physical inefficiency at 20 years. He wanted to enlist but was refused. He insisted and was very proud of the fact that he got in as the Major said to them, “Let him go in.” He could hardly read, write or calculate but was by reason of his adventurous life full of practical resources. He was irascible and frequently crimed, whereupon he would cry under the Captain’s window, “Robber band, idiots, I shall write to the Minister.” He was passionately fond of military life, though he had but the vaguest notions about the commands, the names of generals and the like. He wanted to drill. His comrades played practical jokes upon him asking him to look for a trajectory, for the squad’s umbrella and the key to the drill ground. They also told him he had been proposed to be corporal, whereupon he was greatly overjoyed and immediately sewed stripes on his sleeve and began to give commands. He said if they put him among the auxiliaries he would throw the adjutant in the water. He sang and swung his gun with joy when he went to the front. He thought there were stripes hanging to the barbed wire and wanted to pick as many as possible. Such a man may be safely sent to the front although he will bear watching. At the date of report this man had been at the front two months doing very well.
A 25-year-old sandwich board man from Paris, with unknown parents and a background as a state ward, was placed with a farmer at age 12. He escaped with a friend to Bordeaux at 14 and then led a wild, reckless life in Lyon, Marseille, and Paris, sleeping in fields and bushes, earning 22 sous a day but avoiding any run-ins with the police. At 20, he was examined for physical fitness. He wanted to join the military but was initially turned down. He was persistent and was proud when the Major said, “Let him join.” He could barely read, write, or do math, but his adventurous life gave him plenty of practical skills. He had a short temper and often complained, yelling beneath the Captain's window, “Robber gang, idiots, I’m writing to the Minister.” He loved military life, even though his knowledge of commands and generals was quite vague. He wanted to train. His comrades played practical jokes on him, asking him to search for a trajectory, the squad’s umbrella, and the key to the drill ground. They also told him he was being considered for corporal, which made him extremely happy, so he stitched stripes on his sleeve and started giving commands. He claimed that if they put him with the auxiliaries, he would throw the adjutant into the water. He sang and swung his gun with excitement when heading to the front. He believed there were stripes caught in the barbed wire and wanted to collect as many as he could. Such a man could safely be sent to the front, though he would need some supervision. At the time of the report, this man had been at the front for two months and was doing very well.
Re the comparative success of the Germans in the matter of excluding imbeciles, Meyer found that 8 per cent of the mental cases in the army were cases of mental defect.
Re the comparative success of the Germans in excluding individuals with mental disabilities, Meyer found that 8 percent of the mental cases in the army were instances of mental deficiency.
Imbecile with sudden initiative.
Fool with sudden initiative.
Case 42. (Lautier, 1915.)
A soldier, 41, a farmer, from the Department of the Marne, married, childless, was called to the colors August 31, 1914. He was on guard duty until May, 1915, watched prisoners until October and was finally sent to the front, February, 1916, where he fell sick.
A 41-year-old soldier and farmer from the Marne region, who was married but had no children, was drafted on August 31, 1914. He was on guard duty until May 1915, monitored prisoners until October, and was finally sent to the front in February 1916, where he became ill.
“He was tired in his head.” “His commanding officer made him drill without rhyme or reason; he would have been able himself to have commanded with greater intelligence.” He once attempted to put himself at the head of the company to lead them against the Boche; this idea arrived to him all of a sudden in a phase of perfect confidence and sang froid. He thought his comrades would follow him and that the officers would do likewise. He hoped thus to be able to end the war one way or the other. He was getting tired of the war and regretted his family life and kept saying that this was no existence for family men. “We ought to attack or ask for peace.” No one followed him and his comrades said he was un peu fou but he did not share this opinion.
“He was mentally exhausted.” “His commanding officer made him drill for no good reason; he could have commanded with more sense himself.” He once tried to take charge of the company to lead them against the Germans; this idea came to him suddenly during a moment of total confidence and composure. He believed his comrades would follow him and that the officers would do the same. He hoped that this way, he could bring an end to the war, one way or another. He was growing weary of the war and missed his family life, constantly saying that this wasn’t a life for family men. “We should either attack or ask for peace.” No one followed him, and his comrades said he was a bit crazy, but he didn’t agree with that.
In point of fact he hardly knew how to read or write and at home lived with his relatives, submitting himself entirely to their guidance. He was much afraid of being punished and often feared that he had done badly as he had trop de conscience. He was non-alcoholic and without hereditary or acquired neuropathic taint. He had no pronounced stigmata of degeneration. He was rather reticent about certain mystical ideas of a political tinge. At Villejuif, whither he was brought February 17, 1916, he received a diagnosis of imbecility.
In fact, he barely knew how to read or write and lived at home with his relatives, completely relying on their guidance. He was very afraid of being punished and often worried that he had done something wrong because he had too much conscience. He was not an alcoholic and had no hereditary or acquired neurological issues. He didn’t have any obvious signs of degeneration. He was quite reserved about certain mystical ideas with a political twist. He was brought to Villejuif on February 17, 1916, where he was diagnosed with imbecility.
Emotional fugue in a subnormal subject.
Emotional confusion in a person with below-average abilities.
Case 43. (Briand, February, 1915.)
A soldier in the Territorial Army, 40, appeared before the examining board in a depressed, dejected-looking state, speaking slowly but collectedly and lucidly. Mobilized the second day, this man was much afraid that he could not get through the marches, and asked for a special examination to determine whether his feet did not make him unsuitable for fatigue. Two physicians thought he was unsuitable for marching, and another thought he put it on. A trial march was not executed well. He was kept in barracks but jumped the wall, put on civilian clothes, and made off for Paris. But a relative, warned by his wife, finally got him to go to the authorities. He was told that he ought to return in the afternoon, when suddenly he was arrested.
A 40-year-old soldier in the Territorial Army appeared before the examining board looking depressed and downcast, speaking slowly but clearly and coherently. Mobilized on the second day, he was really worried that he couldn't handle the marches and requested a special examination to see if his feet made him unfit for physical activity. Two doctors agreed he wasn’t fit for marching, while one thought he was just pretending. He didn’t perform well on the trial march. He was kept in the barracks but jumped the wall, changed into civilian clothes, and ran off to Paris. However, a relative, warned by his wife, eventually convinced him to go to the authorities. He was told to return in the afternoon, and then, unexpectedly, he was arrested.
It seems that the man relied on the opinion of the two physicians and discounted that of the third. He thought himself the victim of an injustice, and not knowing how to get on, it occurred to him that he would abandon the regiment and get out of the difficulty. It was without resistance, however, that he gave himself up as a prisoner. This fugue was neither unconscious nor amnestic, nor was it due to an irresistible impulse; nor can we say that it was due to a genuine intellectual disorder. It was an emotional fugue, and partly due to the man’s long-standing depression. It seems that he had inherited this character from his father. He was below normal intelligence, had a very poor education, lost his wife, and grew more and more sombre. He married again, but this time a neuropath. He began to be preoccupied with his health and he had even some ideas of suicide. At the time of his leaving the regiment, he had passed through a phase of depression of about 6 months’ duration, and at this time had a number of hypochondriacal ideas with poor appetite and loss of weight.
It seems the man relied on the opinions of two doctors and dismissed the third. He felt like a victim of injustice, and unsure of how to move forward, he thought about leaving the regiment to escape the situation. However, he surrendered himself as a prisoner without resistance. This flight was not unconscious or forgetful, nor did it result from an overpowering impulse; we can't say it stemmed from a true intellectual disorder either. It was an emotional escape, partly due to the man’s long-standing depression. It appears he inherited this trait from his father. He had below-average intelligence, received a poor education, lost his wife, and became increasingly gloomy. He remarried, but this time to someone with mental health issues. He started worrying about his health and even had suicidal thoughts. When he left the regiment, he had been in a depressive phase for about six months and had various hypochondriacal ideas along with a poor appetite and weight loss.
Diagnostic dispute between regimental surgeon and alienist.
Diagnostic disagreement between the regimental surgeon and the psychiatrist.
Case 44. (Kastan, January, 1916.)
Julius Q. was sent on guard April 14, 1915, with orders to remain there. While on guard he made a noise and made a movement as if to take a knife from his pocket. Ordered to empty his pockets, he attacked the other guards. The witnesses said that he was drunk.
Julius Q. was assigned to guard duty on April 14, 1915, with instructions to stay there. While on duty, he made noise and acted like he was reaching for a knife in his pocket. When ordered to empty his pockets, he assaulted the other guards. Witnesses stated that he was intoxicated.
Upon examination, it appeared that he had recognized and called by name those present in the guardhouse, despite his supposed intoxication. There were red spots on the skin and a certain amount of analgesia. His powers of computation and reasoning were poor. He was unable to explain the meaning of a picture shown him. He maintained that he had an indomitable desire for drink. A diagnostic draught of alcohol yielded no reaction. Upon dismissal, he got drunk at once again, and had again to be imprisoned in a state of excitement. What the outcome in this case was is not stated by Kastan.
Upon looking closer, it seemed he recognized and named everyone in the guardhouse, despite being supposedly intoxicated. There were red spots on his skin and a level of numbness. His ability to think clearly and reason was weak. He couldn’t explain the meaning of a picture shown to him. He insisted he had an unquenchable thirst for alcohol. A prescribed drink of alcohol didn’t produce any reaction. After being dismissed, he quickly got drunk again and had to be locked up in a state of agitation. Kastan doesn’t mention what happened next in this case.
The previous history seems important. Julius Q. had been a state ward. He had escaped several times from the institution but had always to be brought back again because he could not be trained at home. He had once attacked a supervisor in the state institution with a knife. It seems that he had at this time been drunk, having been brought back drunk to the institution.
The previous history seems important. Julius Q. had been a ward of the state. He had escaped several times from the institution but was always brought back because he couldn’t be trained at home. He once attacked a supervisor in the state institution with a knife. It appears he had been drunk at that time, having been brought back to the institution while intoxicated.
Two years before the war he had been taken to the Breslau Hospital for the Insane on account of fits of insanity. In 1913 he had been a patient in Wuhlgarten on similar grounds. The diagnosis there had been epileptoid degeneration, psychopathic constitution, imbecility, or epilepsy(?). He had been convicted of crimes a number of times and put to labor. He had been given to cruelty in childhood.
Two years before the war, he was admitted to the Breslau Hospital for the Insane due to episodes of insanity. In 1913, he had been a patient at Wuhlgarten for similar reasons. The diagnosis there was either epileptoid degeneration, psychopathic constitution, imbecility, or epilepsy (?). He had been convicted of crimes several times and forced into labor. He had shown signs of cruelty in childhood.
Despite this, he was declared perfectly healthy in mind and body by the regimental surgeon.
Despite this, he was deemed completely healthy in both mind and body by the regimental surgeon.
In 1914, Q. fell suddenly ill in prison (he was presumably in prison for a military offence), and smeared the cell with feces, saying that he was able to do that as he could pay for anything. He stared at the floor and failed to answer questions. He remarked, however, that he had frequently been convicted for breach of the peace and assault and battery, and he said his father had been a drunkard, and he acknowledged hallucinations to the extent of saying that he heard his name called when he was alone.
In 1914, Q. suddenly got sick in prison (he was likely there for a military offense) and smeared the cell with feces, claiming he could do that because he could afford anything. He stared at the floor and didn’t respond to questions. However, he noted that he had often been convicted of disturbing the peace and assault and battery. He mentioned that his father was an alcoholic and admitted to having hallucinations, saying that he heard his name being called when he was alone.
The story of this case warrants our inquiring why such a patient was kept in the army. He was kept there clearly on account of the report of the regimental surgeon, who could not have taken seriously the previous history of the case, or else thought the patient perfectly good cannon fodder.
The story behind this case makes us question why this patient was kept in the army. He was clearly kept there because of the report from the regimental surgeon, who either didn’t take the patient's past history seriously or believed the patient was just expendable.
The hypothesis of syphilis apparently need not be entertained. That of feeblemindedness is possibly the fundamental diagnosis, yet epilepsy was considered by the German diagnosticians, doubtless on account of the sudden violent attacks and breaches of peace on the part of the patient. There is clearly something behind mere alcoholism in the entire story of this state ward. On the whole, the periodicity of the attacks is equally consistent with the picture presented by numerous feeble-minded persons, and the institutions that had to deal with Q. regarded him rather as epileptoid. There seems to be evidence of actual intellectual defect. Accordingly it seems wiser to consider the case of Julius Q. one of feeblemindedness, possibly of the moron group. We should then consider the epileptoid features as part and parcel of the feeblemindedness. We should consider the intellectual defect a part of the process; and the uncontrollable impulse to drink, the sudden violent attacks, and the cruelty in childhood would then be regarded as merely symptomatic of the feeblemindedness. It seems clear that either mental tests by the regimental surgeon or an examination of the patient’s previous history would tend to exclude such a patient from the army.
The idea of syphilis doesn't really need to be considered. The diagnosis of feeblemindedness might be the main issue, but German diagnosticians looked at epilepsy, probably because of the patient's sudden violent outbursts and disruptive behavior. There's clearly more to this situation in the state ward than just alcoholism. Overall, the pattern of the attacks matches what is seen in many feebleminded individuals, and the facilities that dealt with Q. viewed him more as epileptoid. There seems to be proof of actual intellectual impairment. So, it seems more reasonable to classify Julius Q.'s case as one of feeblemindedness, likely in the moron category. We should then see the epileptoid traits as part of the feeblemindedness. The intellectual impairment should be viewed as part of the overall issue; the uncontrollable urge to drink, the sudden violent outbursts, and the childhood cruelty would then be seen as just symptoms of the feeblemindedness. It’s clear that either mental assessments by the regimental doctor or a look into the patient's past would likely disqualify this patient from serving in the army.
How can a rifleman be an imbecile?
How can a rifleman be an idiot?
Case 45. (Kastan, January, 1916.)
Anton K. was down in the list as “missing.” He was found at home. He said his feet had become sore from the marching. He had lain down and become unconscious. Coming to his senses, he was possessed only of trousers and a shirt but he got a civilian suit in a village. He had gone home part way by train, part way on foot. It seems that he did not tell his father any details about his coming back although he expressly denied deserting.
Anton K. was listed as “missing.” He was found at home. He said his feet had gotten sore from marching. He had laid down and passed out. When he came to, he was only wearing trousers and a shirt, but he managed to get a civilian suit in a village. He had traveled part of the way home by train and part on foot. It seems he didn’t tell his father any details about his return, although he clearly denied deserting.
It seems no mental weakness had been noticed in the army. It had been observed, however, that after seeing the first corpses he was deeply impressed and did not want to see any more. On examination in the hospital he gave the impression of indifference and low spirits. He had to be urged to eat and work. No great amount of intelligence defect could be determined, though his knowledge and capacity were below the average. The physician examining him thought his depression was either caused by or increased by his imprisonment; but this examiner thought that the protection of Section 51 did not extend to the patient at the time of his desertion. The examiner thought that an examination by a psychiatrist was not necessary, though both judge and prosecutor urged it.
It seems no mental weakness had been noticed in the army. It was observed, however, that after seeing the first corpses, he was deeply affected and didn’t want to see any more. During his examination in the hospital, he appeared indifferent and downcast. He had to be encouraged to eat and work. There didn’t seem to be a significant intelligence deficit, although his knowledge and abilities were below average. The doctor who examined him believed his depression was either caused by or worsened by his imprisonment; however, this doctor thought that the protection of Section 51 did not apply to the patient at the time of his desertion. The examiner felt that a psychiatric evaluation was unnecessary, even though both the judge and prosecutor insisted on it.
When examined in the clinic, he seemed to be disoriented for time. He claimed to have been able to stand the shooting and the sight of the corpses. After becoming unconscious, he had wakened and eaten cucumbers and carrots in the fields, wandering on for a period of three or four weeks, until he came to a place where he had formerly worked. The reason he had thrown away his uniform was because Russians had been about. He had not known that it was his duty to report to the army again.
When he was looked at in the clinic, he seemed confused about time. He said he had managed to cope with the shooting and the sight of the bodies. After passing out, he woke up and ate cucumbers and carrots in the fields, wandering around for about three or four weeks, until he got to a place where he had worked before. He had discarded his uniform because there had been Russians nearby. He didn't realize it was his responsibility to report back to the army.
It was found that the patient’s father was poorly developed as to mind, that his brother was subject to periodic mental disturbance so that he had to be watched. It was found also that K. himself had had a similar mental disturbance,[56] lasting a week, two years before. Moreover he was not considered mentally right in his home town. In fact, no one there wondered really at his desertion because he was so stupid. His school work had been poor and limited.
It was discovered that the patient’s father was not very mentally developed, and that his brother experienced occasional mental issues that required supervision. It was also revealed that K. himself had a similar mental episode lasting a week, two years earlier. Furthermore, he was not regarded as mentally stable in his hometown. In reality, no one was surprised by his leaving because he was seen as quite foolish. His academic performance had been poor and minimal.[56]
He himself said that his people were of sound mind; that during school days he had felt bad in his head, once running into the woods after being told something. He was able to give the names of his former superiors. His calculations were only partly correct. He was poor at reasoning and at simple distinctions; for example, asked the difference between a bird and a butterfly, he replied that a butterfly was a bird too. He did not know the difference between a river and a lake. He thought Russia, England, and Austria were the enemies of Germany.
He said his people were of sound mind; that during his school days he’d felt bad in the head, once running into the woods after hearing something. He could name his former superiors. His calculations were only partly correct. He was bad at reasoning and making simple distinctions; for example, when asked the difference between a bird and a butterfly, he said a butterfly was a bird too. He didn’t know the difference between a river and a lake. He thought Russia, England, and Austria were Germany’s enemies.
He sat about or lay on the floor, motionless and indifferent, with a newspaper stuffed into his trousers, unoccupied although saying that he wanted to work, and even allowing his fingers to be burned by cigarettes he was smoking.
He sat around or lay on the floor, motionless and indifferent, with a newspaper stuffed into his pants, unoccupied even though he claimed he wanted to work, and even letting his fingers get burned by the cigarettes he was smoking.
He was tried once more and the first medical expert still adhered to his former opinion, pointing out that K. was a rifleman and that only an intelligent man could be a rifleman. The court, however, accepted Kastan’s opinion and granted K. the protection of Section 51.
He was tried again, and the first medical expert maintained his previous opinion, emphasizing that K. was a rifleman and that only a smart person could be a rifleman. However, the court accepted Kastan’s opinion and granted K. the protection of Section 51.
In comment upon this case, it seems clear that ever so slight a knowledge of K’s home town reputation would have naturally excluded him from the army. However, what is to be said “when doctors disagree,” as noted by Kastan in this very case? It seems impossible, also, that his comrades should not have noticed something odd about him (over and above the deep impression on seeing the first dead) which might have given occasion to the regimental surgeon for a special mental examination. However, to the military mind, mayhap the man seemed to be sufficiently “effective.”
In commenting on this case, it’s clear that even a little knowledge of K’s hometown reputation would have naturally kept him out of the army. But what can we say “when doctors disagree,” as Kastan points out in this very case? It also seems unlikely that his fellow soldiers wouldn’t have noticed something unusual about him (in addition to the strong impact of seeing the first dead) that might have prompted the regimental surgeon to conduct a special mental evaluation. However, to the military mindset, perhaps the man seemed “effective” enough.
Re imbecility in a rifleman, the compiler has studied somewhat elaborately the brain of a feeble-minded murderer with some North American Indian blood in him. This man was a crack shot despite his subnormality. It would seem that the German regimental surgeons castigated by Kastan as above were very properly so castigated.
Re imbecility in a rifleman, the compiler has looked into the brain of a mentally deficient murderer with some North American Indian heritage. This man was an excellent marksman despite his limitations. It seems that the German regimental surgeons criticized by Kastan were rightly criticized.
Hypomania in an imbecile.
Hypomania in a fool.
Case 46. (Haury, August, 1915.)
A brusque little man, of a somewhat bold and talkative disposition, though giving a good first impression, was evidently a bit feebleminded, though (as Haury says) of the active group. He had a sister like himself, whose children were taken care of by the State, and at home he had had a number of fugues, about which details were lacking. It was soon evident what sort of soldier he would make, and he was put in one of the Territorial regiments, but it was not noted that he had a genuine mental disorder, as he was thought to be just a peculiar person.
A gruff little man, somewhat bold and chatty, who initially made a good impression, was clearly a bit slow-witted, though (as Haury notes) part of the active group. He had a sister who was just like him, and her kids were cared for by the State. At home, he had experienced several episodes of mental breakdowns, but there weren’t many details about them. It quickly became clear what kind of soldier he would be, and he was assigned to one of the Territorial regiments. However, it went unnoticed that he actually had a serious mental disorder; people just thought he was an odd individual.
His new relations caused him to do a number of eccentric things. He shortly proved to be in a sort of rudimentary maniacal state; talkative, restless, scheming rather feebly to go back to his village. He said that he couldn’t walk on account of corns, and that these corns required a certain drug, which he wanted to get from home. He said that he had been struck by lightning twice; that he had fires in his body, etc. He wanted only to be retired on a pension of one or two hundred francs so he could take care of his farm, his hay and his fields. There was no need of trying to get land by means of bullets, he said, since he had enough.
His new connections led him to act in a lot of strange ways. He soon seemed to be in a kind of frenzied state; he was overly talkative, restless, and weakly plotting to return to his village. He claimed he couldn’t walk because of corns, which needed a specific medication he wanted to get from home. He mentioned that he had been struck by lightning twice and that he felt like there were fires inside him, among other things. All he wanted was to retire on a pension of one or two hundred francs so he could look after his farm, hay, and fields. He argued that there was no need to acquire land with force since he already had enough.
The mental disorder of this man was much deeper than appeared, and in fact, he did a number of dangerous things compromising the security of the entire regiment.
The mental disorder of this man was much more serious than it seemed, and in fact, he did several dangerous things that put the entire regiment's safety at risk.
Insubordinate desire to remain at the front.
Insubordinate desire to stay at the front.
Case 47. (Kastan, January, 1916.)
Friedrich L., on March 4, 1915, was ordered to go back to the baggage-train. He did not obey. He said to the non-commissioned officer who then came to him, “I am not going; you have nothing to say anyhow, you ox-tender!” He stood with his hands in his pockets, and, when the officer seized him angrily by the collar, L. struck the officer’s face.
Friedrich L. was ordered on March 4, 1915, to return to the baggage train. He refused to comply. He told the non-commissioned officer who approached him, “I’m not going; you don’t have any authority, you ox-tender!” He stood there with his hands in his pockets, and when the officer grabbed him angrily by the collar, L. punched the officer in the face.
He stated at his hearing that no one had the right to send him back. At that time even he conveyed the impression of being not quite normal and was let off with his arrest only. Later he refused again to go on guard duty, saying, “You have nothing to say at all. Perhaps you will find out that we shall meet each other again in hell tomorrow morning.” He was taken before the physician, who considered him mentally inferior and not entirely appreciative of the nature of his acts. He was told that the death penalty would meet such behavior, whereupon he remarked, “I am not afraid of the death penalty,” staring excitedly at the officer and trembling throughout his body. It seems that he had already made an impression of mental inferiority in the troop, and had once before said to an officer who wanted to send him to the front, that he would not go; this had been regarded as almost a breach of discipline. He had been in the habit of not reacting to the calls of his superiors, and had smiled at their reproaches. He seemed to hold the opinion that not even a company commander had power to order him to go back. Examined in the clinic he held to the same opinion, that there was no need of his going back; that they took volunteers; and that he wanted to remain at the front. On the day of the deed, he had drunk a rye whiskey. He had shaken off the non-commissioned officer because the leader had seized him by the throat. In the clinic he often smiled and wrinkled his forehead. He gave evasive and inadequate answers. Asked about oaths and perjury, he remarked,[59] “I prefer to remain silent.”
He said at his hearing that no one had the right to send him back. At that time, he even gave off the impression of not being quite normal and was only charged with his arrest. Later, he refused to go on guard duty again, saying, “You have nothing to say at all. Maybe you'll find out we’ll meet again in hell tomorrow morning.” He was taken to see the physician, who thought he was mentally inferior and didn't fully understand the nature of his actions. He was told that the death penalty would apply for such behavior, to which he replied, “I’m not afraid of the death penalty,” staring intensely at the officer and trembling all over. It seems that he had already made a reputation for mental inferiority among the troops and had once told an officer who wanted to send him to the front that he wouldn’t go; this was seen as almost a breach of discipline. He often ignored his superiors' commands and smiled at their reprimands. He seemed to believe that not even a company commander had the authority to order him to go back. When examined in the clinic, he maintained the same belief, that there was no need for him to go back; that they were taking volunteers, and that he wanted to stay at the front. On the day of the incident, he had drunk some rye whiskey. He had shaken off the non-commissioned officer because the leader had grabbed him by the throat. In the clinic, he often smiled and frowned. He gave vague and unsatisfactory answers. When asked about oaths and perjury, he said, “I prefer to remain silent.”
He said that one of his sisters was a little stupid. Study of his previous history indicates that Friedrich L. had formerly been a quiet and steady man, although he often had attacks of rage, breaking out upon sudden excitements. As to his capacity in school, nothing could be learned, since the Russians had taken the school registers away.
He mentioned that one of his sisters was a bit slow. A look at his background shows that Friedrich L. had been a quiet and reliable guy, although he often experienced fits of anger triggered by sudden excitement. As for his performance in school, nothing could be found out because the Russians had taken the school records.
The analysis of this case seems to reduce to the question of feeblemindedness and schizophrenia, unless some form of inborn qualitative inferiority of mind be preferred as the diagnosis. On the whole, possibly, the diagnosis of feeblemindedness seems preferable. The entire symptom picture seems to relate to the patient’s one mental attitude about sticking at the front, ruat coelum.
The analysis of this case seems to come down to the question of intellectual disability and schizophrenia, unless you prefer to diagnose it as some kind of inherent mental inadequacy. Overall, it seems that the diagnosis of intellectual disability is more fitting. The entire set of symptoms appears to connect to the patient’s singular mindset about persevering, ruat coelum.
A French soldier who admired Germans.
A French soldier who looked up to Germans.
Case 48. (Lautier, 1915.)
A man with the extraordinary first name of Agapithe (Laurent insists on the frequency of strange first names in degenerate families) came from Val-de-Grâce to Villejuif June 5, 1916, with the diagnosis of mental weakness, interpretative ideas of persecution, mental excitement, recrimination, logorrhoea, and a tendency to revengeful reactions.
A man with the unusual first name of Agapithe (Laurent emphasizes how common odd first names are in dysfunctional families) arrived from Val-de-Grâce to Villejuif on June 5, 1916, diagnosed with mental weakness, paranoid ideas, emotional agitation, tendency to blame others, excessive talking, and a desire for vengeful responses.
On arrival the patient said he must be in an insane asylum because he heard spiritiques talking together. He, however, was “not insane” and began expounding his plans for revenge with the words “Kill,” “Cut-throat.”
Upon arrival, the patient claimed he must be in a mental hospital because he heard spirits talking to each other. He insisted he was “not insane” and started sharing his plans for revenge with words like “Kill” and “Cut-throat.”
This man had been placed in the auxiliary service by the Council, called to the colors December 13, 1914, and finally sent to the front in May, 1915. In July he was made prisoner in a brush. He said, “I cried out, ‘Comrades, what difference does it make to me whether I am German or French? My officers are imbeciles that drink the blood of us unlucky ones!’” He was interned in some camp whose name he could not exactly give and reported that the Germans were very gentle with him, that his real enemies were the French, for the French were against him night and day. “As a matter of fact, among Germans the French are nothing but cochons malades. The Germans are fine types.”
This man had been placed in auxiliary service by the Council, called up on December 13, 1914, and finally sent to the front in May 1915. In July, he was captured in a skirmish. He said, “I shouted, ‘Comrades, what difference does it make to me whether I’m German or French? My officers are fools who drink the blood of us unlucky ones!’” He was interned in a camp whose name he couldn’t exactly remember and reported that the Germans were very kind to him, that his real enemies were the French, because the French were against him day and night. “In fact, among Germans, the French are nothing but cochons malades. The Germans are great people.”
He was repatriated in May, 1916. He kept making verbose and neologistic eulogia of the Germans. He had been a farm boy in Brittany, where he had had headaches. He had been at Quimper Asylum in 1910. In fact, he said his parents had tried to poison him and to have him assassinated; they had charged him with setting fire to their house. His mother was an imbecile, he said, who believed she was the Queen of France. His recriminations did not stop short of himself. He had been accused of kissing a girl and stealing apples; as a matter of fact he knew what to do with girls.
He was sent back home in May 1916. He kept giving long-winded and new-age praises of the Germans. He had been a farm boy in Brittany, where he often had headaches. He had been at the Quimper Asylum in 1910. In fact, he claimed his parents tried to poison him and have him killed; they accused him of setting their house on fire. He said his mother was an idiot who believed she was the Queen of France. His complaints didn’t just stop with them; he also blamed himself. He had been accused of kissing a girl and stealing apples; in reality, he knew exactly how to handle girls.
He had a coarse face and a number of stigmata besides his name Agapithe. He was kept at Villejuif as an imbecile.
He had a rough face and several marks aside from his name Agapithe. He was kept at Villejuif as someone with an intellectual disability.
Unfit for service: Question of feeblemindedness.
Unfit for service: Question of mental disability.
Case 49. (Kastan, January, 1916.)
Walter N. was declared unfit for military service in 1912, on the ground of mental incapacity. He had shown this clearly during his period of training. He committed a number of slight offences secretly, but not so secretly but that they were immediately discovered and punishment meted out therefor. He could do nothing without aid. It appears that his mental weakness had not been noticed in school, but that his employers had thought him both feebleminded and irresponsible. Nevertheless he always executed orders properly. While in hospital in 1912, he had occupied himself very little, sitting indifferently, quiet and dreaming. At that time, he had shown poor calculating ability and decreased power of perception. It also appears that he did not grasp the nature of simple orders, the requisite associations being disturbed.
Walter N. was deemed unfit for military service in 1912 due to mental incapacity. He clearly demonstrated this during his training. He committed several minor offenses that he tried to hide, but they were obvious enough to be quickly discovered, leading to punishment. He couldn’t do anything without help. It seems that his mental challenges went unnoticed in school, but his employers considered him both slow-witted and irresponsible. Still, he always followed orders correctly. While in the hospital in 1912, he hardly engaged in any activities, sitting passively, quiet, and lost in thought. At that time, he showed poor math skills and reduced perception ability. It also appears that he didn’t understand the nature of simple commands because the necessary connections were disrupted.
Despite this history, on September 11, 1914, he found himself being transported. He claimed to be very tired. Upon reaching the city, he picked up a large stone and raised his arm as if to strike the transport leader. While N. was being bound by the transport leader in consequence, he kicked at his leader’s shins.
Despite this history, on September 11, 1914, he found himself being transported. He said he was really tired. Once they got to the city, he picked up a big stone and raised his arm as if he was going to hit the transport leader. While N. was being tied up by the transport leader as a result, he kicked at the leader’s shins.
In the clinic he resisted examination, moving his legs without speaking, staring at the floor, moaning frequently, sitting motionless with head hanging, answering monotonously repeated questions, but turning his head at a loud noise. He felt ill. It appeared that he was oriented and that his knowledge was well preserved although his calculation ability was poor.
In the clinic, he resisted being examined, shifting his legs without speaking, staring at the floor and moaning often, sitting still with his head down, responding in a monotone to repeated questions, but turning his head at loud noises. He felt unwell. It seemed like he was aware of his surroundings and that his knowledge was intact, although his ability to do calculations was lacking.
It would seem that psychiatric examination, possibly with the aid of psychological work, would have excluded Walter N. from the army.
It seems that a psychiatric evaluation, perhaps with some psychological support, would have kept Walter N. from joining the army.
Oniric delirium (Régis) in a somewhat feebleminded Esthonian.
Oniric delirium (Régis) in a somewhat dim-witted Estonian.
Case 50. (Soukhanoff, November, 1915.)
An Esthonian, 21, a soldier in a reserve regiment, came to a psychiatric section towards the close of 1914. He was negativistic, mumbling, restless, fugacious; later more tranquil. One day he entered the physician’s office, walking up and down, mute, looking at articles and attempting to take them away.
An Estonian, 21, a soldier in a reserve regiment, came to a psychiatric section toward the end of 1914. He was negative, mumbling, restless, and fleeting; later he became more calm. One day he walked into the physician's office, pacing back and forth, silent, looking at items and trying to take them.
February 21, 1915, he was evacuated to the Notre Dame Hospital for the insane at Petrograd,—a tall, healthy, agitated-looking youth with a rapid pulse. He explained in poor Russian how he was now among Germans and feared that they were going to hurt him. At first in the hospital he was seclusive and morose. March 9 he became excited, and tried to break through the door. He was placed in the bath, agitated and yelling. An Esthonian interpreter did not quiet him. The Germans were going to make a martyr of him. After an hour of this he grew quieter, and next day complained only of head weakness and malaise, was in good humour, smiling, and reading an Esthonian paper, and well behaved in church, though tired and pale.
On February 21, 1915, he was taken to the Notre Dame Hospital for the mentally ill in Petrograd—a tall, healthy-looking young man who seemed agitated and had a fast heartbeat. He struggled to communicate in broken Russian, saying he was surrounded by Germans and was afraid they were going to harm him. At first, he was withdrawn and sullen in the hospital. On March 9, he became agitated and attempted to break through the door. He was put in the bath, screaming and restless. An Estonian interpreter couldn't calm him down. He feared the Germans would make a martyr out of him. After about an hour, he settled down, and the next day he only complained of feeling weak and unwell. He was in good spirits, smiling, reading an Estonian newspaper, and behaved well in church, although he appeared tired and pale.
He now got better, began to work and wrote letters. It seemed as if he had waked up from a painful dream. He explained how he thought he had been in captivity; that he was going to be hanged. He had thought that the Germans could talk Russian. He had had hard work in his regiment, as he did not understand Russian and had never before left his little village in Livonia. His mental disorder had started in the autumn, but all that was now like a dream. He said that he had had a mental disorder of short duration following some bodily disease, at the age of thirteen. According to Soukhanoff, this is a case of Meynert’s amentia, in a somewhat feebleminded person. The twilight state might well receive (according to Soukhanoff) the term “oniric delirium” invented by Régis.
He was feeling better, started to work, and wrote letters. It felt like he had just woken up from a painful dream. He explained how he thought he had been in captivity and was going to be hanged. He believed that the Germans could speak Russian. He had struggled in his regiment because he didn’t understand Russian and had never left his small village in Livonia. His mental issues had begun in the autumn, but all of that now felt like a dream. He mentioned that he had experienced a brief mental illness after some physical illness when he was thirteen. According to Soukhanoff, this is a case of Meynert’s amentia in a somewhat mentally challenged person. The twilight state might well be called “oniric delirium,” a term coined by Régis, according to Soukhanoff.
Shell-shock; burial: Incapacity to rationalize the situation.
Shell-shock; burial: Inability to make sense of the situation.
Case 51. (Duprat, October, 1917.)
A soldier, 39, a herdsman, was shell-shocked at Hill 304 May 23, 1916, buried twice, slightly wounded in right eye, and carried unconscious to Bar-le-Duc. He was then forty days in a semi-confusional state with headaches and dreams of the Boches wanting to behead him. Some of these dreams came in the waking state, in which state he could recognize them as imaginary. In April, 1917, he said he had always been afraid, even in daytime, that he would be hurt and had been especially troubled by the fear of shells. He was also bothered by nocturnal enuresis which might become an incurable disease and bring impairment of memory and attention. Although not feebleminded the man was of but moderate intelligence, and his emotions, according to Duprat, were such as to defeat any complete resolution of his plight by the intellect.
A 39-year-old soldier, who was a herdsman, experienced shell shock at Hill 304 on May 23, 1916. He was buried twice, had a minor injury to his right eye, and was taken unconscious to Bar-le-Duc. He spent forty days in a semi-confused state, suffering from headaches and nightmares about the Germans wanting to behead him. Some of these nightmares happened while he was awake, and in those moments, he could recognize them as fake. By April 1917, he mentioned that he had always been scared, even during the day, of being injured and was particularly troubled by the fear of shells. He also struggled with bedwetting, which could potentially develop into a chronic condition and affect his memory and focus. While he wasn't considered mentally deficient, he had only average intelligence, and his emotions, according to Duprat, were strong enough to prevent any complete understanding or resolution of his situation through reasoning.
An affective complex, passing from the surprise of the shell-shock over to a fright based on clear though wrong ideas of what might happen to him, had left him without sufficient power of autocritique.
An emotional mix, shifting from the shock of trauma to a fear rooted in clear but inaccurate ideas of what could happen to him, had left him without enough ability for self-reflection.
Weakling, twice buried by shell explosions in one day: Change of character; fear; three fugues (“It is stronger than I am”).
Weakling, twice buried by shell explosions in one day: Change of character; fear; three breakdowns (“It is stronger than I am”).
Case 52. (Pactet and Good fellow, July, 1917.)
An infantryman, Class of 1913, at the front from September, 1914, had a somewhat infantile build physically but was intellectually of average powers, having been a type-setter (three years in a job). However, the confined life had borne hard upon him and his father put him on a farm. He passed through his military service successfully, though he was given two weeks in the guardhouse for overstaying Easter leave. He was suggestible enough at this time to think that he would not be punished very severely, since there were other men whose leaves did not expire at the same time as his own.
An infantryman from the Class of 1913 had been at the front since September 1914. He had a somewhat youthful physique but was of average intelligence, having worked as a typesetter for three years. However, the confined life had taken a toll on him, and his father sent him to work on a farm. He completed his military service successfully, although he spent two weeks in the guardhouse for overstaying his Easter leave. During this time, he was impressionable enough to believe he wouldn’t be punished too harshly, since there were other men whose leaves didn’t end at the same time as his.
He was buried twice in the same morning, March, 1915, at Bois Le Prêtre, spent four or five days in hospital, and went back to his battalion. But now there was a change in his character. Formerly indifferent to danger, he was now apprehensive every time he went to the line and felt an almost irresistible impulse to make for the rear. He was condemned to five years in prison, June, 1915, but was finally sent back to the front.
He was buried twice in the same morning, March 1915, at Bois Le Prêtre, spent four or five days in the hospital, and then returned to his battalion. But now, there was a change in his character. He used to be indifferent to danger, but now he felt anxious every time he went to the front and had an almost overpowering urge to retreat. He was sentenced to five years in prison in June 1915, but eventually, he was sent back to the front.
However, in July he left his company a second time as it was going into the trenches, and this time the captain simply asked him to do better. A third fugue, a few weeks later, sent him back to court-martial, and thence to be examined by alienists. He was perfectly conscious at the time of the fugues and understood his duties and possible punishments. All he would say was, “It is stronger than I am.” Fear outweighed every consideration after the episode of the shell burials.
However, in July he left his company for the second time as it was heading into the thick of battle, and this time the captain just asked him to improve. A third episode a few weeks later sent him back to court-martial and then to be examined by mental health professionals. He was fully aware during the episodes and understood his responsibilities and potential consequences. All he would say was, “It is stronger than I am.” Fear overshadowed every consideration after the incident with the shell burials.
The man may be regarded as a hypobulic, somewhat feebleminded person, able to get on in civil life but thrown out of gear by war. Of course, the concept of fear as a disease can easily be overdone; however, here was a case in which three desertions occurred; the third after severe punishment. In the differential diagnosis, epilepsy, alcoholism, impulsive poriomania, must be considered, as well as feeblemindedness.
The man could be seen as someone with limited willpower and a somewhat weak mind, capable of getting by in everyday life but disturbed by his experiences in war. Naturally, the idea of fear being a sort of illness can be exaggerated; however, this situation involved three desertions, the last one happening after serious punishment. In the process of differential diagnosis, we should take into account epilepsy, alcoholism, impulsive wandering behavior, along with mental weakness.
III. EPILEPTOSES
(THE EPILEPTIC GROUP)
Diagnosis “epilepsy” revised to neurosyphilis.
Diagnosis “epilepsy” changed to neurosyphilis.
Case 53. (Hewat, March, 1917.)
A Scotch soldier, in the Royal Navy, 43, was admitted to the Royal Victoria Hospital at Netley, as major epilepsy. He had been 12 years a stoker, and 16 years before admission had suffered from syphilis, a chancre locally treated with black wash, without secondary rash.
A Scottish soldier in the Royal Navy, 43, was admitted to the Royal Victoria Hospital at Netley due to severe epilepsy. He had worked as a stoker for 12 years and had suffered from syphilis 16 years prior to his admission, which was treated locally with black wash, without any secondary rash.
After leaving the Navy, he had worked in a fire-brigade and as dock laborer. He had been very alcoholic when funds permitted, although never “primed.” His first convulsive seizures came at 40, while working at the docks, following a night on which he had drunk a bottle of whiskey. He thought he had been about half an hour in the fit.
After leaving the Navy, he worked in a fire brigade and as a dock worker. He had been quite an alcoholic when he could afford it, although he was never “primed.” His first seizures happened when he was 40, while he was working at the docks, after a night when he had drunk a bottle of whiskey. He thought he had been in the seizure for about half an hour.
He joined the A. S. C., January, 1915; served in France; later at Salonica. He had eight convulsive seizures, some in France, and others at Salonica, always after much rum.
He joined the A. S. C. in January 1915 and served in France, then later in Salonica. He experienced eight convulsive seizures, some while in France and others in Salonica, always after drinking a lot of rum.
The man was tall, powerfully built, without visceral disease, speech defect, or other symptoms except that both pupils showed the typical Argyll-Robertson phenomenon. The deep reflexes of arms and lower legs were increased. The superficial reflexes were diminished, and the Wassermann reaction strongly positive. A seizure was observed by Hewat and the diagnosis of major epilepsy was revised. The diagnosis of cerebrospinal syphilis, non-paretic, was preferred to that of paresis on account of the absence of all the ordinary symptoms of paresis and of tremor. It might be asked whether these fits were chiefly alcoholic in origin. However, the patient had two or three fits while in hospital during a period of eight teetotal weeks. Hewat remarks that the case suggests that the serum of any patient developing epileptiform seizures for the first time say between 35 and 50 years of age, should be given the Wassermann test.
The man was tall, well-built, and didn't have any serious health issues, speech problems, or other symptoms, except that both of his pupils showed the typical Argyll-Robertson phenomenon. His deep reflexes in his arms and lower legs were heightened. The superficial reflexes were reduced, and the Wassermann reaction was strongly positive. Hewat observed a seizure and reconsidered the diagnosis of major epilepsy. The diagnosis of non-paretic cerebrospinal syphilis was favored over paresis due to the lack of the usual symptoms of paresis and tremor. One might wonder if these seizures were mainly due to alcohol. However, the patient had two or three seizures while in the hospital during a time of eight weeks without alcohol. Hewat notes that this case suggests that the serum of any patient experiencing epileptiform seizures for the first time, say between the ages of 35 and 50, should undergo the Wassermann test.
Syphilis may bring out epilepsy in a subject having taint.
Syphilis can trigger epilepsy in someone with the condition.
Case 54. (Bonhoeffer, July, 1915.)
A man of 35 in the Landwehr acquired syphilis some time in the summer of 1914. He was a good soldier, passed through several clashes, and was promoted to Unteroffizier.
A 35-year-old man in the Landwehr contracted syphilis sometime in the summer of 1914. He was a good soldier, saw action in several battles, and was promoted to Unteroffizier.
To understand what followed it must be stated that he had been a bed-wetter to 11, had been practically a teetotaler (Bonhoeffer’s point is perhaps that otherwise epilepsy might have developed sooner?), and, when he did drink, vomited almost at once, and had amnesia for the period of drunkenness. His father drank. His sister had fits as a child.
To understand what happened next, it’s important to note that he had been a bed-wetter until he was 11, was mostly a teetotaler (Bonhoeffer seems to suggest that otherwise, epilepsy might have developed earlier?), and when he did drink, he would almost immediately throw up and forget the time he was drunk. His father drank. His sister had seizures as a child.
February, 1915, the Unteroffizier lost appetite, got headaches, and went to hospital for a time. Upon getting better, he was sent on service to Berlin. In a Berlin hotel he had his first convulsions and unconsciousness, biting his tongue. He was confused for several days, and, when he had become clear, had a pronounced retrograde amnesia together with a tendency to fabricate a filling of events for the lost period.
February 1915, the Unteroffizier lost his appetite, got headaches, and went to the hospital for a while. Once he got better, he was sent to serve in Berlin. In a hotel in Berlin, he had his first convulsions and lost consciousness, biting his tongue. He felt confused for several days, and when he finally regained clarity, he had significant retrograde amnesia along with a tendency to fill in the gaps with fabricated events from the lost period.
This retrograde amnesia is uncommon in epilepsy and suggests organic disease. No sign of such was found, or signs of the epileptic make-up. The serum W. R. was negative. On the whole, Bonhoeffer regards the epilepsy as “reactive” to the syphilis, as a syphilogenic epilepsy.
This type of memory loss is rare in epilepsy and indicates an underlying health issue. No evidence of such was found, nor any signs typical of epilepsy. The serum W. R. was negative. Overall, Bonhoeffer considers the epilepsy to be “reactive” to the syphilis, describing it as syphilogenic epilepsy.
Alcoholism caused amnesia in this man in the same way as the syphilitic epilepsy now did.
Alcoholism caused memory loss in this man just like the syphilitic epilepsy does now.
Re epilepsy and syphilis, Bonhoeffer states that he has repeatedly seen syphilis giving no other symptoms than epilepsy develop in the campaign. At the same time, Bonhoeffer does not find that the incubation period in paresis can be shortened by war factors; at all events, by the exhaustion factor in war (see Case 25). It might be questioned whether the above case (54) was not psychogenic; that is, whether the syphilis did not act in combination with being sent to Berlin on service as a psychic factor. However, this epilepsy on the whole seemed not psychogenic.
Re epilepsy and syphilis, Bonhoeffer mentions that he has often observed syphilis causing no other symptoms than epilepsy developing during the campaign. At the same time, Bonhoeffer does not believe that the incubation period in paresis can be shortened by factors of war; at any rate, not by the exhaustion factor related to war (see Case 25). It could be debated whether the case mentioned above (54) was not psychogenic; that is, whether the syphilis did not interact with being sent to Berlin on duty as a psychological factor. However, this epilepsy overall seemed not to be psychogenic.
Syphilis in a psychopathic subject. Convulsions 5 days after Dixmude.
Syphilis in a psychopathic individual. Seizures 5 days after Dixmude.
Case 55. (Bonhoeffer, July, 1915.)
A soldier in the reserves, 23, was, subsequently to his being brought to hospital, described by his wife as a rather over-sensitive fellow, who could hardly look at blood and was meticulous about the household. He had always been subject to headaches, especially after hard work. However, he had passed through his military training well in 1910, not even having been bestraft.
A 23-year-old soldier in the reserves, after being brought to the hospital, was described by his wife as a pretty sensitive guy who could hardly handle the sight of blood and was very particular about the household. He had always dealt with headaches, especially after strenuous work. However, he had gotten through his military training just fine in 1910, without even being punished.
He began service in October and fought at Dixmude on the 19th. On the 24th in the trench and while being carried back, he had several spells of pallor, falling stiff, and then having convulsions. Brought finally to the Charité in Berlin, he had more spells of sudden pallor, collapse with brief convulsions, tossings in bed, as well as absences, post-convulsive headaches, and mild bad humor.
He started his service in October and fought at Dixmude on the 19th. On the 24th, while in the trenches and being carried back, he experienced several episodes of pale skin, falling stiff, and then having seizures. Eventually taken to the Charité in Berlin, he had more sudden bouts of paleness, collapsing with brief seizures, tossing in bed, as well as episodes of staring off into space, headaches after the seizures, and a bit of irritability.
There were numerous attacks several days apart in the first seven weeks. The patient was not of an “epileptic” disposition, though readily dissatisfied and headachey.
There were several attacks a few days apart in the first seven weeks. The patient did not have an "epileptic" tendency, though was often unhappy and had headaches.
The serum W. R. was positive. Treatment by mercurial inunctions. No further convulsions. Prognosis doubtful.
The serum W. R. was positive. Treatment involved mercurial ointments. No more convulsions occurred. Prognosis uncertain.
Re epilepsy and the war, during the first six months Bonhoeffer observed 33 cases in the Charité Clinic in Berlin. Twenty of these 33 cases, unlike Case 55, had attacks before the war, although ten of these had become epileptic rather late, namely, after the period of active military service, at ages from 22 to 27. The development of epilepsy like Case 55’s is not without frequent precedent.
Re epilepsy and the war, during the first six months Bonhoeffer noted 33 cases at the Charité Clinic in Berlin. Twenty of these 33 cases, unlike Case 55, had seizures before the war, though ten of them developed epilepsy relatively late, specifically after their active military service, at ages ranging from 22 to 27. The onset of epilepsy like Case 55’s is not uncommon.
Bonhoeffer states that aside from epilepsy directly due to brain injury by shells, there has been no certain case in which we have the right to regard the war itself as the total cause of the epilepsy. Some, like Case 55, are of syphilitic origin. No subject with a severe long-standing epilepsy has been able to get into the field, according to Bonhoeffer; when they do, they prove constitutional subjects.
Bonhoeffer says that aside from epilepsy caused directly by brain injury from shells, there hasn't been any clear case where we can fully attribute the condition to the war itself. Some cases, like Case 55, are due to syphilis. According to Bonhoeffer, no one with severe, long-lasting epilepsy has managed to serve in the field; when they do, they end up being fundamentally unsuitable.
An epileptic imbecile, court-martialed.
A court-martialed person with epilepsy.
Case 56. (Lautier, 1916.)
A Belgian soldier was condemned by court-martial February 27, 1915, to five years imprisonment for leaving his post in the presence of the enemy. It seems that he was mounting guard with two of his comrades and all three left to eat as no food had been brought to them.
A Belgian soldier was sentenced by court-martial on February 27, 1915, to five years in prison for abandoning his post in the presence of the enemy. It appears that he was on guard duty with two of his fellow soldiers, and all three left to eat since no food had been delivered to them.
A physician examined the Belgian soldier and declared him responsible, although a little sick. All three were condemned to imprisonment. The Belgian attracted attention in prison through crises of anxiety and agitation; he had terrible nightmares, seeing Germans in his cell and hearing gunshots. He was accordingly sent to a special infirmary of the dépôt, whence July 24 to Sainte-Anne, July 26 to Villejuif. He talked Flemish, hardly understanding French, and spoke slowly and with difficulty. He hardly knew how to read or write. He had been a truckman.
A doctor evaluated the Belgian soldier and said he was accountable, though somewhat unwell. All three were sentenced to prison. The Belgian stood out in prison due to episodes of anxiety and restlessness; he experienced horrific nightmares, seeing Germans in his cell and hearing gunfire. As a result, he was transferred to a special infirmary at the dépôt, from there on July 24 to Sainte-Anne, and then on July 26 to Villejuif. He spoke Flemish, barely understood French, and talked slowly and with difficulty. He had little ability to read or write. He used to work as a truck driver.
At 18, this soldier, according to his own account, began to have nervous crises in which he fell, lost consciousness, bit his tongue, foamed at the mouth and urinated involuntarily. The attacks were somewhat rare. His father sent him in 1910 to Gheel where he stayed two years. Returning home he helped his father in the trucking work.
At 18, this soldier, based on his own account, started experiencing nervous breakdowns where he would collapse, lose consciousness, bite his tongue, foam at the mouth, and accidentally urinate. The episodes were somewhat infrequent. His father sent him to Gheel in 1910, where he stayed for two years. After returning home, he assisted his father with the trucking work.
When the Germans came the family fled to France and, about the end of 1914, he was put into the military service and sent to the front after a very short period of instruction.
When the Germans arrived, the family escaped to France, and around the end of 1914, he was drafted into the military and sent to the front after a brief training period.
The man had followed the example of his two comrades without taking the slightest thought. He did not understand the gravity of his act. He was not remorseful, regretful or angry against his judges. He was well oriented but quite indifferent. He was a tall, intelligent looking man with adherent lobules, slight facial asymmetry and evidence of tongue biting. He wrote like a child and read slowly, spelling out the complicated words. He was employed at various manual tasks during his sojourn at the asylum and had no epileptic attack. He was given over to the Belgian military authorities October 5, 1915.
The man had followed the example of his two companions without giving it any thought. He didn’t grasp the seriousness of his actions. He felt no remorse, regret, or anger towards his judges. He was aware but completely indifferent. He was a tall, intelligent-looking man with attached earlobes, slight facial asymmetry, and signs of tongue biting. He wrote like a child and read slowly, sounding out the complicated words. He was engaged in various manual tasks during his stay at the asylum and didn’t experience any epileptic seizures. He was handed over to the Belgian military authorities on October 5, 1915.
Seizures in a feebleminded subject—psychogenic components.
Seizures in a person with cognitive impairment—psychogenic factors.
Case 57. (Bonhoeffer, July, 1915.)
A 21-year old tailor, unused to marching, went into the field in August. A month later, after a period of long standing, he was nauseated and fell in a faint. Upon waking, his fingers were stiff and he had pains in his legs. He got better in the reserve hospital and was sent back to the line. On the way he had a similar seizure, with nausea and fainting. On the way back to Berlin, he had a seizure in the railway station, and was carried to the Charité Clinic. At the clinic he stated that he could feel an attack come on; that he first had Angst all over his body, and that it was hot inside of his head. Latterly he had been able to stop an attack by clenching his teeth, after which the attack would not proceed except that all became black before his eyes.
A 21-year-old tailor, who wasn’t used to marching, entered the field in August. A month later, after standing for a long time, he felt nauseous and fainted. When he woke up, his fingers were stiff and his legs hurt. He recovered in the reserve hospital and was sent back to the front. On his way, he experienced a similar episode, with nausea and fainting. While returning to Berlin, he had another episode at the train station and was taken to the Charité Clinic. At the clinic, he mentioned that he could sense an attack coming on; that he first felt a wave of anxiety throughout his body and that his head felt hot inside. Recently, he had been able to halt an attack by clenching his teeth, after which the attack wouldn't continue except that everything turned black before his eyes.
He was observed for four weeks but no seizure appeared. He was somatically negative; his Wassermann reaction was negative. There was nothing hysterical about his make-up; he was somewhat surly and of low mental grade. He was unwilling to walk alone for fear of attacks.
He was monitored for four weeks, but no seizures occurred. He tested negative for physical issues; his Wassermann reaction was also negative. There was nothing hysterical about his personality; he was a bit grumpy and had a low level of intelligence. He was reluctant to walk alone due to fear of attacks.
As to the heredity of this soldier nothing is known. He had been an illegitimate child; he was a sleep-walker in childhood; he had sometimes spoken out loudly in sleep as a boy. At school he had been somewhat backward, fought readily with his mates, and often complained of dizziness and headaches. He could not stand smoking or drinking well, getting drunk upon two glasses of beer. He had not held positions well. He became a pionier in 1914, working chiefly as a tailor.
As for this soldier's background, not much is known. He was an illegitimate child, a sleepwalker as a kid, and occasionally talked in his sleep when he was young. He had some trouble in school, often got into fights with his peers, and frequently complained about feeling dizzy and having headaches. He couldn't handle smoking or drinking well, getting drunk after just two beers. He didn't do well in jobs either. He became a pionier in 1914, mainly working as a tailor.
Early in his time as a soldier he had obtained an ulcer of the glans, which had been excised and burned. There had been no secondary symptoms.
Early in his time as a soldier, he developed an ulcer on his glans, which was surgically removed and cauterized. There were no additional symptoms.
According to Bonhoeffer, this is an example of a not infrequent condition. Although the attack itself and the habitus of the patient did not look hysterical, the manner in[70] which the attacks repeated themselves speaks for psychogenic components. Just as genuine hysterical attacks may be looked on as reactions to unpleasant situations, so may these attacks. In fact, we are probably dealing with an hysterical fixation of the symptoms of emotional fright like those in the true hysterias following shell explosion. A great many of the phenomena of Shell-shock, to use the English phrase, are not in and of themselves of a psychogenic nature, but they are, according to Bonhoeffer, psychogenically liberated under the influence of unpleasant ideas.
According to Bonhoeffer, this is a common condition. While the attack itself and the patient's demeanor didn't appear hysterical, the way the attacks recurred suggests there are psychogenic factors at play. Just as genuine hysterical attacks can be seen as reactions to distressing situations, these attacks can be viewed in the same light. In fact, we are likely dealing with a hysterical fixation of symptoms stemming from emotional fright, similar to those seen in genuine hysteria after a shell explosion. Many of the symptoms of Shell-shock, as it’s known in English, aren't inherently psychogenic, but according to Bonhoeffer, they are triggered by unpleasant thoughts.
Re reactive epilepsies, Bonhoeffer considers that there is a group of reactive epilepsies in which the war process plays an important part. The prognosis of these cases ought to be relatively favorable. In point of fact, Case 57, although a feebleminded subject, seems to have had a relatively favorable prognosis: at all events, no new seizures appeared under prolonged medical observation. These reactive seizures may occur in cases with a labile vasomotor system. They are, according to Bonhoeffer, aligned rather more with hysteria than with genuine epilepsy. Genuine epilepsy has not been developed in the war cases observed by Bonhoeffer except where an endogenous factor was clearly in evidence; or else where there was the requisite antebellum soil for the development of an epilepsy. In short, genuine epilepsies developing in the war are all, according to Bonhoeffer, predispositional. The antebellum soil was clearly in evidence in Case 57. Even before the war, according to Bonhoeffer, many German soldiers during the period of military service gave evidence of their epileptic soil by sundry suspicious phenomena. Among these were fainting spells during hard drilling and other exercises, spells of enuresis, abnormally deep sleep, and even phenomena of somnambulism. One of the Bonhoeffer epileptics had been released during his reservist practice as unfit for military service, and had only been put into the line at his own urgent request at the outbreak of the war. Three volunteers concealed their epileptic history. One man, who had had merely petit mal attacks before the war, regarded them as of little consequence, entered the service, and developed epilepsy.
Re reactive epilepsies, Bonhoeffer believes there is a category of reactive epilepsies where the war process plays a significant role. The outlook for these cases should be relatively positive. In fact, Case 57, even though an intellectually challenged individual, seems to have had a fairly good prognosis: in any case, no new seizures were observed during extended medical monitoring. These reactive seizures can happen in individuals with an unstable vasomotor system. According to Bonhoeffer, they are more closely related to hysteria than to true epilepsy. True epilepsy has not developed in the war cases studied by Bonhoeffer unless there was a clear endogenous factor involved, or where there was the necessary pre-war environment for the development of epilepsy. In summary, true epilepsies arising from the war are all, according to Bonhoeffer, predispositional. The pre-war situation was clearly evident in Case 57. Even before the war, Bonhoeffer noted that many German soldiers during their military service showed signs of their epilepsy through various suspicious symptoms. Among these were fainting spells during intense training and drills, episodes of bedwetting, abnormally deep sleep, and even signs of sleepwalking. One of the individuals Bonhoeffer studied had been discharged during his reservist duty as unfit for military service and had only joined the front lines at his own strong insistence when the war started. Three volunteers hid their history of epilepsy. One man, who had only experienced petit mal seizures before the war, considered them insignificant, enlisted, and subsequently developed epilepsy.
Responsibility of a drunken epileptic.
Responsibility of an intoxicated epileptic.
Case 58. (Jeweler, March, 1917.)
The question of responsibility arose in the case of a soldier who left his camp the morning of October 23, 1916, and went to a neighboring place, where he drank, with four others, two quarts of wine. At about three o’clock in the afternoon, his captain met him on the street, lost, and looking drunk. He told him that he would send him to the trenches in the evening. The man lay down and went to sleep. At about six o’clock, it was found that he could not put on his equipment alone, and in fact threatened the other men with his bayonet, and then went to sleep. He woke up and explained that he had had one of his nervous crises. He remembered the matter of the bayonet but had forgotten everything else about the struggle.
The question of responsibility came up in the case of a soldier who left his camp on the morning of October 23, 1916, and went to a nearby place, where he drank, with four others, two quarts of wine. At around three o’clock in the afternoon, his captain saw him on the street, looking lost and drunk. He told him that he would send him to the trenches in the evening. The soldier lay down and fell asleep. By about six o’clock, it was clear that he couldn't put on his equipment by himself, and he even threatened the other men with his bayonet before lying down again to sleep. He later woke up and explained that he had experienced one of his nervous crises. He remembered the incident with the bayonet but had forgotten everything else about the struggle.
This soldier was 29 years old, the son of an alcoholic, and the ninth child of a mother who died shortly after her tenth pregnancy. He had had measles and bronchitis as a child, and in childhood had had bad dreams; at the age of ten he had swooning spells. He became a quarryman and a habitual drinker, subject to dyspepsia, nightmares, and nocturnal cramps. There had never been any crises, however, up to wartime.
This soldier was 29 years old, the son of an alcoholic, and the ninth child of a mother who died shortly after her tenth pregnancy. He had measles and bronchitis as a child and suffered from bad dreams; at the age of ten, he experienced fainting spells. He became a quarry worker and a regular drinker, prone to indigestion, nightmares, and nighttime cramps. However, there had never been any crises until wartime.
January, 1916, when a shell burst near him, the first sharply-defined epileptoid crisis came, and was followed by a number of others, either on leave or on service, March 8, June 2, and July 13. These attacks showed a sudden fall without warning, loss of consciousness, convulsions, tongue biting, incontinence of urine, a period of more or less coördinate agitation at the time consciousness was reappearing, sometimes a fugue, and often amnesia for the whole. He had a scar on the left border of the tongue.
January 1916, when a shell exploded nearby, he experienced the first clear epileptoid seizure, followed by several others during leave or service, on March 8, June 2, and July 13. These episodes were marked by a sudden collapse without warning, loss of consciousness, convulsions, tongue biting, urinary incontinence, and a phase of varying levels of coordinated movement as consciousness returned, sometimes with a fugue state, and often a complete loss of memory for the episode. He had a scar on the left side of his tongue.
Should this epilepsy be regarded as entailing irresponsibility? He left camp before the crisis, accordingly in a period when he was in full possession of consciousness and will, and he had gotten into an irregular situation by drunkenness[72] before his epileptic crisis started in. His struggle with his comrades, however, appears to be a portion of a post-critical dazed state. The medicolegal decision, therefore, was that he was guilty of leaving his command but not of the other misdemeanor. Considering the general nature of epilepsy, the responsibility of this man for the whole adventure is rather slight. The Council, however, condemned the man to five years of labor, without admitting that the crisis following so soon the actual misdemeanor should argue a diminution of responsibility.
Should this epilepsy be seen as a reason for irresponsibility? He left camp before the crisis, at a time when he was fully aware and in control, and he had gotten himself into a difficult situation due to drinking[72] before his epileptic episode began. His struggle with his comrades seems to be part of a confused state after the attack. Therefore, the legal decision was that he was guilty of abandoning his post but not of the other offense. Considering the general nature of epilepsy, this man’s responsibility for the entire incident is relatively minimal. However, the Council sentenced him to five years of hard labor, without acknowledging that the crisis occurring so soon after the actual offense should lessen his responsibility.
Re epilepsy in the army, Lépine notes the serious theoretical and practical problems to which it gives rise. In the first place, epilepsy occurs in the army more frequently than in the same number of men in civilian life. Consequently, the diagnosis as to the really epileptic nature of the attacks observed is not too easy. Again, the situation affords much opportunity for simulation (see, for example, the case of sham fits (Case 78, Hurst), and the case of epileptoid attacks controllable by the will (Case 79 of Russell)). Wounds may produce it, and even wounds which do not affect the brain; besides which, a variety of war conditions, short of trauma, may produce it. When the ordinary impulsiveness of the epileptic turns into automatism and to epileptic equivalents (états seconds), much of medicolegal interest may happen. Case 58 was just short of a murderer. Cases of actual murder in epileptic equivalents have been known under military conditions. Fugues with amnesia for the phenomena (which look to the military man like intentional desertions) form another group of epileptic events; but aside from the manias and the fugues, there are still more dubious epileptoid phenomena of a delusional and confusional nature, such that the proof of epilepsy comes only afterward, when frank convulsions supervene. Re fugues and desertion (the most frequent of military delinquencies according to Régis), we may think of the fugue reaction, according to Lépine, as a natural reaction on the part of both the true delinquent and the mentally sick subject. The loss of liberty, alcohol, fatigue, minor phenomena of commotio cerebri, may lead to states of mental depression that favor the fugue. It is an[73] affair of the greatest delicacy for the expert to build up again the exact plight of the soldier at the time of his desertion. Special inquiry must be made of the man’s mates. Only in this way can the wheat be separated from the chaff and punishment allotted to those only who deserve it.
Re epilepsy in the army, Lépine points out the significant theoretical and practical issues it raises. First of all, epilepsy occurs in the military more often than in the same number of civilians. As a result, determining the true epileptic nature of the observed attacks is quite challenging. Moreover, the environment provides ample opportunity for feigning symptoms (see, for example, the case of fake seizures (Case 78, Hurst), and the instance of epileptoid attacks that can be controlled by will (Case 79 of Russell)). Injuries can cause it, even those not affecting the brain; in addition, various wartime conditions, without trauma, may also trigger it. When the usual impulsiveness of an epileptic turns into automatism and epileptic equivalents (états seconds), many medicolegal issues can arise. Case 58 was nearly a murderer. There have been instances of actual murder during epileptic equivalents in military contexts. Fugues with amnesia for the events (which look to military personnel like intentional desertions) form another category of epileptic incidents; but aside from manias and fugues, there are still vaguer epileptoid phenomena of a delusional or confusional nature, where proof of epilepsy only comes later, when clear convulsions occur. Re fugues and desertion (the most common military offenses according to Régis), we might consider the fugue reaction, as described by Lépine, to be a natural response from both the true offender and the mentally ill individual. Factors like loss of freedom, alcohol, fatigue, and minor incidents of commotio cerebri can contribute to mental states that promote the fugue. It is a[73] highly sensitive matter for an expert to reconstruct the exact situation of the soldier at the time of his desertion. Special inquiries must be made of the soldier’s comrades. Only in this way can we differentiate between those truly guilty and those who should not be punished.
According to Lépine, there are fewer guilty fugitives than there are innocent ones, or at least partially innocent ones. In the decision, one takes account of the duration, the course, and the peculiarities in the termination of the suspicious flight. According to the military code, there are cases like Case 58 in which the fugue itself was carried out in an unconscious state, and yet in which the martial responsibility of the man was absolute. Drunkenness is no excuse for the fugue, even if the latter is automatically carried out. Of course, the paretic is not responsible for his fugue any more than the organic dement, the delirious uremic, or the chronic alcoholic, who is already severely demented. For a case of this sort, see Case 1 (Briand).
According to Lépine, there are more innocent fugitives than guilty ones, or at least partially innocent ones. In the decision, factors like the duration, the course, and the specific details of the suspicious escape are considered. According to military code, there are situations like Case 58 where the escape was done in an unconscious state, yet the person is still fully responsible for their actions. Being drunk is not a valid excuse for the escape, even if it happens automatically. Of course, someone with paretic conditions is not responsible for their escape any more than someone with organic dementia, delirious uremia, or a chronic alcoholic who is already significantly demented. For a case of this kind, see Case 1 (Briand).
In the differential diagnosis, we must also consider that fugues may be carried out in confused states as well as at times in various paranoid states, and even in melancholia.
In differential diagnosis, we also need to consider that fugues can occur during confused states, as well as sometimes in various paranoid states, and even in depression.
A disciplinary case: Epilepsy.
A disciplinary case: Seizures.
Case 59. (Pellacani, March, 1917.)
A Milanese workman, 28, was exposed to the sun on sentry-go and had an attack of convulsions, on awaking from which he found himself in hospital. He always had attacks in reaction to emotion. One day, in a quarrel provoked by jealousy concerning a prostitute, he apparently lost his mind, whipped out a hunting-knife, and wounded a comrade. Thereafter he lay unconscious until the next day. The court-martial decided that he was not fully responsible.
A 28-year-old worker from Milan was out in the sun while on duty and had a seizure. When he came to, he found himself in the hospital. He had always experienced seizures in response to strong emotions. One day, during a heated argument fueled by jealousy over a prostitute, he seemingly lost control, pulled out a hunting knife, and injured a fellow worker. After that, he was unconscious until the following day. The court-martial ruled that he wasn't completely responsible for his actions.
Eventually, he was sent from the front for having insulted and struck a superior officer. The report read also that he was a prey to delirium and had frothed at the mouth. In the interior he had convulsive attacks, with falling and loss of consciousness. He told of arguing with a sergeant about a bicycle, of seeing darkness before his eyes like a veil, and of subsequent amnesia. In hospital he had intense headaches at times, with spells of sullenness, hostility, and complaints concerning nurses and attendants and other patients. At other times, he was quiet and comfortable. One day he went into an excitement and wept, asking to be sent back to the army, striking the table with his fist and head. He then screamed, flew into a passion, and fell to the ground in semi-stupor, shaking his body and trying to kick and knock away those who intervened. He was placed in bed but remained agitated and unconscious, with anesthesia and frothing at the mouth. The abdominal and cremaster reflexes were absent in this attack, and the pupils were rigid and myotic. The pulse was rapid and the blood pressure high. Afterwards he was sleepy, stupid and weary, and showed fine rapid tremors of hands, tongue, and eyelids. The abdominal reflexes now returned in excess, and a marked dermatographia developed.
Eventually, he was sent back from the front for insulting and hitting a superior officer. The report also stated that he was experiencing delirium and had frothing at the mouth. Inside, he had convulsive episodes, with fainting and loss of consciousness. He talked about arguing with a sergeant over a bicycle, seeing darkness like a veil before his eyes, and then forgetting everything afterward. In the hospital, he sometimes had severe headaches, along with episodes of irritability, hostility, and complaints about the nurses, attendants, and other patients. At other times, he was calm and comfortable. One day, he became very upset and cried, begging to be sent back to the army, hitting the table with his fist and head. Then he screamed, lost his temper, and collapsed on the ground in a daze, shaking his body and trying to kick and push away those who tried to help. He was put in bed but stayed restless and unconscious, with anesthesia and frothing at the mouth. The abdominal and cremaster reflexes were absent during this episode, and his pupils were stiff and constricted. His pulse was fast and his blood pressure was high. Later, he was sleepy, confused, and exhausted, showing fine, rapid tremors in his hands, tongue, and eyelids. The abdominal reflexes returned excessively, and he developed noticeable skin markings.
Upon investigation, it was found that the patient’s father was also an epileptic and was alcoholic; that one paternal uncle had died in an asylum; another of apoplexy; that two[75] maternal uncles were chronic alcoholics (one in an institution); that an alcoholic brother had been six times convicted of assault and battery; that a sister had howling, crying, and hair-pulling spells, throwing herself to the ground. The patient himself had had an early Bright’s disease and had always been an undisciplined, excitable, and impulsive boy, sometimes kept out of school. His first conviction was at 18, for assaulting a policeman, and he had been arrested four further times for assault and battery. He stated that his convulsive attacks with the veil before the eyes came on when he was irritated or had taken cold, or had drunk to excess, or had over-exerted himself. He said he suffered from intense headache, weariness, and sleepiness after an attack. He always bit his tongue at the same period. Irritation and exertion sometimes caused attacks of dizziness and vertigo without unconsciousness. Alcoholism; ulcer in an inguinal gland. He had been confined in an asylum 40 days for epilepsy, attacks of which had become more frequent after he had heard of his father’s death.
Upon investigation, it was found that the patient’s father was also an epileptic and struggled with alcoholism; one paternal uncle had died in a mental institution, another from a stroke; two maternal uncles were chronic alcoholics (one in an institution); an alcoholic brother had been convicted six times for assault and battery; and a sister had episodes of howling, crying, and hair-pulling, often throwing herself to the ground. The patient himself had suffered from early kidney disease and had always been an undisciplined, excitable, and impulsive boy, sometimes missing school. His first conviction was at 18 for assaulting a policeman, and he had been arrested four more times for assault and battery. He reported that his convulsive episodes with a blurry vision occurred when he was irritated, caught a cold, drank excessively, or overexerted himself. He mentioned experiencing intense headaches, fatigue, and sleepiness after an attack. He consistently bit his tongue during these episodes. Irritation and exertion sometimes led to dizziness and vertigo without loss of consciousness. Alcoholism; ulcer in a groin gland. He had been held in a mental institution for 40 days for epilepsy, which had become more frequent after learning about his father’s death.
Re violence and epilepsy, Lépine remarks that a pure epilepsy unclouded by alcoholism may occasionally give rise to acts of extreme violence, but these pure epileptic violences are infinitely rarer than the alcoholic ones. The Milanese was in point of fact alcoholic, and in his ancestry were a number of alcoholics as well as epileptics. According to Lépine, when subjects are “out for blood,” they are almost always either, like this Milanese, hereditary alcoholics, or else strongly predisposed subjects, or even the offspring of the insane.
Re violence and epilepsy, Lépine notes that pure epilepsy not mixed with alcoholism can sometimes lead to extreme acts of violence, but these pure epileptic outbursts are much rarer than those caused by alcoholism. The Milanese man was indeed an alcoholic, and his family history included both alcoholics and epileptics. According to Lépine, when people are "out for blood," they are almost always hereditary alcoholics like this Milanese man, or they have a strong predisposition to it, or they might even be the children of those with mental illness.
A disciplinary case: Epileptic attacks with amnesia.
A disciplinary case: Seizures with memory loss.
Case 60. (Pellacani, March, 1917.)
A Veronese, 23, quarrelled with his comrades, and one day wounded one. Another time, when reproved by a superior, he struck him with a shoe; and at still another time, hurled himself upon his superior officer and bore him to the ground. Yet he seemed to have a perfect amnesia for all these violent acts. At other times, he had convulsive attacks with a mental state which seemed to combine anger and depression, after which he would fall to the ground, lose consciousness, go into clonic spasms, spit bloody saliva, and cause wounds and abrasions upon his body. Once, after such an attack, he passed into a brief excited spell. Finally he was so insubordinate and violent to superior officers, that he was brought under hospital observation, having been excited and confused for a day.
A 23-year-old from Verona got into fights with his friends, and one day he injured one of them. Another time, when scolded by a superior, he hit him with a shoe; and on yet another occasion, he attacked his superior officer and knocked him to the ground. However, he seemed completely oblivious to all these violent actions. At other times, he experienced convulsive fits with a mental state that seemed to mix anger and depression, after which he would collapse, lose consciousness, have muscle spasms, spit out bloody saliva, and injure himself. Once, after such an episode, he went into a brief period of excitement. Eventually, he became so rebellious and aggressive towards his superiors that he had to be placed under hospital observation after being agitated and confused for a day.
Next day he was lucid, oriented, and tranquil; entirely amnestic for what happened the day before, though his acts were sufficiently unusual. He had threatened his superior officer and been reproved and sent to prison to think it over. In prison he had suddenly thrown himself against another innocent person and clutched him tightly about the neck. He threw another violently to the ground and then ran to help the previous victim! Bound fast, he had succeeded in freeing himself and thrown himself furiously against the prison door, whereupon he had fallen to the ground in an epileptic fit. He had tachycardia (120) and a generalized hypalgesia. The vasomotor reactions were excessive.
The next day, he was clear-headed, aware of his surroundings, and calm; completely unaware of what had happened the day before, even though his actions were quite strange. He had threatened his superior officer and was reprimanded and sent to prison to reflect on it. While in prison, he suddenly attacked another innocent person, grabbing them tightly around the neck. He violently threw another person to the ground and then ran to help the first victim! Bound tightly, he managed to free himself and charged furiously at the prison door, collapsing on the ground in an epileptic seizure. He had a rapid heartbeat (120) and reduced sensitivity to pain. The blood flow responses were excessive.
Upon investigation it proved that his mother had been subnormal and that the patient had been constitutionally excitable and unstable, given to attacks of anger and impulsiveness from youth up. In fact, he had been in prison several times for violence. He described himself in his restless spells as feeling a trembling all over his body as if his blood were boiling in his heart and his head, whereupon he would lose knowledge of what he was doing. He had been a[77] quarrelsome boy, pursuing his mates with knives and stones. Once, after arguing with a car conductor, he had broken the car windows, turned everything upside-down, and thrown the conductor into the street.
Upon investigation, it turned out that his mother had been below average in mental capacity, and the patient himself had always been excitable and unstable, prone to anger outbursts and impulsive behavior since he was young. In fact, he had been imprisoned several times for acts of violence. He described his restless episodes as feeling a tremor throughout his body, as if his blood were boiling in his heart and head, after which he would lose awareness of his actions. He had been a[77] confrontational child, chasing his peers with knives and stones. Once, after an argument with a streetcar conductor, he smashed the car windows, wreaked havoc, and threw the conductor onto the street.
Case 60 is clearly in the same group as Case 59. The Veronese falls into the same frame with the Milanese except that he appears not to have been alcoholic. The insubordinations of the Veronese were apparently carried out in a state of unconsciousness. The majority of insubordinates appear not to be epileptics. Some authors have called attention to pathological politeness as an occasional symptom in epilepsy. Perhaps the majority of insubordinate cases are feebleminded or schizophrenic.
Case 60 is clearly in the same group as Case 59. The Veronese fits in the same category as the Milanese, except he doesn’t seem to have struggled with alcoholism. The Veronese's acts of insubordination were likely done without awareness. Most insubordination cases don’t seem to be linked to epilepsy. Some writers have pointed out that excessive politeness can sometimes be a symptom of epilepsy. It’s possible that most insubordinate individuals are either intellectually disabled or have schizophrenia.
Desertion in epileptic fugue.
Desertion during epileptic episode.
Case 61. (Usher, February, 1916.)
A blacksmith from the Rochefort Arsenal, 27 (nothing known as to grandparents; father, now in the fifties, for 30 years in an asylum with frequent attacks of furor; mother, 45, well and apparently well-balanced; brother with the colors, wounded and decorated with the military medal; a cousin-german, who has had a typical epilepsy—in the patient himself enuresis up to 13 or 14, later, less frequently; apparently no tongue-biting; no information as to infectious diseases; graduate from primary school, apprenticed to a blacksmith; an unskilful worker; never able to rise to the level of a frappeur), in 1909 had passed the board of review and been put in the sixth division of the line. Antebellum there was a history that one night at supper, he had slipped away from quarters and gone 30 kilometres, home. His astonished mother sent him back to the military post by railway.
A blacksmith from the Rochefort Arsenal, 27 (no information about grandparents; father, now in his fifties, has been in an asylum for 30 years with frequent bouts of rage; mother, 45, healthy and seemingly well-adjusted; brother in the military, injured and awarded a military medal; a cousin with a typical case of epilepsy—he experienced bedwetting until about 13 or 14, then less frequently; apparently no signs of tongue-biting; no details on infectious diseases; graduated from primary school, trained as a blacksmith; not a skilled worker; never managed to become a frappeur), in 1909 passed the review board and was placed in the sixth division of the line. Before the war, there was an incident when one night at dinner, he slipped away from his quarters and walked 30 kilometers home. His shocked mother sent him back to the military post by train.
Upon the night of May 26-27, 1915, this soldier found himself in the position of a sentry, opposite the enemy. He told his comrade that he had to go away for a time, leaned his gun against a tree, disappeared, and did not return. It was then one o’clock in the morning. At six o’clock, he was found two kilometres away from the lines, in a village. He was in front of a barn where his company had been quartered before taking possession of the advanced posts.
On the night of May 26-27, 1915, this soldier was on sentry duty facing the enemy. He informed his comrade that he needed to step away for a bit, propped his gun against a tree, and vanished without coming back. It was one o’clock in the morning. By six o’clock, he was discovered two kilometers away from the front lines, in a village. He was standing in front of a barn where his company had been stationed before moving to the forward posts.
He was brought up before the military authorities; but upon stating that in civil life he had wandered off several times without knowing where he was going, he was submitted to neurological examination. There was available a letter from his family physician relative to his antebellum military service. It appeared that he had committed a number of breaches of discipline, and that he was regarded by the physicians as a déséquilibré. He had lived with his mother a very quiet and good life; there was no history of sexual irregularity, and no history of illness except a slight catarrhal jaundice. He had frequently suffered from headaches; there[79] had been slight attacks of vertigo of very brief duration. He had never fallen in these fits. From his story it was elicited that he had had absences; his comrades had noticed that he sometimes stopped stock-still with vague eyes, then shortly regained his wits and continued upon his task. Sometimes he would not work without being able to explain why he went away. He would go off for a period and, upon coming to, discover that he had not eaten his meals. There were never, however, any convulsive crises by day or night. He sometimes felt sick, and although there was no medical treatment, from time to time he took bromides upon his own authority, saying he had been ordered to do so by his father. Although habitually of a gentle demeanor, nevertheless he was subject to excessive anger upon slight occasion.
He was taken in front of the military authorities, but when he mentioned that in civilian life he had wandered off several times without knowing where he was going, he was referred for a neurological examination. A letter from his family doctor was available regarding his military service before the war. It seemed that he had broken several disciplinary rules and was considered to be déséquilibré by the doctors. He had lived a very quiet and good life with his mother; there was no record of sexual misconduct, and no history of illness except for a mild case of jaundice. He frequently experienced headaches and occasionally had brief bouts of vertigo, but he never had any falls during these episodes. From his account, it was found out that he had moments of absence; his peers noticed that he would sometimes stand still with a blank look in his eyes, then quickly come back to himself and continue working. Sometimes he couldn’t explain why he had to leave. He would go away for a while and, when he came back to himself, realize that he hadn’t eaten his meals. However, there were never any convulsive attacks during the day or night. He sometimes felt unwell, and although he wasn't under any medical treatment, he occasionally took bromides on his own, saying it was prescribed by his father. Although he usually had a gentle nature, he was prone to excessive anger over minor issues.
During the mobilizing and first months of the war, both in quarters and at the front, however, his conduct had been that of a good soldier. Suddenly, about March or April, 1915, the nocturnal enuresis began to be frequent again, occurring twice or three times a week; but the patient hid this misfortune as far as possible from his comrades. The captain thought he looked tired and depressed sometimes. Upon the days following the nights with enuresis, there was intense headache and marked moral and physical depression. There was no proof of nocturnal convulsions, and it is very problematical whether there was tongue-biting.
During the mobilization and the first months of the war, both in the barracks and at the front, he behaved like a good soldier. Suddenly, around March or April 1915, the bedwetting started happening frequently again, occurring two or three times a week; however, he did his best to hide this issue from his fellow soldiers. The captain sometimes noticed that he looked tired and down. On the days after nights with bedwetting, he experienced intense headaches and significant emotional and physical exhaustion. There was no evidence of nighttime seizures, and it’s very uncertain whether he bit his tongue.
Another odd feature was that the patient, who had been sober in civil life, had become intoxicated several times after going into the army. Physically, he was of low stature, but otherwise well built. Neurologically, he was entirely negative. There was no sign of venereal disease. There were a few stigmata of degeneration; for instance, there was very little hair upon the face, the ears were unequal in size, and the teeth were somewhat anomalously set. Mentally, he was below par; for instance, he could not add mentally two numbers of two digits.
Another strange trait was that the patient, who had been sober in civilian life, had become drunk several times after joining the army. Physically, he was short but otherwise well-built. Neurologically, he showed no abnormalities. There were no signs of sexually transmitted diseases. There were a few signs of degeneration; for example, he had very little facial hair, his ears were uneven in size, and his teeth were somewhat misaligned. Mentally, he was below average; for instance, he couldn't mentally add two two-digit numbers.
As to his desertion, the patient says he does not know what he did; that he learned of his act only from his comrades in the morning; that he remembered having left his duty pour aller satisfaire un besoin.
As for his desertion, the patient says he doesn't know what he did; that he found out about his actions only from his comrades in the morning; that he remembers leaving his duty to satisfy a need.
A specialist in escapes (epileptic fugues).
A specialist in escapes (epileptic seizures).
Case 62. (Logre, March, 1917.)
An epileptic fugue with recidivism is described by Logre. He described himself as a specialist in escapes. As a schoolboy, he had practised escapes and run away without purpose, and without remembering fully what he had done. His father would bring him back to school. At first they had punished him and then would pardon him. These escapades in his work as a shoemaker caused him to lose various places, but he had been kept by one employer for a long time nevertheless. From 11 years on, this patient had never ceased living either in foreign parts or in prison.
An epileptic fugue with recurrent episodes is described by Logre. He identified himself as an expert in getting away. As a kid, he practiced running away without any real purpose and often didn't fully remember what he'd done. His father would take him back to school. At first, they would punish him, but then they would forgive him. These escapades during his time as a shoemaker led him to lose several jobs, but one employer kept him for a long time nonetheless. Since he was 11, this patient had never stopped living either in foreign places or in prison.
The fugues on military service began to multiply. The military chiefs did not abide the escapades like the schoolmaster or the employer. Every punishment he received had to do with some fugue. Three times he gave himself up to the military authorities. Three times after a few more days’ service or a week in prison, he left the barracks or escaped. There had never been any appeal throughout this history to an alienist. On the declaration of war, he had returned to Belgium and was put into the army; whereupon in January, he carried out a fugue of a few hours which was rewarded with eight days in prison. There was a five-days fugue in July, whereupon he was taken before the council.
The escapes from military service started to increase. The military leaders didn’t tolerate these antics like a schoolteacher or an employer would. Every punishment he faced was because of an escape. He turned himself in to the military authorities three times. Each time, after just a few more days of service or a week in prison, he either left the barracks or broke free. There had never been any consultation with a psychiatrist during this time. When war broke out, he returned to Belgium and was drafted into the army; then in January, he managed to escape for a few hours, which earned him eight days in prison. In July, he escaped for five days, after which he was brought before the council.
Upon investigation, these fugues seemed to have the classical features of epileptic fugues. They were sudden, unconscious, blindly automatic, almost completely forgotten afterwards and of a stereotyped and recidivistic nature. Most of the fugues had been preceded by a slight excess in drinking. An investigation was made to see if there were any convulsive antecedents; none were found. This mental epilepsy, then, it was thought, must be an isolated symptom, free from every motor symptom. But his mother and one of his brothers had also shown a number of attacks of some sort of epilepsy. In all three cases there was impulsivity, unconsciousness, absurdity, recidivism, and refractoriness to[81] treatment. On these grounds the fugue was regarded as pathological and as epileptic probably. The patient himself thought that these coups-de-tête and this mania for running away without knowing where, made really a very ugly fault, particularly in a soldier.
Upon investigation, these fugues appeared to have the typical characteristics of epileptic fugues. They came on suddenly, were unconscious, automatic without any awareness, almost entirely forgotten afterward, and had a repetitive nature. Most of the fugues were preceded by a bit too much drinking. An investigation was conducted to see if there were any prior convulsive episodes; none were found. It was believed that this mental epilepsy must be an isolated symptom, without any motor symptoms. However, his mother and one of his brothers had also experienced several types of epilepsy attacks. In all three cases, there were signs of impulsivity, lack of awareness, irrational behavior, recurrence, and resistance to[81] treatment. Based on this, the fugue was considered pathological and probably epileptic. The patient himself believed that these coups-de-tête and this urge to run away without knowing where were really a significant flaw, especially for a soldier.
Re such specialists in escapes as Case 62, Lépine speaks of a type of military delinquent which he calls Ceux qui sautent le mur. Some of the fugue subjects, as well as other types of imbalance can apparently be held by no possible kind or degree of discipline. They jump any guardhouse or any other form of imprisonment through what amounts to a wild instinct for liberty. In some cases, this instinct appears in a relatively pure form; that is, without any combined tendency to dipsomania and without any sexual factor. Some of them are, in fact, very good soldiers, especially in shock troops. They, in fact, belong to what one might call the good element among delinquents. In the French Army some of them have been old legionaries and have even been, as in Case 62, previously condemned for desertion. They form a curious minority among the wall jumpers. Wall-jumping makes, so to say, the entire pathological phenomenon, and the recidivism is a part of the disease.
Regarding specialists in escapes like Case 62, Lépine discusses a type of military delinquent he calls Those Who Jump the Wall. Some of the escapees, along with other types of instability, can't be contained by any kind of discipline. They leap over any guardhouse or other form of confinement driven by a wild instinct for freedom. In some cases, this instinct seems to emerge in a fairly pure form; that is, without any tendency toward alcoholism or any sexual elements. Some of them are actually very good soldiers, especially in assault units. They represent what could be referred to as the good element among delinquents. In the French Army, some have been old legionnaires and have even been, as in Case 62, previously sentenced for desertion. They form an interesting minority among the wall jumpers. Wall-jumping, so to speak, constitutes the entire pathological phenomenon, and the recidivism is a part of the condition.
A disciplinary case: Epilepsy and other factors.
A disciplinary case: Epilepsy and other factors.
Case 63. (Advice, 1917.)
An Italian private in the artillery (father dead of general paresis) had been a victim of infantile convulsions and of convulsions with loss of consciousness up to 18 (convulsions with shouts and violence in the streets of Rome; had to be put in a straight-jacket at the municipal hospital).
An Italian soldier in the artillery (father died of general paresis) had suffered from childhood seizures and loss of consciousness until he was 18 (had seizures with shouting and aggression in the streets of Rome; he had to be restrained in a straightjacket at the city hospital).
He developed more convulsions during antisyphilitic treatment in the military hospital. He was a very poor soldier, of the rough and violent sort, and after eight months of service had to be assigned to a special disciplinary company, with which he remained for fifteen months. Here also he was punished frequently, and was given a period of four months’ imprisonment for refusal to obey the officers. Then for a period of several years he had no convulsions whatever.
He had more seizures while undergoing treatment for syphilis at the military hospital. He was not a very good soldier; he was rough and aggressive, and after eight months of service, he was transferred to a special disciplinary unit, where he stayed for fifteen months. During this time, he was often punished and spent four months in prison for refusing to follow orders from the officers. After that, he experienced no seizures for several years.
During the war he was given to alcoholism, and one day in June, 1916, he struck an officer and ran away to arm himself. He was at this time observed by psychiatrists and declared sane. He was regarded as an emotional and alcoholic epileptic but not as neurotic or psychopathic. He was again placed in a special disciplinary corps.
During the war, he developed a problem with alcoholism, and one day in June 1916, he hit an officer and ran off to get a weapon. At this time, psychiatrists evaluated him and deemed him sane. He was seen as an emotional alcoholic with epilepsy, but not as neurotic or psychopathic. He was put back into a special disciplinary unit.
Re the convulsions which this Italian developed during antisyphilitic treatment, it would be interesting to know whether intravenous injections were used. In case they were used, one might compare the case of this Italian with Bonhoeffer’s volunteer who developed epileptic convulsions after antityphoid inoculation.
Re the convulsions this Italian experienced during antisyphilitic treatment, it would be interesting to know if intravenous injections were used. If they were, one could compare this Italian's case with Bonhoeffer’s volunteer who developed epileptic convulsions after antityphoid vaccination.
An epileptic goes through Mons and two years fighting without symptoms. Then strange conduct with amnesia.
An epileptic goes through Mons and spends two years without any symptoms. Then they exhibit strange behavior along with amnesia.
Case 64. (Hurst, March, 1917.)
A private, 26, epileptic from 11 to 18 (mother also epileptic) entered the army at 20, attempted to commit suicide in 1912 (amnestic for this attempt), and went to France with the expeditionary force in August, 1914. The retreat from Mons and further fighting caused no recurrence of the symptoms. September, 1916, he was in fact put in charge of eight men doing guard duty. At this time he was able to get to bed only every other night. The charge of the telephone worried him, as he had never before been made to assume responsibility. After two months of this, he was found one night arresting civilians without cause and driving them before him with fixed bayonet. He was let off court-martial on the medical evidence, and at hospital remained confused and suspicious. November 16, he was seen by a medical officer in a typical attack of petit mal. Of all this, on reaching England December 19, he had no recollection, and was keen to return to duty.
A 26-year-old man, who had epilepsy from ages 11 to 18 (his mother also had epilepsy), joined the army at 20. In 1912, he tried to take his own life (he had no memory of this attempt) and went to France with the expeditionary force in August 1914. The retreat from Mons and the subsequent fighting didn't trigger any return of his symptoms. In September 1916, he was put in charge of eight men on guard duty. During this time, he could only get to bed every other night. Managing the telephone caused him stress, as he had never been responsible for anything before. After two months, one night he was found arresting civilians without a reason and forcing them to walk in front of him with a fixed bayonet. He avoided court-martial due to medical evidence, and while in the hospital, he remained confused and suspicious. On November 16, a medical officer witnessed him having a typical petit mal seizure. When he arrived back in England on December 19, he had no recollection of any of this and was eager to return to duty.
Re the remarkable delay in the return of epilepsy to this soldier of Mons, Bonhoeffer remarks that one of the epileptics observed by him at the Charité Clinic had passed through nine battles, and another through 18 battles before the first attack of epilepsy. Bonhoeffer regarded the strenuous marching as a liberating factor of epilepsy in five cases, actual fighting in seven cases, shell explosions in two cases, and bullet wounds in three.
Re the significant delay in the return of epilepsy for this soldier from Mons, Bonhoeffer points out that one of the epileptics he observed at the Charité Clinic had fought in nine battles, and another in 18 battles before experiencing their first epilepsy attack. Bonhoeffer viewed the intense marching as a triggering factor for epilepsy in five cases, actual combat in seven cases, shell explosions in two cases, and bullet wounds in three.
Re the apparently psychogenic factor in Hurst’s case (epilepsy coming on after assumption of too great responsibilities), compare remarks of Bonhoeffer under Case 57 concerning psychogenic factors. Sir George Savage has called attention to a form of functional epilepsy following shock or injury, in which recovery occurs after removal from the strain, but in which there is a relapse if the men go back to duty.
Re the seeming psychological factor in Hurst’s case (epilepsy occurring after taking on too much responsibility), compare Bonhoeffer's remarks under Case 57 about psychogenic factors. Sir George Savage has pointed out a type of functional epilepsy that happens after shock or injury, where recovery takes place once the strain is removed, but there is a relapse if the individuals return to duty.
Therapeutic (antityphoid inoculation) epilepsy.
Therapeutic antityphoid vaccination for epilepsy.
Case 65. (Bonhoeffer, July, 1915.)
A volunteer without psychopathic signs except a slight stuttering, and without psychopathic history of any sort, went into service at 17. After he had been a short time in the field, a shell fragment injured him in the upper part of the thigh. He lay up in hospital four weeks. He then spent four weeks in the reserve.
A volunteer with no signs of psychopathy except for a slight stutter, and without any history of psychopathy, started serving at 17. After a brief time in the field, a shell fragment hit him in the upper thigh. He stayed in the hospital for four weeks. Then he spent another four weeks in the reserve.
He was then given antityphoid inoculation, and a half hour afterward had epileptic convulsions. These appeared four times more during the next fortnight, as a rule followed by a delirious excitement. No fever was reported. After the fourth attack, he was transferred to the Charité Clinic.
He was then given an antityphoid vaccination, and half an hour later, he had epileptic seizures. These occurred four times more over the next two weeks, typically followed by a state of delirious excitement. No fever was reported. After the fourth seizure, he was moved to the Charité Clinic.
At the clinic there were no attacks, and there was nothing epileptic to discern in the make-up of the patient. His nervous system was normal to examination. There was, however, one fact in the family history of note, namely, that an older brother of the patient, 20 years of age, suffered from convulsions.
At the clinic, there were no seizures, and nothing epileptic was found in the patient's makeup. His nervous system checked out as normal. However, there was one noteworthy detail in the family history: the patient's older brother, who is 20 years old, has convulsions.
What is the relation of the antityphoid inoculation to the epilepsy? According to Bonhoeffer, we must not forget the family history even if we regard the inoculation as the liberating factor. Curiously enough, the shell injury did not itself serve apparently to bring out the epilepsy. Bonhoeffer has seen three other instances of epileptic attacks or epileptoid phenomena following antityphoid inoculation. However, in the hundreds of thousands of inoculations, it is not to be wondered at perhaps that there should be a number of instances of epileptic attacks. One was a man with severe epileptic taint; in the others, there was a question of pathological intoxication.
What is the link between the antityphoid vaccine and epilepsy? According to Bonhoeffer, we shouldn’t overlook the family background, even if we consider the vaccine to be the triggering factor. Interestingly, the shell injury didn’t seem to cause the epilepsy directly. Bonhoeffer has observed three other cases of epileptic seizures or epileptoid symptoms following antityphoid vaccination. However, given the hundreds of thousands of vaccinations, it’s not surprising that some instances of epileptic seizures have occurred. One was a man with a strong family history of epilepsy; in the other cases, it involved pathological intoxication.
Re antityphoid inoculations, a French observer—Paris—remarks that these inoculations may occasionally start up the symptoms of general paresis. Compare in this connection also Case 63, in which a syphilitic developed convulsions during antisyphilitic treatment. The psychogenic factor of intravenous injection itself, with its possible effect[85] upon glands of internal secretion, can hardly be distinguished from purely serological effects. Paris goes so far as to state that he regards it as imprudent to vaccinate a syphilitic subject. He thinks it might be better for a syphilitic subject to contract typhoid or paratyphoid fever than to run the risk of developing paresis. If the soldier happened to be not only syphilitic but alcoholic, then the danger would be larger. Possibly, however, both Bonhoeffer’s case of antityphoid inoculation epilepsy and the cases alluded to by Paris of antityphoid inoculation, are merely statistical accidents.
Regarding antityphoid vaccinations, a French observer—Paris—notes that these vaccinations might sometimes trigger symptoms of general paresis. Also refer to Case 63, where a syphilitic patient experienced convulsions during antisyphilitic treatment. The psychological aspect of intravenous injection itself, along with its potential impact[85] on internal gland secretion, is difficult to separate from purely serological effects. Paris even claims that he considers it unwise to vaccinate someone with syphilis. He believes it might be preferable for a syphilitic individual to contract typhoid or paratyphoid fever than to risk developing paresis. If the soldier were not only syphilitic but also an alcoholic, the risk would be greater. However, it’s possible that both Bonhoeffer’s case of epilepsy following antityphoid vaccination and the cases mentioned by Paris regarding antityphoid inoculation are simply statistical anomalies.
Shell-shock; (apparently slight) scalp wound: Jacksonian seizures. Operation, decompressing the edematous upper Rolandic region. Recovery.
Shell shock; (apparently minor) scalp injury: Jacksonian seizures. Surgery to relieve pressure on the swollen upper Rolandic area. Recovery.
Case 66. (Leriche, September, 1915.)
A Moroccan of the Seventh Tirailleurs was thrown to the ground by the explosion very near him of a large calibre shell, lost consciousness, and woke up with a slight contusion of the right side of the head. The date of this injury is unknown. He was evacuated to the interior, but stopped May 25, 1915, at the evacuation hospital because his pulse in the train stood at 51. An hour later in the hospital he had a Jacksonian epileptic attack, followed by a left-sided flaccid, brachial monoplegia, and after a quarter of an hour a second crisis, and then a third,—a sort of epileptic status occupying an hour. The attack seemed to start in the left hand. After the crisis, hand and arm became flaccid and inert.
A Moroccan from the Seventh Tirailleurs was thrown to the ground by the nearby explosion of a large caliber shell, lost consciousness, and woke up with a slight bruise on the right side of his head. The date of this injury is unknown. He was taken to the interior but was stopped on May 25, 1915, at the evacuation hospital because his pulse on the train was at 51. An hour later, in the hospital, he experienced a Jacksonian epileptic attack, followed by a left-sided flaccid brachial monoplegia. After about fifteen minutes, he had a second crisis, and then a third—essentially a prolonged epileptic status lasting an hour. The attack seemed to start in his left hand. After the crisis, his hand and arm were left flaccid and limp.
Lumbar puncture in the crisis gave fluid under small tension in a few absolutely limpid drops. The wound was a superficial skin wound as big as a 25-centime piece, near the middle line, roughly corresponding with the upper Rolandic region. It was hardly a wound—a mild abrasion not passing the epidermis; periosteum and bone intact.
Lumbar puncture during the crisis produced some clear fluid under low pressure, just a few drops. The injury was a superficial skin wound about the size of a 25-cent piece, located near the midline, roughly in line with the upper Rolandic area. It was barely considered a wound—just a minor abrasion that didn’t go beyond the epidermis; the periosteum and bone were intact.
The patient was trephined and a thin layer of clot was found over the dura mater. The clot was removed and a crucial incision was made into the dura mater. The brain seemed a little edematous, hemorrhagic and bruised. It soon began to beat and was tamponed.
The patient underwent trephination, and a thin layer of clot was discovered over the dura mater. The clot was removed, and a vital incision was made into the dura mater. The brain appeared slightly swollen, with signs of bleeding and bruising. It soon started to pulsate and was then tamponaded.
May 26, complete brachial monoplegia without seizure.
May 26, complete paralysis of one arm without seizure.
May 27, seizure at 2 in the afternoon, starting in left arm.
May 27, seizure at 2 PM, starting in the left arm.
The wound was going well and from this time forward no more seizures. May 28, a cast was made for the hand.
The wound was healing well, and from this point on, there were no more seizures. On May 28, a cast was put on the hand.
June 4, lumbar puncture yielded a clear liquid under the pressure of 58. That evening an hour after the puncture, the brachial monoplegia disappeared. The arm was still a little weak June 5. June 8 the man was evacuated to the auxiliary hospital at Laversine. June 18, complete recovery.
June 4, the lumbar puncture produced a clear fluid under a pressure of 58. That evening, an hour after the procedure, the brachial monoplegia went away. The arm was still a bit weak on June 5. On June 8, the man was transferred to the auxiliary hospital in Laversine. By June 18, he had fully recovered.
Fall and blow to head: Hysterical convulsions. Cure by studied neglect.
Fall and hit your head: Hysterical seizures. Cure through careful disregard.
Case 67. (Clarke, July, 1916.)
Clarke had seen in the war but one case of hysterical convulsions, though this particular patient had severe hystero-epileptic fits occurring in series. The man had never suffered from epilepsy and was 20 years of age. He received a slight wound and fell back into the trench a distance of six feet, striking but not contusing the back of his head.
Clarke had witnessed only one case of hysterical convulsions during the war, although this specific patient experienced severe hystero-epileptic seizures in succession. The man had never been diagnosed with epilepsy and was 20 years old. He sustained a minor wound and fell back into the trench from a height of six feet, hitting the back of his head but not causing a bruise.
On admission to the hospital he was found drowsy and dull. Fits occurred a week later, following one another at brief intervals in series that lasted one or two hours. The arms would be raised and extended in clonic spasm; the patient would resist violently if held, and then turn to his right side with rigid extension of legs and back in opisthotonos. The eyeballs underwent irregular movements, and there was a well marked hippus. Though the tongue was protruded in these attacks, it was never bitten. It was doubtful whether there was a complete loss of consciousness. Between attacks, the patient was morose and sullen, and showed a varying incoördination of the movements of the left leg, which was anesthetic to the knee. There was also a glove anesthesia of the right forearm and hand. Fields of vision were contracted.
Upon admission to the hospital, he was found to be drowsy and lethargic. Seizures occurred a week later, happening in quick succession for one or two hours. His arms would jerk and extend in a clonic spasm; he would resist strongly if held and then roll to his right side with rigidly extended legs and back in opisthotonos. His eyes displayed irregular movements, and there was a pronounced hippus. Although his tongue was stuck out during these episodes, it was never bitten. It was unclear whether he experienced complete loss of consciousness. Between seizures, he appeared morose and withdrawn, showing inconsistent coordination in the movements of his left leg, which was numb up to the knee. There was also a glove-like numbness in his right forearm and hand. His fields of vision were narrowed.
The fits recurred with intervals of a day or two, for a fortnight. The patient was then strictly isolated in a small room with an observation window. His bed was made up on the floor. He then had very slight attacks, as a rule when the nurse came into the ward; no notice was taken of these attacks and in a fortnight they ceased. The paresis of the leg and the anesthesia also cleared up without treatment. He remained in the general ward three weeks longer, at first dull and listless, but later cheerful and active. Clarke suggests that this patient was below normal intelligence.
The episodes happened every day or two for two weeks. The patient was then placed in strict isolation in a small room with a window for monitoring. His bed was set up on the floor. He then experienced very minor episodes, usually when the nurse entered the ward; these episodes were not noted, and after two weeks, they stopped. The weakness in his leg and the numbness also improved without any treatment. He stayed in the general ward for three more weeks, initially feeling dull and lethargic, but later becoming cheerful and active. Clarke suggests that this patient had slightly below-average intelligence.
Shell injury with unconsciousness; delayed attacks of epilepsy: superposed hysterical hemihypesthesia. Previous history consistent with the hypothesis that a genuine epilepsy had been developed.
Shell injury with unconsciousness; delayed seizures of epilepsy: combined hysterical hemihypesthesia. Previous history supports the idea that a true epilepsy had developed.
Case 68. (Bonhoeffer, July, 1915.)
An excellent soldier, of good build, 29 years, a member of the Landwehr, passed unscathed through eleven battles in the 1914 campaign, but finally succumbed to fragments of shell which struck his chest and the lower part of his thigh. He fell down, nauseated, and lost consciousness. He is said to have struck about him with his arm and to have voided urine. There was a second attack three weeks later, in which he fell upon his face.
An excellent soldier, well-built, 29 years old, a member of the Landwehr, came through eleven battles during the 1914 campaign without a scratch, but ultimately succumbed to shell fragments that hit his chest and the lower part of his thigh. He collapsed, feeling nauseous, and lost consciousness. It's said that he flailed his arms and urinated. There was a second attack three weeks later, during which he fell face down.
In the Charité Clinic he had three attacks, two of them nocturnal, one in the daytime, followed by a long period of somnolence. He once cried out suddenly in the night as if warding off an attack. He complained of headaches, and was often irritated and out of humor. Somatically, there was a hemihypesthesia on the side of the injury.
In the Charité Clinic, he had three episodes, two of them at night and one during the day, which were followed by a long period of drowsiness. He suddenly shouted one night as if he were trying to fend off an attack. He complained of headaches and was often irritable and in a bad mood. Physically, there was a reduced sense of feeling on the side of the injury.
The history indicates that this patient up to his sixteenth year had been a victim of occasional enuresis, often cried out in his sleep or even rose from bed. Occasionally he suffered from such violent sudden headaches that he would have to sit down. He was easily irritated, and had once been arrested for assault. As a soldier, however, he had never been guilty of any breach of discipline. Mild headaches would follow drinking. These phenomena in the history pointed in the direction of epilepsy. According to Bonhoeffer, we cannot entirely exclude contusion of the brain from the shell injury. However, there were no cerebral symptoms, and the interval before the occurrence of the attacks rather indicates that we are dealing with a genuine epilepsy. As for the hemihypesthesia, this is a hysterical “superposition,” which does not interfere, according to Bonhoeffer, with the genuineness of the epilepsy.
The history shows that this patient had been dealing with occasional bedwetting until he turned sixteen, often crying out in his sleep or even getting out of bed. Sometimes he experienced sudden, intense headaches that would force him to sit down. He was easily annoyed and had been arrested once for assault. However, he never violated any military rules while serving as a soldier. Mild headaches would follow drinking. These issues suggest the possibility of epilepsy. According to Bonhoeffer, we cannot completely rule out brain injury from the shell explosion. However, there were no signs of brain issues, and the time between the attacks indicates that we are likely looking at genuine epilepsy. As for the half-sensitivity loss, this is a hysterical “superposition,” which, according to Bonhoeffer, does not affect the reality of the epilepsy.
Shell-wound; musculocutaneous neuritis: Brown-Séquard’s epilepsy.
Shell-wound; musculocutaneous neuritis: Brown-Séquard syndrome epilepsy.
Case 69. (Mairet and Piéron, January, 1916.)
An infantryman, 30, a gardener, was wounded in the right forearm by a shell fragment, which fractured the ulna, September 7, 1914, at Revercourt. Despite much fragmentation of the bone and suppuration, the wound healed with two cicatrices, where the fragments had gone in and had come out. The scarring process was over in December.
An infantryman, 30, a gardener, was injured in his right forearm by a shell fragment that broke the ulna on September 7, 1914, at Revercourt. Despite significant bone fragmentation and infection, the wound healed, leaving two scars where the fragments entered and exited. The scarring process finished in December.
However, in the middle of January, 1915, this man began to suffer from headaches and insomnia, with vertigo and buzzing in the head, “as if an airplane inside.” Sometimes arms and legs would stiffen, and the man would tremble, have to lie down, and even lose consciousness for a quarter of an hour, waking up tired, wandering, and with feelings in his head. These crises, at first occurring every week, later grew frequent. Finally there was a very complete attack, in which he fell out of bed, got up, made several turns about the room, and went back to bed; and in the morning, was dull and disoriented. Accordingly, he was sent to the central military neuropsychiatric service of the general hospital at Montpellier, November 10.
However, in the middle of January 1915, this man started experiencing headaches and insomnia, along with dizziness and a buzzing sensation in his head, “as if an airplane was inside.” Sometimes his arms and legs would stiffen, causing him to tremble, lie down, and even lose consciousness for about fifteen minutes, waking up feeling exhausted, disoriented, and with strange sensations in his head. These episodes, which initially happened weekly, began to occur more frequently. Eventually, he had a severe attack where he fell out of bed, got up, made several laps around the room, and then returned to bed; in the morning, he felt dull and confused. As a result, he was sent to the central military neuropsychiatric service of the general hospital in Montpellier on November 10.
Besides the two extensive cicatrices, there were motor disorders. Pronation and supination were almost impossible, as well as extension of the hand and fingers and abduction of the thumb. There was a radial paralysis without R. D. Electrical excitability of the extensors was diminished on the right. The hand was weak. The right thumb was atrophic. There was a hypertrichosis as well as redness, heat and perspiration of the right hand. There was a hypesthesia for all forms of stimulation in the hand, especially in the radial region; less in the ulnar region. This hypesthesia rose along the posterior surface of the forearm and covered all the territory of the ulnar nerve; but there was a corresponding hyperesthesia in the musculocutaneous distribution, as well as in the internal cutaneous distribution. Above the[90] scar there was a region of complete anesthesia. The hyperesthesia rose higher along the circumflex nerve and the posterior branches of the cervical nerves and included the great occipital distribution, even involving the superficial cervical plexus, though not the territory of the trigemini. There was some hyperesthesia of areas governed by a few dorsal intercostal nerves. There were also spontaneous pains in these hyperalgesic regions. The musculocutaneous nerve could be felt to be thick and swollen, indicating a perineuritis. There were no neuropathic stigmata, but the knee-jerks were exaggerated a little more on the right side.
Besides the two large scars, there were motor issues. Rotating the hand inwards and outwards was almost impossible, as was extending the hand and fingers or moving the thumb away from the palm. There was radial paralysis without any reflex response. Electrical activity in the extensors was reduced on the right side. The hand was weak, and the right thumb had wasted away. There was excess hair growth, along with redness, warmth, and sweating of the right hand. The hand was less sensitive to all types of stimulation, especially on the radial side; the sensitivity was somewhat better on the ulnar side. This reduced sensitivity extended up the back of the forearm, covering the area supplied by the ulnar nerve, but there was increased sensitivity in the areas supplied by the musculocutaneous and internal cutaneous nerves. Above the [90] scar, there was a zone of complete lack of sensation. The increased sensitivity extended higher along the circumflex nerve and the back branches of the cervical nerves, including the distribution of the greater occipital nerve and even affecting the superficial cervical plexus, though not the area supplied by the trigeminal nerve. There was some increased sensitivity in areas supplied by a few dorsal intercostal nerves. Additionally, there were sharp pains in these overly sensitive areas. The musculocutaneous nerve felt thick and swollen, suggesting perineuritis. There were no signs of nerve damage, but the knee-jerk reflexes were a bit more pronounced on the right side.
The convulsions appeared two or three times a day, the pain would get worse along the arm, rise to the head, following the hyperesthetic zone, then invade the interior of the head, whereupon objects would appear to turn and the ears would buzz. The right leg, and especially the right arm, would begin to tremble. The man would have to support himself to avoid falling. He saw shadows moving, colored trees, occasionally persons. When the vertigo got stronger, he lost consciousness. The extremities of the right side stiffened and carried on jerky movements. These sometimes extended to the left side. The seizure lasted from five to fifteen minutes, and sometimes occurred in the middle of the night. Fatigue followed but headache disappeared after an attack.
The convulsions happened two or three times a day. The pain would worsen along the arm, rise to the head, follow the sensitive area, and then invade the inside of the head, making objects seem to spin and causing a buzzing in the ears. The right leg, especially the right arm, would start to shake. The man had to brace himself to avoid falling. He saw shadows move, colorful trees, and occasionally people. When the dizziness intensified, he would lose consciousness. The extremities on the right side would stiffen and move in a jerky manner, sometimes affecting the left side as well. The seizure lasted from five to fifteen minutes and sometimes occurred in the middle of the night. Fatigue followed, but the headache would go away after the episode.
The diagnosis of Brown-Séquard’s epilepsy was made. If the musculocutaneous trunk was compressed, a crisis was produced with pain radiating to the head, obscuration of vision, numbness in the arm, and tremors. Electrical treatment was resorted to for analgesic effect. There was a certain improvement during May, so that the diurnal dizziness disappeared. May 19 he had a period of 24 hours without any vertigo. In June no further improvement occurred.
The diagnosis of Brown-Séquard’s epilepsy was confirmed. If the musculocutaneous trunk was compressed, it triggered a crisis with pain radiating to the head, blurred vision, numbness in the arm, and tremors. Electrical treatment was used for pain relief. There was some improvement in May, and the daytime dizziness went away. On May 19, he had a 24-hour period without any vertigo. In June, there was no further improvement.
An operation was performed June 23, 1915. The two cicatrices were excised, and some fragments of cloth were removed. Three Jacksonian crises followed the operation, and there was another seizure next day. Frequent headaches followed without crises. More seizures appeared in[91] the night during July, and their frequency increased. Pains persisted along the arm and in the back of the head; the musculocutaneous perineuritis was still intense. Prolonged baths for the arm were begun August 4, two baths of two hours each, at 40 deg. each day. Following August 10 there was an improvement, which stopped as soon as the baths were omitted, with diminution of the vertigo and the hyperesthesia. This improvement continued; the baths were made to last three hours. There were no attacks from August 21 to 26 whereupon they then returned for two days. The pains had much diminished in the arm but persisted in the occiput. A few night attacks occurred August 30 and 31, September 5 and 6, as well as September 19 and 20, 25 and 26, and 27.
An operation took place on June 23, 1915. The two scars were removed, and some pieces of cloth were taken out. Three Jacksonian crises occurred after the operation, and there was another seizure the next day. Frequent headaches followed without any crises. More seizures happened at night during July, and their frequency increased. Pain continued along the arm and in the back of the head; the musculocutaneous perineuritis remained severe. Starting August 4, prolonged baths for the arm were initiated, two baths of two hours each, at 40 degrees every day. After August 10, there was improvement, which ceased as soon as the baths were skipped, leading to a decrease in vertigo and increased sensitivity. This improvement continued; the baths were extended to three hours. There were no attacks from August 21 to 26, after which they returned for two days. The pain in the arm had greatly decreased but persisted in the back of the head. A few night attacks occurred on August 30 and 31, September 5 and 6, as well as September 19 and 20, 25 and 26, and 27.
The occipital pain had now become less; the musculocutaneous nerve was not so large. Only a few headaches followed during the months of October, November, and December. After November 3 the baths were stopped and the arm was kept wrapped in a warm compress. There was still a certain hyperesthesia, the knee-jerks had become less exaggerated. Massage and mechanotherapeutic exercises were begun. There were no more attacks after September 27.
The pain in the back of the head had decreased; the musculocutaneous nerve was no longer as prominent. Just a few headaches occurred during October, November, and December. After November 3, the baths were discontinued, and the arm was kept wrapped in a warm compress. There was still some sensitivity, but the knee-jerk reflexes had become less intense. Massage and therapeutic exercises were started. There were no more episodes after September 27.
Re Brown-Séquard’s epilepsy, Lépine remarks that besides the case of Mairet and Piéron, Hurst and Souques have published cases. Lépine himself has observed two cases: one followed a nerve wound in the foot; another, a penetrating wound of the chest. As a rule, such Brown-Séquard epilepsies appear a number of months after trauma; as a result of irritation in the scar. Lépine’s subjects were taken for simulators because they had not received any cranial wound. The prognosis should be guarded, though the outcome in Case 69 appears to have been favorable.
Re Brown-Séquard’s epilepsy, Lépine notes that besides the case of Mairet and Piéron, Hurst and Souques have reported cases as well. Lépine himself has seen two cases: one followed a nerve injury in the foot; the other involved a penetrating injury to the chest. Typically, these Brown-Séquard epilepsies show up several months after the trauma, due to irritation in the scar. Lépine’s patients were considered to be faking because they had not sustained any cranial injury. The prognosis should be cautious, although the outcome in Case 69 seems to have been positive.
Epileptic episode at 24 years following bullet-wound of hand, in a soldier who had had convulsions in childhood (sister epileptic). Reactive epilepsy? Epilepsia tarda?
Epileptic episode at 24 years after a bullet wound to the hand, in a soldier who had convulsions as a child (sister is epileptic). Reactive epilepsy? Epilepsia tarda?
Case 70. (Bonhoeffer, July, 1915.)
A man in the reserve, 24, bore the stresses of the war very well in the campaign in East Prussia until he was shot in the hand at Deutsch-Eylau. He had always been well aside from rheumatism, and was discharged with a good record from his military service.
A 24-year-old man in the reserves handled the pressures of the war quite well during the campaign in East Prussia until he was shot in the hand at Deutsch-Eylau. He had always been healthy except for some rheumatism and was discharged with a solid record from his military service.
Sent to the reserve hospital for his hand injury, he had, two or three times in the night, convulsions with loss of consciousness and dilated pupils; after which there was a thirty-six hour period of depression with refusal of food. Thereafter this soldier had amnesia for both the seizures and the subsequent depression. He was observed six weeks longer in the Charité Clinic but had no more attacks, and indeed nothing more of note either mentally or somatically.
Sent to the reserve hospital for his hand injury, he experienced convulsions with loss of consciousness and dilated pupils two or three times during the night; after which he went through a thirty-six hour period of depression and refused to eat. After that, this soldier couldn't remember either the seizures or the subsequent depression. He was observed for six more weeks in the Charité Clinic but had no further attacks and nothing else significant either mentally or physically.
The history showed that there had been convulsions in the third and fourth years of the patient’s life. There had been, however, nothing epileptoid in the later childhood or developmental years of the patient. However, a sister of the patient had suffered since childhood from convulsions. It remains a question whether this episode is to be regarded as reactive epilepsy—reactive, namely, to experiences in the war—or whether we are dealing with a true epilepsia tarda.
The history indicated that there were convulsions in the third and fourth years of the patient's life. However, there was nothing resembling epilepsy in the patient's later childhood or developmental years. On the other hand, the patient's sister had experienced convulsions since childhood. It's still uncertain whether this episode should be considered reactive epilepsy—specifically in response to experiences in the war—or if we are actually dealing with true late-onset epilepsy.
Re this episode following bullet wound, the compiler has placed it after Mairet and Piéron’s case of Brown-Séquard epilepsy, but apparently Bonhoeffer regards his case as probably a reactive one. Unlike the case of Mairet and Piéron, Bonhoeffer’s case had an epileptic soil (convulsions in childhood and epileptic sister). Re the so-called reactive epilepsies, see remarks by Bonhoeffer under Case 57.
Regarding this episode after the gunshot wound, the compiler has positioned it after Mairet and Piéron’s case of Brown-Séquard epilepsy, but it seems Bonhoeffer views his case as likely a reactive one. Unlike the situation with Mairet and Piéron, Bonhoeffer’s case had a predisposition to epilepsy (convulsions in childhood and an epileptic sister). For the so-called reactive epilepsies, refer to Bonhoeffer’s comments under Case 57.
Epilepsia tarda in a lance-corporal without hereditary taint or previous history save dizzy spells and excitability.
Epilepsy later in life in a lance corporal without a family history or prior issues, except for dizziness and high energy.
Case 71. (Bonhoeffer, July, 1915.)
A reserve lance-corporal, 24 years—a soldier from 1911 to 1913 without disciplinary record, and in his second year becoming lance-corporal—was in the campaigns in Belgium, East Prussia, and Poland, making long marches and going through several battles. In the middle of October, 1914, he fell from a horse and suffered a contusion of the thorax, after which blood appeared in the sputum. In November he was brought to the reserve hospital in Berlin, and there had convulsive seizures. Before transfer to the Charité Clinic, a seizure occurred, and he was brought into the clinic in a characteristic dazed state. Thereafter he was clear but often out of humor and irritated. Three weeks later came a brief attack, probably epileptic in nature, with restless half-delirious sleep following.
A reserve lance-corporal, 24 years old—a soldier from 1911 to 1913 with no disciplinary issues, who became a lance-corporal in his second year—served in the campaigns in Belgium, East Prussia, and Poland, enduring long marches and engaging in several battles. In mid-October 1914, he fell off a horse and sustained a chest injury, which led to blood in his sputum. In November, he was taken to the reserve hospital in Berlin, where he experienced convulsive seizures. Before being moved to the Charité Clinic, he had a seizure and was admitted to the clinic in a dazed state. After that, he was clear-headed but often in a bad mood and irritable. Three weeks later, he had a brief episode, likely an epileptic seizure, followed by restless, half-delirious sleep.
There was nothing in childhood or in the family history to indicate epilepsy. However, the patient himself stated that from 1913 onward, after his period of military service, he had from time to time felt attacks of dizziness after exertion, and that he had become more easily excitable than before.
There was nothing in his childhood or family history to suggest epilepsy. However, the patient stated that starting in 1913, after his time in the military, he occasionally experienced dizziness after physical activity and had become more easily excited than before.
The attacks in the lance-corporal are probably not to be attributed to the thoracic contusion, according to Bonhoeffer, because of the long period that elapsed after the thoracic injury, and their development nocturnally without special occasion. According to Bonhoeffer, we are probably here dealing with a late epilepsy.
The attacks in the lance-corporal are likely not caused by the chest injury, according to Bonhoeffer, due to the long time that passed after the chest injury, and their occurrence at night without any specific trigger. According to Bonhoeffer, we are likely looking at a case of late-onset epilepsy.
Re late epilepsy, see also under Case 57. Bonhoeffer makes a considerable point of the lateness in attacks of epilepsy in some of the military cases, pointing out their beginning at the ages of 22 to 27 in the period of peace practice undergone by soldiers. The theory is that cases of severe and long-standing epilepsy are known to the authorities, so that[94] they would not ordinarily be in military service except under conditions of concealment or in case of error. The present case (71) appears to be the nearest that Bonhoeffer has found to a case of epilepsy without heredity and without acquired soil. All that can be regarded as evidence of soil is the dizzy spells and excitability.
Re late epilepsy, see also under Case 57. Bonhoeffer emphasizes the significance of the late onset of epilepsy attacks in some military cases, noting that they typically start between the ages of 22 and 27 during the peace training that soldiers undergo. The theory suggests that severe and long-standing epilepsy cases are known to the authorities, and therefore[94] they wouldn’t normally be allowed in military service unless concealed or due to an oversight. The current case (71) seems to be the closest Bonhoeffer has found to an epilepsy case without hereditary factors or prior conditions. The only indications of a predisposition are the dizzy spells and excitability.
Re thoracic contusion, compare remarks of Lépine under Case 69, on Brown-Séquard epilepsy following thoracic wound.
Re thoracic contusion, see Lépine's comments under Case 69, regarding Brown-Séquard epilepsy after a thoracic injury.
Convulsions by autosuggestion.
Convulsions from autosuggestion.
Case 72. (Hurst, November, 1916.)
A private, 27, is described as a typical martial misfit—in private life a music hall falsetto singer, and afterward a valet. He joined the army in 1915 and proceeded to France, and worked in a canteen. A week later, men broke in and threw a mallet at him, whereupon he immediately had a fit, and was dazed, dumb, and unable to walk for two days. Thereafter occasional further fits occurred, with nervousness and insomnia. He was sent home in September, 1916. Discharged to duty, he again in December returned to France, had six fits in the first week—three in hospital, two on the boat, and between two and four for four days after admission. The diagnosis of genuine epilepsy was made in France by a medical officer who had seen one of the convulsions. However, he had never passed urine or bitten his tongue, had no family history, and had never had fits before going to France.
A 27-year-old private is described as a typical outcast—he was a falsetto singer in music halls and later worked as a valet. He joined the army in 1915 and went to France, where he worked in a canteen. A week later, some men broke in and threw a mallet at him, causing him to have a fit right away; he was dazed, mute, and unable to walk for two days. After that, he experienced occasional further fits, along with nervousness and insomnia. He was sent home in September 1916. Once he was discharged, he returned to France in December and had six fits in the first week—three in the hospital, two on the boat, and between two and four for four days after being admitted. A medical officer in France diagnosed him with genuine epilepsy after witnessing one of the convulsions. However, he had never passed urine or bitten his tongue, had no family history of seizures, and had never had fits before going to France.
He was hypnotized and given the suggestion that he would have a fit. In the convulsion which followed the plantar reflexes remained flexor, but otherwise the convulsion was quite like the genuine epilepsy. He was told that he would not have any more convulsions, nor did he have any more except on Feb. 16, 1917, when some talk was made to him about returning to duty. Bromides used in France did not help the epilepsy at all. This patient developed a gait and speech defect copied from two patients in the wards. These symptoms, due to autosuggestion, disappeared on persuasion.
He was put under hypnosis and given the suggestion that he would have a seizure. During the convulsion that followed, the reflexes in his feet stayed flexed, but otherwise, the seizure was very similar to real epilepsy. He was told that he wouldn't have any more seizures, and he didn't, except on February 16, 1917, when they talked to him about returning to duty. The bromides used in France did not help his epilepsy at all. This patient developed walking and speech problems similar to two other patients in the wards. These symptoms, caused by autosuggestion, went away after some persuasion.
Re autosuggestion, Bernheim has returned to the fray (1917) in a book on automatism and suggestion, dealing only in small part with war problems. The most general formula for suggestion appears to be that it is an idea accepted. A suggestion offered but not accepted is in effect not a suggestion at all. Any accepted idea, says Bernheim, is from the psychological point of view as well as from the medical point of view, a suggestion. A suggestion may be direct or indirect, reasonable or unreasonable, brought about by
Re autosuggestion, Bernheim has jumped back into the discussion (1917) in a book about automatism and suggestion, which only briefly touches on war issues. The broadest definition of suggestion seems to be that it is an idea that’s accepted. A suggestion that is offered but not accepted doesn't really count as a suggestion at all. Any accepted idea, according to Bernheim, is considered a suggestion both psychologically and medically. A suggestion can be direct or indirect, reasonable or unreasonable, created by
(a) mere verbal assertion,
(a) just a verbal claim,
(b) hypnotic state,
hypnotic state,
(c) persuasive explanation, rational or emotional,
(c) convincing explanation, whether logical or emotional,
(d) emotion (that is, emotion not the effect of any form of suggestion offered by the physician, but emotion brought about by some event affecting the sentiments of the subject).
(d) emotion (that is, emotion not influenced by any type of suggestion from the doctor, but emotion triggered by a specific event impacting the feelings of the individual).
Epilepsy of emotional origin.
Emotional epilepsy.
Case 73. (Westphal and Hübner, April, 1915.)
A lieutenant without neuropathic tendencies (except that his mother was in a hospital for the insane) was under shell fire for some time. Finally, a shell burst near him, whereupon headaches and transient spells of confusion followed. Shortly upon the news of the death of his Major, he had a spell of violent excitement and confusion, dancing about on the ground and breaking things up. He passed into a stuporous condition with a suggestion of catatonia. There were a few isolated delusions to the effect that he was poisoned. After sleeping a long time, he suddenly cleared up. There was an extensive amnesia covering a period of weeks. He had forgotten the Major’s death and everything thereafter. He complained of headache, difficulty of thinking, and forgetfulness. An agoraphobia developed, as well as great sensitivity to sounds, and a feeling as if the bed and surrounding barracks were moving. There were a few illusions of a visual nature. He had complete insight into his condition. Conduct was normal. There was general hyperesthesia and ageusia.
A lieutenant without any neurological issues (other than his mother being in a psychiatric hospital) was under enemy fire for a while. Eventually, a shell exploded nearby, leading to headaches and occasional confusion. Shortly after learning of his Major’s death, he experienced a fit of intense excitement and confusion, dancing around and causing destruction. He then fell into a stupor with signs of catatonia. There were a few isolated delusions where he believed he had been poisoned. After sleeping for a long time, he suddenly became clear-headed. He had significant amnesia that covered several weeks, completely forgetting about the Major’s death and everything that happened afterward. He complained of headaches, trouble thinking, and memory loss. He developed agoraphobia and became very sensitive to sounds, feeling as if his bed and the surrounding barracks were moving. There were also a few visual illusions. He had a clear understanding of his condition. His behavior was normal. He experienced general heightened sensitivity and a loss of taste.
According to Westphal, this case of deep disorder of consciousness of some duration in a healthy person is probably one of a dazed state following the so-called “affect epilepsy.”
According to Westphal, this situation of prolonged deep unconsciousness in an otherwise healthy person is likely a dazed condition following what is known as “affect epilepsy.”
Is Case 73 Shell-shock? Note that, in Case 73, the shell explosion at first occasioned mere headaches and confusional spells. The true occasion of the convulsions appears to have been the news of the death of a superior officer. It is, of course, possible that the transient spells of confusion were actually epileptic equivalents. Lépine remarks that Pierret and others, observing such spells of confusion often accompanied by agitation, have inquired whether manic depressive psychosis is not a kind of epilepsy. This question remains unresolved. These phenomena of epilepsia larvata (see also Case 81 of Juquelier and Quellien) are to be sharply distinguished from attacks of confusion occurring in pronounced epileptics. These latter attacks often follow a crisis and suggest exhaustion; sometimes they last several days.
Is Case 73 Shell-shock? Note that, in Case 73, the shell explosion initially caused just headaches and confusion. The real trigger for the convulsions seems to have been the news of a superior officer's death. It’s possible that the temporary confusion episodes were actually epileptic equivalents. Lépine notes that Pierret and others, observing these confusion episodes often accompanied by agitation, have questioned whether manic depressive psychosis is a form of epilepsy. This question remains unanswered. These phenomena of epilepsia larvata (see also Case 81 of Juquelier and Quellien) should be clearly distinguished from confusion attacks seen in obvious epileptics. The latter attacks often follow a crisis and indicate exhaustion; sometimes they can last several days.
Fatigue; fear; hysterical convulsions. Visual aura (approaching fire wheel) built up after the third crisis (scotoma after look at sun).
Fatigue, fear, and hysterical convulsions. Visual aura (approaching fire wheel) developed after the third crisis (scotoma after looking at the sun).
Case 74. (Laignel-Lavastine and Faye, July, 1917.)
A sapper, 23, with his company under heavy bombardment, October, 1916, was overcome by weariness and fear (he had always been of a timorous disposition). The order for the rear came, but the convoy was hardly en route when the sapper felt a griping in the pit of the stomach and the blood going to his head; whereupon he lost consciousness and went into convulsions.
A 23-year-old sapper, with his unit under heavy fire, October 1916, was overwhelmed by fatigue and fear (he had always been naturally timid). The order to retreat came, but the convoy was barely underway when the sapper felt a tightening in his stomach and dizziness; then he lost consciousness and began convulsing.
This incident seems to have made a powerful impression upon the sapper. A fortnight later, while working in the trenches, he had more epigastric sensations with vague discomfort. He thought about the earlier crisis and about his wounded comrades, and again fell down and had more convulsions lasting a quarter of an hour. The tongue may have been slightly bitten in this seizure. In the genesis of this second seizure we may consider that the feeling of discomfort and the epigastric sensations served to recall the first seizure, so that the second one may be regarded as due to autosuggestion—that is, as hysterical.
This incident seems to have made a strong impact on the sapper. Two weeks later, while working in the trenches, he experienced more discomfort in his stomach along with vague unease. He thought about the previous episode and his injured comrades, and again collapsed, having convulsions that lasted about fifteen minutes. He might have bitten his tongue during this episode. In understanding this second seizure, we can consider that the feeling of discomfort and stomach sensations reminded him of the first seizure, so we can see the second one as a result of autosuggestion—that is, as hysterical.
A little later, on a hot day in the trench, while working, the sapper turned to a comrade and saw a great black spot on his face. He turned toward another and saw another great black spot on this face also. He was frightened, felt strange sensations, fell, and had a third convulsive crisis. The black spots that he saw were due to a scotoma, the result of a transient glance at the sun.
A little later, on a hot day in the trench, while working, the sapper turned to a comrade and noticed a big black spot on his face. He turned to another person and saw another big black spot on his face too. He got scared, felt weird sensations, collapsed, and had another convulsive episode. The black spots he saw were caused by a scotoma, the result of a brief glance at the sun.
After this scotomatous episode, his crises always had a visual aura. He would feel rather uncomfortable, leave the supper table, feel a gastric sensation, warmth in the face, and oppression. He would go out in the cold for the air, look about for something, appear frightened, fix his gaze upon a certain point, and cease to reply to questions. His head would jerk back suddenly, and he would utter strangled cries[99] of fear. He was now evidently prey to a terrifying hallucination. In ten minutes, everything had gone again, leaving him trembling with emotion. He would then relate how, after the epigastric sensation had begun, he tried to see if he could make out something abnormal; whereupon a little fiery wheel would appear and roll up nearer and nearer, so as to almost touch his eyelids. He could see his comrades to the right and to the left of the wheel; he could hear questions but could not answer. Just as the fire wheel was about to blast him, consciousness was lost and the fits came on.
After this episode with vision problems, he always experienced visual symptoms before his crises. He would feel pretty uncomfortable, excuse himself from the dinner table, have a sinking feeling in his stomach, warmth in his face, and a sense of tightness. He would step outside for fresh air, search for something, look scared, fix his gaze on a certain spot, and stop responding to questions. His head would jerk back suddenly, and he would let out sounds of fear that were almost strangled[99]. It was clear he was having a terrifying hallucination. Within ten minutes, it would all fade away, leaving him shaky with emotion. He would then explain how, after the stomach discomfort started, he tried to see if there was anything unusual; then a little fiery wheel would appear and roll closer and closer, nearly touching his eyelids. He could see his friends to the right and left of the wheel; he could hear their questions but couldn't respond. Just as the fiery wheel was about to explode in front of him, he lost consciousness and the seizures began.
War strain; anxiety; confusion; fugue. Demotion and detail to the interior.
War strain; anxiety; confusion; amnesia. Lowered status and focus on the inner self.
Case 75. (Barat, November, 1914.)
A lieutenant, 25, an officer in a regiment on active duty near the front, was called before a special board charged with desertion in the face of the enemy. He had been assigned to a certain position but not only had not complied with the order, but had wandered off to the British sector and been arrested there as a spy.
A 25-year-old lieutenant, an officer in a regiment actively deployed near the front lines, was summoned before a special board investigating desertion in the face of the enemy. He had been given a specific assignment but not only failed to follow the order, he had strayed into the British sector and was arrested there as a spy.
The prisoner was well developed, without stigmata; heredity, negative. His career in the army had been courageous and he had been advanced several ranks and was about to be given a medal for bravery. He said that he had been under a severe strain for several days.
The prisoner was physically fit, with no noticeable issues; his background was unremarkable. He had served bravely in the army, received multiple promotions, and was about to be awarded a medal for his courage. He mentioned that he had been under a lot of stress for several days.
One evening he had been given the order to attack. The artillery opened fire. He found that the Germans had erected barbed wire defences. The loss of men was terrific. His order was to shoot all who held back. A poor territorial crouched down and would not go forward—supplicating the prisoner not to shoot him. The prisoner spared him.
One evening he received the order to attack. The artillery started firing. He realized the Germans had set up barbed wire defenses. The loss of life was immense. His orders were to shoot anyone who hesitated. A frightened soldier crouched down and refused to move forward—begging the prisoner not to shoot him. The prisoner let him go.
The next night the order to attack the German trenches was again given. This time he was overcome with anxiety and discouragement. The last he remembers was the order to attack. Next day he felt sick and his mind was foggy. He remembered leaving his regiment and wandering round for several days until he fell into the hands of the British and was arrested. Then he understood what he had done.
The next night, the order to attack the German trenches was given again. This time, he was flooded with anxiety and despair. The last thing he remembers is the command to attack. The next day, he felt nauseous and his thoughts were cloudy. He recalled leaving his regiment and wandering for several days until he was captured by the British and arrested. Then he realized what he had done.
The prisoner asked to be allowed to return to the front. The testimony of one of the lieutenant’s men verified his statements. On the day before he left the front he had been anxious, had cried often, and would speak to no one. On the day he left the trenches without permission, he was nervous and disoriented.
The prisoner asked to be allowed to go back to the front. One of the lieutenant’s men confirmed what he said. The day before he left the front, he was anxious, cried often, and didn’t talk to anyone. On the day he left the trenches without permission, he seemed nervous and disoriented.
There was no doubt that simulation could be ruled out; the differential diagnosis lay between a “confused state of emotional origin” and an[101] “epileptic dazed state.”
There was no doubt that simulation could be dismissed; the differential diagnosis was between a “confused state of emotional origin” and an[101] “epileptic dazed state.”
For epilepsy there was a history of attacks with falling to the ground and loss of consciousness, without involuntary micturition or biting of tongue, during the time when he was a sergeant. Moreover, irritability and unwarranted suspiciousness had been present at these periods. However, there were no other epileptic symptoms; these two attacks were isolated and of quite long duration, leaving no headache or malaise after them. Also there was no basis for the diagnosis “epileptic dazed state,” since there was no abrupt commencement; the loss of consciousness was never complete (the subject was able to converse with persons while the attacks were on); and some remembrance was present of incidents during the attacks.
For epilepsy, there was a history of seizures that involved falling to the ground and losing consciousness, without any involuntary urination or tongue-biting, during the time he served as a sergeant. Additionally, irritability and unjustified suspicion were noticeable during these episodes. However, there were no other signs of epilepsy; these two seizures were isolated and quite lengthy, leaving no headache or discomfort afterward. There was also no reason to diagnose an “epileptic dazed state,” since there was no sudden onset; the loss of consciousness was never complete (the person could talk to others while the seizures occurred); and there was some memory of events during the seizures.
For Barat, the important points are that the attacks were preceded by long periods of anxiety and the disturbances resulted more from moral than physiological causes.
For Barat, the key points are that the attacks were preceded by long periods of anxiety and the disturbances were caused more by moral issues than by physical ones.
The importance of the psychological factors lead the author and his colleagues to the diagnosis “Mental confusion of emotional origin.”
The significance of psychological factors led the author and his team to diagnose “Mental confusion of emotional origin.”
The board decided to return him to the interior and give him a barracks position at the reduced rank of drill sergeant.
The board decided to move him back to the interior and assign him a barracks position as a drill sergeant at a lower rank.
A solitary epileptic episode in an artillery officer (slight concussion of the brain two years before) following extraordinary campaign stress (38 artillery battles in two months).
A single seizure in an artillery officer (slight concussion of the brain two years earlier) after intense campaign stress (38 artillery battles in two months).
Case 76. (Bonhoeffer, July, 1915.)
A first lieutenant of artillery, 35, was able to count 38 artillery clashes in which he had taken part in two months of very strenuous, almost daily fighting. Then appeared headaches, anxiety, dizzy feelings, insomnia. Finally one day suddenly, after eating, the lieutenant sustained a loss of consciousness with convulsions, which sent him to his home reserve hospital. The officer had felt nothing before his convulsions came on. The medical report, however, yields no doubt of the epileptic character of the attack.
A 35-year-old first lieutenant in artillery was able to report 38 artillery clashes he had participated in over two months of intense, almost daily fighting. Then he started experiencing headaches, anxiety, dizziness, and insomnia. One day, after eating, the lieutenant suddenly lost consciousness and had convulsions, which landed him in his home reserve hospital. He hadn't felt anything before the convulsions hit. The medical report, however, leaves no doubt about the attack being of an epileptic nature.
When he was examined, there was a slight psychopathic depression with a feeling of insufficiency, anxiety, insomnia, restless dreams, over-sensitiveness, and a pessimistic outlook on the future. There were no epileptic traits whatever. There was nothing alcoholic, luetic, or arteriosclerotic about the officer. There was nothing in the childhood or youth of the patient, though there had been a fall two years before, with phenomena of concussion without sequelae. In fact, this fall with concussion had led to no medical examination.
When he was examined, there was mild psychopathic depression along with feelings of inadequacy, anxiety, insomnia, restless dreams, heightened sensitivity, and a negative outlook on the future. There were no signs of epilepsy at all. The officer showed no signs of alcoholism, syphilis, or arteriosclerosis. There was nothing notable from the patient's childhood or adolescence, although he had experienced a fall two years earlier with symptoms of a concussion that had no lasting effects. In fact, this fall with concussion had not resulted in any medical examination.
As to the relation of the concussion two years before to the epileptic attack, Bonhoeffer is inclined to interpret the case as one of genuine “reactive” epilepsy on the basis of continuous overstrenuous work for a period of weeks. He regards the previous concussion as soil for this epilepsy.
As for the connection between the concussion from two years ago and the epileptic seizure, Bonhoeffer tends to view this case as a genuine instance of "reactive" epilepsy, resulting from weeks of constant overexertion. He sees the earlier concussion as a contributor to this epilepsy.
Re amount of stress occasionally required to bring out epilepsy, compare Hurst’s Cases 64 and 80. It may be recalled that Bonhoeffer is decidedly of the belief that exhaustion has not brought about any actual psychoses, calling attention to the remarkable absence of psychoses among the Serbians after their exhausting campaigns. A general review of war experience indicates, according to Bonhoeffer, the marked power of resistance of the healthy brain.
Re the amount of stress sometimes needed to trigger epilepsy, check out Hurst’s Cases 64 and 80. It's worth noting that Bonhoeffer firmly believes that exhaustion hasn't caused any real psychoses, pointing out the striking lack of psychoses among the Serbians after their intense campaigns. A broad look at war experiences suggests, according to Bonhoeffer, that the healthy brain has a strong ability to resist.
Nocturnal narcoleptic seizures accompanied by spells of somnolence in the day, both to be regarded as due to the “brain fag” of trench life.
Nocturnal narcoleptic seizures along with episodes of drowsiness during the day, both considered to be caused by the "brain fatigue" of trench life.
Case 77. (Friedmann, July, 1915.)
A tradesman, 23, had been in the German infantry since the beginning of the war. Never sick, he had been, in a general way, nervous; and a brother had had, at the age of 30 years, some sort of severe brain disease, in which he became blind, dying a year later.
A 23-year-old tradesman had been in the German infantry since the war started. He had never been sick, but he was generally anxious. His brother, at the age of 30, suffered from a serious brain illness that caused him to go blind, and he died a year later.
The man was for a long time in the trenches and proved himself a courageous and stalwart soldier. He went to hospital after a slight bullet wound of the leg, with a benign paralysis of the peroneus.
The man had been in the trenches for a long time and showed himself to be a brave and strong soldier. He went to the hospital after getting a small bullet wound in his leg, which resulted in a mild paralysis of the peroneus.
In the hospital he began to show a somewhat pronounced emotional depression, with a nervous tachycardia.
In the hospital, he started to display a noticeable emotional depression along with a racing heartbeat.
Friedmann reports the case on account of certain peculiar seizures which, upon the man’s own story, had begun five weeks before, in the field, although he had told no one about them. He had never felt anything like them before. At first, they came three to five times almost every night. He would suddenly wake and find himself unable to move, to speak, or even to think. These seizures, however, were not accompanied by any feeling of anxiety or any respiratory distress. Consciousness remained clear, and after 10 or 15 seconds, he could begin to think normally again. It was clearly a question of psychopathic absences of a mild narcoleptic type, occurring, however, only at night.
Friedmann reports the case due to some unusual seizures that the man claimed started five weeks ago while he was in the field, though he hadn’t told anyone about them. He had never experienced anything like this before. Initially, they occurred three to five times almost every night. He would suddenly wake up and find himself unable to move, speak, or even think. However, these seizures weren’t accompanied by any feelings of anxiety or breathing difficulties. His consciousness remained clear, and after about 10 or 15 seconds, he could start to think normally again. It was clearly a case of mild narcoleptic-like episodes that happened only at night.
Daytimes, also, throughout the whole period in which the nocturnal absences occurred, there were seizures of another description. During the many hours in which he had to sit in the trench, about twice a day for half an hour long, he would plunge suddenly into a sort of irresistible lethargy. Without any external occasion whatever, there would be a feeling of great fatigue. In the spell he could not move or think, would lean his head upon his hand. He was unable to overcome the feeling of weariness and became convinced[104] that he was ill, and that the fatigue could not be natural. However, he did his work like the rest. Friedmann interprets these spells as a kind of imperfect sleep.
During the day, throughout the entire time he experienced those nighttime absences, he also suffered from a different kind of seizure. While sitting in the trench for many hours, about twice a day for half an hour each time, he would suddenly fall into an overwhelming lethargy. For no apparent reason, he would feel a profound fatigue. During these episodes, he couldn't move or think and would rest his head on his hand. He couldn't shake off the feeling of exhaustion and became convinced that he was sick, believing that the tiredness wasn't normal. Still, he carried out his tasks like everyone else. Friedmann interprets these episodes as a kind of incomplete sleep.
The patient was physically healthy and stalwart, mentally not excitable, and tolerably tranquil in the midst of shell fire. He would never have been reported sick had it not been for his wound. Aside from the tachycardia, of which he himself complained little, nothing wrong was found in the hospital. There was, to be sure, a feeling of discomfort without any hysterical tinge, and sleep was restless. Aside from the peroneus palsy, the injury made a good recovery. The nocturnal attacks persisted; bromides and even luminal failed of effect. There was, however, no longer any somnolence by day. In fact, for the five weeks of observation, there was no change in his condition.
The patient was physically healthy and strong, mentally calm, and fairly relaxed even during shelling. He would never have been reported as sick if it weren't for his wound. Aside from the tachycardia, which he barely mentioned, nothing was wrong when he was in the hospital. There was definitely a sense of discomfort that wasn't hysterical, and his sleep was restless. Besides the peroneus palsy, the injury healed well. The nighttime episodes continued; bromides and even luminal didn’t help. However, he was no longer drowsy during the day. In fact, throughout the five weeks of observation, his condition showed no change.
Friedmann states that mild emotional alterations are not infrequent in the trenches with minds disposed thereto, although emotional shock, especially in shell fire, is the most frequent cause. However, these particular seizures are quite unusual. The stresses of field service lead to a sometimes complete paralysis of mental power, interfering transiently with service. There is no evidence of sudden circulatory disturbances such as would bring about dizziness, pallor, nausea, or fainting spells. According to Friedmann, the regulative brain functions, especially those that maintain consciousness, become weak on account of a condition which he terms Gehirnmüdigkeit, or, as we should say in English, brain fag. The situation forbids due completion of sleep. Thus, the explanation of the daytime attacks follows rather obvious lines of brain fag. The accidental awakening it is, which at night produces the absences; the wakenings are due to the general restlessness of the patient. The general weakening of cerebral function produces the disorder at the moment of wakening, since the regulative factors of consciousness are already out of order. The condition in the absence rather closely resembles the state of consciousness just before going to sleep, and also perhaps the state of consciousness during the process of awakening. It is as if the process of waking were somehow delayed a few moments. Friedmann[105] is interested to show the relation of such absences to the so-called gehäuften kleinen Anfälle, originally described by him in 1906 as occurring in children, and distinguished from epileptic attacks. These attacks, after lasting for years, finally disappeared completely. The same sort of thing in adults was symptomatic of some other disease, such as neurasthenia, and was not a true entity. In children these attacks failed to be attended with any mental injury, nor were there any pronounced epileptic phenomena. Bromides had no effect upon them, and they already showed a somewhat striking and peculiar appearance, involving interruptions ten seconds long of capacity to think, speak, or move, without disturbance of consciousness or automatic movements. Sometimes the attacks occurred from six to 100 times in the day, without in any respect interfering with the general condition of the child. The occurrence of such series of mild seizures is nothing but a syndrome. To be sure, some cases turn out to be cases of genuine epilepsy with an eventual degenerative process. Some forms belong in the spasmophilia group, and some among the hysterias. However, according to Friedmann, there is a narcoleptic petit mal that is an entity by itself, proceeding after a period of years to complete recovery without complications. It is this form which may be regarded as a peculiar kind of brain fag. The case of the soldier may be supposed to be one which will prove to have this benign outcome.
Friedmann notes that mild emotional changes are fairly common in the trenches where people are already inclined to them, although emotional shock, particularly from shellfire, is the most common cause. However, these specific episodes are quite rare. The pressures of field service can lead to a near-total paralysis of mental ability, temporarily affecting performance. There is no evidence of sudden circulatory issues that might cause dizziness, paleness, nausea, or fainting. According to Friedmann, the brain's regulatory functions, especially those that keep consciousness in check, weaken due to a condition he calls Gehirnmüdigkeit, or what we'd refer to as brain fag. Sleep is often disrupted, preventing proper completion. Hence, the daytime episodes can be attributed to brain fag. It’s the accidental awakenings at night that cause absence episodes; these awakenings stem from the patient’s general restlessness. The overall weakening of brain function leads to issues upon waking, since the consciousness-regulating factors are already malfunctioning. The state experienced during these absences closely resembles the period just before falling asleep and possibly that during awakening. It feels as if the waking process is somehow delayed by a few moments. Friedmann[105] aims to connect these absences to the so-called gehäuften kleinen Anfälle, which he first described in 1906 as occurring in children, distinguishing them from epileptic fits. These episodes eventually disappeared after occurring for years. A similar phenomenon in adults was a symptom of other conditions, like neurasthenia, and wasn’t a standalone issue. In children, these episodes didn’t cause any mental harm, nor were there notable epileptic symptoms. Bromides had no effect on them, and they showed a distinctive and unusual pattern, with interruptions lasting about ten seconds during which they couldn’t think, speak, or move, yet consciousness remained intact and there were no automatic movements. Sometimes these would happen six to 100 times a day without affecting the child’s overall condition. Such mild seizure episodes are simply a syndrome. Of course, some cases turn out to be true epilepsy with eventual degeneration. Some fall into the spasmophilia category, while others are classified as hysterias. However, Friedmann argues that there is a narcoleptic petit mal that exists as its own entity, leading to complete recovery over the years without complications. It’s this form that might be considered a unique version of brain fag. One could speculate that this soldier’s case might also lead to a similar benign outcome.
Sham fits.
Sham works.
Case 78. (Hurst, March, 1917.)
An unwilling conscript developed numerous fits on board ship coming from Jersey, three days after enlisting. Fifty more developed during two days in hospital. He was sent to Netley.
An unwilling recruit had several episodes on the ship coming from Jersey, three days after signing up. Fifty more episodes occurred during two days in the hospital. He was sent to Netley.
On the hypothesis of hysteria or malingering, he was hypnotized. A fit was suggested to him, but did not come off. The Sister was informed in the patient’s hearing that the man was clearly shamming, as in all genuine cases a fit would occur after this treatment. A fit with marked opisthotonos immediately occurred. This fit immediately stopped when he was ordered to stop it and to wake up.
On the assumption of hysteria or faking, he was hypnotized. A seizure was suggested to him, but it didn’t happen. The nurse was told within the patient's hearing that the man was clearly faking, as in all genuine cases a seizure would happen after this treatment. A seizure with pronounced opisthotonos immediately occurred. This seizure instantly stopped when he was told to stop it and to wake up.
The man after waking promised to have no more fits.
The man, after waking up, promised to have no more outbursts.
Epileptoid attacks, controllable by will.
Will-controlled epileptoid seizures.
Case 79. (Russell, August, 1917.)
A man was received in No. 3, General Hospital: Diagnosis, epilepsy. He was shortly sent to the convalescent camp and then returned, having had two attacks. Russel watched for another attack, felt it was not genuine and “put the situation up to” the soldier whose story was as follows: He had been at the front without leave for twelve months since the German retreat. Leave was due him. A sister’s letter said his brother was severely wounded and his mother was praying for his return. When he thought these things over an attack came. He could, however, control the attacks. Russel told him, if he would play the game, he would be sent to the base with a recommendation for leave. In ten days the man was remarkably changed and had no further attacks.
A man was admitted to No. 3 General Hospital with a diagnosis of epilepsy. He was soon sent to the recovery camp and then returned after experiencing two seizures. Russel observed him for another attack, sensed it wasn't legitimate, and "laid it out" for the soldier, whose story was as follows: He had been at the front without leave for twelve months since the German retreat. He was due for leave. A letter from his sister mentioned that his brother was seriously injured and that his mother was praying for his return. When he reflected on these things, an attack occurred. However, he realized he could control the attacks. Russel told him that if he played it straight, he would recommend him for leave to the base. In ten days, the man had changed significantly and had no further seizures.
Hereditary epileptic taint brought out by two years service with eventual shell-shock and burial thrice in one day.
Hereditary epilepsy triggered by two years of service, culminating in shell shock and being buried three times in one day.
Case 80. (Hurst, March, 1917.)
A private, 24, in the army from 16, never epileptic (sisters epileptic), was wounded four times in the war from September, 1914. Shell fire did not worry the man, but he gradually became depressed after his father and five brothers had died in active service. He was blown up and buried three times in one day in July, 1916. He was unconscious for two hours after the second blowing up, but carried on for two hours more until blown up for the third time.
A private, 24, who had been in the army since he was 16 and had never had epilepsy (his sisters did), was injured four times in the war starting in September 1914. He wasn't bothered by shellfire, but he gradually fell into depression after his father and five brothers were killed in action. In July 1916, he was blown up and buried three times in one day. He was unconscious for two hours after the second explosion but continued for another two hours until he was blown up for the third time.
After this, he became nervous and shaky, and began to sleep badly, and a month later had a typical attack of major epilepsy. Fits occurred with increasing frequency. As many as 19 occurred in a single day. Rest and bromides caused the fits to cease, and there had been none for six weeks at the time of his discharge.
After this, he became anxious and jittery, and started to sleep poorly, and a month later he had a serious seizure episode. The seizures happened more often, with as many as 19 occurring in one day. Rest and bromides helped stop the seizures, and there hadn’t been any for six weeks by the time he was discharged.
Re Shell-shock and its relations to epilepsy, see below, discussion under Cases 82-84 of Ballard, who has erected a theory of Shell-shock as in some sense epileptic.
Re Shell-shock and its connections to epilepsy, see below for the discussion under Cases 82-84 of Ballard, who has developed a theory that suggests Shell-shock is, in some way, related to epilepsy.
Shell-shock: Epilepsia larvata.
Shell shock: Epilepsia larvata.
Case 81. (Jeweler and Quellien, May, 1917.)
A soldier, 29 (father alcoholic, died in hospital for the insane), a decorative painter without plumbic history, non-alcoholic, non-syphilitic, was wounded once, September, 1914, but returned to the front in 1915.
A 29-year-old soldier (with an alcoholic father who died in a mental hospital), a decorative painter with no history of lead poisoning, not an alcoholic, and not syphilitic, was wounded once in September 1914 but went back to the front in 1915.
May, 1915, a shell burst near him. He lost consciousness, regained it a few days later at Brest, and was so far recovered that he could go on leave in seven days. While on leave, he had short attacks of delirium, followed by a total amnesia; there was, however, no crisis, fall, or convulsion. After the first attack, he had for 24 hours malaise and headache, but got well and went back to his dépôt. Shortly afterward more attacks of this sort recurred, and he went to hospital and thence to the neurological centre at Tours. Whence, August 9, 1915, he got a two-months’ leave for “mental disorder post-confusional, second état, probably hysterical (commotio cerebri), and organic hemiparesis.”
May 1915, a shell exploded nearby. He lost consciousness and regained it a few days later in Brest. He had recovered enough to go on leave in seven days. While on leave, he experienced brief episodes of delirium followed by total amnesia; however, there was no crisis, fall, or convulsion. After the first episode, he felt unwell and had a headache for 24 hours, but then he got better and returned to his depot. Soon after, similar episodes occurred again, and he went to the hospital and then to the neurological center in Tours. From there, on August 9, 1915, he received a two-month leave for "mental disorder post-confusional, second état, probably hysterical (commotio cerebri), and organic hemiparesis."
November, 1915, after returning to the dépôt, there were more spells and he went again to hospital. Invalided December, 1915, he passed a year at home, but the spells continued. Although the epileptic nature of these attacks was maintained by Francais at Évreux, he was placed in the auxiliaries, December, 1916, but had to go to hospital almost at once, and, February 28, 1917, entered the neurological centre of the 9th Region for the second time. Here, when called to be examined two days after admission, he was observed in an attack. He suddenly rose from the bench, made a few steps, seemed to be listening and anxious, as if he ought to be on guard. He looked up, seemed to be looking for something whose noise was approaching, lowered his head, made a slight jerking movement, and said, “Poum!” as if to express the noise of an explosion. He took a few more steps, the same movements were repeated, and the same “Poum!” was uttered. This lasted for about a quarter of an hour, during which the patient was unaware of his surroundings. He could be guided all about the hall without[109] resistance, but did not respond to orders, commands, noises, or contact. In short, the patient was in the midst of a hallucinatory dream at his post in the trenches, undergoing a bombardment. He was placed in a chair; remained motionless for a few seconds, woke up, and answered questions. “Where am I? Oh, yes; I must have been sick because my head feels bad.” In answer to the question. “What did you see; what was there?”, he said, “I don’t remember anything. I never remember. I don’t know.” The patient was dull and weak after the spell.
November 1915, after returning to the base, he had more episodes and went to the hospital again. Discharged in December 1915, he spent a year at home, but the episodes continued. Although the epileptic nature of these attacks was noted by Francais at Évreux, he was assigned to the auxiliaries in December 1916, but had to go to the hospital almost immediately and, on February 28, 1917, entered the neurological center of the 9th Region for the second time. Here, when he was called for examination two days after admission, he was observed having an episode. He suddenly got up from the bench, took a few steps, seemed to be listening and anxious, as if he needed to be on guard. He looked up, appeared to be searching for something whose sound was approaching, lowered his head, made a slight jerking movement, and said, “Poum!” as if to mimic the sound of an explosion. He took a few more steps, repeated the same movements, and uttered the same “Poum!” This lasted about a quarter of an hour, during which he was unaware of his surroundings. He could be guided around the hall without resistance but didn’t respond to orders, commands, noises, or touch. In short, he was lost in a hallucinatory dream at his post in the trenches, enduring a bombardment. He was placed in a chair, stayed motionless for a few seconds, then woke up and answered questions. “Where am I? Oh, yes; I must have been sick because my head feels bad.” When asked, “What did you see; what was there?”, he replied, “I don’t remember anything. I never remember. I don’t know.” He was dull and weak after the episode.
These spells varied in number but occurred once a week. The patient was able to tell of certain attacks that had occurred while he was out of doors at home.
These episodes varied in frequency but happened once a week. The patient was able to describe specific incidents that took place while he was outside at home.
Now and then, there was another theme in the hallucinatory delirium, namely, a pencil drawing of a woman’s picture, of no great artistic worth but carefully done, at which the patient was much astonished on awaking.
Now and then, there was another theme in the hallucinatory delirium, namely, a pencil drawing of a woman’s picture, of no great artistic worth but carefully done, at which the patient was much astonished on waking.
It seems as if auto- and hetero-suggestion can be eliminated from the genesis of these attacks. Neither hysterical nor epileptic crises have preceded or ever alternated with these seizures. Nevertheless, on the organic side, the patient had a general increase of tendon reflexes on the left side, most marked in the knee-jerk, and fell to the left in voltaic vertigo. There was a left hemiparesis, apparently of organic origin, which had been determined as far back as July, 1915.
It looks like both self-suggestion and outside suggestion can be ruled out as causes of these attacks. Neither hysteria nor epilepsy has come before or alternated with these seizures. However, on the physical side, the patient had a noticeable increase in tendon reflexes on the left side, most significantly in the knee-jerk response, and experienced leftward falling in electrical vertigo. There was a left hemiparesis that seemed to have an organic cause, identified back in July 1915.
There was no true dementia. Past memories were but slowly recalled, and inattention interfered with the fixation of recent memory. He complained of troubles in his sleep and dreamed of war experiences somewhat analogous to those in his attack of amnestic delirium. After the seizure, there was a marked hebetude and mental inactivity, torpor, and a severe headache. The case was presented to a special commission as one of epilepsia larvata in a person hereditarily predisposed who had never before presented epileptic signs, suffering from a disease characterized by frequent short attacks of hallucinatory and delirious automatism, following shell explosion which had at the same time produced a slight left-sided hemiparesis and mental inhibition.
There was no actual dementia. Past memories were slowly retrieved, and a lack of focus made it hard to form new ones. He reported issues with sleep and dreamed of war experiences similar to those during his episode of amnestic delirium. After the seizure, he showed significant lethargy and mental inactivity, along with a severe headache. The case was brought before a special commission as a case of latent epilepsy in someone with a hereditary predisposition who had never shown signs of epilepsy before, experiencing a condition marked by frequent short episodes of hallucinations and delirious behavior, following a shell explosion that also caused a slight weakness on the left side and mental inhibition.
To illustrate an epileptic theory of Shell-shock; three cases:
To explain a theory about Shell-shock related to epilepsy; three cases:
1. Fugue; minor symptoms: later, epilepsy.
1. Fugue; minor symptoms: later, epilepsy.
2. Epileptic confusion eight months after explosion.
2. Seizure-related confusion eight months after the explosion.
3. Mine explosion: stammering replaced by mutism; mutism replaced by epilepsy.
3. Mine explosion: stuttering replaced by silence; silence replaced by seizures.
Case 82. (Ballard, 1917.)
Atmospheric concussion from shell explosion, October, 1915, was followed by unconsciousness in a soldier described by Ballard.
Atmospheric blast from a shell explosion in October 1915 led to a soldier's unconsciousness, as described by Ballard.
Blindness for a month followed recovery of consciousness. “Neurasthenia” (anxiety neurosis) after return of sight. Apparently nearly complete recovery after latent period of a few weeks. Return of blindness in one eye in December. Five days automatic wandering (the man was found in a west country town five days after leaving home to rejoin his dépôt and seen by a medical officer who reported that he was dazed and amnestic for that period); admission to second Eastern General Hospital, December 15.
Blindness lasted for a month after gaining consciousness. "Neurasthenia" (anxiety neurosis) followed the return of sight. There seemed to be almost a complete recovery after a few weeks of waiting. One eye went blind again in December. He wandered aimlessly for five days (the man was found in a town in the west, five days after leaving home to go back to his depot, and was seen by a medical officer who reported that he was dazed and couldn’t remember that time); he was admitted to the second Eastern General Hospital on December 15.
On admission he proved to be suffering from minor hysterical symptoms such as an inability to open his eyes and to see clearly when the lids were raised. The symptoms rapidly cleared up under suggestive conversation and did not return except for amnesia and slight emotional depression. He remained well until December 25. On that day he began for the first time to have definite epileptic fits and nocturnal epileptic delirium. In January he was discharged as an epileptic. There was no epileptic temperament or feeblemindedness. Finally, there had never been any personal or family neuropathic or psychopathic history.
On admission, he appeared to be experiencing minor hysterical symptoms, such as difficulty opening his eyes and seeing clearly when his eyelids were lifted. These symptoms quickly resolved with suggestive conversation and didn't come back, except for some amnesia and mild emotional depression. He stayed well until December 25. On that day, he began to experience clear epileptic seizures and nighttime epileptic delirium for the first time. In January, he was discharged as an epileptic. There was no sign of an epileptic temperament or intellectual disability. Additionally, there had never been any personal or family history of neuropathic or psychopathic issues.
Case 83. (Ballard, 1917.)
A soldier was blown up, April, 1915, and had a spell of unconsciousness. Later, pains in the head, slight amnesia and a condition of asthenia developed.
A soldier was injured by an explosion in April 1915, resulting in a period of unconsciousness. Later, he experienced headaches, mild memory loss, and fatigue.
He was eventually admitted to the second Eastern General Hospital at Brighton, January, 1916. At the time of admission he was semiconscious, stuporous, confused, disoriented, anxious in a dull sort of way, talking about his expectation of “a sailor with a card.” Speech was intelligible, though fragmentary and infrequent. The man obeyed commands but gave no replies to questions. The mental processes were slow and impaired.
He was finally admitted to the second Eastern General Hospital in Brighton in January 1916. When he arrived, he was semi-conscious, unresponsive, confused, disoriented, and anxious in a muted way, talking about his expectation of “a sailor with a card.” His speech was understandable but fragmented and rare. He followed commands but didn’t respond to questions. His mental processes were slow and impaired.
According to Ballard, we have here a case of epileptic confusion, eight months after the initial concussion. This particular attack ceased three days later, leaving amnesia for the attack and a certain amount of mental retardation. The man was not epileptic in temperament and his personal and family history proved negative.
According to Ballard, this is a case of epileptic confusion, eight months after the original concussion. This specific attack ended three days later, resulting in amnesia from the attack and some degree of cognitive impairment. The man did not have an epileptic temperament, and both his personal and family history were clear.
Case 84. (Ballard, 1917.)
A soldier was buried in a mine explosion, October, 1915, and for several days thereafter was unconscious or semi-conscious. He emerged deaf and subject to stammering and a condition termed “neurasthenic.” The stammering was soon replaced by mutism, which lasted several weeks. The mutism was then supplanted by epileptic fits.
A soldier was buried in a mine explosion in October 1915, and for several days after that, he was either unconscious or semi-conscious. He came out of it deaf and prone to stuttering, along with a condition called "neurasthenia." The stuttering was quickly replaced by mutism that lasted for several weeks. After that, the mutism gave way to epileptic seizures.
He was observed by Ballard in a dreamlike, disoriented and inaccessible state, in which he was anesthetic to pin pricks, lay awestruck, dumbly following with his finger hallucinatory airplanes. Flexibilitas cerea was also shown at this time.
He was seen by Ballard in a dreamlike, disoriented, and unreachable state, where he was numb to pinpricks, laying in awe, silently tracing hallucinatory airplanes with his finger. Flexibilitas cerea was also evident at that time.
Next day he emerged from the dreamlike state with mental processes somewhat slowed, disorientation for time, amnesia for the attack, memory disturbance and a return of the stammer. On the next day following, all these symptoms had disappeared except amnesia for the attack. Another spell of epileptic fits occurred later. It seems that the man had had a convulsion thirteen years before and occasional convulsions since. In fact, he, seven years before, had had what was called “a stroke” and residuals of a slight hemiplegia were still present. (There is no statement in the case report relative to syphilis.)
The next day, he came out of the dreamlike state with his thinking somewhat slow, feeling disoriented about time, unable to remember the attack, experiencing memory issues, and his stutter returning. The day after that, all these symptoms had disappeared except for the memory loss related to the attack. Another episode of seizures happened later. It turns out that he had a seizure thirteen years earlier and had occasional seizures since then. In fact, seven years prior, he had what was referred to as “a stroke,” and slight residual weakness on one side was still noticeable. (There is no mention in the case report regarding syphilis.)
Emotion; shell fire: Epileptic equivalents.
Emotion; shelling: Epileptic equivalents.
Case 85. (Mott, January, 1916.)
A man, 19, suffered from shock due to emotional stress and shell fire. He had terrifying dreams. After a short time, he developed paroxysmal attacks of maniacal excitement. Just before the first attack he had been helping in the kitchen, lay down on his bed, went to sleep, woke, startled, flushed, and sweating, and made for the door as if terrified. He remained in this state as if suffering from hallucinations of sight and hearing, and without ability to recognize his wife, the doctors, or the Sisters. When two strangers in uniform came in to observe him, the adjutant became violent, as if the uniforms had started terror anew. The attacks lasted from a few hours to a few days, coming on suddenly, without apparent cause. One day he tried to get over the wall of the playground. He came back and buried his head in his hands. Major Mott spoke to him, whereupon he got up, looking terrified, made for the door, and four orderlies were required for his restraint. At Napsbury Hospital, to which he was sent, he made a complete recovery.
A 19-year-old man experienced shock from emotional stress and artillery fire. He had horrible nightmares. Soon after, he started having sudden episodes of extreme excitement. Just before the first episode, he was helping in the kitchen, lay down on his bed, fell asleep, woke up startled, flushed, and sweating, and rushed to the door as if he were in panic. He stayed in this state, seemingly suffering from visual and auditory hallucinations, unable to recognize his wife, the doctors, or the nurses. When two unfamiliar soldiers entered to observe him, he became aggressive, as if the uniforms triggered his terror again. The episodes lasted from a few hours to several days, occurring suddenly and without any clear reason. One day, he tried to climb over the playground wall. He returned and buried his head in his hands. Major Mott spoke to him, and he got up looking scared, headed for the door, and it took four orderlies to restrain him. At Napsbury Hospital, where he was taken, he made a full recovery.
Mott suggests that we are dealing with a psychic equivalent of epilepsy.
Mott suggests that we are facing a mental equivalent of epilepsy.
Re epileptic equivalents, compare notes from Lépine under 58 and 59.
Re epileptic equivalents, check notes from Lépine under 58 and 59.
IV. PHARMACOPSYCHOSES
(THE ALCOHOL, DRUG, AND POISON GROUP)
Pathological intoxication.
Pathological intoxication.
Case 86. (Boucherot, 1915-6.)
A Territorial infantryman, aged 37, was in the habit of drinking a good deal without getting drunk, and at the front drank a good deal of bad brandy. He had just taken a considerable quantity when his regiment got the order to charge. The charge was hardly over when the man became greatly excited and hallucinated. He thought he was surrounded by Germans and tried to transfix his comrades with the bayonet. Howling and struggling he was carried to the rear.
A 37-year-old territorial infantryman often drank a lot without getting drunk, and at the front, he consumed a lot of poor-quality brandy. He had just downed a significant amount when his regiment received orders to charge. The charge had barely finished when he became extremely agitated and started hallucinating. He believed he was surrounded by Germans and attempted to stab his fellow soldiers with his bayonet. Screaming and thrashing, he was taken to the rear.
He was soon brought to the asylum at Fleury after howling all night and seeing the Boches and animals fighting among themselves. His hands and tongue were tremulous and there were cramps in the calves of his legs. On the 6th he expressed astonishment to find himself in hospital and was found to have but slight memory of what had happened. He remembered, however, that he had tried to kill his comrades. With the deprivation of alcohol he became rapidly normal and was sent back to the dépôt in a few days.
He was quickly taken to the asylum at Fleury after screaming all night and witnessing the Germans and animals fighting among themselves. His hands and tongue were shaky, and he had cramps in his calves. On the 6th, he was surprised to find himself in a hospital and had only a faint memory of what had occurred. However, he did remember that he had tried to attack his comrades. As he went without alcohol, he quickly returned to normal and was sent back to the depot in just a few days.
Re alcoholism under army conditions, Lépine remarks that alcohol has played in this war a rôle analogous to that of malaria in the epidemiology of some countries. Many of the victims are, to start with, unbalanced subjects and détraqués who are hereditary alcoholics. Alcoholism, according to Lépine, dominates the pathology of the interior and has a marked bearing upon conditions at the front. In fact, alcoholism would have been disastrous in France had not measures been taken against it; measures still insufficient (1917). More than one-third of 6000 cases studied by Lépine during three years have shown alcohol as a sole or, at all events, principal cause of the difficulty. It would be within[114] reason to state, according to Lépine, that if we throw in cases in which alcoholism was a partial factor, more than half, or even more than two-thirds, of the mental cases had been strongly influenced by alcohol. Lépine thinks there may be effects like those of anaphylaxis. Certainly, the startling and sudden effects in so-called pathological intoxication, as in Case 86, suggest the critical and vehement effects seen in the sensitized anaphylactic subject.
Regarding alcoholism in army conditions, Lépine notes that alcohol has played a role in this war similar to that of malaria in the epidemiology of some countries. Many of the victims are, to begin with, individuals with psychological imbalances and disturbances who are hereditary alcoholics. According to Lépine, alcoholism is a major factor in internal health issues and significantly affects conditions at the front. In fact, alcoholism could have been disastrous in France if measures hadn’t been implemented against it; however, these measures are still insufficient (1917). More than one-third of 6000 cases studied by Lépine over three years showed alcohol as the sole or, at the very least, the main cause of the issue. It would be reasonable to say, according to Lépine, that if we include cases where alcoholism was a contributing factor, more than half, or even over two-thirds, of the mental health cases were strongly influenced by alcohol. Lépine suggests there might be effects similar to anaphylaxis. Certainly, the shocking and sudden effects seen in so-called pathological intoxication, as in Case 86, hint at the severe and intense effects observed in sensitized anaphylactic individuals.
Chart 4
PHASES OF WAR PSYCHIATRY IN FRANCE
| I. | Antebellum phase of Mental Health Neglect: Groundless fear that recruiting would be disorganized by psychiatric sifting processes. |
| II. | Phase of Mobilization Alcoholism: Hospitals unprepared. |
| III. | Phase of the Marne: Alcoholism restrained by law; psychoses few; psychiatrists optimistic. |
| IV. | Phase of Trench Combat: Overemotionality; and of High Explosives (January, 1915); now psychiatric services were systematically established along evacuation lines. |
| V. | Phase of War Psychotherapy: Filterwise system of management (a) near trenches, (b) in main body of army, (c) on evacuation lines, (d) special hospitals. |
Chiefly from data of Chavigny, 1915.
Chiefly based on data from Chavigny, 1915.
Pathological intoxication: criminal prosecution stopped.
Pathological intoxication: criminal charges dropped.
Case 87. (Loewy, 1915.)
An orderly, in private life a teacher, one day about noon-time, when going on duty, called the commanding officer to account because he (the orderly) had had to wait. He said he had been ordered to come at two o’clock and it was already long thereafter! He was severely reprimanded but addressed a number of the officers present with questions having no relation to military service. In fact, he seemed to have forgotten entirely that he was on military service.
An orderly, who was a teacher in his personal life, one day around noon, called the commanding officer to task because he (the orderly) had to wait. He said he was told to come at two o’clock and it was already well past that time! He received a harsh reprimand but then directed several unrelated questions to the officers present, seemingly forgetting entirely that he was supposed to be on duty.
This was the more remarkable as the teacher-orderly had many times distinguished himself upon dangerous patrol expeditions and in critical situations, winning the confidence of his superiors and the likelihood of promotion to corporal. He had been a discreet, earnest, and clever soldier.
This was even more impressive since the teacher-orderly had often distinguished himself on dangerous patrols and in critical situations, earning the trust of his superiors and the possibility of a promotion to corporal. He had been a careful, dedicated, and smart soldier.
Loewy observed him during this affair and noticed that he did not by language or movement suggest intoxication or hilarity but merely a certain excitement. He was entirely oriented for time, place and person, and his outward behavior was correct enough except for his military rank.
Loewy watched him during this situation and noticed that he did not show signs of drunkenness or laughter through his words or actions, just a kind of excitement. He was completely in tune with the time, place, and people around him, and his outward behavior was appropriate enough except for his military rank.
Sent to his quarters near by, he gave the impression to his immediate superior officer of deep drunkenness. He murmured something and soon fell into a deep sleep. After waking, he had an almost complete amnesia, knowing only that something disagreeable had transpired. He remembered that he had been offered several little glasses of cognac brandy by a comrade, and that he had drained them off quickly before going on duty. He said that he had never drunk cognac before, and in fact had drunk nothing for a long time.
Sent to his nearby quarters, he gave his immediate superior officer the impression that he was extremely drunk. He mumbled something and soon fell into a deep sleep. After waking up, he had almost total amnesia, only knowing that something unpleasant had happened. He recalled that a comrade had offered him several small glasses of cognac brandy, which he quickly downed before starting his shift. He mentioned that he had never had cognac before and, in fact, hadn't drunk anything for a long time.
The diagnosis of pathological intoxication was made, and the soldier was thereby cleared of his dangerous situation; a criminal prosecution was not instituted. He thereafter behaved with entire sobriety and modesty, and he achieved his corporalcy and later became file leader.
The diagnosis of pathological intoxication was made, and the soldier was cleared of his dangerous situation; there was no criminal prosecution. He then behaved with complete sobriety and modesty, and he earned his corporal rank and later became a file leader.
Desertion in alcoholism may deserve the term “pathological.” Case of fugue.
Desertion in alcoholism might be considered "pathological." Example of a fugue.
Case 88. (Logre, July, 1916.)
A “deserter” said: “I went because I drank a glass. I just went, comme ça, without any motive.” He was somewhat feebleminded and, in explaining the impulsivity of his act, he added: “I went like a broken-down beast. I walked straight ahead, without knowing where I was going and if I had been going to be killed, it would have been all the same to me.” He could not that afternoon remember very well; but next morning, after having slept, he regained full consciousness. He said that he then found himself in a field near a cemetery. He had carried his gun and equipment with him, but had lost them somewhere, and from a military point of view, his desertion was complicated by loss of effects. On coming to, he said to himself, “Where am I? How foolish after fifteen months in the line! Probably I have deserted again.” In fact, he had a month before left his post under exactly the same conditions in the midst of a period of alcoholic excitement.
A “deserter” said: “I left because I had a drink. I just walked away, like that, without any reason.” He was somewhat slow-witted and, while explaining his impulsive choice, he added: “I moved like a worn-out animal. I walked straight ahead, not knowing where I was going, and if I had been about to be killed, it wouldn’t have mattered to me.” He couldn’t remember very clearly that afternoon; but the next morning, after sleeping, he became fully aware again. He said he then found himself in a field near a cemetery. He had taken his gun and gear with him but had lost them somewhere, and from a military perspective, his desertion was complicated by the loss of his equipment. When he came to, he thought to himself, “Where am I? How stupid after fifteen months at the front! I probably deserted again.” In fact, he had left his post under exactly the same circumstances a month earlier during a period of heavy drinking.
This alcoholic fugue is typical: drunkenness, impulsive and subconscious ambulatory automatism, with partial amnesia, disorientation, with mislaying of objects, followed by sleep and immediate return to normality.
This state of being drunk is pretty typical: feeling intoxicated, acting on impulse without thinking, moving around almost like a robot, with some memory loss, confusion, losing things, then dropping off to sleep and quickly getting back to normal.
Re fugue, see discussion under Cases 58 and 59. The French military code cannot excuse victims of fugue even though executed in a quite unconscious state, if the fugue is due to alcohol. There was a certain procursive suggestion in the fugue of Case 88, who went “like a broken-down beast,” straight ahead, without knowing where he was going.
Re fugue, see discussion under Cases 58 and 59. The French military code cannot excuse victims of fugue even if it occurs in an unconscious state, if the fugue is caused by alcohol. There was a certain driving force in the fugue of Case 88, who moved forward “like a broken-down beast,” directly ahead, without knowing where he was headed.
Alcoholism: Amnesia experimentally reproduced.
Alcoholism: Amnesia recreated in tests.
Case 89. (Kastan, January, 1916.)
February 15, 1915, a German soldier drank beer in the canteen and at roll-call appeared tipsy. He then went to bed, but rose an hour later to go to town. A quarter of an hour later, he went to a clerk’s house and asked for paper, on the ground that the next day he was going to march to Warsaw. The clerk gave him no paper, which he then tried to get by force. A policeman arrested him and he said, “You just wait, lame dog!” Upon examination he denied that he had ever been guilty of any crime but had been in institutions on account of delirium. In point of fact, this man had grown up in very bad surroundings, amongst quarrels and disputes of his parents, who kept a disorderly house. At 19 he had been convicted of incest. He finally admitted having been convicted for rape. It was found that he had once run out into the front trenches; had been removed by an advance guard to a stable, and then wondered why he was not in school. He described a number of attacks of delirium although he had not drunk more than moderately.
February 15, 1915, a German soldier drank beer in the canteen and appeared tipsy at roll call. He then went to bed but got up an hour later to go to town. A quarter of an hour later, he went to a clerk’s house and requested paper, claiming that he was going to march to Warsaw the next day. The clerk didn’t give him any paper, which he then tried to obtain by force. A policeman arrested him, and he said, “You just wait, lame dog!” During the examination, he denied ever committing any crime, saying he had been in institutions because of delirium. In reality, this man had grown up in terrible conditions, surrounded by the arguments and disputes of his parents, who ran a disreputable house. At 19, he had been convicted of incest. He eventually admitted to being convicted of rape. It was discovered that he had once run out into the front trenches, was removed by an advance guard to a stable, and then wondered why he wasn’t in school. He described several episodes of delirium even though he hadn’t drunk excessively.
He was given an experimental dose of 50 c.c. of alcohol, and in ten minutes became excited, tried to get out of bed, attacked other patients without reason, and was able to speak neither spontaneously nor in response to questions. In a period of two hours he became clear and asked what the trouble was. He knew only that he had taken alcohol.
He was given an experimental dose of 50 c.c. of alcohol, and within ten minutes, he became agitated, attempted to get out of bed, attacked other patients for no reason, and couldn't speak either spontaneously or in response to questions. After two hours, he became clear and asked what was going on. He only knew that he had consumed alcohol.
Re the experimental excitement produced in Kastan’s case by the exhibition of alcohol, it is of note that Bérard has been much impressed by the agitation that surgical cases of alcoholism undergo when anesthetized. It may be that the anesthetics act similarly to the experimental alcoholism of Kastan’s case. According to Bérard, these phenomena of the anesthetized wounded (who are men recently evacuated from the front and other hospital cases) are of larval alcoholism brought out by the anesthesia. Bérard wonders whether rum issues at the front are at all responsible therefor.
Re the experimental excitement shown in Kastan's case from alcohol exposure, it's worth noting that Bérard has been significantly struck by the agitation that surgical cases of alcoholism experience when anesthetized. It’s possible that the anesthetics have a similar effect to the experimental alcoholism seen in Kastan's case. Bérard suggests that the phenomena observed in the anesthetized wounded (who are men recently evacuated from the front and other hospital cases) reflect a form of latent alcoholism triggered by the anesthesia. Bérard is curious if the rum supplies at the front have any part in this.
Desertion, drunk. Contributory factors.
Desertion, intoxicated. Contributing factors.
Case 90. (Kastan, January, 1916.)
Gottlieb S. left the barracks, January 25, 1915, met friends and drank with them, remaining all night in the railway restaurant and waiting room. He was promptly arrested.
Gottlieb S. left the barracks on January 25, 1915, met up with friends, and spent the whole night drinking with them in the railway restaurant and waiting room. He was quickly arrested.
According to the patient, he had always drunk a good deal and had once fallen from his horse in the campaign, and become unconscious. After this fall, he said he had been able to stand less alcohol than before.
According to the patient, he had always drank a lot and had once fallen off his horse during the campaign and lost consciousness. After this fall, he said he could handle less alcohol than he could before.
There is doubt as to the syphilis of Gottlieb. He said he had been infected once, but his further statement that he had six relapses is, of course, questionable. As to the hypothesis of feeblemindedness, it appears that in childhood he had learned badly and had been a stammerer. He had been a herdsman, and after that a laborer. He finally became a travelling man for a specialty photographer.
There is uncertainty about Gottlieb's syphilis diagnosis. He claimed he had been infected once, but his later statement that he had six relapses is definitely questionable. Regarding the possibility of feeblemindedness, it seems he struggled with learning as a child and had a stuttering problem. He worked as a herdsman and later as a laborer. Eventually, he became a traveling salesman for a specialty photographer.
He had previously been convicted of an embezzlement, brawling, and breach of the peace.
He had previously been convicted of embezzlement, fighting, and disturbing the peace.
As to his military crime, he said he had been celebrating the emperor’s birthday the last three days, being urged on by acquaintances and drinking whiskey. He was, in fact, on a spree and did not eat properly. He had met a student in the railway station and had forgotten all about his military service. He remembered having spoken with the waiter, remembered telling the student that he was going to commit suicide, and the student had drunk seltzer with him. January 29, he for some reason drank no more, and then it occurred to him that he ought to go back to duty. He remembered that he was easily led astray. He had once thought of becoming a tanner but had been dissuaded from the trade because of its bad smell.
Regarding his military offense, he stated that he had been celebrating the emperor’s birthday for the past three days, encouraged by his friends while drinking whiskey. He was, in fact, on a bender and hadn’t been eating properly. He had run into a student at the train station and completely forgotten about his military obligations. He recalled talking to the waiter, remembered telling the student that he was planning to commit suicide, and the student had shared seltzer with him. On January 29, for some reason, he stopped drinking, and then it hit him that he needed to return to duty. He recognized that he was easily influenced. He had once considered becoming a tanner but was talked out of it because of the unpleasant smell.
The analysis of this case must consider, first, syphilis. Supposing, however, that this hypothesis is not substantiated by laboratory findings, the hypothesis of feeblemindedness might well be raised. It seems possible, if not probable, that this patient was in the subnormal group, lying between normality and feeble-mindedness[120] proper. The value of mental tests would here be extreme. There seems to be no evident epilepsy, and the majority of the phenomena can perhaps best be explained by alcoholism. Possibly the case is one of so-called pathological intoxication. The patient’s own story that, although he had been always subject to drink, he had been less tolerant of alcohol since a fall from his horse, seems to be entirely consistent with the post-traumatic history of numerous cases, so that it would hardly be wise to consider that alcohol accounts for the whole story. We must raise then in succession the hypothesis of syphilis, feeblemindedness, alcoholism, and coarse brain disease, bearing in mind also early stammering. As to the utilization of such a man, it would appear that a supervision of him with absolute countermanding of alcohol in view of the decrease in tolerance of alcohol since the fall from his horse might perhaps preserve this man for some form of military service.
The analysis of this case must first consider syphilis. However, if laboratory findings do not support this hypothesis, we might need to consider feeblemindedness. It seems possible, if not likely, that this patient falls into the subnormal category, existing somewhere between normality and feeblemindedness[120]. The role of mental tests in this scenario would be crucial. There appears to be no clear sign of epilepsy, and most of the symptoms might be best explained by alcoholism. It's possible that this case represents what is known as pathological intoxication. The patient’s claim that, although he has always struggled with alcohol, his tolerance has decreased since he fell off his horse, aligns with the post-traumatic accounts of many similar cases. Therefore, it may not be wise to assume that alcohol explains the entire situation. We need to consider, in order, the hypotheses of syphilis, feeblemindedness, alcoholism, and severe brain disease, while also keeping in mind early stammering. Regarding how to manage this man, it seems that close supervision, coupled with a strict ban on alcohol due to his decreased tolerance since the horse accident, might allow him to be fit for some form of military service.
Re German and French war alcoholism, Soukhanoff remarks that the conditions in these countries were in strong contrast to those in Russia. In Russia there was a great decrease in the number of cases of acute alcoholic psychosis; particularly at the time of mobilization, there were few cases of alcoholic psychosis. He says that during the Russo-Japanese war, alcoholic psychoses constituted a third of all the mental cases observed. This figure corresponds with that quoted above from Lépine (see under Case 86). Soukhanoff, writing in 1915, had not observed personally a single case of alcoholic psychosis. Incidentally, the number of cases of psychosis in the Russian army had remained in general small.
Re German and French war alcoholism, Soukhanoff notes that the conditions in these countries were very different from those in Russia. In Russia, there was a significant drop in the number of acute alcoholic psychosis cases; especially during mobilization, there were very few instances of alcoholic psychosis. He mentions that during the Russo-Japanese war, alcoholic psychoses made up a third of all the mental cases observed. This statistic aligns with what Lépine reported (see under Case 86). Soukhanoff, writing in 1915, had not seen a single case of alcoholic psychosis himself. Additionally, the overall number of psychosis cases in the Russian army remained relatively low.
Desertion by mild alcoholic dement.
Desertion by mild alcoholic dementia.
Case 91. (Kastan, January, 1916.)
Emil S. made a number of statements when he came for examination. He had once had a treatment by injections. Both his mother and his grandmother had been insane. He said that his brother was an officer in the navy, but this statement was found to be false.
Emil S. made several statements when he came in for an evaluation. He had previously received treatment through injections. Both his mother and grandmother had been mentally ill. He claimed that his brother was a navy officer, but this turned out to be untrue.
According to his story, he had lost touch with his troop at the end of September, 1914, and had lived in several lodgings in T—— up to October 19, when he was arrested. He said that he did not know that a man who had lost touch with his troop had to report.
According to his account, he lost contact with his unit at the end of September 1914 and stayed in various places in T—— until October 19, when he was arrested. He mentioned that he didn’t realize a soldier who had lost contact with their unit needed to report that.
A week after his arrest, S. entered a shop and asked for coffee, saying that he had a furlough of 24 hours and wanted cake for his comrades. He said he was the owner of an estate and would send a roebuck for the cakes. The shop-man gave him cakes to the value of one mark. Bystanders said that he had been lodging in T—— for about two weeks. It seems that he had told his landlady that a city official had quartered him upon her and that he was on furlough. He went away in the morning and came back in the evening. He had written to a bank of which he had once been a representative, asking for money. One night he had lodged with another landlady, being given a meal, and he had there stated that he was in the City of T—— on duty and that his horse was in the barracks. He offered a thousand marks for his board and lodging.
A week after his arrest, S. walked into a shop and asked for coffee, saying he had a 24-hour leave and wanted cake for his friends. He claimed to be the owner of an estate and would send a roebuck for the cakes. The shopkeeper gave him cakes worth one mark. People nearby said he had been staying in T—— for about two weeks. It seemed he had told his landlady that a city official had assigned him to her place and that he was on leave. He left in the morning and returned in the evening. He had written to a bank where he had once worked, asking for money. One night, he stayed with another landlady, where he was provided a meal, and he told her he was in the City of T—— on official duty and that his horse was in the barracks. He offered a thousand marks for his room and board.
At another lodging he had given himself out as a courier. In fact, the letter to the above-mentioned bank had been signed “Otto S., Land-owner, at present, courier.”
At another place he had pretended to be a courier. Actually, the letter to the bank mentioned above had been signed “Otto S., Land-owner, currently working as a courier.”
“If I do not revoke this in person or by writing on January 1, 1915, I beg you to pay to Mr. and Mrs. M. of T——, one thousand marks and deduct it from my balance.
“If I do not cancel this in person or in writing by January 1, 1915, please pay Mr. and Mrs. M. of T—— one thousand marks and deduct it from my balance.
“This is to be considered as my last will. As witness: present: Joseph B.”
“This is my last will. Witness: Joseph B.”
The letter was addressed “To the direction of Commercial-Counsellor P——.” There was no stamp on the letter.
The letter was addressed "To the attention of Commercial-Counsellor P——." There was no stamp on the letter.
A second letter reads:
A second letter says:
“Honored Sir, Commercial Counsellor:
"Dear Sir, Commercial Counsellor:"
I beg you to send by return mail to the address given below 1000 marks, and deduct this amount from my account. I have been in Russia. Well, things are moving now. Thank God, we have reached the point we have. Write me please more in detail about my property and estate and give me your very valuable advice.
I kindly ask you to send 1000 marks to the address below through return mail and deduct this amount from my account. I've been in Russia. Things are moving now. Thank God we've made it this far. Please write to me with more details about my property and estate and share your valuable advice.
With best regards to your esteemed wife, I remain
With best regards to your respected wife, I remain
Sincerely and respectfully yours,
Sincerely,
Otto S., at present courier, otherwise, land-owner.”
Otto S., currently a courier, otherwise a landowner.
As for this Commercial-Counsellor P., P.’s son stated that his father had been dead for three years and a half.
As for this Commercial-Counsellor P., P.'s son said that his father had been dead for three and a half years.
S. gave himself out in T—— as a land-owner, falsifying his name, asking for beer to the amount of a mark a day, borrowing from his landlady ten marks, paying nothing, but remaining on friendly terms with the landlady and her women lodgers, making a contract with a superintendent ostensibly for his estate, and borrowing money from him.
S. claimed to be a landowner in T——, using a fake name, requesting beer worth a mark a day, borrowing ten marks from his landlady without repaying her, yet staying on good terms with her and the other female tenants. He made a deal with a superintendent under the pretense of managing his estate and borrowed money from him as well.
Observed in the clinic, he said he was a bank representative and had been very nervous since being divorced in 1911. The divorce was due to his wife’s adultery. Sometimes he would not know really what he was doing, once even tried to shoot himself, and again once threw a burning lamp into his wife’s face without knowing it.
Observed in the clinic, he said he was a bank representative and had been very nervous since getting divorced in 1911. The divorce happened because of his wife's infidelity. Sometimes he wouldn’t really know what he was doing; he even once tried to shoot himself and another time threw a burning lamp in his wife's face without even realizing it.
He had gone to the City of T—— without furlough in October because others used to, too. Only five days later had he noticed that his troop was no longer there; and upon inquiring about the troop he could find nothing as to its whereabouts.
He went to the City of T—— without permission in October because others did too. Just five days later, he realized that his troop was gone; and when he asked about the troop, he couldn't find out where they were.
He had been a heavy drinker and was always somewhat intoxicated, which, according to the patient, made him forget everything. He had drunk 20 glasses of beer and liquor daily. He wrote to P. because he knew his father.
He used to drink a lot and was often a bit drunk, which, according to him, made him forget everything. He consumed 20 drinks of beer and liquor every day. He wrote to P. because he knew his father.
As for the frauds, he said he knew nothing about them. He did not know even the baker from whom he had gotten the cakes. In fact, he had been drunk the whole day long.
As for the frauds, he said he knew nothing about them. He didn't even know the baker from whom he had gotten the cakes. In fact, he had been drunk the whole day long.
He said that he had learned badly in school and had not passed any examinations. In active service he had already been convicted of drunkenness once. Referring to his treatment by injections, he said he would rather be dead. He had only sought diversion in looking over estates. Both his ability to reckon and his memory had suffered greatly. He and another patient eloped from the clinic one day but were captured a few hours later.
He said he hadn’t done well in school and hadn’t passed any exams. While in active service, he had already been convicted of drunkenness once. Regarding his treatment with injections, he said he would rather be dead. He had only sought escape by looking at properties. Both his math skills and memory had taken a big hit. He and another patient ran away from the clinic one day but were caught a few hours later.
Remarks: Details are lacking as to the physical and laboratory side of this case. On the whole, there appeared to be no convincing features of paresis or cerebrospinal syphilis. The phenomena are very possibly in part alcoholic. There appeared to be no sensory disorders, and in particular no hallucinations. The intellectual disorder is chiefly amnestic. There is little or no evidence of emotional abnormality. The curious conduct seems hardly to indicate a primary disorder of will. The main feature psychologically appears to be amnesia coupled with an inability to reckon. To be sure, the letters are written externally in sufficiently good form; the amnesia does not appear to extend to details. It is a question of whether the disorientation which one suspects is not merely amnestic. On the whole, however, it would appear that there must have been at various times disorder of consciousness, as indeed is indicated by the patient’s own account of his ignorance of the cake-roebuck episode.
Remarks: There are some details missing about the physical and lab aspects of this case. Overall, there didn't seem to be any convincing signs of paresis or cerebrospinal syphilis. The symptoms might partly be related to alcohol use. There appeared to be no sensory issues, particularly no hallucinations. The main intellectual problem seems to be amnesia. There’s little to no evidence of emotional abnormalities. The odd behavior doesn’t seem to suggest a primary issue with willpower. Psychologically, the main feature appears to be amnesia along with difficulty in calculating. The letters are written well enough; the amnesia doesn’t seem to affect the details. It raises the question of whether the disorientation suspected is just amnesia. Overall, it seems likely that there were times of disorder in consciousness, as suggested by the patient’s own account of not remembering the cake-roebuck incident.
Dismissing the hypothesis of a syphilitic dementia, we might cling to that of alcoholic dementia more or less punctuated by acute alcoholism. Yet it is also possible that the patient was actually somewhat feeble-minded; this would be consistent with his own statement. The question might arise whether this soldier could have been excluded by careful psychiatric examination before entering service. It would seem that a knowledge of the insanity of the mother and grandmother, and an inspection of school records, if available,—to say nothing of the episodes which may or may not have been accurately related, between himself and his afterwards divorced wife—would have sufficed to throw doubt upon the military effectiveness of this man. We know also that he had already been convicted of drunkenness on military service before the episodes mentioned.
Setting aside the idea of syphilitic dementia, we might consider the possibility of alcoholic dementia, possibly interrupted by episodes of acute alcoholism. However, it's also possible that the patient was a bit intellectually challenged; this aligns with his own comments. One might wonder if this soldier could have been flagged by a thorough psychiatric evaluation before joining the service. It seems that knowledge of his mother's and grandmother's mental health issues, along with a review of school records, if available—not to mention the incidents that may or may not have been accurately described between him and his eventually divorced wife—would have been enough to raise concerns about his military capability. We also know that he had previously been convicted of drunkenness while on military duty before the incidents mentioned.
Desertion by alcoholic. Contributory factors.
Desertion by alcoholic. Contributing factors.
Case 92. (Kastan, January, 1916.)
Carl B. was a soldier about whom the captain thought that his intellectual power had been weakened by drink. An inquiry after arrest showed that he had been odd also at home. He had once been sued for perjury, but the suit had been stopped for lack of evidence. He had been several times convicted of drunkenness. It appears that on March 30, 1915, after mounting guard, he said nothing and went home, remaining at home until the next day and then returned to the guardhouse in the street-car. He declared, this time, that the non-commissioned officer had given him permission to leave, although this statement was not correct.
Carl B. was a soldier whom the captain believed had his mental sharpness dulled by alcohol. An investigation after his arrest revealed that he had also been unusual at home. He had once been sued for perjury, but the case was dropped due to insufficient evidence. He had been convicted of drunkenness several times. It turns out that on March 30, 1915, after completing his guard duty, he didn't say a word and went home, staying there until the next day before taking the streetcar back to the guardhouse. He claimed that the sergeant had allowed him to leave, but that statement was false.
Again, on April 6, B. was about to leave the quarters, but the surgeon, finding him drunk, kept him back. He did not go home that night, and the next day when he was wanted at the hearing, he could be found only in the afternoon. He replied confusedly and somewhat irrelevantly to the questions asked. On arrival at the clinic he was in tears and much depressed. Given 50 grams of alcohol, he became somewhat livelier. Upon examination, his perceptions were found diminished; he felt, he stated, a cracking and crackling in his neck. In his cell he had felt as if sparrows were roosting in his face; he had heard voices and seen pictures, and had not known what he was doing. He asserted his innocence, blaming his imprisonment for all his troubles. He had been in the habit of drinking three liqueurs and two glasses of beer a day. He had been drawing a pension since a fall from a scaffold.
Again, on April 6, B. was about to leave the quarters, but the surgeon, finding him drunk, stopped him. He didn’t go home that night, and the next day when they needed him for the hearing, he could only be found in the afternoon. He answered the questions in a confused and somewhat off-topic manner. When he arrived at the clinic, he was in tears and feeling very down. After given 50 grams of alcohol, he perked up a bit. Upon examination, his perceptions were found to be diminished; he stated he felt a cracking and crackling in his neck. In his cell, he had felt like sparrows were roosting on his face; he had heard voices and seen images and didn't know what he was doing. He claimed he was innocent, blaming his imprisonment for all his issues. He had been drinking three liqueurs and two glasses of beer a day. He had been receiving a pension since he fell from a scaffold.
A sister had suffered from continual headaches. The patient himself had three sickly children and ten of his children were dead; there were also two premature births.
A sister had been dealing with constant headaches. The patient himself had three unhealthy kids, and ten of his children had died; there were also two miscarriages.
The analysis of this case would clearly show the benefit of considering, first, the hypothesis of syphilis. Not only is the history of his children suggestive, but the impairment of mind noted by the captain as due to alcohol may very possibly be syphilitic in origin.[125] Examples in division he could not solve, and it is a question whether his leaving guardmount is not in part related to disorientation for time. There appears to be no evidence of feeblemindedness and none of epilepsy (though a sister suffered from continual headaches). Alcohol may account possibly for the entire picture and is particularly consistent with the false voices and figures, the sparrows in the face, and the sensations in neck and the tickling in the ears. It is possible, also, that intolerance to alcohol had set in since the fall from the scaffolding for which a pension was being received. It does not appear necessary to consider any further of the groups of mental disease. Syphilis, alcohol, and a post-traumatic brain condition, all may play a part. Alcohol is able probably by itself to produce a number of these symptoms, and these alcoholic symptoms would be probably the more readily produced in virtue of the post-traumatic intolerance that we may assume.
The analysis of this case clearly shows the benefit of considering, first, the possibility of syphilis. Not only is the history of his children suggestive, but the mental impairment noted by the captain, which he attributed to alcohol, could very well be due to syphilis. [125] He struggled with problems in division, and it's questionable whether his leaving guardmount is partly related to confusion about time. There doesn’t seem to be any evidence of intellectual disability or epilepsy (although his sister suffered from chronic headaches). It's possible that alcohol accounts for the whole situation, which aligns particularly with the false voices and figures, the sparrows appearing in his vision, and the sensations in his neck and the tickling in his ears. It's also possible that he developed an intolerance to alcohol after his fall from the scaffolding for which he was receiving a pension. It doesn't seem necessary to consider any other groups of mental disorders. Syphilis, alcohol, and a post-traumatic brain condition could all be contributing factors. Alcohol alone might be able to produce several of these symptoms, and these alcohol-related symptoms would likely be exacerbated by the post-traumatic intolerance that we can assume.
A disciplinary case: Alcoholism.
A disciplinary case: Alcohol use disorder.
Case 93. (Kastan, January, 1916.)
A German soldier, brought up for examination for disobedience and insubordination with intoxication, was found already to have been convicted 33 times of a variety of crimes. Once he had drunk a bottle of shoemaker’s polish, evidently with suicidal intent.
A German soldier, summoned for a hearing due to disobedience and insubordination while drunk, was discovered to have already been convicted 33 times for various crimes. At one point, he had consumed a bottle of shoemaker’s polish, clearly with the intent to harm himself.
In the canteen he had assaulted superior officers and tried to strike a sergeant. He said he had been attacked by the sergeant and pushed into a cell, whereupon he had lost his mind.
In the cafeteria, he had attacked higher-ranking officers and attempted to hit a sergeant. He claimed he had been assaulted by the sergeant and shoved into a cell, which made him lose his mind.
He came from a family of drunkards, and had been himself very alcoholic formerly. On the day in question, however, he had drunk very little. According to his account, he had fits of this sort if any one injured him. He was amnestic and had forgotten his previous convictions. Anything he might have done, he said, had happened a long time ago, in his youth. For example, concerning a theft, he said that it was merely that he had fallen into some Christmas trees and stuck fast there, and no one wanted to be paid. Tremors of hands, feet, head. Analgesia of thorax.
He came from a family of heavy drinkers and had struggled with alcoholism himself in the past. However, on that particular day, he hadn’t consumed much alcohol. According to him, he would have episodes like this if anyone wronged him. He couldn’t remember his past convictions. Anything he might have done, he claimed, happened a long time ago, in his youth. For instance, regarding a theft, he said it was just that he’d gotten caught in some Christmas trees and couldn’t get out, and no one wanted to be compensated. He exhibited tremors in his hands, feet, and head. There was also a lack of feeling in his chest.
Re alcoholism and disciplinary cases, we find alcoholism bulking large in Lépine’s account of military delinquency. Fugue subjects are not infrequently alcoholic. Minor disobedience is also often alcoholic. Acts of violence are characteristically alcoholic, or executed by subjects with hereditary alcoholic taint. (Such acts were in France especially common before the anti-absinthe law in 1915.) Alcoholic episodes and impulses often culminate in arson. No doubt, espionage employs alcoholism for a portion of its technique, though delusional mystics and subnormal hypersuggestibles are more often the purveyors of information to the enemy. The theft list, also, shows its share of alcoholics. Alcoholics are less common amongst those who, contrary to rules, assume shoulder-straps or other decorations. Here the sub-normals and victims of imbalance, as well as the drug cases, are more likely to figure if the matter is psychiatric at all.
Re alcoholism and disciplinary cases, we see that alcoholism plays a significant role in Lépine’s account of military misconduct. People experiencing fugue states are often alcoholic. Minor acts of disobedience frequently stem from alcoholism as well. Acts of violence are typically driven by alcoholism or carried out by individuals with a hereditary predisposition to alcoholism. (These acts were particularly prevalent in France before the anti-absinthe law was enacted in 1915.) Episodes of alcohol use and impulses often lead to arson. It's likely that espionage uses alcoholism as part of its strategy, although delusional mystics and individuals who are easily influenced are more often the ones providing information to the enemy. The theft records also indicate a number of alcoholics. Alcoholics are less common among those who, in violation of rules, take on shoulder straps or other decorations. In these cases, individuals with subnormal intelligence and those suffering from imbalances, as well as drug users, are more likely to be involved if the situation pertains to psychiatry at all.
Remarks upon an atrocity.
Comments on a tragedy.
Case 94. (Kastan, January, 1916.)
April 15, 1915, a German soldier went with three comrades to a farm, to select a sheep for slaughter; they were obliged to go to three farms. The man carried a revolver and cartridges in his pocket. He threatened the farmer that he met with this revolver, and desired to rape the farmer’s daughter. He was very drunk, and said to the non-commissioned officer who was called in at the time, “You have served only a year longer than I have.” He staggered, struck violently with his hand at the sergeant, and gave insolent replies.
April 15, 1915, a German soldier went with three friends to a farm to pick out a sheep for slaughter; they had to visit three farms. The man had a revolver and ammo in his pocket. He threatened the farmer he encountered with this revolver and tried to assault the farmer’s daughter. He was really drunk and told the non-commissioned officer who was called in at the time, “You’ve served only a year longer than I have.” He stumbled, violently swung his hand at the sergeant, and gave disrespectful answers.
He had already choked the peasant’s daughter, scratched her face, and bitten her fingers, hand and arm. She could not run away as she was lame. The soldier held the revolver to her face and shot it off several times, offered sex assault, scratched her feet with his spurs, and tried to twist her neck. The non-commissioned officer threatened to shoot him, and he then became still. He said to the first-lieutenant before whom he was taken, that he would do anything but allow himself to be beaten, and at this moment moved his arms about in the air, and bloody foam came from his mouth. The first-lieutenant previously had always thought him to be normal except for a strange flicker and unrest of the eyes. There was a history that he had already once attacked a servant girl. The man had amnesia for the affair, only remembering how the non-commissioned officer had come on a white horse. He remembered nothing about the peasant and the girl. He said that he had been given to earache on the right side in winter. There was a history of his having fallen from a tree in childhood, becoming unconscious. He had been a sufficiently good scholar up to the second class in school. He had been an excellent soldier.
He had already choked the peasant’s daughter, scratched her face, and bitten her fingers, hand, and arm. She couldn’t run away because she was lame. The soldier held the revolver to her face and fired it several times, attempted sexual assault, scraped her feet with his spurs, and tried to twist her neck. The non-commissioned officer threatened to shoot him, and he then stopped moving. He told the first lieutenant, to whom he was brought, that he would do anything but let himself be beaten, and at that moment, he flailed his arms in the air, and bloody foam came from his mouth. The first lieutenant had always thought he was normal except for a strange flicker and unrest in his eyes. There was a record that he had once attacked a servant girl. The man had amnesia about the incident, only recalling that the non-commissioned officer had arrived on a white horse. He remembered nothing about the peasant or the girl. He said he had suffered from earache on the right side in winter. There was a history of him falling from a tree during childhood and becoming unconscious. He had been a decent student up to the second grade in school. He had been an excellent soldier.
Alcoholism: Atrocity.
Alcoholism: A tragedy.
Case 95. (Kastan, January, 1916.)
September 15, 1914, a German soldier was missed. He had said that he wanted to get to the enemy quickly, and that he was going to march alone against the Russians. A shot was fired that night by this soldier, on the ground that he had been insulted by a civilian, although no civilian was present.
September 15, 1914, a German soldier went missing. He had stated that he wanted to reach the enemy quickly and that he was going to march alone against the Russians. That night, this soldier fired a shot, claiming he had been insulted by a civilian, even though no civilian was around.
September 21, a farmer in a wagon reached a farm, where he found the soldier aiming at a woman. He fired, wounded the woman severely, and jumped on the farmer’s wagon and rode off with him. It seems that the soldier had come to the farm at noontime and accused the woman of treachery, ordering her to come with her husband to a certain farmhouse, where she should be placed against the wall and be shot. The soldier had shot her and wounded her husband also. According to the woman, the idea was to take revenge because she had denounced certain persons as spies.
On September 21, a farmer in a wagon arrived at a farm, where he saw a soldier aiming at a woman. The soldier fired, seriously injuring the woman, then jumped onto the farmer’s wagon and rode off with him. It appears the soldier had come to the farm at noon, accusing the woman of betrayal and demanding that she go with her husband to a specific farmhouse, where she would be lined up against the wall and shot. The soldier had shot her and also injured her husband. According to the woman, the motive was revenge because she had reported certain individuals as spies.
He was arrested during the night, and told how he had left his troop because he could not get at the enemy. He had been informed that there were spies who ought to be shot; there had been talk in a certain inn about it. He did not know he had wounded the husband, and he only wanted to give that dangerous woman a piece of his mind.
He was arrested at night and explained that he had left his group because he couldn’t reach the enemy. He had heard there were spies who should be executed; it had been discussed at a certain bar. He didn’t realize he had injured the husband, and he just wanted to confront that dangerous woman.
After wounding the woman, he had given himself no further thought about her, but had gone to partake of the holy sacrament at the pastor’s. He then had drunk another glass of beer and gone to bed. He was, in fact, still drunk at the time of arrest. He had not been aware that he would be punished for the crime of going alone against the Russians.
After injuring the woman, he didn’t think about her anymore and just went to take part in the holy sacrament at the pastor’s. He then had another glass of beer and went to bed. He was still drunk when he was arrested. He hadn't realized that he would be punished for acting alone against the Russians.
Some days later, he wrote that he did not intend to kill the woman, that he had been drunk at the time and was always a bad man when drunk; that he had other times when he absented himself from home for days when drunk. He had had, he said, a number of attacks of delirium, in which he had seen animals. At one time, he had fallen on his head. On the day in question, he had drunk 1½ litres of liquor. He was remorseful for his deed.
Some days later, he wrote that he didn't mean to kill the woman, that he had been drunk at the time and always acted badly when he was drinking. He mentioned having nights where he disappeared from home for days while drunk. He said he had experienced several bouts of delirium, during which he hallucinated animals. At one point, he had fallen and hit his head. On the day in question, he had consumed 1½ liters of alcohol. He felt regret for what he had done.
A disciplinary case: Alcoholism; amnesia.
A disciplinary case: Alcoholism; memory loss.
Case 96. (Kastan, January, 1916.)
A German soldier, New Year’s Eve, 1915, got away from his company, drank whiskey, and came back drunk. He bothered his comrades so that the non-commissioned officer had to call for help; whereupon the soldier said, “A man who comes on late and hasn’t been in much, hasn’t much to say. If it is a non-commissioned officer, I shall hit him in the snout.” The officer kept talking to him kindly but he cried “Halt’s Maul, you crooked …!” He staggered up to the lieutenant without saluting, but at a slight push fell prone into the straw.
A German soldier, New Year’s Eve, 1915, slipped away from his company, drank whiskey, and returned drunk. He irritated his fellow soldiers so much that the sergeant had to call for backup; then the soldier said, “Someone who shows up late and hasn’t done much doesn’t have much to say. If it’s a sergeant, I’ll punch him in the face.” The officer kept speaking to him nicely, but he shouted, “Halt’s Maul, you crooked …!” He stumbled up to the lieutenant without saluting, but a little shove made him fall flat into the straw.
It transpired that the man had not been intoxicated enough to lose all control of himself. He did not remember anything about what he had done; he had drunk a half-bottle of rum during the evening. There was a demonstrable lack of memory. He did not know the German provinces, and thought that Bismarck had once been war minister. There was a tremor, hypalgesia of the left leg and analgesia of the left arm and left shoulder.
It turned out that the man wasn't drunk enough to completely lose control. He couldn’t recall anything about what he had done; he had consumed half a bottle of rum that evening. His memory was clearly impaired. He didn't know the German provinces and believed that Bismarck had once been the war minister. He was shaking, experiencing reduced sensitivity in his left leg, and numbness in his left arm and shoulder.
It was found that he came from a strongly tainted family, with two insane sisters and three insane cousins. He had been a good soldier during his service, but had accused his father of alcoholism baselessly. He had always been difficult to manage when drunk and had been convicted nine times: five for dangerous assault and battery. He drank up to 1⅓ litres of whiskey a day if he got time, and also took ether. For some ten years he had been amnestic for what he did while drunk; nor, according to his wife, had he been able recently to stand so much alcohol. He said that he had had a fall from a wagon in 1911 or ’12, after which he had been unconscious.
He came from a seriously troubled family, with two sisters and three cousins who were all mentally ill. He had been a decent soldier during his service but had falsely accused his father of being an alcoholic. He had always been hard to handle when drunk and had a total of nine convictions: five for violent assault and battery. He could drink up to 1⅓ liters of whiskey a day if given the chance, and he also used ether. For about ten years, he had no memory of what he did while drunk; according to his wife, he also couldn't handle as much alcohol lately. He mentioned that he had fallen off a wagon in 1911 or ’12 and had been unconscious afterward.
Antebellum, run over by an automobile; intolerance of alcohol; episodes of amnesia after moderate alcohol.
Antebellum, hit by a car; intolerance to alcohol; episodes of memory loss after moderate drinking.
Case 97. (Kastan, January, 1916.)
A German soldier was advanced in rank February 26, 1915, and in honor thereof drank six or seven glasses of beer. On his way home, he met a captain and failed to salute him. When called to account, he said he could not see, and made remarks about regrettable behavior. He refused to go along with the officer. Afterwards he remembered that he had been stopped by an officer but had forgotten subsequent happenings.
A German soldier got promoted on February 26, 1915, and to celebrate, he drank six or seven glasses of beer. On his way home, he ran into a captain and didn't salute him. When questioned about it, he claimed he couldn’t see and made comments about his regrettable behavior. He refused to comply with the officer. Later, he recalled that he had been stopped by an officer but had forgotten what happened next.
March 24, he was riding in an electric car with a lieutenant. He said to the lieutenant who had unbuckled his sabre, “It is a piece of insolence and improper to unbuckle the sabre.” He repeated the phrase on questioning. He was then asked to give his name, and replied, “I know my name but what is your name, Mr. Lieutenant?” He looked drunk at the time but afterwards remembered nothing.
March 24, he was riding in an electric car with a lieutenant. He said to the lieutenant, who had unbuckled his saber, "It's disrespectful and inappropriate to unbuckle the saber." He repeated this when asked about it. He was then prompted to give his name and replied, "I know my name, but what’s your name, Mr. Lieutenant?" He appeared drunk at the time but later didn’t remember anything.
Physically he was tremulous and showed blepharospasm. His face grew red on bending over.
Physically, he was shaky and had muscle spasms around his eyes. His face turned red when he bent over.
This man had been run over by an automobile in 1910, after which he had become excitable, slow-thinking and forgetful. The spinous processes were painful on pressure, as was also the hip joint. The history showed that he had been convicted six times of various crimes, such as disturbing the peace, embezzlement, and the like. Since this accident he had not been able to work effectively. He had gone into the army in a spirit of enthusiasm.
This man was hit by a car in 1910, after which he became easily agitated, slow to think, and forgetful. There was pain in his spine when pressed, and his hip joint also hurt. His history revealed that he had been convicted six times for various offenses, including disturbing the peace and embezzlement. Since the accident, he had not been able to work effectively. He had joined the army with a sense of enthusiasm.
Adventure with a stranger in Paris.
Adventure with a stranger in Paris.
Case 98. (Briand and Haury, 1916.)
A soldier had seven days’ leave in Paris, beginning December 27, 1915, and the first day drank a good deal of wine with another man on leave. They met, in some place that the patient had forgotten, a well-dressed man whom they did not know, and all three fell to drinking. The stranger told them he knew a trick to prolong the leave to 3 or 4 weeks. “All I have got to do is to prick you, and it will cost only 100 sous.” The operation was done at the café after payment in advance. The operation was a puncture with a needle between the middle and ring fingers of the left hand. Next day there was a phlegmon of the dorsal surface of the hand, and he was put into hospital saying that he had gotten a barbed wire prick in the trenches. The surgeon who opened the phlegmon was surprised at its gummy appearance, gangrenous odor, and greenish tint. In point of fact, petrol had been injected.
A soldier had a week off in Paris, starting December 27, 1915, and on the first day, he drank quite a bit of wine with another soldier on leave. They ran into a well-dressed man they didn't know in a place the soldier couldn’t remember, and all three ended up drinking together. The stranger claimed he knew a way to extend the leave by 3 or 4 weeks. “All I have to do is prick you, and it will only cost 100 sous.” The procedure was done at the café after they paid upfront. The procedure involved puncturing the skin with a needle between the middle and ring fingers of the left hand. The next day, he developed an infection on the back of his hand and was taken to the hospital, claiming he had been pricked by barbed wire in the trenches. The surgeon who examined the infection was surprised by its sticky look, foul smell, and greenish color. In reality, petrol had been injected.
Morphinism: Tetanus.
Morphinism: Tetanus.
Case 99. (Briand, 1914.)
Mdm. L. was a morphinist. After the outbreak of the war, she went to a general hospital to recover from morphinism, but was too excited to be kept there. Accordingly, she had to be sent to Sainte-Anne, but upon arrival she developed distinct signs of tetanus.
Mdm. L. was addicted to morphine. After the war started, she went to a general hospital to get treatment for her addiction, but she was too agitated to stay there. As a result, she was sent to Sainte-Anne, but when she arrived, she showed clear signs of tetanus.
It seems that Mdm. L. was the widow of a Colonial who had given her the first injections ten years before, for dysentery. She tried several times to stop. Daily dose 1.5 grams.
It looks like Mdm. L. was the widow of a Colonial who had given her the first injections ten years earlier for dysentery. She attempted to stop multiple times. Daily dose: 1.5 grams.
She was in a cachectic state, and according to her mother, took no care of her syringe, trailing it about everywhere. Her thighs, arms, and anterior aspect of the body were covered with scars. There were small phlegmons in places. Did she inoculate herself with bacillus tetani from an infected needle? In any case, she died of tetanus.
She was in very poor health, and her mother said she didn’t take care of her syringe, leaving it lying around everywhere. Her thighs, arms, and front of her body were covered in scars. There were small abscesses in some areas. Did she infect herself with tetanus bacteria from a dirty needle? In any case, she died of tetanus.
Medicolegal question concerning a morphinist.
Medicolegal question about a morphine addict.
Case 100. (Briand, 1914.)
A man worked in Paris on the ’Change, where there are a number of syringe victims. He had been brought up in Paris but was not a Frenchman. Enthused by his friends and the prey of deep emotion, he enlisted. He was of an introspective nature and himself wondered whether the morphine did not have something to do with his enlisting. He said, “I had been unnerved for a number of days by reading the papers, and after a number of heavy injections, I went to a recruiting station and signed on.” In his regiment, he continued the injections, but shortly found that he would be unable to replenish his diminishing stock of drug. He explained his unhappy fate to the corps physician, and was sent to Val-de-Grâce. He asked to be retired, alleging that he was under the influence of a poison when he went to the recruiting office and had therefore committed an illegal act.
A man worked in Paris at the stock exchange, where there were many victims of drug addiction. He grew up in Paris but wasn't a French citizen. Inspired by his friends and overwhelmed by strong emotions, he enlisted. He was introspective and wondered if the morphine played a role in his decision to join. He said, “I had been agitated for several days from reading the news, and after a few intense injections, I went to a recruiting station and signed up.” In his regiment, he continued using the drug but soon realized he would not be able to restock his dwindling supply. He explained his unfortunate situation to the corps physician and was sent to Val-de-Grâce. He requested to be discharged, claiming that he was under the influence of a drug when he went to the recruiting office and had therefore acted unlawfully.
Cases 101 and 102. (Briand, 1914.)
Fernand and Emilienne were two recidivists in morphinism. Although neither was over 22 years of age, both had been several times convicted of shop-lifting. They stole only if they had no money for morphine. Prostitution served to care for Emilienne, while Fernand was at times a cocaine seller, and at times made money in devious ways at Montmartre. Emilienne’s patronage scattered with the war, and it was the same with Fernand’s. Accordingly, there was no money for either morphine or cocaine. Moreover, the shops being not crowded were easier to watch. As Emilienne did not care to be arrested and sent off as an undesirable, she presented herself at the hospital for the insane at Sainte-Anne. Fernand shortly joined her there.
Fernand and Emilienne were two repeat offenders struggling with addiction to morphine. Even though they were both under 22, they had been convicted multiple times for shoplifting. They only stole when they didn't have money for morphine. Emilienne relied on prostitution to support herself, while Fernand occasionally sold cocaine and sometimes found other shady ways to make money in Montmartre. Emilienne's clients dried up during the war, and the same happened for Fernand. As a result, neither of them had money for morphine or cocaine. Furthermore, with the shops being less crowded, it was easier for them to be watched. Since Emilienne didn't want to be arrested and labeled as undesirable, she admitted herself to the mental hospital at Sainte-Anne. Fernand soon followed her there.
V. ENCEPHALOPSYCHOSES
(THE FOCAL BRAIN DISEASE GROUP.)
Left-sided hemiplegia and aphasia: Contrecoup and local lesions.
Left-sided hemiplegia and aphasia: Contrecoup and local lesions.
Case 103. (Lhermitte, June, 1916.)
A soldier of 23 was wounded in the left parietal region and showed a left-sided hemiplegia with aphasia. The speech difficulty, although very marked, retrograded almost completely, but the hemiplegia remained severe. This hemiplegia was a spastic one, of a classical nature, with Babinski sign and exaggeration of tendon reflexes. Lhermitte thinks that the left hemisphere was directly affected by the contusion, as in point of fact there was an actual loss of bony tissue, but that it would not be necessary to suppose the ipsilateral hemiplegia was due to an absence of pyramidal decussation. The transient aphasia was probably due to direct affection of the tissues on the left side of the brain; the permanent hemiplegia was doubtless due to a lesion of the opposite hemisphere produced by contrecoup. It appears that sometimes a surgeon may be led to superfluous surgical intervention in a case of such paradoxical hemiplegia, since the surgeon may believe that a bullet or shell fragment has traversed the brain substance to the opposite side of the skull, when as a matter of fact the brain parts have been injured merely by contrecoup.
A 23-year-old soldier was injured in the left side of his head and experienced left-sided paralysis along with speech difficulties. Although his speech problems were quite severe, they almost completely recovered, but the paralysis stayed serious. This paralysis was spastic, showing classic symptoms like the Babinski sign and heightened tendon reflexes. Lhermitte believes the left side of the brain was directly damaged by the impact, as there was actual loss of bone tissue, but it's not necessary to think that the paralysis on the same side was caused by a lack of pyramidal crossing. The temporary speech issues were likely caused by direct damage to the tissues on the left side of the brain; the lasting paralysis was probably due to an injury on the opposite side of the brain caused by the force of the impact. It seems that sometimes a surgeon might feel compelled to perform unnecessary surgery in cases of such unusual paralysis, as they might think that a bullet or shell fragment has gone through the brain to the other side of the skull, when in reality, the brain has only been injured by the impact.
Re such amnesia, it is of note that many head cases, even if they do not show amnesia, show a conspicuous euphoria and lack of understanding of the seriousness of the injury in question and of the necessary treatment. According to E. Meyer, there are constantly to be found in head cases disturbances of perception and lack of coördination (especially for time), perseveration, difficulty in thinking and calculating.
Regarding such memory loss, it's important to mention that many head injury patients, even if they don't exhibit memory loss, display a noticeable sense of euphoria and an inability to grasp the seriousness of their injury and the treatment needed. According to E. Meyer, patients with head injuries often experience disruptions in perception and lack of coordination (especially regarding time), repetition of thoughts, and difficulties with thinking and calculations.
Chart 5
COMMOTIO CEREBRI
| I. | Senses: Asymmetrical hyp- or anesthesia (with hyperalgesia and osseous hyperesthesia). |
| II. | Movement: Disorder, muscular or reflex. General or unilateral hyperexcitability. |
| III. | Vascular Control: Dermatographia. Cardiac, splanchnic disorder; also, Headaches, Vertigo. |
| IV. | Feelings: Disorder. |
| V. | Idea Intake: Disorder. Persistent lacunae of memory. |
| VI. | Smarts: Disorder of recollective memory. Speech-disorder. Intellectual inertia. Overimagination (hallucinations, tremors). |
Mairet, Piéron, Bouzansky.
Mairet, Piéron, Bouzansky.
Gunshot wound of head; alcoholism: Amnesia.
Gunshot wound to the head; alcoholism: Memory loss.
Case 104. (Kastan, January, 1916.)
A German soldier had a bullet pass through his right eye and lower jaw, leaving a fistulous opening from the mouth. He said that he was completely blind, but ophthalmological examination cast doubt upon the blindness. There had been immediately after the injury a number of severe attacks of dizziness, which lasted several hours; and another attack developed after he had come back from hospital, to which he had gone by reason of his pains.
A German soldier had a bullet go through his right eye and lower jaw, creating an open wound in his mouth. He claimed that he was completely blind, but an eye exam raised questions about that blindness. Right after the injury, he experienced several severe bouts of dizziness that lasted for hours; another episode occurred after he returned from the hospital, where he had gone because of his pain.
He was to be arrested on account of a disciplinary crime and had ostensibly gone to his mother’s house, there to await arrest. The non-commissioned officer found him in a saloon. As soon as the phrase, “You are my prisoner!” was said, the soldier lost track of his surroundings. He had drunk a few glasses of beer but did not himself think he was drunk at the time. He was insulting and violent when asked to proceed with the officer, and a policeman was called in to take charge. He then lay down in the street and had to be put upon a wagon, still firing abusive phrases at his captors.
He was supposed to be arrested for a disciplinary offense and had supposedly gone to his mom's house to wait for the arrest. The non-commissioned officer found him in a bar. As soon as the officer said, "You are my prisoner!", the soldier lost touch with reality. He had downed a few beers but didn't think he was drunk at that moment. He was belligerent and violent when asked to go with the officer, so a policeman was called to take control. He then lay down in the street and had to be put onto a wagon, still hurling insults at his captors.
Upon examination, aside from the effects of the gunshot, excessive knee-jerks and tremors of the body were found. The eyebrows met but there was no other sign of bodily stigmata. There seems to have been no hereditary disease, or any history of severe alcoholism, though the man had been convicted previously of violence and theft. The amnesia is to be ascribed to effects of the head injury.
Upon examination, aside from the effects of the gunshot, excessive knee-jerks and body tremors were observed. The eyebrows were furrowed, but there were no other signs of physical trauma. There appeared to be no hereditary disease or any history of severe alcoholism, although the man had been previously convicted of violence and theft. The amnesia can be attributed to the effects of the head injury.
Bullet in brain: Crises; cortical blindness; vertigo; hallucinations.
Bullet in brain: Crises; total vision loss; dizziness; hallucinations.
Case 105. (Lereboullet and Mouzon, July, 1917.)
An invalided soldier, 40, was sent to be observed, Oct. 23, 1916, because he wanted his pension renewed. He had been retired a year before for diminution of binocular vision with impaired perspective of objects in the right half of the visual field. He had now become completely blind.
An injured soldier, 40, was sent for evaluation on October 23, 1916, because he wanted to renew his pension. He had been retired a year earlier due to reduced binocular vision and impaired depth perception for objects in the right side of his visual field. He had now become completely blind.
He had been wounded, March 12, 1915, in the Argonne, without losing consciousness. He was wounded at ten o’clock at night and waited until the next day to walk to the ambulance and was at this time able to see perfectly. Arriving at the ambulance he lost consciousness. He was trephined but remembers nothing about the trephining.
He got injured on March 12, 1915, in the Argonne, but didn’t pass out. He was hurt at ten o’clock at night and waited until the next day to walk to the ambulance, and by that time, he could see perfectly. When he got to the ambulance, he lost consciousness. They performed a trephination on him, but he doesn’t remember anything about the procedure.
His memory grew better from his arrival at a hospital in the rear in April. An attempt was made to remove the bullet in May, 1915. Though the surgeon’s finger was pushed as far as the tentorium the patient did not lose consciousness or sight, but on leaving the operating room he fainted and, after a few days of restlessness and delirium, he became completely blind. There was a cerebral hernia difficult to reduce. Vision became a little better and light and persons could be distinguished at the time when he was retired. A month after the operation there was a convulsive crisis beginning in the left arm, affecting the legs and ending in unconsciousness. Several similar crises occurred in August, sometimes with and sometimes without loss of consciousness. Later these crises began to be limited to the left side and then to be ushered in by visual hallucinations. At home he was unable to care for, clothe or feed himself. The crises became more frequent. The visual hallucinations began to dominate.
His memory started to improve after he was taken to a hospital in the rear in April. They tried to remove the bullet in May 1915. Even though the surgeon's finger went as far as the tentorium, the patient didn't lose consciousness or his sight. However, after leaving the operating room, he fainted, and after several days of restlessness and delirium, he became totally blind. There was a cerebral hernia that was hard to treat. His vision got a bit better, and he could tell light and people apart when he was discharged. A month after the operation, he had a seizure that started in his left arm, affected his legs, and ended with him losing consciousness. He had several similar seizures in August, sometimes with and sometimes without loss of consciousness. Eventually, these seizures were confined to the left side and started being triggered by visual hallucinations. At home, he couldn't take care of himself, dress, or feed himself. The seizures became more frequent, and the visual hallucinations began to take over.
This situation lasted to February, 1916, when the blindness which had been increasing since the onset of the hallucinations became complete. The crises now became less frequent and intense. Headaches not severe were exaggerated after seizures. The patient acted like a totally blind[137] person and said that he had before him a uniform and constant gray without any light or dark spots or any color. Upon this background bizarre pictures, caricatures, disguised persons, animals or nameless things appeared colorless without relief, in silhouette, but highly suggestive of reality to such a degree that at first, according to the patient, he had made gestures to reach, or push aside these pictures. The crises were Jacksonian.
This situation continued until February 1916, when the blindness that had been increasing since the onset of the hallucinations became complete. The episodes then became less frequent and intense. Mild headaches were worsened after seizures. The patient behaved like someone who was completely blind[137] and described seeing a uniform and constant gray with no light, dark spots, or any color. Against this backdrop, bizarre images, caricatures, disguised figures, animals, or unrecognizable things appeared colorless, in silhouette, yet incredibly lifelike to the point that initially, the patient claimed he would gesture as if to reach for or push away these images. The episodes were Jacksonian.
Pallor, perspiration, shivering, irresponsiveness, clonic spasms of left arm followed. The patient always had a premonition permitting him to get into bed if he was sitting, for example, in his chair. Sometimes there was a dizzy sensation as if the body were being rotated to the left. This sensation did not occur at the beginning of the seizure and the patient fought against it, turning to the right. Sometimes he felt as if he were sliding at great speed down an inclined plane. Headaches and sleepiness followed, but there was never any complete loss of consciousness of memory.
Pallor, sweating, shivering, unresponsiveness, and clonic spasms in the left arm followed. The patient always had a sense of warning that allowed him to get into bed if he was sitting, like when he was in a chair. Sometimes he experienced a dizzy feeling as if his body were spinning to the left. This sensation didn't happen at the start of the seizure, and the patient resisted it, turning to the right. Occasionally, he felt like he was rapidly sliding down a slope. Headaches and drowsiness followed, but there was never any complete loss of consciousness or memory.
The eye grounds proved normal and all the photomotor reflexes were normal, though there was no pupil reflex to pain. The patient could write readily to dictation printed letters. It would seem that these printed letters mean that he had visual memories, as he traced the characters as if from a design. Speech was monotonous with some stuttering; but his speech had always been of this sort according to information. He walked with difficulty, not merely on account of his visual but on account of his equilibration disorders. Outside of his seizures he always turned to the right and if left to himself standing he turned to the right. If asked to walk straight ahead, he always turned to the right. Silent and uncommunicative, he was amiable and sometimes even gay. He often had troublous dreams, sometimes seeing his relatives. He said he could bring up in his mind the faces of his relatives and even the appearance of the Salpêtrière. Reflexes and sensations were normal. There was a traumatic rupture of the tympanum. Lumbar puncture showed a slight excess of albumin and 1.8 lymphocytes to the cubic millimeter. The Mauser bullet was found by X-ray in the left calcarine region with its base touching the median line, and[138] applied to the inner table of the skull about a centimeter above the internal occipital protuberance pointing forward, outward, and upward. He was treated on a salt free diet with bromides. The seizures grew fewer and at the time of report two months had elapsed with nothing but a slight vertigo and frequent nightmares. Intellectually also the patient had improved.
The eye exam was normal, and all the photomotor reflexes were normal, although there was no pupil reflex to pain. The patient could easily write printed letters from dictation. It seems that these printed letters indicate he had visual memories since he traced the characters as if following a design. His speech was monotonous with some stuttering, but this type of speech had always been noted, according to reports. He walked with difficulty, not just because of his vision but also due to balance issues. Outside of his seizures, he always turned to the right, and if left standing alone, he turned to the right. When asked to walk straight ahead, he always veered to the right. Silent and uncommunicative, he was friendly and sometimes even cheerful. He frequently had troubling dreams, sometimes involving his relatives. He mentioned he could recall his relatives' faces and even the appearance of the Salpêtrière. Reflexes and sensations were normal. There was a traumatic rupture of the eardrum. A lumbar puncture indicated a slight increase in albumin and 1.8 lymphocytes per cubic millimeter. An X-ray revealed the Mauser bullet in the left calcarine region, resting against the median line and applied to the inner table of the skull about a centimeter above the internal occipital protuberance, pointing forward, outward, and upward. He was treated with a salt-free diet and bromides. The seizures decreased, and by the time of the report, two months had passed with only slight vertigo and frequent nightmares. The patient also showed intellectual improvement.
The case is one of cortical blindness. The seizures are explained by the vicinity of the right Rolandic region to the lesion. The rotatory vertigo is to be explained by the contact of the Mauser bullet with the tentorium and vermis of the cerebellum, which may also explain the difficulties in orientation that occurred between the crises. The visual hallucinations are doubtless due to lesion of the calcarine region.
The case involves cortical blindness. The seizures are caused by the proximity of the right Rolandic area to the lesion. The spinning sensation is due to the Mauser bullet impacting the tentorium and vermis of the cerebellum, which may also account for the disorientation experienced between the episodes. The visual hallucinations are likely a result of damage to the calcarine area.
Tunisian theopath with mystical hallucinations; gun-shot wound of occiput (bullet extracted): After the trauma, Lilliputian hallucinations and micro-megalopsia.
Tunisian theopath with mystical hallucinations; gunshot wound to the back of the head (bullet extracted): After the trauma, tiny hallucinations and changes in perception of size.
Case 106. (Laignel-Lavastine and Courbon, 1917.)
A. ben S. was sent to Villejuif with the diagnosis: “depression, feeling of impotence, discouragement,” having been found on the public street. He was indifferent, almost completely mute, and was at first considered not to understand French. In a fortnight, however, he was talking freely and was then found to be afflicted with hallucinations, melancholia, and delusions, apparently following trauma to the skull.
A. ben S. was sent to Villejuif with the diagnosis: “depression, feeling of powerlessness, discouragement,” having been discovered on the public street. He was indifferent, almost entirely mute, and was initially thought to not understand French. However, within two weeks, he was speaking openly and was then found to be suffering from hallucinations, melancholia, and delusions, apparently following a head injury.
A. ben S. might have been about thirty years old, and was of a rich family, indigenous in Tunis, well educated in the Koran and Arabic literature.
A. ben S. was probably around thirty years old and came from a wealthy family, originally from Tunis, well-educated in the Koran and Arabic literature.
Upon examination, this Tunisian gunner showed contraction of visual fields, poor color vision, and general hypalgesia. During examination, the man seized the needle and plunged it deeply under his skin, exclaiming that a prophet felt nothing and that he could be cut into bits without feeling pain.
Upon examination, this Tunisian gunner showed narrowed vision, poor color perception, and a reduced sensitivity to pain. During the exam, the man grabbed the needle and jabbed it deep into his skin, claiming that a prophet feels nothing and that he could be sliced into pieces without feeling any pain.
It seems that he had had divine visions from early childhood. In his youth he had once gone to a mountain near his home and talked with Mohammed and Allah. Of course, Allah did not appear in human form, but he appeared like a ball or a wheel of fire, slowly turning. Mohammed was a tall man, with a long white beard, his eyes darting rays of fire, and his forehead bearing a gleaming bright body. Allah was heard talking to Mohammed. Orders were given concerning the sun and stars. Subterranean treasures were displayed, as well as Paradise full of yellow, blue, and green houris, transparent, such that, when food was taken, it could be seen going down their throats. Hell too was visible, and the devil very tall and black, an eye behind and another on top. There were also many genii—little men who climbed over the Tunisian’s body. Sometimes in dreams, Allah carried him to all countries of the earth. It was hard to tell[140] whether these effects were hallucinations or vivid imaginings. The Tunisian had been wounded after several months of service by two bullets in one day: the one causing an insignificant lip-wound; the other entering the skull behind. After several months the bullet had been extracted by trephining.
It seems he had divine visions from a young age. In his youth, he went to a mountain near his home and spoke with Mohammed and Allah. Of course, Allah didn’t show up in human form; instead, he appeared as a ball or a wheel of fire, slowly spinning. Mohammed was a tall man with a long white beard, his eyes shining with intensity, and his forehead glowing. Allah could be heard speaking to Mohammed, giving orders about the sun and stars. Hidden treasures were revealed, along with Paradise filled with beautiful houris in yellow, blue, and green, so transparent that you could see the food going down their throats. Hell was also visible, with a very tall, black devil, an eye in the back and another on top. There were also many genies—small figures that crawled over the Tunisian’s body. Sometimes in dreams, Allah took him to every corner of the earth. It was hard to determine whether these experiences were hallucinations or vivid imaginations. The Tunisian had been injured after several months of service, hit by two bullets in one day: one caused a minor lip wound, while the other struck his skull from behind. After a few months, the bullet was removed through trephining.
His further history was obscured by the fact that he wove delusional elements into his story. He said, for example, that he had been court-martialed, though there was no evidence that this was a fact. It is probable that after his wound the patient in a delirium felt that he was going to be shot. The visual hallucinations were very interesting, being Lilliputian. He would see three or four hundred Tunisian gunners walking along, knee-high or taller. Sometimes they all would stop and aim at him. He also showed micromegalopsia, real objects changing their height under his eyes. Both the Lilliputian hallucinations and the micromegalopsia dated from the trauma to the skull. There was no change whatever in the mystical delusions concerning Allah and Mohammed. These he had before the trauma.
His later history was clouded by the fact that he mixed delusional elements into his narrative. For example, he claimed that he had been court-martialed, even though there was no evidence to support this. It's likely that after his injury, the patient, in a state of delirium, felt like he was going to be executed. The visual hallucinations he experienced were quite fascinating, appearing as little people. He would see three or four hundred tiny Tunisian soldiers walking by, either knee-high or taller. Sometimes they would all stop and take aim at him. He also experienced micromegalopsia, where actual objects seemed to change height right before his eyes. Both the little people hallucinations and the micromegalopsia started after the trauma to his skull. There was no change at all in his mystical delusions about Allah and Mohammed; he had those before the trauma.
Meningococcus meningitis with apparent recovery: Dementing psychosis.
Meningococcal meningitis with noticeable recovery: Dementing psychosis.
Case 107. (Maixandeau, 1915.)
A soldier in the Heavy Artillery, 42, developed occipital headaches and Kernig’s sign, December 27, 1915.
A 42-year-old soldier in the Heavy Artillery started experiencing headaches at the back of his head and Kernig’s sign on December 27, 1915.
December 31, at the Hôtel-Dieu, he showed myosis, slight photophobia, meningitic tâche, temperature 39.6, pulse 84, heart sounds dull. Lumbar puncture: hemorrhagic fluid.
December 31, at the Hôtel-Dieu, he exhibited myosis, slight sensitivity to light, meningitic rash, temperature 39.6, pulse 84, and dull heart sounds. Lumbar puncture: bloody fluid.
January 1, the headache was intense, neck stiffness increased, Kernig’s sign less marked; morning and afternoon temperature 39.2. Lumbar puncture yielded hypertensive cloudy fluid and 30 cubic centimeters of serum were administered.
January 1, the headache was severe, neck stiffness got worse, Kernig’s sign was less pronounced; morning and afternoon temperature was 39.2. A lumbar puncture produced cloudy fluid under high pressure and 30 cubic centimeters of serum were given.
This dose was repeated January 2 and January 3, on which date there was no headache.
This dose was repeated on January 2 and January 3, and on that date, there was no headache.
January 4, Kernig’s sign and neck stiffness were diminished; fine râles at the bases without dulness. 30 cubic centimeters of electragol were injected intravenously.
January 4, Kernig’s sign and neck stiffness were reduced; fine crackles at the bases without dullness. 30 cubic centimeters of electragol were injected intravenously.
January 5, Kernig and neck stiffness slight. Meningitic tâche; exaggerated knee-jerks; unequal pupils; temp. 36.6 morning, 39.4 afternoon; respiration 36; pulse 120; no râles; splenic enlargement.
January 5, Kernig and slight neck stiffness. Meningitic signs; exaggerated knee-jerk reflexes; unequal pupils; temperature 36.6 in the morning, 39.4 in the afternoon; respiration 36; pulse 120; no abnormal lung sounds; splenic enlargement.
6, no headache or photophobia; constipation; fine râles, right base; spartein; meningococci found in hypertensive spinal fluid. 30 cc. serum.
6, no headache or sensitivity to light; constipation; fine rales, right base; spartein; meningococci found in hypertensive spinal fluid. 30 cc. serum.
7, more râles; exaggerated heart sounds; intestinal worms in stools.
7, more râles; exaggerated heart sounds; intestinal worms in stools.
8, temperature fell to 37; pulse to 90.
8, temperature dropped to 37; pulse to 90.
9, patient worse; involuntary stools; Kernig’s sign; stiff neck; fever. 30 cc. serum injected.
9, patient is worse; involuntary stools; Kernig’s sign; stiff neck; fever. 30 cc. of serum injected.
10, 20 cc. injected.
10, 20 cc injected.
11, delirious all night; tetaniform stiffness of neck; more râles.
11, restless all night; stiff neck; more wheezing.
12, delirious, incoherent words, Cheyne-Stokes breathing.
12, confused, rambling words, Cheyne-Stokes breathing.
13, less stiffness, Kernig almost absent; pupils normal; Romberg sign slightly developed; pulse 120.
13, less stiffness, Kernig sign almost absent; pupils normal; Romberg sign slightly present; pulse 120.
14, a few râles at right base.
14, a few rolls at the right base.
15, pains in elbows, knees and hands with joint swelling; moist râles; temp. 38.4; pulse 140. Digitalon.
15, joint pain in elbows, knees, and hands with swelling; moist crackling sounds in the lungs; temperature 38.4; pulse 140. Digitalis.
16 and 17, serum erythema of thorax; edema of left knee; pulse 150; spartein 16.
16 and 17, red skin on the chest; swelling of the left knee; pulse 150; spartein 16.
17, ice pack over heart.
17, ice pack on heart.
18, edema of knee diminished; no headache, delirium or pupillary sign.
18, swelling in the knee decreased; no headache, confusion, or signs in the pupils.
19, improvement. Temperature normal thereafter.
19, improvement. Temperature normal after that.
20 and 21, fine râles. Then all symptoms disappeared.
20 and 21, fine roles. Then all symptoms disappeared.
Recovery was predicted, but on January 28 it was observed that the patient was untidy, made mistakes in dressing, such as trying to put his legs into the armholes of his shirt, and denied the most evident facts: His képi on his head, he said it was not. Face drawn; skin yellow. Appearance of asthenia. Deep depression and hebetude. At this time the knee-jerks were exaggerated, pupils unequal, vermicular tremor of tongue; the patient walked on a broad base with tremulous legs suggesting contracture and weakness.
Recovery was expected, but on January 28 it was noted that the patient was disheveled, made errors in getting dressed, such as attempting to put his legs through the armholes of his shirt, and denied the most obvious facts: He insisted that the képi on his head was not there. His face was drawn; his skin was yellow. He showed signs of extreme weakness. There was deep depression and dullness. At this time, his knee-jerks were exaggerated, his pupils were unequal, and there was a quivering tremor in his tongue; the patient walked with a wide stance and trembly legs, indicating stiffness and weakness.
February 8, in a similar state the patient wandered about his room, moving his bed and chairs about, answering questions with an absent air. He had now been taught to be less untidy.
February 8, in a similar state the patient wandered around his room, rearranging his bed and chairs, responding to questions with a distant look. He had now learned to be less messy.
March 5, stiff neck and Kernig’s sign were distinct. He made believe he was on his farm. Ecchymosis of right upper eyelid: he had fallen (his sheep had pushed him over!). The improbability of this idea did not persuade him to think it had not happened. He walked after the manner of a tabetic.
March 5, he had a stiff neck and a positive Kernig's sign. He pretended he was on his farm. He had a bruise on his right upper eyelid: he had fallen (his sheep had knocked him over!). The unlikelihood of this story didn’t convince him it hadn’t happened. He walked like someone with tabes.
In April he became bedridden, unable to walk, with marked stiffness and Kernig’s sign. He had at this time periods of excitement in which he would tear the bedclothes. He was invalided as demented.
In April, he became bedridden and unable to walk, experiencing significant stiffness and a positive Kernig's sign. During this time, he had episodes of agitation where he would tear the bedclothes. He was classified as having dementia.
Meningococcus meningitis.
Meningococcal meningitis.
Case 108. (Eschbach and Lacaze, November, 1915.)
During his eleven months captivity at Grafenwöhr, Eschbach and Lacaze had the opportunity of observing the case of a soldier, 24, who sustained a shell-wound in the left lung and was made prisoner August 20, 1914, at Chateau Salins. He got well of his wound, but February 16, 1915, began to cry out and was restless in the night. He was found on the straw muttering words among which only the word, “Head, head,” could be distinguished. He was irresponsive, possibly deaf. Suddenly he had a convulsive crisis and whenever touched he would have jactitations and cry out. Otherwise, he was calm and stuporous. The pupils were widely dilated. In short, he showed a mental confusion associated with paroxysmal excitement due to cerebral and cutaneous hyperesthesia. The first symptoms had occurred the morning before, when he leaned his head against a wall and complained.
During his eleven months in captivity at Grafenwöhr, Eschbach and Lacaze had the chance to observe a soldier, 24, who had a shell wound in his left lung and became a prisoner on August 20, 1914, at Chateau Salins. He recovered from his wound, but on February 16, 1915, he began to cry out and was restless at night. They found him on the straw mumbling, with only the words, “Head, head,” being clear. He was unresponsive, possibly deaf. Suddenly, he had a seizure, and whenever he was touched, he would jerk around and cry out. Other than that, he appeared calm and dazed. His pupils were dilated. In short, he displayed mental confusion along with sudden episodes of agitation caused by heightened sensitivity in his brain and skin. The first symptoms appeared the morning before when he leaned his head against a wall and complained.
Lumbar puncture yielded intra- and extracellular meningococci. The patient was isolated. In the afternoon he became less agitated, kept his eyes closed, mumbled, repeated gestures, would spit in his hands, rub his hands together, rub his neck, shoulders and body, or else he would pass his hands over his forehead and through his hair. Occasionally he would seize the straw and draw it to him with all his strength. Once when asked, “What is your name?” he said, “Not true. Not true.” Hallucinations appeared to have been added to the situation. The neck was a little stiff to forced flexion. Temperature 37.8. Lumbar puncture under chloroform anesthesia; antimeningococcus serum was injected. Next day quieter; able to get up and walk. Slept, mumbled less, was able to answer simple questions, desired to urinate and finally succeeded.
Lumbar puncture revealed meningococci both inside and outside the cells. The patient was isolated. In the afternoon, he became less agitated, kept his eyes closed, mumbled, repeated gestures, would spit in his hands, rub his hands together, rub his neck, shoulders, and body, or pass his hands over his forehead and through his hair. Occasionally, he would grab the straw and pull it towards him with all his strength. Once, when asked, “What is your name?” he replied, “Not true. Not true.” Hallucinations seemed to have developed as well. His neck was slightly stiff when forced to flex. Temperature was 37.8. Lumbar puncture was performed under chloroform anesthesia, and antimeningococcus serum was injected. The next day, he was quieter; able to get up and walk. He slept, mumbled less, could answer simple questions, felt the urge to urinate, and finally succeeded.
February 19, no mental disorder. Headache and lassitude. Neck stiff, Kernig’s sign marked. Lumbar puncture yielded a fluid now puriform; antimeningococcus serum injected. February 20, lifting the head produced opisthotonos. Labial herpes. The fluid yielded, besides meningococci,[144] also endothelial cells. Serum injected. February 21, fibrin in fluid; serum injected. February 22, no head symptoms. Herpes more intense, involving also arms. Tongue coated. Temperature 37.5, evening 38.3. February 23, meningococci and lymphocytes in fluid. February 24, left knee swollen. Serum injected; puncture fluid showed meningococci and polynucleosis. Fluid from knee showed polynuclear cells without organisms. February 25, patient reached evening temperature of 39.5; serum injected. A few meningococci, altered polynuclear leucocytes. February 26, patient rigid, tongue coated, serum injection. Rare meningococci, degenerated polynuclear leucocytes. February 27, rigidity decreased, evening temperature 37.7. February 28, Kernig’s sign absent. Herpes dry. Serum injection. Fluid clear; lymphocytes and polynuclear cells; no meningococci. March 6, painful inguinal gland on the left side. March 7, epididymitis left (mumps two years before, with headache two weeks and double orchitis). March 9, serum eruption. March 17, epididymitis practically absent. Lymph node painful. Later data impossible to get, except that there was apparently an arthritis of the hip and a sacral decubitus with eventual recovery.
February 19, no mental disorder. Headache and fatigue. Neck stiff, Kernig’s sign positive. Lumbar puncture showed fluid now purulent; antimeningococcus serum injected. February 20, lifting the head caused opisthotonos. Labial herpes. The fluid showed, in addition to meningococci, also endothelial cells. Serum injected. February 21, fibrin in the fluid; serum injected. February 22, no head symptoms. Herpes more intense, also affecting the arms. Tongue coated. Temperature 37.5, evening 38.3. February 23, meningococci and lymphocytes in the fluid. February 24, left knee swollen. Serum injected; puncture fluid showed meningococci and polynucleosis. Fluid from the knee showed polynuclear cells without organisms. February 25, patient reached an evening temperature of 39.5; serum injected. A few meningococci, altered polynuclear leucocytes. February 26, patient rigid, tongue coated, serum injection. Rare meningococci, degenerated polynuclear leucocytes. February 27, rigidity decreased, evening temperature 37.7. February 28, Kernig’s sign absent. Herpes dry. Serum injection. Fluid clear; lymphocytes and polynuclear cells; no meningococci. March 6, painful left inguinal gland. March 7, left epididymitis (had mumps two years prior, with headache for two weeks and double orchitis). March 9, serum eruption. March 17, epididymitis nearly absent. Lymph node painful. Later data unavailable, except that there seemed to be arthritis of the hip and a sacral decubitus with eventual recovery.
Shell-explosion: Meningitic syndrome, fourteen months.
Shell explosion: Meningitis syndrome, 14 months.
Case 109. (Pitres and Marchand, November, 1916.)
A soldier sustained shell-shock at the distance of a meter at Saint-Hilaire, September 26, 1915. He lost consciousness and blood flowed from his ears. He arrived, September 28, at the neurological center in Bordeaux in a semistupor, knowing that he had been shocked and had lost consciousness. He groaned, cried out, and kept stroking his head with his right hand; lay on the right side; showed Kernig’s sign right, ptosis, and stiff neck. Headache was increased on moving and noises. Patient constantly asked for food, but refused to drink. Lumbar puncture yielded a yellowish fluid, due to laked blood. October 3, headache, ptosis, left internal strabismus, temperature 38.5. October 4, lumbar puncture, slightly blood-tinted fluid. October 5, improvement; gap in memory for period since shock. No strabismus, ptosis diminished, temperature normal, improvement continued. Kernig’s sign and headache persisted. He lay doubled up on the right side, eyes closed, right hand on pillow. Defense movements on touching the neck or occipital region. The condition of semistupor often passed off in the afternoon, when he could talk, write or play cards. He had always smoked, even at the beginning of his disease. Lumbar puncture yielded a normal fluid December 12, 1915. He was sent February 23, 1916, to a hospital in the country, but came back May 9.
A soldier experienced shell shock at a distance of one meter in Saint-Hilaire on September 26, 1915. He lost consciousness and blood flowed from his ears. He arrived at the neurological center in Bordeaux on September 28, in a semistupor, aware that he had been shocked and had lost consciousness. He groaned, shouted, and kept rubbing his head with his right hand; he lay on his right side; showed right-sided Kernig’s sign, had drooping eyelids, and a stiff neck. His headache worsened with movement and noise. The patient constantly asked for food but refused to drink. A lumbar puncture yielded a yellowish fluid, due to laked blood. On October 3, he had a headache, drooping eyelids, left internal strabismus, and a temperature of 38.5. On October 4, a lumbar puncture revealed slightly blood-tinted fluid. By October 5, there was improvement; he had a gap in memory for the time since the shock. There was no strabismus, drooping decreased, temperature returned to normal, and improvement continued. Kernig’s sign and headache persisted. He lay curled up on his right side, eyes closed, right hand on the pillow. He had defense movements when his neck or the back of his head was touched. His semistupor condition often lifted in the afternoon, allowing him to talk, write, or play cards. He had always smoked, even at the onset of his illness. A lumbar puncture yielded normal fluid on December 12, 1915. He was sent to a hospital in the countryside on February 23, 1916, but returned on May 9.
It seems that several days after transfer he had had an attack of delirium in the night, having lost consciousness, and tried continually to get up out of bed, saying that he wanted to go to Verdun to fight. This spell lasted several hours and on the days following came mutism, refusal of food, and a state of stupor. Nutritive enemata were given. As he grew better he sometimes ate a great deal, sometimes nothing, even wanted poison from his family, and wrote to a comrade that he wanted to commit suicide.
It appears that a few days after his transfer, he experienced a night of delirium, losing consciousness and repeatedly trying to get out of bed, claiming he wanted to go to Verdun to fight. This episode lasted several hours, and in the days that followed, he became mute, refused food, and fell into a stupor. Nutritional enemas were administered. As he started to recover, he sometimes ate a lot, other times nothing at all, even asked his family for poison, and wrote to a friend saying he wanted to commit suicide.
May 9, he was clearer, told of seeing the shell, which he said he had not heard, nor did he know how he had gotten to a hospital. His head and spine had hurt him ever since the shock. He had had difficulty in urination for two days after the shock. He could not remember the delirious attack in the country hospital. He gave various data about his life, but not fully. He refused to lie on the left side, or to walk, because of pain. He could lift either leg from the bed, but hardly both. There was an irregular coarse tremor of the extremities. The right hand was weaker than the left; there were no reflex disorders; no change in the eye grounds. There was a patchy analgesia. May 26, stupor reappeared as before, with semimutism. June, the patient presented the appearance of a dementia praecox in stupor, with stereotyped gestures and attitudes, without catatonia. The patient was sent to a hospital for the insane at Cadillac. November 9, 1916, he returned to the neurological center, as mental and cerebral disorder had disappeared. There still persisted a difficulty in remembering facts since the shock and there was still a functional paresis of the legs.
On May 9, he was clearer and talked about seeing the shell, which he said he hadn’t heard, nor did he know how he ended up in a hospital. His head and spine had been hurting him since the shock. He had trouble urinating for two days after the shock. He couldn’t remember the delirious episode in the country hospital. He shared various details about his life, but not completely. He refused to lie on his left side or to walk because of the pain. He could lift either leg from the bed, but hardly both. There was an irregular coarse tremor in his limbs. The right hand was weaker than the left; there were no reflex issues; no changes in the eye grounds. There was patchy loss of sensation. On May 26, stupor returned as before, along with semi-mutism. In June, the patient showed signs of dementia praecox in stupor, with stereotyped gestures and postures, but without catatonia. The patient was sent to a mental hospital in Cadillac. On November 9, 1916, he returned to the neurological center, as the mental and brain issues had disappeared. However, he still had difficulty remembering facts since the shock, and there was still functional weakness in his legs.
We here deal with a case of a meningitic syndrome following shell-shock and lasting fourteen months.
We are dealing with a case of meningitis following shell shock that lasted for fourteen months.
Brain abscess in a syphilitic: Matutinal loss of knee-jerks.
Brain abscess in a person with syphilis: Morning loss of knee-jerk reflexes.
Case 110. (Dumolard, Rebierre, Quellien, 1916.)
An unmarried subaltern officer, 30, entered an army neuropsychiatric center, April 8, 1915, looking exhausted and bearing a ticket “nervous asthenia, evacuated for neurological examination.” He said he had had scarlet fever at ten; strongly denied syphilis, of which he presented no trace; had not been excessively alcoholic and had had no nervous seizures. Detailed information showed that he had been a normal child. He left his two years’ military service with promotion and was a man of above the ordinary intelligence.
An unmarried junior officer, 30, walked into an army neuropsychiatric center on April 8, 1915, looking worn out and carrying a note that said "nervous asthenia, evacuated for neurological examination." He mentioned that he had scarlet fever at age ten; he firmly denied having syphilis, for which he showed no signs; he hadn't been excessively drinking and had experienced no nervous seizures. Further details revealed he had been a normal child. He completed two years of military service with a promotion and was a man of above-average intelligence.
He was wounded in the right buttock with a shrapnel bullet about the end of September, 1914. He went back to his regiment two months later and had shared in a number of actions up to the time of his evacuation. He said he had been very tired for several weeks, and had finally been sent to the physician. There were pains in the kidney region and in the head, especially on the right side. The head felt empty. He could not sleep, but did not dream. Ideas were not distinct. Memory had become impaired. He could not keep his accounts right, and was afraid something might go wrong.
He was wounded in the right buttock by a shrapnel bullet around the end of September 1914. He returned to his regiment two months later and took part in several actions until he was evacuated. He mentioned feeling very tired for weeks and was eventually sent to see a doctor. He experienced pain in his kidney area and in his head, particularly on the right side. His head felt empty. He couldn't sleep and didn't have dreams. His thoughts weren't clear. His memory had worsened. He couldn't keep his accounts straight and was worried something might go wrong.
There was no pain or nervous or reflex disorder of any sort except for the knee-jerks and Achilles jerks (see below). A special examination proved complete normality of eyes. There was a slight hesitation in words, but no dysarthria. There was a slight tremor of the tongue and fingers.
There was no pain, anxiety, or reflex issues at all except for the knee-jerks and Achilles jerks (see below). A specific examination showed that the eyes were completely normal. There was a slight hesitation in speech, but no difficulty in articulating words. There was a slight tremor in the tongue and fingers.
As to the tendon reflexes, April 9, on waking, the knee-jerks were absent, but later in the day gradually came in evidence again. The Achilles jerks were also absent at first, but could be obtained after a prolonged examination and after percussion of the calf. In the afternoon, after exercise, the knee-jerks and Achilles jerks were easily demonstrable. The left Achilles jerk was always a little weaker than the right. Massage brought these jerks out to virtual normality. April[148] 10 and thereafter, similar findings; percussion of the muscular masses of the thighs and calves always brought out the reflexes.
Regarding the tendon reflexes, on April 9, when I woke up, the knee-jerks were absent, but they gradually returned later in the day. The Achilles reflexes were also absent at first, but they could be elicited after a lengthy examination and some tapping on the calf. In the afternoon, following some exercise, both the knee-jerks and Achilles reflexes were easily noticeable. The left Achilles jerk was consistently a bit weaker than the right. Massage nearly returned these reflexes to normal. From April[148] 10 onward, similar results were observed; tapping the muscles in the thighs and calves consistently triggered the reflexes.
Lumbar puncture yielded a clear fluid with hyperalbuminosis, 20 cells per c.mm. (lymphocytes and mononuclear cells 95 per cent) and a positive W. R. Iodide of mercury treatment was given April 18.
Lumbar puncture produced a clear fluid with high albumin levels, 20 cells per cubic millimeter (95 percent being lymphocytes and mononuclear cells), and a positive W. R. Iodide of mercury treatment was administered on April 18.
April 23, the patient went into a coma, with trismus, stiff neck, Kernig’s sign, sluggish pupils, incontinence. He was transferred to a special hospital, showed on lumbar puncture, April 23, 85 per cent polynuclear leucocytes, and died April 27. The autopsy showed a yellowish, quasidiffluent softening of the size of a small egg in the first occipital gyrus on the right side. The authors comment on the fact that the only objective sign in this case was the variable tendon reflexes of the lower extremities,[149] “l’unique cri de souffrance des centres nerveux.”
April 23, the patient fell into a coma, exhibiting trismus, a stiff neck, a positive Kernig’s sign, sluggish pupils, and incontinence. He was moved to a specialized hospital, and a lumbar puncture on April 23 revealed 85 percent polynuclear leukocytes. He passed away on April 27. The autopsy showed a yellowish, quasi-diffuse softening the size of a small egg in the first occipital gyrus on the right side. The authors note that the only objective sign in this case was the variable tendon reflexes in the lower limbs, [149] “l’unique cri de souffrance des centres nerveux.”
Early recovery from a spinal cord lesion.
Early recovery from a spinal cord injury.
Case 111. (Mendelssohn, January, 1916.)
Mendelssohn reports a soldier, who was sent to a Russian hospital, April 12, 1915, with a diagnosis of chronic appendicitis. Operated on next day, the patient appeared to be passing through a normal convalescence, when ten days later, he had an intense headache and some trouble in vision, which disappeared the next day, only to be followed, two days later, by the patient’s complaint that he could no longer urinate or rise from bed.
Mendelssohn reports about a soldier who was sent to a Russian hospital on April 12, 1915, with a diagnosis of chronic appendicitis. After being operated on the next day, the patient seemed to be recovering normally, but ten days later, he developed a severe headache and some vision problems, which went away the following day. However, two days later, the patient complained that he could no longer urinate or get out of bed.
In fact, Mendelssohn found a complete flaccid paraplegia with urinary retention, without fever or pain. Knee-jerks and Achilles jerks were absent, and there was a slight extension of the great toe on plantar stimulation. There was disorder of sensation, with heat sensibility abolished, painful points poorly localized, and position sense poor. Electric reactions normal. Pain on pressure in and about the lumbar vertebral region. Cerebrospinal fluid showed lymphocytosis and an excessive albuminosis.
In fact, Mendelssohn observed a complete loss of movement in the legs with urinary retention, no fever or pain. The knee and Achilles reflexes were absent, and there was a slight extension of the big toe when the bottom of the foot was stimulated. There was a sensory disorder, with the ability to feel heat completely gone, poorly localized painful spots, and sense of position being poor. Electric responses were normal. There was pain when pressing in and around the lower back area. The cerebrospinal fluid showed an increase in lymphocytes and excessive protein levels.
This paraplegia lasted six weeks. At the end of May, the patient began to be able to move his toes and to lift his heel. Improvement was gradual and progressive. Early in June he could walk if supported. The weak knee-jerk then began to reappear and the urinary retention gradually disappeared.
This paraplegia lasted six weeks. At the end of May, the patient started to be able to move his toes and lift his heel. Improvement was gradual and steady. Early in June, he could walk with support. The weak knee reflex then began to come back, and the urinary retention gradually went away.
This patient was not hysterical, although a bit emotional. Perhaps, according to Mendelssohn, an organic lesion was grafted on a neurosis. Perhaps the spinal lesion was infectious. At any rate, a presumably organic paraplegia had recovered in two months and a half.
This patient wasn't hysterical, although they were a bit emotional. According to Mendelssohn, an organic issue might have been added to a neurosis. It's possible that the spinal issue was infectious. In any case, what seemed like an organic paraplegia had improved in two and a half months.
Shell-explosion: Meningeal hemorrhage: Pneumococcus meningitis.
Shell explosion: Meningeal hemorrhage: Pneumococcus meningitis.
Case 112. (Guillain-Barré, August, 1917.)
An infantryman, 20, came to the Sixth Army Neurological Center, October 13, 1916, as a case of “choluria, due to shell explosion; epistaxis needs watching.” He was somnolent, had waked vomiting, pulse 108. Kernig’s sign, defensive movements of the legs on stimulation, with flexion of leg on thigh and of thigh on pelvis, plantar reflexes flexor. Puncture showed typical meningeal hemorrhage. Two days later, temperature 40, pulse 70, that is to say, a bradycardia in proportion to the fever. Vomiting, pulse persisted. Next day the patient was moaning and semi-delirious and showed stiff neck, Kernig’s sign, accentuation of vasomotor disorder, plantar response flexor with leg retracted, thigh flexion both homolateral and contralateral. The spinal fluid upon the next day, that is, four days after his arrival at the clinic, showed a purulent fluid in which there was an excess of albumin, no sugar, diplococci extracellular (proving on culture to be pneumococci and able to kill a mouse in twenty-four hours).
An infantryman, 20, arrived at the Sixth Army Neurological Center on October 13, 1916, with a diagnosis of “choluria, due to shell explosion; epistaxis needs monitoring.” He was drowsy, had vomited upon waking, and his pulse was 108. Kernig’s sign was present, with defensive movements of the legs when stimulated, showing flexion of the leg on the thigh and of the thigh on the pelvis, and plantar reflexes were flexor. A puncture revealed typical meningeal hemorrhage. Two days later, his temperature was 40°C, and his pulse was 70, indicating bradycardia in relation to the fever. Vomiting persisted, and the next day the patient was moaning and semi-delirious, displaying a stiff neck, Kernig’s sign, increased vasomotor disorders, and a flexor plantar response with the leg retracted, flexion of the thigh both on the same side and the opposite side. The spinal fluid the following day—four days after his arrival at the clinic—showed purulent fluid with excess albumin, no sugar, and extracellular diplococci (which were later confirmed by culture to be pneumococci capable of killing a mouse within twenty-four hours).
As a rule such hemorrhages remain aseptic, and in fact meningeal hemorrhage is said by Guillain and Barré to have, as a rule, a favorable prognosis. The above described case was the only one of infected meningeal hemorrhage that had occurred in the Sixth Army Neurological Center.
As a rule, these types of hemorrhages are not infected, and in fact, Guillain and Barré suggest that meningeal hemorrhage generally has a good prognosis. The case described above was the only instance of infected meningeal hemorrhage that occurred at the Sixth Army Neurological Center.
ANTEBELLUM cortex lesion: right hemiplegia; recovery. Struck by shrapnel on right shoulder: Athetosis.
ANTEBELLUM cortex lesion: right hemiplegia; recovery. Hit by shrapnel on right shoulder: Athetosis.
Case 113. (Batten down the hatches, January, 1916.)
A British soldier, aged 27, showed a somewhat remarkable phenomenon. It appears that at five years of age, this man had had poliomyelitis, affecting the left leg. At 20 years of age, he had had pneumonia, and this had been followed by a paralysis of the right arm and leg with a loss of speech. The man recovered from this illness, although he never quite regained full control of the right hand. It is evident that this lack of control was not marked, else the man would not have been enlisted, and it is Dr. Batten’s opinion that at all events he could not have shown pathological movements of the right hand at the time of enlistment.
A 27-year-old British soldier demonstrated a rather remarkable case. It seems that at the age of five, he had polio, which affected his left leg. When he was 20, he suffered from pneumonia, which was followed by paralysis in his right arm and leg, along with loss of speech. He recovered from this illness, although he never fully regained control of his right hand. It's clear that this lack of control wasn't severe, otherwise he wouldn't have been able to enlist, and Dr. Batten believes that, in any case, he wouldn't have shown any pathological movements in his right hand at the time of enlistment.
However this may be, in October, 1914, the soldier was struck on the right shoulder with shrapnel. Apparently he was not wounded, but thereafter he was not able to use the right arm well, and in two months’ time he had become unable to manipulate his rifle. On January 13, 1915, he was sent home. The remnants of the old poliomyelitis of the left leg were shown in a general weakness of that leg as compared with the right. The movements of the right hand were those seen in athetosis. The movements were independent of volition. The patient had difficulty in releasing his grasp. He improved rapidly during the six weeks he was in hospital, although the movements of the right hand never became entirely normal.
However this may be, in October 1914, the soldier was hit in the right shoulder by shrapnel. It seemed that he wasn't seriously hurt, but afterwards he couldn't use his right arm well, and within two months he couldn't handle his rifle at all. On January 13, 1915, he was sent home. The lingering effects of old poliomyelitis in his left leg were evident in a general weakness of that leg compared to the right. The movements of his right hand were similar to those seen in athetosis. The movements were involuntary. He had trouble letting go of things. He improved quickly during the six weeks he spent in the hospital, although the movements of his right hand never returned to being completely normal.
In this case, according to Batten,[152] “the stress was sufficient to bring into prominence the symptoms due to an old cerebral lesion.”
In this case, according to Batten,[152] “the stress was enough to highlight the symptoms from an old brain injury.”
Hysterical versus thalamic hemianesthesia.
Hysterical vs. thalamic hemianesthesia.
Case 114. (Leri, October, 1916.)
A soldier, 40, had been suffering for a number of months with pains in the left side of the trunk and feelings of weakness in the left arm and leg. In the summer of 1915 he was on leave and while walking, fell, lay down, and found he could hardly move his left arm and leg. Two or three weeks later he got up, walking with a stick. After some time in hospital, he was sent back to the trenches, a little weak.
A 40-year-old soldier had been dealing with pain in the left side of his body and weakness in his left arm and leg for several months. During his leave in the summer of 1915, he was walking when he suddenly fell, lay down, and realized he could barely move his left arm and leg. Two or three weeks later, he got up and was able to walk with a cane. After spending some time in the hospital, he was sent back to the trenches, feeling a bit weak.
He had shortly, however, to be examined neurologically again. He could hardly raise the left leg and his passive resistance was poor on this side. The left side was almost completely anesthetic to all forms of stimulus, although an intense faradic current yielded a feeling like that of a fly. Nor was the tactile sensation absolutely nil, as it could be got with a flat finger on the upper arm and thigh. Cold and heat sensations not well localized. The hemianesthesia was sharply limited at the median line and affected the buccal, lingual and nasal mucosa. Deep sensibility was almost abolished on the left side. Stereognostic sense was lost and the sense of position was lost absolutely for hand and foot.
He was soon scheduled for another neurological exam. He could barely lift his left leg, and his resistance to passive movements on that side was weak. The left side was almost completely numb to all types of stimuli, although a strong electrical current felt like the sensation of a fly landing. The tactile sensation wasn’t completely absent, as it could be felt with a flat finger on the upper arm and thigh. He struggled to accurately identify cold and heat sensations. The numbness was sharply defined along the middle of his body and affected the lining of the mouth, tongue, and nose. Deep sensation was nearly gone on the left side, his ability to recognize objects by touch was lost, and he completely lost the sense of position for his hand and foot.
The patient said that he heard less well on the left side. There was also a slight contraction of the left visual field. The reflexes were lively, but equal on both sides. A diagnosis of hysterical hemianesthesia was apparently called for, but psychoelectric treatment failed. The plantar reflex was, in fact, completely absent on the left side, as well as the corneal reflex. The faradic current failed to produce as marked a dilatation of the pupil on the left side as on the right. The forehead wrinkles were less marked on the left side. The mouth deviated slightly to the right. The left nasolabial fold was a little less marked. The tongue did not deviate, but was a little narrow on the left side. The palate deviated a little to the left. The left side of the trunk seemed a little less developed than the right, and the scapula stuck a little less closely to the body on the left side, when the arms were raised. The left buttock was a little narrower than the right[153] and the left gluteal fold was less marked. In combined flexion of thigh and trunk the left foot readily left the floor. There was a left-sided hypotonia in forced flexion of the forearm. There were no tremors of the limbs in repose, except a few contractions of the left lower extremity. In movement, however, there was a marked tremor and in coördination the finger to nose test could not be performed. Speech was slow and hesitant, sometimes stuttering. Food was sometimes taken into the air passages. Headaches were localized on the right side. They had begun when the first symptoms began. There was mental disorder, with gaps in memory. In short, the case is probably one of thalamic disease, though there were no pains except a few in the left side of the trunk at the beginning of the disease. The diagnosis of hysteria was at first made in this case, but the rule that hysterical hemianesthesia is never found without auto- or hetero-suggestion caused the alteration of diagnosis to thalamic.
The patient reported that he had reduced hearing on the left side. There was also a slight reduction in the left visual field. The reflexes were brisk but equal on both sides. A diagnosis of hysterical hemianesthesia seemed appropriate, but psychoelectric treatment didn’t work. The plantar reflex was completely absent on the left side, as was the corneal reflex. The faradic current didn’t cause as noticeable pupil dilation on the left side as it did on the right. The wrinkles on his forehead were less pronounced on the left side. His mouth slightly tilted to the right. The left nasolabial fold was a bit less prominent. The tongue didn't deviate but appeared slightly narrower on the left. The palate shifted a little to the left. The left side of the trunk seemed somewhat less developed than the right, and the left scapula was a little less closely aligned with the body when the arms were lifted. The left buttock was slightly narrower than the right, and the left gluteal fold was less defined. During combined flexion of the thigh and trunk, the left foot easily lifted off the floor. There was left-sided hypotonia during forced flexion of the forearm. No tremors were present in the limbs at rest, aside from a few contractions in the left lower extremity. However, there was noticeable tremor during movement, and he couldn’t perform the finger-to-nose test due to lack of coordination. His speech was slow and hesitant, sometimes stuttering. Food occasionally entered the air passages. Headaches were localized on the right side, starting when the initial symptoms emerged. There was a mental disorder with gaps in memory. In summary, this case likely involves thalamic disease, although there were no pains except for some in the left side of the trunk at the onset of the illness. Initially, the diagnosis was hysteria, but the principle that hysterical hemianesthesia is never observed without auto- or hetero-suggestion led to a change in diagnosis to thalamic.
Shell-explosion: Syndrome suggesting multiple sclerosis.
Shell explosion: Syndrome indicating multiple sclerosis.
Case 115. (Pitres and Marchand, November, 1916.)
A soldier, 40, carriage painter, underwent shell-shock at Voquois, May 2, 1915, following ten hours’ bombardment. At the time he felt tinglings. The bombardment had just ceased when he fainted suddenly while repairing a telegraph line. There was no loss of consciousness. He could not move his arms or legs, was able to spit, and did not suffer at all except for the tingling. He was evacuated to the interior, where the diagnosis of psychopathic double paraplegia, Kernig’s sign, zones of anesthesia in the legs, was made. He was immediately treated with gray oil, and got an injection of neosalvarsan, and iodides. He grew slowly better. He could lift a leg from the bed, but then both legs began to tremble. The arms had recovered their movement, before the legs, but always trembled in movement.
A 40-year-old soldier and carriage painter experienced shell shock at Voquois on May 2, 1915, after undergoing ten hours of bombardment. At that moment, he felt tingling sensations. The bombardment had just stopped when he suddenly fainted while fixing a telegraph line. He did not lose consciousness. He couldn't move his arms or legs, could spit, and didn't feel any pain, except for the tingling. He was evacuated to the interior, where he was diagnosed with psychopathic double paraplegia, Kernig’s sign, and areas of numbness in his legs. He was immediately treated with gray oil and given an injection of neosalvarsan and iodides. He slowly began to improve. He was able to lift a leg off the bed, but both legs then started to tremble. His arms regained movement before his legs, but they always trembled when moving.
November, 1915, he was able to get up; two months later, he walked alone.
November 1915, he was able to get up; two months later, he walked by himself.
At the neurological center, which he entered December 17, his gaze was fixed and there was a slight exophthalmos. The folds of the face were smoothed out. The nose was deep set (as a result of a fall at the age of eight). In the upright position he could not remain still, but trembled markedly on the left side, so that he had to make a few steps to keep his balance. He was unable to stand on his left leg. He walked on a broad base, in little steps, and rather unsteadily on account of tremors augmenting upon movement. General muscular weakness; left hand slightly weaker than right. He could not lift both legs more than 20 cm. from the bed and in the process they both trembled, trembling together. There was also intention-tremor of the arms, a little less marked than that of the legs, of an irregular rhythm. The arms trembled as a whole. In a state of rest there was no tremor. There was a slight muscular stiffness and the patient himself felt difficulty in relaxing. Patellar reflexes absent,[155] even on reinforcement; Achilles jerks absent. Speech monotonous and tremulous, but not scanning; syllable doubling observed by the patient. Manuscript tremulous and, on account of tremors, illegible. Hypalgesia of legs, more marked distally. Deep sensibility of tendo Achillis and patellar reflexes lost. Pain on compression of eyes diminished. Formication in arms. W. R. of blood negative. Slow improvement followed and the patient left the neurological service May 4, 1916, able to walk more easily and without tremor. The knee-jerks and Achilles jerks were still absent.
At the neurological center, which he entered on December 17, his gaze was fixed and there was a slight bulging of the eyes. The wrinkles in his face were smoothed out. His nose was deeply set due to a fall he had at age eight. He couldn't stay still while standing; he trembled noticeably on the left side and had to take a few steps to keep his balance. He was unable to stand on his left leg. He walked with a wide stance, in small steps, and rather unsteadily because the tremors increased with movement. He had general muscle weakness, with his left hand being slightly weaker than his right. He couldn't lift both legs more than 20 cm off the bed, and they shook together when he tried. There was also an intention tremor in his arms, which was a little less pronounced than that in his legs, and had an irregular rhythm. His arms trembled as a whole. There was no tremor at rest. He experienced slight muscle stiffness and had difficulty relaxing. The patellar reflexes were absent, even with reinforcement; the Achilles reflexes were also absent. His speech was monotone and shaky, but not choppy; he noticed syllable doubling. His handwriting was shaky and, due to the tremors, difficult to read. He had reduced sensitivity in his legs, which was more pronounced distally. Deep sensitivity in the Achilles tendon and patellar reflexes were lost. Pain from eye pressure was diminished. He felt a tingling sensation in his arms. The blood work was negative. He showed slow improvement and left the neurological service on May 4, 1916, able to walk more easily and without tremors. The knee jerks and Achilles reflexes were still absent.
We here deal with a syndrome in part that of a multiple sclerosis, that is, the intention-tremor, gait disturbance, muscular rigidity, and weakness.
We are dealing with a syndrome that is partly related to multiple sclerosis, including intention tremors, difficulty walking, muscle stiffness, and weakness.
Re multiple sclerosis, Lépine remarks that there are numerous army cases of pseudo multiple sclerosis which are actually hysterical or hystero-traumatic cases of hypertonus and tremor. The true cases of multiple sclerosis, according to Lépine, are of interest inasmuch as they are usually found in officers. These men have apparently at first but a slight motor disorder, quite compatible with desk work. We have usually under-rated the cortical element in multiple sclerosis. Spells of confusion, delusional ideas, sometimes grandiose, start up without warning in these cases. To be sure, alcohol and syphilis sometimes also enter these cases etiologically. Any case of localized tremor ought to be carefully examined psychically, and such cases in general ought not to be given responsibility.
Re multiple sclerosis, Lépine notes that there are many army cases of pseudo multiple sclerosis that are actually hysterical or hystero-traumatic cases of hypertonia and tremors. True cases of multiple sclerosis, according to Lépine, are particularly interesting because they are usually found in officers. These individuals initially exhibit only slight motor disorders, which are compatible with desk work. We have often underestimated the cortical element in multiple sclerosis. Episodes of confusion and delusional thoughts, sometimes grandiose, appear suddenly in these cases. Certainly, alcohol and syphilis can also play a role in these cases. Any instance of localized tremor should be examined carefully from a psychological perspective, and such cases in general should not be assigned responsibilities.
Coexistence of hysterical and organic symptoms in two cases of mine explosion.
Coexistence of hysterical and physical symptoms in two cases of mine explosions.
Cases 116 and 117. (Smyly, April, 1917.)
A soldier was blown up by a mine and rendered unconscious. Upon recovery of consciousness, he was dumb, unable to work, very nervous, paralyzed as to left arm and leg. The paralysis improved so that in the hospital at home the patient became able to get about. However, he threw his legs about in an unusual fashion. Several months later, the patient was much improved.
A soldier was blown up by a mine and knocked out. When he came to, he couldn't speak, was unable to work, was very anxious, and had paralysis in his left arm and leg. His paralysis got better, and in the hospital at home, he was able to move around. However, he moved his legs in a strange way. Several months later, he had improved a lot.
Shortly, however, there was a relapse. Transferred to a hospital for chronic cases, the patient was unable to walk without assistance on account of complete paralysis of the leg. Insomnia, general tremor, and a bad stuttering developed, with a habit of starting in terror at the slightest noise.
Shortly after, though, there was a setback. Moved to a hospital for chronic cases, the patient couldn't walk without help due to complete paralysis of the leg. Insomnia, general trembling, and severe stuttering developed, along with a tendency to jump in fear at the slightest noise.
Hypnotic treatment was followed by almost complete disappearance of the tremor. The patient began to sleep six or seven hours a night; nervousness diminished, and the stuttering slowly improved; but neither the paralysis nor the anesthesia of the left leg was affected by suggestion. The leg remained cold, livid, anesthetic, and flaccidly paralyzed to the hip. Though a slight improvement has since been produced by faradization, the patient still can walk only with assistance.
Hypnotic treatment led to nearly complete elimination of the tremor. The patient started sleeping six or seven hours a night; anxiety decreased, and the stuttering gradually got better; however, neither the paralysis nor the numbness in the left leg improved with suggestion. The leg remained cold, pale, numb, and weakly paralyzed up to the hip. Although a bit of improvement has been achieved through faradization, the patient can still only walk with help.
A man was injured in 1906 by the fall of a heavy weight on his back. In 1914 he went to France as a soldier, and eight months later was hurled into a shell hole so that his back struck the edge. He was rendered unconscious. Upon recovery of consciousness, the right leg was found to be swollen, and there were severe pains in the legs and back.
A man was hurt in 1906 when a heavy weight fell on his back. In 1914, he went to France to serve as a soldier, and eight months later, he was thrown into a shell hole, causing his back to hit the edge. He lost consciousness. When he came to, his right leg was swollen, and he was experiencing intense pain in his legs and back.
Since return home the patient had gone from one hospital to another, for the most part unable to walk, suffering from agonizing pain in the head and eyes, unable to sleep, and in the night subject to horrible waking dreams.
Since returning home, the patient had moved from one hospital to another, mostly unable to walk, suffering from intense pain in the head and eyes, unable to sleep, and at night plagued by terrifying nightmares.
Chart 6
MINOR SIGNS OF ORGANIC HEMIPLEGIA
(LHERMITTE)
| I. | Hyperextension of forearm (hypotonia). |
| II. | Platysma sign: Contraction absent on paralyzed side. |
| III. | Babinski’s flexion of thigh on pelvis (spontaneous, upon suddenly throwing seated subject into dorsal decubitus). |
| IV. | Hoover’s sign: Complementary opposition (on request to raise paralyzed arm, presses opposite arm strongly against mattress). |
| V. | Heilbronner’s sign of the broad thigh (hypotonia). |
| VI. | Rossolimo’s sign: flexion of toes on slight percussion of sole. |
| VII. | Mendel-Bechterew sign: flexion of small toes on percussion with hammer of dorsal surface of cuboid bone. |
| VIII. | Oppenheim’s sign (extension of great toe on deep friction of calf muscles); or Schaefer, or Gordon (on pinching tendo Achillis). |
| IX. | Marie-Foix sign: withdrawal of lower leg on transverse pressure of tarsus or forced flexion of toes, even when leg is incapable of voluntary movement. |
At first able only to bring himself to an upright position and to rush a few steps, he later acquired considerable control of his feet and legs through crutches. The insomnia persisted.
At first, he could only manage to get himself upright and take a few hurried steps. Later, he gained significant control of his feet and legs using crutches. The insomnia continued.
Smyly regards this case, like Case 116, as more neurological than mental.
Smyly sees this case, like Case 116, as more about the nervous system than about the mind.
Re organic neurology, much of great value has been reported.
Re organic neurology, a lot of valuable information has been shared.
Sargent and Holmes say that, contrary to expectation, there have been few war cases of bad sequelae of cerebral injuries, such as insanity and epilepsy. During early stages, after infection of the head wounds, there is dulness and amnesia, irritability and childishness,—symptoms which disappear during and after repair of the wounds. Mental disorder requiring internment is surprisingly rare. During 12 months only eight cases were transferred from the head hospital in a year to the Napsbury war hospital, where cases of insanity attributable to the service are sent; and in but two of these could the persisting mental symptoms be attributed to head injury.
Sargent and Holmes note that, surprisingly, there have been few war-related cases of severe aftereffects from head injuries, such as insanity and epilepsy. In the early stages, following infections from head wounds, symptoms like dullness, amnesia, irritability, and childish behavior can appear, but these symptoms typically fade during and after the wounds are treated. It's surprisingly rare for someone to need to be hospitalized for mental disorders. In 12 months, only eight cases were transferred from the head hospital to the Napsbury war hospital, where they send cases of insanity related to military service; and only two of these cases had persistent mental symptoms linked to head injuries.
Col. F. W. Mott confirms the opinion of Col. Sargent and Col. Holmes, remarking that from all the London County Council Asylums, only one case of insanity associated with gunshot head wound had been admitted, and that this was one of a Belgian who died from septic infection of the cerebral ventricles. Yet all cases of insanity in invalided soldiers belonging to the London County Council area (about one-seventh of the population of the United Kingdom) are transferred to these asylums.
Col. F. W. Mott agrees with Col. Sargent and Col. Holmes, noting that out of all the London County Council Asylums, only one case of insanity linked to a gunshot head wound was admitted, and that was a Belgian who died from a septic infection in the brain's ventricles. However, all cases of insanity among injured soldiers in the London County Council area (which makes up about one-seventh of the UK’s population) are sent to these asylums.
Again Sargent and Holmes point out that both generalized and Jacksonian epileptiform seizures are comparatively rare in patients suffering from recent head wounds; even convulsions in later stages have been as yet less common than was feared. Thus, after evacuation to England, fits occurred in 37 (6 per cent) of 610 cases with complete notes, and in only eleven of these 37 cases were the convulsions frequent. Sargent and Holmes remark, however, that the practice of giving bromides regularly to all serious cranial injuries until the wound is healed, and for some months afterwards, seems[159] advisable. In 33 of the 37 convulsive cases there have been severe compound fractures of the skull, and in four of these a missile was still present in the brain. Five secondary operations were performed with good results, after drainage of small abscesses in two and removal of spicules of bone in three. The In-patient and Out-patient records of the National Hospital for the Paralyzed and Epileptic were searched for epileptics already discharged from the army, but notes of but two patients attending this hospital for epilepsy were found.
Again, Sargent and Holmes note that both generalized and Jacksonian epileptiform seizures are relatively rare in patients with recent head injuries; even seizures in later stages have been less common than expected. After evacuation to England, fits occurred in 37 (6 percent) of 610 cases with complete records, and only eleven of these 37 cases experienced frequent convulsions. Sargent and Holmes suggest, however, that it is advisable to routinely administer bromides to all patients with serious cranial injuries until the wound heals, and for several months afterward. In 33 of the 37 convulsive cases, there were severe compound fractures of the skull, and in four of these cases, a missile remained lodged in the brain. Five secondary operations were performed with good outcomes, following the drainage of small abscesses in two cases and the removal of bone fragments in three. The inpatient and outpatient records of the National Hospital for the Paralyzed and Epileptic were searched for epileptics who had already been discharged from the army, but only two patients attending this hospital for epilepsy were found.
As for other neurological complications aside from septic infection and hernia formation, there are a few subjective symptoms that may necessitate the invaliding of soldiers. The most common of these is headache, usually in the form of a feeling of weight, pressure, or throbbing in the head, which headache is increased by noise, fatigue, exertion, or emotion. Attacks of dizziness also occur, and nervousness or deficient control over emotions and feelings. Changes of temperament are found in some soldiers, who become depressed, moody, irritable, or emotional, and unable to concentrate attention.
As for other neurological issues besides infections and hernias, there are a few symptoms that may require soldiers to be discharged. The most common of these is headaches, often felt as a heavy, pressing, or throbbing sensation in the head, which worsens with noise, fatigue, exertion, or strong emotions. Dizziness also happens, along with feelings of nervousness or a lack of control over emotions. Some soldiers experience changes in temperament, becoming depressed, moody, irritable, or overly emotional, which affects their ability to focus.
Foix, under the direction of P. Marie, worked upon aphasia in 100 cases, reporting results at a surgical and neurological meeting, May 24, 1916, in Paris. Only lesions on the left side of the brain have produced important and lasting speech disorder, although lesions on the left side may leave behind them a little dysarthria or difficulty in finding words in conversation. It is, of course, hard to tell speech disorder from stupor or clouding of consciousness. Foix notes certain specialties in speech defect according to which region of the left brain is affected.
Foix, led by P. Marie, studied aphasia in 100 cases and presented the findings at a surgical and neurological conference on May 24, 1916, in Paris. Only damage to the left side of the brain has resulted in significant and lasting speech disorders, although damage to the left side may also cause mild dysarthria or difficulty finding words in conversation. It’s important to note that distinguishing between speech disorder and stupor or altered consciousness can be challenging. Foix observes specific speech defects based on which area of the left brain is impacted.
First: Prefrontal lesions produce a transient dysarthria, lasting but a few weeks, and right-sided prefrontal lesions produce just as much disorder.
First: Prefrontal lesions cause temporary speech difficulties that last only a few weeks, and lesions on the right side of the prefrontal area cause just as much disruption.
Occipital lesions produce no speech disorder.
Occipital lesions do not cause any speech issues.
Second: Patients with right-sided hemianopsia due to lesions of occipital regions were not aphasic and could read or write perfectly. Lesions of the left visual centers certainly do not affect reading. If, however, the injury is not to the[160] visual centers, but is upon the lateral part of the occipital lobe, then alexic phenomena appear, and these the more the lesion approaches the temporal-parietal region.
Second: Patients with right-sided hemianopsia from occipital region lesions were not aphasic and could read or write perfectly. Lesions in the left visual centers definitely don’t impact reading. However, if the damage is not to the[160] visual centers but instead affects the lateral part of the occipital lobe, then alexia occurs, and these symptoms increase as the lesion gets closer to the temporal-parietal region.
Third: Central convolutional lesion produces a variety of disorders according to the site and extent of the lesion. There is no aphasia with the crural monoplegia due to superior paracentral disorder. But slight aphasic disorder accompanies the brachial monoplegia of middle central lesion, though writing, reading, and calculation are slightly affected, and the more so the more the lesion extends posteriorly to the stereognostic regions. The lower down in the precentral region the lesion appears, the more likely is the Broca syndrome to be observed. But if the hemiplegia is chiefly a brachial monoplegia, the aphasic disorder may remain slight, involving reading, writing, understanding of words, the spoken word, articulation, and calculation.
Third: A central convolutional lesion causes different disorders depending on its location and extent. There is no aphasia with crural monoplegia due to a superior paracentral disorder. However, a mild aphasic disorder occurs with brachial monoplegia from a middle central lesion, although writing, reading, and calculations are only slightly affected, and this impact increases as the lesion extends further back into the stereognostic areas. The lower the lesion is in the precentral region, the more likely it is to observe Broca syndrome. But if the hemiplegia mainly involves brachial monoplegia, the aphasic disorder may remain minimal, affecting reading, writing, word comprehension, spoken language, articulation, and calculations.
Fourth: Lesions of the lateral-frontal region produce more or less marked aphasic disorder, just as do those of the inferior part of the precentral gyrus. This aphasia is more apt to occur when the wound is deep. However, no case of permanent aphasia has been observed in cases of lesion of the lateral-frontal region (termed in Foix’s nomenclature, the precentral region, but referring to the tissues in front of the precentral (or ascending frontal) gyrus of the more familiar nomenclature). Almost absolute, or absolute, anarthria follows the wound, and the patient is hemiplegic. This hemiplegia may last from ten days to two or three months. After a time there is no longer more than a slight dysarthria, and writing becomes good again; reading remains, perhaps, a little difficult. A complete or almost complete cure is the rule.
Fourth: Injuries to the lateral-frontal area lead to varying degrees of speech disorders, similar to those caused by damage to the lower part of the precentral gyrus. This speech issue is more likely to happen if the injury is severe. However, there have been no cases of permanent speech impairment reported from injuries to the lateral-frontal area (which Foix refers to as the precentral region, but it actually pertains to the tissues located in front of the precentral, or ascending frontal, gyrus in more familiar terms). Almost total or total inability to speak follows the injury, and the patient experiences hemiplegia. This hemiplegia may last anywhere from ten days to two or three months. After some time, only a slight difficulty in speaking remains, and writing returns to a good level; reading might still be a bit challenging. Generally, a complete or nearly complete recovery is the norm.
Fifth: When the retrocentral region is injured, various aphasic syndromes appear. The retrocentral region is the parietal-temporal lobe except the superior part of the parietal lobe and the anterior part of the temporal lobe, which latter two regions when injured do not allow any marked aphasic disorder. Lesions of the middle or posterior temporal region are particularly important for speech, and produce more marked disorder than lesions of the angular gyrus or the[161] supramarginal gyrus. At first, words cannot be spoken, for a period of a fortnight to three months. Speech returns progressively, with an increased power of comprehension. At the same time, the patients begin to read and write. But there is no further spontaneous progress after a period of six or eight months, and then special reëducation must be started. These speech disorders of retrocentral (parietal-temporal) origin are either aphasic syndromes or slight remains of psychical disorders, or again, a disorder practically limited to alexia. The true aphasic syndromes concern the spoken word, understanding the words, writing, and calculation. The disorder is not especially dysarthric and consists particularly in loss of vocabulary. It might be called an amnestic aphasia (Pitres). These cases have well-marked intellectual disorder and their power of calculation is especially poor. As to the aphasic traces, which are more important to understand than they are extensive in point of fact, they relate particularly to calculating power, to vocabulary (slowness in finding words), and to reading (reading without comprehension). As to the cases of alexia, these are cases of lesions of the posterior part of the parietal-temporal lobe, and are usually accompanied by a hemi- or a quadrantanopsia.
Fifth: When the retrocentral area is damaged, different types of aphasia can occur. The retrocentral area refers to the parietal-temporal lobe, excluding the upper part of the parietal lobe and the front part of the temporal lobe. Damage in these two areas doesn’t typically cause significant aphasia. Lesions in the middle or back part of the temporal region are particularly crucial for speech and create more pronounced issues than lesions in the angular gyrus or the [161] supramarginal gyrus. Initially, patients may be unable to speak for about two weeks to three months. Speech begins to return gradually, along with an improved ability to understand. At the same time, patients start to read and write. However, there is usually no further natural improvement after six to eight months, and specific rehabilitation needs to begin. The speech issues from the retrocentral (parietal-temporal) area can manifest as either aphasic syndromes or minor remnants of psychological disorders, or they may be mostly related to alexia. The true aphasic syndromes involve difficulties with spoken language, understanding words, writing, and math. The disorder isn’t typically dysarthric but mainly involves a loss of vocabulary. This type of aphasia might be referred to as amnestic aphasia (Pitres). These individuals often exhibit clear intellectual difficulties, especially with math. As for the aphasic traces, which are more crucial for understanding than they are widespread, they mainly pertain to calculations, vocabulary (difficulty finding words), and reading (reading without understanding). Regarding cases of alexia, these are associated with lesions in the back part of the parietal-temporal lobe and are usually accompanied by a hemi- or quadrantanopsia.
To sum up, cases with central lesions (precentral and postcentral gyrus) have hemiplegia and a Broca aphasia without much tendency to cure. Cases with lesions anterior to the central convolutions have a transient anarthria and their recovery is ordinarily complete. Cases with retrocentral lesions have an aphasia suggestive of Wernicke’s aphasia, and ordinarily leave behind them extensive defects in intelligence and language. These cases should be taken account of from the standpoint of compensation, since they are much worse off for work than many cases with amputations; and though their disorder looks slight, it quite interferes with working at a trade. From the point of view of military effectiveness, the retrocentral cases are not very good soldiers, and especially not good officers, as they do not understand commands completely.
To sum up, cases with central lesions (precentral and postcentral gyrus) result in hemiplegia and Broca's aphasia with little tendency to improve. Cases with lesions in front of the central convolutions experience a temporary inability to speak and usually recover completely. Cases with retrocentral lesions present with Wernicke’s aphasia and typically leave behind significant impairments in intelligence and language. These cases should be considered in terms of compensation, as they are often worse off in the workplace than many individuals with amputations; and even though their condition might seem minor, it seriously disrupts their ability to work in a trade. From a military effectiveness standpoint, the retrocentral cases are not very effective soldiers, and particularly not good officers, as they struggle to fully understand commands.
Neuropsychiatric phenomena in rabies.
Neuropsychiatric symptoms in rabies.
Case 118. (Cardinal's Attic, Legrand, Benoît, September, 1917.)
A farmer, 34, mobilized in veterinary work, fell sick at a station for sick horses, April 25, 1917. He breakfasted well, drank coffee, and went to the abreuvoir at eleven o’clock. He told his mates that he felt bad in his head. He fainted over a table at the eating house, refused to eat or drink. At noon he went out into the court, vomited and went to lie down. A physician thought he was suffering from angina because of the pronounced dysphagia. He entered the hospital at eleven o’clock at night on the 25th. He was found next morning on his back, with a fixed and haggard look, crimson face, masseter and phalangeal spasm at times. Respiration irregular, interrupted by moans. The pulse would go up to 120 during agitation and then go down to 50 as soon as the patient lay down again. Pupils slightly dilated and unequal. As the patient came from a sick horse dépôt, the first question was that of tetanus, suggested somewhat by the jactitation of the limbs and the trismus. A violent headache began and the patient cried out, “My head! My head!” Painful vomiting movements, with very slight bilious material. Convulsive movements increased. The pulse was slow. The diagnosis “meningitis” was suggested, despite the absence of fever and the absence of Kernig’s sign. Lumbar puncture gave limpid fluid with a normal lymphocytosis, without increase of albumin or reducing substance. The bacteriological smear and culture were negative.
A 34-year-old farmer involved in veterinary work fell ill at a location for sick horses on April 25, 1917. He had a good breakfast, drank coffee, and went to the trough at eleven o’clock. He told his colleagues that he felt unwell in his head. He fainted over a table at the mess hall and refused to eat or drink. At noon, he went outside, vomited, and lay down. A doctor thought he was suffering from angina due to severe difficulty swallowing. He was admitted to the hospital at eleven o’clock that night. The next morning, he was found lying on his back, with a fixed and haggard expression, a red face, and occasional spasms in his jaw and fingers. His breathing was irregular, interrupted by moans. The pulse rose to 120 during agitation and then dropped to 50 as soon as he lay down again. His pupils were slightly dilated and unequal. Since the patient came from a sick horse depot, the first concern was tetanus, suggested by the twitching of his limbs and jaw clenching. A severe headache started, and the patient exclaimed, “My head! My head!” He experienced painful vomiting, with only a little bile. The convulsions worsened. The pulse was slow. A diagnosis of meningitis was considered, despite the lack of fever and the absence of Kernig’s sign. A lumbar puncture revealed clear fluid with normal lymphocyte levels, no increase in albumin, or reducing substances. The bacteriological smear and culture were negative.
Soon another sort of symptoms appeared. The patient would rise, cry out, threaten his neighbors. He was calmed with morphine. There were periods of excitement alternating with periods of calmness, during which he would reply sharply but accurately, being somewhat vexed by the questions, and would walk up and down without offering a word. When a glass of water was offered to him, as soon as his glance met the glass his eyes expressed fear. He drew back in repulsion[163] and cried out in terror. When the liquid was out of his sight the hydrophobic spasm ceased. This hyperesthesia of the sensorium was so intense that the mere sight of the shining glassware of the laboratory brought out a sharp crisis.
Soon, another set of symptoms appeared. The patient would get up, shout, and threaten his neighbors. He was calmed with morphine. There were times of excitement alternating with calm periods, during which he would respond sharply but accurately, clearly annoyed by the questions, and would pace back and forth without saying a word. When a glass of water was offered to him, as soon as he saw the glass, his eyes showed fear. He recoiled in disgust and yelled in terror. When the liquid was out of his sight, the hydrophobic spasm stopped. This heightened sensitivity was so intense that just seeing the shiny glassware in the lab triggered a severe crisis.
He was sent that evening to the neuropsychiatry center, walking jerkily and as if slightly drunk, with a number of small gesticulations and murmurings. He was immediately isolated, undressed himself and went to bed. He did not move in his bed, and seemed to sleep. The next day he got up, dressed and had a small spell of excitement, but was quiet enough on the medical visit, though the floor was soiled with urine and vomitus and the clothing was in disorder. He now had a pronounced phase, deep sunk eyes, drawn features and anxious look; dilated pupils and an expression of mixed fear and anger. His breathing was hard and he kept his hand on his heart. He was oriented. He suddenly rose and said, “I am thirsty.” A glass of milk was given him. He hesitated a moment, plunged his mouth and hands into it and aspirated the drink without making any swallowing movements. He pushed away the glass, spat a little, and vomited a small quantity of a black liquid. Then followed an anxious crisis, and he fell upon his side, absolutely immobile, without breathing for a few seconds. Again in the sitting posture, he was taken with contractions of the limbs and face. The tendon reflexes were at this time normal.
He was sent that evening to the neuropsychiatry center, walking awkwardly and seeming a bit drunk, with lots of small gestures and murmurs. He was immediately isolated, undressed, and went to bed. He didn’t move in his bed and appeared to be sleeping. The next day, he got up, dressed, and experienced a brief moment of excitement, but remained calm enough during the medical visit, even though the floor was dirty with urine and vomit and his clothes were disheveled. He now had a noticeable phase, with deeply sunken eyes, drawn features, and an anxious expression; his pupils were dilated, and his face showed a mix of fear and anger. Breathing heavily, he kept his hand on his heart. He was aware of his surroundings. Suddenly, he got up and said, “I am thirsty.” He was given a glass of milk. He hesitated for a moment, then plunged his mouth and hands into it, drinking without swallowing properly. He pushed the glass away, spat a little, and then vomited a small amount of black liquid. After that, he had a panic attack and fell onto his side, completely still, and stopped breathing for a few seconds. When he sat up again, he had spasms in his limbs and face. The tendon reflexes were normal at that time.
A quarter of an hour later the attendant found him dead, in the sitting posture, leaning against the wall, mouth open, arms dependent, hands extended, pupils dilated—a death in syncope. The brain was found congested. There was a slight effusion of blood over the posterior aspect of the brain. There were no hemorrhages or softenings in the brain substance. The muscles were of a dark red to black. The adherent lungs were very slightly congested at the base. The stomach contained a quarter of a liter of black, inodorous fluid in which there was much bile and little blood. There were numerous small hemorrhages of the mucosa near the great curvature. The spleen was large, the liver congested. The Pasteur Institute confirmed the diagnosis of rabies. There is no history of the man’s having been bitten by a dog.
A quarter of an hour later, the attendant found him dead, sitting upright, leaning against the wall, mouth open, arms hanging down, hands extended, pupils dilated—a death from fainting. The brain was congested. There was a small amount of blood over the back of the brain. There were no hemorrhages or soft spots in the brain tissue. The muscles were a dark red to black. The lungs were mildly congested at the base. The stomach held a quarter of a liter of black, odorless fluid that contained a lot of bile and a little blood. There were several small hemorrhages in the mucosa near the greater curvature. The spleen was enlarged, and the liver was congested. The Pasteur Institute confirmed the diagnosis of rabies. There is no record of the man being bitten by a dog.
Tetanus: Psychosis.
Tetanus: Mental health crisis.
Case 119. (Lumière and Astier, 1917.)
A soldier wounded May 18, 1916, was given antitetanic serum May 26th. The wounds healed, but on June 16, that is, 29 days after the trauma, contractures began, at first localized. There had been numerous wounds of legs and scrotum by shell fragments and the contractures were limited to the right leg and scrotum. There was no trismus or any lumbar symptom.
A soldier who was injured on May 18, 1916, received antitetanic serum on May 26th. The wounds healed, but on June 16, 29 days after the injury, contractures started, initially localized. He had multiple wounds on his legs and scrotum from shell fragments, and the contractures were confined to his right leg and scrotum. There was no jaw clenching or any lower back symptoms.
During the next few days the contractures became general, the temperature rose, a shell fragment was found by X-ray at the root of the thigh and was surgically extracted. B. tetani was found upon inoculation of media with material from the shell fragment. Persulphide of soda and antitetanic serum 90 cc. in three days were given intravenously. The temperature fell and the general health was greatly improved. July 6, hallucinations and terrors, worse at night, set in. The man believed himself surrounded by flames, that daggers were being plunged into his old wounds, that his hair was being pulled. These symptoms lasted a fortnight only, whereupon the patient recovered.
Over the next few days, the contractures became widespread, the temperature increased, and an X-ray revealed a shell fragment lodged in the thigh, which was surgically removed. B. tetani was detected after inoculating media with material from the shell fragment. Persulphide of soda and 90 cc of antitetanic serum were administered intravenously over three days. The temperature dropped, and the overall health improved significantly. On July 6, hallucinations and nightmares began, becoming worse at night. The man felt surrounded by flames, believed that daggers were stabbing his old wounds, and thought his hair was being pulled. These symptoms lasted for only two weeks, after which the patient recovered.
This case and six others accompanied by cerebral disturbances all recovered, and all the patients retained a perfect memory of their delirium and of their hallucinations.
This case, along with six others that involved brain issues, all recovered, and all the patients had a complete memory of their delirium and their hallucinations.
The chronological distribution of these cases was odd. One case was found early in the war; then no other cases of cerebral disorder presented themselves until the group observed at the end of 1916. Besides flames and daggers, zoöpsia was several times observed. One of the cases showed these symptoms without having been given antitetanic serum.
The timeline of these cases was strange. One case was identified early in the war; then no other cases of brain issues appeared until the group noted them at the end of 1916. In addition to flames and daggers, zoöpsia was observed several times. One of the cases showed these symptoms without having received antitetanic serum.
Re tetanus in the war, see in the Collection Horizon a book by Courtois-Suffit and Giroux on Les formes anormales du tétanos.
Regarding tetanus in the war, see in the Collection Horizon a book by Courtois-Suffit and Giroux on Les formes anormales du tétanos.
Tetanus fruste versus hysteria.
Tetanus fruste vs. hysteria.
Case 120. (Claude and Lhermitte, 1915.)
Claude and Lhermitte describe a condition of tetanos fruste. The neck was absolutely rigid. The patient had not been wounded in any way and, being regarded as a pure neuropath, was sent to the Centre Neurologique at Bourges.
Claude and Lhermitte describe a condition of tetanos fruste. The neck was completely stiff. The patient hadn’t sustained any injuries and, seen as purely a neuropath, was referred to the Centre Neurologique in Bourges.
The differential diagnosis lay between true tetanus and the hysterical pseudotetanus or pseudomeningitis. In pseudotetanus there is a contracture of the superficial and deep neck muscles, especially the trapezii, sternomastoid, and deep muscles. The condition somewhat suggests that of acute meningitis or tetanus, and especially suggests tetanus because it is often associated with masseter contracture (hysterical trismus). The head is immobile, stiff, and inclined backward; eyes directed above, throat slightly prominent. Upon attempts to move the head, intense pain occurs. The pain and contracture sometimes even suggest a suboccipital Pott’s disease. This form of hysterical pseudotetanus is of sudden onset, as a rule following burial in a trench or else contusion, or a slight wound in the cervical region. Pressure on the spinous processes produces no pain, nor does a blow upon the head; and an X-ray examination will definitely eliminate the hypothesis of Pott’s disease.
The differential diagnosis was between true tetanus and hysterical pseudotetanus or pseudomeningitis. In pseudotetanus, there's a contraction of the superficial and deep neck muscles, especially the trapezius, sternocleidomastoid, and deep muscles. This condition somewhat resembles acute meningitis or tetanus, particularly suggesting tetanus because it’s often linked with masseter contraction (hysterical trismus). The head is immobile, stiff, and tilted backward; the eyes look upward, and the throat is slightly protruding. When attempts are made to move the head, intense pain occurs. The pain and contraction may even indicate suboccipital Pott’s disease. This type of hysterical pseudotetanus usually has a sudden onset, often following burial in a trench or a blow, or a minor injury to the neck area. Pressing on the spinous processes doesn’t cause pain, nor does a hit to the head; and an X-ray will clearly rule out Pott’s disease.
To return to the Claude-Lhermitte case of limited true tetanus: It showed marked modifications in the tendon and bone reflexes. Upon percussion of the zygoma, of the occiput, or of the clavicle, there was a marked further contraction in the contractured muscles. Although there was no apparent spasticity in the legs, there was an ankle clonus and a bilateral patella clonus, combined with a distinct exaggeration of all bone and tendon reflexes. In such cases also there is hyperexcitability of the nerves and muscles to faradic and galvanic currents.
To revisit the Claude-Lhermitte case of limited true tetanus: It showed significant changes in the tendon and bone reflexes. When the zygomatic arch, occiput, or clavicle were tapped, there was a noticeable increase in contraction of the tight muscles. While there was no visible spasticity in the legs, there was ankle clonus and bilateral patellar clonus, along with a clear exaggeration of all bone and tendon reflexes. In these cases, there is also increased sensitivity of the nerves and muscles to faradic and galvanic currents.
An officer’s letter concerning local tetanus.
An officer's letter about local tetanus.
Case 121. (Turrell, January, 1917.)
The following letter from an officer who had had local tetanus and was treated by Turrell by ionization Dec. 6 and 7, 1915, by diathermia Dec. 7 to 22, and occasionally by static breeze ionization and chlorine ion to relieve contractions from Dec. 29, 1915, to Feb. 4, 1916. The tetanus was in the muscles of the legs. Of course diathermia is a purely symptomatic treatment and does not replace antitoxin serum or other specific treatment; thus its effect in relieving the contractions of local tetanus is precisely like its effect in the treatment of sciatic neuritis or lumbago.
The following letter is from an officer who had local tetanus and was treated by Turrell using ionization on December 6 and 7, 1915, diathermy from December 7 to 22, and occasionally with static breeze ionization and chlorine ion to ease contractions from December 29, 1915, to February 4, 1916. The tetanus was in the leg muscles. Diathermy is purely a symptomatic treatment and does not substitute for antitoxin serum or other specific treatments; therefore, its effect in easing the contractions of local tetanus is similar to its effect in treating sciatic neuritis or lumbago.
November 15, 1916.
November 15, 1916.
“Dear Major Turrell,
“Hi Major Turrell,
“I have been meaning to write to you for some time, as I knew you would be interested to hear how I was getting on. Your letter has just been received, and I am only too happy to give you any information I can with regard to my leg. I was wounded in the left leg on October 13, 1915, by high explosive shell, and arrived at Oxford on October 22. There was no operation as the surgeon in charge did not consider it advisable to remove the pieces of shell: my leg seemed to be getting better, and after about a month I was able to hobble round with sticks. My foot at this time used to swell a great deal towards night, and the foot seemed then to gradually stiffen up with violent pains at intervals, this gradually spread up the whole leg to about the knee, and I was compelled to take to my bed again. The pain at times was very bad, similar to a very bad attack of cramps, and then my leg became rigid and stiff, and at other times used to get horrible jumps and it was impossible to keep it still, and whenever the doctor or nurse looked at it it used to stiffen up at once. The night seemed to be the worst, and consequently I got very little sleep. I often had to get up in the middle of the night on crutches to try and obtain relief, my leg was so cramped and sore. It was about this time that you first visited me and prescribed a course of electric treatment for my leg, and I shall never be able to thank you enough for the relief it gave me. I cannot remember the names of the different treatments, but the first one—diathermy, or heat pads—certainly relieved the pain, and after the first two or three visits to you I got immense relief. I never looked back after this, and, although the progress was slow, I gradually lost all pain and was able to get sleep at night. The nervous jumps slowly disappeared and my leg became gradually normal except for contraction of the tendons. I was unable to straighten my ankle or knee, and it was thought at one time that my tendo Achillis would have to be severed. Gradually the knee straightened and I was able to get my heel to the ground. I was for some time on crutches, and was able to leave the hospital on February 5, 1916, walking with sticks.… I am now able to walk comfortably, but am unable to flex the ankle more than at right angle to my leg. The circulation is not very good, and I feel anything tight round my calf. I am still getting Boards, and have not been passed fit for overseas yet.”
"I've been wanting to write to you for a while since I knew you'd be interested in how I'm doing. I just received your letter, and I'm more than happy to give you any updates on my leg. I was injured in my left leg on October 13, 1915, by a high-explosive shell, and I arrived in Oxford on October 22. No surgery was performed because the surgeon didn't think it was wise to remove the shell fragments; my leg seemed to be improving, and after about a month, I was able to get around with crutches. During that time, my foot often swelled up in the evenings and would become stiff with intense pain at intervals, which spread up to my knee, forcing me back to bed. The pain was sometimes awful, like a severe case of cramps, and my leg would become rigid and stiff; at other times, it would twitch uncontrollably, making it impossible to keep it still, and it would immediately stiffen whenever the doctor or nurse looked at it. Nights were the worst, so I barely got any sleep. I often had to get up in the middle of the night on crutches to find some relief because my leg was so cramped and sore. It was around this time that you visited me for the first time and recommended a series of electric treatments for my leg, and I'll never be able to thank you enough for the relief it provided. I can't recall the names of the various treatments, but the first one—diathermy, or heat pads—definitely helped ease the pain, and after the first couple of visits to you, I felt significant relief. I never looked back after that, and even though progress was slow, I gradually became pain-free and was able to sleep at night. The nervous spasms slowly faded away, and my leg returned to almost normal, except for some tendon contraction. I couldn't fully straighten my ankle or knee, and there was a time when they thought my Achilles tendon might have to be cut. Slowly, my knee straightened, and I was able to get my heel on the ground. I used crutches for some time and was discharged from the hospital on February 5, 1916, walking with sticks. I can now walk comfortably, but I still can't flex my ankle beyond a right angle to my leg. The circulation isn't great, and I feel discomfort if anything is tight around my calf. I'm still getting boards, and I haven't been deemed fit for overseas yet."
VI. SOMATOPSYCHOSES
(THE SYMPTOMATIC, NON-NERVOUS, GROUP)
Dysentery: Psychosis.
Dysentery: Mental illness.
Case 122. (Loewy, November, 1915.)
Out of a large number of dysentery patients, many of whom had very serious symptoms, but one of Loewy’s patients became psychotic. Loewy in fact had discharged this one as normal, and he had been put on the wagon train (no opium or alcohol) to go to a sanatorium. As the fighting shifted, the sanatorium site changed and could not be reached with the wagon. Finally, the wagon train met the battalion once more and Loewy was told that the man was “dying.” At this time he was afebrile, without collapse symptoms, with a strong and normally frequent pulse, and with few signs of exhaustion. Yet the guard had thought that he looked moribund. Both upper eyelids were drawn rigidly up but conveyed a different impression from that in maniacal or anxious conditions. The expression was that of staring astonishment, helplessness, and apathetic lack of orientation. The patient recognized Loewy, spoke to him as “Herr Doctor,” said he was doing quite well; he was found to be well oriented. There was no fabricating tendency even as to the number of stools (although Loewy had noted such in bad dysenteries of the Shiga-Kruse type). He was apparently hard of hearing, as if at the beginning of a typhoid fever. He showed a retardation in his intake of ideas, and his voice in answering sounded absent-minded. There was an expression of absent-mindedness, and the patient seemed markedly unconcerned about his health, the direction of the journey, the terrible rain, etc. These phenomena are attributed by Loewy to attention disorder.
Out of a large number of dysentery patients, many of whom had very serious symptoms, one of Loewy’s patients became psychotic. Loewy had actually discharged this patient as normal, and he had been placed on the wagon train (no opium or alcohol) to go to a sanatorium. As the fighting shifted, the sanatorium location changed and could not be reached by the wagon. Eventually, the wagon train rejoined the battalion, and Loewy was informed that the man was “dying.” At that moment, he was without fever, showed no signs of collapse, had a strong and normal pulse, and exhibited few signs of exhaustion. However, the guard thought he appeared near death. Both of his upper eyelids were held open rigidly but conveyed a different impression than someone in a maniac or anxious state. Instead, his expression showed a stare of astonishment, helplessness, and a lack of awareness. The patient recognized Loewy, addressed him as “Herr Doctor,” claimed he was doing quite well; he was found to be well oriented. There was no tendency to fabricate information, even regarding the number of stools (although Loewy had noted such tendencies in severe dysentery cases of the Shiga-Kruse type). He seemed to be hard of hearing, as if at the onset of typhoid fever. He displayed a delay in processing ideas, and his responses sounded distracted. His demeanor reflected a lack of focus, and he appeared to be significantly unconcerned about his health, the journey ahead, the terrible rain, and so on. Loewy attributed these phenomena to a disorder of attention.
The patient had been out of reach of fire for days. Loewy reports the case as one of beginning amentia or as an exhausted state resembling a Korsakow condition, recalling one of emotional hyperesthetic weakness (Bonhoeffer).
The patient had been out of reach of fire for days. Loewy reports the case as one of early dementia or as an exhausted state resembling a Korsakoff condition, which recalls a kind of emotional hypersensitivity and weakness (Bonhoeffer).
Typhoid fever: Hysteria.
Typhoid fever: Panic.
Case 123. (Sterz, December, 1914.)
A soldier entering hospital for typhoid fever, October 2, 1914, was discharged to another hospital and again, November 10, to a hospital for nervous disease. The typhoid was serious and complicated by delirium. After defervescence, the patient was weak and could not stand or walk, especially on account of pains and weakness in the left leg. Sometimes he had had pains in the sacrum and left hip. He complained of tinnitus, deafness, dizziness, headache. He said he had fallen from a cart, had been sick for three months, since which time he had been under medical treatment for his present condition. He had, he said, been given a small pension.
A soldier admitted to the hospital for typhoid fever on October 2, 1914, was transferred to another hospital and again on November 10, to a hospital for nervous disorders. The typhoid was severe and complicated by delirium. After the fever broke, the patient was weak and unable to stand or walk, particularly due to pain and weakness in his left leg. Occasionally, he experienced pain in his lower back and left hip. He reported symptoms of ringing in the ears, hearing loss, dizziness, and headaches. He mentioned that he had fallen from a cart and had been sick for three months, during which he had been receiving medical treatment for his current condition. He stated that he had been awarded a small pension.
The gait disorder sometimes amounted to a real astasia-abasia. The left leg became stiff and was dragged behind. There was a paresis demonstrable in dorsal decubitus, of the left side, especially of the leg, without atrophy. There was a hypesthesia of the whole left side of the body, with the exception of the head. Hyperesthesia of the left leg, hip and upper sacrum. The left corneal reflex was diminished. Moody, hypochondriacal, lachrymose. The general attitude of the patient was affected and theatrical. Paradoxical innervations were frequently found on test. There was no neurological disorder except for the absence of the right Achilles jerk.
The walking issue sometimes resulted in a real inability to stand or walk. The left leg became stiff and dragged behind. There was noticeable weakness when lying on the back, particularly in the left leg, but no muscle wasting. The entire left side of the body felt less sensitive, except for the head. There was increased sensitivity in the left leg, hip, and upper sacrum. The left corneal reflex was reduced. The patient was moody, hypochondriacal, and tearful. Their overall attitude was affected and dramatic. Unusual nerve responses were often seen during tests. There was no neurological issue except for the absence of the right Achilles reflex.
The absence of this Achilles jerk may be regarded as a residuum of the previous accident. The localization of the pains points to a neurotic lumbosacral plexus disorder on the left side. Superimposed upon this picture are the hysterical phenomena. The typhoid fever and its attendant neuritis are therefore to be interpreted as the liberating factor for a severe hysteria in a subject already disposed to such symptoms through previous accident.
The lack of this Achilles reflex might be seen as a leftover from the earlier injury. The area where the pain occurs suggests a neurotic issue with the lumbosacral plexus on the left side. Adding to this situation are the hysterical symptoms. The typhoid fever and its related neuritis should be viewed as the triggering factor for a severe hysteria in someone who was already prone to such symptoms from the past injury.
Dementia praecox versus post-typhoidal encephalitis.
Dementia praecox vs. post-typhoidal encephalitis.
Case 124. (Nordman, June, 1916.)
A butcher, 29 (aunt insane, sister melancholy, one child stillborn, deformed), had had several days convulsions at eight; went through military service without incident; was at the Marne and was evacuated October 19, 1914, with typhoid fever,—a severe fever with a delirium prolonged into the last weeks. Three months convalescent leave was given, passed at Paris with the man’s aunt, but he had become strange. One day he wanted to strangle neighbors of German origin; another day departed for Dunkirk and then returned, having lost all his documents.
A 29-year-old butcher (with an insane aunt, a melancholy sister, and one stillborn child who was deformed) had convulsions for several days when he was eight. He went through military service without issues, fought at the Marne, and was evacuated on October 19, 1914, due to typhoid fever—a severe illness with delirium that lasted into the final weeks. He was granted three months of medical leave, which he spent in Paris with his aunt, but he had become strange. One day he wanted to strangle neighbors of German descent; another day he left for Dunkirk and later returned, having lost all his documents.
February, 1915, he went back to the front, did strange things and was soon evacuated to Tarascon. In April he went back to his dépôt; May 18, to the hospital at Rennes for erythema. June 15, he was given 15 days in prison for setting off a cannon too quickly and then running off through the fields. August 11, he was interned at Rennes for stealing a priest’s cap. September 12, two months convalescence. December 10, headaches. Back to Rennes January 14, February 18, Val-de-Grâce, then Maison Blanche.
In February 1915, he returned to the front lines, did some odd things, and was soon evacuated to Tarascon. In April, he went back to his unit; on May 18, he went to the hospital in Rennes for erythema. On June 15, he received a 15-day prison sentence for firing a cannon too quickly and then running off through the fields. On August 11, he was confined in Rennes for stealing a priest's cap. On September 12, he had two months of recovery. On December 10, he experienced headaches. He went back to Rennes on January 14, and on February 18, he was at Val-de-Grâce, then Maison Blanche.
Here he was found sometimes sad, immobile; at other times laughing and singing. He was very irritable on small occasion. Once on leave he had a fugue with complete amnesia, though alcohol may account for the latter. His memory was vague, especially for his crimes and for recent events. He was emotional, indifferent even in the presence of his wife or aunt. Sexual indifference. He often complained of his head, saying that he felt it blocked and that he could not think. The headache was frontal and would last several hours. The man would, however, not complain spontaneously. He was physically, in general, negative.
Here he was sometimes found feeling sad and still; at other times, he was laughing and singing. He got really irritable over minor things. Once, while he was on leave, he experienced a fugue state with total amnesia, although alcohol might explain that. His memory was fuzzy, especially regarding his crimes and recent events. He was emotional but indifferent, even around his wife or aunt. He showed a lack of interest in sex. He often said he had a headache, describing it as feeling blocked and that he couldn't think clearly. The headache was located in the front of his head and could last for several hours. However, he wouldn’t complain unless prompted. Overall, he seemed physically negative.
This case might possibly be due to a post-typhoidal encephalitis, but Nordman believes rather that it is a case of dementia praecox. Perhaps the convulsions at eight produced a slight brain lesion, brought to an issue by the typhoid fever.
This case might be due to post-typhoidal encephalitis, but Nordman thinks it’s more likely a case of dementia praecox. Maybe the seizures at eight caused a minor brain injury, triggered by the typhoid fever.
Paratyphoid fever: Psychosis outlasting fever.
Paratyphoid fever: Psychosis persists after fever.
Case 125. (Merklen, December, 1915.)
A Breton farmer, 34, had paratyphoid alpha. Admitted to hospital September 3, 1915, he had headache, anorexia, asthenia, coated tongue and tense abdomen, algosuria; later, abdominal swelling, borborygmi in the right iliac fossa, rose spots, dicrotism, albuminuria, bronchitic rales. The disease was severe, and was complicated by sacral decubitus and ran a month.
A 34-year-old Breton farmer was diagnosed with paratyphoid alpha. He was admitted to the hospital on September 3, 1915, experiencing headaches, loss of appetite, weakness, a coated tongue, a tense abdomen, and painful urination. Later, he developed abdominal swelling, rumbling sounds in the right lower abdomen, rose spots on his skin, a dicrotic pulse, and protein in his urine, along with bronchial wheezing. The illness was severe and was complicated by pressure sores on his lower back, lasting for a month.
At first somnolent, September 8th the patient went into a state of mental excitement with agitation and delirium. He got out of bed, cried out, sang, talked to his neighbors, complained that his papers (colis) had been stolen, as well as his watch and tobacco; that his horses’ hoofs had been injured, and the like.
At first, the patient was drowsy, but on September 8th, he became mentally agitated and delirious. He got out of bed, shouted, sang, talked to those around him, and complained that his papers had been stolen, along with his watch and tobacco; he also said that his horses' hooves had been hurt, among other things.
He grew calmer in a few days, and now no longer tried to get up, remaining inert in his bed. The occupation delirium persisted—he was not being paid what he owed, and the like. He had hallucinations; looked for scissors, and one day said, “Here they are!” At intervals he appeared lucid and responded appropriately to questions.
He became calmer after a few days and no longer attempted to get up, staying still in his bed. The delusions about work continued—he wasn't being paid what he was owed, among other things. He experienced hallucinations, searched for scissors, and one day exclaimed, “Here they are!” At times, he seemed clear-headed and answered questions appropriately.
The fever dropped and the paratyphoid disease appeared past, but the mental state remained for three weeks without change, having the same periods of lucidity when he would be regarded as cured, but falling again forthwith into his post oniric ideas. He was soon sent to a convalescent hospital and was not wholly well for another month.
The fever went down and the paratyphoid illness seemed to have passed, but his mental state stayed the same for three weeks without any change. He had moments of clarity when he was seen as cured, but then he quickly fell back into his confusing thoughts. He was soon sent to a recovery hospital and wasn’t completely well for another month.
Psychopathic taint brought out by paratyphoid fever.
Psychopathic effects triggered by paratyphoid fever.
Case 126. (Merklen, December, 1915.)
A soldier, 31, was a victim of paratyphoid alpha, entering hospital October 21, 1915, with the usual symptomatology: fever, asthenia, headache, abdominal swelling, tongue coated and red along its edges, diarrhoea. After admission he passed into a deep toxic state.
A 31-year-old soldier was diagnosed with paratyphoid alpha and was admitted to the hospital on October 21, 1915, showing typical symptoms: fever, weakness, headache, abdominal swelling, a coated tongue with red edges, and diarrhea. After being admitted, he entered a severe toxic state.
He woke up in the night with a cry, got up afraid, and refused to go back into his own bed. He was mute, except for curses addressed to the nurses. After two hours he went to bed and to sleep. Next day he sat quietly with a depressed look, occasionally groaning deeply, talking in brief phrases about his anxiety, wanting his wife telephoned to, saying that he would not see his children, was going into the four planks, and the like.
He woke up in the middle of the night with a shout, got up scared, and wouldn’t go back to his own bed. He didn’t say much, except for swearing at the nurses. After two hours, he got back in bed and fell asleep. The next day, he sat quietly with a sad expression, occasionally groaning loudly, speaking in short phrases about his worries, wanting them to call his wife, saying that he didn’t want to see his kids, that he was heading into the coffin, and so on.
This situation lasted about a week. He became afraid of medicines and thought he had been poisoned, saying that he would rather be shot than poisoned and complaining that, though he had served France for fourteen months, they now wanted to kill him. In the night time he was agitated. He gave vent to cries, and threats, but this delirious state rapidly decreased and he became calm the night of September 27th. The upper extremities showed a tendency to catatonia. From this time forth, during the remaining month, the patient was immobile, mute, fearful, and mistrusting, depressed and always wore a cunning look. His disorientation decreased and he passed good nights. He would answer questions by groaning. He would say, “They think I am a Tartar.” The end of the mental disorder coincided with the cure of the paratyphoid fever. According to Merklen, the paratyphoid bacillus in these cases serves to bring out a psychopathic taint. This particular patient had always been of a sad demeanor, uncommunicative, very impressionable and emotional. Two other cases had always been somewhat below normal.
This situation lasted about a week. He became afraid of medications and thought he had been poisoned, saying he would rather be shot than poisoned and complaining that, even though he had served France for fourteen months, they now wanted to kill him. At night, he was agitated. He cried out and made threats, but this delirious state quickly faded, and he became calm on the night of September 27th. His upper limbs showed signs of catatonia. From that point on, during the remaining month, the patient was immobile, silent, fearful, and mistrustful, depressed and always had a cunning look. His disorientation lessened, and he started to have better nights. He would respond to questions with groans. He would say, “They think I am a Tartar.” The end of the mental disorder coincided with the recovery from paratyphoid fever. According to Merklen, the paratyphoid bacillus in these cases serves to reveal a psychopathic tendency. This particular patient had always been somber, uncommunicative, very impressionable, and emotional. Two other cases had always been somewhat below normal.
Diphtheria: Post-diphtheritic symptoms.
Diphtheria: Post-diphtheria symptoms.
Case 127. (Marchand, 1917.)
A farmer, 37, was evacuated March 20, 1916, for diphtheria. April 1, paralysis of tongue and uvula, impairment of vision. These symptoms rapidly improved, but paralysis of the legs appeared and then of the arms. This paralysis lasted until he was sent to the neurological center June 28 for post-diphtheritic paralysis, wherein it was found that voluntary movements of the legs could be performed, though painfully and of slight extent, that walking was impossible, that there was a considerable atrophy of legs and arms, that the knee-jerks, Achilles jerks and plantar reflexes were absent. There was complaint of pains in the legs and over nerve trunks.
A 37-year-old farmer was evacuated on March 20, 1916, due to diphtheria. On April 1, he experienced paralysis of the tongue and uvula, along with impaired vision. These symptoms improved quickly, but then he developed paralysis in his legs and later in his arms. This paralysis lasted until he was transferred to the neurological center on June 28 for post-diphtheritic paralysis. It was determined that he could perform voluntary movements of his legs, although they were painful and limited. Walking was impossible, and there was significant atrophy in his legs and arms. His knee-jerks, Achilles jerks, and plantar reflexes were absent. He also complained of pain in his legs and along the nerve trunks.
Improvement followed, the atrophy gradually passed away, and the voluntary movements of the legs became more extensive; but by October the reflexes had not yet reappeared. Yet the patient had begun to walk on crutches and soon was able to get on with canes only. The improvement did not continue. He did not raise his heels and dragged his toes. There was now a clonic tremor of the legs as soon as the weight of the body was put on them. During movements of legs carried on in dorsal decubitus there was found an irregular tremor of the legs with twisting of the trunk. The muscular strength was well preserved. There was a slight muscular atrophy. The tendon reflexes had now come back, though the right Achilles jerk was weak and the plantar reflexes were absent. There was a hypalgesia of the legs which ceased sharply at the middle of the thighs. There was a slight hypoacusia on the left side. Visual fields normal. The patient complained of feelings in the inside of his bones. Electrical reactions normal.
Improvement followed, the muscle wasting gradually faded away, and the voluntary movements of the legs became more extensive; however, by October the reflexes still hadn’t come back. Yet the patient had started to walk with crutches and soon was able to use just canes. The improvement didn’t last. He didn’t lift his heels and dragged his toes. Now there was a clonic tremor of the legs as soon as weight was put on them. When moving his legs while lying on his back, there was an irregular tremor of the legs accompanied by twisting of the trunk. Muscle strength was well preserved, though there was slight muscle wasting. The tendon reflexes had returned, but the right Achilles reflex was weak and the plantar reflexes were absent. There was decreased sensitivity in the legs that stopped abruptly midway up the thighs. There was slight hearing loss on the left side. Visual fields were normal. The patient reported feeling sensations inside his bones. Electrical responses were normal.
Diphtheria: Hysterical paraparesis.
Diphtheria: Panic-induced paraparesis.
Case 128. (Marchand, 1917.)
A soldier, 24, was evacuated June 24, 1915, from Roussy for diphtheria and was treated by serum, receiving 80 cc. in 8 injections. A few days later there was a paralysis of the uvula with regurgitation of liquids from the nose; but patient was able to go on convalescence July 21. A few days later, however, he noticed that his legs were weak. Vertigo, vomiting and painful walking followed, and his convalescence was increased a month. The paralysis got progressively worse. September 10, he went by automobile to Libourne where he stayed two months. He arrived at the Neurological Center at Bordeaux November 9 with diagnosis “polyneuritis of legs.” He could not walk and could hardly flex thighs on pelvis or legs on thighs. Voluntary movements of extension and flexion of feet and toes were limited. There was neither atrophy, pain nor reflex disorder. Both legs were analgesic, as was also the abdomen up to the umbilicus. There was complaint of dorsolumbar pains and of stomach trouble and lack of appetite; vomiting after meals frequent, pulse 120.
A 24-year-old soldier was evacuated on June 24, 1915, from Roussy due to diphtheria and was treated with serum, receiving 80 cc across 8 injections. A few days later, he experienced paralysis of the uvula, causing liquids to regurgitate from his nose; however, he was able to start recovering on July 21. A few days after that, he noticed weakness in his legs. This was followed by vertigo, vomiting, and painful walking, extending his recovery by another month. The paralysis got progressively worse. On September 10, he traveled by car to Libourne, where he stayed for two months. He arrived at the Neurological Center in Bordeaux on November 9 with a diagnosis of "polyneuritis of legs." He was unable to walk and could barely flex his thighs on his pelvis or his legs on his thighs. His voluntary movements for extending and flexing his feet and toes were limited. There was no atrophy, pain, or reflex issues. Both legs and his abdomen up to the umbilicus were numb. He reported dorsolumbar pain, stomach issues, and lack of appetite; vomiting after meals occurred frequently, and his pulse was 120.
January 3, the patient was able to lift his legs a few centimeters above the bed but not together. There was now a slight muscular atrophy especially on the left side. Knee-jerks lively, analgesia limited to legs, no vomiting, pulse rapid.
January 3, the patient was able to lift his legs a few centimeters above the bed, but not together. There was now a slight muscle atrophy, especially on the left side. Knee reflexes were lively, there was limited numbness in the legs, no vomiting, and the pulse was rapid.
The patient was sent to a hospital in the country May 8 to July 8. He was now much better. His legs were able to support his body but he could not walk. Slight atrophy of left leg. There was hypalgesia now in the feet and legs below the knee. There was no pain on pressure over the nerve trunks. The electric reactions normal. The patient could now walk on crutches. He was invalided on the temporary basis, December 12, 1916.
The patient was admitted to a hospital in the countryside from May 8 to July 8. He was feeling much better now. His legs could support his body, but he couldn’t walk. There was slight atrophy in the left leg. He experienced reduced sensitivity in the feet and legs below the knee. There was no pain when pressure was applied to the nerve trunks. The electric responses were normal. The patient could now walk using crutches. He was deemed temporarily disabled on December 12, 1916.
It does not appear that in this case the hysterical paralysis was preceded by polyneuritis.
It doesn’t seem like the hysterical paralysis in this case was preceded by polyneuritis.
Malaria: Amnesia.
Malaria: Memory loss.
Case 129. (De Brun, November, 1917.)
A soldier lost all memory of his hospital stay in Salonica and the voyage home. He could only remember a little about the hospital at Bandol. There is a period of transition to full memory in malarial cases characterized by sure memory, vague on certain points, alternating with phases of almost complete amnesia. The soldier in question had very inexact memories of the Bandol Hospital, and could only remember about his fevers, that they began about noon and terminated about four o’clock. Twice he had been found in his shirt, walking, unconscious, in the passageway of the hospital. Having obtained leave for convalescence, three months after his memory gap began, he went to Paris, and probably had attacks at home. He vaguely remembered afterward being carried by automobile to the Pasteur Hospital, December 1. There he remained to the end of March, 1917, without preserving anything but the vaguest memories of an intermediary period of more than six months. The memory in these malarial cases often remains permanently altered and there may even be a retrograde amnesia, carrying back to facts prior to the gap and an anterograde amnesia relative to facts after the main gap.
A soldier forgot everything about his hospital stay in Salonica and the journey home. He could only remember a little about the hospital in Bandol. There’s a transition period to full memory in cases of malaria, marked by clear memories that are fuzzy on certain details, alternating with phases of nearly complete amnesia. The soldier in question had very unclear memories of the Bandol Hospital and could only recall that his fevers started around noon and ended around four o’clock. Twice, he was found in his shirt, wandering unconscious in the hospital hallway. After getting leave for recovery, three months after his memory loss began, he went to Paris and likely had episodes at home. He vaguely remembered being taken by car to the Pasteur Hospital on December 1. He stayed there until the end of March 1917, retaining only the faintest memories of a more than six-month period in between. Memory in these malaria cases often remains permanently altered, and there may even be retrograde amnesia, which goes back to events before the memory gap, as well as anterograde amnesia concerning events that happened after the main gap.
Thus, there is in the febrile period a retrograde amnesia and in the post-febrile period a retrograde or anterograde amnesia. One group of subjects are severe cerebral cases, and the memory gap appears to run back to a period of true mental confusion. But there is another group of patients who preserve throughout the febrile period an absolute consciousness of all acts, and yet the memory gap is just as sharp and definite as in the confusional cases.
Thus, during the fever phase, there is retrograde amnesia, and in the post-febrile phase, there is either retrograde or anterograde amnesia. One group of subjects consists of severe brain injury cases, and the memory loss seems to go back to a time of real mental confusion. However, there is another group of patients who maintain complete awareness of everything happening during the fever phase, yet their memory gap is just as distinct and pronounced as in the confused cases.
Malaria: Korsakow syndrome.
Malaria: Korsakoff syndrome.
Case 130. (Carlill, April, 1917.)
A stoker, 45, was admitted to the Royal Naval Hospital, Haslar, November 6, 1916, from the Fifteenth General Hospital in Alexandria, to which he had come from a hospital in Bombay about three weeks before. At Alexandria he was anemic and showed an edema of legs which had been present for six weeks. Cylindruria; no albuminuria. At Haslar there was no cylindruria and no edema, and nothing but weakness, gouty arthritis of left wrist, right ear and left great toe. Red cells 4,650,000, leucocytes 10,000 (52 per cent polymorphonuclear, 46 per cent lymphocytes). He was rather dull mentally. December 10th, Dr. Fildes found malarial organisms in the blood on the occasion of a hyperpyrexia (104°). Quinine was given. December 14th, he was transferred neurological. According to the patient’s own story, he was born June 10, 1868, lived in Fulham, had a daughter aged 12 years, had recently seen his wife at the hospital: all this seemed plausible enough.
A 45-year-old stoker was admitted to the Royal Naval Hospital, Haslar, on November 6, 1916, from the Fifteenth General Hospital in Alexandria, where he had arrived from a hospital in Bombay about three weeks earlier. In Alexandria, he was anemic and had swelling in his legs that had been occurring for six weeks. There was cylindruria but no albuminuria. At Haslar, there was no cylindruria or swelling, only weakness, gouty arthritis in his left wrist, right ear, and left big toe. His red blood cell count was 4,650,000, and his white blood cell count was 10,000 (52% polymorphonuclear, 46% lymphocytes). He was somewhat mentally sluggish. On December 10th, Dr. Fildes discovered malarial organisms in his blood during a high fever (104°). Quinine was administered. On December 14th, he was transferred for neurological evaluation. According to the patient's account, he was born on June 10, 1868, lived in Fulham, had a 12-year-old daughter, and had recently visited his wife at the hospital: all of this seemed quite believable.
Later, however, he said that the year was 1899, that King Edward was king, that the war was between England and some field forces, etc. This well-nourished, pale, simple-looking stoker spoke quietly and politely; told about intermittent fever; about being eight years on the active list, becoming a reservist and being called up for the war. He read intelligently, could do sums, but did not know the name of the hospital and was confused about the war. He recognized that his memory was not as it should be; constantly stroked his moustache and chin. He was happy and contented.
Later, though, he mentioned that the year was 1899, that King Edward was the king, and that the war was between England and some field forces, etc. This well-nourished, pale, and simple-looking stoker spoke quietly and politely; he talked about intermittent fever, about being on the active list for eight years, becoming a reservist, and being called up for the war. He read thoughtfully, could do math, but didn’t know the name of the hospital and was confused about the war. He recognized that his memory wasn’t what it should be; he constantly stroked his mustache and chin. He was happy and content.
The gait was normal, systolic blood pressure 140 mm.; no evidence of alcoholism. Blood, January 15, 1917, contained 5,050,000 reds, 10,300 leucocytes (63 per cent polymorphonuclear, 37 per cent lymphocytes). There was a bilateral absence of the ankle-jerks, repeatedly confirmed at subsequent examinations. Wassermann reaction was negative. Puncture fluid contained no cells.
The walking was normal, systolic blood pressure was 140 mm.; no signs of alcoholism. Blood from January 15, 1917, showed 5,050,000 red blood cells, 10,300 white blood cells (63 percent polymorphonuclear, 37 percent lymphocytes). There was a consistent lack of ankle reflexes, confirmed in multiple follow-up exams. The Wassermann test was negative. The fluid from the puncture showed no cells.
Instead of living at Fulham, this stoker lived at Portsmouth, and had not been seen by his wife for four years. He had done 18 years’ active service and had last sent his wife a letter from the Sailors’ Home at Bombay, November, 1916. They had been married 21 years. He caused astonishment with his wife and friends by announcing that Lord Roberts and General Buller were in command at the battle of the Falklands. He continued to say that he lived at Fulham. He was discharged home, January 22. It seems as if he were living through the period of the Boer war.
Instead of living in Fulham, this stoker lived in Portsmouth and hadn't seen his wife in four years. He had served actively for 18 years and last sent his wife a letter from the Sailors’ Home in Bombay in November 1916. They had been married for 21 years. He surprised his wife and friends by announcing that Lord Roberts and General Buller were in charge at the Battle of the Falklands. He went on to say that he lived in Fulham. He was discharged home on January 22. It felt like he was stuck in the time of the Boer War.
Carlill considers that alcoholism may be ruled out, and there is no likelihood that the gout was the cause of the neuritis. He believes that the neuritis was probably malarial. Possibly the illness suffered in Bombay may have been beriberi or it may have been malarial nephritis.
Carlill believes that alcoholism can be dismissed, and it’s unlikely that gout caused the neuritis. He thinks the neuritis was probably due to malaria. It’s possible that the illness experienced in Bombay was either beriberi or malarial nephritis.
A complication of malaria.
A malaria complication.
Case 131. (Crepe, August, 1916.)
A Senegalese corporal of machine gunners, 21 (early life normal save for sore throats and coughing), was a robust, well-developed man of 75 kilos when he entered the hospital at Konakry, February 15, 1916. He was given the diagnosis: malarial anterior spinal paralysis.
A 21-year-old Senegalese corporal in the machine gun unit, whose early life was typical except for sore throats and coughing, was a strong, well-built man weighing 75 kilos when he was admitted to the hospital in Konakry on February 15, 1916. He was diagnosed with malarial anterior spinal paralysis.
It seems that he had joined a Colonial regiment, April 8, 1915, attended classes as a recruit, left Bordeaux November 1 for Dakar, arriving there November 11. He stayed there some sixteen days, during which time he slept without mosquito-netting. November 16, he left for Konakry, and had his first febrile symptoms November 27, with vomiting, headache, and prostration. His temperature ran as high as 41, but by December had fallen to normal, after quinine.
It looks like he joined a Colonial regiment on April 8, 1915, attended training as a recruit, and left Bordeaux on November 1 for Dakar, arriving there on November 11. He stayed there for about sixteen days, during which he slept without a mosquito net. On November 16, he left for Konakry and experienced his first fever symptoms on November 27, including vomiting, headache, and extreme fatigue. His temperature reached as high as 41, but by December, it had returned to normal after taking quinine.
The corporal was sent away, cured, to his company at Kouronesa, December 6. There was more fever, headache, and vomiting during the railway trip. Quinine again relieved the fever, but a bloody diarrhoea set in so that it was only at the end of January that he could go on service.
The corporal was sent back, healed, to his company at Kouronesa on December 6. He experienced more fever, headaches, and vomiting during the train ride. Quinine once again eased the fever, but he started having bloody diarrhea, so it wasn't until the end of January that he could return to duty.
February 6, another attack of fever, with shivering and perspiration, lasted for some three hours. He could hardly stand by himself and had to be helped in walking. Next day, another spell of three hours of fever; definite paralysis set in, affecting both legs. February 8 the arms were attacked by paralysis which, unlike that of the legs, was a progressive one, attacking first the shoulders, then the elbows, the wrists, and finally the hands. All the body muscles were in a state of flaccid paralysis, as well as the muscles of the face. The patient was now afebrile. February 9 there was a slight speech defect; the tongue was slightly paralyzed, and swallowing became painful. The jaw movements remained normal. The muscles of the face were intact and the patient could whistle, move his lips, and move his eyeballs normally. Vision normal. The pupils were fixed in dilatation, more widely on the left side. There was a slight[179] contracture of the vesical sphincter, necessitating the catheter. The tendon and cutaneous reflexes were lost.
On February 6, he had another fever attack with shivering and sweating that lasted about three hours. He could barely stand on his own and had to be assisted while walking. The next day, he experienced another three-hour fever; definite paralysis had set in, affecting both legs. By February 8, paralysis had spread to his arms, which progressed differently than in his legs, first impacting the shoulders, then the elbows, wrists, and finally the hands. All of his body muscles were in a state of flaccid paralysis, including the facial muscles. At this point, the patient was no longer febrile. On February 9, he showed a slight speech defect; his tongue was slightly paralyzed, and swallowing became painful. Jaw movements were still normal. The facial muscles remained intact, and he could whistle, move his lips, and move his eyeballs normally. His vision was normal, but his pupils were fixed and dilated, more so on the left side. There was a slight[179]contracture of the bladder sphincter, requiring a catheter. His tendon and cutaneous reflexes were absent.
By February 14, when the patient was sent to the Bellay Hospital, muscular atrophy had made its appearance. No plasmodia could now be found in the blood, which showed 71 per cent polynuclear leukocytes, 20 per cent mononuclears, 9 per cent lymphocytes.
By February 14, when the patient was sent to Bellay Hospital, muscular atrophy had started to show up. No plasmodia were detectable in the blood, which displayed 71 percent neutrophils, 20 percent mononuclears, and 9 percent lymphocytes.
This state lasted til February 25. Despite the fact that the patient ate well, emaciation rapidly progressed. The buttock showed a very few signs of decubitus. Upon this date there was pain from a marked orchitis of the left side, the cause for which remains unknown (no history of gonorrhœa; catheter used for the last time, February 15). The temperature which attended the orchitis came down in three days; the patient’s appetite was singularly good, but the muscular atrophy increased. The speech defect meantime disappeared, and the patient swallowed more readily.
This condition lasted until February 25. Even though the patient was eating well, they quickly lost weight. The buttock showed very few signs of bedsores. On that date, there was pain from significant inflammation of the left testicle, the cause of which is still unknown (no history of gonorrhea; last catheter use was on February 15). The fever associated with the inflammation subsided in three days; the patient's appetite was surprisingly good, but muscle wasting increased. Meanwhile, the speech issue disappeared, and the patient was swallowing more easily.
March 7 a slight and hardly perceptible movement could be noted in the fingers of the left hand. Two days later, similar movements appeared in the right. March 11 he could spread his fingers in a kind of creeping movement. Next day slight movements were possible with the legs, and March 13 the knees were movable. March 14 the patient could lift his head from the pillow. The range of movement now increased all over the body. According to the patient, those parts were the first to regain power that had been attacked last. This certainly seemed to be the case with respect to the left upper limb, in which first the hand and wrist, then the elbow and shoulder, successively recovered power. The legs regained their power in the same way proximad. March 17 the patient could sit up and grasp objects with the left hand. The cremaster and plantar reflexes appeared,—the former, more on the right; the latter, more on the left. The left pupil remained in wider dilatation than the right.
March 7, there was a slight and barely noticeable movement in the fingers of the left hand. Two days later, similar movements showed up in the right hand. On March 11, he could spread his fingers in a sort of creeping motion. The next day, he was able to make slight movements with his legs, and on March 13, he could move his knees. By March 14, the patient was able to lift his head off the pillow. The range of movement began to increase all over his body. According to the patient, the parts that had been affected last were the first to regain strength. This definitely seemed true for the left upper limb, where the hand and wrist recovered power first, followed by the elbow and shoulder. The legs regained strength in the same order, moving upward. By March 17, the patient could sit up and grasp objects with his left hand. The cremaster and plantar reflexes were present; the cremaster reflex was stronger on the right side, while the plantar reflex was stronger on the left side. The left pupil remained more dilated than the right.
The treatment was by quinin and potassium iodide, with massage. The patient was apparently on the highroad to complete recovery, and left for France March 21, weighing 63 kilos.
The treatment involved quinine and potassium iodide, along with massage. The patient seemed to be on the path to complete recovery and left for France on March 21, weighing 63 kilos.
Trench-foot: Acroparesthesia.
Trench foot: Acroparesthesia.
Case 132. (Cottet, September, 1917.)
A fantassin, 36, carpenter by trade, went into the trenches October, 1914, and had two attacks of trench-foot, first in January, 1915, when there was a painful swelling of the foot and secondly in July, 1916, when there were some bullae on the dorsal aspect of the feet. These were not serious and the fantassin did not report sick.
A foot soldier, 36, a carpenter by trade, went into the trenches in October 1914 and suffered two episodes of trench foot: the first in January 1915, when his foot swelled painfully, and the second in July 1916, when blisters formed on the top of his feet. These weren't serious, and the foot soldier didn't report sick.
He was wounded, August 27, 1916, by shell fragment on the right elbow, was evacuated to the ambulance where the fragment was extracted and then to a hospital which he left cured with a seven days’ leave. Although he had not suffered in any way from his feet while in hospital, and had not been exposed to cold, the bullae reappeared on the feet just as they had been in July. They in fact now formed a sort of exanthem occupying symmetrically the dorsal surfaces of the toes. The bullae contained serum. They were confluent, varying from pin head to a nut in size, were as a rule round, but sometimes irregular. The eruption went on to a cure rapidly and on the twelfth day the bullae had dried up. This patient had hypesthesia up to the knees, hypesthesia of the dorsal surfaces of the feet, hyperesthesia of the plantar surfaces and ankles, hypesthesia of the forearm and the elbow and of the dorsal surfaces of the hands with possibly exaggerated sensibility of the palma surfaces. Hypesthesia of the face was limited to a small part of the right ear. The reflexes were normal and there was no atrophy. The name “paresthetic trench acrotrophodynia” was given to it.
He was injured on August 27, 1916, by a shell fragment on his right elbow. He was taken to the ambulance where the fragment was removed, then transferred to a hospital, from which he left fully recovered with a seven-day leave. Although he hadn’t experienced any issues with his feet while in the hospital and hadn’t been exposed to cold, the blisters came back just like they had in July. They had actually formed a kind of rash that symmetrically covered the tops of his toes. The blisters were filled with serum and were merged together, varying in size from that of a pinhead to a nut; they were usually round but sometimes irregular. The rash healed quickly, and by the twelfth day, the blisters had dried up. This patient experienced reduced sensitivity up to the knees, reduced sensitivity on the tops of his feet, increased sensitivity on the bottoms of his feet and ankles, reduced sensitivity in his forearm and elbow, and on the tops of his hands, with possibly heightened sensitivity on the palms. Reduced sensitivity in his face was confined to a small area on the right ear. His reflexes were normal, and there was no muscle wasting. It was termed “paresthetic trench acrotrophodynia.”
In a service of eighty beds Cottet found within two months fifteen instances of these acroparesthetic disorders regarded as neuritic changes in trench-foot of a latent and lasting character which would have remained unobserved unless there were disorders of sensibility. In fact similar disorders of sensibility may be found without any history of gelure des pieds, forming a latent type of neuritic alteration hardly noticed by the patient himself. In twenty-six cases Cottet found sixteen with hypesthesia of the ears and of the nose.
In an eighty-bed facility, Cottet discovered fifteen cases of these acroparesthetic disorders within two months, viewed as nerve changes in trench foot that are hidden and persistent, and would have gone unnoticed if not for sensitivity issues. In fact, similar sensitivity disorders can occur even without any history of gelure des pieds, creating a subtle type of nerve alteration that the patient hardly notices. In twenty-six cases, Cottet found sixteen with reduced sensitivity in their ears and nose.
Bullet injury of spine; bronchopneumonia: état criblé of spinal cord.
Bullet injury of the spine; bronchopneumonia: damaged condition of the spinal cord.
Case 133. (Roussy, June, 1916.)
As to the development of eschars, Roussy reports the case of a lieutenant wounded September 25, 1915. There was a penetrating wound of the interscapular region. The bullet had entered on the posterior aspect of the right scapular region and had emerged at the level of the first dorsal vertebra. October 1, a neurological examination showed flaccid paraplegia, knee-jerks normal, Achilles jerk weak on the right, plantar reflexes flexor, cremasteric reflex absent on the right, and both abdominal reflexes absent. There were pains in the legs and arms. There was retention of urine with overflow. A slight dulness on the right; temperature from 38 to 39 degrees.
As for the development of eschars, Roussy describes the case of a lieutenant who was wounded on September 25, 1915. He had a penetrating wound in the area between his shoulder blades. The bullet entered through the back of his right shoulder and exited at the level of the first dorsal vertebra. On October 1, a neurological exam revealed flaccid paraplegia, normal knee-jerks, a weak Achilles reflex on the right, flexor plantar reflexes, and an absent cremasteric reflex on the right, along with absent abdominal reflexes on both sides. He experienced pain in his legs and arms. There was urinary retention with overflow, slight dullness on the right side, and a temperature ranging from 38 to 39 degrees.
Four weeks later the knee-jerks had become very weak, and the Achilles jerks were now absent. There was an extensive diffuse atrophy of the lower leg and thigh muscles, and a hypesthesia of pronounced degree had developed throughout the legs, over the buttocks, and in the lumbar region. Anal and vesical sphincters relaxed; dejections voluminous; sacral decubitus as well as healed eschars. December 5, the patient was transferred to the Army neurological center; temperature rose; there was much expectoration; paracentesis yielded no fluid; pneumococcus in the sputum. Cystitis had developed despite extreme care. Extensive edema of the legs developed. There was increased dulness on the right side, coughing and dyspnea. Death, January 17.
Four weeks later, the knee reflexes had become very weak, and the Achilles reflexes were now absent. There was significant muscle wasting in the lower leg and thigh, and a notable loss of sensation had occurred throughout the legs, over the buttocks, and in the lower back. The anal and bladder sphincters were relaxed; there were large bowel movements; pressure sores had developed as well as previously healed ones. On December 5, the patient was moved to the Army neurological center; the temperature increased; there was a lot of coughing up phlegm; a procedure to remove fluid yielded none; pneumococcus was found in the sputum. A bladder infection had developed despite careful management. There was also significant swelling in the legs. There was increased dullness on the right side, along with coughing and shortness of breath. Death occurred on January 17.
The autopsy showed a bronchial pneumonia of the right lower lobe, confluent, imitating a lobar pneumonia. The left lung also showed extensive confluent bronchopneumonia at the base as well as disseminated areas and edema of the middle and apical portions. Infectious splenitis, large fatty liver, swollen kidneys, no pyonephritis.
The autopsy revealed bronchial pneumonia in the right lower lobe, which was dense and resembled lobar pneumonia. The left lung also displayed widespread bronchopneumonia in the base, along with scattered areas and swelling in the middle and upper sections. There was infectious splenitis, an enlarged fatty liver, swollen kidneys, but no signs of pyonephritis.
The spinous processes of the 6th and 7th cervical vertebrae[182] were injured. There was no obvious gross disease within the theca except that there was a slight adhesion between the dura mater and the anterior surface of the spinal cord at the level of the 7th cervical and highest dorsal vertebrae. There was, however, a depression on the anterior surface of the spinal cord at a lower level, namely, at the level of the 4th dorsal vertebra. Microscopic examination showed myelomalacia with small cavities in the 1st and 4th dorsal segments, suggesting the état criblé.
The spinous processes of the 6th and 7th cervical vertebrae[182] were damaged. There was no clear disease visible within the protective covering, except for a small adhesion between the dura mater and the front surface of the spinal cord at the level of the 7th cervical and the highest dorsal vertebrae. However, there was an indentation on the front surface of the spinal cord at a lower level, specifically at the level of the 4th dorsal vertebra. Microscopic examination revealed myelomalacia with small cavities in the 1st and 4th dorsal segments, indicating the état criblé.
According to Roussy, these patients injured in the spinal region are particularly sensitive to cold and support transfer badly even when the disease is short. Such patients should be evacuated to the interior after the shortest delay possible. Sometimes these patients show rib fractures; these are in the posterior portions of the ribs and are due to the fall of the man when struck. It might be possible even that the spinal lesions should through the action of the sympathetic nervous system favor lung infection.
According to Roussy, patients with spinal injuries are especially sensitive to cold and struggle with transfers, even if their condition is not long-lasting. These patients should be moved to a warmer location as quickly as possible. Occasionally, these patients may have rib fractures, typically located on the back parts of the ribs, caused by falling when they were hit. It's also possible that the spinal injuries could trigger lung infections due to the effects of the sympathetic nervous system.
Shell-explosion: Hystero-organic symptoms; decubitus; radicular sensory disorder.
Shell explosion: Hystero-organic symptoms; bed sores; nerve root sensory disorder.
Case 134. (Heitz, May, 1915.)
A soldier, 32, was bowled over in a first-line trench by the bursting of a shell that he did not see coming, September 14, 1914. He regained consciousness only in the middle of the night, finding himself half covered with water. He was taken up by the stretcher-bearers at eleven in the morning. Paralysis in the legs was then absolute. There were pains in the legs and in the back, but there was no evident lesion. Knee-jerks, plantar reflexes, and abdominal reflexes absent; cremasteric reflex absent on the left, weak on the right. Tactile sensations, on the contrary, were almost intact except for a slight diminution over the feet and the external aspects of the lower legs. Sensitiveness to pin-prick, however, was abolished throughout both lower extremities, and diminished in the abdomen and back up to two or three centimeters above the level of the umbilicus; that is, including the territory of the first lumbar and the last three dorsal roots. Sensibility to heat was abolished in the feet, the external aspect of the lower legs, and the posterior aspect of the thighs, but was preserved in the second and third lumbar territory, in the anterior aspect of the thighs, as well as in the region below the umbilicus. Micturition was impossible. Constipation the first few days yielded spontaneously September 20. There were signs in the bases of both lungs, corresponding with a suffocating feeling. September 22, he was evacuated, almost well, without signs of pulmonary congestion, having regained the power of urination and some capacity to move the legs sidewise. February, 1915, after evacuation to a hospital at Vic, he showed sacral decubitus, soon reaching the size of a hand, as well as trochanteric decubitus; traces of albumin in the urine, sacral and sciatic pains (recalcitrant to morphine).
A 32-year-old soldier was knocked down in a front-line trench by a shell explosion that he didn’t see coming on September 14, 1914. He regained consciousness only in the middle of the night, finding himself partially submerged in water. Stretcher-bearers picked him up at eleven in the morning. He had complete paralysis in his legs. He felt pain in his legs and back, but there were no visible injuries. Knee-jerk, plantar, and abdominal reflexes were absent; the cremasteric reflex was absent on the left side and weak on the right. However, his sense of touch was mostly intact, except for a slight reduction over his feet and the outer parts of his lower legs. He had no sensitivity to pin-pricks in both lower limbs and diminished sensitivity in his abdomen and back up to two or three centimeters above his belly button, affecting the area of the first lumbar and last three thoracic nerve roots. He couldn't feel heat in his feet, the outer parts of his lower legs, and the back of his thighs, but he maintained sensitivity in the second and third lumbar regions, in the front of his thighs, as well as below his belly button. He couldn’t urinate. Constipation during the first few days resolved on its own by September 20. There were signs in the lower parts of both lungs, which corresponded with a feeling of suffocation. On September 22, he was evacuated, nearly well, with no signs of lung congestion, having regained the ability to urinate and some movement in his legs to the side. In February 1915, after being moved to a hospital in Vic, he developed pressure sores on his sacrum that soon grew to the size of a hand, as well as pressure sores on his trochanters; there were traces of protein in his urine, and he experienced sacral and sciatic pain that didn’t respond to morphine.
He began to improve December 25. Camphorated oil and the sitting posture relieved the pulmonary congestion;[184] the temperature, which had oscillated round 38 degrees, fell; the decubitus scarred over; the knee-jerks reappeared to some extent, and movements began. February 5, the patient had become able to walk without crutches. There was still a two-franc sized area of decubitus over the sacrum, and still a little spinal pain in walking.
He started to improve on December 25. Camphorated oil and the sitting position helped ease the lung congestion; [184] his temperature, which had been around 38 degrees, decreased; the bed sore began to heal; his reflexes returned somewhat, and movement started. By February 5, he was able to walk without crutches. There was still a small area the size of a two-franc coin on his lower back, and he still experienced some back pain while walking.
It is difficult to consider this case only functional in view of the decubitus, to say nothing of the radicular distribution of the sensory disorder. Heitz brings this and the previously given case (No. 1) into relation with Elliot’s case of transient paraplegia (see Case 210) and Ravaut (see Case 201).
Shell-shock (windage?); typhoid fever; “neuritis” actually hysterical.
Shell shock (windage?); typhoid fever; “neuritis” is actually hysteria.
Case 135. (Roussy, April, 1915.)
A Colonial soldier was sent back from the front, September 12, 1914, for nervous disorder due to the shock of the windage of a bullet. He had not lost consciousness. Under observation at his station, he got typhoid fever, and was cared for at Paris from the beginning of October. About October 15 he began to feel pains in his left shoulder, neck, and arm. The diagnosis, neuritis, was made and was strongly borne in upon the patient, so that upon the cure of his typhoid, he went out on two months’ leave with a complete impotence and much pain of the left arm. At the end of his relief, he was evacuated to Villejuif. January 24, it was found that he had no somatic phenomena whatever, despite the fact that the left arm and a part of the forearm was powerless, and so painful that the patient cried out when his arm was moved. There were a few cracklings in the scapulo-humeral joint.
A Colonial soldier was sent back from the front on September 12, 1914, for a nervous disorder caused by the shock of a bullet passing nearby. He hadn't lost consciousness. While being observed at his station, he contracted typhoid fever and was treated in Paris starting in early October. Around October 15, he began experiencing pain in his left shoulder, neck, and arm. The diagnosis of neuritis was made, and this heavily impacted the patient, so that once his typhoid was cured, he took a two-month leave with complete weakness and significant pain in his left arm. After his leave, he was moved to Villejuif. On January 24, it was determined that he had no physical symptoms at all, even though his left arm and part of his forearm were completely weak and so painful that he cried out when his arm was moved. There were a few crackling sounds in the shoulder joint.
Hot air and reëducation cured the man in less than two months (March 20), though the disorder had lasted for four months. The patient had been retired for hysteria before the war and had re-enlisted.
Hot air and re-education cured the man in under two months (March 20), even though the issue had lasted for four months. The patient had been discharged for hysteria before the war and had re-enlisted.
Bullet wound of pleura: Reflex hemiplegia and double ulnar syndrome.
Bullet wound of pleura: Reflex hemiplegia and double ulnar syndrome.
Case 136. (Phocas and Gutmann, May, 1915.)
A soldier, 26, was wounded in the enfilading of an Argonne trench December 17, 1914. He felt the bullet like an electrical shock, and fell. He had been leaning forward at the time and suddenly felt the left half of his body go paralyzed and his mouth pulled to one side. He did not lose consciousness, and spat up a good deal of blood five minutes after falling. He lay in the trench all night, unable to move his left leg except by the aid of his right. He was evacuated next day. There was a five-franc piece wound at the upper border of the left scapula, four finger-breadths from the median line. There were a few lung signs which rapidly cleared up. December 28, the hemiplegia was better, although neurological examination showed weakness of left upper extremity, abolition of deep reflexes, and certain skin changes of the left hand with edema (main succulent), decreased resistance of muscles of lower extremity to passive motion, especially of adductors and flexors, exaggerated polykinetic left knee-jerk, ankle clonus, Babinski reflex, abdominal and cremasteric reflexes absent on left, platysma paralysis left, with complete paralysis in the inferior distribution of the facialis; whistling impossible. Also the left eye could not be closed singly. Synergic movements of the lower part of the paralyzed face when the right hand of the patient was grasped.
A 26-year-old soldier was injured in an ambush in an Argonne trench on December 17, 1914. He felt the bullet hit him like an electric shock and collapsed. He had been leaning forward and suddenly felt the left side of his body go numb and his mouth pull to one side. He stayed conscious and coughed up a lot of blood five minutes after he fell. He lay in the trench all night, unable to move his left leg without using his right leg for assistance. He was evacuated the next day. There was a five-franc coin-sized wound at the upper edge of his left shoulder blade, about four finger-widths from the middle of his back. He showed some lung signs that quickly cleared up. By December 28, his partial paralysis had improved, but a neurological exam revealed weakness in his left arm, loss of deep reflexes, and some skin changes on his left hand with swelling, decreased muscle resistance in the lower leg during passive movement, especially in the adductors and flexors, an exaggerated reflex in his left knee, ankle clonus, absent Babinski reflex, and absent abdominal and cremaster reflexes on the left. He also had left platysma paralysis with complete paralysis affecting the lower part of his face; he couldn't whistle. Additionally, he couldn't close his left eye on its own. There were coordinated movements in the lower part of his paralyzed face when his right hand was held.
There were also sensorimotor disorders in the ulnar distribution on both sides, with complete anesthesia to pin prick. There was also an area of hyperesthesia of the anterior and postero-internal aspect of the right forearm from below the elbow to the wrist. The tendon reflexes were weak but distinct on the right side. The left arm had feelings of pain, with élancements and formication from the shoulder to the fingers on the ulnar distribution. There was, of course, also, local hyperesthesia due to the wound of the thorax.
There were also sensorimotor issues in the ulnar area on both sides, with complete loss of feeling to pinpricks. There was an area of increased sensitivity on the front and back inner side of the right forearm, extending from below the elbow to the wrist. The tendon reflexes were weak but noticeable on the right side. The left arm experienced pain, with sharp sensations and a tingling feeling from the shoulder to the fingers in the ulnar area. Additionally, there was local sensitivity due to the chest wound.
Lumbar puncture showed a fluid normal in all respects. We deal with a hemiplegia of organic nature, associated with the bilateral ulnar syndrome. The hemiplegia followed the trauma immediately. When the ulnar phenomena appeared is unknown.
Lumbar puncture showed normal fluid in every way. We are dealing with an organic hemiplegia, linked to bilateral ulnar syndrome. The hemiplegia occurred right after the trauma. It is unclear when the ulnar symptoms appeared.
The lung complications cleared. The pains disappeared; motion returned up to the level of the facialis. The patient got up and three months later went on convalescence, still presenting Babinski, exaggerated knee-jerk and weak arm reflexes on the left side. The bilateral ulnar syndrome had disappeared six weeks after the patient entered hospital. Phocas and Gutmann cite a considerable literature on nerve complications of pleural trauma, among them syncopes of grave prognosis; a relatively frequent pleural epilepsy (forty-five per cent fatal) or epileptic status (seventy per cent fatal); and the rare hemiplegia. Accidents and death have followed exploratory puncture of the pleura. Air embolism is probably not the cause. Phocas and Gutmann prefer the theory of a reflex disorder starting from the pleura.
The lung issues resolved. The pain faded away; movement returned to the level of the facial nerve. The patient got up and three months later began recovery, still showing signs of Babinski, an exaggerated knee-jerk reflex, and weak arm reflexes on the left side. The bilateral ulnar syndrome had vanished six weeks after the patient was admitted to the hospital. Phocas and Gutmann reference a substantial amount of literature on nerve complications related to pleural trauma, including severe syncopes, relatively common pleural epilepsy (with a forty-five percent fatality rate) or epileptic status (with a seventy percent fatality rate), and the rare occurrence of hemiplegia. Accidents and fatalities have occurred following exploratory puncture of the pleura. Air embolism is likely not the cause. Phocas and Gutmann favor the theory of a reflex disorder originating from the pleura.
Hysterical tachypnoea.
Rapid breathing.
Case 137. (Gaillard, December, 1915.)
A man, 23, came to the Lariboisière November 29, 1915, in a hurry to show evidence that he had been invalided for valvular lesion of the heart. In point of fact, the interne found a murmur at the base. Yet there were things in the military papers suggesting caution. The patient next morning showed no malaise, dyspnoea, or any evidence of serious disorder. The contractions of the thorax beat in time with contractions of the alae of the nose, about 112 per minute. Here, then, was a cardiopulmonary patient. The heart impulse was exaggerated; the patient could not or would not stop breathing to aid the auscultation, but almost absolutely normal sounds could be heard at the apex and the base. A valvular lesion could be excluded. The lungs were perfectly normal. The patient was requested to stop his gymnastics, which might have succeeded elsewhere but could not at the Lariboisière!
A 23-year-old man came to the Lariboisière on November 29, 1915, eager to prove that he had been discharged due to a heart valve issue. In fact, the intern detected a murmur at the base of his heart. However, some details in his military records suggested caution. The next morning, the patient showed no signs of discomfort, shortness of breath, or any evidence of a serious condition. His chest contractions lined up with the movements of his nostrils, around 112 times per minute. Here was a case of a cardiopulmonary patient. The heart's beat was heightened; the patient could not or would not stop breathing to assist with the examination, but nearly normal sounds could be heard at the apex and the base. A valve issue could be ruled out. The lungs were completely normal. The patient was advised to stop his exercises, which might have worked elsewhere but definitely could not at the Lariboisière!
How could the man have established the synchronism of pulse and respiration and synchronous tachypnoea and tachycardia? Why should he persist in this form of sport, since he had already been invalided? The family history was not especially suggestive (father albuminuric, died at 59; mother well, probably tuberculous). Scarlet fever at eight; occupation, tourneur. After four months of service there was gastric disorder followed by typhoid fever (despite vaccination, according to the patient). Convalescent leave at Paris, during which leave he had swollen legs and albuminuria. May, 1915, gastric difficulty; valvular lesion determined; examination; invalided. At home, a variety of complaints, for which treatment was unsuccessful.
How could the man have determined the connection between his pulse and breathing, along with his rapid breathing and fast heart rate? Why did he continue this type of activity when he had already become ill? The family history wasn’t particularly telling (father had albuminuria and died at 59; mother was healthy but probably had tuberculosis). He had scarlet fever at eight; his job was a turner. After four months of service, he experienced stomach issues followed by typhoid fever (despite being vaccinated, according to him). He took convalescent leave in Paris, during which he had swollen legs and albuminuria. By May 1915, he had stomach problems; a heart valve issue was found; he was examined and decided unfit for service. At home, he had various complaints, for which treatment didn’t help.
During further examination it was noted that in auscultation the head of the examiner was lifted, as if there were hypertrophy of the heart or an aortic aneurysm. The synchronism was less exact on December 2; 112 beats to 128 respiration. Was this man a simulator? Had he become[189] the victim of his own enterprise? There was no evidence of simulation. It was a question of a monosymptomatic hysteria. Gaillard discontinued the manière forte and undertook a softer treatment, but the manière forte had caused the family to want to take him away. Perhaps they feared a too efficacious treatment. He then escaped observation. It is probable that the tachypnoea ceased during sleep. It was not so marked after the medical visit was over.
During further examination, it was observed that the examiner’s head was raised during auscultation, as if there were an enlargement of the heart or an aortic aneurysm. The synchronization was less precise on December 2; 112 beats to 128 breaths. Was this man just pretending? Had he become[189] a victim of his own performance? There was no evidence of deception. It was a case of monosymptomatic hysteria. Gaillard stopped the manière forte and started a gentler treatment, but the manière forte had made the family want to take him away. Perhaps they were afraid of too effective a treatment. He then went unnoticed. It’s likely that the rapid breathing stopped during sleep. It wasn’t as pronounced after the doctor’s visit was over.
Soldier’s heart.
Hero's heart.
Case 138. (Parkinson's disease, July, 1916.)
A corporal, 21, who had been a miner and entirely well up to enlistment in August, 1914, went to France in 1915. In June, came shortness of breath and palpitation on exertion; later, precordial pain (fifth space, between nipple and median line) and giddiness on walking. Like all cases of true so-called “soldier’s heart,” this soldier had no physical signs indicative of heart disease, yet reported sick for cardiac symptoms on exertion. In this particular case, as in about half of forty cases reported by Parkinson, there had been no disability in civil life.
A 21-year-old corporal, who had worked as a miner and was completely fit until he enlisted in August 1914, went to France in 1915. In June, he began experiencing shortness of breath and heart palpitations when exerting himself; later, he also had chest pain (in the fifth space, between the nipple and the middle line) and felt dizzy while walking. Like all true cases of what’s called “soldier’s heart,” this soldier showed no physical signs of heart disease, but he still reported sick due to cardiac symptoms during exertion. In this specific case, as with about half of the forty cases reported by Parkinson, there had been no disability during his civilian life.
August, 1915, the soldier was admitted to the casualty clearing station, where the apex beat was found in fifth intercostal space internal to the left nipple line. The first sound was duplicated in all areas. The second sound was duplicated, though not loudly, at the base. After nine months’ treatment, this man went back to light duty with slight symptoms.
August 1915, the soldier was taken to the casualty clearing station, where the apex beat was detected in the fifth intercostal space, just inside the left nipple line. The first sound was heard consistently in all areas. The second sound was also heard consistently, although not loudly, at the base. After nine months of treatment, this man returned to light duty with mild symptoms.
According to Parkinson, the absence of abnormal physical signs in the heart of a soldier should not prevent his discharge from the army if under training or on active service he shows breathlessness and precordial pain whenever he undergoes exertion well borne by his fellows. A simple exertion test, such as climbing 25 to 50 steps, reproduces the symptoms in such a patient. The rate of the heart at rest is a little higher than that of normal men, though the increase on exertion is greater. Nevertheless, it has been proved that the increase of rate on exertion bears no relation to the symptoms elicited and is therefore without value in judging the functional efficiency of the heart.
According to Parkinson, the lack of any abnormal physical signs in a soldier's heart shouldn’t stop him from being discharged from the army if he experiences breathlessness and chest pain during exertion that his peers handle fine. A simple test, like climbing 25 to 50 steps, can trigger these symptoms in such a patient. The resting heart rate is slightly higher than that of normal men, but the increase during exertion is more significant. However, it has been shown that the increase in heart rate during exertion does not correlate with the symptoms observed and is therefore not useful for assessing the heart's functional efficiency.
Soldier’s heart?
Soldier's heart?
Case 139. (Parkinson's disease, July, 1916.)
A sergeant, 36, had been in the army from 17 to 29, but in 1908 he had acute rheumatism and was discharged from the army. He then became a furnace man and had shortness of breath and palpitation on severe exertion with syncope three times.
A 36-year-old sergeant had served in the army from the age of 17 to 29, but in 1908 he suffered from acute rheumatism and was discharged. After that, he became a furnace worker and experienced shortness of breath, palpitations during intense physical activity, and fainting spells three times.
He re-enlisted in August, 1914, and had an attack of orthopnea and edema after exposure at a review. However, he improved and went to France in May, 1915, where he again had symptoms; namely, precordial pain and breathlessness on severe exertion. One day while carrying telephone wire under fire, the sergeant felt a sudden pain in the region of the apex beat, shooting down the right arm. “I thought I was shot.” He fell down, very short of breath. His left arm remained sore and weak. Two days later came a similar attack, this time with unconsciousness, and the left arm was now useless. Two days later he was admitted to hospital, where slight breathlessness but no pain and no enlargement of cardiac dulness could be found. No further details are available but it seems clear that this man is unfit for duty. According to Parkinson, it is probable that the infection indicates the presence of some degree of myocardial disease.
He re-enlisted in August 1914 and experienced shortness of breath and swelling after being exposed at a review. However, he improved and went to France in May 1915, where he had symptoms again, specifically chest pain and breathlessness during intense activity. One day, while carrying telephone wire under fire, the sergeant felt a sudden pain in the area of his heart, shooting down his right arm. "I thought I was shot." He collapsed, seriously short of breath. His left arm remained sore and weak. Two days later, he had a similar episode, this time losing consciousness, and his left arm became useless. Two days later, he was admitted to the hospital, where slight breathlessness but no pain and no enlargement of cardiac dullness was found. No further details are available, but it seems clear that this man is unfit for duty. According to Parkinson, it is likely that the infection indicates some degree of heart disease.
Strain and shell-shock: Acceleration of diabetes mellitus.
Strain and shell-shock: Speeding up diabetes.
Case 140. (Karplus, February, 1915.)
An infantryman, aged 22, previously healthy and from a healthy family, was struck by a shell fragment in the forehead and lay for several hours unconscious. He did not vomit. He had a number of furuncles on his body and his urine, upon examination, showed a severe diabetes mellitus which increased despite treatment. Upon an attempt to withdraw carbohydrate, the sugar suddenly sank from six to four per cent. Acetone at the same time increased. An abrasion had been noticed by the patient a few days before the shell explosion on the spot rubbed by the tornister. The patient said that since his accident he had had to urinate every night several times and was often very thirsty, neither of which tendencies had he had before. A month before he became merod he had had an injury of the hand produced by a shell fragment. He had undergone tremendous strain.
An infantryman, 22 years old, previously healthy and from a healthy family, was hit in the forehead by a shell fragment and lay unconscious for several hours. He didn’t vomit. He had several boils on his body, and his urine, when tested, showed severe diabetes that worsened despite treatment. When an attempt to reduce carbohydrates was made, his blood sugar dropped suddenly from six to four percent. At the same time, acetone levels increased. A few days before the shell explosion, the patient noticed a scrape in the area where his backpack had rubbed. He reported that since the accident, he had to urinate several times every night and was often very thirsty—both of which he hadn’t experienced before. A month before he became ill, he sustained a hand injury from a shell fragment. He had gone through a lot of stress.
The chances are that the excitement and the strain had more to do with the diabetes mellitus than the shell explosion.
The chances are that the excitement and the stress had more to do with the diabetes than the explosion.
Dercum’s disease.
Dercum's disease.
Case 141. (Hollande and Marchand, March, 1917.)
An adjutant in a chasseur battalion was buried by a shell explosion, which killed his lieutenant beside him, January 5, 1915, at Hartmannsweilerkopf. Hematuria followed; ten days later, fever with anorexia, and the appearance of two or three lipomata on the anterior surface of the thighs. Remaining at his post, the adjutant took part in an attack, March 5; was evacuated on the 8th; “lipomatosis with febrile reactions.” He spent eight days at Bussang, and thence went to the hospital at Pont-de-Claix. Here marked albuminuria was noted; the lipomata increased in volume; others appeared in the arms. The patient was transferred to the Des-Genettes, where the diagnosis nephritis was added to the previous diagnosis, and a milk diet was prescribed. Convalescence of five months was proposed. The lipomata increased in volume and in number. The patient was then hospitalized at Avenue Berthelot, placed in the auxiliaries, and stationed eight months at his dépôt.
An adjutant in a chasseur battalion was buried by a shell explosion, which killed his lieutenant next to him, on January 5, 1915, at Hartmannsweilerkopf. He experienced blood in his urine shortly after; ten days later, he had a fever and loss of appetite, along with the appearance of two or three fatty tumors on the front of his thighs. Staying at his post, the adjutant participated in an attack on March 5 and was evacuated on the 8th, diagnosed with “lipomatosis and fever.” He spent eight days at Bussang and then went to the hospital at Pont-de-Claix. There, significant albumin in the urine was noted; the fatty tumors increased in size, and more developed in his arms. The patient was transferred to Des-Genettes, where nephritis was added to his previous diagnosis, and a milk diet was recommended. A convalescence period of five months was suggested. The fatty tumors continued to grow in size and number. The patient was then hospitalized at Avenue Berthelot, placed in the auxiliaries, and spent eight months at his depot.
When he was observed by Hollande and Marchand, four nut-sized tumors were found on the anterior surface of the left thigh; two smaller tumors: one of them painful to pressure, lay on the inner aspect, another the size of a small egg lay in the right thigh, and there were two others on the internal aspect and two on the external aspect of the thigh. A nut-sized tumor was found on the inner border of the right forearm, and below it another lenticular tumor. A nut-sized tumor was found on the left forearm below the elbow on the internal border. Small tumors were found on the buttocks. There were no tumors below the knees, in the upper arms, or on the thorax. There were 14 tumors in all. The smaller the tumor the more sensitive, and there was more pain when the tumor had just appeared and during the first days of its growth. There was no spontaneous pain; pain only upon a blow or pressure. Diminished knee-jerks, especially the right; no other neurological disorder, although the patient complained of often having something before his[194] eyes. There was a marked diminution in the memory. Heart was in the 5th space on the nipple line, pulse 110; Wassermann reaction negative; red blood cells, 3,520,000, white cells, 6500; albuminuria, hematuria, leucocytes, and urethral cells in the urine. The temperature had now become normal. The lateral lobes of the thyroid were slightly larger than normal, but not painful. Sella turcica was unchanged upon X-ray. Exploratory puncture of a tumor showed much free fat, without fatty acid crystals and with some fat cells. The cells could not be cultivated in test tube. The authors believe it doubtful whether this instance of Dercum’s disease is related with the shell explosion.
When Hollande and Marchand examined him, they found four nut-sized tumors on the front of his left thigh; two smaller tumors: one of which was painful to touch, located on the inner side, and another the size of a small egg on the right thigh. There were two additional tumors on the inner side and two on the outer side of the thigh. A nut-sized tumor was found on the inner edge of his right forearm, with another lenticular tumor below it. On his left forearm, below the elbow, there was a nut-sized tumor on the inner border. Small tumors were also found on the buttocks. No tumors were present below the knees, in the upper arms, or on the chest. In total, there were 14 tumors. The smaller the tumor, the more sensitive it was, and there was increased pain when the tumor first appeared and in the initial days of its growth. There was no spontaneous pain; discomfort was only felt when struck or pressed. Knee reflexes were diminished, particularly on the right; no other neurological issues were noted, though the patient reported frequently seeing something before his[194]eyes. His memory significantly decreased. The heart was positioned in the 5th intercostal space along the nipple line, with a pulse of 110; Wassermann test was negative; red blood cell count was 3,520,000, and white blood cell count was 6,500; there was albumin in the urine, blood in the urine, and the presence of leukocytes and urethral cells. His temperature had returned to normal. The lateral lobes of the thyroid were slightly enlarged but not painful. The sella turcica showed no changes on X-ray. An exploratory puncture of a tumor revealed a lot of free fat, without fatty acid crystals, and some fat cells. The cells could not be grown in a test tube. The authors express doubts about whether this case of Dercum's disease is connected to the shell explosion.
Hyperthyroidism.
Hyperthyroidism.
Case 142. (Tombleson, September, 1917.)
A private, 22, was selected by Col. Garrod for hypnotic treatment by Tombleson from among the hyperthyroid cases. He was admitted April 3, 1916, with a typical hyperthyroidism, with manual tremor, enlarged thyroid, pulse 120, blood pressure 136-40, and hemic murmur. Tombleson induced deep somnambulism at the first hypnotic sitting and suggested an increase of nerve strength and steadiness. The suggestions under somnambulism were repeated for ten days. An occasional added suggestion was given as to lessening of the thyroid. At the end of the ten days the patient declared himself quite well.
A private, 22, was chosen by Col. Garrod for hypnotic treatment by Tombleson from the hyperthyroid cases. He was admitted on April 3, 1916, with classic hyperthyroidism, showing manual tremors, an enlarged thyroid, a pulse of 120, blood pressure of 136-40, and a hemic murmur. Tombleson put him into deep somnambulism during the first hypnotic session and suggested an increase in nerve strength and steadiness. The suggestions during somnambulism were repeated for ten days, with occasional additional suggestions to reduce the thyroid issue. By the end of the ten days, the patient reported that he felt completely well.
Eight of twenty consecutive functional cases treated by hypnotism by Tombleson were cases of hyperthyroidism and in virtually all of these an effect like the above was registered.
Eight out of twenty consecutive cases treated with hypnotism by Tombleson were cases of hyperthyroidism, and in nearly all of these, a similar effect was observed.
Shell-shock; thrown against wall, stunned, emotional: Paroxysmal heart crises six days later, observed for two months. Neurasthenia? Mild Graves’ disease?
Shell shock; slammed against the wall, dazed, emotional: Severe heart crises six days later, watched for two months. Neurasthenia? Mild Graves’ disease?
Case 143. (Dejerine and Gascuel, December, 1914.)
An infantryman, 29, was sent to auxiliary hospital No. 274, for heart trouble, a little thin but looking vigorous enough (typhoid fever at 13 and some diseases of unknown nature and of brief duration while in military service).
An infantryman, 29, was sent to auxiliary hospital No. 274 for heart issues. He was a bit thin but appeared strong enough (he had typhoid fever at 13 and some other minor illnesses of unknown types that lasted a short time during his military service).
September 24, a large calibre German shell burst and threw him against a wall, producing no wound or contusion. He was momentarily stunned, emotionally much affected, and noted at the time extreme palpitation. He was evacuated to Paris September 30, six days after the shock. His pulse was 130-134, regular, and the heart seemed not to be anomalous in any respect.
September 24, a large-caliber German shell exploded and knocked him against a wall, but it didn’t cause any injuries or bruises. He was briefly dazed, emotionally impacted, and experienced significant rapid heartbeat. He was evacuated to Paris on September 30, six days after the incident. His pulse was 130-134, regular, and his heart appeared to be normal in every way.
But there were paroxysmal crises in which the pulse rose to 180 and in which the patient fell into a state of great anxiety. The mouth temperature in the midst of such crises would always rise to 38°, and this temperature would outlast the rest of the seizure. The man was mentally depressed and apparently indifferent, preoccupied with his heart and his insomnia, but at the same time emotionally easily affected. In short, he was a neurasthenic. There was no change in mental state, tachycardia, or paroxysmal seizures in two months, except that he gained weight. Walking and climbing stairs produced dyspnoea. Urine was negative. According to Dejerine, such a case should be treated by psychotherapy.
But there were episodes where his heart rate shot up to 180, and he became extremely anxious. During these episodes, his mouth temperature consistently rose to 38°C, and this temperature would linger even after the main episode was over. The man was mentally down and seemed indifferent, fixated on his heart issues and insomnia, yet he was also easily emotionally affected. In short, he was suffering from neurasthenia. There were no changes in his mental state, tachycardia, or episodes in two months, except he had gained weight. Walking and climbing stairs caused shortness of breath. Urine tests came back negative. According to Dejerine, this kind of case should be treated with psychotherapy.
Alquier, in discussion, called attention to the slight but distinct tremor in this case, dermographia, and spells of perspiration. He suggested that the case might be one of mild Graves’ disease.
Alquier, during the conversation, pointed out the slight but noticeable tremor in this case, along with dermographia and episodes of sweating. He proposed that it might be a mild case of Graves’ disease.
Hyperthyroidism three months, following ten months’ service, at times under protracted shell fire.
Hyperthyroidism for three months, after ten months of service, at times under extended shellfire.
Case 144. (Rothacker, January, 1916.)
A man in service ten months, under strong excitement and at times under protracted shell fire, complained of palpitation, insomnia, dizziness, and dyspnoea. Hospital notes showed that the left lobe of the thyroid was somewhat enlarged. Before the war his neck could not have been very thick; he had served his year out without difficulty. His mother is said to have suffered at one time from thick neck. According to the patient, he had never suffered with heart trouble. Heart not enlarged; blowing first sound over the apex. Graefe, Stellwag and Möbius signs negative. Heart rapid, not irregular; pulse strong. There was fine tremor of the hands, as well as a tremor of the tongue. Knee-jerks increased.
A man who had been in service for ten months, under intense stress and sometimes prolonged shell fire, reported symptoms of a racing heart, insomnia, dizziness, and shortness of breath. Hospital records indicated that the left lobe of his thyroid was slightly enlarged. Before the war, his neck didn't seem particularly thick; he had completed his service without issues. It's said that his mother once had a thick neck. The patient claimed he had never experienced heart problems. His heart wasn't enlarged; there was a blowing sound in the first heartbeat at the apex. Graefe, Stellwag, and Möbius signs were negative. His heart was fast but not irregular; his pulse was strong. There was slight tremor in his hands and also a tremor of the tongue. His knee-jerks were increased.
The patient was at first sleepless and excited, but after three weeks in bed the heart murmur had disappeared. After three months, he was ordered to Ersatz with the left side of the neck measuring 20 as against 18 cm. on the right. There was a soft pulsating swelling of the thyroid. First sound over apex still impure; heart action now regular; pulse 64; blood pressure 120 Riva-Rocci; after test exercises, slight dyspnoea. No cyanosis. The outstretched hands were no longer very tremulous. The knee-jerks were still increased. The man had begun to sleep well. His neck was apparently much diminished in girth.
The patient was initially restless and agitated, but after three weeks in bed, the heart murmur had gone away. After three months, he was sent for a follow-up, with the left side of his neck measuring 20 cm compared to 18 cm on the right. There was a soft, pulsating swelling of the thyroid. The first heart sound over the apex was still unclear; heart action was now regular; pulse was at 64; blood pressure was 120 Riva-Rocci; after doing some test exercises, there was slight shortness of breath. No cyanosis was present. His outstretched hands were no longer very shaky. The knee-jerk reflexes were still heightened. The man had started sleeping well. His neck seemed to have noticeably decreased in size.
Here then was a case of Graves’ disease of acute development, brought out by nervous stress and excitement as well as by 10 months of war work and exposure to shell fire,—with approximate recovery after three months of rest.
Here was a case of Graves' disease that developed quickly, triggered by stress and excitement, as well as 10 months of working in wartime and being exposed to shellfire—with a nearly full recovery after three months of rest.
Graves’ disease, forme fruste.
Graves' disease, incomplete form.
Case 145. (Babonneix and Célos, June, 1917.)
A farmer, 31, entered the Rosendael Hospital, Jan. 25, 1917. He had been two years in active service. The family history was negative except that one of his sisters had had dyspepsia. The patient denied venereal disease and alcoholism and had always been well. At the Battle of the Marne he was slightly wounded in the left knee. January, 1915, he was exposed to gas bombs and explosive shells. He was several days in the hospital spitting, or perhaps vomiting blood and was sent on a long convalescence. On returning to the front, he had to be sent back to hospital with a note, “not fit for service, nervous troubles and paroxysmal tachycardia.” In point of view he now showed a number of symptoms suggestive of Graves’ disease, such as a definite exophthalmia which, according to the patient, started up a short time after the shock and a tachycardia (110-120) with circulatory excitement, a tumultuous heart, neck arteries contracting, almost dancing in their contractions, together with a systolic murmur maximal in the pulmonary area, not retaining, variable,—in short, suggestive of an inorganic murmur. There was also a generalized rapid tremor and a variety of vasomotor disorders, such as blushing and paling, perspiration, exaggerated reflexes, emotionality, logorrhea, jactitation. There were also digestive troubles, regurgitation after meals and the patient had become thin and weak.
A 31-year-old farmer was admitted to Rosendael Hospital on January 25, 1917. He had been in active service for two years. His family history was mostly clear, with the exception of one sister who had experienced indigestion. The patient denied having any sexually transmitted diseases or issues with alcoholism and reported that he had always been healthy. He was slightly wounded in his left knee during the Battle of the Marne. In January 1915, he was exposed to gas bombs and explosive shells, leading to several days in the hospital with symptoms like coughing or possibly vomiting blood, after which he underwent a long recovery period. When he returned to the front, he had to be sent back to the hospital with a note stating he was “not fit for service” due to nervous issues and episodes of rapid heart rate. Currently, he exhibited several symptoms indicative of Graves’ disease, including noticeable bulging eyes that, he reported, started shortly after the traumatic experiences, as well as a heart rate of 110-120 beats per minute with heightened circulatory activity, a tumultuous heartbeat, and neck arteries that appeared to be contracting erratically. There was also a systolic murmur that was variable and prominent in the pulmonary area, suggesting it was an inorganic murmur. Additionally, he experienced widespread rapid tremors and various vasomotor issues like flushing and paleness, excessive sweating, heightened reflexes, emotional instability, rapid speech, and restlessness. He also had digestive issues, such as regurgitation after meals, and had become thin and weak.
There was, however, no swelling of the thyroid gland nor any eye signs other than the exophthalmia. In short this case is doubtless one of the forme fruste of Graves’ disease. It seems to show that Graves’ disease may have a traumatic origin.
There was, however, no swelling of the thyroid gland nor any eye signs other than the bulging eyes. In short, this case is definitely one of the forme fruste of Graves’ disease. It suggests that Graves’ disease might have a traumatic origin.
Somatic complication in a shell-shock hysteria (Trauma).
Somatic complications in shell-shock hysteria (Trauma).
Case 146. (Oppenheimer, February, 1915.)
Musketeer. No faulty heredity, but was always somewhat nervous. On October 26, a shell burst one meter in front of him, burying him under the anterior wall of the trench. He was dug out and taken to the field hospital, where he remained unconscious until the next morning. On October 29, he was taken to the reserve hospital. Severe pain in the head, entire scalp tender on pressure, especially in the left frontal region, left side upper lip swollen, bluish and discolored. Left tenth and sixth ribs broken. Fracture of skull(?). November 10, at eight o’clock at night, sudden attack of vomiting, and the patient was found in a faint in the water closet. Almost complete paralysis of speech and all of the four extremities. Consciousness obscured; no sensory disturbances. November 11, severe headache and vertigo. Speech somewhat more intelligible. Pulse, 60 to 68. “Evidently secondary hemorrhage in the brain.” November 12, to Augusta Hospital. November 20, admission to nerve hospital. Typical aphonia. Limitation of motion in all four extremities, but no paralysis—anergy. Reflexes normal. Unable to stand and walk. Sensibility preserved. Under suggestive treatment, curative gymnastics, as well as electrotherapeutics, the aphonia and abasia disappeared in a few days, but the patient continued to complain of headache and insomnia. December 16, an attack of nausea, headache, vomiting, loss of consciousness, followed by epistaxis, marked tachycardia. January 4, in his sleep he felt a prick in his left upper arm, as if he had pushed a sewing needle into the arm. X-ray examination showed a needle in the arm. This was extracted under local anesthesia.
Musketeer. No genetic issues, but always a bit anxious. On October 26, a shell exploded just a meter in front of him, trapping him under the front wall of the trench. He was dug out and taken to the field hospital, where he remained unconscious until the next morning. On October 29, he was moved to the reserve hospital. He had severe pain in his head, his entire scalp was tender to touch, especially on the left front side, his left upper lip was swollen, bluish, and discolored. His left tenth and sixth ribs were broken, and there was a possible skull fracture. On November 10, at eight o’clock at night, he suddenly threw up and was found fainting in the bathroom. He had almost complete paralysis of speech and all four limbs. His consciousness was clouded; there were no sensory issues. On November 11, he experienced severe headaches and dizziness. His speech was slightly more understandable. His pulse ranged from 60 to 68. "Evidently secondary hemorrhage in the brain." On November 12, he was transferred to Augusta Hospital. On November 20, he was admitted to a nerve hospital. He had typical aphonia. There was a limitation of motion in all four limbs, but no paralysis—just weakness. Reflexes were normal. He couldn't stand or walk. Sensation was intact. With suggestive treatment, therapeutic exercise, and electrotherapy, his aphonia and inability to walk improved within a few days, but he continued to complain of headaches and insomnia. On December 16, he had nausea, headaches, vomiting, loss of consciousness, followed by nosebleeds and rapid heartbeat. On January 4, while sleeping, he felt a prick in his left upper arm, as if a sewing needle had been pushed into it. An X-ray showed a needle in his arm, which was removed under local anesthesia.
VIII.[5] SCHIZOPHRENOSES
(DEMENTIA PRAECOX GROUP)
The Sister’s ear boxed for blow to a German soldier’s pride: Diagnosis PSYCHOPATHIC CONSTITUTION! A true psychosis develops: hate of Prussia and the Junkertum: Diagnosis, DEMENTIA PRAECOX!!
The Sister’s ear rang from the blow to a German soldier’s pride: Diagnosis PSYCHOPATHIC CONSTITUTION! A true psychosis develops: hatred of Prussia and the Junkertum: Diagnosis, DEMENTIA PRAECOX!!
Case 147. (Bonhoeffer.)
A sick soldier in a military hospital kept complaining of being waked up too early, and of poor food. His reactions looked like the irritable weakness of a psychopath. One day he went into a room where a woman was being examined, without knocking. When ordered out, he boxed the Sister’s ear.
A sick soldier in a military hospital kept complaining about being woken up too early and the bad food. His reactions seemed like the irritability of someone mentally unstable. One day, he walked into a room where a woman was being examined, without knocking. When he was told to leave, he slapped the nurse.
He said himself, on transfer to the psychiatric clinic, that he had always been quarrelsome as a child with his brothers and sisters, subject to fainting spells, and poor and stubborn in military service,—all of which seemed to clinch the diagnosis of psychopathic constitution.
He himself said, upon being transferred to the psychiatric clinic, that he had always been argumentative as a child with his siblings, prone to fainting spells, and difficult during his military service—which all seemed to confirm the diagnosis of a psychopathic personality.
But he seemed to show a decided lack of autocritique. About boxing the Sister’s ear on her saying “Please go out,”—his idea was that he could not let a thing like that happen to him,—a German soldier and a patient! Moreover, “It should not be thought that perhaps I had a love affair with her! There was a cynicism about her.” The Sister had a strong sex impulse, he could see that by her nose: she was, so to speak, “hypochondriacal.” Both in speech and writing he used stilted phrases. The ego at last swelled to the point of his saying that he was an inhabitant of the World and hated Prussia and Prussian Junkertum.
But he really showed a total lack of self-criticism. When it came to slapping the nurse for telling him to "please go out," his thought was that he couldn’t allow something like that to happen to him—being a German soldier and a patient! Also, “It shouldn’t be assumed that I had a romantic involvement with her! She had a certain cynicism.” He could tell the nurse had a strong sexual drive, which he could see just by looking at her nose: she was, in a way, “hypochondriacal.” Both in conversation and writing, he used overly formal phrases. His ego finally grew to the point where he claimed he was a citizen of the World and despised Prussia and Prussian Junkertum.
Then came unmotivated states of excitement, with pressure of speech and motion, and eventually negativism. Accordingly, the diagnosis hebephrenia finally replaced that of psychopathic constitution.
Then came states of excitement that lacked motivation, along with increased speech and movement, and eventually a sense of negativism. As a result, the diagnosis of hebephrenia finally took the place of psychopathic constitution.
Dementia praecox, arrested as spy.
Dementia praecox, stopped as spy.
Case 148. (Kastan, January, 1916.)
A German private, called to the colors, was supposed to take his civilian clothes to the post office along with his comrades on March 21, 1915. He did not get his package ready in time and was ordered to go with another troop. At an opportune moment, he left the barracks with the package of clothing. When later arrested, he said that he had gone by railroad to Dirschau; then he had visited Berlin. After this, he had walked to Bromberg, Schneidemühl, and Landsberg.
A German private, called to serve, was supposed to take his civilian clothes to the post office with his friends on March 21, 1915. He didn’t get his package ready in time and was ordered to join another group. At a convenient moment, he left the barracks with the clothing package. When he was arrested later, he said that he had taken the train to Dirschau; then he had visited Berlin. After that, he had walked to Bromberg, Schneidemühl, and Landsberg.
At last he had ridden back to Küstrin. At Küstrin some children told a railway official that the man was making drawings. There was a petroleum tank near by. Accordingly, he was arrested as a possible spy. He claimed that he was not a soldier.
At last, he had ridden back to Küstrin. In Küstrin, some kids told a railway official that the man was making drawings. There was a petroleum tank nearby. As a result, he was arrested as a potential spy. He insisted that he was not a soldier.
In the clinic, he looked dull and smiled a good deal. It seems that, before being called to the colors, he had been very angry with his wife and had even threatened her. He now explained this anger as his wife’s fault. She had attacked him, he said. He said that he sometimes had attacks of weakness, which used to last two days at a time, but they had recently lasted for a shorter time. He said that his thoughts always wanted to be somewhere else. In fact, he had not performed military duty. His uniform had been gotten for him, but he had had no further orders. Sometimes in a fever or dream his head seemed to be as big as a room, as if there were no space for it. There was an itching in his legs, he said, which often fell asleep so he could not stand on them. He had had syphilis seven years before, after which he had been hoarse, forgetful, and anxious.
In the clinic, he looked tired and smiled a lot. It seems that, before being drafted, he had been very angry with his wife and had even threatened her. He now blamed this anger on her, saying she had attacked him. He mentioned that he sometimes experienced bouts of weakness that would last two days, but lately they had been shorter. He said his mind always wanted to be somewhere else. In reality, he hadn't been on active duty. His uniform was arranged for him, but he hadn't received any further orders. Sometimes, in a fever or dream, his head felt like it was as big as a room, as if there was no space for it. He mentioned an itching in his legs, which often went numb so he couldn't stand on them. He had contracted syphilis seven years ago, after which he became hoarse, forgetful, and anxious.
Examination showed perceptive power and knowledge to be good. He played the violin, but always the same tunes. He said that he had not worked in Berlin during the winter of 1914. He spoke as if he had been in another sanitarium, where he did nothing but dream by himself, taking no interest[202] in things, and lying indifferently, with a blanket over him.
Examination showed his insight and knowledge to be good. He played the violin, but always the same tunes. He claimed he hadn’t worked in Berlin during the winter of 1914. He spoke as if he had been in another sanitarium, where he just dreamed alone, showed no interest in anything, and lay there indifferently, wrapped in a blanket.
He said that when he received the uniform he had a longing for clean underclothes. Requested to explain the meaning of the uniform, he remarked: “Why, many have these things on.”
He said that when he got the uniform, he really wanted some clean underwear. When asked to explain what the uniform meant, he replied, “Well, a lot of people wear these things.”
Re dementia praecox, Lépine states that in the French army instances of dementia praecox have been numerous in the interior, both at the time of mobilization and at the time of calling out sundry new classes. He notes that the courtmartial and invaliding experts have neither the leisure nor the experience necessary to keep these men from going into the army. The somewhat frequent remissions in dementia praecox make the task all the more difficult. To be sure, the stuporous and catatonic cases are not very much in evidence in the army; when such cases do occur, it is easy enough to evacuate the patients to a hospital for observation. Far more troublesome are cases of a less advanced or milder nature. Here are cases in which judgment is deficient, and in which quite unsystematic, incoherent, and transient delusional ideas occur. The patient looks quite normal to the non-psychiatric expert. Something odd happens which quite suddenly reveals the delusional ideas. For example, there is a fugue, or else the soldier goes to his superior and aggressively chides him for having troubled him the night before. These particular psychopaths are among the most dangerous to be found in the army.
Regarding dementia praecox, Lépine mentions that in the French army, there have been many cases of dementia praecox, both during mobilization and when new groups were called up. He points out that the court-martial and disability assessment experts don't have the time or experience needed to prevent these individuals from entering the army. The somewhat frequent remissions in dementia praecox make the situation even more challenging. Sure enough, the stuporous and catatonic cases are not very common in the army; when they do occur, it's fairly easy to send the patients to a hospital for observation. However, the cases that are less developed or milder are much more troublesome. In these situations, judgment is lacking, and there are disorganized, incoherent, and temporary delusional thoughts. The patient appears completely normal to those without psychiatric training. An unusual incident can suddenly unveil the delusional thoughts. For example, there might be a fugue state, or the soldier might confront his superior and angrily accuse him of bothering him the night before. These specific individuals with psychopathology are some of the most dangerous in the army.
Fugue, catatonic.
Fugue state, catatonic.
Case 149. (Boucherot, 1915-6.)
A gunner, aged 23, enlisted on the expiration of his regular period of service and was a good soldier, in excellent health, up to June, 1915. He then began to have a few vague ideas of persecution. In a short time these became more definite and he caused talk by requesting to go into another corps because his comrades did not like him. He told his brigadier that the soldiers were frightening him by magnetism. He had hallucinations of hearing people say, “He will get it.” He kept by himself, would not eat and stood motionless for long periods of time before his mess-tin. He was often found in a dreamy state of apathy. One day he left the cantonment without leave, wandered through fields, had coffee in a village and then started off in no special direction. The police took him without resistance the next day. He said, “My comrades are in politics; they are going to cheat me.” He was brought to Fismes and the ambulance surgeon said that he found he did not know what he was about. He was amnestic for the fugue, explaining that he went because he was frightened. It was hard to get him to eat.
A 23-year-old gunner re-enlisted after his regular service ended and was a good soldier in great health until June 1915. Around that time, he started having some vague feelings of persecution. Soon, these feelings became clearer, and he caused a stir by asking to transfer to another unit because his fellow soldiers didn’t like him. He told his brigadier that the other soldiers were scaring him with magnetism. He experienced hallucinations where he heard people say, “He will get it.” He kept to himself, refused to eat, and stood still for long periods staring at his mess tin. He was often found in a daze, showing signs of apathy. One day, he left the camp without permission, wandered through fields, had coffee in a village, and then walked off in no particular direction. The police found him the next day without any resistance. He said, “My comrades are involved in politics; they’re going to trick me.” He was taken to Fismes, and the ambulance surgeon stated that he seemed confused and unaware of his situation. He had no memory of his time wandering, explaining that he left because he was scared. It was difficult to get him to eat.
July 14, he was evacuated to Fleury protesting arrogantly, but this phase of excitement passed and he became absolutely indifferent and disoriented. He became untidy in his person and in no way could his attention be attracted whether by mentioning his family or the war. He sometimes made ape-like grimaces and sometimes laughed causelessly. He was occasionally negativistic, but in general was perfectly compliant with the requirements of the hospital. Now and then he started off impulsively to escape but was brought back quite indifferent. Now and then he went into bizarre contortions on a medical visit or aped gestures of bystanders. He began then to go into stereotypical attitudes. This case is the only catatonic one found by Boucherot in his war group.
On July 14, he was evacuated to Fleury, acting arrogantly in protest, but this excitement soon faded, and he became completely indifferent and disoriented. He became disheveled and showed no interest, whether it was talk about his family or the war. Sometimes he made strange, monkey-like faces, and at other times he laughed for no reason. He was occasionally resistant but mostly followed the hospital rules without issue. Every now and then, he impulsively tried to escape but was brought back without any concern. He would sometimes engage in odd movements during medical visits or mimic the actions of onlookers. Eventually, he started adopting repetitive postures. This case is the only catatonic one found by Boucherot in his group from the war.
Desertion: Schizophrenic-looking behavior. Adjudged responsible.
Desertion: Erratic behavior. Found responsible.
Case 150. (Advice, 1915.)
An Italian private in the artillery, a telephone operator at the front, came up for desertion in the face of the enemy. It seems that he had often left his post, going off for a number of hours and drinking. At last he lost his position in the battery, went off and got drunk again, and was removed to a hospital and held as a neurasthenic and psychopathic patient. At the territorial hospital he was regarded as a melancholic. He still showed signs of alcoholism, was hallucinated, did a number of peculiar things, was impatient of medical examination, and was given a furlough of two months for convalescence. He apparently grew somewhat better in his father’s home, but went to a physician there and presented his certificate as a mental case. His behavior was so peculiar on subsequent arrest that he was sent for observation to Consiglio.
An Italian private in the artillery, who worked as a telephone operator at the front, was charged with desertion in the face of the enemy. It seems he frequently left his post for several hours to drink. Eventually, he lost his position in the battery, went off again to get drunk, and was sent to a hospital where he was classified as a neurasthenic and psychopathic patient. At the territorial hospital, he was seen as melancholic. He still showed signs of alcoholism, had hallucinations, acted strangely, was impatient during medical examinations, and was granted a two-month leave for recovery. He appeared to improve a bit at his father's home but visited a doctor there and showed his mental health certificate. His behavior was so odd during his subsequent arrest that he was sent for observation at Consiglio.
It appeared that he had been in military service from August, 1912, and had been imprisoned for a space of eight weeks for disobedience when he had been in military service for six months. He had been punished in the army nine times, once being given 70 days for lying. He was regarded as an undisciplined soldier but not as a nervous or mental case.
It seemed that he had been in the military since August 1912 and had spent eight weeks in prison for disobedience after serving six months. He had been disciplined in the army nine times, with one instance resulting in a 70-day sentence for lying. He was seen as an undisciplined soldier but not as someone with a nervous or mental issue.
At hospital he was in a semi-stupor, claimed that he was forgetful, was apathetic concerning home and relatives, complained of pain in the head, and altogether preserved a strange and stolid attitude with occasional gestures, mimicry, and stereotyped reactions. As he had come to be operated upon, he looked about for the cannon that was to be used in the operation. Accordingly the question of dementia praecox might well be raised.
At the hospital, he was in a dazed state, said he was forgetful, seemed indifferent about home and family, complained of headaches, and generally showed a weirdly expressionless demeanor with occasional gestures, facial expressions, and repetitive reactions. Since he had come in for surgery, he looked around for the equipment that was going to be used in the operation. Therefore, the possibility of a diagnosis of schizophrenia could be considered.
His indifference turned out actually to be assumed and pretentious. He preserved throughout an arrogant tone, and there were features in his voice that strongly suggested simulation.
His indifference turned out to be fake and pretentious. He maintained an arrogant tone the whole time, and there were qualities in his voice that clearly indicated he was pretending.
According to Consiglio, we are dealing with an epileptic degenerate, addicted to alcohol, lying, and immorality. The question concerning responsibility was settled in the affirmative. Of course, it might be thought that the case was one of pathological intoxication, in which case, the man might be regarded as only semi-responsible. However, the phenomena of simulation, not merely in the observation hospital but also in the period of apparent depression and strange conduct immediately following his arrest for desertion, led to the decision that the man, despite his nervous abnormality, was responsible for his act. He was condemned to 20 years in prison.
According to Consiglio, we are dealing with an alcoholic who has epilepsy, is deceitful, and engages in immoral behavior. The question of responsibility was answered in the affirmative. It might be argued that this case involved pathological intoxication, which could mean the man was only partially responsible. However, the signs of faking, not just in the observation hospital but also during the period of noticeable depression and odd behavior right after his arrest for desertion, led to the conclusion that the man, despite his nervous disorder, was responsible for his actions. He was sentenced to 20 years in prison.
Re dementia praecox, Buscaino and Coppola found a number of cases of dementia praecox amongst soldiers admitted to hospital during the period of mobilization; cases amongst men who had not yet been at the front. These mobilization cases, in fact, were as a rule either cases of dementia praecox, cases of a psychopathic constitution, or cases of alcoholism.
Re dementia praecox, Buscaino and Coppola found several cases of dementia praecox among soldiers admitted to the hospital during the mobilization period; cases involving men who had not yet been at the front. These mobilization cases, in fact, tended to be either cases of dementia praecox, cases of a psychopathic constitution, or cases of alcoholism.
A disciplinary case: Schizophrenia, alcoholism.
A disciplinary case: schizophrenia, alcoholism.
Case 151. (Kastan, January, 1916.)
In October, 1914, a German soldier returned to his barracks late from a drinking bout. He insolently called for order, brandishing his arms, and when the captain rebuked him, he kept a cigar in his mouth. Examined in hospital (Allenberg), he was very reticent at first but wrote his name up over the bed with the additional word “Dead.” He answered, “I don’t know” to most questions. Although it was December, he said the season was summer. He was to be shot for disrespect, he said, but showed more disrespect at every remonstrance. “What is your regiment?” “I am no soldier at all, you know. I have already been discharged as unfit for service.” “Have you been in prison?” “I don’t know. My father often thrashed me.” Then suddenly, after a moment, “I was in prison five, seven, and two years, and my father was in prison four, six, and three years.” He said that he had drunk ether and urged the physician to try it, as one saw all sorts of beautiful pictures and figures and heard music.
In October 1914, a German soldier came back to his barracks late after a night of drinking. He arrogantly called for order while waving his arms around, and when the captain scolded him, he kept a cigar in his mouth. When examined in the hospital (Allenberg), he was initially very quiet but wrote his name above the bed, adding the word “Dead.” He replied, “I don’t know” to most questions. Even though it was December, he claimed it was summer. He said he was going to be shot for disrespect, but he showed even more disrespect every time someone confronted him. “What is your regiment?” “I’m not a soldier at all, you know. I’ve already been discharged as unfit for service.” “Have you been in prison?” “I don’t know. My father often beat me.” Then suddenly, after a moment, he added, “I was in prison for five, seven, and two years, and my father was in prison for four, six, and three years.” He mentioned that he had drunk ether and encouraged the doctor to try it, saying it made you see all kinds of beautiful images and shapes and hear music.
Upon investigation, it was found that the man had been in a provincial sanatorium for some form of degenerative mental disease with excitement. He, at this time, had given a number of fantastic stories concerning his wanderings. For example, he said he had come from Australia, where he had eaten snipes and crows; that he was on his way home and would get there in half an hour (real distance 10 hours). Or again, he would roll his eyes, assume a false name and say that he had come from Morocco, or that he was the emperor and would not play soldier. When asked to repeat digits, he habitually omitted the last digit. He had been a poor scholar, and of a tricky and treacherous character.
Upon investigation, it was discovered that the man had been in a provincial sanatorium for some form of degenerative mental illness with agitation. At that time, he shared a number of wild stories about his travels. For instance, he claimed he had come from Australia, where he had eaten snipes and crows; that he was on his way home and would arrive in half an hour (the actual distance was 10 hours). Or he would roll his eyes, use a fake name, and say that he had come from Morocco, or that he was the emperor and wouldn’t play soldier. When asked to repeat numbers, he would routinely skip the last digit. He had been a poor student and had a tricky and deceitful nature.
Despite this history, he had behaved well in the army at first, though insolent to superiors. On July 5 he had a heavy drinking bout, and wrote next day to his mother that he was going to commit suicide. At this time he had been put for safe keeping in a cell, where he saw foxes making as if to bite[207] him. He also said that he was a rich nobleman, a cavalry captain with a servant (asked to be given his pressed clothes and his cigarettes), and was being pursued. He rode his pillow as if it were his horse, and hid it in the horse’s stable, namely, the bed. He ate nothing, as he thought everything was poisoned; smeared himself with faeces and drank urine as “strawberry punch.”
Despite this background, he initially acted well in the army, although he was disrespectful to his superiors. On July 5, he went on a heavy drinking spree and wrote to his mother the next day saying he was going to commit suicide. At that time, he had been placed in a cell for his own safety, where he saw foxes acting like they were going to bite him. He also claimed that he was a wealthy nobleman, a cavalry captain with a servant (he asked for his pressed clothes and cigarettes), and said he was being chased. He rode his pillow as if it were a horse and hid it in the horse's stable, which was actually the bed. He ate nothing because he believed everything was poisoned; he covered himself in feces and drank urine, calling it “strawberry punch.”
We are evidently here dealing with a psychopath of schizophrenic tendencies, strongly colored, however, by alcoholism. The patient’s father was a drunkard, and a brother and sister were insane.
We are clearly dealing with a psychopath with schizophrenic tendencies, heavily influenced by alcoholism. The patient's father was an alcoholic, and a brother and sister were mentally ill.
Re schizophrenia in the German army, Saenger remarks that like paresis, so also latent dementia praecox becomes acute under war conditions. E. Meyer states that amongst 1126 officers admitted to his hospital, August 1, 1915, there were 352 that had either psychoses or neuroses, amongst which were 148 psychogenic cases (either psychopathic or hysterical), 128 with what he terms a congenital psychopathic diathesis, and 76 with traumatic neuroses. The cases of congenital diathesis were somewhat difficult to diagnose, since but 44 of these were clearly psychopathic and in the remainder the question of dementia praecox or of cyclothymic conditions arose.
Regarding schizophrenia in the German army, Saenger notes that, similar to paresis, latent dementia praecox becomes more severe in wartime. E. Meyer reports that among 1,126 officers admitted to his hospital on August 1, 1915, 352 were suffering from either psychoses or neuroses. This included 148 psychogenic cases (either psychopathic or hysterical), 128 with what he calls a congenital psychopathic predisposition, and 76 with traumatic neuroses. Diagnosing the cases of congenital predisposition was somewhat challenging, as only 44 were clearly psychopathic, leaving the others uncertain between dementia praecox and cyclothymic conditions.
Stier gives statistics for 1905 and 1906 in the German army, namely 35 per cent of dementia praecox cases. Under war conditions the army has developed far fewer cases: Bonhoeffer, 7 per cent; Meyer, 7.5 per cent; Hahn, 13 per cent. But although dementia praecox figures so much less frequently in the mobilized army than in the army of peace times (manic depressive psychosis is also less in evidence under war conditions), the psychopathic constitutions, hysterias, traumatic neuroses, and the like, run from 17.5 per cent (Stier, 1905-1906) to 54 per cent (Bonhoeffer), 37.5 (Meyer), 43 per cent (Hahn).
Stier provides data for the German army in 1905 and 1906, showing that 35 percent of cases were dementia praecox. In wartime, the army has seen significantly fewer cases: Bonhoeffer reports 7 percent; Meyer, 7.5 percent; and Hahn, 13 percent. Even though dementia praecox is much less common in the mobilized army compared to peacetime (and manic depressive psychosis is also less prevalent during wartime), psychopathic traits, hysterias, traumatic neuroses, and similar conditions range from 17.5 percent (Stier, 1905-1906) to 54 percent (Bonhoeffer), 37.5 percent (Meyer), and 43 percent (Hahn).
Schizophrenic symptoms. Aggravation by service.
Schizophrenic symptoms. Worsened by service.
Case 152. (De la Motte, August, 1915.)
A Landsturm recruit, 20, and somewhat peculiar in early life, got whipped by his comrades for getting back too late from leave. The next day he was commanded to carry a machine gun. He threw the gun down and made for the barracks. He was put under psychiatric observation, as he said he did not know what he was doing. His conduct seemed normal at first and he explained that he had heard noises and singing in his head,—pointing to the left ear where there was an otitis media. His skill, knowledge, and general experience seemed well in hand. However, he was not very communicative. Eventually a series of schizophrenic symptoms came to light. He had been hearing threatening voices of varying intensity for two years, sometimes a veil seemed to be before his eyes, sometimes he heard his thoughts, and felt that his whole personality was changing. He began to think that his facial traits were gradually turning into those of the physician. The hallucinations were so insistent that sometimes he did not know what he should do. He was evidently unfit for military service, and the decision was also made that the mental disease had been aggravated by service.
A Landsturm recruit, 20, who had always been a bit odd, got punished by his fellow soldiers for coming back late from leave. The next day, he was ordered to carry a machine gun. He dropped the gun and headed straight for the barracks. He was placed under psychiatric observation because he claimed he didn’t know what he was doing. His behavior seemed normal at first, and he said he heard noises and singing in his head, pointing to his left ear where he had an ear infection. His skills, knowledge, and overall experience appeared solid. However, he wasn't very talkative. Eventually, a range of schizophrenic symptoms surfaced. He had been hearing threatening voices of varying intensity for two years; sometimes it felt like a veil was in front of his eyes, occasionally he heard his own thoughts, and he felt like his whole personality was shifting. He started to believe that his facial features were slowly resembling those of the doctor. The hallucinations were so persistent that he often didn't know what to do. It was clear he was unfit for military service, and it was also determined that his mental illness had been worsened by his time in service.
Re schizophrenia in the service, most authors point out that there was either patent or latent schizophrenia before mobilization. E. Meyer attempted to make a study of the influence of the war on psychopaths. He found that the ego of the psychopath remained relatively unaffected by the war. Naturally, the paretics and the seniles were unaffected. The grandiosity and self-centredness of the alcoholics remained as prominent as ever. Seventeen schizophrenic cases were studied, and some of these yielded entire apathy with respect to the war; others had the content of their delusions somewhat affected. Saaler remarks on the military tinge which dementia praecox assumes under war conditions. Dementia praecox and manic-depressive psychosis alike show war changes.
Re schizophrenia in the military, most authors note that there was either obvious or hidden schizophrenia before deployment. E. Meyer tried to study the impact of the war on psychopaths. He found that the psychopath's sense of self remained relatively unchanged by the war. Naturally, those with paresis and senility were also unaffected. The grandiosity and self-absorption of alcoholics continued to be as noticeable as ever. Seventeen cases of schizophrenia were examined, and some of these showed complete indifference to the war; others had their delusions slightly altered. Saaler comments on the military aspect that dementia praecox takes on during wartime. Both dementia praecox and manic-depressive psychosis display changes due to the war.
Shot himself in hand. Delusions.
Accidentally shot his hand. Delusions.
Case 153. (Red, 1915.)
An infantryman, 26, left for the front August, 1914, was slightly wounded, recovered, went back to the front, and then is said, in March, 1915, to have shot himself in the hand. When up for military review a delusional state set in. It seems that he had been interned in several hospitals for examination, but escaped four or five times because physicians wanted to poison him and had partially succeeded.
An infantryman, 26, went to the front in August 1914, was slightly wounded, recovered, returned to the front, and is said to have shot himself in the hand in March 1915. When he was up for military review, he experienced a delusional state. It appears he had been placed in several hospitals for evaluation but escaped four or five times because the doctors wanted to poison him and had partially succeeded.
He came to the Lemioux Custodial Institution, July 12, 1915. His brother, 15, was a voyou; his sister, 16, was an imbecile. The patient told about his military history and how he had shot himself in the left hand, to be with a certain woman, how attempts had been made to poison him, especially a certain man in Bordeaux, who wanted to possess the woman in the case. In point of fact, the physicians could not save him from this enemy.
He arrived at the Lemioux Custodial Institution on July 12, 1915. His brother, 15, was a troublemaker; his sister, 16, had a mental disability. The patient recounted his military background and how he had shot himself in the left hand to be with a particular woman, explaining that attempts had been made to poison him, especially by a man in Bordeaux who wanted to be with her. In reality, the doctors couldn’t protect him from this threat.
The patient now became calm and indifferent, lived secluded and almost immobile. In November, however, he began to sit down and eat like others, making low, timorous answers, vague and confused. He smiled cheerfully on questioning, but had many sad ideas. He would smilingly say that he was going to die soon.
The patient became calm and indifferent, living in isolation and almost motionless. However, in November, he started to sit down and eat like everyone else, giving quiet, timid responses that were vague and confused. He would smile cheerfully when asked questions, but he had many sad thoughts. He would smile and say that he was going to die soon.
Re schizophrenia in the French army, Boucherot found eight cases amongst 107 soldiers admitted to Loiret in the first year of the war. He remarks upon the fact that the schizophrenic cases were often disciplinary. The group is a disciplinary group. Damaye remarks upon the difficulty of diagnosis betwixt feeblemindedness and dementia praecox as observed in the French army.
Re schizophrenia in the French army, Boucherot found eight cases among 107 soldiers admitted to Loiret in the first year of the war. He notes that the cases of schizophrenia were often related to disciplinary issues. The group is a disciplinary group. Damaye comments on the difficulty of diagnosing between feeblemindedness and dementia praecox as seen in the French army.
Volunteer: Dementia praecox.
Volunteer: Schizophrenia.
Case 154. (Haury, 1915.)
N. enlisted voluntarily for three years in the Infantry, September 10, 1912, and immediately gave indications of abnormal mentality by his conduct. He made mistakes all day long. At reveille he had to be called several times, and when his corporal objected, he said, “It is cold; I don’t see why I must get up; I am free to remain in bed until 8 o’clock.” In reply to his corporal’s remonstrance about his continued latenesses, he once said, “I can’t get ready; I have no mirror to wash before.” This was rather surprising conduct from an intelligent printer-engraver, who had lived and gone to school in the town of Lyons. He was unable to make his own bed or to perform the simplest of exercises in the manual of arms. He was violent on several occasions, once attacking a comrade who had given him an order, and again when another had taken his place in the line. His reasoning faculties were those of a young child. He continued doing these strange things, and was finally discharged.
N. voluntarily enlisted for three years in the Infantry on September 10, 1912, and quickly showed signs of unusual behavior with his actions. He made mistakes all day. At reveille, he had to be called several times, and when his corporal complained, he said, “It’s cold; I don’t see why I have to get up; I’m free to stay in bed until 8 o’clock.” When his corporal pointed out his repeated tardiness, he once responded, “I can’t get ready; I don’t have a mirror to wash my face.” This was quite surprising coming from an intelligent printer-engraver who had lived and gone to school in the town of Lyons. He couldn’t make his own bed or do the simplest tasks in the manual of arms. He was violent on several occasions, once attacking a comrade who had given him an order, and another time when someone took his place in line. His reasoning skills were those of a young child. He kept acting strangely and was eventually discharged.
Re dementia praecox amongst American troops, Edgar King, before the war, concluded that some 5 to 8 per cent of the American cases of mental disease in the army belonged to the paranoid form of dementia praecox. King lays special emphasis upon dementia praecox, finding that more than one-half of the army admissions for mental disease belong to this group. He calls attention to the number of desertions and undesirables in the group. He found that 70 per cent of the cases showed some heredity.
Re dementia praecox among American troops, Edgar King, before the war, concluded that around 5 to 8 percent of the American mental health cases in the army were categorized as the paranoid form of dementia praecox. King stresses the significance of dementia praecox, noting that over half of the army admissions for mental health issues fell into this category. He highlights the high number of desertions and undesirables within this group. He discovered that 70 percent of the cases exhibited some hereditary link.
Hysteria versus catatonia.
Hysteria vs. catatonia.
Case 155. (Bonhoeffer, 1916.)
A reservist, 31, was in the hospital about Christmas, 1914, for rheumatism, when suddenly he became excited and was sent to the Charité Psychiatric Clinic. He was restless all night, moving about in bed, grinding his teeth, and continually getting up. He had a blank and astonished expression; his breathing was rapid and forced. There were no pyramidal tract symptoms, but muscular power was diminished,—more on the right than on the left. While the knee-jerks were being tested, the legs moved (seemingly psychogenic). Irregular hypalgetic zones were found, and pain was less well felt on the right side than on the left. Answers to questions on mental examination were made with the appearance of effort, the patient breathing deeply and rapidly, head drooping, forehead wrinkling, and eyes glancing about in an astonished way. “How many legs has a horse?” After long cogitation, the man counted slowly,—1, 2, 3, 4. “What’s your wife’s name?” “Marie—Marie, I think.”
A 31-year-old reservist was in the hospital around Christmas 1914 for rheumatism when he suddenly became agitated and was transferred to the Charité Psychiatric Clinic. He was restless all night, tossing in bed, grinding his teeth, and constantly getting up. He had a blank and shocked look on his face; his breathing was rapid and labored. There were no signs of pyramidal tract symptoms, but his muscle strength was reduced—more on the right side than the left. While the doctors were testing his knee-jerk reflexes, his legs moved (seemingly due to psychological factors). They found irregular areas of decreased sensitivity, and he registered less pain on the right side than on the left. During a mental exam, his responses seemed effortful; he was breathing deeply and quickly, his head drooping, forehead wrinkled, and his eyes darting around in disbelief. “How many legs does a horse have?” After a long pause to think, he counted slowly—1, 2, 3, 4. “What’s your wife’s name?” “Marie—Marie, I think.”
In the interpretation of this case, the functional paresis and hypalgesia of the right side, the functional pseudoclonus obtained during the knee-jerk test, the mental situation,—rather suggestive of a hysterical pseudodementia or a “Ganser” dazed state,—make the probable diagnosis at first sight psychogenic. Left to himself, however, the patient assumed a stereotyped unchanging posture; he would suddenly cry out, without particular emotion, that he was to be shot or executed; there was a tendency to rhythmic repetition of certain answers to questions, with the suggestion of perseveration.
In this case, the weakness and reduced sensitivity on the right side, the unusual reflex response observed during the knee-jerk test, and the mental state—which seems to indicate a type of hysterical pseudodementia or a “Ganser” dazed state—suggest that the likely diagnosis is psychogenic at first glance. However, when left alone, the patient took on a fixed, unchanging posture; he would suddenly shout out, without much emotion, that he was going to be shot or executed; there was a tendency to repetitively answer questions in a way that suggested perseveration.
After a time, pronounced rhythmic, and then stereotyped, movements started in. Suddenly negativistic phenomena, with refusal of food and self-accusatory ideas set in; speech stopped altogether. Information from his relatives showed that he had been peculiar for some time and had for years occasionally said that he was going to be shot.
After a while, rhythmic and then repetitive movements began. Suddenly, negative behaviors emerged, including refusing food and having self-blaming thoughts; he completely stopped speaking. Information from his relatives indicated that he had been acting strangely for some time and had occasionally mentioned for years that he was going to be shot.
Here then, instead of a hysterical pseudodementia, was a case of hebephrenia or perhaps catatonia. Possibly there had been no pseudodementia, but actually an elementary disorder in the associative process. Possibly the defects which the patient early showed, in his responses, for example, were really genuine schizophrenic blocking.
Here instead of a dramatic pseudodementia, there was a case of hebephrenia or maybe catatonia. It’s possible there wasn’t any pseudodementia, but rather a basic disorder in how the patient connected thoughts. The issues the patient initially displayed in his responses, for instance, might actually be genuine schizophrenic blocking.
According to Lewandowsky, almost all cases of neurasthenia, of hysteria, and of the so-called traumatic neuroses, stand out very clearly as functional. Bonhoeffer is far less certain that the diagnosis can be made readily in all cases. Antebellum conditions have not been continued in wartime; hysteria was a female affair antebellum, but under war conditions, it is found necessary to draw many differential diagnoses in the male betwixt schizophrenics, epileptics, and psychotics, on the one hand, and hysterics on the other.
According to Lewandowsky, nearly all cases of neurasthenia, hysteria, and the so-called traumatic neuroses are clearly functional. Bonhoeffer is much less confident that the diagnosis can be easily made in all situations. The conditions before the war haven't carried over into wartime; hysteria used to be seen as a female issue, but during the war, it's important to make many different diagnoses between men who are schizophrenic, epileptic, and psychotic, on one side, and those who are hysterical, on the other.
Re the so-called Ganser symptom, Hesnard has dealt especially with the value of what he calls the symptom of “absurd answers,” finding the differential diagnosis between dementia praecox and simulation particularly difficult. Hesnard states that incoherence is very hard to simulate. The answers of the Ganser patient are not always incorrect, and not always absurd. The patient strikes one as intact except for the absurd answers; intimidation and other external conditions affect the symptom greatly. Drugs are refused by the Ganser patient.
Re the so-called Ganser symptom, Hesnard has particularly focused on the significance of what he calls the symptom of “absurd answers,” finding it especially challenging to distinguish between dementia praecox and simulation. Hesnard notes that incoherence is very difficult to fake. The responses of the Ganser patient aren’t always wrong or absurd. The patient appears mostly intact apart from the absurd answers; external factors like intimidation significantly impact the symptom. The Ganser patient refuses medication.
“Hysteria”—actually dementia praecox.
“Hysteria”—actually schizophrenia.
Case 156. (Hoven, Henri, 1917.)
A shell burst about twenty-five meters away from a soldier, 21, but he continued in the military service thereafter for one month, having only one symptom, a trembling of the arm. This persisting, he was evacuated to Calais, then to Dury to the hospital for the insane where he stayed six months. He was transferred from Dury to the Belgian Hospital for the Insane at Chateaugiron on August 20, 1915. He remembered nothing of his stay at Dury, Calais, or of anything that happened after the shell-shock. He had no complaint and wanted to go back to the front. He was well oriented for time and space and had no disorders of association or perception. Besides the persistent, retrograde amnesia, he showed certain neurological disorders, occasional slight vertigo, a generalized tremor especially affecting the arms but disappearing almost completely at rest, lively tendon reflexes, intense dermographia and cardiac erethism. Diagnosis was made of acute, convulsional psychosis with agitation, convalescent phase.
A shell exploded about twenty-five meters away from a soldier, 21, but he continued his military service for another month, showing just one symptom: a trembling arm. When this continued, he was evacuated to Calais and then to Dury, where he stayed for six months in a mental hospital. He was transferred from Dury to the Belgian Hospital for the Insane at Chateaugiron on August 20, 1915. He remembered nothing about his time in Dury, Calais, or anything that happened after the shell shock. He had no complaints and wanted to return to the front lines. He was well oriented in time and space and had no issues with thought or perception. Apart from the ongoing retrograde amnesia, he displayed some neurological problems, occasional slight dizziness, a generalized tremor mainly affecting his arms that almost completely vanished at rest, strong tendon reflexes, intense skin reactions, and heightened heart sensitivity. The diagnosis was acute convulsional psychosis with agitation in the convalescent phase.
During March he was quiet and worked about the hospital. In April the patient had a number of seizures of an hysterical nature. In June it was possible to evacuate him to full convalescence. He went back to the front and stayed there, but shortly developed catatonic signs with visual hallucinations and delusions of persecution of a non-systematized nature, such as poisoning, being magnetized, etc. He was at this time poorly oriented for time, assumed bizarre and theatrical attitudes, showed Ganser’s symptom, was oversuggestible and agitated and sleepless. Diagnosis of dementia praecox was now clear.
During March, he kept to himself and worked around the hospital. In April, the patient experienced several hysterical seizures. By June, he was able to be discharged for full recovery. He returned to the front lines and remained there but soon started showing catatonic symptoms along with visual hallucinations and unfounded feelings of being persecuted, like fears of poisoning and being magnetized, among others. At this point, he was poorly oriented to time, exhibited strange and dramatic behaviors, displayed Ganser’s syndrome, was overly suggestible, and was restless and unable to sleep. The diagnosis of dementia praecox was now clear.
Hoven remarks that this case is important in that it suggests that a diagnosis of hysteria may easily be mistaken.
Hoven points out that this case is significant because it implies that a diagnosis of hysteria can easily be misinterpreted.
Influence of war experience on the content of hallucinations and delusions.
Influence of war experience on the content of hallucinations and delusions.
Case 157. (Gerver, 1915.)
In one of the divisional field hospitals Gerver examined a patient with a very vivid paranoic condition. The following were some of his hallucinations and delusions:
In one of the field hospitals, Gerver examined a patient with a very intense paranoid condition. Here are some of his hallucinations and delusions:
The patient asserted that everyone considered him a spy. Voices continually told him: “You are a spy.” “What? Spy? Caught? What?” “You will be shot by the Germans for espionage.” About three months before his present trouble, the patient had been wounded in left shoulder by a fragment of a large projectile. The wound healed and examination showed a big scar with attachments to the bone. The patient asserted that now he could not touch anything with his left hand, as there immediately go from it “some currents” to the Germans in the trenches and they at once begin shooting at the Russian position. Later, the patient could not even look in the direction of the German front, for all he had to do was to throw a glance in that direction and the Germans would at once begin a bombardment.
The patient claimed that everyone thought he was a spy. Voices constantly told him: “You are a spy.” “What? A spy? Caught? What?” “The Germans will shoot you for espionage.” About three months before his current issues, the patient had been injured in the left shoulder by a fragment of a large projectile. The wound healed, and an examination revealed a large scar attached to the bone. The patient insisted that now he couldn’t touch anything with his left hand because “some currents” immediately sent signals to the Germans in the trenches, prompting them to start shooting at the Russian position. Later, the patient couldn’t even look in the direction of the German front; all it took was a glance that would make the Germans begin a bombardment.
All these phenomena he explained as being due to the fact that the fragments of the large projectile which entered his shoulder were poisoned and charmed. Through these fragments there went currents from his hands to the Germans. The patient always supported his left hand with his right, in order not to touch anything with it. He slept only on his right side, so as not to touch the bed or floor with his left hand. During the examination and conversation the patient tried always to look downwards, so as not to throw a chance look in the direction of the German front and call out their fire.
All these phenomena he explained as being due to the fact that the fragments of the large projectile that entered his shoulder were poisoned and enchanted. Through these fragments, currents flowed from his hands to the Germans. The patient always supported his left hand with his right to avoid touching anything with it. He only slept on his right side to prevent his left hand from touching the bed or floor. During the examination and conversation, the patient consistently looked downwards to avoid glancing in the direction of the German front and provoking their fire.
An Iron Cross winner had a hysterical-looking attack (reminiscence of a bayoneted Gurkha). Later he begins to talk of “this damned war that is so vulgar” and of “atrocities, concrete and abstract”: Shortly the diagnosis, hebephrenia, had to be made.
An Iron Cross winner had a hysterical-looking attack (reminiscent of a bayoneted Gurkha). Later he starts talking about “this damn war that is so crude” and about “atrocities, both real and imagined”: Soon after, the diagnosis of hebephrenia had to be made.
Case 158. (Bonhoeffer, 1915.)
An Iron Cross winner, 21, in the field from August, 1914, to the middle of March, 1915, at first in France, later in Russia, finally went to hospital for rheumatism and sciatica. Three months later he had to be transferred to the Charité in a state of delirious excitement.
An Iron Cross winner, 21, served from August 1914 to mid-March 1915, initially in France and later in Russia, and eventually had to go to the hospital for rheumatism and sciatica. Three months later, he had to be moved to the Charité in a state of delirious excitement.
The attack began suddenly. He thought he was in the field telephoning with his captain, trembled, threatened to injure people about him, said he could not hold the position with the few men he had, and the like. Next day he quieted down and became oriented for time and place. He explained that he had seen a Gurkha coming upon him with a mallet, by way of revenge upon him because he had stuck his bayonet in the Gurkha’s breast. Behind a little hill he had seen Frenchmen and Englishmen, from which he drew the conclusion there was going to be an attack that night. A little cloud of dust he thought was enemy cavalry. In point of fact, he said he had once on patrol stuck a Gurkha through and the Gurkha’s eyes had since followed him in his mind. He had seen him crawling along the ground one evening and heard his step. The patient had imperfect insight into these hallucinations when questioned about them during the daytime, and still talked somewhat as if the experience was a real one.
The attack started all of a sudden. He believed he was in the field talking on the phone with his captain, he shook, he threatened to harm people around him, and he said he couldn’t hold the position with the few men he had, and so on. The next day, he calmed down and became aware of time and place. He explained that he had seen a Gurkha approaching him with a mallet, seeking revenge for having stabbed him in the chest with a bayonet. Behind a small hill, he had spotted French and English soldiers, leading him to conclude that there would be an attack that night. A small cloud of dust he thought was enemy cavalry. In fact, he mentioned that once while on patrol he had stabbed a Gurkha, and ever since, the Gurkha’s eyes had been following him in his mind. He had seen him crawling along the ground one evening and could hear his footsteps. The patient had a limited understanding of these hallucinations when asked about them during the day, and he still spoke as if the experience were real.
At first the situation seemed probably one of hysterical delusion, for which the Gurkha experience served as material. In point of fact, further observation in the clinic showed that the diagnosis of hysteria was wrong. He was induced to write out his experience in a style quite like his conversation; and there was a queer tendency in his writing to the use of[216] foreign words, somewhat improperly used. After a time he began to sit about dully and at times to run about and throw himself into and out of bed, or strike rhythmically with his shoes on the floor, or draw his shoulders together, making grimaces, rolling his eyes and breathing deeply. He said he had to make these movements involuntarily if he were in some way excited. But the peculiar conduct also often occurred without any emotional prod. His emotions were variable, but on the whole indifferent and not always quite suitable.
At first, the situation seemed like it was due to a hysterical delusion, drawing from the Gurkha's experience. However, further observation in the clinic revealed that the diagnosis of hysteria was incorrect. He was encouraged to write down his experiences in a way that reflected his conversational style; yet, there was a strange tendency in his writing to misuse foreign words. After a while, he began to sit around vacantly and sometimes would dart around, throw himself in and out of bed, or rhythmically tap his shoes on the floor. He would hunch his shoulders, make grimaces, roll his eyes, and breathe deeply. He claimed that he had to make these movements involuntarily if he was in any way stimulated. However, this peculiar behavior often occurred without any emotional trigger. His emotions were inconsistent, but generally indifferent and not always appropriate.
He frequently said he wanted to get into the field again, giving vent to superficial phrases, such as “atrocities, concrete and abstract,” and “this damned war that is so vulgar.” Yet a few minutes later he would say he wanted to go to war at Amsterdam as Amsterdam had pleased him very much. He said he now had a good many thoughts and ideas which formerly he had not had. He had not been promoted, he said, because he had once angered an officer in another company.
He often mentioned that he wanted to get back into the field, expressing superficial comments like “atrocities, both real and imagined,” and “this stupid war that is so crude.” Yet just a few minutes later, he would say he wanted to go to war in Amsterdam because he liked it a lot. He claimed he now had many thoughts and ideas that he hadn’t had before. He said he hadn’t been promoted because he had once upset an officer in a different company.
His field hospital history told of certain oddities, such as his lying stiffly in bed heedless of what was going on about him, falling into causeless depression, failing to sleep, and wandering about.
His field hospital history mentioned some strange behaviors, like him lying rigidly in bed, oblivious to everything happening around him, falling into unexplained bouts of depression, having trouble sleeping, and aimlessly wandering around.
As to previous life, only his own data were available. He had been a moderate scholar, had been rather irritable and thought a peculiar character. In the ward, he showed baseless antipathy to certain patients and said they were well. He seemed to have no insight into his condition, yet wrote in a letter that the insane state in which he was had very much “augmented his mental organism.” The diagnosis of early hebephrenic disorder could now be considered established.
As for his past life, only his own information was available. He had been an average student, somewhat irritable, and had a strange personality. In the facility, he expressed unreasonable dislike for certain patients, claiming they were fine. He appeared to lack understanding of his own condition, yet wrote in a letter that the insane state he was in had significantly “enhanced his mental capacity.” The diagnosis of early hebephrenic disorder could now be deemed confirmed.
Occipital trauma. Mystical visual hallucinations and explanatory delusions.
Occipital injury. Strange visual hallucinations and confusing delusions.
Case 159. (Claude, Lhermitte, Vigouroux, 1917.)
A soldier, 33, single, was wounded in the right occipital region by a shell burst September 25, 1915. There was no sign of focal lesion, but a trephining operation was done, which healed perfectly. No disturbance of vision ensued. The soldier was sent to convalesce two months after having been examined by P. Marie at the Salpêtrière. He went back to his regimental station and was put into the auxiliary service April 26, 1916.
A 33-year-old single soldier was injured in the right back of his head by a shell explosion on September 25, 1915. There were no signs of a specific injury, but a trepanation procedure was performed, which healed completely. There was no vision disturbance afterward. The soldier was sent to recover two months after being examined by P. Marie at the Salpêtrière. He returned to his unit and was assigned to auxiliary service on April 26, 1916.
In the early days of September, that is to say, a year after his injury, he had a vision. Above the church cross at Chantenay, where he then was, he saw a rainbow-colored bird, passing slowly in the sky. He lowered his eyes and the apparition followed and was projected on the white walls around him. After some time it disappeared. The soldier himself wondered whether his brain injury might not have something to do with the vision, but none of his comrades wounded in the head had had any such vision. So then he thought of tobacco, of which he was a moderate user, and stopped smoking, but the vision returned in the same intensity four months later. On examining the bird’s face carefully, he found that it was the Holy Virgin’s. In dreams he also had analogous visions and in the dreams the Holy Virgin spoke to him, but what she said he did not remember. The bird’s head did not speak to him. The soldier was now convinced that it really was the Holy Virgin who had visited him in the form of a bird. He remembered that he had asked Notre Dame de Lourdes to protect him on the day when he was injured. He had, in fact, eaten a bit of cheese that day upon which he had inscribed a prayer to the Holy Virgin.
In early September, a year after his injury, he had a vision. Above the church cross at Chantenay, where he was at that moment, he saw a rainbow-colored bird slowly flying in the sky. He looked down, and the vision followed him, casting shadows on the white walls around him. After a while, it vanished. The soldier wondered if his brain injury could have contributed to the vision, but none of his fellow injured comrades had experienced anything like it. So, he thought about tobacco, which he used moderately, and decided to stop smoking, but the vision returned with the same intensity four months later. When he carefully examined the bird’s face, he realized it resembled the Holy Virgin’s. He also had similar visions in his dreams, during which the Holy Virgin spoke to him, but he couldn't remember the words. The bird's head didn’t speak to him. The soldier was now convinced that it truly was the Holy Virgin who had appeared to him as a bird. He recalled that he had asked Notre Dame de Lourdes to protect him on the day of his injury. In fact, he had eaten a piece of cheese that day on which he had written a prayer to the Holy Virgin.
Sometimes he saw a red globe shining like a church lamp; sometimes white or black ladies descending from the sky; sometimes other visions. Now the Holy Virgin was to direct[218] all the soldier’s life, but why should he be specially favored? Was he not to be called sooner or later to hold a high rank? He confessed, in fact, that he was to be the King of France, and, like Joan of Arc, was to save his country. Now the soldier began to understand the hidden significance of his surroundings. Everything around him was symbolic, thus, white, of purity, order and royalty; red, of anarchy, disorder and atheism. Some white ship which he saw outstripping some darker ship showed him how the kingdom of France was arriving once more. In fact, there was a symbolism in the whites and yolks of eggs, and the proportion of yolk to white was as one to five. He made talismans to exorcise bad spirits.
Sometimes he saw a red globe shining like a church lamp; sometimes white or black figures coming down from the sky; sometimes other visions. Now the Holy Virgin was meant to guide[218] the soldier’s life, but why should he be singled out? Was he not destined to rise to a high rank sooner or later? He admitted, in fact, that he was going to be the King of France, and, like Joan of Arc, was meant to save his country. Now the soldier began to grasp the deeper meaning of his surroundings. Everything around him was symbolic; thus, white represented purity, order, and royalty; red symbolized anarchy, disorder, and atheism. A white ship he saw outpacing a darker ship showed him how the kingdom of France was making a comeback. In fact, there was a significance in the whites and yolks of eggs, and the ratio of yolk to white was one to five. He created talismans to ward off evil spirits.
Were there auditory hallucinations? If so, they were only episodic and took no part in either the construction or the fixation of the man’s delusional system. Thus, a voice once said to him, “All is not lost. You will be ——.” May 25, 1917, he entered the neurological center at Bourges.
Were there any auditory hallucinations? If so, they were just occasional and didn't play a role in the creation or solidification of the man's delusional system. One time, a voice told him, “All is not lost. You will be ——.” On May 25, 1917, he checked into the neurological center at Bourges.
As to the interpretation of this case, it seems that the patient’s mother had crises of depression which at one time caused her to be interned in the Charité. The contributors of this case do not believe that there can be any causal link set up between the mystical delusions and the brain injury.
As for the interpretation of this case, it appears that the patient's mother experienced episodes of depression that at one point led to her being admitted to the Charité. The contributors of this case do not think there is any causal connection between the mystical delusions and the brain injury.
As an auxiliary the soldier has a right to twenty per cent compensation for his head wound with loss of substance without bulging of the dura mater. Of course, as an insane person he must be retired. The aggravating or accelerating part played by fatigue, emotion and cranial trauma must, from the standpoint of compensation, be taken into account.
As an auxiliary, the soldier is entitled to twenty percent compensation for his head injury that resulted in a loss of tissue without bulging of the dura mater. Naturally, he must be discharged due to his mental illness. The contributing factors of fatigue, emotion, and head trauma must be considered when determining compensation.
Shell-shock dementia praecox.
Shell shock, dementia praecox.
Case 160. (Weygandt, 1915.)
A subaltern who had been in the service since 1909 was on patrol under shell fire from the enemy, but shortly thereafter came with his detachment into the zone of the German fire. Six men, two steps away from him, were killed by a shell. The officer remained stationary with the rest of his detachment until darkness set in, then returned, made his report in due order, but thereafter tremors set in over his whole body and he lost consciousness. He was carried to the hospital and on the way met his best friend whom he did not recognize. Arrived at the hospital he was unable to give answers to questions or obey requests for two or three hours. He thought he was hearing calls, commands and a dull dröhnen. If an automobile passed he was frightened and cried, “Auto! Auto!” He remained subject to inhibition, anxiety and insomnia for a long time; pulse accelerated; visual fields somewhat contracted for red. Face asymmetrically innervated and dermatographia. Sent to the reserve hospital, he was still apprehensive, especially at night, but in the course of a few days became perfectly tranquil. Only if he took part in the singing of war songs did he feel transient sensations in his knees.
A subaltern who had been in service since 1909 was on patrol under enemy shell fire when he and his unit found themselves in the German firing zone. Six men, just a couple of steps away from him, were killed by a shell. The officer stayed put with the rest of his team until it got dark, then returned and filed his report as required. However, after that, he started to shake all over and lost consciousness. He was taken to the hospital and on the way, he ran into his best friend but didn’t recognize him. Once at the hospital, he couldn’t answer questions or follow requests for two or three hours. He thought he was hearing calls, commands, and a dull rumble. Every time a car passed by, he would panic and shout, “Car! Car!” He dealt with anxiety, insomnia, and nervousness for a long time; his pulse was quickened; he had narrowed visual fields for red. His face was unevenly affected and showed signs of dermatographia. After being sent to the reserve hospital, he was still anxious, especially at night, but after a few days, he became completely calm. The only time he felt any temporary sensations in his knees was when he joined in singing war songs.
Here is a case of psychic shock with many traits, such as inhibition and hallucinations, suggestive of dementia praecox. The Abderhalden reactions (cortex, white matter, testes, not thyroid) all, according to Weygandt, are suggestive also of dementia praecox.
Here is a case of psychic shock with several characteristics, like inhibitions and hallucinations, that suggest dementia praecox. The Abderhalden reactions (cortex, white matter, testes, not thyroid) are also considered by Weygandt to suggest dementia praecox.
Shell-shock dementia praecox.
Shell shock dementia.
Case 161. (Dupuoy, 1916.)
A machine gunner, 23, was the sole survivor, March 18, 1915, of the explosion of a large calibre shell in a block house containing ten men. He worked himself out of the débris and came to Dupuoy’s attention in September, when an extension of leave was asked for him.
A 23-year-old machine gunner was the only survivor of a large shell explosion in a block house that held ten men on March 18, 1915. He managed to dig his way out of the rubble and caught Dupuoy's attention in September when someone requested an extension of his leave.
There were two groups of symptoms; persistent headache, painful hyperacousia, vertigo, tremulous walk, cervical spinal column stiff and painful both spontaneously and to pressure, muscular weakness, tremor of hands, hypesthesia of extremities especially upper, exaggeration of tendon and bone reflexes with tendency to ankle clonus and patellar clonus, sterno sign lively, frequent nosebleeds (two to four times a week), profound sweating, unequal pupils.
There were two groups of symptoms: a constant headache, sensitivity to sound, dizziness, shaky movements, a stiff and painful neck, muscle weakness, trembling hands, reduced sensitivity in the limbs, especially the upper ones, heightened reflexes with a tendency for ankle and knee jerks, a strong sterno sign, frequent nosebleeds (two to four times a week), excessive sweating, and uneven pupils.
On the mental side it was clear that the man’s character had changed, according to information supplied by the mother. Aprosexia, impairment of memory, recollective and retentive, inability to give age, birth date and similar data. Words came with difficulty. Some disorder of comprehension; stereotyped replies; negativism; indifference; he would sit hours in a chair or on a bed silent and inactive. Fixed attitudes; dull glance; eyelids half closed. In short, it seemed as if this patient was a case of catatonic dementia praecox.
On the mental side, it was obvious that the man's character had changed, based on what his mother said. He had aprosexia, which means he struggled with memory, both remembering and retaining information, and couldn't recall his age, birth date, or similar details. Words came to him with difficulty. There was some comprehension disorder; he responded in a stereotypical way; showed negativism; and was indifferent; he would sit for hours in a chair or on a bed, silent and inactive. He maintained fixed postures; had a dull look in his eyes; and his eyelids were half-closed. In short, it appeared that this patient was experiencing catatonic dementia praecox.
Re dementia praecox and shell-shock, Stansfield remarks upon the similarity of certain symptoms found in Shell-shock to those of dementia praecox; for example, apathy, retardation, amnesia and speech defect. According to Stansfield, one often gets the impression in a Shell-shock case as though the trench and shell fire stress had merely brought out a latent dementia praecox.
Regarding dementia praecox and shell shock, Stansfield points out the similarities in certain symptoms observed in shell shock and those of dementia praecox; for instance, apathy, slowing down, memory loss, and speech difficulties. Stansfield notes that in cases of shell shock, it often feels like the stress of trench warfare and shell fire has simply revealed a hidden dementia praecox.
Re his new “sterno” sign (sternomastoid contraction on percussion of neck at level of third dorsal vertebra), Dupouy claims it negative in normal subjects, positive in concussion, meningitis, and general paresis.
Re his new “sternal” sign (sternomastoid contraction when tapping the neck at the level of the third dorsal vertebra), Dupouy states it’s negative in normal subjects, positive in cases of concussion, meningitis, and general paresis.
Shell-shock; fatigue; fugue; delusions. Recovery.
PTSD; exhaustion; disassociation; hallucinations. Healing.
Case 162. (Red, 1915.)
A sergeant, 40, had had nineteen years of service and had been married five months when he was recalled to the colors when war broke out, and sent to the front. March, 1915, he was exposed to bomb explosions during a very intense bombardment. He then got into the way of saying that he was akin to everybody. April 20, he was evacuated on the score of general fatigue, rejoined the company May 17, left his comrades at the end of June, and was taken up as a deserter by the police, who, observing his state, brought him to a hospital. He there showed “cerebral overexcitement” with “incoherence and nervousness.” In two or three days he was much better. He was evacuated on the sixth day to the hospital at Vichy.
A 40-year-old sergeant had nineteen years of service and had been married for five months when he was recalled to duty when the war started and sent to the front lines. In March 1915, he was exposed to bomb explosions during heavy shelling. He then began to say that he felt a connection to everyone. On April 20, he was evacuated due to general fatigue and rejoined his unit on May 17. He left his comrades at the end of June and was detained by the police as a deserter. Noticing his condition, they took him to a hospital. There, he exhibited signs of “cerebral overexcitement” with “incoherence and nervousness.” In two or three days, he felt much better. On the sixth day, he was moved to the hospital in Vichy.
There was amnesia for the fugue and he could remember no further back than the extraction of a tooth at the Vichy hospital. In fact, he attributed the fugue to this dental operation. His wife took him home, but he soon threatened her with a revolver; got better in the night and next day went about apparently normal, buying things, however, extravagantly. His delusional state began once more, and two days later he was brought to Limoux. It seems that, while in Mauretania, he had formerly shown signs of mental disorder, having a mania for wireless and airplane inventions and the like. A cousin-german had also been in a hospital for the insane twice, recovering each time. There was a lingual and manual tremor. The man had not been recently alcoholic. He was a little irritable and showed a little megalomania, but worked hard and made himself useful. He went out, recovered, November 12, 1915.
He couldn't remember anything before the tooth extraction at the Vichy hospital due to amnesia from the fugue. He actually linked the fugue to the dental procedure. After his wife brought him home, he quickly threatened her with a gun; then he improved overnight and the next day acted completely normal, although he was spending money extravagantly. His delusions returned, and two days later, he was taken to Limoux. It turned out that while in Mauretania, he had previously shown signs of mental illness, having a strong obsession with radio and airplane inventions. A cousin had also been in a mental hospital twice and had recovered each time. He had a tremor in his hands and speech. He hadn't been drinking heavily recently. He was a bit irritable and exhibited some megalomania, but he worked hard and was helpful. He was released, fully recovered, on November 12, 1915.
Analysis indicated that this sergeant received a moral shock as a consequence of his fatigue and the shell fire, which emerged in a spell of confusion. It may be that his predisposition had something to do also with this spell and the fatigue. In any event, it seems as if the latter phenomena were not all assignable to war stress.
Analysis showed that this sergeant experienced a moral shock due to his exhaustion and the shelling, which resulted in a period of confusion. It's possible that his underlying disposition contributed to this confusion and fatigue as well. Regardless, it appears that these experiences weren’t solely related to the stress of war.
IX. CYCLOTHYMOSES
(THE MANIC-DEPRESSIVE GROUP)
A maniacal volunteer.
An overzealous volunteer.
Case 163. (Boucherot, 1915-6.)
An Alsatian became the object of much attention when he enlisted at the outbreak of the war in the infantry at the age of 59. He was interviewed and soon became more than naturally exuberant. The peculiar things he did soon brought him to Fleury in a gay and expansive mood, singing and talking as hail fellow with everyone he met.
An Alsatian attracted a lot of attention when he signed up for the infantry at the start of the war at the age of 59. He was interviewed and quickly became very lively. The unusual things he did soon brought him to Fleury in a cheerful and outgoing mood, singing and chatting comfortably with everyone he encountered.
The next day he grew more excited, disrobed and threw his things out of the window, filled his bed with excrement and wanted to smear the orderly therewith. He took other attendants for old friends and wanted to kiss them. His language and ideas were incoherent. He broke glass.
The next day, he became even more excited, stripped off his clothes, and threw his belongings out of the window. He filled his bed with waste and wanted to smear the orderly with it. He mistook other attendants for old friends and tried to kiss them. His speech and thoughts were jumbled. He shattered glass.
This situation of alternate joy and anger lasted one month, leaving him in an excitable, unruly state. He wrote many prolix letters to the prefects and the ministers, insisting on the discharge of certain patients and offering plans for the defense of France. He got better and finally, in October, 1914, was invalided home still slightly exalted.
This cycle of mixed joy and anger went on for a month, leaving him in a restless, agitated state. He wrote long, detailed letters to the prefects and ministers, pushing for the release of certain patients and suggesting strategies for defending France. He eventually improved and, by October 1914, returned home still a little high-spirited.
Re the cyclothymias, Montembault remarks that manias have been less numerous than melancholias in the present war, whereas in 1870, manias were more common than melancholias. Morselli likewise remarks upon the rarity of manias amongst the Italian soldiers. Butenko reports upon the maniacal cases amongst the Russians and how the men wish to enter the ranks, the women the nurse corps. E. Meyer, for Germany, found 4 per cent manic-depressives. Birnbaum quotes from Bonhoeffer (3 per cent) and Hahn (2 per cent) for war times as against Stier’s 9.5 per cent of cyclothymic cases in the antebellum period, 1905-1906.
Re the cyclothymias, Montembault notes that there have been fewer manic episodes compared to depressive ones in the current war, while in 1870, manic episodes were more frequent than depressive ones. Morselli also observes that manic episodes are rare among Italian soldiers. Butenko reports on the manic cases among the Russians and how the men want to join the ranks, while the women aspire to join the nursing corps. E. Meyer, for Germany, found 4 percent of manic-depressives. Birnbaum references Bonhoeffer (3 percent) and Hahn (2 percent) for wartime occurrences compared to Stier’s 9.5 percent of cyclothymic cases during the pre-war period, 1905-1906.
Fugue: melancholia.
Fugue: sadness.
Case 164. (Logre, 1916.)
Logre classifies as a melancholic fugue the adventures of a man who had been depressed for some days, had stopped talking and eating, and ran away suddenly in the middle of an attack of anxious agitation. He was very anxious over the health of his daughter, whom he thought to be severely ill. It was, in fact, to go to Paimpol that he deserted, but he deserted with his arms and without any money. He went off on foot “in the Brittany direction.” He had gone 50 kilometers, the next day, and was picked up near Chateau-Thierry by two gendarmes, who fell upon him, seeing his regalia, and cried, “Give yourself up!” He replied in a firm voice, “No, I shall not give myself up!” and seizing his gun he made at one of the gendarmes. There was a fight. The gendarme declared in his report that he judged it opportune to retreat behind a tree. The soldier, knowing his trench lore very well, barricaded himself behind a pile of beets. There he would have held the gendarmes in check for some time if another had not succeeded by a détour through some woods, in catching him. He gave himself up after firing several ineffective shots, but not without getting a bullet in his left thigh himself. With the charge of desertion and attempt to murder, he was handed over for mental examination. He was, in fact, a melancholic patient, subject to attacks of anxiety, and requiring long observation at a neuropsychiatric center for diagnosis.
Logre describes the story of a man who had been feeling down for a few days, stopped talking and eating, and suddenly ran away during a moment of intense anxiety. He was extremely worried about his daughter's health, believing she was very sick. He actually set off for Paimpol, but he left without his gear and any money. He started walking “in the direction of Brittany.” By the next day, he had covered 50 kilometers and was found near Chateau-Thierry by two police officers, who, upon seeing his appearance, shouted, “Surrender!” He responded firmly, “No, I won’t surrender!” and, grabbing his gun, charged at one of the officers. A struggle ensued. One officer later reported that he felt it was wise to take cover behind a tree. The soldier, well-versed in combat tactics, took refuge behind a pile of beets. He managed to hold off the officers for a while until another officer, taking a different route through the woods, caught him. He surrendered after firing several ineffective shots, but not without sustaining a bullet wound in his left thigh. He was then charged with desertion and attempted murder and was sent for a mental evaluation. It turned out he was dealing with depression and anxiety and needed extended observation at a neuropsychiatric facility for a proper diagnosis.
Chavigny observed numerous victims of melancholia characterized by war terror. He remarks a somewhat curious fact that, whereas the melancholics were numerous and their mental states related to the war, on the other hand, the paretics were rather apt to be maniacal than melancholic. Soukhanoff, however, remarks on the occurrence of depression in a great number of types of psychosis, as was found in the Russo-Japanese war. Soukhanoff found frequent instances of schizophrenia, wherein the melancholia tends to conceal the actual dementia praecox. Soukhanoff predicted that depression will figure largely in the war.
Chavigny noted many victims of depression caused by the terror of war. He points out an interesting fact: while there were many people suffering from depression related to the war, those with paralysis were more likely to be manic than depressed. Soukhanoff, however, mentions the presence of depression in many types of psychosis, similar to what was observed in the Russo-Japanese war. He frequently encountered cases of schizophrenia where the depression tended to hide the actual dementia praecox. Soukhanoff predicted that depression would play a significant role in the war.
Apples in No-Man’s-Land.
Apples in No Man's Land.
Case 165. (Weygandt, 1915.)
A soldier in November, 1914, suddenly climbed out of the trench and began to pick apples from an apple-tree between the firing lines. The idea was to get a bag of apples for his comrades, but he began to pelt the French trenches with apples. He was called back and on account of his strange conduct sent to hospital. Here he was at times given to pressure of speech and restlessness; he would climb the posts of the sleeping room and then loudly declare he wanted to get back to the trenches; he did not want to go back to Germany alive; did not want to live over to-morrow; was guilty of a sin; had a spot of sin, Schand, on his heart. Sometimes he refused food and said anything else tasted better. It seemed he had formerly talked about the Iron Cross.
A soldier in November 1914 suddenly climbed out of the trench and started picking apples from a tree between the firing lines. His plan was to gather a bag of apples for his fellow soldiers, but instead, he began to throw the apples at the French trenches. He was called back and, due to his bizarre behavior, was sent to the hospital. While there, he occasionally struggled with pressured speech and restlessness; he would climb the posts in the sleeping room and loudly say he wanted to return to the trenches; he didn't want to go back to Germany alive; he didn't want to live to see tomorrow; he felt guilty about a sin; he had a spot of sin, Schand, on his heart. At times, he refused food, claiming anything else tasted better. It seemed he had previously talked about the Iron Cross.
After being transported to Germany, he was at first a little negativistic and apparently blocked. He talked about his experiences and said he wanted to go to Russia. He explained the episode of the apples on the basis that they were all really hungry and that he had sought to encourage his comrades who were unused to war. He had noticed the French all shot too high.
After being taken to Germany, he was initially a bit negative and seemed stuck. He shared his experiences and mentioned wanting to go to Russia. He explained the apple incident by saying they were all really hungry, and he tried to motivate his comrades who were inexperienced with war. He had observed that the French always aimed too high.
Physically there was a somewhat uneven innervation of the face, unilateral epicanthus and an areflexia of pharynx. Now and then the man was very irritable, but in general he was in an elevated frame of mind.
Physically, there was a bit of uneven nerve supply in his face, one-sided epicanthus, and a lack of reflexes in the pharynx. Occasionally, the man was quite irritable, but overall, he was in a pretty good mood.
Weygandt interprets this case as one of hypomania, remarking that war influences may serve to bring out preëxisting manic depressive tendencies.
Weygandt interprets this case as a form of hypomania, noting that wartime factors can trigger existing manic depressive tendencies.
Re differential development of mania and depression, see remarks under Cases 163 (Boucherot) and 164 (Logre).
Re the different development of mania and depression, see comments under Cases 163 (Boucherot) and 164 (Logre).
Four months in trenches: Depression; war hallucinations, arteriosclerosis (aged 38).
Four months in the trenches: Depression; war-related hallucinations, artery hardening (at 38 years old).
Case 166. (Gerver, 1915.)
A Russian reservist, a private, 38, went into the trenches, March, 1915. Without taking part in any battles or sustaining any injury, he four months later became depressed and had to be evacuated to a hospital and thence to the interior, little changed for the better.
A 38-year-old Russian reservist, a private, went into the trenches in March 1915. Without engaging in any battles or getting hurt, he became depressed four months later and had to be evacuated to a hospital, then transferred to the interior, which offered little improvement.
He was an ill-nourished man, of middle height, with pallid skin and membranes; arteries sclerotic; face, eyelids, and tongue finely tremulous; hands tremulous; slight dermatographia; exaggerated tendon reflexes; pulse 100.
He was a poorly nourished man of average height, with pale skin and thin membranes; his arteries were hardened; his face, eyelids, and tongue trembled slightly; his hands shook; he had mild skin sensitivity; his tendon reflexes were exaggerated; his pulse was 100.
He seemed disoriented for time and place; looked weary; walked with back bent over; spoke in whispers, and appeared somewhat unclear. Thinking was slow and difficult.
He seemed confused about the time and place; looked tired; walked with a hunched back; spoke in whispers, and appeared a bit unclear. Thinking was slow and hard.
He occasionally shuddered and looked to one side, said he was afraid, and was constantly troubled by thoughts of fire. The Germans were pursuing him; he could hear their voices and footsteps. He himself was doomed, and his family also; he felt he was the cause of all the domestic woe. His own heart was dying away; he had fits of anguish and causeless fear, and was under the constant expectation of death.
He sometimes shuddered and glanced to one side, admitting he was scared and was always troubled by thoughts of fire. The Germans were after him; he could hear their voices and footsteps. He felt he was doomed, and so was his family; he believed he was responsible for all the misery at home. His own heart was fading; he experienced bouts of intense pain and irrational fear, living in constant anticipation of death.
One day, he escaped from the hospital and went to the chief physician’s tent, where he lay on the ground. When he was found and asked why he was there, he begged the physician to save him from the Germans. The man was not alcoholic and had no previous history of mental disease.
One day, he ran away from the hospital and went to the chief physician’s tent, where he lay down on the ground. When they found him and asked why he was there, he pleaded with the doctor to save him from the Germans. The man was not an alcoholic and had no prior history of mental illness.
Re early arteriosclerosis, Maitland in the second interim report of the British Association Committee on Fatigue in Warfare, speaks of the many Serbians, who, after six years of nearly continuous Balkan war, show a marked arteriosclerosis. Maitland remarks that the line officers were already showing (1916) a growing delicacy of perception as to the “breaking point.” Men that do not break may return from the lines, pale, with low blood pressure, and a faiblesse irritable, shown by restlessness of hands and feet.
Re early arteriosclerosis, Maitland in the second interim report of the British Association Committee on Fatigue in Warfare, talks about the many Serbians who, after six years of almost continuous Balkan war, show significant arteriosclerosis. Maitland notes that the line officers were already displaying (1916) a heightened sensitivity to the “breaking point.” Men who don’t break might return from the front lines looking pale, with low blood pressure, and an irritable weakness, shown by restless hands and feet.
War stress: Manic-depressive psychosis.
War stress: Bipolar disorder.
Case 167. (Dumesnil, 1915-6.)
A naval officer, 22, transferred from sea service, went into Belgium, November, 1914, in a Fusilleur brigade of marines and there greatly distinguished himself, growing very weary and enervated, however, about the middle of April, 1915. His attitude to the men altered: he sometimes struck them; gently, though, according to his account. They must do in ten seconds what they really could not do under ten minutes. The officer, in fact, had lost all notion of time. He went about agitatedly, contradicted his superior officers and was troubled because, as he said, they often were men of inexperience as compared to himself. He grew irritated, too, because there were Free Masons in the army and when he was sent to the asylum in July, 1915, said it was the doing of the Free Masons. He did not seem to have any hallucinations. His ideas and sentiments were very labile, and a bit confused, and not all his interpretations dealt with Free Masons and occultism. August 5, however, the phase of calmness was again followed by agitation; he broke things and laughed explosively. August 10, another attack occurred, with destructiveness. During the next few days there were alternate phases of depression and excitation. He was negativistic, resistive and struck attendants.
A 22-year-old naval officer, who had transferred from sea service, arrived in Belgium in November 1914 as part of a marine Fusilier brigade. He distinguished himself but grew increasingly exhausted and worn out by mid-April 1915. His attitude toward the men changed; he sometimes hit them, though he described it as gentle. He expected them to do tasks in ten seconds that they realistically couldn't complete in less than ten minutes. He had completely lost track of time. He moved around restlessly, contradicted his superiors, and was frustrated because, as he claimed, they often lacked experience compared to him. He became angry, too, about the presence of Free Masons in the army, and when he was sent to the asylum in July 1915, he said it was because of the Free Masons. He didn’t appear to have any hallucinations. His thoughts and feelings were very unstable and somewhat confused, and not all his concerns were about Free Masons and the occult. However, on August 5, he experienced another wave of agitation after a period of calm; he broke things and laughed uncontrollably. On August 10, he had another destructive episode. In the following days, he went through alternating phases of depression and excitement. He was negative, resistant, and struck the attendants.
Re war stress and psychoses, Morselli finds the acute cases on psychopathic soil. First in the list, he places the neurasthenias and psychasthenias, and second, the hysterias, two groups which, more than the remainder, may be said to constitute the so-called Shell-shock group. Third, he found depressions ranging over into a delusional state with suicidal ideas; fourth, a species of stupor, occasionally catatonic, recalling dementia praecox; fifth, transient hallucinatory states; sixth, confusions (Meynert’s amentia?); last, manias.
Re war stress and psychoses, Morselli identifies the acute cases on a psychopathic background. He first lists neurasthenias and psychasthenias, followed by hysterias, which are two groups that, more than the others, can be said to make up what we now call the Shell-shock group. Third, he found depressions that escalated into a delusional state with suicidal thoughts; fourth, a type of stupor, sometimes catatonic, reminiscent of dementia praecox; fifth, temporary hallucinatory states; sixth, confusions (Meynert’s amentia?); and finally, manias.
The above case of Dumesnil appears to be a pure case of manic-depressive psychosis developing on the war basis, but perhaps merely comes from a latent cyclothymia.
The case of Dumesnil looks like a straightforward instance of manic-depressive psychosis triggered by the war, but it might just stem from an underlying cyclothymia.
Predisposition; war stress: Melancholia.
Predisposition; war stress: depression.
Case 168. (Dumesnil, 1915-6.)
A farmer, 30, was mobilized August 2, 1914, and was wounded in the hand September 27. He went back to his dépôt in December and stayed there until March, 1915, when he was sent to Dunkirk. Before leaving the dépôt he said that he had heard soldiers declaring that he was not doing his duty, that he was going to be court-martialed, that life was at an end for him. At Dunkirk he said these same soldiers continued to say the same things about him, forming a band about him, led off by a subaltern officer who meant to frighten him and to make him talk. One night sulphur was thrown at him for poisoning purposes; he complained of this to a sergeant and declared he did not understand why he should be thus pursued. After the bombardment of Dunkirk the hallucinations grew more intense. He was sent to hospital and was so harried by the voices that he wanted to throw himself down a staircase but was caught in time. At the hospital for the insane he complained that his thoughts were being heard and loudly repeated; he was made to make incoördinate movements; was treated as a spy. He thought he must be a German or they would not treat him so. He waited for death as he wanted to be executed at once.
A 30-year-old farmer was called up on August 2, 1914, and got injured in his hand on September 27. He returned to his unit in December and stayed there until March 1915, when he was sent to Dunkirk. Before leaving, he mentioned that he heard soldiers saying he wasn't doing his duty, that he would be court-martialed, and that his life was over. In Dunkirk, those same soldiers continued to say the same things about him, forming a group around him, led by a junior officer who aimed to intimidate him and make him talk. One night, someone threw sulfur at him, supposedly to poison him; he reported this to a sergeant and expressed confusion about why he was being targeted. After the bombing in Dunkirk, his hallucinations intensified. He was sent to the hospital and was so tormented by voices that he wanted to throw himself down the stairs but was stopped in time. In the psychiatric hospital, he complained that his thoughts were being heard and repeated loudly; he was forced to make disjointed movements and was treated like a spy. He thought he must be treated as a German, or else they wouldn’t treat him this way. He longed for death, wanting to be executed immediately.
This man’s father was alcoholic. He himself at the age of fourteen had had a period of neurasthenia with some sort of nervous seizure for a period of five months. At 28 he had a rheumatic seizure which kept him in bed fifty days. A daughter born to his wife had died a few days after birth.
This man's father was an alcoholic. By the time he was fourteen, he experienced a phase of anxiety with some kind of nervous breakdown that lasted for five months. When he was 28, he suffered a rheumatic episode that kept him in bed for fifty days. A daughter born to his wife passed away just a few days after birth.
Dumesnil’s analysis is melancholia with delusions of persecution, due to war stress in a predisposed person.
Dumesnil’s analysis is depression with paranoia, caused by war stress in someone who's already vulnerable.
Re melancholia and the war stress, see remarks under Case 167. Re manic-depressive psychosis in the Russians, Khoroshko found 9.4 per cent of manic-depressive cases, the same percentage of epilepsies, 10 per cent of paretics, and 20.4 per cent of schizophrenic cases amongst a group of 318 neuro-psychiatric cases. Almost all his manic-depressive cases had been patently so antebellum.
Regarding melancholia and the stress from the war, see comments under Case 167. As for manic-depressive psychosis in the Russians, Khoroshko found 9.4 percent of manic-depressive cases, the same percentage of epilepsies, 10 percent of paretics, and 20.4 percent of schizophrenic cases among a group of 318 neuro-psychiatric cases. Almost all his manic-depressive cases had clearly been so before the war.
Depression; low blood pressure. Pituitrin.
Depression; low blood pressure. Pituitrin.
Case 169. (Green, 1917.)
A private, 22, was sent back from Germany as insane. He had been in the asylum at Giessen seven months, and a prisoner in all fifteen months.
A private, 22, was returned from Germany as insane. He had spent seven months in the asylum at Giessen and had been in custody for a total of fifteen months.
August 16, 1916, he was admitted to Mott’s wards at Maudsley in a markedly depressed and lethargic condition. He had improved somewhat in October, but still had periods of depression. He was put on thyroid extract (Green’s treatment was in doses measuring from gr. ¼ to gr. 1, t.d.s.; according to Green, the effect of thyroid extract is more rapid when coupled with pituitrin). In December he was given pituitrin extract gr. 2, t.d.s. In January, 1917, he was no longer depressed or lethargic. He complained of pain in his back, found to be due to a bullet. This was removed.
On August 16, 1916, he was admitted to Mott’s wards at Maudsley in a noticeably depressed and lethargic state. He improved somewhat in October but still experienced bouts of depression. He was prescribed thyroid extract (Green’s treatment ranged from ¼ grain to 1 grain, taken three times a day; according to Green, thyroid extract works faster when combined with pituitrin). In December, he was given pituitrin extract at 2 grains, taken three times a day. By January 1917, he was no longer depressed or lethargic. He mentioned having back pain, which was found to be caused by a bullet. This was removed.
Re prisoners, Imboden found amongst 20,000 French soldiers taken prisoner at Verdun after the severest drum fire and strain, only five neurotic cases (data of Mörchen), and Wilmanns found but five neurotic cases amongst 80,000 prisoners. Lust reviewed 20,000 war prisoners in Germany and found singularly few instances of neurosis. Shunkoff notes, however, that there are a number of psychotic cases amongst the prisoners because the mentally diseased who do not disturb the military routine are kept in the line. Bonhoeffer found amongst Serbians taken prisoners by Germany, emaciation, atrophy, heart disease, and frequently tuberculosis. (See Case 166.) Bonhoeffer noted the absence of psychoses amongst these Serbians, drawing the general conclusion that campaign stress was unable to bring out psychoses. But, although the exhaustion psychoses are not found, there are exhaustion neuroses or states of acute nervous exhaustion, characterized by somnolence and depression, followed by a mild degree of overemotionality. vum Busch states that interned German civilians have gone into psychosis frequently. It is said that one in 10,000 war prisoners in Germany has committed suicide. Bishop Bury found at Ruhleben 60 or 70 cases of psychosis.
Re prisoners, Imboden found among 20,000 French soldiers captured at Verdun after intense artillery fire and stress, only five cases of neurotic disorders (data from Mörchen), while Wilmanns found just five neurotic cases among 80,000 prisoners. Lust reviewed 20,000 war prisoners in Germany and discovered remarkably few instances of neurosis. Shunkoff notes, however, that there are several psychotic cases among the prisoners because those with mental illness who do not disrupt the military routine are kept in the line. Bonhoeffer found among the Serbians captured by Germany signs of malnutrition, atrophy, heart disease, and often tuberculosis. (See Case 166.) Bonhoeffer observed the absence of psychoses among these Serbians, concluding that campaign stress was unable to trigger psychoses. However, while exhaustion psychoses are not present, there are exhaustion neuroses or states of acute nervous exhaustion, characterized by sleepiness and depression, followed by a slight degree of overemotionality. vum Busch states that interned German civilians frequently develop psychosis. It is reported that one in 10,000 war prisoners in Germany has committed suicide. Bishop Bury found 60 to 70 cases of psychosis at Ruhleben.
X. PSYCHONEUROSES
Hallucination in the field (surprise by BOCHES); scalp wound: Three psychopathic phases—(a) over-emotionality, (b) obsessions, (c) loss of feeling of reality (victim a “constitutional intimiste”).
Hallucination in the field (surprise by BOCHES); scalp injury: Three psychopathic phases—(a) over-emotionality, (b) obsessions, (c) loss of sense of reality (victim a “constitutional intimiste”).
Case 170. (Laignel-Lavastine and Courbon, July, 1917.)
A cashier, 31 (of rather weak constitution but without hereditary or acquired mental taint—a religious man and for religious reasons chaste, always given to metaphysical speculation and introspection, but on the other hand, much interested in sports and very sympathetic with English manners), was about to go to live in the country on the advice of his physician when the war broke out. He was called to the colors and shortly lost his tendency to bronchitis, put on flesh, and felt delighted with his situation.
A 31-year-old cashier (who had a somewhat fragile constitution but no inherited or developed mental issues—a religious man who remained chaste for his beliefs, usually inclined toward deep thinking and self-reflection, but also very interested in sports and quite appreciating of English customs) was planning to move to the countryside on his doctor’s advice when the war started. He was drafted and soon overcame his tendency for bronchitis, gained weight, and felt pleased with his circumstances.
After almost two years of effective service, June 2, 1916, when his troop was cautiously advancing into a trench at the end of which they might be taken by surprise, suddenly the officer cried, “Sauve qui peut! The Boches are on us!” The patient remembered seeing Germans emerge from every side, remembered his fear, how he had turned about and crossed over a palisade, and then no more until he found a scalp wound being staunched by his comrades in the trench. He put on his own dressing and followed his comrades on foot.
After almost two years of dedicated service, on June 2, 1916, while his troop was cautiously moving into a trench where they could be caught off guard, the officer suddenly shouted, “Save yourselves! The Germans are upon us!” The soldier recalled seeing Germans coming from all directions, remembered his fear, how he turned around and climbed over a barricade, and then everything went blank until he found his comrades in the trench treating a head wound he had. He applied his own bandage and followed his comrades on foot.
He quickly got well of his scalp-wound but remained in hospital, very weak, extremely impressionable, jumping at every noise. He got somewhat better with the rest in bed, though even a month after his hallucination, he had a spell of insomnia, thinking about his future and the possibility of a relapse, and having war dreams from which he would awake in a sweat. Once on awaking, he distinctly heard a voice saying, “Well, Charles?” This hallucination occurred five times, under exactly the same circumstances, except that once it was in the daylight. Adrenalin was given, 1:1000, 10[230] drops the first day, 20 the second, 30 the third, and a like amount on the following days. After three days of such treatment, the patient said he felt much better. Later he had a period in which he had lost self-control and could no longer take any initiative. Thus, if he wanted to reply to his mother, it seemed to him that some one not himself was ordering him to write. He now asked himself if he were not really dreaming. He would not be sure of his actual existence unless something happened to prove it, such as the nurse’s bringing him a plate.
He quickly recovered from his scalp wound but stayed in the hospital, feeling very weak, extremely sensitive, and startled by every noise. He improved a bit with the rest in bed, but even a month after his hallucination, he experienced insomnia, worrying about his future and the chance of a relapse, and having war nightmares that made him wake up in a sweat. One time when he woke up, he clearly heard a voice saying, “Well, Charles?” This hallucination happened five times, under exactly the same conditions, except for once when it was during the day. He was given adrenaline, 1:1000, 10[230] drops the first day, 20 the second, 30 the third, and similar amounts in the days that followed. After three days of this treatment, he said he felt much better. Later, he experienced a time when he lost self-control and could no longer take any initiative. So, if he wanted to respond to his mother, it felt like someone other than himself was telling him to write. He began to wonder if he was really dreaming. He wouldn’t be sure of his actual existence unless something happened to prove it, like the nurse bringing him a plate.
In short as the first phase of diffuse over-emotionality had been succeeded by a second of obsessions, so the obsessive phase was succeeded by a third phase of mild loss of the feeling of reality. The first phase following the wound was one of disorder of attention, of memory, and in fact of all the mental functions, associated with tremors, tachycardia and dizziness. The second phase seemed, as it were, to crystallize intellectually the anxious apprehensiveness of the first phase. There were fears that the ceiling would fall; there were scruples concerning the past; there were fearful premonitions for the future (such as, that any bomb he might pick up would burst). According to Laignel-Lavastine and Courbon, there may have been a predisposition in the vegetative system of this subject, or even a basis in his tuberculosis, of which, in fact, the X-ray showed still some slight evidences. The obsessions appeared at night, at a time, namely, when the vital rhythm is passing from a sympathotonic period over into a vagotonic period, at a time when the organic sensations are apt to swim to the fore. According to this analysis, these somatic sensations, precisely those that the battlefield had also brought out, brought out again the other emotions which he had felt on service. It was always the emotions first developed in military service that were revived in the disease. In the third phase, the physical condition of the patient had grown much better pari passu with disappearance of the obsessions and the onset of the personality disorder. The adrenalin raised arterial tension, and going down to the sympathetic caused the anxiety and war emotions linked therewith to disappear; but the adrenalin treatment,[231] according to Laignel-Lavastine and Courbon, disturbed the organic sensations so suddenly that there was a break between the new conscious status and the old. In consequence, the patient felt that these new sensations no longer really belonged to him but were of a xenic character, imposed upon him from without in such wise that he continually asked himself whether he was really dreaming or no. This man was a constitutional intimiste; a psychasthenic en herbe.
In brief, just as the first phase of overwhelming emotions was followed by a second phase of obsessions, the obsessive phase was then followed by a third phase marked by a mild sense of disconnection from reality. The initial phase after the injury involved issues with attention, memory, and indeed all mental functions, along with symptoms like tremors, rapid heartbeat, and dizziness. The second phase seemed to crystallize the anxious feelings of the first phase on an intellectual level. There were worries that the ceiling would collapse; there were regrets about the past; there were anxious predictions about the future (like worrying that any bomb he might come across would detonate). According to Laignel-Lavastine and Courbon, there may have been a predisposition in the subject's autonomic nervous system, or even a link to his tuberculosis, which X-rays still showed some slight signs of. The obsessions surfaced at night, at a time when the body's vital rhythms shift from a sympathetic state to a parasympathetic one, making organic sensations more prominent. This analysis suggested that these bodily sensations, which the battlefield had also triggered, brought back the other emotions he had experienced during his service. It was always the feelings first developed during military service that reemerged during the illness. In the third phase, the patient's physical condition had improved significantly alongside the fading of the obsessions and the emergence of personality issues. The adrenaline increased blood pressure, and its effect on the sympathetic nervous system caused the anxiety and related wartime emotions to dissipate; however, according to Laignel-Lavastine and Courbon, adrenaline treatment disturbed the organic sensations so abruptly that there was a disconnect between the new conscious state and the previous one. As a result, the patient felt that these new sensations no longer truly belonged to him but seemed foreign, as if imposed on him from the outside, leading him to constantly question whether he was actually dreaming or not. This man was a natural intimiste; a budding psychasthenic en herbe.
Re neurasthenia, Lépine notes that there are transient and relatively permanent cases. The term is often used to cover graver disorders, such as various melancholias and anxieties. As a rule, in France, the neurasthenics are evacuated for fatigue. There have been a number of cases in officers, who find themselves unable to make decisions on the minute and to remember military facts, or perhaps are unable to make any physical or intelligent effort whatever. A true neurasthenic, however, ought not to be a confused person. He is a man with a rather unusual clarity of view as to his situation; and his trouble appears to him to be somatic rather than as of the nature of a depression. He feels that, if he could only rest, he could be cured. Neurasthenia, according to Lépine’s war experience, is practically always the disease of a highly cultivated nervous system, and appears in men who have undertaken responsibilities. There is a group of young men who have never been physically strong, bowled over at last by some small event, such as a diarrhoea, and unable to carry on. Such men, perhaps, are likely to have some traces of an old tuberculosis, an adrenal insufficiency, or insufficient hepatic function. Martinet has found them hypotensive and rather poorly aerated. There is another group of neurasthenics (Maurice of Fleury) that are old arthritics, with increased tension. These cases are not found at the front because conditions there rather tend to reduce the trouble; but they are found doing office work in the interior. Besides these cases of the “cultivated” group, Lépine also finds a number of neurasthenics amongst the peasants, in whom anxious ideas may lead to hypochondria.
Re neurasthenia, Lépine points out that there are temporary and more lasting cases. The term is often used to refer to more serious conditions, like various forms of depression and anxiety. Generally, in France, those with neurasthenia are treated for fatigue. There have been several cases among soldiers who find themselves unable to make quick decisions or remember military information, or who struggle to make any physical or mental effort at all. However, a true neurasthenic should not be confused. He has a clear understanding of his situation; he perceives his issue as physical rather than depressive. He believes that if he could just get some rest, he could recover. According to Lépine’s experience during the war, neurasthenia typically affects those with highly developed nervous systems and is seen in men who have taken on significant responsibilities. There’s a group of young men who have never been very strong, who finally break down after experiencing a minor incident, like diarrhea, and become unable to cope. These men might show signs of old tuberculosis, adrenal insufficiency, or poor liver function. Martinet has found them to be hypotensive and somewhat under-oxygenated. There’s another group of neurasthenics (Maurice of Fleury) who are older individuals with arthritis and increased tension. These cases aren’t found at the front lines because the conditions there tend to alleviate the problem; instead, they are seen working in offices inland. Besides these "cultivated" cases, Lépine also identifies a number of neurasthenics among farmers, where anxious thoughts may lead to hypochondria.
Fugue, hysterical.
Fugue state, panicked.
Case 171. (Milano, May, 1915.)
The fugue of an adjutant who left his regimental relief post at Palameix Farm and was found several days later with his family at Castelsarrasin, was reconstructed from partial records as follows:
The story of an adjutant who abandoned his duty at Palameix Farm and was discovered several days later with his family in Castelsarrasin was pieced together from incomplete records as follows:
November 27, 1914, after a night in the trenches, when two shells burst near him, the adjutant turned up at the relief post with wild eyes and a complaint of fatigue, and of an old wound and headaches. The wound he had gotten in a fight which gained him his grade of adjutant. The physician prescribed rest. He sat down by the stove, silent and dejected, and at about four o’clock, in the presence of the medical assistant, made preparations to go, leaving sack and saber behind, but taking outer garments and revolver case. On the way from the farm, he met comrades and told them he had been evacuated to his dépôt on the colonel’s order, and walked with them, Indian file, in the midst of falling shells, the others talking but the adjutant himself silent. At nightfall, he said, “Good evening,” and parted from them. Of his further course to his home, all recollection was lost by the adjutant; in fact, he did not remember anything beyond the Palameix Farm, where he had seen a comrade wounded in the head. He got home November 29th, at eight in the morning. He had most of his money with him, having traveled by train some distance without a ticket; moreover, without asking for a ticket, and without having eaten. When the ticketman in his home town asked him whether he was back from the war, he looked at him vaguely and went out without replying; nor did he reply to a newspaper man on the road home. This was the more strange as he was ordinarily an affable person.
On November 27, 1914, after a night in the trenches, the adjutant showed up at the relief post with wild eyes, complaining of fatigue, an old injury, and headaches after two shells exploded nearby. He had gotten the injury in a fight that earned him his rank as adjutant. The doctor advised him to rest. He sat by the stove, quiet and downcast, and around four o'clock, with the medical assistant present, he got ready to leave, leaving behind his sack and saber but taking his outer clothes and revolver case. On his way from the farm, he encountered some comrades and told them he had been ordered by the colonel to return to his dépôt. They walked in a line, dodging falling shells, with everyone chatting except for the adjutant, who remained quiet. As night fell, he said, "Good evening," and parted ways. After that, he couldn’t recall anything until he got to the Palameix Farm, where he had seen a comrade who was wounded in the head. He arrived home on November 29th at eight in the morning. He still had most of his money because he had traveled some distance by train without a ticket, and also without asking for one, and without having eaten. When the ticket collector in his hometown asked if he was back from the war, he looked at him blankly and left without answering; he also didn't respond to a reporter on the way home. This was odd since he was usually a friendly person.
He had a convulsive crisis at home, after which he was exhausted and apparently unable to move or reply. A physician said that he had had a cerebral shock. When the police arrived, two hours later, he was apparently delirious, saying[233] such things as, “The Christians want to shoot me but I know the rules! Come, boys, stay in the trenches!” “There are two more dead ones!” etc. During the day he recovered consciousness and was greatly disturbed at his military crime.
He had a seizure at home, after which he was exhausted and seemed unable to move or respond. A doctor said he had experienced a cerebral shock. When the police showed up two hours later, he appeared to be delirious, saying[233] things like, “The Christians want to shoot me but I know the rules! Come on, guys, stay in the trenches!” “There are two more dead ones!” and so on. During the day he regained consciousness and was really upset about his military actions.
In point of fact, he had had, at the age of 17, analogous crises, as was certified by Régis, who had cared for him from 1907 to 1909 for hysteria with sudden somnambulistic attacks and amnesia.
In fact, he had experienced similar crises at the age of 17, as confirmed by Régis, who treated him for hysteria with sudden sleepwalking episodes and memory loss from 1907 to 1909.
While in prison after his arrest, he also had hysterical crises with agitation, flushed face, hard attempts to vomit, respiratory disorder due to interference in the throat (globus hystericus), and delirious phenomena (“Germans had followed him home”).
While in prison after his arrest, he also experienced hysterical episodes characterized by agitation, a flushed face, intense nausea, breathing difficulties caused by a sensation in his throat (globus hystericus), and delusional thoughts (“Germans had followed him home”).
After his birth his mother had had two miscarriages and a stillborn child. The adjutant was declared irresponsible and acquitted. This is apparently an instance of hysteria without stigmata.
After his birth, his mother had two miscarriages and a stillborn baby. The adjutant was found not responsible and cleared of charges. This seems to be a case of hysteria without any visible signs.
Hysterical Adventist.
Hysterical Adventist.
Case 172. (De la Motte, August, 1915.)
An engineer, 31, in the Landwehr at the outset of the campaign, was first put on sentry service in Berlin on the ground that he was an Adventist. He was later put into the military service and had difficulty because he did not want to serve on Sunday. He was shoved from one company to another. He refused to be inoculated and was arrested therefor. In the prison, he began to hear God’s voice calling to him distinctly to tell his fellow-men that the end of this was going to be the end of all things. Back in the barracks, he again heard a voice—“Come forth!”—“Go!” He went! He had his revelations then published in the form of tracts, and held Bible readings day and night among his friends in Bremen—looking for the signs of the times in the Bible sayings. One of his fellow Adventists finally warned the police, and the military authorities put him under psychiatric observation. He proved to have numerous stigmata of hysteria. He talked freely about his visions, and was aware that he was punishable.
An engineer, 31, in the military at the start of the campaign, was first assigned to guard duty in Berlin because he was an Adventist. He was later enlisted in the military but faced challenges because he didn’t want to serve on Sundays. He was moved from one unit to another. He refused to get vaccinated and was arrested for it. In prison, he started to hear God’s voice clearly telling him to warn others that the end of all things was coming. Back in the barracks, he heard a voice—“Come forth!”—“Go!” So he went! He published his revelations as tracts and held Bible readings day and night with his friends in Bremen, searching for signs of the times in the Bible. One of his fellow Adventists eventually tipped off the police, and the military authorities placed him under psychiatric observation. He showed many symptoms of hysteria. He spoke openly about his visions, aware that he could be punished.
Here, then, was a case of hysterical psychosis, liberated by military service.
Here, then, was a case of hysterical psychosis triggered by military service.
Fugue, psychoneurotic.
Fugue, mental health issue.
Case 173. (Logre.)
The question, Is this escape really a fugue? is brought up not only in epileptic, alcoholic, and melancholic cases, but also in cases suggestive of psychoneurosis. A son of an insane person was subject to what may be called a phobic or obsessive fugue. The case may be called one of morbid cowardice and was observed in a soldier in the trenches. In point of fact, the man had always been an anxious and fearsome person, given to phobias. He had night terrors and fear of diseases and death. He was agoraphobic in adolescence, and had to have a policeman or passerby go with him through a public place. He had had also suicidal and homicidal obsessions, and periods of psychoneurotic anxiety.
The question, "Is this escape really a fugue?" comes up not just in cases of epilepsy, alcoholism, and depression, but also in situations suggesting psychoneurosis. A son of someone with mental illness experienced what could be described as a phobic or obsessive fugue. This case could be seen as an example of extreme cowardice and was noted in a soldier in the trenches. In reality, the man had always been anxious and fearful, prone to phobias. He suffered from night terrors and had fears of illnesses and death. He was agoraphobic during his teenage years and needed a policeman or a passerby to accompany him through a crowded area. He also dealt with suicidal and violent obsessions, along with episodes of anxiety related to psychoneurosis.
This man’s sojourn at the front put his morbid personality to a cruel test. He was soon known by all in the trenches as a froussard. He had a terrible fear of the guns, jumped, grew pale, trembled, complained of palpitations, lumps in the throat, etc. He was the laughing-stock of his comrades; but according to the patient himself, he was more afraid of his own emotion than of the shells, although his comrades couldn’t understand it. He was employed as a kitchenman, in a post not much exposed. A more resolute comrade helped him to escape, escaping also himself, thus bringing up the problem of fugue á deux. Limited responsibility was decided for the case, although the fugue had been aided by his morbid anxiety. Of course, his place was not in the trenches at all. He was condemned to two years in prison. After his sentence, he was given a chance to rehabilitate himself by sending him again to the trenches, but he had to be evacuated a few weeks later on account of his increasing emotionality.
This guy's time at the front really tested his anxious personality. Everyone in the trenches quickly dubbed him a froussard. He was terrified of the guns, would flinch, go pale, shake, and complain about heart palpitations and a tight throat, among other things. His comrades found him laughable; however, he claimed to be more scared of his own feelings than of the shells, which his friends just couldn’t grasp. He worked as a kitchen staff member, in a role that wasn’t too exposed. A more courageous comrade helped him escape, also managing to flee himself, raising the issue of fugue à deux. They decided on limited responsibility for him, even though his nervousness contributed to the fugue. Clearly, he didn’t belong in the trenches at all. He was sentenced to two years in prison. After his sentence, he got a chance to prove himself again by being sent back to the trenches, but he had to be evacuated a few weeks later due to his growing emotional instability.
Shell-shy; war bride pregnant: Fugue with amnesia and mutism.
Shell-shocked; a war bride expecting: a fugue with memory loss and silence.
Case 174. (Myers, January, 1916.)
A rifleman, 30 years old, was brought to a casualty clearing station, looking like an imbecile, with a history of having wandered about aimlessly, not knowing where he was or what he was doing. On questioning, he remained absolutely speechless and terrified. Four days later, in conversation with Major Myers, he was got to speak in a faint voice about his wife, home, and occupation, saying that the month was October (when it was actually August) and that he had been in France two months, when it was actually twelve. He described emotionally certain trench scenes, and then thought of his wife sewing.
A 30-year-old rifleman was brought to a casualty clearing station, looking confused, with a history of wandering aimlessly, not knowing where he was or what he was doing. When asked questions, he remained completely mute and terrified. Four days later, during a conversation with Major Myers, he managed to speak in a faint voice about his wife, home, and job, claiming it was October (when it was really August) and that he had been in France for two months, when it was actually twelve. He emotionally described certain scenes from the trenches and then thought about his wife sewing.
Hypnotized, he remembered going into a dug-out after running away from shells; he was made to talk in a loud voice. Next day, during hypnosis, proper orientation for time reappeared. He was got to write an ordinary soldier’s letter to his wife. The following day he was active, making beds, but was mute (there was a case of mutism in the same ward). Under hypnosis speech returned. He had gone to a horse show, and upon his return, something hit his back; shells had begun to fall. Found hiding in a shack, he was carried to a hospital in an ambulance. After this hypnotic treatment, the power of speech was maintained, although his voice became faint or failed whenever he was asked about the incidents described above. Next day he waked speaking normally, nudging his neighbor and asking, “Is it me that’s talking?” He had before appeared dull and depressed, but now appeared an intelligent, agreeable, and garrulous fellow. It appears that his wife was a war bride and he had heard some months since that she was pregnant. He had been troubled, thinking she was in money difficulties and kept thinking about a friend whose wife had lost her first baby. Recovery appears to be complete except for occasional headaches, and the patient is now serving in his reserve battalion.
Hypnotized, he remembered going into a dugout after running away from shells; he was made to speak loudly. The next day, during hypnosis, he regained his sense of time. He was asked to write a typical soldier's letter to his wife. The following day, he was active, making beds, but he was mute (there was another case of mutism in the same ward). Under hypnosis, his speech returned. He had gone to a horse show, and upon his return, something hit his back; shells had started to fall. Found hiding in a shack, he was taken to a hospital in an ambulance. After this hypnotic treatment, he maintained the ability to speak, although his voice became faint or faded whenever he was asked about the events he had described. The next day, he woke up talking normally, nudging his neighbor and asking, “Is it me that’s talking?” He had previously seemed dull and depressed, but now he appeared bright, friendly, and chatty. It turned out his wife was a war bride, and he had heard months ago that she was pregnant. He had been worried, thinking she was facing financial difficulties and kept remembering a friend whose wife had lost their first baby. Recovery seems to be complete except for occasional headaches, and the patient is now serving in his reserve battalion.
A neurasthenic volunteer.
An anxious volunteer.
Case 175. (E. Smith, June, 1916.)
A man who volunteered for service at the outbreak of the war (he had recently been an inmate of a sanatorium) was sent back to England as neurasthenic after three trying months at the front. The case sheet read that he was subject to dazed conditions. In hospital he suffered from insomnia, and before his slight periods of sleep he constantly had visions of two comrades who had been terribly lacerated at his side. These hallucinations in their reality aroused in him a fear that he was insane.
A man who volunteered for service when the war started (he had recently been staying in a sanatorium) was sent back to England as a neurasthenic after three tough months at the front. The case notes stated that he experienced episodes of confusion. In the hospital, he dealt with insomnia, and just before his brief moments of sleep, he repeatedly saw visions of two comrades who had been badly injured beside him. These vivid hallucinations made him fear that he was losing his mind.
There were also terrifying dreams, beginning with episodes at the front and ending with sex experiences. These dreams were ended by seminal emissions. These formed a second cause for the patient’s belief that he was insane, as he said he remembered literature read as a boy concerning spermatorrhoea.
There were also terrifying dreams, starting with experiences at the front and ending with sexual encounters. These dreams concluded with ejaculation. This became another reason for the patient’s belief that he was insane, as he recalled reading about spermatorrhoea in literature when he was a boy.
In the treatment of this case the writings of psychologists who had studied hypnagogic experiences were used and the absence of hallucinations during waking hours was stressed. The remembered literature regarding spermatorrhoea was discounted by the rational explanation of his state.
In addressing this case, the works of psychologists who studied hypnagogic experiences were utilized, highlighting the absence of hallucinations during waking hours. The existing literature on spermatorrhea was dismissed through a logical explanation of his condition.
He seemed to be getting on well when a trivial accident caused a relapse. While he was saying goodby to his wife, who had visited him, she was taken ill, and he went home with her. He was punished for being late in returning to the hospital. Although no moral stigma attaches to confinements in barracks in most soldiers’ minds, in this man a depression was produced and suicidal talk followed. It seems that his father had been sent to jail when he was a child, and he felt he had been tainted by his father in such wise that his “criming” was due to heredity. With the removal of this misconception he became more rational and immensely improved.
He seemed to be doing well until a minor accident caused a setback. While he was saying goodbye to his wife, who had come to see him, she fell ill, and he went home with her. He was penalized for returning late to the hospital. Although most soldiers don't see staying in barracks as a moral issue, it led to depression in this man, and he started talking about suicide. It turns out his father had been imprisoned when he was a child, and he believed he was affected by his father’s actions, thinking his "crimes" were inherited. Once he let go of this belief, he became more rational and made significant progress.
Five months’ war experience: Neurasthenia in subject without heredity or soil.
Five months of war experience: Neurasthenia in a person without hereditary influences or background.
Case 176. (Cheerful, January, 1916.)
A 38-year old soldier is Jolly’s example of a neurasthenia produced in a person without previous neurasthenic traits or hereditary factors. This soldier had been a moderately good student and never ill. He went into the battle line in December, 1914, and came out in May, 1915, on account of exhaustion. The case is not wholly convincing since the patient had a shrapnel injury of the skull, described as of so inconsiderable a degree that he was not put on the sick list on its account. The patient finally arrived at the Nuremberg Hospital, complaining of pressure in the head, as if there was a band around the head, and dizziness. He wept a good deal saying that the sight of the dead had frightened him. Sleep was restless and there were unpleasant dreams of the battle field. Intelligence was not in any degree disturbed. The supra-orbital points were sensitive to pressure. The tongue showed a marked tremor and was coated; the mechanical excitability of the muscles was increased; and there was reddening of the skin on stroking. There was a fine tremor of the extended fingers, less tremor of the head and of the body at large. Knee-jerks normal. Nutrition well preserved. Partial recovery in the hospital.
A 38-year-old soldier is Jolly’s example of neurasthenia arising in someone without prior neurasthenic traits or hereditary factors. This soldier had been a moderately good student and had never been ill. He went to the front lines in December 1914 and returned in May 1915 due to exhaustion. The case isn’t completely convincing since the patient had a shrapnel injury to the skull, described as minor enough that he wasn’t placed on the sick list for it. The patient eventually reached the Nuremberg Hospital, complaining of pressure in his head, as if there was a band around it, and dizziness. He cried a lot, saying that witnessing the dead had terrified him. His sleep was restless, filled with nightmares about the battlefield. His intelligence was not affected at all. The supra-orbital points were sensitive to pressure. His tongue showed a noticeable tremor and was coated; his muscle excitability was heightened; and there was redness of the skin upon stroking. There was a fine tremor in his extended fingers, with less tremor in his head and body overall. Knee-jerk reflexes were normal. His nutrition was well maintained. He showed partial improvement in the hospital.
Importance of arterial hypotension in the diagnosis of psychasthenia.
Importance of low blood pressure in diagnosing psychasthenia.
Case 177. (Crouzon syndrome, March, 1915.)
A man of 32 (never well, with general weakness, ideas of consumption and vacuous thinking following a good recovery from bronchitis at 28, unsuccessful in business, subject to weaknesses) had had eighteen months antebellum of what might be called psychasthenia. There were spells of loss of consciousness without convulsions, and probably of hysterical nature. There had been for two years insomnia and a general hypobulic slowing down of work.
A 32-year-old man (who has never felt well, suffering from general weakness, thoughts of illness, and empty thinking after a decent recovery from bronchitis at 28, unsuccessful in business, and dealing with various weaknesses) had experienced eighteen months before the war of what could be described as psychasthenia. He had episodes of losing consciousness without convulsions, likely of a hysterical nature. For two years, he had been dealing with insomnia and a general slowing down in his ability to work.
In military service the crises became more frequent, coming two or three times a week. Tuberculosis could not be shown, nor was there any organic lesion of the nervous system. The arterial tension (Potain sphygmomanometer) stood at 11.
In military service, the crises happened more often, occurring two or three times a week. Tuberculosis couldn't be detected, nor was there any physical damage to the nervous system. The blood pressure (measured with a Potain sphygmomanometer) was at 11.
According to Crouzon, arterial hypotension is an objective sign tending to assure the organic nature of a psychasthenia. Whereas simple neurasthenics are hypertensive, others have long been recognized as hypotensive; but heart experts have recognized this asthenic hypotension more than psychiatrists or neurologists. In differential diagnosis it is necessary to consider and exclude the early hypotensions of pulmonary tuberculosis and those of Addison’s disease. This hypotension is most frequently observed in constitutional neurasthenics and psychasthenics. Hypertensive drugs, adrenalin, tincture of colchicum, have produced a transitory improvement in a number of cases, but the amelioration has halted with the stoppage of the drugs.
According to Crouzon, low blood pressure is a clear sign that suggests the physical basis of a psychasthenia. While those with simple neurasthenia tend to have high blood pressure, many others have been known to have low blood pressure for a long time; however, heart specialists have identified this weak low blood pressure more than psychiatrists or neurologists. In differential diagnosis, it's important to consider and rule out the early low blood pressure associated with pulmonary tuberculosis and Addison’s disease. This condition is most often seen in those with constitutional neurasthenia and psychasthenia. Medications that raise blood pressure, like adrenaline and tincture of colchicum, have shown temporary improvement in several cases, but the benefits stopped when the medications were discontinued.
Service in France and Salonica: Psychasthenia.
Service in France and Salonica: Psychasthenia.
Case 178. (Eder, March, 1916.)
A man, 29, after some months’ service (three months in France and later in Salonica) was invalided for backache, insomnia, and enuresis. It seems that this married man had never done any work after leaving school at 18, having substantial private means. He had been married for 3½ years, had a son, and was, according to Eder, perhaps morbidly attached to his wife and child. He had been a sportsman and was selected for sniping work in France. The son of a shipbuilder, he had always planned all kinds of ships and engines, never to be used. After seeing the world, he was about to enter his father’s business when he had to take care of his father in a nervous breakdown. After a second attack, the man never entered business.
A 29-year-old man, after a few months of service (three months in France and later in Salonica), was discharged due to back pain, insomnia, and bedwetting. It turns out that this married man had never worked since leaving school at 18, as he had significant personal finances. He had been married for 3½ years and had a son, and according to Eder, he was perhaps excessively attached to his wife and child. He had been a sports enthusiast and was chosen for sniping duties in France. As the son of a shipbuilder, he had always designed various ships and engines, none of which were ever built. After traveling the world, he was about to join his father's business when he needed to care for his father during a nervous breakdown. After a second episode, he never returned to work.
February 6, 1916, wide-spread patchy analgesia and lumbar hyperesthesia were found. He thought sluggishly, being restless and holding attention poorly. He began twenty letters, destroying each after finishing a few lines. He was shy and felt that everybody was looking at him. He became speechless if he had to address his commanding officer. He had an obsession to mark each flagstone and touch each post, and various counting and arranging obsessions.
February 6, 1916, widespread patchy numbness and increased sensitivity in the lower back were observed. He felt sluggish, restless, and struggled to focus. He started writing twenty letters, tearing each one apart after just a few lines. He felt shy, as if everyone was watching him. He froze up whenever he had to speak to his commanding officer. He had an urge to touch each flagstone and each post, along with various counting and organizing compulsions.
The Horme (Jung) was elusive. A dream: “I was in a cargo boat in the river; we were steering straight into ferry and harbor. The pilot rang down ‘Full speed to stern’; I pushed him out of the way, and rang down ‘Full speed ahead, two points to starboard.’ We went straight past ferry and harbor without accident.” Again, a few days later, “In a motor car, came to some rocks which sprang up in front of me. The machine broke down. I abandoned it and clambered over the rocks. It was tough work. My object was a ship. I got to the ship, took hold of the wrench, and signalled ‘Let go.’” Herein, according to Eder, are certain obvious symbolic conversions.
The Horme (Jung) was hard to pin down. A dream: “I was on a cargo boat in the river; we were heading straight for the ferry and the harbor. The pilot shouted ‘Full speed in reverse’; I pushed him aside and shouted ‘Full speed ahead, two points to the right.’ We zoomed right past the ferry and the harbor without any issues.” Again, a few days later, “In a car, I encountered some rocks that popped up in front of me. The car broke down. I left it behind and climbed over the rocks. It was tough work. My goal was a ship. I reached the ship, grabbed the wrench, and signaled ‘Release.’” According to Eder, there are some clear symbolic transformations here.
Antebellum attacks, with dizziness: Fainting on horseback. Neurasthenia.
Antebellum attacks, feeling dizzy: Passing out on horseback. Neurasthenia.
Case 179. (Binswanger, July, 1915.)
A harness-maker, 37, a corporal, was called to the colors on the second day of mobilization. He was attacked by a slight dizziness in the evening (see previous history below). He went into the field on August 7 and had repeated attacks of dizziness, despite which he took part in several skirmishes. He could not ride on horseback, since dizziness, ringing in the ears, headaches, and trembling of the whole body would develop. October 27 a severe fainting attack came while he was sitting on a horse. He woke ten hours later, vomited several times and felt dazed. Two weeks later hearing in the right ear began to be impaired. During several transfers from hospital to hospital near the East front, there were two more severe attacks of dizziness and vomiting. Brought back to Germany, the patient finally came to the Jena Hospital, May 20.
A harness-maker, 37, and a corporal, was called to serve on the second day of mobilization. That evening, he experienced mild dizziness (see previous history below). He went into the field on August 7 and had multiple episodes of dizziness, yet he participated in several skirmishes. He couldn’t ride horseback because he would develop dizziness, ringing in his ears, headaches, and shaking throughout his body. On October 27, he had a severe fainting spell while sitting on a horse. He woke up ten hours later, vomited several times, and felt disoriented. Two weeks later, his hearing in the right ear started to decline. During several transfers from hospital to hospital near the Eastern front, he experienced two more severe episodes of dizziness and vomiting. Brought back to Germany, the patient ultimately arrived at the Jena Hospital on May 20.
The estimate of this case depends somewhat on the previous history. He appears to have come from a healthy family, was married, and had two healthy children. His bodily and mental development had been normal; he had been an unusually good scholar, but he stammered from his tenth year without apparent reason. He had had treatment in an institution for stammerers at 17, achieving a complete cure in six weeks. His military service was as a cavalryman, 1897-1900, after which he had married. There was no excess in alcohol; he was not a smoker. From his own account, he had always been somewhat nervous, had trembled easily, and had fallen to stammering when excited. In 1913 there had occurred, after physical exertion, three violent attacks of fainting, with dizziness, vomiting, and excessive perspiration, each attack lasting from two to three hours. However, from that time to just before the war, he had been free from attacks.
The assessment of this case relies somewhat on the individual’s background. He seems to have come from a healthy family background, was married, and had two healthy kids. His physical and mental development had been normal; he was an exceptionally good student, but he started stuttering at age ten without any clear reason. He received treatment at a stuttering clinic at 17, where he was completely cured in six weeks. He served in the military as a cavalryman from 1897 to 1900, after which he got married. He didn’t drink excessively and didn’t smoke. According to him, he had always been a bit nervous, easily trembling, and he started stuttering when he got excited. In 1913, after physical exertion, he experienced three severe fainting spells, accompanied by dizziness, vomiting, and excessive sweating, each lasting two to three hours. However, from that time until just before the war, he had no more episodes.
On examination at the Jena Hospital, the patient complained of general weariness, a feeling of pressure in the back[242] of his head, a hammering all over the head, ringing in the right ear, impairment of hearing in this ear, a feeling of dizziness on raising the head, palpitation of heart, especially at night, occasional trembling of the whole body, and absolute inability to walk.
At the Jena Hospital, the patient reported feeling overall tired, pressure in the back of his head, a pounding sensation throughout his head, ringing in his right ear, reduced hearing in that ear, dizziness when lifting his head, a racing heart, especially at night, occasional shaking of his entire body, and complete inability to walk.
The man was slenderly built, of medium height, in moderate nutrition; pale of face and mucosae; pulse small, regular, and 114. Neurologically, the deep reflexes were generally increased, and the skin reflexes decreased. Percussion on the back of the head elicited marked pain. There were no pressure points. The movements of the arms were free; there was a marked tremor of both hands, more marked on the right. The left grasp was 45, the right, 20, by the dynamometer.
The man was slim, of average height, and had a moderate nutritional status; his face and mucous membranes were pale; pulse was small, regular, and 114. Neurologically, his deep reflexes were generally heightened, while his skin reflexes were diminished. Tapping on the back of his head caused significant pain. There were no pressure points. His arm movements were unrestricted; however, he had a noticeable tremor in both hands, more pronounced in the right hand. The grip strength was 45 in his left hand and 20 in his right, measured by the dynamometer.
When lying upon his back, the patient could move his legs, but he moved them only slowly and with tremor. The heel-to-knee test was successfully executed despite the tremor; nor could it be demonstrated that there was a genuine ataxia. Placed upon his feet, he would collapse, nor could he be made to walk at all. With trunk supported, he was able to make only a few unsuccessful attempts to drag the feet forward.
When lying on his back, the patient could move his legs, but he only moved them slowly and with a tremor. He was able to complete the heel-to-knee test successfully despite the tremor; it could not be shown that he had true ataxia. When put on his feet, he would collapse, and he could not walk at all. With his trunk supported, he could only make a few unsuccessful attempts to drag his feet forward.
Associated with this apparent paralysis, the sensitiveness to touch had entirely ceased in the legs, as well as sensitiveness to pain. The zone of analgesia, however, was more extensive than the anesthesia, spreading upwards three or four cm. farther in front. Ticking of the watch could not be heard even at the meatus of the right ear, although hearing of the left ear was entirely normal; bone transmission on the left side. Whispers could be heard close to the meatus. On speaking, the patient stammered in starting sentences.
Linked to this apparent paralysis, sensitivity to touch had completely disappeared in the legs, along with sensitivity to pain. However, the area of numbness was larger than the area of loss of feeling, extending three or four centimeters further upwards in front. The ticking of the watch couldn’t be heard even at the opening of the right ear, while hearing in the left ear was completely normal; bone conduction was intact on the left side. Whispers could be heard near the ear opening. When speaking, the patient stammered at the beginning of sentences.
He looked extremely anxious during the first few days in the Jena wards, claiming that he could not raise himself. When his trunk was raised, he would let himself sink feebly back into dorsal decubitus. However, when believing himself unobserved, he was found to be able to move himself in bed somewhat quickly. He was able to get a box from beneath the bed, to open the drawer of the night-stand, and to take remarkable care of his moustachios. He complained[243] more and more of headache, though his appetite and sleep were good. He was often irritable.
He looked really anxious during the first few days in the Jena wards, saying that he couldn't lift himself up. When his trunk was raised, he would weakly sink back down onto his back. However, when he thought no one was watching, he was seen moving himself in bed fairly quickly. He was able to get a box from under the bed, open the drawer of the nightstand, and take great care of his mustache. He complained[243] more and more about headaches, even though his appetite and sleep were good. He was often irritable.
Treatment at first consisted of cold packs of the legs twice a day, salt-water baths, active and passive exercises of the legs in the position of dorsal decubitus. The patient declaimed against this treatment. There was slight improvement after a week of treatment. He was then able to raise himself in bed, seat himself on the edge of the bed, and stand without support, all the time, however, groaning and moaning. After a few moments, he would fall back on the bed, complaining of violent headache and dizziness. While standing, both legs trembled.
Treatment initially involved cool compresses on the legs twice a day, saltwater baths, and both active and passive exercises of the legs while lying on his back. The patient protested against this treatment. After a week, there was some slight improvement. He could then lift himself in bed, sit on the edge, and stand without support, although he was constantly groaning and moaning. After a few moments, he would collapse back onto the bed, complaining of severe headaches and dizziness. While standing, both legs shook.
Antityphoid inoculation: Neurasthenia.
Typhoid vaccination: Neurasthenia.
Case 180. (Advice, 1917.)
A corporal, 39, began to be sleepless and weary, with headache, pains in the back, and dizziness. He was homesick. Upon hospital examination he was very variable in mood, rather hostile in attitude, and at the same time suggestible. He was so confident of being sent home that he anticipated the diagnosis by sending his belongings back to Sicily at the time he was transferred to hospital from his regiment.
A 39-year-old corporal started experiencing sleeplessness and fatigue, along with headaches, back pain, and dizziness. He felt homesick. During a hospital examination, his mood was quite unpredictable, he seemed somewhat hostile, yet he was also easily influenced. He was so sure he would be sent home that he proactively sent his belongings back to Sicily when he was transferred to the hospital from his unit.
After a month’s rest and psychotherapy, the man’s general condition was greatly improved; he was no longer sleepless and had no longer any sign of neurotic disorder. He still maintained that his memory was weak, although in point of fact his memory was very good and quick. He could narrate all the facts about his neurasthenic state. The man’s complaints were out of all proportion to any demonstrable somatic disorder. He was discharged, cured, to be put to work at shoemaking, with the diagnosis, neurasthenia. This neurasthenic state developed after antityphoid injection.
After a month's rest and therapy, the man's overall condition had improved significantly; he was no longer sleepless and showed no signs of neurotic disorder. He still insisted that his memory was weak, even though his memory was actually very good and quick. He could recount all the details about his neurasthenic state. The man's complaints were far greater than any visible physical issue. He was discharged, cured, and assigned to work in shoemaking, with a diagnosis of neurasthenia. This neurasthenic state developed after receiving an antityphoid injection.
Re the occasional curious effects of antityphoid injection, see Case 65.
Re the occasional interesting effects of antityphoid injection, see Case 65.
Neurasthenia (monosymptomatic: Sympathy with the enemy).
Neurasthenia (monosymptomatic: Sympathy with the enemy).
Case 181. (Steiner, October, 1915.)
A non-commissioned reserve officer, 26, in civil life a merchant, had a strong hereditary taint, having been also in peace times very nervous and on that account obliged to give up his studies. At the age of 14, he had seen a man fall down from a roof and was much excited about it.
A 26-year-old non-commissioned reserve officer, who worked as a merchant in civilian life, had a significant family history of mental health issues. He had also been very anxious during peacetime, which forced him to abandon his studies. When he was 14, he witnessed a man fall from a roof, which greatly affected him.
At the beginning of mobilization he suffered a functional aphonia for a few days. He could not let his men shoot at the enemy because of an idea that occurred forcibly to him: that the enemy’s soldiers had wives and children! He felt badly on this account. Later he had a constant taste of blood in his mouth and a smell of corpses in his nose. Toward nightfall all these symptoms would change for the worse, and the symptoms would become especially bad whenever he had anything to do with the wounded. He tended to weep much and was easily frightened and had also various physical symptoms of neurasthenia.
At the start of mobilization, he experienced a temporary loss of voice for a few days. He couldn’t allow his men to shoot at the enemy because an idea struck him hard: the enemy soldiers had wives and kids! He felt really bad about that. Later on, he constantly had a metallic taste of blood in his mouth and the smell of decay in his nose. As night approached, all these symptoms would worsen, especially whenever he dealt with the wounded. He often found himself tearful, was easily scared, and also had various physical signs of exhaustion.
Shell-shock CLAUSTROPHOBIA: Preferred shell exposure to shell-proof tunnel.
Shell-shock CLAUSTROPHOBIA: Preferred shell exposure to a shell-proof tunnel.
Case 182. (Steiner, October, 1915.)
A colleague of Steiner, an army physician, 35 years of age, with strong hereditary taint, having two sick sisters (one dementia praecox), had been incapacitated for work through a neurasthenia a few months before mobilization. However, at first he felt very well, marching through Belgium and into Northern France.
A colleague of Steiner, an army doctor, 35 years old, with a strong family history of illness, had two sick sisters (one with schizophrenia) and had been unable to work due to neurasthenia a few months before mobilization. However, at first he felt great, marching through Belgium and into Northern France.
On the night of the 17th of October, 1914, a shell struck the house next where he was and startled him up out of sleep. After that, especially at nightfall, upon entering a cellar he would have the feeling of the ceiling falling down, and he would go restlessly from one space to another. Afterwards, any closed room, however secure or distant from the front and free from shells, would give him the feeling of the ceiling about to fall down. He could no longer sit quietly anywhere, but walked about and avoided the company of others.
On the night of October 17, 1914, a shell hit the house next door and jolted him awake. After that, especially at dusk, when he entered a cellar, he felt like the ceiling was going to collapse, and he would anxiously move from one place to another. Later, any closed room, no matter how safe or far from the front line and free of shells, made him feel like the ceiling was about to fall in. He couldn't sit still anywhere anymore, so he walked around and stayed away from other people.
A characteristic observation is the following as described by the physician himself: There was an absolutely shell-proof tunnel running to the position at the front where he was on duty. It took about 25 minutes to go through the tunnel, but on account of his feelings he could not bring himself to use this tunnel but walked over the exposed hill which was frequently shelled. Curiously enough, after the appearance of the first symptoms, a shell exploded nearby without any marked psychical effect. This happened about noon. The obsessions were stronger in the evening. Objectively, there were neurasthenic symptoms of a bodily nature; there was vasomotor excitability. He was depressed, wept easily, and showed lack of decision; he had tormenting thoughts that he had not fulfilled his duty.
A notable observation is as follows, described by the physician himself: There was a completely safe tunnel leading to the front position where he was on duty. It took about 25 minutes to get through the tunnel, but because of his feelings, he couldn’t bring himself to use it and instead walked over the exposed hill that was often shelled. Interestingly, after the first symptoms appeared, a shell exploded nearby without any noticeable psychological effect. This occurred around noon. The obsessions became stronger in the evening. Objectively, there were physical signs of neurasthenia; he experienced vasomotor excitability. He felt depressed, cried easily, and showed indecision; he was plagued by thoughts that he hadn’t fulfilled his duty.
XI. PSYCHOPATHOSES
(GROUP OF VARIOUS PSYCHOPATHIAS)
A case of Pathological Lying occurring in a soldier.
A case of pathological lying happening in a soldier.
Case 183. (Henderson, July, 1917.)
No. 27369, a private, attached to the 15th Battalion Durham Light Infantry, was admitted Oct. 14, 1916, to Lord Derby War Hospital from Netley.
No. 27369, a private in the 15th Battalion Durham Light Infantry, was admitted on October 14, 1916, to Lord Derby War Hospital from Netley.
September 11, 1916, he had been admitted to Number 3 General Hospital, France, in a noisy, excited, insolent state: said he saw spirits of the dead; heard his sister urging him to lead a better life. Admitted to Netley early in October, 1916: now said he was a spiritualist, a Frenchman, had a quarrel with parents and enlisted in British Army, in army service; went to France August 12, 1914, was wounded at Loos, September, 1915, returned to front in February, 1916, “shell-shocked” June 1, 1916; lost consciousness after this—did not know where he was until July 22, 1916, when he had been arrested as deserter.
On September 11, 1916, he was admitted to Number 3 General Hospital in France, in a loud, agitated, and disrespectful condition. He claimed to see the spirits of the dead and heard his sister urging him to live a better life. He was admitted to Netley in early October 1916, and now stated that he was a spiritualist, a Frenchman who had a conflict with his parents and joined the British Army. He went to France on August 12, 1914, was wounded at Loos in September 1915, returned to the front in February 1916, and was "shell-shocked" on June 1, 1916. He lost consciousness after that and didn’t know where he was until July 22, 1916, when he was arrested as a deserter.
Admitted to Lord Derby Hospital October 14, 1916,—quiet, orderly, coöperative: desired to return to his regiment. He now gave a history: Enlisted British Army 1908, went to France, August, 1914, wounded February, 1915, at Neuve Chapelle; recovered; then attached to 45th Durham Light Infantry; blown up July 22, 1916, came to August 5, 1916, in hospital in Boulogne; then back to his regiment—but month later left without leave to pay off old score on a former comrade who had insulted his sister—arrested later by military police; put under observation in 65th Field Ambulance. No deterioration noted, school knowledge fairly well retained; no hallucinations or delusions (maintained he was a spiritualist, also that following shell-shock had suffered from insomnia and seemed to hear sister’s voice). Physically—small, well nourished, effeminate looking.
Admitted to Lord Derby Hospital on October 14, 1916—calm, organized, cooperative: wanted to return to his regiment. Here’s his history: Enlisted in the British Army in 1908, went to France in August 1914, wounded in February 1915 at Neuve Chapelle; recovered; then assigned to the 45th Durham Light Infantry; injured in an explosion on July 22, 1916, and arrived on August 5, 1916, at a hospital in Boulogne; then returned to his regiment—but a month later, he left without permission to settle a score with a former comrade who had insulted his sister—was later arrested by military police and placed under observation in the 65th Field Ambulance. No deterioration observed, academic knowledge retained fairly well; no hallucinations or delusions (claimed to be a spiritualist, also said that after shell-shock, he had insomnia and seemed to hear his sister’s voice). Physically—small, well-nourished, and with an effeminate appearance.
Oct. 23, 1916, he broke parole, but a month later returned to hospital under arrest. The police reported he had been[248] masquerading as wounded French soldier attached to British army as interpreter; imposed on people; had two leaden types in his possession: “Interpreter R. le Auldere, attached to 1st Division.”
Oct. 23, 1916, he broke his parole, but a month later he returned to the hospital under arrest. The police reported that he had been[248]pretending to be a wounded French soldier attached to the British army as an interpreter; he had deceived people and was found with two leaden types in his possession: “Interpreter R. le Auldere, attached to 1st Division.”
Story in hospital on return:—Born in France, did well in school, entered military academy at Paris. Quarreled with father—ran away to sea. Adopted by a French lady at Pembroke Dock. On account of drunken habits, quarreled again; joined army at Bristol, 1908. Went to France in August, 1914; January, 1915, invalided home because of “trench feet”—discharged as unfit. Reënlisted June, 1915, in Durham Light Infantry. January, 1916, again ordered to France. Blown up on Somme, July, 1916, by shell—remembered nothing until brought to No. 3 General Hospital. He remembers being accused of desertion but sentence was not passed, as he was held by the medical officer to have been irresponsible (as a matter of fact he was, at that time, considered to be a case of dementia praecox.)
Story in hospital on return:—Born in France, did well in school, and entered a military academy in Paris. Had a fight with my father—ran away to sea. Adopted by a French lady in Pembroke Dock. Because of my drinking habits, I quarreled again; joined the army in Bristol in 1908. Went to France in August 1914; in January 1915, I was sent home due to "trench foot"—discharged as unfit. Reenlisted in June 1915 in the Durham Light Infantry. In January 1916, I was ordered back to France. Blown up on the Somme in July 1916 by a shell—I remember nothing until I was brought to No. 3 General Hospital. I recall being accused of desertion, but no sentence was given, as the medical officer determined I was not responsible (in fact, at that time, I was considered to have dementia praecox).
Said that during twenty-five days, due to drunkenness, his friends had taken him to Manchester with them; arrested by police as he attempted to get back to hospital. He was now accused of wilfully lying and, confronted with his police record, at first denied it, but later gave following approximately true story:
Said that for twenty-five days, because of his drinking, his friends had taken him to Manchester with them; he got arrested by the police while trying to return to the hospital. Now he was accused of intentionally lying and, when faced with his police record, initially denied it but later told the following mostly true story:
Born, England, 1890; early life of a roving disposition, good at school, liked books of adventure. Drank early. Ran away at sixteen; was returned home. Ran away again—convicted of drunkenness. Three-year sentence to reformatory in 1910 for stealing: escaped. Rearrested for stealing in 1911: released in 1913, enlisted in army and deserted. Arrested in January, 1914, for stealing; sentenced to three years: released to rejoin army in June, 1915. Arrested as deserter: imprisoned but released in January, 1916; left for France. August, 1916, “shell-shocked,” sent to Field Ambulance No. 3, General Hospital, Netley, and Lord Derby War Hospital. Court-martialed for desertion: nothing came of it on account of medical evidence.
Born in England in 1890; had a free-spirited early life, did well in school, and enjoyed adventure books. Started drinking early. Ran away at sixteen but was brought back home. Ran away again and was convicted of drunkenness. Sentenced to three years in a reformatory in 1910 for stealing; escaped. Rearrested for stealing in 1911; released in 1913, then enlisted in the army and deserted. Arrested in January 1914 for stealing; sentenced to three years but released to rejoin the army in June 1915. Arrested as a deserter, imprisoned, but released in January 1916; went to France. In August 1916, "shell-shocked," sent to Field Ambulance No. 3, General Hospital, Netley, and Lord Derby War Hospital. Court-martialed for desertion; nothing came of it due to medical evidence.
After breaking his hospital parole, he masqueraded in district as “R. le Auldere,” “Le Marchal” and imposed on various persons.
After violating his hospital parole, he pretended to be “R. le Auldere” and “Le Marchal” in the area and deceived various people.
Psychopath almost Bolshevik.
Psychopath nearly Bolshevik.
Case 184. (Hovel, 1917.)
A sergeant, accountant in civil life (father insane, mother pulmonary, grandfather alcoholic, cousin insane; patient himself anemic as a boy, victim of chronic gastritis and gonorrhea), was evacuated from the front to Chateaugiron in March, 1916. It appeared that instead of watching over his men as a sergeant should, he gave utterance to baroque theories of the divine right, the influence of the grace of God on man, and the end of the war. He went so far as to ask leave to transmit to the Inventions Bureau of the War Ministry an invention with respect to the problem of locomotion, and he sent to the King of Belgium a manuscript to the effect that he had received from heaven a mission to reëstablish the world’s balance. He was, in fact, the victim of delusions of a mystical nature with visual hallucinations. To explain his mission, he wrote, “It was my duty to take supreme command of war operations.… I have the power, the right and the duty to give the following order … general armistice … peace will be symbolized by the house undivided and will be constituted by general Christian religious unity … as a consequence of what we shall say they will give up our territory to us of their own accord.”
A sergeant, who was an accountant in civilian life (his father was insane, his mother had lung issues, his grandfather was an alcoholic, and his cousin was also insane; he himself had been anemic as a boy and suffered from chronic gastritis and gonorrhea), was evacuated from the front to Chateaugiron in March 1916. Instead of looking after his men as a sergeant should, he shared intricate theories about divine rights, the influence of God's grace on people, and the purpose of the war. He even went so far as to request permission to share an invention with the War Ministry regarding locomotion issues, and he sent a manuscript to the King of Belgium claiming that he had received a divine mission to restore the world's balance. He was, in fact, suffering from mystical delusions along with visual hallucinations. To explain his mission, he wrote, “It was my duty to take supreme command of war operations.… I have the power, the right, and the duty to give the following order … general armistice … peace will be symbolized by a united house and will be established through general Christian religious unity … as a result of what we will say, they will voluntarily give up our territory.”
This case of paranoia apparently took its coloring in part from the war situation itself.
This paranoia seems to have been influenced in part by the war situation itself.
Hysterical mutism: Persistent delusional psychosis.
Hysterical mutism: Ongoing delusional psychosis.
Case 185. (Dumesnil, 1915.)
A sergeant, aged 23, evacuated from the front to a hospital for the insane, had been mute, though not deaf, since February 28, 1915. If asked to cry out he grew black in the face and could utter only a raucous scream which made everyone jump. He wrote very frequently, stating in February that as he was still a sergeant and had no hope of advancement, he cared nothing more for life. “The idea of death got anchored in my head.” In this state of mind, on the afternoon of the 27th two bombs came. “I saw the first one coming and cried out a warning. Coming back I saw the second one. The bombs were coming rather softly. From this moment on and up to the time when they burst, I thought I had gone, that I had been carried off and crushed. I was quite astounded at finding myself covered with earth and stones … but I could not talk any more, I could just say in a low voice ‘Papa,’ and the next day in an ambulance I could not talk at all.”
A 23-year-old sergeant, evacuated from the front to a mental hospital, had been mute, though not deaf, since February 28, 1915. When asked to shout, he turned pale and could only let out a harsh scream that startled everyone. He wrote often, mentioning in February that since he was still a sergeant and had no hope for promotion, he no longer cared about life. “The idea of death settled in my mind.” In this mental state, on the afternoon of the 27th, two bombs fell. “I saw the first one coming and yelled a warning. When I looked back, I saw the second one. The bombs were coming down quietly. From that moment until they exploded, I thought I was gone, that I had been taken away and crushed. I was shocked to find myself buried under earth and stones … but I couldn’t speak anymore; I could only say softly ‘Papa,’ and the next day in an ambulance, I couldn’t talk at all.”
There was complete pharyngeal anesthesia. The man had been a foundling and was clearly a degenerate. He had always been of a depressed disposition and given to thoughts about his misfortunes. Over and above the mutism gradually ideas of persecution and revindication developed (such as that he merited adjutant’s rank and was being mocked and treated as a simulator). He drew up a long letter to the War Ministry in which he stated his desire to be sent back to the front. He complained to the police about a hospital sergeant and offered a duel in an elaborate and inflammatory style, “with whatever weapons shall please you, either sabre of 1845, revolver of 1902 or bayonet of 1886 or the chassepot. One of us two must disappear.” He had become dangerous enough to be interned and in hospital remained mute with the same ideas of persecution and revindication, the same alternate phases of calmness and excitation. According to Dumesnil: hysterical mutism with persecutory delusional psychosis.
There was total numbness in his throat. The man had been abandoned as a baby and was clearly troubled. He had always been in a low mood and often thought about his bad luck. Along with his silence, feelings of being persecuted and a desire for revenge grew (like thinking he deserved a promotion and was being mocked and treated like a fraud). He wrote a lengthy letter to the War Ministry expressing his wish to return to the front lines. He complained to the police about a hospital sergeant and challenged him to a duel in a detailed and dramatic way, “with any weapons you prefer, whether it’s the 1845 sabre, the 1902 revolver, the 1886 bayonet, or the chassepot. One of us must go.” He had become dangerous enough to be committed, and in the hospital, he remained silent, still fixated on feelings of persecution and revenge, alternating between calmness and agitation. According to Dumesnil: hysterical mutism with delusions of persecution.
A peasant’s psychopathic inferiority brought out by the war.
A peasant’s twisted mental issues revealed by the war.
Case 186. (Bennati, October, 1916.)
An Italian peasant began to feel sick on being called to arms. Antebellum he had been an even-tempered, good-natured man, according to his own story, satisfied even with stale food, and always enjoying his sleep. He had been in the war about a month, doing construction work, sentry duty, and chores. Though he lived in the trenches under damp conditions, there had really not been much excessive war strain. He shortly developed migraine and war-weariness, as well as middle-ear disease.
An Italian farmer started to feel unwell when he was called to fight. Before the war, he described himself as a calm and friendly guy who was content even with old food and always enjoyed his sleep. He had been in the war for about a month, doing construction, guard duty, and other tasks. Even though he lived in the trenches under damp conditions, the stress of war hadn’t really been that overwhelming. Soon, he developed migraines and general fatigue from the war, along with an ear infection.
A number of times he heard shooting nearby, and was subject in his sentry duty to a good deal of anxiety and painful associations. On sentry duty he had digestive disorder, vomited, and became intolerably weary; in point of fact, a fever, regarded as malarial, then developed, together with diarrhea.
Several times he heard gunfire nearby and felt a lot of anxiety and painful memories during his guard duty. While on guard, he had stomach issues, vomited, and became extremely exhausted; in fact, he later developed a fever that was thought to be malaria, along with diarrhea.
Upon hospital observation, he was found fatigued, given to terrible dreams, tremulous in the fingers, with skin reflexes a little excessive, and the Moebius phenomenon. The thyroid was somewhat swollen. The pulse stood at 80. The Mannkopf sign was well marked, as well as that of Thomayer (80-120), and Erben (120-87). The oculocardiac reflex was prominent.
Upon being observed in the hospital, he appeared tired, plagued by disturbing dreams, shaky in his fingers, with slightly heightened skin reflexes, and exhibiting the Moebius phenomenon. His thyroid was somewhat enlarged. His pulse was at 80. The Mannkopf sign was clearly evident, along with Thomayer’s (80-120) and Erben’s (120-87) signs. The oculocardiac reflex was pronounced.
Psychopathic episodes.
Psychopathic episodes.
Case 187. (Pellacani, April, 1917.)
A Neapolitan, 26 (neuropathic stock: mother epileptic, brother psychopathic; patient had previous criminal record; married and then appeared to behave himself for several years; had always been excitable and of violent temper), after but one severe day in the trenches, woke and found his night clothes soaked in urine. Another time, his comrade had awakened him because he was gnashing his teeth in his sleep. Again, his grief became very violent at learning of his wife’s infidelity, and during the night he bit his finger. He thereafter suffered from severe headaches, dizziness and vertigo though without falling. He was granted a furlough, but the condition was aggravated on account of his wife’s abandonment of him, and one day, finding her with her lover, he threw himself at them, wounding her severely in the face: he did not remember this impulse later. Many hours later, on awakening in prison with his wounded hand, he recalled the entire episode. He showed a confused and excited condition, which, however, quickly diminished. He became lucid and tranquil, though easily aroused. He cried at the thought of his daughter, whom he wanted to save. Insomnia, instability of reaction, habitual migraine, and dizziness. Tremors of the fingers and of the eyelids. Exaggerated reflexes. Very striking cutaneous analgesia.
A Neapolitan man, 26 (family history of nerve disorders: mother had epilepsy, brother had psychopathic tendencies; the patient had a prior criminal record; he was married and then appeared to be well-behaved for several years; he had always been excitable and had a violent temper), after just one tough day in the trenches, woke up to find his nightclothes soaked in urine. Another time, his comrade woke him up because he was grinding his teeth in his sleep. Again, he became extremely distressed upon learning of his wife's infidelity, and during the night, he bit his finger. After that, he experienced severe headaches, dizziness, and vertigo, but didn’t lose consciousness. He was given a leave of absence, but his condition worsened due to his wife leaving him, and one day, when he found her with her lover, he attacked them, injuring her severely in the face: he didn’t remember this impulsive act later. Many hours later, upon waking in prison with his injured hand, he remembered the entire incident. He exhibited confusion and agitation, which quickly subsided. He became clear-headed and calm, though still easily stirred up. He cried at the thought of his daughter, whom he wanted to protect. He suffered from insomnia, unstable reactions, chronic migraines, and dizziness. He had tremors in his fingers and eyelids. His reflexes were exaggerated. There was very noticeable skin insensitivity.
Maniacal and hysterical delinquent.
Manic and hysterical delinquent.
Case 188. (Buscaino & Coppola, January, 1916.)
An Italian soldier, 25, a foundling, was always off and on in a military prison. At a tavern one night the man unsheathed his sword and threw three bottles at the host. Bystanders overpowered him and carried him to the local police station. Handcuffs were put on to stop the mania. His pupils were dilated and he was sweating profusely. Alcohol could absolutely be excluded from the history of this incident.
An Italian soldier, 25, who was a foundling, was frequently in and out of military prison. One night at a tavern, he pulled out his sword and threw three bottles at the host. People nearby subdued him and took him to the local police station. Handcuffs were put on him to restrain his outburst. His pupils were dilated, and he was sweating heavily. Alcohol could definitely be ruled out as a factor in this incident.
Observed in clinic, the patient was rather silent, but on the whole normal and without delusions or hallucinations. It seems that he had committed a number of crimes in the army that were always excused on account of his mental state. He had been strongly alcoholic, although not at the time of the incident mentioned. He was covered with tattooings of an obscene and violent nature.
Observed in the clinic, the patient was mostly quiet, but generally normal and free of delusions or hallucinations. It appears he had committed several crimes while in the army, but they were always overlooked due to his mental state. He had a significant history of alcoholism, though he wasn't under the influence during the incident mentioned. His body was covered in tattoos that were obscene and violent in nature.
He showed pharyngeal and conjunctival anesthesia and concentric limitation of the visual fields of unusual degree, and a remarkable hypalgesia. The knee-jerks were lively. The man was, in point of fact, sent back to military service, with, however, the suggestion of reform school.
He displayed numbness in his throat and eyes, a significant restriction in his visual fields, and an unusual insensitivity to pain. His knee-jerk reflexes were active. In fact, the man was returned to military service, although there was a recommendation for reform school.
Psychopathic delinquent.
Psychopathic criminal.
Case 189. (Buscaino and Coppola, January, 1916.)
An Italian, 20 (family history negative), was described by officers as of an odd disposition, at times thoughtful and again chattering and presumptuous, and often very vulgar in talk and manner. He had tried several trades, with little success.
An Italian, 20 (no family history), was described by officers as having a strange personality, sometimes thoughtful and other times talkative and arrogant, often very crude in speech and behavior. He had attempted several jobs, but with little success.
While in the army he discharged his gun three times, claiming to have heard noises in a nearby field. On account of the inopportune repeated discharges, he was condemned to the barracks for ten days. The following day, instead of returning to the barracks, he abandoned his musket, cartridge box and uniform, and, returning to town, left for Leghorn. Being sent to prison, he began to scream that he was thirsty. He tore his jacket into strips with his teeth, and making a noose of it, attempted to hang himself.
While in the army, he fired his gun three times, claiming he heard noises in a nearby field. Because of the annoying repeated firings, he was sentenced to spend ten days in the barracks. The next day, instead of going back to the barracks, he left behind his musket, cartridge box, and uniform, and returned to town to head to Leghorn. After being sent to prison, he started screaming that he was thirsty. He ripped his jacket into strips with his teeth and made a noose out of it, trying to hang himself.
On being transferred to the military hospital, he was often very restless, screaming and making a great uproar. On being questioned, he answered indifferently and had a vacant stare. During his stay at the clinic, patient was always quiet. Once, however, he had a spell of intense psycho-motor agitation, brought on without any known cause and followed by a short period of bewilderment, lasting altogether half an hour.
Upon being moved to the military hospital, he was frequently very agitated, yelling and causing a huge commotion. When asked questions, he responded in a disinterested manner and had a blank expression. Throughout his time at the clinic, the patient was usually calm. However, there was one instance where he experienced a sudden episode of extreme restlessness, triggered without any obvious reason, followed by a brief period of confusion that lasted a total of half an hour.
Patient had insomnia and his visual fields showed concentric contraction for white. He was sent to a military convalescent hospital.
Patient had trouble sleeping and his visual fields showed a narrowing for white. He was sent to a military rehabilitation hospital.
Psychopathic excitement.
Psychopathic thrill.
Case 190. (Buscaino and Coppola, January, 1916.)
An Italian soldier, 22 (father and brother both committed to insane asylums), since his enlistment had been conducting himself strangely, being impulsive, undisciplined and unbalanced. He had been in Libia from January to August, 1913, and was returned to Italy on account of persistent severe headaches. A month later he was returned to a regiment in camp.
An Italian soldier, 22 (with his father and brother both in mental hospitals), had been acting strangely since he enlisted, showing impulsive, undisciplined, and unstable behavior. He had been in Libya from January to August 1913 and was sent back to Italy due to ongoing severe headaches. A month later, he was reassigned to a regiment in camp.
September 23, 1914, the patient, who had been reproved by a superior officer to whom he had given a disrespectful answer, began to be excitable. He was calm during the day, but acted in a sullen and gloomy way and kept entirely to himself, avoiding even his most intimate friends. When, however, he suddenly recalled his punishment of the morning, he began to race around the yard and finally threw himself upon the ground, remaining there in a cowering and squatting position. At the beginning of the attack he was possessed of a paroxysm of fury, which made a great impression upon those present: eyes agape, face swollen and distorted. He resisted being transferred to the hospital and a furious struggle followed. He tried to bite and scratch everyone. It required ten persons to carry him by his hands and feet safely to the hospital, where he arrived in a state of great excitement and rage.
On September 23, 1914, the patient, who had been reprimanded by a superior officer for a disrespectful response, started to become irritable. He seemed calm during the day but acted moody and withdrawn, avoiding even his closest friends. However, when he suddenly remembered his punishment from the morning, he began to run around the yard and eventually threw himself on the ground, staying there in a cowering and squatting position. At the onset of the episode, he was overwhelmed with a fit of rage that left a strong impression on those watching: his eyes wide, face swollen and contorted. He resisted being taken to the hospital, which led to a fierce struggle. He tried to bite and scratch everyone. It took ten people to carry him by his hands and feet safely to the hospital, where he arrived in a state of extreme agitation and anger.
At the clinic, during the period of observation, he was always tranquil, rather silent, gloomy, somewhat hostile; said he did not remember why he was brought there. Often he was not able to sleep, especially during the first few days of his stay. Has had painful headaches and feeling of dizziness. Several times he showed a tendency to be untruthful. Bodily examination revealed the absence of conjunctival and pharyngeal reflexes. W. R. of serum was negative.
At the clinic, during the observation period, he was usually calm, pretty quiet, gloomy, and somewhat unfriendly; he claimed he didn't remember why he was brought there. He often struggled to sleep, especially in the first few days of his stay. He experienced painful headaches and feelings of dizziness. Several times, he seemed to have a tendency to lie. A physical examination showed no conjunctival or pharyngeal reflexes. The W. R. of serum was negative.
Patient was sent to an interior hospital for convalescence.
Patient was sent to an internal hospital for recovery.
Desertion: Dromomania.
Running away: Dromomania.
Case 191. (Suggestion, 1917.)
An Italian private, 19, came up for desertion in the face of the enemy. He had had a good record during a year of military service and his army conduct in the war was regarded as very good.
An Italian private, 19, was charged with desertion in the face of the enemy. He had a solid record after a year of military service, and his behavior during the war was considered very good.
He felt sad and preoccupied for a number of days, but all of a sudden “some indomitable force” thrust the idea into him to go out into the country a distance of some 20 kilometers from the front, with the definite object of praying in a certain church. It seems that this same impulse had occurred to him several times before but not so forcibly. These prayers were to be said in memory of some sad events in his life.
He felt down and distracted for several days, but suddenly “some unstoppable force” pushed him to head out to the countryside about 20 kilometers from the front, with the clear intention of praying in a specific church. It seemed that this same urge had crossed his mind a few times before, but not as strongly. These prayers were meant to honor some painful events in his life.
Upon examination he was found in a sad and self-accusatory state, much discouraged with ideas of his guilt, unworthiness, and ruin. He had a variety of gloomy fears and obsessions, all of which contributed to the dromomania that culminated in desertion.
Upon examination, he was found in a sad and self-blaming state, feeling very discouraged by thoughts of his guilt, unworthiness, and downfall. He had a range of dark fears and obsessions, all of which contributed to the dromomania that led to his abandonment.
As to his previous history, he had had a depressive psychosis two years before, but the delusions at that time were of persecution. He had also suffered from typhoid fever a few weeks thereafter.
As for his past, he had experienced a depressive psychosis two years earlier, but his delusions at that time were primarily about being persecuted. He also battled typhoid fever a few weeks later.
Suppressed homosexuality.
Repressed homosexuality.
Case 192. (R.P. Smith, October, 1916.)
A man, 32 years, of high intellectual attainments and unblemished moral character—a teacher—enlisted as a private. He apparently found his associates in camp very uncongenial and undesirable. He grew physically tired, then mentally tired and unable to concentrate attention. He began to neglect his uniform, could not keep his equipment in order, became introspective and depressed. The drums he heard seemed to point to his funeral. There was but one thing to do in his opinion: that was to humiliate himself by committing sodomy. He thought of committing suicide.
A 32-year-old man, who was highly educated and had a spotless moral character—a teacher—signed up as a private. He seemed to find his fellow soldiers in camp very unwelcoming and undesirable. He became physically exhausted, then mentally drained and unable to focus. He started to neglect his uniform, couldn’t keep his gear organized, and became withdrawn and depressed. The drumbeats he heard felt like they were signaling his death. In his view, there was only one option: to shame himself by engaging in sodomy. He considered taking his own life.
Upon discharge from military duty, he began to show improvement. Smith regards this case as one of suppressed homosexuality.
Upon leaving the military, he started to show progress. Smith sees this case as one of repressed homosexuality.
Of the cases in which change or excessive work is the precipitating cause, four out of six of Smith’s cases were men.
Of the cases where change or too much work was the main cause, four out of six of Smith's cases were men.
Re homosexuality in the Italian army, Lattes has made a special study. The effeminate homosexual is decidedly unfit for the army, being unable to stand the war stress. Homosexuals diminish army morale. The cases of functional effeminacy with normal physique are likewise unfortunate for the morale of active units, though they may be employed in garrison duty and office work. The medical decision in these cases may prove difficult unless a broad interpretation of the concept “psychopathic” is allowed to prevail.
Re homosexuality in the Italian army, Lattes has conducted a special study. The effeminate homosexual is clearly unfit for military service, as they cannot handle the stress of war. Homosexuals lower army morale. Cases of functional effeminacy in those with a normal physique are also detrimental to the morale of active units, though they might be suitable for garrison duties and administrative work. The medical evaluation in these situations can be challenging unless a wide interpretation of the term “psychopathic” is permitted to take precedence.
Psychopathic: suicidal, then self-mutilative.
Psychopath: suicidal, then self-harming.
Case 193. (MacCurdy, July, 1917.)
An English soldier as a child had night terrors and fear of the dark; as a youth wanted to throw himself down from heights; took delight in seeing animals killed; was shy with both sexes; was never able to run great distances; was taken from school at the age of fifteen for weakness, and had always been subject to headaches, somewhat improved by lenses.
An English soldier as a child had nightmares and was afraid of the dark; as a teenager wanted to jump from heights; enjoyed watching animals being killed; was shy around both boys and girls; could never run long distances; was taken out of school at fifteen due to weakness, and had always suffered from headaches, which were somewhat relieved by glasses.
During training sharp pains appeared in the left groin that grew better when the man lay down. These pains were regarded as hysterical. Thereafter began shortness of breath, pain above the heart, with palpitations and occasional attacks of dizziness. After a short sick leave he insisted upon going to the front, though his superior officer thought it unwise, and, after a period of seventeen months training, was finally sent to France in September, 1916.
During training, sharp pains developed in the left groin that improved when the man lay down. These pains were considered hysterical. After that, he started experiencing shortness of breath, pain above the heart, palpitations, and occasional dizziness. After a brief sick leave, he insisted on going to the front, even though his superior officer thought it was unwise, and after seventeen months of training, he was finally sent to France in September 1916.
He was at first somewhat afraid of shells and, though he soon got used to the shells, the horror of the war grew on him, with pity for the Germans as much as for the British. He became depressed over his weakness and when his commanding officer committed suicide got obsessed with the idea of committing suicide himself. He went so far as to drive a knife into his upper lip and to smash a looking-glass to avoid seeing himself. After a long spell of trench duty he had to be sent home incapacitated.
He was initially a bit scared of the shells, but even though he quickly got used to them, the horror of war started to weigh heavily on him, making him feel pity for both the Germans and the British. He became frustrated with his own weakness, and when his commanding officer took his own life, he became fixated on the idea of doing the same. He even went so far as to stab a knife into his upper lip and smash a mirror to avoid seeing his reflection. After a long time in the trenches, he had to be sent home due to being unable to cope.
In hospital in England he was depressed and suicidal. He began to want to mutilate himself, yet found that a slight pain and the drawing of blood was all that he really craved. Of course, he had been a failure, but now he rationalized the failure by a comfortable conviction that he should never have been sent to the front. He complained of memory and attention disorder, insisted that he was physically incapable of outdoor exercise, complained of headache if he stayed indoors. He said he wanted to go back to the front; knew, however, that he could not, and even refused to consider the possibility of getting well to work at home. At the time of report he argued there was nothing left but suicide.
In a hospital in England, he felt depressed and suicidal. He started to have urges to harm himself, but realized that he only really wanted a little pain and the act of drawing blood. Of course, he felt like a failure, but he comforted himself with the belief that he never should have been sent to the front. He complained about memory issues and trouble focusing, insisted that he was physically unable to exercise outdoors, and said he got headaches if he stayed inside. He claimed he wanted to return to the front but knew he couldn't, and even rejected the idea of getting better to work at home. At the time of the report, he argued that there was nothing left for him but suicide.
Bombardment: Psychasthenia?
Bombing: Psychasthenia?
Case 194. (Laignel-Lavastine and Courbon, July, 1917.)
A twenty-year old engineering student of high grade and without hereditary taint, a scientific and non-introspective man of a brilliant and gay disposition, not very religious, without special sexual abnormality, was mobilized in class 1914, was put into the artillery, and was soon appointed maréchal des logis. He left for the front April, 1915, yet had to be evacuated in November. One afternoon, at the end of a bombardment, he rose from a recumbent attitude and immediately felt a dreamy, bizarre feeling, as if a fog lay between him and his surroundings. Next day, after a good night, he woke in the same state. Everything was bizarre and novel despite the fact that he recognized men and things. A physician ordered rest and after a few days evacuated him.
A twenty-year-old engineering student with excellent grades and no family history of issues, a scientific and non-introspective man with a bright and cheerful personality, not very religious and with no unusual sexual traits, was drafted in class 1914. He was assigned to the artillery and quickly became a sergeant. He left for the front in April 1915 but had to be evacuated in November. One afternoon, after a bombardment, he sat up and immediately felt a strange, dreamy sensation, as if a fog was between him and everything around him. The next day, after a good night's sleep, he woke up still feeling the same way. Everything felt strange and new, even though he recognized the people and things around him. A doctor recommended rest, and after a few days, they evacuated him.
He was cared for in various hospitals, but the psychasthenia increased. He felt a terrible and causeless anguish, with precordial constriction. He felt as if he were about to be executed. His fears appeared after seeing some turning object, such as a wheel or a cane twirling. Gradually this fear was transformed into a genital excitation, though lascivious pictures did not excite him. Seeing anything turning gave him a voluptuous feeling in proportion to the speed of the rotation. It seems that all sexual interest had been at a standstill for several months in the early part of his disease, when suddenly this new aberration appeared. It seems that a portion of the man’s work in the artillery caused him to use screws and cogwheels every day. Attacks of vertigo occurred, with the appearance of an infinity of small, colorless spheres turning over one another, the whole forming a sort of animated system of rotation. In the night this system was luminous and somewhat like what one feels on compressing the globes of the eye. There was a retraction of the visual field. The man would be found in the dream state, especially after waking in the morning or when some novel kind of act was being performed. He[260] got somewhat better and did not wish to go on leave, because he feared the recurrence of these psychasthenic paroxysms. However, he took a leave July 14th. In the first part of his journey he had some vertigo and some of the voluptuous sensations, but in the next two days he was much better. He returned to hospital without trouble.
He was treated in various hospitals, but his psychasthenia worsened. He experienced intense, pointless anxiety, with a tightness in his chest. It felt like he was about to be executed. His fears surfaced after seeing any rotating object, like a wheel or a spinning cane. Over time, this fear morphed into a sexual arousal, although erotic images didn’t stimulate him. Watching anything rotate gave him a pleasurable feeling proportional to the speed of the rotation. For several months at the start of his illness, it seemed like all sexual interest had stalled, until suddenly this new obsession emerged. It appears that part of his work in the artillery involved using screws and gears every day. He experienced episodes of dizziness, with countless small, colorless spheres spinning around each other, creating an animated system of rotation. At night, this system glowed and felt somewhat similar to the sensation when pressing on the eyeballs. His visual field retracted. He would often find himself in a dreamy state, especially after waking up in the morning or when performing some novel action. He[260] improved somewhat and didn’t want to take leave because he was afraid the psychasthenic episodes would return. However, he went on leave on July 14th. At first, he experienced some dizziness and some of the pleasurable sensations, but over the next two days, he felt much better. He returned to the hospital without any issues.
The authors somewhat doubtfully term this case one of a quiet psychasthenia, but in discussion still further talk arose as to the diagnosis.
The authors somewhat doubtfully call this case one of quiet psychasthenia, but during the discussion, further conversation emerged regarding the diagnosis.
Re psychasthenics, Lépine notes that the lack of any out-standing symptoms in many psychasthenics allows them to stay in the army longer than would epileptics or hysterics of the same degree of disease. The line officers tend to consider them exaggerators or simulators. The fact that they besiege the line officers and the physicians with their troubles may add to the impression of falsification. The basis of the psychasthenia is often also, genuinely enough, a fear. Lépine divides the military cases into anxiety neuroses and hypochondrias. The anxiety cases are hypotensive and given to tachycardia. They have very labile vasomotors. When it comes to the necessary exclusion of malingering, it is the history, with its hereditary and collateral taint, that tells the tale. A history in the patient himself of alcoholism, typhoid fever, syphilis, or especially cranial trauma may play a part. An agoraphobic may actually be in general a courageous man except for his crises of anxiety about open spaces.
Regarding psychasthenics, Lépine points out that the absence of significant symptoms in many psychasthenics allows them to remain in the army longer than epileptics or hysterics with the same severity of condition. Line officers tend to see them as exaggerators or pretenders. The fact that they approach line officers and doctors with their concerns may contribute to the impression of deceit. The root of psychasthenia often stems from a genuine fear. Lépine categorizes the military cases into anxiety neuroses and hypochondriasis. The anxiety cases are typically hypotensive and experience tachycardia. They have very unstable vasomotor responses. When it comes to confirming that there is no malingering, it is the patient’s history, particularly any hereditary or associated conditions, that reveals the truth. A history of alcoholism, typhoid fever, syphilis, or especially head trauma in the patient can play a significant role. An agoraphobic may actually be a generally brave person, except when faced with anxiety attacks related to open spaces.
As to the hypochondriacs, fear of syphilis must be noted. Akin to the syphilophobics are a group of pseudo genitourinary cases that fear effects of an old gonorrhoea. See Case 195 (Colin and Lautier) below.
As for the hypochondriacs, fear of syphilis should be acknowledged. Similar to the syphilophobics, there’s a group of pseudo-genitourinary cases that are worried about the impacts of an old gonorrhea. See Case 195 (Colin and Lautier) below.
Gonorrhoea: NOSOPHOBIA, depression, suicidal attempt. Recovery, thirteen months.
Gonorrhea: NOSOPHOBIA, depression, suicidal attempt. Recovery, thirteen months.
Case 195. (Colin and Lautier, July, 1917.)
A munition worker came to Villejuif, December 6, 1915, with cord marks on his neck and conjunctival ecchymoses. He had tried to hang himself.
A munitions worker arrived in Villejuif on December 6, 1915, with cord marks on his neck and bruising in his eyes. He had attempted to hang himself.
Non-alcoholic, he had, however, long since shown signs of imbalance; his father had died insane, in an institution. When the man came in, he wept and groaned and made vague complaints of having contracted a venereal disease, insisting that his genital organs were purple.
Non-alcoholic, he had, however, long since shown signs of imbalance; his father had died insane, in an institution. When the man came in, he cried and groaned and made vague complaints about having contracted a venereal disease, insisting that his genitals were purple.
After a few days, he grew less anxious and told how he was married and how his wife had made life a hell for him, giving herself up to drink and becoming a sloven; how several months since he had contracted gonorrhoea; how though told that the condition was cured, he had found filaments in the urine and had tried a variety of drugs, spending most of his money; how he found more and more filaments, thought himself incurable and unable to live with his wife; how at last, desperate, he had tried to hang himself.
After a few days, he became less anxious and shared that he was married and how his wife had made his life miserable, giving in to drinking and becoming careless; how several months ago he had contracted gonorrhea; how, even after being told it was treated, he kept finding strands in his urine and had tried numerous medications, spending most of his money; how he kept discovering more strands, convinced he was incurable and unable to live with his wife; and how, in the end, desperate, he had tried to hang himself.
He got well quickly, though his convalescence was interrupted by several periods of depression a few days in duration, with anxiety and tears. February, 1916, he was discharged well.
He recovered quickly, but his healing was interrupted by several bouts of depression lasting a few days, filled with anxiety and tears. By February 1916, he was discharged as fully healthy.
He returned four months later; he was still occupied with his disease, still going to physicians and buying drugs. It took six months more before the man could be discharged from the service, at the end of 1916.
He came back four months later; he was still dealing with his illness, still visiting doctors and buying medication. It took another six months before he could be released from the service, at the end of 1916.
This man appears to be a hereditarily predisposed subject, who simply affixed his delusional ideas to a disease which had begun some time before the mental trouble itself. The family plight is important and practically constant in this group of cases. The fear lest the disease shall be revealed by the physician to the family is deep-grounded and impossible to overcome by mere statements concerning professional secrecy. The impulse to suicide is extraordinarily keen.
This man seems to be genetically predisposed, who just attached his delusional thoughts to a condition that started well before the mental issues arose. The family background is significant and almost always relevant in these cases. The fear that the doctor will disclose the illness to the family is deeply rooted and can't be overcome by simply claiming professional confidentiality. The urge to commit suicide is extremely intense.
A soldier (neuropathic taint) after hardships for two days stumbles over a corpse; unconsciousness: Stupor; episodes of fright with war hallucinations; look of premature old age; paresis; anesthesia.
A soldier (neuropathic taint) after enduring hardships for two days stumbles over a corpse; unconsciousness: stupor; episodes of fear with war hallucinations; appearance of premature aging; weakness; numbness.
Case 196. (Lattes and Goria, 1917.)
An Italian soldier (a shoemaker with an epileptic mother and two nervous brothers; himself always irritable and for long periods melancholic; at 15 condemned to nine years in prison for homicide in a quarrel) took part in a number of attacks at the beginning of the war. His company was heavily engaged in October, 1915, and there was no sleep two nights, and only a bit of cold food. He was dazed.
An Italian soldier (a shoemaker with an epileptic mother and two anxious brothers; he was always irritable and often melancholic for long stretches; at 15, he was sentenced to nine years in prison for killing someone in a fight) participated in several attacks at the start of the war. His company was heavily involved in October 1915, with no sleep for two nights and only a little cold food. He felt dazed.
October 24, the company had to advance at night in the rain and under a heavy rifle fire. The shoemaker stumbled over a corpse, fell, and lost consciousness for a time that he thought was very long. He woke up in a camp hospital, remembering all the experiences he had undergone up to the time of losing consciousness. He now fell into a state of torpor, occasionally jumping out of bed and shouting with fear, hurling himself at non-existent persons, assuming a position of defence, and suddenly awaking in anxiety.
October 24, the company had to move at night in the rain while under intense gunfire. The shoemaker tripped over a corpse, fell, and passed out for what felt like a long time. He woke up in a field hospital, recalling everything he had gone through before he lost consciousness. He then slipped into a daze, sometimes jumping out of bed and yelling in fear, throwing himself at imaginary figures, assuming a defensive stance, and abruptly waking up in panic.
October 29, he was transferred to a second hospital, and October 30, in a third hospital, was examined and found well and strongly built, but looking prematurely old. He was inactive, depressed, and stuporous looking. He fell to weeping often and rarely gave any answer to questions. Sometimes he refused food. There was a slight paresis of the left arm, and the left pupil was smaller than the right; both pupils reacted poorly to light. The larynx and cornea did not respond to stimulation. Skin reflexes were poor, and the plantar reflex lacking. The left side about the shoulder and hip showed large patches of anesthesia to touch, pain and heat; but deep sensibility was present in these areas. He slept well at night. Status unchanged for two weeks. He was experimentally sent to the guardhouse, but was soon back in hospital with the same symptoms as ever.
On October 29, he was moved to a second hospital, and on October 30, he was examined at a third hospital. He was found to be healthy and well-built but looked prematurely aged. He seemed inactive, depressed, and appeared stuporous. He often started crying and rarely answered questions. At times, he refused to eat. There was slight weakness in his left arm, and his left pupil was smaller than his right; both pupils reacted poorly to light. His larynx and cornea did not respond to stimulation. His skin reflexes were weak, and the plantar reflex was absent. The area on the left side around his shoulder and hip had large patches where he could not feel touch, pain, or heat, but he could still sense deep pressure in those areas. He slept well at night. His condition remained unchanged for two weeks. He was temporarily sent to the guardhouse, but he returned to the hospital with the same symptoms as before.
B. SHELL-SHOCK: NATURE AND CAUSES.
Bombardment; shell explosion nearby: Mania; death in 24 hours. The AUTOPSY showed superficial punctate hemorrhages of brain and congestion of pia mater. CAUSE OF DEATH—small bulbar hemorrhage, congestion of veins, and nerve-cell changes of a local and differential nature (chromatolysis of vago-accessorius nucleus). SHELL-SHOCK SYMPTOMS due to capillary anemia and chromatolysis of various regions.
Bombardment; a shell exploded nearby: Mania; death in 24 hours. The autopsy showed small superficial bleeding spots in the brain and swelling of the pia mater. Cause of death—small bulbar hemorrhage, swollen veins, and changes in nerve cells of a local and specific type (chromatolysis of the vagal-accessory nucleus). Shell-shock symptoms were due to capillary anemia and chromatolysis in various regions.
Case 197. (Mott, November, 1917.)
A soldier became rather nervous at the Somme, and later underwent intense bombardment for some four hours, February 22, 4 to 8 P.M. Although he said he “could not stand it much longer” he carried on for twelve hours more when perhaps six shells went over, February 23. One of the shells burst about ten feet away, just behind the dugout. The first day of the bombardment he was tremulous and depressed; later coarsely tremulous in the limbs. February 23 there was crying and inability to walk or do any sort of work. Questions were not answered. The pupils were dilated. The evening of February 23 the man was admitted to the field ambulance in acute mania, shouting: “Keep them back! Keep them back!” He was quieted with morphine and chloroform and slept well during the night. There were at least two hypodermic injections of morphine in the ambulance. He woke up the morning of February 24 apparently well, but suddenly died.
A soldier got really nervous at the Somme and then faced heavy shelling for about four hours on February 22, from 4 to 8 P.M. Even though he claimed he “couldn't take it much longer,” he pushed through for twelve more hours when around six shells exploded on February 23. One of the shells detonated about ten feet away, right behind the dugout. On the first day of the shelling, he was shaky and downcast; later, he was noticeably shaky in his limbs. By February 23, he was crying and unable to walk or do any kind of work. He didn't answer any questions, and his pupils were dilated. That evening, on February 23, the man was taken to the field ambulance in acute mania, shouting: “Keep them back! Keep them back!” He was calmed down with morphine and chloroform and slept well during the night. There were at least two injections of morphine given in the ambulance. He woke up on the morning of February 24 apparently fine, but then suddenly died.
The autopsy showed small scratches on the anterior chest wall, but otherwise no sign of external violence. Both lungs were edematous; the left lower lobe showed a considerable hemorrhage. The heart was enlarged and the right side dilated. The liver was somewhat congested. The kidneys were small, but otherwise showed no gross change (urine without sugar or albumin).
The autopsy revealed tiny scratches on the front of the chest, but there were no other signs of external injury. Both lungs were swollen; the left lower lobe had significant bleeding. The heart was enlarged and the right side was stretched. The liver was a bit congested. The kidneys were small but otherwise showed no major changes (urine tested negative for sugar and protein).
Chart 7
EFFECTS OF HIGH EXPLOSIVE SHELLS
- EMOTIONAL
- COMMOTIONAL
- LESIONAL
After Vincent and others
After Vincent and friends
Chart 8
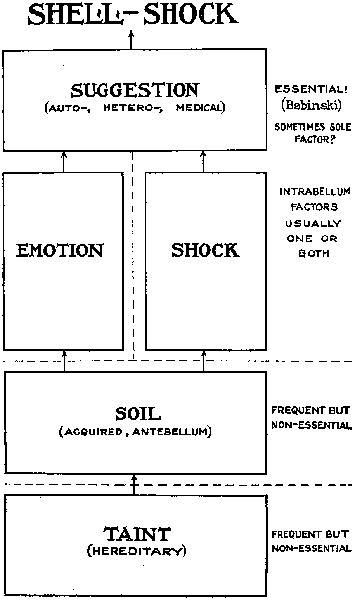
The scalp showed a slight frontal bruise. The brain was extremely congested. On each side of every superficial vessel there was an ecchymosis. A number of minute punctate hemorrhages was found on the surface of the brain in connection with very small vessels. The brain substance was soft, but not markedly edematous. The cerebrospinal fluid was tinged with blood. On each side of the great sinuses of the skull there was considerable ecchymosis. This examination was made by Capt. A. Stokes, R.A.M.C., in the mobile laboratory. There were no areas of large hemorrhage anywhere in the brain substance and no smaller petechiae, except the superficial ones above noted.
The scalp had a small bruise at the front. The brain was very swollen with blood. There was bruising around every superficial blood vessel. Several tiny spots of bleeding were found on the surface of the brain near small blood vessels. The brain tissue was soft, but not excessively swollen. The cerebrospinal fluid had traces of blood in it. There was significant bruising around the large sinuses in the skull. This examination was conducted by Capt. A. Stokes, R.A.M.C., in the mobile lab. There were no large areas of bleeding within the brain tissue and only the minor superficial spots mentioned earlier.
Microscopically Mott confirmed the pial congestion and macroscopic subpial hemorrhages described in the gross. He found besides congestion also actual hemorrhage in the vascular sheaths of the corpus callosum, internal capsule, pons and bulb. Now and then blood corpuscles were found extravasated into the nervous tissue.
Microscopically, Mott confirmed the swelling of the brain's outer layer and the visible subpial bleeding described in the gross examination. He discovered not only congestion but also actual bleeding in the blood vessels surrounding the corpus callosum, internal capsule, pons, and medulla. Occasionally, blood cells were found leaking into the nervous tissue.
The microscopic examination showed a generalized early chromatolysis in the nerve cells of varying intensity, especially affecting the small cells. The Nissl granules of the larger cells were also somewhat abnormal, being smaller and packed rather loosely together.
The microscopic examination revealed widespread early chromatolysis in the nerve cells with varying intensity, particularly impacting the smaller cells. The Nissl granules in the larger cells also appeared somewhat abnormal, being smaller and less densely packed.
The small cells of the bulb and pons were slightly swollen and their nuclei large and clear. As to the larger cells of the bulb and pons, there was less evidence of this swelling and nuclear change.
The small cells in the bulb and pons were a bit swollen, and their nuclei were large and clear. In contrast, the larger cells in the bulb and pons showed less evidence of swelling and changes in the nuclei.
According to Mott, this chromatolysis may perhaps be regarded as a sign of loss of biochemical neuropotential. The chromatolysis indicates a relative degree of exhaustion of the kinetoplasm. Mott assumes that the cells of this victim of shell-shock are in a state of beginning nervous exhaustion. He remarks that the cells of the vago-accessorius nucleus show more signs of this nervous exhaustion than others. With respect to cerebellar findings Mott remarks that the changes found are very similar to those described by Crile in the case of an exhausted and wounded soldier. Mott correlates the mania shown on the evening of February 23 with the venous congestion of the cortex, the small subpial hemorrhages and evidence of scattered arterio-capillary collapse.
According to Mott, this chromatolysis could be seen as a sign of diminished biochemical neuropotential. The chromatolysis shows a certain level of exhaustion of the kinetoplasm. Mott believes that the cells of this shell-shocked victim are starting to experience nervous exhaustion. He points out that the cells in the vago-accessorius nucleus exhibit more signs of this nervous exhaustion than others. Regarding the cerebellar findings, Mott notes that the changes observed are very similar to those described by Crile in the case of an exhausted and injured soldier. Mott connects the mania displayed on the evening of February 23 with the venous congestion of the cortex, small subpial hemorrhages, and evidence of scattered arterio-capillary collapse.
HISTOPATHOLOGY OF CASE OF SHELL-SHOCK, BURIAL, GAS POISONING? (F. W. MOTT)
Punctate hæmorrhages in corpus callosum from a case of shell-shock and burial; very probably accompanied by gas poisoning while lying unconscious and buried. Observe the small white area in the centre of the hæmorrhage, in the middle of which is a small vessel which, under a higher magnification, will be seen to contain a hyaline thrombus. (× 20.)
Punctate hemorrhages in the corpus callosum from a case of shell shock and burial; likely also accompanied by gas poisoning while lying unconscious and buried. Notice the small white area in the center of the hemorrhage, in the middle of which is a small vessel that will show a hyaline thrombus under higher magnification. (× 20.)

Hyaline thrombus of vessel in centre of a punctate hæmorrhage. The thrombus was stained brown by dissolved pigment. Around the blocked vessel is a white area of brown substance containing numbers of leucocytes; outside this is the hæmorrhage, not very distinctly seen. The specimen was prepared from the subcortical white matter of the frontal lobe. (× 345.)
Hyaline thrombus of the vessel in the center of a small hemorrhage. The thrombus was stained brown by dissolved pigment. Surrounding the blocked vessel is a white area of brown substance containing many leukocytes; outside this is the hemorrhage, which is not very clearly seen. The specimen was taken from the subcortical white matter of the frontal lobe. (× 345.)

Leash of small perforating optostriate arteries filled with pigment granules. Two of the arterioles show miliary aneurisms. (× 350.)
Leash of small perforating optostriate arteries filled with pigment granules. Two of the arterioles show miliary aneurysms. (× 350.)

Three punctate hæmorrhages showing optostriate arterioles filled with pigment granules. (× 30.)
Three small hemorrhages showing striped blood vessels filled with pigment granules. (× 30.)
HISTOPATHOLOGY OF SHELL-SHOCK (F. W. MOTT)
NOTE THAT THE CHANGES IN CELLS OF FIG. 3 ARE DIFFERENTIAL FOR NUCLEUS AMBIGUUS: CELLS NEARBY PROVED NORMAL
NOTE THAT THE CHANGES IN CELLS OF FIG. 3 ARE DIFFERENTIAL FOR NUCLEUS AMBIGUUS: CELLS NEARBY PROVED NORMAL

Fig. 1.—Photomicrograph of section of corpus callosum from case of shell-shock showing the capillary punctate hæmorrhages. In several a small white area is seen of brain tissue in the centre of which is a small artery or vein. (Magnification 20 diameters.)
Fig. 1.—Photomicrograph of a section of the corpus callosum from a case of shell shock, showing the tiny punctate hemorrhages. In several of these, a small white area is visible, with a small artery or vein at the center. (Magnification 20 diameters.)
Fig. 2.—Section of medulla oblongata from case of gas poisoning, stained by Nissl method, showing the swollen cells of the nucleus ambiguus. Observe the enlarged, clear, eccentric nucleus; the surrounding cytoplasm shows an absence of Nissl granules. In not a single cell is the nucleus seen in the centre as it should be. (Magnification 450.)
Fig. 2.—Section of the medulla oblongata from a case of gas poisoning, stained using the Nissl method, showing the swollen cells of the nucleus ambiguus. Notice the enlarged, clear, off-center nucleus; the surrounding cytoplasm lacks Nissl granules. In every cell, the nucleus is not positioned in the center as it normally should be. (Magnification 450.)
Fig. 3.—Section of medulla oblongata from case of shell-shock with burial, stained by Nissl method, showing the swollen cells of the nucleus ambiguus. Observe the enlarged, clear, eccentric nucleus; the surrounding cytoplasm shows an absence of Nissl granules. In not a single cell is the nucleus seen in the centre as it should be. (Magnification 450.)
Fig. 3.—Section of the medulla oblongata from a case of shell-shock with burial, stained using the Nissl method, showing the swollen cells of the nucleus ambiguus. Notice the enlarged, clear, off-center nucleus; the surrounding cytoplasm lacks Nissl granules. In none of the cells is the nucleus positioned in the center as it should be. (Magnification 450.)

Fig. 4.—Section of third cervical segment of spinal cord from case of concussion, stained by Nissl method, showing the medium group of anterior horn cells corresponding to the nucleus diaphragmaticus. They show certain amount of perinuclear chromatolysis. But all the cells exhibit the Nissl granules. Even at the seat of concussion, the fourth segment, an external group of cells remains showing Nissl granules. Concussion therefore does not destroy the Nissl granules. Probably the cells of the nucleus diaphragmaticus show a certain amount of chromatolysis because they were continually discharging impulses along the phrenic nerves, and the few cells that were left of the nucleus had therefore much more work to do. (Magnification 300.)
Fig. 4.—Section of the third cervical segment of the spinal cord from a concussion case, stained using the Nissl method, showing the medium group of anterior horn cells related to the nucleus diaphragmaticus. They show some perinuclear chromatolysis. However, all the cells display Nissl granules. Even at the site of concussion, the fourth segment, an external group of cells still shows Nissl granules. Therefore, concussion does not eliminate the Nissl granules. It’s likely that the cells of the nucleus diaphragmaticus show some chromatolysis because they were constantly sending impulses along the phrenic nerves, so the few remaining cells in the nucleus had to work harder. (Magnification 300.)
Mott suggests that the sudden death of the case may be due to a hemorrhage into a sheath of a fair-sized vessel in the median raphe of the bulb; the general venous congestion; and the almost complete chromatolysis of the vago-accessorius nucleus (adjacent hypoglossal nucleus normal).
Mott suggests that the sudden death of the case might be due to bleeding into a sheath of a medium-sized vessel in the median raphe of the bulb; the overall venous congestion; and the nearly complete breakdown of the vago-accessorius nucleus (the adjacent hypoglossal nucleus is normal).
According to Mott, also, many Shell-shock symptoms, e.g., headache, giddiness, amnesia (anterograde and retrograde), dizzy feelings, lack of power of attention, and fatigue, stupor, inertia, mental confusion, terrifying dreams, are to be explained on the basis of capillary anemia and chromatolytic changes.
According to Mott, many symptoms of Shell shock, such as headaches, dizziness, memory loss (both short-term and long-term), feelings of vertigo, difficulty focusing, fatigue, lethargy, mental fog, and terrifying dreams, can be explained by capillary anemia and chromatolytic changes.
Mine explosion. Ecchymoses; no bone or visceral consequences seen at AUTOPSY (third day after explosion) except SUBDURAL HEMORRHAGE and PUNCTATE HEMORRHAGES OF BRAIN.
Mine explosion. Bruises; no bone or internal damage found at AUTOPSY (third day after explosion) except for SUBDURAL HEMORRHAGE and PUNCTATE HEMORRHAGES OF BRAIN.
Case 198. (Chavigny, January, 1916.)
A sergeant in a Chasseur Battalion was in a mine explosion and entered hospital June 19, 1915, so agitated that he had to be tied to the stretcher during transfer from the railway. There were remains of epistaxis and blood in the right ear, not proved to be due to otorrhagia; blue-black ecchymoses of both eyelids; and small ecchymoses of the bulbar conjunctiva of the right eye. No other sign of trauma or fracture. The explosion had probably taken place on June 17 or 18. Patient was but semiconscious and irresponsive; rolled upon the mattress, beating the air with arms and legs, assuming fighting postures and uttering cries. Urinary incontinence. No fever.
A sergeant in a Chasseur Battalion was involved in a mine explosion and was admitted to the hospital on June 19, 1915, so agitated that he had to be tied to the stretcher during the transfer from the train. There were traces of nosebleed and blood in the right ear, although this was not confirmed to be due to ear bleeding; he had dark bruises on both eyelids and small bruises on the bulbar conjunctiva of the right eye. There were no other signs of trauma or fractures. The explosion likely occurred on June 17 or 18. The patient was only semi-conscious and unresponsive; he rolled around on the mattress, flailing his arms and legs, taking up fighting poses and shouting. He also had urinary incontinence. There was no fever.
There was doubt as to the diagnosis, which lay between fracture and concussion. The persistent agitation and oniric delirium pointed rather to concussion. Without further sign, however, the patient died on the night of June 20.
There was uncertainty about the diagnosis, which was somewhere between a fracture and a concussion. The ongoing restlessness and dreamlike delirium seemed more indicative of a concussion. However, without any additional signs, the patient died on the night of June 20.
The autopsy was extremely careful and showed no sign of cranial fracture of vault or base. The cerebrospinal fluid was strongly bloodstained. The inner surface of the dura mater had a thin sheet of hemorrhage, hardly 1 mm. thick, covering both hemispheres and the cerebellum and spreading over the bulb. There was no distension of the lateral ventricles. Serial sections of the brain showed no lesions of the substance, except for slight hemorrhagic points.
The autopsy was very detailed and showed no signs of fractures in the skull or the base. The cerebrospinal fluid was heavily stained with blood. The inner surface of the dura mater had a thin layer of bleeding, barely 1 mm thick, that covered both hemispheres and the cerebellum and extended over the brainstem. There was no swelling in the lateral ventricles. Serial sections of the brain revealed no damage to the tissue, aside from a few small hemorrhagic spots.
According to Chavigny, so slight a meningeal hemorrhage is incapable of producing a mechanical disturbance of the brain and the cause of death could not be said to be meningeal hemorrhage. Massive multiple gas embolism through sudden decompression is not a suitable explanation of a case with death delayed, as in this instance, even if Arnoux’s explanation is suitable for cases of immediate death.
According to Chavigny, such a minor meningeal hemorrhage can't cause a mechanical disturbance in the brain, so we can't attribute the cause of death to meningeal hemorrhage. A massive multiple gas embolism from sudden decompression doesn't fit as an explanation for a case with a delayed death, like this one, even though Arnoux's explanation applies to cases of immediate death.
Mine explosion: no skin, bone, or visceral consequences seen at AUTOPSY (death in seven days) except slight LOCALIZED MENINGEAL HEMORRHAGE.
Mine explosion: no skin, bone, or internal damage seen at AUTOPSY (death in seven days) except for slight LOCALIZED MENINGEAL HEMORRHAGE.
Case 199. (Roussy and Boisseau, August, 1916.)
A soldier entered Val-de-Grâce February 27, 1915, in a state of confusion following mine explosion the night before. He was delirious, thought himself on leave, and had spells of excitement. Lumbar puncture, February 29, showed a slightly darkened fluid, with approximately normal amount of albumin, one or two lymphocytes and rare red blood cells.
A soldier arrived at Val-de-Grâce on February 27, 1915, feeling disoriented after a mine explosion the previous night. He was in a delirious state, believed he was on leave, and experienced moments of excitement. A lumbar puncture on February 29 revealed slightly darkened fluid, with a generally normal amount of albumin, one or two lymphocytes, and a few red blood cells.
A brief period of slight improvement followed, but the restlessness and delirium increased once more, became particularly severe March 3, and the patient died on the night of the third, seven days after the explosion.
A short time of minor improvement came next, but the restlessness and delirium intensified again, becoming especially severe on March 3, and the patient passed away that night, seven days after the explosion.
The autopsy showed slightly congested lungs; no other lesion except a sharply defined hemorrhage in the cervical spinal meninges and over the meninges of the temporal and occipital lobes. Microscopic section of the brain failed to show any hemorrhages within the brain substance.
The autopsy revealed slightly congested lungs; no other lesions other than a clearly defined hemorrhage in the cervical spinal meninges and over the meninges of the temporal and occipital lobes. A microscopic examination of the brain did not show any hemorrhages within the brain tissue.
Here is a case of death following explosion without external wound. The meningeal hemorrhages are hardly enough to explain the death. The explanation of the death must probably be made after histological examination.
Here is a case of death after an explosion without any external injuries. The bleeding in the membranes around the brain doesn't seem to fully explain the death. The cause of death will likely be clarified after a histological examination.
Concussion of spinal cord from shell burst—WITHOUT spinal fracture, WITHOUT penetration of splinters of shell or bone into canal or cord substance: Microscopic demonstration of intraspinal AREAS OF SOFTENING with classical secondary degenerations. Such a case forms a link in the argument that serious lesions of the nervous system may develop as a result of VIOLENCE directly TRANSMITTED through investing tissues EN BLOC.
Concussion of the spinal cord from a shell burst—WITHOUT spinal fracture, WITHOUT any splinters of shell or bone penetrating into the canal or spinal cord: Microscopic evidence of intraspinal AREAS OF SOFTENING with typical secondary degenerations. This case supports the idea that serious nervous system injuries can occur as a result of VIOLENCE directly TRANSMITTED through the surrounding tissues EN BLOC.
Case 200. (Claude and Lhermitte, October, 1915.)
A man, 23, was struck in the left thorax and shoulder, in both thighs and the neck, by fragments from a bursting shell March 27, 1915. One fragment was imbedded near the vertebral column.
A 23-year-old man was hit in the left side of his chest and shoulder, as well as in both thighs and the neck, by debris from an exploding shell on March 27, 1915. One piece was lodged near his spine.
Twenty days later there was an absolute, flaccid paraplegia, yet the legs occasionally gave spontaneous, jerky movements. Tactile anesthesia reached the fourth dorsal root-level, except that the perineoscrotal region and the penis were somewhat sensitive. There was anesthesia to pain and heat, as well as in bones and joints, along with the tactile anesthesia. There was a hyperesthetic region on the right side, corresponding with the distribution of the fourth dorsal root. All the cutaneous reflexes up to the abdominals were gone; but defense reflexes could be brought out in foot and leg by skin, bone or joint stimulation. The deep reflexes of the legs were also lost, whereas those of the arms were increased. Retention of urine without incontinence; no retention of feces. Sacral, trochanteric and heel decubitus had developed in the course of the three weeks following injury. A lymphangitis ran all the way up the right thigh from one of the sores, with a corresponding hyperpyrexia.
Twenty days later, there was complete, flaccid paralysis of the legs, although they occasionally had spontaneous, jerky movements. Sensation was fully absent up to the fourth dorsal root level, except for some sensitivity in the perineoscrotal area and the penis. There was a loss of sensation to pain and heat, as well as in bones and joints, alongside the loss of touch sensation. There was a hypersensitive area on the right side, matching the area supplied by the fourth dorsal root. All skin reflexes up to the abdominal area were absent, but defense reflexes could still be triggered in the foot and leg through skin, bone, or joint stimulation. The deep reflexes in the legs were also absent, while those in the arms were heightened. There was retention of urine without incontinence; however, there was no retention of feces. Pressure sores developed on the sacral, trochanteric, and heel areas during the three weeks following the injury. A lymphangitis extended up the right thigh from one of the sores, causing corresponding high fever.
Surgical intervention was indicated from the evidence of spinal compression at a definite level, but the lymphangitis grew worse. Oniric delirium, and finally a stuporous state, set in, with death May 6, forty days after the wound, a death[273] due to septicemia, without special alteration in the paraplegia itself or in the sensory and reflex situation.
Surgery was necessary because there was clear evidence of spinal compression, but the lymphangitis worsened. Then, oniric delirium developed, leading to a stupor, and death occurred on May 6, forty days after the injury, due to septicemia, without any significant changes in the paraplegia or in the sensory and reflex situation itself.[273]
At autopsy the spine and dura mater proved normal; but microscopically serial sections through the fourth and fifth dorsal segments showed softening of the right anterior horn and posterior columns, with cavitation in the radicular zones, and the white matter of the fifth dorsal segment was in a state of acute degeneration. There were also ependymal changes, namely, at the fifth dorsal level a dilatation with deposit of albumin; in the lumbar region, breakage of the ependymal wall, with cellular gliosis. The dilated ependyma was surrounded by an area of fibrillary gliosis which had proliferated in the form of a septum in the interior of the canal. (According to Claude and Lhermitte, these data concerning hydromyelia, which they regard as secondary to trauma, are an argument in favor of the traumatic origin of certain syringomyelias. They regard the breakage of the ependymal wall as due to hypertension of the spinal fluid due to mechanical lesions.) Their interpretation of such acute degeneration as was found in the fifth segment is that this degeneration, as well as that of the posterior roots, is due to the direct impact of the cerebrospinal fluid upon the cord structure. As for the softenings with cavitation, they regard them as surely due to spinal concussion and as very possibly due to an ischemic necrosis, suggesting that older work by Duret and Michel on concussion of the brain indicates the possibility of a temporary ischemia of the spinal cord from the violent impact of the spinal fluid upon the cord due to shock of the spinal column. The transient hypertension of the spinal fluid might well induce, they believe, a vascular spasm with anemia, to which the gray matter is well known to be especially sensitive. In the present case, a period of somewhat less than six weeks had sufficed to produce secondary degenerations above and below the fifth dorsal segment, of a quite classical sort.
At the autopsy, the spine and dura mater appeared normal; however, microscopic examination of serial sections through the fourth and fifth dorsal segments revealed softening of the right anterior horn and posterior columns, along with cavitation in the radicular zones. The white matter of the fifth dorsal segment was in a state of acute degeneration. There were also changes in the ependyma, specifically at the fifth dorsal level where there was dilatation and a deposit of albumin; in the lumbar region, there was a break in the ependymal wall, accompanied by cellular gliosis. The dilated ependyma was surrounded by an area of fibrillary gliosis that had proliferated in the form of a septum within the canal. (According to Claude and Lhermitte, these findings related to hydromyelia, which they believe is secondary to trauma, support the idea that certain syringomyelias have a traumatic origin. They attribute the break in the ependymal wall to high pressure in the spinal fluid caused by mechanical injuries.) They interpret the acute degeneration observed in the fifth segment, as well as that of the posterior roots, as a result of the direct impact of cerebrospinal fluid on the cord structure. Regarding the softening with cavitation, they are certain it is due to spinal concussion and possibly also due to ischemic necrosis, suggesting that earlier research by Duret and Michel on brain concussion indicates the potential for temporary ischemia of the spinal cord from the violent impact of spinal fluid against the cord due to shock to the spinal column. They believe that the transient high pressure in the spinal fluid could induce a vascular spasm leading to anemia, which the gray matter is known to be particularly sensitive to. In this case, a period of just under six weeks was sufficient to cause secondary degenerations above and below the fifth dorsal segment, which are quite characteristic.
Accordingly, we here deal with a severe form of spinal concussion due to a shellburst, in which intraspinal lesions were produced without spinal fracture or penetration either of bone or of shell fragments into the spinal cord or the spinal fluid.
Accordingly, we are discussing a serious type of spinal concussion caused by a shell explosion, where intraspinal injuries occurred without any spinal fractures or penetration of bone or shell fragments into the spinal cord or the spinal fluid.
Shell explosion (1 meter distant) kills a soldier by bursting both lungs within the intact thoracic cage.
Shell explosion (1 meter away) kills a soldier by rupturing both lungs inside the intact rib cage.
Case 201. (Sencert, January, 1915.)
A man of the 26th Regiment of Infantry was brought October 26, 1914, to Ambulance No. 6 of the Twentieth Army Corps at the Chateau d’Henu. Weakly and jerkily the man was able to tell how, as he was going forward, a large calibre shell fell less than a meter in front of him and exploded. He fell back and lost consciousness, was picked up in the evening and carried to the relief post and then to the ambulance, where he arrived ten hours after the fall. There were signs of a considerable shakeup, with pale and anxious face, nose pinched, hollow eyes, rapid superficial respiration, small pulse, 120, and a feeble voice. There were small skin wounds of the right arm, a finger, and ear, but there was otherwise no wound. The thorax and abdomen were somewhat painful all over, but there was no especial point of pain. The chest showed a slight dulness at the bases. Examination of the abdomen produced defensive movements and the man vomited blood during examination. He was put on his back, kept warm, given artificial serum, hypodermic injections of camphorated oil and caffeine, and carefully watched. In the night he had another bloody vomiting, his pulse became smaller and smaller, dyspnea became more and more intense, and he died late in the night.
A soldier from the 26th Infantry Regiment was brought to Ambulance No. 6 of the Twentieth Army Corps at the Chateau d’Henu on October 26, 1914. Weak and shaky, he managed to explain that while advancing, a large caliber shell landed less than a meter in front of him and exploded. He fell back and lost consciousness, was picked up in the evening, and taken to the relief station before reaching the ambulance, arriving ten hours after the explosion. He showed signs of significant shock, with a pale and anxious face, pinched nose, hollow eyes, rapid shallow breathing, a faint pulse of 120, and a weak voice. There were small skin wounds on his right arm, a finger, and an ear, but no other significant injuries. His chest and abdomen were tender all over, but there wasn't any specific point of pain. The chest showed slight dullness at the bases. An abdominal exam caused him to tense up, and he vomited blood during the assessment. He was laid on his back, kept warm, given artificial serum, and received hypodermic injections of camphorated oil and caffeine, with careful monitoring. During the night, he had another episode of bloody vomiting, his pulse dramatically weakened, his difficulty breathing increased, and he died late that night.
The autopsy showed that the abdomen was free of lesions and that all the organs were of a normal appearance and color. There was no sign of perforation or of peritonitis. The stomach itself was filled with blood and there was a generalized ecchymotic appearance of the mucosa, with small, submucous hematomata and a number of tears in the pyloric portion.
The autopsy revealed that the abdomen had no lesions and all the organs looked normal in appearance and color. There were no signs of perforation or peritonitis. The stomach was filled with blood, showing a widespread bruised appearance of the mucosa, along with small submucous hematomas and several tears in the pyloric section.
The pleurae were found filled with blood, almost a quart in each cavity. The right lung showed a large tear at the level of the middle lobe, 15 cm. long. An orange-size, black bit of lung protruded through the tear. There was no sign of rib fracture opposite this tear, and no subpleural, intercostal[275] or subcutaneous contusion. The thorax wall was perfectly normal.
The pleurae were filled with blood, nearly a quart in each cavity. The right lung had a large tear at the level of the middle lobe, 15 cm long. An orange-sized, black piece of lung was sticking out through the tear. There were no signs of rib fractures opposite this tear, and no subpleural, intercostal, or subcutaneous bruising. The thoracic wall was completely normal.
The left lung showed, in the middle portion of the upper lobe, a somewhat analogous pleural tear, almost as big as that on the right, with another large hernia of black lung. Bits of the herniated lung sank in water. The thorax wall was intact. The pericardium was free from blood. There was nothing else abnormal about the body.
The left lung had a similar pleural tear in the middle part of the upper lobe, almost as large as the one on the right, along with another big hernia of black lung. Pieces of the herniated lung floated in water. The chest wall was intact. The pericardium was clear of blood. Everything else about the body was normal.
Re effects of an explosion upon structures with intervening objects left intact, Fauntleroy notes that a shell bursting three yards from an aneroid barometer may force its levers into an abnormal position. A further fact will indicate how permanent is the physical state into which the levers are forced; for when the barometer with its levers placed right was placed under a bell-jar and the pressure therein was reduced to 410 mm., the levers resumed the position into which the explosion of the big shell had thrown them.
Re effects of an explosion on structures with nearby intact objects, Fauntleroy points out that a shell exploding three yards away from an aneroid barometer can push its levers into an unusual position. Another observation shows how permanent the physical state is that the levers end up in; when the barometer, with its levers in the correct position, was placed under a bell jar and the pressure was lowered to 410 mm, the levers returned to the position they were forced into by the blast of the large shell.
Re windage and internal effects in the human body, Ravaut recalls the fact that the internal and intraneural hemorrhages of Caisson disease (“bends”) are well known. The external hemorrhages of aeronauts and mountain climbers belong in the same physical class. Dynamite exploded in a pond kills fish. Dynamite may break pillars inside a building without damaging its front. Cases like Chavigny’s (198), Roussy and Boisseau’s (199), Claude and Lhermitte’s (200), as well as Ravaut’s own case (202) are in point.
Re windage and internal effects in the human body, Ravaut notes that the internal and intraneural bleeding associated with Caisson disease (“the bends”) is well understood. The external bleeding experienced by aviators and mountain climbers falls under the same physical category. Dynamite detonated in a pond kills fish. Dynamite can damage pillars inside a building without harming its exterior. Cases such as Chavigny’s (198), Roussy and Boisseau’s (199), Claude and Lhermitte’s (200), as well as Ravaut’s own case (202), illustrate this point.
Shell explosion near by: Paraplegia, interpreted as due to windage. Two foci of HEMORRHAGE (SPINAL CANAL, BLADDER) clinically proved to exist in a case without external sign of injury.
Shell explosion nearby: Paraplegia, considered due to windage. Two areas of HEMORRHAGE (SPINAL CANAL, BLADDER) confirmed clinically in a case with no external signs of injury.
Case 202. (Ravaut, February, 1915.)
An infantry sergeant was brought to the ambulance, one day in November, 1914, with a paralysis which had set in immediately upon the explosion of a large shell a short distance away. Both legs were paralyzed and there was anesthesia to the navel. He could not urinate. It was early in the war, and Ravaut thought he would find an injury to the vertebral column, but on undressing the soldier there was no wound. The skin was intact, and there was not even an ecchymosis. The patient was suffering not at all, but said that after the shell exploded he felt a forcible shock, was stunned for a moment, and when he wanted to rise, found that his legs were inert. His state did not change during the day and he did not urinate. Catheterization showed a urine full of blood. This indicated a lumbar puncture, and a bloody fluid emerged under great pressure. Thus two foci of hemorrhage were proven to exist in this patient despite the fact that there was no external lesion.
An infantry sergeant was brought to the ambulance one day in November 1914, suffering from paralysis that began immediately after a large shell exploded nearby. Both of his legs were paralyzed, and he had lost sensation down to his navel. He was unable to urinate. It was early in the war, and Ravaut expected to find an injury to the spinal column, but when he examined the soldier, there was no visible wound. The skin was intact, and there wasn't even a bruise. The patient felt no pain but reported that after the explosion, he experienced a strong shock, felt stunned for a moment, and, when he tried to get up, realized his legs were completely unresponsive. His condition didn't improve throughout the day, and he still could not urinate. Catheterization revealed urine full of blood. This pointed to a lumbar puncture, and bloody fluid flowed out under high pressure. Thus, two sources of hemorrhage were confirmed to exist in this patient, even though there was no external injury.
Re windage effects, see suggestions of Ravaut under Case 201. Ravaut also suggests that certain cases of emotional jaundice may be similarly explained on the basis of internal lesion due to windage. Sundry cases of gastro-intestinal disorder and of hemoptysis fall into the same class; possibly the cases of death in a fixed posture belong there, too. Ravaut thinks, despite the look of hysteria about the shell-shock cases of paraplegia, deafness, mutism, and the like, that the cases are actually ones in which there has been at the beginning a slight or severe hemorrhage, clearing up in a few days. He states that there is a pretty definite parallelism between the course of the clinical symptoms and the chemical characteristics of the spinal fluid.
Re windage effects, see Ravaut's suggestions under Case 201. Ravaut also suggests that some instances of emotional jaundice could be similarly explained by internal injuries due to windage. Various cases of gastrointestinal disorders and hemoptysis fall into this category; possibly the cases of death in a fixed position might belong there as well. Ravaut believes that, despite the appearance of hysteria in shell-shock cases involving paraplegia, deafness, and mutism, these cases are actually ones where there was initially a slight or severe hemorrhage, resolving within a few days. He states that there’s a fairly clear parallel between the progression of the clinical symptoms and the chemical characteristics of the spinal fluid.
Shell-explosion in confined space; paraplegia after fifteen minutes; slight hemorrhage and LYMPHOCYTOSIS of spinal fluid; Hematomyelia.
Shell explosion in a confined space; paralysis after fifteen minutes; slight bleeding and lymphocytosis of spinal fluid; hematomyelia.
Case 203. (Froment, July, 1915.)
A Sergeant lying down in a small dugout space, 2 × 1 m. high, had a 77 shell burst behind his head and between his head and the back of the dugout. The patient was not moved by the explosion, but was buried in a small amount of earth and stones to a depth of about 20 cm. He was not wounded and showed no ecchymoses either then or later. Aided by stretcher bearers, he was able to walk to the relief post about 400 meters from the trench. He did not lose consciousness, and got to the relief post about a quarter of an hour after the shell burst. Thereafter, however, he was unable to move his legs. The accident happened February 6 at 4 o’clock. He was examined 24 hours after the trauma. The accompanying diagrams show the variations in sensory disorder at intervals during six months.
A sergeant lying in a small dugout space, 2 × 1 m high, experienced a 77 shell explode behind his head and between him and the back of the dugout. He wasn't knocked out by the explosion but was buried under a small amount of earth and stones to a depth of about 20 cm. He wasn’t injured and had no bruises then or later. With the help of stretcher bearers, he was able to walk to the relief post about 400 meters from the trench. He didn't lose consciousness and reached the relief post around fifteen minutes after the shell exploded. However, after that, he was unable to move his legs. The incident occurred on February 6 at 4 o’clock. He was examined 24 hours after the injury. The accompanying diagrams show the changes in sensory disorder at intervals over six months.
A lumbar puncture, February 8, 1915, showed hypertensive clear fluid without macroscopic clot on centrifuging, but showing a number of red blood cells and lymphocytes—3 or 4 to the microscopic field. There was a slight hyperalbuminosis. The development of the muscular atrophy and hypo-excitability of the left lower extremity, the exaggeration of the left knee-jerk, together with the spinal fluid appearances, seemed to prove the organic nature of the paraplegia. There was an intense rhachialgia, with radiation along the sciatic nerve. This outlasted all other symptoms. Thermo-analgesia was the most prominent sensory disorder. There were no sphincter disorders.
A lumbar puncture on February 8, 1915, showed clear, hypertensive fluid without any visible clots when centrifuged, but it contained quite a few red blood cells and lymphocytes—about 3 or 4 per microscopic field. There was a slight increase in albumin levels. The progression of muscle wasting and reduced responsiveness in the left leg, along with the spinal fluid findings, seemed to confirm the organic nature of the paraplegia. There was intense back pain that radiated along the sciatic nerve, which lasted longer than all other symptoms. The most significant sensory issue was a lack of temperature sensation. There were no issues with sphincter control.
During the first days, the anesthesia was of a pure segmentary type, with nothing about it to suggest that it was later to be supplanted by a radicular type of disorder. Hematomyelia was, years ago, thought—according to Froment—to tend to yield sensory disorders of a segmentary nature. At the outset this anesthesia was total, though there was a[278] vague, poorly localized feeling on intense painful excitations,—as with energetic pricking or burning. Thus the protopathic sensibility of Head had remained, whereas the epicritic sensibility had disappeared.
During the first few days, the anesthesia was purely segmental, showing no signs that it would later be replaced by a radicular type of disorder. Hematomyelia was believed—according to Froment—years ago to usually lead to sensory disorders of a segmental nature. Initially, this anesthesia was total, although there was a[278] vague, poorly localized sensation during intense painful stimuli—like strong pricking or burning. Thus, the protopathic sensitivity described by Head remained, while the epicritic sensitivity had vanished.
Detailed examination of this case showed extreme errors in the position sense. For example, pricking the foot might be localized as pinching above the knee. The cremaster reflex was extremely marked and would appear upon even slight excitation of any part of the lower extremity, even at times when the patient declared he felt nothing. These phenomena at the beginning early gave place to a syringomyelic type of anesthesia.
A detailed examination of this case revealed significant mistakes in the sense of position. For instance, a pinprick on the foot could feel like it was happening above the knee. The cremaster reflex was very pronounced and would trigger even with minor stimulation of any part of the lower leg, sometimes when the patient claimed to feel nothing at all. These symptoms initially evolved into a syringomyelic type of numbness.
At the time of report, July 29, 1915, Froment regarded this case as analogous to hematomyelias of divers, although there is not such a degree of decompression; the suddenness of the decompression is more marked in these Shell-shock cases than in divers.
At the time of the report, July 29, 1915, Froment viewed this case as similar to hematomyelias seen in divers, even though the level of decompression isn't as severe; the abruptness of the decompression is more pronounced in these Shell-shock cases than in divers.
Shell explosion; bowled over; loss of consciousness: Hemiplegia with reflex signs thought to be organic; hypertensive spinal fluid; LYMPHOCYTOSIS.
Shell explosion; knocked down; loss of consciousness: Hemiplegia with reflex signs believed to be organic; high blood pressure in spinal fluid; LYMPHOCYTOSIS.
Case 204. (Guillain-Barré Syndrome, August, 1915.)
A corporal in the engineers was going the night of June 7th to a creneau of mitrailleuses, when he was bowled over by a bursting shell. He lost consciousness and was carried to the cantonment by his comrades. Next morning he complained of headache and pain in the back; had a convulsion; and proved on examination to have a left-sided hemiplegia. He was given the diagnosis of hysterical hemiplegia.
A corporal in the engineers was heading to a machine-gun position on the night of June 7th when he was knocked down by an exploding shell. He lost consciousness and was taken to the camp by his comrades. The next morning, he reported a headache and back pain; experienced a seizure; and upon examination, it was found that he had left-sided hemiplegia. He was diagnosed with hysterical hemiplegia.
He was sent to the 6th Army neurological center, and there showed a complete left-sided hemiplegia with tendency to contracture. The left knee-jerk and arm reflexes were exaggerated, and there was ankle and patella clonus with Babinski sign. There was a dysesthesia on the left side, with wrong interpretation and poor localization of painful stimuli, and non-recognition of cold and heat sensations. Muscle sense and stereognosis were impaired. There was a slight dysarthria. Lumbar puncture yielded a clear hypertensive fluid with a slight lymphocytosis.
He was sent to the 6th Army neurological center, where he exhibited complete left-sided paralysis with a tendency for contractures. The reflexes in his left knee and arm were overactive, and there was clonus in his ankle and knee, along with a positive Babinski sign. He experienced abnormal sensations on the left side, with difficulty interpreting and localizing painful stimuli, and he couldn't recognize cold or heat sensations. His ability to sense muscle position and his stereognosis were impaired. There was a slight speech impairment. A lumbar puncture revealed clear, high-pressure fluid with a slight increase in lymphocytes.
The situation remained without change for a month, when the patient was evacuated to the rear. Thus, a shell-burst can produce destructive nerve lesions without evidence of external injury.
The situation stayed the same for a month, until the patient was moved to the rear. Therefore, a shell explosion can cause severe nerve damage without any visible external injury.
Re hypertensive spinal fluid, Sollier and Chartier cite Dejerine as having brought the proof of hypertension in the cerebrospinal fluid in Shell-shock cases. They also believe that the Shell-shock hysteria is built up on a physical basis, more or less after the model of Charcot’s hysterotraumatism. Shock, windage, and gas may bring about the same kind of result. They rely especially on the cases of Sencert (201) and Ravaut (202) for their argument (1915). They recall the fact that Charcot found a hysteria due to lightning stroke and to high tension electric accidents. They quote Lermoyez as attributing like results in ear cases to labyrinthine shock, tympanic rupture, and ear hemorrhages.
Re hypertensive spinal fluid, Sollier and Chartier reference Dejerine, who provided evidence of hypertension in the cerebrospinal fluid in cases of Shell shock. They also suggest that Shell shock hysteria is based on a physical foundation, somewhat following the model of Charcot’s hysterotraumatism. Shock, wind blast, and gas can produce similar effects. They particularly support their argument with the cases of Sencert (201) and Ravaut (202) (1915). They recall that Charcot identified hysteria resulting from lightning strikes and high-tension electrical accidents. They quote Lermoyez, who attributes similar outcomes in ear cases to labyrinthine shock, tympanic rupture, and ear hemorrhages.
Shell-shock: Hemiparesis, amnesia. Lumbar punctures early (but here as late as one month after shock and after disappearance of hemiparesis) showed PLEOCYTOSIS and hyperalbuminosis.
Shell shock: Weakness on one side, memory loss. Spinal taps done early (but in this case, as late as one month after the shock and after the weakness went away) showed an increase in white blood cells and high levels of albumin.
Case 205. (Souques, Megevand and Donated, October, 1915.)
A French sergeant, a machine gunner, was the victim of shell-burst September 25, 1915, was evacuated with a diagnosis of commotio cerebri, and, when examined at Paul-Brousse October 5, showed a right-sided hemiparesis, clouding of consciousness and somnolence, the hemiparesis involving the face, with deviation of tongue to right, Babinski reflex right, cremasteric and abdominal reflexes abolished on right. Normal respiration and pulse.
A French sergeant, a machine gunner, was injured by a shell explosion on September 25, 1915. He was evacuated with a diagnosis of concussion and, when examined at Paul-Brousse on October 5, showed right-sided weakness, confusion, and excessive sleepiness. The weakness affected his face, with his tongue deviating to the right, the Babinski reflex present on the right, and the cremasteric and abdominal reflexes absent on the right. His respiration and pulse were normal.
Lumbar puncture October 7, that is, thirteen days after the injury, yielded a clear fluid with an excess of albumin, 144 small lymphocytes (some degenerate) and a single endothelial cell.
Lumbar puncture on October 7, which was thirteen days after the injury, produced clear fluid with high levels of albumin, 144 small lymphocytes (some of which were degenerate), and a single endothelial cell.
October 12, the knee-jerk was a little less lively on the right side. The plantar reflex varied between extension and flexion on the right side. The cremasteric reflex had been weakly regained on the right side.
October 12, the knee-jerk reaction was a bit less responsive on the right side. The plantar reflex fluctuated between extension and flexion on the right side. The cremasteric reflex had been weakly restored on the right side.
The patient was now less stupid and could tell how he jumped when the shell burst, and how he had been in the air ten minutes (!) and fell, getting up at once, with nothing wrong except nosebleed. After a half-hour he felt weaker and was ordered to leave the post, whereupon, on the road, his weakness increased and he tended to fall to the right, but reached the ambulance on foot.
The patient was now less dazed and could remember how he jumped when the shell exploded, how he had been in the air for ten minutes, and how he fell, getting up immediately with nothing wrong except a nosebleed. After half an hour, he felt weaker and was told to leave his post. On the way, his weakness got worse, and he tended to lean to the right, but he made it to the ambulance on foot.
October 23, there was no longer any evidence of hemiparesis, the Babinski reflex had entirely disappeared; there was no complaint except of dizziness and headaches. He got back his autocritique on the matter of remaining in the air ten minutes, but there was still an amnesia for the ten day period between the shock and his arrival at Paul-Brousse. He forgot that he had had a lumbar puncture October 7.
October 23, there was no longer any sign of weakness on one side, the Babinski reflex had completely disappeared; the only complaints were dizziness and headaches. He reflected on the situation about staying in the air for ten minutes, but he still had no memory of the ten days between the shock and his arrival at Paul-Brousse. He forgot that he had undergone a lumbar puncture on October 7.
Another puncture, October 25, yielded some 14 or 15 lymphocytes to the cmm. There was still an excess of albumin. The lymphocytes decreased further according to a puncture November 2. Had this patient been examined some weeks after the shock there would have been no signs of an organic paresis, no special modification of the spinal fluid, and no reason for regarding the man as other than an hysteric. Early spinal puncture is, accordingly, important.
Another puncture on October 25 yielded about 14 or 15 lymphocytes in the cerebrospinal fluid. There was still too much albumin present. The lymphocytes decreased even more according to a puncture on November 2. If this patient had been examined a few weeks after the shock, there would have been no signs of an organic paralysis, no specific changes in the spinal fluid, and no reason to consider the man anything other than hysterical. Therefore, early spinal puncture is crucial.
Of course, the question whether the lymphocytes and hyperalbuminosis of the fluid might not be syphilitic must be raised. At the Hospital Medical Society meeting, October 29, 1915, Souques states that Ravaut and Guillain believe that simple shell-shock often produces “syphilitic” chemical, physical or cytological changes in the spinal fluid. Roussy is cited as thinking such changes rare.
Of course, we have to consider whether the lymphocytes and high albumin levels in the fluid could be related to syphilis. At the Hospital Medical Society meeting on October 29, 1915, Souques mentioned that Ravaut and Guillain believe that simple shell shock can often cause "syphilitic" chemical, physical, or cytological changes in the spinal fluid. Roussy is noted as believing that such changes are rare.
Shell-shock; burial: Coma and semicoma; BLOOD-STAINED SPINAL FLUID. Improvement on puncture. Persistent astasia abasia with spasticity.
Shell shock; burial: Coma and semi-coma; BLOOD-STAINED SPINAL FLUID. Improvement after puncture. Ongoing inability to walk with spasticity.
Case 206. (Leriche, September, 1915.)
A man was buried March 15, 1915, following the bursting of a large calibre shell. He is said to have had hemoptysis and arrived at hospital March 17 in coma. He kept moaning while asleep. March 18, he was still stupid and as if stunned. He did not talk or understand what was said, but was able to write a few words. The knee-jerks were a little exaggerated. There was a slight spasticity of the limbs, which was exaggerated on emotion into a sort of spasmodic crisis.
A man was buried on March 15, 1915, after a large shell exploded. He reportedly had coughing up blood and got to the hospital on March 17 in a coma. He continued to moan in his sleep. By March 18, he was still dazed and unresponsive. He didn’t speak or understand what was said, but he was able to write a few words. His knee reflexes were slightly heightened. There was a bit of stiffness in his limbs, which intensified with emotional stress into a kind of spasmodic episode.
Lumbar puncture gave a reddish fluid under strong tension. After lumbar puncture the man came out of coma and the next day, after another puncture (fluid slightly yellowish), there was further improvement and the patient spoke. The third puncture, March 20, yielded yellow fluid. The spastic phenomena still persisted, however. The patient could not walk or stand. Every time he touched the ground he had a clonic crisis. He was evacuated to a neurological center.
Lumbar puncture revealed a reddish fluid under high pressure. After the lumbar puncture, the man woke up from his coma, and the next day, after another puncture (which produced slightly yellowish fluid), he showed further improvement and was able to speak. The third puncture on March 20 resulted in yellow fluid. However, the spastic symptoms continued. The patient was unable to walk or stand. Every time he made contact with the ground, he experienced a clonic seizure. He was transferred to a neurological center.
Re astasia-abasia, Nonne found these cases heading a group of 63 cases of war hysteria treated in a twelvemonth. Figures as follows:
Re astasia-abasia, Nonne discovered that these cases were part of a group of 63 cases of war hysteria treated over the course of a year. The figures are as follows:
| Astasia-abasia | 14 |
| Generalized tremor | 12 |
| Brachial monoplegia | 11 |
| Isolated contracture | 6 |
| Crural paraplegia | 5 |
| Mutism | 5 |
| Isolated tic | 4 |
| Hemiplegia | 3 |
| Isolated respiratory convulsions | 2 |
| Isolated sensory disorder | 1 |
Fifty-one of the 63 cases were freed by therapy from their main symptoms (twenty-eight cases cured in one or two hypnotic sittings).
Fifty-one of the 63 cases were relieved of their main symptoms through therapy (twenty-eight cases were cured in one or two hypnotic sessions).
Prolonged bombardment; shell explosion (nearby?): Depression; suicidal attempt; hypertensive spinal fluid.
Prolonged bombardment; nearby shell explosions: Depression; attempted suicide; high blood pressure in spinal fluid.
Case 207. (Leriche, September, 1915.)
A patient entered an evacuation hospital June 27, having come from an ambulance with a ticket reading, “Melancholic depression, with stupor—attempt at suicide (threw himself into a pond)—sprained ankle—to be evacuated, lying down, on a milk diet.” The patient was depressed, indifferent to surroundings, irresponsive, and did not even look at an interlocutor. There was no other somatic sign except a pulse of 62. He did not eat, and remained lying down, without movement. Lumbar puncture in a sitting posture yielded a clear liquid under pressure of 34. June 30, another lumbar puncture yielded clear fluid of a dichroic appearance when looked at from above. 25 c.c. were removed. July 1, there had been a good deal of improvement. The patient said he was better and began to take a little milk. July 2, there was still some improvement. Pulse 60. He said that his condition had lasted a month and that it followed a violent and prolonged bombardment for ten days in his sector. July 3, he was much better, began to look about, talk, and eat a little. July 4, lumbar puncture yielded a clear fluid with a pressure of 30, reduced to 22 after withdrawal of 20 c.c.
A patient arrived at an evacuation hospital on June 27, coming from an ambulance with a ticket stating, “Melancholic depression, with stupor—attempted suicide (jumped into a pond)—sprained ankle—to be evacuated, lying down, on a milk diet.” The patient was depressed, indifferent to his surroundings, unresponsive, and didn’t even look at anyone talking to him. The only other physical sign was a pulse of 62. He didn’t eat and lay still, without moving. A lumbar puncture done while sitting produced a clear fluid under a pressure of 34. On June 30, another lumbar puncture yielded clear fluid that appeared dichroic when viewed from above. 25 c.c. were removed. By July 1, he showed significant improvement. The patient said he felt better and started to drink a bit of milk. On July 2, he continued to improve. Pulse was 60. He mentioned that his condition had lasted a month and that it began after a violent and prolonged bombardment lasting ten days in his area. By July 3, he was much better, began looking around, talking, and eating a little. On July 4, a lumbar puncture produced clear fluid with a pressure of 30, which dropped to 22 after removing 20 c.c.
According to Leriche, explosion of large calibre shells or of a mine can produce cerebral or spinal symptoms, some of which are removed by lumbar puncture. The fluid is red shortly after the explosion and under hypertension for some days. Such hypertension may be found even in shell cases that have no other sign of cerebral condition. This particular melancholy patient had a relapse and another depression with fugue.
According to Leriche, the explosion of large-caliber shells or a mine can cause symptoms affecting the brain or spine, some of which can be alleviated by a lumbar puncture. The fluid is red shortly after the explosion and can remain under pressure for several days. This pressure can be observed even in shell cases that show no other signs of brain issues. This particular sad patient experienced a relapse and another episode of depression with fugue.
Example of HEMATOMYELIA, indirect result of bullet wound. Partial recovery.
Example of HEMATOMYELIA, an indirect result of a bullet wound. Partial recovery.
Case 208. (Mendelssohn, January, 1916.)
An infantry subaltern, 23 years old, was injured September 24, 1914, by a rifle bullet, which entered above the left clavicle and emerged between the right scapula and the vertebral column. The patient leaped into the air when he was struck, but fell at once and found that his legs were paralyzed. A feeling of cold crept up from the feet to the region of the umbilicus. Consciousness was preserved. There was hemoptysis because of the bullet’s passing through the left lung. The wounds all healed quickly. There was retention, followed by incontinence, of urine and feces; and the situation was complicated by eschars in the gluteal and trochanteric region.
An infantry second lieutenant, 23 years old, was injured on September 24, 1914, by a bullet that entered above his left collarbone and came out between his right shoulder blade and spine. He jumped into the air when he was hit, but fell immediately and realized his legs were paralyzed. A cold sensation spread from his feet up to his belly button. He remained conscious. There was coughing up blood due to the bullet passing through his left lung. The wounds all healed quickly. He experienced retention followed by incontinence of urine and feces, and the situation was complicated by sores in the buttocks and hip area.
For three months there was no change in the paraplegia, except that at the beginning of the third month the patient could move his fingers a little and raise his knees slightly. He was transferred back through three hospital units, with a diagnosis of spinal cord lesion or fracture due to a vertebral column lesion at the second and third dorsal vertebrae.
For three months, there was no change in the paraplegia, but at the start of the third month, the patient could move his fingers a bit and lift his knees slightly. He was moved through three hospital units with a diagnosis of spinal cord injury or fracture due to an injury to the vertebral column at the second and third dorsal vertebrae.
Seven months after injury, he reached a Russian hospital for a laminectomy, incapable of standing or walking without support, although able to sit and rise with extreme difficulty. He could now very slightly flex and extend the knees, and very slightly flex and rotate the ankle, and weakly move the toes. Passive movements could be carried out without much difficulty, though there was a slight joint and muscle stiffness. Both quadriceps muscles were markedly atrophied. There was slight amyotrophy of the lower legs. Tendon reflexes were exaggerated, and there was a marked ankle clonus, a Babinski reflex, and an abolition of the abdominal and cremasteric reflexes.
Seven months after his injury, he arrived at a Russian hospital for a laminectomy, unable to stand or walk without help, though he could sit and get up with great difficulty. He could now slightly bend and straighten his knees, and very slightly bend and rotate his ankle, as well as weakly move his toes. Passive movements could be done with some ease, although there was a bit of stiffness in his joints and muscles. Both of his quadriceps muscles were noticeably weakened. There was some muscle wasting in his lower legs. His tendon reflexes were heightened, and there was significant ankle clonus, a Babinski reflex, and a loss of the abdominal and cremasteric reflexes.
There was a sensory disorder of an incomplete syringomyelic pattern, with diminished sensibility to heat and complete abolition of pain sensibility. Touch and electric[285] sensations were somewhat delayed. There was a diminution in the faradic and galvanic excitability of the legs and feet; vasomotor disturbance (slight hyperidrosis) of the paralyzed limbs. Two of the eschars had not yet cicatrized. The sphincteric disturbances had diminished. For the rest the patient was normal. The second and third vertebrae showed deformity and were painful to pressure and percussion of spinous processes.
There was a sensory issue resembling an incomplete syringomyelic pattern, with reduced sensitivity to heat and complete loss of pain sensitivity. Touch and electric sensations were slightly delayed. There was a decrease in the responsiveness of the legs and feet to faradic and galvanic stimuli; the paralyzed limbs showed some signs of vasomotor issues (slight sweating). Two of the sores had not yet healed. The problems with the sphincters had lessened. Aside from that, the patient was normal. The second and third vertebrae were deformed and painful to touch and when tapped.
The patient was treated by galvanization of the spine, with a current descending at first and then ascending, and by faradization of the paralyzed muscles. There was progressive improvement, irregular but constant. At the time of report, July 1, 1915, he was perfectly well, able to take long walks, and without sphincter or sensory disturbance. The tendon reflexes were still exaggerated, and there was still a slight ankle clonus and Babinski. The abdominal and cremasteric reflexes were still abolished. The last of the seven eschars had not yet healed over.
The patient received treatment for their spine using galvanization, starting with a descending current and then switching to an ascending one, along with faradization of the paralyzed muscles. There was ongoing, though irregular, improvement. As of the report on July 1, 1915, he was completely well, able to take long walks, and had no issues with sphincter control or sensation. The tendon reflexes were still heightened, and there was a slight ankle clonus and Babinski response. The abdominal and cremasteric reflexes had not returned. The final one of the seven eschars had not yet healed.
For the organic nature of this lesion, the numerous early eschars, the persistent sphincter disturbances, the limited paresis of the legs, the reflex disorders, and the dissociation of sensations seem abundant evidence. It is probable that there was no fracture of the vertebrae (X-ray confirmation), and it is probable that there was a meningeal hemorrhage, together with some hemorrhagic foci in the spinal cord substance, especially in the gray matter. A good deal remains doubtful: Mendelssohn remarks that the sphincter disturbances ought to be related to disorder of the fourth and fifth sacral segments, and the knee-jerk and Achilles jerk absence with disorder of the lower lumbar, and sacral region; the abdominal reflex disorder with the low thoracic lesion; the distribution of the anesthesia ought to indicate a lesion in the lower part of the spinal cord. Was not the hemorrhage therefore lower down than the spot where the vertebrae were displaced? It is surely of prognostic note that the eschars did not necessarily foretell a fatal outcome; in fact, the patient had become functionally well before the seventh eschar was healed over.
The organic nature of this lesion, the multiple early sores, the ongoing sphincter issues, the limited weakness in the legs, the reflex problems, and the separation of sensations all provide strong evidence. It's likely that there wasn't a fracture of the vertebrae (as confirmed by X-ray), and it’s likely that there was a bleeding in the meninges, along with some hemorrhagic spots in the spinal cord tissue, particularly in the gray matter. A lot remains uncertain: Mendelssohn points out that the sphincter issues should be linked to problems with the fourth and fifth sacral segments, while the absence of the knee-jerk and Achilles reflex suggests issues in the lower lumbar and sacral areas; the abdominal reflex disorder relates to a low thoracic lesion; and the pattern of anesthesia should indicate a lesion in the lower part of the spinal cord. So, could the hemorrhage have been lower down than where the vertebrae were displaced? It’s definitely worth noting that the sores didn’t necessarily predict a fatal outcome; in fact, the patient had improved functionally before the seventh sore was healed.
Shell explosion with subject lying down applied to machine-gun; no contusion: HEMATOMYELIA. Partial recovery.
Shell explosion with the person lying down applied to a machine gun; no bruising: HEMATOMYELIA. Partial recovery.
Case 209. (Babinski reflex, June, 1915.)
A veterinary student, six months captive in Germany, wrote out for Babinski the following:
A veterinary student, held captive in Germany for six months, wrote this to Babinski:
“September 1, 1914, I was about to operate a machine gun when a shrapnel shell exploded very near me,—probably about two or three metres overhead. I base this estimate on comparisons made with shells I saw exploded beside me before this one.
“September 1, 1914, I was about to use a machine gun when a shrapnel shell exploded very close to me—probably about two or three meters overhead. I base this estimate on comparisons with shells I had seen explode beside me before this one.”
“Just after the explosion, which deafened me and at the same time took my breath away a little, from the powder, I felt a rather severe pain in the kidney region,—a pain which then persisted without interruption. I moved my left arm, to find the effect produced by a bullet which I heard whistle by my ear and which struck the upper part of the left shoulder without entering. At the same time, I tried to turn to see what had become of my legs, and had a feeling that they had vanished. Almost immediately I felt little prickings, not very painful, in the lumbar region and in the upper part of the thighs. Just then, seeing my comrades going away I tried to imitate them, but could not. All these feelings passed very rapidly.
“Just after the explosion, which deafened me and slightly took my breath away from the powder, I felt a pretty severe pain in my kidney area—a pain that then continued without stopping. I moved my left arm to check the effect of a bullet I heard whizzing by my ear, which hit the upper part of my left shoulder without going in. At the same time, I tried to turn to see what had happened to my legs and had the sensation that they had disappeared. Almost immediately, I felt little prickling sensations, not very painful, in my lower back and the upper part of my thighs. Just then, seeing my comrades leaving, I tried to follow them, but I couldn't. All these feelings passed by very quickly.”
“A comrade then came near to tell me to go back. I told him that I could not move and that I must have been wounded in the lumbar region. He looked at my kit and my coat and said there was no trace of shot or tear. Not wanting to leave me, he lifted me by the armpits and knees. I could not help him get me up, and my legs hung flexed and inert. After a few steps he had to put me down, and tried to stand me up. I immediately crumpled. I had no sensation of my feet touching the ground. I sent my comrade back, asking him to tell my brother, who was in my squad. I did not lose consciousness or any feeling of my situation, or of the danger being run by my comrade.”
“A comrade then came over to tell me to go back. I told him I couldn’t move and that I must have been injured in the lower back. He looked at my gear and my coat and said there was no sign of a bullet or tear. Not wanting to leave me behind, he lifted me by the armpits and knees. I couldn’t help him get me up, and my legs just hung there, bent and unresponsive. After a few steps, he had to set me down and tried to stand me up. I immediately collapsed. I had no feeling of my feet touching the ground. I sent my comrade back, asking him to tell my brother, who was in my squad. I didn’t lose consciousness or any awareness of my situation, or of the danger my comrade was facing.”
The man remained four days on the battle field without food. He was on the edge of a stream. He did not defecate, nor for two days did he urinate. Eventually the bladder and[287] rectal functions were re-established, though they remained irregular. Catheterization was never resorted to. The lumbar pains were diffuse, fixing themselves a few days after the accident in the region below the umbilicus. There were pains at the waist predominating on the left side. The paralysis of the lower extremities grew rapidly better. Movements in the right leg reappeared, and 27 days after the accident the man was able to stand and walk around his bed. Still further movement followed (left leg weaker).
The man stayed on the battlefield for four days without food. He was near a stream. He didn’t have a bowel movement, and for two days, he didn’t urinate. Eventually, his bladder and rectal functions returned, although they were still irregular. He never needed catheterization. The lower back pain was widespread, settling in the area below the navel a few days after the incident. He felt pain in his waist, mostly on the left side. The paralysis in his legs improved quickly. Movement in his right leg came back, and 27 days after the accident, he was able to stand and walk around his bed. More movement followed, though his left leg was still weaker.
At the time of the report, May 28, 1915, the patient could walk without a cane, but he could get about only slowly. The left toes would rub against the ground, and he could not support himself for any length of time on his legs. The knee-jerks were exaggerated, especially the left. The Achilles jerks were increased. There was a Babinski reflex on the left side and an abduction of the fifth toe on plantar stimulation. The same reflexes were found on the right side, but less marked. Abdominal reflexes absent, except the right superior reflex, which was distinctly present. Cremasteric reflexes absent. Anal reflexes preserved. The defense reflexes were exaggerated, but more markedly on the left side. The zone from which the defense reflexes could be elicited on the left side included the whole lower extremity and rose as far as 2 or 3 cm. above the nipple. Stimulation of the lateral parts of the left lower extremity would even produce defense reflex movements on both sides of the body. On the right side, however, the defense reflex movements could only be tried out by scratching the anterior surface of the ankle, which was then followed by a flexion of the foot.
At the time of the report on May 28, 1915, the patient was able to walk without a cane, but he did so very slowly. His left toes dragged on the ground, and he couldn't stand on his legs for long periods. The knee reflexes were heightened, especially on the left side. The Achilles reflexes were also increased. There was a Babinski reflex on the left and an abduction of the fifth toe when the plantar was stimulated. These same reflexes were present on the right side but were less pronounced. Abdominal reflexes were absent, except for the right superior reflex, which was clearly present. Cremasteric reflexes were absent, while anal reflexes were intact. Defense reflexes were exaggerated, more so on the left side. The area from which the defense reflexes could be triggered on the left encompassed the entire lower limb and extended as much as 2 or 3 cm above the nipple. Stimulation of the lateral parts of the left lower limb would even cause defense reflex movements on both sides of the body. On the right side, however, the defense reflex movements were only provoked by scratching the front of the ankle, leading to a flexion of the foot.
Sensibility to touch and deep sensibility were preserved; but sensibility to temperature and pain, normal on the left,—i.e., paralyzed—side, was weak in the right leg. There was a marked sudation on the left side, limited by the white line, the inguinal fold, the iliac spines, and a horizontal line passing through the umbilicus.
Sensitivity to touch and deep sensitivity were maintained; however, sensitivity to temperature and pain, which was normal on the left—meaning the paralyzed side—was weak in the right leg. There was noticeable sweating on the left side, confined by the white line, the groin fold, the iliac spines, and a horizontal line running through the navel.
Here, then, paralysis followed a shell explosion while the subject was lying down. No contusion therefore was possible. According to Babinski, we are dealing probably with a hematomyelia, the result of shell explosion.
Here, paralysis occurred after a shell explosion while the subject was lying down. So, no bruising was possible. According to Babinski, we are likely dealing with a hematomyelia, caused by the shell explosion.
Struck by missile in back; unconsciousness; no wound: Hysterical paraplegia? HERPES and SEGMENTARY Hyperalgesia suggest radicular and spinal injury. Recovery.
Struck by a missile in the back; unconscious; no wound: Hysterical paraplegia? Herpes and segmental hyperalgesia suggest radicular and spinal injury. Recovery.
Case 210. (Elliot, December, 1914.)
November 1, 1914, a sergeant in the 20th Hussars, with other dismounted cavalrymen, was chasing Germans with a bayonet, over turnip fields pitted by shells. Several hours later, he found himself in a house in a nearby village, to which he had been carried unconscious. Probably he had been struck by some missile in the back, as the bottom of his haversack had been torn off. His face was blackened with smoke, and his clothes were muddy. He had no wound. His left arm was weak and his legs powerless and numb. The passing of water was painful, but there was no blood in the water and no hemoptysis.
November 1, 1914, a sergeant in the 20th Hussars, along with other dismounted cavalrymen, was pursuing Germans with a bayonet over turnip fields scarred by shells. Several hours later, he found himself in a house in a nearby village, where he had been taken while unconscious. He probably got hit by some kind of missile in the back, as the bottom of his haversack had been ripped off. His face was covered in smoke and his clothes were dirty. He had no visible wounds. His left arm felt weak, and his legs were powerless and numb. Urinating was painful, but there was no blood in the urine and no coughing up blood.
Five days later, he was examined at a base hospital and found to be paralyzed and numb in the legs. The knee-jerk and ankle-jerk were retained upon the right side only. Pain occurred on passive movements of the legs, which were flaccid; there was a hyperalgesia about Poupart’s ligament, more marked on the left side. Lower abdominal reflexes were weak on the left side; pain in lower abdomen with bladder full and at outset of micturition. Pain and paresis also affected the left arm, but there was no numbness. Pain on pressure over lumbar and cervical vertebral spines. There was no evidence of bruising.
Five days later, he was checked at a base hospital and found to be paralyzed and numb in his legs. The knee-jerk and ankle-jerk reflexes were present only on the right side. He experienced pain with passive movements of his legs, which were floppy; there was increased sensitivity around Poupart’s ligament, especially on the left side. Lower abdominal reflexes were weak on the left side; he felt pain in his lower abdomen when his bladder was full and at the beginning of urination. Pain and weakness also affected his left arm, but there was no numbness. He felt pain when pressure was applied to the lumbar and cervical vertebral spines. There was no sign of bruising.
The physicians were inclined to regard the phenomena as hysterical. Three days later, the arm movements became much freer, and after another three days, the arm movements were fairly powerful, and the legs much stronger, although the patient could not yet stand or walk. He still had pain if his bladder was full.
The doctors tended to think the symptoms were just hysterical. Three days later, the arm movements got a lot more fluid, and after another three days, the arm movements were quite strong, and the legs were much stronger too, although the patient still couldn’t stand or walk. He still felt pain when his bladder was full.
Chart 9
CAUSES OF SHELL-SHOCK
- HEAD INJURY
- ATMOSPHERIC CONCUSSION
- MENTAL STRAIN
- NON-NERVOUS TRAUMA
- NEUROPATHIC HEREDITY
After Ballard
Post-Ballard
As against the diagnosis of hysteria, three herpetic clusters appeared on the skin of the left thigh, from three to six inches above the knee. Elliot regards it as certain that the posterior root ganglia were injured. He regards the case as one of injury to the spinal nerve roots. The hyperalgesia about the body of course suggested damage to the spinal cord. According to Elliot, therefore, this case is one of organic disease; whether of the roots or of the cord was uncertain. At any rate the cases of this type, though not functional, recovered.
As opposed to the diagnosis of hysteria, three clusters of herpes appeared on the skin of the left thigh, about three to six inches above the knee. Elliot is confident that the posterior root ganglia were damaged. He believes the case involves an injury to the spinal nerve roots. The increased sensitivity around the body, of course, indicated possible damage to the spinal cord. According to Elliot, this case is one of organic disease; it’s unclear whether it affects the roots or the cord. Regardless, cases like this, although not functional, did recover.
Mine-explosion; burial; labyrinthine lesions and head bruises, more marked on left side: Focal canities (WHITE HAIR developing OVERNIGHT) on left side.
Mine explosion; burial; complex injuries and head bruises, more noticeable on the left side: Localized white hair (WHITE HAIR appearing OVERNIGHT) on the left side.
Case 211. (Lebar, June, 1915.)
A soldier, 23, in the Argonne was blown up by a mine in a trench, fell, and was covered by a mass of earth, from which he extricated himself. He immediately became deaf from what was medically determined to be a double hemorrhagic labyrinthitis. There were also superficial powder burns of the face, as well as several bruises on the head, especially on the left side.
A 23-year-old soldier in the Argonne was blown up by a mine in a trench, fell, and was buried under a pile of dirt, from which he managed to free himself. He instantly became deaf due to what doctors identified as double hemorrhagic labyrinthitis. He also had some superficial powder burns on his face, along with several bruises on his head, particularly on the left side.
The next day, at the English hospital at Arc-en-Barrois, the patient noticed tufts of white hair on the left side of the head. There were four islets of gray hair in the left fronto-parieto-occipital region, separated from one another by normal hairs. The gray hairs were gray completely from the roots to the ends of the hair. The longest hairs were as white as the shortest. There was not a brown hair amongst them. The gray hairs were solidly implanted, and could be pulled out only by strong traction. There was a discoloration also of the bulbar swelling of the hair. The rest of the head hair was dark brown. His hair was described in the military description: “deep chestnut brown.” There was no other symptom aside from an incessant twitching of the left eyelids. The place of whitening was apparently determined by the region of the scalp injured. Not only were the bruises on the left side of the head and face, but the labyrinthine lesions were more marked on this side and the twitching of the eye-lids was confined to the left side.
The next day, at the English hospital in Arc-en-Barrois, the patient noticed clumps of white hair on the left side of his head. There were four patches of gray hair in the left fronto-parieto-occipital area, each separated by normal hair. The gray hairs were completely gray from the roots to the tips. The longest hairs were as white as the shortest. There wasn't a single brown hair among them. The gray hairs were firmly rooted and could only be pulled out with significant force. There was also a discoloration in the bulbar swelling of the hair. The rest of his head hair was dark brown. His hair was described in the military records as “deep chestnut brown.” There were no other symptoms aside from constant twitching of the left eyelids. The areas of whitening seemed to be linked to the region of the scalp that was injured. Not only were there bruises on the left side of the head and face, but the labyrinthine damage was more pronounced on this side, and the eyelid twitching was limited to the left side.
Shrapnel wound of skull; focal canities over wound; shell-shock and shrapnel wound of right leg. Head tremors and contractions, changing in relation to posture; glove anesthesia and local anesthesia of trunk.
Shrapnel injury to the skull; localized gray hair over the wound; shell shock and shrapnel injury to the right leg. Head tremors and muscle spasms, varying with posture; glove anesthesia and localized numbness of the torso.
Case 212. (Arinstein, September, 1915.)
A Russian private, 24, was wounded twice: once in the head by a bullet, and at another time by a bit of shrapnel that imbedded itself in the skull. The hair over the injured spot became gray.
A 24-year-old Russian soldier was wounded twice: first in the head by a bullet, and later by a piece of shrapnel that got embedded in his skull. The hair over the injured area turned gray.
Later, September 16, 1915, the soldier was subjected to shell-shock, and at the same time wounded by shrapnel fragment in the right leg (operated next day).
Later, on September 16, 1915, the soldier experienced shell shock and was also injured by a shrapnel fragment in his right leg (surgery the next day).
Upon examination at Petrograd, the hearing was found diminished and the eardrum was pulled in. At first the patient could not speak or open his eyes, and made incessant lateral movements of the head, jerking backwards and to the right. The right half of the face gave convulsive movements, which began at the lip and spread upwards. During sleep, there was an entire cessation of these head shakings and jerks. In the lying posture, the head shook at a rate of 100 to 120 per minute. The jerking movements became more marked when the patient sat up or walked. He carried his head bent toward the right shoulder. When he sat down, the side-shaking movements disappeared, only to reappear when he lay down. The swallowing reflexes were absent. The sensitiveness to touch, pain, and temperature was lost in the upper part of the trunk including the neck, to the level of the tenth dorsal vertebra. There was anesthesia of the arms as far as the elbow on the right, and as far as the shoulder on the left. The mucosae of the mouth were anesthetic. Dermatographia was strongly marked.
Upon examination in Petrograd, the hearing was found to be reduced and the eardrum was retracted. At first, the patient couldn’t speak or open his eyes and was making constant side-to-side movements of his head, jerking backward and to the right. The right side of his face was convulsing, starting from the lip and moving upwards. While he was asleep, all of these head movements and jerks completely stopped. When lying down, his head shook at a rate of 100 to 120 times per minute. The jerking movements became more pronounced when the patient sat up or walked. He tilted his head toward his right shoulder. When he sat down, the side-to-side movements disappeared, only to come back when he lay down again. The swallowing reflexes were absent. Sensitivity to touch, pain, and temperature was lost in the upper part of the trunk, including the neck, down to the level of the tenth dorsal vertebra. There was a loss of sensation in the arms up to the elbow on the right and up to the shoulder on the left. The mucous membranes of the mouth were numb. Dermatographia was very pronounced.
Shell explosion; burial: Hemiplegia, probably organic.
Shell explosion; burial: Hemiplegia, likely organic.
Case 213. (Marie and Tax, January, 1917.)
A soldier was blown up by a shell and then buried at Vaux, March 29, 1916, and entered the Salpêtrière, July, 1916, with a right-sided hemiplegia and contracture without evidence of wound. He remembered nothing for the first fortnight after the trauma. When he came to himself, he was paralyzed and was unable to say more than a few words, but at the end of a month his aphasia ceased and he began to walk.
A soldier was blown up by a shell and then buried at Vaux on March 29, 1916. He entered the Salpêtrière in July 1916 with paralysis on his right side and contracture, but no visible injuries. He had no memories of the first two weeks after the trauma. When he regained consciousness, he was paralyzed and could only say a few words. However, after a month, his speech difficulties improved, and he began to walk again.
The hemiplegia was spastic. There was pronounced contracture. The arm was extended, hand open, fingers stretched. Finger movements were diminished, as well as extension of the wrist, but the arm was otherwise normal. The leg was not so stiff. The great toe was in a state of continuous extension. The toes could not be moved, and the foot scarcely; but the leg could be strongly flexed and extended on the thigh. The tendon reflexes of the right side were more lively than on the left. Cloniform movements followed tapping the patellar tendon on the right side, and a patellar clonus and ankle clonus could also be demonstrated. Plantar reflex, flexor on the right. Distinct adduction of the foot. Slight disturbance of tactile sensibility in the paralyzed limbs; marked disorder of position sense and gross disturbance of stereognostic sense. Moderate dysarthria.
The hemiplegia was spastic. There was significant contracture. The arm was extended, the hand was open, and the fingers were stretched. Finger movements were reduced, as well as wrist extension, but the arm was otherwise normal. The leg wasn’t as stiff. The big toe was constantly extended. The toes couldn't be moved, and the foot barely could; however, the leg could be flexed and extended strongly at the thigh. The tendon reflexes on the right side were more active than on the left. Clonus movements followed tapping the patellar tendon on the right side, and patellar clonus and ankle clonus were also present. The plantar reflex was flexor on the right. There was clear adduction of the foot. There was a slight disturbance in tactile sensation in the paralyzed limbs, marked disorientation in position sense, and significant issues with stereognostic sense. Moderate dysarthria.
Ten months after the traumatism, the hemiplegia and spastic walk remained. The upper limb was now carried in extension back of the body, with hand supinated, fingers sometimes in extension, sometimes in flexion, index finger separately from the others. Finger movements difficult and shoulder movements limited. The leg, however, was almost normal except that the toes could not be moved. The tendon reflexes were more lively and cloniform on the right, but there was no longer patellar or ankle clonus. Stereognosis slow, but finger movements were naturally difficult. W. R. of blood, negative. Probably this is an organic case.
Ten months after the injury, the paralysis and stiff walking were still present. The affected arm was now held extended behind the body, with the hand facing up, fingers sometimes extended and sometimes bent, with the index finger moving separately from the others. Finger movements were difficult and shoulder movements were limited. However, the leg was almost normal except that the toes could not be moved. The tendon reflexes were more active and had a clonic response on the right side, but there was no longer any patellar or ankle clonus. Stereognosis was slow, and finger movements were naturally challenging. Blood work was negative. This is likely an organic case.
Blown up by a shell; no skin or bone lesion: Mixture of organic (e.g., lost knee-jerks) and functional (e.g., urinary retention) disorders.
Blown up by a shell; no skin or bone injury: Mix of organic (e.g., lost knee-jerk reflexes) and functional (e.g., urinary retention) issues.
Case 214. (Claude and Lhermitte, October, 1915.)
A man, 38, was blown up in a trench without sustaining skin or skeletal lesions, April 5, 1915. He lost consciousness for a half hour and, coming to, found a crural paraplegia and urinary retention. Examined July 24, in addition to the paraplegia were found tactile and algesic hypesthesia of the legs with preservation of deep sensibility. Pains were felt in the legs, especially in the hips. The knee-jerks were abolished; the Achilles jerks were preserved, as well as the flexor plantar reflexes and somewhat weakened cremasteric and abdominal reflexes. Micturition was difficult. Constipation. Slight paresis of left arm. Lumbar puncture, July 28, yielded a clear fluid of normal tension without chemical or cytological changes.
A 38-year-old man was injured in a trench explosion on April 5, 1915, but did not have any skin or bone injuries. He lost consciousness for about half an hour. When he came to, he had paralysis in his legs and difficulty urinating. An exam on July 24 revealed that, in addition to the leg paralysis, he had reduced sensitivity to touch and pain in his legs, but deep sensation was intact. He experienced pain in his legs, especially in the hips. His knee reflexes were absent, but Achilles reflexes were normal, as were the flexor plantar reflexes, although the cremasteric reflex and abdominal reflexes were slightly diminished. He also had trouble urinating and was constipated. There was slight weakness in his left arm. A lumbar puncture on July 28 showed clear fluid at normal pressure with no chemical or cellular abnormalities.
The sphincter disorders gradually disappeared. The knee-jerks reappeared in a weakened form August 31. The legs could, at the time of report, be moved somewhat, though not above the level of the bed.
The sphincter issues gradually went away. The knee-jerk reflexes returned in a weakened form on August 31. At the time of the report, the legs could be moved a bit, but not above the level of the bed.
We here deal, presumably, with a mild form of concussion of the spinal cord, in which, however, some of the transient symptoms are very possibly merely functional in origin.
We are likely dealing with a mild concussion of the spinal cord, where some of the temporary symptoms are probably just functional in nature.
Re complicated pictures of organic and functional nature, some experimental work has been carried out. Mairet and Durante set off explosives, such as melinite, at a distance of 1 to 1.5 metres, near rabbits. Some died at intervals from an hour to thirteen days; others lived. Pulmonary apoplexy was found in the cases dying early. Spinal cord and root hemorrhages, hemorrhages in the cortical and bulbar gray, perivascular and ependymal hemorrhages were found, always small and without diffusion, suggesting rupture by rapid decompression following the first wave of aerial compression. The functional effects are thought to be brought about through the anemia of the areas supplied by the ruptured[295] vessels. Russca of Berne got similar results and notes direct and contrecoup brain lesions, tympanic perforations, intra- and extra-ocular hemorrhages, thoracic, cardiac, and splenic hemorrhages, ruptures of kidney, stomach, intestine, and diaphragm. As in the work of Mairet and Durante, the lung proved the most sensitive organ. (Compare also the human case of Sencert [Case 201].) Some experiments with fishes yielded lesions of the swimming bladder. Persalite and other explosives were used.
Re complicated images of organic and functional nature, some experimental work has been conducted. Mairet and Durante detonated explosives, like melinite, at a distance of 1 to 1.5 meters from rabbits. Some died within a timeframe of one hour to thirteen days; others survived. Pulmonary apoplexy was observed in the cases that died early. Hemorrhages in the spinal cord and roots, in the gray matter of the brain, perivascular and ependymal hemorrhages were found, always small and without diffusion, suggesting rupture due to rapid decompression after the initial wave of aerial compression. The functional effects are believed to result from the anemia of the areas supplied by the ruptured[295] vessels. Russca of Berne observed similar results and noted both direct and contrecoup brain injuries, tympanic perforations, intra- and extra-ocular hemorrhages, as well as thoracic, cardiac, and splenic hemorrhages, and ruptures of the kidney, stomach, intestine, and diaphragm. As with the work of Mairet and Durante, the lungs proved to be the most sensitive organ. (See also the human case of Sencert [Case 201].) Some experiments with fish resulted in lesions of the swim bladder. Persalite and other explosives were utilized.
GASSING: Organic-looking picture.
GASSING: Looking like an organic picture.
Case 215. (Needing, May, 1917.)
A German soldier, 21, was a serious case of gassing. He was unconscious two days (venesection twice). When he came to, he could not walk and felt as if he were drunk. October 22, 1916, he was incoördinate in walking and tended to fall forward when standing with eyes closed. The ataxia of the legs was demonstrable in the position of dorsal decubitus, and there was also a slight ataxia of the arms. The pupils were dilated and reacted poorly to light.
A 21-year-old German soldier experienced a severe case of gas exposure. He was unconscious for two days (undergoing two bloodlettings). When he regained consciousness, he was unable to walk and felt drunk. On October 22, 1916, he showed uncoordinated walking and tended to fall forward when standing with his eyes closed. The lack of coordination in his legs was noticeable while lying on his back, and there was also a slight lack of coordination in his arms. His pupils were dilated and reacted poorly to light.
December 12, all symptoms had disappeared. The clinical picture in this case was somewhat like that of a multiple sclerosis. According to Neiding, the disorder is not a functional one but an organic cerebellar disorder.
December 12, all symptoms had disappeared. The clinical picture in this case was somewhat like that of multiple sclerosis. According to Neiding, the disorder is not a functional one but an organic cerebellar disorder.
Re the neurology of gas poisoning, Neiding regards the condition as a new nosological unit. We do not know what the ultimate results of apparently cured cases will be. Court questions of importance will doubtless arise with reference to their compensation. Ninety-six of Neiding’s 274 cases failed to show any nerve symptoms whatever; forty-six cases showed one symptom only, such as headache, dizziness, abnormality of reflexes, or abnormality in sensation. One hundred and thirty-two cases presented a fairly full picture. The picture of a complete traumatic neurosis not infrequently appears, aided perhaps by the psychic features of the gas attacks; and possibly some cases are entirely psychogenic from the beginning. Such symptoms, for example, as dermatographia, rapid and irregular heart, hyperidrosis, blepharospasm, mental perturbation, hypochondria, etc., do not necessarily point to any directly toxic effect of the gases. Thirty-seven of Neiding’s cases showed pupillary changes, hyperreflexia, and analgesia. Thirty-one showed analgesia and absence of laryngeal and corneal reflexes. Twenty-six showed pupillary changes and hyperreflexia, four of these latter showing also an absence of laryngeal and corneal reflexes. One case yielded hyperalgesia alone; ten yielded headache, dizziness, and analgesia.
Re the neurology of gas poisoning, Neiding sees this condition as a new medical category. We don’t know what the long-term effects of cases that seem to be cured will be. Important legal questions will likely come up regarding their compensation. Out of Neiding’s 274 cases, ninety-six showed no nerve symptoms at all; forty-six cases showed just one symptom, like headache, dizziness, unusual reflexes, or abnormal sensations. One hundred and thirty-two cases displayed a fairly complete picture. A full-blown traumatic neurosis often appears, possibly influenced by the psychological aspects of the gas attacks; and some cases might be entirely psychogenic from the start. Symptoms such as dermatographia, rapid and irregular heartbeat, excessive sweating, eyelid spasms, mental disturbances, hypochondria, etc., don’t necessarily indicate any direct toxic effect from the gases. Thirty-seven of Neiding’s cases had changes in pupils, increased reflexes, and loss of pain sensation. Thirty-one showed loss of pain sensation and absence of laryngeal and corneal reflexes. Twenty-six had changes in pupils and increased reflexes, four of whom also had absent laryngeal and corneal reflexes. One case showed only increased sensitivity to pain; ten cases showed headache, dizziness, and loss of pain sensation.
GASSING: Mutism, tremors, depression, battle dreams.
GASSING: Silence, shaking, sadness, war dreams.
Case 216. (Wiltshire, June, 1916.)
An infantryman, aged 27, had been at the front for three months. He was wounded a month before coming to hospital; but when the wound healed he went back to the front, quite mute but intelligent and able to write the following:
An infantryman, 27 years old, had been at the front for three months. He got injured a month before arriving at the hospital; but when the wound healed, he returned to the front, completely silent yet smart and able to write the following:
“We were on our way to the trenches, and as we were going through the railway cutting they started to shell us, with gas shells mostly, and we had not been there more than quarter of an hour when I was compelled to lie down from temporary blindness and weakness through getting a dose of gas through my mouth and eyes. I was lying down for about ten minutes when a shell came somewhere near, and was struck by something in the face and on my left knee and I remembered no more until I found myself in hospital. I was all of a shake and while lying down would frequently jump up and wonder where I was.”
“We were heading to the trenches, and as we passed through the railway cutting, they started shelling us, mostly with gas shells. We hadn’t been there more than a quarter of an hour when I had to lie down due to temporary blindness and weakness from inhaling gas through my mouth and eyes. I lay there for about ten minutes when a shell landed nearby, and I felt something hit my face and my left knee, and I don’t remember anything else until I woke up in the hospital. I was shaking, and while lying down, I would often jump up and wonder where I was.”
The patient had been mute thereafter, depressed, and given to dreams about fighting and shells. There was a fine tremor controllable by the will; the knee-jerks were increased. On lateral deviation, there was difficulty in fixing the eyes. There was a slight deafness due to an old discharging left ear. According to Wiltshire, Shell-shock is only exceptionally caused by chemical poisoning from gas.
The patient had been silent since then, depressed, and experiencing dreams about fighting and explosions. There was a noticeable tremor that could be controlled by willpower; the knee reflexes were heightened. When looking to the side, there was trouble focusing the eyes. There was also slight hearing loss due to an old issue with the left ear that had been discharging. According to Wiltshire, shell shock is only rarely caused by chemical poisoning from gas.
Re poisoning by certain German asphyxiating gases, Sereysky reports in 1917 that these gases contained, among other poisons, a nerve poison. He found that poor heredity was a favorable soil for the action of this nerve poison. The clinical pictures in the gassed soldiers rather suggested cerebral arteriosclerosis. He remarks that the logical distance between the “exogenous” and “endogenous” is greatly reduced in these gassed cases, as the syndrome of “exogenous” gassing closely approximates that of various “endogenous” disorders.
Re poisoning by certain German asphyxiating gases, Sereysky reports in 1917 that these gases contained, among other toxins, a nerve poison. He found that poor genetics provided a conducive environment for the effects of this nerve poison. The clinical symptoms in the gassed soldiers resembled cerebral arteriosclerosis. He notes that the clear boundary between “exogenous” and “endogenous” conditions is significantly blurred in these gassed cases, as the symptoms of “exogenous” gassing closely resemble those of various “endogenous” disorders.
Hysterical speech disorder related to mechanical disorder of auditory apparatus.
Hysterical speech disorder associated with mechanical issues of the hearing system.
Case 217. (Binswanger, July, 1915.)
Whenever a German officer’s servant, 23 years, was addressed on the ward in the Jena Nerve Hospital, his hands would tremble and the muscles of his face would fall into grimacing associated movements. He had a peculiar infantile type of speech, talking with a fixed glance and an anxious mien. He would carefully utter, as a rule, separate words, chiefly only nouns or infinitives. He would gesticulate with both hands to make what he said understood. Thus (freely translating the German) runs his description of a battle:
Whenever a German officer’s servant, 23 years old, was spoken to in the ward of the Jena Nerve Hospital, his hands would shake and the muscles in his face would contort into grimacing movements. He had a strange, childlike way of speaking, communicating with a fixed stare and a worried expression. Usually, he carefully articulated individual words, mainly just nouns or infinitives. He would gesture with both hands to clarify what he meant. So, his account of a battle goes like this:
“Well—because—I—we had—no artillery and so many losses—then got in position again, then we—laid down a long time—perhaps until four o’clock in the afternoon—five—and—and it happened that—lay in Rübenfeld—couldn’t go back—then shell near me—fell in and I right near, how—how far—I don’t know and—grown better. Comrade said—10 meters—don’t know—un—unconscious.”
“Well—because—I—we had—no artillery and so many losses—then we got into position again, then we laid down for a long time—maybe until four o’clock in the afternoon—five—and it happened that we were lying in Rübenfeld—I couldn’t go back—then a shell fell near me—I was right by it, how far—I don’t know—and it got better. A comrade said—10 meters—I don’t know—un—unconscious.”
Long compound German words could not be repeated, since after the first or second syllable there was a severe emotional excitement; syllable articulation and phonation ceased. Finally, however, the patient could be gotten to pronounce the whole word. Reading aloud was very difficult: syllable sounding and omission of difficult syllables; after a time, weeping.
Long compound German words could not be repeated, since after the first or second syllable, there was intense emotional excitement; syllable articulation and phonation stopped. However, the patient could eventually be prompted to say the entire word. Reading aloud was very challenging: struggling with syllable sounds and skipping over difficult syllables; after a while, it ended in tears.
The patient was a somewhat small, muscular, well-nourished man, with a murmur at the apex, a somewhat rapid pulse, increased reflexes, especially skin reflexes, painful supra- and infra-orbital points, temples painful to percussion, pressure over spine painful from second thoracic to third lumbar vertebrae. There was an increased sensitiveness to touch and pain over the whole body. There was a bilateral, somewhat marked tremor, more marked on the left side than on the right. Swaying in Romberg position was slight. Tremor of tongue.
The patient was a slightly small, muscular, well-nourished man, with a heart murmur at the apex, a somewhat rapid pulse, heightened reflexes, especially in the skin, painful spots above and below the eyes, and temples that hurt when tapped. Pressure on the spine was painful from the second thoracic to the third lumbar vertebrae. He showed increased sensitivity to touch and pain all over his body. There was a noticeable tremor on both sides, more prominent on the left than the right. Swaying in the Romberg test was slight. There was also a tremor in his tongue.
This patient was first brought to Jena November 23, 1914. An illegitimate child, a moderately good scholar, he had worked as a mason until he went into the army, in 1912. He worked as a soldier chiefly in the officers’ casino because he got pains in his legs and knees in long drills. At the outset of the campaign, however, he withstood the heavy marching, although with difficulty. He was in his first actual skirmish September 20. A shell struck nearby and threw him several meters; whereupon he became unconscious and was carried away by the hospital corps. When he woke up he could not speak or hear. Ten days later, however, speech returned, and hearing returned in right ear; October, deaf in the left ear, and he could not hear a watch tick on the right side at a distance of 16 centimeters. He was examined at the otological clinic in Jena October 12, where the drum membranes were both found opaque, without reflexes or normal contours; hysterical attack on the caloric test. The next day, on the medical visit, there was a screaming attack. His plight seemed not so much simulation as one of traumatic hysteria.
This patient was first brought to Jena on November 23, 1914. An illegitimate child and a decent student, he had worked as a mason until he joined the army in 1912. While serving, he primarily worked in the officers’ casino because he suffered from leg and knee pain during long drills. At the beginning of the campaign, he managed the heavy marching, although it was tough for him. He experienced his first actual skirmish on September 20. A shell exploded nearby, throwing him several meters; he lost consciousness and was taken away by the hospital corps. When he woke up, he couldn't speak or hear. However, ten days later, his speech returned, and he regained hearing in his right ear; in October, he was deaf in his left ear and couldn't hear a watch ticking from 16 centimeters away on the right side. He was examined at the otological clinic in Jena on October 12, where both eardrums were found to be opaque, lacking reflexes or normal shapes; a hysterical episode occurred during the caloric test. The following day, during a medical visit, he had a screaming episode. His condition seemed more like traumatic hysteria than simple simulation.
Again, after his stay at the nerve hospital, another hysterical outburst was produced by a hearing test with vestibular apparatus, in the ear clinic, February 6, 1915. The diagnosis was nervous deafness with involvement of left ear.
Again, after his time at the mental health hospital, another emotional outburst was triggered by a hearing test using vestibular equipment at the ear clinic on February 6, 1915. The diagnosis was nervous deafness affecting the left ear.
The insomnia was successfully treated by sodium bicarbonate. There was a slight improvement in speech. In March body weight had improved, but there was a marked tremor of the right hand. In the next few months there was a progressive improvement in general well-being, in speech disorder, and in tremor. The auditory disorder remained unchanged. The man now works in his father’s garden.
The insomnia was effectively treated with sodium bicarbonate. There was a slight improvement in his speech. By March, his body weight had increased, but there was a noticeable tremor in his right hand. Over the next few months, there was a consistent improvement in his overall well-being, speech issues, and tremor. However, the hearing problem stayed the same. The man now works in his father's garden.
This case appears to show a combination of psychic and mechanical injury. There are severe hysterical auditory and speech disorders. Although the auditory disorder is of mechanical origin, the speech disorder appears to be of psychogenic nature. It is somewhat remarkable that the ear tests almost every time produce hysterical attacks in the form of convulsive crying. Rather unusual is the general cutaneous hyperalgesia, more marked about the ears.
This case seems to reflect a mix of psychological and physical injury. There are serious hysterical issues with hearing and speech. While the hearing problem is due to a physical cause, the speech issue seems to come from psychological factors. It's quite striking that hearing tests often trigger hysterical episodes, manifesting as intense crying. What’s also unusual is the overall heightened sensitivity to pain, especially around the ears.
Shell-shock (distant, neither seen nor heard); left tympanum ruptured; semicoma eight days: Cerebellar syndrome and hemianesthesia. Recovery, nine months.
Shell shock (distant, neither seen nor heard); left eardrum ruptured; semicoma for eight days: Cerebellar syndrome and partial loss of sensation. Recovery took nine months.
Case 218. (Pitres and Marchand, November, 1916.)
A lieutenant underwent “shell-shock” either at night or in the early morning, September, 1915, the shell bursting at a distance. He neither saw nor heard the shell, lost consciousness and was eight days semicomatose, failing to recognize his wife.
A lieutenant experienced “shell-shock” either at night or early in the morning of September 1915, with the shell exploding nearby. He neither saw nor heard the shell, lost consciousness, and was in a semi-comatose state for eight days, failing to recognize his wife.
On recovering his senses, he could not get about, as he had lost his memory, having to write down his room number and be warned of meal times. He was led about like a child. He had a continuous headache on the right side and pains in the occiput and along the spinal column, as well as in the right leg as far as the heel. These leg pains were lightning pains. Walking was difficult, staggering, leaning to left. Weakness of right arm and leg; right-sided hemianalgesia. Complete insomnia. During November there were frequent urgent desires to urinate day or night. Evacuated to the oto-rhino-laryngological center in Bordeaux, December 13, for examination of ears. The right ear was found normal, but there was a rupture of the left tympanum. There was at this time a trismus. The jaws were opened with the dilator and the man had a syncope during this operation. The question of surgical intervention for a cerebral lesion was raised, but he was first sent to the neurologists at Bordeaux. There, December 31, he was found with a facies of anguish, unstable gait, inclination to the left in walking; no Rombergism; occasional dizzy spells. In walking, the right foot was pointed outward and on request to direct it forward he complained of pain in the loins, reaching as far as the scapula. Walking with eyes closed, he leaned to the left and lost balance. With eyes open, no disorder of balance. With eyes closed, the body leaned backward. If requested to go back, he failed to flex his legs to keep balance. If he was asked to[301] put a foot upon the chair in front of him, he immediately fell backwards. He could not support his body on the right leg more than a few moments. He had difficulty in raising both legs from the bed at one time and he could lift the right leg not so high as the left. Movements of the legs were performed hesitatingly and slowly and with greater difficulty with eyes closed.
Once he regained consciousness, he struggled to get around because he had lost his memory, needing to write down his room number and be reminded of meal times. He was led around like a child. He experienced a constant headache on the right side, along with pain in the back of his head, down his spine, and in his right leg all the way to his heel. The pain in his leg felt like lightning. Walking was tough; he staggered and leaned to the left. His right arm and leg felt weak, and he had right-sided numbness. He couldn't sleep at all. Throughout November, he often felt a strong urge to urinate, day or night. He was sent to an ear, nose, and throat center in Bordeaux on December 13 for an ear examination. His right ear was normal, but his left eardrum was ruptured. At that time, he also had difficulty opening his jaw. They used a dilator to pry his jaws open, and he fainted during the procedure. There was a discussion about possible surgery for a brain injury, but first, he was referred to neurologists in Bordeaux. There, on December 31, he appeared anxious, walked unsteadily, and leaned to the left while walking; he did not have Romberg’s sign and experienced occasional dizziness. When walking, his right foot pointed outward, and when asked to straighten it, he complained of pain in his lower back that reached his shoulder blade. With his eyes closed, he leaned to the left and lost his balance. With his eyes open, he showed no balance issues. With his eyes closed, he leaned backward. When asked to walk backward, he struggled to bend his knees to maintain balance. If asked to place a foot on the chair in front of him, he immediately fell backward. He could only support his weight on his right leg for a few moments. He had trouble raising both legs from the bed at the same time, and he couldn't lift his right leg as high as his left. His leg movements were hesitant, slow, and more difficult when his eyes were closed.
He could not thread a needle and could hardly dress himself. Eyes closed, he could with difficulty perform the finger to nose test; eyes open, with much less difficulty. Adiadochokinesis; muscular strength less in right than left; plantar reflexes absent; knee-jerks lively; hemianalgesia, right side. Loss of deep and bony sensibility on right side and diminution of testicular sensibility. Retraction of visual field, right; diminution of smell and loss of hearing, right; position sense absent on this side; stereognostic sense preserved. Mentally, memory was poor; he was unable to read or do mental work. He slept little and had bad battle dreams. He was very impressionable and emotional and constantly complained of occipital pain. He had lost 8 kilos weight.
He couldn't thread a needle and had trouble dressing himself. With his eyes closed, he struggled to do the finger-to-nose test; with his eyes open, it was much easier. He showed signs of adiadochokinesis; his muscle strength was weaker on the right side than the left; there were no plantar reflexes; knee-jerks were active; he had reduced sensitivity to pain on the right side. He lost deep and bony sensibility on the right side and had decreased sensitivity in the testicles. His visual field was retracted on the right; he had reduced smell and lost hearing on that side; he had no sense of position on the right; however, his stereognostic sense was intact. Mentally, his memory was poor; he couldn't read or do any mental tasks. He slept very little and had troubling dreams about battles. He was very sensitive and emotional and constantly complained of pain in the back of his head. He had lost 8 kilograms.
He grew gradually better. In May he could go out alone. The muscular strength increased. The adiadochokinesis and synergic disturbances lessened; the hemianesthesia persisted. In June there was greater improvement; in fact, there was no sign of disorder left except irregular sleep.
He gradually got better. By May, he could go outside by himself. His muscle strength improved. The issues with rapid alternating movements and coordination decreased; however, the numbness on one side remained. In June, he showed more improvement; in fact, the only remaining issue was irregular sleep.
We here deal with a cerebellar syndrome plus a hemianesthesia.
We are dealing with a cerebellar syndrome along with hemianesthesia.
Mine explosion: Tremors, mutism, hemiplegia. Tremors cleared by hypnosis. Mutism replaced by stuttering. Persistent hemiplegia, probably organic.
Mine explosion: Tremors, inability to speak, paralysis on one side. Tremors resolved through hypnosis. Inability to speak turned into stuttering. Ongoing paralysis, likely caused by a physical issue.
Case 219. (Smyly, April, 1917.)
A soldier was blown up by a mine and rendered unconscious. Upon recovery of consciousness, the patient was dumb, unable to work, very nervous, paralyzed as to left arm and leg. The paralysis improved so that in the hospital at home the patient became able to get about. However, he threw his legs about in an unusual fashion. Several months later the patient was much improved.
A soldier was blown up by a mine and lost consciousness. When he regained consciousness, he was mute, unable to move, extremely anxious, and had paralysis in his left arm and leg. His paralysis improved, so once he was back at the hospital, he could get around. However, he moved his legs in a strange way. Several months later, he had made significant progress.
Shortly, there was a relapse. Transferred to a hospital for chronic cases, the patient was unable to walk without assistance on account of complete paralysis of the leg. There was insomnia, a general tremor, bad stuttering, and a habit of starting in terror at the slightest noise.
Shortly after, there was a setback. The patient was moved to a hospital for long-term cases and couldn't walk without help due to total paralysis of the leg. They experienced insomnia, a general tremor, severe stuttering, and would jump in fear at the slightest sound.
Hypnotic treatment was followed by almost complete disappearance of the tremor. The patient began to sleep six or seven hours a night; nervousness diminished, and the stuttering slowly improved; but neither the paralysis nor the anesthesia of the left leg was affected by suggestion. The leg remained cold, livid, anesthetic, and flaccidly paralyzed to the hip. A slight improvement has followed upon faradization but the patient still can walk only with assistance.
Hypnotic treatment led to almost complete relief of the tremor. The patient started sleeping six or seven hours each night; anxiety decreased, and the stuttering gradually got better; however, the paralysis and numbness in the left leg didn't improve with suggestion. The leg stayed cold, discolored, numb, and weakly paralyzed up to the hip. There has been some slight improvement with faradization, but the patient still can only walk with help.
Smyly regards this case as probably not a true case of Shell-shock, depending as he states[303] “more on a lesion in the nervous system than in the psyche.”
Smyly views this situation not as a genuine case of Shell-shock, arguing that it relies[303] “more on damage in the nervous system than in the mind.”
Shrapnel bullet WOUND of skull: Unconsciousness (three weeks), followed by agraphia (three weeks), insomnia (six weeks), amnesia (six to eight weeks), hemiplegia (twelve weeks), impairment of vision (twelve to sixteen weeks), dreams (seven months). Recovery save for slight overfatiguability.
Shrapnel bullet WOUND of skull: Unconsciousness (three weeks), followed by agraphia (three weeks), insomnia (six weeks), amnesia (six to eight weeks), hemiplegia (twelve weeks), vision impairment (twelve to sixteen weeks), dreams (seven months). Recovery except for slight fatigue.
Case 220. (Binswanger, October, 1917.)
A French tailor, aged 22, of healthy stock, was wounded in the left frontal bone in August, 1914. The shrapnel bullet, from an unknown distance, made a penetrative wound. The man was able to remember how at the moment he was injured he felt a sort of strain in his brain, felt his head with his hand, found he was bleeding, took out a bandage from his kit, removed it from its cover and without unfolding it put it on his head. At this moment he fell unconscious and there was then complete loss of memory for three weeks. This patient, who was intellectually keen, distinguished exactly between what he could himself remember and what he was told by his comrades. One of these had told him that he had cried out indistinctly that in a matter of fifteen days he would be well. He estimated the interval between his wound and the loss of consciousness as about five minutes.
A 22-year-old French tailor from a healthy background was injured in the left frontal bone in August 1914. The shrapnel bullet, fired from an unknown distance, caused a penetrating wound. He remembered feeling a kind of pressure in his brain at the moment he got hurt, touching his head with his hand, realizing he was bleeding, and pulling a bandage from his kit. He took it out of its cover and, without unfolding it, placed it on his head. At that moment, he lost consciousness and experienced complete loss of memory for three weeks. This patient, who was intellectually sharp, could clearly differentiate between what he remembered and what his comrades told him. One of them mentioned that he had cried out indistinctly that he would be better in about fifteen days. He estimated that the time between his injury and the loss of consciousness was around five minutes.
After three weeks, the tailor came to and remembers that the first word he heard was Munich. Astonished to be in Bavaria he asked for paper and pen to write to his people, but found he could not write, though still able to dictate a little to his comrades. Besides agraphia there was hemiplegia on the right side, marked exhaustion, rapid fatiguability of vision, power of concentration but slightly diminished, and apathy for his surroundings; emotions normal.
After three weeks, the tailor regained consciousness and remembered that the first word he heard was Munich. Surprised to be in Bavaria, he asked for paper and a pen to write to his family, but discovered he couldn't write, although he could still dictate a bit to his friends. In addition to being unable to write, he had paralysis on the right side, significant fatigue, quick tiredness in his vision, slightly reduced concentration, and a lack of interest in his surroundings; his emotions were normal.
Three weeks later the power to write returned; after six weeks, sleep; memory was restored in from six to eight weeks; the paralysis disappeared in twelve weeks; vision became normal in three or four months; the dreams ceased after seven months. The mood for the first two months after regaining consciousness was slightly elevated; for another two months slightly depressed. The mood then became normal.[304] There was, then, in this case complete recovery save for slight overfatiguability in a period of seven months. There were still a few residuals of hemiplegia. An operation in November, 1916, removed a shrapnel ball, one centimeter in diameter, from a dural scar.
Three weeks later, the ability to write came back; after six weeks, sleep returned; memory was restored in about six to eight weeks; the paralysis went away in twelve weeks; vision became normal in three to four months; the dreams stopped after seven months. For the first two months after regaining consciousness, the mood was a bit elevated; for the next two months, it was slightly depressed. After that, the mood became normal.[304] In this case, there was a complete recovery except for slight overfatigue over a period of seven months. There were still a few residual effects of hemiplegia. An operation in November 1916 removed a shrapnel ball, one centimeter in diameter, from a dural scar.
This is a case of acute reaction psychosis of exogenous origin lasting three weeks and leading to complete recovery in an after phase of from four to seven months.
This is a case of acute reaction psychosis caused by external factors, lasting three weeks and resulting in full recovery within four to seven months afterward.
Normal subject, wounded and thrown to ground by shell explosion: Recurring MEMORIES of battle scene; persistently HYPERESTHETIC healed shell WOUND, with pupil and pulse changes on pressure of the scar.
Normal subject, injured and knocked to the ground by a shell explosion: Recurring memories of the battle scene; persistently hypersensitive healed shell wound, with changes in pupil size and pulse when pressure is applied to the scar.
Case 221. (Bennati, October, 1916.)
A lieutenant of artillery, student (one of his brothers dead of meningitis), suffered somewhat from diarrhœa on the battlefield. He was, however, always able to obtain the best of food. External conditions did not seriously interfere with sleep. In particular there was no excessive dampness where he was. He was preoccupied with having to act as substitute for the commandant of the battery. He was not afflicted by the thought of his parents far away; their financial affairs were entirely satisfactory.
A lieutenant in the artillery, a student (one of his brothers had died from meningitis), dealt with some diarrhea on the battlefield. However, he always managed to get the best food. The external conditions didn’t seriously disrupt his sleep. In particular, it wasn't overly damp where he was. He was focused on having to take the place of the commandant of the battery. He wasn’t troubled by thoughts of his parents far away; their financial situation was completely fine.
This almost normal man was wounded after a day of incessant fighting five months after going to the front. When firing ceased, he withdrew with his soldiers to a trench. Here he was followed by an enemy gas shell which killed some and wounded others. While outside the trench shifting mutilated soldiers to the rear, he was hit by another shell of which a chip wounded him in the left thigh. He felt a terrible spanking blow that threw him to the ground and gave him great pain. He was carried on a stretcher to the medical post across the zone of fire; thence to a field hospital and from there to a hospital further from the front. He had been for almost seven hours in a sector of the fighting line which had been almost continuously active.
This almost normal man was injured after a day of nonstop fighting five months after arriving at the front. When the shooting stopped, he retreated with his soldiers to a trench. Here, he was hit by an enemy gas shell that killed some and injured others. While he was outside the trench moving mutilated soldiers to safety, another shell hit, and a fragment wounded him in the left thigh. He felt a terrible impact that knocked him to the ground and caused him severe pain. He was carried on a stretcher to the medical post across the danger zone; from there, he was taken to a field hospital and then to a hospital located further away from the front. He had spent nearly seven hours in a combat area that had been almost continuously active.
The wound healed in less than a week. But what he had seen and felt kept tormenting his mind. There remained slight numbness in the wound where there was to be seen a spot of pigment, the size of a two-cent coin, with somewhat obscure outlines. The pain was irritated by damp weather, in certain positions, and by touch, and the pain on pressure was reflected in the pupils and in the pulse.
The wound healed in under a week. But what he had seen and felt continued to haunt him. There was still slight numbness around the wound, where a spot of pigmentation, about the size of a two-cent coin, had somewhat blurred edges. The pain worsened in damp weather, in certain positions, and when touched, and the pain felt when pressed was reflected in his pupils and pulse.
No other disturbance, organic or functional, was found.
No other issues, whether physical or operational, were found.
Wounds; operation: Hysterical FACIAL SPASM.
Wounds; procedure: Severe facial spasm.
Case 222. (Batten down, January, 1917.)
A 23-year old soldier was admitted to the National Hospital for the Paralyzed and Epileptic, June 18, 1915, in the following state: He sat in bed, gasping, with the left side of the face set in a strong tonic spasm and jaws tightly set. The contraction of the masseters was such that his mouth could not be forcibly opened. He himself could separate his teeth for about a half a centimeter, but the jaws came together when a spatula was brought for insertion and then failed to relax. The facial spasm increased as the jaw was clenched more tightly. The patient said he was unable to breathe excepting when sitting upright, and when put into dorsal decubitus he breathed violently through his clenched teeth and held his breath as long as he could, “assuming a purple tinge,” as Dr. Batten states, “which was apt to be disconcerting until one was accustomed to it.” Faradism and force permitted the removal of false teeth but only to the accompaniment of shrieks, foaming, and violent movements of the arms, lacrimation, and sweating. During sleep, the face was at rest. The spasm of left face and of jaw would come on a few seconds after waking, when an observer was perceived. Attempts to force the mouth open invoked the same procedure as before in spite of the fact that the patient ate well. In a month he was virtually normal.
A 23-year-old soldier was admitted to the National Hospital for the Paralyzed and Epileptic on June 18, 1915, in the following condition: He was sitting up in bed, gasping, with the left side of his face locked in a strong tonic spasm and his jaws tightly clenched. The contraction of the masseters was so intense that his mouth couldn’t be forcefully opened. He could manage to separate his teeth by about half a centimeter, but they would close again when a spatula was brought in, and they failed to relax. The facial spasm worsened as his jaw clenched tighter. The patient reported that he could only breathe when sitting upright, and when he was laid on his back, he breathed heavily through his clenched teeth, holding his breath for as long as he could, "turning a purple color," as Dr. Batten noted, "which could be quite unsettling until one got used to it." Faradism and force allowed for the removal of his false teeth, but this was accompanied by shrieks, foaming at the mouth, and violent arm movements, along with tears and sweating. While sleeping, his face was relaxed. The spasm of the left side of his face and jaw would begin a few seconds after he woke up, particularly when he noticed someone observing him. Attempts to force his mouth open led to the same reactions as before, even though the patient was eating well. After a month, he was practically normal.
It appears that May 13, about five weeks before, the patient had been struck by shrapnel on the right hand, forearm, and shoulder, and base of the nose, while in France. He had been dazed but had not lost consciousness, and the wounds had completely healed before arrival at hospital. It was about a week after being wounded that the patient was operated upon for removal of shrapnel from the face. Upon recovery from the anesthetic, the patient found himself unable to move the right side of the face. Unable to remove his teeth, he had been fed by rubber tube.
It appears that on May 13, about five weeks prior, the patient was hit by shrapnel in the right hand, forearm, shoulder, and base of the nose while in France. He had been dazed but did not lose consciousness, and the wounds had completely healed before he arrived at the hospital. About a week after being wounded, the patient underwent surgery to remove shrapnel from his face. After waking up from the anesthesia, he realized he couldn't move the right side of his face. Unable to eat solid food, he had been fed through a rubber tube.
Shell-shock: Hyperesthesia and over-reaction.
Shell shock: Sensitivity and overreaction.
Case 223. (Myers, March, 1916.)
A stretcher-bearer, 19, who had had 18 months’ service and 6 months’ service in France, sent to Lieut-Col. Myers the day after admission to a base hospital, showed a remarkable condition of hyperesthesia and over-reaction.
A stretcher-bearer, 19, who had 18 months of service and 6 months of service in France, sent to Lt. Col. Myers the day after being admitted to a base hospital, displayed a remarkable condition of heightened sensitivity and overreaction.
It appears that four days before, he had been blown up three times by aero torpedo mortar shells while attending the wounded. One had blown him into the air, another had blown him into a dug-out, and a third had knocked him down. Two or three hours later, having finished the job of carrying wounded to the dressing station, everything seemed to “go black” in the dug-out where he was resting, and from that time on he had been shaky. It seemed that he had hardly slept for several days before he finally gave in.
It looks like four days ago, he got blown up three times by aerial torpedo shells while helping the injured. One blast sent him flying, another threw him into a shelter, and a third knocked him down. A couple of hours later, after he had finished taking the wounded to the medical station, everything went “black” in the shelter where he was resting, and since then he had been unsteady. It seemed like he had hardly slept for several days before he finally collapsed.
There were irregular spasmodic movements of the head, arms (especially the right), and legs (especially the left). There were coarse tremors and incoördination in moving the arms. With eyes closed, he touched his nose with uncertainty. Cotton-wool touch on arms or head provoked lively movements. “I was always ticklish,” he explained, “but never like this; I can’t stand it, Sir.” Pinpricks produced almost convulsions. There was perspiration, rigidity of legs, and spasm such that knee-jerks were unobtainable. Plantar reaction, flexor. There were also visual hallucinations of bursting shells, and these were also heard when dozing.
There were irregular, sudden movements of the head, arms (especially the right), and legs (especially the left). There were noticeable tremors and a lack of coordination in moving the arms. With his eyes closed, he touched his nose hesitantly. A cotton-wool touch on his arms or head caused intense reactions. “I was always ticklish,” he explained, “but never like this; I can’t take it, Sir.” Pinpricks caused almost convulsive reactions. He was sweating, his legs were rigid, and there were spasms that made knee-jerks impossible. Plantar response was flexor. He also experienced visual hallucinations of bursting shells, which he could also hear while dozing off.
Improvement followed with rest, but about two weeks later, on waking to find himself being carried back to his tent to avoid a shower, he was so terrified that a special nurse became necessary. He was still jumpy the next day, alarmed at footsteps, and afflicted with headache. He improved further in three days; remained two months in hospital in England, had one month’s leave, and then returned to light duty.
Improvement came with rest, but about two weeks later, when he woke up and found himself being carried back to his tent to avoid a rain shower, he was so scared that a special nurse was needed. He was still on edge the next day, startled by footsteps and suffering from a headache. He got better over the next three days; spent two months in the hospital in England, had a month off, and then went back to light duty.
Shell-shock; thrown against wall; comrades killed; no visible trauma, or loss of consciousness: Persistent TREMORS, augmented in intentional movements; CRISES of agitation following noise or emotion.
Shell shock; thrown against a wall; comrades killed; no visible injury or loss of consciousness: ongoing tremors, worsened by deliberate movements; episodes of agitation triggered by noise or strong emotions.
Case 224. (Meige, February, 1916.)
A corporal (an expert gunner) and his squad had just entered a mine shaft on Nouvron Plateau, January 13, 1915, when a shell, bursting above them, threw him violently against the wall and killed or wounded several of his comrades. The corporal himself was not wounded, nor is it clear that consciousness was lost. The man lay waiting on the ground for some time until a communication trench could be finished and he could be evacuated without much danger from the mine shaft. He had already begun to tremble, and trembled still more while going back in the trench.
A corporal (an expert gunner) and his squad had just entered a mine shaft on Nouvron Plateau on January 13, 1915, when a shell exploded above them, throwing him violently against the wall and injuring or killing several of his comrades. The corporal wasn’t injured himself, nor is it clear if he lost consciousness. He lay on the ground for a while, waiting for a communication trench to be completed so he could be evacuated safely from the mine shaft. He had started to tremble, and trembled even more as they moved back through the trench.
He carried on there for a fortnight, always trembling, but not eating and no longer able to handle a gun. He was evacuated a month later and sent successively to Villers-Cotterets, to Meaux, to Courneuve (a month), again to Meaux, and finally to the neurological center at Villers-Cotterets, where he remained for two months (April 13 to June 15, 1915). Here he was given the diagnosis of hysterical chorea by Guillain, and showed lively knee-jerks and Achilles jerks and great emotionality. The tremors were greatly increased when the cannon grew loud or bombs burst nearby. Lumbar puncture here showed a perfectly normal spinal fluid. He was then sent to the Salpêtrière, June 19, 1915, and was evacuated July 13 to a civil hospital until September 24, whence he was sent for convalescence to his home village, October 6 to December 15, from which he was returned to the Salpêtrière.
He stayed there for two weeks, always shaking, unable to eat and no longer able to handle a gun. A month later, he was evacuated and sent to Villers-Cotterets, then to Meaux, then to Courneuve (for a month), back to Meaux, and finally to the neurological center at Villers-Cotterets, where he stayed for two months (from April 13 to June 15, 1915). Here, Guillain diagnosed him with hysterical chorea, and he displayed strong knee and Achilles reflexes along with intense emotional responses. The tremors worsened when there was loud cannon fire or nearby explosions. A lumbar puncture showed perfectly normal spinal fluid. He was then sent to the Salpêtrière on June 19, 1915, and was evacuated on July 13 to a civilian hospital until September 24, after which he was sent back to his home village for recovery from October 6 to December 15, before returning to the Salpêtrière.
Throughout these transfers there had been no change whatever in his status. For almost a year, as the result of a shell explosion, he had been trembling in precisely the same way. All four extremities trembled equally, unless the right arm and the left leg might be thought to tremble a bit more. The[309] tremor was equally pronounced in dorsal decubitus as in the sitting or upright postures, but ceased during sleep. The tremors were worse in the evening and it was hard for the man to get to sleep. The eyelids and tongue showed a few irregular, jerking movements, not synchronous with the tremor of the extremities. The head showed few tremors. The patient was able to diminish the trembling of the arms somewhat by keeping the elbows flexed at a right angle and held firmly to his body. If the tremor of the legs got more energetic, the patient would get up and take a few steps. Any movement, such as laying hold of an object, carrying a spoon or a glass to the mouth, led to an exaggeration of the tremors in such wise that the tremor of multiple sclerosis in its most extreme form was recalled. It was very hard for the man to eat. If the eyes were closed, the tremors grew more marked. The emotion caused by sudden noise or sharp command or memory of his trench life caused motor crises, with coarse, generalized movements, and even loss of balance. This agitation grew gradually less marked, but the tremors persisted. An attempt to test reflexes led to violent generalized contractions. There was no sensory disorder. The pulse was variable; at rest it stood at 60; if a table near by was struck suddenly, the pulse would go up to 120.
Throughout these transfers, there had been no change in his condition. For almost a year, due to a shell explosion, he had been trembling in exactly the same way. All four limbs trembled equally, although the right arm and left leg seemed to shake a little more. The tremor was noticeable whether he was lying down or sitting up, but it stopped when he slept. The tremors worsened in the evening, making it difficult for him to fall asleep. His eyelids and tongue had some irregular, jerky movements that didn't sync with the tremors in his limbs. His head had only a few tremors. He could reduce the shaking of his arms slightly by keeping his elbows bent at a right angle and pressed against his body. If the tremor in his legs intensified, he would stand up and take a few steps. Any movement, like grabbing an object or bringing a spoon or glass to his mouth, exaggerated the tremors, reminding one of the most severe forms of multiple sclerosis. It was very challenging for him to eat. When his eyes were shut, the tremors became more pronounced. Sudden noises, sharp commands, or memories of his time in the trenches triggered motor crises, causing rough, widespread movements and even loss of balance. This agitation gradually lessened, but the tremors continued. Trying to test his reflexes led to intense, widespread contractions. There were no sensory issues. His pulse varied; at rest, it was at 60, but would spike to 120 if a nearby table was suddenly hit.
Sharp gunfire: TREMORS; TREMOPHOBIA. A patient’s (an artist) description of his feelings.
Sharp gunfire: TREMORS; TREMOPHOBIA. A patient’s (an artist) description of his feelings.
Case 225. (Meige, February, 1916.)
One of Meige’s victims of shell-shock tremors was an artist. He stood the hardest sort of trench life for many months without disorder. Under particularly sharp fire, “the machine went off the track,” as the artist said, and he began to tremble. Both arms and head trembled, but especially the head, which was subject to small sidewise oscillations, variable in degree, and almost permanent,—a sort of vibration which the patient could diminish somewhat by stiffening his neck muscles. His manual tremor was not exaggerated by voluntary movements. Superficially he resembled a Parkinsonian case. He presented a curious appearance of combined vibrations and stiffness.
One of Meige’s victims of shell-shock was an artist. He endured the toughest kind of trench life for many months without any issues. Under particularly heavy fire, “the machine went off the track,” as the artist described it, and he started to tremble. Both his arms and head shook, but especially his head, which experienced small side-to-side movements that varied in intensity and were nearly constant—a kind of vibration that he could somewhat reduce by tensing his neck muscles. His hand tremor was not intensified by voluntary movements. On the surface, he resembled a case of Parkinson’s. He had a strange combination of vibrations and stiffness.
There was no doubt that this tremor had an emotional origin. In fact, the psychopathic status of the patient was described by the artist himself.[311] “My nervous state, which I thought ought to last not more than a fortnight, still persists more than three, or almost four, months after being evacuated, although the trembling is a little less. I am calmer and palpitate less, and my hands perspire less when I am emotional or making an effort. At first, the slightest shock immediately ran through me, followed by an uncontrollable trembling. Now there is an appreciable delay between the shock and the trembling; I can control it for a few seconds but not longer. The subway gate noises, a flaring light, a locomotive whistle, the barking of a dog, or some boyish prank is enough to set off the trembling; going to the theater, listening to music, reading a poem, or being present at a religious ceremony, acts the same way. Recently when a flag was being raised at the Invalides, I thought at first that I was going to be cured by so moving a spectacle, but then I suddenly began to tremble so violently that I had to cry out, and I had to sit down, weeping like a child. Sometimes the trembling comes on suddenly without any cause. I went to a novelty shop to do some errands with my wife. The crowd, the lights, the rustling of the silk, the colors of the goods—everything was a delight to me to look upon,—a contrast to our trench misery. I was happy and chatted merrily, like a schoolboy on a vacation. All of a sudden I felt that my strength was leaving me. I stopped talking; I felt a bad sensation in my back; I felt my cheeks hollowing in. I began to stare, and the trembling came on again, together with a great feeling of discomfort. If I can lean against something, sit down, or better, lie down, the trembling gets better and pretty soon stops. There are three conditions in which I feel well: first, upon waking after 11 or 12 hours’ sleep; next, after a meal, especially if it is a good one; and lastly, and above all, when I get the electric douche. Then, as if by magic, my ideas get clear, cheerful, and regain color; I feel myself again. That lasts for an hour or so; then I relapse into my sad state.”
There’s no doubt that this tremor comes from an emotional place. Actually, the artist himself described the patient’s psychopathic condition.[311] “My nervous condition, which I thought would last no more than two weeks, has continued for over three, almost four, months since I was evacuated, although the shaking is a bit less now. I’m calmer and my heart races less, and my hands sweat less when I’m emotional or exerting myself. At first, even the slightest shock would send me into uncontrollable shaking. Now there’s a noticeable delay between the shock and the shaking; I can hold it back for a few seconds but no longer. The sounds of subway gates, a bright light, a train whistle, a dog barking, or even a childish prank can trigger the trembling; going to the theater, listening to music, reading a poem, or attending a religious service does the same thing. Recently, when a flag was being raised at the Invalides, I thought I might be cured by such an emotional event, but I suddenly started trembling so hard that I had to cry out and sit down, weeping like a child. Sometimes the tremors hit me out of nowhere. I went to a novelty shop to run some errands with my wife. The crowd, the lights, the rustling silk, and the colorful goods were all so delightful to see, a stark contrast to our misery in the trenches. I was happy and chatting cheerfully, like a schoolboy on break. Suddenly, I felt my strength fading. I stopped talking; a weird sensation hit my back; my cheeks felt like they were caving in. I started staring, and the trembling returned, along with a deep sense of discomfort. If I can lean on something, sit down, or even better, lie down, the shaking eases and soon stops. There are three times I feel okay: first, when I wake up after 11 or 12 hours of sleep; second, after a meal, especially a good one; and third, most importantly, when I get an electric shower. Then, as if by magic, my thoughts become clear, cheerful, and vibrant; I feel like myself again. That lasts for about an hour; then I fall back into my gloomy state.”
As to the tremophobia, this patient says “In the tramway or in the subway, I perceive that people are looking at me, and that gives me a terrible feeling. I feel that I am inspiring pity. Some excellent woman offers me her seat. I am deeply touched; but if they look at me and say nothing, what are they thinking of me? This anxiety makes me suffer a good deal. If I am able to speak it is less painful to me, for then it is obvious that, despite my trembling, I am not a coward. What a sad situation this is!”
As for the tremophobia, this patient says, “On the tram or in the subway, I feel like people are watching me, and that gives me a terrible feeling. I think I'm making them feel pity for me. Some kind woman offers me her seat. I'm really touched by that, but if they look at me and don't say anything, what are they thinking about me? This anxiety causes me a lot of suffering. When I'm able to talk, it's less painful for me because then it's clear that, even though I'm trembling, I'm not a coward. What a sad situation this is!”
Meige remarks that therapeutics is not especially successful in these cases of tremor. Sedative drugs, hyoscyamin, hyoscin, duboisin, and scopolamin, do not last long and should be used cautiously. Static electricity works well in some cases. Rest, isolation, and calm.
Meige notes that treatments aren't particularly effective for these tremor cases. Sedative medications like hyoscyamine, hyoscine, duboisin, and scopolamine don't have lasting effects and should be used carefully. Static electricity can be helpful in some situations. Rest, isolation, and tranquility are important.
As for the military prognosis, a period of observation of some three to four months may be necessary to learn the nature of the tremor. If the tremor then fails to alter, a convalescent leave for one or two months may be given. The patient should then be re-observed by the same physician. Upon persistence of tremor, temporary invaliding. Tremors may be wittingly cultivated for medicolegal purposes (Brissaud’s sinistrosis.)
As for the military assessment, we might need to observe for about three to four months to understand the character of the tremor. If the tremor doesn’t change, a recovery leave of one or two months might be granted. The patient should then be re-evaluated by the same doctor. If the tremor continues, temporary medical discharge may be necessary. Tremors can also be intentionally developed for legal reasons (Brissaud’s sinistrosis.)
Letters of a German soldier about his shell-shock.
Letters of a German soldier about his PTSD.
Case 226. (Gaupp, April, 1915.)
A volunteer, 21, who had been in civil life a lackey, wrote as follows upon arrival in Gaupp’s clinic:
A 21-year-old volunteer, who had previously worked as a servant, wrote this upon arriving at Gaupp’s clinic:
“On account of our privations and the various terrible scenes that you have to see, my nerves went back on me. Like the rest of the front, we too had to suffer terribly heavy artillery fire from December 20 onwards. December 29 at eight o’clock in the evening, when I was about to mount guard at the camp, I was thrown down by a shell that unexpectedly struck near me across the earth pushed out into a trench. I ran at once to cover as some more shots followed directly. I couldn’t be made to do anything on the thirtieth nor can I very clearly remember the events of that day. There was a terrific cannonade again, then cries of the wounded and the sight of the dead, etc. I was told afterwards that I fell down, cried, struck about me, and remained lying, dazed. The first that I can remember was that I was lying on a floor. I was then carried into another house, into a better room. Then I regained consciousness and could hear again after the noise in the ears had stopped, but I could not talk or walk. I was unconscious for two days. I got into the hospital train at R. the next day but had to be carried in as I could not walk. Travelling in the train made me quite foolish in my head and gave me bad headaches; I could not form any clear thoughts.”
“Because of our struggles and the terrible scenes we had to witness, my nerves gave out. Like the rest of the front, we endured extremely heavy artillery fire starting December 20. On December 29, at eight o’clock in the evening, just as I was about to take my place on guard duty, a shell unexpectedly hit nearby and threw me into a trench created by the blast. I immediately ran for cover as more shots followed right after. I couldn't do anything on the thirtieth, and I barely remember what happened that day. There was intense cannon fire again, followed by cries from the wounded and the sight of the dead, among other things. I was told later that I had collapsed, cried out, flailed around, and lay there, stunned. The first thing I remember is lying on a floor. I was then carried to another house, into a better room. I regained consciousness and could hear again after the ringing in my ears stopped, but I couldn’t talk or walk. I was unconscious for two days. The next day, I was loaded onto a hospital train at R., but I had to be carried in since I couldn’t walk. Traveling on the train made me feel completely out of it and gave me terrible headaches; I couldn't think clearly at all.”
It seems that this volunteer had not been quite up to the hardships of the war from the beginning; always a weakling, he had to be spared on the marches. In fact, he had been refused by the army at the first examination as unfit. He had been a nervous, tender, somewhat anxious fellow since childhood.
It seems that this volunteer had never really been able to handle the hardships of the war from the start; always a bit of a weakling, he had to be given a break on the marches. In fact, the army had turned him down at the first examination for being unfit. He had been a nervous, sensitive, somewhat anxious guy since he was a child.
At the clinic there was an astasia and an abasia without any signs of organic disease. The striking feature was mutism. He could understand things spoken and written, but he was entirely mute, nodding and shaking his head properly for affirmatives and negatives. He carried with him a few slips[313] of paper with written requests, like: “Please, can I have salt; otherwise I can’t eat the soup;” “Are we going to ride farther, I have such a bad headache. The doctor must not come. The one who wanted to shoot me if I couldn’t speak. They are all bad.”
At the clinic, there was a lack of movement and inability to walk without any signs of physical disease. The most noticeable issue was mutism. He could understand spoken and written communication, but he couldn’t speak at all, responding with nods and shakes of his head for yes and no. He had a few slips[313] of paper with written requests, such as: “Please, can I have salt; otherwise I can’t eat the soup;” “Are we going to ride further? I have such a bad headache. The doctor must not come. The one who wanted to shoot me if I couldn’t speak. They are all bad.”
Treatment by suggestion (laryngeal faradization, lively verbal suggestion to pronounce single vowels, syllables, and whole words and sentences with enunciation of them) removed the mutism in a few days. At first the man’s speech was low and somewhat retarded, but later it became entirely normal. Within ten days the abasia cleared up and the patient became lively and cheerful. He was depressed on finding that he had lice, but after losing them became happy and childlike again.
Treatment through suggestion (laryngeal faradization, energetic verbal prompts to pronounce single vowels, syllables, and whole words and sentences clearly) eliminated the mutism in just a few days. Initially, the man's speech was quiet and somewhat slow, but eventually, it returned to normal. Within ten days, the abasia resolved, and the patient became lively and cheerful. He felt down after discovering he had lice, but once he got rid of them, he became happy and childlike again.
February 1, however, on learning that he would be able to do garrison duty again, he took the news very soberly, and grew more quiet, trembled and seemed anxious.
February 1, however, upon hearing that he would be able to do garrison duty again, he took the news very seriously, became quieter, trembled, and seemed anxious.
February 7, he was sent to the garrison, increasingly excited. His own account of it in a letter written to a hospital nurse, runs as follows:
February 7, he was sent to the garrison, feeling more and more excited. His own description of it in a letter to a hospital nurse goes like this:
“As you will see, I did not reach Dn. but only got as far as here [Another hospital]. I will tell you how it happened. Probably I ought to have remained in Tübingen for a while longer and perhaps then nothing would have happened to me. You will remember that I was more nervous and excited the last days than I had been before, and the cause was also known to you. I wanted to get home in some way and so I pretended to be as well as possible. That crying attack, or whatever it was [an outcry in a frightful dream] had not been thought of by the physician any further, you know, and so I didn’t think anything about it either. Then the head doctor asked me once if I had any trouble left. Well, I spoke out everything I had to say, but no further attention was paid to that either. Then when I took a walk and after walking slowly two hours could hardly stand, was trembling all over and had a high pulse and also a violent acute pain in the region of the heart, that wasn’t of any importance either. Well, then I just got better from day to day and so I got what I wanted only too easily because they wanted the space and I certainly would have gone home and not to Dn. as I should have. [His reserve battalion was at Dn.] I got into the wrong train at St. so as to go home. I kept saying to myself, ‘You can’t do that, it will be punished.’ Nevertheless I couldn’t act any other way because I was really sick from longing for home.”
“As you’ll see, I didn’t make it to Dn. but only got as far as here [Another hospital]. Let me explain what happened. I probably should have stayed in Tübingen a bit longer; maybe then nothing would have happened to me. You remember I was more nervous and anxious in the last days than I had been before, and you already knew the reason for that. I wanted to get home in some way, so I pretended to be as well as I could. That crying episode, or whatever it was [an outcry from a nightmare], wasn't considered significant by the doctor, so I didn’t think much of it either. Then the head doctor asked me once if I still had any problems. Well, I voiced everything I needed to say, but no one focused on that either. Later, when I took a walk and after strolling for two hours could barely stand, trembling all over with a high pulse and sharp pain in my chest, that didn’t seem important either. So, I just improved day by day, and I got what I wanted a little too easily because they were looking to free up space, and I definitely would have gone home instead of to Dn. as I should have. [His reserve battalion was at Dn.] I got on the wrong train at St. trying to go home. I kept telling myself, ‘You can’t do this; it’ll be punished.’ Still, I couldn’t act differently because I was genuinely unwell from missing home.”
Here he described an episode in a comrade who had lain beside him in the clinic, had gone off with him and had a hysterical excitement in Heidelberg so that he had to be detrained.
Here he described an incident involving a fellow soldier who had been lying next to him in the clinic, had left with him, and had been so hysterically excited in Heidelberg that he had to be taken off the train.
“I was so awfully sorry to see him so miserable. I began to cry and was startled by every train coming from the opposite direction and by every loud noise. I was stared at by everybody in Frankfort and I could only cry more. Then a soldier scolded me because I was running senselessly up and down. Finally I got into the Leipzig train. Another guard questioned me. Everything then got more and more confused in me; I heard my mother call; then I heard shooting again; and finally I was entirely confused. I came to my senses in a room in the station toward evening, and was frightened again at a loud noise somewhere or a passing train. Then I was told what I had done in the train. I had cried out and raved, tried to get out of the car, called for my father and mother, wanted to go home, imitated shooting; allowed myself to be calmed a little, but began to shout again at every loud noise. When I was out of the train I bit a soldier and tore his whole coat open, so then I was carried to the hospital here in an auto. Up to this time I have been able to calm myself very well. The physician said that it was quite natural that I should not have very strong nerves yet. I must have beaten about and got knocked against things a good deal. There are bruises on my head and I am covered with black-and-blue spots.”
“I was really sorry to see him so unhappy. I started crying and flinched at every train coming from the other direction and every loud noise. Everyone in Frankfurt stared at me, which only made me cry more. Then a soldier yelled at me for running around aimlessly. Eventually, I got on the Leipzig train. Another guard questioned me. Everything just became more and more confusing; I heard my mother calling; then I heard gunfire again; and finally, I was completely lost. I came to my senses in a room at the station in the evening and was startled again by a loud noise or a passing train. Then I was informed about what I had done on the train. I had shouted and raved, tried to get out of the car, called for my dad and mom, wanted to go home, pretended to shoot; I managed to calm down a little, but started shouting again at every loud noise. When I got off the train, I bit a soldier and ripped his whole coat open, so I was then taken to the hospital here in a car. Up until now, I’ve been able to calm myself pretty well. The doctor said it was natural for me not to have very strong nerves yet. I must have been bouncing around and hitting things a lot. I have bruises on my head and I’m covered in black-and-blue spots.”
A British soldier’s account of his shell-shock.
A British soldier's story of his shell shock.
Case 227. (Batten down, January, 1916.)
A British soldier, 22 years, who went out to France in November, 1914, remained well until March 12, 1915, when after shell explosion, he became unconscious for half an hour, and on recovery found he was deaf and dumb. He was able to think of words but could not say them. He remained dazed and frightened for a time, and still wakes up with a start at night.
A 22-year-old British soldier who went to France in November 1914 was doing fine until March 12, 1915. After a shell explosion, he lost consciousness for half an hour. When he came to, he realized he was deaf and mute. He could think of words but couldn't say them. He felt dazed and scared for a while and still wakes up suddenly at night.
He was admitted to the National Hospital for the Paralyzed and Epileptic, March 25, 1915, and on March 27 recovered his speech suddenly and spontaneously. By March 29 he had completely recovered and talked well. Dr. Batten remarks “how perfect the memory may be up to the time of concussion, and how complete the mechanism is for expressing the ideas in written words when that for spoken words is abolished”; which may be seen from the patient’s own account, as follows:
He was admitted to the National Hospital for the Paralyzed and Epileptic on March 25, 1915, and on March 27, he suddenly and spontaneously regained his speech. By March 29, he had fully recovered and spoke well. Dr. Batten notes "how perfect the memory can be up to the time of the concussion, and how complete the mechanism is for expressing ideas in written words when the one for spoken words is lost"; this can be observed in the patient’s own account, as follows:
I went out to France on the 3/11/14 and I was two days at Le Havre and then we went on to our 1st Batt. When we arrived at our destination the regiment was in the trenches so we had to go in. It was snowing hard and I felt it very cold. This was at Givenchy. We were relieved the following night and we went back for a rest. The next place we went to was just opposite Neuve Chapelle on the La Bassée Road and it was awful, the trenches were up to the knees in mud and water. The first night was very quiet, but the following morning about 9 p.m. the Germans started shelling and continued all day; the next was the same, but about 1 o’clock the Germans were seen to be coming up in masses. They got to within a distance of about twenty-five yards, then they turned. They commenced shelling us again and they had another try about three o’clock but they did not get far. One of the men on my left had the half of his face blown away and we had about ninety-two killed and wounded. We got relieved after being in five days, then we went back for three days’ rest. The next place we went to was Rue[316] de l’Epinette and we had an awful time there just before Christmas. We went into the trenches and we were up to our middle in water and in some places it would have taken you over the head. We were in these trenches for twenty-four hours. There was nothing unusual happened and we got relieved by the Royal North Lancs.; but we did not get far away; we had just got into our billets and were making some tea when the fall-in went and we were told that the Germans had broken through the North Lancs. We went away without any great-coats, and into the trenches we went for other seventy-two hours, and if the Germans had attacked again we could not have fired a shot as we were hardly able to stand for the cold and with the wet kilts on our legs it was awful. We got nothing to eat except three biscuits that some of the men went out and got. When we came out of the trenches on Christmas Eve we looked all like old men and a lot of them had to be carried. We went back for a rest to (Nervaille?) about thirty kilometers from the firing line for a month. When we came back again we went to La Bassée and had a pretty hot time there. The next place we were at was at that big fight at Neuve Chapelle when 472 guns bombarded the German trench for thirty-five minutes. At about 7 p.m. the word was passed along that we were to charge the German trench in front supported by the City of London Territorials. We got the trench all right and I got orders about 4 p.m. to go back to our own trench and bring along the belt-filling machine belonging to the machine gun. There was not a proper communication trench, there was a small dry ditch that ran out in the direction of the trench we had taken for a distance of 150 yards, the other 100 yards you had to come across the open. We got into our trench all right, and I got this box on my back and started back to the trench. I was just stepping out of the trench when a shell burst just over my head and I went down. When I came to my senses I was lying in our support trench where I had been carried by two of the men of the 4th Black Watch. One of them said something but I could not hear him and I tried to tell him so, then I discovered that I could not speak.
I went to France on November 3, 1914, and spent two days in Le Havre before heading to our first battalion. When we got to our destination, the regiment was already in the trenches, so we had to go in. It was snowing heavily, and I felt really cold. This was at Givenchy. We were relieved the following night and went back for a rest. The next place we moved to was just opposite Neuve Chapelle on the La Bassée Road, and it was terrible— the trenches were knee-deep in mud and water. The first night was very quiet, but the next morning around 9 a.m., the Germans started shelling and continued all day. The same happened the following day, but around 1 o'clock, we saw the Germans coming up in large numbers. They got to within about twenty-five yards before turning back. They started shelling us again and attempted another attack around three o'clock, but they didn’t get far. One of the men to my left had half his face blown off, and we had about ninety-two killed and wounded. After being there for five days, we were relieved and went back for three days of rest. Our next stop was Rue[316] de l’Epinette, where we had a terrible time just before Christmas. We went into the trenches and were waist-deep in water, with some places even deeper. We spent twenty-four hours in those trenches. Nothing unusual happened, and we were relieved by the Royal North Lancs.; but we didn’t get far—we had just settled into our billets and were making some tea when the call came in, and we were told that the Germans had broken through the North Lancs. We went back without greatcoats and into the trenches for another seventy-two hours, and if the Germans had attacked again, we wouldn’t have been able to fire a shot because we were barely able to stand due to the cold and the wet kilts on our legs—it was awful. We barely had anything to eat, just three biscuits that some of the men managed to grab. When we finally came out of the trenches on Christmas Eve, we all looked like old men, and many of them had to be carried. We returned to a rest area at Nervaille, about thirty kilometers from the front line, for a month. When we got back, we went to La Bassée and experienced quite a tough time there. The next place we were at was during the major battle at Neuve Chapelle when 472 guns bombarded the German trenches for thirty-five minutes. Around 7 p.m., we received orders to charge the German trench ahead, supported by the City of London Territorials. We successfully took the trench, and at about 4 p.m., I was ordered to return to our own trench to bring back the belt-filling machine for the machine gun. There wasn’t a proper communication trench; there was a small dry ditch that extended 150 yards toward the trench we had captured, and for the remaining 100 yards, we had to cross open ground. I got back to our trench and strapped the box on my back, starting my way back. Just as I was stepping out of the trench, a shell exploded right above me, and I fell. When I regained consciousness, I was lying in our support trench, where two men from the 4th Black Watch had carried me. One of them said something, but I couldn't hear him, and when I tried to respond, I realized I couldn’t speak.
Shell-shock by windage: Hysterical crural monoplegia, of gradual development beginning four days after accident. Recovery by suggestion.
Shell shock caused by wind: Hysterical leg paralysis that developed gradually starting four days after the incident. Recovery through suggestion.
Case 228. (Léri, February, 1915.)
A number of chasseurs were doing the “tortoise-shell” under bombardment, when the last chasseur in the line was blown forward above his comrades by a shell bursting about a meter behind him. He was projected some four or five meters, got up, walked four or five kilometers, found an automobile, and was carried to Nancy. He passed, according to his story, red urine three or four times. He was six days at Nancy, where a slight abrasion of the side was treated. He began to feel heavy in his left leg on the fourth day. At Vendôme, the paralysis got worse, and by November 17 he had apparently a complete paralysis of the left lower extremity, called “spinal contusion.” He walked upon two canes, dragging left leg behind and had to be carried upstairs on a stretcher. The reflexes were normal except that there might have been a very slight excess of the left knee-jerk. There was a slight hypesthesia of the left leg, sharply limited above.
A group of soldiers was taking cover during a bombardment when the last soldier in line was thrown forward over his comrades by a shell that exploded about a meter behind him. He was propelled about four or five meters, got up, walked four or five kilometers, found a car, and was taken to Nancy. He reported passing red urine three or four times. He spent six days in Nancy, where a minor side abrasion was treated. On the fourth day, he started feeling heaviness in his left leg. In Vendôme, the paralysis worsened, and by November 17, he appeared to have complete paralysis of the left leg, termed “spinal contusion.” He walked with two canes, dragging his left leg behind, and had to be carried upstairs on a stretcher. The reflexes were normal except for a slight increase in the left knee-jerk response. There was a slight decrease in sensation in the left leg, sharply limited above.
These phenomena were strikingly modified, at a single sitting, by verbal suggestion and faradism, but the man was one of those with mauvaise volonté. He did not want to get well so quickly, so that his complete cure was delayed a while.
These phenomena were significantly altered in just one session through verbal suggestion and faradism, but the man had bad intentions. He didn't want to recover so quickly, which delayed his full recovery for some time.
NATURE OF SHELL-SHOCK: At the nerve clinic the patient presents, e.g., sundry CONTRACTURES, of such a nature that they may be caused to DISAPPEAR BY SUGGESTION, e.g., by mental influences during recovery from chloroform narcosis (note battle-dreams). PAINS and ANESTHESIAS disappear PARI PASSU with the contractures. The history is of shell explosion so near as to burn patient’s clothing, fall with nosebleed, eight hours unconsciousness, crural monoplegia with anesthesia (crawled 3 meters, however).
NATURE OF SHELL-SHOCK: At the nerve clinic, the patient shows various CONTRACTURES that can be made to DISAPPEAR THROUGH SUGGESTION, such as mental influences during recovery from chloroform anesthesia (note battle-dreams). PAINS and ANESTHESIAS fade AWAY alongside the contractures. The history includes a shell explosion that was close enough to burn the patient’s clothing, resulting in a nosebleed, eight hours of unconsciousness, and crural monoplegia with anesthesia (though the patient managed to crawl 3 meters).
Case 229. (Binswanger, July, 1915.)
The treatment of a German private, 22, for contracture of the left leg and other phenomena, culminated in narcosis. Binswanger lays stress upon the mental influence to be exerted upon the patient at the conclusion of narcosis, at the moment in which the patient is particularly accessible to verbal suggestion. Treatment (see diagnostic details below) was carried out as follows:
The treatment of a 22-year-old German private for a contracted left leg and other issues ended with him being put under anesthesia. Binswanger emphasizes the importance of the mental influence on the patient at the end of the anesthesia, when the patient is especially open to verbal suggestion. The treatment (see diagnostic details below) was carried out as follows:
After a few days of essentially suggestive treatment with continued attempts at passive movements of the contracted joints (knee, ankle, toe), with steady concentration of the patient’s attention upon the joints, a slight mobility in the toe joint on passive movement was obtained.
After a few days of mostly gentle treatment, along with ongoing efforts to passively move the stiff joints (knee, ankle, toe), and keeping the patient's focus on those joints, we achieved a slight improvement in mobility in the toe joint during passive movement.
After a few more days, the ankle became passively mobile to some degree; the patient exerted a certain resistance to passive flexion of toes and ankle. A week later, reflex contractions of the toes could be evoked by deep pin-prick. There had been an analgesia of both lower thighs and of the soles of the feet, and this analgesia remained unchanged. At this point, the subjective complaints of the patient, namely, noises in the head, especially in the left ear, and other cephalic sensations, tended to disappear and the patient felt subjectively better; yet there was still an intolerable itching of the head and spine.
After a few more days, the ankle had some passive movement; the patient showed some resistance to the passive bending of the toes and ankle. A week later, reflex contractions of the toes could be triggered by a deep pin-prick. There had been a loss of sensation in both lower thighs and the soles of the feet, and this loss of sensation stayed the same. At this point, the patient’s subjective complaints, like noises in the head, especially in the left ear, and other head sensations, started to fade, and the patient felt somewhat better; however, there was still an unbearable itching on the head and spine.
A month after the admission of the patient to the nerve hospital of the psychiatric clinic in Jena, there had been no essential change in the immobility and contracture in extension in the left leg. Accordingly, with the permission of the patient, he was placed in deep chloroform narcosis, and the knee-joint was bent at a right angle and fixed in approximately that position with a bandage. This experiment failed because, while the patient was waking out of his narcosis, the leg slipped back into extension, breaking the bandage. Accordingly, deeper narcosis was undertaken, and the leg fixed at a right angle in a plaster cast.
A month after the patient was admitted to the nerve hospital of the psychiatric clinic in Jena, there had been no significant change in the immobility and contracture in extension in the left leg. Therefore, with the patient's consent, he was put under deep chloroform anesthesia, and the knee joint was bent at a right angle and held in that position with a bandage. This attempt failed because, as the patient was waking up from the anesthesia, the leg slipped back into extension, breaking the bandage. As a result, a deeper level of anesthesia was administered, and the leg was固定在一个右角的石膏绷带中。
While the patient was coming out of narcosis, it was evident that he had been dreaming of battle scenes. In fact, Binswanger remarks that these dream pictures and the words spoken while going under and coming out of narcosis, are curiously demonstrative of “sympathy with the enemy,” for while waking out of narcosis, he cried: “Dost see, dost see the enemy there? Has he a father and mother? Has he a wife? I’ll not kill him.” At the same time, he cried hard and continually made trigger-movements with his right forefinger.[6] In point of fact, throughout his waking treatment, no one was able to learn what was going on in his mind, his sleep was good and deep, and his emotional state was entirely quiet and patient.
While the patient was coming out of anesthesia, it was clear that he had been dreaming of battle scenes. In fact, Binswanger notes that these dream images and the things he said while going under and waking up from anesthesia are oddly revealing of “sympathy with the enemy,” because as he was coming to, he cried out: “Do you see, do you see the enemy there? Does he have a father and mother? Does he have a wife? I won't kill him.” At the same time, he cried hard and repeatedly made trigger movements with his right forefinger.[6] In reality, throughout his treatment while awake, no one was able to figure out what was on his mind; his sleep was good and deep, and his emotional state was completely calm and patient.
As the patient was coming out of chloroform and regaining consciousness of his surroundings, he was repeatedly and persistently assured that the bending of his leg was now accomplished and the cramp removed. All that he would now have to do was to get back the strength of his leg.
As the patient was waking up from chloroform and becoming aware of his surroundings, he was consistently reassured that his leg had been straightened and the cramp was gone. All he needed to do now was regain the strength in his leg.
During the next few days he complained of violent pains in his left knee-joint and in the ankle-joint, but he remained in good spirits and full of confidence. Accordingly, in five days the plaster was removed and the contracture in the knee-joint was found to be completely absent; the knee was easily movable. The ankle-joint was but slightly movable. He could accomplish slight active flexion of the knee-joint[320] while lying in bed, and the toe-joint had already, before the narcosis, been both actively and passively mobile. After a few days, exercises in walking were begun. The patient had a little difficulty with his left knee-joint in walking, walking in fact as if with knock-knee. The foot was not well raised from the ground on account of the persistent stiffness of the ankle-joint. Walking, however, improved daily. He walked for three hours, resting at intervals.
Over the next few days, he complained of severe pain in his left knee and ankle, but he kept a positive attitude and remained confident. So, after five days, the cast was removed, and there was no contraction in the knee joint; it moved easily. The ankle joint was only slightly flexible. He could manage a little active bending of the knee while lying in bed, and even before the anesthesia, the toe joint had already been able to move actively and passively. After a few days, he started practicing walking. He had some trouble with his left knee while walking, actually moving as if he had knock knees. His foot didn't lift well off the ground because of the ongoing stiffness in the ankle joint. However, his walking got better each day. He walked for three hours, taking breaks in between.
A sensory examination showed that the upper limit of the analgesia had come down five centimeters from its former level, now occupying the left foot and leg up to the junction of the lower with the middle third. There was now a zone of anesthesia interposed between the normal skin of the upper thigh and the anesthetic-and-analgesic skin of the lower thigh and leg. Upon the posterior aspect of the leg, the analgesia and anesthesia had disappeared to a point at about the middle of the upper thigh.
A sensory exam revealed that the upper limit of the pain relief had decreased by five centimeters from its previous level, now reaching the left foot and leg up to where the lower third meets the middle third. There was now an area of numbness between the normal skin of the upper thigh and the numbed and pain-free skin of the lower thigh and leg. On the back of the leg, the pain relief and numbness had faded to about the middle of the upper thigh.
About five weeks after the narcotic experiment, the extended left leg could be actively raised while lying in bed, up to the full extent, with slight tremors. The patient described himself as fatigued by the active movements of this leg. The ankle-joint remained less effective. There was still a trace of resistance to passive movements. Although the passive movements of the toes were normal, active movements of these were weak and hard to execute. There was still a trace of difficulty at the knee in walking and the gait was awkward, trepidant, precipitate. He could get about without a cane, however. If unobserved, his posture was more certain and free. If he exerted himself hard, severe parietal headache on the right side would develop.
About five weeks after the narcotic experiment, the extended left leg could be actively raised while lying in bed, fully, with slight tremors. The patient said he felt fatigued by the active movements of this leg. The ankle joint was still less effective. There was still some resistance to passive movements. Although the passive movements of the toes were normal, active movements were weak and difficult to perform. There was still some difficulty at the knee while walking, and the gait was awkward, shaky, and hurried. He could walk without a cane, though. When unnoticed, his posture was more stable and relaxed. If he pushed himself too hard, he would develop a severe headache on the right side of his head.
It was then proposed to the patient that another narcosis would rid him of the stiffness in his ankle-joint. He feared narcosis and was told that regular and energetic voluntary movements would also rid him of the stiffness. These will exercises consisted in his directing his whole attention to his left ankle-joint until he felt it. Then he was given the command: “Let go the joint”—whereupon he would take his attention away from the ankle-joint at once. In this way, he was told, his will would make the ankle-joint mobile.[321] Meantime he was given twice daily a gram of bromophenacetine for his parietal headache.
It was suggested to the patient that another round of anesthesia would help ease the stiffness in his ankle joint. He was anxious about the anesthesia and was informed that consistent and vigorous voluntary movements could also alleviate the stiffness. These exercises involved him focusing all his attention on his left ankle joint until he could actually feel it. Then he was instructed to "Forget about the joint"—at which point he would shift his attention away from the ankle joint immediately. He was told that this way, his willpower would help make the ankle joint more flexible.[321] In the meantime, he was given a gram of bromophenacetine twice a day for his parietal headache.
The result was a rapid recovery. There were still a few traces of difficulty at date of report. The zone of sensory loss had retreated to the ankle, with a cuff-like zone of hypalgesia above the definite zone of analgesia and anesthesia.
The result was a quick recovery. There were still a few signs of difficulty at the time of the report. The area of sensory loss had moved back to the ankle, with a band-like area of reduced sensitivity above the clear zone of no pain and numbness.
As to the previous nature of this case, although there was neuropathic heredity on the mother’s side, there had been no sign of any individual neuropathic disposition. He had been a volunteer since 1911 in a guard regiment of infantry. His military training had been well borne; in the war he had fought through 20 battles. On November 11, 1914, in a storming attack, he had had his breeches burned from the effects of a shell. He had fallen, unconscious; the unconsciousness lasted about eight hours. He found on awaking that he had had nosebleed. When he wanted to get up, he found that his left leg was completely paralyzed and insensible; in fact, he thought it had been cut away. He crawled for about three meters to a trench in which there were several wounded. In the evening he was taken by automobile to a field hospital, and on the 17th was removed to a reserve hospital at Erfurt. Thence he was transferred to the Jena Hospital, January 25, 1915.
Regarding the earlier condition of this case, even though there was a history of neuropathy on the mother’s side, there were no indications of any individual neuropathic tendencies. He had been a volunteer in an infantry guard regiment since 1911. He handled his military training well; during the war, he fought in 20 battles. On November 11, 1914, during a storming attack, his pants were burned by a shell explosion. He fell unconscious, and this state lasted about eight hours. When he woke up, he discovered he had a nosebleed. When he tried to get up, he realized his left leg was completely paralyzed and numb; in fact, he thought it had been amputated. He crawled for about three meters to a trench where several wounded soldiers were located. In the evening, he was taken by car to a field hospital, and on the 17th, he was moved to a reserve hospital in Erfurt. From there, he was transferred to Jena Hospital on January 25, 1915.
A strongly built man, with many reflexes increased and a lively dermatographia. The reflexes of the left, or contractured, leg were lacking; the mastoid processes were painful, and the occiput and temples were painful to percussion. The spinous processes of the vertebral column in the lumbar region were painful. The other phenomena have been sufficiently indicated above. The head sensations were peculiar; there were no pains but a peculiar itching. Contraction of the fingers of the left hand was painful. There was a feeling as if there were lice under the skin in the left upper thigh. There was itching in the nose, which the patient described as due to the sulphur “out there,” meaning shell gases. Sleep and appetite were good. Memory was imperfect: he could no longer remember the names of the battles, and of late had had to count on his fingers to find out how much was 2 times 2. As to the curious parietal headache, contralateral[322] to the contractured leg, Binswanger inquires whether we may not here have to do with localized vascular phenomena of the brain part which might conceivably be related with the innervation of the leg. Binswanger remarks that if the plaster cast be left on too long, it may happen that hysterical contracture will take place in the new position.
A well-built man, with heightened reflexes and noticeable skin sensitivity. The reflexes in his left leg, which was contracted, were absent; his mastoid areas were painful, and the back of his head and temples were sensitive to touch. The spinal processes in his lower back were painful as well. Other symptoms have been adequately mentioned above. He experienced unusual sensations in his head; there was no pain but a strange itching. The fingers of his left hand contracted painfully. He felt like there were bugs crawling under the skin on his left thigh. He had an itchy nose, which he attributed to the sulfur “out there,” referring to shell gases. He slept well and had a good appetite. His memory was poor: he could no longer remember the names of battles and recently had to count on his fingers to figure out 2 times 2. Regarding the strange headache on the parietal side, opposite the contracted leg, Binswanger questions if this could be linked to localized blood flow changes in the part of the brain that might be connected to the leg's nerve functions. Binswanger notes that if the plaster cast is left on for too long, it could result in hysterical contraction in the new position.
As to the will exercises used in the present case, Binswanger remarks that the patients must be intelligent and attentive, and naturally they must desire to get well. Fortunately, many of the war hysterics do want to get well, since the contrary experience is had in various industrial cases.
As for the will exercises used in this case, Binswanger notes that patients need to be intelligent and focused, and of course, they must want to get better. Fortunately, many of the war hysterics do want to recover, unlike in various industrial cases where the opposite is true.
Wound of thigh: Pseudocoxalgic monoplegia with anesthesia. Cure of anesthesia by faradism at one sitting. Cure of lameness by reëducation and electricity in one month.
Wound of thigh: Pseudocoxalgic monoplegia with loss of feeling. Treatment of loss of feeling by faradism in one session. Treatment of lameness through re-education and electricity in one month.
Case 230. (Roussy and Lhermitte, 1917.)
An infantryman, observed at Villejuif, February 9, 1915, was suffering from a right-sided crural monoplegia of a pseudocoxalgic type, following a wound September 9, 1914. The wound had been a through-and-through one in the upper right thigh. Every active movement could be performed as well on the right side as on the left; but the strength of the movements was less on the right, especially that of leg-extension. The reflexes were normal, the lameness was slight, with toeing out; the sole came down flat upon the ground. There was an absolutely complete anesthesia of the entire right leg and side up to the umbilicus.
An infantryman, observed at Villejuif on February 9, 1915, was experiencing right-sided leg weakness similar to hip pain, following a wound on September 9, 1914. The injury had gone through the upper right thigh. He could perform all active movements on both sides, but the strength of the movements was weaker on the right, especially in extending the leg. The reflexes were normal, he had a slight limp with his toes pointed outward; his foot landed flat on the ground. There was complete loss of feeling in the entire right leg and the side up to the belly button.
Energetic faradization of the skin caused the anesthesia to disappear the day the patient was brought to the hospital. The cure of the lameness required a month of reëducation and electricity.
Energetic faradization of the skin caused the anesthesia to wear off the day the patient was brought to the hospital. The treatment for the lameness required a month of rehabilitation and electrical therapy.
According to Roussy and Lhermitte, crural monoplegia is less frequent than brachial monoplegia. The flaccid form is rare, and when it occurs, complete, though the patient always remains capable of executing some voluntary movements and can walk with crutches or cane. During the automatic movements of walking, some muscles may be observed to contract that remain immobile when the patient is being examined recumbent. Naturally such a difference in contractions standing and lying, would be very exceptional in a case of organic monoplegia.
According to Roussy and Lhermitte, crural monoplegia is less common than brachial monoplegia. The flaccid form is rare, and when it does happen, it's complete. However, the patient can still perform some voluntary movements and can walk with crutches or a cane. During automatic walking movements, some muscles may be seen contracting that stay inactive when the patient is lying down. Naturally, such a difference in muscle contractions between standing and lying down would be very unusual in a case of organic monoplegia.
Contusion of thigh: HYSTERICAL right crural MONOPLEGIA. An ORGANIC CRUTCH PARALYSIS develops in the right arm, unobserved by the patient whose main concern is his useless leg. Cure of leg by psychotherapy.
Contusion of thigh: HYSTERICAL right leg MONOPLEGIA. An ORGANIC CRUTCH PARALYSIS develops in the right arm, unnoticed by the patient whose main focus is his useless leg. Treatment of leg through psychotherapy.
Case 231. (Babinski reflex, 1917.)
A certain lieutenant, following contusion of the right thigh, developed a crural monoplegia of hysterical nature. In fact, although the paralysis had lasted several months, the tendon reflexes, the skin reflexes, and the electrical responses of the muscles, were absolutely normal. Moreover, the good effects of psychotherapy confirmed the hypothesis. But besides the hysterical crural monoplegia, there was a radial paralysis on the right side, clearly organic in nature, due to the nerve compression by the crutch which the patient had employed on account of the paralysis of his leg.
A lieutenant, after injuring his right thigh, developed a hysterical paralysis in his leg. Even though the paralysis lasted several months, the tendon reflexes, skin reflexes, and the electrical responses of the muscles were all completely normal. Additionally, the positive effects of psychotherapy supported this idea. However, alongside the hysterical leg paralysis, there was also a clear organic radial paralysis on the right side, caused by nerve compression from the crutch the patient was using due to his leg paralysis.
Babinski notes that this association of conditions was remarkable in that it demonstrated that hysteria and simulation should not be confounded with one another. To be sure, it is difficult to tell simulation from suggested phenomena, for there are no objective characters that demarcate the two. Babinski had himself said that hysteria was a demi-simulation; but a demi-simulation is not a simulation. The patient was in fact, sincere enough in his belief that he could not move his leg. To obviate this paralysis, he had in fact leaned so conscientiously upon his crutch that an organic paralysis had resulted. In fact the radial palsy had only been discovered incidentally, and the paradox appeared that a purely imaginary trouble occupied in the patient’s mind for a long time a much more important place than the genuine organic trouble which accompanied it.
Babinski points out that this connection between conditions was significant because it showed that hysteria and faking should not be confused with each other. It's true that it's hard to tell faking apart from suggested issues, as there are no clear characteristics that separate the two. Babinski himself stated that hysteria was a kind of half-faking; however, a half-fake is not the same as a fake. The patient genuinely believed that he couldn't move his leg. To counteract this paralysis, he had relied so heavily on his crutch that it actually led to an organic paralysis. The radial palsy was discovered incidentally, and it was curious that a purely imagined issue took up a much more significant mental space for the patient than the real organic problem that went along with it.
Bombardment; war strain; gassing?; collapse; arthritis: Hysterical MONOPLEGIA and ANESTHESIA of leg, interpreted as a “PROTECTIVE” reaction. Later, monoplegia and anesthesia of arm.
Bombardment; war stress; gas exposure?; breakdown; arthritis: Hysterical MONOPLEGIA and ANESTHESIA of the leg, seen as a “PROTECTIVE” response. Later, monoplegia and anesthesia of the arm.
Case 232. (MacCurdy, July, 1917.)
A corporal described as normal (“except for some shyness with the opposite sex”) adapted himself well to training and went to France in May, 1915, where he was at once thrown into 18 days of almost continuous bombardment. After some initial fright, he settled down to work well enough, but, when the weather got bad in September, 1915, grew tired of the situation. Bad dreams began (falling into a deep hole; being shelled). He thought of suicide, wanted a shell to incapacitate or kill him, began to have pains in the head, arms and legs, and was already groggy when a gas attack came. Whether he got a whiff of the gas or not, he at any rate felt giddy, got a swallow of water, and when the gas passed got out of his dugout in the open air. He was fatigued and much relieved when the company was ordered back. Now, however, he got shaky and fell in a collapse on a pile of straw, without, however, losing consciousness.
A corporal described as just average (“except for being a bit shy around women”) adjusted well to training and went to France in May 1915, where he was immediately exposed to 18 days of nearly nonstop bombardment. After some initial fear, he managed to settle down and do his job pretty well, but when the weather turned bad in September 1915, he grew frustrated with the situation. He started having nightmares (like falling into a deep hole or being shelled). He thought about suicide, wished for a shell to injure or kill him, began experiencing pain in his head, arms, and legs, and felt woozy when a gas attack occurred. Whether he inhaled any gas or not, he felt dizzy, took a sip of water, and once the gas cleared, he stepped out of his dugout into the fresh air. He was exhausted and relieved when the company was told to retreat. However, he then started shaking and collapsed onto a pile of straw, though he didn't lose consciousness.
Apparently he had an attack of acute articular rheumatism. There was a sore throat and a pain in the head, radiating to left shoulder and to finger tips, with pain also in legs. The pain was worse in the right leg on moving the knee-joint. These pains lasted for a month in hospital. The leg had been like a log since the collapse on the pile of straw. Even after the pains left him a month later, the right leg was paralyzed and anesthetic. He walked with a crutch and developed a crutch palsy. After a month a hysterical paralysis of the right arm, with superficial anesthesia, supervened. During a period of eight months thereafter improvement was steady under reëducative measures.
He apparently had a severe case of joint rheumatism. He experienced a sore throat and headaches that spread to his left shoulder and fingertips, along with pain in his legs. The pain was worse in his right leg when he moved his knee. These pains lasted for a month while he was in the hospital. His leg felt like a log since he collapsed on the pile of straw. Even after the pain went away a month later, his right leg remained paralyzed and numb. He used a crutch to walk, which led to issues with his crutch. A month later, he developed hysterical paralysis in his right arm, along with superficial numbness. Over the next eight months, he steadily improved with rehabilitation measures.
According to MacCurdy’s analysis, the acute arthritis led to paralysis as a protective reaction. The paralyses are disabilities that would ensure absence from the front.
According to MacCurdy’s analysis, the severe arthritis caused paralysis as a protective response. The paralysis is a disability that would guarantee being kept away from the front lines.
Lance-thrust in back, rapidly healed. Paralysis of right leg, disappearing with rest and exercises. Later, psychotic symptoms, with recovery.
Lance wound in the back, healing quickly. Paralysis in the right leg improved with rest and exercise. Later on, experiencing psychotic symptoms, followed by recovery.
Case 233. (Binswanger, July, 1915.)
N. H., 21, a laborer, industrious and sober (mother healthy, father insane and a suicide; patient somewhat sickly in childhood after pneumonia, a good scholar) volunteered at the outbreak of the war. Early in November he was on the Eastern front. November 17 to 22 he was in a number of small reconnoitring skirmishes almost daily, as a cavalryman. On the 22d, there was a clash with a Cossack patrol of far superior numbers. Eight German horsemen cut their way through, riding about 4 kilometers back to their squadron.
N. H., 21, a hardworking and responsible laborer (his mother is healthy, his father was mentally ill and committed suicide; he had some health issues in childhood after pneumonia, but he was a good student) volunteered when the war started. By early November, he was on the Eastern front. From November 17 to 22, he participated in several small reconnaissance skirmishes almost daily as a cavalryman. On the 22nd, there was a confrontation with a Cossack patrol that had far superior numbers. Eight German horsemen managed to break through, riding about 4 kilometers back to their squadron.
While dismounting, N. H. discovered that his back was wet. It occurred to him at once that he had been wounded. However, he successfully dismounted and then collapsed, feeling as if his right leg had fallen asleep. His companions found a wound in his back, which had come from a lance-thrust. The wound was bandaged. He was transported to Germany on a peasant’s wagon, the trip occupying six days, and on December 6 he came to the surgical clinic in Jena. The wound was insignificant and healed quickly.
While getting off his horse, N. H. noticed that his back was wet. He immediately realized that he had been injured. Still, he managed to get off and then collapsed, feeling like his right leg had gone numb. His friends discovered a wound in his back caused by a lance. They bandaged the wound and transported him to Germany in a peasant's wagon, which took six days. On December 6, he arrived at the surgical clinic in Jena. The wound was minor and healed quickly.
The leg remained motionless, and on December 10 the patient was referred to the nerve hospital. He was a small, slenderly-built man, with poor nutrition, weighing 108 pounds. The scar, about 1 cm. long, alongside the thoracic vertebra, was still somewhat red and but slightly sensitive to pressure. Neurologically, the knee-jerks and Achilles jerks were greater on the right than on the left, and there was on the right side a distinct patella and ankle clonus. There was no Babinski reaction on either side.
The leg stayed still, and on December 10, the patient was sent to the nerve hospital. He was a small, thin man with poor nutrition, weighing 108 pounds. The scar, about 1 cm long, next to the thoracic vertebra, was still a bit red and only slightly sensitive to pressure. Neurologically, the knee-jerk and Achilles reflexes were more pronounced on the right than on the left, and there was noticeable patellar and ankle clonus on the right side. There was no Babinski reflex on either side.
The movements of the right leg were not of wide excursion, and flexion and extension of the knee and ankle-joints, while lying on the back, were slowly and hesitatingly performed, with an expression of pain, and with visible effort by the[327] quadriceps muscles. Flexion and extension of the toes were likewise difficult, and when the toes were stretched there was a distinct contraction of the tibialis anticus. Electrically the muscles were normal. On passive motion, there was slight spastic tension in the musculature of the right leg, and the patient said he felt marked pain. In walking, the right leg was moved with a limp and with the evident design of sparing it. The knee was imperfectly bent and the sole of the foot was dragged along the ground. There were short out-throwing movements of the lower leg.
The movements of the right leg were limited, and bending and straightening the knee and ankle joints while lying on the back were done slowly and hesitantly, with a look of pain and visible effort from the quadriceps muscles. Bending and straightening the toes were also challenging, and when the toes were stretched, there was a noticeable contraction of the tibialis anticus. Electrically, the muscles appeared normal. During passive movement, there was slight tightness in the muscles of the right leg, and the patient reported significant pain. When walking, the right leg was moved with a limp, clearly trying to avoid putting weight on it. The knee was not fully bent, and the sole of the foot dragged along the ground. There were quick jerking movements of the lower leg.
Pain sense was normal, or possibly slightly in excess. There were painful points on pressure on the lower part of the os sacrum and coccyx and over the right sciatic and tibial nerves. Intelligence examination showed school knowledge to be extremely poor and calculation ability poor. Critical judgment and reasoning power were deficient. Memory and perception were without marked disturbance. The patient was dull and without interest in his surroundings. He complained that his right leg was as if dead and that he felt great pain in any attempt to move it. He also complained of pains at night in the region of the right shoulder and neck. His nerves, he said, had been very weak since his trip back from the front, during which trip he had been very cold and poorly cared for.
Pain sensation was normal, or maybe just a bit heightened. There were painful spots when pressure was applied to the lower part of the sacrum and coccyx, as well as over the right sciatic and tibial nerves. An intelligence assessment revealed extremely poor school knowledge and weak calculation skills. Critical thinking and reasoning abilities were lacking. Memory and perception did not show significant issues. The patient appeared dull and lacked interest in his surroundings. He said his right leg felt dead and that he experienced intense pain when trying to move it. He also reported nighttime pain in the right shoulder and neck area. He mentioned that his nerves had been very weak since his trip back from the front, during which he had been very cold and poorly cared for.
Treatment consisted of rest in bed, application of moist packs to the right leg, active and passive exercises of the right leg. After ten days he made his first independent attempts to walk, and active movements of the right leg in dorsal decubitus became unrestricted and painless. He remained somewhat unsteady in station, showing bilateral twitchings and movements of the right leg muscles. In walking the right leg was dragged behind in a spastic-paretic fashion. Appetite improved; spasms decreased; but at the end of December foot clonus was still persistent.
Treatment included bed rest, using warm compresses on the right leg, and doing both active and passive exercises for that leg. After ten days, he made his first attempts to walk independently, and the active movements of the right leg while lying on his back became unrestricted and pain-free. He still appeared somewhat unsteady while standing, showing twitching and movements in the muscles of his right leg. When walking, the right leg dragged behind him in a spastic, weak manner. His appetite improved, and the spasms decreased, but by the end of December, foot clonus was still present.
Upon January 10 there was an odd mental change. He became seclusive and suspicious. January 15 he expressed ideas of poisoning; his sister, he said, wanted to poison him, and others were watching him suspiciously; his room-mates were talking about him; in fact, he thought one[328] comrade was an Englishman. Sleep was poor. At the end of January, after a short period of improvement, he again had ideas of being poisoned, and had dream-like, unclear thoughts. His actions became incoherent: he would undress suddenly in the daytime and go to bed, getting up five minutes later and dressing. Senseless postcards were written.
On January 10, something strange happened in his mind. He became withdrawn and distrustful. By January 15, he began to express thoughts about being poisoned; he claimed that his sister wanted to poison him, and that others were watching him with suspicion; he believed one[328] of his roommates was an Englishman. He wasn't sleeping well. At the end of January, after a brief period of feeling better, he again thought he was being poisoned and experienced hazy, dream-like thoughts. His behavior became erratic: he would suddenly undress during the day and go to bed, only to get up five minutes later and get dressed again. He wrote meaningless postcards.
This condition lasted a few days only, whereupon the mental and bodily condition greatly improved. Daily walks were then taken in the garden and in the city without exertion. The ankle-clonus on the right side was now decidedly weaker but did not entirely disappear. The muscle power on the right side was somewhat less than on the left.
This condition lasted only a few days, after which both the mental and physical states greatly improved. Daily walks were then taken in the garden and in the city without any strain. The ankle clonus on the right side was noticeably weaker but didn't completely go away. The muscle strength on the right side was slightly less than on the left.
The patient was very homesick, and on March 14 was sent home.
The patient was really homesick and was sent home on March 14.
Shell-shock—six days later, crural monoplegia, cured by suggestion. “Metatraumatic” hysteria. HYPERSENSITIVE PHASE AFTER SHELL-SHOCK.
Shell shock—six days later, leg paralysis on one side, treated with suggestion. “Metatraumatic” hysteria. HYPERSENSITIVE PHASE AFTER SHELL SHOCK.
Case 234. (Schuster, January, 1916.)
On August 13, 1915, a soldier was knocked unconscious by the explosion of a shell nearby. He woke up several hours later with headache, noises in the ears, itching, but no trace of paralysis.
On August 13, 1915, a soldier was knocked out by the explosion of a nearby shell. He woke up several hours later with a headache, ringing in his ears, itching, but no signs of paralysis.
Six days later, on August 19, he was released from hospital, still free from paralysis. On the railway journey he met some people of his district by whom he sent greetings to his wife, meanwhile becoming greatly excited. When he tried to get out of the train he noted a weakness of the left arm and left leg; this weakness somewhat quickly grew into a severe paralysis, so that when observed in Berlin the left leg was entirely paralyzed, not a single muscle of which could be moved when the patient was examined by Schuster one month after the accident. There was also a hypesthesia on the left side with total anesthesia of the left leg, which anesthesia was related stocking-wise to the hypesthesia of the trunk. There was tremor of the hands as well as generalized increase of reflexes. The plantar reflex, though weak, was flexor. The pulse rapidly ran up under excitement. In short, the patient seemed to be suffering from hysterical palsy. Waking suggestion did so well with the man that after three weeks normal sensibility was restored to the leg, and he could walk tolerably well without a cane.
Six days later, on August 19, he was discharged from the hospital, still free from paralysis. During the train ride, he met some people from his area and sent greetings to his wife, which made him very excited. When he tried to get off the train, he noticed weakness in his left arm and left leg; this weakness quickly developed into severe paralysis, so that when examined in Berlin, his left leg was completely paralyzed, with no muscle movement when the patient was checked by Schuster a month after the accident. There was also decreased sensitivity on the left side, with total numbness in the left leg, which was related in a stocking-like pattern to the decreased sensitivity of the trunk. He had hand tremors and generalized increased reflexes. The plantar reflex was weak but still flexor. His pulse increased rapidly due to excitement. In short, the patient appeared to be suffering from hysterical paralysis. Suggestive therapy worked so well with him that after three weeks, normal sensitivity was restored to his leg, and he could walk fairly well without a cane.
The point of interest in this case is that the symptom of greatest importance, namely paralysis of the left leg, did not arise until six days after the shell explosion and then only after the man became excited by thoughts of his home and family through meeting his town people. The term metatraumatic is suggested by Schuster for cases of this sort. The emotions and stresses of war may be regarded as labilizing and sensibilizing the nervous system sometimes for months.
The interesting thing here is that the most significant symptom, which is paralysis of the left leg, didn't show up until six days after the shell explosion, and it only happened after the man got emotional thinking about his home and family when he saw people from his town. Schuster suggests the term metatraumatic for cases like this. The emotions and stresses of war can be seen as labilizing and sensibilizing the nervous system, sometimes for months.
Wound of left foot: ACROCONTRACTURE. Psychoelectric cure, about seven months later, at one sitting, except for some residuals that cleared shortly afterwards.
Wound on the left foot: ACROCONTRACTURE. Psychoelectric treatment, about seven months later, in one session, except for some residual effects that disappeared shortly after.
Case 235. (Roussy and Lhermitte, 1917.)
A soldier, 21 years, was observed at the Centre Neuropsychiatrique, August 30, 1916. He had been wounded in battle, March 16, 1916, near the left internal malleolus. Infection followed and inguinal adenitis, for which he was in hospital a month.
A 21-year-old soldier was seen at the Neuropsychiatric Center on August 30, 1916. He had been injured in battle on March 16, 1916, near the left inner ankle. He developed an infection and inguinal adenitis, which required him to stay in the hospital for a month.
Even before the abscess began, the foot had begun to twist inward. After the abscess had been cured, a contracture set in permanently, and at entrance to hospital was irreducible. The knee-jerk and Achilles jerk were more active on the side of the equinovarus contracture. There was even a slight amyotrophy of the calf. There was no appreciable vasomotor disorder. The foot and lower part of the leg were a little warmer on the left side.
Even before the abscess started, the foot began to twist inward. After the abscess was treated, a permanent contracture developed, and by the time the patient entered the hospital, it couldn't be reversed. The knee-jerk and Achilles reflexes were more active on the side with the equinovarus contracture. There was even a slight muscle wasting in the calf. There was no significant vasomotor disorder. The foot and lower leg were slightly warmer on the left side.
Cure followed a single sitting with psychoelectric treatment, at least so far as the contracture went. Pain and swelling remained in the evening, followed by fatigue. The patient was discharged cured, October 12, 1916.
Cure followed a single session of psychoelectric treatment, at least regarding the contracture. Pain and swelling persisted in the evening, along with fatigue. The patient was discharged as cured on October 12, 1916.
Hysterical pes equinovarus shows the foot immobile as if frozen (figé). The foot is extended with the toes lowered and the internal border incurved, as if revolved about the axis of the leg. The surface of the sole is directed inwards and much furrowed. The tendon of the tibialis anticus is very prominent. The internal malleolus is hardly visible, while the head of the astragalus is easily made out. No passive movement is possible and the tibiotarsal and mediotarsal joints are quite out of function. Upon palpation, the excessive contracture of the anterior muscles of the leg is striking. Upon request to move the foot, the foot is not moved, but muscles of the lower leg may contract, and even those of the thigh.
Hysterical pes equinovarus appears with the foot immobilized as if frozen. The foot is extended, with the toes pointed down and the inner edge curving inward, as if twisted around the leg's axis. The sole's surface faces inward and is deeply furrowed. The tendon of the tibialis anterior is very prominent. The inner ankle bone is barely visible, while the head of the talus is easily identifiable. No passive movement is possible, and the tibiotarsal and mediotarsal joints are completely non-functional. When palpated, the excessive tightness of the front muscles in the leg is noticeable. When asked to move the foot, it doesn't move, but the muscles in the lower leg may contract, and even those in the thigh.
There were no sensory disorders in the present case, though they often do occur in this form of acrocontracture. It is doubtful whether the skin changes sometimes seen, such as hypothermia, hyperidrosis, cyanosis, and glossiness are due to circulatory disorder induced by the contracture or to the prolonged immobility. It has been proved by Meige, Benisty and Lévy, that even in a normal subject prolonged immobility may cause a difference of temperature of several degrees. Circulatory disorders sometimes cease immediately upon cessation of the contracture. Roussy and Lhermitte insist upon energetic and early treatment of these psychoneuropathic acrocontractures, which are apt to proceed less favorably than the acroparalyses. If not treated energetically and early, actual nerve, tendon, and bone lesions may ensue.
There were no sensory disorders in this case, although they often occur with this type of acrocontracture. It’s unclear whether the skin changes sometimes observed, like coldness, excessive sweating, bluish discoloration, and shininess, are caused by circulatory issues from the contracture or from being inactive for a long time. Meige, Benisty, and Lévy have shown that even in healthy individuals, prolonged immobility can lead to temperature differences of several degrees. Circulatory problems can sometimes go away right after the contracture ends. Roussy and Lhermitte emphasize the need for prompt and vigorous treatment of these psychoneuropathic acrocontractures, which tend to have a worse outcome than acroparalyses. Without vigorous and timely treatment, actual damage to nerves, tendons, and bones may occur.
Shell-shock; shell-wound; emotion: Hysterical paraplegia. Approximate recovery.
Shell shock; shell wound; emotion: Hysterical paraplegia. Rough recovery.
Case 236. (Abrahams, July, 1915.)
A private of the First East Lancs could remember a shell’s bursting and striking a wagon near him when he was carrying food to the firing-line. He also thought a spare wagon wheel might have fallen on him. A period of unconsciousness of four or five days duration elapsed, on recovery from which he found himself suffering from a shell-wound in the left buttock, complete paralysis of both legs, and pain in the back, by the fourth lumbar vertebra. He thought that he had suffered from sphincteric paralysis for eleven days after the accident; but by September 25, there was no sign of this. Besides the paraplegia, there was complete loss of sensation below Poupart’s ligament in the right leg, reaching as high as the iliac crest behind; and an anesthesia of the left foot including heel and sole, with anesthesia to light touch throughout the limb (pin-pricks being appreciated in a normal way as far as the ankle); and there was an anesthesia to touch and pain in the ulnar distribution.
A private from the First East Lancs remembered a shell exploding and hitting a wagon nearby while he was bringing food to the front lines. He also thought a spare wagon wheel might have landed on him. He lost consciousness for about four or five days, and when he came to, he found he had a shell wound in his left buttock, complete paralysis in both legs, and pain in his lower back near the fourth lumbar vertebra. He believed he experienced sphincter paralysis for eleven days after the incident, but by September 25, there were no signs of it. In addition to the paralysis, he completely lost feeling below Poupart’s ligament in his right leg, extending up to the iliac crest in the back; he also had no sensation in his left foot, including the heel and sole, and couldn’t feel light touch throughout the limb (but could feel pin pricks normally up to the ankle); and he had no sensation to touch and pain in the ulnar distribution.
April 20, 1915, the patient was found to be a robust, somewhat microencephalic slowly cerebrating subject. Total flaccid paralysis of legs; right knee-jerk slightly exaggerated; no plantar response of any sort was obtainable. Right leg entirely anesthetic; left leg and both arms showed a diminution of sensibility; suggestion of glove and stocking anesthesia; trophic changes absent. The scar of the healed bullet-wound lay over the trunk of the left sciatic nerve.
April 20, 1915, the patient was found to be a strong, somewhat microcephalic individual with slow mental processing. There was complete flaccid paralysis in the legs; the right knee-jerk reflex was slightly exaggerated; no plantar response could be elicited. The right leg was completely numb; the left leg and both arms showed reduced sensitivity; there was a suggestion of glove and stocking anesthesia; no trophic changes were present. The scar from the healed bullet wound was located over the trunk of the left sciatic nerve.
It seems that the man’s companion had both his legs blown off at the time the shell burst. It is questionable whether the paraplegic patient actually saw the legs blown off, or merely heard about the accident. Another psychic feature lay in the fact that the patient had a paralyzed sister—a possible financial burden.
It looks like the man’s companion had both legs blown off when the shell exploded. It's unclear whether the paraplegic patient actually witnessed the legs being blown off or just heard about it. Another psychological aspect is that the patient had a paralyzed sister, which could be a potential financial strain.
April 30, nitrous acid anesthesia. During the temporary rigidity, the legs were found to stiffen slightly; the legs were[333] flexed. Upon the return of consciousness, the patient was told that the legs had moved during anesthesia, and was asked to place them in a more convenient position. The thighs moved slightly, and throughout the day movements were encouraged against resistance.
April 30, nitrous acid anesthesia. During the temporary stiffness, the legs were found to stiffen slightly; the legs were[333] flexed. When the patient regained consciousness, they were informed that their legs had moved during anesthesia and were asked to position them more comfortably. The thighs shifted slightly, and throughout the day, movements were encouraged against resistance.
The next day he was gradually raised to the vertical position and supported upright. But at this stage he had become mentally resistant and resentful. During the day the upright position was at intervals resumed, and the patient was made to walk between two attendants. The next day he walked alone and his mental resistance had broken down. There was no longer any evidence of exhaustion and effort in the movements, and the patient began to take pleasure in his recovery.
The next day, he was slowly brought to a standing position and held upright. However, at this point, he had become mentally resistant and bitter. Throughout the day, he was periodically put back in the upright position, and he was assisted in walking between two caregivers. The following day, he walked on his own, and his mental resistance had faded. There was no longer any sign of exhaustion or strain in his movements, and he started to enjoy his recovery.
Improvement was progressive. A pronounced hysterical element persisted, encouraged by the perpetual attentions of visitors. When discharged, there was a slight hemi-anesthesia throughout the right side, and a doubtful patch of anesthesia on the dorsum of the foot, sole, and plantar surface of the heel.
Improvement was gradual. A noticeable hysterical aspect remained, fueled by the constant attention from visitors. Upon discharge, there was slight numbness on the right side and an uncertain area of numbness on the top of the foot, the sole, and the underside of the heel.
Shell-shock; burial; flexion of spine: Paraplegia.
Shell shock; burial; bending of the spine: Paraplegia.
Case 237. (Eli, December, 1914.)
A reservist, 34, formerly army instructor in gymnastics, a member of the 1st Battalion King’s Royal Rifles, was subject to injury from the bursting of a “Black Maria” on his trench. He was sitting with bent back in his shelter, with legs fully extended. He was in a small dug-out, a recess excavated under the earth backward from a narrow trench and not timbered. The “Black Maria” burst and covered him up to the chin in a heavy clay soil. After building up the breach twenty minutes later, his comrades dug him out.
A 34-year-old reservist, who used to be a gymnastics instructor in the army and was part of the 1st Battalion King’s Royal Rifles, was injured when a “Black Maria” exploded in his trench. He was sitting in his shelter with his back bent and legs fully extended. It was a small dug-out, a space dug into the earth behind a narrow trench, and it wasn’t reinforced with timber. When the “Black Maria” exploded, it buried him in heavy clay soil up to his chin. His comrades dug him out twenty minutes later after repairing the breach.
He had received on his body the violent impact of the mass of earth pushed laterally from the crater excavated by the bursting of the shell. Accordingly his vertebral column was forcibly flexed, its ligaments were stretched, and hemorrhages were produced in the great muscles of the back. As the twelfth thoracic vertebra is the weakest spot in the spine, the roots of the cauda equina opposite this weak spot were probably injured. Such accidents are met in mines.
He had felt the harsh impact of the mass of earth pushed sideways from the crater created by the explosive shell. As a result, his spinal column was sharply bent, its ligaments were stretched, and bleeding occurred in the major muscles of his back. Since the twelfth thoracic vertebra is the weakest point in the spine, the nerves of the cauda equina near this vulnerable area were likely damaged. Such injuries commonly happen in mines.
The legs were powerless and numb. There was nausea, no vomiting, no gas, no dizziness or trouble in the head, not even pain in the small of the back. The accident had occurred at 8 A.M. Upon nightfall, he was removed on a stretcher to the field hospital, arriving at the base hospital four days later; and on the fifth day power began to return to the legs. Knees, ankles, and toes would move slightly November 6, though passive movements of the legs caused pain in the back. The deep reflexes were weak, the plantar reflexes flexor. The left cremasteric reflex was weaker than the right. Impairment of sensation was slight in both extremities, but the left leg was a little more numb than the right. The left lower abdominal reflex was lost. A band of hyperalgesia corresponded with the left eleventh and twelfth thoracic segments November 12, slight reflex disorders and some degree of paresis of the legs.
The legs felt weak and numb. There was nausea, but no vomiting, gas, dizziness, or headaches, and no pain in the lower back. The accident happened at 8 AM By nightfall, he was taken on a stretcher to the field hospital and got to the base hospital four days later; on the fifth day, feeling started to come back to his legs. On November 6, his knees, ankles, and toes could move slightly, although moving his legs caused pain in his back. The deep reflexes were weak, and the plantar reflexes were flexor. The left cremasteric reflex was weaker than the right. Sensation was only slightly impaired in both legs, but the left leg was a bit more numb than the right. The left lower abdominal reflex was gone. A band of heightened sensitivity coincided with the left eleventh and twelfth thoracic segments on November 12, with slight reflex issues and some degree of weakness in the legs.
Shell explosion: Paraplegia; sensory symptoms.
Shell explosion: Paralysis; sensory issues.
Case 238. (Hurst, January, 1915.)
A lieutenant, 23, came to the ambulance September 15, 1914, having the morning before been to the firing-line with his company and thrown to the ground on his back by the explosion of a shell which he had seen falling behind him. He had not lost consciousness, but was unable to rise. After a night in the relief post, he was brought by automobile 12 kilometers to the ambulance. He complained of pain in the back, though no wound or ecchymosis could be found there, nor any painfulness of spinous processes or irregularity of bone. He had not emptied the bladder from the time of the shock. Preparations were made to catheterize on the morning of the 16th, when the patient after effort became able to micturate. There was crural paraplegia such that he could not sit or walk even when supported. Lying down, he could move his legs slightly sidewise. Anesthesia to pin-prick and temperature was complete to the groin; but tactile anesthesia was found only in the sacral root territory, namely in the feet, the outer aspect of the legs, the posterior surface of the thighs, and the scrotum. There was loss of sense of position for the toes. The plantar reflexes were abolished; but there were no other reflex disorders; nor was there any evidence of other disorder.
A 23-year-old lieutenant arrived at the ambulance on September 15, 1914, having been thrown to the ground on his back the day before by a shell explosion that he saw falling behind him. He wasn't unconscious, but he couldn't get up. After spending a night at the relief post, he was driven 12 kilometers to the ambulance. He reported back pain, but there were no visible wounds or bruises, and no tenderness of the spinal processes or irregularities in the bones. He hadn't been able to empty his bladder since the shock. Preparations were made to catheterize him on the morning of the 16th, but he was eventually able to urinate after some effort. He had crural paraplegia, which made it impossible for him to sit or walk even with support. While lying down, he could slightly move his legs side to side. He had complete loss of sensation to pin-prick and temperature up to the groin, but tactile sensation loss was found only in the sacral root area, specifically in the feet, outer legs, back of the thighs, and scrotum. He lost the sense of position in his toes. The plantar reflexes were absent, but there were no other reflex issues or signs of additional disorders.
September 20, the man was evacuated by sanitary train in the same status as at entry. January 27, 1915, the patient could walk on crutches, supporting himself in part on the left leg. The lumbar pain had largely disappeared.
September 20, the man was evacuated by ambulance train in the same condition as when he arrived. On January 27, 1915, the patient was able to walk with crutches, partially supporting himself on his left leg. The lower back pain had mostly disappeared.
Hurst regarded this case as one of organic origin due to commotio spinalis.
Hurst considered this case to be of organic origin because of spinal shock.
Wet, cold, heavy marching; leg pains, rheumatic; no other somatic factor or any emotional factor discoverable: Transient paraplegia; two months after period of exposure, brachial tremor, hysterical. Recovery incomplete.
Wet, cold, heavy marching; leg pain, rheumatism; no other physical or emotional factors identified: Temporary paralysis; two months after the period of exposure, arm tremors, hysterical. Recovery is incomplete.
Case 239. (Binswanger, July, 1915.)
A German soldier, 34 (non-alcoholic; married, father of five healthy children; on military service 1901-3; regarded as a very good soldier; father alcoholic), got bad leg pains from wet and cold in West front trenches September 8-13, 1914. Still he was able to march some 30 kilometers. But two days later (he had lain down in wet clothes in a barn), his legs became quite immobile. He was in a reserve hospital from November 3. The rheumatism disappeared, and suddenly, early in the morning of November 8, when he was washing, a lively tremor and shaking of the right arm set in.
A German soldier, 34 (non-drinker; married, father of five healthy kids; served in the military from 1901 to 1903; known as a very good soldier; father was an alcoholic), experienced severe leg pain due to the wet and cold in the Western Front trenches from September 8 to 13, 1914. Despite this, he managed to march about 30 kilometers. However, two days later (after lying down in wet clothes in a barn), his legs became completely immobile. He was in a reserve hospital starting November 3. The rheumatism went away, but suddenly, early in the morning of November 8, while washing, he began to experience a lively tremor and shaking in his right arm.
Examination at Jena January 30, 1915, showed no special physical disorder. The sense of touch was slightly diminished on the right side; the pain sense was normal; movements were free. While at rest there was a continuous shaking tremor of the right arm and hand, which consisted of very rapid pronations and supinations, and shaking movements of the upper arm. At times the tremor would completely cease, and when attention was diverted the tremor became slighter or quite disappeared. The tremor increased when it was talked about in the man’s presence. The left grip was stronger than the right.
Examination at Jena on January 30, 1915, showed no significant physical issues. The sense of touch was slightly reduced on the right side; the pain sensation was normal; movements were unrestricted. While at rest, there was a continuous shaking tremor in the right arm and hand, characterized by very quick rotations of the forearm and shaking movements of the upper arm. Sometimes the tremor would stop completely, and when attention was diverted, the tremor became less noticeable or even disappeared. The tremor increased when it was discussed in the man’s presence. The grip strength in the left hand was stronger than in the right.
January 31, after he had been in bed one day and treated with moist packs, the shaking suddenly ceased. He then complained only of mild pains in the right shoulder and wanted to get up.
January 31, after he had been in bed for a day and had received treatment with wet packs, the shaking suddenly stopped. He then only complained of slight pain in his right shoulder and wanted to get up.
February 23, he was given three days’ home leave, which he stood very well. He now began to take part in the medical gymnastic work, but complained afterwards of more pains in right shoulder and arm. There was a lapse into the[337] shaking tremor, which lasted with varying intensity for several weeks. Loud noises or calling made it worse.
February 23, he was granted three days of home leave, which he handled quite well. He started participating in the medical gym exercises, but later complained of increased pain in his right shoulder and arm. There was a return of the[337]shaking tremor, which persisted with varying intensity for several weeks. Loud noises or calling made it worse.
Hypnotism and suggestive treatment of the tremor were without effect March 25. March 26, on passive extension of the right arm, patient complained of pain in shoulder and arm. Next day the tremors were more marked, but March 29, the tremors suddenly stopped altogether. April 4, the pains stopped never to return. April 15, he was given leave to go home for spring farm work.
Hypnotism and suggestive treatment of the tremor didn’t work on March 25. On March 26, when the right arm was passively extended, the patient complained of pain in the shoulder and arm. The next day, the tremors were more noticeable, but on March 29, they suddenly stopped completely. By April 4, the pains were gone and never came back. On April 15, he was allowed to go home for spring farm work.
Four weeks later he returned, sparing his right arm, which he held stiffly beside his body when walking. If he let the arm hang free in walking, rhythmical movements in it began. He complained of painful involuntary contractions in the right arm even when in complete rest. Nor did the condition afterward essentially change; the patient went home at the beginning of July.
Four weeks later, he came back, keeping his right arm stiff by his side as he walked. If he let the arm hang loose, it started to move rhythmically. He complained about painful involuntary contractions in his right arm even when he was completely still. The condition didn't really change afterward; the patient went home at the start of July.
The remarkable feature of this case is the complete lack of any emotional shock. The total genesis seems to have consisted in the prolonged exposure to wet and cold, and the heavy marching. The tremors, limited to the right upper extremity, occurred without any demonstrable psychic or bodily trouble, and set in after the disappearance of the so-called rheumatic disorder. Although there is no one psychogenic factor to single out, the psychic influencibility of the case is unmistakable; moreover, the incompleteness of the cure is doubtless, according to Binswanger, a matter of the imperfect suggestive therapy employed.
The notable aspect of this case is the complete absence of any emotional shock. The main factors seem to have been the prolonged exposure to wet and cold conditions and the heavy marching. The tremors, which were confined to the right arm, occurred without any clear psychological or physical issues and emerged after the so-called rheumatic disorder had disappeared. While there isn't one specific psychogenic factor to identify, the psychological susceptibility of this case is clear; furthermore, the incomplete nature of the recovery is likely, as Binswanger suggests, due to the inadequate suggestive therapy used.
Fever patient watches barrage coming: unconsciousness, paraplegia: recovery.
Fever patient watches the onslaught coming: unconsciousness, paralysis: recovery.
Case 240. (Man, June, 1915.)
A lieutenant was lying with fever in a farmhouse in upper Alsace, watching from his window the shelling of a battery about 400 meters away. He saw that the enemy was to reach the farm with shell in due course of time. The shells came nearer, say up to about 100 meters, and the lieutenant was able to reckon closely when he would be reached. He was quite defenseless and unable to get to safety. At the very moment, he thinks, when the shells began to strike the house, the lieutenant lost consciousness from fear. He was unconscious an hour before being carried to the cellar. The shelling lasted several hours more. Immediately upon coming to the patient found that, although he bore no external wound, both legs and the right arm were paralyzed.
A lieutenant was lying in a farmhouse in upper Alsace with a fever, watching from his window as a battery was shelled about 400 meters away. He realized that the enemy shells would eventually reach the farm. The shells came closer, down to about 100 meters, and the lieutenant could calculate when they would hit. He was completely defenseless and unable to escape. Just as the shells began to hit the house, he lost consciousness from fear. He was out cold for an hour before being carried to the cellar. The shelling continued for several more hours. When he came to, he found that although he had no external injuries, both of his legs and his right arm were paralyzed.
There were never any signs of organic disorder. The patient recovered completely with purely suggestive treatment.
There were never any signs of physical illness. The patient fully recovered with just suggestion-based treatment.
Incentives to paraplegia.
Incentives for paraplegics.
Case 241. (Russell, August, 1917.)
A young Canadian paid $150 to have his teeth repaired to be accepted for service and then married. The wife became pregnant. He reported sick after falling out on a route march in a heavy rainstorm. The medical officer said he had weak feet and ankles. He lay around the huts, was excused duty, and got worse in the wet and cold. He was admitted to hospital and came to Russel’s wards on a stretcher showing paralysis of both legs with slight power of movement at the knee. Stroking anesthesia to pin prick from the knee down. Reflexes not abnormal. He walked back upstairs!
A young Canadian paid $150 to get his teeth fixed so he could be accepted for service and get married. His wife became pregnant. He reported sick after he fell out during a route march in a heavy rainstorm. The medical officer said he had weak feet and ankles. He spent his time lying around the huts, was excused from duty, and got worse in the wet and cold. He was admitted to the hospital and arrived in Russel’s wards on a stretcher, showing paralysis in both legs with slight movement at the knee. He had loss of feeling from the knee down but normal reflexes. He walked back upstairs!
According to Russel the wife’s pregnancy had furnished a sufficient incentive, and the M. O.’s suggestion had fallen on fertile soil.
According to Russel, the wife's pregnancy provided a strong motivation, and the M.O.'s suggestion had taken root in good ground.
CAMPTOCORMIA (MLLE. ROSANOFF-SALOFF)
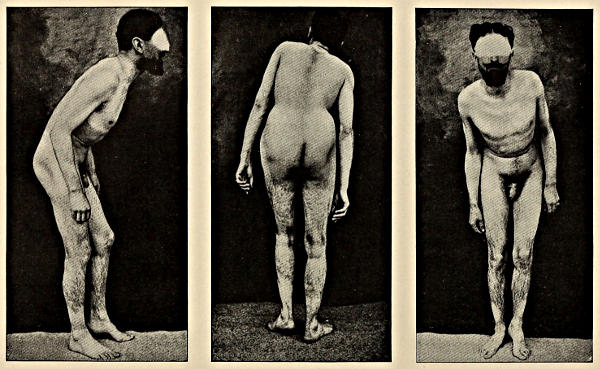
WOUNDED SEPTEMBER 3, 1914. THROWN INTO AIR BY SHELL-BURST; UNCONSCIOUS. FEBRUARY, 1915: PLASTER JACKET, 3 WEEKS; SECOND JACKET, 3 WEEKS. CURED. SENT TO GRAND-PALAIS.
WOUNDED SEPTEMBER 3, 1914. THROWN INTO THE AIR BY A SHELL EXPLOSION; UNCONSCIOUS. FEBRUARY 1915: PLASTER CAST FOR 3 WEEKS; SECOND CAST FOR 3 WEEKS. RECOVERED. SENT TO GRAND-PALAIS.
Bullet wound of back: Hysterical bent-back—camptocormia.
Bullet wound of back: Hysterical bent-back—camptocormia.
Case 242. (Souques, February, 1915.)
A man was wounded September 6, 1914, by a bullet that entered along the axillary border of the scapula and emerged near the spine. He spat blood for several days; but the skin wounds quickly healed.
A man was injured on September 6, 1914, by a bullet that went in along the outer edge of the shoulder blade and came out near the spine. He coughed up blood for several days, but the skin wounds healed quickly.
When he got up, his trunk and thighs were found to be in a state of moderate flexion upon the pelvis, the trunk being bent almost at a right angle; the legs were flexed somewhat upon the thighs. The man could not voluntarily extend his trunk, but he could extend his thighs to a moderate degree. He could bend his trunk still further forward than its habitual contractured position, being able to pick up an object from the ground. If the man was put in the ventral position, the trunk could be straightened to a considerable degree. Curiously enough, the man felt no pain, nor had there been any pain since the healing of the wound. No motor, sensory, reflex, trophic, vasomotor, electrical, visceral, or X-ray disorders could be found. It was evident that there was a contraction of the muscles of the abdominal wall and of the iliopsoas, yet it was also clear that these muscles were not contractured on account of the subject’s ability to flex his trunk and to extend his thighs.
When he got up, his torso and thighs were slightly bent at the hips, with his upper body leaning almost at a right angle; his legs were also bent a bit at the thighs. The man couldn't voluntarily straighten his torso, but he could extend his thighs to some extent. He could lean his torso even further forward than its usual contracted position, allowing him to pick something up off the ground. When placed on his stomach, his torso could be straightened quite a bit. Interestingly, the man felt no pain, nor had he experienced any pain since the wound healed. There were no issues found related to movement, sensation, reflexes, nutrition, blood flow, electrical activity, internal organs, or X-rays. It was clear that the muscles in his abdominal wall and iliopsoas were contracted, but it was also evident that these muscles weren't so tight that they prevented him from bending his torso or extending his thighs.
Here, then, is a vicious attitude crystallized (in the phrase of Souques) in the form of a pseudocontracture.
Here, then, is a harmful attitude solidified (in Souques' words) as a pseudocontracture.
Blown up by shell; unconsciousness: Camptocormia (bent-back, “cintrage”). Cure by corsets.
Blown up by shell; unconsciousness: Camptocormia (bent-back, "cintrage"). Treatment with corsets.
Case 243. (Roussy and Lhermitte, 1917.)
Camptocormia with antero lateral bending is described by Roussy and Lhermitte in an infantryman observed at Villejuif, February, 1915, after having been wounded September 3, 1914. The infantryman had been thrown into the air by the bursting of a shell, had lost consciousness, and came to with violent pains in the back. The trunk was found to be bent strongly forward and to the right side, and remained in this position thereafter. There was no evidence of wound.
Camptocormia with forward and sideways bending is reported by Roussy and Lhermitte in a soldier observed at Villejuif in February 1915, after he was injured on September 3, 1914. The soldier had been thrown into the air by an exploding shell, lost consciousness, and then woke up with severe back pain. His torso was found to be bent sharply forward and to the right, and it stayed in that position afterward. There was no sign of a wound.
In February, 1916, a plaster corset was applied by Souques, which brought the patient partly to normal station in three weeks. The trunk was now no longer bent forward, but was still bent to the right. A second corset was applied for three more weeks, with which the patient became absolutely straightened out again. He was discharged cured and sent to the Grand-Palais for the reëducation course.
In February 1916, a plaster corset was applied by Souques, which brought the patient partly back to a normal position in three weeks. The trunk was no longer bent forward but was still leaning to the right. A second corset was used for another three weeks, after which the patient was completely straightened out again. He was discharged as cured and sent to the Grand Palais for the rehabilitation course.
This condition is a form of trunk contracture in the nature of a kyphosis (scoliotic and lordotic forms of contracture are also found in the hysterical group), for which the terms plicature of trunk, traumatic kyphosis, pseudo-spondylitis, and camptocormia have been in use. The term camptocormia has been proposed by Souques and Rosanoff-Saloff. The poilus speak of the condition as cintrage (arching). In these cases the trunk is held almost horizontally, with the head in hypertension and neck muscles and thyroid cartilage jutting. The patient looks fixedly straight forward, with eyes wide open, and carries his legs extended or half flexed. The normal folds of the abdominal wall are very deeply marked, and at the level of the groins, the epigastrium and the pubis, there are deep folds. Viewed from behind, the median lumbar fold has disappeared or is faintly marked, as are the sacro-lumbar and other masses of spinal muscles. The whole lumbar region is elongated and flattened. The dorsal[341] spines of the back are accentuated; the buttocks are flattened and broadened transversely. The back of the neck is marked by deep transverse folds, and the seventh spine does not stand out. The patient can walk perfectly, though sometimes there is a pseudocoxalgia and lameness. Attempts to straighten the body lead to visible forcible contractions of various muscles, but the kyphosis remains persistent. There is a sense of active resistance on the part of the patient, which can be demonstrated by palpation. If an active attempt at straightening is made, lumbar or sacral pain develops, followed by a very lively and emotional state of anxiety on the part of the patient, with interrupted and accelerated breathing, an expression of terror in the face, and a rapid pulse. The patient then subsides into his earlier attitude, and his anxiety disappears in a few seconds. It is much easier in many subjects to reduce the camptocormia in the position of dorsal decubitus than upright.
This condition is a type of trunk contracture resembling kyphosis (scoliotic and lordotic forms of contracture are also seen in the hysterical group), with terms like plicature of the trunk, traumatic kyphosis, pseudo-spondylitis, and camptocormia being used. The term camptocormia was introduced by Souques and Rosanoff-Saloff. The poilus refer to the condition as cintrage (arching). In these cases, the trunk is held almost horizontally, with the head tilted back and neck muscles and thyroid cartilage jutting out. The patient gazes straight ahead, with eyes wide open, and keeps their legs extended or slightly bent. The normal folds of the abdominal wall are very pronounced, and at the level of the groins, epigastrium, and pubis, there are deep folds. Viewed from behind, the median lumbar fold is absent or barely visible, along with the sacro-lumbar and other groups of spinal muscles. The entire lumbar area is elongated and flattened. The dorsal [341] spines of the back are prominent; the buttocks are flattened and wider. The back of the neck has deep transverse folds, and the seventh spine is not prominent. The patient can walk perfectly well, though there may be occasional pseudo-coxalgia and limping. Attempts to straighten the body cause visible muscle contractions, but the kyphosis remains unchanged. The patient exhibits a sense of active resistance that can be felt by touch. If there is an active attempt to straighten, lumbar or sacral pain occurs, followed by a heightened emotional state characterized by anxiety, quickened breathing, a look of terror, and a racing pulse. The patient then returns to their previous posture, with the anxiety fading within seconds. For many individuals, it’s much easier to correct the camptocormia when lying on their back than when standing.
Burial after shell explosion; lumbar ecchymoses; regionary pains; camptocormia, 5½ months. Cure by three months’ plaster cast about trunk.
Burial after a shell explosion; bruises in the lower back; localized pain; stooped posture, 5½ months. Treated with a plaster cast around the torso for three months.
Case 244. (Roussy and Lhermitte, 1917.)
An infantryman was buried after shell explosion August 25, 1914, but he sustained no wound or bone injury. There was, however, a large ecchymosis of the lumbar region, and he had felt violent lumbar pains. The trunk was carried flexed, symmetrically bent over and quite incapable of being straightened completely. A plaster corset was applied March 16 by Souques. Three months of this was followed by a complete straightening, which lasted after the corset was removed. The patient was discharged well.
An infantryman was buried after a shell explosion on August 25, 1914, but he had no wounds or broken bones. However, there was a large bruise in the lower back area, and he experienced severe lower back pain. His body was bent forward and couldn't be fully straightened. A plaster corset was put on him on March 16 by Souques. After three months of wearing it, his back was completely straightened, and this improvement lasted even after the corset was taken off. The patient was released in good health.
As to these cases of camptocormia, some authors regard them as due to anatomical changes in the vertebral column itself, or in the ligaments and muscles, and accordingly regard the condition as a form of spondylitis, syndesmitis, or psoitis. This view is held by Sicard, who bases the idea upon the local pains and the results of cerebrospinal fluid examination. According to Roussy and Lhermitte, hyperalbuminosis of the fluid is extremely rare, and one case of their own with hyperalbuminosis was nevertheless cured with great rapidity. Roussy and Lhermitte even inquire whether the fluid albumin may not be due in some way to an interference with venous and lymphatic circulation.
In cases of camptocormia, some authors believe it's caused by anatomical changes in the vertebral column, ligaments, and muscles, considering it a type of spondylitis, syndesmitis, or psoitis. Sicard supports this view, linking it to local pain and findings from cerebrospinal fluid tests. Roussy and Lhermitte note that hyperalbuminosis in the fluid is very rare, yet they observed one case with hyperalbuminosis that was quickly cured. They even question whether the presence of albumin in the fluid might somehow be linked to issues with venous and lymphatic circulation.
In some cases, this condition may be at first a response to pain, a pseudospondylitis dolorosa, such as may be sometimes observed in hospitals near the front. Later, however, the suffering in camptocormia is due more to the abnormal position of the trunk, with strain upon vertebral ligaments, than to the persistence of any original pain. Moreover, these patients recover almost immediately from their pains when the contraction is relieved.
In some cases, this condition might initially be a reaction to pain, similar to what might sometimes be seen in hospitals near the front lines. However, later on, the discomfort in camptocormia is more about the unusual position of the torso, which puts strain on the vertebral ligaments, rather than any ongoing original pain. Additionally, these patients often feel instant relief from their pain once the contraction is eased.
In differential diagnosis, one has to consider, according to Roussy and Lhermitte, Pott’s disease, traumatic spondylitis, as well as Bechterew’s vertebral ankylosis, Pierre Mari[343]e’s rhizomelic spondylosis, Kocher’s intervertebral disc contusions, and Schuster’s myogenic ankylosis of the vertebral column; but in Pott’s disease, the fixed pain points, rigidity of column, fluid examination, and signs of myelitis, should suffice for the differential diagnosis. Traumatic spondylitis follows the contusion after months and after a phase of neuralgia. Ankyloses do not so much concern the trunk as the vertebral column itself; disc contusion produces disorders in standing and gait as well as pains and edema. Schuster’s disease shows paresis, hyper reflexia, and amyotrophy not shown in camptocormia.
In differential diagnosis, one has to consider, according to Roussy and Lhermitte, Pott's disease, traumatic spondylitis, as well as Bechterew's vertebral ankylosis, Pierre Marie’s rhizomelic spondylosis, Kocher’s intervertebral disc contusions, and Schuster’s myogenic ankylosis of the vertebral column; but in Pott's disease, the fixed pain points, rigidity of the spine, fluid examination, and signs of myelitis should be enough for the differential diagnosis. Traumatic spondylitis occurs after months of a contusion and a phase of neuralgia. Ankyloses primarily affect the vertebral column itself rather than the trunk; disc contusion causes problems with standing and walking, as well as pain and swelling. Schuster’s disease shows weakness, hyperreflexia, and muscle wasting that aren’t present in camptocormia.
Shell explosion; partial burial; forcible flexion of spine. Paraplegia, cured by suggestion. Then camptocormia, also cured.
Shell explosion; partial burial; forced bending of the spine. Paraplegia, resolved through suggestion. Then camptocormia, also resolved.
Case 245. (Jolt Train, March, 1917.)
An infantryman in the Côte du Poivre was sitting on the ground in the opening of a dugout eating soup, when a shell burst and the roof of the sap fell in on him. The planks and the stonework fell heavily on the dorsolumbar region. The patient was almost bent in two, head to knees, legs buried, hardly able to breathe. He did not lose consciousness and cried out, feeling for a moment very anxious and fearful that his comrades had left. Only two hours later was it possible to dig him out. He said he had been absolutely unable to make any movement, had kept his body bent, and felt violent pains in the back. He was carried back twelve hours later and reached the dressing station in eight more hours, eventually reaching the neurological service two days and a half after the accident. On entrance he was prostrated, complained of lumbar pains and of inability to move, and was able to make only a few contractions on the left side when asked to try. The right leg was flaccid. The left knee-jerk was stronger than the right. Other reflexes normal. Hyperesthesia to pin prick on the right side. Slight saddle hypesthesia, reaching to the iliac crests above and perineum below with preservation of touch sensation. Slight forward posture of vertebral column. The patient complained of pain on pressure of the spinal processes and the lumbar spine. There was slight ecchymosis about the left iliac crest.
An infantryman in the Côte du Poivre was sitting on the ground in the opening of a dugout eating soup when a shell exploded, causing the roof of the sap to collapse on him. The debris fell heavily on his lower back. He was almost bent in half, with his head to his knees, legs buried, and struggled to breathe. He didn't lose consciousness and cried out, feeling very anxious and afraid that his comrades had abandoned him. It was only two hours later that they could dig him out. He said he couldn't move at all, kept his body bent, and felt severe pain in his back. He was transported back twelve hours later and reached the dressing station eight hours after that, eventually arriving at the neurological service two and a half days after the accident. Upon arrival, he was in a weakened state, complained of lower back pain, and couldn't move, managing only a few contractions on the left side when asked to try. The right leg was limp. The left knee-jerk reflex was stronger than the right. Other reflexes were normal. He had increased sensitivity to pinprick on the right side, and slight decreased sensation in the saddle area, extending to the iliac crests above and the perineum below, while touch sensation was preserved. There was a slight forward curve of the spine. The patient reported pain when pressure was applied to the spinal processes and the lower back. There was some bruising around the left iliac crest.
Lumbar puncture showed clear fluid without hypertension, in which were a few lymphocytes. There was a large amount of albumin. The blood pressure was normal. There had been a slight diarrhea following the accident which disappeared on entrance to the hospital. The question was raised whether the case was one of slight hematomyelia or was pithiatic.
Lumbar puncture revealed clear fluid without elevated pressure, containing a few lymphocytes. There was a significant amount of albumin present. Blood pressure was normal. There had been slight diarrhea after the accident, which resolved upon entering the hospital. The question arose whether the case was a minor hematomyelia or was pithiatic.
Suggestive therapy was tried, and liquid was injected into the muscles of the lumbar region and the posterior surfaces[345] of the thighs. In a quarter of an hour the patient found himself able to raise the foot above the bed. There remained an extensor paralysis of the right leg. When the patient was made to raise the foot he began to show the phenomenon of Souques, called camptocormia. He could walk, nevertheless, and took a few steps sustaining the weight of his body by placing his arms on his thighs. Though he complained of lumbar pain, it was finally possible for him to pick up an object from the ground and lean sidewise. He could not, however, stand up. Yet when the patient was made to lie down, his back was spontaneously straightened. Treatment of the camptocormia was also successful.
Suggestive therapy was attempted, and liquid was injected into the muscles of the lower back and the back of the thighs[345]. Within fifteen minutes, the patient was able to lift his foot off the bed. However, there was still extensor paralysis in his right leg. When asked to raise his foot, he began to exhibit the Souques phenomenon, known as camptocormia. He was able to walk, taking a few steps while supporting his weight by putting his arms on his thighs. Although he complained of lower back pain, he could eventually pick up an object from the floor and lean to the side. However, he couldn’t stand up. Yet when he lay down, his back straightened on its own. Treatment for the camptocormia was also successful.
Astasia-abasia: Two cases from (a) thigh wound, and (b) shell-shock and wound of thorax. Cures by faradism.
Astasia-abasia: Two cases from (a) thigh injury, and (b) shell shock and chest wound. Treated with faradism.
Case 246. (Roussy and Lhermitte, 1917.)
An infantryman was wounded September 23, 1914, by a bullet in the anterior and middle part of the left thigh. From the moment of the trauma, he had not been able to walk, but gradually regained his ability to stand, and then to walk. He was returned to the front (January, 1915).
An infantryman was injured on September 23, 1914, by a bullet in the front and middle part of his left thigh. From the moment of the injury, he was unable to walk but gradually regained his ability to stand and then to walk again. He was sent back to the front in January 1915.
Slightly wounded again in the neck, January 6, 1915, he was evacuated and operated on. After the operation he could neither walk nor stand. His reflexes were normal; he could perform all movements when lying down, although the movements were executed very slowly. As soon as he could sit upright, he was taken with tremors and could not hold himself in a vertical standing position, nor take a single step. If he was given crutches, he dragged the two legs.
Slightly injured again in the neck on January 6, 1915, he was evacuated and underwent surgery. After the operation, he was unable to walk or stand. His reflexes were normal; he could perform all movements while lying down, although they were done very slowly. Once he could sit up, he experienced tremors and couldn't maintain a vertical position or take a single step. When given crutches, he dragged his legs.
Under the influence of electric treatment—a mild faradic current—he was cured at a sitting so that he could both stand and walk (March, 1916).
Under the influence of electric treatment—a mild faradic current—he was cured in one session, enabling him to both stand and walk (March, 1916).
Case 247. (Roussy and Lhermitte, 1917.)
Astasia-abasia after shell explosion occurred in an infantryman observed by Roussy and Lhermitte at Villejuif, July 8, 1915.
Astasia-abasia after a shell explosion was observed in an infantryman by Roussy and Lhermitte in Villejuif on July 8, 1915.
The patient had been wounded September, 1914. The wound was a superficial one in the thoracic wall, under the right nipple. He had been cast into a very deep shell hole, but had been able to get back to the aid station alone, taking very short steps only.
The patient was injured in September 1914. The injury was a superficial one on the chest wall, beneath the right nipple. He had fallen into a deep shell hole but managed to return to the aid station by himself, taking only very small steps.
As soon as he reached the station, his gait became spastic, trembling and hesitant. Given two canes, he could walk painfully, trembling. At each step, he would balance his body back and forth. He gave the impression of a man drawing some sort of vehicle, who had to make a considerable effort at each step.
As soon as he arrived at the station, his walk became unsteady, trembling, and hesitant. With two canes, he managed to walk painfully, shaking as he went. At every step, he balanced his body back and forth. He seemed like a person pulling some kind of vehicle, struggling with each step.
The faradic treatment cured this patient at one sitting.
The faradic treatment healed this patient in one session.
War strain; fall into water-filled trench: Dysbasia, tremors, vasomotor disorders. Cure by hypnosis. Case to demonstrate “traumatic” hysteria WITHOUT somatic TRAUMA.
War strain; fall into a water-filled trench: Difficulty walking, shaking, circulation issues. Treatment through hypnosis. Example to show "traumatic" hysteria WITHOUT physical INJURY.
Case 248. (Nuns, December, 1915.)
An artilleryman (without hereditary or acquired neuropathic taint) underwent much stress and strain in the war in Belgium, Lorraine and Flanders. One night, on leaving his observation post, he fell into a trench filled with water. He felt pricks in the groin and gradually developed a pseudospastic tremor of the lower extremity, paraparesis inferior, depression, irritability, pressure sensations in the head, and sleeplessness. He passed through three hospitals before arriving at Hamburg and received the diagnosis of concussion of the brain and cord.
An artilleryman (without any inherited or acquired nerve issues) experienced a lot of stress during the war in Belgium, Lorraine, and Flanders. One night, as he was leaving his observation post, he fell into a trench full of water. He started feeling pain in his groin and gradually developed a twitching tremor in his legs, weakness in his lower body, depression, irritability, pressure sensations in his head, and insomnia. He went through three hospitals before reaching Hamburg, where he was diagnosed with concussion of the brain and spinal cord.
Nonne found an emotional state of depression with hypochondriacal fear, disturbance of sleep, deficient appetite, constipation and pollakisuria. He walked upon two crutches, dragging his legs inertly after him. There was marked cyanosis, lowered temperature and hyperidrosis of the feet and lower legs; exaggeration of tendon and skin reflexes and pseudoclonus; no Babinski or Oppenheim reaction. There was anesthesia of the lower extremities and of trunk as high as the ribs. Pulse 130. Visual fields normal. Sensory disorders absent.
Nonne identified a depressed emotional state accompanied by excessive worry about health, sleep disturbances, a poor appetite, constipation, and frequent urination. He walked using two crutches, dragging his legs limply behind him. There was noticeable bluish discoloration, low body temperature, and excessive sweating in the feet and lower legs; his tendon and skin reflexes were heightened, and he exhibited pseudoclonus, but there was no Babinski or Oppenheim response. He experienced numbness in the lower limbs and torso up to the rib area. His pulse was 130. Visual fields were normal. There were no sensory disorders present.
After the first hypnotic treatment the patient was able to stand and take a number of steps, and the tremor gradually diminished. After two treatments standing became normal and walking was much improved, the tremor ceased, cyanosis and hyperidrosis disappeared, and the movements of the bowels and urination became normal. Thereafter the patient had no attention paid to him deliberately and in a week’s time became well.
After the first hypnosis session, the patient could stand and take several steps, and the tremor slowly reduced. After two sessions, standing became normal and walking improved significantly; the tremor stopped, the bluish skin and excessive sweating disappeared, and bowel and urinary movements returned to normal. After that, no special attention was given to the patient, and within a week, he recovered.
Here is a case in which, as Nonne states, the somatic trauma required by Oppenheim as the basis of every traumatic neurosis did not occur. Moreover, the sudden cures[348] by hypnotism, or by any other method in these cases, warrant us in supposing that there are no such fine molecular changes as Oppenheim and von Sarbo assert. Such experience as the cures in this group of cases confirms, according to Nonne, the surprising result first achieved in this war (Bonhoeffer, Wagner von Jauregg, Karplus, Wollenberg, Westphal) that the most severe neuroses produced by somatic and psychic traumata can be cured in an astoundingly rapid manner without residuals.
Here is a case where, as Nonne says, the physical trauma that Oppenheim considered essential for every traumatic neurosis didn’t happen. Furthermore, the sudden cures[348] through hypnosis or other methods in these cases lead us to believe that there are no subtle molecular changes, as Oppenheim and von Sarbo claim. According to Nonne, the experiences from these cures support the surprising findings from this war (Bonhoeffer, Wagner von Jauregg, Karplus, Wollenberg, Westphal) that even the most severe neuroses caused by physical and mental trauma can be treated remarkably quickly without lasting effects.
Re the controversy over Oppenheim’s traumatic neurosis, Nonne holds with the Charcot school that traumatic neurosis is clinically identical with hysteria. Oppenheim admits the part played by psychogenesis, but has always laid a greater emphasis upon the actual injury of the neuronic apparatus in which he believes. He thinks that small hemorrhages, inflammatory processes, and degenerative processes affect the neurones unfavorably, and permit the psychogenic effects to occur more readily. Of course the insurance-company attitude and the attitude of railway corporations saw malingering in all cases, and to this day, neurologists are inclined to see a great deal of “indemnity neurosis” in these cases. Opposed to the corporation men and the neurologists were the psychiatrists, who chiefly upheld an emotional theory of genesis—whence we began to hear of the neuroses of fright and of accident.
Re the controversy over Oppenheim’s traumatic neurosis, Nonne aligns with the Charcot school, asserting that traumatic neurosis is clinically the same as hysteria. Oppenheim acknowledges the role of psychogenesis but has always emphasized the actual injury to the neuronic system, which he believes is significant. He argues that small hemorrhages, inflammatory processes, and degenerative changes negatively impact the neurones, making it easier for psychogenic effects to manifest. Naturally, insurance companies and railway corporations viewed all cases as potential malingering, and even today, neurologists tend to see a lot of “indemnity neurosis” in these situations. In contrast to the corporate interests and neurologists, psychiatrists primarily supported an emotional theory of origin, which is how we started hearing about the neuroses related to fright and accidents.
Oppenheim claims to have established with war cases the fact that an entirely normal person without heredity and without antebellum acquired soil, may develop a neurosis through war stress. Oppenheim concedes that there may be purely psychic cases, but holds that there are nevertheless, numerous purely physical cases and a great number of cases of a compound nature, which are both physical and psychical in their etiology. Oppenheim’s point is not that every single symptom described may not be upon occasion psychogenic, but that the data of this war prove that neuronic injury, particularly injury of the peripheral neurones, can also produce these effects. Nonne, Forster, Lewandowsky, and others, opposed Oppenheim’s views vehemently. See especially comments by Zeehandelaar.
Oppenheim claims to have shown through war cases that an entirely normal person, without hereditary issues or previous conditions, can develop a neurosis due to war stress. Oppenheim acknowledges that there may be purely psychological cases, but argues that there are still many purely physical cases and a significant number of cases that are a combination of both physical and psychological factors. Oppenheim's main argument is not that every single symptom described could occasionally be psychogenic, but that the evidence from this war indicates that neuronal damage, especially damage to the peripheral neurons, can also cause these effects. Nonne, Forster, Lewandowsky, and others strongly opposed Oppenheim's views. See especially the comments by Zeehandelaar.
Shell-shock; BURIAL HEAD DOWN: Brachial monoplegia, head-shaking, speech disorder, corneal and conjunctival reflexes absent. Determination of hysterical phenomena to parts buried.
Shell-shock; BURIAL HEAD DOWN: Brachial monoplegia, uncontrollable head shaking, speech issues, no corneal or conjunctival reflexes. Identification of hysterical symptoms in areas that are buried.
Case 249. (Arinstein, 1916.)
A Russian private was buried after a shell explosion, September 13, 1915, head down, so that only his legs stuck out of the débris. Afterward his right hand refused to move, and there was edema of the right wrist, with pain referred to the shoulder joint. The head shook and made jerky movements during the day, but ceased them in sleep. Speech was retarded; words were uttered clearly enough but in a sing-song fashion; sometimes the man stammered. Hearing was diminished in the right ear. Pupillary responses were lively, but the swallowing reflexes were diminished, and the corneal and conjunctival reflexes were absent. The tendon reflexes were lively on both sides. There were no pathological reflexes.
A Russian soldier was buried after a shell explosion on September 13, 1915, head down, so only his legs stuck out of the rubble. Later, his right hand wouldn't move, and his right wrist was swollen, with pain that radiated to his shoulder. His head shook and made jerky movements during the day but stopped when he slept. His speech was slow; he pronounced words clearly, but in a sing-song way; sometimes he stuttered. His hearing was reduced in his right ear. His pupils reacted quickly, but his swallowing reflexes were weaker, and the corneal and conjunctival reflexes were absent. The tendon reflexes were active on both sides, and there were no abnormal reflexes.
At the end of October—six weeks later—the patient was sent home on convalescence for three months, and improved rapidly after a short time in family surroundings. He was examined again, two months after discharge, and found normal in all respects. He returned to the ranks.
At the end of October—six weeks later—the patient was sent home to recover for three months, and he quickly got better after a little time with his family. Two months after being discharged, he was examined again and found to be normal in every way. He returned to active duty.
Re Shell-shock in Russians, Arinstein concludes that concussion hysteria may occur in a perfectly normal person, yet be innocent of all organic signs indicating destruction of peripheral or central neurones. Rifle or machine-gun fire had not in his experience brought about concussion hysteria, which was invariably due to the bursting of a large projectile. With reference to Schuster’s remark that a sleeping man never acquires hysteria from the bursting of a shell near by, Arinstein confirms Schuster, finding amongst 2000 cases no instance in a soldier sleeping at the time the shell burst.
Re Shell-shock in Russians, Arinstein concludes that concussion hysteria can occur in someone who is otherwise completely normal, but without any physical signs indicating damage to peripheral or central nerves. In his experience, rifle or machine-gun fire didn't cause concussion hysteria; it was always linked to the explosion of a large projectile. In response to Schuster’s comment that a sleeping person never experiences hysteria from a shell exploding nearby, Arinstein supports Schuster's assertion, stating that among 2000 cases, he found no instances of soldiers who were asleep when the shell exploded.
Re effects of cannonading, Gerver reports Russian instances of a kind of hysterical clavus, or sensation of a nail being driven into the back of the head, in men who have been a number of days under stiff shelling.
Re effects of cannon fire, Gerver reports Russian cases of a type of hysterical clavus, or the feeling of a nail being driven into the back of the head, in men who have endured several days of intense shelling.
Multiple wounds and bullet wound of palm: ACROPARALYSIS. Cure, five months.
Multiple wounds and bullet wound to the palm: ACROPARALYSIS. Recovery, five months.
Case 250. (Roussy and Lhermitte, 1917.)
A patient was observed at Villejuif, February 5, 1915. He had been wounded, January 2, 1915, and showed scars of a bayonet wound on the anterior surface of the right thigh, of a lance wound on the dorsal surface of the right foot, and of a bullet wound in the palm of the left hand.
A patient was observed in Villejuif on February 5, 1915. He had been injured on January 2, 1915, and had scars from a bayonet wound on the front of his right thigh, a lance wound on the top of his right foot, and a bullet wound in the palm of his left hand.
There was left wrist drop with fingers extended. On the sensory side, there was a glove anesthesia and analgesia up to the bend of the elbow. The right leg showed a paresis and contracture, but there were no sensory disorders in the legs. Reflexes were normal. The patient was discharged cured, in May, 1915 (psychoelectric method).
There was a left wrist drop with fingers extended. On the sensory side, there was glove anesthesia and analgesia up to the bend of the elbow. The right leg showed weakness and stiffness, but there were no sensory issues in the legs. Reflexes were normal. The patient was discharged cured, in May 1915 (psychoelectric method).
This is an example of the so-called acroparalyses, paralyses limited to the hand or foot, many of which have developed in this war, after grazing wounds or more severe injury. More rarely they appear as if spontaneously. Sometimes they are preceded by slight arthralgia or vague pains.
This is an example of the so-called acroparalyses, which are paralysis limited to the hand or foot. Many of these have developed during this war, often after grazing wounds or more severe injuries. More rarely, they seem to appear on their own. Sometimes, they are preceded by mild joint pain or vague discomfort.
The condition in the hand suggests a radial paralysis. The patient is unable to flex his fingers, though he probably is able to make some movements with his thumb. Sometimes, on request to move the hand, a series of coarse oscillations follows, somewhat like a tremor. These oscillations are, according to Roussy and Lhermitte, apparently pathognomonic, and depend upon the contraction of the muscles antagonistic to those whose movement has been requested. These antagonistic muscles, themselves entirely incapable of voluntary movement, are seen to be contracting effectively and jerkily to meet the action of the agonists, also seen making jerky movements. If the forearm is moved passively and rapidly, the hand flops about inert, like the hand of a marionette, although not to the degree of hypotonia in organic paralysis. The hand is often cold, moist, and cyanotic, and even possibly analgesic and hypesthetic.
The condition in the hand points to radial paralysis. The patient can't bend his fingers, but he might be able to make some movements with his thumb. When asked to move the hand, he sometimes produces a series of rough tremors. According to Roussy and Lhermitte, these tremors are likely characteristic of the condition and are due to the contraction of the muscles that oppose those being asked to move. These opposing muscles, which can't move voluntarily, can be seen contracting in a jerky manner to counter the action of the active muscles, which are also making jerky movements. If the forearm is moved quickly and passively, the hand flops around limply, like a marionette, although not as much as in organic paralysis. The hand often feels cold, moist, and bluish, and it may also be insensitive or have reduced sensation.
Bullet wound of arm: Apparent radial paralysis, not resolved by self-preservative swimming movements. Paralysis actually hysterical.
Bullet wound in the arm: Clear radial paralysis, not improved by instinctive swimming movements. Paralysis is actually hysterical.
Case 251. (Chartier, October, 1915.)
A professional acrobat, 22, Corporal in an African Chasseur regiment, was rather instructively tattooed and had apparently performed some of his service in disciplinary companies. In short, one might have a legitimate suspicion of the objective value of any manifestations he might present. However, one of his chiefs had written a favorable letter concerning his services. He had had various crises of a hysterical character since adolescence, and there was alcoholism in the family.
A 22-year-old professional acrobat and Corporal in an African Chasseur regiment had quite a few tattoos and had seemingly served in disciplinary units. In short, one could reasonably doubt the true value of any performances he might offer. However, one of his superiors had written a positive letter about his service. He had experienced several hysterical episodes since his teenage years, and there was a history of alcoholism in his family.
He was wounded May 4, 1915, by a bullet which passed through the outer and lower part of the right upper arm, and thereafter the forearm and hand became completely inert, both for flexion and extension. There was a considerable hyperesthesia. The wound healed quickly, without complications.
He was injured on May 4, 1915, by a bullet that went through the outer and lower part of his right upper arm, resulting in his forearm and hand becoming completely unresponsive, unable to move either up or down. There was significant sensitivity to touch. The wound healed quickly and without any issues.
August 5, about 10 o’clock at night, the man—then at his dépôt—tried to commit suicide (motive not related with the war). He threw himself into the Rhône from a height, where the water was deep and the current rapid. His brother and a comrade, who knew that he was going to make the attempt, saved him. Chartier himself happened to see the whole scene, and noted that throughout the affair the forearm and hand of the patient remained inert. It seemed as if there was a radial paralysis. This was the more likely as the man had been wounded in the arm. First care was given. The man had not known of Chartier’s presence. He had been under water about two minutes.
August 5, around 10 o’clock at night, the man—who was at his station—tried to commit suicide (the reason wasn’t related to the war). He jumped into the Rhône from a high point, where the water was deep and the current was strong. His brother and a friend, who knew he was going to try this, saved him. Chartier happened to witness the whole scene and observed that throughout the incident, the man’s forearm and hand remained completely still. It appeared he had a radial paralysis, which was likely since he had been injured in the arm. He received immediate care. The man was unaware of Chartier's presence. He had been underwater for about two minutes.
From hospital he was evacuated three weeks later with a diagnosis of radial paralysis, coming on service September 11. Examination showed a slight paralysis of the extensors and flexors of hand and fingers, and of the hand muscles. There was also a slight contracture of these muscles, more marked in[352] the flexors. There was pain upon reduction, with some jerking of the muscles. Electrical reactions proved normal in nerves and muscles. There was a segmentary anesthesia to pin prick, reaching to the level of the elbow; deep hyperesthesia of the finger joints. There was no trophic or vasomotor disorder.
From the hospital, he was discharged three weeks later with a diagnosis of radial paralysis, starting on September 11. Examination revealed slight paralysis of the extensors and flexors of the hand and fingers, as well as the hand muscles. There was also a minor contracture of these muscles, more pronounced in the flexors. Pain was present upon reduction, accompanied by some muscle jerking. Electrical responses in the nerves and muscles were normal. There was segmental anesthesia to pinprick, extending up to the elbow, and deep sensitivity in the finger joints. There were no trophic or vasomotor issues.
In short, here was a case of functional paralysis with contracture of the right hand, to be regarded as hysterical in the classical sense of the term, both by reason of the anesthesia and absence of trophic disorder, and on account of the hysterical history of the patient. Functional reëducative treatment quickly improved the paralysis, so that two weeks later the patient was able to extend fingers and hand. His total recovery was hoped for, when, September 26, wishing to get out of the hospital without leave, the patient jumped from a window and broke his right leg. The functional paralysis of the hand persisted and even grew more marked.
In short, this was a case of functional paralysis with a contracture of the right hand, considered hysterical in the traditional sense due to the anesthesia and lack of tissue damage, as well as the patient’s previous hysterical history. Functional re-educational treatment quickly improved the paralysis, so that two weeks later the patient could extend his fingers and hand. Total recovery was anticipated, but on September 26, wanting to leave the hospital without permission, the patient jumped from a window and broke his right leg. The functional paralysis of his hand continued and even became more pronounced.
The interesting point in this case is that despite the powerful nature of instinctive efforts with drowning persons, this patient, subject to an hysterical arm paralysis, did not make defensive movements with the paralyzed arm; yet this paralysis was such as to be greatly improved by psychotherapy.
The interesting point in this case is that even though the instinctive reactions of drowning people are strong, this patient, who had hysterical paralysis in one arm, did not make any defensive movements with the paralyzed arm; however, this paralysis responded significantly to psychotherapy.
Bullet wound in brachial plexus region: SUPINATOR LONGUS CONTRACTURE, hysterical-looking. Callus of fractured rib probably at fault: Treatment surgical.
Bullet wound in the brachial plexus area: SUPINATOR LONGUS CONTRACTURE, appearing hysterical. Callus from a fractured rib likely to blame: surgical treatment required.
Case 252. (Leri and Roger, October, 1915.)
A man was wounded, December 21, 1914, by a bullet which entered about the middle of the spinous process of the left scapula and was extracted a few days later from the posterior border of the sternocleidomastoid muscle, two finger-breadths from the left clavicle, that is, at about Erb’s point. The left upper extremity was inert for ten days, but then began to move again, although extension and flexion of the fingers did not begin at once.
A man was shot on December 21, 1914, by a bullet that entered near the middle of the spinous process of the left shoulder blade and was removed a few days later from the back edge of the sternocleidomastoid muscle, two finger-widths from the left collarbone, which is about at Erb’s point. The left arm was inactive for ten days but then started to move again, although the ability to extend and flex the fingers didn’t come back right away.
October, 1915, movements were normal, except those of extension of the forearm, due to contracture of the supinator longus muscle, a contracture that had developed about three weeks after the wound and stood out along the external border of the forearm, almost suggesting a musculotendinous retraction. There was a palpable, hard callus of a fractured rib, presumably a cause of the permanent irritation of the supinator longus, being precisely at the point where lesions usually produce superior brachial plexus palsy.
October 1915, movements were normal except for the extension of the forearm, which was limited due to tightness in the supinator longus muscle. This tightness developed about three weeks after the injury and was noticeable along the outer edge of the forearm, almost resembling a retraction of the muscle and tendon. There was also a noticeable, hard callus from a broken rib, likely causing ongoing irritation to the supinator longus, exactly at the location where injuries typically lead to superior brachial plexus weakness.
Why should the supinator longus alone of the Duchenne-Erb group be affected? Perhaps a single root was involved in the irritative lesion. The biceps showed also a partial R. D. The deltoid was normal electrically and in contraction.
Why is only the supinator longus from the Duchenne-Erb group affected? Maybe just one root was involved in the irritative injury. The biceps also showed some reduced function. The deltoid was normal both electrically and in contraction.
The treatment planned for this case of isolated contracture of the supinator longus was surgical operation of the irritative focus. According to Léri and Roger, it is sometimes dangerous to use such measures as massage and electric baths for a paralyzed limb, since the massage or electricity excite not only the affected muscles, but also the other sound muscles,—muscles that are already more powerful than the paralyzed muscles and may go into antagonistic contracture. Even in limited galvanization, it is desirable to work with weak currents, so as not to diffuse the current into non-paralyzed muscles. In case of radial or sciatic paralysis,[354] apparatus permitting the extremities to rest without over-action of the muscles antagonistic to the paralyzed ones may well be applied.
The treatment planned for this case of isolated contracture of the supinator longus was surgery to address the irritating focus. According to Léri and Roger, using methods like massage and electric baths for a paralyzed limb can sometimes be risky, as they can stimulate not just the affected muscles, but also the other healthy muscles—muscles that are already stronger than the paralyzed ones and might go into conflicting contracture. Even with limited galvanization, it’s better to use weak currents to avoid spreading the current to non-paralyzed muscles. In cases of radial or sciatic paralysis,[354] devices that allow the limbs to rest without causing overexertion of the muscles opposing the paralyzed ones can be beneficial.
We here deal with a case, therefore, which looked purely functional, but in which careful examination and X-ray served to show an organic focus of irritation.
We’re dealing with a case that seemed purely functional, but a close examination and X-ray revealed an underlying issue causing irritation.
Re nerve concussion, Tubby offers the following definition: Nerve concussion is damage to a nerve trunk without actual destruction of the axis cylinders. The damage may consist of an effusion of blood between the nerve fibres following compression of a nerve against the bone by rapid passage of a foreign body near the nerve. Sometimes, however, the lesion which causes damage to the nerve trunk without actual destruction to the axis cylinders is nothing more than a temporary anemia or hyperemia. In most instances, both motor and sensory function are together interfered with, but in the case of large nerve trunks, e.g., the popliteal, there may be a separate concussion of motor or sensory bundles.
Re nerve concussion, Tubby provides the following definition: Nerve concussion is damage to a nerve trunk without any actual destruction of the axis cylinders. The damage can be due to bleeding between the nerve fibers after the nerve is compressed against the bone by the quick movement of a foreign object near the nerve. However, sometimes, the issue causing damage to the nerve trunk without actual destruction of the axis cylinders is simply a temporary lack of blood flow or excessive blood flow. In most cases, both motor and sensory functions are affected together, but with larger nerve trunks, e.g., the popliteal, there may be a separate concussion affecting either motor or sensory bundles.
Contusion may effect a sort of STUPEFACTION OF MUSCLE and paralyze it by a non-psychic process: The SYNERGY in contraction of biceps and supinator longus is thus SPLIT. Biceps restored to synergy with the supinator by massage and faradism.
Contusions can cause a kind of MUSCLE STUPEFACTION and paralyze it through a non-psychological process: The SYNERGY in the contraction of the biceps and supinator longus is disrupted. The biceps can regain synergy with the supinator through massage and electrical stimulation.
Case 253. (Tinel, June, 1917.)
A man was wounded at about the middle of his biceps and three weeks later was found to be able to flex the forearm only by means of the supinator longus. The biceps remained absolutely flaccid and soft, so that the diagnosis of a lesion of the musculocutaneous nerve (unlikely as this seemed on account of the low site of the wound) was entertained.
A man was injured around the middle of his biceps, and three weeks later, he could only bend his forearm using the supinator longus. The biceps remained completely limp and soft, so doctors considered the possibility of damage to the musculocutaneous nerve (which seemed unlikely due to the low position of the wound).
However, the biceps and the musculocutaneous nerve proved electrically normal. In short, this paralysis of biceps was functional in nature. But, according to Tinel, there could be no voluntary suggestive or hysterical element in such a paralysis, since flexion of the forearm is normally produced by a synergic contraction of biceps and supinator longus that cannot be separated voluntarily.
However, the biceps and the musculocutaneous nerve were found to be electrically normal. In short, this paralysis of the biceps was functional. But, according to Tinel, there couldn’t be any voluntary suggestive or hysterical aspect to this paralysis, since bending the forearm usually happens through a combined contraction of the biceps and supinator longus that can't be separated voluntarily.
Treatment by massage and rhythmic faradization caused the biceps function to return to normal, so that voluntary synergic contractions of the biceps took place along with those of the supinator longus.
Treatment through massage and rhythmic faradization restored normal function to the biceps, allowing for voluntary synergistic contractions of the biceps alongside those of the supinator longus.
We here deal, according to Tinel, with a genuine functional paralysis, nonhysterical—a paralysis due to a kind of stupor of the muscle. Such paralyses due to muscular stupor ought to get well in a few days or weeks. Should they persist, it is clear that a stuporous paralysis might be transformed into a hysterical paralysis. In short, the direct contusion of a muscle or group of muscles may be the point of departure for various persistent paralyses.
We are discussing, according to Tinel, a true functional paralysis that is not hysterical—it's a paralysis caused by a sort of muscle stupor. These types of paralysis from muscular stupor should recover in a few days or weeks. If they continue, it's evident that a stuporous paralysis could change into a hysterical paralysis. In summary, a direct injury to a muscle or group of muscles can be the starting point for different long-lasting paralyses.
Wound of arm: Blocking of impulses to certain hand movements. Recovery with splint.
Wound on the arm: Disruption of signals for certain hand movements. Healing with a splint.
Case 254. (Chubby, January, 1915.)
A private was wounded by a shell fragment, September 16, 1914, and admitted to the London General Hospital, September 27. A high-velocity shell fragment had passed through the soft parts of the left arm at a spot exactly corresponding to the musculospiral groove. He could extend the middle finger of the left hand, but the other fingers were held in flexion. The last two phalanges of index finger could not be moved, it was found, on account of severance of the extensor tendon some years previously. Accordingly, the loss of function due to the shell injury was that of thumb, ring, and little fingers. Supination could not be executed completely to the extent of 15 degrees; there was no R. D. upon electrical test, October 2. The sensation of affected fingers was woolly. November 3, the little finger had recovered, but supination could not be completely executed.
A private was injured by a shell fragment on September 16, 1914, and was admitted to the London General Hospital on September 27. A high-velocity shell fragment had gone through the soft tissue of the left arm at a spot that exactly matched the musculospiral groove. He was able to extend the middle finger of his left hand, but the other fingers were flexed. It was found that the last two phalanges of the index finger couldn't be moved because the extensor tendon had been severed some years earlier. Therefore, the loss of function from the shell injury affected his thumb, ring, and little fingers. He was unable to fully execute supination to the extent of 15 degrees; there was no R. D. upon electrical testing on October 2. The sensation in the affected fingers felt fuzzy. By November 3, the little finger had recovered, but he still couldn't fully execute supination.
The treatment consisted in a bent malleable iron splint, with the wrist and affected fingers hyperextended. November 20 all power had returned with full supination, except for the two phalanges of index finger previously injured.
The treatment involved a flexible iron splint that kept the wrist and affected fingers hyperextended. By November 20, all strength had returned with full supination, except for the two phalanges of the previously injured index finger.
Major Tubby thinks this a case of physiological blocking, as from a small hemorrhage amongst the fibers or around the nerve.
Major Tubby believes this is a case of physiological blocking, possibly due to a minor hemorrhage among the fibers or around the nerve.
Re inhibition, Myers thinks it is the functional cause of the effects of shell-shock. He thinks it is not a fixation of the idea of the paralysis of volition, but that it is a fixation of the process of inhibition itself that produces the effects we see in Shell-shock. It is a block of ascending paths that produces the anaesthesia so characteristic of Shell-shock. It is a blocking of sensory paths that produces mutism or aphonia. But according to Myers, there is also a block in certain cases of descending paths that control and coördinate various mechanisms. The result of a block in the descending paths is shown in spastic, clonic, or ataxic phenomena of, e.g., functional dysarthria. See also Case 253 (Tinel).
Regarding inhibition, Myers believes it is the key factor behind the effects of shell shock. He argues that it's not just a fixation on the idea of paralysis of will, but rather a fixation on the process of inhibition itself that leads to the effects seen in shell shock. It creates a blockage in ascending pathways, causing the numbness characteristic of shell shock. It also blocks sensory pathways, resulting in mutism or loss of voice. However, according to Myers, there can also be a blockage in certain cases of descending paths that manage and coordinate various mechanisms. A blockage in these descending paths manifests in spastic, clonic, or ataxic conditions like e.g. functional dysarthria. See also Case 253 (Tinel).
Eight months of war experience (often under heavy fire) without reaction; then, shell-shock; unconsciousness: Right hemiparesis; pain in the left side of head; heat sensations of right half of body; diminution of hearing in left ear; a variety of asymmetrical bilateral phenomena.
Eight months of wartime experience (often under heavy fire) without any response; then, shell shock; loss of consciousness: weakness on the right side; pain on the left side of the head; sensations of heat on the right side of the body; reduced hearing in the left ear; a range of asymmetrical bilateral symptoms.
Case 255. (Gerver, 1915.)
A Russian private, 24, sustained shell-shock April 14, 1915. He was observed, when the shell burst, to crouch down, and then to fall to the ground, unconscious. The unconsciousness lasted about two days, after which he was found to be oriented, though slow and stammering of speech, hardly able to concentrate attention or sustain a conversation, and giving the impression of a man stunned. There was difficulty in the expression of thoughts, and a marked over-fatigueability. After adding and subtracting accurately two-digit figures for a time, the man quickly grew confused and said that trying to solve such a problem made him dizzy.
A 24-year-old Russian private experienced shell shock on April 14, 1915. When the shell exploded, he was seen crouching down and then collapsing to the ground, unconscious. He remained unconscious for about two days, after which he seemed aware of his surroundings but spoke slowly and stammered, struggling to focus or hold a conversation, appearing like a stunned person. He had trouble expressing his thoughts and showed significant fatigue. After accurately adding and subtracting two-digit numbers for a while, he quickly became confused and said that trying to solve such problems made him feel dizzy.
His imagination was filled with gunshots, shell-bursts, and the killing of comrades, and during any conversation the man frequently shuddered. Concerning the shell-shock, he remembered only that a number of shells had burst near him and that he came to in the hospital. He kept looking to one side and to a distance, as if listening, sometimes bending his head downwards. He would cry and sigh during conversation, and then be quite unable to explain why. He said there were loud noises in his ears, and that his head and the whole right side of his body felt hot. Pain was felt in the left side of the head. The right hand and the right foot were weak (on distraction, this hemiparesis remained unaltered). Tremors affected all the extremities. He had a sensation, possibly hallucinatory, of the creeping of insects on his skin. The hearing of the left ear was objectively diminished. There was palpitation of the heart and difficulty of breathing. Tendency to Romberg. There was a general hypalgesia, more marked on the left side of the body. Both conjunctival[358] reflexes were diminished. Knee-jerks and Achilles jerks were exaggerated. All the reflexes on the right side were livelier than on the left. There was a moderate Babinski reaction on the right side. Mechanical over-excitability of muscles. Dermatographia. Both sides of the skull were sensitive on tapping, but especially the left side. Mannkopf sign on pressure of the left side of the cranium.
His mind was filled with gunshots, explosions, and the deaths of friends, and during any conversation, he often shuddered. When it came to his shell-shock, he could only remember that several shells had exploded near him and that he woke up in the hospital. He kept glancing to one side and into the distance, as if he were listening, sometimes bending his head down. He would cry and sigh while talking, and then be completely unable to explain why. He said there were loud noises in his ears and that his head and the entire right side of his body felt hot. He felt pain on the left side of his head. His right hand and right foot were weak (despite distraction, this weakness remained unchanged). Tremors affected all his limbs. He experienced a sensation, possibly hallucinations, of insects crawling on his skin. His left ear’s hearing was noticeably diminished. He had a racing heart and trouble breathing. There was a tendency to lose balance. Overall sensitivity to pain was reduced, more so on the left side of his body. Both conjunctival[358] reflexes were less responsive. The knee and Achilles reflexes were heightened. All reflexes on the right side were more active than on the left. There was a moderate Babinski response on the right side. His muscles showed excessive reactivity. He had dermatographia. Both sides of his skull were sensitive when tapped, especially the left side. The Mannkopf sign was positive when pressure was applied to the left side of the skull.
Hemorrhagic points without injury to the skin were noted on the skin of the left hand and foot. Speech was stammering. There was a marked digital tremor, sometimes spreading to the rest of the body during examination. The muscles of the face, eyelids, and tongue showed sharp fibrillary twitching. The pulse stood at 100 and frequently missed beats. Battle hallucinations, visual and auditory, sometimes occurred, the commands of superiors and the noise of guns, rifles, yelling, and groans; the man would see trenches or redoubts, or a field full of wounded soldiers or attacking columns of the enemy. He recognized the hallucinations as such. His sleep was troubled by nightmares of the same general description.
Hemorrhagic spots without skin injury were observed on the skin of the left hand and foot. Speech was stammering. There was a noticeable tremor in his fingers that sometimes extended to the rest of his body during the examination. The muscles of his face, eyelids, and tongue displayed sharp twitching. His pulse was at 100 and frequently skipped beats. He experienced vivid hallucinations, both visual and auditory, often hearing commands from superiors, and the sounds of gunfire, rifles, shouting, and groans; he would see trenches or strongholds, or a field filled with wounded soldiers or advancing enemy troops. He recognized the hallucinations as such. His sleep was disturbed by nightmares of a similar nature.
For eight months the man had been in action at the front, under heavy gun and rifle fire. He was a courageous man, who had never felt fear, regarding himself as used to battle and the bursting of shells. He had not been wounded. The entire situation seems to have developed after the single shell burst of April 14, 1915.
For eight months, the man had been active at the front, facing heavy artillery and gunfire. He was brave, never feeling fear, considering himself experienced in battle and the explosion of shells. He had not been injured. The whole situation appeared to have escalated after the single shell exploded on April 14, 1915.
LOCALIZATION OF SHELL-SHOCK SYMPTOMS: Hemiparesis and hemianalgesia on side of body exposed to explosion; contralateral irritative symptoms of face and tongue.
LOCALIZATION OF SHELL-SHOCK SYMPTOMS: Hemiparesis and hemianalgesia on the side of the body exposed to the explosion; contralateral irritating symptoms of the face and tongue.
Case 256. (Oppenheimer, January, 1915.)
A soldier had a shell explode to his right, October 23, 1914. He declared that the concussion launched him through the air. When he recovered consciousness three hours later, he lay in a bog and was unable to move either leg. Gradual improvement followed. The symptoms were sensations of formication in the legs, pain in the back, blurred sight, hardness of hearing, disturbance of speech, headache, vertigo, weak memory. After a fortnight weakness in right arm.
A soldier experienced a shell explosion to his right on October 23, 1914. He said the blast sent him flying through the air. When he came to three hours later, he was lying in a swamp and couldn’t move either leg. He started to improve gradually. His symptoms included tingling sensations in his legs, back pain, blurred vision, difficulty hearing, trouble speaking, headaches, dizziness, and poor memory. After two weeks, he also felt weakness in his right arm.
He was admitted to hospital a week after the injury, unable to walk, restless, given to palpitation and attacks of anxiety. On attempts to walk, leg spasms and tachycardia.
He was admitted to the hospital a week after the injury, unable to walk, restless, experiencing heart palpitations and anxiety attacks. When he tried to walk, he had leg spasms and rapid heartbeat.
Transferred to nerve hospital, December 2. Sleep poor, uneasy with dreams. Tic on left side of face. On opening the mouth, left-sided faciolingual spasm. Paresis of right arm. At first, right-sided ankle-clonus and paresis of leg. Knee-jerks increased. Speech hesitating. Right hemianalgesia. Concentric contraction of visual fields. Tachycardia (120). In walking the right arm failed to swing normally. Attacks of vertigo, with falling. Patient got up at night and pushed against objects in his room.
Transferred to the nerve hospital on December 2. Sleep is poor, restless with dreams. There's a twitch on the left side of the face. When opening the mouth, there’s a spasm on the left side of the face and tongue. Weakness in the right arm. Initially, there’s ankle clonus and weakness in the right leg. Knee-jerk reflexes are heightened. Speech is hesitant. There's a lack of feeling on the right side of the body. Visual fields are narrowing. Heart rate is fast (120). When walking, the right arm doesn't swing normally. Experiencing attacks of vertigo, leading to falls. The patient gets up at night and pushes against objects in the room.
There was only slight improvement while under observation. He became psychically more frank and even talkative, and was moving more readily when transferred.
There was only a slight improvement while he was being observed. He became more open and even a bit talkative, and he moved more easily when being transferred.
Re Oppenheim’s conception of the strongly peripheral element in traumatic neurosis, he sums up by saying that a traumatism attacking the organism at its periphery is in line to produce a neurosis without any psychic mediation whatever. The rôle of the psychic process, in Oppenheim’s view, is contributory to the fixation of neuroses. Even when there is a free interval betwixt shell burst and neurosis, still there are physical effects of trauma upon neurones.
Re Oppenheim’s idea about the strongly peripheral element in traumatic neurosis is that trauma affecting the body at its outer edges can cause neurosis without any psychological involvement. According to Oppenheim, the psychological process plays a supportive role in solidifying neuroses. Even if there is a gap between a shell explosion and the onset of neurosis, the physical effects of trauma on neurons are still present.
Shell-shock; unconsciousness; after improvement in symptoms (4 months) return to trenches; more symptoms after 5 days: Sensory disorders, especially on left side (the side more exposed to explosion); exaggerated reflexes on right side with slight clonus and with Babinski sign. Improvement.
Shell shock; unconsciousness; after improvement in symptoms (4 months) return to the trenches; more symptoms after 5 days: sensory disorders, especially on the left side (the side more exposed to the explosion); exaggerated reflexes on the right side with slight clonus and with Babinski sign. Improvement.
Case 257. (Gerver, 1915.)
A Russian Captain, 45 (heredity good; non-alcoholic, non-syphilitic; always in good health) sustained shell-shock in a battle in southeastern Prussia, August 13, 1914, and was unconscious for two days. He was carried to one of the provisional field hospitals, and then evacuated to Petrograd, where during a period of four months, he was given electricity, suggestion, and baths. He was feeling so much better in December, 1914, that he went back to the front and headed his company in the trenches. He stood only five days of trench work, and was sent for mental examination December 29, 1914.
A Russian captain, 45 (good family background; non-alcoholic, non-syphilitic; always in good health) suffered from shell shock during a battle in southeastern Prussia on August 13, 1914, and was unconscious for two days. He was taken to one of the temporary field hospitals and then evacuated to Petrograd, where he received electrical treatment, suggestion therapy, and baths over a period of four months. By December 1914, he was feeling much better, so he returned to the front and led his company in the trenches. However, he only lasted five days of trench duty before being called in for a mental evaluation on December 29, 1914.
The captain was of middle height, well developed but poorly nourished, of a dejected and preoccupied appearance, looking to one side in conversation, and finding difficulty in the expression of his thoughts. He talked almost exclusively of his illness. He found difficulty in adding or subtracting 2-digit figures. He seemed to have amentia, frequently being mistaken as to the most important dates in his life. He complained of general weakness and inability to work. Any endeavor to concentrate caused vertigo, irritation, and pains in the head. Day and night he was troubled about his health, his future, and his family’s future. He was going to become an invalid and a burden. He was tormented with the idea that people thought him a simulator. He complained of lumbar pains. It seems that the explosion had affected the left side of the body more than the right and he complained more of pains upon that side. In the dark his gait was unsteady, and he often had marked tremors of feet and hands. In excitement the tremor would increase uncontrollably. The patient thought that his hearing was diminished,[361] especially upon the left side, and that his left ear was weaker than the right. He slept poorly and had many nightmares; his appetite was poor, and he was constipated. There was difficulty in respiration; the pupils were slightly dilated and sluggish in their responses. There was a marked tendency to Rombergism; dermatographia marked; the skull and especially the lumbar spine was painful on tapping; hyperesthesia of the lumbar skin; paresis of left hand and left foot. The tendon reflexes were more marked on the right side than on the left, and there was even a slight ankle and patellar clonus. The Babinski sign was present on the right side. There were frequent fibrillary contractions of the muscles of the trunk and back.
The captain was of average height, well-built but undernourished, appearing downcast and distracted, looking to one side while talking, and struggling to express his thoughts. He primarily discussed his illness. He had trouble adding and subtracting two-digit numbers. He seemed to have mental fog, often confusing the most significant dates in his life. He complained of overall weakness and an inability to work. Even trying to concentrate brought on dizziness, irritation, and headaches. Night and day, he worried about his health, his future, and his family's future. He feared he would become an invalid and a burden. He was plagued by the thought that others saw him as faking his condition. He reported lower back pain. It appeared that the explosion had impacted the left side of his body more than the right, and he experienced more pain on that side. In the dark, his walking was unsteady, and he often had noticeable tremors in his feet and hands. During moments of excitement, the tremor would become uncontrollable. The patient believed his hearing was diminished, especially on the left side, and that his left ear was weaker than the right. He had poor sleep and frequently experienced nightmares; his appetite was low, and he was constipated. He had difficulty breathing; his pupils were slightly dilated and slow to react. There was a noticeable tendency toward balance issues; skin writing was pronounced; his skull and especially the lower back were painful when tapped; heightened sensitivity of the lumbar skin; weakness in his left hand and left foot. The tendon reflexes were more pronounced on the right side than the left, and there was also a slight clonus in the ankle and knee. The Babinski reflex was present on the right side. There were frequent muscle twitches in the trunk and back.[361]
Objectively the hearing was somewhat decreased in the left ear, and the vision of the left eye appeared to be somewhat impaired also. If the eyes had been held closed for a time, there was difficulty in opening them quickly. Aside from a somewhat elevated pulse and slight cardiac arrhythmia, there was no disorder of the internal organs.
Objectively, there was a slight decrease in hearing in the left ear, and the vision in the left eye also seemed somewhat impaired. If the eyes had been closed for a while, there was difficulty opening them quickly. Aside from a slightly elevated pulse and mild irregular heartbeat, there were no issues with the internal organs.
This patient remarkably improved but was not absolutely well at the date of the report.
This patient showed significant improvement but wasn't completely well at the time of the report.
Re organic signs in Shell-shock cases, Oppenheim warns practitioners and experts against undervaluing war neuroses. He does not like to have them set down in too offhand a way, as hysteria, wish-fulfilment, and simulation. Hysteria is not likely, according to Oppenheim, in cases with permanent cyanosis, disappearance of the radial pulse, trophic disturbances, hyperidrosis, alopecia, fibrillary tremors, myokymia, cramps, dilated and sluggish pupils, and weakening of tendon reflexes. Hyperthyroidism also has been found by Oppenheim.
Re organic signs in shell-shock cases, Oppenheim cautions practitioners and experts to take war neuroses seriously. He doesn't want them casually categorized as hysteria, wish-fulfillment, or simulation. Oppenheim believes hysteria is unlikely in cases with lasting cyanosis, loss of the radial pulse, trophic disturbances, excessive sweating, hair loss, fibrillary tremors, myokymia, cramps, dilated and sluggish pupils, and weakened tendon reflexes. Hyperthyroidism has also been identified by Oppenheim.
Shell-shock, explosion on left side: Sensory disorders especially on left side; ecchymosis of right (uninjured) leg, possibly conditioned upon shock of left hemisphere.
Shell shock, explosion on the left side: Sensory issues, especially on the left side; bruising on the right (uninjured) leg, possibly caused by the shock to the left hemisphere.
Case 258. (Gerver, 1915.)
An artillery officer had had a shell burst to the left side of his horse, which veered to the right but did not fall. The officer’s left hand immediately became so numb and weak that he could not hold his reins with it; it shortly became more painful. The left foot showed a tendency to the same anesthesia and paresis.
An artillery officer experienced a shell explosion on the left side of his horse, causing the horse to swerve to the right but not fall. The officer's left hand quickly went numb and weak, making it impossible for him to hold the reins; soon, the pain intensified. His left foot was showing signs of the same numbness and weakness.
Curiously enough, a number of punctate hemorrhages appeared on the right thigh and lower leg, upon the outer aspect. According to Gerver, these hemorrhages into the skin of the right leg may have something to do with a disturbance of circulation related with effects wrought upon the left hemisphere. During the course of the disease, pains occurred not only in the left arm and leg but also in the right leg.
Curiously, several small bleeding spots appeared on the outer part of the right thigh and lower leg. Gerver suggested that these skin bleedings in the right leg might be linked to circulation issues related to disturbances in the left hemisphere. Throughout the illness, pain was experienced not just in the left arm and leg, but also in the right leg.
Re brain injuries produced by shell explosions without external wound, Roussy and Boisseau have not found a single clinical instance amongst 133 cases observed, which suggested cerebral softening, or even hemorrhage into the brain substance, the cord substance, or the meninges. These 133 cases were observed in army neurological centres and contained instances of (a) mental disease (confusion, delirium, amnesia), (b) nervous disease (astasia-abasia, tremors, paralyses, contracture), and (c) an intermediary group (either mental confusion with stupor, or hysterical deafmutism).
Re brain injuries caused by shell explosions without external wounds, Roussy and Boisseau did not find a single clinical instance among 133 observed cases that suggested cerebral softening, or even hemorrhage into the brain tissue, spinal cord, or meninges. These 133 cases were noted in army neurological centers and included instances of (a) mental illness (confusion, delirium, amnesia), (b) neurological disorders (astasia-abasia, tremors, paralysis, contracture), and (c) an intermediate group (either mental confusion with stupor or hysterical deaf-mutism).
Shell-shock; unconsciousness: Hysterical deafness, speech-disorder, gait. Recovery by reëducation. Brief relapse to deaf-mutism at noise of drums. Improvement. Relapse to numerous and severe hysterical symptoms at small guns fired on King’s birthday. Improvement. Speech wholly regained in a quarrel. Recovery.
Shell shock; unconsciousness: Hysterical deafness, speech disorder, unsteady walking. Recovery through re-education. Brief relapse to deaf-muteness at the sound of drums. Improvement. Relapse to many and severe hysterical symptoms when small guns were fired on the King’s birthday. Improvement. Speech completely regained during a fight. Recovery.
Case 259. (Gaupp, March, 1915.)
A musketeer, 22, had been blind for a time at 11 on account of some spinal cord disease.
A 22-year-old musketeer had been blind for a while at 11 due to a spinal cord disease.
He was a soldier up to Christmas eve, 1914, when he was hurled backward in a trench in the Argonne by an exploding hand grenade. He lay unconscious for several hours, though without sign of physical injury. Coming to his senses, he worked himself out of the trench and crawled to another, but again fell unconscious. When he awoke he was in a physician’s care in quarters, to which he had been taken by ambulance men. Thence to the field hospital, and then to a private hospital at B.
He was a soldier until Christmas Eve, 1914, when an exploding hand grenade knocked him backward in a trench in the Argonne. He was unconscious for several hours but had no visible injuries. When he regained consciousness, he managed to get out of the trench and crawled to another one, but he passed out again. When he woke up, he was under the care of a doctor in a place where ambulance personnel had taken him. From there, he was moved to a field hospital and then to a private hospital in B.
Upon admission, January 17, he was hard of hearing on both sides, and his speech was peculiar: choked off and retarded. His gait was heavy, on a broad base. He was subject to headaches.
Upon admission on January 17, he had hearing difficulties in both ears, and his speech was unusual: interrupted and slow. His walk was heavy, with a wide stance. He often experienced headaches.
Exercises gradually improved the speech and the walking disorder was quickly overcome. February 5 came a relapse through fright at the rolling of drums near by. Speech was completely lost, deafness set in, and the patient ran restlessly to and fro in tears. After a few hours speech returned with still some minor difficulty.
Exercises gradually improved the speech, and the walking issue was quickly resolved. On February 5, a setback occurred due to a scare from the nearby sound of drums. Speech was entirely lost, deafness followed, and the patient moved around anxiously, crying. After a few hours, speech returned, though there were still some minor difficulties.
From time to time came fainting spells and attacks of disorder of consciousness, with loss of orientation and the idea of being in the trench or under cover. He would ask whether it were raining through. His mood herein was at times cheerful and excited. Speech further improved from the middle of February, as well as did the other symptoms.
Occasionally, he experienced fainting spells and moments of confusion, losing track of where he was and feeling like he was in a trench or hiding. He would ask if it was raining. His mood during these episodes was sometimes cheerful and excited. By mid-February, his speech had improved, along with his other symptoms.
On the King s birthday, February 25, occurred another relapse due to his hearing small guns fired: Apathetic stupor, clonic spasm, aphonia, abasia, severe deafness, poor sleep, refusal of food. The next day he was still mute, but the spasms had ceased. He lay apathetically in bed, taking a little liquid food. February 27 he was still mute, though more active, not deaf, getting up alone, walking unsteadily on a broad base, and playing cards at the table. March 2 the word yes was again enunciated. March 3 he talked more freely and took a short walk. March 4 speech of a sudden came completely back on the occasion of getting excited in a quarrel among some other patients. The patient thereafter began to talk a great deal, was bright and cheerful, but still complained of a variety of nervous troubles. Speech was somewhat difficult, but he was free from any definite aphasia or paraphasia.
On the King’s birthday, February 25, he had another setback after hearing some small cannons being fired: he was in a daze, had muscle spasms, couldn’t speak, had trouble walking, was severely deaf, couldn’t sleep well, and refused to eat. The next day he was still unable to speak, but the spasms had stopped. He lay in bed with no expression, taking in some liquid food. By February 27, he was still mute, but more active, not deaf anymore, getting up by himself, walking unsteadily with a wide stance, and playing cards at the table. On March 2, he managed to say the word yes again. On March 3, he started to talk more openly and took a short walk. By March 4, he suddenly regained his speech during an argument with some other patients. After that, he began to talk a lot, seemed bright and cheerful, but continued to complain about various nervous issues. Speaking was a bit challenging for him, but he no longer had any clear signs of aphasia or paraphasia.
Re Shell-shock deafness, Jones Phillipson states that concussion deafness is due to three contributory factors: (a) cerebral concussion, (b) fatigue (violent oscillation of the perilymph, continued noises, strain of organ of Corti), and (c) temporary or permanent disorganization of the conductive apparatus.
Re Shell-shock deafness, Jones Phillipson says that concussion deafness is caused by three main factors: (a) brain concussion, (b) fatigue (violent movement of the perilymph, constant noises, strain on the organ of Corti), and (c) temporary or permanent disruption of the conductive system.
Re concussion deafness, J. S. and S. Fraser found in four cases of actual explosion injury, a ruptured drumhead and hemorrhage into the fundus of the internal meatus in three cases. They did not find evidence of neuro-epithelial changes. Possibly the fundus hemorrhages, besides giving rise to deafness, may start up the tinnitus and giddiness that are sometimes found. In one case, there were changes in the delicate nerve endings of the auditory ampullae.
Regarding concussion deafness, J. S. and S. Fraser discovered in four cases of actual explosion injuries a ruptured eardrum and bleeding into the bottom of the internal auditory canal in three cases. They did not find any signs of neuro-epithelial changes. It's possible that the bleeding in the canal, in addition to causing deafness, might trigger the tinnitus and dizziness that are sometimes present. In one case, there were changes in the delicate nerve endings of the auditory ampullae.
Shell-shock: Deafness
Shell shock: Hearing loss
Case 260. (Wedding, February, 1917.)
A shell burst behind an English lieutenant in 1914 without causing any wound but making him unconscious for an hour. During the hour the Germans passed by and stripped him of all articles of value. He came to and felt himself markedly deaf in both ears with an intense headache. There was no hemorrhage, no discharge, no tinnitus, no vertigo. Four days after the shell burst he could hear spoken words on each side at two feet, but could not hear a watch that could usually be heard from 3½ to 4 feet. With tuning fork C air and bone conduction proved much subnormal, though air conduction was better than bone conduction. With tuning fork C-5 air conduction was subnormal. Drums healthy. Improvement followed; hearing became normal eighteen days after explosion. The treatment was rest in bed with bromides early and strychnine later.
A shell exploded behind an English lieutenant in 1914, leaving him unconscious for an hour but without any injuries. During that time, the Germans passed by and stole all his valuable items. When he woke up, he realized he was significantly deaf in both ears and had a severe headache. There was no bleeding, no discharge, no ringing in his ears, and no dizziness. Four days after the explosion, he could hear conversations from two feet away on either side, but he couldn’t hear a watch that was normally audible from 3½ to 4 feet away. When tested with a tuning fork C, he showed much lower air and bone conduction, although air conduction was better than bone conduction. With tuning fork C-5, air conduction was also below normal. His eardrums were healthy. He improved over time, and his hearing returned to normal eighteen days after the explosion. The treatment involved resting in bed, taking bromides early on, followed by strychnine later.
Marriage states that the psychical deafness due to shell-shock is usually bilateral and absolute. It is accompanied also, as a rule, by other nervous signs and symptoms, such as aphonia, tubular vision, paralyses, and anesthesias. Milligan and Westmacott state that the deafness is due to a functional suspension of neuronic impulses. They regard the brain as in a state of physical fatigue, and the mind as in a state of strain. There is no organic lesion. The neuronic impulses which are temporarily suspended are those which run from the higher cortical cells to the periphery.
Marriage states that the psychological deafness caused by shell shock is usually both ears affected and complete. It is typically also accompanied by other nervous signs and symptoms, such as loss of voice, tunnel vision, paralysis, and numbness. Milligan and Westmacott explain that the deafness results from a temporary halt in nerve impulses. They see the brain as being physically exhausted and the mind as being under stress. There is no physical damage. The nerve impulses that are temporarily halted are those that travel from the higher brain cells to the rest of the body.
Mine-explosion: Unconsciousness: Deaf-mutism. Recovery of speech after epistaxis and fever.
Mine explosion: Unconsciousness: Deaf-muteness. Speech recovery after nosebleed and fever.
Case 261. (Liébault, October, 1916.)
A soldier, 24, teacher in civil life, was in a mine explosion November 27, 1914, at Vienne-le-Château. He was unconscious six weeks and remembered nothing of what had passed. They had told him that he had been blind for a month. After regaining consciousness he was a deaf-mute and for seven months he did not speak. His mutism did not bother him, as he thought he had always been mute. He had always been able to write. He could not remember what had interfered with his speech or tell whether he could think the words which he could not utter.
A 24-year-old soldier, who was a teacher in civilian life, was involved in a mine explosion on November 27, 1914, at Vienne-le-Château. He was unconscious for six weeks and didn’t remember anything that had happened. They told him he had been blind for a month. After waking up, he was a deaf-mute and didn’t speak for seven months. His mutism didn’t bother him, as he believed he had always been mute. He had always been able to write. He couldn’t remember what had caused his speech issues or whether he could think the words that he couldn’t say.
May 22, 1915, there was considerable nasal hemorrhage, with fever. Upon this day he began to speak, at first a few words, telegram style, and with aphonia. A week later his voice returned. He was very irritable during the period of mutism and had ideas of persecution and of suicide and complained of becoming easily fatigued and exhausted.
On May 22, 1915, he had significant nosebleeds and a fever. That day, he started to talk, initially just a few words in a telegraphic style and with a hoarse voice. A week later, his voice came back. He was very irritable during his time of silence and had feelings of persecution and suicidal thoughts, along with complaints of being easily tired and worn out.
His voice, however, became completely normal again and his respiration better. On the spirometer he breathed four liters, but still got out of breath easily. His diaphragmatic respiration was still imperfect. His deafness remained at the time of report about as before, though he had now been hearing for some time a slight resonance of his own voice and could hear sounds emitted a few centimeters from his ear. At time of report there was still general fatigue with insomnia.
His voice returned to normal, and his breathing improved. On the spirometer, he breathed four liters but still got winded easily. His diaphragmatic breathing was still not quite right. His deafness was about the same as before, although he had started to hear a faint echo of his own voice and could hear sounds just a few centimeters away from his ear. At the time of the report, he still experienced overall fatigue and insomnia.
Re war deafness, Castex states that not merely shell bursts and explosions are able to cause deafness, but the din of battle alone. There are two big groups of war deafness: one due to drum rupture, and the other due to labyrinthine shock. Labyrinthine shock—a much more serious matter—is produced when a big shell bursts. In these cases, the labyrinthine disorder is simply of the same general nature as commotio cerebri. The labyrinthine shock cases often need to be retired permanently from the front.
Re war deafness, Castex states that it's not just shell blasts and explosions that can cause deafness, but the noise of battle itself. There are two main types of war deafness: one caused by eardrum rupture and the other by labyrinthine shock. Labyrinthine shock—much more serious—is caused when a large shell explodes. In these instances, the labyrinthine disorder is basically similar to commotio cerebri. Cases of labyrinthine shock often require permanent transfer away from the front lines.
Shell-shock: Deaf-mutism.
Shell shock: Deafness.
Case 262. (Mott, January, 1916.)
A deaf-mute, 24, not of a neurotic temperament or of a neuropathic predisposition, was admitted to the Fourth London General Hospital November 16, 1915.
A 24-year-old deaf-mute, who wasn't neurotic or predisposed to neurological disorders, was admitted to the Fourth London General Hospital on November 16, 1915.
He wrote, “I left England the 8th of March, and went to Gallipoli on the 26th of May, and about the middle of August, one of our monitors fired short. I felt something go in my head; then I went to the Canada Hospital. They said it was concussion.” He had seen the monitors firing. He came to in a dug-out about an hour afterward. He was quite deaf and his head felt as if it would burst.
He wrote, “I left England on March 8th and went to Gallipoli on May 26th. Around mid-August, one of our monitors fired short. I felt something hit my head, and then I went to the Canada Hospital. They said it was a concussion.” He had seen the monitors firing. He came to in a dugout about an hour later. He was completely deaf, and his head felt like it was going to explode.
He could see and speak a little but lost his speech completely when Barany’s tests were applied. The headache then passed away, leaving the deaf-mutism. The ears, on examination, proved normal. The patient was able to cough and whistle. He wrote his wife a letter, telling her how he killed a Turkish woman sniper, but he did not remember that he had written the letter. Although he said he did not dream, while asleep he would assume the attitude of shooting with a rifle, as if pulling a trigger, and then the attitude of using the bayonet: the right parry, the left parry, and the thrust. Sometimes while asleep he would jump as if a shell were coming, and he would catch his right elbow as if hit there. He would then open his eyes wide and look under the bed. Then he would wake up and begin to cry, but without sound. Just such habitual attitudes occur in soldiers under anesthesia. In hypnotic sleep, although he trembled at his trench experiences, he did not assume these defensive attitudes.
He could see and talk a little but completely lost his ability to speak when Barany’s tests were done. The headache then faded away, leaving him deaf and mute. The examination of his ears showed nothing wrong. He could cough and whistle. He wrote a letter to his wife, explaining how he killed a Turkish woman sniper, but he didn’t remember writing it. Even though he claimed he didn’t dream, while asleep he would act as if he was shooting with a rifle, mimicking pulling a trigger, and then he would pretend to use a bayonet: making a right parry, a left parry, and then a thrust. Sometimes, while he was asleep, he would jump as if a shell was coming, clutching his right elbow as if he’d been hit there. He would then open his eyes wide and look under the bed. Then he would wake up and start crying, but without making any sound. Such habitual actions occur in soldiers under anesthesia. In hypnotic sleep, even though he trembled recalling his trench experiences, he didn’t display these defensive actions.
Mott states in his Lettsomian lectures that hearing is often absolutely lost, but that sometimes a man is absolutely deaf on one side alone, either from the ruptured drum or from the violence with which wax has been driven against the drum. Mott speaks of the frequency of auditory hallucinations, and of hyperacusis—part of the patient’s general hypersensitivity—which may increase the violence of the neurosis and especially aggravate the headache.
Mott mentions in his Lettsomian lectures that people can completely lose their hearing, but sometimes someone might be totally deaf in just one ear, either due to a ruptured eardrum or from wax being aggressively pushed against it. Mott talks about how common auditory hallucinations are, as well as hyperacusis—which is part of the overall hypersensitivity of the patient—that can intensify the severity of the neurosis and especially worsen headaches.
Shell-shock: Deaf-mutism; convulsions and dream.
Shell shock: Deafness; seizures and dreams.
Case 263. (Myers, September, 1916.)
A private, 28, was seen by Lt. Col. Myers at a base hospital. This deaf-mute wrote, “I was standing and a shell bursted and that is all I can remember.” This might have happened six days previously. The patient wrote vaguely about a walk to “windy corner”; about being billeted in a dug-out, a train journey, and another hospital. He was deaf, deficient in sensibility throughout, especially in the left arm and left side of the face, and had severe headache. Two days later he started distinctly when hands were clapped while he was writing, but at the next hand-clapping there was no response.
A private, 28, was seen by Lt. Col. Myers at a base hospital. This deaf-mute wrote, “I was standing and a shell exploded and that’s all I can remember.” This might have happened six days earlier. The patient wrote vaguely about a walk to “windy corner”; about being housed in a dug-out, taking a train trip, and going to another hospital. He was deaf, had reduced sensitivity overall, especially in his left arm and left side of his face, and suffered from a severe headache. Two days later, he jumped when hands were clapped while he was writing, but at the next clapping, there was no response.
After Lt. Col. Myers wrote down, “Imitate me,” and made consonant sounds, the patient succeeded imitating them. “You hear me a little now,” Lt. Col. Myers wrote. “Is this the first time you have spoken?” Patient replied, “I hope the Lord I can get my speech.” “But you did speak just now. Read this word. Say it.” Whereupon he was got to say his name and number.
After Lt. Col. Myers wrote down, “Imitate me,” and made some sounds, the patient managed to imitate them. “You can hear me a bit now,” Lt. Col. Myers wrote. “Is this the first time you’ve spoken?” The patient replied, “I hope the Lord I can get my speech.” “But you just spoke. Read this word. Say it.” Then he was able to say his name and number.
The therapy was proceeding properly when suddenly he was seized with convulsions, limb movements chiefly clonic, back arched, eyes starting, later upturned. The patient pulled out a crucifix from a locker near the bed and regarded it ecstatically (pulse 85, corneal reflexes preserved). Three minutes later there was quieting down, and the patient was induced to talk. He began to talk about his wife. He had just been “seeing a farm and all the fighting.” A shell must have come in there. He had “seen the Lord Who saved him.” Intense headache and thirst followed. According to the patient the excitement was due to recovery of speech.
The therapy was going smoothly when suddenly he started having convulsions, mainly twitching movements in his limbs, his back arched, and his eyes wide open, later rolling back. The patient pulled a crucifix from a locker near the bed and looked at it in awe (pulse 85, corneal reflexes intact). Three minutes later, he calmed down, and we encouraged him to talk. He began discussing his wife. He had just been “seeing a farm and all the fighting.” A shell must have landed there. He had “seen the Lord Who saved him.” He then experienced a severe headache and intense thirst. According to him, the excitement was because he was recovering his ability to speak.
He later said, “It was just like a dream when I came to. I was sweating awful. I was seeing the Lord while I was in the farm by the Captain. I dreamed that I had the cross in my hand to meet him coming. I saw the trenches and the dug-outs and the wife.” In point of fact, the Captain at the[369] farm had had his arm blown off, and he had found him lying on the straw unconscious. Under hypnosis it appeared that he had gone to a dugout from the farm and that at the clearing station he had been “raving, seeing things, shells, trenches, and things like that, sir.” A slow recovery was made after evacuation to England. Seven months later he returned to the front.
He later said, “It felt just like a dream when I came to. I was sweating a lot. I saw the Lord while I was at the farm by the Captain. I dreamed that I had the cross in my hand to meet Him. I saw the trenches, the dugouts, and the wife.” In reality, the Captain at the[369] farm had lost his arm, and he found him lying unconscious on the straw. Under hypnosis, it turned out that he had gone to a dugout from the farm and that at the clearing station he had been “raving, seeing things, shells, trenches, and stuff like that, sir.” He made a slow recovery after being evacuated to England. Seven months later, he was back at the front.
This case appears to belong to the B group of mutism cases, according to the classification of Myers, namely, to the group in which the effects are psychical rather than physical. According to Myers, whether mutism occurs as an apparent result of physicochemical or of mental causes—that is, as an A or a B case—it is actually always the result of mental—that is, psycho-physiological shock. Mutism in the A cases of physical nature, where the shock must have been grosser and more profound, generally proves more severe than in the B cases. As to the appearance of unconsciousness, apparently confirmed by the patients’ statements that they “lost consciousness,” it is a question whether these cases are not really cases of deep stupor. According to Myers, the mutism is in nearly every instance closely dependent on some form of stupor, being generally the relic of such stupor after it has passed off. Let the loss of consciousness be a profound stupor due to the lifting or burial of the patient, then from this stage there will be a transition to a state of ordinary stupor in which intelligence is active but the patient is unresponsive to stimuli. The patient is in a condition called by Myers excommunication, in which the inhibitory process may be regarded as protecting the individual against further shock. As the stupor now passes away, it is natural that the inhibition should appear lost in the case of hearing and speech, which are two main channels of intercourse with others.
This case seems to fall into the B group of mutism cases, according to Myers' classification, which includes those where the effects are psychological rather than physical. Myers states that whether mutism is a result of physicochemical or mental causes—meaning A or B cases—it is actually always caused by mental factors, specifically psycho-physiological shock. Mutism in the A cases, which are of a physical nature and involve more severe and profound shock, tends to be more intense than in the B cases. Regarding the reports of unconsciousness, as indicated by patients claiming they “lost consciousness,” it is uncertain whether these cases are truly instances of deep stupor. Myers suggests that mutism is almost always closely related to some form of stupor, often just a remnant of that stupor after it has resolved. If the loss of consciousness is indeed profound stupor caused by the patient being lifted or buried, then there will be a shift to a typical stupor state where the person's intelligence is active but they don’t respond to stimuli. In this state, Myers refers to it as excommunication, where the inhibitory process seems to guard the individual against further shock. As the stupor fades, it’s expected that the inhibition will seem lost in terms of hearing and speech, which are two primary ways of communicating with others.
Dumbness is, by far, the commonest disorder of speech, occurring in about ten per cent of shock cases in the first thousand cases of shell-shock seen by Lt. Col. Myers. Stuttering and jerky speech have occurred in about three per cent. Loss of voice is rarer.
Dumbness is, by far, the most common speech disorder, happening in about ten percent of shock cases in the first thousand cases of shell shock seen by Lt. Col. Myers. Stuttering and choppy speech have occurred in about three percent. Loss of voice is less common.
As against the view of Babinski, that mutism, being curable by suggestion, must have been produced by suggestion, Lt. Col. Myers argues that the stupor preceding mutism is the antithesis of suggestibility and is, in fact, a condition of extreme autofixity.
In contrast to Babinski's belief that mutism can be treated through suggestion and must therefore be caused by suggestion, Lt. Col. Myers argues that the stupor that occurs before mutism is the opposite of suggestibility and is, in fact, a state of extreme autofixity.
Naval gun-fire effects on seaman: Aphonia. Two recurrences.
Naval gunfire effects on sailors: Loss of voice. Two occurrences.
Case 264. (Blasé, June, 1915.)
A seaman from the Derfflinger was brought into a naval hospital with loss of voice, December 22, 1914, able to speak only in a whisper. As a child he had had diphtheria, but recovered without complication. He had always had a very well-controlled voice. Early in December he had had a cold owing to sentry deck duty in bad weather. Two days after the shelling of Scarboro,—December 16,—while in the munition chamber of the big guns, he suddenly lost his voice. He had been greatly upset during the firing of the guns. In two weeks he recovered speech.
A sailor from the Derfflinger was admitted to a naval hospital on December 22, 1914, with a loss of voice, only able to speak in a whisper. As a child, he had diphtheria but recovered without complications. He had always had very good control of his voice. Earlier in December, he caught a cold while on sentry duty on deck in bad weather. Two days after the shelling of Scarborough—December 16—while in the ammunition chamber of the big guns, he suddenly lost his voice. He had been very stressed during the gunfire. He regained his speech after two weeks.
February 12, 1915, he returned to the hospital with a complete aphonia. This was immediately after the naval engagement in the North Sea. Three days later he was treated with electricity directly applied to the vocal cords. March 20 he was discharged with speech completely recovered. As soon as he went on leave, however, his voice was lost for the third time, and he was still aphonic at time of report.
February 12, 1915, he returned to the hospital with total loss of voice. This was right after the naval battle in the North Sea. Three days later, he received treatment using electrical stimulation directly on his vocal cords. On March 20, he was discharged with his speech fully restored. However, as soon as he went on leave, he lost his voice again for the third time, and he was still unable to speak at the time of the report.
Shell-shock MUTES observed, then DREAMED OF: MUTISM developed the SECOND NIGHT after shell explosion.
Shell shock MUTES were noted, then DREAMED OF: MUTISM developed the SECOND NIGHT after the shell explosion.
Case 265. (Man, June, 1915.)
A volunteer of 20 was made unconscious for a short time by a shell explosion, but was still fully able to speak when brought to the field hospital.
A 20-year-old volunteer was knocked out for a short time by a shell explosion but was still able to talk when he was brought to the field hospital.
In the second night after the explosion, however, he dreamed that he had lost his speech. In the ward, meantime, he had seen a number of shell-shock mutes. Following this dream of aphasia, came several weeks of mutism, which then cleared up. According to Mann, this is experimental proof of the psychogenic origin of a mutism.
In the second night after the explosion, though, he dreamed that he had lost his ability to speak. Meanwhile, in the ward, he had seen several shell-shock victims who couldn't talk. After this dream about losing his speech, he experienced several weeks of being mute, which eventually improved. According to Mann, this is experimental evidence of the psychological cause of mutism.
Mortar explosion: Hysterical deafness.
Mortar blast: Hysterical deafness.
Case 266. (Lattes and Goria, March, 1917.)
A young soldier, a peasant, fell down unconscious when a mortar exploded killing several men. He regained consciousness a few hours later but was deaf on both sides. He looked dazed and did not spontaneously move, having to be called for meals. Communicating by writing, he could tell all the details of the accident.
A young soldier, a peasant, collapsed when a mortar exploded, killing several people. He woke up a few hours later but was deaf in both ears. He looked stunned and didn’t move on his own, needing to be called for meals. By writing, he was able to share all the details of the incident.
The laryngeal and corneal reflexes were absent and there was a hyperesthesia and hypalgesia of the right side of the body. No anatomical basis for the deafness could be determined.
The laryngeal and corneal reflexes were missing, and there was increased sensitivity and decreased pain response on the right side of the body. No anatomical reason for the hearing loss could be identified.
Shell explosion: Onomatopoeic noises in ears.
Shell explosion: Loud, onomatopoeic sounds in ears.
Case 267. (Ballet, 1914.)
A Zouave was with his squad at Tracy-les-Val Church, October, 1914, when the roof was burst in by a shell which wounded four men. The Zouave felt a strange emotion with trembling, and whistling in his ears. However, he helped his comrades into a neighboring car. From that time forward, he was very emotional, and felt noises in his ear, sometimes humming, sometimes whistling. At Compiègne Hospital a lumbar puncture was made, perhaps with a therapeutic purpose, but this gave no results. The noises were heard as a whistling pseeee followed by a boom,—an onomatopoeia recalling the whistling and bursting of the bomb. There was, in short, no labyrinthine lesion, but merely an obsessive mental phenomenon. There were no ear lesions objectively. The man developed a stuttering some time after the humming and whistling in the ear.
A Zouave was with his squad at Tracy-les-Val Church in October 1914 when a shell hit the roof, injuring four men. The Zouave experienced a strange feeling along with trembling and a whistling sound in his ears. Nevertheless, he assisted his comrades into a nearby vehicle. From that point on, he was very emotional and continued hearing noises in his ear, sometimes humming and sometimes whistling. At Compiègne Hospital, they performed a lumbar puncture, possibly for therapeutic reasons, but it didn’t yield any results. The sounds he heard were a whistling pseeee followed by a boom—an onomatopoeia reminiscent of the whistling and explosion of the bomb. In short, there was no complex injury, just an obsessive mental phenomenon. There were no observable ear injuries. The man developed a stutter some time after the humming and whistling in his ear.
Injury of eyes by gravel from shell-burst: Photophobia, blepharospasm, facial anesthesia, pains.
Injury to the eyes from gravel due to shell explosions: sensitivity to light, eyelid spasms, facial numbness, and pain.
Case 268. (Ginestous, January, 1916.)
A soldier of the Ninth Engineers, 28, a Beaux-Arts student, was wounded, December 19, 1915, by stones and gravel thrown in his eyes by a shell-burst. The eyelids swelled and the eyes filled with tears. He was treated at the relief station and then evacuated to Verdun. The edema disappeared in five weeks, but it was impossible for him to look at light. February 2 he was evacuated to Nice, where he received the diagnosis of traumatic keratalgia, blepharospasm, and photophobia. After eight days’ leave he went back to his corps; but the eye troubles persisted and he was sent to the ophthalmological center at Angers, May 18, 1915.
A soldier from the Ninth Engineers, 28, who was a Beaux-Arts student, was injured on December 19, 1915, when stones and gravel struck his eyes due to a shell explosion. His eyelids swelled and his eyes filled with tears. He received treatment at the relief station and was then evacuated to Verdun. The swelling went down in five weeks, but he could not tolerate light. On February 2, he was moved to Nice, where he was diagnosed with traumatic keratalgia, blepharospasm, and photophobia. After an eight-day leave, he returned to his unit; however, the eye problems continued, and on May 18, 1915, he was sent to the ophthalmological center in Angers.
Both his father, 67, and his mother, 58, were irritable and odd. Three brothers and three sisters were also more or less neuropathic, and one of the sisters had been in a hospital for the insane with a persecutory mania. The patient had a daughter, fourteen months, well.
Both his father, 67, and his mother, 58, were cranky and strange. Three brothers and three sisters also had their quirks, and one of the sisters had been in a psychiatric hospital for persecutory mania. The patient had a healthy daughter who was fourteen months old.
The man was a nervous, impressionable person, who wept at the slightest emotion. With an effort of will he could open his eyes, but if one tried to open them passively there was stout resistance. In the dark the occlusion was not so complete. Both eyelids were wrinkled and folded and made jerky, fibrillary movements. The conjunctiva and cornea were normal (fluorescein test), but the palpebral conjunctiva was red and injected. The patient said he had subcutaneous pains recurring at irregular intervals above and below the left orbit, brought out or exaggerated by pressure; but such pressure had no effect upon the lid movements. Visual acuity was normal, but the use of ophthalmometer was impossible, as was measurement of the visual field. There seemed to be no disorder of chromatic sense. The reflexes could not be fully examined; knee-jerks preserved. There was a zone of anesthesia to pin prick, less marked to heat, on the whole left side of the face. W. R. negative.
The man was a nervous, impressionable person who cried at the slightest emotion. With a strong effort, he could open his eyes, but if someone tried to open them for him, he resisted firmly. In the dark, the obstruction wasn't as complete. His eyelids were wrinkled and folded, moving in jerky, twitchy motions. The conjunctiva and cornea were normal (fluorescein test), but the inside of the eyelids was red and swollen. The patient reported having sharp pains that came and went at irregular intervals above and below the left eye, which were worsened by pressure; however, pressing on the eyelids had no effect on their movement. His vision was normal, but using an ophthalmometer or measuring the visual field was impossible. There didn’t seem to be any issues with color perception. The reflexes couldn't be fully tested; knee-jerks were intact. There was a patch of numbness from pinpricks, less sensitive to heat, on the entire left side of his face. W. R. negative.
Shell-shock; burial; blow on occiput: Blindness.
Shell shock; burial; blow to the back of the head: Blindness.
Case 269. (Greenlees, February, 1916.)
A man in the third Wiltshire regiment was buried in a shell explosion and struck by a large mass of earth on the back of the head. When dug out, he was found blind. It was thought at the time that the severe blow at the back of the head had “concussed” the occipital cells for sight.
A man in the third Wiltshire regiment was buried in a shell explosion and hit on the back of the head by a large amount of earth. When he was dug out, he was found to be blind. At the time, it was believed that the strong blow to the back of his head had “concussed” the occipital cells responsible for sight.
Some months later the man was sent to Mr. Pearson’s home for blind soldiers in London; but two months later was returned to Weymouth, under Greenlees’ charge. He thought himself worse, since now he could not see light at all. He had trained himself to take care of himself and steered confidently aside from obstacles in walking about. He was able even to learn the various colors by the sense of touch, according to Greenlees; thus, blue was diagnosticated against red: according to the patient, a piece of colored card always had a rougher feel if it was blue than if it was red. In fact, his work consisted of making colored net bags.
A few months later, the man was sent to Mr. Pearson’s home for blind soldiers in London, but two months after that, he was sent back to Weymouth, under Greenlees’ care. He felt worse now since he could no longer see light at all. He had trained himself to take care of himself and navigated around obstacles confidently while walking. He was even able to learn the different colors by touch, according to Greenlees; for example, blue felt rougher than red. In fact, his work involved making colored net bags.
As to the possible interpretation of such a case, see Case No. 433 (man who could see large letters sometimes).
As for how to interpret this case, see Case No. 433 (the man who could occasionally see large letters).
Re blindness, H. Campbell states that the number of cases of hysterical blindness appears to be decreasing as the war continues. The blindness he finds to be rarely an absolute one. As a rule, the vision is merely blurred or there is a contraction of the visual fields. The condition is much less frequent than that of deafmutism.
Re blindness, H. Campbell notes that the number of cases of hysterical blindness seems to be going down as the war goes on. He finds that this blindness is rarely complete. Typically, vision is just blurred or there’s a narrowing of the visual fields. This condition is much less common than deafmutism.
Re hysterical blindness, Dieufaloy is cited by Crouzon as describing a triad of conditions characteristic of hysterical blindness, namely, (a) sudden onset, (b) preservation of pupillary reflexes, and (c) normal fundus.
Re hysterical blindness, Dieufaloy is referenced by Crouzon as describing a set of three conditions that are typical of hysterical blindness, namely, (a) sudden onset, (b) preserved pupillary reflexes, and (c) normal fundus.
Shell-shock amblyopia (composite data).
Shell-shock amblyopia (combined data).
Case 270. (Parsons, May, 1915.)
Parsons describes a typical case of shell explosion amblyopia. After more or less prolonged fatigue from marching and trench exposure, the soldier is knocked down or blown into the air, and more or less severely injured or wounded by concussion, fracture, bullets, or shell splinters, losing consciousness, but perhaps not enough to prevent automatic walking in a dazed state to the dressing station. Memory of this phase is lost. The man is instantaneously stricken blind, possibly also deaf; and possibly smell and taste are also lost. Blepharospasm is intense; there is lacrimation; the lids are opened with such difficulty that examination of the eyes is almost impossible (nor, according to Parsons, have the pupils yet been examined at this stage).
Parsons describes a typical case of shell explosion amblyopia. After a period of fatigue from marching and being in the trenches, the soldier gets knocked down or blown into the air, suffering from varying degrees of injury due to concussion, fractures, bullets, or shell fragments. He loses consciousness but may still walk automatically in a dazed state to the medical station. He has no memory of this phase. The soldier suddenly goes blind, and he might also lose his hearing; smell and taste could be lost as well. Blepharospasm is intense, there is tearing, and opening the eyelids is so difficult that examining the eyes becomes nearly impossible (and, according to Parsons, the pupils haven't been examined at this point).
In a week or two the blepharospasm diminishes, and the fundi, which are found to be absolutely normal, can be examined. The eyes may be found to be quite normal, the pupils reactive to light though perhaps sluggishly and perhaps unequally. Sight is now somewhat restored, light can be perceived, and large objects distinguished. The patient can grope about and usually does not stumble against obstacles. The fields of vision are markedly contracted, and more so than the avoidance of obstacles in walking would suggest.
In a week or two, the blepharospasm gets better, and the fundi, which are completely normal, can be examined. The eyes may appear quite normal, with pupils that react to light, although possibly a bit slowly and unevenly. Vision is somewhat restored; light can be seen and large objects can be recognized. The patient can move around and usually doesn’t bump into things. However, the fields of vision are significantly reduced, more than what avoiding obstacles while walking would indicate.
Vision is eventually recovered completely. The right eye (the shooting eye) is often more deeply affected and recovers more slowly. Perhaps a central scotoma may persist. Sometimes on manipulation of lenses the full vision can be produced for the types. Parsons seeks to explain the psychology of traumatic amblyopia in the light of deductions of Lloyd Morgan, Mark Baldwin and McDougall.
Vision ultimately returns fully. The right eye (the shooting eye) is often more significantly impacted and takes longer to recover. A central blind spot may linger. Occasionally, adjusting the lenses can restore full vision for certain types. Parsons aims to explain the psychology of traumatic amblyopia based on insights from Lloyd Morgan, Mark Baldwin, and McDougall.
Shell-shock amblyopia (excitement, blinding flashes, fear, disgust, fatigue).
Shell-shock amblyopia (excitement, bright flashes, fear, disgust, fatigue).
Case 271. (Pemberton, May, 1915.)
Pemberton calls attention to the following factors in a case of amblyopia: First, excitement during a prolonged and somewhat critical attack; second, overstimulation of eyes and ears due to brilliant flashes, night firing from many batteries close together (the gunners are always subject to temporary deafness from this firing); third, natural fear from close bursting of shells; fourth, disgust at decapitated and disemboweled soldiers; fifth, fatigue from twelve hours’ work.
Pemberton highlights the following factors in a case of amblyopia: First, heightened emotions during a long and somewhat critical attack; second, sensory overload of the eyes and ears due to bright flashes and nighttime firing from multiple artillery units near each other (the gunners often experience temporary deafness from this firing); third, natural fear from shells exploding nearby; fourth, revulsion at seeing decapitated and disemboweled soldiers; fifth, exhaustion from working twelve hours straight.
The artillery sergeant worked under heavy shell fire at Gun No. 1. A direct hit killed three men serving No. 2 gun. The sergeant became somewhat excited but worked his gun until the following dawn, when he collapsed across one of the disemboweled corpses. He thus had been at work for about twelve hours. The battery had fired 400 or 500 rounds.
The artillery sergeant operated under intense shell fire at Gun No. 1. A direct hit took the lives of three men at Gun No. 2. The sergeant got pretty worked up but continued to man his gun until dawn, when he collapsed over one of the dismembered bodies. He had been working for about twelve hours. The battery had fired 400 or 500 rounds.
A few hours later, the man was conscious but very feeble and much shaken. There was amblyopia and contraction of the fields of vision to rough tests, but no change in color vision. Taste sense was blunted, and salt could hardly be told from powdered quinin tablets. Smell also was practically absent, although he had never been able to smell accurately. Hearing was not more affected than that of other men in the battery, and there were no tympanic fractures. Both thighs, from about the apex of Scarpa’s triangle to the knee, showed partial anesthesia, such that a pin prick that should have been painful was felt only as a tactile sensation, whereas lighter stimulation caused no sensation whatever. The patient himself complained of numbness in these areas. The gait was slow and spastic. The knee-jerks were brisk. Sent back to the wagon lines for a week, the patient lost his sensory disturbance, but the symptoms of mental distress increased. He walked weakly and stiffly; he continually thought of the dead men at the next gun, one of whom was a friend. He was finally sent to a hospital in England.
A few hours later, the man was awake but very weak and shaken. He had blurred vision and narrowed fields of vision in basic tests, but his color vision was unchanged. His sense of taste was dulled, and he could barely distinguish salt from powdered quinine tablets. His sense of smell was almost non-existent, even though he had never had an accurate sense of smell. Hearing was similar to that of the other men in the unit, and there were no eardrum fractures. Both thighs, from around the top of Scarpa’s triangle to the knee, showed partial numbness, so a pin prick that should have hurt was felt only as a light touch, while lighter sensations registered no feeling at all. The patient himself complained of numbness in those areas. His walk was slow and stiff. The knee reflexes were brisk. After being sent back to the wagons for a week, the patient regained his sensation but his mental distress worsened. He walked weakly and rigidly, constantly thinking about the dead men at the next gun, one of whom was a friend. He was finally sent to a hospital in England.
Shell-shock amblyopia.
Shell shock eye strain.
Case 272. (Myers, February, 1915.)
A private, 20, lay in the booking-hall of a station, October 28-29, not securing much sleep; motored in a bus next day to another place at 7.30 p.m.; went into billets at 8 p.m.; mounted guard 10-11.30 p.m. and 1.45 to 3.45 a.m.; and went to the firing-line for the first time at 11 a.m. October 31. The platoon advanced through two sets of trenches, which were full, and had to retire. About 1.30 p.m. they were found by the German artillery.
A private, 20, spent the night in the booking hall of a station, October 28-29, hardly getting any sleep; took a bus to another location the next day at 7:30 p.m.; went to the barracks at 8 p.m.; stood guard from 10-11:30 p.m. and 1:45 to 3:45 a.m.; and arrived at the front line for the first time at 11 a.m. on October 31. The platoon moved through two sets of trenches, which were occupied, and had to fall back. Around 1:30 p.m., they came under fire from the German artillery.
This man had been rather enjoying it and was in the best of spirits until the shells began to burst. The platoon was retiring over open ground. He was kneeling on both knees, trying to creep under wire entanglements, when two or three shells burst near by. Three more shells burst behind and one in front. The escape was described by an eye-witness as a miracle. He managed to get back under the entanglements and into the trench, and shortly, as the fire slackened, rejoined his company.
This guy had been really enjoying himself and was in great spirits until the shells started exploding. The platoon was falling back across open ground. He was kneeling on both knees, trying to crawl under barbed wire, when two or three shells went off nearby. Three more shells detonated behind him and one in front. An eyewitness described his escape as a miracle. He managed to get back under the wire and into the trench, and soon, as the firing eased up, he rejoined his unit.
His sight had become blurred immediately after the shell burst. Opening his eyes hurt him, and the eyes burned when closed. The right eye “caught it” more than the left. At the same time, he was seized with shivering, and cold sweat broke out, especially about the loins. He thought the shell behind caused the greater shock, like a punch on the head without pain. The shell that burst in front had cut his haversack away, bruised his side, and burned his little finger. This shell he thought caused his blindness.
His vision became blurry right after the shell exploded. Opening his eyes was painful, and closing them made them burn. His right eye was affected more than his left. At the same time, he felt intense shivering, and he broke out in a cold sweat, especially around his lower back. He believed the shell that exploded behind him caused the biggest shock, like getting hit in the head without any pain. The shell that blew up in front had torn his haversack apart, bruised his side, and burned his little finger. He thought that this shell was what caused his blindness.
He was led to the dressing station by two comrades, opening his eyes to see where he was going but finding everything blurred except immediately after opening his eyes. There was no diplopia. Objects seemed to dissolve. He was weeping and worrying about becoming blind. The horse ambulance took him to a hospital and thence to another hospital, and thence he went by motor ambulance at night to the starting point, where he arrived five days after he had entered the field. He could remember nothing about the[377] ambulance trips. There was a slight deafness which soon passed off. In hospital he shivered almost incessantly in bed, and he kept thinking about his experience and the shell bursting. The shivering ceased November 3. No micturition from the afternoon of October 30 until the afternoon of November 2. No movements of bowels from October 30 to November 5.
He was taken to the medical station by two friends, opening his eyes to see where he was going but everything was blurry except right after he opened them. There was no double vision. Objects seemed to fade away. He was crying and worried about going blind. The horse-drawn ambulance took him to a hospital, then to another hospital, and later he traveled by motor ambulance at night back to the starting point, arriving five days after he had entered the field. He couldn’t remember anything about the ambulance rides. He experienced slight deafness that soon went away. In the hospital, he shivered almost constantly in bed, and he kept thinking about his experience and the shell explosion. The shivering stopped on November 3. He had no urination from the afternoon of October 30 until the afternoon of November 2. He had no bowel movements from October 30 to November 5.
It seems that this soldier had been for two months in the Aisne district, sleeping badly on account of lumbar pains and toothache. There had been albuminuria, and the patient said he had failed to pass a medical examination. The fields of vision were found to be distinctly contracted. There was difficulty in taste and smell, which the patient said he had lost since the shell-burst.
It seems this soldier had spent two months in the Aisne area, struggling to sleep because of back pain and a toothache. He had experienced albuminuria and mentioned that he had failed a medical exam. His fields of vision were noticeably narrowed. He also had trouble with his taste and smell, which he said he lost after the explosion.
Hypnosis was tried but the patient “insisted on resisting.” The suggestions were offered during the concentration period. November 13 taste and smell began to return and the fields of vision were less contracted. He was transferred to England for further treatment, and by November 27 had become much improved and not so “nervy.” February 1 he had begun to attend hospital as an out-patient.
Hypnosis was attempted, but the patient “insisted on resisting.” Suggestions were given during the focus period. On November 13, taste and smell started to return, and his field of vision was less restricted. He was moved to England for further treatment, and by November 27, he had significantly improved and was not as “nervy.” By February 1, he had started attending the hospital as an out-patient.
SHELL WINDAGE (NO EXPLOSION): Multiple affection of cranial nerves.
SHELL WINDAGE (NO EXPLOSION): Multiple issues with cranial nerves.
Case 273. (Pachantoni, April, 1917.)
August 22, 1914, a French officer was leading his company to an attack and carried on, though wounded in the side by a bullet. Suddenly he felt as if he had received a terrible blow with a hammer on the left cheek and eye and as if his arm had been torn off. He fell to his knees without losing consciousness. There had been no explosion, and none of his soldiers had been hit. He felt of his arm and carried his hand to his head to make sure of the wounds. There were none, but he was bleeding from the nose and the mouth. His left eye was closed and his left cheek drawn “by an invisible hand.” His tongue had swollen until it had to be pushed out of his mouth. He was breathing hard. He fell upon his side without losing consciousness and he was carried by his men to shelter in a trench. Placed on his back he felt that he could not lift his head as “it had become too heavy.” His voice was lost. He could neither cough nor spit. In order to get air he had to remove bloody saliva from his mouth with his finger. The left side of the head was swollen. On opening his eyes he could no longer see with the left eye. His cheek was covered with ecchymoses but without wound. A few hours later he was made prisoner by the Germans. For two months he had an increase of temperature every evening and for three months he lost his voice. Six months later there was still visual impairment. He was anesthetic in the left cheek, unable to chew, paralyzed in the left facialis region. There was alteration of taste, with atrophy of the left side of the tongue deviating to the paralyzed side, and nasal regurgitation. There was continual drooling and convulsive coughing. In dorsal decubitus the head could be lifted with difficulty. There was a kind of paresis of the esophagus, as he felt the bolus stop at the level of the third ribs so that with each mouthful he had to swallow a little water. Apparently he had a paralytic state of the following[379] nerves: optic, oculomotor, trigeminal, glossopharyngeal, pneumogastric, spinal accessory and hypoglossal. There was evidence of a slight old tuberculosis at apices. The man was slightly pale. There was an atrophy of the optic nerve and some retinal swelling. No pupillary reactions to light on the left side; but the accommodation reflex and sensory reaction were preserved. Divergent strabismus of the left eye. The taste on the left side and on the anterior part of the tongue was slightly diminished. Diminution of galvanic and faradic excitability on the left side of the face. No reaction of degeneration. Bitter, salt and sweet tastes altered. Left-sided atrophy of the tongue. No reaction of degeneration in the tongue and thyroid muscles although there was a marked diminution in faradic excitability.
On August 22, 1914, a French officer was leading his unit into an attack and kept going, even though he had been shot in the side. Suddenly, he felt like he had been hit hard on the left cheek and eye, as if his arm had been ripped off. He dropped to his knees but didn’t lose consciousness. There had been no explosion, and none of his men had been hit. He checked his arm and felt his head to confirm his injuries. There were none, but he was bleeding from his nose and mouth. His left eye was shut, and his left cheek felt tight, “like an invisible hand.” His tongue had swollen so much that it was forced out of his mouth. He was breathing heavily. He fell onto his side but still didn’t lose consciousness, and his men carried him to safety in a trench. Lying on his back, he realized he couldn’t lift his head because “it felt too heavy.” He had lost his voice and couldn’t cough or spit. To breathe, he had to use his finger to clear out the bloody saliva from his mouth. The left side of his head was swollen. When he opened his eyes, he couldn’t see out of his left eye anymore. His cheek was bruised but had no open wounds. A few hours later, he was taken prisoner by the Germans. For two months, he had a fever every evening and lost his voice for three months. Six months later, he still had vision problems. The left side of his cheek was numb, making it hard to chew, and he had paralysis in the left side of his face. He experienced changes in taste, with the left side of his tongue shrinking and leaning toward the paralyzed side, and he had nasal regurgitation. He was constantly drooling and had fits of coughing. Lying on his back, he could lift his head with difficulty. He felt like food got stuck at the level of his third ribs, so he had to swallow a bit of water with each bite. He seemed to have paralysis of the following[379] nerves: optic, oculomotor, trigeminal, glossopharyngeal, pneumogastric, spinal accessory, and hypoglossal. There were signs of a slight old tuberculosis in his lung apices. The man appeared a bit pale. The optic nerve was atrophied, and there was some swelling in his retina. There were no pupillary reactions to light on the left side, but he could still accommodate and had a sensory reaction. His left eye had divergent strabismus. His taste on the left side and the front part of his tongue was slightly reduced. There was decreased galvanic and faradic response on the left side of his face. No degeneration response. His sense of bitter, salty, and sweet tastes was altered. There was atrophy on the left side of his tongue. No reaction of degeneration in the tongue or thyroid muscles, although faradic excitability was notably reduced.
The author records this case of multiple lesions of cranial nerves as due to shell windage. Thirty-one months after the onset of the paralysis the cranial nerves, although manifestly regenerated, had not regained conductivity. The officer was examined by Pachantoni at Louèche-les-Bains in Switzerland.
The author notes this case of multiple lesions of cranial nerves caused by shell wind. Thirty-one months after the paralysis began, the cranial nerves, while clearly regenerated, had not regained conductivity. The officer was examined by Pachantoni in Louèche-les-Bains, Switzerland.
Re windage, see remarks under Case 201.
Re windage, see remarks under __A_TAG_PLACEHOLDER_0__.
Wound of thigh: Claudication, vasomotor disorder, hypothermia, but no exaggeration of tendon reflexes. Under CHLOROFORM, ELECTIVE EXAGGERATION OF REFLEXES, i.e., in this case, hyperreflexia of affected thigh, including patellar clonus, after other reflexes (including conjunctival) had become extinct. The case described led to the new formula of THE PHYSIOPATHIC SYNDROME (BABINSKI).
Wound of thigh: Pain when walking, blood vessel issues, coldness, but no heightening of tendon reflexes. Under CHLOROFORM, VOLUNTARY HEIGHTENING OF REFLEXES, i.e., in this case, increased reflexes in the affected thigh, including patellar clonus, after other reflexes (including conjunctival) had disappeared. The case described led to the new formula of THE PHYSIOPATHIC SYNDROME (BABINSKI).
Case 274. (Babinski and Froment, 1917.)
Babinski examined in August, 1915, at the Pitié, a soldier who had been wounded in the upper and outer part of the thigh. He showed a most marked claudication with outward rotation of the foot. There was a muscular atrophy of the thigh but no appreciable disorder of the electrical reactions. There was a slight limitation in the movements of the hip, namely, the movements of flexion and internal rotation of the thigh upon the pelvis; yet this limitation of movements did not seem to be in proportion to the rest of the motor disorder. The X-ray showed no joint lesion. The right knee-jerk was a bit stronger than the left, though this was controversial. Achilles reflexes were normal and equal; epileptoid trepidation of the foot, and clonus of the patella absent; the limb showed marked and permanent vasomotor disorders and local hypothermia; both phenomena were of a sharp and definite nature.
Babinski examined a soldier at the Pitié in August 1915 who had been wounded in the upper outer part of his thigh. He showed significant limping with his foot turned outward. There was noticeable muscle wasting in the thigh but no significant issues with electrical responses. There was a slight limitation in hip movements, particularly in flexion and internal rotation of the thigh relative to the pelvis; however, this limitation didn’t seem to match the overall motor impairment. X-rays showed no joint damage. The right knee-jerk reflex was slightly stronger than the left, though this was debated. Achilles reflexes were normal and equal; there were no signs of foot tremors or patellar clonus; the limb exhibited marked and persistent blood circulation issues and local coldness, both clearly defined.
On the basis of the intensity of these vasomotor disorders, Babinski felt that, in accordance with his general ideas, he was not dealing with hysteria, and that he was in fact dealing with the so-called physiopathic syndrome. Lacking for this syndrome was the exaggeration of the tendon reflexes of the affected limb. Might it not be that the improper attitude and muscular stiffness of the limb were based simply on retractions of tendons? The patient was chloroformed. This procedure was the more warrantable as a number of physicians had thought of the patient as an exaggerator or[381] even as a simulator. Under chloroform there was in fact a slight tendon retraction; yet on the whole it was clear that the attitude and stiffness of the limb were largely dependent upon a contracture. When during narcosis all the other tendon reflexes and skin reflexes had become extinct, there was still to be observed on the affected side a hyperreflexia, and even a clonus of the patella; and the clonus lasted an hour after recovery from the anesthetic. This curious phenomenon of elective exaggeration of tendon reflexes in narcosis, Babinski has observed to be not infrequent. It is a valuable diagnostic sign for a sure proof of excess tendon reflexes in cases where doubt prevails under ordinary circumstances. Sometimes the contracture will yield, but only in the deepest sleep, outlasting even the conjunctival reflex and the reactions to pricking of the normal extremities. Moreover, the contracture would return from 20 to 25 minutes before any manifestation of consciousness. If an endeavor was made to reduce the contracture under full anesthesia and in complete unconsciousness, a spasmodic movement was provoked which exaggerated the abnormal attitude of the limb. Sometimes even the leg would be thrown into flexor contracture.
Based on the severity of these vasomotor disorders, Babinski believed that, according to his overall theories, he was not dealing with hysteria, but rather with what is known as the physiopathic syndrome. This syndrome lacked the exaggerated tendon reflexes typically seen in the affected limb. Could it be that the improper positioning and muscle stiffness of the limb were simply the result of tendon retractions? The patient was put under chloroform. This was justified, as several doctors had regarded the patient as someone who exaggerated or[381] even simulated symptoms. While under chloroform, there was indeed a slight tendon retraction; however, it became clear that the position and stiffness of the limb were mainly due to a contracture. During the anesthesia, when all other tendon and skin reflexes had disappeared, hyperreflexia was still noted on the affected side, along with a clonus of the patella that lasted for an hour after waking from the anesthetic. Babinski observed this intriguing phenomenon of selective exaggeration of tendon reflexes during narcosis to be quite common. It serves as a valuable diagnostic indicator of excessive tendon reflexes in cases where there's uncertainty during regular assessments. Sometimes the contracture would ease, but only during the deepest sleep, lasting even beyond the conjunctival reflex and responses to pricking of normal limbs. Furthermore, the contracture would return 20 to 25 minutes before any sign of consciousness. If an attempt was made to relieve the contracture while fully anesthetized and completely unconscious, a spasmodic movement would occur, further exaggerating the abnormal posture of the limb. At times, the leg would even be forced into a flexor contracture.
The case above described was the one which led Babinski to his new formula of the Physiopathic Syndrome. This he describes in general terms as follows:
The case mentioned above was the one that led Babinski to his new concept of the Physiopathy Syndrome. He describes it in broad terms as follows:
These disorders consist in post-traumatic contractures, paralyses or paretic states, but are not attended by any of the signs of the so-called organic diseases, either of lesions of the central nervous system, or of the peripheral nervous system, or of the great arterial systems. In fact, these disorders somewhat resemble hysterical manifestations. The underlying lesions appear to be sometimes extremely small; in fact, so minimal as to be out of proportion with the functional disorders that they produce. These disorders do not correspond with any known anatomical regions, but they are singularly tenacious, and, unlike truly hysterical (pithiatic) phenomena, they are completely resistant to suggestion. Yet it is not merely in resistance to suggestive therapy that these reflex disorders differ from hysteria; for besides the[382] contracture and the paralysis or paresis found in the different segments of the extremity concerned, the complete Babinski syndrome includes also muscular atrophy, exaggeration of tendon reflexes, alterations of skin reflexes (even amounting to areflexia), hypotonia, mechanical over-excitability of the muscles with retardation of the muscular contraction; quantitative changes in electrical excitability of muscles (excess or diminution without R. D.), mechanical over-excitability, and occasionally electrical over-excitability of the nerves, disturbances in objective and subjective sensibilities (anesthesia and pains), heat regulation disorders (especially hyperthermia), and disorder of the vasomotors (cyanosis, skin redness, oscillometric lowering at the periphery of the extremity in the presence of low temperature), secretory disorders, and various trophic disorders of the bony system, the skin, and the nails.
These disorders involve post-traumatic contractures, paralysis, or weak states, but they don't show any of the signs associated with so-called organic diseases, whether from injuries to the central nervous system, the peripheral nervous system, or the major arterial systems. In fact, these disorders are somewhat similar to hysterical manifestations. The underlying issues sometimes appear to be extremely small; in fact, they can be so minimal that they seem disproportionate to the functional disorders they cause. These disorders don't align with any known anatomical regions, but they are remarkably persistent, and unlike true hysterical (pithiatic) phenomena, they are completely resistant to suggestion. However, it's not just the resistance to suggestive therapies that sets these reflex disorders apart from hysteria; in addition to the contracture and paralysis or weakness observed in different parts of the affected limb, the complete Babinski syndrome also includes muscle atrophy, exaggerated tendon reflexes, changes in skin reflexes (even to the point of areflexia), hypotonia, mechanical over-excitability of the muscles with delayed muscle contraction, quantitative changes in the electrical excitability of muscles (either excessive or reduced without R. D.), mechanical over-excitability, and sometimes electrical over-excitability of the nerves. There are also issues with objective and subjective sensations (such as numbness and pain), heat regulation problems (especially hyperthermia), disruptions to vasomotor functions (like cyanosis, skin redness, and blood pressure drops in the extremities when exposed to low temperatures), secretory disorders, and various trophic issues affecting the bones, skin, and nails.
Despite the permutations and combinations of these symptoms, according to Babinski they amount to a new group of disorders and represent a nosological species: a species of disease phenomena that lies midway between the organic affections and hysterical disorders. Babinski proposes the term physiopathic for these phenomena, a term which excludes the connotation of hysteria and all forms of psychopathia, on the one hand, and seems, on the other, to express the fact of their correspondence to a physical material perturbation in the nervous system of a novel sort.
Despite the variations and combinations of these symptoms, Babinski suggests that they make up a new group of disorders and represent a distinct category of disease. This category of conditions exists between physical ailments and hysterical disorders. Babinski proposes the term physiopathic for these conditions, a term that avoids the implications of hysteria and any types of psychopathology, while also indicating that they correspond to a unique physical disturbance in the nervous system.
Bullet wound of ankle: Contracture effect of chloroform.
Bullet wound of ankle: Contracture effect of chloroform.
Case 275. (Babinski and Froment, 1917.)
A man was wounded, September 1, 1914, by a bullet in the left ankle. Contracture of the foot and of the four outer toes in extension followed, with a flaccid paralysis of the great toe. The left knee-jerk was a little stronger than the right; the left Achilles jerk also appeared weaker but observation was difficult on account of contracture of the foot.
A man was shot in the left ankle on September 1, 1914. This caused his foot and four outer toes to contract in extension, along with a weak paralysis of the big toe. The left knee-jerk reflex was slightly stronger than the right; the left Achilles reflex seemed weaker, but it was hard to assess due to the foot's contraction.
Chloroformed, October 22, 1915: There was no sharply defined asymmetry of the tendon reflexes. The left Achilles reflex appeared a little weaker. In the phase of muscular resolution, the contracture disappeared entirely, but it reappeared a little after the return of the tendon reflexes. The reappearance of the contracture preceded the reappearance of consciousness from twenty to twenty-five minutes.
Chloroformed, October 22, 1915: There was no clear asymmetry in the tendon reflexes. The left Achilles reflex seemed slightly weaker. During the phase of muscle relaxation, the tightness disappeared completely, but it came back shortly after the tendon reflexes returned. The return of the tightness occurred twenty to twenty-five minutes before the patient regained consciousness.
Post-typhoidal reflex or physiopathic disorder of right leg. Elective exaggeration under chloroform.
Post-typhoidal reflex or physiopathic disorder of the right leg. Planned exaggeration under chloroform.
Case 276. (Babinski and Froment, 1917.)
A typhoid patient, October 20, 1914, showed phlebitis and abscess of the right buttock with contracture of pelvic trochanteric muscles. He was sent to the Pitié on medicolegal grounds.
A typhoid patient, October 20, 1914, showed phlebitis and abscess of the right buttock with muscle tightness in the pelvic area. He was sent to Pitié for legal medical reasons.
September 22 there was found a slight laxity of the patella tendon, as well marked on the left side as on the right. The right side was more cyanotic, due to the inactivity of the limb. There was no edema. Tendon and skin reflexes were normal. The lack of power was diagnosticated as purely functional, and the report was rendered that the soldier could begin to walk as soon as he desired. The two knee-jerks were noted to be stronger and polykinetic, and the right knee-jerk appeared a little stronger.
On September 22, a slight looseness of the patellar tendon was found, noticeable on both the left and right sides. The right side showed more bluish discoloration due to the limb's inactivity. There was no swelling. Tendon and skin reflexes were normal. The lack of strength was diagnosed as purely functional, and it was reported that the soldier could start walking whenever he wanted. Both knee-jerks were observed to be stronger and had multiple movements, and the right knee-jerk seemed slightly stronger.
The patient was chloroformed, October 25, 1915. Almost immediately, the knee-jerks, Achilles jerks, plantar, and cremasteric reflexes disappeared. During the first period of anesthesia, there was no accentuation of the reflexes, but at the beginning of recovery the anticipated reappearance of the right knee-jerk was observed. This knee-jerk was already sharply defined at a moment when the left knee-jerk was still abolished. In a later phase of recovery, the right knee-jerk was very markedly exaggerated and a patellar clonus was demonstrable on the right side. Even percussion of the left patellar tendon brought about a contraction of the right adductors. There was a true clonic and tonic spasm of these muscles. On the other hand, percussion of the right patellar tendon was able to provoke no contraction of either right or left adductors. Nor was there at any time any ankle clonus.
The patient was given chloroform on October 25, 1915. Almost immediately, the knee-jerk, Achilles jerk, plantar, and cremasteric reflexes disappeared. During the initial phase of anesthesia, there was no increase in the reflexes, but as recovery began, the expected return of the right knee-jerk was noted. This knee-jerk was already clearly defined at a point when the left knee-jerk was still absent. In a later stage of recovery, the right knee-jerk was significantly exaggerated, and there was a noticeable patellar clonus on the right side. Even tapping the left patellar tendon caused a contraction of the right adductors. There was a genuine clonic and tonic spasm of these muscles. Conversely, tapping the right patellar tendon did not trigger any contraction of either the right or left adductors. At no point was there any ankle clonus.
Hysterical lameness (bullet wound of calf) cured, but the associated “reflex” disorder (in the sense of Babinski and Froment) NOT cured.
Hysterical lameness (gunshot wound to the calf) has been treated, but the related “reflex” disorder (in the sense of Babinski and Froment) has NOT been resolved.
Case 277. (Vinny, April, 1916.)
A corporal was wounded by a bullet in the calf, September 8, 1914. At the end of July, 1915, his lameness continued and he disliked to lean on his left leg which bent under him. There was a slight atrophy of the left calf. The lower leg could not be extended upon the thigh if the foot was in dorsal flexion, and the dorsal flexion of the foot was itself limited. There were no reflex, vasomotor or electrical disorders. The man was given the usual treatment by Vincent and soon learned to carry his body on either foot, and, being well disposed, speedily abandoned his lameness, acquiring such skill in movements that he became monitor over the other soldiers, watching over them in his capacity as corporal.
A corporal was shot in the calf on September 8, 1914. By the end of July 1915, he was still limping and didn’t like putting weight on his left leg, which buckled under him. There was a bit of muscle wasting in his left calf. He couldn’t extend his lower leg on his thigh if his foot was pointed upward, and that upward flexion of the foot was limited as well. There were no reflex, blood flow, or electrical issues. The standard treatment was provided by Vincent, and he quickly learned to balance his weight on either foot. With a positive attitude, he soon stopped limping and became so skilled in movement that he took on a supervisory role over the other soldiers, overseeing them in his position as corporal.
For about a year he thus served as monitor, and when fully dressed did not seem abnormal or look as if he were walking lame. However, after walking, say 6 kilometers, rapidly, he dragged his leg; nor was extension of the lower leg upon the thigh absolutely complete in habitual walking, though he was able to extend perfectly if requested. Dorsal flexion of the foot was also still somewhat limited, and the measurements of the two lower extremities at both calf and thigh showed a persistent slight atrophy on the left side. He was then sent into the auxiliary service and did good work as draughtsman. In the winter the left foot got cold rather easily.
For about a year, he served as a monitor, and when fully dressed, he didn’t appear unusual or walk with a limp. However, after walking about 6 kilometers quickly, he would drag his leg; also, when he walked normally, he couldn’t fully extend his lower leg on his thigh, though he could do so perfectly if asked. The upward movement of his foot was still a bit limited, and measurements of both his calves and thighs showed a consistent slight shrinkage on the left side. He was then assigned to auxiliary service and did well as a draftsman. In the winter, his left foot got cold pretty easily.
This case is instanced by Vincent to support the contentions of Babinski and Froment that the truly “physiopathic” or “reflex” disorders do not completely clear up in the recovery from the associated hysterical disorders. That limb, which is the seat of physiopathic disorder, is not in a state of meiopragia.
This case is pointed out by Vincent to back up the arguments of Babinski and Froment that the genuinely “physiopathic” or “reflex” disorders do not fully resolve during the recovery from the related hysterical disorders. That limb, which is affected by the physiopathic disorder, is not in a condition of meiopragia.
Foot trauma: Pains and dysbasia, hysterical; slight atrophy of calf, physiopathic. Differential disappearance of hysterical symptoms; increase of physiopathic symptoms.
Foot injury: Pain and difficulty walking, hysteria; slight muscle wasting in the calf, caused by physical factors. Gradual reduction of hysterical symptoms; increase in physical symptoms.
Case 278. (Vinny, April, 1917.)
Clovis Vincent examined a man who had been wounded in the foot but without injury to the bones. He was first examined in July, 1915, when he complained of foot pains and was walking with crutches. The left calf was smaller than the right (4 cm.). The tendon reflexes were normal. There was no abnormality of electrical reaction. There was no proportionality between the trouble with walking and the organic status. A large part of the trouble appeared to be hysterical. In fact, upon treatment, the man was soon able to abandon the crutches and to walk, though lamely. He was put into the auxiliary military service.
Clovis Vincent examined a man who had hurt his foot but didn’t damage any bones. He was first seen in July 1915, when he complained of foot pain and was using crutches. His left calf was smaller than his right (by 4 cm). The tendon reflexes were normal, and there were no unusual electrical reactions. There was no clear connection between his walking difficulties and his physical condition. A significant part of the problem seemed to be psychological. In fact, after treatment, the man was quickly able to stop using the crutches and walk, albeit with a limp. He was placed into auxiliary military service.
However, the pains grew more marked and the lameness increased. Incapable of working, the patient was sent to the neurological center at Montpellier, whence he came to the neurological center at Tours in September, 1916. He had never been confined to bed, and had never ceased his daily walking, aided by a cane. The walking disorder was very pronounced. The patient said he was still suffering much. The difference between the two calves was now 8 cm. and the thigh was atrophied, though the atrophy had been absent in July, 1915. There was hyperexcitability of leg muscles. The right foot was colder than the left. The hysterical phenomena, so pronounced in July, 1915, were now absent, yet the reflex phenomena were sufficient to invalid the man.
However, the pain became more intense and the limp got worse. Unable to work, the patient was referred to the neurological center in Montpellier, from where he was sent to the neurological center in Tours in September 1916. He had never been bedridden and had kept up his daily walks with the help of a cane. The walking issue was very noticeable. The patient reported that he was still in a lot of pain. The difference between the two calves was now 8 cm, and the thigh was atrophied, even though there had been no atrophy in July 1915. The leg muscles showed hyperexcitability. The right foot was colder than the left. The hysterical symptoms that had been so evident in July 1915 were now gone, but the reflex issues were enough to render the man disabled.
Shell-shock paraplegia may AFTER TWENTY MONTHS develop vasomotor and secretory disorders: The whole to vanish on treatment.
Shell-shock paraplegia may AFTER TWENTY MONTHS develop vasomotor and secretory disorders: The whole to vanish on treatment.
Case 279. (Roussy, April, 1917.)
A foot chasseur, 22, a farmer in civil life, sustained shell-shock à distance, June 2, 1915. He had no wound, but lost consciousness. He was evacuated for “contusion of back” to a hospital June 4 to 12; for “contusion of back and commotio cerebri” to Portarlier, to July 21; for “internal contusions and commotio cerebri” to Besançon, where he was in three hospitals up to May 31, 1916, and the diagnosis “hysteria, old commotio cerebri and trepidant astasia-abasia” was rendered and psychotherapy tried. The man was then evacuated to Saint Ferréol and the diagnosis “hysterical paraplegia” rendered. He finally reached Veil-Picard in February, 1917, still victim of paraplegia.
A foot soldier, 22, a farmer in civilian life, experienced shell shock at a distance on June 2, 1915. He had no visible injuries but lost consciousness. He was evacuated for "back contusion" to a hospital from June 4 to June 12; for "back contusion and concussion" to Portarlier, until July 21; and for "internal contusions and concussion" to Besançon, where he stayed in three hospitals until May 31, 1916. The diagnosis of "hysteria, old concussion, and tremulous astasia-abasia" was made, and psychotherapy was attempted. The man was then evacuated to Saint Ferréol where he was diagnosed with "hysterical paraplegia." He finally arrived at Veil-Picard in February 1917, still suffering from paraplegia.
Up to this point there had been no signs suggestive of organic lesion of the spinal cord or any hysteroörganic intimation whatever. But in February, 1917, besides the motor disorder there was a hypothermia of several degrees, with cyanosis and hyperidrosis of both feet, with a marked diminution (and absence on one side) of the plantar cutaneous reflexes. The man was also victim of “hysterical pregnancy.” The cyanosis, hypothermia and hyperidrosis lasted six weeks.
Up until now, there were no signs indicating any organic damage to the spinal cord or any hints of hystero-organic issues. However, in February 1917, in addition to the motor disorder, there was a drop in body temperature of several degrees, along with blue discoloration and excessive sweating of both feet, and a significant decrease (with none on one side) in the plantar reflexes. The man was also suffering from “hysterical pregnancy.” The blue discoloration, low body temperature, and excessive sweating lasted for six weeks.
March 23 the man was given treatment and for the first time in 21 months was able to stand and walk. The foot now turned from blue to red, and instead of cold became warm, even hot. In about a week the hyperthermia diminished, and, with the other troubles, disappeared. There remained only a slight swelling of the foot and ankle joints, due to the painful exercises given the patient.
March 23, the man received treatment and for the first time in 21 months was able to stand and walk. The foot changed from blue to red, and instead of being cold, it became warm, even hot. In about a week, the hyperthermia decreased, and along with the other issues, vanished. Only a slight swelling of the foot and ankle joints remained, due to the painful exercises prescribed for the patient.
It would seem, then, that a hysterical paraplegia of long duration may finally associate itself with marked vasomotor and secretory disorders and that these may be altered with extreme rapidity on the very day in which the hysterical phenomena are removed, and quite disappear in a fortnight.
It seems that a long-term hysterical paraplegia can eventually be linked to significant issues with blood flow and gland functions, and these can change very quickly on the same day the hysterical symptoms are resolved, often disappearing completely within two weeks.
Tetanus clinically cured: Phenomena in part reproduced UNDER CHLOROFORM ANESTHESIA five weeks afterward.
Tetanus was clinically cured: Some phenomena were partially reproduced under chloroform anesthesia five weeks later.
Case 280. (Monier-Vinard, July, 1917.)
An infantryman, wounded at Notre Dame de Lorette, May 9, 1915, by a shell fragment in the right popliteal space, was given a preventive injection of 5 c.c. of antitetanic serum, evacuated to a hospital, May 12, and developed signs of tetanus August 1, with trismus and pains and spasms in the right leg.
An infantryman, injured at Notre Dame de Lorette on May 9, 1915, by a shell fragment in the right kneecap area, received a preventive injection of 5 c.c. of antitetanic serum, was evacuated to a hospital on May 12, and showed symptoms of tetanus on August 1, experiencing jaw stiffness and pain and spasms in the right leg.
The disease progressed with dysphagia, stiffness and paroxysmal hypertonia of the legs, especially of the right leg, fixed orthotonus of the trunk, neck hyperextended, arms stiff but able to move. Antitetanic serum was given daily. At the end of eight days there was a marked improvement and the whole course ran to approximate recovery in 25 days from the onset of tetanic symptoms, at which time the man was able to get up and walk on a crutch. The external popliteal nerve had been sectioned, and the foot was in a marked equinovarus.
The disease progressed with difficulty swallowing, stiffness, and sudden muscle tightness in the legs, especially the right leg, with the trunk held rigidly upright, the neck bent back, and arms stiff but movable. They administered antitetanic serum daily. By the end of eight days, there was significant improvement, and the overall recovery took about 25 days from the start of the tetanic symptoms, at which point the man could get up and walk with a crutch. The external popliteal nerve had been cut, and his foot had a noticeable inward and downward position.
Chloroform was administered for the purpose of straightening the foot, September 2, that is, about five weeks after the apparent end of the tetanus. The first stage of the anesthesia lasted about two minutes, but at this point the trunk and leg muscles passed into a state of diffuse contracture. In fact, a tetanic syndrome took place in the midst of the anesthesia. At a time when the corneal reflex was completely abolished, it was still impossible, with the exertion of the greatest strength, to flex the segments of the lower extremities. Moreover, the trunk was stiffly extended and the jaws were in trismus. Tonic and clonic contractions were produced by the efforts made to straighten the foot, and these contractions passed from the right side to the left. The chloroform was now increased and a transient resolution of the muscles was obtained, lasting hardly more than a half minute. As all efforts to reduce the pedal deformity failed, anesthesia was[389] stopped. The contractures and paroxysms lasted a few minutes. The knee-jerks were extremely exaggerated and there was a bilateral ankle clonus. After a brief phase of excitement, the patient emerged from anesthesia, began to talk with his comrades, and ate his usual meal without inconvenience. The chloroform anesthesia had lasted twenty minutes, and 60 grams had been administered.
Chloroform was given to straighten the foot on September 2, about five weeks after the apparent end of the tetanus. The first stage of anesthesia lasted around two minutes, but at this point, the trunk and leg muscles went into a state of generalized contraction. In fact, a tetanic syndrome occurred during the anesthesia. At a moment when the corneal reflex was completely gone, it was still impossible, even with maximum effort, to bend the parts of the lower limbs. Additionally, the trunk was rigidly extended and the jaw was locked. Tonic and clonic contractions happened due to the attempts to straighten the foot, and these contractions moved from the right side to the left. The chloroform dosage was increased, resulting in a temporary relaxation of the muscles that lasted less than half a minute. Since all attempts to correct the foot deformity failed, anesthesia was[389] stopped. The contractions and spasms lasted a few minutes. The knee-jerks were very exaggerated, and there was clonus in both ankles. After a brief period of excitement, the patient came out of anesthesia, started talking with his companions, and ate his usual meal without any issues. The chloroform anesthesia lasted twenty minutes, and 60 grams had been used.
It was now determined to section the tendo Achilles and the tibialis posticus. September 8 the man was chloroformed again and the same phenomena were exactly reproduced. Sixty grams of chloroform was again administered. The tendon resections permitted placing the foot in the proper attitude. Next day the patient was examined neurologically. The skin reflexes were found normal. The Achilles and knee-jerks were somewhat exaggerated, but equal on the two sides. There was no ankle clonus. Sensations proved normal. There was a mechanical hyperexcitability of the muscles of the anterior aspect of the thighs and of the calf.
It was decided to cut the Achilles tendon and the posterior tibial tendon. On September 8, the man was put under chloroform again and the exact same effects were observed. Sixty grams of chloroform were administered once more. The tendon resections allowed the foot to be positioned correctly. The following day, the patient underwent a neurological examination. The skin reflexes appeared normal. The Achilles and knee reflexes were somewhat exaggerated but equal on both sides. There was no ankle clonus. Sensations were normal. The muscles on the front of the thighs and the calf showed mechanical hyperexcitability.
In another case chloroformed 17 months after recovery from tetanus no such phenomena appeared. It would seem that the impregnation with tetanic virus or toxin must last in the nervous system a good deal longer than the apparent disease clinically lasts, but that this belated and concealed intoxication eventually passes.
In another case, someone was chloroformed 17 months after recovering from tetanus, and no such phenomena showed up. It seems that the presence of the tetanic virus or toxin must remain in the nervous system for a significantly longer time than the clinical symptoms of the disease, but this delayed and hidden intoxication eventually goes away.
The phenomena are perhaps analogous to those of Babinski and Froment’s so-called post-traumatic physiopathic or reflex phenomena. It was following the special work of Babinski and Froment upon the use of chloroform anesthesia in detecting physiopathic conditions that Monier-Vinard made his observations in cases of tetanus.
The phenomena are perhaps similar to those of Babinski and Froment’s so-called post-traumatic physiopathic or reflex phenomena. It was after the specialized work of Babinski and Froment on using chloroform anesthesia to identify physiopathic conditions that Monier-Vinard made his observations in cases of tetanus.
Shell-shock from falling of shell at a distance: Hysterical hemiplegia, terminating in brachial monoplegia. Case to show that the reflex or physiopathic disorders of Babinski and Froment may occur without mechanical injury in the region involved.
Shell shock from distant shell explosions: Hysterical half-paralysis, leading to arm paralysis. This case demonstrates that the reflex or physiopathic disorders of Babinski and Froment can happen without any physical injury in the affected area.
Case 281. (Ferrand, June, 1917.)
A soldier of the class of 1917 who never went to the front, while in training at Belfort, felt violent emotion on the occasion of the falling of a big shell in the town of Belfort. The explosion was a good distance from him. He lost consciousness a few moments, February 23, 1917, and almost at once found himself unable to move his left side. He was hemiplegic three months, but his leg shortly regained power. December 23 he entered a neurological center with his arm flaccid and a paralysis affecting the shoulder also. There was an almost complete anesthesia of the arm terminating in segmentary fashion about the shoulder, and the whole of the left side was slightly hypesthetic, although there was no disorder of motion except in the arm. The tendon reflexes of the left arm were exaggerated, and there was even contracture upon percussion of the muscles themselves. Percussion of the thenar and hypothenar eminences produced movements of the hand. There were several vasomotor disorders. Percussion led to large vasomotor plaques, and rubbing of the skin produced a reddening which passed away slowly. The hand was red and cold. Slight electrical hyperexcitability of flexors with feeble galvanic current; excitation of the extensors not associated with any contractions of the antagonist muscles. Threshold lower for flexors on the affected side in the forearm. Half centimeter atrophy of the biceps. The forearm and hand were possibly slightly increased in volume from a blue edema of the dorsal surfaces. The man was very timid, complained little, and accepted all treatment, which, however, was not very effective. This is presented by Ferrand as a case with physiopathic disorder in the sense of Babinski and Froment, though it does not present any sign of organic lesion whatever.
A soldier from the class of 1917 who never went to the front lines, while in training at Belfort, experienced intense emotions when a large shell fell in the town. The explosion was a good distance away from him, but he lost consciousness for a few moments on February 23, 1917, and soon found himself unable to move his left side. He was hemiplegic for three months, but his leg regained strength relatively quickly. On December 23, he entered a neurological center with a weak arm and paralysis affecting his shoulder as well. There was almost complete loss of feeling (anesthesia) in the arm, which ended abruptly around the shoulder, and the entire left side was slightly less sensitive (hypesthetic), although there were no issues with movement except in the arm. The tendon reflexes in the left arm were heightened, and there was even muscle tightness when tapped. Tapping the fleshy parts of the hand produced movements in the hand. He had several blood flow issues; tapping caused large blood flow changes, and rubbing the skin caused a redness that faded slowly. The hand was red and cold. There was slight electrical sensitivity in the flexor muscles with a weak galvanic current, and excitement in the extensor muscles did not trigger contractions in the opposing muscles. The threshold was lower for the flexors on the affected side in the forearm. There was half a centimeter of muscle wasting (atrophy) in the biceps. The forearm and hand might have been slightly swollen due to a bluish swelling on the backs of the hands. The man was very timid, hardly complained, and accepted all treatments, which, however, were not very effective. Ferrand presents this as a case of a physiopathic disorder in the sense of Babinski and Froment, although it shows no signs of any organic lesion at
Shell fire: Delayed shell-shock symptoms, sub-lethal, appearing in England.
Shell fire: Delayed symptoms of shell shock, non-fatal, showing up in England.
Case 282. (McWalter, April, 1916.)
A soldier was picked up insensible in the public street and brought to hospital by ambulance, unconscious, breathing stertorously, pupils dilated, lips parched, unresponsive to stimuli, but without signs of injury or alcoholism.
A soldier was found unconscious on the street and taken to the hospital by ambulance. He was breathing heavily, his pupils were dilated, his lips were dry, and he didn’t respond to any stimuli. However, there were no signs of injury or alcohol use.
The pulse grew slower, the respirations more sighing, the heart-beat more diffused and labored; but towards evening, about eight hours after admission, he began to move the eyelids and lips, and muttered a response to the request for his name. After ten more hours, respiration grew better, and Croton oil led to a movement of the bowels. Natural sleep intervened, and 18 hours after the onset of unconsciousness, the man woke up, and in the course of a few days became fairly well though still dazed and confused.
The pulse slowed down, the breathing became more like sighs, and the heartbeat felt more spread out and heavy; but around evening, about eight hours after he was admitted, he started to move his eyelids and lips, and mumbled a reply when asked for his name. After another ten hours, his breathing improved, and Croton oil prompted a bowel movement. He then fell into a natural sleep, and 18 hours after losing consciousness, the man woke up. Over the next few days, he recovered fairly well, though he still felt a bit dazed and confused.
This soldier had never received any definite injury in his war service, but McWalter attributes his break-down to the effects of the constant shocks from the bursting of shells, and the scattering of shrapnel.
This soldier had never suffered any specific injury during his time in the war, but McWalter believes his breakdown is due to the ongoing shocks from exploding shells and flying shrapnel.
McWalter generalizes that a soldier, in the course of some civil occupation after the war, might develop symptoms, even fatal symptoms, and still the death in the case would be a direct consequence of the war.
McWalter suggests that a soldier, during a civilian job after the war, might show symptoms, even life-threatening ones, and yet the death in that situation would still be a direct result of the war.
Shell-shock symptoms, some initial, with recovery—others late and gradual, with deterioration.
Shell-shock symptoms, some appearing initially with recovery—others showing up later and slowly, with worsening.
Case 283. (Smyly, April, 1917.)
A soldier became blind, deaf and dumb, as well as paralyzed, as a result of shell explosion. When he arrived at the hospital, he was able to see but had visual hallucinations. In a few days he recovered his hearing. There was a fine tremor of the hands, controllable by suggestion. There was an almost complete amnesia, but the patient remained able to read and write.
A soldier became blind, deaf, and mute, as well as paralyzed, due to a shell explosion. When he got to the hospital, he could see but was experiencing visual hallucinations. After a few days, he regained his hearing. His hands had a slight tremor that could be controlled with suggestion. He had almost complete amnesia, but he could still read and write.
The pain persisted several months. The patient was physically well and seemed perfectly intelligent despite his aphasia and amnesia. One night, he sprang out of bed, shouting, “The guns are coming over us!” and from that time forward was able to speak. Amnesia, however, supervened for the months in the Dublin Hospital, and the patient believed that he was still in France. He also became unable to read or write, and was unable to recognize any letters except those he had been taught to speak during his period of dumbness. Still later he got a flaccid paralysis of the legs. From seeming perfectly intelligent, he began to seem markedly deteriorated. Hypnosis with waking suggestions had no power upon him. After a time, intelligence reappeared, but there had not been any recovery of locomotion at the time of report.
The pain lasted for several months. The patient was physically fine and appeared completely intelligent despite his inability to speak and memory loss. One night, he jumped out of bed, yelling, “The guns are coming over us!” and from that moment on, he could speak. However, he developed amnesia during his months in the Dublin Hospital, believing he was still in France. He also lost the ability to read or write and could only recognize the letters he had learned to say during his time of silence. Later on, he experienced a weak paralysis in his legs. From seeming perfectly intelligent, he began to show significant decline. Hypnosis with waking suggestions had no effect on him. After some time, his intelligence returned, but there had been no recovery of movement at the time of the report.
Wounds, gas, burial: Collapse on home leave.
Wounds, gas, burial: Break down during time off at home.
Case 284. (E. Smith, June, 1916.)
A non-commissioned officer went through the first eleven months of the war in France and Flanders and was subjected to every kind of strain therein. He was wounded twice, gassed twice, and buried under a house, in each instance being treated in the field ambulance and returning to the trenches. Some time thereafter he was granted five days’ leave.
A non-commissioned officer spent the first eleven months of the war in France and Flanders, facing every kind of stress along the way. He was injured twice, gassed twice, and buried under a house, each time receiving treatment in a field ambulance before going back to the trenches. After some time, he was given five days of leave.
On reaching home, while waiting for a train, the officer suddenly collapsed and became unconscious. For months thereafter, he was the subject of a severe neurasthenia; “the whole of his trouble seemed to be due to the dread, lest on his return to the front, the added responsibilities which would fall upon his shoulders might be too much for him.” He thought his intelligence had been numbed by his experience. He thought his memory was unreliable, and that he could understand neither complex orders nor even the newspapers.
On getting home, while waiting for a train, the officer suddenly collapsed and lost consciousness. For months after that, he suffered from severe neurasthenia; “all of his issues seemed to come from the fear that when he returned to the front, the extra responsibilities he would have to take on might be too overwhelming for him.” He felt like his mind had been dulled by his experiences. He believed his memory was unreliable and that he couldn’t grasp complicated orders or even the newspapers.
As to the reason for his maintenance of composure at the front, this may be laid to the excitement, the officer’s sense of responsibility, and the example he felt he should set his men. This kind of case[394] “demands a great deal of patient and sympathetic attention before the real cause is elicited, and then months of daily reëducation to build up anew the man’s confidence in himself.”
As for why he stayed calm at the front, it could be attributed to the excitement, the officer’s sense of responsibility, and the example he wanted to set for his men. This kind of situation[394] “requires a lot of patient and caring attention before uncovering the real cause, and then months of daily retraining to rebuild the man’s confidence in himself.”
Bullet wound of neck: Late sympathetic nerve effect.
Bullet wound of neck: Delayed sympathetic nerve response.
Case 285. (Chubby, January, 1915.)
A Belgian was wounded, October 21, 1914, at Dixmude. The bullet wound was just below the right mastoid process. He was admitted to the London General Hospital, October 29. He said that the bullet had passed into the tonsil, lodging there, but that on the third day, while vomiting, he brought up the tonsil with the bullet in it. There was in fact a large ragged wound at the site of the right tonsil. He could swallow fluids only, but articulated clearly. There was a question of injury to the following nerves: facial, glossopharyngeal, vagus, hypoglossal, spinal accessory, and sympathetic. None of these nerves, however, appeared actually to have been injured. The difficulty in swallowing was due probably to the faucial wound, and it is hard to see how the pharynx could have been involved on account of the perfect articulation. November 3 the right sympathetic nerve was slightly affected; the right pupil was smaller than the left although it reacted to light. November 12 the patient left the hospital and nothing further is known of his history. Thus there was a late effect upon the sympathetic nerve thirteen days after the wound.
A Belgian was injured on October 21, 1914, in Dixmude. The bullet wound was just below the right mastoid process. He was admitted to the London General Hospital on October 29. He mentioned that the bullet had passed into his tonsil and became lodged there, but on the third day, while vomiting, he expelled the tonsil with the bullet still in it. There was actually a large, ragged wound at the site of the right tonsil. He could only swallow liquids, but he spoke clearly. There was a concern about damage to the following nerves: facial, glossopharyngeal, vagus, hypoglossal, spinal accessory, and sympathetic. However, none of these nerves seemed to be actually injured. The difficulty in swallowing was probably due to the wound in the back of the throat, and it’s hard to see how the pharynx could have been affected given the clear speech. On November 3, the right sympathetic nerve was slightly impacted; the right pupil was smaller than the left, although it did react to light. On November 12, the patient left the hospital, and nothing further is known about his history. Thus, there was a delayed effect on the sympathetic nerve thirteen days after the injury.
Re peripheral nerve disorders, see remarks under Case 252 (Tubby).
Re peripheral nerve disorders, see comments under Case 252 (Tubby).
Fall from horse under shell fire: Crural monoplegia, hysterical. Reminiscence? Autosuggestion?
Fall from horse under artillery fire: Leg paralysis, hysterical. Memory? Self-suggestion?
Case 286. (Forsyth, December, 1915.)
A patient of Forsyth had been exercising a high-spirited horse. Artillery fire close by made the horse leap sidewise, and the rider fell, his back striking the ground. He seemed to be curiously shaken out of proportion to the gravity of the fall. In a day or so, he lost the use of one leg.
A patient of Forsyth had been riding a spirited horse. Nearby artillery fire startled the horse, causing it to jump sideways, throwing the rider off his horse and onto the ground. He appeared to be oddly shaken, especially given how serious the fall was. Within a day or so, he lost the ability to use one of his legs.
He recalled a rather similar incident: He had taken a hand in a local uprising in a distant quarter of the world. While he was escaping up a mountain track, a rifle-shot from the enemy brought down his horse, which rolled over and threw him violently against a boulder, where the small of the back met the force of the impact. He felt intense pain and lost consciousness. Upon recovery he found he was paralyzed. At the end of several days, in a hiding-place in the rocks, he found himself still unable to move his legs. The friend who had carried him to the hiding-place refused to leave him. He thought of suicide, but then discovered that he could move: at first, the big toes, then the ankles, then the knees, and finally the hips. He was finally able to get into the saddle.
He remembered a similar incident: he had been involved in a local uprising in a faraway part of the world. While he was escaping up a mountain path, a gunshot from the enemy took down his horse, which stumbled and threw him hard against a rock, causing pain in his lower back from the impact. He felt intense pain and lost consciousness. When he woke up, he found he was paralyzed. After several days in a hiding spot in the rocks, he realized he still couldn’t move his legs. The friend who had carried him there refused to leave him. He considered suicide but then discovered he could move: first his big toes, then his ankles, then his knees, and finally his hips. Eventually, he was able to get back on his horse.
Moreover, years before, he had heard that a man who broke his back was paralyzed in the legs.
Moreover, years earlier, he had heard that a man who broke his back was paralyzed from the waist down.
Re autosuggestion, Babinski remarks that suggestion may work in hystero-organic cases not precisely as in hysterical cases. Autosuggestion may here replace or accompany the ordinary heterosuggestion. Some temporary disturbance—a slight pain, a trivial injury, or a mere bruise—may start up a complex process of autosuggestion in which it may be difficult to unravel the part played by the patient’s own reflexes, his previous experience and beliefs (in this case, the reminiscences of a similar accident), the solicitude of his friends, and the medical examination itself. Babinski believes that hysterical paraplegia or monoplegia never appears automatically under the influence of emotion; never appears after the manner of sweating, diarrhea, or blushing.
Regarding autosuggestion, Babinski notes that suggestion might not function in hysterical cases the same way it does in hystero-organic cases. In these situations, autosuggestion can either replace or complement the usual heterosuggestion. Some temporary issue—a minor pain, a small injury, or just a bruise—can trigger a complex process of autosuggestion, making it hard to untangle the roles played by the patient's own reflexes, their past experiences and beliefs (in this instance, memories of a similar incident), the concern of their friends, and the medical examination itself. Babinski argues that hysterical paraplegia or monoplegia does not arise automatically from emotional influence; it doesn't occur like sweating, diarrhea, or blushing.
Shell explosion; struck in cave-in: Symptoms in right leg (antebellum experience).
Shell explosion; caught in collapse: Symptoms in right leg (antebellum experience).
Case 287. (Myers, March, 1916.)
A private, 26 years old, had 11 months’ service and one month’s service in France. He arrived at a base hospital the day after his shock. Concussion had caused the dug-out in which he was standing to collapse. A beam struck him on the left side of the face, and pinned him to the ground on his right side. A piece of iron fell on the left side of his back, and his right leg was pinned by a cross beam on the back of his thigh. He was dazed by the shock; was released and was able to walk, but complained of a pain in the right groin and a giving-way of the right knee. The medical officer arrived about an hour later. A numbness, or state of no feeling, in the right thigh appeared, and increased to the point of total analgesia to the level of the upper margin of the patella save for a narrow strip in the mid-line on the posterior aspect of the leg. The only area of complete anesthesia and algesia was on the outside of the lower half of the leg.
A private, 26 years old, had 11 months of service and one month of service in France. He arrived at a base hospital the day after his shock. Concussion caused the dugout he was standing in to collapse. A beam hit him on the left side of the face and pinned him to the ground on his right side. A piece of iron fell on the left side of his back, and his right leg was pinned by a cross beam on the back of his thigh. He was stunned by the shock; he was released and managed to walk, but he complained of pain in the right groin and a feeling of instability in the right knee. The medical officer arrived about an hour later. Numbness, or a lack of feeling, in the right thigh developed and increased to the point of complete insensitivity up to the upper edge of the kneecap, except for a narrow strip in the center on the back of the leg. The only area of total lack of sensation was on the outside of the lower half of the leg.
According to the patient, it seems that about three years before, he had been buried four feet deep in a brick yard, beneath a heap of clay. He had felt it most in the right leg, but the thigh had been merely stiff and sore, and not numb. The patient admitted that the present accident immediately reminded him of his previous experience. There were no tremors or sensory disorders in the face, arms, chest, back, or abdomen. There was diminished sensibility to cotton wool of the left buttock (across which a plank had fallen), and there was a degree of hypalgesia of the buttock. The right thigh showed a degree of thermanalgesia and slight loss of vibratory sense. The corneal and conjunctival reflexes were diminished, and the knee-jerk was unobtainable on the right side. Three days later, there was a marked improvement with almost complete return to normal, whereupon the patient was sent to a convalescent camp.
According to the patient, it seems that about three years ago, he had been buried four feet deep in a brick yard under a pile of clay. He felt it mostly in his right leg, but his thigh was just stiff and sore, not numb. The patient admitted that the current accident immediately brought back memories of his previous experience. There were no tremors or sensory issues in his face, arms, chest, back, or abdomen. He had decreased sensitivity to cotton wool on his left buttock (where a plank had fallen), and there was some reduced pain sensitivity in that area. His right thigh showed some loss of temperature sensation and a slight decrease in vibratory sense. The corneal and conjunctival reflexes were diminished, and his knee-jerk reflex was absent on the right side. Three days later, there was significant improvement with almost a complete return to normal, after which the patient was sent to a recovery camp.
Emotional subject, ALWAYS WEAK IN LEGS; shell explosion; wound of back: PARAPARESIS.
Emotional subject, ALWAYS WEAK IN LEGS; shell explosion; back injury: PARAPARESIS.
Case 288. (Dejerine, February, 1915.)
A Lieutenant, 25, was wounded at Arras about 10 a.m. October 20, 1914, just as he was leaning on another officer’s shoulder looking at a card in a chateau room. A shell burst in the court yard. A fragment came in the window, struck him in the back and pushed him forward, whereupon he felt pain in the back and a severe dyspnea, due to the gas from the shell. He lost consciousness several times and the dyspnea lasted for about two hours. When he was picked up he could not walk.
A 25-year-old lieutenant was injured at Arras around 10 a.m. on October 20, 1914, just as he was leaning on another officer’s shoulder while looking at a map in a room in a chateau. A shell exploded in the courtyard. A fragment came through the window, hit him in the back, and pushed him forward, causing him pain in the back and severe shortness of breath from the gas released by the shell. He lost consciousness several times, and the shortness of breath lasted for about two hours. When he was picked up, he couldn't walk.
He was carried on a stretcher to the ambulance at Avin-le-Compte. During the fortnight there, he was also several times dyspneic. Strength left his legs and he could only get about on crutches. There was now a suppurating wound in the interscapular region where he had been struck by the shell fragment. Evacuated to Paris, he was operated upon on account of a tremendous abscess in the back, and the shell fragment and some bits of cloth were removed. The wound healed; but vague pains in the left thorax remained, especially when the man walked.
He was taken on a stretcher to the ambulance at Avin-le-Compte. During the two weeks he was there, he also had trouble breathing several times. His legs felt weak, and he could only move around on crutches. There was now an infected wound in the area between his shoulder blades where he had been hit by the shell fragment. After being evacuated to Paris, he underwent surgery for a large abscess on his back, and the shell fragment along with some pieces of cloth were removed. The wound healed, but he still felt vague pains in the left side of his chest, especially when he walked.
On examination, July 28, 1915, he would in the standing position hold his legs together with the feet resting on their external borders, especially on the left side. The toes were in plantar flexion, and the soles were arched upward more on the left side than on the right. In walking, the legs were always held in extension, the feet twisting outward. If an attempt was made to walk quickly, the man walked more and more upon the external borders of his feet, in such wise that the plantar surface and the heel turned up and became visible from above. He would get tired after five minutes’ walking even if he spread his legs out for a broader base of action. He could lift his legs only about 10 cm. from the bed, but could flex and slowly extend his lower leg on the thigh. He could not adduct or abduct the feet. Movements[398] of extension and flexion of leg on thigh were jerky and abruptly terminated, as also movements of thigh on hip. The patient could not sit, and when leaning forward he could not straighten up against resistance. The reflexes were normal. There was no sensory disorder. The electric reactions were normal. Pupils normal. There was slight hypertension of the spinal fluid and a slight excess of albumin. There were no lymphocytes.
On examination, July 28, 1915, he would stand with his legs together, resting his feet on their outer edges, particularly on the left side. His toes pointed downward, and the arches of his feet were more pronounced on the left than on the right. While walking, his legs were always straight, and his feet turned outward. If he tried to walk quickly, he ended up walking more on the outer edges of his feet, causing the soles and heels to lift and become visible from above. He would get tired after just five minutes of walking, even when he spread his legs out for a wider stance. He could only lift his legs about 10 cm off the bed but was able to flex and slowly extend his lower leg from the thigh. He couldn’t bring his feet together or move them apart. The movements of extension and flexion of the leg at the thigh were jerky and would stop abruptly, as did the movements of the thigh at the hip. The patient couldn’t sit, and when he leaned forward, he couldn’t straighten up against resistance. His reflexes were normal. There were no sensory issues. The electric reactions were normal. Pupils were normal. There was slight hypertension of the spinal fluid and a minor excess of albumin. There were no lymphocytes.
In accordance with Dejerine’s idea that these neuropaths always have antecedents looking in the same direction, it was found that he had always been an emotional person, easily affected, sympathetic with other people’s troubles, given to weeping. As Lieutenant, he had not had the courage to harangue his soldiers. He had often during his life felt his legs weaken during times of emotion and had sometimes been unable to walk, though nothing of the sort had happened during the campaign. He was sure he could get well, and wanted two months’ leave in order to get back to the front. There were no hereditary features in the case. A physician had told him that he had had meningitis. This possibly followed whooping cough. He had had orchitis after mumps at 16. He had not had children, nor had there been miscarriages since marriage at 21.
According to Dejerine’s idea that these neuropaths always have causes pointing in the same direction, it was found that he had always been an emotional person, easily affected, sympathetic to other people’s troubles, and prone to tears. As a Lieutenant, he hadn’t had the courage to give speeches to his soldiers. Throughout his life, he often felt his legs weaken during emotional moments and sometimes couldn’t walk, although this hadn't happened during the campaign. He was convinced he could recover and wanted two months of leave to return to the front. There were no hereditary factors in his case. A doctor had informed him that he had experienced meningitis, possibly following whooping cough. He had also had orchitis after mumps at 16. He hadn’t had children, nor had there been miscarriages since he got married at 21.
Wound near heart; delayed medical care; fear of having been shot through heart: Paraparesis (antebellum always “hit in the legs.”)
Wound near the heart; medical care delayed; fear of being shot through the heart: Paraparesis (before the war always “hit in the legs.”)
Case 289. (Dejerine, February, 1915.)
An infantryman, 20, was sent as a Colonel’s bicyclist about 1 p.m. September 30, 1914, with a message to one of the battalions. He was exposed on the way to shell and rifle fire, and was wounded by a bullet which entered 8 cm. below and internal to the left mammillary line and came out in the region of the left hypochondrium. He crawled to some village houses 20 or 25 meters away. Another cyclist came to transfer the order, but could not help him. A friend came to his aid but was struck by a bullet 10 meters off and remained on the ground for an hour while the young cyclist lay behind a tree on the roadside. At 3 o’clock it was possible to take him to a house around which shells were raining. Shortly afterward the house caught fire. The man was evacuated 6 kilometers to an ambulance in the night, and that night six of his wounded comrades died in the same room. The man had lost much blood and began to think that his heart had been hit. He choked, had violent palpitations, and intense thirst. By automobile next day he was taken to the railway station at Maison and was there for a day practically without food.
An infantryman, 20, was assigned as a Colonel’s cyclist around 1 p.m. on September 30, 1914, to deliver a message to one of the battalions. He was exposed to shell and rifle fire along the way and was shot by a bullet that entered 8 cm below and inside the left nipple line and exited in the area of his left upper abdomen. He crawled to some village houses about 20 or 25 meters away. Another cyclist came to deliver the order but couldn’t assist him. A friend rushed to help but got hit by a bullet 10 meters away and lay on the ground for an hour while the young cyclist hid behind a tree by the roadside. At 3 o'clock, it was possible to move him to a house that was getting bombarded. Shortly after, the house caught fire. He was evacuated 6 kilometers to an ambulance during the night, and that night, six of his wounded comrades died in the same room. The man had lost a lot of blood and began to think that his heart had been hit. He felt like he was choking, experienced violent heart palpitations, and had intense thirst. The next day, he was taken by car to the train station at Maison, where he spent a day nearly without food.
That evening, 36 hours after the wound, he was evacuated to Juivisez and stayed there one night in the temporary hospital. The hemorrhage had now practically ceased. When he arrived next morning at Vincennes he could hardly move, was unable to walk, had violent palpitation, precordial pain, and two nervous seizures, with outcries and weeping. Several days later he could not walk at all or raise himself in bed. He was operated on May 29; he afterward felt the same leg weakness and was still unable to walk. Early in December, when observed by Dejerine, he was able to stand on crutches with legs flexed, toes on the ground, and heels up. In walking he would scrape the ground with the dorsum of the foot.[400] The wound was now healed. Suppuration had been intense and the scars were extensive. Lying down, the man could move, though slowly, his lower extremities in every way, nor was there any diminution in the strength of his flexors and extensors. The patient in making movements against resistance would let go quickly and jerkily. The plantar reflexes were flexor but weak. There was no other reflex disorder, no evidence of sensory disorder, nor any sign of neuritis or arthritis. Lumbar puncture gave a normal fluid without tension.
That evening, 36 hours after the injury, he was evacuated to Juivisez and spent one night in the temporary hospital. The bleeding had mostly stopped. When he arrived the next morning at Vincennes, he could barely move, couldn't walk, was experiencing severe heart palpitations, chest pain, and two nervous breakdowns, with cries and tears. Several days later, he couldn’t walk at all or lift himself in bed. He had surgery on May 29; afterward, he felt the same weakness in his leg and still couldn’t walk. Early in December, when examined by Dejerine, he was able to stand on crutches with his legs bent, toes on the ground, and heels raised. While walking, he would drag the top of his foot along the ground.[400] The wound was now healed. The infection had been severe, and the scars were extensive. While lying down, he could move his lower limbs in every direction, albeit slowly, and there was no decrease in the strength of his flexors and extensors. When the patient attempted movements against resistance, he would release quickly and jerkily. The plantar reflexes were flexor but weak. There were no other reflex issues, no signs of sensory problems, nor any indication of neuritis or arthritis. A lumbar puncture showed normal fluid without pressure.
There were no hereditary features in the case. The man had been in childhood nervous and irascible, rolling on the ground, crying and weeping when crossed. He had had three attacks of appendicitis—one at 15 years and two at 19 years. After each attack he had felt weakness in the legs. He remembered, too, that after his nervous crises on being crossed, he had always felt this same weakness.
There were no hereditary traits in this case. The man had been anxious and irritable during childhood, often rolling on the ground, crying and upset when things didn't go his way. He had three bouts of appendicitis—one at 15 and two at 19. After each episode, he felt weak in his legs. He also recalled that after his emotional outbursts when he was upset, he always experienced that same weakness.
According to Dejerine, these paraplegic neuropaths, like functional gastropaths, cardiopaths, and victims of urinary disorder, have had earlier spells of the same kind, though milder than the attack which brings them to medical notice.
According to Dejerine, these paraplegic neuropaths, like those with functional gastric issues, heart problems, and urinary disorders, have experienced earlier episodes of the same kind, although they were milder than the incident that brings them to medical attention.
Wounds: Tic on attempts to walk; tremors. Recovery except for frontalis tic (ANTEBELLUM HABIT emphasized).
Wounds: Tic when trying to walk; tremors. Recovery, except for frontalis tic (ANTEBELLUM HABIT emphasized).
Case 290. (Westphal and Hübner, April, 1915.)
A substitute officer (mother nervous; always slightly excitable, easily fatiguable; had had a habit of wrinkling his forehead) sustained wounds September 8, 1914, in the foot and thigh. The wounds healed well, but in the hospital he slept badly and had battle dreams. When he essayed to walk, he had contractions of face muscles. There was a lively tic involving both face and neck muscles, with the head pulled to one side and backward. This grimacing was but slightly influencible by the will. There was a marked tremor of the arms. Gait was trippelnd. There were tremors of the whole body. There was also a slight hemi-hyperesthesia. The tendon reflexes were very lively; vasomotor disorders (feelings of cold and perspiration).
A substitute officer (his mother was nervous, always a bit excitable, and easily fatigued; he had a habit of wrinkling his forehead) suffered injuries on September 8, 1914, to his foot and thigh. The wounds healed well, but while in the hospital, he had trouble sleeping and experienced battle dreams. When he tried to walk, he had facial muscle contractions. There was a noticeable tic affecting both his facial and neck muscles, causing his head to tilt to one side and backward. This grimacing could hardly be controlled by willpower. His arms shook noticeably. His gait was trippelnd. His whole body trembled. There was also a slight hemi-hyperesthesia. The tendon reflexes were very active; he experienced vasomotor disorders (feelings of cold and sweating).
Seven months later the phenomena had all disappeared except for slight tic-like frontalis contractions.
Seven months later, all the symptoms had vanished except for some minor twitching in the forehead.
Re heredity and soil, Mairet investigated 22 cases of Shell-shock, and found a hereditary taint in eight, and an acquired predisposition in nine. He found hereditary taint definitely absent in seven, and acquired soil definitely absent in six; whereas the rest of the cases were doubtful. He found both the taint and the soil in five cases; two cases with hereditary taint alone; no case acquired, non-hereditary.
Re heredity and environment, Mairet examined 22 cases of Shell shock and discovered a hereditary factor in eight cases, and an acquired predisposition in nine. He identified hereditary factors as definitely absent in seven cases, and environmental factors definitely absent in six; while the remaining cases were uncertain. He found both hereditary factors and environmental factors in five cases; two cases with hereditary factors only; and no cases that were acquired and non-hereditary.
In eight cases with head trauma, Mairet found three with hereditary taint, four without such; against one with an acquired predisposition, four without such, others doubtful.
In eight cases of head trauma, Mairet found three with hereditary factors, four without any; compared to one with an acquired predisposition, four without, and others uncertain.
Re cases of somatic trauma (not affecting the head), among five examined, there were none with hereditary taint, three definitely without taint, and five definitely without predisposition. According to Babinski, neither hereditary taint nor prepared terrain needs be found in hysterics.
Re cases of physical trauma (not affecting the head), among the five examined, there were none with hereditary issues, three definitely without issues, and five definitely without predisposition. According to Babinski, neither hereditary issues nor a prepared terrain needs to be found in hysterics.
A predisposition is not thought important by Oppenheim, especially as so many normal persons are predisposed.
A predisposition isn't considered significant by Oppenheim, particularly since many normal people have predispositions.
War strain (fatigue, emotion): Hysterical hemiplegia. Precisely similar hemiplegia ANTEBELLUM.
War strain (fatigue, emotion): Hysterical hemiplegia. Exactly the same hemiplegia BEFORE THE WAR.
Case 291. (Roussy and Lhermitte, 1917.)
A sergeant in a regiment of cuirassiers was observed at Villejuif, January 25, 1915. He had lost power on the left side as a result of fatigue and emotion, November, 1914. He had a complete paralysis of the left arm and a paresis of the left leg. There was an anesthesia of hysterical type in the left arm, and also of the left leg as far as the middle of the thigh. He dragged his leg in walking (démarche en draguant: the toe is dragged along the ground, the trunk is bent forward, and at every step plunges somewhat toward the paralyzed side. The patient is able to walk, however, by means of a cane or crutches. This walk is characteristic of hysterical hemiplegia. According to Roussy and Lhermitte, the number of cases of hysterical hemiplegia (better, hemiparesis) is not large). The plantar reflexes on both sides were those of flexion. Upon treatment (not specified), at the end of six months he went back to service in the cavalry.
A sergeant in a cuirassier regiment was seen at Villejuif on January 25, 1915. He had lost function on his left side due to fatigue and emotional stress in November 1914. He experienced complete paralysis of his left arm and weakness in his left leg. He also had a hysterical-type numbness in his left arm and in his left leg up to the middle of his thigh. When walking, he dragged his leg (a “dragging gait”: the toe drags along the ground, his trunk leans forward, and with each step, it tends to dip toward the paralyzed side. However, he could walk using a cane or crutches. This gait is typical of hysterical hemiplegia. According to Roussy and Lhermitte, the number of cases of hysterical hemiplegia (or better, hemiparesis) is not very high. The plantar reflexes on both sides showed flexion. After treatment (not specified), he returned to cavalry service after six months.
The point of note in this case is that this patient had had a precisely similar phenomenon on the same side, which lasted a month, at the age of sixteen years and a half. It is noteworthy that in this case there was no traumatism and only the factors of fatigue and emotion to serve as an occasion for the hemiplegia. In fact, hysterical hemiplegia is said very rarely to follow physical trauma to an extremity. There are, however, some cases in which hemiparesis follows a slight head wound, particularly if over the region controlling the paralyzed limbs.
The important point in this case is that this patient experienced a very similar issue on the same side, which lasted a month, when they were sixteen and a half years old. It’s notable that in this instance, there was no injury, and only factors like fatigue and emotional stress triggered the hemiplegia. In fact, hysterical hemiplegia is said to rarely occur after physical trauma to a limb. However, there are some cases where hemiparesis follows a minor head injury, especially if it's over the area controlling the limbs that are paralyzed.
During the six-months’ course of successful treatment, no atrophy of limbs appeared, and there was never any inequality of the reflexes.
During the six months of successful treatment, there was no atrophy of the limbs, and the reflexes were always equal.
A good soldier (son of a tabetic sometimes hemiplegic), at 17 victim of hysterical hemiplegia, has AT 24 A RECURRENCE after two months’ field service. “Functional excommunication” of left arm and leg.
A good soldier (son of a tabetic sometimes hemiplegic), at 17 was a victim of hysterical hemiplegia, has AT 24 A RECURRENCE after two months of field service. “Functional excommunication” of left arm and leg.
Case 292. (Dupré and Rist, November, 1914.)
A cuirassier, 24, one month in the field, began to feel in September, 1914, crawling sensations in left arm and leg; then fingers, later hand and forearm, and finally upper arm began to work awkwardly and feel heavy, and there was a little of the same sort of thing in the leg. Hand and forearm were by the middle of October completely paralyzed, whereas the arm and shoulder were only paretic. Anesthesia at this time reached the elbow. The man had to be evacuated, after two months’ active and skilful field service, in one instance (September 19) carrying out a clever and useful interception of hostile telephone messages.
A cuirassier, 24, who had been in the field for a month, started to feel tingling sensations in his left arm and leg in September 1914. Soon, his fingers, then his hand and forearm, and finally his upper arm began to move awkwardly and felt heavy, with a bit of the same sensation in his leg. By mid-October, his hand and forearm were completely paralyzed, while his arm and shoulder were only partially affected. At this point, the numbness had reached his elbow. He had to be evacuated after two months of active and skilled service in the field, including a clever and effective interception of enemy telephone messages on September 19.
It seems that at the age of 17 also the man had had a left-sided hemiplegia, with sensory and motor symptoms, lasting two months, cured by electricity applied with a small electrode in his village. The war situation was therefore actually a recurrence of the transient hysterical paraplegia.
It appears that at the age of 17, the man experienced left-sided hemiplegia, with both sensory and motor symptoms, lasting two months, which was treated with electricity using a small electrode in his village. The war situation was essentially a relapse of the temporary hysterical paraplegia.
Moreover, the patient’s father, 52, an old tabetic, had also several times shown a hemiplegia (however on the right side), a phenomenon which had strongly affected his son.
Moreover, the patient's father, 52, an elderly man with tabes dorsalis, had also experienced hemiplegia several times (though on the right side), a condition that had a significant impact on his son.
It was curious that the slight residuals of movement which the cuirassier could perform could be made only while he was looking at the parts he was requested to move, and were impossible with eyes closed. The anesthesia was a total one when observed in November, 1914, coming to a sharp and circular termination at the shoulder and garter-wise above the knee—tuning fork insensibility in the same areas. The left patellar reflex was diminished when the eyes of the patient were leveled at the knee; but a surprise test brought the knee-jerk out normally. The hand and fingers were a little darker in color, and the whole left arm a little colder[404] than the right. There was also a slight amblyopia on the left side.
It was interesting that the slight movements the cuirassier could make were only possible when he was looking at the specific parts he was asked to move and were impossible with his eyes closed. The anesthesia was complete when observed in November 1914, ending sharply and circularly at the shoulder and just above the knee, showing a loss of sensation in those areas. The left kneecap reflex was weaker when the patient was looking at his knee, but a surprise test revealed a normal knee-jerk response. The hand and fingers appeared slightly darker in color, and the entire left arm felt a bit colder than the right. There was also a slight vision impairment on the left side.[404]
This hysterical paraplegia proved rather resistant to psychotherapy. The patient seems to have systematically eliminated from consciousness and from action the entire function of the left arm and a good deal of the left leg. Duprés and Rist speak of this as a kind of functional excommunication of the parts.
This hysterical paraplegia turned out to be quite resistant to therapy. The patient appears to have completely erased the function of the left arm and much of the left leg from both awareness and movement. Duprés and Rist describe this as a sort of functional exclusion of those body parts.
Re relapses, Wiltshire remarks that the frequency of relapses and the ways in which they are produced favor the conception that the original cause of Shell-shock must be psychic. Sir George Savage remarks that cases of Shell-shock should not return to the service under a period of six months on account of the frequency of relapse. Others have recently argued that such cases should not be sent back to the front at all. Harris notes that relapse may follow so apparently slight a factor as a vivid dream. Remarks concerning the true nature of relapses are made by Russell. Russell, for example, disapproves anesthetics in curing such a hysterical phenomenon as deafmutism. This sort of treatment does not get at the real cause of the condition, so that the man is very liable to relapse with the same symptoms. Ballet and de Fursac note the many cases of relapse after treatment and after discharge. Sometimes the relapses were due to some unfortunate happening, but in other instances no external cause could be made out. Fear of having to return to the front is a factor in certain cases, so that the true answer to the relapse question may not come until after the war.
Re relapses, Wiltshire points out that the frequency of relapses and the ways they happen suggest that the original cause of Shell shock must be psychological. Sir George Savage notes that cases of Shell shock should not return to service for at least six months because of the high rate of relapse. Others have recently argued that these cases shouldn’t be sent back to the front lines at all. Harris mentions that relapse can occur due to surprisingly minor triggers, like a vivid dream. Russell also comments on the true nature of relapses. For instance, he is against using anesthetics to treat conditions like hysterical deafness. This type of treatment doesn’t address the real cause of the issue, making it likely for the person to relapse with the same symptoms. Ballet and de Fursac highlight many instances of relapse after treatment and discharge. Sometimes the relapses were triggered by unfortunate events, but in other cases, no external cause could be identified. In certain situations, fear of having to return to the front is a contributing factor, so the real answer to the relapse issue may not become clear until after the war.
Roussy and Boisseau insist upon the value of rapid cures (psychotherapy, electricity, cold shower, etc.), in diminishing the number of relapses. They maintain that these rapid cures abolish any chance for the man to brood over symptoms and thus to exaggerate and fixate them. These workers send their hospital return back to the regiments with a statement relative to diagnosis and the request that he be immediately returned to hospital if neurotic symptoms appear.
Roussy and Boisseau emphasize the importance of quick treatments (like psychotherapy, electrical therapy, cold showers, etc.) in reducing the likelihood of relapses. They argue that these quick treatments eliminate the opportunity for individuals to dwell on their symptoms, which can lead to exaggeration and fixation. These professionals send patients back to their regiments with a report on the diagnosis and a request for immediate readmission to the hospital if neurotic symptoms arise.
War strain; burial: Deafmutism. ANTEBELLUM speech difficulty.
War strain; burial: Deafmutism. ANTEBELLUM speech difficulty.
Case 293. (MacCurdy, July, 1917.)
A private 20 (always rather tenderhearted, disliking to see animals killed; rather self-conscious; a bit seclusive; “rather more virtuous than his companions”; shy with girls; sore throat a year or more before the war, with inability to sing or talk; always a lisper) enlisted in May, 1916, spent five advantageous months in training and became increasingly sociable. However, on going to the front October, 1916, he was frightened by the first shell fire and horrorstricken by the sight of wounds and death. He grew accustomed to the horrors and five months later was sent to Armentières, where he had to fight for three days without sleep. He grew very tired and began to hope that he would receive wounds that might incapacitate him at least temporarily for service.
A private 20 (always pretty soft-hearted, hating to see animals killed; kind of self-conscious; a bit of a loner; “more virtuous than his friends”; shy around girls; had a sore throat a year or so before the war, making it hard to sing or talk; always a lisper) enlisted in May 1916, spent five productive months training, and became more social. However, when he went to the front in October 1916, he was terrified by the first shell fire and horrified by the sight of injuries and death. He got used to the horrors and five months later was sent to Armentières, where he had to fight for three days straight without sleep. He became really exhausted and started hoping that he would get injured in a way that would at least temporarily take him out of action.
He was suddenly buried by a shell, did not lose consciousness, but on being dug out was found to be deaf and dumb. On the way to the field dressing station he had a fear of shells. The deafmutism persisted unchanged for a month and then was completely and permanently cured in less than five minutes. He was made to face a mirror and observe the start he gave when hands were clapped behind him. He was assured that this start was an evidence of hearing; that his hearing was not lost, nor was his speech. He had no relapses during two months.
He was suddenly buried by a shell. He didn’t lose consciousness, but when they dug him out, he was found to be deaf and mute. On the way to the first aid station, he was terrified of the shells. The deafness and muteness lasted without
According to MacCurdy, this case is a typical one of war neurosis of the type of a simple conversion hysteria. The man never suffered from anxiety or nightmares.
According to MacCurdy, this case is a typical example of war neurosis resembling simple conversion hysteria. The man never experienced anxiety or nightmares.
Re burial cases, Grasset suggests that some of the patients probably think that they have actually died; both sensation and motion have been lost, and it is naturally these that permit a man to believe that he is still alive. The classical case is recalled, of the almost absolutely anesthetic boy who, with eyes closed, at once fell asleep. Foucault’s patient also said he actually thought he was dead after an explosion.
Re burial cases, Grasset suggests that some of the patients likely believe they have actually died; both sensation and movement have been lost, which are the things that allow a person to feel they are still alive. The classic example is the boy who was almost completely anesthetic, who, with his eyes closed, immediately fell asleep. Foucault’s patient also mentioned that he genuinely thought he was dead after an explosion.
War strain: Shell-shock and psychotic symptoms, with determination to parts injured ANTEBELLUM.
War strain: Shell shock and psychological symptoms, with a resolve to parts damaged before the war.
Case 294. (Singer, July, 1915.)
Several years before the war, a cavalry officer had a severe concussion of the brain after a fall from his horse, but got no manifest symptoms therefrom except a mild transient deafness. There must have been a vestibular nerve injury, however, since there was a marked bilateral subexcitability of this apparatus later determined.
Several years before the war, a cavalry officer suffered a serious concussion after falling off his horse, but he only experienced mild temporary deafness as a symptom. However, there must have been damage to his vestibular nerve, as later evaluations showed significant bilateral subexcitability of that system.
In September, 1914, as the result of strains and privation in the field, he got vertigo and lachrymose spells, with some obsessions as though he would have to shoot himself in the foot or spring out at the enemy from the trench.
In September 1914, due to the stress and hardships in the field, he experienced vertigo and bouts of crying, along with some compulsions as if he felt the urge to shoot himself in the foot or jump out at the enemy from the trench.
In hospital at Jena, insomnia, anxiety, excessive perspiration and salivation, feelings of the death of various parts of the body, especially the forearms and hands, associated with hypesthesia of the parts, were determined. He had a feeling of vertigo on walking and was very sensitive to noise. He now developed a very intense and very variable degree of deafness on both sides, diagnosticated as nervous deafness. The caloric test demonstrated vestibular subexcitability above mentioned. We may suppose that in this already injured organism fresh disorder had set in on a psychogenic basis in the same region that had been injured years before.
In the hospital in Jena, the patient experienced insomnia, anxiety, excessive sweating and drooling, and sensations of numbness in various parts of his body, especially his forearms and hands, accompanied by decreased sensitivity in those areas. He felt dizzy while walking and was highly sensitive to noise. He then developed severe and fluctuating deafness in both ears, diagnosed as nervous deafness. The caloric test showed the previously mentioned vestibular subexcitability. We can assume that in this already compromised body, a new disorder had emerged on a psychological basis in the same area that had been injured years earlier.
Mine explosion; emotion at death of comrades: Unconsciousness eight days with hallucinatory delirium; later, dizziness. History of previous trauma to head with unconsciousness and dizziness.
Mine explosion; feelings of loss for fallen comrades: Unconscious for eight days with hallucinations; later, experienced dizziness. History of previous head trauma with episodes of unconsciousness and dizziness.
Case 295. (Lattes and Goria, March, 1917.)
Sent at end of May to the front, an Italian soldier (Class 1895, laundryman) was placed in an advanced post where he at once sustained great hardships.
Sent at the end of May to the front lines, an Italian soldier (Class 1895, laundry worker) was stationed at an advanced post where he immediately faced significant hardships.
Father drunkard, mother healthy, sister nervous. Two brothers healthy, one brother died of tuberculosis. Patient had scrofula, scarlet fever, and bronchitis (tendency to rave intensely when in fever). At four, sustained a trauma on the head (skull depression), dizziness, loss of consciousness.
Father was an alcoholic, mother was healthy, sister was anxious. Two brothers were healthy, one brother died of tuberculosis. The patient had scrofula, scarlet fever, and bronchitis (tended to become very agitated during fever). At the age of four, experienced a head injury (skull depression), leading to dizziness and loss of consciousness.
June 7, a mine exploded in his vicinity, smashing several of his comrades. He did not himself fall to the ground, but was overwhelmed by a violent feeling of anguish. After a while, he lost consciousness. He woke up at Bologna, June 15, as after a long sleep. During the interval he had been in a state of intense hallucinatory delirium day and night. Then his mind began gradually to clear, first with amnesia of the shock which had caused the trauma. Then he recalled this fact too. Dizziness, however, grew in intensity so that he fell to ground many times during the day. There were intermittent tremors in the limbs.
June 7, a mine exploded nearby, killing several of his fellow soldiers. He didn’t fall to the ground but was overwhelmed by a wave of intense anguish. After a while, he lost consciousness. He woke up in Bologna on June 15, feeling like he had just come out of a long sleep. During that time, he had been in a state of severe, hallucinatory delirium, both day and night. Gradually, his mind began to clear, starting with a lack of memory about the shock that caused the trauma. Eventually, he remembered that too. However, the dizziness grew stronger, causing him to fall to the ground multiple times throughout the day. He also experienced intermittent tremors in his limbs.
Under observation, August 7, a sturdy, robust man. Somewhat dull in demeanor. Senses intact. Cranial nerves negative. Tendon and skin reflexes lively, especially on the right. Memory intact, except for above-mentioned oniric delirium with restlessness and shouting at night, especially while falling asleep and waking up. Frequent intense dizziness.
Under observation on August 7, a strong, solid man. A bit dull in demeanor. Senses are intact. Cranial nerves are normal. Tendon and skin reflexes are active, especially on the right side. Memory is intact, except for the previously mentioned dream-like delirium with restlessness and shouting at night, particularly while trying to fall asleep and upon waking. Experiencing frequent intense dizziness.
The condition remained unchanged for a week. Patient transferred to another department, for acute catarrhal bronchitis with fever.
The condition stayed the same for a week. The patient was moved to another department for acute catarrhal bronchitis with a fever.
Sniper stricken blind in shooting eye.
Sniper blinded in his shooting eye.
Case 296. (Eder, March, 1916.)
An Australian, 19, was admitted to hospital for loss of sight in the right eye. There had been a right ptosis from childhood. January 7 nothing could be perceived but light.
An Australian, 19, was admitted to the hospital due to loss of vision in the right eye. He had experienced right eyelid drooping since childhood. On January 7, he could only perceive light.
According to the patient, he was sniping through a loop-hole, November 15, when a bullet knocked a piece from the stock of his rifle. He continued at his post. There were five more shots, when another bullet struck the sand around the loop-hole. His right eye began to water. He shut the loop-hole and retired for an hour. His eye improved, he returned, opened the loop-hole, braced the rifle, and found he could not see the sights. He went to the physician. Vision grew rapidly worse, and in a few hours perception of light failed. He had been stricken blind in the shooting eye (the seat of a congenital deformity).
According to the patient, he was aiming through a loophole on November 15 when a bullet hit the stock of his rifle. He stayed at his post. After five more shots, another bullet hit the sand around the loophole. His right eye started watering. He closed the loophole and took a break for an hour. His eye got better, so he returned, opened the loophole, steadied the rifle, and realized he couldn’t see the sights. He went to see the doctor. His vision quickly worsened, and within a few hours, he could no longer perceive light. He had gone blind in his shooting eye (which had a congenital deformity).
Anticipation of warfare: Hysterical blindness.
Anticipation of war: Hysterical blindness.
Case 297. (Forsyth, December, 1915.)
Anticipation of warfare may provoke a neurosis as in a case of Forsyth’s. The man went blind training in England.
Anticipating war can trigger a neurosis, similar to Forsyth's case. The man went blind while training in England.
It seems that four months before, while mounting sentry at night, marauding gypsies had felled him by a blow on the head from behind. He had returned to duty after a day or two and was now expecting to be moved to France. He said that while sitting with a friend, he began to feel giddy, turned a somersault, and fell unconscious; and that on coming to, his mind was clear but everything was dark. For ten days he had been blind, although once he could see his parents, who visited him in hospital, almost clearly. His appearance under examination strongly recalled that of a blind man. He was induced to read some large print, then smaller print, and finally very small print. He then lapsed into blindness.
It seems that four months ago, while on night watch, a group of wandering gypsies attacked him from behind, hitting him on the head. He returned to duty after a couple of days and was expecting to be sent to France. He mentioned that while sitting with a friend, he started to feel dizzy, did a somersault, and passed out; when he regained consciousness, his mind was clear, but everything was dark. He had been blind for ten days, although at one point he could almost see his parents, who came to visit him in the hospital. His appearance during the exam strongly resembled that of a blind person. He was encouraged to read some large print, then smaller print, and finally very small print. After that, he went completely blind again.
He remembered that before enlisting, he had trained in a smithy, and heard that blacksmiths often went blind at the forge.
He remembered that before joining the military, he had trained in a blacksmith shop and heard that blacksmiths often went blind from working at the forge.
Bareback riding: Spasmodic neurosis (similar ANTEBELLUM episode).
Bareback riding: Spasmodic neurosis (similar to an antebellum episode).
Case 298. (Schuster, December, 1914.)
A soldier, 32, had to do a long stretch of riding bareback. As a result, he later suffered from tonic muscular spasms whenever he had to exert himself seriously, especially whenever he had to move his legs and when sudden movements or sudden strong contacts were made. The attack appeared to be reflexly dependent on the pain. The case is regarded as one of the Wernicke Crampusneurosen, a disease somewhat related with hysteria.
A 32-year-old soldier had to endure a long time riding without a saddle. As a result, he later experienced painful muscle spasms whenever he had to exert himself significantly, especially when moving his legs or during sudden movements or impacts. The spasms seemed to be reflexively linked to the pain. This case is considered one of the Wernicke Crampusneurosen, a condition somewhat related to hysteria.
A condition somewhat like the one developed in the war had occurred in this man at the age of seventeen after a drenching, but the attack was at that time much milder. He had, however, frequently had cramps in his legs.
A condition similar to what he experienced during the war had happened to this man at the age of seventeen after he got soaked, but the episode back then was much less severe. However, he often suffered from cramps in his legs.
ANTEBELLUM spasm of hands, functional.
ANTEBELLUM hand spasm, functional.
Case 299. (Hewat, March, 1917.)
A boy, 19, had been passed as fit for laboring work at home. He had been a farm boy from 14. Once at 17 he had developed whilst working amongst turnips in wet weather, pain in the hands, which got worse and was followed by pains in legs, arm, and neck, that kept him in bed a week, and from work ten days. Even on returning to work, his hands were swollen, though he was able to drive a horse. The fingers had been somewhat firmly flexed on the palms ever since this illness at 17.
A 19-year-old boy had been cleared for labor work at home. He had been a farm boy since he was 14. When he was 17, while working with turnips in wet weather, he started experiencing pain in his hands, which worsened and was followed by aches in his legs, arms, and neck, keeping him in bed for a week and away from work for ten days. Even after returning to work, his hands were swollen, though he could drive a horse. His fingers had been somewhat curled against his palms since the illness at 17.
He was sent to Netley after three weeks of army work, as having a spasm of both hands. He was found to be mentally below par, nervous, apprehensive, stuttering in speech and not readily responsive, with defective vasomotor control, though of good average bodily development except for asymmetry of chest.
He was sent to Netley after three weeks of military service due to experiencing spasms in both hands. It was determined that he had below-average mental functioning, was nervous, anxious, stuttered in his speech, and wasn't very responsive. He also had poor vasomotor control, but his overall physical development was good except for chest asymmetry.
Both hands were found firmly closed; tips of fingers applied to palms; thumbs freely movable; forearms well developed, especially the flexors. Counterforce was exerted upon passive extension of fingers. There was no sensory or reflex disorder, and while the patient was asleep, it was found that the first and second fingers of both hands could be fully extended. Yet there was a definite contracture of the palmar fascia which prevented full extension of the third and fourth fingers. He was awakened by this test and the fingers became firmly flexed at once.
Both hands were tightly closed; the tips of the fingers pressed against the palms; the thumbs were able to move freely; and the forearms were well-developed, particularly the flexor muscles. A counterforce was applied to the passive extension of the fingers. There were no sensory or reflex issues, and while the patient was asleep, it was observed that the first and second fingers of both hands could fully extend. However, there was a noticeable contracture of the palmar fascia that prevented full extension of the third and fourth fingers. When this test was performed, he woke up, and his fingers immediately flexed tightly.
The man was treated by milk isolation behind screens, without permission to read, smoke, or talk. Twice a day he was encouraged to move the fingers and made to perform finger exercises. He became able to extend the fingers over half their normal excursion in three days, and was then able to abduct and adduct the fingers. He was allowed up in two weeks’ time, with full diet and screens removed. The contracture of the palmar fascia was still in evidence, but the power of movement in the hands and fingers was so satisfactory that he could be sent back to duty in three weeks. The interpretation of Fergus Hewat is that the painful condition of the hands which set in in the illness at the age of 17, had caused an obsession which had developed into a functional spasm of the hands.
The man was treated by isolating him with milk behind screens, without any permission to read, smoke, or talk. Twice a day, he was encouraged to move his fingers and perform finger exercises. In three days, he was able to extend his fingers for more than half their normal range and could then move them apart and together. He was allowed to get up after two weeks, with a full diet and the screens removed. The tightening of the palmar fascia was still noticeable, but the movement in his hands and fingers was satisfactory enough for him to return to duty in three weeks. Fergus Hewat interpreted that the painful condition of his hands, which began during his illness at age 17, had created an obsession that developed into a functional spasm of the hands.
Quarrel: Hysterical HEMICHOREA, DOUBLY REMINISCENT, of a former hysterical chorea, itself related with an organic chorea of the patient’s mother.
Quarrel: Hysterical HEMICHOREA, DOUBLY REMINISCENT, of a former hysterical chorea, itself connected with an organic chorea of the patient’s mother.
Case 300. (Dupuoy, October, 1915.)
A nineteen year old soldier, for some months a bit distressed and irritable, had a dispute with an old man whose jug he unluckily happened to smash. The old man said something was going to happen to him for that. That day, in point of fact, he fell and sustained an injury with water on the right knee. He was upbraided by the captain and evacuated to the ambulance. The fellow thought the old man with the broken jug had interfered, dreamed of the old man’s threats, and felt his hand on his shoulder.
A nineteen-year-old soldier, who had been feeling a bit distressed and irritable for several months, got into an argument with an old man after he accidentally broke the man's jug. The old man warned that something would happen to him because of it. That day, in fact, he fell and hurt his right knee. The captain chewed him out and sent him to the ambulance. The soldier believed the old man with the broken jug had cursed him, dreamed about the old man's threats, and felt a hand on his shoulder.
Next day hemichorea developed on the right side, a partial and rhythmic chorea with jerky, regular contractions, fifty to sixty per minute, affecting synchronously the muscles of the leg, arm, face and tongue.
The next day, hemichorea appeared on the right side, characterized by a partial and rhythmic chorea with quick, regular contractions, fifty to sixty per minute, affecting the muscles of the leg, arm, face, and tongue simultaneously.
Dupuoy speaks of the reason for the hysterical “choice” of this disease, since his mother had had a probably organic hemichorea, also on the right side, with which she died at thirty years in a stroke. The boy was at that time thirteen years old and had had a rhythmic chorea six weeks, limited to the extensors of the hand on the forearm, treated in hospital.
Dupuoy talks about why there was a seemingly irrational “choice” of this disease, noting that his mother likely had an organic hemichorea on the right side, which led to her death from a stroke at the age of thirty. The boy was thirteen years old at that time and had experienced rhythmic chorea for six weeks, affecting only the extensors of his hand on the forearm, and had been treated in the hospital.
This new hemichorea was quickly and completely cured by psychotherapy.
This new hemichorea was quickly and fully cured through psychotherapy.
Hallucinations and delusions in a soldier, of antebellum origin. Treatment by explanation of causes.
Hallucinations and delusions in a soldier from before the war. Treatment through understanding the causes.
Case 301. (Rows, March, 1916.)
A private, 31,—a case of Capt. W. Brown,—was admitted to hospital suffering from hallucinations of hearing and delusions of supervision by his family and friends; he heard his relatives telling him what to do and what not to do. He thought they belonged to a secret police entrusted with the task of supervising his actions and seeing that he did not again transgress as he had done. An inquiry into his past revealed the following facts:
A private, 31—a case of Capt. W. Brown—was admitted to the hospital experiencing auditory hallucinations and delusions that his family and friends were watching him. He heard his relatives instructing him on what to do and what not to do. He believed they were part of a secret police assigned to monitor his behavior and ensure he didn't repeat his previous mistakes. An investigation into his background uncovered the following facts:
He had been a bank clerk before the war and once because of a nervous breakdown as a result of drinking and smoking had been given a three months’ vacation. On this occasion he went with a prostitute—his first and only offence in sex matters. He later thought the behavior of his family indicated that they knew of his misdeed. He heard the voices of members of his family, became rapidly worse and more depressed, and attempted suicide.
He had worked as a bank clerk before the war and once, due to a nervous breakdown from drinking and smoking, he was granted a three-month vacation. During that time, he went with a prostitute—his first and only sexual encounter. He later felt that his family's reactions suggested they were aware of his mistake. He started hearing voices from his family members, grew increasingly worse and more depressed, and attempted suicide.
He went to a private asylum. Later, he emigrated to Canada, but he was still pursued by the voices and he returned to England. He enlisted at the outbreak of the war and went to France. He was soon invalided and sent to Maghull.
He went to a private mental health facility. Later, he moved to Canada, but he was still haunted by the voices, so he returned to England. He joined the military when the war started and went to France. He was quickly injured and sent to Maghull.
The cause of his condition, according to Rows, was his affair with the prostitute and his previous drinking. This was explained to him as the basis of his strong feeling of self-reproach. The hallucinations and idea of suicide had developed therefrom. Recovery[413] “to a large extent.”
The reason for his condition, according to Rows, was his relationship with the prostitute and his past drinking. This was explained to him as the reason for his deep sense of guilt. The hallucinations and thoughts of suicide had come from that. Recovery[413] “to a large extent.”
A poor risk (hereditary and acquired); emotionality: Tremors and convulsive crises with lowering of pulse.
A poor risk (genetic and acquired); emotional instability: Tremors and convulsions with a drop in pulse.
Case 302. (Fursac Rogues, July, 1915.)
A man, 36 (boat painter to 30 and thereafter a wine seller; paternal grandmother insane, father alcoholic and suicide; gonorrhea, 20; two attacks of lead colic, 25 to 30; purulent pleurisy, 31; phlegmon of mouth, 34; also a chronic alcoholic), at the time of examination showed arteriosclerosis and slightly hypertrophic liver; unequal pupils, slightly contracted and sluggish to light. He complained of frequent headaches, possibly due to a combination of plumbism and alcoholism. He was not in any respect demented, and had an excellent memory. He had always been emotional, being unable to go to a funeral without many tears, or remain in a house where there was a corpse without threatening to faint. He was always overcome if he saw a fight going on; and even in his wine shop he would escape when there was a fight and get a neighbor to bring the police.
A 36-year-old man (a boat painter until he was 30, then a wine seller; his paternal grandmother was insane, his father was an alcoholic and committed suicide; had gonorrhea at 20; experienced two episodes of lead poisoning between ages 25 and 30; suffered from purulent pleurisy at 31; had a phlegmon of the mouth at 34; also a chronic alcoholic) was examined and showed signs of arteriosclerosis and a slightly enlarged liver; his pupils were unequal, slightly constricted, and slow to react to light. He reported frequent headaches, likely caused by a mix of lead poisoning and alcoholism. He was not at all demented and had a great memory. He had always been emotional, unable to attend a funeral without crying or stay in a house with a corpse without threatening to faint. He would be overwhelmed if he witnessed a fight; even in his wine shop, he would run away during fights and ask a neighbor to call the police.
He was mobilized on the fifth day, sent first to a territorial regiment and then, in October, put into the reserve of an active regiment and sent to the front. He reached the first line trenches in the night, greatly affected by ruins he saw on the road. He slept poorly and had nightmares. At daybreak he woke up to see a pile of corpses near by, and felt an indescribable terror on account of the corpses and the noise of bullets, machine guns, and shells. By superhuman efforts—according to the man—he mastered his emotions and took his turn at the observation post. Another sleepless night. Next day he got such tremors that his sergeant sent him to the hospital where he was at first thought to be suffering from a fever. But his temperature was found normal, and he was sent back to the trenches.
He was called up on the fifth day, initially assigned to a local regiment, and then in October, moved to the reserve of an active regiment and sent to the front. He arrived at the front line trenches at night, deeply disturbed by the destruction he witnessed on the way. He had trouble sleeping and experienced nightmares. At dawn, he woke up to find a pile of corpses nearby and felt an indescribable terror from the bodies and the sounds of bullets, machine guns, and shells. With extraordinary effort—according to him—he controlled his emotions and took his turn at the observation post. Another night without sleep. The next day he was shaking so much that his sergeant sent him to the hospital, where he was initially thought to have a fever. However, his temperature was found to be normal, and he was sent back to the trenches.
He passed another night without sleep, and next day he could not hold his gun for trembling. The Captain sent him back to be a kitchen man in the rear, and here he remained[414] six weeks—restless, trembling, eating very little. He would have anxious spells. In the morning, as he was carrying coffee to the men in his company, on seeing a pile of corpses, he dropped his pot and ran back to the kitchen declaring that whoever wanted to carry coffee might, but he would not go back. He spilled a pot of soup on his left foot. The Captain had him evacuated, saying: “Go! when you come back, I hope the war will be over!”
He went another night without sleep, and the next day he could barely hold his gun because he was shaking. The Captain sent him back to work in the kitchen in the rear, and he stayed there for six weeks—restless, trembling, and hardly eating. He often felt anxious. One morning, while he was carrying coffee to the men in his company, he saw a pile of bodies and dropped his pot, running back to the kitchen. He declared that whoever wanted to carry coffee could do it, but he wasn’t going back. He also spilled a pot of soup on his left foot. The Captain had him evacuated, saying, “Go! When you come back, I hope the war will be over!”
He was sent back to a hospital near Paris, where he was all right for a few days, happy as a prince. The burn got well, and as the time approached when he would probably have to go back to the front, the terror returned. He had visions of corpses, and imagined bullets whistling, machine guns popping, and shells bursting. He wept, lost appetite, hid in corners, made three suicidal attempts by poisoning,—though the sincerity of these attempts was doubtful (zinc oxide ointment; rose laurel leaves; verdigris). Sent back to a dépôt before getting leave, he had crises of tremor with anxiety, and was then sent to Val-de-Grâce on the mental service, and finally to Ville-Évrard. He unhesitatingly confessed his terror, becoming more and more anxious and tremulous, and almost losing his pulse while describing his experiences. He said he would commit suicide rather than return to the front. He stayed at the Hospital, working in the garden rather calmly, but when it was a question of leaving, even on convalescence, his terror and anxiety returned. Every time he was examined there was an emotional explosion, with expressions of anguish, generalized tremors and crises of clonic convulsions with respiratory disturbance even of threatening suffocation, depression of pulse. It is this latter which is the most important element in the proof that such a case is not a case of simulation.
He was sent back to a hospital near Paris, where he felt fine for a few days, happy as can be. The burn healed, but as the time came closer for him to likely return to the front, the fear came back. He had nightmares about corpses and imagined bullets whistling, machine guns firing, and shells exploding. He cried, lost his appetite, hid in corners, and made three suicide attempts by poisoning—though the seriousness of these attempts was questionable (zinc oxide ointment; rose laurel leaves; verdigris). After being sent back to a depot before getting leave, he experienced anxiety tremors and was then sent to Val-de-Grâce for mental health care, and finally to Ville-Évrard. He openly admitted his terror, becoming increasingly anxious and shaky, almost losing his pulse while recounting his experiences. He claimed he would rather commit suicide than go back to the front. He remained in the hospital, working calmly in the garden, but when it came to leaving, even for convalescence, his fear and anxiety returned. Every time he was examined, there was an emotional outburst, displaying anguish, widespread tremors, and episodes of convulsions with breathing disturbances that felt like suffocation, along with a decreased pulse. This last symptom is the most significant evidence that his case is not one of faking.
Re war cases, Bennati remarks upon the great number that do not fall into known categories. There is, he thinks, an anaphylactic group in which the trauma acts as the secondary toxic agent; and there is another group in which exhaustion works after the manner suggested by Edinger: that is, by a physiological overwork of certain structures.
Re war cases, Bennati notes the large number that don't fit into known categories. He believes there is an anaphylactic group where the trauma serves as the secondary toxic agent; and there is another group where exhaustion operates in the way Edinger suggested: that is, through a physiological overwork of certain structures.
Martial misfit, dwelling on horrors of war at home; exposure; shell fire: Mental exhaustion with depression, emotionality, tachycardia.
Martial misfit, living with the horrors of war at home; exposure; shellfire: mental exhaustion with depression, intense emotions, rapid heartbeat.
Case 303. (Bennati, October, 1916.)
An Italian corporal, in civil life a writer (mother very nervous; patient himself rickety, unmarried; relatives well off), was in front line trenches for some fifty days. He was repeatedly excused from service on account of fatigue, distress, poor appetite, insomnia, depression and even confusion (aimless shots fired off in the night). It turned out that he had been in just this state of mind when he left home and family and that the very thought of war had seemed dreadful to him. He did not at all enjoy leaves at night, as he stumbled and fell about in the darkness and had shells burst near by. He lived immersed in mud. He reacted unfavorably to antityphoid injection.
An Italian corporal, who was a writer in civilian life (his mother was very anxious; he was himself frail, single; his relatives were well-off), spent about fifty days in the front-line trenches. He was frequently excused from duty due to exhaustion, anxiety, poor appetite, insomnia, depression, and even confusion (firing aimless shots into the night). It turned out that he had been in this troubled state of mind when he left home and family, and just the thought of war had seemed terrifying to him. He didn’t enjoy nighttime leaves at all, as he stumbled and fell in the dark and had shells exploding nearby. He lived surrounded by mud. He had an adverse reaction to the antityphoid vaccination.
The very day he went on winter furlough he greatly improved, but then suddenly relapsed into depression, emotionality, inattentiveness, sluggishness of mind, and exhaustion. The tendon reflexes were lively, the abdominal reflexes sluggish. There was tachycardia (120), the Mannkopf-Thomayer tests were positive at 76 and 80, oculocardiac reflexes 84 and vagotonic. Stellwag and v. Graefe symptoms.
The very day he went on winter break, he showed a lot of improvement, but then he suddenly fell back into feelings of depression, mood swings, lack of focus, mental sluggishness, and fatigue. His tendon reflexes were brisk, but his abdominal reflexes were slow. He had a fast heartbeat (120), the Mannkopf-Thomayer tests were positive at 76 and 80, oculocardiac reflexes were at 84 and vagotonic. He showed Stellwag and v. Graefe symptoms.
Hereditary instability.
Genetic instability.
Case 304. (Wolfsohn, 1918.)
An English soldier, 23, had been ten months on active service in France, when he was buried by a shell December 19, 1915. He became unconscious and later suffered from nervousness and stuttering, depression, insomnia, frightful dreams, and tremor. Improvement was such, under treatment, that he was again returned to the front. A shell burst near him once more and again he grew dazed, trembled, had lapses of memory and fell into a state of general nervousness. He improved again in hospital.
An English soldier, 23, had been on active duty in France for ten months when he was buried by a shell on December 19, 1915. He lost consciousness and later experienced nervousness, stuttering, depression, insomnia, terrifying dreams, and tremors. He showed enough improvement with treatment that he was sent back to the front. A shell exploded near him again, and he became dazed, trembled, had memory lapses, and fell into a state of general anxiety. He improved once more in the hospital.
On returning to the front in a few days he saw a bomb burst some distance away. He began to stammer and to wander about aimlessly. Insomnia, tremor of legs, arms and head, fatiguability, feeling of lassitude, occipital and vertical headache, fear of aircraft and crowds, frightful dreams, absences and aimless wanderings appeared. There was one attack of deafmutism. Whenever the patient saw aircraft he ran. He was easily startled by noises.
On returning to the front in a few days, he saw a bomb explode some distance away. He started to stammer and wander around aimlessly. He experienced insomnia, tremors in his legs, arms, and head, extreme fatigue, a sense of weakness, headaches at the back and top of his head, fear of planes and crowds, terrifying nightmares, moments of absence, and aimless wandering. There was one episode of being temporarily unable to speak. Whenever he saw an aircraft, he would run. He was easily startled by sounds.
He was the son of an excitable, alcoholic father and of a nervous and bad tempered mother. A sister had had nervous prostration. The man himself had always been more or less moody and a nail-biter. According to Wolfsohn, 74 per cent of the war neuroses have a family history of neurotic or psychotic stigmata, including insanity, epilepsy, alcoholism and nervousness; 72 per cent show previous neuropathy.
He was the son of an overly emotional, alcoholic father and a nervous, ill-tempered mother. A sister had suffered from nervous exhaustion. The man himself had always been somewhat moody and a nail-biter. According to Wolfsohn, 74% of war neuroses have a family history of neurotic or psychotic traits, including insanity, epilepsy, alcoholism, and anxiety; 72% show previous nerve issues.
According to Wolfsohn, wounded soldiers do not show war neuroses except in rare instances. In the wounded soldiers studied by him no neuropathic or psychopathic stigmata occurred in the family history and previous neuropathic tendencies in the patients themselves were found in about 10%.
According to Wolfsohn, injured soldiers rarely exhibit war-related psychological issues. In the injured soldiers he studied, there were no signs of neuropathic or psychopathic traits in their family histories, and about 10% of the patients showed previous neuropathic tendencies.
A soldier that is excessively fatigued or has been under undue mental anxiety, expecting to be blown to pieces, may go into psychoneurosis more easily than one without such emotional strain.
A soldier who is extremely tired or has been under intense mental stress, fearing for their life, may fall into psychoneurosis more easily than someone without that kind of emotional pressure.
Genealogical tree of a shoemaker.
Family tree of a shoemaker.
Case 305. (Wolfsohn, 1918.)
An English private, shoemaker, 37, was partially buried in a shell explosion and came to, stupid, shaky, weak and fearful of the dark. Twice, in a dazed state, he attempted to murder companions and was afterwards amnestic. He had always been of a violent temper and his outbursts had been followed by petit mal. He had also always been afraid of the dark. One of his children had fits; three were hysterical and had temper fits. The man’s father was in an insane hospital. Sundry other facts are shown in the genealogical tree presented herewith.
An English private, a shoemaker, 37 years old, was partially buried in a shell explosion and woke up feeling dazed, shaky, weak, and scared of the dark. Twice, in a confused state, he tried to attack his companions and later couldn’t remember it. He had always had a violent temper, and his outbursts were often followed by seizures. He had also always been afraid of the dark. One of his children suffered from seizures, and three were prone to hysteria and temper tantrums. The man's father was in a mental hospital. Several other details are detailed in the genealogical tree attached here.

Fall from horse in battle; fear of being crushed: Hysterical crises. Case offered as showing TRAUMATIC HYSTERIA in a young physician WITHOUT HEREDITARY OR ACQUIRED PSYCHOPATHIC TENDENCY.
Fall from a horse in battle; fear of being crushed: Hysterical crises. This case illustrates TRAUMATIC HYSTERIA in a young physician WITHOUT HEREDITARY OR ACQUIRED PSYCHOPATHIC TENDENCY.
Case 306. (Donath, 1915.)
A physician of twenty went into the war as a volunteer Hussar. During an attack, he fell from his horse without losing consciousness, though he was at the time much afraid of being crushed. The attack ceased and he returned to the lines on horseback.
A twenty-year-old doctor joined the war as a volunteer Hussar. During an attack, he fell from his horse but didn’t lose consciousness, even though he was really scared of getting crushed. The attack ended, and he made his way back to the lines on horseback.
Immediately there developed an emotional crisis, and thereafter he broke into weeping on the slightest occasion. He was afraid he was going to lose his reason; that some spiritual power was going to suppress his ego and madden him. He wept as he was going under narcosis to be operated[419] upon for an intercurrent appendicitis. He became so sensitive to noise that he wanted to choke the offender. One day he bit himself on the arm in his excitement. Sensory tests could not be executed on account of his fear of the brush. Reflexes were normal.
Immediately, an emotional crisis developed, and from then on, he broke down in tears at the slightest thing. He was afraid he was going to lose his mind; that some spiritual force would take over his thoughts and drive him crazy. He cried as he was going under anesthesia to have surgery for an unexpected appendicitis. He became so sensitive to noise that he wanted to silence the source. One day, he bit his own arm in his agitation. Sensory tests couldn’t be done because he was too scared of the brush. Reflexes were normal.
It took four hypnotic seances to get him in proper rapport with his physician for psychotherapy.
It took four hypnotic sessions to establish a good connection between him and his therapist for psychotherapy.
This case is cited by Donath as one in which traumatic hysteria has been proven to exist in a man without any sign of neuropathic or psychopathic taint, either in his previous history or in his relatives.
This case is mentioned by Donath as one where traumatic hysteria has been shown to exist in a man with no signs of neurological or psychological issues in his past or in his family.
A perfect soldier type. Mine explosion; burial; superficial wounds: War neurosis.
A perfect soldier type. Mine explosion; burial; superficial wounds: combat stress.
Case 307. (MacCurdy, July, 1917.)
A lieutenant, 29, had been a regular soldier for eight years before the war and was made a non-commissioned officer almost at once after enlisting. He went out as a sergeant with the original expeditionary force and got through the retreat from Mons and the first battle of Ypres intact. He enjoyed the fighting hugely and even got indifferent to the burial work. The death of chums saddened him, but he carried on and soon forgot about the incidents. He might be regarded as a perfect soldier.
A 29-year-old lieutenant had been a career soldier for eight years before the war and quickly became a non-commissioned officer after enlisting. He served as a sergeant with the original expeditionary force and made it through the retreat from Mons and the first battle of Ypres unscathed. He loved the fighting and eventually became indifferent to the burial work. The deaths of his friends made him sad, but he pushed through and soon moved on from those experiences. He could be seen as the ideal soldier.
In August, 1915, there was a slight touch of rheumatism. Two or three months later the Germans exploded a mine immediately in front of the trench where he was. He went pale for the first time in his life, but kept his men “standing to.” Thereafter he began to think for the first time about danger. Mining was hereabouts the chief form of attack, and he frequently heard Germans digging beneath a dug-out. He slept well in billets, but was too restless for sleep on active duty.
In August 1915, he experienced a bit of rheumatism. A couple of months later, the Germans set off a mine right in front of the trench he was in. He turned pale for the first time in his life but kept his men ready. After that, he started to actually consider the idea of danger. Mining was the main type of attack in this area, and he often heard Germans digging under a dugout. He slept well while in billets, but he couldn’t settle down for sleep during active duty.
He got more and more on edge during the next weeks. Six weeks after the mine explosion he was buried in a dug-out. Though he did not lose consciousness, he was dazed and had to lie down for two hours. Nervousness, chronic headache and insomnia, even in billets, followed. His imagination played upon the blowing out of dug-outs and the bowling over of men by shells. He had become company sergeant-major and the responsibility made him grow worse and worse. At times he tended to jump when the shells came, but was outwardly perfectly calm. He began to take morphia, though with little result. He had suicidal thoughts.
He became increasingly anxious over the next few weeks. Six weeks after the mine explosion, he found himself trapped in a dugout. Although he didn't lose consciousness, he felt disoriented and had to lie down for two hours. He suffered from nervousness, chronic headaches, and insomnia, even when in billets. His mind was consumed by thoughts of dugouts collapsing and men being hit by shells. He had been promoted to company sergeant-major, and the added responsibility only made his condition worse. At times, he instinctively flinched when the shells landed, but he appeared calm on the outside. He started using morphine, but it didn't help much. He experienced suicidal thoughts.
After two months of these symptoms he was sent to England. He began to sleep fairly well and three months later applied for light duty; was greatly bored by the company accountant work given him; got a commission and was sent[420] back to the front nine months later, January, 1917. He got on with the active fighting very well, sleeping four or five hours a night. In April he was sent to Arras. He had had a dream that he was going to be bowled over, buried and wounded in the neck. Sleep got poorer. In April he led his men in an advance and actually was bowled over, buried and hit in the neck as well as in the knee and the hand, though all the wounds were superficial. He was carried back, dazed, to hospital, where he grew fairly comfortable in ten days and even undertook a journey down to the base.
After two months of these symptoms, he was sent to England. He started sleeping pretty well and, three months later, applied for light duty; he was really bored with the accounting work he was given. He received a commission and was sent[420] back to the front nine months later, in January 1917. He adapted well to the active fighting, sleeping four or five hours a night. In April, he was sent to Arras. He had a dream that he was going to be knocked down, buried, and wounded in the neck. His sleep worsened. In April, he led his men in an advance and actually got knocked down, buried, and hit in the neck, as well as his knee and hand, though all the wounds were superficial. He was carried back, dazed, to the hospital, where he became relatively comfortable in ten days and even took a trip down to the base.
He arrived in collapse, remained in camp at the base three weeks, getting steadily worse. Something, he could not tell what, was going to happen and kill him. He could not concentrate, even to read. He thought of suicide. He slept practically not at all, waking from a doze with a start, feeling that something had hit him. He had dreams of being taken prisoner and on waking would in fancy start a fight to escape from imagined imprisonment back to the British lines. After two weeks in various hospitals he spent ten days in a hospital for nervous cases and grew better. Riding on trains he was terrorized in every tunnel lest he should be crushed.
He collapsed when he arrived, stayed in camp at the base for three weeks, and just kept getting worse. He felt like something he couldn't identify was about to happen and kill him. He couldn’t focus, not even enough to read. He thought about suicide. He barely slept, waking up from a light doze with a jolt, feeling like something had struck him. He dreamed of being captured and would wake up imagining starting a fight to break free and return to the British lines. After two weeks in various hospitals, he spent ten days in a facility for nervous patients and started to get better. While riding on trains, he was scared in every tunnel, worried he would be crushed.
According to MacCurdy, an anxiety neurosis would have developed had not his superiors sent the lieutenant back to hospital after the final burial in April. As this perfect soldier said:[421] “There is no man on earth who can stick this thing forever.”
According to MacCurdy, an anxiety disorder would have developed if his superiors hadn't sent the lieutenant back to the hospital after the final burial in April. As this perfect soldier said:[421] “There is no man on earth who can handle this forever.”
Shell-shock; thrown against a wall: Tremors—TREMOPHOBIA.
Shell shock; slammed against a wall: Tremors—TREMOPHOBIA.
Case 308. (Meh, February, 1916.)
Meige has studied shell-shock tremors, especially those occurring without external wound.
Meige has researched shell-shock tremors, particularly those that happen without any visible injury.
A corporal was with his squad on the Nouvron Plateau, January 13, 1915, when he was thrown against the wall by a bursting shell, which killed or wounded several comrades but did not wound the corporal. Whether he lost consciousness is unknown, but he lay on the ground for some time, until he could be moved through a communication trench. After the explosion he began to tremble, and was still trembling on his trip back. Constantly trembling, he lived on at the front for a fortnight, but without eating; and, although he had been a good rifleman, he had lost all his former skill with a gun.
A corporal was with his squad on the Nouvron Plateau on January 13, 1915, when a shell exploded, throwing him against the wall and killing or injuring several of his comrades, but he wasn’t hurt. It’s unclear if he lost consciousness, but he lay on the ground for a while until he could be moved through a communication trench. After the explosion, he started to shake, and he kept shaking during his trip back. He continued to tremble at the front for two weeks, though he didn’t eat anything; and despite being a good marksman before, he had lost all his previous skill with a gun.
There was a delay of a month before evacuation, but the trembling did not cease, and he was passed through various units, to the neurological center at Villers-Cotterets, where he remained for two months,—April 13 to June 15, 1915,—with a diagnosis of hysterical chorea. He was examined by Guillain, who found, besides the generalized tremors, lively knee-jerks and Achilles jerks, an excessive emotionality, particularly marked when the guns were going or bombs bursting. Lumbar puncture yielded a perfectly normal fluid.
There was a month-long delay before evacuation, but the shaking didn't stop, and he was moved through different units to the neurological center at Villers-Cotterets, where he stayed for two months—from April 13 to June 15, 1915—with a diagnosis of hysterical chorea. He was examined by Guillain, who noted that, in addition to the generalized tremors, there were strong knee-jerks and Achilles reflexes, along with an extreme emotional response, especially noticeable when the guns were firing or bombs were exploding. A lumbar puncture showed completely normal fluid.
June 19 the corporal went to the Salpêtrière under P. Marie. July 14 he was evacuated to the civil hospital of Arcueil, where he remained till September 24, when he was sent home to convalesce, from October 26 to December 15.
June 19, the corporal went to the Salpêtrière under P. Marie. July 14, he was moved to the civilian hospital in Arcueil, where he stayed until September 24, when he was sent home to recover, from October 26 to December 15.
He returned to the Salpêtrière December 15, 1915. Throughout these various movements from hospital to hospital, his status was unchanged. At the time of report about a year after shell-shock, he was still constantly and uniformly trembling. All four limbs were affected, perhaps the right arm and the left leg more markedly. There was no tremor[422] during sleep, but there was a tremor when the patient lay awake in dorsal decubitus just as when he was sitting or standing. The tremor was worse in the evening than in the morning, and the patient could get to sleep only very late. There was slight tremor of the head; the eyelids and the tongue showed a few tremors, which were not synchronous with those of the limbs. Nystagmus was absent. To diminish the effect of the trembling, the patient held his forearms flexed and kept his elbows close to his body. If the trembling of the legs got intense, the patient would rise and walk a few steps. Any movement, such as carrying a spoon or a glass to the mouth, led to an exaggeration of the tremors; and there was at this time a suggestion of the intention tremor of multiple sclerosis. The tremor was increased when the eyes were closed. Any sudden noise or sharp command, or recalling to mind of trench service, would bring about extraordinary motor crises, in which there was an intense and generalized tremor, so the patient would lose his balance. Any attempt at eliciting reflexes would produce generalized violent tremor. Sensations were normal; tendency to hyperidrosis; pulse in repose, 60, rising to 120 if one struck the table sharply.
He returned to the Salpêtrière on December 15, 1915. Throughout his various moves from hospital to hospital, his condition remained the same. About a year after experiencing shell shock, he was still consistently trembling. All four limbs were affected, with the right arm and left leg showing more noticeable tremors. There was no tremor while he slept, but when awake and lying on his back, just like when sitting or standing, he experienced trembling. The tremors were worse in the evening than in the morning, and he could only fall asleep very late at night. There was a slight tremor in his head; his eyelids and tongue had some tremors too, which did not sync with those in his limbs. Nystagmus was not present. To lessen the impact of the trembling, he kept his forearms bent and his elbows close to his body. If his leg tremors intensified, he would stand up and walk a few steps. Any movement, like lifting a spoon or glass to his mouth, exaggerated the tremors; at this time, there were hints of intention tremor seen in multiple sclerosis. The tremor increased when his eyes were closed. Any sudden noise, sharp command, or a memory of trench service would trigger intense motor crises, resulting in a severe and widespread tremor that caused him to lose his balance. Attempts to elicit reflexes would lead to a strong, generalized tremor. His sensations were normal, but he showed a tendency for excessive sweating; his pulse was 60 at rest but could rise to 120 if someone struck the table sharply.
Meige remarks that a number of examples of tremors suggestive of Parkinson’s disease were observed in the War of 1870. Might the explosion have caused properly situated lesions in the encephalon of such a nature as to produce a Parkinsonian tremor? The tremors were stationary, and if due to some lesion, the lesion remains now exactly what it was at the beginning. There was no digital tremor such as is characteristic of Parkinson’s disease. Moreover, the intention tremor of such a patient, rather than Parkinson’s disease, suggests multiple sclerosis, of which latter disease, however, there is no other sign. Nor does there seem any evidence that these tremors were of cerebellar, paretic, goitrous, or of any definite toxic origin. On the whole, Meige regards it as a neuropathic manifestation resembling what is found in traumatic neurosis. He believes that there is not sufficient evidence that it is the consequence of any structural change in the nervous system.
Meige notes that several cases of tremors resembling Parkinson’s disease were observed during the War of 1870. Could the explosion have caused lesions in the brain that result in a Parkinsonian tremor? The tremors were consistent, and if they were caused by a lesion, that lesion is exactly the same now as it was at the start. There were no digital tremors typical of Parkinson’s disease. Additionally, the intention tremor seen in these patients, rather than indicating Parkinson’s, suggests multiple sclerosis, although there are no other signs of that disease. There also appears to be no evidence that these tremors originated from cerebellar issues, paralysis, thyroid problems, or any specific toxic cause. Overall, Meige considers it a neuropathic symptom similar to what is observed in traumatic neurosis. He believes there isn’t enough evidence to support that it results from any structural changes in the nervous system.
Meige remarks that the analysis of any case of tremor must take the mental state into account. This patient, perfectly conscious of his tremors and their critical exacerbations, was much chagrined thereby. He suffered mentally from his impotence, especially when bystanders would intentionally bring about his paroxysms. He looked like one shuddering from fear, and it is actually probable that he was afraid of his own tremors and shuddering. He was, besides subject to tremor, also a victim of tremophobia,—a kind of phobia described some years since by Meige, somewhat resembling ereutophobia, or fear of blushing, described by Pitres and Régis.
Meige points out that when analyzing any case of tremors, it’s important to consider the patient’s mental state. This patient was fully aware of his tremors and their severe episodes, which made him feel very upset. He struggled mentally with his inability to control them, especially when people around him would deliberately provoke his attacks. He appeared to be shivering from fear, and it’s quite likely he was actually afraid of his own tremors and shaking. In addition to the tremors, he also suffered from tremophobia—a specific phobia that Meige described a few years ago, somewhat similar to ereutophobia, or the fear of blushing, which was described by Pitres and Régis.
Four hours in a freezing bog: Hysterical glossolabial hemispasm twelve hours after rescue. No sensory disorder of face or tongue; sensory disorder of arm, but no motor disorder.
Four hours in a freezing swamp: Frantic lip and facial spasms twelve hours after being rescued. No loss of feeling in the face or tongue; loss of feeling in the arm, but no loss of movement.
Case 309. (Binswanger, July, 1915.)
A man, 27, in good health, called on the second day of the mobilization, got into the line two weeks from mobilization, first in the West, and then, from mid-September, in the East. He was in the artillery and stood shell fire in a big battle very well.
A 27-year-old man in good health reported for duty on the second day of mobilization, lined up two weeks after the mobilization started, first in the West and then, from mid-September, in the East. He was part of the artillery and handled the intense shelling during a major battle quite well.
However, December 27, 1914, while engaged in transport service, on the way back with his horse, he fell into a bog and gradually sank to his neck. Attempts to get the man and his horse out failed. All that saved him from drowning was the freezing of the bog surface. After four hours he was freed by his comrades, apparently frozen stiff, but with consciousness completely preserved. On the next day, at about five o’clock,—twelve hours after his release from the frozen bog,—he had a seizure. It began with headache on the left side and loss of consciousness that lasted 24 hours. The right leg was paralyzed and very painful. He passed through various hospitals and finally arrived at the Jena Nerve Hospital, January 25, 1915.
However, on December 27, 1914, while he was doing transport service and on his way back with his horse, he fell into a bog and slowly sank up to his neck. Efforts to rescue him and his horse were unsuccessful. The only thing that prevented him from drowning was the freezing of the bog's surface. After four hours, his comrades managed to pull him out, apparently frozen solid, but still conscious. The next day, around five o’clock—twelve hours after being freed from the frozen bog—he had a seizure. It started with a headache on the left side and a loss of consciousness that lasted for 24 hours. His right leg was paralyzed and extremely painful. He went through various hospitals and finally arrived at the Jena Nerve Hospital on January 25, 1915.
He was a tall, powerful man, with a slow regular pulse, accelerated heart sounds, lively dermatographia, increased muscular excitability, general increase of knee and Achilles reflexes (left greater than right), slight patellar and ankle clonus present on the left side, Babinski reaction absent, plantar reflex more lively on the left than on the right, but abdominal reflex more lively right than left. Head painful to percussion in the left temporal region. Touch and pain sense segmentally absent in both right extremities. Arm movements free; tremors absent. Active movements almost impossible in the right leg; on passive movement marked pain. Slight muscular tension about knee-, hip-, and ankle-joints.[425] The patient got about with a cane, trailing the left leg. Romberg sign.
He was a tall, strong man, with a slow, regular pulse, fast heart sounds, noticeable skin reaction to scratching, heightened muscle excitability, overall increased knee and Achilles reflexes (left side more than the right), slight clonus in the patellar and ankle areas on the left, no Babinski reflex, more active plantar reflex on the left than the right, but a more active abdominal reflex on the right than the left. His head was painful to touch in the left temporal area. There was a segmental loss of touch and pain sensation in both right limbs. His arm movements were free; no tremors were present. Active movement in the right leg was nearly impossible, with significant pain during passive movement. There was slight muscle tension around the knee, hip, and ankle joints.[425] The patient used a cane to walk, dragging the left leg. Romberg sign.
The right angle of the mouth was withdrawn slightly upward and outward, and lagged a little in active movements. The protruded tongue deviated completely into the right angle of the mouth and there remained, but without tremor. The uvula deviated to the right, and the right palate was held higher than the left. Lively palatal reflex. Speech intact. The patient’s chief complaint was attacks of coughing, which increased his headache to the point of intolerability. A harmless drug caused the coughing and headache to disappear. The patient was a quiet, willing man, who industriously went through his exercises, and on the Kaiser’s birthday was already walking in the marketplace. His tongue contractions gradually improved. His body-weight increased.
The right side of the mouth was pulled slightly up and out, and it lagged a bit in movement. The tongue stuck out toward the right side of the mouth and stayed there, but there was no shaking. The uvula shifted to the right, and the right side of the palate was higher than the left. The palatal reflex was active. Speech was normal. The patient mainly complained of coughing fits that made his headache unbearable. A harmless medication made the coughing and headache go away. The patient was a quiet and cooperative man who diligently worked through his exercises, and by the Kaiser’s birthday, he was already walking in the marketplace. His tongue movements gradually got better, and his weight increased.
In the course of two months the glossolabial and palatal contractions had largely disappeared. The walking movements of the right leg had improved, although there was still a distinct paresis, and a stiffness in the right knee and ankle joints. Climbing stairs was impossible on account of difficulty at the hip. March 30, 1915, the sensory improvement was marked. There was a feeling as though the last three fingers of the hand were asleep; walking was improved; he could walk one or two hours a day. The walk was still slightly spastic-paretic, May 28, when he was discharged.
In the two months that followed, the contractions of the lips and palate had mostly gone away. The movement of the right leg had gotten better, although there was still noticeable weakness, along with stiffness in the right knee and ankle joints. Climbing stairs was impossible due to difficulty with the hip. On March 30, 1915, there was a significant improvement in sensation. It felt like the last three fingers of his hand were numb; his walking had improved, and he could walk for one or two hours a day. The walk was still slightly stiff and weak on May 28 when he was discharged.
It is remarkable that the hysterical attack had such a long incubation period in this case: twelve hours after his removal from the marsh. There were doubtless physical factors of refrigeration, on the one hand, and on the other, psychic factors of fear of sinking alive in the marsh, at the bottom of the phenomenon. The most marked feature, of course, was the glossolabial hemispasm. In the presence of this hemispasm, it is remarkable that there should have been no anesthesia or analgesia of the face, cheek, or tongue; and moreover the paresis of the right mouth and tongue was far less marked than the contracture. It is also striking that the right upper extremity, although it had sensory disorder, failed to show motor disorder.
It’s incredible that the hysterical attack had such a long incubation period in this case: twelve hours after he was taken out of the marsh. There were certainly physical factors like the cold, and on the other hand, psychological factors related to the fear of drowning in the marsh, underlying the phenomenon. The most noticeable feature, of course, was the glossolabial hemispasm. With this hemispasm, it’s surprising that there was no numbness or pain relief in the face, cheek, or tongue; furthermore, the weakness in the right side of the mouth and tongue was much less pronounced than the muscle contraction. It’s also interesting that the right arm, despite having sensory issues, showed no motor problems.
Slight bruise by horse: Apparently invincible complaints of pain. Cure by single-handed capture of many Russians.
Slight bruise from the horse: Clearly unstoppable reports of pain. Treatment by single-handedly capturing many Russians.
Case 310. (Loewy, April, 1915.)
An infantryman was standing below an embankment when a horse fell upon him, bruising him slightly on the left hip. This infantryman later continually complained of pains in the opposite hip though there had never been a contusion there, nor anything felt there. These complaints could not be influenced by exhortation, by diversion, or by drugs. If they were purposely ignored, the patient reacted complainingly and in a way to suggest delusions of persecution.
An infantryman was standing below a slope when a horse fell on him, causing a slight bruise on his left hip. Later on, this infantryman kept complaining about pain in his right hip, even though there had never been any injury or sensation there. These complaints couldn't be eased by encouragement, distraction, or medication. If they were intentionally disregarded, the patient responded with complaints that hinted at delusions of persecution.
Nevertheless, this querulous man soon proved an effective soldier in a storming attack in which the whole battalion distinguished itself, putting himself forward particularly. In fact, by himself he captured a whole group of Russians!
Nevertheless, this complaining man soon showed that he could be an effective soldier during a storming attack in which the entire battalion excelled, especially standing out himself. In fact, he single-handedly captured a whole group of Russians!
Thereupon all the pains in the hip ceased, nor did they recur so long as he was under observation. Morose and complaining before, he now became cheerful.
Then all the pain in his hip went away, and it didn't come back as long as he was being monitored. He had been grumpy and complaining before, but now he became cheerful.
Kick in abdomen by horse: General spasticity; tremors; eye symptoms (e.g. monocular diplopia); convulsions. Improvement.
Kick in abdomen by horse: General muscle stiffness; tremors; eye symptoms (e.g. double vision in one eye); convulsions. Improvement.
Case 311. (Oppenheimer, July, 1915.)
A cuirassier was kicked by a horse on left side of abdomen, November 24, and lost consciousness. A month later, in hospital, hardness and tenderness to pressure of abdominal wall, spastic muscles everywhere, pseudospastic tremor of legs, and complaints of double vision were noted. He also had attacks of convulsions, in which he became unconscious, twitchings appeared, but the tongue was not bitten. Urine was often involuntarily passed in these attacks, but he was not always continent outside attacks, as, for instance, in coughing.
A cuirassier was kicked by a horse on the left side of his abdomen on November 24 and lost consciousness. A month later, while in the hospital, he showed hardness and tenderness to pressure in the abdominal wall, spastic muscles everywhere, a pseudospastic tremor in his legs, and complaints of double vision. He also experienced convulsions that caused him to lose consciousness and twitch, but his tongue was not bitten. He often involuntarily passed urine during these attacks, and he was not always able to control himself outside of the attacks, such as when he coughed.
On admission to nerve hospital: Right-sided monocular diplopia; mild ptosis; ocular movements free. Rapid tremor on shaking hands. Stood with straddling legs affected by vibrating tremor. Knee-jerks considerably increased. In the dorsal position movements of the left leg were accompanied by marked tremor. He even could not go to sleep easily on account of twitching of the left leg.
On admission to the nerve hospital: right-sided double vision in one eye; slight drooping of the eyelid; eye movements normal. Rapid shaking tremor when hands were moved. Stood with legs apart due to a vibrating tremor. Knee-jerk reflexes significantly increased. When lying on his back, movements of the left leg were accompanied by a noticeable tremor. He also had difficulty falling asleep because of twitching in the left leg.
His comrades observed that he had convulsions at night, and often spoke in his sleep. Inoculation against typhoid fever was made early in December. Later, permanent rise of temperature to 37.8. Several attacks, lasting about ten minutes, came under observation of the physician.
His friends noticed that he had seizures at night and often talked in his sleep. He was vaccinated against typhoid fever in early December. Later, his temperature consistently rose to 37.8. Several episodes, lasting about ten minutes, were noted by the doctor.
In January, progressive improvement in the motor sphere and also psychically. The urinary disturbance likewise disappeared, but the spasms persisted.
In January, there was a steady improvement in both physical movement and mental state. The urinary issues also went away, but the spasms continued.
Windage from a shell; fear; fall, unconscious: Homonymous hemianopsia (organic? functional?) with blinking and vasomotor excitability.
Windage from a shell; fear; fall, unconscious: Homonymous hemianopsia (organic? functional?) with blinking and vasomotor excitability.
Case 312. (Steiner, October, 1915.)
A volunteer, 19 (never ill; no nervous disease in the family) after a period of training went into the field October 3, 1914. November 5 a shell struck near his trench, but failed to explode. Up to that time everything had been quiet. The soldier had been looking out of the loop-hole, surveying the landscape. He felt a great fear, felt a blow in the neck, and fell down unconscious. How long he was unconscious is unknown. Sometime later he walked back with his comrades.
A volunteer, 19 (never sick; no mental illness in the family) went into the field on October 3, 1914, after some training. On November 5, a shell hit near his trench but didn't explode. Until that point, everything had been quiet. The soldier had been looking out of the loop-hole, observing the scenery. Suddenly, he felt an intense fear, a blow to his neck, and collapsed unconscious. It's unclear how long he was out. Later, he walked back with his fellow soldiers.
About an hour later, this volunteer—who was a very intelligent young man, possessing some knowledge of biology, including the nature of visual fields—noticed a black spot in the field of vision, which came and went, but after a few hours remained continually without disappearing. Otherwise there was no complaint except a feeling of dizziness when stooping.
About an hour later, this volunteer—who was a smart young man, knowledgeable about biology, including how visual fields work—noticed a black spot in his field of vision that appeared and disappeared, but after a few hours, it stayed there without fading away. Other than that, he had no complaints apart from feeling dizzy when bending over.
Upon examination there could be found no disorder of the internal organs. Neurologically there was blinking, vasomotor excitability, slight reddening of the face, and dermatographia. An expert in ophthalmology confirmed the existence of a homonymous defect in the fields of vision. This defect could not be influenced by suggestion or by any other treatment, nor did any other change whatever occur in the condition.
Upon examination, no issues were found with the internal organs. Neurologically, there was blinking, increased sensitivity in the blood vessels, slight reddening of the face, and skin writing. An ophthalmology expert confirmed a homonymous defect in the visual fields. This defect couldn't be affected by suggestion or any other treatment, nor did any other changes occur in the condition.
Steiner inquires whether this hemianopsia is to be taken as organic or functional. The air-pressure of the shell hissing past might have produced a concussion, or the falling unconscious might have produced a commotio cerebri or a slight hemorrhage. The tic-like blinking and vasomotor excitability, however, suggest functionality.
Steiner asks if this hemianopsia should be considered organic or functional. The air-pressure from the shell whizzing by could have caused a concussion, or losing consciousness might have led to a commotio cerebri or a minor hemorrhage. However, the tic-like blinking and increased sensitivity of the blood vessels suggest it's functional.
Shell-shock PSORIASIS. Post-traumatic eczema.
Shell shock psoriasis. Post-traumatic eczema.
Case 313. (Gaucher and Klein, May, 1916.)
A soldier, 28, came to the Saint-Louis skin clinic, May 15, 1916, for leg lesions three months old. These lesions were cicatricial, squamous, irregular-contoured, and had developed following a wound. The lesions were eczematous.
A 28-year-old soldier came to the Saint-Louis skin clinic on May 15, 1916, for leg lesions that had been present for three months. These lesions were scarred, scaly, irregularly shaped, and had developed after a wound. The lesions were eczema-like.
On the trunk, arms and elbow were lesions of psoriasis. These lesions had appeared after shell-shock. The man had been bowled over June 16, 1915, by a marmite. The psoriatic lesions appeared shortly afterwards. The patient had never seen anything of the sort before.
On his trunk, arms, and elbows were patches of psoriasis. These patches showed up after he experienced shell shock. He had been knocked down on June 16, 1915, by a shell. The psoriatic patches appeared shortly after that. The patient had never seen anything like it before.
In this case the trauma provoked eczema; the emotion, psoriasis. Gaucher and Klein say that they have been struck by the recrudescence of psoriasis since the outbreak of the war, and remark, also, that there has been a relative increase of new cases since July, 1914.
In this case, the trauma caused eczema; the emotion triggered psoriasis. Gaucher and Klein mention that they have noticed a resurgence of psoriasis since the war started and also point out that there has been a relative increase in new cases since July 1914.
There are cases of psoriasis following nervous shock, emotion and trauma. Sometimes the psoriatic lesion develops upon the scar of a wound. In the above case, as in the case of a woman of 25, a refugee from the Arras bombardment, the psoriasis began de novo and slowly developed immediately after the catastrophe of the Jena. Five, possibly six, out of eight cases totaled, appear, unlike the case sketched above, to have developed in cases either tuberculous or of tuberculous stock.
There are instances of psoriasis that occur after experiencing a nervous shock, strong emotions, or trauma. Sometimes, the psoriatic lesion appears on the scar from a wound. In the case mentioned above, as well as with a 25-year-old woman who was a refugee from the Arras bombardment, psoriasis began anew and gradually developed right after the disaster at Jena. Out of a total of eight cases, five or possibly six seem, unlike the previously described case, to have developed in individuals who were either tuberculous or had a history of tuberculosis.
Re psoriasis, Vignolo-Nutati remarks that this is a relatively frequent skin disease amongst Italian soldiers. He states that many of these cases are due to nervous shock. Some are related to wounds appearing near the scars. In all cases an emotional disturbance is the chief cause. Vignolo-Nutati had 86 cases of psoriasis in six months, 52 of the men coming from the front. Eighteen of the men said that they had not previously suffered from the disease.
Regarding psoriasis, Vignolo-Nutati notes that this is a common skin condition among Italian soldiers. He mentions that many of these cases stem from nervous shock. Some are linked to wounds near the scars. In every case, emotional disturbances are the main cause. Vignolo-Nutati encountered 86 cases of psoriasis in six months, with 52 of the men coming from the front. Eighteen of the men reported that they had not experienced the disease before.
A sergeant gets the CROIX DE GUERRE and SHELL-SHOCK together: Transient deafness; later pseudohallucinatory electric bell ringing, reminiscent of civilian work; stereotyped movements, reminiscent of war experience.
A sergeant gets the CROIX DE GUERRE and SHELL-SHOCK together: temporary deafness; later, hallucinations of an electric bell ringing, similar to civilian life; repetitive movements, echoing war experiences.
Case 314. (Laignel-Lavastine and Courbon, May, 1916.)
A sergeant, 24, had worked about Parisian hotels from the age of thirteen and a half. He won the croix de guerre and was evacuated for his wounds April 24, 1915.
A 24-year-old sergeant had been working in Paris hotels since he was thirteen and a half. He received the croix de guerre and was evacuated due to his injuries on April 24, 1915.
It seems that he carried the remains of his company, which had been decimated the night before by a mine explosion, on to the enemy trench, getting there first and facing three Germans, whom he beat down. At this time, gas shells began to rain about. Making a number of violent expiratory movements to get rid of the gas, he found himself unable to progress on account of the fall of the shells, and sat motionless with his hands before his face. He was cast to the earth by an explosion, which at the same time blew off a revolver which the wounded lieutenant had passed to him. He sat up, and, observing that the soldiers had gotten the trench, went back to the lines, where he told his story.
It seems he carried the remnants of his squad, which had been wiped out the night before by a mine explosion, into the enemy trench, getting there first and facing three Germans, whom he took down. At that moment, gas shells started to fall around him. Struggling to clear his lungs from the gas, he found he couldn't move because of the falling shells, and sat still with his hands covering his face. He was thrown to the ground by an explosion, which also blew away a revolver that the wounded lieutenant had given him. He sat up and, noticing that the soldiers had secured the trench, returned to his lines, where he recounted his experience.
He then found that he was deaf, and wounded in the left leg. The wounds rapidly healed, but sundry other symptoms developed. He had a peculiar sensation back of the forehead. He could not think, read or write and was very weary. He got better in a few months, but disorders kept returning.
He then realized that he was deaf and had an injury in his left leg. The wounds healed quickly, but several other symptoms appeared. He felt a strange sensation at the back of his forehead. He couldn't think, read, or write and felt extremely tired. He improved after a few months, but the issues kept coming back.
His deafness had left him in about a fortnight, but when his hearing came back spontaneously, there were peculiar sensations. He constantly heard an electric bell, intense and continuous, like that of a French cinema advertising its films. The sounds seemed to begin in the ear and to run out as a sort of whistling. This sensation was preceded by buzzing and associated with noises like those of a musical triangle or a steam whistle. The noise kept up during waking[431] hours, but was often forgotten while he was at work. In sleep he heard nothing, except sometimes battle noises. August 20, 1915, he was given the diagnosis: labyrinthine shock—hearing returned.
His deafness lasted about two weeks, but when his hearing came back suddenly, he experienced some strange sensations. He continually heard an electric bell, loud and ongoing, similar to the sound of a French cinema advertising its films. The sounds seemed to start in his ear and then faded out into a kind of whistling. This sensation was preceded by buzzing and accompanied by noises like those of a musical triangle or a steam whistle. The noise persisted during the day, but he often forgot about it while he was working. At night, he didn’t hear anything, except sometimes the sounds of battle. On August 20, 1915, he received the diagnosis: labyrinthine shock—hearing returned.
About ten weeks after evacuation, when the headaches and thought blocking began to disappear, a generalized tremor, especially of the head, set in, which the patient called St. Vitus’ dance. Then a peculiar gait began, which lasted several weeks and then transiently reappeared. Every few steps his legs would bend, and he could only walk forward in the attitude of a man who is concealing his height. After resting a few minutes he began to walk regularly again and the cycle began over again. He had to walk with two canes. If he felt some sudden emotion, or sometimes without any obvious reason, he would stop short and look straight ahead, with body bent, and arms before his face. This would last but a moment, whereupon he would walk again normally.
About ten weeks after the evacuation, when the headaches and mental blocks started to fade, a general tremor, especially in the head, appeared, which the patient referred to as St. Vitus' dance. Then, a strange way of walking began, which lasted several weeks and would occasionally come back. Every few steps, his legs would buckle, and he could only move forward like someone trying to hide their height. After resting for a few minutes, he would start walking normally again, and then the cycle would repeat. He had to use two canes to walk. If he experienced a sudden emotion, or sometimes for no clear reason at all, he would freeze in place, looking straight ahead with his body hunched and his arms raised in front of his face. This would only last a moment before he would walk normally again.
When this anomalous walking disappeared, curious face movements and gestures began. If a strange person arrived, the forehead and eyebrows would contract, the eyelids would stand wide, which gave him an expression of surprise lasting a few seconds. At the same time the mouth would open and remain so for some moments. A forced expiration would be executed, suggesting a fish out of water. He would then imperatively strike the table with his fist, or the ground with his foot.
When this unusual way of walking stopped, interesting facial movements and gestures started. If an unfamiliar person came around, his forehead and eyebrows would furrow, his eyelids would widen, creating a look of surprise that lingered for a few seconds. At the same time, his mouth would open and stay that way for a bit. He would then let out a forced breath, like a fish out of water. After that, he would slam his fist down on the table or stomp his foot on the ground.
Laignel-Lavastine and Courbon explain the anomalous movements as stereotypies due to secondary automatism. They are not convulsive, are not preceded by emotion or followed by a sense of relief, and are not tics. They are gestures and postures without present significance, but adapted to certain former circumstances. The electric bell effect is a sort of pseudohallucination, differing from true hallucinations in little except the absence of the externalizing feature. The stereotypical movements are reproductions of things done in the battle, and the pseudohallucinations relate to the former hotel work of the soldier.
Laignel-Lavastine and Courbon describe the unusual movements as stereotypies caused by secondary automatism. They’re not convulsive, don’t come after an emotional event, and aren’t followed by a sense of relief; they also aren't tics. They consist of gestures and postures that lack current meaning but are related to certain past situations. The electric bell effect is a type of pseudohallucination, which is similar to true hallucinations except for the absence of an externalizing factor. The stereotypical movements are reenactments of actions taken during battle, and the pseudohallucinations are connected to the soldier's previous hotel work.
Cinema worker, two days after being waked up by a shell, develops a nystagmiform tremor of eyes and tachycardia. Graves’ disease? Tic (“occupational virtuosity”)?
Cinema worker, two days after being woken up by a shell, develops eye tremors and rapid heartbeat. Graves' disease? Tic ("occupational skill")?
Case 315. (Tinel, April, 1915.)
A soldier was waked up with a start Sept. 22, 1914, by a shell burst. The man was not wounded or shocked, and merely felt a good deal moved. The next day but one he felt a little movement of his eyes, which was at first intermittent but in three or four days became continuous and troublesome. These movements were those of nystagmus, almost transverse and very rapid, and suggestive rather of a vibratory trembling than of a true nystagmus of the eye or of labyrinthine disease. When the patient fixed an object, the nystagmus would stop for a few seconds and then immediately reappear. There had never been any vertigo, nausea, vomiting, deafness, ocular disorder, or disorder of equilibration. During the tests for nystagmus, the morbid nystagmus would stop and be replaced by the normal nystagmus which was obviously slower and more regular. The condition had persisted from September, 1914, to the meeting of the Neurological Society, April 15, 1915. The patient said he had become very emotional and got palpitations on the slightest occasion, such as a fast walk, going upstairs, or hearing a loud noise. There was also a slight vibratory trembling of the fingers and a permanent tachycardia (120-140 beats). Tinel regards the case as one of neurosis, due to a neuromuscular hyperexcitability comparable in some ways with that found in Graves’ disease.
A soldier was jolted awake on September 22, 1914, by the sound of a shell exploding. He wasn't injured or shocked, just deeply stirred. The day after that, he noticed some movement in his eyes that started off sporadic but became continuous and bothersome within three or four days. These movements were characteristic of nystagmus, almost sideways and very rapid, resembling more of a vibrating tremor rather than true eye nystagmus or inner ear disease. When the patient focused on an object, the nystagmus would pause for a few seconds and then return immediately. He had never experienced vertigo, nausea, vomiting, deafness, vision problems, or balance issues. During the nystagmus tests, the abnormal nystagmus would stop and switch to normal nystagmus, which was noticeably slower and more regular. This condition lasted from September 1914 until the meeting of the Neurological Society on April 15, 1915. The patient reported feeling very emotional and experiencing palpitations over even minor situations, like brisk walking, climbing stairs, or hearing loud noises. There was also a slight trembling in his fingers and a constant fast heart rate (120-140 beats per minute). Tinel considers the case to be a form of neurosis, stemming from neuromuscular hyperexcitability similar in some aspects to what’s seen in Graves’ disease.
Meige, in discussion, called attention to the fact that not every nystagmus is of organic origin and that there is a rare form of tic of nystagmiform nature. The victim in this case was an employee in a moving picture house, and very possibly his occupation had permitted him to utilize what Meige speaks of as a “occupational virtuosity” of the eye muscles.
Meige pointed out that not all nystagmus comes from organic causes and that there is a rare type of tic that resembles nystagmus. In this case, the person affected worked in a movie theater, and it’s likely that his job allowed him to develop what Meige refers to as an “occupational virtuosity” of the eye muscles.
Synesthesialgia: FOOT pain on rubbing dry HANDS, following bullet wound of leg.
Synesthesialgia: FOOT pain when rubbing dry HANDS, after a bullet wound in the leg.
Case 316. (Lortat-Jacob and Sézary, November, 1915.)
A foot chasseur was wounded, September 15, 1914, low in the right thigh, a bullet entering outside the biceps tendon and emerging on the inner aspect of the leg, 4 cm. below the knee joint. He at once began to feel pains in the right foot, which grew swollen and red. The leg began to flex upon the thigh and, after straightening under anesthesia, was placed in plaster. An arteriovenous aneurysm developed in the popliteal space; operation, October 22nd, followed November 1, by ligature. The pains in the foot grew better after this operation; but as soon as the wound was cicatrized they came back again as before.
A foot soldier was wounded on September 15, 1914, in the right thigh, with a bullet entering just outside the biceps tendon and exiting on the inner side of the leg, 4 cm below the knee joint. He immediately started to feel pain in his right foot, which became swollen and red. The leg began to bend at the thigh, and after being straightened under anesthesia, it was put in a cast. An arteriovenous aneurysm developed in the popliteal space; surgery was performed on October 22nd and again on November 1, involving a ligation. The pain in the foot improved after the surgery; however, as soon as the wound healed, the pain returned just as it was before.
For seven months the foot pains remained sharp and continuous, such that the man could not leave his bed. If a bright light struck his eyes, the pains grew much more marked, especially in the morning on awakening. The patient found that when his hands were dry he could not use them because of the violent pains which rubbing them would cause in the right foot. Accordingly he kept putting his hands to his mouth to moisten them. Finally he kept a wet rag by him which he could pass from one hand to the other.
For seven months, the foot pain stayed intense and constant, preventing the man from getting out of bed. If a bright light shone in his eyes, the pain became even worse, especially in the morning when he woke up. The patient noticed that when his hands were dry, he couldn't use them because the sharp pains from rubbing them would worsen the pain in his right foot. So, he kept putting his hands to his mouth to wet them. In the end, he had a wet cloth nearby that he could pass from one hand to the other.
The pain was what made walking difficult. Foot movements were only a bit less ample on the affected side than on the normal side. There was a general muscular atrophy of the lower extremity (30.5: 34 about calf, and 40: 49 about thigh). Right knee-jerk more lively than left. Right Achilles jerk absent. Negligible disorders of electrical excitability in the territory of the right sciatic nerve. The skin of the foot was a little thin and pale; the temperature was low; and the nails had transverse striations. The pains grew gradually a little less marked, but if the room temperature was increased or lowered or if the foot became cold, the pains became extreme. Pressure on the popliteal[434] space produced pain on the external border of the foot; likewise pressure on the calf. Lasègue’s sign could not be tested for on account of the contracture of the flexors of leg on thigh. Due to the direct action of the bullet, there was an objective hyperesthesia of the dorsum and sole of the foot. The toes were anesthetic. A cold foot bath increased the pains, and a warm foot bath diminished them (contrary to experience in analgesias).
The pain made walking difficult. The movements of the affected foot were only slightly less extensive than those of the normal foot. There was a noticeable muscle wasting in the lower leg (30.5: 34 around the calf, and 40: 49 around the thigh). The right knee reflex was more active than the left. There was no reflex at the right Achilles tendon. There were minor electrical excitability issues in the area of the right sciatic nerve. The skin on the foot was a bit thin and pale; the temperature was low; the nails had horizontal ridges. The pain gradually became less intense, but if the room temperature changed or if the foot got cold, the pain became severe. Pressing on the back of the knee caused pain on the outer side of the foot, as did applying pressure to the calf. Lasègue’s sign couldn’t be tested due to the tightening of the leg's flexor muscles on the thigh. Because of the bullet's direct impact, there was an increased sensitivity on the top and sole of the foot. The toes were numb. A cold foot bath intensified the pain, while a warm foot bath alleviated it (which is the opposite of typical experiences with pain relief).
This was a case of synesthesialgia in the right foot, brought about by rubbing dry hands, exactly as if there were a direct contact with the foot. Milder painful reactions were brought about by bright lights and loud noises; but on the whole, these other effects were insignificant. It must be remembered that the man was wounded and plainly had also organic nervous disorder. He sometimes complained of radiations of the pain up to the left hypochondrium, and sometimes he showed the classical sensation of “esophageal globus” (lump in the throat). In short, there was in him a special excitability of the nervous system which may partly explain the synesthesialgia.
This was a case of synesthesialgia in the right foot, caused by rubbing dry hands, just like having direct contact with the foot. Milder pain responses were triggered by bright lights and loud noises; however, these additional effects were generally not significant. It should be noted that the man was injured and clearly also had an underlying nervous disorder. He occasionally complained of pain radiating to the left side of his abdomen, and sometimes he experienced the classic sensation of a “lump in the throat.” In summary, he had a heightened sensitivity in his nervous system, which may help explain the synesthesialgia.
Shell-shock; burial: Clonic spasms; later, stupor with amnesia.
Shell shock; burial: muscle spasms; later, a daze with memory loss.
Case 317. (Gaupp, March, 1915.)
A reservist, 28 (laborer in civil life, of a nervous family; even before mobilization had attacks of weakness at his work or in the company of others) January 3 or 4, 1915, fainted in the trench while shells were striking around him. On January 5 he was brought to hospital in deep stupor. He went to the reserve hospital at N. by hospital train, January 8, and arrived at the Tübingen clinic January 18.
A 28-year-old reservist (a laborer in civilian life, from a nervous family; he had been experiencing bouts of weakness at work or around others even before mobilization) fainted in the trench on January 3 or 4, 1915, while shells exploded nearby. On January 5, he was taken to a hospital in a deep stupor. He traveled to the reserve hospital at N. by hospital train on January 8 and arrived at the Tübingen clinic on January 18.
A slip of paper stated that after burial in the trench he had been brought from the field unconscious. Clonic spasms of the upper part of the body are said to have occurred. At the reserve hospital in N., January 10, he was still unconscious, at times twitching his face and the upper part of his body, and once at night excited and delirious.
A slip of paper indicated that after being buried in the trench, he was brought in from the field unconscious. It was reported that he experienced clonic spasms in the upper part of his body. At the reserve hospital in N. on January 10, he was still unconscious, occasionally twitching his face and upper body, and once during the night, he became agitated and delirious.
At first in the clinic he was apathetic, speaking not a word, looking vacantly into the air as if lost in a dream. He went to the section passively, and lay passively in bed.
At first in the clinic, he was indifferent, saying nothing, staring blankly into the space as if he were caught in a dream. He went to the section without any enthusiasm and lay in bed without any energy.
In the examining room, he stood speechless with unemotional face, sometimes looking up to the ceiling, slowly scratching his head, failing to answer questions, although fixing his eyes upon the physician. He could not be communicated with in writing, playing uncomprehendingly with the pencil or scratching his head with it. He would start with fright at a sudden noise or an unexpected touch. Sometimes he would heave a deep sigh, grasp his head in his hands, or lay hold of his hair with a hopeless expression of face and shake his head to and fro.
In the examination room, he stood silent with a blank expression, occasionally glancing up at the ceiling, slowly scratching his head, unable to answer questions while keeping his eyes fixed on the doctor. He couldn't communicate in writing, playing aimlessly with the pencil or using it to scratch his head. He would jump at sudden noises or unexpected touches. Sometimes, he'd let out a deep sigh, clutch his head in his hands, or tug at his hair with a look of despair on his face, shaking his head back and forth.
Next day, January 19, he made a few slow, low answers. He was found to be entirely disoriented and with associations impeded, although he could get out his name and residence with difficulty. Some of his color identifications were correct, such as red and green; some impossible, as yellow, brown, violet. A comrade who was called in and could speak the Cologne dialect, was talked with at first with difficulty,[436] later more easily. Although the patient was visibly freer, he remained without apparent emotion, retaining a rigid and dreamlike expression of face. It was hard to find words, although objects were named correctly, and there was no paraphasia or agnosia. Vision and hearing were normal; walking, manual movements, eating were all undisturbed though slow. The patient had to be led to the toilet. It seemed as if all intellectual life was at rest, and that in the absence of impulses from without, there would have been complete apathy. It was made out that the patient thought he was still in the trenches.
The next day, January 19, he gave a few slow, quiet responses. He seemed completely disoriented and struggled to make connections, although he could manage to say his name and where he lived, but with difficulty. Some of his color identifications were correct, like red and green; others were impossible, like yellow, brown, and violet. A fellow soldier who was brought in and spoke the Cologne dialect was initially hard to communicate with, but it became easier over time. Even though the patient appeared more relaxed, he still showed no visible emotion and had a stiff, dreamlike expression on his face. It was challenging to find the right words, even though he named objects correctly, and there were no signs of paraphasia or agnosia. His vision and hearing were normal; he walked, used his hands, and ate without trouble, though slowly. He needed assistance to get to the toilet. It seemed like all his intellectual activity was shut down, and without external stimulation, he would have been completely apathetic. It became clear that the patient believed he was still in the trenches.
Next day, the stupor had decreased and the patient spoke, getting his bearings for a time. There was a complete amnesia as to the cause and duration of his condition. During the next period, up to the beginning of February, 1915, consciousness cleared and the apathy was replaced with anxiety, weariness, and a dull headache.
The next day, the daze had lessened, and the patient started to talk, regaining his sense of reality for a while. He had no memory of what caused his condition or how long it had lasted. In the following weeks, leading up to early February 1915, his awareness improved, and the numbness gave way to feelings of anxiety, fatigue, and a persistent headache.
During February, the patient gradually returned to his senses, and remained in a state of general nervous exhaustion. Amnesia was complete for at least two weeks of his life and recollections were fragmentary for the first three days of his stay in the clinic. He worked willingly in the garden with the other patients. On February 26, the patient was cured and went back to the reserve battalion in a much strengthened condition.
During February, the patient slowly regained his awareness and was still experiencing general nervous exhaustion. He had no memory of at least two weeks of his life, and his memories were just bits and pieces for the first three days he was at the clinic. He willingly helped in the garden with the other patients. On February 26, the patient was fully recovered and returned to the reserve battalion in a much stronger state.
Battles (including liquid fire); eventually shell-shock: Hallucinatory delirium, mutism, asthenia—after a few days puerilism (history of convulsive crisis in adolescence) with regression of personality to late childhood.
Battles (including incendiary weapons); eventually psychological trauma: Hallucinatory delirium, inability to speak, weakness—after a few days childish behavior (history of convulsive episodes in teenage years) with a decline in personality back to early childhood.
Case 318. (Charon and Halberstadt, November, 1916.)
Puerilism (Dupré) appeared in a soldier, 21 (uncle and cousin insane; patient had difficulty in studies at fourteen and nervous spells for two years, with loss of consciousness, fall and convulsions probably at rare intervals; a student at eighteen) after he had taken part in a number of battles with the Chasseurs Alpins. He was exposed once to liquid fire July 21, 1916. He entered the military psychiatric center at Amiens. Mental troubles had followed the bursting of a shell near him. He said a few words, such as, “Alsace; fire; blood; snow; it hurts.” These phrases, spoken in a low tone, with an anxious appearance, eyes fixed, suggested hallucination. He seemed to be listening. Aside from the isolated words above mentioned he showed complete mutism. There was physical weakness, difficulty in walking without support, exaggeration of patellar reflexes, pains in the head and limbs. After several days, he said, “Milk; bread.” After this the anxiety and the slow and difficult walking disappeared, whereupon the puerilism appeared.
Puerilism (Dupré) was observed in a 21-year-old soldier (whose uncle and cousin were mentally ill; the patient had struggled with his studies at fourteen and experienced nervous spells for two years, including loss of consciousness, falls, and convulsions, though probably infrequently; he was a student at eighteen) after he participated in several battles with the Chasseurs Alpins. He was exposed to liquid fire on July 21, 1916. He was admitted to the military psychiatric center in Amiens. His mental issues began after a shell exploded nearby. He uttered a few words like, “Alsace; fire; blood; snow; it hurts.” These words were spoken softly, with a worried look, and his eyes were fixed, suggesting he was having hallucinations. He seemed to be listening intently. Aside from the isolated words mentioned, he was completely mute. He exhibited physical weakness, had trouble walking without assistance, exaggerated patellar reflexes, and experienced pain in his head and limbs. After a few days, he said, “Milk; bread.” Following this, his anxiety and slow, difficult walking improved, but then the puerilism set in.
Now the soldier began to run instead of walking. He galloped and gamboled like a child imitating a horse, or he would sit on a board seeming to paddle. He would skip along the halls. The puerilistic phases were rather brief and for the most part he lay in bed. There was still a certain asthenia. He made little paper boats in bed, keeping them in a small metal box along with bits of bread, looking glass and the like. If a gesture was made to take them away, he would protest and press the box to his breast, looking childish and anxious, and if the box were taken he would weep hot tears. Sometimes he would stick out his tongue at the attendants. His mother came to see him and afterwards he[438] would say, “Mamma told me to be good, to eat well, to get well and to go home.” He would use childish grammar,—“Me eat much.” Asked why he had hollowed out a small hole in the wall of the room, he answered, “I did it for fun, but I will not do it any more. Mother doesn’t want me to.” The patient was unwilling to answer a question correctly; would sometimes answer incorrectly at first and correctly afterward.
Now the soldier started to run instead of walking. He galloped and skipped around like a child pretending to be a horse, or he would sit on a board and seem to paddle. He would bounce down the halls. These childish moments were pretty short, and for the most part, he lay in bed. There was still some weakness. He made little paper boats in bed, keeping them in a small metal box along with bits of bread, a mirror, and other little things. If someone tried to take them away, he would protest and hold the box to his chest, looking childlike and worried, and if the box was taken from him, he would cry real tears. Sometimes he would stick out his tongue at the attendants. His mother came to visit him, and afterward, he would say, “Mom told me to be good, to eat well, to get better, and to go home.” He would use childish grammar, saying, “Me eat much.” When asked why he had made a small hole in the wall of the room, he replied, “I did it for fun, but I won’t do it anymore. Mom doesn’t want me to.” The patient was reluctant to answer a question correctly; he would sometimes give the wrong answer at first and then correct himself later.
It appears that the man had adopted the language, occupations and attitude of a child, showing a regression of personality ten to twelve years backwards. There was a neurotic basis in the convulsive crises of adolescence. On the basis of this predisposition following shock there appeared an attack of confusion, upon which, several days later, supervened ecmnesic phenomena of hysterical nature assuming all the features of puerilism.
It seems that the man had taken on the language, jobs, and mindset of a child, reflecting a regression of personality by about ten to twelve years. There was a neurotic foundation in the convulsive episodes of his teenage years. Following a shock, this predisposition led to a bout of confusion, which a few days later was overtaken by hysterical symptoms that displayed all the characteristics of childishness.
Bomb-dropping from airplane; unconsciousness: Battle dreams. Leaves of absence failed to relieve. Episodes of dizziness and fugue.
Bombing from airplanes; being unconscious: Battle dreams. Time off didn't help. Spells of dizziness and confusion.
Case 319. (Lattes and Goria, March, 1917.)
M. Alessandro, Class ’79, baker (father a drunkard; brother an idiot, in asylum), had typhus in youth, and as a boy had periods of intense “pavor nocturnus,” but no convulsions. He enjoyed good health in the army before the following event:
M. Alessandro, Class ’79, a baker (his father was a drunk; his brother is in a mental institution), had typhus when he was young, and as a child, he experienced episodes of intense night terrors, but no seizures. He was healthy during his time in the army before the next event:
On July 13, 1915, a bomb, dropped by an airplane, fell near an Italian soldier, killing many comrades, and throwing the man to the ground unconscious. He awoke several hours later at a hospital in a stunned condition. During the night, under the influence of terrifying dreams, he would leave his bed to look for enemies who, it seemed to him, were throwing stones and firing. He managed to grasp a rifle and fire at the images he saw. He was given a 60 days’ leave of absence during which he did not improve; and then again 90 days’ furlough, which he spent at his home, where terrifying dreams, tremor of limbs and asthenia continued.
On July 13, 1915, a bomb dropped from an airplane hit near an Italian soldier, killing many of his comrades and knocking him unconscious. He woke up several hours later in a hospital, feeling disoriented. That night, plagued by terrifying dreams, he got out of bed to search for enemies who, in his mind, were throwing stones and shooting at him. He managed to grab a rifle and fired at the visions he saw. He was given a 60-day leave of absence during which he didn’t improve, followed by another 90 days' furlough that he spent at home, where he continued to experience terrifying dreams, trembling limbs, and weakness.
He came under observation February 10, after his second leave. Nutrition fair. Insomnia. Constant terrifying dreams. Coated tongue. Tremor of hands, head, body, ceasing during voluntary movements. Episodically he had spells of dizziness followed by absent-mindedness, whereupon he wandered aimlessly about, of a sudden becoming aware of being in a place, but not knowing how he came there.
He was put under observation on February 10, after his second leave. Nutrition was good. He had insomnia and constant terrifying dreams. His tongue was coated. He experienced tremors in his hands, head, and body, which stopped when he moved voluntarily. Occasionally, he had dizzy spells that were followed by absent-mindedness, during which he would wander around aimlessly, suddenly realizing he was in a location without knowing how he got there.
Special senses intact. Several points of cutaneous hyperesthesia, particularly mammary and pseudo-ovarian on the left, pressure whereon provoked a lively emotional reaction with acceleration of pulse, redness, lacrimation. Knee reflexes lively, cutaneous reflexes normal, except the plantar which were very lively. Restless, hyperemotional, he wept for insignificant reasons and wanted to leave hospital for fear of dying there. He was discharged unimproved after a fortnight.
Special senses are intact. There are several areas of increased sensitivity on the skin, especially around the left breast and pseudo-ovarian area, where applying pressure caused a strong emotional reaction, resulting in an increased heart rate, flushing, and tearing. Knee reflexes are active, and skin reflexes are normal, except for the plantar reflexes, which are very active. He is restless and overly emotional, crying for minor reasons and wanting to leave the hospital out of fear of dying there. He was discharged without improvement after two weeks.
Nostalgic temperament; depression on entering service; rheumatism. A box falls from an airplane near by: Fear and tears; later depression, nostalgia, dreams, hyperthyroidism.
Nostalgic mood; feeling down when starting work; arthritis. A box drops from a nearby plane: Fear and tears; followed by sadness, longing for the past, dreams, hyperthyroidism.
Case 320. (Bennati, October, 1916.)
An Italian private in the infantry was recalled to military service. He was a small farmer, and being disposed to homesickness, grew depressed from the day he left for service. His sleep was disturbed, he was greatly affected by the wet and damp of the trenches, and was in a state of continual fear. Finally, pains, hypersensitiveness, and fever developed.
An Italian private in the infantry was called back to military service. He was a small farmer, and being prone to homesickness, he felt down from the moment he left for duty. His sleep was disrupted, he was significantly impacted by the wet and damp of the trenches, and he lived in constant fear. Eventually, he started experiencing pain, heightened sensitivity, and fever.
As an enemy airplane passed over one day, a box fell at the man’s feet and threw him into a profound fear with tears. He was conducted to a tent to rest; his regiment was shortly sent to the rear, and he remained on active service for a few days despite the fever and pains. Finally the swelling of his leg compelled him to take to bed. (Fatigue in antebellum life had always shown itself in aches of the legs.) He had now been in active service about a month and his homesickness overcame him. He was in a state of deep physical and mental depression. It was not his own troubles so much as those of his family which preoccupied him. His knees hurt him so that he had to weep; or if Sardinia was mentioned, he cried, and said, “Oh, how I love Sardinia!” He grew fatigued very easily. He had many dreams about Sardinia, his father, and the war, especially dreaming about being wounded in the legs (question of being stimulated by the joint aches). The reflexes were normal, though slight tremors set up in the legs after testing. The thyroid gland was somewhat swollen, and it appears that the patient had noticed this five days before entering hospital. The patient was rather vagotonic; pulse-rate stood at 56; oculocardiac-reflex, 56-84; Mannkopf negative; Thomayer and Erben marked (56-88 and 88-60); von Graefe marked; Stellwag present.
As an enemy plane flew overhead one day, a box fell at the man's feet, throwing him into deep fear and tears. He was taken to a tent to rest; his regiment was soon sent to the rear, and he stayed on active duty for a few days despite having a fever and pain. Finally, the swelling in his leg forced him to go to bed. (Fatigue in pre-war life had always shown up as leg aches.) He had been on active duty for about a month, and his homesickness overwhelmed him. He was in a state of deep physical and mental depression. It wasn’t so much his own problems that occupied his mind but those of his family. His knees hurt so much that he cried, or when Sardinia was mentioned, he would cry and say, “Oh, how I love Sardinia!” He got tired very easily. He had many dreams about Sardinia, his father, and the war, especially about being wounded in the legs (possibly stimulated by the joint pain). The reflexes were normal, though there were slight tremors in his legs after testing. The thyroid gland was somewhat swollen, and it seems he had noticed this five days before entering the hospital. The patient was somewhat vagotonic; his pulse rate was at 56; oculocardiac reflex was 56-84; Mannkopf was negative; Thomayer and Erben were marked (56-88 and 88-60); von Graefe was marked; Stellwag was present.
A shell pitches without bursting: Unconsciousness; stupor; MAMA MIA!; oniric delirium; amnesia. Recovery in five weeks.
A shell pitches without breaking: Unconsciousness; confusion; MAMA MIA!; dreamlike delirium; memory loss. Recovery in five weeks.
Case 321. (Lattes and Goria, March, 1917.)
An Italian soldier of the Class of ’95, a mechanic (mother cardiac; as a boy, pains in joints and heart; since boyhood, no illness), had a big Austrian shell pitch near him, July 23, 1915. The shell failed to explode and injured no one. The patient, however, fell to the ground, unconscious, and remained in the camp hospital for two days, quite immobile. This event followed an advance by his company under very fatiguing circumstances without sleep for a period of four days.
An Italian soldier from the Class of ’95, a mechanic (mother had heart issues; as a kid, he had pain in his joints and heart; has had no illnesses since childhood), had a large Austrian shell land near him on July 23, 1915. The shell didn’t explode and didn’t hurt anyone. However, the soldier collapsed and lost consciousness, staying in the camp hospital for two days, completely still. This incident occurred after his company had advanced under very exhausting conditions without any sleep for four days.
July 26, the patient was observed in profound stupor, non-reactive, constantly and monotonously repeating the phrase, Mama mia!, with fixed gaze and smiling as if at visions. He swallowed food. The pupils reacted poorly to light, and the cornea and nasal mucosa seemed anesthetic. The tendon and skin reflexes were lively. The muscles were hypotonic; bradycardia, 56; no control over feces or urine.
July 26, the patient was seen in a deep stupor, unresponsive, continually and monotonously repeating the phrase, Mama mia!, with a fixed gaze and smiling as if seeing things. He was able to swallow food. The pupils barely reacted to light, and the cornea and nasal mucosa appeared numb. The tendon and skin reflexes were active. The muscles were flaccid; heart rate was 56; no control over bowel or bladder.
July 27-28, restlessness at night, gasping movements, and poses of terror.
July 27-28, restless nights, gasping movements, and poses of fear.
July 29, he called for his mother, who had been dead for several years. He was still stuporous and insensible.
July 29, he called for his mother, who had passed away several years earlier. He was still dazed and unresponsive.
From August 1 to 10, he improved slowly and became able to carry bread to his mouth after it had been put in his hands. He still did not speak and made signs when he wished to urinate or defecate. Pulse 50-60.
From August 1 to 10, he slowly got better and was able to bring bread to his mouth after it was placed in his hands. He still didn't talk and used gestures when he needed to urinate or have a bowel movement. Pulse 50-60.
August 12, the patient began to react to intense light and to pain stimuli, as well as to pressure. He ate voraciously.
August 12, the patient started responding to bright light and painful stimuli, as well as to pressure. He ate eagerly.
August 15, visual stimuli were responded to, the pulse had risen to 80, the skin reflexes were no less lively. There began to be terrifying dreams at night, with motor reactions.
August 15, visual stimuli were reacted to, the heartbeat had risen to 80, and the skin reflexes were just as active. Terrifying dreams began to occur at night, accompanied by motor reactions.
August 17, the patient looked about more alertly, promptly seeing bread when placed in the center of the field of vision and saying words to the man who might try to remove the[442] bread. He did not yet react to acoustic stimuli, nor was there any other change up to August 21.
August 17, the patient appeared more alert, quickly spotting bread when it was placed in the center of his field of vision and speaking to the man who might try to take the[442] bread. He still did not respond to sounds, and there were no other changes up until August 21.
August 22 a notable improvement set in. The hearing was now slightly diminished, questions were answered after a brief refractory period. After a few questions, however, a state of exhaustion would ensue, which would disappear only after a short rest. There was amnesia for the entire period following the day of his departure for the front, May, 1915. At this time, instead of eating voraciously, he showed anorexia. The skin and tendon reflexes, instead of being lively, were now dull. There still were battle dreams of enemies trying to kill him.
August 22 brought a noticeable improvement. His hearing was now slightly less impaired, and questions were answered after a brief pause. However, after a few questions, he would feel exhausted, which would only go away after a short rest. He couldn’t remember anything from the time after he left for the front in May 1915. Instead of having a big appetite, he was now experiencing anorexia. His skin and tendon reflexes, which used to be quick, were now sluggish. He still had nightmares about enemies trying to kill him.
August 25, there was an area of hypesthesia on the inner aspect of the right thigh, but otherwise no disorder of sensation. The pulse stood at 80 and there were no other neurological phenomena.
August 25, there was a reduced sensitivity in the inner part of the right thigh, but otherwise no issues with feeling. The pulse was at 80 and there were no other neurological symptoms.
August 31, the patch of hypesthesia of the thigh and the retrograde amnesia disappeared. There was still a slight diminution of hearing. The accident of the non-exploding bomb could now be recalled, but there was a memory gap for all facts up to the latter part of August.
August 31, the numbness in the thigh and the retrograde amnesia went away. There was still a slight decrease in hearing. The incident with the unexploded bomb could now be remembered, but there was a gap in memory for everything that happened until the latter part of August.
September 2, dreamless sleep; no signs of abnormality except a slight diminution of hearing. Discharged, well.
September 2, slept without dreams; no signs of problems except a slight decrease in hearing. Discharged, doing well.
Jostled carrying explosives; no explosion; unconsciousness: Deafmutism and foggy vision. Gradual recovery from these symptoms. Then, on rising from bed, camptocormia.
Jostled while carrying explosives; no explosion; unconsciousness: Deafness and blurry vision. Gradual recovery from these symptoms. Then, upon getting up from bed, a bent posture.
Case 322. (Lattes and Goria, March, 1917.)
An Italian of the Class of 1891 (convulsions and pains in the spine, with rigidity, as a child; typhoid fever at 18; brother sickly, neuropathic; mother subject to periodic convulsions; father alcoholic and nervous), on the night of November 26, 1915, was carrying a number of tubes of explosives. A comrade stumbled and fell over the soldier, who fell to the ground unconscious. None of the glycerine tubes exploded, and none of the soldiers round about were hurt.
An Italian from the Class of 1891 (had convulsions and back pain, with stiffness, as a child; got typhoid fever at 18; brother was sickly and had nerve issues; mother had occasional convulsions; father was an alcoholic and nervous), on the night of November 26, 1915, was carrying several tubes of explosives. A comrade tripped and fell over the soldier, who lost consciousness. None of the glycerine tubes exploded, and none of the nearby soldiers were injured.
The man regained consciousness at the camp hospital, but remained deafmute and also impaired as to vision. It was as if a screen of fog lay between him and objects seen.
The man woke up in the camp hospital, but he couldn't hear or speak and his vision was also blurry. It felt like there was a foggy barrier between him and the things he could see.
During fifteen days of observation at the camp hospital, he had terrible war nightmares. The mutism, the visual disorder, and the deafness then gradually disappeared without special treatment.
During fifteen days of observation at the camp hospital, he experienced terrible nightmares about the war. The mutism, visual disturbances, and deafness eventually faded away on their own without any special treatment.
However, when the patient rose from bed, it was found that his lumbar vertebral column was stiff. He walked bent forward and was unable to bend or straighten the back. There was a hyperesthesia along the vertebrae, especially on pressure. X-ray examination showed no bone lesion. The larynx and cornea were sensitive, and the plantar reflexes were absent. The abdominal reflexes were present. The pupils reacted to light and accommodation. There were two areas of analgesia in the nipple regions. The expression of the patient’s face was relaxed and drooping.
However, when the patient got out of bed, it was found that his lower back was stiff. He walked hunched over and couldn't bend or straighten his back. There was increased sensitivity along the spine, especially when pressure was applied. X-ray examinations revealed no bone damage. The larynx and cornea were sensitive, and the plantar reflexes were absent. The abdominal reflexes were present. The pupils responded to light and focus. There were two areas of numbness around the nipple regions. The patient's facial expression was relaxed and droopy.
A heavy cannon slides and grazes a man: Unconsciousness; stupor; amnesia (anterograde amnesia persistent). Complete recovery in less than seven weeks.
A heavy cannon moves and brushes against a man: Unconsciousness; daze; memory loss (short-term memory loss persistent). Full recovery in under seven weeks.
Case 323. (Lattes and Goria, March, 1917.)
An Italian soldier of the Class of 1895, a peasant (family healthy; non-alcoholic; good scholar) was, July 19, 1915, helping drag a heavy cannon up hill. The big gun slid, hit several men, and grazed the patient, making a slight abrasion on his leg. He immediately lost consciousness, and arrived at the camp hospital in a stupor, which lasted so long that catheterization was necessary.
An Italian soldier from the Class of 1895, who came from a healthy peasant family, didn’t drink alcohol, and was a good student, was helping to haul a heavy cannon uphill on July 19, 1915. The cannon slipped, struck several men, and grazed him, causing a small abrasion on his leg. He instantly lost consciousness and arrived at the camp hospital in a daze, which lasted long enough that a catheter was needed.
A week later he was observed in hospital, immobile and non-reactive, with a swollen abdomen and fecal impaction. The pupils were widely dilated and reacted poorly to light. The corneal reflexes were absent, and the nasal mucosa was anesthetic. Pulse 50. The patient failed to eat. Next day there was no change in his condition. He was quiet throughout the night.
A week later, he was seen in the hospital, unable to move and unresponsive, with a swollen abdomen and a blockage in his bowels. His pupils were very dilated and did not respond well to light. He had no corneal reflexes, and his nasal passages had no sensation. His pulse was 50. The patient did not eat. The next day, there was no change in his condition. He was calm all night.
On the morning of July 29, a number of answers were obtained to questions put in a loud voice, though he was unaware of much more than his name, being ignorant of the name of his country, his age, his division, where he had come from, what had happened to him, or where he was. He had now begun to eat spontaneously.
On the morning of July 29, several answers were given to questions shouted at him, but he didn't know much besides his name. He had no idea what country he was from, how old he was, what division he belonged to, where he had come from, what had happened to him, or where he was. He had now started to eat on his own.
During the following days, up to August 4, the amnesia gradually dissolved for the facts before the trauma. He remembered having been greatly frightened at the time of the accident but could not remember the accident itself, and the gap for subsequent events was still complete. The pharyngeal reflex was still poor. August 5, he began to remember the details concerning the accident. About the middle of August there was no longer any diminution of hearing and ideation became more free and rapid.
During the following days, up until August 4, his memory slowly returned for the events that happened before the trauma. He recalled being very frightened at the time of the accident, but he couldn’t remember the accident itself, and he still had a complete blank for what happened afterward. His pharyngeal reflex was still weak. On August 5, he started to remember details about the accident. By mid-August, he no longer experienced any loss of hearing, and his thoughts became clearer and quicker.
September 4, he was discharged, well.
September 4, he was discharged, feeling good.
Shell explosions SEEN: Emotion; insomnia. Artillery HEARD twelve days later: “finished off.”
Shell explosions SEEN: Emotion; insomnia. Artillery HEARD twelve days later: “finished off.”
Case 324. (Wiltshire, June, 1916.)
A lance-corporal, 36, had had a nervous debility four or five years before the war, caused by an overstudy of music. He had not stopped work at that time, but suffered from depression, anorexia, and insomnia, lasting for some weeks.
A lance-corporal, 36, had experienced a nervous breakdown four or five years before the war, triggered by overstudying music. He didn't quit working at that time, but he struggled with depression, anorexia, and insomnia that lasted for several weeks.
The lance-corporal got on well at the front for 11 weeks, until finally eight shells pitched near him. Although he was unhurt, he began to suffer from anorexia, insomnia, and depression. While in billets 12 days later, some English artillery became heavily engaged, whereupon “The noise promptly finished me off.” The insomnia, depression, and anorexia became more marked, and the patient could not sleep unless heavily drugged.
The lance corporal did well at the front for 11 weeks, but then eight shells landed nearby. Although he wasn't injured, he started experiencing anorexia, insomnia, and depression. Twelve days later, while in billets, some English artillery got heavily involved, and “the noise completely broke me.” The insomnia, depression, and anorexia worsened, and he could only sleep if he was heavily medicated.
Shell-shock: Emotion. More shells: Insomnia; war dreams. Head tremor and tic, two weeks after initial shock.
Shell shock: Emotion. More shells: Insomnia; war dreams. Head tremor and tic, two weeks after the initial shock.
Case 325. (Wiltshire, June, 1916.)
The psychic trauma is, according to Wiltshire, more important than physical trauma in the following case of a sergeant of infantry, 28, a man without neuropathic taint. This man had been nine months at the front and through Mons, but had been quite well until three weeks before coming to hospital.
The psychological trauma is, according to Wiltshire, more significant than physical trauma in the case of a 28-year-old infantry sergeant, who had no history of neurological issues. This man had spent nine months on the front lines and had been through Mons, but he had been in good health until three weeks before arriving at the hospital.
“Twenty-three days ago, I was issuing rations when they got the range of us—and killed the other chaps. I got blown away and knocked over. I saw everything—fellows in pieces. Then a second shell came. I got lifted and knocked about ten yards.” Then he began to shake but carried on.
“Twenty-three days ago, I was handing out rations when they got a fix on us—and killed the other guys. I got blown back and knocked over. I saw everything—guys in pieces. Then a second shell came. I got thrown and landed about ten yards away.” Then he started to shake but kept going.
Two days later, “Shells dropped on the dug-out and killed the other chaps. I have not slept properly since this. If I go to sleep, I wake up seeing people killed, shells dropping, and all kinds of horrid dreams about war.” One or two of the men killed had been pals.
Two days later, “Shells fell on the dugout and killed the other guys. I haven't slept well since then. When I do fall asleep, I wake up seeing people dying, shells falling, and all sorts of terrible dreams about war.” One or two of the killed men had been friends.
A fortnight after the first incident, while in a base hospital, head-shaking began. The patient would jump at the least sound. There were spasmodic tic movements with the extension of the head, protrusion of lower jaw, and contraction of occipitofrontalis muscle. Sometimes the left shoulder girdle was affected in the same way. There was a slight fine tremor of hands and eyelids and difficulty in keeping the eyes fixed on an object.
A couple of weeks after the first incident, while in a military hospital, head shaking started. The patient would flinch at the slightest noise. There were sudden, involuntary movements involving the head, a jutting jaw, and tightening of the occipitofrontalis muscle. Occasionally, the left shoulder area was affected in a similar manner. There was also a slight, shaky tremor in the hands and eyelids, and difficulty in keeping the eyes focused on an object.
Hyperthyroidism, hemiplegia, irritative symptoms after exhaustion (by heat?).
Hyperthyroidism, partial paralysis, irritating symptoms after fatigue (possibly due to heat?).
Case 326. (Oppenheimer, February, 1915.)
A man (not previously nervous, no faulty heredity, heatstroke August 21) suddenly fell down in a great heat, after a fatiguing march, and remained unconscious for several hours, waking with vertigo, headache, paralysis of left side, vomiting, and twitching of the face. On September 23, admitted to reserve hospital. Knee phenomenon increased. Urinary retention; catheter used. Speech disturbance, facial twitching. Vomiting had stopped September 10. Catheterization could be avoided through warm sitz-baths. October 30, on sitting up, occipital pain and vertigo. November 15, urinary symptoms improved. Also improvement otherwise. December 1, gait vacillating and uncertain. Headache. Admission to nerve hospital, December 3. Here complained of twitchings in the frontals and corrugators. Wide palpebral gaps. Rare, or absent, movements of lids. The extended hands showed active, rapid tremor. Tendon phenomena increased in the arms and especially in the legs. Abdominal reflexes increased. Active tremor in the legs. Gluteal tremor. Very pronounced Graves’ symptoms. Syndactylism very pronounced in the feet, between second and third toes. Later on, improvement under half-baths, etc. Worse after ten days’ leave of absence, especially marked increase of tremor (rest tremor), augmented on movement.
A man (not previously nervous, no genetic issues, heatstroke on August 21) suddenly collapsed in extreme heat after a tiring march and remained unconscious for several hours. He woke up feeling dizzy, with a headache, paralysis on his left side, vomiting, and facial twitching. He was admitted to the reserve hospital on September 23. His knee condition worsened. There was urinary retention, and a catheter was used. He had speech difficulties and facial twitching. Vomiting had stopped by September 10. Catheterization could be avoided with warm sitz baths. On October 30, when sitting up, he experienced pain at the back of his head and dizziness. By November 15, his urinary symptoms had improved, and he showed general improvement. On December 1, his gait was unsteady and uncertain, accompanied by a headache. He was admitted to a nerve hospital on December 3, where he complained of twitching in his forehead and frowning muscles. His eyelids were wide open with few or no movements. His outstretched hands showed active, rapid shaking. Tendon reflexes increased in his arms and especially in his legs. His abdominal reflexes were heightened. There was noticeable shaking in his legs and gluteal tremors. He exhibited very pronounced Graves' symptoms, and syndactyly was very pronounced between the second and third toes of his feet. Later on, he showed improvement with half-baths, etc. However, it worsened after a ten-day leave of absence, particularly marked by an increase in tremors (resting tremor), which intensified with movement.
Re heat stroke, Wollenberg has called attention to the effect of the heat of the summer months upon German soldiers. Cases of heat stroke have not been rare in the German army. About half the cases have convulsions or epileptoid seizures, as well as tremors and nystagmus. About a quarter of the cases have shown confusion and delusions, with anxiety and mania. A degree of mental impairment has followed a number of these heat strokes, together with sundry signs of organic disorder, such as reflex changes, pupillary changes, and difficulty in speech.
Regarding heat stroke, Wollenberg has pointed out the impact of summer heat on German soldiers. Cases of heat stroke are not uncommon in the German army. About half of the cases involve convulsions or epileptoid seizures, along with tremors and nystagmus. Around a quarter of the cases exhibit confusion and delusions, along with anxiety and mania. Some of these heat strokes have resulted in a degree of mental impairment, along with various signs of organic disorder, such as changes in reflexes, pupillary changes, and speech difficulties.
Forced marches; skirmishes; rheumatism: Generalized TREMORS. On the road to recovery in six months.
Forced marches; skirmishes; chronic pain: Widespread TREMORS. On the path to recovery in six months.
Case 327. (Binswanger, July, 1915.)
A German letter carrier, 27, entered the war at the outset, made forced marches in great heat, was in a number of skirmishes and in the capture of Namur, and fell ill early in September, with swollen and painful right foot and rheumatic pains in knees and shoulders. He was put on garrison duty; but the rheumatic pains in the joints increased toward the end of September, and he was treated in hospital for rheumatism.
A 27-year-old German mailman joined the war at the beginning, endured forced marches in intense heat, participated in several skirmishes, and was involved in the capture of Namur. Early in September, he fell ill with a swollen and painful right foot and rheumatic pain in his knees and shoulders. He was assigned to garrison duty, but as September came to a close, the pain in his joints worsened, and he was treated in the hospital for rheumatism.
He became able to walk only in the second half of December, marked tremors affecting the whole body. His bodily condition had been good. He slept well, and while at rest in bed he felt entirely well; but upon every attempt to get up and put his feet down, these violent trembling motions would always reappear. Treatment by hydro- and electrotherapy remained entirely unsuccessful. February 8 he was transferred to a nerve hospital.
He was able to walk only in the second half of December, with noticeable tremors affecting his entire body. His physical condition had been good. He slept well, and while resting in bed, he felt perfectly fine; but whenever he tried to get up and put his feet down, those intense shaking movements would come back. Treatment with hydrotherapy and electrotherapy was completely ineffective. On February 8, he was moved to a nerve hospital.
He had been in the postal service from 1903. He was of normal bodily and mental development and had had no previous illnesses. His military service had been executed from 1909 to 1911. He had always been a passionate smoker but had not abused alcohol. His mother is said to have been for some time paralyzed, following a fright.
He had been in the postal service since 1903. He was of average physical and mental development and hadn’t had any previous illnesses. He served in the military from 1909 to 1911. He had always been a heavy smoker but didn't drink excessively. His mother was reportedly paralyzed for a while after a shocking experience.
Physically, the patient was a slender but strongly-built and fairly well-nourished soldier. The first sound at the apex of the heart was rough and impure, and the heart was somewhat enlarged to the left. The pulse was irregular, 106. The arteries were somewhat stiff. Neurologically, there was a marked dermatographia of comparatively long duration. The periosteal reflexes were increased; the deep reflexes could not be properly examined. The whole leg trembled and heaved unsuccessfully on attempts to raise it voluntarily. After even a slight stroke on the patellar tendon, the trembling became excessive and irregular, and[449] the leg passed into a heaving spasm which would outlast the percussion for some time. The patellar clonus could be obtained with the knee extended. The shaking movements were somewhat more marked on the right than on the left side. Similar phenomena occurred when the Achilles reflexes were being examined. The triceps reflexes on both sides were increased but there was no tremor or spasm of the arms. The plantar reflexes were very lively, and following these reflexes appeared tremors of the legs. When the spinous processes of the vertebral column were percussed, a general shaking spasm appeared. Tactile sense was everywhere normal, but the pain sense was increased. Upon slight pin-pricks in the skin of the legs, there would occur a marked shaking spasm of the leg, passing directly to the other leg. These phenomena were more marked on the right side than on the left. When sitting upon a chair with back supported, a slight tremor would appear when the hands were raised and stretched out, more markedly on the right side than on the left. Movements of the arms were normal. However, the hand-grasps were: right, 105; left, 80. In dorsal decubitus the movements of the leg were performed comparatively well at first, but after a few repetitions, the shaking spasm would occur on both sides, and the movements would become very awkward. The heel-to-knee test would then fail. If the patient were put on his feet, he would immediately fall into spasms, first in the right leg, then in the left. The trunk would now be involved, and soon the arms, whereupon the whole body, with the exception of the head, would be seen trembling and shaking, and the patient would fall forward, trying to get support by leaning against a wall, seizing a chair, or sinking down slowly. The spasms disappeared at once in dorsal decubitus and in sitting with supported back. Outward irritation by the acoustic, optic or tactile avenues would bring out spasms in the legs, always more markedly on the right side than on the left. Psychic irritations would cause spasms. The muscles of the limbs were held in great tension, the flexors and extensors being alternately affected. When the patient was moving along a wall with a difficult, swaying gait, his efforts[450] reminded the examiner of the attempts of a heavily intoxicated man to walk. Upon attempts to create passive movements of the lower limbs, severe shaking and trembling movements set in, followed by a general spastic tension of the leg musculature such that it could not be further flexed or extended.
Physically, the patient was a slim but strong and fairly well-fed soldier. The first sound from the apex of the heart was rough and unclear, and the heart was somewhat enlarged to the left. The pulse was irregular, at 106 beats per minute. The arteries felt somewhat stiff. Neurologically, there was significant dermatographia that lasted a relatively long time. The periosteal reflexes were heightened; the deep reflexes couldn’t be properly assessed. The entire leg trembled and jerked unsuccessfully when he tried to lift it voluntarily. Even a light tap on the patellar tendon caused excessive and irregular trembling, and the leg went into a spasm that lasted well beyond the percussion. Patellar clonus could be induced with the knee extended. The shaking was more noticeable on the right side than on the left. Similar reactions occurred during the examination of the Achilles reflexes. The triceps reflexes on both sides were heightened, but there was no tremor or spasm in the arms. The plantar reflexes were very active, and following these reflexes, tremors in the legs appeared. When the spinous processes of the vertebral column were tapped, a general shaking spasm emerged. Tactile sensation was normal throughout, but pain sensation was heightened. With slight pinpricks on the skin of the legs, a pronounced shaking spasm of the leg occurred, which then transferred to the other leg. These reactions were more pronounced on the right side than on the left. While sitting in a chair with back support, a slight tremor appeared when the hands were raised and stretched out, more noticeably on the right side than on the left. Arm movements were normal. However, the hand grips measured: right, 105; left, 80. While lying on his back, he could move his legs relatively well at first, but after a few repetitions, shaking spasms would occur on both sides, making the movements very clumsy. The heel-to-knee test would then fail. If the patient stood up, he would immediately experience spasms, first in the right leg, then in the left. The trunk would become involved, followed by the arms, causing the entire body, except for the head, to tremble and shake. The patient would then fall forward, trying to find support by leaning against a wall, grabbing a chair, or slowly sinking down. The spasms would immediately stop when lying on his back or sitting with support. External stimuli through sound, sight, or touch would trigger spasms in the legs, always more noticeably on the right side than on the left. Psychological stimuli would also cause spasms. The muscles in the limbs were under significant tension, with the flexors and extensors being affected alternately. As the patient moved along a wall with a difficult, swaying gait, his efforts resembled those of a heavily intoxicated person trying to walk. When attempts were made to create passive movements of the lower limbs, severe shaking and trembling occurred, followed by a general spastic tension in the leg muscles that prevented further flexion or extension.
The patient was put in the psychiatric section, as too seriously ill for the nerve hospital. He improved after a few days, being then able to walk without much support although still with some shaking and tremor. If his attention was diverted, passive movement of the leg could be carried out without developing spasm. He was treated in a room by himself with removal of all outward irritation. His legs were treated for an hour, three times daily, by means of moist packs. On account of complaints of insomnia he was given small doses of hypnotics.
The patient was placed in the psychiatric section, as he was too seriously ill for the nerve hospital. He improved after a few days, and was then able to walk with minimal support, although he still experienced some shaking and tremors. If his attention was diverted, his leg could be moved passively without causing spasms. He was treated in a private room, free from any external distractions. His legs were treated for an hour, three times a day, using moist packs. Due to complaints of insomnia, he was prescribed small doses of sleeping pills.
The main thing here, according to Binswanger, is the psychotherapy. The patient was told almost daily in the course of conversation, first, that the illness was being cured; secondly, that upon recovery he would be employed in the future only on the postal service. He was told that he would have to avoid marked physical exertion, of course, but that he still would be fit for office work and could serve the fatherland in this way. Still he could not be transferred back to the hospital, he was told, unless he became entirely well, so that he could move with perfect freedom.
The key point here, according to Binswanger, is the psychotherapy. The patient was told almost daily during their conversations that, first, the illness was being treated; and second, that upon recovery, he would only work in the postal service in the future. He was advised to avoid heavy physical activity, but that he would still be capable of office work and could contribute to the country in this way. However, he was informed that he couldn’t be sent back to the hospital unless he was completely well, allowing him to move around freely.
February 23 the patient was performing daily exercises in walking and standing; the spasm became very slight on standing, and often would entirely cease, but it remained still plainly present in the legs; the trunk and arms were free. External irritations were now less prone to excite spasm. Sleep became quiet and dreamless. He was transferred to the nerve hospital, able to move about freely in house and garden and only tremulous after long walks and considerable bodily and mental fatigue. He was given a week’s furlough home. He wished very much to get into the postal service; at the time of the report he had not attained this goal. He had renewed attacks of trembling upon exertion, and was transferred at the end of June to a convalescent home.
February 23, the patient was doing daily exercises for walking and standing; the spasm was very slight when standing and often would completely stop, but it was still noticeable in the legs; the trunk and arms were unaffected. External stimuli were now less likely to trigger spasms. Sleep became calm and dreamless. He was moved to the nerve hospital, where he could move around freely in the house and garden, only feeling shaky after long walks and significant physical and mental fatigue. He was given a week's leave to go home. He really wanted to get a job in the postal service; at the time of the report, he hadn't achieved this goal. He experienced renewed trembling in response to exertion and was transferred to a convalescent home at the end of June.
Shell-shock; emotion: Hyperkinesis, fear, dreams.
Shell shock; emotions: hyperactivity, fear, nightmares.
Case 328. (Mott, January, 1916.)
A private, 21, was with 30 men carrying sandbags in the daylight, under shell fire. He was thrown into a deep hole by an explosion, climbed out, and saw all his mates dead.
A private, 21, was with 30 men carrying sandbags in the daylight, under shell fire. He was thrown into a deep hole by an explosion, climbed out, and saw all his friends dead.
He was admitted to the Fourth London General Hospital, June 20, 1915, having been at Boulogne for a fortnight. He was lying in bed on his back, making continuous jerky lateral movements of head, and movements of arms, especially of the left arm. He was groaning slightly, now and then raising his eyelids with a staring expression of bewilderment and terror. He was able to mutter answers to questions. He would occasionally raise his right hand to his forehead. If he was observed, these movements became exaggerated. They ceased in sleep. He muttered even when unobserved. He continually said, “You won’t let me back.” Asked as to dreams, he replied, “Guns.” Voluntary movements were made, which prevented obtaining reflexes. When his pupils were to be examined by a man in uniform, he showed a marked facies of terror; his pupils were dilated; the eyes opened wide, the brows were furrowed, and there was an anxious scowl. The flash of an electric light produced the same effect.
He was admitted to the Fourth London General Hospital on June 20, 1915, after spending two weeks in Boulogne. He was lying on his back in bed, making continuous, jerky side-to-side movements with his head and moving his arms, especially his left arm. He was groaning softly, occasionally lifting his eyelids with a blank look of confusion and fear. He could mumble answers to questions and would sometimes raise his right hand to his forehead. If he was being watched, these movements became more exaggerated. They stopped when he fell asleep. He would mumble even when he thought no one was watching. He kept saying, “You won’t let me back.” When asked about his dreams, he replied, “Guns.” He made voluntary movements that made it hard to check his reflexes. When a man in uniform came to examine his pupils, he showed a clear expression of terror; his pupils were dilated, his eyes were wide open, his brows were furrowed, and he had an anxious frown. The flash from a flashlight had the same effect.
June 24 the patient was much better. He said the explosion which had killed his friends after he had been only a few weeks at the front, was the first serious event in his service. He kept seeing it again, with bright lights and bursting shells. Sometimes he would hear the men shouting. In dreams he both saw and heard shells and men. There was pain in the back and right side of the head.
June 24, the patient was feeling much better. He said the explosion that had killed his friends just a few weeks after he arrived at the front was the first major event in his service. He kept replaying it in his mind, with bright lights and exploding shells. Sometimes he would hear the men shouting. In his dreams, he could both see and hear the shells and men. There was pain in the back and right side of his head.
June 26 he was improved but still had pain in the back of the head, especially when trying to remember, and a slight tremor of the hands. He had been given hot baths at Boulogne on account of being very cold and shivering. He had always felt sick at the sight of blood. He was boarded for Home Service six months after admission.
June 26, he was feeling better but still had pain at the back of his head, especially when trying to remember, and a slight tremor in his hands. He had been given hot baths in Boulogne because he was very cold and shivering. He had always felt nauseous at the sight of blood. He was assigned to Home Service six months after he was admitted.
Shell fire and barbed-wire work: Tremors, anesthesias, temperature and pain hallucinations.
Shell fire and barbed wire: Shocks, numbness, temperature changes, and painful hallucinations.
Case 329. (Myers, March, 1916.)
A corporal, 39, had been working under shell fire at barbed-wire entanglements. The man was big and robust, but much depressed, complaining of noises in the head, pricking pains, unsteady legs, fatigue, irritability, loss of confidence. He showed tremors of arms and legs on movement, and stood unsteadily with eyes closed. He said: “My legs have been very unsteady, especially when some one is looking at me. They must have thought me drunk at times.”
A corporal, 39, had been working under shell fire at barbed-wire entanglements. He was big and strong, but really down, saying he heard noises in his head, felt sharp pains, had shaky legs, was tired, irritable, and had lost confidence. He showed tremors in his arms and legs when he moved, and he stood unsteadily with his eyes closed. He said, “My legs have been really shaky, especially when someone is looking at me. They must have thought I was drunk at times.”
The head and tongue were tremulous, the knee-jerks exaggerated, the soles insensitive to touch and pain; but sensibility to deep pressure was retained. There was a gradual return of right answers on further trials, aided by comparison with effects of stimuli applied to the dorsum of the foot. Though he gave correct replies on heat and cold tests over the arms, he gave wrong answers over the dorsum of the feet, less often over legs, sometimes over thighs.
The head and tongue were shaky, the knee-jerk reactions were exaggerated, and the soles were numb to touch and pain; however, sensitivity to deep pressure was still present. There was a gradual improvement in correct responses on further trials, helped by comparing the effects of stimuli applied to the top of the foot. While he answered correctly in heat and cold tests on his arms, he gave incorrect answers on the tops of his feet, less frequently on his legs, and occasionally on his thighs.
Later during examination, the feet became tremulous. He felt a “silly childish fear,” and his hands began to feel cold and clammy; whereupon he began to reply hot or cold when the tubes were not applied at all (temperature hallucinations). There were apparently pain hallucinations in the soles and errors in response to the compasses.
Later during the examination, his feet started to shake. He felt a “silly childish fear,” and his hands became cold and clammy; as a result, he began to respond with hot or cold even when the tubes weren't applied at all (temperature hallucinations). There were also apparently pain hallucinations in the soles of his feet and mistakes in response to the compasses.
Re the temperature hallucinations noted by Myers, these are to be distinguished from true vasomotor disorders. Babinski believes that he has definitely established that, though hysteria may cause a slight thermo-asymmetry, yet never a definite vasomotor or thermic disorder.
Regarding the temperature hallucinations mentioned by Myers, these should be distinguished from actual vasomotor disorders. Babinski believes he has clearly shown that, while hysteria may lead to a slight temperature imbalance, it never causes a definite vasomotor or thermal disorder.
Re hysterical pains, the most frequent are probably those of hysterical pseudo sciatica, in which true signs of sciatica are absent, namely, (1) loss of Achilles jerk, (2) scoliosis, (3) Lasègue’s sign (pain on thigh flexion with leg extension), (4) Neri’s sign (with trunk bent forward, affected knee flexed), and (5) Bonnet’s sign (pain on thigh adduction).
Re hysterical pains, the most common are probably those of hysterical pseudo sciatica, where true signs of sciatica are missing, specifically, (1) loss of Achilles reflex, (2) scoliosis, (3) Lasègue’s sign (pain when flexing the thigh while extending the leg), (4) Neri’s sign (with the trunk bent forward, the affected knee is flexed), and (5) Bonnet’s sign (pain during thigh adduction).
Shell-shock: Emotional crises; twice recurrent mutism; amnesia. A comrade in the same explosion gets off with transient phenomena.
Shell shock: Emotional crises; recurring mutism; amnesia. A comrade in the same explosion only experiences temporary issues.
Case 330. (Mairet, Piéron, and Bouzansky, June, 1915.)
December 15, sitting back of a wall were three minor officers and an homme de liaison, when a 105 shell punctured the wall and burst, killing one and wounding another severely. One of these, a sous-lieutenant, lost consciousness for a quarter of an hour and had some severe headaches for a few days, but nothing more. The other, the homme de liaison, was found standing, bewildered, looking at the dead. When his name was called, he jumped and started off, weeping and crying out.
December 15, three junior officers and a liaison officer were sitting behind a wall when a 105 shell hit the wall and exploded, killing one and seriously wounding another. One of them, a second lieutenant, passed out for about fifteen minutes and had some intense headaches for a few days, but that was it. The other, the liaison officer, was found standing there, stunned, staring at the dead. When someone called his name, he jumped up and started running, crying and shouting.
When caught, he was still somewhat clear, recognized his superior officer, answered yes and no, but kept asking, “Where is the other?” Next day he kept weeping and said not a word.
When he was caught, he was still somewhat coherent, recognized his superior officer, responded with yes and no, but kept asking, “Where is the other?” The next day, he kept crying and didn’t say a word.
He was evacuated through a series of hospitals and was sent to convalesce with his sister at Montpellier, having now got back his speech. He had a seizure of fear in the street and was picked up by the police and was carried to a general hospital January 21. Here he could not speak, could hardly write, being unable to find his words. He walked slowly, bent over, eyes abnormally wide open, with a look of terror. The lighting of a match made him start off weeping. The symptom picture included tinnitus, vertigo, deafness, some reduction of the visual field (especially on the left side), hypesthesia and hypalgesia on the left side, hyperalgesia on the right, painful points (epigastric, inguinal, supra and infra mammary left), reflex, muscular and tendon, hyperexcitability on right side, jactitation, impairment of recollective memory, complete memory gap for the accident and everything thereafter, retentive memory reduced, imagination impaired, nightmares (awaking with a start).
He was moved through a series of hospitals and went to recover with his sister in Montpellier, having regained his ability to speak. He experienced a sudden panic attack in the street and was picked up by the police, then taken to a general hospital on January 21. There, he couldn't speak and could barely write, struggling to find the right words. He walked slowly, hunched over, with his eyes wide open and a terrified expression. The sound of a match being struck made him burst into tears. His symptoms included ringing in the ears, dizziness, hearing loss, some vision loss (especially on the left side), reduced sensitivity and pain response on the left side, heightened sensitivity to pain on the right, and painful areas (in the stomach, groin, and above and below the left breast). He also showed hyperactivity in reflexes, muscles, and tendons on the right side, restlessness, impaired memory recall, a complete memory loss of the accident and everything afterward, reduced short-term memory, impaired imagination, and nightmares (waking up suddenly).
A few days later he was able to pronounce his name with difficulty and to say yes and no. February 4 there was an[454] appendicular crisis, whereupon mutism became absolute again and lasted into May, despite suggestive therapy.
A few days later, he was able to say his name, although it was still hard for him, and to answer yes and no. On February 4, there was an[454] appendicitis crisis, after which he became completely mute again and remained that way until May, despite therapy suggestions.
May 10, improvement in memory for things before the accident grew better, nightmares had become less frequent, the jactitation had continued.
May 10, the improvement in memory for things prior to the accident got better, nightmares became less frequent, but the tossing and turning continued.
There was no neuropathic predisposition in this case except infantile convulsions in two sisters, followed by nervous crises in one.
There was no neuropathic tendency in this case, except for infantile seizures in two sisters, followed by nervous episodes in one.
Re appendicular crisis, which was the occasion of a relapse in mutism, see remarks under relapses under Case 292.
Re appendicular crisis, which caused a relapse in mutism, see comments under relapses under Case 292.
Re mutism, Babinski counts mutism, hysteria major, and rhythmic chorea as so characteristically hysterical that no nervous disturbance of an organic nature can resemble them. The description of hysterical mutism is due to Charcot. According to Babinski, mutism is just as curable as hysterical deafness, and perhaps more curable. Yet mutism persists unchanged for many months unless it is treated properly by some form of suggestion. “It may be almost said that a subject suffering from speech defect, who nevertheless succeeds in making other people understand by all sorts of varied and expressive gestures the circumstances of his condition, is a hysterical mute and not an aphasic.” According to Babinski, no true case of hysterical aphasia has been published since the beginning of the war; all the cases have been cases of mutism.
Re mutism, Babinski includes mutism, major hysteria, and rhythmic chorea as so characteristically hysterical that no organic nervous disturbance can resemble them. The description of hysterical mutism comes from Charcot. Babinski believes that mutism is just as treatable as hysterical deafness, and maybe even more so. However, mutism remains unchanged for many months unless it is properly addressed through some form of suggestion. “It can almost be said that a person with a speech defect, who still manages to communicate their condition through a variety of expressive gestures, is a hysterical mute and not an aphasic.” According to Babinski, there have been no true cases of hysterical aphasia published since the beginning of the war; all cases have been mutism.
Shell explosion; fainting: Hysterical crises of emotion; fright at a frog in the garden. Hereditary and acquired neuropathic taint.
Shell explosion; fainting: Hysterical emotional crises; fear of a frog in the garden. Genetic and acquired nervous disorder.
Case 331. (Claude, Dide, and Lejonne, April, 1916.)
A lieutenant, 28 (mother nervous; father had nervous spells at fifteen; patient himself nervous as a child), was under a great moral strain at the outbreak of war, and was utterly exhausted in a hard battle that lasted more than twenty-four hours.
A 28-year-old lieutenant (his mother was anxious; his father had anxiety attacks at fifteen; he himself was anxious as a kid) was under a lot of moral pressure when the war started and was completely worn out after a grueling battle that lasted over twenty-four hours.
A shell burst near him September 25 at the Somme, whereupon he fainted. He was evacuated to Amiens for three weeks; kept his bed; somnambulistic; subject to nervous crises.
A shell exploded nearby on September 25 at the Somme, and he passed out. He was taken to Amiens, where he spent three weeks in bed, sleepwalking and experiencing nervous breakdowns.
He passed to the hospital of Ferté-Bernard for a month, the crises becoming more frequent. He was sent to a convalescent dépôt for three days, thence for three months to La Plisse; got better; lived at home, but went to a show where they played the Marseillaise, was profoundly moved thereby, and had more crises; accordingly went back under medical care and finally to his dépôt, where, upon seeing his old comrades, he had more crises, and was finally evacuated to the neurological center of the Eighth Region.
He was admitted to the hospital in Ferté-Bernard for a month, with his episodes becoming more frequent. After that, he was sent to a recovery center for three days, then spent three months at La Plisse; he improved and went home, but attended a show where they played the Marseillaise. He was deeply moved by this and experienced more episodes; as a result, he returned for medical care and finally went back to the recovery center, where seeing his old friends triggered more episodes, and he was eventually transferred to the neurological center of the Eighth Region.
He there seemed mistrustful when asked to tell his story. There was a noise of cannon, whereupon he got up, ran in all directions in the garden, bumping into trees in the greatest terror, yelling, “There they are!”; gesticulating, soliloquizing: “Bomb! Shell! Bayonet!” His pulse was rapid. After he was calmed down, he began to talk again in a very clear, distinct, somewhat tremulous voice. A metallic sound made him shudder and cry out, “The drums!” and another scene of rushing about followed.
He seemed suspicious when asked to share his story. There was the sound of cannon fire, and he jumped up, running around the garden in a panic, crashing into trees, yelling, “There they are!” and waving his arms, talking to himself: “Bomb! Shell! Bayonet!” His heart was racing. Once he calmed down, he started to speak again in a very clear, distinct, slightly shaky voice. A metallic sound made him flinch and shout, “The drums!” leading to another episode of frantic running around.
In the consulting office he wept. Battle dreams and nightmares, soliloquies and terror, seminal losses, occurred during the next few days.
In the consulting office, he cried. Over the next few days, he experienced dreams and nightmares about battles, moments of self-reflection and fear, and significant losses.
August 4, while alone in the garden, he heard a noise, went toward it and spied a frog, whereupon he had another crisis[456] of fear and emotion. He got another lieutenant, and both returned, sticks in hand. Pointing to a hole in the earth, Lieutenant A. said, “Trenches! There they are!” “What? Who?” said Lieutenant B. “The Boches!” said Lieutenant A. Whereupon Lieutenant B also saw them and cried out bravely, “Go away!” However, the second lieutenant immediately saw that he had been the subject of suggestive hallucination.
August 4, while he was alone in the garden, he heard a noise, went toward it, and spotted a frog, which triggered another wave of fear and emotion. He got another lieutenant, and they both returned with sticks in hand. Pointing to a hole in the ground, Lieutenant A said, “Trenches! There they are!” “What? Who?” asked Lieutenant B. “The Germans!” replied Lieutenant A. At that, Lieutenant B also noticed them and shouted bravely, “Go away!” However, the second lieutenant quickly realized he had been imagining things.
Fifteen days of calm followed, during which the lieutenant became more sociable and grew better having no more crises.
Fifteen days of peace went by, during which the lieutenant became friendlier and felt better without any more crises.
Four other cases of “hysteroemotive nature” are reported by Claude, all of them showing a special constitutional basis before the war. In the differential diagnosis, alcoholism, cyclothymia, obsessive psychosis and occasionally systematized delusional psychosis may be considered. There were occasional stereotypical features in the cases, but of a very fugitive nature. Dementia praecox is hardly to be considered.
Four other cases of "hysteroemotive nature" are reported by Claude, all showing a unique constitutional basis before the war. In the differential diagnosis, alcoholism, cyclothymia, obsessive psychosis, and sometimes systematized delusional psychosis might be considered. There were occasional stereotypical features in the cases, but they were very fleeting. Dementia praecox is hardly a consideration.
Re “hysteroemotive” cases, Babinski holds that the claim of emotion as a single factor capable of causing hysteria by itself, is a false claim. To be sure, the patients themselves may give accounts which lead to the idea of an emotional hysteria. Dide, one of the authors of the above case, states that functional disorders occur only in subjects whose emotional tone has been relaxed. The heaviest bombardments are not in line to produce these disorders when the morale of the troops is good. The bloodiest affairs may leave no single case of nervous disorder when the morale is good. Dide found in a whole year’s work but a single functional case,—an oniric delirium, following a trench mortar explosion. Roselle and Oberthür also state on the basis of intensive experience, that large projectiles do not cause any intensive emotional reactions. Clunet’s observations upon the shipwrecked La Provence II, quoted by Babinski, run in the same direction. It will be noted that the five cases called “hysteroemotive” showed a special constitutional basis antebellum.
Re “hysteroemotive” cases, Babinski argues that the idea of emotion as the sole factor that can cause hysteria is incorrect. Sure, the patients may describe their experiences in a way that suggests emotional hysteria. Dide, one of the authors of the aforementioned case, mentions that functional disorders only arise in individuals whose emotional state has been relaxed. Significant external stresses don't typically lead to these disorders when the troops' morale is high. Even the most brutal events can result in no cases of nervous disorder when morale is good. Dide found only one functional case in an entire year’s work—an oniric delirium following a trench mortar explosion. Roselle and Oberthür also report based on extensive experience that large projectiles do not trigger intense emotional reactions. Clunet’s observations regarding the shipwrecked La Provence II, cited by Babinski, align with this view. It's worth noting that the five cases labeled “hysteroemotive” displayed a specific constitutional basis before the war.
War strain; slight wound; burials; shell-shock: Neurosis with anxiety; war dreams; apparent recovery. Relapse with depression.
War stress; minor injury; funerals; battle fatigue: Mental disorder with anxiety; nightmares about war; seeming recovery. Setback with depression.
Case 332. (MacCurdy, July, 1917.)
A man, 27 (normal mischievous boy, successful in work, unmarried, shy with women), enlisted October, 1914; adapted himself well to training; at first enjoyed his work, though later bored with routine; and in February, 1915, went to the firing line in France. The first shell-fire experience made him break into a cold sweat with fear and slowed him down for a time. However, he enjoyed the active operations until, after eight months in the trenches, he was invalided home with nephritis. After four months’ convalescence he was recommended for a commission, obtained after two months’ training. After two further months in the regimental dépôt, he went back to France as lieutenant in June, 1916, plunging into four months of heavy fighting on the Somme, in which he was wounded slightly once and was one day buried three times by earth from shell explosion. The last time he was buried he was unconscious for ten minutes and was relieved for three days. He got frequently knocked out for short periods by shell concussion.
A 27-year-old man (a typical mischievous guy, successful at work, unmarried, and shy around women) enlisted in October 1914. He adapted well to training; initially enjoyed his job, but later got bored with the routine. In February 1915, he went to the front line in France. His first experience with shell fire made him break out in a cold sweat from fear and slowed him down for a bit. However, he enjoyed the active operations until, after eight months in the trenches, he was sent home due to nephritis. After four months of recovery, he was recommended for a commission, which he received after two months of training. After another two months in the regimental depot, he returned to France as a lieutenant in June 1916, diving into four months of intense fighting on the Somme, where he was slightly wounded once and buried three times in one day by earth from a shell explosion. The last time he was buried, he was unconscious for ten minutes and took three days to recover. He frequently got knocked out for short periods due to shell concussion.
At the end of October, 1916, he was sent to the Ypres section, where he worked with a pioneer battalion that buried many dead. After a month of this pioneer work he became mildly depressed; fatigue set in, and now for the first time he began to jump nervously when the shells came over. To counteract this nervousness he began to drink and in a fortnight developed insomnia. The Somme front scenes kept constantly in mind as he tried to sleep. He felt as if he had to go up to the trenches next day and that he did not want to go. There were hypnagogic hallucinations of trenches and shells, recognized as imaginary and productive of no fear. Week by week he became more nervous, became unable to locate shell falls, and felt as if they were all coming at him. Early in 1917 he[458] had taken heavily to drink and grew greatly fatigued in the struggle to prevent betraying his fear to his men. The horror at bloodshed, to which he had long since become accustomed, reappeared. He actually wished that he might be killed.
At the end of October 1916, he was sent to the Ypres area, where he worked with a pioneer battalion that buried many dead. After a month of this work, he started to feel a bit depressed; fatigue set in, and for the first time, he began to jump nervously whenever the shells landed. To cope with his nerves, he started drinking, and within two weeks, he developed insomnia. The images from the Somme front haunted him as he tried to sleep. He felt as if he had to go up to the trenches the next day, and he didn’t want to. He experienced vivid hallucinations of trenches and shells, which he recognized were imaginary and didn’t scare him. Week by week, he became more anxious, struggled to pinpoint where the shells were landing, and felt like they were all aimed at him. By early 1917, he had taken to drinking heavily and was completely worn out from trying to hide his fear from his men. The horror of bloodshed, which he had long since gotten used to, returned. He found himself wishing he might be killed.
He carried on until March, when one day on a raid seven men were killed around him and he was immediately thereafter buried. He reported sick and was found to be somewhat febrile. He carried on for two more days; had to report sick again; was sent to hospital and for two or three weeks had bad headaches back of the eyes and a sleep interrupted by sudden wakings with a start. Nightmares now began for the first time. They dealt with the Somme front, merciless shelling coming nearer and nearer. Finally, he would wake with a shriek when a shell landed on top of him. In the day time any noise would be interpreted as a shell. Hypnagogic hallucinations of Germans entering the room appeared. After a little over a week in French hospitals he was transferred to London; grew better; was sent to a hospital in the country where outdoor exercise and recreation helped him.
He kept going until March, when one day during a raid, seven men were killed around him, and he was buried shortly after. He reported feeling unwell and was found to have a slight fever. He pushed through for another two days but had to report sick again. He was sent to the hospital and spent two or three weeks suffering from severe headaches behind his eyes and sleep disrupted by sudden awakenings. Nightmares started for the first time, focused on the Somme front with relentless shelling getting closer and closer. He would wake up screaming when a shell landed near him. During the day, any noise would make him think it was a shell. He experienced hypnagogic hallucinations of Germans entering the room. After just over a week in French hospitals, he was moved to London; he started to improve and was then sent to a hospital in the countryside where outdoor activities and recreation helped him recover.
Two weeks later the death of one of his best friends depressed him a good deal. He failed in an attempt to sing at a concert, and then grew much worse, with the old dreams every night and hypochondriacal complaints of sweats and loss of weight. He was convinced that he was physically and nervously a permanent wreck.
Two weeks later, the death of one of his closest friends really brought him down. He couldn't manage to sing at a concert, and then his condition worsened significantly, plagued by the same nightmares every night and constant worries about sweating and losing weight. He was convinced that he was permanently broken, both physically and emotionally.
According to MacCurdy, this case is a typical case of war neurosis of the anxiety type, except that a relapse with depression is somewhat atypical.
According to MacCurdy, this case is a typical example of war neurosis of the anxiety type, except that a relapse with depression is somewhat unusual.
Re anxiety, Lépine counts trauma as one of the most important factors. The reduction of morale in physically injured cases may at times require their rapid withdrawal to a safety zone. The delirium of the physically injured sometimes takes on a melancholic tinge. Fatigue, loss of sleep, and cold are other factors of a physical nature. Among the moral factors, Lépine thinks responsibility (for certain âmes scrupuleuses) is hardly less important than the factor of felt danger. The contacts of highly cultivated men with the rougher soldier element, may also count, as well as the[459] separation from home and friends, and the factor of despair concerning the ending of the war.
Re anxiety, Lépine identifies trauma as one of the key factors. Sometimes, the decline in morale among those with physical injuries may necessitate their quick relocation to a safe area. The delirium experienced by the physically injured can sometimes carry a melancholic tone. Fatigue, lack of sleep, and cold conditions are other physical factors. Among the psychological factors, Lépine believes that feeling responsible (for certain âmes scrupuleuses) is almost as significant as the perception of danger. The interactions between highly educated individuals and the rougher soldier crowd can also play a role, along with the[459] separation from home and friends, and the feeling of despair about the war's end.
Re sexual influences, the factor of sexual continence, though it may have some importance in producing morbid anxiety, seems to have less importance under war conditions, when self-preservation is more in the eye than the sexual life. On the whole, the pre-existent emotional constitution (Dupré) is of greater importance. A previous wound may cause a man to acquire such a constitution. Amongst physical states, hypotensives are candidates for depression; tuberculosis is particularly important.
Re sexual influences, the factor of sexual self-control, while it might play a role in creating unhealthy anxiety, appears to be less significant during wartime when self-preservation takes priority over sexual life. Overall, a person's emotional makeup (Dupré) is more crucial. A past injury can lead a person to develop that kind of emotional makeup. Among physical conditions, those with low blood pressure may be more prone to depression; tuberculosis is especially noteworthy.
Re MacCurdy’s case, the factor of alcoholism was mentioned. The importance of alcoholism, Lépine has particularly stressed. He particularly emphasizes the number of men who have taken to drink to get over their emotions and to forget. Visual hallucinations, angry excitability, sudden persecutory ideas, nocturnal occurrence of the symptoms, flushing of the face, suggest alcoholism. Some of the cases of encephalitis which are supposed to be due to some unknown bacterium, may really be alcoholic in origin. A third of Lépine’s cases were alcoholic; perhaps two-thirds really alcoholic if one took into account the factor of sensitization.
Re MacCurdy’s case, the issue of alcoholism was brought up. Lépine has particularly highlighted the significance of alcoholism. He emphasizes the number of men who have turned to drinking to cope with their emotions and to escape their problems. Symptoms like visual hallucinations, irritability, sudden feelings of persecution, nighttime symptoms, and flushed faces suggest alcoholism. Some cases of encephalitis thought to be caused by an unknown bacterium might actually be due to alcohol. About a third of Lépine’s cases were alcoholic; probably two-thirds were truly alcoholic if you consider the factor of sensitization.
Bombardment from airplanes: Fear; suicidal thoughts; oniric delirium (“moving picture in the head.”)
Bombing from planes: Fear; suicidal thoughts; dream-like delirium (“a moving picture in the head.”)
Case 333. (Hoven, May, 1917.)
A soldier (born at seven months, somewhat feebleminded, given to depression, early victim of convulsions, talking only at five years, with a history of once leaving his father’s house with suicidal ideas after being scolded, already invalided in peace times) on enlistment remained with the regiment but a few days and was then sent to a workers’ company of blacksmiths.
A soldier (born seven months early, somewhat slow, prone to depression, an early victim of seizures, who only spoke at five years old, with a history of once leaving his father's house with suicidal thoughts after being scolded, and already disabled during peacetime) enlisted but stayed with the regiment for only a few days before being assigned to a workers’ crew of blacksmiths.
Toward the end of February, 1916, his cantonment was bombarded by an airplane escadrille. The patient was much frightened, ran away and hid in a ditch, felt sick, stopped eating, wanted to kill himself and had to be evacuated to Calais and then to Chateaugiron.
Toward the end of February 1916, his camp was bombed by a squadron of airplanes. The patient was very scared, ran away, and hid in a ditch, felt ill, stopped eating, wanted to take his own life, and had to be evacuated to Calais and then to Châteaugiron.
He was there found to be well oriented, but depressed and bewildered. There was an emotional tachycardia. At night he would fall into a delirium like the oniric delirium of Régis, always dreaming of the same bombardment scene, saying it was like a moving picture in his head. The delirium affected him so that he actually tried to make away with himself.
He was found to be aware of his surroundings but feeling depressed and confused. He experienced emotional rapid heartbeats. At night, he would slip into a delirium similar to Régis's dreamlike state, always replaying the same bombing scene, saying it was like a movie in his head. The delirium overwhelmed him to the point that he actually attempted to take his own life.
The dream delirium did not last long but recurred several times on very slight emotional occasions. It was possible to excite his hallucinatory dreams experimentally by showing him battle pictures.
The dream delirium didn’t last long but happened several times during minor emotional moments. It was possible to trigger his vivid dreams by showing him battle pictures.
Some cases of such delirium develop, according to Hoven, after moving picture shows of battle scenes.
Some cases of this kind of delirium, according to Hoven, develop after watching movies of battle scenes.
Re oniric delirium, Chavigny states that mental confusion and oniric delirium are the two forms of mental disorder that come most frequently after explosions. He believes that at least 95 per cent of these cases are rapidly curable; and, in fact, found amongst 60 cases observed in his army service that only two were so severe as to require being sent to the interior: all the others were cured in six days at the outside. These cases, according to Chavigny, ought to be treated in[461] special wards at the front (bed, quiet, purgation, baths). Chavigny prearranges slight emotional shock for these cases by talking with them about their families. Their apparent apathy vanishes in a trice.
Re oniric delirium, Chavigny notes that mental confusion and oniric delirium are the two most common types of mental disorders that occur after explosions. He believes that at least 95 percent of these cases can be quickly treated; in fact, among 60 cases he observed during his military service, only two were severe enough to require transfer to the interior: all the others were cured within six days at the most. According to Chavigny, these cases should be treated in[461] dedicated wards at the front (with a bed, quiet environment, purgation, and baths). Chavigny intentionally creates a mild emotional shock for these cases by discussing their families with them. Their apparent apathy disappears in an instant.
Régis, who has named the state “oniric delirium,” states that the condition never lasts more than a fortnight, is caused by emotional shock, and occurs in all cases with mental disorder following battle; but similar hallucinatory conditions have begun to appear also amongst alcoholics, in garrison or at home. There is emotional constitution in most of these cases. There is not so much evidence of heredity. Out of 50 of Régis’ cases, 22 had been wounded, and 28 not. Régis states that the psychoses are rather more apt to affect men in the reserve, and are severest in officers. These cases should not be committed to institutions, but ought to be treated in special military psychiatric wards containing separate rooms. Very fine-spun diagnosis may be necessary now and again on account of the occurrence of infectious deliria and phenomena of the banal psychoses that may closely resemble oniric deliria.
Régis, who refers to the condition as “oniric delirium,” says that it usually doesn’t last more than two weeks, is triggered by emotional shock, and occurs in all cases of mental disorder following battle. However, similar hallucinatory conditions have also started to show up among alcoholics, whether in the military or at home. Most of these cases involve emotional backgrounds. There’s not a lot of evidence for heredity. Out of Régis’ 50 cases, 22 had been wounded and 28 had not. Régis mentions that these psychoses tend to affect reserve soldiers more frequently and are the most severe in officers. These cases shouldn’t be sent to institutions but should be treated in specialized military psychiatric wards with private rooms. Occasionally, a very detailed diagnosis may be necessary due to the presence of infectious deliria and symptoms of ordinary psychoses that can closely mimic oniric deliria.
Shell-shock; emotion (best friend mangled): Stupor with amnesia.
Shell shock; emotion (best friend destroyed): Numbness with memory loss.
Case 334. (Gaupp, March, 1915.)
A soldier, 23 (in civil life a turner, of Polish descent, and of a somewhat nervous and easily excitable disposition), early in August went from Strassburg into the Vosges and Lorraine. August 26 a number of shells exploded near him. The troop was excited and took refuge in a cellar. His best friend was torn to pieces by a shell. When the body was removed, the man felt sick and lost consciousness. He arrived at the clinic in Tübingen in a stuporous condition, by hospital train, August 31, 1914. He walked weakly to his bed, supported by two men, and lay in the bed, apathetic and reacting to questions only with a stare. Things put in his mouth were swallowed. He remained motionless.
A 23-year-old soldier (a turner in civilian life, of Polish descent, and with a somewhat nervous and easily excitable nature) left Strassburg for the Vosges and Lorraine in early August. On August 26, several shells exploded nearby. The troop became frantic and took shelter in a cellar. His closest friend was killed by a shell. When the body was taken away, he felt nauseous and lost consciousness. He arrived at the clinic in Tübingen in a dazed state via hospital train on August 31, 1914. He walked weakly to his bed, supported by two men, and lay down, apathetic and only responding to questions with a vacant stare. Things placed in his mouth were swallowed. He remained completely still.
Next evening he answered a low Yes to a nurse’s question about eating. A little afterwards, he said he supposed he was a prisoner in the enemy’s country. A while later he got properly oriented but still did not know how he had come. September 2, however, he was much clearer and said he had awakened out of a long dream. There was a complete amnesia, however, from the moment when he went to help remove the torn body of his friend up to September 1. Memories became clearer for the period before the shell explosion. The patient became very lively, talking vividly of war experiences, imitating the hiss of shells with an expression of intense anxiety, getting accustomed to the battle scenes, saying that he was now seeing everything again as if real. He remained anxious for some days, complaining of weight on his chest and of feelings of inner restlessness and tension.
The next evening, he answered a soft Yes to a nurse’s question about eating. A little later, he mentioned that he figured he was a prisoner in enemy territory. After some time, he got his bearings but still had no idea how he had arrived there. By September 2, though, he was much more clear-headed and said he had woken up from a long dream. However, there was total amnesia from the moment he went to help remove the mangled body of his friend until September 1. His memories were clearer for the time before the shell explosion. The patient became very animated, talking vividly about war experiences, mimicking the hissing of shells with a look of intense anxiety, getting used to the battle scenes, and saying that he was now seeing everything again as if it were real. He remained anxious for a few days, complaining of a heavy feeling on his chest and experiencing a sense of inner restlessness and tension.
Amnesia for the period August 26 to September 1 remained; all that he could say was that he had been thrown sidewise for some distance by the air pressure of the shell.
Amnesia for the period from August 26 to September 1 stayed; all he could say was that he had been pushed sideways for some distance by the blast from the shell.
From September 6 onwards, he grew calmer but he was still very labile, given to lively imaginings and emotion. By mid September he could be discharged for garrison duty.
From September 6 onwards, he became calmer, but he was still very unstable, prone to vivid thoughts and emotions. By mid-September, he could be released for garrison duty.
Emotional shock; shooting a comrade: Horror, sweat, stammer, recurrent nightmare. Improvement on “tracing back.” Brief recrudescence on death of child.
Emotional shock; shooting a fellow soldier: Horror, sweat, stuttering, recurring nightmares. Progress on “tracing back.” Brief resurgence upon the death of a child.
Case 335. (Rows, April, 1916.)
A man after a charge was placed on outpost duty. It was dark, and he was in a state of considerable tension. He heard a noise which he thought came from somewhere in front of him. Suddenly the space around him was illuminated by a flare of light, and he saw a man crawling over the bank. Without challenging, he fired and killed the man. Next morning, he found to his horror that he had killed a wounded Englishman, who had advanced beyond his comrades and was crawling back.
A man was assigned to guard duty after a mission. It was dark, and he felt very tense. He heard a noise that he thought was coming from somewhere in front of him. Suddenly, the area around him lit up with a flare, and he saw a man crawling over the bank. Without questioning, he shot and killed the man. The next morning, he was horrified to discover that he had killed a wounded Englishman, who had moved ahead of his comrades and was trying to crawl back.
A physical expression of horror, together with an intense sweating and a very marked stammer, persisted for months. At the same time, he was tormented with a fearful nightmare, and in his sleep he was heard to say, “It was an accidental shot, sir; yes, Major, it was not my fault.” In the day time, also, his attention was concentrated on the memory of the incident, so that “I cannot forget it no matter how I skylark.” Carrying his story back to this trying time led to his recounting his terrible secret, and a marked improvement followed. The physical signs of the intense emotion gradually disappeared. The vividness of the dreams diminished, and his attention was less concentrated on the one subject. It is interesting to note that the production of a marked emotional state by the death of one of his children led to a recrudescence of his former symptoms: an expression of “horror and the stammer.” But they disappeared again in a short time.
A physical reaction of horror, along with intense sweating and a noticeable stutter, lasted for months. At the same time, he was plagued by a terrifying nightmare, and in his sleep, he could be heard saying, “It was an accidental shot, sir; yes, Major, it wasn’t my fault.” During the day, his focus was also on the memory of the incident, to the point where he said, “I can’t forget it no matter how much I try to have fun.” Reflecting on this difficult time led him to share his terrible secret, and he saw a significant improvement afterward. The physical signs of his intense emotions gradually faded. The intensity of his dreams lessened, and he became less fixated on that one topic. It’s worth noting that when he experienced a strong emotional state due to the death of one of his children, his previous symptoms—an expression of “horror and the stutter”—returned, but they disappeared again shortly after.
Emotional shock: Phobias.
Emotional shock: Fears.
Case 336. (Bennati, October, 1916.)
An Italian corporal in the infantry, a robust man of a well-to-do family, took a good deal of pleasure in the war life. One day a comrade was injured by a missile of some sort, and died almost immediately. This comrade, after being hurt, had thrown himself against the corporal, who was asleep at the time. He woke up sharply and immediately felt sick. His status was one of great terror, lacrimation, lack of spontaneity, and insomnia. He would wake up from sleep and start from a terrible dream. He had a number of phobias and was especially interested in other persons who had the same sort of mental state as himself. He was in a state noted by Bennati as one of “emotional anaphylaxis” to various events around him. There was a horizontal nystagmus, the Mannkopf sign was positive (87-72), Thomayer 90-114, Erben 114-90. There was a slight tendency to dizziness when the Erben movements were made.
An Italian corporal in the infantry, a strong man from a well-off family, found a lot of enjoyment in military life. One day, a fellow soldier was hit by some kind of missile and died almost instantly. This soldier, after being injured, had thrown himself against the corporal, who was asleep at that moment. He woke up suddenly and immediately felt nauseous. His condition was marked by intense fear, crying, lack of spontaneity, and insomnia. He would wake up from sleep in a panic due to terrifying dreams. He had several phobias and was particularly interested in others who shared his mental struggles. He was in a state noted by Bennati as one of “emotional anaphylaxis” in response to various events around him. There was a horizontal nystagmus, the Mannkopf sign was positive (87-72), Thomayer 90-114, Erben 114-90. He showed a slight tendency to dizziness when the Erben movements were performed.
Shell-shock; fright: loss of consciousness next day: Generalized tremors; “somebody above with a mallet.”
Shell shock; fear: loss of consciousness the next day: General tremors; “someone above with a mallet.”
Case 337. (Wiltshire, June, 1916.)
A sapper of 19, with a nervous mother, had had an attack two years before his war neurosis, of a somewhat similar nature. This former attack had been caused by overwork; there had been no accident or fright, but the man had been unable to work for five months.
A 19-year-old sapper, who had a nervous mother, had a similar breakdown two years before his war-related trauma. This earlier episode was caused by overwork; there was no accident or shock, but he had been unable to work for five months.
At the front, he had been well up to ten days before observation. In a dugout a shell had pitched on top of the bank, followed by another shell bursting in front. There was a slight falling in of the dugout but no special damage.
At the front, he had been doing fine up until ten days before the observation. A shell had landed on top of the bank in a dugout, followed by another shell exploding in front of it. The dugout showed a minor collapse but no significant damage.
The patient carried on that night but reported sick next morning, feeling queer and shaking slightly above the waist. He remembered getting half-way down the road to see the M. O., but nothing more until he came to in the dressing station (perhaps 2½ hours later). After two days in hospital, he was transferred to a convalescent camp, and then admitted to another hospital. He complained of twitching and slight frontal headache; funny feelings at night prevented his going to sleep. Thus: “A man was over my head with a mallet, going to hit me.” There was a dream of “somebody above me all the time.” Both arms, head, and tongue were in a state of constant tremor, and there were jerky movements of the legs. There was some spasm of the right leg. Both legs went into violent tremor on examination, and during examination there was free perspiration.
The patient managed through that night but called in sick the next morning, feeling strange and shaking slightly from the waist up. He remembered making it halfway down the road to see the medical officer but nothing after that until he regained consciousness at the dressing station (maybe 2½ hours later). After two days in the hospital, he was moved to a recovery camp and then admitted to another hospital. He complained of twitching and a slight headache at the front of his head; weird sensations at night kept him from falling asleep. He said, “A man was over my head with a mallet, about to hit me.” He had a recurring dream of “somebody above me all the time.” Both arms, his head, and his tongue were always trembling, and his legs were making jerky movements. There was some spasm in his right leg. Both legs shook violently during the exam, and he was sweating freely while being examined.
Re tremors, all sorts of tremors of unknown nature are apt to get the designation hysterical. Meige believes that the Shell-shock tremors, which are apt to be very persistent, are very possibly due to changes in the nervous system. Ballet has noted how the tremors, as in the above case, are often associated with expressions of fear. Now and then there is an obsessive disorder dubbed tremophobia by Meige, which produces a vicious circle. Tremors lead to obsessions,[466] and the obsessions in turn exaggerate the tremors. These Shell-shock tremors are apparently not related to (though they may need differential diagnosis from) such conditions as paralysis agitans, multiple sclerosis, hyperthyroidism, cerebellar disease, neurosyphilis, and alcoholic or other intoxication.
Re tremors, various types of tremors of uncertain origin are often labeled as hysterical. Meige suggests that the Shell-shock tremors, which tend to be quite persistent, are likely caused by changes in the nervous system. Ballet has observed that the tremors, as mentioned above, are frequently linked with signs of fear. Occasionally, there is an obsessive condition referred to as tremophobia by Meige, which creates a harmful cycle. Tremors lead to obsessions, [466] and these obsessions, in turn, worsen the tremors. These Shell-shock tremors seem to be unrelated to (although they may require differential diagnosis from) conditions such as Parkinson's disease, multiple sclerosis, hyperthyroidism, cerebellar disease, neurosyphilis, and intoxication from alcohol or other substances.
Roussy and Lhermitte distinguish the tremors into (a) atypical ones; that is, disorderly, irregular movements seemingly determined by the subject’s caprice; and (b) typical tremors, such as those found in the well-known nervous diseases and presumably imitated in hysteria from these well-known diseases. Generalized atypical tremors are, as a rule, combined with a variety of other Shell-shock symptoms, and often exhibit a sort of mimicry of fear.
Roussy and Lhermitte categorize tremors into (a) atypical ones, which are disordered and irregular movements that seem to be influenced by the individual's whims, and (b) typical tremors, like those seen in well-known nervous disorders that are likely mimicked in hysteria from these common conditions. Generally, atypical tremors are accompanied by a range of other shell shock symptoms and often show a kind of mimicry of fear.
Shell-shock; burial-work: Amnesia. Shell whistling conditions idea of something nasty.
Shell shock; burial work: Amnesia. The sound of shells whistling creates an idea of something terrible.
Case 338. (Wiltshire, June, 1916.)
A private, 19, in the R. A. M. C., was sent in with a field ambulance note as follows:
A private, 19, in the R. A. M. C., was sent in with a field ambulance note saying:
“Private —— was close to a shell which burst among a company standing in the road, killing 20 and wounding 20 others. He worked well in assisting the wounded, and then proceeded to clear up the fragments of the killed. Whilst doing this, he suddenly lost his mental balance and has been in his present state nearly 24 hours. He has been given bromides.”
“Private —— was near a shell that exploded among a group standing on the road, killing 20 and injuring 20 more. He performed admirably in helping the wounded, and then went on to clear the remains of the dead. While doing this, he suddenly lost his mental stability and has been in his current state for almost 24 hours. He has been given bromides.”
An M. O. attached to the same ambulance wrote: “This man is suffering from mental shock caused by having to clear away the remains of a number of men killed by a shell. He does not recognize his friends, and at frequent intervals has periods of terror, exclaiming, ‘Cover it up.’ He is sleepless (without drugs); he takes food badly. He is possibly suicidal or may become so.”
An M.O. attached to the same ambulance wrote: “This man is experiencing mental shock from having to clean up the remains of several men killed by a shell. He doesn't recognize his friends and frequently has episodes of panic, shouting, ‘Cover it up.’ He can't sleep (without drugs) and has a poor appetite. He may be suicidal or might become so.”
According to the patient himself, he had been quite well for four months at the front. He was on the La Bassée Road with the troops after a day or two of heavy work under shell fire. “And I remember the flash of some shot and a shell burst I think, and I can’t remember anything more. I awoke in the morning, in the train” (48 hours later). “I can only remember men calling out.” He complained of a feeling in the head, as if expecting something. “Something seems to be coming,—as if something was going to happen,—something nasty, whenever I hear anything like the whistling of a shell coming towards me.” This patient was without tremor and was physically normal. So far as the patient’s own story went, the case might well be regarded as one due to physical concussion, but the notes of the medical officers give evidence of a psychic element.
According to the patient, he had been feeling pretty good for four months at the front. He was on the La Bassée Road with the troops after a day or two of heavy work under shell fire. “And I remember seeing a flash from some shot and a shell bursting, I think, and then I can’t remember anything more. I woke up in the morning, on the train” (48 hours later). “The only thing I remember is men calling out.” He described a sensation in his head, like he was waiting for something. “It feels like something is coming—as if something is about to happen—something bad, whenever I hear anything like the whistling of a shell coming at me.” This patient showed no tremors and was physically normal. Based on the patient's account, the case could easily be seen as due to physical concussion, but the notes from the medical officers indicate a psychological aspect.
Depression with suicidal thoughts after witnessing death of comrade.
Depression with suicidal thoughts after seeing a friend die.
Case 339. (Steiner, October, 1915.)
A farmer, 52, volunteered and was put in charge of a drinking-water still. He had never been ill nor was there any nervous or mental disease in his family. From the end of August he was frequently under shell fire, but the only effect thereof was a somewhat poorer sleep than normal.
A 52-year-old farmer volunteered and was assigned to run a drinking-water still. He had never been sick, and there were no nervous or mental illnesses in his family. Since the end of August, he was often exposed to shelling, but the only impact was that he had slightly worse sleep than usual.
December 14, 1914, a young comrade, a volunteer, wanted to clean his dirty kettle at the drinking-water still. The farmer later described this volunteer as a young fellow “like milk and blood” (as we might say, “like peaches and cream”) and as the handsomest young man he had ever seen in the war. The rules forbade such use of the still, and young “milk-and-blood” was told to go down to the brook, and then come back and get the distilled water. The young man complied, but while at the brook he was shot and killed in full sight of the farmer.
December 14, 1914, a young comrade, a volunteer, wanted to clean his dirty kettle at the drinking-water still. The farmer later described this volunteer as a young guy “like milk and blood” (which we might say, “like peaches and cream”) and as the most attractive young man he had ever seen in the war. The rules prohibited using the still for that purpose, so the young “milk-and-blood” was told to go down to the brook and then come back for the distilled water. The young man agreed, but while he was at the brook, he was shot and killed right in front of the farmer.
The farmer grew much excited and trembled all over. Thereafter he could not eat or sleep; he reproached himself, although he knew he had acted quite correctly; wished he had been in the place of this comrade; and had suicidal thoughts. He was deeply depressed, wept easily, and showed manual tremor. Steiner terms the farmer’s account of the person of the deceased “reactive idealization.” After a week there was considerable improvement. B. was sent back to work, which he felt would be beneficial. He was put in less dangerous surroundings, and this also had a good effect.
The farmer became very excited and trembled all over. After that, he couldn’t eat or sleep; he blamed himself, even though he knew he had acted properly. He wished he could have been in his comrade’s place and had thoughts of ending his own life. He was deeply depressed, cried easily, and showed signs of trembling. Steiner refers to the farmer’s view of the deceased as “reactive idealization.” After a week, there was significant improvement. B. was sent back to work, which he believed would help. He was placed in less dangerous environments, and this also had a positive effect.
Marching and battles: Neurasthenia?
Marching and battles: Neurasthenia?
Case 340. (Bonhoeffer, January, 1915.)
A subaltern had been treated before the war for nervousness, dizziness, and “mattigkeit” (convulsions in infancy), but proved himself a good soldier, having gotten his rank after the first period of practice.
A subaltern had been treated before the war for anxiety, dizziness, and “mattigkeit” (convulsions in infancy), but he proved to be a good soldier, earning his rank after the initial training period.
He was in three battles in Belgium, but on the march one day suddenly had a spell of weakness and is said to have had convulsions. There was, however, no biting of the tongue, and no enuresis. After a week in the field hospital, he was sent back to Berlin where he had some somatic feelings of anxiety without subjective disturbance or any disorders of consciousness except a certain amount of inhibition; he was sleepless and hypersensitive, cried easily, and was apprehensive on being touched; he winked violently on examination of his eyes, and while being tested for reflexes made violent contractions of a semi-voluntary nature.
He fought in three battles in Belgium, but one day during the march, he suddenly felt weak and reportedly had convulsions. However, there was no biting of the tongue or bedwetting. After a week in the field hospital, he was sent back to Berlin, where he experienced some physical anxiety without any emotional disturbances or consciousness issues, except for some inhibition; he couldn’t sleep, was overly sensitive, cried easily, and felt anxious when touched. He blinked severely during the eye exam and during the reflex tests, he had strong, semi-voluntary muscle contractions.
After four days in bed, which was a prescription hard to carry out at first on account of the anxiety sensations, these sensations disappeared, and at the same time the fears. Weight began to increase; memories returned, except that even upon recovery he could not remember that he had ever had any true subjective feelings of fear. He was discharged 19 days later, desirous of going back into the field.
After four days in bed, which was difficult to manage at first because of the anxiety, those feelings went away, along with the fears. His weight started to go up; memories came back, but even after recovering, he couldn’t recall ever having genuine feelings of fear. He was discharged 19 days later, eager to return to the field.
The peculiar absence of subjective feelings of fear in this case is something like what Awtokratow reported from the Russo-Japanese War, terming them neurasthenic psychoses.
The unusual lack of personal feelings of fear in this situation is similar to what Awtokratow described during the Russo-Japanese War, calling them neurasthenic psychoses.
Re neurasthenia, Babinski believes that, by means of his logical dismembering of the old hysteria concept, he has shown that the exhaustion phenomena at the bottom of neurasthenia are precisely these that cannot be cured by suggestion. There are numerous cases in which hysteria and neurasthenia are combined. From these combined cases, suggestion causes the hysterical or pithiatic symptoms to be removed.
Regarding neurasthenia, Babinski believes that through his logical breakdown of the old concept of hysteria, he has demonstrated that the exhaustion symptoms at the root of neurasthenia are precisely those that cannot be treated through suggestion. There are many cases where hysteria and neurasthenia occur together. In these combined cases, suggestion eliminates the hysterical or pithiatic symptoms.
English schoolmaster’s account of his war dreams.
English schoolmaster’s account of his war dreams.
Case 341. (Mott, February, 1918.)
A sergeant, who had been a schoolmaster, was asked to write down his dreams by Captain W. Brown, who had sometimes charge of Mott’s cases at the Maudsley Hospital. The first dream was as follows:
A sergeant, who had been a schoolteacher, was asked to write down his dreams by Captain W. Brown, who sometimes handled Mott’s cases at the Maudsley Hospital. The first dream was as follows:
“I appeared to be resting on the roadside when a woman (unknown) called me to see her husband’s (a comrade) body which was about to be buried. I went to a field in which was a pit, and near the edge four or five dead bodies. In a hand-cart nearby was a legless body, the head of which was hidden from sight by a slab of stone. [He had seen a legless body, which was covered with a mackintosh sheet, which he removed.] On moving the stone I found the body alive, and the head spoke to me, imploring me to see that it was not buried. Burial party arrived, and I was myself about to be buried with legless body when I awoke.”
“I seemed to be resting by the roadside when a woman I didn't know called me over to see her husband’s body, which was about to be buried. I walked over to a field where there was a pit, and nearby were four or five dead bodies. In a hand-cart close by was a legless body, its head hidden from view by a stone slab. [He had seen a legless body covered with a mackintosh sheet, which he removed.] When I moved the stone, I found the body was alive, and the head pleaded with me not to let it be buried. The burial party arrived, and I was about to be buried with the legless body when I woke up.”
The second dream was as follows:
The second dream was:
“After spending an evening with a brother (dead 11 years ago) I was making my way home when a violent storm compelled me to take shelter in a kind of culvert, which later turned into a quarry, situated between two houses. Men were doing blasting operations in the quarry, and whilst watching them I saw great upheavals of rock, and eventually the building all around collapsed (explosion of a mine). Amongst the débris were several mutilated bodies, the most prominent of which was legless. I tried to proceed to the body, but found that I was myself pinned down by masonry which had fallen on top of me. As I struggled to get free the whole scene appeared to change to a huge fire, everything being enveloped in flames, and through the flames I could still see the legless body which now bore the head of my wife, who was calling for me. I was struggling to get free when my mother seemed to be coming to my assistance, and I awoke to find the nurses and orderlies standing over me.”
“After spending an evening with a brother who died 11 years ago, I was on my way home when a fierce storm forced me to take shelter in a kind of culvert, which later became a quarry, located between two houses. Workers were blasting in the quarry, and as I watched, I saw massive rock upheavals, and eventually, the buildings around collapsed (due to a mine explosion). Among the debris were several mangled bodies, the most notable of which was legless. I tried to move toward the body, but I found myself pinned down by rubble that had fallen on me. As I struggled to get free, the entire scene seemed to transform into a huge fire, with everything engulfed in flames, and through the flames, I could still see the legless body, which now had the head of my wife, who was calling for me. I was fighting to get loose when my mother appeared to be coming to help me, and I awoke to find the nurses and orderlies standing over me.”
It appears that the patient had been shouting in his sleep, beginning in a low voice and gradually becoming louder until at last he was shrieking. The legless body occurred in all[471] his dreams; the sight of this had evidently produced a profound emotional shock. He had worried a great deal about his wife, who was much younger than himself, so that we have this incongruous association of the legless body and the head of his wife calling him; finally, what more natural than the mother to come to his help. The emotional complex is not incongruous in this dream, for fear is linked up with the tender emotion.
It looks like the patient had been yelling in his sleep, starting with a quiet voice and getting louder until he was finally screaming. The legless body showed up in all his dreams; clearly, seeing this had a significant emotional impact on him. He had been really worried about his wife, who was much younger than he was, which created this strange connection between the legless body and his wife’s head calling for him; and of course, it makes sense that the mother would come to help him. The emotional mix in this dream actually makes sense, as fear is connected with his feelings of tenderness.
Re war dreams, see remarks under Case 333 concerning oniric delirium. Roussy and Lhermitte say that emotion and concussion are the causal factors; but in a case like 341 we have persistent war dreams of the same general nature. Such a case as Mott’s would not be regarded as one of oniric delirium, for the patient is not living throughout the day in a dream, but merely has certain set dreams. The true oniric delirium cases may lead to fugues of medicolegal importance. Mott’s conception is that the terrifying experiences that come to light in the dreams are repressed by the conscious activity of the mind in the waking state. For this process, the phrase psychic trauma might be used. Rows speaks of a prolongation of mental disorder through memories which get revived in dreams. The memories of past and recent events pile up on one another. Elliot Smith remarks on the number of cases in which the dreams show a coalescence and blending of episodes alien to the war. Re such combinations, see Case 342 of Rows, below.
Regarding war dreams, see comments under Case 333 about oniric delirium. Roussy and Lhermitte state that emotion and concussion are the main causes; however, in a case like 341, we observe consistent war dreams of a similar nature. A case like Mott’s wouldn’t be classified as oniric delirium since the patient isn’t experiencing a continuous dream throughout the day, but only specific dreams. The true oniric delirium cases can result in fugues that are significant in medicolegal contexts. Mott believes that the frightening experiences revealed in dreams are suppressed by the conscious activity of the mind while awake. For this process, the term psychic trauma might be applicable. Rows discusses how mental disorders can be prolonged through memories that resurface in dreams. The memories of past and recent events accumulate on top of each other. Elliot Smith notes the many cases where dreams blend and merge episodes unrelated to the war. Regarding such combinations, see Case 342 from Rows, below.
Trench experience: War dreams, shifting to sex dreams. Recovery on giving the patient an insight into the nature of his dreams.
Trench experience: War dreams turning into sexual dreams. Recovery by helping the patient understand the nature of his dreams.
Case 342. (Rows, April, 1916.)
A patient broke out of a hospital after being refused permission to leave the grounds. He grew much depressed and said he had been disgraced and would commit suicide rather than bring disgrace on his family. Investigation into this emotional outburst showed that his father had deserted the family, that he had gotten into prison, and “tainted me.” The patient was worried also about an idea of loss of sex power, gathered from a book by a quack doctor, read years ago. It appeared also that this doctor had advertised a special bread and special medicine which would preserve the nervous system, and that for years the patient had fed himself and his family with the bread and medicine. When the true state of affairs was shown to the patient, his restlessness at night disappeared. The mental condition of this man in fact became practically normal, and the marked tic of facial muscles and the general tremulousness of the man disappeared.
A patient escaped from a hospital after being denied permission to leave the premises. He became very depressed and claimed he felt disgraced and would rather commit suicide than shame his family. An investigation into this emotional outburst revealed that his father had abandoned the family, ended up in prison, and “tainted me.” The patient was also troubled by concerns about losing his sexual power, stemming from a book by a fraudulent doctor he had read years ago. It turned out that this doctor had promoted a special bread and medicine that supposedly preserved the nervous system, and for years, the patient had been feeding himself and his family that bread and medicine. Once the true situation was explained to the patient, his restlessness at night went away. In fact, this man’s mental state became nearly normal, and the noticeable facial muscle twitching and his overall trembling disappeared.
It is of note that this man’s dreams began with a terrible incident in the trenches and then shifted to sex acts. He woke to find the clothes disturbed.
It’s important to mention that this man’s dreams started with a horrific event in the trenches and then switched to sexual encounters. He woke up to find his clothes messed up.
This is an example of hallucinations dispelled by tracing them to their source, and giving the patient a clear insight into their nature.
This is an example of hallucinations being cleared up by identifying their source and providing the patient with a clear understanding of what they are.
According to Ballet and de Fursac, after the acute phase of stupor and excitement with hallucinations and delirium passes, the patient remains a depressed and psychasthenic subject. In this psychasthenia we find inhibitory phenomena, hyperemotionalism, and over-imagination. Amongst the inhibitory phenomena are many of the hysterical effects. The hyperemotionalism yields anxiety, worry, tremors, respiratory and vasomotor disorder, dizziness, convulsions. The third main disorder of the psychasthenic state into[473] which the patient relapses is over-imagination, whereunder we find bad dreams (bombardments, drum-beating, corpses, attacks), somnambulistic hallucinatory episodes. It is these hyperemotional and hyperfantastic features that distinguish the Shell-shock syndrome from ordinary psychasthenic states.
According to Ballet and de Fursac, after the intense phase of stupor and excitement marked by hallucinations and delirium subsides, the patient remains in a state of depression and psychasthenia. In this psychasthenic state, we observe inhibitory phenomena, heightened emotional sensitivity, and excessive imagination. The inhibitory phenomena include many hysterical effects. The heightened emotional sensitivity leads to anxiety, worry, tremors, respiratory and vasomotor disorders, dizziness, and convulsions. The third major disorder of the psychasthenic state into[473] which the patient falls back is excessive imagination, where we encounter troubling dreams (like bombings, drum beats, corpses, and attacks) and episodes of sleepwalking with hallucinations. It's these hyperemotional and hyperfantastic aspects that set the Shell-shock syndrome apart from typical psychasthenic conditions.
Re the sex element in this case, see remarks under preceding case (341) and also Lépine on the sex factor (Case 332). Rows believes that those cases which do not recover after a short period of rest and quiet in hospital are cases in which there is some emotional state based upon the constant intrusion of the memory of some past event. The physical expression of the emotion of fear or terror may persist for a long time quite unchanged and be proved to be due to this old factor.
Regarding the sex element in this case, refer to comments under the previous case (341) and also Lépine on the sex factor (Case 332). Rows believes that cases which do not improve after a brief period of rest and quiet in the hospital indicate an emotional condition rooted in the continual recollection of a past event. The physical expression of fear or terror can linger for a long time, remaining unchanged, and can be shown to be related to this past factor.
Emotional shock: Recurrent dreams of war and peace incidents. Recovery followed tracing the dreams to their origin.
Emotional shock: Frequent dreams about war and peace events. Recovery came after identifying the origins of the dreams.
Case 343. (Lines, April, 1916.)
A soldier and a comrade were carrying a pail of water to the trenches. It was very cold and they set down the pail in order to warm their hands. The comrade placed his hand against the man’s cheek and said, “That hand is cold.” At that moment he was shot dead.
A soldier and a buddy were carrying a bucket of water to the trenches. It was really cold, so they set the bucket down to warm their hands. The buddy put his hand on the man's cheek and said, “That hand is cold.” In that instant, he was shot dead.
This incident was involved not only in dreams at night, but in the daytime too, if he were quiet and closed his eyes, he could feel the cold hand against his face.
This incident was involved not only in dreams at night, but in the daytime too; if he was quiet and closed his eyes, he could feel the cold hand on his face.
He was troubled at the same time by another dream, in which he ran down a narrow lane at the bottom of which there was a well. He dipped his hands into the water, but on withdrawing them, he was horrified to find they were covered with blood. This dream was connected with a love affair, in which a good friend interfered and angered him so much that he attacked him when next they met. He left him on the ground so injured that it was necessary to take him to a hospital. The patient became anxious as to what the result might be and left the district. He traveled, but never heard whether his victim had died.
He was simultaneously troubled by another dream in which he ran down a narrow path that led to a well. He dipped his hands into the water, but when he pulled them out, he was horrified to see they were covered in blood. This dream was linked to a romantic situation where a close friend got involved and made him so angry that he attacked him the next time they met. He left his friend on the ground, seriously injured, requiring him to be taken to a hospital. The injured man became anxious about the outcome and decided to leave the area. He traveled, but never found out if his friend had survived.
When these two dreams were traced back to their origin they disappeared: the patient made a rapid recovery and was able afterwards to bear a severe trial satisfactorily.
When these two dreams were traced back to their source, they vanished: the patient quickly recovered and was then able to handle a tough challenge with ease.
See remarks under Case 342.
See comments under __A_TAG_PLACEHOLDER_0__.
War dreams, including hunger and thirst.
War dreams, including feelings of hunger and thirst.
Case 344. (Mott, February, 1918.)
(Recorded Dream of a Second Lieutenant.)
(Recorded Dream of a Second Lieutenant.)
“During the five days spent in the village of Roeux I was continually under our own shell fire and also continually liable to be discovered by the enemy, who was also occupying the village. Each night I attempted to get through his lines without being observed, but failed. On the fourth day my sergeant was killed at my side by a shell. On the fifth day I was rescued by our troops while I was unconscious. During this time I had had nothing to drink or eat, with the exception of about a pint of water.
“During the five days I spent in the village of Roeux, I was constantly under our own artillery fire and repeatedly at risk of being spotted by the enemy, who was also in the village. Every night, I tried to slip through their lines unnoticed, but I couldn't manage it. On the fourth day, my sergeant was killed right next to me by shellfire. On the fifth day, I was rescued by our troops while I was unconscious. Throughout this time, I hadn’t had anything to drink or eat, except for about a pint of water.”
“At the present time I am subject to dreams in which I hear these shells bursting and whistling through the air. I also continually see my sergeant, both alive and dead, and also my attempts to return are vividly pictured. I sometimes have in my dreams that feeling of intense hunger and thirst which I had in the village. When I awaken I feel as though all strength had left me and am in a cold sweat.
“At the moment, I’m having dreams where I hear these shells exploding and whistling through the air. I keep seeing my sergeant, both alive and dead, and my attempts to come back are vividly replayed. Sometimes, I even feel that intense hunger and thirst I experienced in the village during my dreams. When I wake up, it feels like all my strength has vanished, and I’m drenched in a cold sweat.”
“For a time after awaking I fail to realize where I am and the surroundings take on the form of the ruins in which I remained hidden for so long.
“For a while after I wake up, I don't realize where I am, and the place around me starts to feel like the ruins where I had been hiding for so long.
“Sometimes I do not think that I thoroughly awaken, as I seem to doze off, and there are the conflicting ideas that I am in the hospital, and again that I am in France.
“Sometimes I don’t feel like I fully awaken, as I seem to drift off, and I have these conflicting thoughts that I’m in the hospital, and then again that I’m in France.”
“During the day, if I sit doing nothing in particular and I find myself dozing, my mind seems to immediately begin to fly back to France.
“During the day, if I sit around doing nothing and start to doze off, my mind instantly begins to drift back to France.
“A dream that keeps on coming up in my mind is one that brings back a motor accident I had about six years ago, which gave me a severe nervous shock. I had, of course, entirely forgotten about it, except when in a motor, when I always thought of it.
“A dream that keeps coming to my mind is one that brings back a car accident I had about six years ago, which gave me a serious shock. I had completely forgotten about it, except when I was in a car, when I always thought of it.
“Of the fifth day I have absolutely no recollections.”
“Honestly, I have no memories of the fifth day at all.”
This is the one instance in which a man has dreamt the experience of hunger and thirst in addition to battle experience.
This is the only time a man has experienced hunger and thirst along with battle.
Olfactory dreams: Hysterical vomiting.
Smelly dreams: Hysterical vomiting.
Case 345. (Wiltshire, June, 1916.)
A lieutenant in the infantry (mother, of a nervous disposition) had been at the front for 3½ months when he started vomiting everything he ate.
A lieutenant in the infantry (his mother, who was quite anxious) had been at the front for 3½ months when he began throwing up everything he ate.
He was transferred a fortnight later to a base hospital as “gastritis.” Physical examination proved negative, but the man complained of his nerves. He slept badly owing to trench-life dreams, from which he would wake in a sweat. He was quite unwilling to refer to these dreams.
He was moved to a base hospital two weeks later for “gastritis.” A physical exam came back clear, but the man said he was struggling with his nerves. He had trouble sleeping because of nightmares from his time in the trenches, waking up in a sweat. He was really hesitant to talk about these dreams.
In point of fact he had had to supervise the burial of many decomposing bodies, after which he had been haunted “by that awful smell of the dead.” Then developed states of abstraction, in which he went over and over the burying experience. He cried by himself.
In reality, he had to oversee the burial of many decaying bodies, and after that, he was haunted “by that awful smell of the dead.” This led to periods of distraction, where he repeatedly replayed the burial experience in his mind. He cried alone.
It seems that the vomiting was secondary to hysterical hallucinations.
It looks like the vomiting was caused by hysterical hallucinations.
Re affections of smell and taste, Roussy and Lhermitte remark that they are rare following shock or trauma in war. Medical suggestion may produce a hemiageusia or a hemianosmia. Mott’s case above (344) showed unusual dreams with hunger and thirst. For another olfactory case, see Case 510 (Rivers) in the Treatment Section of the book, a case in which Rivers was able to find no redeeming feature upon which to ground his re-educative suggestions.
Regarding the senses of smell and taste, Roussy and Lhermitte note that they are uncommon after shock or trauma in war. Medical advice may lead to hemiageusia or hemianosmia. Mott’s case above (344) displayed unusual dreams related to hunger and thirst. For another case involving smell, see Case 510 (Rivers) in the Treatment Section of the book, where Rivers found no redeeming quality to support his re-educative suggestions.
Re vomiting, Roussy and Lhermitte state that this relatively common condition is diagnosticated readily enough but that pyloric ulcer and other organic causes must be eliminated. They remark that there is no tendency to spontaneous cure of neuropathic vomiting, and commend strict dietetic régime and psychotherapy. They ally the condition in its nature and genesis with so-called false or hysterical incontinence of urine in soldiers. Wiltshire’s case early received the diagnosis “gastritis.” It is remarkable how little emaciation need follow such vomiting.
Regarding vomiting, Roussy and Lhermitte note that this fairly common issue can be diagnosed easily enough, but that pyloric ulcer and other organic causes must be ruled out. They point out that there is no tendency for neuropathic vomiting to heal on its own and recommend a strict diet and psychotherapy. They link the condition in its nature and origin to so-called false or hysterical urinary incontinence seen in soldiers. Wiltshire's case was initially diagnosed as "gastritis." It's interesting how little weight loss can occur after such vomiting.
Shell-shock: Amnesia; dreams of falling. POST-ONIRIC suggestion—surprise produced fear of falling.
Shell shock: Memory loss; dreams of falling. POST-ONIRIC suggestion—surprise caused a fear of falling.
Case 346. (Duprat, October, 1917.)
A man was subjected to shell-shock August 11, 1916, at the Somme. He lost consciousness for five hours and was picked up stuporous with verbal amnesia, which soon passed leaving only a difficulty in getting the right word promptly. He began to have frightful dreams of falling into a hole and of exertions to avoid falling, whereupon he would awake with a feeling of anxiety that would last some time. Treatment caused the dreams to disappear.
A man experienced shell shock on August 11, 1916, at the Somme. He lost consciousness for five hours and was found in a daze with verbal memory loss, which soon faded, leaving him with just a struggle to find the right words quickly. He started having terrifying dreams about falling into a hole and trying to avoid the fall, and he would wake up feeling anxious, which would linger for a while. Treatment made the dreams go away.
There remained, however, a powerful post-oniric suggestion. Any slight surprise would cause the fear of falling to reappear. There was a sort of derived phobia, against any military act that would need to be performed upon sudden order. He developed a blind anger against any commanding officer who gave a brusque order. After the crisis of anger he would fall into tears and a feeling of profound depression coupled with precordial anxiety. There was also a chronic aortitis physically determined. The man himself had a vague idea of the relationship of his fear of surprise to the old nightmares.
There was, however, a strong post-oniric suggestion. Any unexpected event would trigger the fear of falling again. He developed a kind of phobia about any military action that required him to act on short notice. He felt a blind rage toward any commanding officer who gave a harsh command. After the outburst of anger, he would break down in tears and experience deep sadness along with anxiety in his chest. There was also a chronic aortitis that was physically caused. The man had a vague sense of how his fear of surprises connected to his old nightmares.
Re persistence of fear and its relationship to nightmares, see remarks under Case 342 (Rows).
Re persistence of fear and its connection to nightmares, see comments under Case 342 (Rows).
Four months’ SERVICE IN THE REAR: Depression; war HALLUCINATIONS (not based upon actual experiences); psychasthenic symptoms.
Four months of service in the rear: depression; war hallucinations (not based on actual experiences); psychasthenic symptoms.
Case 347. (Gerver, 1915.)
A Russian lieutenant, 32, arrived at the front in November, 1914, but never served on the front line, or had occasion to visit the line or the trenches. Toward the close of February, mental symptoms appeared, which caused the man’s evacuation to the interior.
A 32-year-old Russian lieutenant arrived at the front in November 1914, but he never served on the front line or had the chance to visit the line or the trenches. By the end of February, he began to show mental symptoms, which led to his evacuation to the interior.
He was a tall, well-built, well-nourished man, who was physically normal except for sharp twitching movements of the tongue, eyelids, and face; tremors of extended hands, occasionally spreading to the whole body; well-defined dermatographia (in places, stereodermatographia); exaggerated tendon reflexes; tenderness of skull and spine; hyperesthesia of chest; pulse 120.
He was a tall, fit, and healthy man who was physically normal except for some sharp twitching movements of his tongue, eyelids, and face; tremors in his outstretched hands that sometimes affected his entire body; distinct dermatographia (in some areas, stereodermatographia); heightened tendon reflexes; sensitivity in his skull and spine; increased sensitivity in his chest; and a pulse of 120.
Mentally, the patient was markedly depressed, irritable, at times lacrimose. His complaints were of a psychasthenic tinge. He feared incurable disease. He feared to go to the front, and was terrified at what he might do there. He feared crowds of soldiers; he was afraid of forests and mountains; the Germans were going to break through and capture him; shells were about to burst over his head. He was also disturbed about his family, regarding his wife and son as helpless, sometimes even as dead. Suicidal thoughts at times.
The patient was clearly very depressed, irritable, and at times tearful. He expressed worries that had a psychological edge. He was afraid of getting an incurable disease. He didn't want to go to the front and was terrified of what he might do there. He was scared of crowds of soldiers, as well as of forests and mountains; he thought the Germans would break through and capture him, and that shells were about to explode overhead. He was also troubled about his family, viewing his wife and son as helpless, and sometimes even as if they were dead. He occasionally had suicidal thoughts.
At night, though he had never been at the front, he had hallucinations of shots and the voices of soldiers, as well as those of his wife and son. He smelt an unpleasant corpse-like odor. He was unable to distinguish these hallucinations in any respect from reality. He complained of general weakness, headaches, palpitation of the heart, vertigo, and insomnia, and of a variety of pains.
At night, even though he had never been on the front lines, he experienced hallucinations of gunfire and the voices of soldiers, along with those of his wife and son. He smelled a disturbing, corpse-like odor. He couldn’t tell these hallucinations apart from reality. He reported feeling generally weak, having headaches, a racing heart, dizziness, insomnia, and various pains.
He was non-alcoholic and non-syphilitic, and had been in perfect health before the war.
He didn't drink alcohol and didn't have syphilis, and he had been in perfect health before the war.
Re war hallucinations with service back of the line, compare remarks of Régis (see under Case 333).
Re war hallucinations with service back of the line, compare remarks of Régis (see under Case 333).
A case of hysterical astasia-abasia develops “big belly” (“catiemophrenosis”), perhaps by hetero-suggestion from a ward neighbor.
A case of hysterical astasia-abasia develops “big belly” (“catiemophrenosis”), possibly due to suggestion from a neighbor in the ward.
Case 348. (Roussy, Boisseau and Cornil, May, 1917.)
A farmer, 22, of the foot chasseurs, who had been in various hospitals with a variety of diseases before his injury, was evacuated June 2, 1916, for “contusion of back,” to the temporary hospital at Bussant, from which he was evacuated to Pontarlier for “contusion of back and cerebellar shock” and thence, July 21, to Besançon for “internal contusion and cerebellar shock”; thence to four other hospitals from July 31 to February 17, 1917; finally to the Hospital at Veilpicard with “functional disorders, paraplegia, trepidant astasia-abasia.”
A 22-year-old farmer, serving in the foot chasseurs, had been in several hospitals with a range of illnesses before getting injured. He was evacuated on June 2, 1916, for "back contusion" to the temporary hospital in Bussant, from there he was sent to Pontarlier for "back contusion and cerebellar shock," and then on July 21 to Besançon for "internal contusion and cerebellar shock." He went to four other hospitals between July 31 and February 17, 1917, and finally arrived at the hospital in Veilpicard with "functional disorders, paraplegia, tremulous astasia-abasia."
It seems that he had lost consciousness for fifteen days and had thereafter been paraplegic with retention of urine. The abdomen had then increased in size in such wise as to be termed a nervous pregnancy, grossesse nerveuse. The evolution of this pseudotympanites was probably related to the presence of the same so-called “big belly” of a patient who had been in a neighboring bed from May, 1916, onwards. The feet were in equine position with toes flexed, suggestive in all ways of hysterical paraplegia. The abdomen looked like that of a woman six months pregnant and measured 78 centimeters in a plane passing through the anterosuperior iliac spines and the umbilicus. The abdomen was hard, tense, swollen, and on palpation, gave out a low, tympanic note. When the diaphragm was mobilized progressively and slowly, the tympanites could be made to disappear. Slow pressure on the abdomen with flat hands effaced the swelling for the time being; but upon release of the hands the abdomen would swell up again as before. Pressure on the abdomen produced a contracture of the recti. Forced flexion of thighs on pelvis (as suggested by Denéchau and Matrais) also caused the swelling to go down. Faradization of the phrenic nerves in the neck caused respiratory movements with a slight diminution in the volume of the abdomen. There was an obstinate[480] constipation requiring daily lavage. Respiratory movements were short and rapid and of the thoracic type. Abdominal compression caused the respiration to assume almost a normal rhythm. X-ray examination of the abdomen, after 50 grams of bismuth carbonate had been taken in three spaced doses the evening before, showed the intestine to be distended by gas in such wise that the lower border of the liver became clearly visible, as after insufflation of the stomach. The bismuth was found in the large intestine. The splenic angle filled with bismuth was low. On compression the splenic angle was raised with the diaphragm.
It seems that he had been unconscious for fifteen days and was then left paraplegic with urinary retention. His abdomen had enlarged to the point where it could be described as a nervous pregnancy, grossesse nerveuse. The development of this pseudotympanites was likely linked to the same so-called “big belly” of a patient who had been in a nearby bed since May 1916. The feet were in a position resembling that of a horse, with toes flexed, which was characteristic of hysterical paraplegia. The abdomen appeared similar to that of a woman six months pregnant and measured 78 centimeters across a plane passing through the anterosuperior iliac spines and the umbilicus. It was hard, tense, and swollen, and when palpated, produced a low, tympanic sound. Slowly and progressively mobilizing the diaphragm caused the tympanites to disappear. Applying slow pressure to the abdomen with flat hands temporarily reduced the swelling; however, once the hands were lifted, the abdomen would return to its previous size. Pressing on the abdomen resulted in a contraction of the rectus muscles. Forced flexion of the thighs on the pelvis (as suggested by Denéchau and Matrais) also reduced the swelling. Faradization of the phrenic nerves in the neck led to respiratory movements with a slight decrease in abdominal volume. There was persistent[480] constipation that required daily lavage. Respiratory movements were short and rapid, resembling thoracic breathing. Compressing the abdomen allowed the respiration to nearly return to a normal rhythm. An X-ray examination of the abdomen, after taking 50 grams of bismuth carbonate in three spaced doses the evening before, showed the intestines to be distended with gas, making the lower border of the liver clearly visible, similar to what happens after stomach insufflation. The bismuth was located in the large intestine. The splenic angle filled with bismuth was low, but when compressed, the splenic angle was raised along with the diaphragm.
The main features of this disease are the large abdomen, simulating what has hitherto been found chiefly in females under the name of nervous pregnancy, but also suggesting a tuberculous peritonitis (one patient was actually evacuated to a hospital for tuberculosis with this disease); gastro-intestinal disorder with aerophagy, aerocoly, and obstinate constipation (one case also showed almost daily vomiting). The genesis of the condition appears to be a contracture of the diaphragm in a low position of forced inspiration. The condition may be termed a diaphragmatic neurosis.
The main features of this disease include an enlarged abdomen, similar to what has primarily been seen in females, referred to as nervous pregnancy, but also resembling tuberculous peritonitis (one patient was actually transferred to a hospital for tuberculosis with this condition); gastrointestinal issues with air swallowing, gas accumulation, and severe constipation (one case also experienced almost daily vomiting). The cause of the condition seems to be a tightening of the diaphragm due to a low position during forced inhalation. This condition can be called diaphragmatic neurosis.
Psychotherapy was applied, the patient was requested to walk, and the movements made in walking required such an intense respiration that the diaphragm was forced to function, whereupon the “big belly” disappeared. The digestive disorders then rapidly disappeared. These authors suggest the name of catiemophrenosis.
Psychotherapy was used, the patient was asked to walk, and the movements involved in walking required such intense breathing that the diaphragm had to work, which caused the “big belly” to go away. The digestive issues then quickly resolved. These authors propose the name catiemophrenosis.
War stress; collapse going over the top: Neurasthenia (hereditary taint; alcoholism).
War stress; breakdown from excessive strain: Neurasthenia (genetic predisposition; alcoholism).
Case 349. (Cheerful, January, 1916.)
A German soldier, 35, of a nervous make-up (his mother was nervous, and he had been nervous and tremulous and easily excitable, and alcoholic to the extent of at least 5 glasses of beer every night), was called to the colors in September, 1914. He got through his training well; in May, 1915, was on very strenuous duty in a very exposed position, had frequently to stand up under heavy shelling, had a number of frightful experiences, was surrounded by corpses and mutilated bodies, and frequently took part in storming attacks. His nervousness came to a head with some suddenness; just as he was about to “go over the top,” he had no strength for the effort and collapsed. Thereafter he could no longer stand shelling, could not speak, and was inattentive to surroundings. When he was examined by a physician he fell asleep in his presence, although sleep had latterly been almost impossible on account of the shelling. He was immediately put on the hospital train and taken to the reserve hospital in Nuremberg, where he presented an appearance of extreme exhaustion, wept, seemed much fatigued, and trembled all over whenever he started to do anything. He was very easily excited and especially sensitive to noise. There was a fine tremor of the whole body and especially of the head; the knee-jerks were increased; there was a moderate vasomotor reddening of the skin after stroking; his tongue was heavily coated; but there was no other evidence of internal disorder. His pulse was strong and not rapid.
A 35-year-old German soldier with a nervous temperament (his mother was anxious, and he had always been jittery, sensitive, easily excited, and drank at least 5 glasses of beer every night) was drafted in September 1914. He completed his training successfully; by May 1915, he was stationed in a very demanding and exposed position, frequently enduring heavy shelling, experiencing horrific events, surrounded by corpses and mutilated bodies, and often participating in assaults. His nervousness escalated abruptly; just as he was about to "go over the top," he lacked the strength for the effort and collapsed. After that, he couldn’t handle the shelling, was unable to speak, and was not aware of his surroundings. When a doctor examined him, he fell asleep, even though sleep had been nearly impossible lately due to the constant shelling. He was quickly placed on a hospital train and taken to a reserve hospital in Nuremberg, where he appeared extremely exhausted, cried, seemed very fatigued, and trembled whenever he tried to do anything. He was easily startled and particularly sensitive to noise. There was a noticeable tremor throughout his body, especially in his head; his knee-jerks were heightened; there was moderate reddening of the skin after being stroked; his tongue was heavily coated; but there were no other signs of internal issues. His pulse was strong but not fast.
The patient got well gradually, complained at first of bad dreams, and was given to weeping. The tremors slowly improved. The patient grew better in a hospital at home.
The patient gradually got better, initially complained of bad dreams, and was prone to crying. The tremors slowly improved. The patient recovered in a hospital at home.
As to the diagnosis of this case, Jolly regards it as one of nervous exhaustion. The remarkable feature is the tardiness with which the symptoms developed under the stress of war. Such a patient would probably never develop a neurasthenia[482] under normal peace conditions. After recovery these patients may be sent back for garrison duty or for other work not directly connected with the firing line. As for the tendency to desire a pension, this wish, according to Jolly, must be strenuously opposed, both in the interest of the state and that of the patient. If there is no will to get well, some of these patients are found vibrating from garrison service to furlough and to hospital.
As for the diagnosis of this case, Jolly sees it as one of nervous exhaustion. The notable aspect is how slowly the symptoms appeared due to the stress of war. Such a patient would likely never develop neurasthenia[482] in normal peacetime conditions. After recovery, these patients may be assigned back to garrison duty or to other roles not directly related to the front lines. Regarding the desire for a pension, Jolly believes this wish must be strongly opposed, both for the benefit of the state and for the patient. If there’s no motivation to recover, many of these patients are often found moving between garrison service, leave, and the hospital.
The above case is one of the simplest observed; yet there is evidence both of hereditary taint and of alcoholism. According to Jolly, the majority of the severe exhaustion states of a neurasthenic nature have been, in his experience, distinctly nervous before the war, and frequently show hereditary taint as well.
The above case is one of the simplest observed; yet there is evidence of both hereditary issues and alcoholism. According to Jolly, in his experience, most of the severe exhaustion states related to neurasthenia were clearly nervous before the war and often show hereditary problems as well.
Re neurasthenia, see views of Babinski relative to differentiation from hysteria (under Case 340).
Re neurasthenia, see Babinski's views on differentiation from hysteria (under Case 340).
Series of battles: Sudden mania followed by confusion with fixation of mind upon war experiences, possibly hallucinatory; general analgesia.
Series of battles: Sudden episodes of intense excitement followed by confusion, fixating on war experiences, possibly hallucinatory; overall numbness.
Case 350. (Gerver, 1915.)
A Russian private, looking much older than his years (35), had been in a number of battles without mental disorder. Where he was posted, however, there was a heavy artillery fire in the last of the battles. Suddenly the man became excited and leaped upon his comrades’ shoulders crying, “The devil is here! This is hell and murder, and here are the devil’s imps!” The commanding officer accordingly ordered him to the rear. His regiment had suffered severe losses in a succession of attacks upon a certain strategic height.
A Russian soldier, looking much older than his 35 years, had been through several battles without losing his sanity. However, where he was stationed, there was intense artillery fire during the last battle. Suddenly, he got agitated and jumped onto his comrades' shoulders, shouting, "The devil is here! This is hell and murder, and here are the devil’s minions!" The commanding officer then ordered him to move to the rear. His regiment had endured heavy losses in a series of assaults on a critical high point.
Upon evacuation to the field hospital and thence to the interior, his excitement did not lessen. He went about with a lost look, trembling, talking a great deal and gesticulating. His talk was incoherent and pointless. After every few phrases, he would repeat, “Don’t ride there! That’s hell! Murder is being done. Devils and unholy powers are beating and killing people.” As he said this, he would tremble, and hands and feet would stiffen with a suggestion of catalepsy. There was general anesthesia to pain; no response was made to deep pin-pricks. The pupils were dilated and failed to react, either to light or to pain. The tendon reflexes were exaggerated. No contraction of visual fields. The man was disoriented for time and place and much confused. No paralysis. No wound or contusion.
Upon being evacuated to the field hospital and then moved further in, his excitement didn’t fade. He wandered around with a lost expression, trembling, talking a lot, and gesturing wildly. His speech was jumbled and made no sense. After every few sentences, he would repeat, “Don’t go there! It’s hell! They’re committing murder. Devils and evil forces are beating and killing people.” As he said this, he would shake, and his hands and feet would stiffen as if he were in a trance. There was a complete lack of pain response; he didn’t react to sharp pin pricks. His pupils were dilated and didn’t respond to light or pain. The reflexes in his tendons were heightened. There was no contraction of his visual fields. He was confused about time and place and was very disoriented. There was no paralysis. No injuries or bruises.
Re analgesia, we may only say that hysterical anesthesia appears in a variety of forms; sometimes (a) in the form of a classical stigma of hemi-anesthesia; (b) in a segmentary form; again (c) in isolated patches; (d) in a very rough way approximating the peripheral nerve distributions. Babinski gives an unpublished note by Lasègue, in which he states that hysterical patients not enlightened by the doctor’s investigations do not make mention of anesthesia. But in case 350 a psychotic factor may have entered.
Regarding analgesia, we can only say that hysterical anesthesia shows up in different forms; sometimes (a) as a classic sign of hemi-anesthesia; (b) in a segmental form; again (c) in isolated patches; (d) in a very rough approximation of peripheral nerve distributions. Babinski mentions an unpublished note by Lasègue, which states that hysterical patients who haven't been informed by the doctor’s investigations do not report any anesthesia. But in case 350 a psychotic factor may have been involved.
Ten months of military service (several battles) without reaction; then, hot machine gun battle: Mania with disorientation and war hallucinations.
Ten months of military service (in several battles) with no response; then, a fierce machine gun fight: Mania accompanied by confusion and war-related hallucinations.
Case 351. (Gerver, 1915.)
A Russian private, 24, in a scout company, entered the war on mobilization and took part in several battles without reaction. May 11, 1915, he was sent with the scout party into a hot encounter, hand to hand with machine-guns. After the battle, the man began to yell incoherent phrases at the men around him, started to climb over the top, and shot off his gun without permission. He was accordingly sent to hospital, where he was under observation for a week, during which he had occasional flashes of excitement, jumping out of bed and making movements of cutting or shooting, and then in a few minutes subsiding into inactivity.
A 24-year-old Russian private in a scout company was drafted into the war and took part in several battles without any noticeable reaction. On May 11, 1915, he was sent with a scout team into a fierce conflict, face-to-face with machine guns. After the battle, he started shouting nonsensical phrases at the soldiers around him, attempted to climb over the top, and fired his weapon without authorization. As a result, he was sent to the hospital, where he was monitored for a week. During that time, he had occasional bouts of excitement, jumping out of bed and mimicking cutting or shooting motions, only to calm down into inactivity a few minutes later.
He was a short but well-built and well-nourished man; the pupils responded rather weakly in accommodation; there was a small fibrillar tremor of the face, eyes, and tongue. The skin reflexes were diminished and there was a general hypalgesia; considerable mechanical overexcitability of muscles; no other neurological disorders. The mental state was one of confusion. Although he was in one of the corps hospitals, he said he was in a dug-out; the doctors were lieutenants; the attendants were privates in his company. Answers to questions were irrelevant or incoherent; there were a number of delusional expressions. He was to be shot because he had not himself shot enough Germans. If he were not to be shot, anyhow the soldiers would poison him. Rather than this he should be allowed to go into an attack. He would take a German fort and the Czar would name him a colonel. His regimental commander was saying to him, “You will be a hero, you will soon get a company.” His hallucinations sometimes included the voices of Germans saying, in broken Russian, “We will hang you and cut your belly open!” There was considerable amnesia for dates and even his last battle.
He was a short but well-built and well-nourished man; the pupils reacted rather weakly to light; there was a slight tremor in his face, eyes, and tongue. The skin reflexes were reduced, and there was a general lack of sensitivity to pain; his muscles showed significant overexcitability; there were no other neurological issues. His mental state was one of confusion. Even though he was in one of the corps hospitals, he insisted he was in a dug-out; the doctors were lieutenants; the attendants were privates in his unit. His answers to questions were irrelevant or nonsensical; he made several delusional statements. He believed he was going to be shot because he hadn't killed enough Germans. If he wasn't shot, he thought the soldiers would poison him instead. He preferred to be allowed to attack. He said he would capture a German fort and the Czar would promote him to colonel. His regimental commander told him, “You will be a hero; you’ll soon get your own company.” His hallucinations sometimes included voices of Germans saying, in broken Russian, “We will hang you and cut you open!” He struggled with memory loss regarding dates and even his last battle.
Numerous attacks and counter attacks in one day: Sudden incoherence with disorientation and the rapid development of war hallucinations of a scenic type. Suggestion of catatonic phenomena.
Numerous attacks and counterattacks in one day: Sudden incoherence with disorientation and the quick onset of war-related hallucinations of a scenic nature. Indications of catatonic symptoms.
Case 352. (Gerver, 1915.)
A Russian lieutenant, 28 (no mental disease, non-alcoholic), was in battle August 14, 1914, on which day his company attacked and was itself attacked several times. An officer who observed the lieutenant said that he came to him and informed him that the Germans must first be burned and then fought with. Thereafter the lieutenant began to speak loudly and incoherently, sometimes yelling incoherent orders. He was accordingly removed from the battle-field to the hospital back of the line. Upon examination, he was found to be of middle height, with dilated pupils, responding weakly to light and not at all to accommodation; twitchings of face, eyelids, and tongue, digital tremor, marked dermatographia, general analgesia, tendon reflexes somewhat exaggerated, cataleptic tendency in feet and hands.
A 28-year-old Russian lieutenant (no mental illness, non-alcoholic) was in battle on August 14, 1914, when his company attacked and was also attacked multiple times. An officer who witnessed this reported that the lieutenant came to him and stated that the Germans needed to be burned first and then fought. After that, the lieutenant started speaking loudly and incoherently, at times shouting confused orders. He was then taken from the battlefield to a hospital behind the front lines. Upon examination, he was found to be of average height, with dilated pupils that reacted weakly to light and not at all to accommodation; he exhibited facial, eyelid, and tongue twitching, trembling in his fingers, pronounced dermatographia, general insensitivity to pain, somewhat exaggerated tendon reflexes, and a cataleptic tendency in his feet and hands.
Mentally, the patient was in a stupor, sitting or standing in one place, without initiative; uncomplaining but occasionally uttering deep sighs or occasional isolated phrases. He answered no questions or only after a long pause. He was disoriented for time and place, but gave evidence of delusions and hallucinations. He thought, for example, that he was the chief of staff and had brought with him a squad of captured Germans who were standing nearby. Some wanted to be fed and let go; others were yelling and saying they would burn down the house. Sometimes the patient would hear shots and shells bursting, at which he would shudder and turn away. Apparently he would see his comrades falling under the shrapnel hail. However, he stood his ground and commanded the rest of the soldiers to go forward to the attack. Now and then he was negativistic, flexing the hands upon request to extend them, refusing food and drink. He was still apathetic on evacuation to the interior.
The patient was mentally in a daze, sitting or standing in one spot, lacking motivation; he didn’t complain but occasionally let out deep sighs or muttered isolated phrases. He didn’t answer questions or did so only after a long silence. He was confused about time and place but showed signs of delusions and hallucinations. For instance, he believed he was the chief of staff and had brought with him a group of captured Germans who were standing nearby. Some were asking to be fed and released, while others were shouting that they would burn the house down. Sometimes, the patient would hear gunshots and explosions, causing him to flinch and turn away. He seemed to see his comrades falling from the shrapnel. However, he held his ground and ordered the other soldiers to advance to the attack. Occasionally, he was resistant, clenching his hands when asked to extend them, and refusing food and drink. He remained apathetic during evacuation to safety.
Shell-shock after two days in trenches: Hysterical STUPOR seven days. Cure in three weeks, barring amnesia for stuporous period.
Shell shock after two days in the trenches: Hysterical stupor for seven days. Recovery in three weeks, except for memory loss during the stuporous period.
Case 353. (Gaupp, March, 1915.)
F. S., in civil life a wreath-binder in a flower shop, and from childhood very nervous and excited, subject to frequent nosebleeds and fainting spells (e.g., at sight of blood), enlisted at 22, November 3, 1914, as a reservist. January 18 he went into the field.
F. S., who worked as a wreath-binder in a flower shop and was very nervous and anxious since childhood, frequently experienced nosebleeds and fainting spells (for example, at the sight of blood), enlisted at 22 on November 3, 1914, as a reservist. He went into the field on January 18.
The wreath-binder was only two days in the trenches before going unconscious under the whistling and exploding shells. Physically uninjured, he was received in reserve hospital C in a deep stupor, January 22. He was unresponsive at first, once however saying, lost in a dream, “When will mother come?” His gait was unsteady and he had to be led and held. He slept a good deal in the daytime.
The wreath-binder was only two days in the trenches before losing consciousness due to the whistling and exploding shells. Physically uninjured, he was taken to reserve hospital C in a deep stupor on January 22. At first, he was unresponsive, but at one point he murmured, lost in a dream, “When will mom come?” His walk was unsteady, and he had to be guided and supported. He slept a lot during the day.
He became somewhat more active mentally, January 24 (remarking that he had slept well), and made his toilet, but he did not yet have bearings and wanted to go to his place of business. The next day his condition was similar. Asked what troop he was with, he said, “In the flower business.” January 26 he was much better, telling of the army training and a little about the war, and wrote a postcard to his parents. The stupor disappeared after January 27 and the patient became mentally normal. Amnesia persisted for the time, January 20 to 26. Headaches. February 9 he was well, except for the limited amnesia still persisting. He was eventually sent back to garrison duty, cured.
He became a bit more mentally alert on January 24 (noted that he had slept well) and got himself ready for the day, but he still didn't have a clear sense of where he was and wanted to go to work. The next day, his condition was about the same. When asked what unit he was in, he replied, “In the flower business.” By January 26, he was much better, sharing stories about army training and a little about the war, and even wrote a postcard to his parents. The daze he had been in cleared up after January 27, and he became mentally normal. He experienced amnesia from January 20 to 26. There were headaches. By February 9, he was fine, except for some lingering amnesia. He was eventually sent back to garrison duty, recovered.
Re stupor, Grandclaude remarks that stupor is probably the most frequent of the mental symptoms of Shell-shock, and that it may last from a few moments to a week. During the stupor the patient is asthenic, stertorous, and staring. Upon recovery from the stupor, a condition of dulness with amnesia and disorientation ensues. There may be a third phase of a more hyperkinetic character, with hallucinations and delusions concerning the war. These stuporous cases[487] are among the most serious of the conditions found, as some of the victims may even suggest dementia praecox from the persistence of childishness and silliness. As in Gaupp’s case, Grandclaude finds that headaches and amnesia persist. Relapses are frequent on the basis of a kind of sensitization.
Re stupor, Grandclaude notes that stupor is likely the most common mental symptom of Shell shock, and it can last anywhere from a few moments to a week. During stupor, the patient appears weak, breathes noisily, and stares blankly. After coming out of stupor, a state of dullness accompanied by memory loss and confusion follows. There may be a third phase characterized by increased activity, with hallucinations and delusions related to the war. These stuporous cases[487] are among the most severe conditions observed, as some victims may even show signs of early-onset schizophrenia due to lasting childishness and silliness. Similar to Gaupp’s case, Grandclaude observes that headaches and memory loss continue. Relapses are common due to a kind of heightened sensitivity.
Re amnesia and Shell-shock, Roussy and Lhermitte speak of amnesia as ordinarily a phenomenon of confusion. Amongst the mental disorders of the Shell-shock psychoses, these authors describe a group due to inhibition or diminution of mental activity, including the rare narcolepsy, or pathological sleep, and the confusional states proper. Simple confusion involves slowness in thinking, and amnesia often anterograde from the moment of the shock. Simple confusion ought to be distinguished from so-called “obtusion” or torpor, in which there is a disorientation for time and space, such as was shown in Mallet’s case. Chavigny has described an aprosexic form (with “birdlike” movements). More common is the amnestic form of torpor. The amnesia may not merely be anterograde from the moment of shock, but may extend to a prolonged period prior to the accident. Sometimes the amnesias are selective, producing phenomena of pseudo aphasia.
Re amnesia and shell shock, Roussy and Lhermitte discuss amnesia as typically a confusion-related phenomenon. Among the mental disorders associated with shell shock, these authors identify a group caused by reduced or inhibited mental activity, which includes the rare condition of narcolepsy, or pathological sleep, and true confusional states. Simple confusion leads to slow thinking, and amnesia is often anterograde from the moment of the shock. It's important to differentiate simple confusion from what's known as “obtusion” or torpor, where there is a disorientation in time and space, as seen in Mallet's case. Chavigny described a form characterized by aprosexia (with “birdlike” movements). More commonly, however, is the amnestic form of torpor. The amnesia might not only be anterograde from the time of the shock, but it can also reach back to a significant period before the incident. Sometimes, the amnesias are selective, leading to symptoms of pseudo aphasia.
Amnesia, monosymptomatic. Progressive recovery.
Memory loss, single symptom. Gradual recovery.
Case 354. (Hammer, January, 1917.)
An infantryman, 36, arrived without information at a psychiatric center, March 15, 1916, looking confused and knowing little more than his name, believing himself in a distant town. The disorientation lasted to March 21, on which day the man recognized the doctor as such, knew that he was at a hospital, but felt that he had just left home and wife. From this time on, he began to pick up his surroundings, evidently not knowing that there was a war or that he was a soldier. He did not recognize one of his own company. It was not until March 31 that the first memory of the war reappeared, namely, a memory of the call to the colors, drums, bells, and crowds. April 11 he recollected that he was a soldier and that his wife was in the country, where he had left her on the eleventh day of the mobilization. In the next few days, memories came back bit by bit. He had been at first a little thin and showed a slight fever, oliguria, and poor digestion. All these symptoms now lapsed, and the man became apparently perfectly well.
An infantryman, 36, arrived without any information at a psychiatric center on March 15, 1916, looking confused and knowing little more than his name, thinking he was in a distant town. This disorientation lasted until March 21, the day he recognized the doctor and realized he was in a hospital but felt like he had just left home and his wife. From that point on, he started to understand his surroundings, clearly not aware that there was a war going on or that he was a soldier. He didn’t recognize anyone from his own unit. It wasn’t until March 31 that he had his first memory of the war, recalling the call to arms, drums, bells, and crowds. By April 11, he remembered he was a soldier and that his wife was in the countryside, where he had left her on the eleventh day of mobilization. Over the next few days, memories came back slowly. At first, he was a little thin and showed slight fever, decreased urination, and poor digestion. All these symptoms eventually faded, and he appeared to be perfectly well.
Such states, according to Mallet, are relatively frequent in soldiers, both in epilepsy, and in infectious deliria,—more than in the deliria of exhaustion.
Such conditions, according to Mallet, are fairly common in soldiers, occurring more often in epilepsy and infectious deliria than in the deliria caused by exhaustion.
Aviator shot down: Organic mental symptoms.
Aviator shot down: Natural mental symptoms.
Case 355. (MacCurdy, July, 1917.)
A Canadian, 20, of normal makeup, in 1915 lost part of his left foot in a railway accident, but, notwithstanding, was finally commissioned in the Royal Flying Corps. He enjoyed the nine months of English training greatly. In France he made several successful flights over the lines, but was shot down and crashed to the ground within the British lines after two weeks of service. He got black eyes and bruises and lost consciousness for about four days, though a week later he was still hazy about recent events and was not quite sure in what hospital he lay. After another week he arrived in a London hospital.
A 20-year-old Canadian, who was of average build, lost part of his left foot in a railway accident in 1915. Despite this, he was eventually commissioned into the Royal Flying Corps. He really enjoyed the nine months of training in England. In France, he completed several successful flights over enemy lines, but after two weeks of service, he was shot down and crashed back into British territory. He sustained black eyes and bruises and lost consciousness for about four days, but even a week later, he was still fuzzy about recent events and wasn’t quite sure which hospital he was in. After another week, he was transferred to a hospital in London.
Here he would not answer questions, but stared at the examiner, finally shouting: “I want to get up.” He said he was in a certain suburb of Toronto, which, however, he insisted was a part of London not far away. He wanted a taxicab to go thither. He pondered, but seemed content when told that Rosedale was across the ocean. A superficial machine gun wound of the hip the patient said must be the mark of a hospital in France; it was a secret mark, meaning that he could return to the line and fight whenever he wanted to and that he could use the lavatory whenever he wanted to. He sometimes uttered brief phrases after questioning. Asked if he dreamed, he looked up cunningly and said, e.g., “I down the Boche. I am a live wire.”
Here, he wouldn't answer questions but stared at the examiner, finally shouting, "I want to get up." He claimed he was in a suburb of Toronto, which he insisted was part of London not far away. He wanted a taxi to go there. He thought about it but seemed satisfied when told that Rosedale was across the ocean. The patient mentioned a superficial machine gun wound on his hip, claiming it must be a mark from a hospital in France; it was a secret mark, meaning he could return to the front lines and fight whenever he wanted, and that he could use the bathroom whenever he wanted. He occasionally said short phrases after being questioned. When asked if he dreamed, he looked up slyly and said, e.g., "I down the Boche. I am a live wire."
Next day it was clear that he had gained a good deal of information from the nurses, and the day after he had become oriented for time and able to recognize the physician, though still confused about hospital names and his recent movements. The 7 from 100 test he did slowly and made several bad unrecognized mistakes. He was over-fatigueable, complained of foggy eyesight, showed haziness and redness and obscure margins in the optic discs, with the remains of one hemorrhage, and presented nystagmus on looking to the extreme left. Two weeks later he complained less of his memory and said that he was beginning to remember what[490] had happened during the last day of his fighting; the chase by the German airplane and the maneuvers. He worried about being sent back to France by a medical board, which would not realize that he was incompetent to fly again. The left pupil was slightly larger than the right.
The next day, it was clear that he had gathered a lot of information from the nurses, and by the following day, he was aware of the time and able to recognize the doctor, although he was still confused about hospital names and his recent activities. He took the 7 from 100 test slowly and made several serious mistakes that he didn't catch. He was very fatigued, complained of blurry vision, showed haziness and redness in the optic discs with remnants of one hemorrhage, and exhibited nystagmus when looking to the extreme left. Two weeks later, he complained less about his memory and mentioned that he was starting to remember what[490] happened on the last day of his fighting—the pursuit by the German airplane and the maneuvers. He was worried about being sent back to France by a medical board that wouldn't recognize he was unfit to fly again. The left pupil was slightly larger than the right.
In this case there were no neurotic symptoms and according to MacCurdy the difficulties here are strictly those of organic type.
In this case, there were no neurotic symptoms, and according to MacCurdy, the issues here are purely of an organic nature.
Re organic cases of traumatic psychosis, Lépine sums up the subjective phenomena as follows: There is (a) a cephalea, often a feeling of weight, varying at different times of the day; often frontal; often subject to marked alteration on movement. There may be (b) a number of visual phenomena like those mentioned under Case 355, part and parcel of a sort of absence, suggesting an epileptoid effect. Sometimes (c) there is vertigo, but this is rare. There are also congestive attacks. The patients are unable to work, and have strange head sensations when they attempt to work. The memory disorder is not as a rule markedly accentuated. This amnesia is usually a disordered fixation of current events, but there is also a retrograde amnesia. Insomnia and impulsiveness are also found, and more rarely is a depressed and melancholy state suggesting that which Case 355 exhibited. Lépine has tried to define the traumatic psychoses (not neuroses) on the basis of phenomena found in trephined cases. He remarks upon the extreme analogy, not to say identity, between the late sequelae of trephining and the syndrome of commotio cerebri.
Re organic cases of traumatic psychosis, Lépine summarizes the subjective experiences as follows: There is (a) a headache, often felt as a heaviness, which changes at various times of the day; it's often located in the front and may significantly worsen with movement. There may be (b) several visual disturbances similar to those described under Case 355, which are part of a sort of absence, suggesting an epileptoid effect. Sometimes (c) there is dizziness, but this is rare. Congestive episodes also occur. The patients find themselves unable to work and experience strange sensations in their heads when they try to engage in work. Memory problems typically aren’t severely pronounced. This amnesia usually relates to disorganized recall of recent events, but there is also retrograde amnesia. Insomnia and impulsiveness are also present, and less commonly, a state of depression and melancholy that resembles what Case 355 demonstrated. Lépine has attempted to define traumatic psychoses (not neuroses) based on phenomena observed in trephined cases. He notes the striking similarity, if not outright identity, between the late effects of trephining and the syndrome of commotio cerebri.
Daze with relapses; mutism—following shell fire and corpse work.
Dazed by setbacks; silent—after explosions and dealing with bodies.
Case 356. (Man, June, 1915.)
A soldier lost his voice apparently from two factors: shell fire and the emotional shock of helping to fill the big common graves. The man could never tell for certain (retrograde amnesia) whether he went from corpses to shell fire or from shell fire to corpses.
A soldier lost his voice due to two reasons: artillery fire and the emotional impact of helping to fill the large common graves. He could never be sure (retrograde amnesia) whether he went from the corpses to the artillery fire or from the artillery fire to the corpses.
Several weeks of daze followed in which he hardly reacted to outward stimuli, but occasionally said “It smells!” “Leave me still!”
Several weeks passed in a fog where he barely responded to things around him, but occasionally he would say, “It smells!” “Leave me alone!”
He recovered gradually from the daze. But merely hinting at his experiences, especially the smells, sufficed to throw him into another daze.
He slowly came out of the daze. But just mentioning his experiences, especially the scents, was enough to send him back into another daze.
The loss of voice lasted for some time after he had wholly stopped lapsing into the dazed states.
The loss of voice continued for a while after he completely stopped slipping into those dazed states.
There was some alcohol in the previous history of this case, which is the only case among twenty-three Shell-shock cases reported by Mann which had a psychiatric disorder of any lasting nature due to shell fire.
There was some alcohol involved in the earlier history of this case, which is the only one among the twenty-three Shell-shock cases reported by Mann that had a psychiatric disorder of any lasting nature caused by shell fire.
Re mutism and the two factors of shell fire and emotion spoken of by Mann, compare the views of Babinski to the effect that emotion alone is unable to cause such a hysterical manifestation as mutism.
Re mutism and the two factors of shell fire and emotion mentioned by Mann, compare Babinski's views that emotion alone cannot cause a hysterical manifestation like mutism.
Mine explosion: Mental confusion. Amnesia effected through Y. M. C. A.
Mine explosion: Mental confusion. Amnesia caused through Y. M. C. A.
Case 357. (Wiltshire, June, 1916.)
A sapper, 21, was admitted to a base hospital semi-stuporous, unable to answer questions and mistaking the identity of persons about him. At first he slept, but next day found he was in hospital. His mind was “all of a blur.” He did not remember coming to France; “It all seems a mist.” He felt he was ill and was afraid of becoming insane. There was no physical sign of disease except coarse tremor of hands.
A 21-year-old sapper was admitted to a base hospital in a semi-conscious state, unable to answer questions and confusing the identities of those around him. Initially, he slept, but the next day he realized he was in the hospital. His thoughts were “all a blur.” He didn't remember coming to France; “It all feels like a fog.” He sensed that he was unwell and feared he was losing his sanity. There were no physical signs of illness apart from a noticeable tremor in his hands.
At intervals over a period of about half an hour, helped by questions, he was able to get out the following with much emotion:
At various points over about thirty minutes, with the help of questions, he managed to express the following with a lot of emotion:
“Joe, don’t go—Give me my rifle, Joe—Ten killed. Poor old Taffy—Dreamed last night—Saw Harry Edmands with all his ribs broken—when we had the explosion—5000 bombs or two and a half tons of explosives blew up.—Joe—Clay said he would never live three weeks,—Glasses blown in.—Taffy killed by shell in stomach—S— L— All privates blown off him—Just after leaving workshop.”
“Joe, don’t leave—Give me my rifle, Joe—Ten are dead. Poor old Taffy—Had a dream last night—Saw Harry Edmands with all his ribs broken—when the explosion hit—5000 bombs or two and a half tons of explosives went off.—Joe—Clay said he wouldn’t survive three weeks,—Glasses shattered.—Taffy was killed by a shell in the stomach—S—L—All privates blown off him—Just after leaving the workshop.”
Between the above statements, the patient might go off into short trance states, staring and pointing out of the tent.
Between the statements above, the patient might enter brief trance-like states, staring and pointing outside the tent.
Next day he was found in a condition of cheerful emotion, saying that he was ever so much better; an orderly had “saved him!” This orderly had taken him to the Y. M. C. A. recreation tent, played the piano to him, and made him play himself. His whole emotional state suddenly changed over. He now had a good memory for everything previous to his reaching France, and remembered simply that there had been an explosion. He remembered two names that he had mentioned, but he could remember nothing about their fate in France. He did not know where they were but he was not anxious about them.
The next day, he was found in a cheerful mood, claiming he felt so much better; an orderly had "saved him!" This orderly had taken him to the YMCA recreation tent, played the piano for him, and made him play too. His entire emotional state changed in an instant. He now had a clear memory of everything before he got to France and only recalled that there had been an explosion. He remembered two names he had mentioned, but he couldn’t remember anything about what happened to them in France. He didn’t know where they were, but he wasn’t worried about them.
Shell-shock: Hallucinations; alternations of personality.
Shell shock: Hallucinations; personality changes.
Case 358. (Gaupp, March, 1915.)
A soldier, 29, a helper in a wholesale house, came to a hospital by hospital train, uninjured, directly from the field, having become completely deranged under shell fire. He arrived at the clinic January 11, 1915, in deep emotion, anxiously excited, and looking tensely and suspiciously at the bystanders. He seemed to hear very badly and shouted his statements like a deaf person. Led to the sick section, he shouted out of the window, “Frenchmen!”; then he went willingly to the bath and was put to bed, unresisting. He lay in bed on his elbow, listening in the direction of the window or the wall, answering loud questions with a quick, yelling voice after a pause. He gave his name correctly. He seemed to think he was in the trenches and to see hallucinatory pictures of battle.
A 29-year-old soldier, who worked as a helper in a wholesale store, arrived at the hospital by train, unhurt but completely unstable after experiencing shell fire in the field. He got to the clinic on January 11, 1915, overwhelmed with emotion, anxious, and looking around at the people nearby with tension and suspicion. He seemed to have trouble hearing and shouted his words like someone who was deaf. When taken to the patient area, he yelled out the window, “Frenchmen!”; then he willingly went to take a bath and was put to bed without resistance. He lay in bed on his elbow, listening toward the window or the wall, responding to loud questions with a quick, shouting voice after a moment of pause. He correctly stated his name. It seemed like he believed he was still in the trenches, seeing hallucinatory images of battle.
In the examining room he immediately sat down, back to the wall, taking the chair at the desk and leaning it against the wall. Asked why he did so, he said with a horrified expression, “The shells, they are coming over! Whew! they are shooting all the time.” He ducked, imitating the hissing and whistling of the shells. Asked if he had been struck, he said, “There are two dead and one’s head is off.” He declined to be told where he was, and when he was told that he was no longer in the enemy’s country, but in Württemberg, he said, “No, no; they don’t come so far. No, the Frenchmen don’t come so far.” He was very easily frightened and started at every touch as if wakened from a dream. Sometimes his whole body would tremble with anxiety. He would not allow his pulse to be taken, at first. He would suddenly shout, “That’s the Krupp now flying by. Now it has struck.” He cast his eyes along the ceiling as if to follow the course of the shell. Asked what he was doing, he said he was in the trench on the mountain.
In the examination room, he immediately sat down with his back against the wall, taking the chair at the desk and leaning it against the wall. When asked why he did that, he responded with a horrified look, “The shells are coming over! Whew! They’re shooting all the time.” He ducked down, imitating the hissing and whistling of the shells. When asked if he had been hit, he said, “There are two dead and one’s head is gone.” He wouldn’t let anyone tell him where he was, and when he was informed that he was no longer in enemy territory but in Württemberg, he insisted, “No, no; they don’t come this far. No, the French don’t come this far.” He was very easily startled and jumped at every touch as if he had been pulled from a dream. Sometimes his whole body would shake with anxiety. At first, he wouldn’t let anyone take his pulse. He would suddenly shout, “That’s the Krupp flying by now. Now it has hit.” He looked up at the ceiling as if trying to track the shell’s path. When asked what he was doing, he said he was in the trench on the mountain.
He was able to tell about his family, his marriage in Berlin,[494] and his child, and he could tell time by the clock. Then he would suddenly shout: “The shells, they are shooting everything; they are shooting like another earthquake.” Gaupp stepped up to him, in uniform, and asked if the patient knew him. He examined Gaupp suspiciously from top to toe, looked at the shoulder-straps, and then quickly cried loudly, “Physician.”
He could talk about his family, his marriage in Berlin,[494] and his child, and he could read the time on the clock. Then he would suddenly shout, “The shells, they’re firing everywhere; it’s like another earthquake.” Gaupp walked up to him, wearing his uniform, and asked if the patient recognized him. He examined Gaupp carefully from head to toe, glanced at the shoulder straps, and then quickly shouted, “Doctor.”
At another time he described the shell havoc with evidence of extreme anxiety. He would take food only when one broke off a piece and ate of it before him. He would not drink out of ordinary drinking-glasses but only out of his field cup, examining it carefully. He denied he was on patrol duty at Soupis. His comrade was merely asleep just now. A civilian physician in his long coat was termed by the patient “a baker” after careful examination. There seemed to be no pause in the man’s behavior, which looked absolutely genuine and dominated by strong emotion. He had the look of a man in immediate danger of death, exerting himself to escape shell fire.
At another time, he described the chaos from the shelling with signs of intense anxiety. He would only eat if someone broke off a piece and ate it in front of him. He wouldn’t drink from regular glasses but insisted on using his field cup, checking it thoroughly. He claimed he wasn’t on patrol duty at Soupis. His comrade was just sleeping right now. A civilian doctor in his long coat was called “a baker” by the patient after a careful examination. There seemed to be no letup in the man's behavior, which appeared completely genuine and filled with strong emotion. He looked like a man who was in immediate danger of death, making every effort to escape the shelling.
This dream-like disorder of consciousness with war delirium persisted for a number of days. There was no marked motor excitement. He would remain for the most part quietly in bed, absorbed in his thoughts, watching and listening, sometimes looking about in astonishment but not getting his bearings. Gradually his emotions declined and he developed a certain confidence in the nurse. She was able to convince him that he might be in a hospital, although he objected that there were no wounded there. (He was in a mental section where there were no bandaged men.) All the while he was very hard of hearing and shouted loudly in speech. For twelve days he could not be convinced that he was in Germany. The fact that the Sister was speaking German was met promptly by the fact that in France the physicians and Sisters spoke German too.
This dream-like disorientation caused by war delirium lasted for several days. There wasn’t much physical agitation. He mostly stayed quietly in bed, lost in his thoughts, watching and listening, sometimes looking around in confusion but unable to find his bearings. Gradually, his emotions faded, and he began to trust the nurse. She managed to persuade him that he might be in a hospital, even though he pointed out that there were no injured people there. (He was in a mental ward where there were no bandaged men.) Throughout this time, he was very hard of hearing and spoke loudly. For twelve days, he couldn't be convinced that he was in Germany. The fact that the nurse was speaking German was quickly countered by his belief that in France, doctors and nurses spoke German too.
An extraordinary change came over him January 27 (sixteen days after admission). He went into the garden, apparently deaf and shouting his answers, accompanied by Sister Margarethe, whom he always called “Sister Anna” and whom he thought came from Lichterfelde. While walking[495] with the Sister, his condition suddenly disappeared. He began to hear; he spoke in a normal tone, in fact, rather low, and began to address the Sister by her right name, Margarethe. He was astonished at the snow in the garden, and asked the Sister whether she noticed that the artillery had just stopped firing. Gradually getting his bearings, he wondered whether he had been in the hospital since the day before. He certainly was not ill, he thought.
An incredible change happened to him on January 27 (sixteen days after he was admitted). He went into the garden, seemingly deaf and shouting his responses, with Sister Margarethe, whom he always called “Sister Anna” and mistakenly thought was from Lichterfelde. While walking with the Sister, his condition suddenly lifted. He began to hear; he spoke in a normal tone, in fact, rather softly, and started calling the Sister by her correct name, Margarethe. He was surprised by the snow in the garden and asked the Sister if she had noticed that the artillery had just stopped firing. Slowly regaining his senses, he wondered if he had been in the hospital since the day before. He definitely didn’t feel sick, he thought.
This normal state lasted for a half hour. The patient then relapsed into anxious semi-consciousness, becoming deaf again and shouting his words. During the next few days and weeks he had frequent changes of state like the above described. The changes to a normal state would take place spontaneously in the absence of apparent occasion, but the relapses into semi-consciousness took place when there was some outer irritation, especially some noise. Every fright would cause a relapse. Once a small cannon fired at a great distance off caused such a relapse; again, a sudden shouting at the patient.
This normal state lasted for half an hour. The patient then slipped back into an anxious semi-consciousness, becoming deaf again and shouting his words. Over the next few days and weeks, he experienced frequent changes in his condition as described above. The shifts to a normal state would happen spontaneously without any clear trigger, but relapses into semi-consciousness would occur due to some external irritation, especially noise. Any scare would trigger a relapse. Once, a small cannon fired from far away caused such a relapse; another time, it was a sudden shout directed at the patient.
During the clear state there was a complete amnesia for the period of illness. He did not want to believe that he had been in the hospital for weeks, declaring that he must have been in the trenches two days before.
During the clear state, he had no memory of the time he was sick. He refused to believe he had been in the hospital for weeks, insisting that he must have just been in the trenches two days ago.
Gradually the semi-conscious states decreased in length; the deafness and loud speech returned with the semi-consciousness. With the return of orientation, the man looked entirely normal, speaking in a low voice somewhat shyly. He was rather suspicious and could find his way about with difficulty. His memory broke off with the last days of December, 1914, at which time he was in the trenches under intense shell fire. His wife had received no word from him since December 26. Even at the beginning of February he grew anxiously tense when the word shell was mentioned.
Gradually, the semi-conscious states got shorter; the deafness and loud speech came back along with the semi-consciousness. When he became aware of his surroundings again, the man appeared completely normal, speaking quietly and a bit shyly. He seemed pretty suspicious and had trouble navigating his surroundings. His memories ended with the last days of December 1914, when he was in the trenches under heavy shelling. His wife hadn’t heard from him since December 26. Even at the start of February, he became anxious and tense whenever the word shell was mentioned.
February 4, Gaupp presented him in clinic as entirely clear. He mentioned that his relapses to semi-consciousness occurred on the occasion of a loud noise or word spoken. His face was contorted at Gaupp’s remark but there was no other change in him. The next day, however, he told the Sister that Gaupp had shouted out once to[496] “get him away.” He said he had then heard artillery fire for a moment, but pulled himself together though he had almost gone off, and had a violent headache afterward.
February 4, Gaupp introduced him in the clinic as completely clear. He noted that his relapses into a semi-conscious state happened when there was a loud noise or someone spoke abruptly. His face twisted at Gaupp’s comment, but there was no other change in him. The next day, though, he told the Sister that Gaupp had shouted once to[496] “get him away.” He said he heard artillery fire for a moment but managed to pull himself together, even though he had almost lost it, and ended up with a severe headache afterward.
These states of alternating normality and semi-consciousness continued until about February 10. During a clear spell, the patient was quiet, reserved, taciturn, a little ill-tempered and seclusive, occasionally writing his wife a rather empty letter. In the semi-conscious state he was emotional and restless, seeking cover from the enemy. These states stopped altogether about the middle of February. He then became somewhat more open, though he had no idea of the gravity of his condition. He was angered by the window-bars, and offended by the opening of a letter to his wife, declaring that he would never write a word again, as it was just like a prison. These outbursts passed quickly by. He wanted to go home and believed he would soon be able to go to his comrades in the field.
These phases of alternating normalcy and half-consciousness continued until around February 10. During a clearer period, the patient was quiet, reserved, withdrawn, a bit irritable, and reclusive, occasionally writing his wife a rather lackluster letter. In his semi-conscious state, he was emotional and restless, trying to find shelter from the enemy. These episodes completely stopped around mid-February. He then became somewhat more open, although he had no understanding of the seriousness of his condition. He was frustrated by the barred windows and upset by the fact that a letter to his wife had been opened, declaring that he wouldn't write again since it felt just like being in prison. These outbursts quickly faded. He wanted to go home and believed he would soon be able to rejoin his comrades in the field.
At the time of the report, Gaupp felt that he could not be discharged for a number of weeks. He was pallid, gave the impression of being exhausted mentally, complained of restlessness and internal irritation. His memory gap covered at the end of March a period of about five weeks: from the end of December, 1914, to the beginning of February, 1915.
At the time of the report, Gaupp believed he wouldn’t be discharged for several weeks. He looked pale, seemed mentally exhausted, and expressed feelings of restlessness and internal discomfort. His memory gap at the end of March spanned roughly five weeks: from the end of December 1914 to the beginning of February 1915.
Frostbite; thrown into water by horse; horse shot under its rider who becomes: A HORSE IN THE UNCONSCIOUS.
Frostbite; thrown into water by a horse; horse shot under its rider who becomes: A HORSE IN THE UNCONSCIOUS.
Case 359. (Eder, March, 1916.)
A private in the Royal Engineers, 25, went through Gallipoli without injury and without fears. He was sent to the hospital in Malta, December 18. When observed by Eder, February 7, the frostbitten finger of the right hand was well although there was some loss of grip. He was suffering from insomnia, terrifying dreams, shaky hands. It seems that December 6, a horse started and he was thrown into the water from a bridge. The next day his horse was shot under him. A few days later, a finger was frostbitten. Then his hands began to tremble and the insomnia set in, with severe headaches.
A private in the Royal Engineers, 25, went through Gallipoli without getting hurt and without feeling scared. He was sent to a hospital in Malta on December 18. When Eder checked on him on February 7, his frostbitten finger on his right hand had healed, but he had some loss of grip. He was dealing with insomnia, terrifying dreams, and shaky hands. It seems that on December 6, a horse spooked, and he was thrown into the water from a bridge. The next day, his horse was shot while he was riding it. A few days later, he got frostbite on a finger. After that, his hands started to tremble, he couldn't sleep, and he experienced severe headaches.
This patient was a jovial, thickset, farmer’s son, with a diffuse enlargement of the thyroid gland, a high blood pressure, lymphocytosis, a fine tremor of the hands, irregular and rapid pulse, and anginal attacks. Extremities were cold and blue; the palms perspired markedly; there was hypersensitiveness to sound; there were occasional attacks of dizziness, with a feeling of suffocation; there was frequent desire to micturate.
This patient was a cheerful, stout farmer's son, with a swollen thyroid gland, high blood pressure, an increase in lymphocytes, a slight tremor in his hands, an irregular and rapid heartbeat, and episodes of chest pain. His extremities were cold and blue; his palms were noticeably sweaty; he was very sensitive to sound; he occasionally felt dizzy and had a sensation of suffocation; and he frequently felt the urge to urinate.
The patient’s dream was always the same: He saw a Frenchman digging a knife into his horse, getting off a cart to do this somewhere in Serbia. Occasionally he had this dream in the form of a vision in the daytime. It seems that he had actually seen a French soldier plunge a knife into a mule to make it go. He had been busy with horses since childhood: as stableboy and groom. He thought that the sufferings of the mules in Gallipoli were worse than those of human beings. According to Eder, this farmer’s son was the horse of his dreams; instinctive fear had to emerge; he was pitying himself. According to Eder,[498] “That the person should become a horse in the unconscious would not startle one who has dipped into the totems and taboos of the lower races.”
The patient’s dream was always the same: He saw a Frenchman stabbing his horse with a knife after getting off a cart somewhere in Serbia. Sometimes he experienced this dream as a daytime vision. It seemed like he had actually witnessed a French soldier drive a knife into a mule to make it move. He had been involved with horses since childhood, working as a stable boy and groom. He believed that the suffering of the mules in Gallipoli was worse than that of humans. According to Eder, this farmer’s son represented the horse of his dreams; an instinctive fear had to surface; he was feeling sorry for himself. According to Eder,[498] “It would not surprise someone familiar with the totems and taboos of primitive cultures that a person could become a horse in the unconscious.”
Shell-shock; gassing; fatigue: Anesthesias.
PTSD; chemical exposure; exhaustion: Anesthetics.
Case 360. (Myers, March, 1916.)
A stretcher-bearer, 44, eleven years in the service and two months on French service, was seen by Lt. Col. Myers eight days after reporting sick and admission to a base hospital.
A stretcher-bearer, 44, who had served for eleven years and spent two months in France, was seen by Lt. Col. Myers eight days after he reported sick and was admitted to a base hospital.
While he was under cover in a cellar, three days before reporting sick, a shell had jammed the door and the fumes came in. Later in the day, in another cellar, he had been blown off his seat by a shell and six other men had been laid out. The shelling continued that day and two following days. He had worked on the wounded without any rest.
While he was hiding in a cellar three days before calling in sick, a shell had blocked the door and the fumes started coming in. Later that day, in another cellar, a shell blew him off his seat and six other men were knocked out. The shelling went on that day and for the next two days. He worked on the injured without any breaks.
On lying down he found his left arm numb and cold. The numbness then spread to the legs, especially to the left leg. There was continual tingling in terminal joints of fingers of left hand; hypalgesia over both forearms and hands, especially on left side; total analgesia over left dorsum.
Upon lying down, he noticed that his left arm felt numb and cold. The numbness then spread to his legs, particularly the left leg. There was a constant tingling in the fingertips of his left hand; reduced sensitivity over both forearms and hands, especially on the left side; and complete insensitivity over the back of his left hand.
Two days later, the patient could feel articles and reported that the numbness occurred only in the early morning and was followed by a tingling as the numbness passed off. On the same day, the hands and forearms showed a total loss of sensibility to pain, except for a small area on the flexor surface below the elbow joint.
Two days later, the patient was able to feel things and reported that the numbness happened only in the early morning and was followed by a tingling sensation as the numbness faded. On that same day, the hands and forearms experienced a complete loss of sensitivity to pain, except for a small area on the inner side below the elbow joint.
Re spread of anesthesia and alternation of sensory symptoms in this case. Babinski, of course, believes, that the majority of these conditions are the product of medical suggestion, but Babinski meets any critique by pointing out that any other sort of suggestion may produce such results. The heterosuggestion need not be medical. Thus, the sight of a comrade with paralysis or anesthesia, organic or hysterical, may suggest such to the soldier. Léri remarks that these may also be produced by autosuggestion alone. “From a tired feeling in a limb to a loss of power in it, there is but a small step. Another step leads to paralysis and anesthesia. The neuropathic temperament takes these small steps in perfectly good faith.” Léri has found no case in which he could exclude the influence of auto- or heterosuggestion.
Re spread of anesthesia and changes in sensory symptoms in this case. Babinski, of course, believes that most of these conditions arise from medical suggestion, but he counters any criticism by noting that any type of suggestion can lead to such results. The heterosuggestion doesn’t have to be medical. For example, seeing a fellow soldier with paralysis or anesthesia, whether it’s organic or hysterical, might suggest that possibility to another soldier. Léri notes that these conditions can also be caused by autosuggestion alone. “From feeling tired in a limb to losing power in it, there’s just a small leap. Another leap leads to paralysis and anesthesia. Those with a neuropathic temperament take these small leaps in all sincerity.” Léri has never found a case where he could rule out the effects of auto- or heterosuggestion.
Shell-shock; burial; somnambulistic state: Amnesia. Recovery of memory in hypnosis.
Shell shock; burial; sleepwalking state: Amnesia. Recovery of memory through hypnosis.
Case 361. (Myers, February, 1915.)
A healthy-looking man, with flushed face and large dark eyes with wide pupils, complained of pains in abdomen, back, and limbs, chiefly in knees and ankles, and of visual impairment. This corporal said that his sight had been very indistinct since he was buried, and that if he looked at an electric light, he could see nothing for five minutes afterwards. He was admitted to the Duchess of Westminster’s War Hospital at Touquet, December 11, 1914, having been buried for 48 hours, December 8, when a shell blew in the trench where he lay. He said he could remember nothing until he found himself in a dressing station, lying on straw, in a barn. He was at that time unable to see and fell over something when he tried to walk.
A healthy-looking man with a flushed face and large dark eyes with wide pupils complained of pain in his abdomen, back, and limbs, especially in his knees and ankles, along with vision problems. This soldier mentioned that his eyesight had been very blurry since he was buried, and if he looked at an electric light, he couldn't see anything for five minutes afterward. He was admitted to the Duchess of Westminster’s War Hospital at Touquet on December 11, 1914, after being buried for 48 hours on December 8 when a shell hit the trench where he was lying. He said he couldn’t remember anything until he found himself at a dressing station, lying on straw in a barn. At that time, he was unable to see and tripped over something when he tried to walk.
He had gone out August 13, and had been in the last two days at Mons and then at La Bassée. He had slept badly and had taken a good deal of whiskey. He had led a fast life and had had domestic worries recently.
He went out on August 13 and had spent the last two days at Mons and then at La Bassée. He hadn’t slept well and had drunk a lot of whiskey. He had been living fast and had been dealing with personal issues lately.
It appeared that his vision had improved since the day of the explosion; though he could read for a short time only when things became blurred, and only with the type close to the eyes. Bowels had not opened for five days. Vision in right eye was 5/60; left eye, 2/60.
It seemed like his eyesight had gotten better since the day of the explosion, although he could only read for a short time before things got blurry, and only with the text close to his eyes. He hadn't had a bowel movement in five days. His vision was 5/60 in the right eye and 2/60 in the left eye.
Tested for smell, he failed to smell peppermint, ether, iodin tincture, and carbolic acid 1-40. Sugar was tasted only after tongue movements were permitted, as was also a strong solution of salt. Acid tasted salty like alum. The patient complained that he did not sleep, though in point of fact he slept well.
Tested for smell, he couldn’t detect peppermint, ether, iodine tincture, or a 1-40 solution of carbolic acid. Sugar was tasted only after he was allowed to move his tongue, and the same went for a strong salt solution. The acid tasted salty like alum. The patient claimed he couldn’t sleep, even though he actually slept well.
The patient was treated by suggestion, both in hypnosis and without, when he was transferred on the 31st of December, to the London Temperance Hospital, whence he was discharged. The treatment by suggestion occurred daily. At the second trial and thereafter, light hypnosis was easily[500] induced, but the deeper stages, with hallucinations, anesthesia, and post-hypnotic anesthesia, could not be reached. The lighter stages brought about sleep, a gradual restoration of memory, and later an improvement in visual and olfactory acuity; in near vision, in visual fields, and in color sensibility.
The patient was treated with suggestion, both under hypnosis and without it, when he was transferred on December 31st to the London Temperance Hospital, where he was discharged. The suggestion treatment happened daily. During the second attempt and afterwards, light hypnosis was easily[500] induced, but deeper stages, including hallucinations, anesthesia, and post-hypnotic anesthesia, could not be achieved. The lighter stages resulted in sleep, a gradual recovery of memory, and later improvements in visual and smell sensitivity; in near vision, in visual fields, and in color perception.
The stages in the restoration of memory are as follows: December 22, he was able to describe how he was buried, how Sergeant L. dug him out, how men of another regiment than his own took him to a dressing station, whence he was packed off by the M. O. to the dressing station of his own regiment. Capt. S. had spoken to him and given him a drink. Post-hypnotic suggestion caused him to remember this latter fact after he had come out from hypnosis.
The stages in the restoration of memory are as follows: December 22, he could explain how he was buried, how Sergeant L. dug him out, how soldiers from a different regiment than his own took him to a medical station, from where he was sent by the M. O. to the medical station of his own regiment. Capt. S. had talked to him and gave him a drink. Post-hypnotic suggestion made him recall this last detail after he had come out of hypnosis.
December 23, even before hypnosis, he could remember a big hospital with a stove in the center of a big square room, and gave a fragmentary account of struggling in the trench after being buried, and of going to sleep and enjoying himself at home, when somebody started messing him about. In hypnosis, he gave further details of his dreams after falling asleep in the buried state.
December 23, even before hypnosis, he could remember a large hospital with a stove in the middle of a big square room, and he gave a disjointed account of struggling in the trench after being buried, and of going to sleep and having a good time at home when someone started bothering him. During hypnosis, he provided more details about his dreams after falling asleep while buried.
December 26, further details were remembered before hypnosis, such as a ride in the motor ambulance, offers of tea, cocoa, sweets, and cigarettes, a bad headache, and the like.
December 26, more details came back before hypnosis, like a ride in the ambulance, offers of tea, cocoa, snacks, and cigarettes, a terrible headache, and so on.
December 27, in hypnosis, he was able to describe with apparent accuracy the position of the trenches and their appearance. He said:
December 27, under hypnosis, he was able to accurately describe the layout of the trenches and what they looked like. He said:
“The explosion lifted us up and dropped us again. It seemed as if the ground underneath had been taken away. I was lying on my right side, resting on my right hand, when the shell came. I got my right hand loose but my wrist was fixed behind a piece of fallen timber. At last I dropped off to sleep and had funny dreams of things at home. One thing in particular I have thought of many times since, I have not been able to make out why I should dream of the young lady playing the piano. I don’t know her name and I don’t think I have seen her above twice.”
“The explosion lifted us up and then dropped us down again. It felt like the ground beneath us had vanished. I was lying on my right side, resting on my right hand, when the shell hit. I managed to get my right hand free, but my wrist was stuck behind a piece of fallen timber. Eventually, I fell asleep and had strange dreams about things back home. One thing in particular has stuck with me—I can't figure out why I dreamed about the young woman playing the piano. I don’t know her name, and I don’t think I’ve seen her more than twice.”
According to Myers, it is questionable how far the patient’s memory can be trusted; and there is considerable doubt[501] whether the man had remained in the trench for more than an hour after the shell had burst. A comrade said that the doctors at the barn thought the man off his head. Another soldier, familiar with the positions of the regiments in question, gave information suggesting that the patient had wandered in a somnambulistic state from the trench, past his own dressing station to that of another regiment.
According to Myers, it's uncertain how reliable the patient's memory is; there's a lot of doubt [501] about whether the man actually stayed in the trench for more than an hour after the shell exploded. A comrade mentioned that the doctors at the barn believed the man was out of his mind. Another soldier, who knew the positions of the regiments involved, provided information indicating that the patient had wandered in a sleepwalking state from the trench, past his own dressing station, and to that of another regiment.
Re Shell-shock and burial cases, compare remarks of Grasset and of Foucault concerning the feeling as if dead on the part of certain buried persons. Somnambulism is a natural sequel to such feelings. For somnambulism, compare cases of Milian (364, 365, and 366).
Re Shell-shock and burial cases, look at the comments from Grasset and Foucault about the experience of feeling dead among some buried individuals. Somnambulism often follows these feelings. For somnambulism, refer to the Milian cases (364, 365, and 366).
Shell-shock; minor injuries: Somnambulistic “carrying on”; fatigueability, physical and mental.
Shell shock; minor injuries: Sleepwalking "carrying on"; fatigue, both physical and mental.
Case 362. (Donath, July, 1915.)
A lieutenant of infantry, 31, threw himself down on the earth September 9, 1914, as a shell was passing over him. The shell exploded and seriously injured a soldier one meter away. The lieutenant got up and ran for cover about twenty meters distant. Only six and a half hours later did he perceive that there was a small skin lesion between his thumb and index finger, caused by a shell fragment, as well as a superficial burn on his right temple. Neither wound bled or had to be dressed. He carried on, aware that they were marching toward the River D.; but only two or three days later did he find they had already marched to the other side of K., had rested there and spent the night in various places in between. During this whole period the lieutenant led his battalion and held a piece of woods without anyone’s noticing anything striking about him. These dazed states were twice repeated, for periods of ten and twenty-four hours respectively, and finally he was brought behind the firing lines unconscious.
A 31-year-old infantry lieutenant lay down on the ground on September 9, 1914, as a shell flew overhead. The shell exploded and seriously injured a soldier just a meter away. The lieutenant got up and ran for cover about twenty meters away. It wasn't until six and a half hours later that he noticed a small skin lesion between his thumb and index finger from a shell fragment, as well as a superficial burn on his right temple. Neither injury bled or needed dressing. He continued on, knowing they were marching toward the River D., but only two or three days later did he realize they had already crossed to the other side of K., rested there, and spent the night in various spots along the way. Throughout this entire time, the lieutenant led his battalion and held a patch of woods without anyone noticing anything unusual about him. He experienced states of confusion twice more, lasting ten and twenty-four hours respectively, before he was finally brought behind the firing lines unconscious.
The physician found him to be in a state of exhaustion, pulse 108, and had him brought to the nearest station. There Donath found increased tendon reflexes, some dermatographia and increased fatigueability of mind and body. He was especially fatigued by walking, though he had always been a good mountain climber. He was now unable to concentrate on reading, writing or calculating, though he had been accustomed to dictate letters and calculations in his official work in peace times. He had seizures of crying and trembling on September 10 and October 27, both quieted by bromides. There was diminution of sexual power.
The doctor found him to be extremely exhausted, with a pulse of 108, and had him taken to the nearest clinic. There, Donath noticed that his tendon reflexes were heightened, he showed some skin sensitivity, and he was experiencing increased fatigue in both mind and body. He was particularly worn out from walking, even though he had always been a good hiker. He was now unable to focus on reading, writing, or doing calculations, despite being used to dictating letters and calculations in his official work during peacetime. He experienced episodes of crying and shaking on September 10 and October 27, both of which were alleviated by bromides. His sexual ability had noticeably decreased.
Rest, lukewarm baths, cold compresses to the head, and psychotherapy improved his status rapidly.
Rest, warm baths, cold compresses on the head, and therapy quickly improved his condition.
This patient had never been epileptic or hysterical, subject to dazed states of any sort, was weak, delicate and anemic (three sisters leukemic), but had before the war been well.
This patient had never had epilepsy or hysteria, experienced any kind of dazed states, was weak, delicate, and anemic (three sisters with leukemia), but had been healthy before the war.
Emotion of captain who saw men burned by bomb: Stupor “as if dead”; awakening “as if a German prisoner.” Recovery.
Emotion of the captain who saw men burned by the bomb: Stunned “as if dead”; coming to “as if a German prisoner.” Recovery.
Case 363. (Régis, May, 1915.)
A captain, one day seeing some of his men hit by incendiary bombs, felt the deepest kind of emotion. He threw his coat over one of his men and succeeded in smothering the fire. Of a sudden, he completely lost consciousness, only regaining contact with the outer world two days later, in the sanitary train. He did not know where he was, but thought himself a prisoner surrounded by Germans. The disorder of consciousness lasted three days, and the memory of what happened during those days never returned. In fact, the captain declared that he felt as if he had been dead during that time. His dreamlike state lasted for some time, and for several weeks he did not sleep without disturbing nightmares. It was always the same night attack, with the burned men and the anguish of feeling that his men were not about him and that he was alone in the skirmish. He later recovered entirely and made preparations to start for the front.
A captain, one day witnessing some of his men caught in incendiary bombs, felt a deep emotional impact. He threw his coat over one of his men and managed to put out the flames. Suddenly, he completely lost consciousness, only coming back to reality two days later in the medical train. He had no idea where he was and thought he was a prisoner surrounded by Germans. This state of confusion lasted three days, and the memories of what happened during that time never came back. In fact, the captain said he felt as if he had been dead during those days. His dreamlike state continued for a while, and for several weeks, he couldn’t sleep without being plagued by nightmares. It was always the same night attack, with burned men and the fear of knowing that his men were not with him and that he was alone in the battle. He eventually fully recovered and began preparing to return to the front.
Re feelings “as if dead,” see remarks of Régis under Case 293.
Re feelings “like they’re dead,” see Régis’s comments under Case 293.
Emotions over battle scenes: Spontaneous hypnosis or SOMNAMBULISM lasting twenty-four days.
Emotions about battle scenes: Spontaneous hypnosis or sleepwalking lasting twenty-four days.
Case 364. (Milano, January, 1915.)
Upon recovery from a state of apparent hypnosis described below, the victim wrote, in part, as follows:
Upon waking from what seemed like hypnosis, the victim wrote, in part, as follows:
“After marching two days we reached a Breton village near Virtou. Next day we were in a battle that lasted from seven in the morning to eight in the evening. I was somewhat troubled by the first balls and bullets that whistled by, but felt I had to get used to them and we marched on, under our brave captain’s orders. Then we really got under fire. It was sad to see my comrades falling under the murderous bullets, and the captain was soon mortally wounded; but we had reinforcements and went on and chased the enemy from his positions. During the battle I kept thinking of my old mother and father and I felt that I should die without seeing them again. Little things about the family came to my mind. I saw my father’s roof, and his favorite garden seat, and I saw my mother weeping over her only son, her only ambition in old age. The return from the battle was very sad for me. Night began to fall on the frightful field. I saw on the bare earth the bodies of poor comrades whose joys and sorrows I had shared. There they were, cut down in all the strength of youth, leaving their parents in trouble, their widows in despair, and their poor orphans. I wanted to carry them off and I could not. We had to march over their glorious remains. I was able to give a word of encouragement to one of my comrades who now probably is no more. We then retired. Although I was very weary, I was unable to get any rest. My mind was occupied with the frightful things I had seen. I thought of the comrades over there and that no one could help them. I remember I drank coffee the next morning and talked with my relative. Then that is all. From that time I do not know what happened.”
“After marching for two days, we reached a Breton village near Virtou. The next day, we were in a battle that lasted from seven in the morning until eight in the evening. I felt a bit anxious when the first shots and bullets whizzed by, but I knew I had to adjust, so we continued marching under our brave captain’s orders. Then we really came under fire. It was heartbreaking to see my comrades falling to the deadly bullets, and the captain was soon mortally wounded; but we received reinforcements and pressed on, driving the enemy from their positions. During the battle, I kept thinking about my old mother and father, fearing I would die without seeing them again. Little memories of home flooded my mind. I pictured my father’s roof, his favorite garden seat, and I saw my mother crying for her only son, her only hope as she aged. Coming back from the battle was very sad for me. Night began to fall over the terrible field. I saw the bodies of my dear comrades lying on the bare earth, their joys and sorrows intertwined with mine. They were cut down in their youthful prime, leaving their parents in distress, their widows in despair, and their poor orphans. I wanted to carry them away, but I couldn’t. We had to march over their glorious remains. I managed to offer a word of encouragement to one of my comrades, who is probably gone now. We then retreated. Even though I was extremely tired, I couldn’t rest. My mind was filled with the horrific things I had witnessed. I thought about my comrades left behind and how no one could help them. I remember drinking coffee the next morning and talking with my relative. After that, I can’t recall what happened.”
The writer was an infantryman, 20, who had been employed in civil life in the Crédit Lyonnais, and was brought August 24, 1914, to the Saint Nicolas Hospital in a state of hypnosis.
The writer was a 20-year-old infantryman who had worked at Crédit Lyonnais in civilian life and was brought to Saint Nicolas Hospital on August 24, 1914, in a state of hypnosis.
Once placed in the standing position he kept balancing back and forth, with head motionless, eyes fixed and directed to the left side. He did not speak in reply to a request for his name or facts about his life, but as soon as the battle was talked of he began an expressive pantomime, speaking in a very low voice a few words interrupted by sighs. “What were you doing in the fight?” He extended his arms, described a half circle with his hand, as if to show the extent of the field, thrust his hands forward with a finger outstretched, saying, “Zi, zi,” as if to indicate whistling bullets; plunged forward with hands in front of his chest, as if holding a gun in charge bayonet position, saying “Prussians, Prussians,” and threw himself down in a kneeling posture, saying, “Trenches, trenches.” “Do you remember the battle?” “Belgium, Belgium. Germans pushed back,” making a sign as if chasing them. “Captain dead. Two hundred men dead.” With a suitable gesture he sighed, and tears ran down his face.
Once he was set in a standing position, he kept swaying back and forth, his head still, eyes fixed and directed to the left. He didn't respond when asked for his name or details about his life, but as soon as they mentioned the battle, he started an expressive pantomime, speaking in a very quiet voice with a few words interrupted by sighs. “What were you doing in the fight?” He stretched out his arms and made a half-circle with his hand to show the extent of the battlefield, thrusting his hands forward with a finger pointed out, saying, “Zi, zi,” as if to indicate whistling bullets; he lunged forward with his hands in front of his chest, as if he were holding a gun in a charge bayonet position, saying “Prussians, Prussians,” and then dropped to his knees, saying, “Trenches, trenches.” “Do you remember the battle?” “Belgium, Belgium. Germans pushed back,” making a sign as if he were chasing them. “Captain dead. Two hundred men dead.” With a fitting gesture, he sighed, and tears ran down his face.
August 28 the mutism was still almost complete, but he could say his name and lay stretched out on the bed.
August 28, the mutism was still nearly total, but he could say his name and lay stretched out on the bed.
September 4 the hypnosis was less, but the delirious state was more active. He got up in the night and tried to escape to help the wounded. In the daytime, if he saw a man lying down resting he went to him and unbuttoned his coat to see whether he was wounded. Upon seeing the physician he would cry, “Major! Wounded! wounded!” and then pull the physician by his coat. He could hardly be stopped from these maneuvers. He had to be fed like a child, but went alone to stool.
September 4, the hypnosis was less intense, but the delirious state was more pronounced. He got up during the night and tried to escape to help the injured. During the day, if he saw a man lying down resting, he went to him and unbuttoned his coat to check for wounds. Upon seeing the doctor, he would shout, “Major! Wounded! Wounded!” and then tug at the doctor's coat. It was hard to stop him from these actions. He had to be fed like a child but managed to go to the bathroom on his own.
He began to be employed about the hospital a little September 14, in sweeping the room and in guarding another patient in complete somnambulism, over whom he watched as over a child, leading him by the hand and keeping him from bumping into objects.
He started working at the hospital around September 14, sweeping the room and watching over another patient who was completely sleepwalking. He looked after him like a child, guiding him by the hand and preventing him from running into things.
September 16 he awoke suddenly. Some one had talked to him about his own village and his relatives. He was astonished to find himself in a hospital. He wrote out, on request, the above account of his recollections. The man was 177 cm. tall, well proportioned; showed a slight facial asymmetry and a few other facial features of a dystrophic nature, such as an adenoid appearance. There was no stigma of hysteria.
September 16, he woke up suddenly. Someone had talked to him about his village and his relatives. He was shocked to find himself in a hospital. He wrote down, upon request, the account of his memories above. The man was 177 cm tall, well proportioned; he had slight facial asymmetry and a few other facial features that looked dystrophic, like an adenoid appearance. There was no sign of hysteria.
Putative loss of brother nearby in battle: Spontaneous hypnosis or somnambulism; mutism, except “Mamma, Mamma.” Sudden awakening after twenty-seven days.
Putative loss of a brother nearby in battle: Spontaneous hypnosis or sleepwalking; inability to speak, except for “Mom, Mom.” Sudden awakening after twenty-seven days.
Case 365. (Milian, January, 1915.)
A man, 22, was brought to the Saint Nicolas Hospital in a sort of coma August 24, 1914. He lay on the bed, eyes closed as if asleep, insensible to excitation, irresponsive. Flies crawled upon him with impunity. He did not wink. The arms raised fell back inert. The corneal reflex was absent on the left side, diminished on the right. The knee-jerks and the skin reflexes were normal.
A 22-year-old man was taken to Saint Nicolas Hospital in a kind of coma on August 24, 1914. He lay in bed, eyes closed as if asleep, unresponsive to stimulation. Flies crawled over him without resistance. He didn't blink. His arms, when raised, fell back down limply. The corneal reflex was absent on the left side and diminished on the right. The knee-jerk reflexes and skin reflexes were normal.
Next day he had to be fed like a child and looked after. Lifted from bed, once on the ground he stood up with flexed legs, as if to crouch. It seemed as if he was about to fall, but he did not.
The next day he needed to be fed like a kid and taken care of. When he was lifted from the bed and placed on the ground, he stood up with his legs bent, almost like he was about to crouch. It looked like he was going to fall, but he didn’t.
The next day he was in the same immobile state. Upon removal from bed he again made as if to fall, but got his balance. He kept his legs flexed, his head lowered in a fixed posture, with his eyes on the ground. He would walk quickly without falling, if taken by the hand, feet dragging, and even holding back with a certain amount of force. His walk suggested that of a somnambulist. He was left in a standing posture by his bed throughout the medical visit. After a few minutes he began to flex his legs progressively and slowly. The attendant cried out, “He is going to fall.” Instead of falling, he sat down upon the floor near the bed. He was in the same immobile, somnolent state September 1, eyes half open, hidden under long lashes. Flies walked over his eyes and lids, but he did not wink. He would rise only when pushed and walk only when pulled, but had begun to eat a little better. To all questions he replied, from between his teeth, “Mamma. Mamma.”
The next day, he was still in the same frozen state. When he was taken out of bed, he again seemed like he would fall but managed to steady himself. He kept his legs bent and his head lowered in a fixed position, staring at the ground. He could walk quickly without falling if someone held his hand, his feet dragging, and even resisting with some force. His walking resembled that of a sleepwalker. During the medical visit, he was left standing by his bed. After a few minutes, he started to slowly and gradually bend his legs. The attendant shouted, “He’s going to fall.” Instead of falling, he sat down on the floor near the bed. He was in the same motionless, sleepy state on September 1, his eyes half open and hidden under long eyelashes. Flies crawled over his eyes and eyelids, but he didn’t blink. He would only stand if pushed and walk only if pulled, but he had started to eat a little better. To all questions, he replied, through clenched teeth, “Mamma. Mamma.”
The next day there was a bit more spontaneity in his walking.
The next day, he walked with a bit more spontaneity.
Lumbar puncture showed a slight hypertension. There were traces of albumin and very few lymphocytes.
Lumbar puncture revealed slight high blood pressure. There were traces of albumin and only a few lymphocytes.
September 6, he was able to eat soup alone, but kept the same immobile posture, with eyes fixed on the ground, eyelids not winking, in a posture suggesting Parkinson’s disease, but without rigidity. He still replied only, “Mamma. Mamma.”
September 6, he could eat soup by himself, but he maintained the same still position, staring at the ground, his eyelids not blinking, in a stance that suggested Parkinson’s disease, but without stiffness. He still only responded with, “Mamma. Mamma.”
September 19 the patient suddenly waked up completely. Douches and external irritations had not served to wake him up, but a soldier told him upon this day that his brother was not dead, as he believed, but was alive and he then began to speak, opened his eyes, and began to talk. He told how he had been by the side of his brother in battle. Germans had taken them in the flank and opened machine guns upon them. Two men had fallen by his side, and, catching at his garments, kept him from retiring when the order was given. He got loose, looked for his brother among the corpses, could not find him, thought him dead, and from that point forward had been without memory. He shortly became perfectly normal.
On September 19, the patient suddenly woke up completely. Neither showers nor external stimuli had managed to rouse him, but on this day, a soldier told him that his brother, whom he believed was dead, was actually alive. Hearing this, he began to speak, opened his eyes, and started talking. He recounted how he had been beside his brother during battle. The Germans had attacked them from the side and opened fire with machine guns. Two men fell beside him, and as they grabbed onto his clothes, they prevented him from retreating when the order was given. He broke free, searched for his brother among the bodies, couldn't find him, thought he was dead, and from that moment on, had lost his memory. Soon after, he returned to a completely normal state.
Shell-shock; slight trauma; windage felt; fall; loss of consciousness; wandering, conscious, over night; shrapnel burst: Spontaneous hypnosis or somnambulism, lasting four days. Return to the corps.
Shell shock; minor trauma; wind drift felt; fall; loss of consciousness; wandering, aware, overnight; shrapnel explosion: Spontaneous hypnosis or sleepwalking, lasting four days. Return to the unit.
Case 366. (Milian, January, 1915.)
An infantryman, 20, boxer by profession, was brought with other wounded, in the night, to Saint Nicolas Hospital and was seen next morning, August 24, in bed, lying motionless on his back, eyes open, fixed, eyelids not winking. No reply was got to questions. The arm lifted fell back upon the bed, although slowly and not heavily as in apoplexy. There was no catalepsy. The patient was taken from his bed and put upright. In this position he remained immobile, hands at side, head bent forward, eyes fixed on the ground. The eyelids did not move upon approach of the finger or a lighted candle, unless there was a fine beginning of movement. If he was pushed, he made two or three steps forward, with eyes fixed on the ground and head bent forward. The only spontaneous movement was carrying the left hand back to the side as if to take the bayonet. He got into bed alone.
An infantryman, 20, who was a boxer, was brought in with other injured people during the night to Saint Nicolas Hospital and was found the next morning, August 24, lying motionless on his back in bed, eyes open and staring, eyelids not blinking. There was no response to questions. When his arm was lifted, it fell back onto the bed, though it was a slow and light movement, not like a stroke. There was no catalepsy. The patient was taken from his bed and set upright. In this position, he remained still, hands at his sides, head bent forward, eyes fixed on the ground. His eyelids didn’t move when someone approached with a finger or a lit candle, except for a slight hint of movement. If he was nudged, he would take two or three steps forward, still keeping his eyes on the ground and his head down. The only spontaneous movement was bringing his left hand back to his side as if to grab the bayonet. He got back into bed by himself.
Next day the patient could walk better and began to talk, but preserved the same absorbed attitude. He told, in monotonous voice, of the shells that his squad had received and of the dead that he saw about him. August 27 he woke up and was unable to tell how he had come to the hospital. He told how the regiment had been bombarded for a time and how a shell burst near him; how he got a splinter in the buttock (of which the contusion was still visible); and how he had been thrown down by the windage of the shell. His sack had been torn from his shoulders. He had lost consciousness, he thought, for a short time, anyhow he could not find his regiment. He passed the night near Longuyon and next day looked for his regiment again. Shrapnel burst near him, and from that time forward he had lost memory. August 27, at his express request, he started back for his corps. There was no stigma of degeneration or hysteria.
The next day, the patient could walk better and started to talk, but he still had the same distant demeanor. He spoke in a monotone about the shells his squad had endured and the dead bodies he saw around him. On August 27, he woke up and couldn’t remember how he ended up in the hospital. He described how the regiment was bombarded for a while and how a shell exploded nearby; he got a splinter in his buttock (the bruise was still visible) and was knocked down by the shell’s blast. His bag had been ripped off his shoulders. He thought he lost consciousness, but he wasn’t sure how long it lasted; he just couldn’t find his regiment afterward. He spent the night near Longuyon and tried to locate his regiment again the next day. A shrapnel round exploded nearby, and from that moment on, his memory was gone. On August 27, at his direct request, he went back to his corps. There was no sign of degeneration or hysteria.
Burial; struck in head by beam; overcome by gas: Tremors, convulsive movements, confusion, flight toward enemy.
Burial; hit in the head by a beam; suffocated by gas: Shaking, convulsive movements, confusion, running toward the enemy.
Case 367. (Advice, 1916.)
An Italian private, 28, of meager build (infantile eclampsia; brother epileptic) was buried by a shell explosion and overcome by gas. After a month’s leave he went back to the trenches.
An Italian private, 28, with a slight build (childhood eclampsia; brother with epilepsy) was buried by a shell blast and affected by gas. After a month's leave, he returned to the trenches.
But now, whenever a shell burst, he fell into irresistible terror and made convulsive movements which he forgot afterwards. He could not sleep. The mere memory of the scene would throw him into terror. He was tremulous, developed asymmetrical innervation of his face, was generally hypesthetic and mentally blocked.
But now, every time a shell exploded, he was overwhelmed with fear and made jerky movements he couldn't recall later. He couldn’t sleep. Just remembering the scene would send him into a panic. He was shaky, his face showed uneven nerve activity, he felt numb overall, and his mind was foggy.
In the midst of convulsive tremors he fled towards the enemy. He was stopped and brought back, and remained for two days confused and hallucinated.
In the middle of shaking spasms, he ran towards the enemy. He was stopped and brought back, and for two days, he was confused and hallucinating.
In the original accident he had been struck in the head by a beam.
In the original accident, he had been hit in the head by a beam.
Re this Italian’s flight toward the enemy, see various cases of fugue. Clinically and medico-legally, Roussy and Lhermitte remark that these confusional escapades are of great interest, and that many cases are encountered near the front line, put under trial by court-martial, and handed over to specialists. The dream is being lived through. Such a case as this of Consiglio recalls the hystero-emotional psychoses of Claude, Dide, and Lejonne. The relation of oniric delirium to mental confusion is still a matter of polemic. According to Régis, however, the common oniric delirium of toxic or infectious origin is nothing more than a sort of somnambulism. The retrograde amnesia which follows toxic delirium is the same in principle as that which follows hysterical delirium. Régis pointed out that suggestive hypnosis could bring back the memories in both types of disease, as well as from the toxic delirium as from the hysterical somnambulism. However, the differential diagnosis between onirism and hysteria is not easy. Alcoholism and actual brain trauma need to be excluded.
Re this Italian’s flight toward the enemy, see various cases of fugue. Clinically and legally, Roussy and Lhermitte note that these confusing escapades are quite significant, and that many cases are found near the front lines, put on trial by court-martial, and referred to specialists. The dream is being experienced. A case like that of Consiglio reminds us of the hystero-emotional psychoses of Claude, Dide, and Lejonne. The connection between oniric delirium and mental confusion is still a topic of debate. However, according to Régis, the common oniric delirium of toxic or infectious origin is just a form of sleepwalking. The retrograde amnesia that follows toxic delirium is essentially the same as that which follows hysterical delirium. Régis noted that suggestive hypnosis could recover memories in both types of disorders, whether from toxic delirium or hysterical sleepwalking. However, distinguishing between onirism and hysteria is not straightforward. Alcoholism and actual brain injury need to be ruled out.
Shell-shock; windage; unconsciousness: Carried on with fugue tendencies. Variety of hysterical symptoms. Fit for garrison duty four months from explosion.
Shell shock; wind drift; unconsciousness: Continued with dissociative tendencies. A range of hysterical symptoms. Ready for garrison duty four months after the explosion.
Case 368. (Binswanger, July, 1915.)
A non-commissioned officer, 22, entered service at 20, went into the artillery and had been advanced repeatedly. There was no heredity; the man had been a moderately good scholar. It appears that he had had at 17 a febrile angina with delirium.
A non-commissioned officer, 22, joined the service at 20, went into artillery, and had been promoted several times. There was no family background in the military; he had been an average student. It seems that he had a severe throat infection with fever and delirium when he was 17.
September 25, 1914, a big shell load for a cannon was exploded by the enemy. All the men about the cannon were thrown to the ground by air pressure, and the officer became unconscious. On awaking, he had headache, dizziness, and vomiting. There were many corpses lying about him.
September 25, 1914, a large shell loaded into a cannon was detonated by the enemy. All the men near the cannon were thrown to the ground by the blast, and the officer lost consciousness. When he woke up, he had a headache, felt dizzy, and was vomiting. There were many bodies lying around him.
He resumed work at once, but in the evening his headache and dizziness increased and there was “a feeling inside as if he had to run away.” This feeling appeared to come from the heart; it was an oppressive feeling, running to the head. On the next day he did gun duty, noticing, however, that every shot he fired caused him a sharp pain. He was relieved from work at 11 A.M., and was declared ill by the physician. His comrades told him that he had often been noticed trying to run away, but about this he himself declared he knew nothing.
He went back to work immediately, but by evening, his headache and dizziness got worse, and he felt an overwhelming urge to escape. This feeling seemed to come from his heart; it was heavy and spread to his head. The next day, he did his gun duty, but he noticed that every shot he fired caused him sharp pain. He was let off work at 11 a.m. and the doctor declared him ill. His comrades mentioned that they had often seen him trying to get away, but he said he had no idea about it.
He was received at the Jena Hospital, October 9, 1914, a very strongly built and well-nourished man. Neurologically, he showed a marked dermatographia; knee-jerks were obtainable only on reinforcement; Achilles jerks somewhat more marked; there was a weakly positive Oppenheim reflex. The abdominal reflex on the left side was greater than that on the right; and this was also true of the cremaster reflex. Percussion of the head was extremely painful; and there were painful points on pressure of the spine and head.
He was admitted to the Jena Hospital on October 9, 1914, as a very strong and well-nourished man. Neurologically, he displayed significant dermatographia; knee-jerks were only present with reinforcement; Achilles reflexes were somewhat more pronounced; there was a weakly positive Oppenheim reflex. The abdominal reflex on the left side was stronger than on the right, and the same applied to the cremaster reflex. Tapping on the head was extremely painful, and there were painful spots when pressing on the spine and head.
Touch was poor on the entire left side of the body; but there was no diminution of sensibility to pain. There was[511] a fine static tremor of the hands. The strength of both hands appeared to be decreased (dynamometer). Gait was unsteady and stiff; Romberg sign was positive; the patient fell over backward. Hearing was greatly diminished, ordinary speech being heard only close to the ear.
Touch was weak on the entire left side of the body, but there was no decrease in the ability to feel pain. There was a slight shaking in the hands. The strength of both hands seemed reduced (dynamometer). The walking was unsteady and stiff; the Romberg sign was positive; the patient fell over backward. Hearing was significantly impaired, with normal speech only audible when close to the ear.
Toward evening of the second day after admission, there was a marked attack of dizziness while the patient was lying on his back in bed. During this attack the face was very red. It lasted two or three minutes. Hearing was remarkably improved on the left side for some time after the attack. The ear clinic examination, October 19, showed much disturbance of hearing on the right side (direct injury of the vestibular apparatus in both ears).
Toward the evening of the second day after admission, the patient experienced a significant bout of dizziness while lying on his back in bed. During this episode, his face turned very red. It lasted for two to three minutes. His hearing on the left side improved noticeably for a while after the attack. The ear clinic examination on October 19 revealed considerable hearing disturbance on the right side (direct injury to the vestibular apparatus in both ears).
Headaches continued, radiating from the orbit to the top of the head, and sensitiveness to pressure at the exit point of the upper branch of the right trigeminal. The whole of the forehead was somewhat red and swollen (neuralgia of the frontalis). The patient wore dark goggles on account of his marked photophobia.
Headaches kept happening, stretching from around the eyes to the top of the head, with tenderness to pressure where the upper branch of the right trigeminal nerve exits. The entire forehead was a bit red and swollen (frontal neuralgia). The patient wore dark sunglasses due to his significant sensitivity to light.
Improvement was gradual; there was a transient slight swelling and a venous hyperemia of the nasal mucosa, which was treated in the nose clinic. The impairment of hearing was quite gone in two months’ time, though buzzing was now and then heard in the right ear. The supersensitiveness in the right upper trigeminal region vanished also. The patient was discharged January 21, 1915, fit for garrison duty. Later he went into the field again.
Improvement was gradual; there was a temporary slight swelling and increased blood flow in the nasal mucosa, which was treated at the nose clinic. The hearing loss was completely gone in two months, although occasional buzzing was still heard in the right ear. The sensitivity in the right upper trigeminal area also disappeared. The patient was discharged on January 21, 1915, fit for garrison duty. Later, he returned to the field again.
Burial: Dissociation of personality.
Burial: Separation of personality.
Case 369. (Feiling, July, 1915.)
The following are some stories told by a “lost personality” under hypnosis.
The following are some stories shared by a “lost personality” during hypnosis.
The patient, aged 24, was a bandsman in the Second Battalion Wiltshire Regiment, who sometime near the end of October 1914, was buried in a trench near Ypres. This is his account:
The 24-year-old patient was a musician in the Second Battalion Wiltshire Regiment, who was buried in a trench near Ypres sometime around the end of October 1914. This is his account:
“I was dug out at night and taken to a dressing station; it was cold and dark. Then I went on to a hospital at Ypres; it was really a convent, and there were a lot of nuns about, dressed in dark robes with white hats; some of them spoke English. I stopped there for a night and a day. There were a lot of wounded there. Then I was sent on by train; I lay down all the way on a seat in the carriage; we took the whole day to get to ——, and kept on stopping at stations. I was at —— about ten days; I don’t know what hospital it was, but there were English doctors and nurses. It was near the harbor. We came over to England in a hospital ship, the Arethusa; I went straight on to Manchester by train. The hospital there was really a school turned into a hospital.”
“I was dug out at night and taken to a dressing station; it was cold and dark. Then I went to a hospital in Ypres; it was actually a convent, and there were a lot of nuns around, dressed in dark robes with white hats; some of them spoke English. I stayed there for a night and a day. There were many wounded people there. Then I was sent on by train; I lay down the entire trip on a seat in the carriage; it took us all day to get to ——, and we kept stopping at stations. I was at —— for about ten days; I don’t know what hospital it was, but there were English doctors and nurses. It was near the harbor. We came over to England on a hospital ship, the Arethusa; I went straight to Manchester by train. The hospital there was really a school that had been turned into a hospital.”
Here is a brief account of a scrap with some Uhlans.
Here’s a quick story about a skirmish with some Uhlans.
Q. Did you see any Uhlans? Yes.
Q. Did you see any Uhlans? Yes.
Q. What are they like? They’ve got no guts. One time 30 of them were against 8 of us infantry, and they “done a bunk.” Their horses were not bad. They wore helmets with a double eagle on the front.
Q. What are they like? They’ve got no guts. One time 30 of them were against 8 of us infantry, and they “took off.” Their horses were pretty good. They wore helmets with a double eagle on the front.
He was asked to describe the country round the trenches and to give some account of the fighting there:
He was asked to describe the area around the trenches and to provide an account of the fighting there:
“It’s agricultural land, ploughed fields. There were two farms in front of us. One day we saw an old cow between our trenches and the Germans, and we all had pot shots at it. Once the Germans rushed our trenches; we killed hundreds, bayoneted them mostly, and hit them over the heads with the butts of our rifles. It was hellish. The British were all shouting. I saw a German officer behind with a sword and a revolver. I saw a lot of French soldiers, too; they wore long coats with the corners turned back; some had blue and some had red trousers. The French dragoons are like Life Guards, with big steel breastplates and brass helmets with a long plume; they carried swords and rifles and a few had lances.”
“It’s farmland, with plowed fields. There were two farms in front of us. One day, we spotted an old cow between our trenches and the Germans, and we all took shots at it. Once, the Germans charged our trenches; we took out hundreds, mostly with bayonets, and hit them over the heads with the butts of our rifles. It was chaotic. The British were all shouting. I saw a German officer behind us with a sword and a revolver. I also saw a lot of French soldiers; they wore long coats with the corners turned back; some had blue trousers and some had red. The French dragoons are like the Life Guards, with big steel breastplates and brass helmets with a long plume; they carried swords and rifles, and a few had lances.”
He was asked to mention some of his impressions in Belgium and what he thought of the manners and customs of the French and Belgians.
He was asked to share some of his impressions from Belgium and what he thought about the manners and customs of the French and Belgians.
“We cut off all our buttons and gave them to the French girls. The French cigarettes are muck; you buy them in little blue packets; the tobacco is rather dark and strong. When we bivouacked on the march at night we were not allowed any lights, but you could smoke by digging a hole in the ground with your bayonet and smoking into that.”
“We took off all our buttons and gave them to the French girls. The French cigarettes are terrible; you get them in little blue packets; the tobacco is pretty dark and strong. When we set up camp during the night march, we weren’t allowed to use any lights, but you could smoke by digging a hole in the ground with your bayonet and smoking into that.”
The following are some of his remarks about his stay at Gibraltar.
The following are some of his comments about his time at Gibraltar.
“Gibraltar’s like a great big rock; the steep side looks toward Spain. I was in barracks there, and used to spend a lot of time in the band-room practicing. Sometimes we bathed in the sea. I went to Spain two or three times and saw some bull-fights; they were very exciting, but rather too cruel for my taste. They used to kill six or seven bulls a day. The horses got fearfully cut about.”
“Gibraltar is like a huge rock; the steep side faces Spain. I was stationed there and spent a lot of time practicing in the band room. Sometimes we swam in the sea. I went to Spain a couple of times and saw some bullfights; they were really exciting, but a bit too cruel for me. They would kill six or seven bulls a day. The horses were pretty badly hurt.”
This bandsman showed what Feiling calls dissociation of personality. There was an amnesia of such degree that all conscious memories of the patient’s life, as well as all memory of letters, objects, and life in general, were suppressed. The patient was brought, after the burial above noted, to the hospital for epilepsy and paralysis at Maida Vale, January 21, 1915. After his experience, he had been transferred to the Second Western General Hospital, Manchester, where he spoke sensibly, understood and was able to remember things since the burial. His mind was a complete blank for all previous experience. He was unable to recognize his own father or relatives. He was slightly deaf for a time but this defect disappeared.
This musician demonstrated what Feiling refers to as dissociation of personality. There was a level of amnesia that completely suppressed all conscious memories of the patient’s life, as well as memories of letters, objects, and life in general. The patient was taken to the hospital for epilepsy and paralysis at Maida Vale on January 21, 1915, after the burial mentioned earlier. Following his experience, he was moved to the Second Western General Hospital in Manchester, where he spoke logically, understood, and was able to recall things since the burial. His mind was a total blank regarding any past experiences. He could not recognize his own father or relatives. He was slightly deaf for a while, but that issue eventually went away.
At Maida Vale he showed a nervous twitching of eyelids and facial muscles; otherwise he was neurologically and[514] physically normal, dreamless, without complaints, and straightforward about all experiences since coming to himself in the hospital at Manchester. He took his parents on trust. “I don’t know if I ever went to school.” “A bayonet is like a knife; you see soldiers with them on their rifles. I have never seen a bullet.” His memory for recent events was also not good. He once recognized a single tune played at a concert.
At Maida Vale, he showed a nervous twitching of his eyelids and facial muscles; other than that, he was neurologically and[514] physically normal, dreamless, without complaints, and honest about all his experiences since waking up in the hospital in Manchester. He trusted his parents. “I don’t know if I ever went to school.” “A bayonet is like a knife; you see soldiers with them on their rifles. I’ve never seen a bullet.” His memory for recent events was also poor. He once recognized a single tune played at a concert.
Suspected of malingering, he was tried out in various ways. He was told that an elephant was a little furry animal and shown a little 6 inch toy sample. On going to the zoo he was greatly astonished at seeing a real elephant. He did not know what the war was about and he had no interest therein.
Suspected of faking his condition, he was tested in different ways. They told him that an elephant was a small furry animal and showed him a tiny 6-inch toy version. When he went to the zoo, he was shocked to see a real elephant. He didn’t understand what the war was about and didn’t care about it.
March 10 he was hypnotized and proved an easy subject. Powerful suggestions that lost memories would return were unavailing. The next day, during hypnosis, it was found that his previous experience could be readily tapped, and a history of his family, schooling, running away, and eventual enlistment was told. He had been at Gibraltar when war broke out. He was at the first battle at Ypres, and was for ten days in severe trench fighting, and was finally buried in the mud and débris of a trench blown in by a high explosive shell. He had been buried for about 12 hours, was dug out at night, and (according to his father) remained unconscious 24 hours, and deaf and dumb three days. He was transferred to another hospital and then to Manchester, where he came to himself.
On March 10, he was hypnotized and turned out to be an easy subject. Strong suggestions that lost memories would come back didn't work. The next day, during hypnosis, it was discovered that his previous experiences could be easily accessed, and he shared a history of his family, education, running away, and eventual enlistment. He was in Gibraltar when the war started. He participated in the first battle at Ypres, endured severe trench fighting for ten days, and was eventually buried under the mud and debris of a trench that was blown in by a high explosive shell. He was buried for about 12 hours, was dug out at night, and (according to his father) remained unconscious for 24 hours and was deaf and mute for three days. He was then transferred to another hospital and later to Manchester, where he regained consciousness.
Only during the first few sittings did the patient lie with eyes closed. Later, during hypnosis, he behaved exactly like a normal person. The fact came to light that when hypnotized the patient returned to the personality that possessed him just before awakening in Manchester, and accordingly during hypnosis, he had to become acquainted again with his hypnotizer. Maida Vale astonished him, as it should have been Manchester. Thus there were two personalities: No. 1: The personality since the date of the Manchester awakening; No. 2: The personality containing all the memories of the past life as well as the more recent Flanders memories. In State No. 1, the manner was jaunty and cocksure. In State[515] No. 2, the man was more modest and less loud. Moreover, though in State No. 1 he spoke with a Lancashire accent, in State No. 2 his speech was in the West Country dialect—a strange observation, confirmed by several observers. He was asked to write down the answers to questions, and on awakening from hypnosis was shown the things written; whereupon he laughed and said, “Why, that’s not my writing.” On writing out the same sentences again, various minor points of difference were apparent. Hypnotized in the presence of his father, in whom in State No. 1 he took no great interest, he showed every sign of joy, causing his father to think that in State No. 2, his son had “come all right again.” In State No. 2 he could play a euphonium better than in State No. 1; but after practicing in State No. 1 he rapidly became as expert as in the hypnotic state.
Only during the first few sessions did the patient lie with his eyes closed. Later, while under hypnosis, he acted just like a normal person. It turned out that when hypnotized, the patient reverted to the personality he had just before waking up in Manchester. Accordingly, during hypnosis, he had to get to know his hypnotist again. Maida Vale surprised him, just as Manchester should have. Thus, there were two personalities: No. 1: The personality since the date of the Manchester awakening; No. 2: The personality that held all the memories of his past life as well as more recent memories from Flanders. In State No. 1, he was upbeat and overly confident. In State No. 2, he was more humble and quieter. Moreover, while he spoke with a Lancashire accent in State No. 1, in State No. 2, his speech was in the West Country dialect—a peculiar observation confirmed by several witnesses. He was asked to write down answers to questions, and after awakening from hypnosis, he was shown what he had written; he laughed and said, “That’s not my writing.” When he wrote the same sentences again, various minor differences were noticeable. When hypnotized in front of his father, who he didn’t show much interest in during State No. 1, he expressed joy, leading his father to believe that in State No. 2, his son had “returned to normal.” In State No. 2, he played the euphonium better than in State No. 1; but after practicing in State No. 1, he quickly became just as skilled as he was while hypnotized.
If the patient were left for some time before being awaked by a previously-arranged method of counting three, he would experience disturbed dreams, with clenched hands, snarling lips, and muttered phrases, “Give it them,” etc.
If the patient were left for a while before being woken up by a prearranged method of counting to three, he would have disturbed dreams, with clenched hands, snarling lips, and muttered phrases like, “Give it to them,” etc.
Twenty-five hypnotic sittings were given but no improvement took place and the patient was discharged May 5. May 25 there had been no further change and he remained in State No. 1, in which state he was invalided from the service by a medical board, May 28.
Twenty-five hypnosis sessions were conducted, but there was no improvement, and the patient was discharged on May 5. By May 25, there had been no further changes, and he remained in State No. 1, the condition for which he was released from service by a medical board on May 28.
Ear complications and hysteria.
Ear issues and anxiety.
Case 370. (Buscaino & Coppola, 1916.)
An infantryman, 22 (father and mother quite normal; patient showed slight convulsions, attributed to worms, from which he actually suffered; was malarial from 9 to 15; had otitis media and lost hearing completely at 11; had suffered from 9 onwards with joint pains; as an adult had no convulsions), was called to arms August, 1914, and sent to the front May 2, 1915. About the end of August, in a water-filled trench by Monte San Michele, he was covered with mud from a shell explosion, lost consciousness, and in some way got back to the second line. He was told that blood had flowed from the right ear, and on recovery he found himself unable to hear with that ear, although it was the left in which he had had otitis. There were continual noises in the ear. He was, however, sent back to the front line. By mistake, one day, he got with companions in the midst of the enemy’s barbed wire, saw sparks from the guns, heard no shots, saw comrades fall, and threw himself instinctively into the wire network. Leaving the food kettles, he finally got back to the trenches. He was sent to the hospital at Legnano for his ear pains, and was treated by leeches, which he could not feel. He began to hear a little more. Flies walked on the left cheek without being felt. This anesthesia had begun a few days after the shell explosion. He was transferred to a military hospital at Florence.
An infantryman, 22 (his parents were pretty normal; the patient experienced slight convulsions, which were attributed to worms he actually had; he dealt with malaria from ages 9 to 15; had middle ear infections and lost all hearing in his right ear by age 11; suffered from joint pain starting at 9; and as an adult had no more convulsions), was drafted in August 1914 and sent to the front lines on May 2, 1915. Toward the end of August, in a waterlogged trench near Monte San Michele, he was hit with mud from a shell explosion, lost consciousness, and somehow made his way back to the second line. He was told that blood had flowed from his right ear, and upon recovering, he found he couldn't hear from that ear, even though the left was the one that had the ear infection. He was bothered by constant noises in his ear. Nevertheless, he was sent back to the front line. One day, by mistake, he and some comrades ended up caught in the enemy's barbed wire; he saw sparks from the guns, didn’t hear any shots, saw friends fall, and instinctively threw himself into the wire. After leaving behind their food kettles, he finally got back to the trenches. He was sent to the hospital in Legnano for his ear pain and was treated with leeches, which he couldn’t feel. He started to hear a bit better. Flies crawled on his left cheek without him noticing. This numbness began a few days after the shell explosion. He was later transferred to a military hospital in Florence.
One day he wedged a toothpick in cotton into his left ear and was charged with simulation, though he had been absolutely deaf in his left ear since childhood. From the moment the military surgeon told him he would be denounced for simulation, he lost his memory. Reports indicate that he had headache and delirious dreams (October 30), and suddenly he became furious (October 31), about three hours later going into severe collapse, for which camphor injections were given.
One day he stuck a toothpick in cotton into his left ear and was accused of pretending to be deaf, even though he had been completely deaf in that ear since he was a kid. As soon as the military doctor told him he would be reported for faking, he lost his memory. Reports say he experienced a headache and crazy dreams (October 30), and then he suddenly got really angry (October 31), about three hours later he collapsed severely, for which he received camphor injections.
November 1 he had battle dreams and lumbar puncture had to be given up as he was in the midst of an attack. A[517] hypodermic injection was interpreted by the patient as a wound, and he cried as if he were being abandoned on the battle-field. At one point he woke up from his hallucination and asked where he was and shortly relapsed into stupor. November 2, the patient was slightly bewildered and felt pains where the lumbar puncture needle had been tried the previous day. November 5, he was disoriented, thinking himself still at Legnano. The pupils were throughout dilated. November 6, confused and dreamy; November 7, he soiled his bed, was somewhat disoriented, immediately corrected himself; oculo-cardiac reflex 64 full compression, 62 during compression. November 11, headache; November 12, a slight bewilderment reappeared; November 13, remembered for the first time having been stunned by shell explosion, and this day got up and wrote home. November 14, complained of pains in muscles and weariness. Pupils still dilated. November 16, pulse 86; a gradual increase from 50 to 60 during previous days. November 17, patient had begun to remember facts that preceded the dream syndrome. November 18, pulse standing 88; November 20, pulse standing 120. This day cried when he remembered having been suspected of simulation. November 22 and 23, aches in joints and intense otalgia; pulse 86. November 24, diarrhea; deafness somewhat diminished; 26, diarrhea; looked as if he were about to have a new hallucinatory episode. This, however, did not come about until December 1, when he heard cannonading and knew the regiment was near. Next day he had forgotten the cannonading. December 14, the patient had become entirely tranquil and lucid and was able to give his entire history. December 16 and 17 he was given a systematic neurological examination, which showed on the left side complete anesthesia, hyperesthesia to pressure, thermanesthesia, analgesia, loss of bone, tendon, and muscle sensation. Vision was diminished more on the right side than on the left, and the visual fields on this side were more contracted. During examination, the fields became still more tubular. There was complete deafness, anosmia, and ageusia on the left side. On the right side there was a slight diminution of hearing. The pharyngeal[518] reflex was abolished; the cremasteric reflex was somewhat less on the left than the right; and the defensor reflexes of the left leg were less marked than those of the right. There was no clonus or Babinski. The dynamometer grasp on the right was 37; on the left 18; and on this side there was a limitation of voluntary movements.
On November 1, he had battle dreams, and they had to give up on the lumbar puncture because he was in the middle of an attack. A[517] hypodermic injection was seen by the patient as a wound, and he cried as if he were being left behind on the battlefield. At one point, he woke up from his hallucination and asked where he was, but soon slipped back into a stupor. On November 2, the patient was a bit confused and felt pain where the lumbar puncture needle had been inserted the day before. By November 5, he was disoriented, still thinking he was at Legnano. His pupils were dilated the entire time. On November 6, he was confused and dreamy; on November 7, he soiled his bed, was somewhat disoriented, but quickly corrected himself; the oculo-cardiac reflex was 64 during full compression and 62 while compressing. On November 11, he had a headache; on November 12, slight confusion returned; on November 13, he remembered for the first time being stunned by a shell explosion, and that day he got up and wrote home. On November 14, he complained of muscle pain and fatigue. His pupils were still dilated. On November 16, his pulse was 86, gradually increasing from 50 to 60 over the previous days. On November 17, the patient started to recall things that happened before the dream syndrome. On November 18, his pulse was 88; on November 20, it was 120. That day, he cried when he remembered being accused of faking. On November 22 and 23, he had joint pain and severe earache; pulse was 86. On November 24, he had diarrhea; his hearing loss had slightly improved; on the 26th, he had diarrhea again and seemed about to have another hallucinatory episode. This, however, didn’t happen until December 1 when he heard cannon fire and realized the regiment was nearby. The next day, he forgot about the cannon fire. By December 14, the patient had become completely calm and clear-headed and was able to recount his entire history. On December 16 and 17, he underwent a thorough neurological examination, which revealed complete numbness on the left side, heightened sensitivity to pressure, loss of temperature sense, and diminished pain sensation. He had a greater loss of vision on the right side compared to the left, and the visual fields on this side were more restricted. During the exam, his visual fields became even more tubular. He had total deafness, loss of smell, and loss of taste on the left side. On the right side, there was a slight decrease in hearing. The pharyngeal[518] reflex was absent; the cremasteric reflex was somewhat diminished on the left compared to the right; the defensive reflexes of the left leg were less pronounced than those of the right. There were no signs of clonus or Babinski. The dynamometer grip strength was 37 on the right and 18 on the left, where there was also a restriction of voluntary movement.
Chart 10
ETIOLOGY OF SHELL-SHOCK
| WOUNDS | 14 of 150 |
| PHYSICAL | |
| Exhaustion from exposure and hardship (all neuropaths) | 3 of 142 |
| Head injury | 52 of 142 |
| CHEMICAL—Shell Gas | 3 of 150 |
| PSYCHIC | |
| Gradual Burnout, Predisposing (43 neuropaths) | 51 of 132 |
| Same, Acting in Itself (patients chiefly neuropaths) | |
| Sudden Jolt | |
| Terrible sights | 51 of 142 |
| Loss of Friends | |
| Scary Close to Explosion (one neuropath) | |
| Sounds (a few neuropaths) | |
| RELAPSES (41 of 150 observed, three-quarters neuropaths) |
After Wiltshire
After Wiltshire
C. THE DIAGNOSIS OF SHELL-SHOCK
In the course of our study of psychoses incidental in the war (Section A) and especially of Shell-shock’s nature and causes (Section B), we have naturally met most if not all of the major diagnostic difficulties. In the present Section we shall study cases for the light they may throw on the more technical troubles of the diagnostician. Who would à priori have felt that such diseases as tetanus, rabies, malaria, would produce practical difficulties in clinical diagnosis in the field of Shell-shock?
In our study of the psychoses related to the war (Section A) and specifically the nature and causes of Shell-shock (Section B), we have encountered many, if not all, of the major diagnostic challenges. In this Section, we will examine cases to gain insight into the more technical issues facing diagnosticians. Who would à priori have thought that conditions like tetanus, rabies, and malaria would create practical challenges in diagnosing Shell-shock in the field?
Mayhap there was no need to emphasize further the values of lumbar puncture fluid examination. Yet the admixture of “functional” and “organic” symptoms in numerous puzzling cases can hardly be over-emphasized.
Maybe there was no need to stress further the importance of examining lumbar puncture fluid. However, the mix of "functional" and "organic" symptoms in many confusing cases can hardly be overstated.
But the interpolation, through the ingenious inquiries of Babinski, of a new or but vaguely suspected series of “reflex” (“physiopathic”) troubles between the organic neuropathic disorders on the one hand and the hysterical psychopathic disorders on the other—the result of these observations, sampled only in Section B, is given more in detail in the present Section. What a split in therapeutic method a recognition of this new group of “physiopathic” disorders might entail is seen also in further cases in the Section that follows this (Section D on Treatment and Results).
But the interpolation, through the clever investigations of Babinski, of a new or only slightly suspected series of “reflex” (“physiopathic”) issues between the organic neuropathic disorders on one side and the hysterical psychopathic disorders on the other—the outcome of these observations, sampled only in Section B, is discussed in more detail in this Section. The significant divide in treatment methods that acknowledging this new group of “physiopathic” disorders might create is also illustrated in additional cases in the Section that follows this (Section D on Treatment and Results).
A number of simulation cases has been added.
A number of simulation cases have been added.
Chart 11
ETIOLOGICAL GROUPING OF WAR
PSYCHONEUROSES
| I. | NEUROSO-ORGANIC ASSOCIATION (NO CAUSAL LINK) |
| II. | REFLEX NEUROSES (THE LESION IS UNUSUALLY MINOR WHEN COMPARED TO PSYCHONEUROSIS.) |
| III. | NEUROSO-SOMATIC ASSOCIATION (Trench foot, neuritis, radiculitis) |
| IV. | FATIGUE OR EMOTIONAL PSYCHONEUROSES (THINK ABOUT THE IMPACT OF PSYCHIC CONTAGION AND EDUCATION) |
| V. | PSYCHONEUROSES ON ANTEBELLUM BASIS |
After Grasset
After Grasset
Chart 12
WAR PSYCHONEUROSES
SYMPTOMATIC GROUPS
| I. | EMOTIONAL (Hyper- Hypo- Para-) |
| II. | CONFUSIONAL (Attention and Memory Disorders, Dream States; Delirium) |
| III. | CONVULSIVE AND PITHIATIC (Hilarious) |
| IV. | NEURASTHENIC AND PSYCHASTHENIC |
| V. | SENSITIVOMOTOR AND SENSORIMOTOR—e.g., Limited Paralyzes, Contractures, Deafness |
| VI. | COMPLEX |
| VII. | PHYSIOPATHIC (Babinski reflex) |
After Grasset
After Grasset
Value of lumbar puncture.
Importance of spinal tap.
Case 371. (Souques and Don’t, October, 1915.)
A colonial soldier arrived at Paul-Brousse Hospital with a hospital ticket showing that ten days before he had had commotio cerebri. He was dull, had a fixed stare, held his head in his hands, was disoriented for time and place, and had lost memory for everything that had happened for eighteen months. There was no sign of wound. There was no motor disorder save that walking was a bit slow and uncertain. Perhaps the right knee-jerk was stronger than the left. Percussion of the right Achilles tendon produced tremor. The plantar reflexes were flexor on both sides; flexion lasted longer right than left. The cremasteric and abdominal reflexes were a little weaker on the right. Arm reflexes were lively. Sensations proved normal. Complaint of headache, frontal and vertical.
A soldier from a colony arrived at Paul-Brousse Hospital with a hospital ticket indicating that ten days earlier he had experienced a concussion. He appeared dull, had a blank stare, held his head in his hands, was confused about the time and place, and had lost memory of everything that had happened in the past eighteen months. There were no signs of a wound. The only motor issue was that his walking was slightly slow and unsteady. The knee-jerk reaction on the right seemed stronger than on the left. Tapping the right Achilles tendon caused a tremor. The plantar reflexes were flexor on both sides; the flexion lasted longer on the right than on the left. The cremasteric and abdominal reflexes were a bit weaker on the right side. The arm reflexes were responsive. Sensations were normal. He complained of a headache that was frontal and vertical.
Lumbar puncture October 7, that is, on the thirteenth day after the shell-shock, yielded a transparent, slightly greenish fluid, with 92 cells per cm. (lymphocytes with one or two large mononuclear cells and a few sometimes degenerated endothelial cells) and hyperalbuminosis.
Lumbar puncture on October 7, which was the thirteenth day after the shell-shock, produced a clear, slightly greenish fluid, containing 92 cells per cm. (lymphocytes along with one or two large mononuclear cells and a few occasionally degenerated endothelial cells) and hyperalbuminosis.
October 9, the clouding of consciousness was less marked. The headaches and amnesia were constantly complained of; the reflexes were normal. October 12, there was less headache. October 25, another lumbar puncture showed but 14 or 15 lymphocytes per cm. and hyperalbuminosis. There was now no longer any clouding of consciousness. The amnesia, retrograde and anterograde back to May 9, 1914 (date of his daughter’s birth), and up to September 25, 1915, persisted. The man did not remember the declaration of war, or the mobilization, or his regiment, and the like. Meantime, the man’s judgment and reasoning powers were normal.
October 9, the clouding of consciousness was less noticeable. The headaches and memory loss were still frequently reported; the reflexes were normal. On October 12, the headaches were less intense. By October 25, another lumbar puncture revealed only 14 or 15 lymphocytes per cm, and there was hyperalbuminosis. There was no longer any clouding of consciousness. The memory loss, both retrograde and anterograde from May 9, 1914 (the date of his daughter’s birth) to September 25, 1915, continued. The man couldn’t remember the declaration of war, the mobilization, his regiment, or similar events. In the meantime, his judgment and reasoning were normal.
If there had been no early spinal fluid examination of this patient, he might well have been considered an hysteric or even a simulator.
If there hadn’t been an early spinal fluid test for this patient, he might have been seen as hysterical or even faking it.
Meningeal and intraspinal hemorrhage: Lumbar puncture.
Meningeal and intraspinal bleeding: Lumbar puncture.
Case 372. (Guillain-Barré, May, 1915.)
A gunner from Morocco, who lost consciousness for an hour March 28, 1915, upon the explosion of a large-calibre shell in his trench, was carried to the ambulance. He complained of headache and generalized pains. His status was scarcely modified during five weeks, and a generalized contracture of the body developed whenever movements were attempted. In horizontal decubitus, the muscles of the limbs and neck were of a normal tonicity, but the head went into hyperflexion if the patient was asked to sit. The eyes turned upward, and Kernig’s sign developed. The patient could walk only with short steps, with legs apart and arms held away from the body, the head in a sort of tetanoid dorsal hyperflexion. There was a right-sided hemiparesis with trepidation and the Babinski sign.
A gunner from Morocco, who passed out for an hour on March 28, 1915, after a large-caliber shell exploded in his trench, was taken to the ambulance. He reported having a headache and widespread pain. His condition barely changed over five weeks, and he developed a general stiffness in his body whenever any movements were attempted. When lying down, the muscles in his limbs and neck were normally toned, but his head would bend forward sharply if he was asked to sit up. His eyes rolled upwards, and he exhibited Kernig’s sign. The patient could only walk with short steps, legs apart and arms held away from his body, with his head in a sort of rigid backward bend. There was weakness on the right side of his body with trembling and a positive Babinski sign.
Lumbar puncture assured the diagnosis of something organic. The fluid contained blood cells and a marked lymphocytosis. The symptoms evidently depended upon hemorrhages in the meninges and the nervous system, affecting particularly the right pyramidal tract.
Lumbar puncture confirmed the diagnosis of an organic condition. The fluid had blood cells and a significant increase in lymphocytes. The symptoms were clearly linked to bleeding in the meninges and the nervous system, particularly impacting the right pyramidal tract.
Re hypothesis of organic changes in hysterical cases, Roussy and Lhermitte remark in comment upon albuminosis in the cerebrospinal fluid that the albumin is perhaps due (in cases of camptocormia) to the effect upon venous and lymphatic circulation of the spinal curvature. It was Sicard’s claim that camptocormia, or bent back, was due possibly to anatomical changes in the spinal column, that is, that camptocormia was in one sense a spondylitis. In other cases the camptocormia might be due to a ligamentous or muscular change; that is, to a syndesmitis or a psoitis. His idea was that the curvature was in a sense antalgic; that is, a response having the purpose of avoiding pain.
Re hypothesis of organic changes in hysterical cases, Roussy and Lhermitte comment on albuminosis in the cerebrospinal fluid, suggesting that the albumin could be the result (in cases of camptocormia) of the impact on venous and lymphatic circulation caused by the spinal curvature. Sicard argued that camptocormia, or a bent back, might be linked to anatomical changes in the spinal column, effectively making camptocormia a form of spondylitis. In other instances, camptocormia could result from changes in ligaments or muscles, that is, from syndesmitis or psoitis. His theory was that the curvature served an antalgic purpose; in other words, it was a response aimed at avoiding pain.
Slight hyperalbuminosis.
Slightly elevated albumin levels.
Case 373. (Ravaut, August, 1915.)
A farmer, 32, in the 66th Infantry, was lying in a dug-out March 5, 1915, when a bomb threw him on the ground and covered him with earth. He was picked up unconscious, and remained so for an hour. In the ambulance it was found that he could hardly stand, could not speak, and appeared to be completely confused. There was no sign of wound. The next day he recovered consciousness and complained of a violent headache. He was completely deaf in the left ear, and vision was also a little impaired on that side. The puncture fluid was clear, and there was a very slight excess of albumin by the heat test. The next day the headache had entirely disappeared, the left ear was absolutely deaf, but the patient complained of buzzing. Lumbar puncture the following day showed a normal amount of albumin.
A 32-year-old farmer in the 66th Infantry was lying in a dugout on March 5, 1915, when a bomb knocked him to the ground and buried him under dirt. He was found unconscious and stayed that way for an hour. In the ambulance, they discovered he could barely stand, couldn't speak, and seemed completely confused. There were no visible wounds. The next day, he regained consciousness and complained of a severe headache. He was completely deaf in his left ear, and his vision was also slightly impaired on that side. The puncture fluid was clear, with a very slight increase in albumin from the heat test. The following day, the headache was gone, but he remained completely deaf in his left ear and reported a buzzing sound. A lumbar puncture the next day showed a normal level of albumin.
March 16 the patient was evacuated to the rear presenting no abnormal symptom except deafness.
March 16 the patient was moved to the rear with no unusual symptoms other than deafness.
Re the spinal fluid, Armstrong-Jones considers that a shock directly sustained by the spinal apparatus through sudden impact to the surrounding cerebrospinal fluid, ought to be felt more by the anterior horn cells than by the spinal root ganglia, since the latter are shielded by the sheath in the intervertebral spaces. Motor symptoms would, naturally, then be more frequent than sensory symptoms. He also believes that the controlling neurones in the intermedio-lateral tracts that have to do with the sympathetic system, would be affected just as anterior horn cells are. Accordingly, the dilated pupils, rapid heart, dyspnoea, and a variety of precordial pains and disorder of the viscera would ensue. The jar would thus be communicated to the neuronic cells of origin of two types: spinomuscular and preganglionic, leaving the gangliospinal neurones relatively intact.
Re the spinal fluid, Armstrong-Jones believes that a shock directly experienced by the spinal system due to a sudden impact on the surrounding cerebrospinal fluid should be felt more by the anterior horn cells than by the spinal root ganglia, since the latter are protected by the sheath in the intervertebral spaces. Consequently, motor symptoms would, naturally, appear more often than sensory symptoms. He also thinks that the controlling neurons in the intermediolateral tracts related to the sympathetic system would be affected just like the anterior horn cells. As a result, symptoms like dilated pupils, a rapid heartbeat, shortness of breath, and various precordial pains or internal organ issues would follow. The impact would thus be transmitted to the neuronal cells of two types: spinomuscular and preganglionic, leaving the gangliospinal neurons relatively unharmed.
Paraplegia, organic: Lumbar puncture.
Paraplegia, organic: Spinal tap.
Case 374. (Joubert, October, 1915.)
A gunner, 23, was thrown to the ground, according to his story, by the explosion of a large-calibre shell, at eight o’clock in the morning of September 10, 1914. He could not get up but thought he had not lost consciousness. September 13, he arrived at hospital, looking like a man with dorsolumbar fracture of the spine. There was, however, no external injury. There was a marked paresis of the right upper extremity, with diminished sensibility, weakened reflexes, numbness, formication. The right lower extremity was subject to complete flaccid paralysis, with lost reflexes, and anesthesia in all respects reached to the belt level, and stopped sharply at the median line of the abdomen. The left leg, also, was paretic but the muscles could be contracted weakly; the knee-jerk was exaggerated; there was a tendency to epileptoid trepidation, and the sensations were only slightly diminished. There was a Babinski reflex on the right side; the abdominal reflex was absent on the left side; both cremasteric reflexes were present. The feet at times gave formication. Rectal, bladder, and sphincter paralysis. Dark albuminous urine, with a few blood cells, was obtained on catheterization. There was an early sacral decubitus; consciousness was somewhat clouded. The man made no requests except for something to drink, and seemed apathetic.
A 23-year-old gunner was knocked to the ground by the explosion of a large-caliber shell at 8 a.m. on September 10, 1914. He couldn’t get up but thought he hadn’t lost consciousness. By September 13, he arrived at the hospital, looking like a man with a fracture in his lower spine. However, there were no external injuries. He had significant weakness in his right arm, with reduced sensitivity, weak reflexes, numbness, and tingling. The right leg was completely paralyzed, with no reflexes, and the loss of sensation reached up to his beltline, stopping sharply at the middle of his abdomen. The left leg was also weak, but the muscles could still contract slightly; his knee reflex was heightened, he had a tendency to twitch, and his sensations were only slightly reduced. He had a positive Babinski reflex on the right side; the abdominal reflex was absent on the left side; both cremasteric reflexes were present. Occasionally, his feet would tingle. He experienced paralysis of the rectum, bladder, and sphincter. During catheterization, dark, albuminous urine with some blood cells was collected. There was an early pressure sore on his lower back, and his consciousness was a bit hazy. The man only asked for something to drink and seemed indifferent.
Lumbar puncture, September 14, yielded hemorrhagic fluid. Three days later, the upper extremity regained its powers and sensations, but the paraplegia had become complete, with abolition of reflexes on both sides, and absolute anesthesia. The feet yielded formication at times, however. Sacral decubitus increased and healed not. The temperature varied between 38 and 39. The patient died September 24, in coma, with anuria and Cheyne-Stokes breathing.
Lumbar puncture on September 14 showed hemorrhagic fluid. Three days later, the upper body regained its strength and sensations, but the paraplegia had become complete, with no reflexes on either side and total loss of feeling. The feet occasionally experienced tingling, though. The pressure sores on the lower back increased and did not heal. The temperature fluctuated between 38 and 39. The patient passed away on September 24, in a coma, with no urine output and Cheyne-Stokes breathing.
Gunshot wound of spinal column; no penetration or injury of dura mater: At first quadriplegia; later cerebellospasmodic type of disorder.
Gunshot wound to the spine; no penetration or damage to the dura mater: Initially quadriplegic; later developed cerebellospasmodic type disorder.
Case 375. (Claude and Lhermitte, July, 1917.)
A soldier, 22, sustained a gunshot wound in the neck about the level of the fourth cervical vertebra. He immediately became quadriplegic. He recovered arm motion in two months and some weeks later ability to stand and walk.
A 22-year-old soldier was shot in the neck near the fourth cervical vertebra. He instantly became quadriplegic. He regained arm movement within two months and some weeks later was able to stand and walk.
Three months after the injury, station was difficult, better on a broad base. Rombergism, even with eyes open. Cerebellospasmodic gait. There was no weakness of leg muscles, but there was a certain degree of weakness of the upper extremities, especially in finger flexion. There was hypertonia of the muscles of all the extremities and the hands showed the signs of Raimiste, of Klippel and Weil, and of Dejerine. Static equilibrium was preserved to the will, but the kinetic balance was affected, and as much in the upper as in the lower extremities. Ataxia, tremors, dysmetria, adiadocho-kinesia, and disorder of combined movements in thigh and trunk flexion were all in evidence. Meantime, there was no disorder of sensation whatever except that the ulnar border of the right hand showed a hypobaresthesia, and there was a disturbance of tactile discrimination and absolute astereognosis in the hands. The deep reflexes were everywhere increased, and ankle and patellar clonus were easy to excite, especially on the right side. Bilateral defense reflexes. Bilateral Babinski sign. The hypertonia and ataxia ebbed away during the following three months. Walking became normal, and there was little sign of difficulty except astereognosis of both hands, combined with slight disturbance of deep sensibility and poor response to compass test in palm.
Three months after the injury, standing was difficult, but it improved on a broad base. There were signs of Rombergism, even with eyes open. The gait was cerebellar and spastic. The leg muscles weren’t weak, but there was some weakness in the upper extremities, especially with finger movements. All the extremities showed muscle stiffness, and the hands exhibited signs of Raimiste, Klippel and Weil, and Dejerine. Static balance was under control, but dynamic balance was affected in both upper and lower limbs. Ataxia, tremors, dysmetria, adiadochokinesia, and issues with coordinated movements in thigh and trunk flexion were evident. Meanwhile, there was no sensory disorder except for reduced sensitivity on the ulnar side of the right hand, along with impaired tactile discrimination and complete inability to recognize objects by touch in both hands. Deep reflexes were heightened, and it was easy to trigger ankle and patellar clonus, especially on the right side. There were bilateral defense reflexes and a bilateral Babinski sign. Over the next three months, the hypertonia and ataxia subsided. Walking returned to normal, with little difficulty noted except for the inability to recognize objects by touch in both hands, combined with slight disturbances in deep sensation and poor response to the compass test in the palm.
We here deal with a case of spinal column injury without injury to the dura mater. This cerebellospasmodic form of the superior cervical type of spinal concussion is less frequent than a quadriplegic form with Brown-Séquard syndrome. It is striking that both types of concussion may recover.
We are discussing a case of spinal column injury without damage to the dura mater. This cerebellospasmodic type of superior cervical spinal concussion is less common than the quadriplegic form associated with Brown-Séquard syndrome. It's noteworthy that both types of concussion can show signs of recovery.
Spinal column trauma, with local signs: Later, hysterical anesthesia and contracture of back muscles homolateral with the trauma.
Spinal column injury, with local symptoms: Subsequently, hysterical numbness and tightening of the back muscles on the same side as the injury.
Case 376. (Oppenheimer, July, 1915.)
A musketeer, wounded August 20, 1914, by a shell splinter in right side of vertebral column, fell unconscious, but was able afterward to crawl on all-fours out of the firing line. Severe vomiting and epistaxis followed. August 23, there was pain in the small of the back; the last two ribs were painful on right side; and the muscles were slightly swollen up to the iliac crest. August 30, a slight rise of temperature (at first it had been above 38) still persisted, but the muscular swelling was diminished. Treatment by aspirin and baths. No further rise of temperature after early in September.
A musketeer, wounded on August 20, 1914, by a shell fragment in the right side of his spine, fell unconscious but was later able to crawl on all fours out of the danger zone. He experienced severe vomiting and a nosebleed afterward. On August 23, he felt pain in his lower back; the last two ribs on his right side were sore, and the muscles were slightly swollen up to the iliac crest. By August 30, a slight fever (which had initially been above 38°C) still lingered, but the muscle swelling had decreased. He was treated with aspirin and baths. There was no further increase in temperature after early September.
On October 9, patient was permitted to get up, whereupon he showed a peculiar curved attitude of the body, reduced almost completely by passive straightening. Swelling of the longitudinal muscles. Radiograph negative, except that one picture showed a change in left twelfth rib, near the transverse process. Pains in left lumbar region.
On October 9, the patient was allowed to get up, at which point he displayed a strange curved posture of the body, which was nearly fully corrected by passive straightening. There was swelling in the longitudinal muscles. The X-ray was negative, except one image indicated a change in the left twelfth rib, near the transverse process. There were pains in the left lower back.
November 19, on examination, pulse 112. November 23, after massage, vomiting. Temporary use of plaster corset.
November 19, upon examination, pulse 112. November 23, after a massage, vomiting occurred. Temporary use of a plaster corset.
On admission to the nerve hospital December 22, the musketeer was unable to extend the trunk, and the long muscles of the back were on the stretch, often as hard as wood, especially those of the left (longissimus dorsi). Patient lay on right half of pelvis. Hemianesthesia and hemianalgesia, left side. Tachycardia. Formerly the patient had done hard work, especially carrying heavy bags. He declined to be examined under general anesthesia. He seemed to be of unreliable character, and his trouble did not prevent him from returning from leave of absence, on one occasion, drunk.
Upon admittance to the nerve hospital on December 22, the musketeer was unable to extend his torso, and the muscles in his back were tense, often feeling as hard as wood, particularly on the left side (longissimus dorsi). The patient lay on the right side of his pelvis. He exhibited hemianesthesia and hemianalgesia on the left side, along with tachycardia. Previously, he had done physically demanding work, especially carrying heavy bags. He refused to undergo an examination under general anesthesia. He appeared to be of questionable character, and his condition did not stop him from returning from a leave of absence on one occasion while drunk.
Mine explosion: Combined hysterical and lesional effects.
Mine explosion: Combined emotional and physical effects.
Case 377. (Dupouy, September, 1915.)
A lieutenant, 23, was in a mine explosion June 23, coming out in complete torpor, with mutism and retention of urine. He was brought to hospital June 26, with jactitation, irregular pulse, markedly exaggerated tendon reflexes, absent skin reflexes, sluggish, dilated pupils, especially right, and general anesthesia. The spinal fluid contained an excess of albumin, altered blood cells and many lymphocytes.
A 23-year-old lieutenant was involved in a mine explosion on June 23 and came out completely unresponsive, unable to speak, and unable to urinate. He was taken to the hospital on June 26, showing signs of restlessness, an irregular heartbeat, significantly heightened tendon reflexes, absent skin reflexes, sluggish and dilated pupils—especially on the right side—and overall lack of sensation. The spinal fluid showed high levels of albumin, altered blood cells, and a lot of lymphocytes.
Several hours after puncture he suddenly demanded where he was, thought it was the year 1911 when he was in the Dragoons, talked about his camp, and was confused, irritable and stereotyped in questions. There was no verbal amnesia. Speech was hesitant, explosive and scanning, suggestive of multiple sclerosis. Next day there was still retrograde amnesia. He clung to the belief that it was July, 1911, and asked wearisome, stereotyped questions. The words, “German house” caused a jactitation, stiffening and relapse into a second état, out of which he came with hiccoughs and sighs, and amnestic for this conversation. There was general hypesthesia and muscular weakness especially of legs. The reflexes were as before.
Several hours after the injury, he suddenly asked where he was, believed it was the year 1911 when he was in the Dragoons, talked about his camp, and was confused, irritable, and repetitive in his questions. There was no memory loss. His speech was hesitant, explosive, and scanning, suggesting multiple sclerosis. The next day, he still had memory issues. He held on to the belief that it was July 1911 and asked frustrating, repetitive questions. The phrase, “German house,” caused him to twitch, stiffen, and relapse into a second état, from which he emerged with hiccups and sighs, and had no memory of this conversation. He experienced general reduced sensitivity and muscle weakness, especially in his legs. His reflexes were as they were before.
The morning of June 28, he heard the hum of an airplane, whereupon his memory returned. It seems that he had himself once ascended. The memory gap was now limited to the time immediately preceding the mine explosion and the days following, up to the time of hearing the airplane. He told about his military life and also about incidents immediately preceding his blowing up. He complained of malaise and of pains in the vertebral column and limbs.
The morning of June 28, he heard the sound of an airplane, and suddenly his memory came back. It seems that he had once taken flight himself. The memory loss was now just about the time right before the mine explosion and the days after, leading up to when he heard the airplane. He talked about his military life and also about events that happened right before the explosion. He mentioned feeling unwell and having pain in his back and limbs.
There was a quadriparesis, more marked, however, on the left; walking with falls to the left; astasia with left foot; double facial paresis; inability to whistle and to close eyes completely; intestinal and bladder paralysis; nocturnal emissions non-pleasurable; partial anesthesia of right leg, of[531] arm and of hand, with hyperesthesia of thigh, of forearm and of the posterior aspect of the upper arm; anesthesia of the left side, including thorax and abdomen, excepting that the arm was hypesthetic only. Face hyperesthetic. Complete anesthesia of nipple and testis; hypesthesia of neck; anesthesia of tongue, nose and vertex; plantar, cremasteric, abdominal reflexes absent; exaggerated tendon reflexes; pupil reflexes normal; painful heat flashes and profuse sweating on the slightest movement; vertigo and tendencies to syncope after effort; explosive, scanning speech; intermittent convulsive movements of the arms. Palpation and X-ray show separation of the spinous processes of the third cervical vertebra.
There was paralysis in all four limbs, but it was more noticeable on the left side; the person walked with falls to the left; there was difficulty standing without support and issues with the left foot; both sides of the face were weak; they couldn't whistle or fully close their eyes; there was paralysis of the intestines and bladder; involuntary nighttime emissions were uncomfortable; there was partial numbness in the right leg, arm, and hand, along with increased sensitivity in the thigh, forearm, and the back of the upper arm; numbness was present on the left side, including the chest and abdomen, except the left arm had reduced sensitivity. The face was overly sensitive. There was complete numbness of the nipple and testicle; the neck had reduced sensitivity; there was numbness of the tongue, nose, and top of the head; reflexes in the feet, cremasteric, and abdomen were absent; tendon reflexes were exaggerated; pupil reflexes were normal; there were painful hot flashes and excessive sweating with minimal movement; vertigo and fainting tendencies occurred after exertion; speech was explosive and hard to follow; there were intermittent convulsive movements of the arms. Palpation and X-rays indicated a separation of the spinous processes of the third cervical vertebra.
Improvement was marked and progressive in motor, sensory and reflex fields. At the time of report three months later, there was a definite paresis of the left leg, with anesthesia and absent plantar reflexes, and slight paresis of the orbicularis palpebrarum, scanning speech and syncopal tendencies. Here, then, due to diffuse, non-systematic lesions, with superadded hysterical manifestations, were probably some effects of a permanent nature due to destructive processes.
Improvement was noticeable and ongoing in motor, sensory, and reflex areas. Three months later, there was clear weakness in the left leg, along with numbness and absent plantar reflexes, and a slight weakness of the eyelid muscles, slurred speech, and fainting tendencies. Thus, due to widespread, non-specific lesions, along with additional hysterical symptoms, there were likely some lasting effects caused by destructive processes.
Re combination of functional and lesional effects, Sollier and Chartier state that in Shell-shock hysteria, physical causes and conditions are the chief factors; that in the so-called hystero-traumatism of Charcot, the psychic and physical factors are of virtually equal importance, and that in ordinary cases of hysteria, the psychic is the chief genetic factor.
Re combination of functional and lesional effects, Sollier and Chartier state that in shell-shock hysteria, physical causes and conditions are the primary factors; that in the so-called hystero-traumatism of Charcot, the psychological and physical factors are nearly equally important, and that in typical cases of hysteria, the psychological is the main contributing factor.
Shell explosion: Hysterical and organic symptoms.
Shell explosion: Intense panic and physical reactions.
Case 378. (Hurst, 1917.)
A champion heavy-weight boxer, 29, was unconscious for two days after being knocked over by the explosion of a shell in December, 1914. He found at first that he could not move the right arm or left leg; and after power had returned to the limbs, he had forcible involuntary movements in the left leg whenever he tried to stand. Examined, April 1, 1915, he answered questions slowly and with slow words; the right arm was weak. When the left hand was clenched, an associated movement took place in the right hand, but not vice versa. There was, however, no diminution in the girth of the muscles. The man was unable to localize light tactile stimuli accurately. Movements of the left leg were somewhat weak, the left knee-jerk was slightly brisker than the right; ankle clonus could be obtained on the left side and Babinski second sign (paralyzed leg rising higher than the normal leg in combined flexion of thigh and pelvis). When the man tried to walk, the left leg moved rapidly from side to side round the point of contact of the toes. When the right leg moved forward, the left dragged behind in irregular movement.
A champion heavyweight boxer, 29, was unconscious for two days after being knocked out by the explosion of a shell in December 1914. At first, he found that he couldn't move his right arm or left leg; once he regained strength in his limbs, he experienced strong involuntary movements in his left leg whenever he attempted to stand. When examined on April 1, 1915, he responded to questions slowly and with hesitation; his right arm was weak. When he clenched his left hand, his right hand also moved involuntarily, but not the other way around. However, there was no noticeable reduction in muscle size. He struggled to accurately pinpoint light touches. Movement in his left leg was somewhat weak, and the left knee-jerk response was slightly more pronounced than the right; there was ankle clonus on the left side and Babinski's second sign (his paralyzed leg rose higher than the normal leg during combined flexion of the thigh and pelvis). When he attempted to walk, his left leg swayed rapidly from side to side around the point where his toes touched the ground. As his right leg moved forward, the left leg dragged behind in a jerky motion.
Every effort to cure the patient by means of suggestion during hospital care for a month entirely failed. Although the man was easily hypnotizable, he could not be made to move his leg under the deepest hypnosis. The first whiff of ether hypnotized him, so that the method of etherization could not be used in the endeavor to control the leg movements. Over a year later, July, 1916, the patient had greatly improved mentally but was otherwise in precisely the condition that is above described.
Every attempt to treat the patient through suggestion during a month of hospital care completely failed. Even though the man was easy to hypnotize, he couldn't be made to move his leg, even under deep hypnosis. The first smell of ether would put him under, which meant the etherization method couldn't be used to control his leg movements. Over a year later, in July 1916, the patient had significantly improved mentally but was otherwise in the same condition as previously described.
Gunshot wound of buttocks with injury to cauda equina: Urinary disturbance; decubitus; anesthesia. Superimposed paraplegia, regarded as functional and cured by psychotherapy.
Gunshot wound to the buttocks with damage to the cauda equina: Urinary issues; pressure sores; numbness. Overlaid paraplegia, considered functional and treated with psychotherapy.
Case 379. (Oppenheimer, July, 1915.)
A German grenadier, October 11, 1914, was wounded in the left buttock by a missile that passed out through the right buttock. Pains in the abdomen and legs followed. The man had to be catheterized on the battle-field.
A German grenadier, October 11, 1914, was injured in the left buttock by a projectile that exited through the right buttock. He later experienced pain in his abdomen and legs. The man had to be catheterized on the battlefield.
October 23, he suddenly fell down with total paralysis of both legs.
October 23, he suddenly collapsed with total paralysis in both legs.
November 3, numerous small furuncles appeared on the buttocks, and bedsores developed. The patient lay helpless in bed, was unable to sit up without support, or to turn from one side to the other, and had areas of anesthesia.
November 3, several small boils appeared on the buttocks, and bedsores developed. The patient lay helpless in bed, unable to sit up without assistance or to turn from one side to the other, and had areas of numbness.
During November and December, there was persistent high temperature, between 38 and 40; but January 3 the temperature stood at 36.6.
During November and December, the temperature consistently stayed high, around 38 to 40 degrees; however, on January 3, it dropped to 36.6 degrees.
January 7 the patient was admitted to a nerve hospital. At this time he was able to pass urine unaided, though with tenesmus and pain, sometimes nausea and a tendency to vomit. He complained of pain in the back and pelvic region; the legs lay as if paralyzed. No active movement whatever was performed. There was a marked increase of tendon reflexes (even including the semi-membranosus). The muscles were relaxed through disuse but there was no atrophy. The patient moved his legs about with his hands. Sensibility was preserved except in the region of the pubis. The plantar reflexes were absent. Electrical reactions normal.
On January 7, the patient was admitted to a nerve hospital. At that time, he was able to urinate on his own, though he experienced straining, pain, occasional nausea, and a tendency to vomit. He complained of pain in his back and pelvic area; his legs appeared as if they were paralyzed. No active movement was observed. There was a noticeable increase in tendon reflexes (including the semi-membranosus). The muscles were relaxed from lack of use, but there was no atrophy. The patient used his hands to move his legs around. Sensation was intact except in the pubic area. The plantar reflexes were absent, and electrical responses were normal.
The diagnosis was functional paralysis of the legs (previous gunshot injury of cauda equina).
The diagnosis was functional paralysis of the legs (previous gunshot injury to the cauda equina).
Treatment with psychotherapy met with prompt results; within a few days, the patient learned to move his legs and to walk with support, though making enormous efforts which threw the pulse up to about 160 and made the face congested. The bladder disturbance and the sacral anesthesia persisted.
Treatment with psychotherapy quickly produced results; within a few days, the patient learned to move his legs and walk with support, though it took a huge effort that raised his pulse to about 160 and caused his face to flush. The bladder issues and sacral numbness continued.
Spinal concussion with spinal cord lesion: Thermanesthesia and analgesia of right leg and side.
Spinal concussion with spinal cord injury: Reduced sensation and pain relief in the right leg and side.
Case 380. (Buzzard, December, 1916.)
An officer was hit in the back by a shrapnel fragment, fell paralyzed, but after a few minutes was able to walk more than a mile to the dressing station. Eventually arriving in London, he had nothing to complain of except the wound, as the foreign body had been removed in France. The wound healed and the patient went to a convalescent home.
An officer was hit in the back by a piece of shrapnel, fell paralyzed, but after a few minutes was able to walk over a mile to the medical station. Once he arrived in London, he had nothing to complain about except the wound, as the shrapnel had been removed in France. The wound healed, and the patient went to a recovery home.
However, when taking a bath he could not feel the temperature of the water with the right leg. Muscular power was perfect; reflexes normal; but the heat, cold and pain sense was lacking in the right leg and the right side of the body from the seventh costal cartilage downwards.
However, when he took a bath, he couldn't feel the temperature of the water with his right leg. His muscle strength was perfect; reflexes were normal; but he had no sensation of heat, cold, or pain in his right leg and the right side of his body from the seventh rib downwards.
One may make a wrong diagnosis of “Shell-shock.”
One might misdiagnose " PTSD."
Case 381. (Buzzard, December, 1916.)
In August, 1915, an officer was blown many yards by a shell, lay unconscious a while, could find no bruises, and carried on for twenty-four hours. Then, finding legs unreliable, he reported sick and was sent home as “Shell-shock.” He remained “Shell-shock” until February, 1916, then being able to walk five or six miles on smooth ground. Going downstairs he took the step with left foot rather than with right, and the right was apt to turn in. The sense of position and movement in regard to the right foot proved to be faulty. He could not balance himself on the right foot, nor could he appreciate tuning fork vibrations as well on this foot as on the other.
In August 1915, an officer was thrown several yards by a shell, lay unconscious for a while, found no bruises, and kept going for twenty-four hours. Then, realizing his legs were unreliable, he reported sick and was sent home labeled as “Shell-shock.” He remained classified as “Shell-shock” until February 1916, when he was able to walk five or six miles on flat ground. When going downstairs, he would step with his left foot instead of his right, and his right foot tended to turn inward. His sense of position and movement regarding his right foot was off. He couldn’t balance on his right foot, nor could he feel the vibrations of a tuning fork as well on that foot as he could on the left.
An X-ray examination showed a slight fracture, without deformity, in the left post-Rolandic region near the median line. His helmet had been bashed in at this point, and the bruised brain yielded symptoms even eight months later.
An X-ray showed a small fracture, with no deformity, in the left post-Rolandic area near the center line. His helmet was dented at this spot, and the bruised brain continued to show symptoms even eight months later.
Retention of urine after shell-shock.
Retention of urine after PTSD.
Case 382. (Guillain-Barré and Barré, November, 1917.)
An infantryman underwent shell-shock December 19, 1915, from the explosion of a torpedo nearby. He arrived at the ambulance, unable to speak, and next day had a confusional crisis of convulsions with contractures. He had not urinated since the accident, and two liters of clear urine were withdrawn by catheter; after which, the patient rested quietly and gradually regained consciousness. He was catheterized again in the evening and clear urine withdrawn. He remained unable to urinate spontaneously until December 25, and was catheterized accordingly.
An infantryman experienced shell shock on December 19, 1915, from the explosion of a nearby torpedo. He arrived at the ambulance unable to speak, and the next day he had a confused episode with convulsions and muscle spasms. He hadn't urinated since the accident, so two liters of clear urine were removed with a catheter; afterward, the patient rested quietly and slowly regained consciousness. He was catheterized again in the evening, and more clear urine was drained. He remained unable to urinate on his own until December 25, and was catheterized as needed.
There was no motor, sensory, or reflex disorder in this patient. Lumbar puncture yielded a normal fluid; the pupils were normal, and the only appearance was that of a marked asthenia.
There were no motor, sensory, or reflex issues in this patient. The lumbar puncture showed normal fluid; the pupils were normal, and the only observation was significant weakness.
Three months after his shell-shock, in March, 1916, the soldier was once more examined and still complained of headache, weakness, and inability to walk more than four or five hundred meters without a certain trembling of the legs. The reflexes remained normal and no further bladder trouble had supervened.
Three months after his shell shock, in March 1916, the soldier was examined again and still reported headaches, weakness, and an inability to walk more than four or five hundred meters without experiencing some leg tremors. His reflexes were normal, and there had been no new bladder issues.
Re anuria, Babinski remarks that, in days of yore, hysteria was supposed to be able to produce anuria as well as albuminuria, and even such organic changes as vesicles of the skin, ulceration, hemorrhages in the skin or of the viscera, fever, and even gangrene. He remarks that of late years no single identifiable case of this sort proved to be hysterical, has been reported. This is aside, of course, from such superficial and quickly passing vasomotor disorders as erythema and dermatographia. Anuria and albuminuria have consequently passed from the textbooks on hysteria, just as Babinski believes that hysterical edema and hysterical exaggeration of the reflexes are bound to pass. Hysteria cannot imitate everything; it cannot reproduce the characteristic phenomena of organic paralysis.
Re anuria, Babinski notes that, in the past, hysteria was thought to cause anuria as well as albuminuria, and even lead to visible physical changes like skin blisters, ulcers, skin bleeding, internal bleeding, fever, and even gangrene. He points out that in recent years, no clearly identifiable case of this type has been reported as hysterical. This excludes, of course, temporary and superficial vasomotor issues like erythema and dermatographia. As a result, anuria and albuminuria have been removed from the hysteria textbooks, just as Babinski believes that hysterical edema and exaggerated reflexes will also eventually fade away. Hysteria cannot imitate everything; it can't replicate the distinct symptoms of organic paralysis.
Retention of urine after shell-shock.
Urine retention after shell shock.
Case 383. (Guillain-Barré and Barré, November 1917.)
An infantryman, 27, underwent shell-shock August 16, 1916, at four o’clock, from the nearby explosion of a big shell. He lost consciousness for a period of ten minutes, was sent to the regimental aid post, and twelve hours later brought to a hospital center, in a state of profound muscular weakness. He could not walk although he could make every movement of the legs. There was a marked diffuse cutaneous hyperesthesia. The reflexes were normal; the pupils were unequal, the right myotic. The lumbar puncture yielded a clear fluid under normal pressure, but with an excess of albumin. For three days, retention of urine was absolute, requiring the catheter. There was neither sugar nor albumin in the urine withdrawn. On the fourth day he was able to urinate spontaneously; the asthenia and other symptoms had disappeared in two or three weeks.
An infantryman, 27, experienced shell shock on August 16, 1916, at four o’clock, due to the nearby explosion of a large shell. He lost consciousness for about ten minutes, was taken to the regimental aid post, and twelve hours later was moved to a hospital center in a state of severe muscle weakness. He was unable to walk, although he could move his legs. There was noticeable widespread skin sensitivity. The reflexes were normal; his pupils were unequal, with the right one being constricted. A lumbar puncture produced clear fluid at normal pressure but with high levels of protein. For three days, he was completely unable to urinate, requiring a catheter. There was no sugar or protein found in the urine collected. On the fourth day, he was able to urinate on his own; the weakness and other symptoms had disappeared within two or three weeks.
Incontinence of urine after shell-shock and burial.
Inability to control urination after experiencing shell shock and being buried.
Case 384. (Guillain-Barré syndrome and Barré, November, 1917.)
An infantryman was subject to shell explosion and burial May 10, 1917. He lost consciousness for a few hours and spat blood for two days. He was carried to an evacuation hospital and thence to the neurological center at Amiens. Incontinence day and night lasted from the period of shock up to May 29, when the patient was transferred again, to another hospital. The man had never, either in childhood or adult life, had incontinence. He showed a slight tendency to latero-pulsion toward the left. Puncture fluid normal.
An infantryman was caught in a shell explosion and buried on May 10, 1917. He lost consciousness for a few hours and coughed up blood for two days. He was taken to an evacuation hospital and then to the neurological center in Amiens. He experienced incontinence day and night from the shock until May 29, when he was moved to another hospital. The man had never had incontinence in childhood or adult life. He displayed a slight tendency to lean to the left. Puncture fluid was normal.
Guillain and Barré report but 12 cases of sphincter disorder following shell-shock without external wound among hundreds of cases, and among 12 instances of sphincter disorder there were but three of incontinence, of which the above is one example. Incontinence lasted longer in these cases than retention. Guillain and Barré are unable to assign a cause for the findings.
Guillain and Barré report only 12 cases of sphincter disorder following shell shock without any external injury among hundreds of cases, and out of those 12 instances of sphincter disorder, only three involved incontinence, one of which is the example mentioned above. Incontinence lasted longer in these cases than retention. Guillain and Barré could not determine a cause for these findings.
Struck in back by shell splinter: Crural monoplegia; absence of plantar reflex.
Struck in the back by a shell fragment: Crural monoplegia; lack of plantar reflex.
Case 385. (Pauline, February, 1915.)
An infantryman, 20, was struck by a shell fragment in the small of the back while lying in the firing position, about 2 P.M. August 22, 1914, at Eth in Belgium. He felt as if he had been struck by the butt of a gun in the lumbar region. He was unable to get back with his comrades. His sack had been cut. He was without ammunition, and getting to a bridge he was able to jump a distance of about 8 meters. He fell and fainted. On coming to himself, his left side felt bad and he could not move his left leg. He dragged himself to the relief post which was being bombarded just as he arrived, and he got a bullet in the left frontal region.
An infantryman, 20, was hit by a shell fragment in the lower back while lying in his firing position around 2 PM on August 22, 1914, at Eth in Belgium. He felt like he had been hit by the butt of a gun in the lower back. He couldn't make it back to his comrades. His pack had been damaged. He was out of ammunition, and when he reached a bridge, he managed to jump about 8 meters. He fell and passed out. When he regained consciousness, his left side was in pain, and he couldn't move his left leg. He dragged himself to the relief post, which was being bombed just as he arrived, and he got hit by a bullet in the left forehead.
He was evacuated to another ambulance and decided to go back to France. Supported by his Lieutenant, he walked all night making about 35 kilometers on foot. He arrived at Charancy and got by train to Mont-Midi. On alighting, he could not walk. He said he was bent in two, and shuffled on in this position.
He was moved to another ambulance and decided to return to France. With help from his Lieutenant, he walked all night, covering about 35 kilometers on foot. He reached Charancy and took a train to Mont-Midi. When he got off, he couldn't walk. He said he was doubled over and shuffled along like that.
The “bent-back” lasted about a month, when he began to stand up again. He passed through various hospitals and was evacuated to the Salpêtrière. He then walked with the left leg in extension on the thigh and the foot in external rotation. He was hardly able to stand on either foot, and especially fell if he tried to stand on the left foot. He made no resistance to passive movements of the left lower extremity. The reflexes were normal except that the left plantar reflex was abolished. On the right, the plantar reflex was normal, and an attempt to elicit this reflex was followed by strong defensive movements. There was a tactile, thermic, and pain anesthesia of the foot and leg as far up as the lower third of the thigh. Above this anesthesia, there was a zone of hypesthesia. Position sense was also abolished in this region, and there was a bony hypesthesia likewise. A slight muscular atrophy (2 cm.) affected the lower leg and thigh.
The “bent-back” lasted about a month before he started to stand up again. He went through various hospitals and was eventually evacuated to the Salpêtrière. He walked with his left leg extended at the thigh and his foot rotated outward. He could barely stand on either foot and especially fell if he tried to stand on his left foot. He didn’t resist passive movements of his left leg. The reflexes were normal except for the left plantar reflex, which was absent. On the right side, the plantar reflex was normal, and an attempt to elicit this reflex resulted in strong defensive movements. There was a loss of sensation to touch, temperature, and pain in the foot and leg up to the lower third of the thigh. Above this area, there was a region of reduced sensitivity. The sense of position was also lost in this region, along with a diminished bony sensitivity. There was slight muscle atrophy (2 cm) in the lower leg and thigh.
There were no hereditary or acquired features of importance in the case except that there had been at 14 a chorea for a year. In particular this man appears not to have been an emotional person.
There were no important hereditary or acquired traits in this case, except that he had had chorea for a year when he was 14. In particular, this man does not seem to have been an emotional person.
The point in the case is the abolition of the plantar reflex on the left side, in association with a functional paraplegia and hemianesthesia.
The key issue in this case is the loss of the plantar reflex on the left side, along with functional paraplegia and hemianaesthesia.
Re plantar reflex modification in hysteria, Babinski believes that the same law which holds that hysteria is not in line to alter either the tendon reflexes or the pupil reflexes, is true for the skin reflexes. Dejerine brought forward three cases which appeared to him, however, to demonstrate absolutely that functional anesthesia might abolish or greatly diminish the skin reactions of the sole of the foot, that is, the plantar reflexes and movements of defense. Case 385 was alleged in support of Dejerine, as also were cases of Jeanselme and Huet, and of Sollier. Babinski’s critique of Dejerine’s cases ran to the effect that two of them showed contractures, and accordingly were not pure cases in which to demonstrate plantar reflexes or movements of defense. In the third case, Babinski at a meeting of the Neurological Society, himself obtained definite flexion of the little toes by stimulating the planta. According to Babinski, therefore, Dejerine’s cases, far from proving that hysterical anesthesia could abolish the plantar cutaneous reflexes, proved that hysterical contracture might mask reflex movements. Hysterical contracture, therefore, may be as important a factor to consider re reflexes as voluntary muscular contracture itself. As Babinski pointed out, many normal persons can keep the leg immobile when the sole is stimulated. Moreover, Babinski pointed out, many cases regarded as hysterical were actually cases of a physiopathic or reflex nature which had actually undergone trauma. It will be noted that the above case of Paulian is just such a case of trauma.
Re plantar reflex modification in hysteria, Babinski believes that the same principle which states that hysteria doesn't change tendon or pupil reflexes also applies to skin reflexes. Dejerine presented three cases that he thought clearly showed that functional anesthesia could either eliminate or significantly reduce the skin reactions of the sole of the foot, specifically the plantar reflexes and defensive movements. Case 385 was cited in support of Dejerine, as well as cases from Jeanselme, Huet, and Sollier. Babinski's critique of Dejerine's cases argued that two of them exhibited contractures, making them unsuitable examples for demonstrating plantar reflexes or defensive movements. In the third case, during a meeting of the Neurological Society, Babinski was able to induce noticeable flexion of the little toes by stimulating the sole. Therefore, according to Babinski, Dejerine's cases did not prove that hysterical anesthesia could abolish plantar cutaneous reflexes, but rather demonstrated that hysterical contracture might obscure reflex movements. Hysterical contracture, then, may be as significant a factor to consider re reflexes as voluntary muscle contracture itself. As Babinski noted, many normal individuals can keep their leg still when the sole is stimulated. Additionally, Babinski mentioned that many cases thought to be hysterical were actually instances of a physiopathic or reflex nature that had experienced trauma. It is noteworthy that the aforementioned case of Paulian is one such trauma case.
Shell-shock; unconsciousness: Crural monoplegia; sciatica (neural changes).
Shell shock; unconsciousness: one-sided paralysis of the leg; sciatica (nerve changes).
Case 386. (Souques, February, 1915.)
A reserve lieutenant, September, 1914, was blown up by a shell and lost consciousness for an hour. On coming to, he felt pains in the loins, right thigh, knee and heel, and found himself unable to move the right leg at all. Urinary incontinence lasted three or four days. Violent pains lasted weeks, now and then actual crises (sleep only with hypnotics).
A reserve lieutenant, September 1914, was hit by a shell and lost consciousness for an hour. When he regained awareness, he felt pain in his lower back, right thigh, knee, and heel, and was completely unable to move his right leg. He experienced urinary incontinence for three or four days. Intense pain persisted for weeks, sometimes resulting in actual crises (he could only sleep with the help of sedatives).
The pains then passed off. The flaccid crural monoplegia lasted. There was a hydrarthrosis of the right knee and a sciatica (physical nerve changes?) and a crural monoplegia without trophic, electrical, reflex or vesico-rectal trouble. Lumbar puncture showed no lymphocytes or excess of albumin. It would, of course, be difficult to tell whether this case was hysteria or simulation.
The pain eventually went away. The weak leg paralysis persisted. There was swelling in the right knee and sciatic nerve issues (physical nerve changes?) along with leg paralysis without any problems related to nutrition, electrical activity, reflexes, or bowel and bladder control. A spinal tap showed no white blood cells or excess protein. It would definitely be hard to determine if this case was hysteria or simply pretending.
Re hysterical monoplegia, Babinski inquires whether a hysterical monoplegia can automatically appear as a result of emotion without any intellectual element whatever. Emotion produces sweat, diarrhea or erythema, without any intellectual intermediate. Can emotion—that is, emotional shock—produce a monoplegia in the same way as it produces an erythema? The narratives of patients might indicate that emotion can do such things. But according to Babinski there is no genuine case of monoplegia or paraplegia directly produced by emotional shock. One must be careful in this discussion not to confuse emotional shock and emotion of a gradual nature. Babinski wishes to define emotion as a violent affective change as a result of a sudden mental shock upsetting physiologic or psychic balance during a usually brief period. As for the more gradual affective states or emotions, there is obviously so much of the imaginative and intellectual compounded therewith, that plenty of opportunity exists for the production by suggestion of such phenomena as monoplegia, paraplegia, hemi-anesthesia.
Re hysterical monoplegia, Babinski questions whether hysterical monoplegia can arise solely from emotion without any intellectual involvement. Emotion can trigger symptoms like sweating, diarrhea, or redness without an intellectual intermediary. Can emotional shock lead to monoplegia in the same way it causes redness? Patient accounts might suggest this is possible. However, Babinski argues that there is no true instance of monoplegia or paraplegia that is directly caused by emotional shock. It’s important to distinguish between emotional shock and gradual emotional responses in this discussion. Babinski defines emotion as a sudden and intense affective change due to a mental shock that disrupts physiological or psychological balance for a typically short time. In contrast, more gradual emotional states incorporate a significant amount of imagination and intellect, creating ample opportunity for suggestion to produce phenomena like monoplegia, paraplegia, or hemi-anesthesia.
Re sciatica, see remarks above under Case 329.
Re sciatica, refer to the comments above under Case 329.
Functional paraplegia and internal popliteal neuritis.
Functional paraplegia and internal popliteal neuritis.
Case 387. (Roussy, February, 1915.)
A Zouave was taken out from under a trench shelter beam, the night of December 21, 1914, at Tracy-le-Mont. The beam had fallen upon eight men, killing one, and striking the Zouave in the hypogastrium. He was pulled out two hours later, unable to take a step. He was evacuated on his back, to Paris; stayed a month in the hospital at Croix-Rouge, bedfast. According to the patient, he was entirely anesthetic in the legs. He went to Villejuif, January 22, with the diagnosis of spinal contusion and hemiplegia. He could then walk on crutches, leaning on the left leg. He felt a sharp pain at the level of the spinous process of the first lumbar vertebra and all along the sacrum. Spontaneous movements of the left leg were possible, but they were slow and weak. The hypesthesia rose to the navel. There was a suggestion of a cauda syndrome. The knee-jerks were normal, but on the left side the Achilles jerk was absent. There was a partial R. D. in the posterior muscles of the left leg.
A Zouave was taken out from under a trench shelter beam on the night of December 21, 1914, at Tracy-le-Mont. The beam had fallen on eight men, killing one and injuring the Zouave in the lower abdomen. He was rescued two hours later, unable to stand. He was evacuated on his back to Paris, where he spent a month in bed at the Croix-Rouge hospital. According to him, he had no feeling in his legs. He went to Villejuif on January 22, diagnosed with spinal contusion and hemiplegia. At that point, he could walk using crutches, leaning on his left leg. He experienced sharp pain at the level of the spinous process of the first lumbar vertebra and along the sacrum. He had some spontaneous movement in his left leg, but it was slow and weak. There was decreased sensation up to the navel, and symptoms suggested a cauda equina syndrome. His knee reflexes were normal, but the Achilles reflex was absent on the left side. There was partial atrophy in the posterior muscles of the left leg.
The diagnosis was functional paraplegia plus left internal popliteal neuritis. The crutches were removed, he was isolated, and given motor reëducation. In a week he was able to walk alone with ease.
The diagnosis was functional paraplegia along with left internal popliteal neuritis. The crutches were taken away, he was isolated, and he received motor reeducation. Within a week, he was able to walk independently with ease.
Re popliteal nerve lesions, Athanassio-Benisty remarks that the external popliteal nerve of the leg resembles pathologically the musculospiral nerve of the arm, whereas the internal popliteal behaves like the median. The musculospiral nerve of the arm shows very variable and usually slight sensory changes. The median nerve more than any other nerve in the arm yields painful sensations during its recovery from section.
Re popliteal nerve injuries, Athanassio-Benisty notes that the external popliteal nerve in the leg is pathologically similar to the musculospiral nerve in the arm, while the internal popliteal nerve acts more like the median nerve. The musculospiral nerve in the arm shows quite a bit of variability and typically minor sensory changes. The median nerve, more than any other nerve in the arm, experiences painful sensations as it heals from a cut.
Re differentiation of peripheral neuritis and hysterical paralysis, Babinski gives as signs peculiar to neuritis, and never found in hysterical paralysis, the following: (a) diminution or loss of bone and tendon reflexes; (b) muscular[541] atrophy (except for slight amyotrophy exceptionally found in hysteria); (c) the reaction of degeneration (only of value after eight or ten days); (d) hypotonus; (e) distribution characteristic of peripheral motor sensory and trophic disorder.
Re differentiating peripheral neuritis from hysterical paralysis, Babinski identifies signs unique to neuritis, which are never observed in hysterical paralysis, including: (a) reduced or absent bone and tendon reflexes; (b) muscle[541] atrophy (except for minor amyotrophy that may occur in hysteria); (c) the reaction of degeneration (which is only significant after eight or ten days); (d) low muscle tone; (e) specific patterns of peripheral motor sensory and trophic disorders.
Re diagnosis of organic paraplegia as against hysterical paraplegia, the latter is to be recognized chiefly by the absence of the organic signs, as (a) alteration of tendon reflexes, (b) the Babinski sign (toe phenomenon), (c) exaggeration of defense reflexes (dorsal flexion of foot on sharp pinching of dorsum of foot or leg), (d) muscular atrophy with R. D., (e) sphincter disorder, (f) skin changes, such as decubitus.
Re diagnosing organic paraplegia versus hysterical paraplegia, the latter should mainly be identified by the lack of organic signs, such as (a) changes in tendon reflexes, (b) the Babinski sign (toe phenomenon), (c) heightened defense reflexes (dorsal flexion of the foot when pinched sharply on the top of the foot or leg), (d) muscle wasting with R. D., (e) issues with sphincter control, and (f) skin changes, like bedsores.
Bullet in hip: Local “stupor” of leg.
Bullet in hip: Local "numbness" of leg.
Case 388. (Sebileau, November, 1914.)
A Moroccan sharpshooter, 20, was wounded September 27, at Soissons. One bullet scratched the left thigh. A second entered below the anterosuperior iliac spine at least 6 cm. outside the femoral artery and emerged above the ischiotrochanteric line, 2 cm. above and 4 cm. behind the upper extremity of the great trochanter, thus passing through the tensor of the fascia lata and without breaking a bone.
A 20-year-old Moroccan sharpshooter was injured on September 27 in Soissons. One bullet grazed his left thigh. A second bullet entered below the front upper part of the hip bone at least 6 cm away from the femoral artery and exited above the ischiotrochanteric line, 2 cm above and 4 cm behind the top of the greater trochanter, passing through the tensor fasciae latae without fracturing any bones.
There was a complete paralysis of the left leg. The man had to walk with a crutch and a cane, dragging the leg like a weight. There was no active or passive movement of thigh, lower leg and foot muscles, except that there was a slight tendency to abduction of the toes, from innervation of the dorsal interossei of the foot. The iliopsoas was also involved, as well as the gluteal and pelvic trochanteric muscles. There was a certain amount of muscular tone preserved, so that the bony elements of the skeleton were held together. The foot did not fall and the leg did not elongate, as it might have in a case of paralysis of the sciatic nerve. Electro-diagnosis showed an early reaction of degeneration according to one examiner, but Sebileau believes that there was no R. D. There was anesthesia of a large part of the leg, which stretched over the anterior and internal aspects of the thigh, covered the entire territory of obturator and crural nerves but did not stretch above the fold of the groin. The region of the femorocutaneous nerve was slightly sensitive and the posterior aspect of the thigh and buttock was sensitive. There was a slight sensation on the external aspect of the lower leg. Foot and toes were entirely insensitive. The anesthesia was for all forms of common sensation. No vasomotor, thermic or trophic disorder. The reflexes were all abolished, except for a tendency to cremasteric reflex. It is clear that these conditions cannot be simulated. Possibly they are hysteric and to be explained on the basis of a kind of autosuggestion or perhaps, according to Sebileau, the local and nervous[543] apparatus under the mechanical and caloric effects of the fragment had undergone a sort of local stupor. No large nerve could have been affected by the injury, according to the analysis made by Sebileau.
The left leg was completely paralyzed. The man had to use a crutch and a cane, dragging his leg like a heavy weight. There was no movement in the thigh, lower leg, or foot muscles, except for a slight tendency of the toes to move outward due to the activation of the dorsal interossei in the foot. The iliopsoas, gluteal, and pelvic trochanteric muscles were also affected. Some muscle tone was still preserved, keeping the bones of the skeleton in place. The foot didn’t drop, and the leg didn’t stretch, which could have happened if the sciatic nerve had been paralyzed. Electrodiagnostic tests showed early signs of degeneration according to one examiner, but Sebileau argued there was no degeneration. There was loss of sensation over a large part of the leg, covering the front and inner thigh, as well as the entire areas supplied by the obturator and femoral nerves, but it didn’t extend above the groin fold. The area around the femoral cutaneous nerve was slightly sensitive, and the back of the thigh and buttock had some sensitivity. There was a little sensation on the outer side of the lower leg. The foot and toes were completely numb. The loss of sensation affected all normal sensations. There were no issues with blood flow, temperature, or tissue health. All reflexes were missing, except for a slight chance of a cremasteric reflex. It’s clear that these symptoms can’t be faked. They might be hysterical and could be explained by some form of autosuggestion or, according to Sebileau, as the local and nervous system being in a state of temporary shock due to the mechanical and heat effects of the injury. No major nerve seemed to be affected by the injury according to Sebileau’s analysis.[543]
Re stupor, see Case 253 of Tinel. Re such local “stupor” it may be noted that this case was published in 1914, before Babinski’s larger publications on reflex disorders. As for the loss of cutaneous reflexes, Babinski remarks that immersion in hot water may cause the cutaneous reflexes in the so-called physiopathic cases to reappear for a time. He regards the loss of cutaneous reflexes in the physiopathic cases as due to a circulatory disturbance, and recalls the fact that compression by an Esmarch bandage can cause the tendon reflexes to vanish for a time, and can even cause pathologically excessive reflexes to disappear. The cutaneous reflexes have also been caused to disappear by compression.
Re stupor, see Case 253 of Tinel. Re such local “stupor,” it's worth mentioning that this case was published in 1914, before Babinski’s more extensive works on reflex disorders. Regarding the loss of skin reflexes, Babinski notes that soaking in hot water may temporarily restore the skin reflexes in so-called physiopathic cases. He believes that the loss of skin reflexes in these cases is due to circulatory issues and points out that compression from an Esmarch bandage can temporarily eliminate tendon reflexes and even cause pathologically excessive reflexes to vanish. Skin reflexes can also be made to disappear through compression.
According to Babinski, Sebileau’s explanation that such matters as loss of reflexes could be explained by autosuggestion is erroneous.
According to Babinski, Sebileau’s suggestion that things like loss of reflexes can be explained by autosuggestion is incorrect.
Re muscular hypertonus in reflex cases, Babinski remarks that though it may be very pronounced, it is as a rule restricted in area. Re sensory disorders in reflex cases, pains are found (they were very slight ones in the present case); hypesthesia has also been found by Babinski.
Regarding muscle tightness in reflex cases, Babinski notes that while it can be quite severe, it is usually limited in scope. Concerning sensory disorders in reflex cases, pain is present (which was very mild in this instance); hypesthesia has also been observed by Babinski.
Localized catalepsy: Hysterotraumatic.
Localized catalepsy: Hysterical trauma.
Case 389. (Sollier, January, 1917.)
An invalided soldier had been suffering for a year with marked atrophies and the right knee in extension. There had been a bullet wound of the upper third of the tibia, which did not affect the joint. There was a total anesthesia, both superficial and deep, which stopped sharply at the upper part of the thigh. At the time of the very first examination, this apparent ankylosis was reduced, to the great stupefaction of the patient. There was, however, a peculiar phenomenon in this subject. There was a localized catalepsy of the limb, which was able to preserve any desired attitude in which it was placed; and this attitude could be indefinitely prolonged, just as in cataleptic hysterics. Here, then, was a case of localized hystero-traumatism precisely imitating the classical hysteria of Charcot except for its localization.
A disabled soldier had been suffering for a year with significant muscle wasting and a locked right knee. He had a bullet wound in the upper part of the tibia that didn’t affect the joint. There was complete loss of sensation, both superficial and deep, which abruptly stopped at the upper thigh. When he was first examined, this apparent stiffness in the joint was surprisingly reduced, much to the patient’s amazement. However, there was a strange phenomenon in this case. The limb exhibited a localized type of catalepsy, allowing it to hold any position it was put in; this position could be maintained indefinitely, similar to what is seen in cataleptic hysteria. So, this was a case of localized trauma-induced hysteria that closely resembled classical hysteria described by Charcot, except for its specific localization.
Re hysterotraumatism, Charcot developed ideas concerning trauma and localized hysteria in 1886, thereby overthrowing the ideas of Erichsen concerning the organic nature of “railway spine” and “railway brain” as developed twenty years before. In a case of local trauma such as the bullet-wound of Case 388, Babinski’s explanation would be that the pain and inhibition of movement resulting from the bullet wound at the time of injury, formed the focus of a process of autosuggestion. According to Babinski’s figure, the organic factor acts as a bait for the hysterical symptoms. According to the Salpêtrière experience, hysteria is incapable of producing a real superficial and deep anesthesia such as is mentioned for this case. For example, no hysterical patient in the Charcot clinic, according to Sicard, could undergo a scalpel operation without some general or local anesthetic. When, therefore, a true deep anesthesia occurs, Sicard’s conception would be that the anesthesia is not a truly hysterical one but belongs to the group of physiopathic phenomena.
Re hysterotraumatism, Charcot introduced ideas about trauma and localized hysteria in 1886, challenging Erichsen's views on the organic nature of “railway spine” and “railway brain” that had been established twenty years earlier. In a case of localized trauma like the bullet wound of Case 388, Babinski would explain that the pain and restricted movement caused by the bullet wound at the time of injury became the focus of a process of autosuggestion. According to Babinski’s theory, the organic factor serves as a bait for the hysterical symptoms. Based on experiences from the Salpêtrière, hysteria cannot create a true superficial or deep anesthesia as seen in this case. For instance, no hysterical patient at Charcot's clinic, according to Sicard, could undergo a scalpel operation without some form of general or local anesthetic. Thus, when true deep anesthesia occurs, Sicard would argue that it is not genuinely hysterical but falls under the category of physiopathic phenomena.
Contracture: Hysterotraumatic.
Contracture: Trauma-related.
Case 390. (Sollier, January, 1917.)
A sailor, 41, got hygroma of the right knee in 1915, was operated on in July, returned to his dépôt a month later, and thence to Vizille Urage by reason of contracture in extension of the right leg. It was thought he was simulating (since there was no muscular atrophy), and he was sent to the neurological center, where under anesthesia the joint was found free. This man developed, when the knee was bent, extraordinary cracklings in the joint, and he showed pain unequivocally, making a defensive movement, partly reflex, partly voluntary, when the leg was flexed beyond a certain point. There was 3.5 cm. atrophy in the thigh, a reflex atrophy due to the joint disorder. There were no other signs of hysterotraumatic contracture.
A 41-year-old sailor developed hygroma in his right knee in 1915, had surgery in July, returned to his depot a month later, and then went to Vizille Urage due to a contracture in the extension of his right leg. They suspected he was faking it (since there was no muscle wasting), and he was sent to the neurological center, where they found the joint to be free under anesthesia. When the knee was bent, he experienced unusual crackling sounds in the joint and displayed pain clearly, making a defensive movement, partly reflexive and partly voluntary, when his leg was bent beyond a certain point. There was a 3.5 cm muscle wasting in the thigh, a reflex atrophy caused by the joint issue. No other signs of hysterotraumatic contracture were present.
According to Sollier, the diagnosis of hysterotraumatic contractures depends upon: first, a characteristic special attitude of the contractured limb; secondly, the participation of the antagonists as a group (global); thirdly, the superposition of sensory disorder upon motor disorder (Charcot’s law); fourthly, the segmentary topography of sensory disorder; fifthly, the extension of the contractured joint; sixthly, the persistence of the contracture in the same form, whether at rest or in attempted movements; seventhly, muscular rigidity; eighthly, normal tendon reflexes; ninthly, normal electrical reactions (though R. D. is hard to determine in muscles contracted to the maximum); tenthly, special reactions during attempts to reduce, such as pains, and equal and regular resistance to changed attitude, pseudoclonus in cases of foot contracture; eleventhly, immediate reproduction of the contracture after reduction under chloroform; twelfthly, co-existence of various hysterical stigmata.
According to Sollier, diagnosing hysterotraumatic contractures relies on: first, a distinct position of the contracted limb; second, the involvement of the antagonistic muscles as a whole; third, the overlap of sensory issues with motor problems (Charcot’s law); fourth, the specific pattern of sensory issues; fifth, the extent of the contracted joint; sixth, the durability of the contracture in the same way, whether at rest or during attempted movements; seventh, muscle stiffness; eighth, normal tendon reflexes; ninth, normal electrical responses (although it's difficult to assess reflexes in fully contracted muscles); tenth, particular reactions during attempts to correct the position, such as pain, and consistent resistance to changes in position, along with pseudoclonus in cases of foot contracture; eleventh, the immediate reappearance of the contracture after being corrected under chloroform; twelfth, the presence of various hysterical signs.
Crural monoplegia, tetanic. Recovery.
Leg paralysis, spasms. Recovery.
Case 391. (Routier, 1915.)
An ensign was wounded by a shell splinter in the right scapular region September 25, 1915. A large hematoma was drawn off and drains inserted. Antitetanic serum was given 24 hours after the trauma. The wound looked well. The patient complained merely of the heaviness of his arm, and after September 27, the temperature fell to normal. Magnesium chloride solution was applied every other day, and progress was so good that evacuation was ordered.
An ensign was injured by a shell fragment in the right shoulder area on September 25, 1915. A large bruise was drained, and drains were inserted. Antitetanic serum was administered 24 hours after the injury. The wound was healing well. The patient only complained about the heaviness in his arm, and after September 27, his temperature returned to normal. Magnesium chloride solution was applied every other day, and progress was so good that evacuation was scheduled.
However, October 8, the patient suddenly began to complain of a sharp pain in the right thigh, which next day became intolerable and threw the muscles into a slight contracture, the adductors being extremely stiff. Headache developed in the course of the day, with slight stiffness of neck, exaggeration of reflexes in the right leg, and ankle clonus. Temperature: 37.6 morning, 38.5 evening. The patient was isolated and given chloral.
However, on October 8, the patient suddenly started to complain of sharp pain in the right thigh, which became unbearable the next day and caused the muscles to slightly contract, with the adductors being very stiff. By the end of the day, the patient developed a headache, experienced slight stiffness in the neck, and had heightened reflexes in the right leg, along with ankle clonus. Temperature was 37.6 in the morning and 38.5 in the evening. The patient was isolated and given chloral.
October 10, paroxysmal crises of pain, more marked stiff neck, and lumbar stiffness appeared, with nervousness, photophobia, and hyperesthesia to noise. The wound seemed to be doing well. Chloral was given.
October 10, intense episodes of pain, more pronounced neck stiffness, and lower back tightness emerged, along with anxiety, light sensitivity, and increased sensitivity to noise. The wound appeared to be healing well. Chloral was administered.
Slight trismus developed October 11. The tongue became dry and the patient drank little. The condition held and the same treatments were repeated up to October 15, when the temperature fell and the contractures and pains were diminished. The chloral was continued. There were still a few cramps in the neck. October 22, however, the patient was practically well.
Slight jaw stiffness developed on October 11. The tongue became dry and the patient drank very little. This condition persisted, and the same treatments were repeated until October 15, when the temperature dropped and the muscle tightness and pain decreased. The chloral treatment continued. There were still a few cramps in the neck. By October 22, however, the patient was almost fully recovered.
We are here dealing with an instance of local tetanus of monoplegic form, developing a fortnight after the wound (there is an early group developing, as a rule, from the fifth to the tenth day, and a group of later development, after the twentieth day; the interval in this case was of intermediate duration). According to Courtois-Suffit and Giroux, the differential diagnosis is not easy, since, besides[547] tetanus, must be considered tetany, spastic monoplegia of cerebral or spinal origin, partial hemiplegia, peripheral neuritis, contractures due to bone, joint, muscle or tendon lesions, strychnine intoxication and hysterical contractures. Three cases out of six described by Routier were fatal.
We are dealing with a case of local tetanus in the monoplegic form that developed two weeks after the injury (usually, there's an early development group that appears between the fifth and tenth day, and a later development group after the twentieth day; in this case, the duration was in between). According to Courtois-Suffit and Giroux, it’s not easy to make a differential diagnosis since, in addition to [547] tetanus, you also have to consider tetany, spastic monoplegia from cerebral or spinal causes, partial hemiplegia, peripheral neuritis, contractures due to bone, joint, muscle, or tendon injuries, strychnine poisoning, and hysterical contractures. Three out of six cases described by Routier were fatal.
Re differential diagnosis of tetanic conditions, see Courtois-Suffit and Giroux in the Collection Horizon. The cases as a rule appear in subjects that have had serum treatment, and may occur in subjects in whom no trismus ever develops (the above case showed slight trismus).
Re differential diagnosis of tetanic conditions, see Courtois-Suffit and Giroux in the Collection Horizon. The cases usually appear in individuals who have undergone serum treatment, and may occur in those who never develop trismus (the above case showed slight trismus).
The recognition of localized tetanic contracture is based upon (a) the intensity of the contracture, which causes the limb to feel wooden (in one case the foot, leg, and thigh were welded to the pelvis like an iron bar); (b) paroxysmal contractions resembling those of tetanus, confined to one limb, and started by a variety of external causes, forming the principal symptom in the disease; (c) contracture of comparatively brief duration (hardly ever over two or three weeks). A slight fever may help in the differential diagnosis.
The identification of localized tetanic contracture is based on (a) the severity of the contracture, which makes the limb feel stiff (in one case, the foot, leg, and thigh were stuck to the pelvis like an iron rod); (b) sudden contractions similar to those in tetanus, limited to one limb, triggered by various external factors, making it the main symptom of the condition; (c) contracture that lasts for a relatively short time (rarely more than two or three weeks). A mild fever may assist in the differential diagnosis.
Wound of left leg: Local spasms, later contracture, and painful crises (these associated with suppuration), the whole treated as tetanic.
Wound on the left leg: Local spasms, followed by contracture and painful episodes (these linked to infection), all treated as tetanus.
Case 392. (Mériel, 1916.)
An infantryman was wounded by shell fragments September 28, 1915, at Virginy and was given a first dressing an hour later and a second at the ambulance, where antitetanic injection was also made. October 3, the patient arrived at Foix, showing a superficial wound of the left frontal region, a penetrating wound of the upper third of the left thigh, and another in the lower third of the left lower leg.
An infantryman was injured by shell fragments on September 28, 1915, at Virginy and received a first dressing an hour later and a second one at the ambulance, where he also got an antitetanic injection. On October 3, the patient arrived at Foix, showing a superficial wound on the left frontal area, a penetrating wound in the upper third of the left thigh, and another in the lower third of the left lower leg.
The evening of October 8, the man began to feel pain in the left leg, though the wounds looked well and there was no fever. October 9, sudden involuntary contractions of the left leg developed, and these increased in amplitude if the limb was touched. The other extremities were normal. Temperature 38.2; pulse 102. Restlessness at night.
The evening of October 8, the man started to feel pain in his left leg, although the wounds looked fine and there was no fever. On October 9, he experienced sudden, uncontrollable spasms in his left leg, which got worse when the limb was touched. The other limbs were normal. Temperature was 38.2; pulse was 102. He was restless at night.
Next day 10 c.c. of antitetanic serum was administered and more on the 11th, with chloral and isolation; but on the evening of the 11th, with the contractions still completely localized to the left lower extremity, came an extremely painful crisis interfering with sleep and at last requiring morphine. Up to the 15th the antitetanic injections, chloral and morphine were continued, but on the 15th the contractions were replaced in part by a contracture affecting the muscles of the posterior aspect of the thigh. In the meantime, the patient howled with pain, especially in the night. Chloral and morphine were given.
The next day, 10 c.c. of antitetanic serum was given, with more on the 11th, along with chloral and isolation. However, on the evening of the 11th, with the contractions still only affecting the left lower leg, there was an extremely painful crisis that disrupted sleep and ultimately required morphine. Until the 15th, the antitetanic injections, chloral, and morphine continued, but on the 15th, the contractions were partially replaced by a contracture affecting the muscles on the back of the thigh. In the meantime, the patient cried out in pain, especially at night. Chloral and morphine were administered.
During the next five days the contractures and pains became still more violent, and on the 21st the antitetanic injections were begun once more and kept up through the 26th in 5 c.c. doses.
During the next five days, the contractions and pain became even more intense, and on the 21st, the anti-tetanus injections were resumed and continued until the 26th in 5 c.c. doses.
The patient began to urinate in bed and to be delirious. The contractions now disappeared, but the contracture persisted. Antitetanic serum was given every other day from October 28 to November 2; every third day from November[549] 4 to November 19; every fourth day from November 22 to December 3; and every fifth day from December 3 to December 17. The chloral was diminished from 15 to 5 grams per diem and by the 20th of December all administration of chloral had ceased. The morphine was given up December 25.
The patient started wetting the bed and was experiencing delirium. The contractions stopped, but the stiffness remained. Antitetanic serum was administered every other day from October 28 to November 2; every third day from November[549] 4 to November 19; every fourth day from November 22 to December 3; and every fifth day from December 3 to December 17. The dose of chloral was reduced from 15 to 5 grams a day, and by December 20, chloral was no longer given. The morphine was stopped on December 25.
The tetanic symptoms of the left leg now gradually diminished. The leg, which had been flexed at a right angle, began to extend little by little, and the toes, which had been strongly flexed, reassumed their normal position. The wounds suppurated freely during the tetanic crises, but then healed. In January the man could get up and walk, dragging his leg somewhat, and January 20 a complete recovery had been obtained. There was no hysteria in the history of this patient, although the man was subject to “professional” alcoholism, being carter for a wholesale wine dealer, drinking 5 liters of wine a day.
The tetanic symptoms in his left leg gradually faded. The leg, which had been bent at a right angle, began to straighten out little by little, and the toes, which had been tightly curled, returned to their normal position. The wounds drained freely during the tetanic episodes but eventually healed. By January, the man was able to get up and walk, dragging his leg a bit, and by January 20, he had made a complete recovery. There was no history of hysteria in this patient, although he was prone to "professional" alcoholism, working as a cart driver for a wholesale wine dealer, consuming 5 liters of wine a day.
Shell-shock by windage: Hysterical paraplegia, flaccid type, develops 10 days later, after strain, capture, privation, recapture. Paraplegia at first complete. Recovery by suggestion (one séance).
Shell-shock from windage: Hysterical paralysis, flaccid type, develops 10 days later, after stress, capture, deprivation, and recapture. Paralysis is initially complete. Recovery through suggestion (one session).
Case 393. (Leri, February, 1915.)
A corporal, 21, told how at Goselmind, during the Sarrebourg retreat, August 20, 1914, a shell burst a meter behind him, flattening his knapsack, throwing him to the ground, blowing him forward (as he said, by the pressure of the air) seven or eight meters, leaving him stunned though conscious for about twenty minutes. Uhlans fell upon him but did not trouble themselves further with him as he could not walk. He crawled along on elbows and knees about a kilometer and a half to some Frenchmen in a wood. He now found himself able to walk a whole day supported by two comrades, making about 12 kilometers. He got by carriage to Gerbéviller, but here fell again into the hands of Germans, who left him nine days in the corner of a barn without care. Gerbéviller was retaken, and he was evacuated to Bayon.
A corporal, 21, recounted how at Goselmind, during the Sarrebourg retreat on August 20, 1914, a shell exploded a meter behind him, crushing his knapsack and knocking him to the ground. He was propelled forward (as he described it, by the force of the air) seven or eight meters, left dazed but aware for about twenty minutes. Uhlans attacked him but didn’t bother with him once they realized he couldn’t walk. He crawled on his elbows and knees for about a kilometer and a half to reach some French soldiers in a nearby wood. He then managed to walk for an entire day, supported by two comrades, covering around 12 kilometers. He took a carriage to Gerbéviller, but there he fell into the hands of the Germans again, who left him in a corner of a barn without care for nine days. Gerbéviller was recaptured, and he was evacuated to Bayon.
He had now had for some time pains in the kidney region below the point struck, some difficulty in turning his head, and some numbness and jerkings in the legs; and the legs that had carried him 14 kilometers were unable to move at all, even in bed. It was only 8 days later that he could perform the slightest movement, and two months followed before he could go a few steps on crutches. December 14, three months and a half after his accident,—he was demonstrated as “spinal contusion.” Upon examination, however, there were no reflex disorders, no sensory disorders, and the muscular weakness was equal in all parts of the lower extremities and trunk. On crutches, he lunged the trunk forward, painfully dragging his legs one after the other, the right foot in external rotation, never passing the left foot, toes scraping ground,—a functional flaccid paraplegia, completely dissolved by suggestion at a single sitting.
He had been experiencing pain in his kidney area for a while now, along with some difficulty turning his head and numbness and spasms in his legs. The legs that had carried him 14 kilometers were completely unable to move, even in bed. It took him eight days before he could make the slightest movement, and it was two months later that he could take a few steps using crutches. On December 14, three and a half months after his accident, he was diagnosed with “spinal contusion.” However, upon examination, there were no reflex disorders, no sensory disorders, and the muscular weakness was consistent throughout all parts of his lower body and trunk. Using crutches, he leaned forward, painfully dragging his legs one after the other, with his right foot turned outward and never moving past his left foot, his toes scraping the ground—a condition of functional flaccid paraplegia, completely resolved by suggestion in a single session.
Scalp wound; probably no loss of consciousness: Quadriparesis, later paraplegia; tremors; profound sensory disorders, some apparently hysterical; cataleptic rigidity of (anesthetic) legs on passive movement. Diagnosis?
Scalp wound; likely no loss of consciousness: Weakness in all four limbs, later loss of movement in the legs; tremors; severe sensory issues, some seemingly hysterical; cataleptic stiffness in the (anesthetic) legs during passive movement. Diagnosis?
Case 394. (Clarke, July, 1916.)
A soldier, 40, got a scalp wound but probably did not lose consciousness. However, when observed three months after the injury, though fat and well-looking, the patient could not stand or walk, and his hands and arms were feeble. He complained of headache, insomnia and anorexia, and remained in a state of mental inertia. All efforts to read and write produced fatigue. Memory was bad both for remote and for recent events. He was able to feed himself slowly, execute a few movements of arms and hands, and raise his feet from the bed. Upon passive movement, there was a sort of spastic state, which did not amount to a true rigidity. Now and then a clonic spasm was induced by such passive movements. After the repetition of those few voluntary movements which were possible, the muscles passed into a flaccid condition. There was a tremor of a type called swooping; the tremor resembled that of Friedreich’s disease, such as is thought to occur in cases of marked loss of muscular sense. The deep reflexes were exaggerated. Concentric narrowing of the visual fields was easily induced by testing them. There was a general slight dulness of perception on sensory tests. There was astereognosis, and apparently an absolute loss of position sense. Movements of the large joints through an angle of 90 degrees were, however, vaguely recognized. Although the patient could not touch, for example, his left forefinger with his right, yet, if he had once seen the position of a limb and it was not moved, he could remember its position and touch it after some time. His localizing sense was from two to four inches out in the hands, the localization being generally of points proximal to the point tested.
A 40-year-old soldier suffered a scalp wound but likely didn’t lose consciousness. However, when examined three months later, he appeared healthy and overweight but couldn’t stand or walk, and his hands and arms were weak. He complained of headaches, insomnia, and loss of appetite, and seemed to be in a state of mental sluggishness. Any attempts to read or write made him tired. His memory was poor for both past and recent events. He could feed himself slowly, make a few movements with his arms and hands, and lift his feet off the bed. When moved passively, his muscles showed some spasticity, but it wasn’t full rigidity. Occasionally, passive movements caused clonic spasms. After repeating the few possible voluntary movements, his muscles would become weak and floppy. He had a type of tremor called swooping, resembling that seen in Friedreich’s disease, which is thought to occur with significant loss of muscle awareness. His deep reflexes were heightened. Constricting the visual fields was easily achieved during tests. Overall, there was a slight dullness in sensory perception. He had astereognosis and seemingly a complete loss of positional awareness. However, he could vaguely recognize movements of large joints through a 90-degree angle. Although he couldn’t touch his left forefinger with his right hand, if he had seen a limb’s position and it remained still, he could remember where it was and touch it later. His ability to localize stimuli was off by two to four inches in his hands, with the localization generally pointing to areas above the tested point.
Two months later the patient was somewhat less dull and apathetic. His memory had improved. He was able to read, and he was successfully making a rug; but the legs were worse, having become anesthetic to touch and pain. When the legs were placed in any position, they would assume a cataleptic rigidity, and remain rigidly fixed in any position for some time. The patient could sit up in bed. The muscles were well nourished and the electric reactions were normal.
Two months later, the patient was a bit less dull and apathetic. His memory had improved. He could read and was successfully making a rug, but his legs were worse, having lost feeling to touch and pain. When his legs were put in any position, they would become stiff and stay rigidly fixed for a while. The patient could sit up in bed. The muscles were well-nourished, and the electric responses were normal.
Re catatonic rigidity, see Case 389 (Sollier).
Re catatonic rigidity, see __A_TAG_PLACEHOLDER_0__ (Sollier).
Shell explosion; pitched in air: Spasmodic contractions of sartorii, persistent in sleep.
Shell explosion; propelled into the air: Uncontrollable muscle contractions of the sartorius, lingering even in sleep.
Case 395. (Myers, January, 1916.)
A private, 23, was admitted to a casualty clearing station and the next day told the examiner, Major Myers, that the Germans had been sending whizz-bangs and coal-boxes over, and the last he remembered was being on guard and then digging himself out of fallen sandbags. His comrades told him that he had been pitched in the air, but this he did not remember. He remembered running to the shell trench, but finding this “too hot,” he returned to the firing trench, noticing on the way that he could not see well. He lay in the dug-out, flinching at each shell, and “trying to get into the smallest possible corner.” He tried to do guard duty that night, but, when some one noticed involuntary spasmodic movements, he was ordered to go back to the dug-out, was helped to the regimental aid post by two men, and was sent to hospital. He had been in France eight months and had been shaken up somewhat four months before, when bombs threw dirt in his face. At that time, his hands and handwriting had become tremulous, but he had not reported sick. He was depressed and wanted Major Myers to make him well. It seems that he had shrugged his shoulders and made leg movements, diving beneath the bedclothes, and bringing his knees to his chin. When Major Myers examined him, the leg movements were due solely “to strong periodic simultaneous contractions of the two sartorius muscles, the rate of contraction of which varied from 60 to 70 per minute, increasing to 90 during the excitement of examination.” There were special changes of sensibility in the right leg and arm and right side of the face and chest, not involving the abdomen. The patellar reflex was exaggerated; plantar reflexes could not be obtained. The legs were tremulous, especially when the patient lifted them, whereas the hands and tongue were only faintly tremulous.
A private, 23, was admitted to a casualty clearing station and the next day told the examiner, Major Myers, that the Germans had been sending artillery shells and heavy explosions over, and the last thing he remembered was being on guard and then digging himself out from under fallen sandbags. His buddies told him that he had been thrown into the air, but he didn’t recall that. He remembered running to the shell trench, but finding it “too hot,” he went back to the firing trench, noticing on the way that his vision was blurry. He lay in the dug-out, flinching at each explosion and “trying to get into the smallest possible corner.” He attempted to do guard duty that night, but when someone saw him having involuntary spasms, he was ordered back to the dug-out. Two men helped him to the regimental aid post, after which he was sent to the hospital. He had been in France for eight months and had been shaken up a bit four months prior when bombs threw dirt in his face. At that time, his hands and handwriting had become shaky, but he hadn’t reported sick. He felt depressed and wanted Major Myers to make him better. It seems he had shrugged his shoulders and made leg movements, diving underneath the bedcovers and pulling his knees to his chin. When Major Myers examined him, the leg movements were solely due to “strong periodic simultaneous contractions of the two sartorius muscles, the rate of contraction of which varied from 60 to 70 per minute, increasing to 90 during the excitement of examination.” There were specific changes in sensitivity in his right leg and arm as well as the right side of his face and chest, excluding the abdomen. The patellar reflex was exaggerated; plantar reflexes could not be tested. His legs were shaky, especially when he lifted them, while his hands and tongue were only slightly tremulous.
Under light hypnosis, events in the amnestic period were recalled, and details as to the shell’s direction, process of lifting up, and fall. Under deeper hypnosis, the sartorius contractions diminished but did not disappear. Appropriate suggestion was made, and upon arousal from hypnosis, the movements ceased, the headache disappeared, memory was recovered, and the unilateral disturbances of sensibility had vanished.
Under light hypnosis, memories from the amnestic period were recalled, including details about the shell's direction, how it was lifted, and how it fell. With deeper hypnosis, the contractions of the sartorius muscle lessened but didn’t go away completely. A suitable suggestion was given, and once the person was brought out of hypnosis, the movements stopped, the headache was gone, memory returned, and the one-sided sensitivity issues disappeared.
As to the possibility of malingering in this case, Major Myers calls attention to the disorders of sensibility which he believes could hardly have been simulated, to the persistence of spasmodic movements during sleep, to their confinement to the sartorii, and to the spastic condition of legs, such that when the thighs were passively raised the knees remained extended.
Regarding the possibility of faking symptoms in this case, Major Myers points out the sensitivity disorders that he believes could hardly be pretended, the ongoing spasmodic movements during sleep, their restriction to the sartorius muscles, and the spastic condition of the legs, so much so that when the thighs were passively lifted, the knees stayed straight.
Re persistence of hysterical phenomena in sleep, Ballet felt that he could prove that some hysterical contractures persisted during sleep, and Sollier has written a special article to the same effect. Ballet’s case had a contracture developing after an operation on the first metacarpal bone. The contracture which followed would be then probably, upon Babinski’s analysis, a reflex contracture and not a hysterical one. Duvernay, Sicard, and Babinski himself have noted the persistence of reflex contractures during sleep, to say nothing of their persistence under an advanced stage of chloroform narcosis. In fact, these reflex contractures are exactly as fixed and persistent as contractures of clearly organic origin. It is probable that Babinski would define Myers’ case (395) as a physiopathic one; yet against this diagnosis would be the disappearance of the movements after hypnosis. As against hysteria, it will be noted that the patellar reflex was exaggerated, and that the plantar reflexes could not be obtained.
Re persistence of hysterical phenomena in sleep, Ballet believed he could demonstrate that some hysterical contractures continued during sleep, and Sollier has written a specific article supporting this idea. Ballet’s case involved a contracture that developed after surgery on the first metacarpal bone. According to Babinski’s analysis, the subsequent contracture would likely be a reflex contracture rather than a hysterical one. Duvernay, Sicard, and Babinski himself have observed that reflex contractures persist during sleep, not to mention their persistence during a deep stage of chloroform anesthesia. In fact, these reflex contractures are just as stable and persistent as those with a clearly organic cause. It's likely that Babinski would categorize Myers’ case (395) as physiopathic; however, the disappearance of movements after hypnosis contradicts this diagnosis. Additionally, contrary to hysteria, it should be noted that the patellar reflex was heightened, while the plantar reflexes could not be elicited.
Shell-shock: Brown-Séquard syndrome, hematomyelic?
Shell shock: Brown-Séquard syndrome, hematomyelia?
Case 396. (Ballet, August, 1915.)
A soldier, 24, went to the front November 12, 1914, and June 1, 1915, had a shell burst near him in the trench, on the occasion of which he felt a violent shock, as if a blow in the kidneys. He felt suddenly paralyzed in both legs. He was crouching at the time of the shell burst. His legs felt dead, and he had such violent pain in the thorax as to make breathing difficult. He was carried to a shelter. After a few hours, the left leg began to move again.
A 24-year-old soldier went to the front on November 12, 1914, and on June 1, 1915, a shell exploded near him in the trench. At that moment, he felt a violent shock, like a blow to his kidneys. He suddenly felt paralyzed in both legs while crouching during the blast. His legs felt lifeless, and he experienced such intense pain in his chest that it made breathing difficult. He was taken to a shelter. After a few hours, his left leg started to move again.
He was carried to the ambulance, remaining there five days, unable to walk, though able to move and turn in bed, slightly constipated, with persistent pains in back. He was then carried to Auxiliary Hospital 231, at Paris, and a bullet (!) was found superficially lodged in the region of the left scapula. Neither patient nor physicians had hitherto observed the bullet, which could have had nothing to do with any spinal lesion.
He was taken to the ambulance, where he stayed for five days, unable to walk but able to move and turn in bed. He was slightly constipated and had ongoing back pain. He was then moved to Auxiliary Hospital 231 in Paris, where a bullet (!) was found lodged just under the skin in the area of his left shoulder blade. Neither he nor the doctors had noticed the bullet before, and it was unrelated to any spinal injury.
The pains, in the course of a month, grew less, and at the end of two or three weeks he began to walk and was sent to the psychoneurosis service at Ville-Évrard, July 10. He then complained of pain in the right thorax, especially on movement or after sitting up some time. He could hardly bring himself to the sitting posture from the bed, and found difficulty in raising the right leg therefrom. In walking, the right leg was dragged behind. The reflexes were increased on the right side. There was ankle clonus without Babinski sign. Anesthesia to touch over the whole of the left leg. Anesthesia to pin prick and temperature as far as the umbilicus. Cold was not felt on the left side.
The pains gradually decreased over the month, and by the end of two or three weeks, he started walking again and was admitted to the psychoneurosis service at Ville-Évrard on July 10. He then reported pain in the right side of his chest, especially when moving or after sitting up for a while. He struggled to sit up from the bed and had difficulty lifting his right leg. When walking, his right leg lagged behind. The reflexes on the right side were heightened. There was ankle clonus, but no Babinski sign. He experienced numbness to touch throughout his left leg and had reduced sensation to pinprick and temperature up to the level of the umbilicus. He could not feel cold on the left side.
The water of a bath seemed lukewarm on the left side and warm on the right. The left side of the scrotum and the left half of the penis showed the same disorder of sensibility. There was a zone of hypesthesia on the right side of the thorax in the region of the lower ribs. The patient compared his[556] sensations while at rest and without contact to a sensation of painful pressure occurring intermittently, or rather in paroxysms, not advancing beyond the median line of the back. Here was a question of Brown-Séquard syndrome, probably due to a slight hematomyelia, but associated with no external lesion or any injury to the vertebral column.
The water in the bath felt lukewarm on the left side and warm on the right. The left side of the scrotum and the left half of the penis had the same sensory issue. There was an area of reduced sensitivity on the right side of the chest near the lower ribs. The patient described his[556] sensations while resting and without any touch as a feeling of painful pressure that happened intermittently, or more precisely in bursts, not extending past the middle line of the back. This indicated Brown-Séquard syndrome, likely due to a small hematomyelia, but without any external injury or damage to the spinal column.
Re Brown-Séquard’s syndrome, see Athanassio-Benisty with respect to spinal cord symptoms associated with lesions of the brachial plexus. It appears that the combination of spinal cord and brachial plexus injury is not uncommon. Note in this case that a bullet was found in the left scapula region. According to Ballet, this bullet could have had nothing to do with a spinal lesion.
Re Brown-Séquard’s syndrome, see Athanassio-Benisty regarding spinal cord symptoms linked to injuries of the brachial plexus. It seems that the combination of spinal cord and brachial plexus injuries is quite common. In this case, a bullet was discovered in the left shoulder area. According to Ballet, this bullet may not have been related to a spinal injury.
Violence to back: Dysbasia. Antebellum injury.
Violence to back: Difficulty walking. Pre-war injury.
Case 397. (Smyly, April, 1917.)
A man (also injured in 1906 by the fall of a heavy weight on his back) went to France in 1914 as a soldier, and eight months later was hurled into a shell hole so that his back struck the edge. He was rendered unconscious. Upon recovery of consciousness, the right leg was found to be swollen, and there were severe pains in the legs and back.
A man (who was also hurt in 1906 when a heavy weight fell on his back) went to France as a soldier in 1914, and eight months later, he was thrown into a shell hole, causing his back to hit the edge. He was knocked unconscious. When he regained consciousness, his right leg was swollen, and he experienced intense pain in his legs and back.
Upon return home the patient went from one hospital to another, for the most part unable to walk, suffering from agonizing pain in head and eyes. Insomnia and waking dreams.
Upon returning home, the patient went from one hospital to another, mostly unable to walk and experiencing excruciating pain in their head and eyes. They suffered from insomnia and vivid dreams.
He was able to bring himself to an upright position and to rush a few steps. He has now acquired considerable control of the feet by the aid of crutches. Insomnia persisted.
He managed to get himself upright and took a few quick steps. He has now gained significant control of his feet with the help of crutches. He still struggled with insomnia.
Dysbasia: Psychogenic (cerebellar nucleus (?))
Dysbasia: Psychogenic (cerebellar nucleus (?))
Case 398. (Cassirer, February, 1916.)
On March 9, 1915, a shell wounded a man slightly, and burned off some of the hair of his head. He was unconscious two days, and on waking vomited for a time. Shortly after the injury difficulties in standing and walking set in, with headache, noises in the left ear, difficulty in the intake of ideas, excitability, and poor memory. Then, slight improvement. About the middle of June he was no longer closely confined to bed and could take a few steps with two canes; but the gait was still unsteady and the left leg tended to make abnormal-looking movements. There was nystagmus, rapid, though constant, on looking to the left,—more in the left eye; and nystagmus on looking to the right,—more in the right eye. Adiadochokinesis absent. Vestibular nerve somewhat excitable. Deviation outward in finger-pointing test.
On March 9, 1915, a shell injured a man slightly and burned some of the hair on his head. He was unconscious for two days, and when he woke up, he vomited for a while. Shortly after the injury, he started experiencing difficulties with standing and walking, along with headaches, ringing in his left ear, trouble processing thoughts, irritability, and poor memory. Then, there was a slight improvement. By mid-June, he was no longer confined to bed and could take a few steps using two canes; however, his gait was still unsteady, and his left leg tended to make unusual movements. There was nystagmus, rapid but constant, when looking to the left—more pronounced in the left eye; and nystagmus when looking to the right—more pronounced in the right eye. Adiadochokinesis was absent. The vestibular nerve was somewhat excitable. There was an outward deviation in the finger-pointing test.
According to Cassirer, this case is one largely of psychogenic origin, with possibly an organic cerebellar nucleus. The knee-jerks absent (even up to March 31). W. R. negative.
According to Cassirer, this case is primarily of psychogenic origin, possibly involving an organic cerebellar nucleus. The knee-jerk responses are absent (even as of March 31). W. R. is negative.
Shell-shock; unconsciousness: Dysbasia, in part hysterical, in part organic (?).
Shell shock; unconsciousness: Dysbasia, partly hysterical, partly physical (?).
Case 399. (Hurst, May, 1915.)
A private, 29, was knocked over by a shell explosion December, 1914. He was unconscious two days, found that he could not move either right arm or left leg, got some power back shortly, but, if he tried to stand, experienced involuntary violent movements in the left leg.
A private, 29, was knocked over by a shell explosion in December 1914. He was unconscious for two days and discovered that he couldn’t move his right arm or left leg. He regained some strength shortly after, but whenever he tried to stand, he had involuntary, violent movements in his left leg.
April 1, 1915, response to questions was slow and speech slow. The right arm and grip were weak. If the left hand was clenched, there was an associated movement of the right hand; but on clenching the right hand, no associated movement was produced in the left. The musculature was equal on the two sides, and the tendon reflexes of the arms were brisk and equal. Light tactile stimuli were hard to localize. Movements of the left leg were somewhat weak, though the musculature was equal on the two sides. The knee-jerks were brisk, the left slightly brisker. Sometimes a well-marked ankle clonus could be obtained on the left side, but sometimes not. The plantar reflex was constantly flexor. Babinski’s second sign (combined flexion of thigh and pelvis) was well marked on the left side.
April 1, 1915, responses to questions were slow and speech was also slow. The right arm and grip were weak. When the left hand was clenched, there was some movement in the right hand; however, when the right hand was clenched, there was no movement in the left. The muscle tone was equal on both sides, and the tendon reflexes in the arms were quick and equal. Light touch stimuli were hard to pinpoint. Movements in the left leg were somewhat weak, but the muscle tone was equal on both sides. The knee reflexes were quick, with the left being slightly quicker. Sometimes there was a noticeable ankle clonus on the left side, but sometimes there wasn’t. The plantar reflex was consistently flexor. Babinski’s second sign (the combined flexion of the thigh and pelvis) was clearly marked on the left side.
On attempts to walk, the left leg would move rapidly from side to side, round the point of contact of toes with ground. When a step forward was taken with the right leg, the left one dragged, and made irregular movements.
On trying to walk, the left leg would swing quickly from side to side around where the toes touched the ground. When the right leg took a step forward, the left one dragged and moved erratically.
This gait seemed obviously hysterical. The patient was kept in hospital for a month. He was very easily hypnotizable, but even in deep hypnosis leg movements could not be controlled when he was told to walk. The first whiff of ether hypnotized but did not cure him.
This way of walking clearly seemed over the top. The patient stayed in the hospital for a month. He was very suggestible to hypnosis, but even in a deep trance, he couldn't control his leg movements when he was instructed to walk. The first hint of ether put him under but didn’t fix the problem.
On the whole, upon review, Hurst believes that there may have been organic brain changes, which (a) the associated movement of the paralyzed hand when the normal hand was contracting, (b) the slightly increased left knee-jerk, (c) tendency to ankle-clonus, and (d) Babinski’s second sign, may show.
Overall, after reviewing everything, Hurst thinks there might have been changes in the brain that could be indicated by (a) the movement of the paralyzed hand when the normal hand was contracting, (b) the slightly heightened left knee-jerk, (c) a tendency toward ankle clonus, and (d) Babinski’s second sign.
Peculiar walking tic.
Strange walking tic.
Case 400. (Chavigny, April, 1917.)
A soldier was found with a peculiar walking tic. He would rest a good deal longer on the left leg than on the right. He would make a sudden movement of the right leg forward, as if on a spring. At the same time, the man’s head would give a violent movement to the right just as the right leg was receiving the weight of the body. The idea of this movement seemed to be that the center of gravity would be shifted and the work of the right leg would be relieved. This peculiar walk was naturally very slow. If the walk was slowed down, it became quite normal. There was no pain at the basis of this walk. If the man hopped, he hopped no more painfully on the right leg, nor with greater difficulty, than upon the left.
A soldier was found with a strange walking tic. He would spend much longer resting on his left leg than on his right. He would suddenly move his right leg forward, almost like a spring. At the same time, his head would jerk violently to the right just as his right leg took on the weight of his body. The idea behind this movement seemed to be that it shifted his center of gravity, making it easier for his right leg to carry the load. This unusual way of walking was naturally very slow. If he walked more slowly, it became quite normal. There was no pain associated with this way of walking. If the man hopped, he didn’t hop any more painfully on his right leg than on his left.
This man was guilty of desertion in the face of the enemy, and of desertion in the interior in time of war. He said he could not walk well and that he needed to take care of himself at his mother’s house, as he was not considered sick in his regiment. He had been wounded with two bullets, September 28, 1914, which struck him on the internal aspects of the knees. He was treated in hospital from October to the end of November, 1914; was held at the dépôt of his regiment from December to August, 1915. He was then put in hospital a month, and returned to his dépôt for three more months. He was examined by three physicians in August, 1915, and the commission decided that he was fit for service, and a simulator.
This man was guilty of abandoning his post in battle and of leaving his unit during wartime. He claimed he couldn't walk well and needed to take care of himself at his mother's house since he wasn't considered sick in his regiment. He had been shot twice on September 28, 1914, with bullets hitting the inner parts of his knees. He received hospital treatment from October to the end of November 1914, then was held at his regiment's depot from December to August 1915. After a month in the hospital, he returned to the depot for another three months. He was examined by three doctors in August 1915, and the board determined that he was fit for duty and was pretending to be unwell.
Thorough examination, including electrical and X-ray examinations, showed no lesion. Chavigny observed the patient for a long time, from the 21st of November, 1916, to January 5, 1917. Shells dropped near the hospital, December 2, and, following orders, the patients were taken into a vaulted cellar, and they ran thither very rapidly; but this patient could not hurry. He walked slowly, with the same tic. Surely the tic would be rather a difficult one to imagine,[560] and a somewhat more probable set of symptoms would ordinarily be chosen. The man has not the unstable nature of the ordinary victim of tic. On the contrary, he has rather the invincible obstinacy of a hysterotraumatic. On being shown that he could walk properly without these “para” movements, he would reply, “I can’t do anything else,” and he shook his head upon being told that he could be cured.
A thorough examination, including electrical tests and X-rays, showed no lesions. Chavigny monitored the patient closely, from November 21, 1916, to January 5, 1917. Shells fell near the hospital on December 2, and, following orders, the patients were quickly taken into a vaulted cellar; however, this patient couldn't hurry. He walked slowly, with the same tic. The tic would definitely be hard to picture, and typically, a more likely set of symptoms would be expected. This man doesn’t have the unstable nature of a typical tic sufferer. Instead, he displays a stubbornness characteristic of someone with hysterotraumatic issues. When shown that he could walk normally without these "para" movements, he would respond, "I can't do anything else," and he shook his head when told he could be cured.[560]
Reëducation of his anesthetic areas (there was a zone of diminution in sensibility to pin-prick in the knee region, and a complete anesthesia of the sole of the foot, with abolition of the plantar reflex), reëducation by appropriate gymnastics, and mental reëducation, might be attempted in a special neurological hospital.
Re-education of his numb areas (there was a section with reduced sensitivity to pin-prick in the knee area, and complete numbness of the sole of the foot, eliminating the plantar reflex), re-education through suitable exercises, and mental re-education, could be attempted in a specialized neurological hospital.
Re disorders of gait, Laignel-Lavastine and Courbon divide functional gait disorders into three groups: (a) A group called dynamogenic; (b) an inhibitory group; and (c) a group showing both forms of disorder.
Re gait disorders, Laignel-Lavastine and Courbon classify functional gait disorders into three categories: (a) a dynamogenic group; (b) an inhibitory group; and (c) a group that exhibits both types of disorders.
Roussy and Lhermitte have attempted to divide the gait disorders into two groups: (a) A group termed by them basophobic, in which there is a marked psychogenic and emotional basis; and (b) a dysbasic group, the basis of which is suggestion rather than emotion. Following is a skeleton of their classification:
Roussy and Lhermitte have tried to categorize gait disorders into two groups: (a) a group they call basophobic, which has a strong psychogenic and emotional foundation; and (b) a dysbasic group, which is based more on suggestion than on emotion. Below is a summary of their classification:
1. Astasia-abasia and dysbasia group.
Astasia-abasia and dysbasia team.
- Astasia-abasia.
- Pseudo tabetic dysbasia.
- Pseudo polyneuritic dysbasia.
- Tight-rope walker’s gait.
- Scrubber’s gait.
- Choreiform dysbasia.
- Knock-kneed gait.
- Walking as if on sticky surface.
- Bather’s gait.
2. Stasobasophobia group.
Stasobasophobia support group.
3. Habit limping.
3. Habitual limping.
Mine explosion; unconsciousness: Camptocormia. Hospital rounder twenty months (bedfast five months) without complete neurological examination. Cure by persuasive electrotherapy in one hour.
Mine explosion; unconsciousness: camptocormia. Hospital stay for twenty months (bedridden for five months) without a complete neurological exam. Cured by effective electrotherapy in one hour.
Case 401. (Marie, Meige, Béhagne, February, 1917; Souques and Mégevand, February, 1917.)
A man became a hospital rounder to all points of the compass in France during a period of twenty months, with such diagnoses as myelopathic disorder, complex spinal trouble, ataxic phenomena.
A man spent twenty months visiting hospitals all over France, dealing with diagnoses like myelopathic disorder, complex spinal issues, and ataxic symptoms.
As a matter of fact he was a camptocormic: trunk bent, knees semi-flexed, legs in external rotation. He used two canes in locomotion, made a bowing movement with each 20 cm. step, then another bowing movement, and another little step with the other foot. Made to lie down, his legs would elongate, the right completely but the left with some difficulty, the feet going into hyperextension, with the big toe raised, others flexed; the feet externally rotating, plantae turned in. In horizontal decubitus, there was only slight lumbar discomfort, but the legs stiffened and gave quick convulsive jerks. Taking the posture several times in succession would diminish these phenomena. Kneeling, he could bring his heels within 10 cm. of the buttock, whereas in spontaneous flexion of the leg on the thigh, the knee remained a distance of 40 cm. from the buttock.
He was actually a camptocormic: his trunk was bent, knees slightly flexed, and legs turned outward. He used two canes to walk, bending forward with each 20 cm step, then bending again, followed by a small step with the other foot. When lying down, his legs would stretch out, with the right leg completely but the left leg with some difficulty; his feet hyperextended, the big toe raised and the others bent; his feet were turned outward, and the soles pointed inward. While lying on his back, he only felt slight discomfort in his lower back, but his legs would stiffen and jerk suddenly. Repeating the posture several times would reduce these reactions. When kneeling, he could bring his heels within 10 cm of his buttocks, but in a spontaneous leg flexion on the thigh, his knee stayed 40 cm away from the buttocks.
A complete examination showed no joint disorder or any diminution in muscular strength, or any reflex disorder except that all the tendon reflexes were rather powerful. There was a question of possible X-ray demonstration of lesions and ankylosis of the fourth and fifth lumbar vertebrae, and there was a question of some incontinence of urine. On the basis of these phenomena apparently, this camptocormic patient had been saddled with the diagnosis of myelopathic and ataxic disorder for a period of 16 months. A neurologist was at last consulted, and on his advice, it proved possible to get the patient evacuated to a neurological center in a period of[562] four months. Facts of this species are unfortunately still too common, state Marie, Meige and Béhagne, February 1, 1917, despite the remarkable and rapid cures obtained in camptocormia by Souques. In point of fact, no complete neurological examination had been performed upon this man during a period of 20 months.
A full examination showed no joint problems, no decrease in muscle strength, and no reflex issues, except that all the tendon reflexes were surprisingly strong. There was a possibility of seeing lesions and ankylosis in the fourth and fifth lumbar vertebrae on X-ray, and there was a question of some urinary incontinence. Based on these signs, this camptocormic patient had been given a diagnosis of myelopathic and ataxic disorder for 16 months. Finally, a neurologist was consulted, and following his advice, it became possible to transfer the patient to a neurological center within four months. Unfortunately, cases like this are still too common, state Marie, Meige, and Béhagne, February 1, 1917, despite the impressive and swift recoveries achieved in camptocormia by Souques. In fact, no complete neurological examination had been carried out on this man for 20 months.
This particular patient was given to Souques for treatment (Souques and Mégevand). His cure was completed by persuasive electrotherapy, in an hour.
This patient was sent to Souques for treatment (Souques and Mégevand). His recovery was achieved through effective electrotherapy, in just an hour.
It appears that the man was buried in a mine explosion, June 5, 1915, lost consciousness and came to twenty hours later, able to rise and take a few steps, but bent in two with a sharp dorsolumbar pain. The pain grew more violent and generalized during the next few days, and he began to lose all power in his legs, so that he could walk with the greatest difficulty. He was practically bedfast for five months. He then tried to rise and walk, but suffered so much that he could not get up except in a camptocormic position. It was in fact only January 23, 1917, at the Salpêtrière, that the diagnosis of camptocormia was made. The man complained of pains at the lower dorsal and lumbar regions of the spinal column with slight irradiation sidewise. The following diagnoses had been made:
It seems that the man was buried in a mine explosion on June 5, 1915. He lost consciousness and woke up twenty hours later, able to stand and take a few steps, but hunched over with sharp pain in his lower back. The pain became stronger and spread over the next few days, and he started to lose all strength in his legs, making it very difficult to walk. He was almost unable to get out of bed for five months. When he tried to stand and walk again, the pain was so intense that he could only get up in a bent-over position. It wasn't until January 23, 1917, at the Salpêtrière, that they diagnosed him with camptocormia. The man reported pain in the lower back and lumbar areas of his spine that sometimes radiated to the sides. The following diagnoses had been made:
June 8, 1915. Severe contusion of chest and back.
June 8, 1915. Serious bruising of the chest and back.
July 9, 1915. Multiple contusions, commotio spinalis; lesions and ankylosis of the 4th and 5th lumbar vertebrae (X-ray examination).
July 9, 1915. Several bruises, spinal concussion; damage and fusion of the 4th and 5th lumbar vertebrae (X-ray exam).
Sept. 3, 1916. Lumbar intervertebral arthritis with compression of roots.
Sept. 3, 1916. Arthritis of the lumbar intervertebral joints with compressed nerve roots.
Nov. 4, 1916. Myelopathic disorder.
Nov. 4, 1916. Myelopathy.
Dec. 5, 1916. Old complex spinal disorder.
Dec. 5, 1916. Long-standing complicated spinal condition.
Souques remarks that these diagnoses show that knowledge about camptocormia has not penetrated into most of the sanitary formations (1917).
Souques notes that these diagnoses reveal that understanding of camptocormia hasn't spread to most health organizations (1917).
Astasia-Abasia.
Astasia-Abasia.
Case 402. (Guillain-Barré and Barré, January, 1916.)
A soldier was evacuated to the 6th Army neurological center for paraplegia with tremor. He had been in various hospitals for a period of a year. The tendon reflexes of the arms appeared increased; there was a suspicion of patellar clonus and of foot clonus, and it had been proposed to invalid the man for spastic paralysis. In point of fact, the man was suffering from an epileptoid trepidation of the foot and of the patella. When he was lying down, his motor disorders practically passed away, though they had been very marked when he tried to stand upright or to walk. He had much trouble in walking, but could readily stand for some time on one leg.
A soldier was taken to the 6th Army neurological center for paraplegia with tremors. He had spent about a year in various hospitals. The tendon reflexes in his arms seemed heightened; there was a concern about patellar clonus and foot clonus, and it had been suggested that he be classified as disabled due to spastic paralysis. In reality, the man was experiencing an epileptoid tremor in his foot and knee. When he was lying down, his motor issues nearly disappeared, although they were quite severe when he tried to stand or walk. He had significant difficulty walking, but he could easily stand on one leg for a while.
The man was forthwith treated by persuasive methods. It is important to find out the organic lesion which in all probability served as a starting point for the functional disease, and important to remove or abolish this lesion however minute if a complete and lasting cure is to be obtained.
The man was immediately treated with persuasive methods. It's important to identify the underlying issue that likely triggered the functional disease, and crucial to remove or eliminate this issue, no matter how small, if a complete and lasting cure is to be achieved.
Re astasia-abasia, writers have remarked that it is one of the commonest hysterical syndromes in the war, though somewhat rare in its complete form. Roussy and Lhermitte state that it usually follows the explosion of a large calibre projectile and has a rapid onset. It is often an isolated phenomenon, without emotional or other Shell-shock complications. The victim has been thrown to the ground and rolled into a trench or hollow. Sometimes the victim gets back to the first-aid post, only to find himself on arrival at the ambulance wholly unable to walk. The legs, however, are drawn along inertly, as in paraplegia, or a pronounced contracture interferes with walking.
Re astasia-abasia, writers have noted that it is one of the most common hysterical syndromes during the war, although it is somewhat rare in its complete form. Roussy and Lhermitte state that it usually occurs after the explosion of a large projectile and has a quick onset. It often appears as an isolated phenomenon, without emotional or other Shell-shock complications. The victim may have been thrown to the ground and rolled into a trench or depression. Sometimes, the victim makes it back to the first-aid post, only to find that they are completely unable to walk upon arrival at the ambulance. The legs, however, are dragged along passively, similar to paraplegia, or a significant contraction makes walking difficult.
Astasia-abasia is classified with hysteria major, hysterical hemiplegia, hysterotraumatic brachial monoplegia, glossolabial hemispasm, hysterical mutism, and rhythmic chorea, as so characteristic that differential diagnosis is superfluous. According to Babinski, no functional spasm and no organic disease can reproduce hysterical astasia-abasia.
Astasia-abasia is categorized along with major hysteria, hysterical hemiplegia, hysterotraumatic brachial monoplegia, glossolabial hemispasm, hysterical mutism, and rhythmic chorea, so much so that distinguishing it from other conditions is unnecessary. Babinski states that neither a functional spasm nor an organic disease can replicate hysterical astasia-abasia.
Multiple shell wounds, with persistent slight suppuration of thigh: Abdominothoracic contracture, tetanic, four months after original injury.
Multiple shell wounds, with ongoing slight pus discharge from the thigh: Abdominothoracic tightening, in a state of tetany, four months after the initial injury.
Case 403. (Marie, 1916.)
A soldier, 31, was wounded in the left arm January, 1915, and received 10 c.c. antitetanic serum; was wounded again July 10 in the face, scalp, upper part of the thorax, left arm and left leg by shell fragments, and again received, two days later, 10 c.c. antitetanic serum. July 13, at the ophthalmological center at Rouen the left eye was enucleated on account of a shell wound, and four days later a fragment was removed from a phlegmon of the forearm. Later a number of operations were made for blepharoplasty. The wounds all healed well except for an apparently insignificant, small suppuration of the thigh. November 10, four months after the shell wounds, while apparently in perfect health, the man began to complain of lancinating, intermittent pains in the abdomen, thorax and lumbar region. With these pains was associated a persistent abdominolumbar contracture.
A 31-year-old soldier was injured in his left arm in January 1915 and received 10 c.c. of antitetanic serum. He was wounded again on July 10 in the face, scalp, upper thorax, left arm, and left leg by shell fragments, and two days later received another 10 c.c. of antitetanic serum. On July 13, at the ophthalmology center in Rouen, his left eye was removed due to a shell wound, and four days later, a fragment was extracted from an infected area in his forearm. Later, several surgeries were performed for eyelid reconstruction. All the wounds healed well except for a small, seemingly minor infection in the thigh. On November 10, four months after the shell wounds, he started complaining of sharp, intermittent pain in his abdomen, chest, and lower back. Along with these pains, he also had a persistent contraction of the abdominal and lower back muscles.
On the suspicion of an abdominal form of local tetanus, chloral was given; but the condition grew worse. The sudden contractions spread from the waist to the feet, from November 20 onward, and were felt by the patient as electric shocks. The arms were not affected. Trouble with breathing supervened on the night of December 3. Sometimes there were respiratory pauses for as long as 15 seconds, followed by a slight polypnea. December 6 the man presented an intense contracture of the lower part of the trunk. The slightly retracted abdominal wall was of marbly hardness, but quite painless. Analgesic muscular rigidity took the place of the former crises of pain. The dorsolumbar contracture was so marked as to make an appreciable hollow in the back. The patient could pick up an object from the ground only by flexing his knees to the maximum, as the trunk could not be flexed. There was a very slight trismus, but he could open his mouth, drink, eat and talk without difficulty. There was[565] no trace of neck stiffness or of Kernig’s sign. The tendon reflexes, normal in the arms, were exaggerated in the lower extremities, especially on the left (wounded) side. The skin reflexes were also more marked on the left side, especially the reflex of the tensor of the fascia lata. There was no longer any evidence of suppuration of the wound of the left thigh, which had been dried up for a fortnight. The pulse was somewhat exaggerated (92) and there was a general hyperidrosis, especially of the face.
On suspicion of an abdominal form of localized tetanus, chloral was administered, but the patient's condition worsened. Starting from November 20, sudden contractions spread from the waist down to the feet, and the patient experienced them like electric shocks. The arms were unaffected. Breathing difficulties arose on the night of December 3, with respiratory pauses lasting up to 15 seconds, followed by rapid breathing. On December 6, the man showed intense contraction in the lower part of his torso. The slightly retracted abdominal wall felt very hard, like marble, but was pain-free. Analgesic muscle rigidity replaced the previous episodes of pain. The dorsolumbar contraction was so pronounced that it created a noticeable hollow in the back. The patient could only pick up objects from the ground by bending his knees as his torso couldn’t flex. There was minimal trismus, but he could open his mouth, drink, eat, and talk without trouble. There was[565] no sign of neck stiffness or Kernig’s sign. The tendon reflexes in the arms were normal but exaggerated in the lower limbs, particularly on the left (injured) side. Skin reflexes were also more pronounced on the left, especially the reflex of the tensor of the fascia lata. There were no signs of infection in the left thigh wound, which had been dry for two weeks. The pulse was somewhat elevated (92) and there was overall excessive sweating, especially on the face.
Forty c.c. antitetanic serum were given without reaction, and 4 grams of chloral; five days later, 30 c.c. more serum. After ten days the abdomen remained hard, though there was a trifling improvement of the lumbar contracture. There were no longer any spasmodic crises or respiratory disturbances. There was a slight serous exudation from the wound. X-ray showed a small shell fragment 6 cm. below the orifice of the wound.
Forty cc of antitetanic serum were administered without any reaction, along with 4 grams of chloral; five days later, an additional 30 cc of serum was given. After ten days, the abdomen was still firm, although there was a minor improvement in the lumbar contraction. There were no more spasmodic episodes or breathing issues. A slight serous fluid was oozing from the wound. An X-ray revealed a small shell fragment 6 cm below the wound opening.
The third injection was given December 27 to prevent mobilization of the bacilli at operation, and on the 28th, the projectile was removed under local anesthesia from a small, walled-off, old pus pocket, from which were cultivated bacillus perfringens and other organisms.
The third injection was given on December 27 to prevent the movement of the bacilli during the operation, and on the 28th, the projectile was removed under local anesthesia from a small, enclosed, old pus pocket, from which bacillus perfringens and other organisms were cultured.
December 31 a distinct improvement set in and January 13 there was little or no trace of previous disease, except that testing the plantar cutaneous reflex on the left side produced an exaggerated contraction of the tensor of the fascia lata. February 15 he was reëxamined and found quite normal.
December 31, a clear improvement began, and by January 13, there was hardly any trace of the previous illness, except when testing the plantar cutaneous reflex on the left side, which caused an exaggerated contraction of the tensor of the fascia lata. On February 15, he was reexamined and found to be completely normal.
This case of tetanus limited to the abdominothoracic muscles (except for a very mild contracture of the masticators) had as its locus of origin, doubtless, a wound of the thigh from which the toxin rose along branches of the lumbar plexus to impregnate the corresponding level of the spinal cord. Although there was no stiffness of the wounded leg, yet there was an exaggeration of the tendon reflexes thereof. The first phase of painful contractures and spasms with respiratory disorder was succeeded by an analgesic phase of characteristically tetanic rigidity. The nonfebrile nature of the disease and the preservation of good general health are worth noting.
This case of tetanus affected only the muscles in the abdomen and chest (except for a very slight tightening in the jaw muscles) and likely originated from a thigh wound. From there, the toxin traveled through the nerves to affect the corresponding level of the spinal cord. Even though the injured leg wasn't stiff, the tendon reflexes were heightened. The initial phase included painful contractions and spasms, along with breathing issues, which was followed by a phase of characteristic tetanic rigidity without pain. It's important to note that the illness wasn't accompanied by a fever, and the overall health of the patient remained good.
Shoulder blade unslung in knock-down by shell splinter: Hysterical (!) paralysis of arm with anesthesia. Recovery by electricity, massage, and reëducation (dislocation remaining).
Shoulder blade dislocated by shell fragment: Hysterical (!) paralysis of arm with numbness. Recovery through electricity, massage, and re-education (dislocation still present).
Case 404. (Walther, December, 1914.)
A soldier was struck September 27, near Berry au Bac, by a shell fragment in the right scapular region and was thrown, according to his story, 15 meters. Upon entrance at Val-de-Grâce, October 13, the shoulder-girdle was found intact. There was a very painful point in the spinous process of the scapula, suggesting a fracture; but the bone was proved intact on X-ray. The scapula was very mobile, as if unslung from the thorax. The arm was paralyzed. On raising the arm the scapula followed its movements and detached itself completely from the thorax, dislocating upwards with lively pain. The fingers could be pushed under the anterior surface of the scapula, and its internal border proved to be entirely free of attachment. Pressure along this internal border was very painful. It seems as if there had been a tearing of the rhomboid and serratus magnus muscles and probably a part of the latissimus dorsi under the influence of the violent shock conveyed by the shell fragment, which had pushed the scapula forward and upward without injuring the skin.
A soldier was hit on September 27, near Berry au Bac, by a shell fragment in the right shoulder area and was reportedly thrown about 15 meters. Upon arrival at Val-de-Grâce on October 13, his shoulder was found intact. There was a very painful spot on the spinous process of the scapula, indicating a possible fracture; however, X-rays showed the bone was intact. The scapula was very mobile, almost as if it was unhooked from the thorax. The arm was paralyzed. When raising the arm, the scapula moved with it and completely detached from the thorax, dislocating upwards with significant pain. It was possible to slide fingers under the front surface of the scapula, and its inner edge was completely free of attachments. Pressing along this inner edge caused intense pain. It appears there was a tearing of the rhomboid and serratus magnus muscles and probably part of the latissimus dorsi due to the violent shock from the shell fragment, which pushed the scapula forward and upward without damaging the skin.
There was also a complete paralysis of sensation. Paralysis of motion was complete except for the extensor longus of the thumb. This motor paralysis had come on progressively three days after the accident. A radicular paralysis from an evulsion of the plexus was suspected.
There was also a total loss of sensation. Movement was completely paralyzed except for the long extensor of the thumb. This motor paralysis developed progressively three days after the accident. A nerve root paralysis from a tear of the plexus was suspected.
Babinski, however, made the diagnosis of psychic paralysis, finding the muscles reacting perfectly to percussion. After a few electric tests with the faradic current voluntary movements were obtained in all the muscles of the arm and hand.
Babinski, however, diagnosed psychic paralysis, noting that the muscles responded perfectly to tapping. After conducting a few electric tests with the faradic current, voluntary movements were achieved in all the muscles of the arm and hand.
Treatment was then continued by electricity, massage and reëducation, so that all movements soon regained strength. The patient can now himself, by raising his arm, still produce his dislocation, which still provokes a lively pain.
Treatment was then continued with electricity, massage, and rehabilitation, so that all movements soon regained strength. The patient can now, by raising his arm, still cause his dislocation, which still triggers sharp pain.
Gunshot wound of left forearm: PARALYSIS of the arm gradually INCREASING IN DEGREE and extent and associated with pains and anesthesias.
Gunshot wound to the left forearm: Paralysis of the arm gradually increasing in severity and extent, accompanied by pain and numbness.
Case 405. (Oppenheimer, July, 1915.)
A reservist sustained, October 2, 1914, a gunshot wound of the left forearm from a distance of about 1400 meters. He fainted, lost much blood, and was treated surgically, October 7, in hospital (at this time no complete paralysis of the arm).
A reservist sustained a gunshot wound to his left forearm on October 2, 1914, from about 1400 meters away. He fainted, lost a lot of blood, and underwent surgery in the hospital on October 7 (at that time, there was no complete paralysis of the arm).
In November, however, an incomplete paralysis at first developed. November 12, the patient was able to flex his thumb but showed some anesthesia.
In November, however, incomplete paralysis initially developed. On November 12, the patient could flex his thumb but showed some numbness.
Transferred to nerve hospital in December, the patient said that at the first change of dressings, October 10, he had not been able to move his arm, and said that pains and paresthesia had existed in the arm ever since the injury. There was still some evidence of suppuration at the exit orifice of the bullet. The left arm was now completely paralyzed and atonic, and hung down in walking, without swinging. The supinator phenomenon, though present on the right side, was absent on the left. The triceps reflex was present. The shoulder acted like a flail joint. On passive elevation of the left arm, the deltoid seemed to contract slightly at first; later it failed to contract. Fibrillary tremor of the left thumb.
Transferred to a nerve hospital in December, the patient reported that during the first dressing change on October 10, he was unable to move his arm and had experienced pain and numbness in the arm since the injury. There was still some sign of infection at the bullet exit wound. The left arm was now completely paralyzed and without tone, hanging down while walking without swinging. The supinator reflex was present on the right side but absent on the left. The triceps reflex was intact. The shoulder functioned like a flail joint. During passive elevation of the left arm, the deltoid muscle seemed to contract slightly at first; later, it did not contract at all. There was fibrillary tremor in the left thumb.
Suggestive therapy was unsuccessful. There was an anesthesia of the left arm and the left trunk. The disorder diminished proximally, being most severe in the hand and the arm. The legs were normal. The electrical irritability of the left arm was only slightly diminished. There was a well-marked hypertrichosis of the left forearm, the skin of which was slightly purple and discolored. The patient himself made an attempt to burn his arm with a lighted cigar, to see if he could feel the pain. He showed the scar but had felt nothing. The pectoralis major muscle did not contract. If the left arm was started actively swinging, it kept on swinging inertly. The left hand showed hyperidrosis. The small hand muscles were emaciated but electrically normal.
Suggestive therapy was not effective. There was numbness in the left arm and trunk. The symptoms were less severe further up, being worst in the hand and arm. The legs were normal. The electrical sensitivity in the left arm was only slightly reduced. There was noticeable excessive hair growth on the left forearm, which had a slight purple and discolored appearance. The patient even tried to burn his arm with a lit cigar to see if he could feel anything. He pointed out the scar but had felt nothing. The pectoralis major muscle didn’t contract. If the left arm was started swinging actively, it continued to swing passively. The left hand exhibited excessive sweating. The small muscles in the hand were thin but showed normal electrical activity.
Glass wound of wrist: Differential glove anesthesias (cold to mid forearm, pain somewhat higher, touch as far as elbow).
Glass wound of wrist: Differential glove anesthesias (cold to mid-forearm, pain slightly higher, touch as far as elbow).
Case 406. (Romner, March, 1915.)
A German soldier, 37, wounded his right wrist in the glass of a door. The hand was put up six weeks long with very few changes of the bandage on account of suppuration, and he noticed that the arm was getting weaker and weaker, that he was losing feeling in it, and that it was beginning to sweat a good deal, so that now and then drops of sweat would stream off. The right hand was found markedly congested and 1.5 cm. larger in circumference. The fingers and hand were especially weak. There was a marked tremor of the arm. Electric excitability normal. The sensory disorder was in glove form. Hypesthesia to touch reached the elbow, analgesia to a point three fingers’ breadth below the elbow, and anesthesia to cold to a point two fingers’ breadth still lower, a sort of stepwise dissociation of sensibility resembling what is found in spinal lesions. The case was presented as one of local traumatic hysteria.
A 37-year-old German soldier injured his right wrist on a glass door. His hand was in a bandage for six weeks with very few changes due to infection, and he noticed that his arm was getting weaker, he was losing feeling in it, and it was sweating a lot, causing drops of sweat to run off now and then. His right hand was significantly swollen, about 1.5 cm larger in circumference. The fingers and hand were particularly weak, and there was a noticeable tremor in the arm. Electric excitability was normal. The sensory issues were in a glove pattern, with reduced sensitivity to touch extending to the elbow, painlessness reaching three fingers' breadth below the elbow, and loss of cold sensation stretching two fingers' breadth lower, resembling the sensory dissociation seen in spinal injuries. The case was presented as one of local traumatic hysteria.
Re hysterical anesthesia, the rule is that it obeys no definite rule; that is, it may be a hemianesthesia, a segmentary, an isolated, or even a pseudo-peripheral anesthesia. It is a question whether Babinski would attempt to explain Romner’s case on the basis of medical suggestion, hetero-suggestion, or autosuggestion.
Re hysterical anesthesia, the rule is that it follows no specific guideline; it can be hemianesthesia, segmentary, isolated, or even pseudo-peripheral anesthesia. It's uncertain whether Babinski would try to explain Romner’s case through medical suggestion, hetero-suggestion, or autosuggestion.
Myers has had a few instances in which anesthesia spread gradually, and in which analgesia increased after its onset.
Myers has experienced a few cases where anesthesia gradually spread, and where pain relief increased after it started.
Re reëducation of cutaneous sensations, Chavigny recommends the faradic current in successive applications, marking the extent of the zone of anesthesia with ink upon the skin. Each time the current is applied, the inked limits of the area are lessened. By this form of suggestion, not only does the anesthesia disappear, but very often the accompanying paralysis also.
Regarding the re-education of skin sensations, Chavigny suggests using a faradic current in repeated applications, marking the boundaries of the numb area with ink on the skin. Each time the current is applied, the inked edges of the area shrink. Through this method of suggestion, not only does the numbness fade away, but the related paralysis often disappears as well.
Hysterical contracture, edema and vasomotor disorder.
Hysterical contracture, swelling, and blood flow disorder.
Case 407. (Ballet, July, 1915.)
For some unknown reason, a soldier developed a contracture of the right upper and lower extremities at a time when a basin of water was offered to him for toilet purposes. Three days later, this contracture disappeared in the leg but persisted in the arm at the radiocarpal joint and in the finger joints. There was also an anesthesia to touch and pain and temperature which ran up the arm to the shoulder. The tendon reflexes were normal. On the whole, there seemed to be no doubt that the case was one of hysterical arm contracture. Associated with this contracture was a white edema of the hand. On account of the chances of simulation, the hand was done up and sealed in such wise that the seals would have been broken if the splint had been lifted down during the night. The bandage was in place from June 25 to June 29. Upon its removal, there was no edema, but the contracture was still there. The arm was put up upon a cushion so that the hand would drain to the forearm. The edema was found capable of returning when the hand was placed below the level of the shoulder, disappearing when the hand was raised. The contractured hand was warmer than its fellow. According to Ballet, we here have an anesthetic instance of contracture associated with edema and vasomotor disorder.
For some unknown reason, a soldier developed a contracture in his right arm and leg while he was offered a basin of water for personal use. Three days later, the contracture in the leg disappeared, but it remained in the arm at the wrist joint and in the finger joints. There was also a lack of sensation to touch, pain, and temperature that extended up the arm to the shoulder. The tendon reflexes were normal. Overall, there seemed to be no doubt that this case was one of hysterical arm contracture. Accompanying this contracture was a white swelling in the hand. To prevent any chance of faking, the hand was wrapped and sealed in a way that would break the seals if the splint was removed during the night. The bandage stayed on from June 25 to June 29. When it was taken off, there was no swelling, but the contracture was still present. The arm was placed on a cushion so that the hand could drain towards the forearm. The swelling was found to return when the hand was below shoulder level but would disappear when the hand was raised. The affected hand was warmer than the other one. According to Ballet, this is an anesthetic case of contracture associated with swelling and vasomotor dysfunction.
Re edema, Babinski states that no case of hysterical edema has stood the test of scientific critique. Sometimes a case turns out one of tuberculous synovitis. Sometimes the patient is shown artificially to have brought about the edema. The hysterical “blue edema” of Charcot has not been proved to exist. Some during the war have been found due to voluntary constriction. Some of these constriction edemas even become relatively permanent. Babinski regards the above case of Ballet, as well as cases of Lebar and of Raynaud, as not true cases. Raynaud’s case was probably vascular.
Regarding edema, Babinski says that no case of hysterical edema has survived scientific scrutiny. Sometimes a case turns out to be one of tuberculous synovitis. Other times, the patient is shown to have artificially caused the edema. The hysterical “blue edema” described by Charcot has not been proven to exist. Some cases during the war were found to be due to voluntary constriction. Some of these constriction edemas even become relatively permanent. Babinski considers the above case of Ballet, along with the cases of Lebar and Raynaud, to be not true cases. Raynaud’s case was probably vascular.
Re vasomotor disorders in Ballet’s case, the Babinski school, of course, holds that hysteria cannot cause such disorders.
Re vasomotor disorders in Ballet’s case, the Babinski school, of course, believes that hysteria cannot cause such disorders.
Hemiparesis with syringomyelic dissociation of sensations.
Hemiparesis with syringomyelic differences in sensations.
Case 408. (Ravaut, August, 1915.)
A road-laborer, 42, in the 268th Infantry, had a bomb burst about a meter away, March 4, 1915. Three men nearby were killed, and two wounded. The laborer himself was turned over, covered with earth, and stunned. He could hardly get up. He was carried to shelter and found paralyzed on the left side, and unable to speak.
A road worker, 42, in the 268th Infantry, had a bomb explode about a meter away on March 4, 1915. Three men nearby were killed, and two were injured. The worker himself was knocked over, covered in dirt, and dazed. He could barely get up. He was taken to safety and was found paralyzed on his left side and unable to speak.
Next day, he was carried to the ambulance, and hemianesthesia was found to exist in addition to the hemiplegia. He could now speak with some difficulty and stammered. Vision and hearing were also impaired on the left side. Reflexes weak; no sign of wound. There was a convulsive crisis of some sort during the day, and afterwards the man complained of a violent headache, whereupon a lumbar puncture showed a clear fluid and a marked excess of albumin by the heat test.
The next day, he was taken to the ambulance, and it was discovered that he also had hemianesthesia along with the hemiplegia. He could speak with some difficulty and stammered. His vision and hearing were also affected on the left side. Reflexes were weak, and there were no signs of a wound. He experienced some kind of convulsive episode during the day, and afterward, he complained of a severe headache, which led to a lumbar puncture that revealed clear fluid and a significant excess of albumin based on the heat test.
The following day, March 6, the patient had much improved; his hemiplegia was less marked and the arm paralysis had almost entirely disappeared. He still stammered.
The next day, March 6, the patient was much better; his half-body paralysis was less noticeable and the arm paralysis had almost completely vanished. He was still stammering.
Upon the next day, vision and hearing were normal, and the sensation was practically normal. A second lumbar puncture, March 8, showed a diminution in the amount of albumin, although it was still supernormal.
The next day, vision and hearing were normal, and the sensation was almost normal. A second lumbar puncture on March 8 showed a decrease in the amount of albumin, although it was still above normal.
March 9, leg contractured in extension; stammering.
March 9, leg stiff and straight; stuttering.
March 12, there was no evidence of disease. March 13, albumin was very slightly increased over the normal in the puncture fluid. March 16, there was a slight trace only of weakness in the left leg. The urine was throughout normal. The patient wrote Bavo April 12, and May 7 he was well but still felt heaviness and pulling sensations.
March 12, there was no sign of disease. March 13, albumin was only slightly elevated in the puncture fluid. March 16, there was just a minor trace of weakness in the left leg. The urine was normal throughout. The patient wrote Bavo on April 12, and by May 7, he was doing well but still experienced feelings of heaviness and pulling sensations.
July 15 it was reported at Tours that he was not yet well, presenting a left-sided hemiparesis, especially in the leg, with a syringomyelic dissociation of sensations, with atrophy of the quadriceps and diminution of reflexes on the left side. The patient had had a hematomyelia (Laignel-Lavastine).
July 15, it was reported in Tours that he was still not well, showing weakness on the left side, especially in the leg, along with a disconnect in sensations due to syringomyelia. There was also atrophy of the quadriceps and reduced reflexes on the left side. The patient had experienced hematomyelia (Laignel-Lavastine).
Brachial monoplegia, tetanic.
Brachial monoplegia, tetanus.
Case 409. (Routier, 1915.)
A soldier sustained a penetrating wound of the back of the thorax on the left side and received an injection of antitetanic serum. A few days later, May 18, 1915, he came on hospital service very sick, with high temperature and marked suppuration. The next day he had an anxious facies, temperature of 40 degrees, and sharp pains in the left arm. This arm May 21 was still very painful and then began to make involuntary movements in the shape of incessant clonic contractions. The forearm would suddenly flex upon the upper arm, and the upper arm itself would violently push itself forward and outward. Meantime, the wrist and fingers were not involved in the contractions. The movements were continuous, but paroxysmally increased in extent.
A soldier had a serious wound on the left side of his back and received an injection of antitetanic serum. A few days later, on May 18, 1915, he came to the hospital very sick, with a high fever and significant pus formation. The next day, he appeared anxious, had a temperature of 104 degrees, and experienced sharp pain in his left arm. By May 21, that arm was still very painful and started making involuntary movements that looked like constant, repetitive contractions. The forearm would suddenly bend towards the upper arm, and the upper arm would push forward and outward forcefully. Meanwhile, the wrist and fingers were not affected by the contractions. The movements were ongoing but would occasionally become more intense.
Babinski, called in consultation, confirmed the diagnosis of an anomalous form of tetanus. Next day trismus, pleurosthotonos, and stiff neck developed. Antitetanic serum and chloral had been given from the beginning, with morphine at night. The patient, however, died with asphyxia June 3.
Babinski, called for a consultation, confirmed the diagnosis of an unusual form of tetanus. The next day, trismus, pleurosthotonos, and a stiff neck developed. Antitetanic serum and chloral had been administered from the start, along with morphine at night. However, the patient died from asphyxia on June 3.
Re brachial monoplegia, the hysterotraumatic form first observed by Charcot has an anesthesia with the shoulder of mutton distribution, slightly affecting the thorax in front and behind, in addition to the paralysis.
Re brachial monoplegia, the hysterotraumatic type first noted by Charcot, has a numbness that spreads over the shoulder in a mutton-like pattern, slightly impacting the front and back of the chest, along with the paralysis.
Paralysis of right leg: Hysterical? Organic? “Micro-organic?”
Paralysis of right leg: Hysterical? Biological? “Micro-organic?”
Case 410. (Von Sarbo, January, 1915.)
A Lieutenant, aged 28, lost consciousness September 6, 1914, as the result of a shell explosion. When consciousness returned in the hospital, he could not remember what had happened. The last he remembered was that he had been pushing forward with his troop. There had been no psychic shock whatever. Examined September 15, he showed a right-sided hemiplegia with stiffness of the right lower extremity so that it could not be even passively flexed. It was with difficulty he could walk and he dragged his right foot. Patellar reflex could not be elicited on the right. Oppenheim and Babinski were absent. There was a slight nystagmus on looking to the right. Pupils normal. Tongue deviated to the left. Speech was slow and the man had to think a little over some expressions. He could not feel touch so well on the right as on the left and this hypesthesia grew more marked distally. He was greatly bothered because certain words did not come to him readily, especially names.
A 28-year-old Lieutenant lost consciousness on September 6, 1914, due to a shell explosion. When he regained consciousness in the hospital, he couldn’t remember what had happened. The last thing he remembered was pushing forward with his troop. There was no sign of psychological shock. When examined on September 15, he showed right-sided hemiplegia with stiffness in his right leg, making it impossible to even passively flex. He found it difficult to walk and dragged his right foot. The patellar reflex could not be triggered on the right side. Oppenheim and Babinski tests were negative. He had slight nystagmus when looking to the right. His pupils were normal. His tongue deviated to the left. His speech was slow, and he struggled to find certain words, particularly names. He also had reduced sensitivity to touch on the right side compared to the left, and this loss of feeling increased distally. He was very frustrated that some words didn't come to him easily, especially names.
The absence of the Babinski and Oppenheim reflexes was against an organic hypothesis and the absence of hysterical stigmata and the non-characteristic sensory disorder, as well as the absence of any psychic shock in the history, spoke against hysteria. The hypoglossus paralysis spoke in favor of the organic nature of the disease.
The lack of the Babinski and Oppenheim reflexes went against an organic explanation, and the absence of hysterical signs, the unusual sensory issue, and any history of psychological trauma argued against hysteria. The hypoglossal paralysis supported the idea that the disease had an organic origin.
According to von Sarbo we must look for the background of so-called functional nervous disorders, hysteria and neurasthenia, in structural changes of the nervous system, the changes that Charcot called molecular. But the lesions, he believes, do not lead to a degeneration of neurons. Accordingly we get only the external form of organic paralysis without concomitant symptoms, such as Oppenheim and Babinski reflexes. Von Sarbo terms his hypothesis that of “microörganic” changes. To prove the hysterical nature of a condition we must show first that the symptoms have taken their rise on a mental or moral basis.
According to von Sarbo, we need to look for the background of what we call functional nervous disorders, hysteria, and neurasthenia in structural changes of the nervous system, which Charcot referred to as molecular changes. However, he believes that these lesions do not cause degeneration of neurons. As a result, we only observe the outward appearance of organic paralysis without associated symptoms, such as the Oppenheim and Babinski reflexes. Von Sarbo refers to his theory as the hypothesis of "microorganic" changes. To demonstrate the hysterical nature of a condition, we first need to show that the symptoms have originated from a mental or moral basis.
Shell-shock and momentary burial: Muscular weakness, followed (third day) by complete paralysis (save neck and head). Diagnostic hypotheses.
Shell shock and temporary immobilization: muscle weakness, followed (on the third day) by total paralysis (except for the neck and head). Diagnostic assumptions.
Case 411. (Léry, Froment and Mahar, July, 1915.)
A big shell burst October 3, 1914, a little over 3 meters from a soldier crouching in a shallow Saint Mihiel trench. The shell made a hole two meters in diameter and 1.5 meters deep, and covered the man with loose earth, from which he was readily released. During the next few days, the man found difficulty in following his comrades on short marches (1 to 4 kilometers). He was unable to buckle on his knapsack. The patient was himself not alarmed at his condition.
A large shell exploded on October 3, 1914, just over 3 meters away from a soldier crouching in a shallow trench in Saint Mihiel. The shell created a hole 2 meters wide and 1.5 meters deep, covering the man with loose dirt, but he was quickly freed. In the following days, the man had trouble keeping up with his comrades on short marches (1 to 4 kilometers). He couldn't strap on his backpack. The soldier himself wasn't worried about his condition.
Up to the time of his accident, this man, a farmer, had never had any motor trouble, nor was there any nervous disorder in any of his relatives. He had been in several conflicts, August 24-25, September 4-6, in the Argonne and in the Haute Meuse, and he had never found it hard to keep up with his comrades. In fact, once in the Haute Meuse, he took part in an exceedingly difficult and hasty retreat, and only a week before the shell-shock above described he had put in a very long march. Thus a man, perfectly normal before the shock, had fallen into a general state of slight muscular paralysis.
Up until his accident, this man, a farmer, had never experienced any physical issues, nor did any of his relatives have any neurological conditions. He had participated in several battles, from August 24-25 and September 4-6, in the Argonne and Haute Meuse, and had never struggled to keep pace with his fellow soldiers. In fact, during one exceptionally tough and rapid retreat in the Haute Meuse, and just a week before the shell shock mentioned, he had completed a very long march. Thus, a man who was completely normal before the shock had ended up in a general state of mild muscular paralysis.
On the third day very suddenly this paralysis became complete. The wounded man, while sitting in the trench, found that he could not stand up either with or without the use of his hands. Now, that very morning he had marched three kilometers from his cantonment to the trench. He was supported on the way to the relief post, hardly 200 meters away, and was then sent to the hospital at Bar-le-Duc. At this time he was so weak that he had to be fed like a child.
On the third day, this paralysis suddenly became total. The injured man, sitting in the trench, realized he couldn’t stand up, whether he tried to use his hands or not. That same morning, he had marched three kilometers from his camp to the trench. He was helped the last 200 meters to the relief post and was then sent to the hospital in Bar-le-Duc. By this point, he was so weak that he had to be fed like a child.
For a period of three weeks he lay, unable to rise or sit up. There was one exception to the generalization of the paresis: the movements of the head and neck were normal. A general muscular atrophy set in during the three months, but gradually diminished in amount. The diagnosis of myopathy was made, based upon the evident degree of lumbar wasting,[574] kyphosis, the man’s attitude, gait, manner of rising, galvanotonic contractions.
For three weeks, he lay there, unable to stand or sit up. There was one exception to the overall weakness: the movements of his head and neck were normal. General muscle wasting began during the three months but slowly decreased over time. The diagnosis of myopathy was made based on the noticeable degree of lumbar wasting,[574] kyphosis, the man's posture, how he walked, how he got up, and the galvanotonic contractions.
The history was, of course, rather against the diagnosis of myopathy, as well as the marked atrophy of the hands and the existence of an incomplete R. D. Moreover the fact that he improved may be regarded as rendering the diagnosis of myopathy doubtful.
The history was, of course, somewhat against the diagnosis of myopathy, along with the significant atrophy of the hands and the presence of an incomplete R. D. Additionally, the fact that he showed improvement can be seen as making the diagnosis of myopathy questionable.
Other diagnoses, less likely than that of myopathy, may be considered,—hematomyelia, recurrent traumatic poliomyelitis affecting the anterior horns, polyneuritis.
Other diagnoses, which are less likely than myopathy, may be considered: hematomyelia, recurrent traumatic poliomyelitis affecting the anterior horns, and polyneuritis.
Without making decision as to the nature of this case, Léri proposes the question whether there is a shell-shock myopathy and whether there is a myopathy due to gas or to hemorrhage?
Without deciding on the nature of this case, Léri asks whether there is a shell-shock myopathy and whether there is a myopathy caused by gas or by hemorrhage?
Shell-shock: Right hemiplegia with contracture and mutism. Cure by isolation and suggestion. Question of the relation between plantar areflexia and (a) anesthesia (hysterical) or (b) contracture.
Shell shock: Right side paralysis with stiffness and inability to speak. Treatment involves isolation and suggestion. Explores the connection between no reflex in the foot and (a) anesthesia (hysterical) or (b) stiffness.
Case 412. (Dejerine, February, 1915.)
A territorial infantryman, 36, of a nervous and impressionable temperament (father alcoholic), was blown up by a bomb October 3, 1914, between Bapaume and Arras. He was evacuated forthwith to the relief post. According to his own story, he spat blood, could not talk, and felt his right side weak. He was three weeks at a hospital in Paimpol, with the diagnosis of right hemiplegia with contracture and mutism. At Guingamp, an electrical treatment was followed by a gradual disappearance of the arm contracture.
A 36-year-old territorial infantryman, who was nervous and impressionable (his father was an alcoholic), was blown up by a bomb on October 3, 1914, between Bapaume and Arras. He was immediately evacuated to the relief post. According to his own account, he spat blood, couldn’t speak, and felt weakness on his right side. He spent three weeks in a hospital in Paimpol, diagnosed with right hemiplegia, contracture, and mutism. In Guingamp, he received electrical treatment that gradually reduced the arm contracture.
Examined by Dejerine, January 2, 1915, he was found to be a tall, stalwart man with right leg contractured in extension, foot in equinovarus, heel raised. He walked, dragging the leg, which trembled; the trembling then extended to the rest of the body. In dorsal decubitus, the leg lay in adduction and internal rotation. He could lift the leg only 5 cm. above the bed, could only slightly flex leg on thigh, and could not at all flex thigh on hip. The leg could not be bent at all if he was requested to hold it stiff. Ankle joint movements were impossible from contracture. The equinovarus was in contracture which could not be corrected. Right hip movements were limited and painful. Muscular atrophy absent.
Examined by Dejerine on January 2, 1915, he was found to be a tall, strong man with his right leg held straight, foot turned inward and upward, and heel raised. He walked by dragging the leg, which trembled; then the trembling spread to the rest of his body. While lying on his back, the leg was positioned inward and rotated. He could lift the leg only 5 cm above the bed, could slightly bend the leg at the thigh, and could not bend the thigh at the hip at all. The leg could not be bent if he was asked to keep it straight. Movements in the ankle joint were impossible due to the contracture. The foot's position was locked in a way that couldn't be corrected. Movements in the right hip were limited and painful. There was no muscle wastage.
Whereas on the left side plantar stimulation produced not only the normal flexor reflex but also the classical defense movements of flexion of leg on thigh and thigh on hip,—on the right side neither a needle nor a match, nor any other form of stimulation of the sole, produced any kind of reaction on the part of the toes, the fascia lata, or any leg muscles. Tested every day for some weeks, the result was always the same. The cremasteric reflex was weak on the affected side. Abolition of the plantar reflex and of the defense movements[576] on the right side was associated with an anesthesia and a hypesthesia of the right side of the body, involving complete anesthesia below the knee and hypesthesia of superficial and deep sensation above the knee. The buccal and lingual mucous membranes were also hypesthetic. The bony sensibility was lost in the foot and lower leg, and was diminished in all of the bones of the right side of the body. There was no contraction of the visual fields. The right corneal reflex was diminished. There were no other sensory defects.
On the left side, when the bottom of the foot was stimulated, it triggered not only the usual flexor reflex but also the typical defense movements, like bending the leg at the thigh and the thigh at the hip. However, on the right side, no matter if a needle, a match, or any other type of stimulation was applied to the sole, there was no reaction from the toes, the fascia lata, or any muscles in the leg. Testing was done every day for several weeks, and the result was consistently the same. The cremasteric reflex was weak on the affected side. The absence of the plantar reflex and defense movements on the right side was linked to a loss of sensation and reduced sensitivity on the right side of the body, with total loss of sensation below the knee and reduced sensitivity to superficial and deep sensations above the knee. The mucous membranes in the mouth and tongue were also less sensitive. Sensitivity to pain in the bones was lost in the foot and lower leg, and decreased in all the bones on the right side of the body. There was no contraction in the visual fields. The right corneal reflex was reduced. No other sensory issues were noted.
The man was also aphonic, being unable to utter a word or a sound except a jerky whistling sound like the letting off of steam. He was able to write out his history intelligently. He was very emotional, wept, and trembled all over when talking of wife and children. The spinal puncture fluid was in all respects normal. A laryngoscopic examination showed that the vocal cords were functioning normally. The long a could be pronounced distinctly, at the expense of great effort so that the larynx would finally be blocked. The laryngeal reflex was abolished. The laryngeal mucosa could be touched with a probe without producing the slightest pain or coughing reflex. By way of treatment, this case of hysterotraumatism was given isolation and psychotherapy for two months without effect. But about the middle of March he began to get better, the symptoms rapidly faded, cure was effected at the end of March, and the man was evacuated to his dépôt.
The man was also unable to speak, making only a jerky whistling sound like steam escaping. He could write about his life clearly. He was very emotional, crying and shaking all over when talking about his wife and kids. The spinal fluid was completely normal. A laryngoscopy showed that his vocal cords were working fine. He could pronounce a long a distinctly, but it took a lot of effort, and eventually, he would become blocked. The laryngeal reflex was absent. The laryngeal mucosa could be touched with a probe without causing any pain or coughing reflex. For treatment, this case of hysterotraumatism was given isolation and psychotherapy for two months without any result. But around mid-March, he started to improve, the symptoms quickly faded, he was cured by the end of March, and the man was moved back to his depot.
Re reflexes and contracture, see the views of Babinski reproduced under Case 385 of Paulian.
Re reflexes and contracture, see the opinions of Babinski reproduced under Case 385 of Paulian.
Shell-shock: Tic VERSUS spasm.
Shell shock: Tic vs spasm.
Case 413. (Meiji, July, 1916.)
A soldier was bowled over in a trench by a big shell that burst nearby. He lost consciousness and was carried to the ambulance. But he came to, and was so absolutely well with a few hours’ rest that he took part in a lively attack shortly thereafter and got a wound in the left arm, affecting slightly the ulnar nerve. He was sent to the Salpêtrière for this ulnar nerve affection, when certain movements of his scalp were incidentally noted.
A soldier was knocked over in a trench by a large shell that exploded nearby. He lost consciousness and was taken to the ambulance. However, he regained consciousness and felt completely fine after a few hours of rest, so he joined in a vigorous attack shortly after and sustained a wound in his left arm, which slightly affected the ulnar nerve. He was sent to the Salpêtrière for this ulnar nerve issue when certain movements of his scalp were incidentally observed.
The scalp movements were quick, affecting the fronto-occipitalis muscles as well as the auricular muscles. The displacement was from behind forward, and then from before backward, with slight oscillations of the ear; and at the same time, the forehead wrinkled or became smooth. The movement was involuntary and more convulsive than the somewhat similar movements that many persons can execute with scalp and ears. The phenomenon appeared after the shock for the first time. He had not noticed it himself but the physician at the ambulance had called his attention to it. The soldier was not disturbed by the matter, either at that time or later.
The movements of the scalp were rapid, involving both the fronto-occipitalis and the ear muscles. The motion went from back to front, and then from front to back, with slight wiggling of the ear; at the same time, the forehead would either wrinkle or smooth out. The movement was involuntary and more convulsive than the similar movements that many people can make with their scalp and ears. This phenomenon first appeared after the shock. He hadn’t noticed it himself, but the doctor at the ambulance pointed it out to him. The soldier was not bothered by it, either at that moment or later.
The diagnostician would consider, on the one hand, tic, and on the other, spasm. According to Meige, the man was a victim of tic. No case of such limited spasm appears to have been observed previously. However, the sudden development of these movements without previous history of tic renders the diagnosis somewhat doubtful. There was also a complete anesthesia to pin-prick in the present case over the whole right side of the scalp, face, and neck, even passing below to involve the chest, shoulder, back, and upper part of the right arm, with hypesthesia decreasing toward the nipple and the elbow. The soldier was quite ignorant of this sensory disorder and had never before been examined for sensations. The examination was made with due precautions to avoid suggestion. The question of anastomosis[578] between the facial nerve and the auriculo-temporal branch of the trigeminus and the auricular branch of the cervical plexus, and of their relations to the anesthesia and tic of this case, is raised.
The diagnostician would consider, on one hand, tic, and on the other, spasm. According to Meige, the man was a victim of tic. No case of such limited spasm seems to have been observed before. However, the sudden appearance of these movements without any prior history of tic makes the diagnosis somewhat questionable. There was also complete numbness to pin-prick on the entire right side of the scalp, face, and neck, even extending down to involve the chest, shoulder, back, and upper part of the right arm, with reduced sensitivity decreasing towards the nipple and elbow. The soldier was completely unaware of this sensory disorder and had never been examined for sensations before. The examination was carried out with proper precautions to avoid suggestion. The question of anastomosis[578] between the facial nerve and the auriculo-temporal branch of the trigeminal nerve, as well as the auricular branch of the cervical plexus, and their relation to the numbness and tic in this case, is raised.
Re pathological movements such as tremors, tics, and choreiform movements, Roussy and Lhermitte divide the tremors (see also under Case 337) into typical and atypical.
Re pathological movements like tremors, tics, and choreiform movements, Roussy and Lhermitte categorize the tremors (see also under Case 337) into typical and atypical.
The atypical ones are either limited, or more usually generalized when they are merely parts of the Shell-shock syndrome. Sometimes the tremors are paroxysmal, aggravated by noises. Now and then, a condition of tremophobia appears (see Case 225). As for the typical tremors, see classifications under Case 337.
The unusual cases are either limited or, more commonly, generalized when they are just parts of the Shell-shock syndrome. Sometimes, the tremors are sudden and made worse by loud noises. Occasionally, a fear of tremors, known as tremophobia, occurs (see Case 225). For information on the typical tremors, refer to the classifications under Case 337.
Re tics, the tonic or postural tic is, according to Roussy and Lhermitte, much less common than clonic or spasmodic movements, which are Shell-shock phenomena like tremors and usually yield to psychotherapy if treated early. These tics are usually observed in and about the head, involving the sternomastoid, trapezius, and platysma muscles to produce clonic contractions of the neck. Other tics involve coarser head movements, nodding, eyelid and facial spasms, bilateral or unilateral, and shoulder movements. Babinski has suggested that some of the tremors are possibly due to organic disease, in view of the fact that they are not readily influenced by psychotherapy. Meige has suggested that some of the tics may also be in some sense organic. As for the differential diagnosis of tremor and tic, according to Roussy and Lhermitte, the Shell-shock onset may be an indicator. The non-rhythmic and irregular nature of the tic movements, and their exaggeration on voluntary movement, may be of some importance. Most of the tremors appear to be attended by a certain degree of permanent contraction of the muscle groups concerned. Tremors cease when these contractions disappear.
Re tics, the tonic or postural tic is, according to Roussy and Lhermitte, much less common than clonic or spasmodic movements, which are Shell-shock phenomena like tremors and usually respond well to psychotherapy if addressed early. These tics are generally seen around the head, involving the sternomastoid, trapezius, and platysma muscles, leading to clonic contractions in the neck. Other tics include more pronounced head movements, nodding, eyelid and facial spasms, either on one side or both, and shoulder movements. Babinski has suggested that some of the tremors could be caused by an organic disease, since they don't easily respond to psychotherapy. Meige proposes that some of the tics might also have an organic component. Regarding the differential diagnosis of tremor and tic, Roussy and Lhermitte point out that the onset related to Shell-shock may be a key indicator. The non-rhythmic and irregular quality of tic movements, alongside their amplification during voluntary actions, could be significant. Most tremors seem to be associated with a degree of ongoing contraction in the affected muscle groups. Tremors stop when these contractions go away.
A point in treatment is that complete muscular relaxation should be obtained by having the patient open his mouth and breathe deeply.
A key aspect of treatment is that total muscle relaxation should be achieved by having the patient open their mouth and breathe deeply.
Re diagnosis of neurasthenia in this case, it may be inquired whether the term is properly used, and whether[579] there is not some confusion here betwixt neurasthenia and hysteria.
Re diagnosis of neurasthenia in this case, it may be questioned whether the term is used correctly, and whether[579] there is some confusion between neurasthenia and hysteria.
Re hyperalgesia, Myers states that about 25 per cent of his Shell-shock cases have shown a variety of disorders of the skin sense. Hyperesthesia and over-reaction is one phenomenon in the list, but is far less common than hyperesthesia. According to Myers, the hyperesthesia was more relative than absolute, and was probably due to increased affective response.
Re hyperalgesia, Myers says that around 25 percent of his Shell-shock cases have displayed various skin sensitivity disorders. Hyperesthesia and over-reaction are one of the phenomena on the list, but they are much less common than hyperesthesia. According to Myers, the hyperesthesia was more relative than absolute and was likely caused by an increased emotional response.
Shell-shock; unconsciousness: Tremors, anesthesias. Recovery by suggestion.
Shell shock; unconsciousness: Tremors, numbness. Recovery through suggestion.
Case 414. (Mott, January, 1916.)
August, 1915, between Ypres and Flamentières, a Jack Johnson exploded one day about three o’clock in the morning near an experienced gunner, who had been on service in the R. F. A. for 15 years, and in France during the present war 10 months. He came to in the military hospital at Chatham, two weeks later, and was told he was lucky to be there at all as the shell had killed many comrades. He was transferred to Colchester, and thence to the Fourth London General Hospital.
August 1915, between Ypres and Flamentières, a Jack Johnson went off one morning around three o'clock near a seasoned gunner who had served in the R. F. A. for 15 years and had been in France for 10 months during the current war. He woke up in the military hospital in Chatham two weeks later and was told he was lucky to be alive since the shell had killed many of his comrades. He was moved to Colchester, and then transferred to the Fourth London General Hospital.
Sitting in a chair, the man showed continuous rhythmic movements of legs, hands, and jaw, exaggerated when he was spoken to. The tremor was almost a clonic spasm. Every now and then, the patient would start and look sidewise and upwards, as if a shell were about to drop. Hyperacusis was such that the firing of the guns as far off as Woolwich alarmed him. In telling his story, he would repeat the same words over and over. He dreamt of shells bursting. His sleep was disturbed with groaning and moaning. The face was flushed, and the palms sweating. Because of the constant tremor, he could not stand or walk without assistance, and it was difficult to test reflexes. The tremor somewhat resembled the intention tremor of multiple sclerosis. He was unable to feel the prick of the needle on legs, left arm, or hand. He could not feel vibrations of the tuning-fork on feet, legs, or hands, though he could on the forehead. The fork was heard quite well six inches from the ears. There was some difficulty in recognizing colors. Bitter fluids could be tasted, but vinegar, salt, and various fluids, could not be recognized. He could not recognize tincture of assafetida, attar of roses, or oil of cloves, though nitrite of amyl, ammonia and glacial acetic acid were recognized.
Sitting in a chair, the man exhibited continuous, rhythmic movements of his legs, hands, and jaw, becoming more pronounced when spoken to. The tremor was almost like a clonic spasm. Occasionally, the patient would startle and glance sideways and upwards, as if anticipating a shell's impact. His sensitivity to sound was such that even the distant firing of guns from Woolwich startled him. When recounting his story, he would repeat the same phrases multiple times. He dreamt of shells exploding. His sleep was unsettled with groans and moans. His face was flushed, and his palms were sweaty. Due to the constant tremor, he couldn't stand or walk without help, and it was challenging to assess his reflexes. The tremor resembled the intention tremor seen in multiple sclerosis. He was unable to feel the prick of a needle on his legs, left arm, or hand. He couldn't sense vibrations from a tuning fork on his feet, legs, or hands, though he could feel it on his forehead. The fork was audible from six inches away. He had some trouble recognizing colors. He could taste bitter fluids, but couldn't identify vinegar, salt, or other liquids. He failed to recognize tincture of assafetida, attar of roses, or oil of cloves, but could identify amyl nitrite, ammonia, and glacial acetic acid.
Major Mott felt that, though this prolonged severe disease in a long-service man might possibly be related to some organic[581] change in the brain, he might well treat him by suggestion. Major Mott told him that the careful examination just made showed that there was no organic disease, and made it certain that he would recover. In a fortnight, he sat in a chair without tremors and with a profound belief in Major Mott.
Major Mott felt that although this extended serious illness in a long-serving man might be linked to some physical change in the brain, he could effectively treat him through suggestion. Major Mott informed him that the thorough examination just conducted indicated there was no physical disease and assured him that he would recover. Two weeks later, he sat in a chair without shaking and had a deep trust in Major Mott.
Hysteria as appendix to traumata.
Hysteria as a result of trauma.
Case 415. (MacCurdy, July, 1917.)
A private, 25, something of a liar and of rather a low personality, had enlisted in the regular army in 1911, but deserted to become a football player. He reënlisted, and went to France in September, 1914, enjoying the first six months. He broke his ankles by falling into a deep dug-out, and got frost-bite. After three or four months in England, he found that he did not wish to go back to France. He was two months in barracks, and then went up the line in a good deal of a panic. Soon after, he was wounded in the thigh and was able to remain in hospital a fortnight, exposed, however, to shell-fire and given to starting at noise and occasional war dreams. Sent to his base, he remained jumpy and was now permanently afraid of the line. After three weeks in the trenches, he again got wounds, spent five months in England, came back to France in May, and fought till September, 1916. He tried to convince the medical officer that he had appendicitis and trench fever.
A private, 25, who was somewhat of a liar and had a pretty low character, joined the regular army in 1911 but deserted to become a football player. He rejoined and went to France in September 1914, enjoying the first six months. He broke his ankles after falling into a deep dugout and got frostbite. After three or four months back in England, he decided he didn’t want to return to France. He spent two months in barracks, then went back to the front line in quite a panic. Shortly after, he was injured in the thigh and was able to stay in the hospital for two weeks, although he was still exposed to shell-fire and began to jump at loud noises and have occasional war-related nightmares. Sent back to his base, he remained anxious and was now permanently scared of the front line. After three weeks in the trenches, he got wounded again, spent five months in England, returned to France in May, and fought until September 1916. He tried to convince the medical officer that he had appendicitis and trench fever.
About the middle of September he saw with horror a man crushed by a tank, and thereafter was markedly affected by the sight of blood. Another slight wound sent him to a rest camp for two weeks, whence he was again thrown into the line, suffering acutely from fear and horror of blood. In three days he fractured his left collarbone and wrist. He gave a pint and a half of blood for transfusion purposes, and in turn was shipped to England. On removal of the splint, he found “probably not without satisfaction” that the arm was paralyzed. It remained paralyzed for five months, until treatment in a special hospital eventually cured the arm; but upon cure of the arm, nightmares developed,—an indication, according to MacCurdy, of the strong resistance he felt to the idea of returning to the front.
About the middle of September, he watched in horror as a man was crushed by a tank, and after that, he was deeply affected by the sight of blood. A minor injury sent him to a rest camp for two weeks, after which he was thrown back into the line, suffering intensely from fear and horror of blood. In just three days, he fractured his left collarbone and wrist. He donated a pint and a half of blood for transfusion and was then sent to England. When the splint was removed, he discovered “probably not without satisfaction” that his arm was paralyzed. It stayed paralyzed for five months until treatment in a special hospital eventually healed it; however, once his arm was healed, he began having nightmares—an indication, according to MacCurdy, of the strong resistance he felt about the idea of going back to the front.
Neurasthenic hyperalgesia after peripheral nerve injury.
Neurasthenic hyperalgesia after peripheral nerve injury.
Case 416. (Weygandt, January, 1915.)
A German volunteer, a sportsman, was under heavy shell fire after the middle of October, 1914, and was wounded in the upper arm in November, with an injury to the median nerve that occasioned severe pain. These strictly localized pains increased upon any sort of physical or mental strain. If he walked down steps he kept thinking he might have an accident, and then the pains set in with greater force. He became apathetic so that he did not eat, drink or urinate. If his head were touched he felt pain as if from an electric shock. He also felt the pain when he saw anybody approaching a door to close it, through apprehension of the noise. Meantime, the wound was well healed. The pulse was accelerated. The visual fields were only slightly contracted. The patient wanted to get well and go back to the service.
A German volunteer, an athlete, was under heavy shell fire after mid-October 1914 and was wounded in the upper arm in November, suffering an injury to the median nerve that caused severe pain. These localized pains worsened with any physical or mental stress. When he walked down steps, he kept thinking he might have an accident, which intensified the pain even more. He became apathetic to the point that he stopped eating, drinking, or urinating. If someone touched his head, it felt like an electric shock. He also experienced pain when he saw anyone approaching a door to close it, out of fear of the noise. Meanwhile, the wound had healed well. His pulse was fast, and his visual fields were only slightly narrowed. The patient was eager to recover and return to service.
Weygandt regards this hyperalgesia after peripheral nerve injuries as neurasthenic.
Weygandt sees this increased sensitivity to pain after peripheral nerve injuries as neurasthenic.
Military training: Peripheral neuritis in lead workers.
Military training: Peripheral neuritis in lead workers.
Case 417. (Shufflebotham, April, 1915.)
Among fourteen cases of lead poisoning, members of the territorial forces, largely from North Staffordshire, was a patient suffering from peripheral neuritis. He had been in the dipping-house. Two years before going into the service he had been suspended for lead poisoning by the factory surgeon. Giving up his work at the pottery, he became a general laborer in a non-lead process factory.
Among fourteen cases of lead poisoning, a patient from the territorial forces, mostly from North Staffordshire, had peripheral neuritis. He had worked in the dipping-house. Two years before joining the service, he had been suspended for lead poisoning by the factory doctor. After leaving his job at the pottery, he became a general laborer in a factory that didn’t use lead.
Three weeks after enlistment, the man began to complain of pains, tenderness in the arms, weakness of the wrists, headache, giddiness, nausea, and constipation. The bowels were opened by a large dose of epsom salts. On blood examination the hemoglobin was found diminished 40 per cent; cells with basophilic granules were found to the number of 500 per cu. mm. The face was characteristically pasty. There was albuminuria. Alcohol could be excluded. The man had to be discharged.
Three weeks after joining up, the man started to complain of pain, tenderness in his arms, weakness in his wrists, headaches, dizziness, nausea, and constipation. His bowels were cleared with a large dose of Epsom salts. A blood test showed his hemoglobin was down by 40 percent; there were 500 cells with basophilic granules per cubic millimeter. His face looked notably pale. There was albumin in his urine. Alcohol could be ruled out. The man had to be discharged.
All Shufflebotham’s cases occurred from three to seven weeks after mobilization, nor have any cases ever been reported in territorials after their annual training. Constipation was invariable. In two cases returned to service, there was a recurrent attack. An epidemic could be excluded. Shufflebotham suggests that the altered conditions of life, especially the marching and drilling, caused increased metabolism, setting free lead compounds from the muscles and organs of the body. It is true that a glost placer always works very hard with his muscles, but not with the muscles used by the soldier.
All of Shufflebotham's cases happened three to seven weeks after mobilization, and there have been no cases reported in territorials after their annual training. Constipation was consistent. In two cases that returned to service, there was a recurring episode. An epidemic can be ruled out. Shufflebotham suggests that the changes in lifestyle, particularly due to marching and drilling, led to increased metabolism, releasing lead compounds from the muscles and organs of the body. It's true that a glost placer works their muscles very hard, but not with the same muscles used by a soldier.
“Peripheral neuritis” cured by faradism.
“Peripheral neuritis” treated with faradism.
Case 418. (Cargill, February, 1916.)
A Naval Service man, 20, was thought to have peripheral neuritis. A long history of pain and numbness in arms and legs, a well-marked analgesia and anesthesia over the anterior aspects of forearms and legs, and an anesthetic band across the front of the chest, seemed consistent with the diagnosis. The calf muscles tightly squeezed yielded no pain. Pins could be thrust without pain into the anesthetic areas. When told to say yes when the pin was felt, and no when it was not felt, the man persistently said no when the areas noted above were touched. The deep reflexes were normal. Faradism by wire brush at two sittings yielded a complete cure. It seems that once this man, after seeing his sister fall in a fit on returning from a funeral, retired to the garden and had a similar fit himself.
A 20-year-old member of the Naval Service was believed to have peripheral neuritis. He had a long history of pain and numbness in his arms and legs, along with noticeable sensitivity loss and numbness on the front sides of his forearms and legs, as well as a numb band across his chest, which aligned with the diagnosis. His calf muscles were tightly squeezed without causing any pain. Pins could be poked into the numb areas without eliciting pain. When asked to say yes when he felt the pin and no when he didn’t, the man consistently said no when the areas mentioned earlier were touched. His deep reflexes were normal. Treatment with Faradism using a wire brush over two sessions resulted in a complete recovery. It appears that after witnessing his sister have a seizure following a funeral, he went to the garden and experienced a similar seizure himself.
Cargill found in 1052 sailors fifteen cases of total absence of one or both ankle-jerks; seven of the fifteen were probably cases of tabes.
Cargill discovered in 1052 sailors that fifteen cases showed a complete lack of one or both ankle reflexes; seven out of the fifteen were likely cases of tabes.
Re peripheral neuritis and hysteria (see under Case 387).
Re peripheral neuritis and hysteria (see under Case 387).
Re differential diagnosis between peripheral neuritis and reflex (physiopathic) paralysis, Babinski and Froment offer the following table:
Re differential diagnosis between peripheral neuritis and reflex (physiopathic) paralysis, Babinski and Froment provide the following table:
| Peripheral Neuritis. | Reflex Paralysis and Contracture. |
|---|---|
| 1. Motor disorder, degenerative amyotrophy, and sensory disorder corresponding topographically to anatomical distribution of nerve (neuritic) topography. | 1. More or less segmentary topography. |
| 2. Amyotrophy very pronounced, regardless of localization. | 2. Amyotrophy variable; ordinarily well-marked but not so severe as that of neuritis. |
| 3. Reaction of degeneration, especially weakening or abolition of faradic excitability of muscles. | 3. Reaction of degeneration absent, never marked weakening of faradic excitability, which is often normal and may even be exaggerated. |
| 4. Tendon reflexes, corresponding to the muscular territory of the nerve, weakened or abolished. | 4. If reflexes are altered, they are as a rule exaggerated and never abolished. |
Multiple wounds; signs of late tetanus 7-8 weeks later: Pain and contracture of neck, tetanic, 14 weeks after trauma. Dysentery. Recovery.
Multiple wounds; signs of late tetanus 7-8 weeks later: Pain and stiffness in the neck, tetanic, 14 weeks after the injury. Dysentery. Recovery.
Case 419. (Flower arrangement, 1916.)
A soldier invalided for endocarditis July 8, 1908, went back to the colors on his own request August 8, 1914. He was wounded at noon September 6, 1914, in the attack at Abbaye Woods. He lay in the woods, with several comrades as badly wounded as himself, until September 10, eating berries and drinking rain water. He had five wounds in all; in left lower leg, thigh, left external malleolus, right calf, and left forearm. Moreover, he had dysentery.
A soldier who was discharged due to endocarditis on July 8, 1908, requested to rejoin his unit on August 8, 1914. He was injured at noon on September 6, 1914, during the attack at Abbaye Woods. He lay in the woods with several other severely wounded comrades until September 10, eating berries and drinking rainwater. He had five wounds in total: one in his left lower leg, one in his thigh, one on his left outer ankle, one in his right calf, and one in his left forearm. Additionally, he suffered from dysentery.
He was picked up by the Germans September 10 and carried by them to the ambulance at Saint André, where he was given belated first dressing. When the enemy retreated September 12 he was left behind and finally carried back September 13 into the French lines by a French physician who had been a prisoner likewise. A second dressing was given September 14 at Rambluzin. He was then carried in a sanitary train to Bar-sur-Aube, where, September 15, injection of antitetanic serum was given. He left Bar-sur-Aube on December 18, 1914, practically cured, though one of the wounds still needed care. The dysentery was still present and walking was difficult. He was then cared for at Auxiliary Hospital No. 102 in Paris.
He was picked up by the Germans on September 10 and taken to the ambulance at Saint André, where he received delayed first aid. When the enemy retreated on September 12, he was left behind and finally brought back into the French lines on September 13 by a French doctor who had also been a prisoner. A second dressing was done on September 14 at Rambluzin. He was then transported in a sanitization train to Bar-sur-Aube, where, on September 15, he received an injection of antitetanic serum. He left Bar-sur-Aube on December 18, 1914, almost fully recovered, though one of the wounds still needed care. He still had dysentery and found walking difficult. He was then looked after at Auxiliary Hospital No. 102 in Paris.
It seems that about six weeks after his entrance in the hospital at Bar-sur-Aube he had had some difficulty in opening his jaws, with acute pains at the temporomaxillary joint. Similar pains appeared a few days later in the neck, with a sensation of stiffening. The jaws still opened easily enough December 18, yet the man got pains in his jaws as soon as he began to speak. The pain and contracture in the neck region were sharp and permanent. Sometimes the contracture got more marked, and the board-like muscles could be felt stiffening under the examining finger. During such crises the patient had to lie or sit down. Sometimes the[587] pains descended below the shoulders along the vertebral column. The crises occurred more often in the night, in bed.
It seems that about six weeks after he was admitted to the hospital in Bar-sur-Aube, he started having trouble opening his mouth, with sharp pain in his jaw joint. A few days later, similar pain appeared in his neck, accompanied by a feeling of tightness. On December 18, he could still open his mouth fairly well, but he experienced pain in his jaw as soon as he started to talk. The pain and tightness in his neck were intense and persistent. Sometimes the tightness became more pronounced, and the muscles felt stiff under the examining finger. During these episodes, the patient had to lie down or sit. At times, the pain radiated down below the shoulders along the spine. These episodes occurred more frequently at night while he was in bed.
The diagnosis of late tetanus was made, and alcohol rubs were given. The phenomena gradually disappeared. The dysentery also had not yielded to therapeutics until eight or ten days before the patient left the hospital. There was still, at the time of report, a certain difficulty in walking, with a tendency to use the external border of the left foot rather than the sole.
The diagnosis of late tetanus was confirmed, and alcohol rubs were applied. The symptoms gradually went away. The dysentery had not responded to treatment until about eight or ten days before the patient was discharged from the hospital. At the time of the report, there was still some difficulty walking, with a tendency to use the outer edge of the left foot instead of the sole.
Shell-shock: Spasmodic neurosis and neurasthenia. Treatment without great success.
Shell-shock: Sudden anxiety disorder and fatigue. Treatment without much success.
Case 420. (Oppenheimer, July, 1915.)
August 19, 1914, a shell exploded very close to a soldier, whose bread bag, cartridge container, and field flask were pulled away from him, but who was not himself wounded. He fell down. Shortly developed headache, vertigo, palpitation. In running he fell down repeatedly. Spasms soon appeared in the legs. He had previously suffered from gastric disturbances, and heavy food did not agree with him.
August 19, 1914, a shell exploded very close to a soldier, whose bread bag, cartridge container, and canteen were ripped away from him, but he wasn't hurt. He fell down. He quickly developed a headache, dizziness, and a racing heart. While running, he kept falling down. Soon, spasms appeared in his legs. He had previously experienced stomach issues, and heavy foods didn't sit well with him.
At the time of admission to hospital he complained of great irritability, nervous twitching, formication in his limbs, war dreams, tachycardia. The heart boundaries were normal. The muscles of lower extremities were attacked by tonic spasms, and felt board-like. This tonic spasm occurred on each attempt at motion, very gradually disappearing when at rest. Passive movements also had the same effect. Fibrillary tremor affected the left quadriceps. On each attempt at motion, pains were felt in the legs. At first the cramps were so severe that all locomotion or even standing was impossible.
At the time he was admitted to the hospital, he reported feeling extremely irritable, had nervous twitching, a tingling sensation in his limbs, recurring war dreams, and a rapid heartbeat. The boundaries of his heart were normal. His lower leg muscles were experiencing tonic spasms and felt stiff like a board. These spasms occurred with every attempt to move and gradually faded away when he was at rest. Passive movements had the same effect. The left quadriceps showed fibrillary tremors. Each time he tried to move, he felt pain in his legs. Initially, the cramps were so intense that he couldn't walk or even stand.
Treatment: Cold-water pack (Priessnitz), hyoscin injections, magnesium sulphate injections (5 to 10 c.c. of ten per cent solution), perineural injections, lumbar spinal analgesia,—all without success. Fibrillary tremors persisted in the quadriceps and in the extensors of the toes. The tonic spasms on increased attempts at motion became combined with clonic twitchings. From the end of November on the patient made attempts to walk with straddling legs, and under considerable vibratory tremor. Picture of severe crampus-neurosis, combined with neurasthenia gravis.
Treatment: Cold-water pack (Priessnitz), hyoscine injections, magnesium sulfate injections (5 to 10 c.c. of ten percent solution), perineural injections, lumbar spinal analgesia—all without success. Fibrillary tremors continued in the quadriceps and in the toe extensors. The tonic spasms during increased attempts at movement became mixed with clonic twitching. From the end of November on, the patient attempted to walk with legs spread apart, and experienced significant vibratory tremors. The picture resembles severe cramp neurosis combined with severe neurasthenia.
Chart 13
SHELL CONCUSSION
SHELL SHOCK
Cause physical from explosives—amnesia for shell episode and for a subsequent period—followed by traumatic neurosis
Physical effects from explosives include memory loss related to the shelling event and for a period afterward, leading to traumatic neurosis.
SHELL HYSTERIA
SHELL PANIC
Shell heard—victims already unstable—rum issue preparatory?—overemotionalism—sensory and motor disorder
Shell heard that the victims, who were already unstable, had a problem with their preparation for the situation—excessive emotions—along with sensory and motor disorders.
SHELL NEURASTHENIA
SHELL ANXIETY DISORDER
Headache, dizziness, insomnia, anorexia, visceral pain—victims, older men
Headache, dizziness, trouble sleeping, loss of appetite, internal pain—victims, older men
After H. P. Wright
After H. P. Wright
(a) Bullet-wound of forearm: Combination of hysterical (brachial) monoplegia, and reflex (physiopathic) disorders. (b) Refrigeration: Combination of hysterical paraplegia and reflex (physiopathic) disorders.
(a) Bullet wound to the forearm: A mix of hysterical (brachial) monoplegia and reflex (physiopathic) disorders. (b) Refrigeration: A mix of hysterical paraplegia and reflex (physiopathic) disorders.
Case 421. (Babinski reflex, 1916.)
The forearm of a soldier was pierced in its lower part by a bullet, which produced no lesion of large nerve trunks or blood vessels. A complete brachial monoplegia followed. Every movement of the different segments of the arm was abolished. The hand and forearm were slightly atrophied, and were of a reddish salmon color. The temperature of the affected hand and forearm was about three or four degrees lower than that on the other side. The sphygmometric oscillations of the forearm were twice as small in the paralyzed limb as in the healthy limb, but the systolic blood pressure was normal. There was a mechanical over-excitability of the muscles, and a slight exaggeration of the bone and tendon reflexes. The paralysis was in part of reflex (physiopathic) nature. On account however, of the completeness of the monoplegia, and the fact that the reflex paralyses as a rule affect only the distal portion of the limb, the diagnosis of hysteria had to be made in addition to the diagnosis of reflex disorder.
The lower part of a soldier's forearm was pierced by a bullet, which didn’t damage any major nerves or blood vessels. This resulted in complete brachial monoplegia. All movement in the different parts of the arm was lost. The hand and forearm were slightly atrophied and had a reddish salmon color. The temperature of the affected hand and forearm was about three to four degrees lower than the other side. The blood pressure oscillations in the forearm were half as much in the paralyzed limb compared to the healthy limb, but the systolic blood pressure was normal. There was mechanical over-excitability in the muscles and a slight increase in bone and tendon reflexes. The paralysis had partially reflex (physiopathic) origins. However, due to the total loss of function in the monoplegia and the fact that reflex paralysis usually only impacts the distal part of the limb, a diagnosis of hysteria was also necessary in addition to the diagnosis of reflex disorder.
As a result of freezing, this patient had also a complete crural paraplegia. He showed vasomotor disorders and hypothermia of both feet, together with mechanical over-excitability of the muscles; and these latter disorders appeared to be of a reflex nature. The paraplegia, however, was of a hysterical nature.
As a result of freezing, this patient also had complete leg paralysis. He showed issues with blood flow and coldness in both feet, along with heightened muscle responsiveness, and these latter issues seemed to be reflexive. However, the paralysis was of a hysterical nature.
Re refrigeration, see Case 309 (Binswanger) of glossolabial spasm.
Re refrigeration, see __A_TAG_PLACEHOLDER_0__ (Binswanger) of glossolabial spasm.
Differential diagnosis of organic (central) monoplegia and reflex (physiopathic) contracture and paralysis. (Babinski-Froment.)
Differential diagnosis of organic (central) monoplegia and reflex (physiopathic) contracture and paralysis. (Babinski-Froment.)
| Organic Monoplegia | Reflex Contracture and Paralysis |
|---|---|
| 1. Paralysis often affects the whole extremity, either arm or leg. | 1. Paralysis almost always partial. In arm paralysis, affects as a rule fingers and hand. The leg is often affected at its origin, and then only partially. |
| 2. After several weeks of flaccid paralysis, as a rule contracture occurs. | 2. Paralysis may remain flaccid for a long time, and frequently coexists with contracture, hypertonicity and hypotonicity of different muscular groups. |
| 3. The upper extremity shows flexion with clawhand. The lower extremity shows contracture of extensors. The patient walks throwing his leg sidewise (Démarche helicopode). | 3. The upper extremity in hypertonic cases often shows the main d’accoucheur, the main en bénitier (holy-water vessel hand), the doigts en tuile (crowded fingers). The lower extremity does not exhibit the sidewise movements. |
| 4. Tendon reflexes, a few weeks after paralysis begins, exaggerated. | 4. Reflex status variable. Hyperreflexia often absent even in hypertonic forms. |
| 5. Babinski sign in crural monoplegia. | 5. Babinski sign absent. The skin reflex may be abolished but may be reproduced on warming the foot. |
Slight bullet wound of hand: Flaccid paralysis with vasomotor and thermic disorder. A case “non-organic” in the ordinary sense and non-hysterical, i.e., reflex or physiopathic.
Slight bullet wound to the hand: Weak paralysis with issues related to blood flow and temperature regulation. A case that's "non-organic" in the usual sense and not hysterical, i.e., reflexive or physiopathic.
Case 422. (Babinski reflex and Froment, 1917.)
Struck by his observations upon the persistence of tendon reflexes in narcosis in a wounded soldier, Babinski continued observations in the same general direction in a case which may be termed briefly one of hypotonia of the extensors of the hand following the passage of a bullet through the arm without nerve trunk lesion.
Struck by his observations on the persistence of tendon reflexes during narcosis in a wounded soldier, Babinski continued his observations in a similar case that can be briefly described as hypotonia of the hand extensors following a bullet passing through the arm without damage to the nerve trunk.
This patient had flaccid paralysis of hand and fingers following wound in second dorsal interosseous space and vasomotor disorder and local hypothermia in the hand. There was a slight diffuse atrophy of the muscles of the hand, forearm, and arm; but this atrophy was not systematized, and there was no R. D. The tendon reflexes of the extremity were preserved. There were no signs of organic disease of the central or peripheral nervous system; that is, in the ordinary sense of these terms.
This patient experienced weak paralysis in the hand and fingers after a wound in the second dorsal interosseous space, along with circulation problems and local coldness in the hand. There was slight overall muscle wasting in the hand, forearm, and arm; however, this wasting was not consistent, and there were no reflex abnormalities. The tendon reflexes in the extremity were intact. There were no signs of any organic diseases affecting the central or peripheral nervous system, at least not in the usual sense of those terms.
Was it a question of hysteria or of simulation?
Was it a case of hysteria or pretending?
Babinski was struck by the following symptoms:
Babinski was affected by the following symptoms:
First, the remarkably intense hypotonia, especially noteworthy in the thumb, a hypotonia quite equal if not superior to that observed in paralysis following marked nerve lesions;
First, the exceptionally severe hypotonia, particularly noticeable in the thumb, is a hypotonia that is just as severe, if not more so, than what is seen in paralysis resulting from significant nerve damage;
Second, mechanical over-excitability of high degree in the muscles of the hand and forearm, with retardation of the muscular response; and
Second, a high level of mechanical over-excitability in the muscles of the hand and forearm, along with a delay in the muscular response; and
Third, electric over-excitability of the muscles, with what Babinski calls “anticipated fusion” of the faradic reactions.
Third, electric over-excitability of the muscles, with what Babinski refers to as “anticipated fusion” of the faradic reactions.
It appears that this patient had been wounded in September, 1914, and that the paralysis had developed five months later. Before the development of this paralysis, there had been simply a meiopragic state.
It seems that this patient was injured in September 1914, and the paralysis appeared five months later. Before this paralysis set in, there was just a mild impairment.
Without perforating the hand, the bullet had remained[593] in the wound, being excised therefrom three months after the trauma.
Without piercing the hand, the bullet had stayed[593] in the wound, being removed three months after the injury.
In January, 1916,—that is, some sixteen months after the injury and eleven months after the recovery of the paralysis,—the vasomotor disorder and the hypothermia, and the faradic, voltaic and mechanical over-excitability of the hand and forearm muscles, were in evidence. Hypotonia was marked, permitting an overflexion of the hand upon the forearm. If the patient moved his forearm, the affected hand would hang and oscillate inertly; likewise in walking, seeming to obey only the laws of physics.
In January 1916—about sixteen months after the injury and eleven months after the paralysis had recovered—the issues with blood flow regulation and low body temperature, along with the excessive sensitivity of the hand and forearm muscles to electrical and mechanical stimuli, were still noticeable. There was significant weakness, leading to an excessive bending of the hand towards the forearm. If the patient moved his forearm, the affected hand would hang limply and swing back and forth; similarly, during walking, it appeared to respond only to the laws of physics.
In May, 1916, the patient was invalided and found to be still in possession of the above-mentioned signs. Similar phenomena have been found in the main figée acrocontracture, and main d’accoucheur, and belong, in the opinion of Babinski, to a group which is neither hysterical nor organic in the ordinary sense of the terms. Vasomotor and thermic phenomena are in the foreground of the picture, and are, in fact, practically constant, though they vary somewhat in degree. They react abnormally to the temperature of the surrounding medium; there is undoubtedly a local perturbation of the vasomotor and heat-regulating mechanism. There is also certain evidence of vascular spasm. The vasomotor and thermic disorders run parallel with the mechanical over-excitability of the muscles and the slowness of the response.
In May 1916, the patient was discharged from care and still showed the previously mentioned signs. Similar phenomena have been observed in the main figée acrocontracture and main d’accoucheur, which, according to Babinski, belong to a group that is neither hysterical nor organic in the usual sense of those terms. Vasomotor and thermal phenomena are prominently featured and are, in fact, nearly constant, although they do vary somewhat in intensity. They react abnormally to the temperature of the surrounding environment; there is definitely a local disturbance in the vasomotor and heat-regulating mechanisms. There is also some evidence of vascular spasm. The vasomotor and thermal disturbances parallel the mechanical over-excitability of the muscles and the delayed response.
Chloroform to demonstrate asymmetry of reflexes.
Chloroform to show the imbalance of reflexes.
Case 423. (Babinski's reflex and Froment, 1917.)
A soldier, 26, sustained, September 22, 1914, a bullet injury of the right calf. There was no fracture, as X-ray showed, but healing was slow, taking no less than three months. The right knee-jerk was a little stronger and a little sharper than the left, but the difference was controversial; and the difference between the two Achilles reflexes was still more doubtful.
A 26-year-old soldier suffered a bullet injury to his right calf on September 22, 1914. The X-ray showed no fracture, but the healing process was slow, taking at least three months. The knee-jerk reflex on the right side was slightly stronger and sharper than on the left, though this difference was debated; and the comparison between the two Achilles reflexes was even more uncertain.
Chloroformed October 10, 1915: As the patient was going to sleep, even before the phase of excitation and motor agitation had passed, the two knee-jerks and left Achilles jerk had disappeared. They grew rapidly less marked before disappearing, and none of the tendon reflexes presented any phase of exaggeration while the patient was going under. At this point anesthesia was arrested. The right Achilles reflex, which had not disappeared, was sharply defined. It was even stronger than in the normal state and polykinetic. During the whole phase of awaking from the chloroform, the right Achilles reflex remained strong and polykinetic, without, however, any ankle clonus. Thus, the difference between the two Achilles reflexes became indisputable; also the right knee-jerk reappeared before the left, and became stronger without any patellar clonus. At this time, the difference between the two knee-jerks was sharp and beyond cavil. This status, in which the knee-jerk and Achilles reflexes were asymmetrical, lasted about ten minutes after anesthesia ceased and lasted a little longer for the knee-jerks than for the Achilles jerks.
Chloroformed October 10, 1915: As the patient was drifting off to sleep, even before the stage of excitement and restlessness had passed, the two knee-jerks and left Achilles reflex disappeared. They quickly became less pronounced before vanishing, and none of the tendon reflexes showed any signs of being heightened while the patient was going under. At this point, anesthesia was stopped. The right Achilles reflex, which had not disappeared, was clearly defined. It was even stronger than in the normal state and showed multiple movements. Throughout the entire process of waking up from the chloroform, the right Achilles reflex remained strong and showed multiple movements, without any ankle clonus. Thus, the difference between the two Achilles reflexes became obvious; also, the right knee-jerk returned before the left and became stronger without any patellar clonus. At this time, the difference between the two knee-jerks was clear and undeniable. This condition, where the knee-jerk and Achilles reflexes were unequal, lasted about ten minutes after anesthesia stopped, with the knee-jerks lasting a bit longer than the Achilles reflexes.
Reflexes under chloroform.
Reflexes under anesthesia.
Case 424. (Babinski reflex and Froment, October, 1915.)
A soldier sustained a clean-cut wound of the supero-external aspect of the right thigh without much destruction of tissue or any adherent scar. He showed marked lameness, September 15, 1915, walking with his right leg extended and the foot in external rotation. There was a slight limitation of the movements of the hip joint in respect to internal rotation and flexion of thigh. The right knee-jerk was a little stronger than the left, and this condition persisted several days. After a few tests, the knee-jerk became even slightly polykinetic. The Achilles jerks were normal and equal. There was no epileptoid trepidation of the foot, and no patella clonus. There was a slight hypothermia of right leg, with ill-defined muscular atrophy. Walking caused pain.
A soldier had a clean cut on the outer upper part of his right thigh, with minimal tissue damage and no noticeable scar. He was noticeably limping on September 15, 1915, walking with his right leg straight and his foot turned outward. There was a slight limitation in the hip joint's ability to rotate internally and flex the thigh. The right knee-jerk reflex was a bit stronger than the left, and this condition lasted several days. After a few tests, the knee-jerk became slightly more active. The Achilles reflexes were normal and equal. There was no shaking of the foot or clonus in the patella. The right leg was slightly cooler, with some unclear muscle wasting. Walking caused pain.
Chloroform anesthesia, September 20, 1915, yielded an exaggeration of the knee-jerks with a suggestion of patella clonus even before the phase in anesthesia of motor excitation had set in. As anesthesia proceeded the exaggeration was rapidly lost on the left side but progressively increased on the right. In the phase of complete muscular resolution, when all the other tendon reflexes (such as the knee-jerk, Achilles jerk on the left side, the radial and olecranon reflexes on the left side) were abolished, the patella clonus on the right side was perfectly distinct and could be elicited either by the usual method or by raising the thigh and letting it fall. On percussion of the patella tendon, a strong polykinetic reflex was obtained; right Achilles jerk preserved; right leg in external rotation. Internal rotation could be passively performed better than in the waking state, but this movement was still limited. As the man was waking from anesthesia, when reflexes were reappearing, there was a suggestion of left patella clonus—right clonus as strong as before. At no time any trepidation of the foot. The patella clonus on the right side lasted an hour after waking, at which time all the reflexes returned to their previous state.
Chloroform anesthesia, September 20, 1915, showed an increase in knee-jerk reflexes with a hint of patellar clonus even before the phase of motor excitement in anesthesia began. As the anesthesia continued, the exaggeration quickly diminished on the left side but progressively increased on the right. In the stage of complete muscle relaxation, when all other tendon reflexes (like the knee-jerk, Achilles reflex on the left side, and the radial and olecranon reflexes on the left side) were absent, the patellar clonus on the right side was clearly present and could be triggered either by the usual method or by lifting the thigh and letting it drop. Tapping the patellar tendon resulted in a strong polykinetic reflex; the right Achilles reflex remained intact; the right leg was externally rotated. Internal rotation could be passively done more easily than when awake, but this movement was still restricted. As the patient was waking up from anesthesia, with reflexes beginning to return, there was a sign of left patellar clonus—right clonus was as strong as before. There was never any tremor in the foot. The right side patellar clonus lasted an hour after waking, at which point all reflexes returned to their normal state.
Reflexes under chloroform.
Reflexes under anesthesia.
Case 425. (Babinski reflex and Froment, October, 1915.)
A soldier sustained a bullet wound, September 22, 1914, in the right calf. There was no fracture, as X-ray showed. Cicatrization was slow and took at least three months. He was examined October 2, 1915, at the Pitié,—not complaining of pains, but lame. There were no pains, limitation of movement, or joint sounds in the hip joint, and X-ray was negative. There was a slight atrophy of the limb, 1.5 c.m. less in circumference on the right. There was a sharply defined local hypothermia of the right leg up to the knee. The right knee-jerk was a little stronger and brisker than the left, yet it was difficult to be sure of this, and there was a still more doubtful difference between the Achilles reflexes.
A soldier got shot in the right calf on September 22, 1914. The X-ray showed no fracture. Healing was slow and took at least three months. He was examined on October 2, 1915, at the Pitié—not complaining of any pain, but he was limping. There were no pains, movement restrictions, or joint noises in the hip joint, and the X-ray came back negative. The limb showed slight atrophy, measuring 1.5 cm less in circumference on the right side. There was noticeably lower temperature in the right leg up to the knee. The right knee-jerk reflex was slightly stronger and more brisk than the left, though it was hard to be certain about this, and there was even more uncertainty regarding the Achilles reflexes.
The man was anesthetized with chloroform, October 10. As he was going to sleep, before the phase of excitement and agitation had ceased, the two knee-jerks had disappeared. At the same time, the left Achilles jerk vanished, followed by the plantar cutaneous reflexes. Anesthesia was then stopped. The right Achilles jerk, which had not disappeared at any time, remained distinct. It was stronger than in the waking state, and polykinetic. During the waking phase, this reflex remained strong and polykinetic, but there was no epileptoid trepidation of the foot. Accordingly, under chloroform, the difference of the two Achilles reflexes had become very sharp. The right knee-jerk reappeared before the left and became stronger, though without patella clonus. This difference was much more striking than in the waking state. This asymmetry of the patella and Achilles reflexes lasted about 10 minutes after anesthesia was stopped, and lasted a little longer for the patella reflexes than for the Achilles reflexes.
The man was put under with chloroform on October 10. As he was drifting off to sleep, before the feelings of excitement and agitation fully went away, the two knee reflexes disappeared. At the same time, the left Achilles reflex also disappeared, followed by the skin reflexes on the bottom of his foot. Anesthesia was then halted. The right Achilles reflex, which had never disappeared, remained clear. It was stronger than when he was awake and showed multiple movements. During the waking phase, this reflex remained strong and showed multiple movements, but there was no sudden foot shaking. Thus, under chloroform, the difference between the two Achilles reflexes became very pronounced. The right knee reflex returned before the left and grew stronger, though there was no knee jerk clonus. This difference was much more noticeable than when he was awake. This asymmetry between the patella and Achilles reflexes lasted about 10 minutes after the anesthesia was stopped, and lasted a little longer for the patella reflexes than for the Achilles reflexes.
Shrapnel wound above clavicle: Brachial monoplegia, partly hysterical, partly organic.
Shrapnel wound above the collarbone: Partial paralysis of the arm, partly hysterical, partly physical.
Case 426. (Babinski reflex and Froment, 1916.)
Babinski speaks of certain symptomatic incompatibilities which emerged in the study of cases of combinations of hysteria, organic nervous disease, and the so-called physiopathic disorders. An example of such an incompatibility might be that of a patient who should, three months after a sudden hemiplegia, show complete or almost complete flaccid paralysis and but slight exaggeration of tendon reflexes—yet the Babinski reflex. Of course, the Babinski reflex would permit a diagnosis of pyramidal tract disease. Yet a sudden intense hemiplegia lasting three months, if it were merely a matter of pyramidal tract disorder, ought to show hyperreflexia of a pronounced degree as well as contracture. An example from the arm is as follows:
Babinski talks about certain symptomatic inconsistencies that came up while studying cases where hysteria, organic nervous disorders, and so-called physiopathic issues were combined. For instance, a patient who experiences sudden hemiplegia should, three months later, display complete or nearly complete flaccid paralysis with only slight exaggeration of tendon reflexes—yet also show the Babinski reflex. Naturally, the presence of the Babinski reflex would indicate the possibility of pyramidal tract disease. However, if a person has sudden severe hemiplegia for three months, and it’s just a pyramidal tract problem, there should be pronounced hyperreflexia and some contracture. Here's an example using the arm:
A soldier got a shrapnel wound in the left supraclavicular region, and had a complete paralysis of the arm, which had lasted more than a month. Electrical examination showed marked reaction of degeneration in the muscles controlled by the musculo-cutaneous nerve, as well as a diminution of electrical excitability in the muscles innervated by radial branches. On the contrary, in the circumflex territory, ulnar and median, electrical excitability was normal. There were no vasomotor disorders. The diagnosis of an association of hysteria and organic disease was made. Babinski affirmed that electrification would effect a partial cure; and in point of fact, the patient, after having submitted to the current for several minutes, was able to use all the muscles whose faradic contractility was normal or almost normal. Thus, he could raise his arm, flex the thumb, flex the fingers, close the hand, and extend the hand and fingers. Flexion of the forearm on the arm was still difficult, since there was, in fact, a reaction of degeneration in the muscles of the anterior region of the arm. The fact that the movements could be partially executed was dependent upon action of the supinator longus.
A soldier suffered a shrapnel wound in the left supraclavicular area and experienced complete paralysis of his arm for over a month. An electrical examination revealed significant signs of muscle degeneration in the muscles controlled by the musculo-cutaneous nerve, along with a decrease in electrical excitability in the muscles served by radial branches. In contrast, the electrical excitability was normal in the circumflex, ulnar, and median nerves. There were no issues with blood vessel regulation. The diagnosis indicated a combination of hysteria and an organic disorder. Babinski stated that electrical stimulation would lead to a partial recovery; in fact, after undergoing treatment with the current for several minutes, the patient was able to use all the muscles that had normal or nearly normal faradic contractility. He could raise his arm, flex his thumb, bend his fingers, close his hand, and extend his hand and fingers. However, flexing the forearm on the arm remained challenging due to ongoing signs of degeneration in the anterior arm muscles. The ability to partially perform these movements relied on the action of the supinator longus.
Gunshot fracture of upper arm; recovery with motor power in five weeks: Six weeks later, Erb’s palsy (plus). Hypothesis: “Reflex paralysis” preferred.
Gunshot fracture of the upper arm; recovery with motor function in five weeks: Six weeks later, Erb’s palsy (plus). Hypothesis: “Reflex paralysis” preferred.
Case 427. (Oppenheimer, January, 1915.)
A reservist, 26, was shot through the middle of the left upper arm, sustaining an oblique fracture of the humerus, August 26. The external wounds healed in a month; the fracture somewhat later. The left arm was at first stiff and motionless, but in five weeks it could again be moved. Pains disappeared with return of motility.
A 26-year-old reservist was shot in the middle of his left upper arm, causing an angled fracture of the humerus, on August 26. The external wounds healed within a month; the fracture took a bit longer. At first, his left arm was stiff and immobile, but after five weeks, he was able to move it again. The pain went away as movement returned.
About the middle of November the arm began to lose power to move again, especially the muscles of the upper arm. November 20, the patient showed atrophic paralysis (left deltoid, biceps, brachialis internus, and supinator longus) suggesting at first glance the appearance of an Erb’s palsy; but the triceps and the adductor of the upper arm were also unable to move and there was a slight paresis in the distal muscles of the extremity. There were no pains or other objective disorders.
About mid-November, the arm started to lose its ability to move again, especially the muscles in the upper arm. On November 20, the patient exhibited atrophic paralysis (left deltoid, biceps, brachialis internus, and supinator longus) that initially resembled Erb’s palsy; however, the triceps and the adductor of the upper arm were also unable to move, and there was slight weakness in the distal muscles of the limb. There were no pains or other observable disorders.
The diagnosis of subacute poliomyelitis was considered. Electric excitability, however, was found to be normal, both faradically and galvanically.
The diagnosis of subacute poliomyelitis was considered. However, electrical excitability was found to be normal, both faradically and galvanically.
When patient walked, the left arm swung helpless without sign of innervation or any tonus. Abduction of the shoulder could also not be performed, though a slight flexion of the forearm shortly began to be demonstrable. If the patient inclined his head to the right, extended his hand at the wrist, and flexed the fingers forcibly, he could then flex the forearm somewhat, and a slight tension of the biceps and supinator longus developed. Sometimes fibrillary tremors developed in deltoid and biceps.
When the patient walked, the left arm swung limply with no sign of nerve function or any muscle tone. The shoulder couldn't be lifted either, but a bit of bending in the forearm started to show. If the patient tilted his head to the right, straightened his hand at the wrist, and forcefully bent his fingers, he was able to flex the forearm a little, and there was slight tightness in the biceps and supinator longus. Occasionally, there were twitching movements in the deltoid and biceps.
Of course a transient peripheral palsy can be produced by pressure of the radial nerve without any change of electrical excitability, but such a change is not associated with atrophy.
Of course, a temporary peripheral palsy can be caused by pressure on the radial nerve without any change in electrical excitability, but this type of change is not linked to atrophy.
Neuritis and poliomyelitis producing an Erb’s palsy without[599] any effect upon the electrical reactions is an hypothesis not to be entertained.
Neuritis and poliomyelitis causing Erb’s palsy without[599] any impact on the electrical responses is a hypothesis that shouldn't be considered.
Accordingly, the hypothesis of psychogenic or hysterical palsy may be set up. Yet an atonic atrophic palsy with loss of tendon reflexes (supinator) is inappropriate. According to Oppenheim, this case falls into the category of the arthrogenic atrophies. A simple muscular atrophy may follow disease of joints and bones. However, such cases have rarely shown a complete palsy, as in Oppenheim’s case.
Accordingly, the idea of psychogenic or hysterical paralysis can be proposed. However, an atonic atrophic paralysis with the loss of tendon reflexes (supinator) is not appropriate. According to Oppenheim, this case fits into the category of arthrogenic atrophies. Simple muscle atrophy can occur due to diseases of the joints and bones. However, such cases have rarely shown a complete paralysis, as in Oppenheim’s case.
In short, we return to the old doctrine of reflex paralysis, conceiving that a stimulus passing from the periphery influences the gray matter in its trophic functions.
In short, we go back to the old idea of reflex paralysis, thinking that a signal moving from the edges affects the gray matter in its nutrient functions.
How much effect had the psyche upon this condition? The patient had stuttered from childhood and had sustained a fracture of the skull at 9, following which his school work, especially mental arithmetic, had been poor. The lack of psychic inhibitions may play some part in the situation, but on the whole, the reflex hypothesis is preferred by Oppenheim, the nerve conceived to be dynamically affected, the muscles organically.
How much impact did the mind have on this condition? The patient had stuttered since childhood and suffered a skull fracture at age 9, after which his school performance, especially in mental math, declined. The absence of psychological barriers might contribute to the situation, but overall, Oppenheim favors the reflex hypothesis, suggesting that the nerves are dynamically affected while the muscles are affected in an organic way.
Paralysis: Hysterical? organic?
Paralysis: Hysterical or organic?
Case 428. (Gougerot and Carpenter, May, 1916.)
A soldier, 20, was wounded May 15, 1915, by a large number of shell fragments, 15 of which struck the right leg, two producing serious injuries,—the one, a penetrating wound of the popliteal space followed by stiffness of the knee, later cured by extraction of the fragments; the other, causing a deep wound at the internal malleolus. The fragment was extracted June 3, but osteomyelitis persisted and a fistulous contraction was developed in January, 1916. There was a slight equinism.
A 20-year-old soldier was injured on May 15, 1915, by numerous shell fragments, 15 of which hit his right leg. Two of those injuries were serious: one was a penetrating wound in the area behind the knee that caused stiffness and was later treated by removing the fragments; the other resulted in a deep wound at the inner ankle. The fragment was removed on June 3, but osteomyelitis continued, and a fistulous contraction formed in January 1916. There was a slight case of equinism.
By contrast with these deep bony lesions of the right leg, on the left side a fragment had struck the dorsum of the left foot at about its middle point, along the extensors of the fourth and fifth toes. The fragment was removed toward the end of June, 1915. The wound closed in a fortnight, leaving a loose 20 mm. scar. The man complained of pains, which he called electrical, in the third and fourth toes, if one bore down on this scar, a symptom suggesting that the dorsal nerves had been injured. Immediately after the wound both legs had been paralyzed, according to the soldier. He had been able only to drag himself along on his shoulders. This indeterminate paralysis lasted three days. It may have been hystero-traumatic, or it may have been a sort of diffuse inhibition. Just after the injury, the left foot was in contracture, which gave place a month later to paralysis. Only the great toe was still able to move a little. In December, 1915, the patient still could extend and flex the toes on the left side very badly, though he could execute movements easily on the right side. There was no stiffness of joints; there were no tendon reflex disorders. There were no trophic vasomotor or secretory disturbances.
In contrast to the severe bony injuries on the right leg, the left side had a fragment that hit the top of the left foot roughly in the middle, along the tendons of the fourth and fifth toes. The fragment was taken out toward the end of June 1915. The wound healed in two weeks, leaving a loose 20 mm scar. The man reported experiencing pains, which he described as electrical, in the third and fourth toes if pressure was applied to the scar, indicating that the dorsal nerves might have been damaged. Right after the injury, both legs were paralyzed, according to the soldier. He could only drag himself on his shoulders. This vague paralysis lasted for three days. It might have been hystero-traumatic, or it could have been a kind of diffuse inhibition. Right after the injury, the left foot was in a state of contracture, which turned into paralysis a month later. Only the big toe still had a bit of movement. As of December 1915, the patient could still barely extend and flex the toes on the left side, while he could move them easily on the right. There was no joint stiffness; there were no issues with tendon reflexes. There were no problems with trophic, vasomotor, or secretory functions.
The diagnosis of hysterical paresis seemed warranted, but electrical examination showed that the troubles were organic. There was an increase in the faradic and galvanic excitability of the external popliteal nerve. The response was more[601] sudden than normal, and there was an increase in faradic and galvanic excitability in the tibialis anticus. There was a decrease of faradic and galvanic excitability in the extensor communis of the toes and in the external peroneus.
The diagnosis of hysterical paresis seemed appropriate, but electrical tests revealed that the issues were actually organic. There was an increase in the faradic and galvanic responsiveness of the external popliteal nerve. The response was more[601] abrupt than usual, and there was also increased faradic and galvanic responsiveness in the tibialis anterior. However, there was a decrease in faradic and galvanic responsiveness in the extensor communis of the toes and in the external peroneus.
Thus, this patient after being wounded in both feet May 15, 1915, paralyzed in both feet for a period of three days, undergoing a contracture of the left foot for a month, giving place to paralysis of foot and toes, with slow improvement from the end of July, 1915, was still in this latter state in March, 1916; though without trophic disorder, he showed faradic and galvanic over-excitability of the external popliteal nerve and of the tibialis anticus, pari passu with diminished electrical excitability for other muscles.
Thus, this patient, after being injured in both feet on May 15, 1915, was paralyzed in both feet for three days, experiencing contracture of the left foot for a month, leading to paralysis of the foot and toes, with slow improvement from the end of July 1915. By March 1916, he was still in this condition; although without any trophic disorder, he showed over-excitability to faradic and galvanic stimulation of the external popliteal nerve and the tibialis anterior, along with reduced electrical excitability in other muscles.
Paralysis: Hysterical? organic?
Paralysis: Hysterical or organic?
Case 429. (Gougerot and Carpenter, May, 1916.)
A man was wounded Oct. 11, 1914, on the back of the right hand. Two hours later, he was attended at the relief post. At this time, his hand was straight, with fingers extended. He said that he could not move his fingers, although there was no pain in them. Three hours after the wound, the hands swelled and the edema spread as far as the middle of the forearm. There was a long suppuration, complicated by lymphangitis. All of the fragments were removed October 26, 1914; healing was complete in three months. The swelling, however, persisted to June, 1915, and when the swelling disappeared, the hand began to show drop-wrist. The wound was sutured between the second and third metacarpals, and the X-ray showed that the bones had not been injured, nor had the nerves of the forearm muscles been touched. The situation was such that the case was catalogued “functional paralysis.”
A man was injured on October 11, 1914, on the back of his right hand. Two hours later, he received treatment at the relief post. At that time, his hand was straight, with his fingers extended. He reported that he couldn’t move his fingers, although there was no pain. Three hours after the injury, his hands swelled, and the swelling spread up to the middle of his forearm. He experienced prolonged suppuration, complicated by lymphangitis. All of the fragments were removed on October 26, 1914, and healing was complete in three months. However, the swelling lasted until June 1915, and when the swelling finally went down, his hand started to show signs of drop-wrist. The wound was sutured between the second and third metacarpals, and X-rays revealed that the bones were unharmed, and the nerves of the forearm muscles were intact. The situation was classified as “functional paralysis.”
October 5, 1915, the hand was still drooping, fingers extended, and middle finger and ring finger trembling. A slight stiffness of wrist and fingers did not interfere with movements. Extension of the wrist could be made very slightly above horizontal. Flexion was not quite complete, nor were adduction or abduction. Extension of the fingers could be performed normally, as well as that of the thumb, but flexion was not quite complete. There was a slight palmar retraction. Such were the movements that could be produced electrically. Voluntarily, flexion of the wrist was good, abduction and adduction incomplete; extension could not be executed to the horizontal position. There was a tendency to flexion of the ring finger. When the patient tried to flex the middle and index fingers, these fingers trembled but did not flex. Weak extension and abduction of the thumb but without opposition could be voluntarily performed; adduction good; flexion of the first phalanx, weak; of second phalanx, better. Slight muscular atrophy of the forearm,[603] which was one centimeter less in circumference than the left. The hand was subject to a general atrophy; the skin reddish and moist. The X-ray showed a decalcification of all the bones of the hand and wrist; trophic disturbance of the small carpal bones although the trauma had affected only the second interosseous space. No joint lesions or periosteal thicknesses were found by X-ray. There was a slight hypesthesia of the palmar surface of the middle finger and of the index finger. The patient complained of sharp transient pains in hand and fingers.
On October 5, 1915, the hand was still drooping, with fingers extended, and the middle and ring fingers trembling. There was slight stiffness in the wrist and fingers, but it didn’t interfere with movement. The wrist could be extended just slightly above horizontal. Flexion wasn’t quite complete, nor were adduction or abduction. The fingers could extend normally, as could the thumb, but flexion wasn’t fully complete. There was slight retraction of the palm. These were the movements that could be triggered electrically. Voluntarily, wrist flexion was good, but abduction and adduction were incomplete; extension couldn't reach horizontal. There was a tendency for the ring finger to flex. When the patient attempted to flex the middle and index fingers, those fingers trembled but didn’t flex. There was weak extension and abduction of the thumb, but no opposition could be voluntarily performed; adduction was good; flexion of the first phalanx was weak, while for the second phalanx, it was better. There was slight muscular atrophy in the forearm, which was one centimeter less in circumference than the left one. The hand showed general atrophy; the skin was reddish and moist. The X-ray revealed decalcification of all the bones in the hand and wrist, with trophic disturbance of the small carpal bones, even though the trauma had only affected the second interosseous space. No joint lesions or periosteal thickening were found on the X-ray. There was slight hypesthesia on the palmar surface of the middle and index fingers. The patient complained of sharp, transient pains in the hand and fingers.
In this case, therefore, a wound of the back of the hand produced an immediate inhibition of muscular action in the forearm, a rapid edema of the hand and arm, lasting for eight months and followed by reflex disorders.
In this case, a wound on the back of the hand immediately caused a decrease in muscle function in the forearm, led to quick swelling in the hand and arm that lasted for eight months, and was followed by reflex issues.
There was a considerable diminution in faradic excitability of the flexor brevis of the thumb, the anterior cubital, the flexor brevis minimi digiti, and of the dorsal interossei, and slighter evidence of diminution of galvanic excitability in some of the muscles.
There was a significant decrease in the faradic excitability of the thumb's flexor brevis, the anterior cubital, the flexor brevis of the little finger, and the dorsal interossei, along with some minor evidence of reduced galvanic excitability in a few of the muscles.
Sollier is said to have been the first to remark trophic bone disorders in cases of neuropathic contracture.
Sollier is believed to be the first to note bone disorders related to nutrition in cases of nerve-related contracture.
Re bone changes, Babinski enumerates trophic changes in the tissue of bones and joints amongst objective signs that permit us to distinguish the reflex or physiopathic disorders from the hysterical or pithiatic disorders. Objective signs of this group (indicators of reflex or physiopathic disorders) are: (a) Well-marked and persistent vasomotor and thermic disorder; (b) alterations of muscular tone (either hypotonus, hypertonus, or a combination of the two); (c) increase in the mechanical excitability of the muscles and sometimes nerves; (d) quantitative changes in the electrical excitability of the muscles, but without R. D.; (e) muscular atrophy and atrophy of skin, bones, and joints. For cases of this nature, see especially Cases 431 and 432 of Delherm.
Re bone changes, Babinski lists the tissue changes in bones and joints among the objective signs that allow us to differentiate reflex or physiopathic disorders from hysterical or pithiatic disorders. The objective signs in this category (indicators of reflex or physiopathic disorders) include: (a) prominent and ongoing vasomotor and thermal disorders; (b) changes in muscle tone (whether low tone, high tone, or a mix of both); (c) increased mechanical excitability of muscles and sometimes nerves; (d) measurable changes in the electrical excitability of muscles, but without R. D.; (e) muscle atrophy and atrophy of skin, bones, and joints. For cases of this kind, see especially Cases 431 and 432 of Delherm.
Paralysis: Hysterical? organic?
Paralysis: Psychogenic? Physical?
Case 430. (Gougerot and Carpenter, May, 1916.)
A man, 22, was wounded September 17, 1914, in the left hand, the bullet passing from the lower part of the fourth interosseous space out through the palmar face. The bones were not injured, and it was evident that only a few nerve filaments could have been injured; but he had a paralysis extending far beyond this region, which increased little by little from November, 1914, to August, 1915. Babinski, examining him in November, 1914, had made the diagnosis of psychic paresis of the extensors with diminution of electric excitability, with a very slight slowing of the contraction of the last two interossei and the hypothenar eminence, connected with lesion of the branches of the ulnar nerve. The disorder spread to the flexors of the fingers and the thumb muscles. The fifth finger was flexed at rest; there was no stiffness of joint or tendon retraction. The extensors and flexors of all the fingers and the thumb, and the abductor of the thumb showed paresis. The thumb was able to oppose; the hands were cyanotic. Augmentation of these phenomena in a period of months, their bizarre distribution, and the preservation of the opposing power of the thumb suggested a hystero-organic disease, and Babinski’s notes read, “Partial and incomplete paralysis of the ulnar nerve, attacking slightly the hypothenar eminence and the last two interossei; psychic paresis of the extensors and flexors of the fingers and thumb and of the abductors of the thumb.” Electrical examination showed, however, that there was not only electrical disorder of the common extensors of the fingers, the extensor proprius of the index and of the ring fingers, of the long and short extensors of the thumb, but also there was a considerable diminution to faradic and galvanic reaction in extensor ossis metacarpi pollicis, the radials, the supinator longus, the pronator teres, the large and small palmar, the common and superficial flexors of the fingers, the muscles of the thenar eminence, the anterior ulnar, and the[605] anterior biceps and brachial. In short, there was an irradiation of seemingly organic phenomena in the domain of the radial, median, and the non-injured part of the cubital distribution, as well as in the distribution of the musculo-cutaneous. Apparently, organic paralytic disorder had spread even to the biceps and had increased over a period of many months after the wound had healed.
A 22-year-old man was injured on September 17, 1914, in his left hand, with the bullet entering the lower part of the fourth interosseous space and exiting through the palm. The bones were unharmed, and it seemed that only a few nerve fibers might have been affected; however, he experienced paralysis that gradually spread from November 1914 to August 1915. Babinski, who saw him in November 1914, diagnosed him with psychic paresis of the extensors, along with reduced electrical excitability, and a slight delay in the contraction of the last two interossei and the hypothenar eminence, which were linked to damage to the branches of the ulnar nerve. The issue extended to the finger flexors and the thumb muscles. The fifth finger was flexed while at rest, with no joint stiffness or tendon retraction. The extensors and flexors of all the fingers and thumb, as well as the abductor of the thumb, showed weakness. The thumb could still oppose; his hands appeared cyanotic. The worsening of these symptoms over several months, their unusual distribution, and the preservation of the thumb's opposing function suggested a hystero-organic disease. Babinski noted, "Partial and incomplete paralysis of the ulnar nerve, slightly affecting the hypothenar eminence and the last two interossei; psychic paresis of the extensors and flexors of the fingers and thumb as well as the abductors of the thumb." However, electrical tests revealed that there was not only an electrical disorder in the common extensors of the fingers, the extensor proprius of the index and ring fingers, and the long and short extensors of the thumb, but also a significant decrease in faradic and galvanic reactions in the extensor ossis metacarpi pollicis, the radial muscles, the supinator longus, the pronator teres, the large and small palmar muscles, the common and superficial flexors of the fingers, the thenar eminence muscles, the anterior ulnar, and the anterior biceps and brachial. In short, organic symptoms seemed to radiate into the radial, median, and unaffected parts of the ulnar distribution, as well as into the distribution of the musculocutaneous nerve. It appeared that an organic paralytic disorder had spread to the biceps and had worsened over many months after the wound healed.
Re what he terms organo-hysterical association, Babinski proposes to distinguish it from hystero-organic association. In Babinski’s organo-hysterical association, the organic symptoms are preceded by hysterical symptoms. These cases of organo-hysterical association,—e.g., a case in which a hysterical monoplegia is followed by a musculospiral crutch paralysis,—are one of the mainstays of the proof that hysteria and simulation cannot be confounded. Babinski concedes that he has sometimes said that hysteria was a sort of semi-simulation; yet a semi-simulation is not a simulation.
Regarding what he calls organo-hysterical association, Babinski suggests differentiating it from hystero-organic association. In Babinski’s organo-hysterical association, the organic symptoms occur after hysterical symptoms. These cases of organo-hysterical association—for example, a case where hysterical monoplegia is followed by musculospiral crutch paralysis—are one of the key pieces of evidence that demonstrate that hysteria and simulation can’t be mixed up. Babinski acknowledges that he has sometimes claimed that hysteria is a kind of semi-simulation; however, a semi-simulation is not the same as a simulation.
As for Babinski’s hystero-organic association, we here deal with cases of organic paralysis or contracture in which the fundamental disorder is organic, and the psychic disorder is grafted upon it. Both the fundamentally organic and the fundamentally hysterical associations are instances, according to Babinski’s phrase, of symptomatic incompatibilities. In such instances, the hysterical part of the disorder, whether grafted or original, is dissolved by psychotherapy. There is a third group of symptomatic incompatibilities, namely, the hystero-reflex associations, in which, e.g., a hysterical gait is combined with vasomotor and thermal disturbances. There may even be combinations of all three types of disease, namely, the type of structural disease, of vasomotor disorder, and of hysteria, in what would then be termed a hystero-reflex-organic association.
As for Babinski’s hystero-organic association, we are looking at cases of organic paralysis or contractures where the main issue is organic, and the psychological issue is added on. Both fundamentally organic and fundamentally hysterical associations are examples, based on Babinski’s terminology, of symptomatic incompatibilities. In these cases, the hysterical component of the disorder, whether it is a result of the underlying issue or present from the beginning, can be resolved through psychotherapy. There is also a third group of symptomatic incompatibilities, which includes hystero-reflex associations, where, for example, a hysterical gait is accompanied by vasomotor and thermal disturbances. It is also possible to have combinations of all three types of disorders: structural disease, vasomotor disorder, and hysteria, which would then be referred to as a hystero-reflex-organic association.
Wound of toes—Wound of arm: Reflex or physiopathic paralyses, diagnosis and treatment.
Wound of toes—Wound of arm: Reflex or physiopathic paralysis, diagnosis and treatment.
Cases 431 and 432. (Delherm, September, 1916.)
A soldier was wounded in the soft parts of the last two toes and in the furrow between toes on the left side, September 15, 1914, arriving in the Central Physiotherapeutic Service of the 17th Army Region, December 27, 1915, left foot in varus, with marked contracture of tibialis anticus, though passive movements of flexion, extension, adduction and abduction were well performed. There was a slight atrophy of the leg (33 cm. left to 34 cm. right). The scar was a little painful, and there was a slight degree of hypesthesia of foot and lower leg. The foot was cold and cyanotic; the reflexes were normal. An electric examination in the region of the external popliteal branch of the sciatic nerve showed that there was no electrical disorder either faradic or voltaic.
A soldier was injured in the soft tissue of his last two toes and in the space between those toes on the left side on September 15, 1914. He arrived at the Central Physiotherapeutic Service of the 17th Army Region on December 27, 1915, with his left foot turning inward, along with noticeable tightening of the tibialis anterior muscle, although he could move his foot well in flexion, extension, adduction, and abduction. There was slight atrophy of the leg (33 cm. left to 34 cm. right). The scar was somewhat painful, and there was a slight loss of feeling in the foot and lower leg. The foot felt cold and appeared bluish; the reflexes were normal. An electrical examination around the external popliteal branch of the sciatic nerve showed no electrical issues, whether faradic or voltaic.
Another case was wounded in the right arm by a shell fragment September 7, 1914, and showed two scars above the epitrochlea and along the internal border of the triceps. Examination December 30 showed a normal elbow movement, pronation and supination, with slight flexion in repose of the palm of the hand and the fingers. Active flexion movements of the fingers could be performed only imperfectly, and the finger pad could only be brought within three fingers breadths of the palm, despite the greatest effort on the part of the patient. Minute passive movements were entirely possible. The fifth finger could not be abducted and both abduction and adduction of the third and fourth finger could not be made on account of the nerve lesion. The thumb was in a condition of contracture which placed it in abduction in front of the index finger, and the thumb could not oppose. Passive movements, on the other hand, were entirely possible. The hand was flexed upon the forearm through hypertonia of the flexors, which could be easily overcome with slight but distinct resistance. The hand was in the position of a radial paralysis. There was a slight degree[607] of muscular atrophy. Tendon reflexes were normal. Electric examination showed that stimulation of the ulnar nerve at the elbow was unable to produce flexion of the last two fingers or any movement in the hypothenar eminence, of which the muscles were also not excitable. The interossei could, however, be made to contract. The median and radial nerves were normal electrically. The above examinations were with the faradic current.
Another case involved an injury to the right arm from a shell fragment on September 7, 1914, leaving two scars above the elbow and along the inner edge of the triceps. An examination on December 30 revealed normal elbow movement, pronation and supination, with slight flexion at rest in the palm and fingers. The patient could only perform active flexion movements of the fingers imperfectly, with the finger pad able to come within three fingers' breadth of the palm, despite their best efforts. Minute passive movements were completely possible. The fifth finger couldn't be moved away from the hand, and both movements of the third and fourth fingers could not be done due to nerve damage. The thumb was contracted, positioned in abduction in front of the index finger, and couldn't oppose. However, passive movements were fully possible. The hand was flexed onto the forearm due to increased tone in the flexors, which could be overcome with slight but noticeable resistance. The hand was in a position consistent with radial paralysis. There was a slight amount of muscular atrophy. The tendon reflexes were normal. Electric testing showed that stimulating the ulnar nerve at the elbow couldn't produce flexion in the last two fingers or any movement in the muscle mass of the little finger, which also couldn't be excited. However, the interossei muscles could be made to contract. The median and radial nerves showed normal electrical activity. The examinations above were conducted using the faradic current.
With the galvanic current the ulnar nerve proved unexcitable at the elbow, and the muscles of the hypothenar eminence contracted more slowly. The median and radial nerves and their muscles were electrically normal.
With the electric current, the ulnar nerve showed no response at the elbow, and the muscles of the hypothenar eminence contracted more slowly. The median and radial nerves and their muscles were electrically normal.
In short, there was a complete R. D. of the hypothenar and partial R. D. of the interossei as a result of the lesion of the ulnar nerve. There was nothing abnormal in the other nerves or muscles of the arm. The attitude of radial pseudoparalysis is due to the contracture of the muscles of the thenar eminence.
In short, there was a complete relaxation of the hypothenar muscles and partial relaxation of the interossei due to the ulnar nerve injury. The other nerves and muscles in the arm were normal. The position of radial pseudoparalysis is caused by the tightening of the muscles in the thenar eminence.
As to therapy, the general movements of flexion of the fingers, thumb and hand yielded a marked improvement, but such results cannot be expected in like cases unless a physician or experienced masseur treats the case. Babinski and Froment have tried thermotherapy and diathermy in these cases, finding that the paralysis diminishes and becomes partial if the limb is warm, although it is important that it should not become too warm. Sometimes a few treatments with diathermy will produce movements in a case of long standing paralysis. Babinski and Froment counsel not only diathermy, but a general motor reëducation. The idea of the diathermy is that the deeply penetrating heat affects blood vessels and muscles, bringing about a vasodilatation or even a direct addition of needed calories. In like manner, galvanism, light baths, or simple baths in combination, and with diathermy, especially with the diathermy, act favorably. Casts and apparatus have also proved without avail, as well as faradic or galvanic reëducation.
In therapy, general movements like bending the fingers, thumb, and hand showed significant improvement, but similar results can't be expected in other cases without treatment from a doctor or an experienced masseur. Babinski and Froment have used heat therapy and diathermy in these situations, discovering that paralysis lessens and becomes partial when the limb is warm, though it’s crucial that it doesn’t get too hot. Sometimes just a few diathermy sessions can trigger movement in cases of long-standing paralysis. Babinski and Froment recommend not only diathermy but also a comprehensive motor retraining. The purpose of diathermy is for the deeply penetrating heat to affect blood vessels and muscles, promoting vasodilation or even directly providing needed calories. Similarly, methods like galvanism, light baths, or simple baths, especially combined with diathermy, have positive effects. However, casts and devices have been ineffective, as well as faradic or galvanic retraining.
The above two cases show how in one instance there may be no electrical change and in another instance a slight one. In these cases, reflex hypertonic contracture, hypotonic paralysis,[608] vasomotor disorder, decalcification of the skeleton (X-ray), mechanical overexcitability of muscles, unmodified tendon reflexes (except elective exaggeration of reflex under anesthesia, e.g., a persistent unilateral patellar clonus when all other reflexes have been abolished), and disorders of electrical excitation are enumerated by Babinski and Froment.
The two cases above demonstrate how, in one situation, there may be no electrical change, while in another, there might be a slight one. In these instances, Babinski and Froment list reflex hypertonic contracture, hypotonic paralysis,[608] vasomotor disorders, decalcification of the skeleton (X-ray), mechanical overexcitability of muscles, unchanged tendon reflexes (except for the selective exaggeration of reflexes under anesthesia, e.g., a persistent unilateral patellar clonus when all other reflexes have been abolished), and electrical excitation disorders.
Delherm sums up the electrical disorders as follows: Muscle faradized:
Delherm summarizes the electrical disorders like this: Muscle faradized:
(a) No change.
No change.
(b) Subexcitability.
Subexcitability.
(c) Overexcitability.
Overexcitement.
(d) Diminished contractility to faradism, associated with increased contractility by galvanism (Charpentier).
(d) Reduced contractility to faradism, linked with enhanced contractility by galvanism (Charpentier).
(e) Anticipated fusion of shocks (Babinski and Froment).
(e) Expected combination of reactions (Babinski and Froment).
(f) Slow contraction and decontraction on faradism (Charpentier).
(f) Gradual tightening and loosening on faradism (Charpentier).
(g) Rapid exhaustion of rhythmic faradic contraction with metronome.
(g) Quick fatigue of rhythmic faradic contraction with a metronome.
Muscle galvanized:
Muscle activated:
(a) No change.
No change.
(b) Subexcitability.
Subexcitability.
(c) Overexcitability.
Overexcitability.
(d) Suddenness of galvanic contraction with subexcitability.
(d) Sudden galvanic contraction with reduced excitability.
Re decalcification and osteo-articular changes, Babinski points out that the reflex or physiopathic phenomena run historically back to John Hunter, Charcot, and Vulpian. Charcot and Vulpian called especial attention to the peculiar amyotrophy and paralysis which occurred in joint disease, and upon the lack of parallelism betwixt the intensity of the joint disease and the severity of the paralysis or atrophy. The atrophy was without R. D.
Regarding decalcification and bone and joint changes, Babinski points out that the reflex or physiological phenomena date back to John Hunter, Charcot, and Vulpian. Charcot and Vulpian highlighted the unusual muscle wasting and paralysis that happened in joint disease, as well as the lack of correlation between the severity of the joint disease and the degree of paralysis or atrophy. The atrophy occurred without R. D.
Shell-shock: Functional blindness (monosymptomatic).
Shell shock: Functional blindness (monosymptomatic).
Case 433. (Crouzon syndrome, January, 1915.)
A shell burst above the head of a sergeant in a battle near Neuf château, August 22, 1914. The man was kneeling at the time; felt a terrible shock, slipped prone, lost consciousness and woke in the evening blind. Next day he could hardly distinguish light from dark. Yet the light reflexes were normal; the fundus was normal.
A shell exploded above a sergeant's head during a battle near Neufchâteau on August 22, 1914. He was kneeling at the time, felt a massive shock, fell to the ground, lost consciousness, and woke up in the evening unable to see. The next day, he could barely tell light from darkness. Still, his light reflexes were normal, and the eye examination was typical.
This Crouzon calls the symptomatic triad for functional nerve blindness of Dieulafoy. There have been similar cases following eclipse of the sun and nervous shock. The eclipse cases suggest that the bright flash might have something to do with the sudden blindness (yet blindness has appeared in cases in which the shell burst behind the patient).
This Crouzon refers to the symptomatic triad for the functional nerve blindness of Dieulafoy. There have been similar cases occurring after a solar eclipse and due to nervous shock. The eclipse cases indicate that the bright flash could be related to the sudden onset of blindness (though blindness has also occurred in situations where the shell burst behind the patient).
The diagnosis of temporary blindness, with a prognosis of early recovery, was made. The neurological examination was normal.
The diagnosis of temporary blindness was made, with a prognosis of quick recovery. The neurological exam was normal.
For its suggestive effect, glycerophosphate injections and progressive reëducative measures were adopted. The patient was shown that he could see, first, the contour of objects, then details and colors, then large letters and later small letters. In a month the blindness was almost well. Five months afterwards there was still a certain haze over the field of vision and a slight difficulty in distinguishing certain colors.
For its suggestive effect, glycerophosphate injections and progressive rehabilitation measures were used. The patient was shown that he could initially see the outline of objects, then details and colors, then large letters, and later small letters. After a month, the blindness was almost completely resolved. Five months later, there was still a slight haze over his field of vision and some difficulty in distinguishing certain colors.
Jousset states that aside from visual alterations as the result of cranial trauma, and aside from various transitory amblyopias such as scintillating scotoma, the main varieties of amblyopia are:
Jousset states that besides visual changes caused by head injuries, and apart from various temporary amblyopias like scintillating scotoma, the main types of amblyopia are:
First, Congenital amblyopia.
First, Lazy eye.
Second, Amblyopia due to cerebral intoxication.
Second, Amblyopia caused by brain poisoning.
Third, Retrobulbar neuritis and toxic amblyopia.
Third, retrobulbar neuritis and toxic amblyopia.
Fourth, Amblyopia ex anopsia.
Fourth, Amblyopia from disuse.
Fifth, Hysterical amblyopia.
Fifth, hysterical amblyopia.
The most frequent amblyopias among the soldiers are[610] exanopsia. Aside from a few amblyopias caused by prolonged occlusion of the eyelids, ptosis, or blepharospasm, the most frequent are due to opacities, ametropia, and strabismus. The hysterical amblyopias are, as a rule, associated with blepharospasm due to intense photophobia, and are sometimes associated with constant lacrimation. Vision at a distance is poor. The patient succeeds in reading but shows an asthenopia of fatigue. The cornea and the conjunctiva are anesthetic, and sometimes the eyelids also,—the so-called anesthesia en lunettes. The pupils are large but react properly. The patient complains of many species of disorder; loss of the sense of the third proportion, micropsia, megalopsia, diplopia, erythropsia, diplopia in two colors, inverted image, hemierythropsia, rotatory amblyopia. There is concentrated limitation of visual fields, exaggerated by fatigue and by intense light; reduced in dim light or when the patient is provided with smoked glasses; enlarged upon the instillation of atropin or with convex glasses. As a rule, with unilateral amblyopia, the functional disorders start in binocular vision. Practically the most important diagnostic feature is the anesthesia, since this cannot be readily simulated. Sometimes corneal anesthesia is found in non-hysterical persons, who may perhaps be regarded as potential hysterics.
The most common types of amblyopia among soldiers are[610]exanopsia. Other than a few cases caused by prolonged eyelid closure, ptosis, or blepharospasm, the most frequent causes are opacities, ametropia, and strabismus. Hysterical amblyopias are usually linked to blepharospasm due to severe photophobia, and they are sometimes accompanied by constant tearing. Distances appear blurry. The patient can read but experiences eye strain. The cornea and conjunctiva are numb, and sometimes the eyelids are too—referred to as anesthesia en lunettes. The pupils are enlarged but react normally. The patient reports various issues, including loss of the sense of proportion, micropsia, megalopsia, diplopia, erythropsia, diplopia in two colors, inverted images, hemierythropsia, and rotatory amblyopia. There is a concentrated limitation of visual fields, made worse by fatigue and bright light; reduced in dim light or when the patient wears smoked glasses; and expanded with atropine drops or convex glasses. Typically, with unilateral amblyopia, functional disorders begin with binocular vision. The most crucial diagnostic feature is the anesthesia, as this is not easily faked. Occasionally, corneal anesthesia may be found in non-hysterical individuals, who could potentially be seen as latent hysterics.
Retrobulbar neuritis (nitrophenol).
Retrobulbar neuritis (nitrophenol).
Case 434. (Sollier and Jousset, April, 1917.)
A soldier of the 54th Artillery entered hospital 45, November 4, 1916. He had had a slight paralysis of the left brachial plexus in 1913, following a shoulder dislocation, but the only relic of this when the war began was a deltoid paresis. He had been working from August 13, 1915, at the factory in Saint-Fons, and was as yellow as the majority of the workers there. He had never shown xanthopsia.
A soldier from the 54th Artillery was admitted to hospital 45 on November 4, 1916. He had experienced mild paralysis of the left brachial plexus in 1913, after a shoulder dislocation, but the only lasting effect by the time the war started was weakness in the deltoid muscle. Since August 13, 1915, he had been working at the factory in Saint-Fons and had a complexion like many of the other workers there. He had never exhibited signs of xanthopsia.
The first symptoms of his left brachial plexus neuritis had begun six months before, after 9 months’ work in the factory, and showed themselves in an increase of the deltoid paresis, with pains in the hand and forearm, and cramps of the hand, interfering with work, formication in the right hand and in the feet, diminution of visual peculiarity (objects forgotten and reading difficult). It was only in November that he got perturbed about these difficulties, which had begun in May. There was a paralysis of the levators and rotators of the left shoulder, with a slight atrophy of the deltoid and of the supra- and infraspinatus muscles. The arm could be extended almost to the horizontal with difficulty. There was one centimeter atrophy. The forearm and hand were not atrophic but slightly weak. There was an anesthesia of the shoulder-joint region, and of the outer surface of the arm; a hypesthesia of the posterior surface of the forearm and dorsal surface of the hand and fingers; tendon and periosteal reflexes normal. Sometimes the hand would contract firmly and could be opened only by the aid of the other hand. The nerve trunks of the axilla, upper arm, and forearm, were painful on pressure, especially on the left side, and the ulnar nerve was thickened and rolled under the finger. The knee-jerk and Achilles jerk were abolished on the right; plantar reflex diminished; right posterior tibial nerve painful on pressure, and its territory was hypesthetic. There were cramps in the feet.
The first signs of his left brachial plexus neuritis began six months ago, after nine months of working in the factory. He experienced increased weakness in his deltoid muscle, along with pain in his hand and forearm, and cramps in his hand that affected his work. He also felt tingling in his right hand and feet, and had trouble with his vision, finding it hard to read and often forgetting objects. It wasn't until November that he became concerned about these issues that started in May. He had paralysis of the muscles that lift and rotate his left shoulder, with some muscle wasting in the deltoid and supraspinatus and infraspinatus muscles. He could extend his arm almost to horizontal, but it was difficult. There was a one-centimeter muscle wasting. His forearm and hand were not wasted but were slightly weak. He had a loss of sensation around the shoulder joint and the outer surface of the arm, a decreased sensitivity on the back of his forearm and the tops of his hand and fingers; his tendon and bone reflexes were normal. Sometimes his hand would tightly contract and could only be opened with help from the other hand. The nerves in his armpit, upper arm, and forearm were painful to touch, especially on the left side, and the ulnar nerve was swollen and could be felt distinctly. His knee-jerk and Achilles reflexes were absent on the right; his plantar reflex was reduced; the right posterior tibial nerve was painful to pressure, and the area it affected had decreased sensitivity. He also had cramps in his feet.
Gymnastics and electrotherapy and rest reduced these phenomena. The eye grounds were normal; there was a[612] paresis of accommodation, and an absolute blindness to green, with retraction of fields to 15 degrees in the right eye, and 20 on the left. There later developed a slight edematous neuritis of the nerve, corresponding to the evolution of a chronic retrobulbar neuritis of toxic origin.
Gymnastics, electrotherapy, and rest lowered these issues. The eye exams were normal; there was a[612] paralysis of accommodation, and complete blindness to green, with the visual fields retracted to 15 degrees in the right eye and 20 degrees in the left. Later on, a slight swollen neuritis of the optic nerve developed, aligning with the progression of a chronic retrobulbar neuritis caused by toxicity.
It is the chronic retrobulbar neuritis which is typical of the so-called nitrophenol neuritis, developing in soldiers employed in making explosives. The above case is accordingly exceptional in its association of a severe peripheral neuritis with the optic neuritis. Typically, after six months to a year in the factory, the cramps and formication of the legs are felt, and the gradual diminution of vision with transient blindness, finally leading to inability to read, sets in. The green blindness, the accommodative paresis, and diminution of central vision, the concentric contraction of the visual fields, are the usual story. At first the eye grounds are normal; there is then an edematous neuritis, and finally a white atrophy. According to Sollier, the accommodative paresis is like that in post-diphtheritic paralysis—a disease due to cerebral cortex intoxication. In fact, the photomotor reflex is normal, and what we have is an inversion of the Argyll-Robertson sign. These symptoms are those of retrobulbar neuritis, of nicotino-ethylic origin, and it may be thought that the melinite was simply acting by creating a soil for alcoholic intoxication, but none of the patients examined has been alcoholic, nor has any been permitted to smoke in the factory. The injurious agent is probably a body in the nitrophenol series, perhaps dinitrochlorobenzol, but whether this substance is absorbed through the skin, inhaled, ingested from the hands, or by all three routes, is doubtful. These workers are often cyanotic while at work because the nitre products produce vasodilatation. Possibly this dilatation of vessels has something to do with the neuritis. The workmen will not use the spectacles and antitoxic masks given them, and even do not use the rubber gloves constantly. In some factories only, a liter of milk is given as counterpoison, every day.
It is the chronic retrobulbar neuritis that's typical of the so-called nitrophenol neuritis, which develops in soldiers involved in making explosives. The case described above is unusual because it combines severe peripheral neuritis with optic neuritis. Usually, after six months to a year in the factory, employees start to experience cramps and tingling in their legs, along with a gradual loss of vision and temporary blindness, eventually leading to an inability to read. Symptoms like green blindness, accommodative paresis, reduced central vision, and a narrowing of the visual fields are common. Initially, the eye examinations look normal; then there’s edematous neuritis, and eventually, white atrophy. According to Sollier, the accommodative paresis resembles that seen in post-diphtheritic paralysis, a condition caused by intoxication of the cerebral cortex. In fact, the photomotor reflex remains normal, and what we see is an inversion of the Argyll-Robertson sign. These symptoms are indicative of retrobulbar neuritis of nicotino-ethylic origin, and it might be thought that the melinite is simply facilitating alcoholic intoxication, but none of the patients examined have been alcoholics, nor have they been allowed to smoke in the factory. The harmful agent is likely something from the nitrophenol series, possibly dinitrochlorobenzene, but it’s unclear whether this substance is absorbed through the skin, inhaled, or ingested via hands, or if all three routes are involved. These workers often show cyanosis while working because the nitre products cause blood vessels to dilate. This vascular dilatation might have something to do with the neuritis. The workers refuse to use the glasses and antitoxic masks provided, and they often don’t consistently wear rubber gloves. In some factories, workers are given a liter of milk daily as a counterpoison.
Slight wound of occiput: Ophthalmoplegia externa, influencible, however, by tests and replaced by spasmodic convergence of globes with myosis; hysterical stigmata and convulsions.
Slight wound to the back of the head: External ophthalmoplegia, which can be influenced by tests and is replaced by spasmodic convergence of the eyes with miosis; signs of hysteria and convulsions.
Case 435. (Westphal, September, 1915.)
A German volunteer, 20, was slightly wounded in the occiput by revolver-shot at Ypres. Then followed headaches, vertigo, and complaints of pains in the eyes such that he could not open them or see sidewise. May 5, 1915, he showed a picture of an ophthalmoplegia externa: complete immobility of the two bulbi, lively blepharoclonus, rapidly passing into blepharospasm, photophobia. The visual field for white was practically limited to the fixation point. Central scotoma for all colors. Otherwise normal.
A 20-year-old German volunteer was slightly injured in the back of the head by a gunshot at Ypres. After that, he experienced headaches, dizziness, and pain in his eyes to the point where he couldn’t open them or see sideways. On May 5, 1915, he exhibited symptoms of external ophthalmoplegia: complete immobility of both eyes, intense eye twitching that quickly escalated into eye spasms, and sensitivity to light. His visual field for white was nearly limited to the fixation point, with a central blind spot for all colors. Everything else was normal.
On further examination, the apparently immobile bulbi were found to pass into convergence upon request to look to the right or left. Thereafter, this position of convergence was assumed if any test made by a strong light, such as that of a pocket flash, was used. The pupils contracted to the maximum during this assumption of the convergent position of the globes, and no further light reaction could be observed. The convergence gradually passed off when the light was removed. The appearance of bilateral external ophthalmoplegia had disappeared.
Upon further examination, the seemingly immobile pupils were found to converge when asked to look to the right or left. After that, this converged position was maintained if any test used strong light, like that from a pocket flashlight. The pupils contracted fully during this converged state of the eyes, and no further light reaction could be observed. The convergence slowly subsided when the light was taken away. The signs of bilateral external ophthalmoplegia had vanished.
If the patient was requested to follow a finger moved to one side, the globe of that side to which the finger was being moved, stood unmoved in its central position, but the other globe followed the eye and placed itself in the convergent position. The patient complained of diplopia. Even after the closure of one eye a double vision appeared (monocular diplopia). There was achromatopsia. The cornea failed to react to stimulation.
If the patient was asked to follow a finger moving to one side, the eye on that side stayed centered, while the other eye moved and converged towards the finger. The patient reported seeing double. Even after closing one eye, they still experienced double vision (monocular diplopia). There was also loss of color vision. The cornea didn't respond to stimulation.
There was an analgesia of the skin of the whole body, with a hypesthesia for tactile stimuli on the left side. Smell and taste absent. The convergent position of the globes with myosis was preserved in the midst of convulsive seizures,[614] which could be produced by exciting the patient. When it was attempted to dissolve the eye troubles by hypnosis, convulsive attacks occurred. The patient was pronouncedly hysterical.
There was a loss of sensation in the skin of the entire body, with reduced sensitivity to touch on the left side. Smell and taste were absent. The inward positioning of the eyes with constricted pupils remained during the convulsive seizures, [614] which could be triggered by stimulation of the patient. When attempts were made to resolve the eye issues through hypnosis, convulsive episodes happened. The patient was clearly hysterical.
The case is beyond question hysterical,—the phenomena consisting of an ophthalmoplegia externa, alternating with spasmodic contracture of the internal recti, associated with myosis and loss of light reaction. The influencibility of this situation during the process of tests, to say nothing of the other stigmata, clinches the diagnosis—an important one, since the development of an external ophthalmoplegia after occipital trauma might possibly be regarded as an organic disease due to hemorrhage in the region of the eye-muscle nuclei.
The case is clearly hysterical—the symptoms include external ophthalmoplegia that alternates with spasmodic contractions of the internal rectus muscles, along with constricted pupils and a loss of light reaction. The way this condition changes during testing, not to mention the other signs, confirms the diagnosis—an important one, since the onset of external ophthalmoplegia after trauma to the back of the head could potentially be seen as an organic disease caused by bleeding around the eye muscle nuclei.
Sandbag drops on head: Internal strabismus and diplopia. Various diagnoses. Cure by lenses.
Sandbags falling on your head: Crossed eyes and double vision. Different diagnoses. Treatment with lenses.
Case 436. (Harwood, September, 1916.)
A four-pound wet sandbag fell eight feet on the head of a sergeant-major, 28, lying in a Gallipoli dug-out, November 24, 1915. The sergeant-major was removed to Lemnos with headache and giddiness, and a week later developed bilateral internal strabismus with double vision and head noises. The diagnosis was “brain tumor” or “syphilitic meningitis of the base.” On the voyage home, the diagnosis was altered to “multiple neuritis or neurasthenia.”
A four-pound wet sandbag fell eight feet onto the head of a 28-year-old sergeant major lying in a dugout in Gallipoli on November 24, 1915. The sergeant major was taken to Lemnos with a headache and dizziness, and a week later he developed double vision and noise in his head due to bilateral internal strabismus. The diagnosis was either “brain tumor” or “syphilitic meningitis at the base.” During the journey home, the diagnosis was changed to “multiple neuritis or neurasthenia.”
He was admitted to the King George Hospital, January 1, 1916, unable to move the eyes outwards; they moved rather poorly up and down. There was a slight lateral nystagmus. The patient had been unable to read or stand since the accident. The visual acuity of each eye was less than 6/60, but with an arrangement of lenses he could get 6/5 with either eye. He had perfect binocular vision and could read ordinary type comfortably. In a week’s time he was able to stand without support and walk with a stick. Whenever he took off the glasses, the strabismus and diplopia immediately returned. Other combinations were tried but failed to relieve symptoms. The lenses given were +0.375 c. Vert. and L. +0.25 S. +0.25 C. 75 do.
He was admitted to King George Hospital on January 1, 1916, unable to move his eyes outward; they moved rather poorly up and down. There was slight lateral nystagmus. The patient had been unable to read or stand since the accident. The visual acuity of each eye was worse than 6/60, but with a set of lenses, he could achieve 6/5 with either eye. He had perfect binocular vision and could read regular print comfortably. Within a week, he was able to stand without support and walk with a cane. Whenever he removed the glasses, the strabismus and diplopia immediately returned. Other combinations were tried but failed to relieve the symptoms. The prescribed lenses were +0.375 c. Vert. and L. +0.25 S. +0.25 C. 75 do.
Hemianopsia: organic or functional?
Hemianopsia: organic or functional?
Case 437. (Steiner, October, 1915.)
A 19-year old volunteer, never ill (no nervous disease in the family), after a period of training went into the field, October 3, 1914. November 5, a shell struck the trench nearby but failed to explode. Up to that time everything had been quiet. The soldier had been looking out of the loophole, surveying the terrain. He felt a great fear, got a blow in the neck, fell down unconscious, remained unconscious for an unknown time, and later walked back with his comrades. About an hour later, this volunteer,—who was a very intelligent young man, possessing much knowledge of biology, including the nature of visual fields,—noticed a black spot in the field of vision, which came and went, but after a few hours remained continually without disappearing. Otherwise, there was no complaint except a feeling of dizziness when stooping.
A 19-year-old volunteer, who had never been sick (no history of mental illness in the family), went into the field after some training on October 3, 1914. On November 5, a shell hit a nearby trench but didn’t explode. Up until that point, everything had been quiet. The soldier was watching through the loophole, observing the landscape. Suddenly, he felt an intense fear, was struck in the neck, collapsed unconscious, and remained out for an unknown period. Eventually, he got up and walked back with his comrades. About an hour later, this volunteer—who was a very bright young man with a lot of knowledge in biology, including how visual fields work—noticed a black spot in his vision that appeared and disappeared, but after a few hours, it stayed and didn’t go away. Other than that, he had no complaints except for feeling dizzy when bending over.
Upon examination there could be found no disorder of the internal organs. Neurologically there was blinking, vasomotor excitability, slight reddening of the face, and dermatographia. An expert in ophthalmology confirmed the existence of a homonymous defect in the fields of vision. This defect could not be influenced by suggestion or by any other treatment, nor did any other change whatever occur in the condition.
Upon examination, there were no issues with the internal organs. Neurologically, there was blinking, increased sensitivity in the blood vessels, slight redness of the face, and skin writing. An ophthalmology expert confirmed the presence of a homonymous defect in the visual fields. This defect couldn't be affected by suggestion or any other treatment, and there were no other changes in the condition.
Steiner inquires whether this hemianopsia is to be taken as organic or functional. The air-pressure of the shell hissing past might have produced a concussion, or the falling unconscious might have produced a commotio cerebri or a slight hemorrhage. The tic-like blinking and vasomotor excitability, however, suggest functionality.
Steiner asks whether this hemianopsia should be considered organic or functional. The air pressure from the shell whizzing by could have caused a concussion, or losing consciousness might have led to a brain injury or a minor hemorrhage. However, the tic-like blinking and changes in blood flow suggest that it's functional.
Hysterical pseudoptosis.
Hysterical pseudoptosis.
Case 438. (Laignel-Lavastine and Ballet, January, 1916.)
Laignel-Lavastine and Ballet present a case of what they term hysterical pseudoptosis in a patient who showed no signs of organic disease of the nervous system, and moreover no special mental disorder. This soldier, 30 years of age, working in the auxiliary service, suffered from a troublesome lowering of his left upper eyelid. He went to the front in February, 1915. Aside from suffering a few mild and temporary blindnesses (éblouissements), he was entirely well up to the time of being wounded, March 18, 1915, by a bullet in the arm, and a bullet occasioning a superficial and slight wound 2½ centimeters above the middle of the left eyebrow. About three years later, a shell burst near him and made a large contusion about the right eye, without hurting the globus. He was then evacuated to Châlons-sur-Marne, and there remained for 48 hours, totally blind, probably on account of spasmodic closure of his eyelids. He then began to be able to use the left eye, which remained, however, very photophobic. A fortnight later, the wounds were healed, but the patient found himself unable to open his right eye. Three months later he returned to his dépôt, and left for the front October 24.
Laignel-Lavastine and Ballet discuss a case of what they call hysterical pseudoptosis in a patient who showed no signs of any organic nervous system disease or any specific mental disorder. This soldier, 30 years old and serving in the auxiliary service, experienced a bothersome drooping of his left upper eyelid. He went to the front in February 1915. Aside from experiencing some mild and temporary blindness (éblouissements), he was completely fine until he was wounded on March 18, 1915, by a bullet in his arm and another bullet that caused a superficial and minor wound 2½ centimeters above the middle of his left eyebrow. About three years later, a shell exploded near him, resulting in a large bruise around his right eye, but it did not damage the eyeball itself. He was evacuated to Châlons-sur-Marne, where he stayed for 48 hours, completely blind, probably due to spasms of his eyelids. He then began to regain some vision in his left eye, which remained very sensitive to light. Two weeks later, his wounds had healed, but he found he could not open his right eye. Three months later, he returned to his depot and left for the front on October 24.
He was reëvacuated November 4, as unsuitable for service. He was then examined by an ophthalmologist at Chartres, who found a very mobile right pupil and a slightly atrophic right papilla; vision ½; left eye normal; vision ⅔; total paralysis of right levator palpebrae superioris without contracture of orbicularis. There was also paresis of the left upper lid, which ceased when the right eye was closed. The right half of the face was anesthetic, but there was no corneal anesthesia.
He was re-evacuated on November 4 because he was deemed unfit for service. He was then examined by an eye doctor in Chartres, who found that his right pupil was very mobile and that the right optic disc was slightly shriveled; his vision was ½ in the right eye and normal in the left eye with a vision of ⅔. There was total paralysis of the right eyelid muscle without any tightening of the surrounding muscles. He also had weakness in the left upper eyelid, which went away when the right eye was closed. The right side of his face was numb, but he did not have any numbness in the cornea.
November 15: Right eyebrow lower than left; if the head was moved backward, the right eyelid followed the movements, and in this position there was no ptosis.
November 15: Right eyebrow lower than left; when the head was tilted back, the right eyelid moved along with it, and in this position, there was no drooping.
November 16: Analgesia in the super- and sub-orbicular region. November 17: frontalis and orbicularis functions normal.
November 16: Pain relief in the upper and lower eyelid area. November 17: Functions of the forehead and eyelid muscles are normal.
At time of examination, patient complained of not being able to open his right eye, and that he could only partly open the left eye. To catch a view of his examiner, he had to throw his head back and to the right. He could not open his eyelids, and in the effort to do so, the forehead muscles contracted; and whereas the left eyebrow was properly elevated, the right eyebrow was only partially elevated. Associated movements could be noted in the musculature of the lower part of the face. In looking to the right, the eyelids, especially the left, were elevated slightly. The patient complained of photophobia. From time to time, he felt completely blind, and at the end of these spells of blindness, he had a severe headache. His head felt heavy. Sometimes on looking to the left, he saw objects double, although this diplopia had grown less marked of late. All the muscles of both eyes appeared to work normally. Upon pressure on the right globus, especially pressure directed from above and behind on the internal part, the patient would raise his left eyelid, but the paresis reappeared the moment the pressure was released; a fact which the patient himself noted while a tampon was being placed upon his eye.
At the time of the examination, the patient reported being unable to open his right eye and could only partly open his left eye. To see his examiner, he had to tilt his head back and to the right. He couldn't open his eyelids, and when he tried, the muscles in his forehead contracted; while the left eyebrow was properly raised, the right eyebrow only lifted partially. There were noticeable movements in the muscles of the lower part of his face. When he looked to the right, his eyelids, especially the left one, lifted slightly. The patient expressed sensitivity to light. Occasionally, he felt completely blind, and at the end of these episodes of blindness, he experienced severe headaches. His head felt heavy. Sometimes, when looking to the left, he saw double, although this double vision had become less pronounced recently. All the muscles in both eyes seemed to function normally. When pressure was applied to the right eye, particularly from above and behind on the inner part, the patient would raise his left eyelid, but the weakness returned as soon as the pressure was released; a detail that the patient himself noticed while a compress was being placed on his eye.
It seems there had been a wound at the external angle of the eye, some nine or ten years before, as a consequence of which the eyelid of this side could never be parted as well as before. The accident in question had happened in 1905, and there had been a slight suppuration of a wound 2½ centimeters from the external angle of the palpable fissure.
It appears that there was an injury at the outer corner of the eye about nine or ten years ago, as a result of which the eyelid on that side could never open as well as it used to. The incident happened in 1905, and there was some mild infection from a wound 2.5 centimeters from the outer corner of the visible tear.
The patient then went through a period of reëducation. It seemed that when he was trying to raise his eyelids, there was a mental inhibition which could be overcome only by effort. An attempt may be made to resolve the phenomena into three groups:
The patient then went through a period of reeducation. It seemed that when he was trying to lift his eyelids, there was a mental block that could only be overcome through effort. An attempt can be made to categorize the phenomena into three groups:
First, enophthalmia of the right side (post-traumatic, antebellum, a predisposing cause).
First, enophthalmos of the right side (post-traumatic, pre-Civil War, a contributing factor).
Secondly, a situation corresponding to so-called hysterical pseudoptosis of Charcot and Parinaud (eyelid falling without[619] wrinkles, head thrown back, frontalis contraction on effort to open eyes, eyelid lowered). The diagnosis of hysteria was supported by the transient opening of both eyelids when a sudden sharp order was given to move the eye-balls, and further supported by synergic automatic lid-movements when the patient voluntarily raised his eyes. He could not raise his eyelids to order.
Secondly, there's a situation that matches what's known as hysterical pseudoptosis, as described by Charcot and Parinaud (eyelid drooping without wrinkles, head tilted back, forehead contracting when trying to open the eyes, eyelid lowered). The diagnosis of hysteria was backed up by the temporary opening of both eyelids when a sudden sharp command was given to move the eyeballs, and it was further supported by the automatic lid movements that occurred when the patient voluntarily looked up. He couldn't lift his eyelids on command.
Thirdly, functional ocular palpable synergy (left eye opening upon compressing the right eye).
Thirdly, functional eye coordination (the left eye opens when the right eye is pressed).
Shell-shock Rombergism.
Shell shock Romberg's syndrome.
Case 439. (Beck, June, 1915.)
A soldier, 24, had sundry signs of traumatic neurosis. A curious and unexplained feature is the fact that in the course of testing for Rombergism he would fall forward like a log if his head were held in the vertical position, but if it were turned to the right he fell to the right; if it were turned to the left, he fell backward. Tests showed that he had no disease of the vestibular apparatus and no sign either of cerebral or of cerebellar disease.
A 24-year-old soldier displayed various signs of traumatic neurosis. An interesting and puzzling aspect was that during tests for Rombergism, he would tip forward like a log if his head was held upright, but if it was turned to the right, he would fall to the right; if it was turned to the left, he would fall backward. Tests indicated that he had no issues with his vestibular system and showed no signs of cerebral or cerebellar disease.
The question is raised whether shell-shock can produce a differential Rombergism such as hitherto would have been explained on the basis of some organic vestibular disease.
The question is raised about whether shell shock can cause a different type of Rombergism that would previously have been explained by some kind of organic vestibular disease.
Re Rombergism, see especially Bourgeois and Sourdille’s (edited by Dundas Grant) remarks on disturbances of balance which, if of labyrinthine origin, obey Romberg’s law, namely, are greatly increased with the eyes closed. Upon test, however, normal equilibrium, tottering, or a tendency to fall will be usually found. The tendency to fall is, as a rule, toward the side of the affected labyrinth, yet it varies according to the position of the head; that is to say, actually upon the position of the labyrinth with relation to the body. If there is a lesion of the right labyrinth, for example, and the head is turned to the right, falling is to the right; but if the head is turned 90 degrees toward the right, the patient tends to fall backward because in fact the injured right labyrinth has now become posterior in position. But if the head with the injured right labyrinth is displaced 90 degrees to the left, the tendency would be to fall forwards.
Re Rombergism, see especially Bourgeois and Sourdille’s (edited by Dundas Grant) comments on balance disturbances that, if they originate from the labyrinth, follow Romberg’s law—specifically, they worsen significantly when the eyes are closed. When tested, normal balance, swaying, or a tendency to fall is usually observed. The tendency to fall generally leans toward the side of the affected labyrinth, though it can change depending on the head's position; in other words, it depends on how the labyrinth is positioned relative to the body. For example, if there’s damage to the right labyrinth and the head is turned to the right, the patient will tend to fall right. However, if the head is turned 90 degrees to the right, the patient may fall backward because the injured right labyrinth is now positioned at the back. Conversely, if the head with the injured right labyrinth is turned 90 degrees to the left, the tendency would be to fall forward.
According to Beck, there was in his case of Shell-shock Rombergism no ear disease or any evidence of cerebellar or cerebral disease.
According to Beck, in his case of Shell-shock Rombergism, there was no ear disease or any signs of cerebellar or cerebral disease.
Walking with the eyes open yields in marked instances a sidewise bending or even the classical staggering called the duck’s walk and drunken gait upon a broad base. The most delicate test, according to Bourgeois and Sourdille, is[621] the Babinski-Weil test of walking with the eyes shut. A man with labyrinthine disease deviates from the straight path (he is made to walk forwards and backwards ten times in a clear space); bends pretty constantly to one side when walking forward, and pretty constantly to the other side when walking backwards. Spontaneous and Babinski’s induced nystagmus (rotation; caloric) and Babinski’s voltaic vertigo test are the other tests commonly employed in equilibrium investigation.
Walking with your eyes open often results in noticeable side-to-side bending or even what’s known as the duck walk or the unsteady gait seen in someone who’s drunk, all on a wide base. The most sensitive test, according to Bourgeois and Sourdille, is[621] the Babinski-Weil test of walking with your eyes closed. A person with inner ear disease tends to stray from a straight path (they’re asked to walk forward and backward ten times in a clear space); they lean to one side when walking forward, and lean to the other side when walking backward. Spontaneous and Babinski’s induced nystagmus (rotation; caloric) and Babinski’s voltaic vertigo test are the other tests commonly used in balance assessments.
Otology and neuropsychiatry should go hand in hand.
Otology and neuropsychiatry should work together.
Case 440. (Roussy and Boisseau, May, 1917.)
A soldier in the engineers, 29, entered the neuropsychiatric center at Scey-sur-Saône, August 23, 1916. His diagnosis was: organic shock syndrome with right-side deafness and tremors. He carried a ticket showing an otological examination: tympanum normal; Rombergism absent; walks with eyes closed swerving to right; tends to fall, eyes closed, on standing on one foot; vertigo produced by rotation in either direction; no nystagmus either spontaneous or by test; deafness especially on the right side; equilibrium function insufficient.
A 29-year-old engineer soldier entered the neuropsychiatric center at Scey-sur-Saône on August 23, 1916. His diagnosis was organic shock syndrome with hearing loss on the right side and tremors. He had a ticket showing an ear examination: eardrum normal; no Romberg sign; sways to the right while walking with eyes closed; tends to fall with eyes closed when standing on one foot; experiences dizziness when rotated in either direction; no spontaneous or tested nystagmus; hearing loss is particularly on the right side; balance function is inadequate.
The patient had undergone shock in April, 1915, being buried and then losing consciousness for twenty-four hours. The tremors appeared next day, and also deafness but without speech disorder. Nine comrades are said to have been killed beside him. The hospital ticket, April 13, said: deafness and multiple contusions from shell explosion. The patient was evacuated to Clarmont-Ferrand and went back to service with the same tremor and auditory disorder. He was shortly sent back to the interior for six months and returned improved to the front August, 1915. But he heard the cannon in the distance, and, under the influence of emotion and the fatigue of the journey, the tremors and deafness reappeared.
The patient experienced shock in April 1915 after being buried and losing consciousness for twenty-four hours. Tremors and deafness showed up the next day, but there was no speech issue. It's reported that nine comrades were killed beside him. The hospital record from April 13 noted: deafness and multiple bruises from a shell explosion. The patient was evacuated to Clermont-Ferrand and returned to duty with the same tremor and hearing issues. He was soon sent back deeper into the interior for six months and then returned to the front in August 1915. However, he could still hear the distant cannons, and due to emotional stress and the fatigue of the journey, the tremors and deafness came back.
The tremor was generalized, involving both arms and legs and a slight lateral movement of negation of the head every ten or twelve seconds. Occasionally tonic contracture of the face, lips, cheeks, forehead; tremors of tongue; winking. The tremors were somewhat suggestive of toxic tremors.
The shaking was widespread, affecting both arms and legs, with a slight side-to-side movement of the head every ten to twelve seconds. Sometimes, there was a stiffening of the face, lips, cheeks, and forehead; shaking of the tongue; blinking. The tremors seemed a bit like toxic tremors.
The deafness was evidently exaggerated. Voltaic vertigo tested normal. Reflexes normal.
The deafness was clearly overblown. Voltaic vertigo tested normal. Reflexes were normal.
The diagnosis psychoneurosis was made and the patient was rigorously isolated, given a long psychotherapeutic talk concerning the nonreality of his deafness and his vertigo and[623] the possibility of cure by means of a very disagreeable electrical treatment. He made improvement upon psycho-electrical treatment and the next day both tremors and deafness had greatly diminished. September 4, the patient was considered completely well. There was a slight diminution of hearing in the right ear, the whispered voice was heard at 50 centimeters on the right side, the watch at 25 centimeters on the right and 60 on the left.
The diagnosis of psychoneurosis was made, and the patient was strictly isolated. He had a long talk about the unreality of his deafness and vertigo and the potential for a cure through a very unpleasant electrical treatment. He showed improvement after the psycho-electrical treatment, and by the next day, both his tremors and deafness had greatly decreased. By September 4, the patient was considered completely well. There was a slight reduction in hearing in his right ear; he could hear a whispered voice from 50 centimeters away on the right side, and a watch from 25 centimeters on the right and 60 centimeters on the left.
October 5 the patient was sent back to his corps. On the evening of his departure, angry at not having received leave, he boasted to his comrades of having passed but three days at the front since his injury.
October 5, the patient was sent back to his corps. On the evening of his departure, upset about not getting leave, he bragged to his comrades that he had only spent three days at the front since his injury.
It is remarkable, according to Roussy and Boisseau that this patient had passed sixteen months without ever having been taken for a neuropath or treated as one. The otologists gave the diagnosis of labyrinthine shock, but did not attend to the tremors. The pseudo-symptoms disappeared in six days at the neurological center and the cure had lasted six weeks at the time of report.
It’s striking, according to Roussy and Boisseau, that this patient had gone sixteen months without ever being recognized as a neuropath or treated as one. The ear specialists diagnosed labyrinthine shock but overlooked the tremors. The fake symptoms vanished in six days at the neurological center, and the recovery had lasted six weeks by the time of the report.
Re otology in these cases, see Bourgeois and Sourdille’s book mentioned under Case No. 439, particularly Chapter III, upon the functional examination of hearing. In the present instance, it will be noted that voltaic vertigo tested out normal. According to Bourgeois and Sourdille, the Babinski electrical test is the most convenient one to begin with, to learn in a few moments whether the vestibular system is working normally or not. These authors found amongst twelve patients, three normal reactions and one instance of hypo-excitability amongst four subjects who, by other tests, failed to show vestibular disturbance. Inexcitability as to voltaic vertigo was found in one man with a destroyed labyrinth. There were four instances of hyperexcitability in Babinski’s cases with marked equilibrium disorder. A case of Ménière’s disease yielded the same results. According to the intensity of the current, the following phenomena (in addition to the pricking sensation) are noted; (a) salty taste; (b) sidewise swaying with slight vertigo; (c) nystagmus with more pronounced vertigo; (d) sensations of sound. In short, nerve branches that go through[624] the petrous bone, namely, the chorda tympani, the vestibular nerve, and the cochlear nerve, have been successively stimulated. Babinski’s test was published before the Barany work on induced nystagmus, but Barany’s rotation test for the physiological excitation of the semi-circular canals, and his caloric test for the investigation of the ears and canals separately are to be utilized in addition to the Babinski voltaic test. Babinski’s law of voltaic vertigo is that a normal subject inclines to the side of the positive pole; a pathologic subject falls to the side to which he tends to incline spontaneously. If the labyrinth has been destroyed, there has been no reaction.
Re otology in these cases, see Bourgeois and Sourdille’s book mentioned under Case No. 439, especially Chapter III, on the functional examination of hearing. In this instance, it’s noted that the voltaic vertigo test came out normal. According to Bourgeois and Sourdille, the Babinski electrical test is the easiest one to start with, as it quickly shows whether the vestibular system is functioning normally or not. These authors found that among twelve patients, there were three normal reactions and one case of hypo-excitability among four subjects who, through other tests, did not show any vestibular disturbance. One man with a damaged labyrinth showed no response to voltaic vertigo. There were four cases of hyperexcitability in Babinski’s patients with significant equilibrium issues. A patient with Ménière’s disease had similar results. Depending on the current's strength, the following effects (besides the pricking sensation) are observed; (a) salty taste; (b) slight swaying to the side with mild vertigo; (c) nystagmus with more intense vertigo; (d) sensations of sound. In summary, nerve branches running through[624] the petrous bone, specifically the chorda tympani, the vestibular nerve, and the cochlear nerve, have been stimulated in succession. Babinski’s test was published before Barany’s work on induced nystagmus, but Barany’s rotation test for the physiological stimulation of the semi-circular canals and his caloric test for investigating the ears and canals separately should also be used along with the Babinski voltaic test. Babinski’s law of voltaic vertigo states that a normal subject sways towards the positive pole; a pathological subject tips towards the side they naturally lean. If the labyrinth is destroyed, there is no reaction.
Re Case 440, Roussy and Boisseau in their capacity as neuropsychiatrists, point out the inadequacy of an otological examination taken by itself. They insist that neuropsychiatrists should be called in. It is probably equally true that neuropsychiatric work upon deaf cases is often inadequate on account of the lack of otological examinations. According to Bourgeois and Sourdille, the expert otologist’s problems are as follows: (a) Deafmutism; here Gault’s cochleopalpebral reflex is of value. The hearing of a sudden noise causes contraction of the orbicularis palpebrarum on the side upon which the noise is suddenly and unexpectedly made. Eyelash tips are particularly watched.
Re Case 440, Roussy and Boisseau, as neuropsychiatrists, highlight that an otological exam on its own is not sufficient. They stress that neuropsychiatrists need to be involved. It’s likely that neuropsychiatric assessments of deaf cases can also be lacking due to missing otological exams. According to Bourgeois and Sourdille, the challenges faced by expert otologists include: (a) Deafmutism; in this case, Gault’s cochleopalpebral reflex is useful. Hearing a sudden noise results in the contraction of the orbicularis palpebrarum on the side where the noise occurs unexpectedly. Special attention is given to eyelash tips.
(b) Complete bilateral deafness. This is practically never organic; complete bilateral deafness is a phenomenon either of traumatic hysteria or of simulation. Sundry methods of surprising the patient into hearing have been adopted. The practice of teaching lip-reading to simulators and hysterics has led to some difficulties in diagnosis, but tests have been produced by Gosset (of one sound with the lips set to form another, and the like) which are of service.
(b) Complete bilateral deafness. This is almost never caused by organic issues; complete bilateral deafness is usually a result of traumatic hysteria or faking. Various methods have been used to startle the patient into hearing. Teaching lip-reading to those faking or experiencing hysteria has created some challenges in diagnosis, but tests developed by Gosset (using one sound while the lips form another, among other techniques) have proven helpful.
(c) Extreme bilateral dulness of hearing.
(c) Severe hearing loss in both ears.
(d) Total unilateral deafness. For the minutiae of tests for these types of hearing disorder and their simulation and exaggeration, see the War Manual of Bourgeois and Sourdille.
(d) Total unilateral deafness. For the details of tests for these types of hearing issues and their simulation and amplification, refer to the War Manual of Bourgeois and Sourdille.
Jacksonian syndrome: Hysterical.
Jacksonian syndrome: Hysterical.
Case 441. (Jeans and Huet, July, 1915.)
A Lieutenant of Infantry, 32, was struck by a bullet September 6, 1914, in the upper part of the left temporal fossa 4 cm. above the external auditory meatus. He did not lose consciousness, but had the sensation as if his head had been shot off, and about three minutes later he turned about, fell down, and lost consciousness. However, he regained consciousness a few minutes later and walked with support for about an hour. At the ambulance, he lost consciousness again, for half an hour. He was then carried to Amalie-les-Bains. The trip lasted 108 hours. The left side of the face was now swollen so that he could not open the eye nor could he chew from swollen mucosa folded between the jaws. The bullet was removed Sept. 12, from just below the scalp outside the bone, the point being slightly bent back. The bone had been depressed slightly for an area the size of a franc piece, and pressure at this point yielded a feeling of pain and discomfort. There was no suppuration. After a week, the man got up. He returned to his dépôt October 3 or 4 and was about to rejoin his corps when he had a sensation of pressure in the head and fell. When he came to himself he found that there was a frothy saliva at the left side of the mouth and that the whole left side of the body felt weak. The tongue had not been bitten nor had urine been passed, and twenty minutes later he felt as well as ever. He returned to the front in the Argonne, having from time to time similar crises,—at least once a week. Ordered to take a trench the night of January 17, he failed the first time, about midnight, but succeeded at four in the morning,—just afterward falling exhausted in another crisis, with unconsciousness. The stretcher bearers took him back and he was evacuated to Perpignan. He had two convulsions.
A 32-year-old Infantry Lieutenant was shot on September 6, 1914, in the upper left side of his head, 4 cm above the ear. He didn’t lose consciousness initially but felt like his head had been blown off. About three minutes later, he turned around, collapsed, and lost consciousness. However, he woke up a few minutes later and was able to walk with help for about an hour. At the ambulance, he lost consciousness again for half an hour. He was then taken to Amalie-les-Bains, which took 108 hours. By then, the left side of his face was so swollen that he couldn’t open his eye or chew due to the swollen tissue between his jaws. The bullet was removed on September 12 from just below the scalp, outside the bone, and the tip was slightly bent backwards. The bone had a slight dent about the size of a franc coin, and pressure at that spot caused pain and discomfort. There was no infection. After a week, he got up and returned to his unit on October 3 or 4. Just before he was about to rejoin his corps, he felt pressure in his head and collapsed. When he came to, he noticed frothy saliva on the left side of his mouth and weakness on the whole left side of his body. His tongue wasn’t bitten, and he hadn’t passed urine, but twenty minutes later he felt completely fine. He returned to the front lines in the Argonne but experienced similar episodes about once a week. On the night of January 17, he was ordered to take a trench; he failed the first attempt around midnight but succeeded at 4 in the morning. Soon after, he collapsed again in another episode, losing consciousness. Stretcher bearers took him back and he was evacuated to Perpignan, where he had two convulsions.
While with his family the crises grew in number to three or four a week, and sometimes twice a day. Upon request, he was sent to hospital in the Pantheon May 5.
While he was with his family, the crises increased to three or four a week, and sometimes even twice a day. Upon request, he was admitted to the hospital in the Pantheon on May 5.
There was always a sensory aura, consisting in a violent shock felt in the left side of the cranium like a blow of a club. There immediately followed a crawling sensation in the fingers and hand of the left side, running up the arm, with loss of consciousness coming on before the crawling reached the elbow. The seizure would last two or three minutes. There was no initial cry. The face grew pale. There was apnea, and frothy fluid running out of the left side of the mouth. There was no jerking of face or limbs; at the end of the seizure there were no deep inspirations. The extremities of the left side were rather flaccid during the attack.
There was always a strong sensation, like a hard blow to the left side of the head. This was quickly followed by a tingling feeling in the fingers and hand on the left side, moving up the arm, with loss of consciousness happening before the tingling reached the elbow. The episode would last two to three minutes. There was no initial scream. The face became pale. There was no breathing for a moment, and frothy fluid came out of the left side of the mouth. There was no jerking of the face or limbs; at the end of the episode, there were no deep breaths. The left side limbs were quite limp during the attack.
A hemianesthesia was found affecting both skin and mucosae of the left side, and a slight retraction of the visual field on the left side was found. There were no other sensory disorders; the knee-jerks were lively on both sides but not actually exaggerated. Plantar stimulation was not perceived on the left side. The toes, except the great toe, were slightly extended. The fascia lata reflex failed to demonstrate itself. On the right side the great toe went into flexion on forcibly stimulating the sole. Sometimes the abdominal reflex on the left side was weak or even absent. The patient, who had never been nervous, had now become so since his attacks. He had had nocturia up to 12. There was no evidence of neurosis or psychosis in the family. Bromides diminished the crises a little in number. Static electricity was given from January 8,—no attacks for 8 to 10 days.
A hemianesthesia was found affecting both the skin and mucous membranes on the left side, and there was a slight reduction in the visual field on the left side as well. No other sensory issues were present; knee-jerk reactions were lively on both sides but not overly so. The left side did not react to plantar stimulation. The toes, except for the big toe, were slightly extended. The fascia lata reflex did not show up. On the right side, the big toe flexed when the sole was forcefully stimulated. Occasionally, the abdominal reflex on the left side was weak or completely absent. The patient, who had never been anxious, had become so since his episodes began. He experienced nocturia up to 12 times. There was no indication of neurosis or psychosis in the family. Bromides slightly reduced the number of episodes. Static electricity treatment started on January 8, with no episodes for 8 to 10 days.
According to Jeanselme and Huet, this is a case of Jacksonian syndrome of an hysterical nature, about which it may be noted that the bullet struck the left side of the skull and the hemianesthesia and muscular resolution appeared on the same side as the injury.
According to Jeanselme and Huet, this is a case of Jacksonian syndrome of a hysterical nature, and it's worth noting that the bullet hit the left side of the skull, with hemianesthesia and muscle weakness appearing on the same side as the injury.
Leg tic: Phobia against crabs.
Crustacean phobia: Fear of crabs.
Case 442. (Duprat, October, 1917.)
A man, shell-shocked in 1916 (with loss of consciousness, disorientation and confusion followed by nightmares, memory disorder, attention disorder, irritability, mental instability and over-emotionalism) later still showed a choreiform tic. He had a knife-grinding movement of the left leg which made standing and walking difficult. There were no signs in the reflexes or reactions of organic disease. The man himself said that he felt a sensation like little electric shocks when his foot touched the ground, a sensation like pinching. He also had certain hysteriform crises. He was able to remember nightmares in which he felt as if he had fallen into a hole where there were crabs. In point of fact, he had a true phobia against crabs, crayfish, lobsters and the like; if he saw one, he always felt as if he were going to have a new crisis. The defense movement of the leg and foot was against a supposed pinch of the crab. At rest, there was no trace of the choreiform movement. The tic was especially marked when the man was suddenly asked to get up and walk. In a few days, when he had become more clearly conscious of his phobia and had slept better, the tic grew appreciably less.
A man, traumatized in 1916 (experiencing loss of consciousness, disorientation, and confusion, along with nightmares, memory issues, attention problems, irritability, mental instability, and heightened emotions) later developed a choreiform tic. He had a knife-grinding movement in his left leg that made standing and walking difficult. There were no signs of organic disease in his reflexes or reactions. The man reported feeling sensations like tiny electric shocks when his foot touched the ground, a sensation similar to pinching. He also experienced certain hysterical episodes. He could remember nightmares where he felt like he had fallen into a hole filled with crabs. In reality, he had a genuine phobia of crabs, crayfish, lobsters, and similar creatures; whenever he saw one, he felt like he was about to have another episode. The defensive movement of his leg and foot was in reaction to an imagined pinch from the crab. When he was at rest, there was no trace of the choreiform movement. The tic was particularly pronounced when he was suddenly asked to get up and walk. In just a few days, as he became more aware of his phobia and slept better, the tic significantly reduced.
Convulsions reminiscent of fright.
Seizures like those from fear.
Case 443. (Duprat, October, 1917.)
A soldier, 28, was blown up February 8, 1915, by a shell burst. He sustained no contusions but became completely mute. On July 3, he began to speak in a low voice. The torpillage treatment was unsuccessful because the man felt a morbid apprehension that the vibration of a loud voice or even of a rapid walk would resound in his brain. He had a sort of noise phobia, probably maintained by nightmares which frequently woke him up with a jerk though he could not remember their content. On the way back to his dépôt this man got off the train at the first station and went to a hospital complaining that the vibration of the train was going to be transmitted to his brain. Hysteriform crises developed in a few days.
A soldier, 28, was blown up on February 8, 1915, by a shell explosion. He didn’t have any injuries but became completely mute. On July 3, he started to talk in a low voice. The torpillage treatment didn’t work because he felt an intense fear that the sound of a loud voice or even the impact of a fast walk would echo in his brain. He developed a kind of noise phobia, likely fueled by nightmares that often jolted him awake, though he couldn’t remember what they were about. On his way back to his depot, he got off the train at the first station and went to a hospital, saying that the vibrations from the train were going to affect his brain. Hysteriform crises developed within a few days.
According to Duprat these crises are nothing but a psychomotor development of the initial complex. The clonic and tonic convulsions are reminders of his states of extreme fright, a phenomenon of revival of the ideo-affective process, aggravated however by the oniric or post-oniric images.
According to Duprat, these crises are just a psychomotor development of the initial complex. The clonic and tonic convulsions are reminders of his moments of intense fear, a revival of the ideo-affective process, which is worsened by the dreamlike or post-dream images.
Re diagnosis of hysterical fits, the absence of facial cyanosis, sub-conjunctival hemorrhages, petechiae of skin, and the Babinski reflex are suggestive for hysteria. Babinski points out that the initial cry, the fall, the loss of consciousness, the tongue-biting, the bloody frothing at the mouth, the urinary incontinence, and the post-convulsive prostration can all be consciously or unconsciously imitated. Hysterical convulsive movements are apt to be of wide range, gesticulatory, and opisthotonic.
Re diagnosis of hysterical fits, the lack of blue skin, eye bleeding, skin spots, and the Babinski reflex suggest hysteria. Babinski notes that the initial scream, the collapse, the loss of consciousness, the tongue-biting, the bloody foam at the mouth, the urinary incontinence, and the fatigue after convulsions can all be imitated, either intentionally or unintentionally. Hysterical convulsive movements tend to be varied, expressive, and arching backward.
Babinski announces to the supposed hysteric that he is going to reproduce the attack, as he is perfectly able to do by electricity. A mild current or mere electrode application suggests a fit in a hysteric, often very quickly. Babinski now announces that he can arrest the fit; carries out some selected procedure, and stops the fit. During the hysterical fit, the patient of course hears what is being said and during this time wrong suggestions must not be offered.
Babinski tells the supposed hysteric that he’s going to recreate the attack using electricity, which he can easily do. A mild current or just applying electrodes can trigger a fit in someone with hysteria, often quite rapidly. Babinski now claims he can stop the fit; he performs a specific procedure and halts the fit. During the hysterical fit, the patient can hear what is being said, and it’s important not to offer any misleading suggestions at this time.
Fugue in a motor cyclist, with prodromal fatigue and subsequent delusions—recovery in six weeks.
Fugue in a motorcyclist, with early signs of fatigue and later delusions—recovery in six weeks.
Case 444. (Mallet, July, 1917.)
A motor-cyclist, 36, with the colors from the outbreak of the war, about April, 1916, grew very weary, suffering from headache and seizures without loss of consciousness. Finally there was a voice: “Sleep, you must sleep.” Then other voices; then ideas of thought transference with people around him.
A 36-year-old motorcyclist, wearing the colors from the start of the war around April 1916, became very exhausted, suffering from headaches and seizures without losing consciousness. Eventually, he heard a voice say, “You need to sleep.” Then more voices followed, along with thoughts about transferring ideas to the people around him.
Observed in the psychiatric center, May 12, 1916, he had the same ideas of thought transference, and he made as if to talk with the attendants by responsive-looking gestures. Sometimes, he said, fluid struck his forehead, calling on his thought. Whereupon he listened. The man made no complaints about his plight, was not astonished in any wise at what was happening, nor did he seek to explain it. There was nothing in his history to suggest psychopathy except perhaps that his father was unknown.
Observed in the psychiatric center, May 12, 1916, he had the same ideas about thought transference, and he gestured as if he wanted to communicate with the attendants. Sometimes, he mentioned, a sensation would hit his forehead, prompting his thoughts. After that, he would listen. The man didn’t complain about his situation, wasn’t surprised at what was happening, nor did he try to explain it. There was nothing in his background to indicate any mental illness except perhaps that his father was unknown.
The diagnosis of a chronic hallucinatory psychosis was made, but the outcome promptly overset the diagnosis. The man talked with ward-mates, and particularly with another patient who also talked about thought transference. This shook the man in his convictions, and he decided that it was but imagination and delirium.
The diagnosis of chronic hallucinatory psychosis was given, but the outcome quickly overturned that diagnosis. The man spoke with his fellow patients, especially with another patient who also discussed thought transference. This made him question his beliefs, and he concluded that it was just imagination and delirium.
He now told his story: How it seemed that he had in his thoughts the phrase, “Sleep, you must sleep;” how he had gotten up, saying, “No;” had noticed the others paying no attention to him; had gone back to his work and from that moment had begun to go into delirium. During this delirium or delusional state, his whole life from birth up, came back to him, as if some one were telling him. The headaches, which he at first felt due to Hertzian waves, suddenly ceased.
He started sharing his story: how he had the phrase, “You need to sleep,” on his mind; how he had gotten up, saying, “No;” noticed that the others were ignoring him; and returned to his work, which was when he started to go into a delirious state. During this delirium, his whole life from birth flashed before him, as if someone were narrating it to him. The headaches, which he initially thought were caused by Hertzian waves, suddenly went away.
Shortly, however, a new phase had set in, in which he felt himself surrounded by spies and that others had control of his thoughts and were reading them. In fact, he grew a[630] little proud of the fact that people reading newspapers all around him were actually reading his own thoughts. The letters he wrote were being dictated. May 9, he spent a night with a succession of nightmares, and woke up with the firm purpose of going back to Paris by motor cycle to find the spies. He described his fugue and the thousand ideas he had on the way, his arrest, his imprisonment in a cell of Hertzian waves with a smell of sulphur and poisoned bread—a necessary fate on account of the spies.
Shortly after, he entered a new phase where he felt surrounded by spies, convinced that others had control over his thoughts and were able to read them. In fact, he started to feel a bit proud that people reading newspapers around him were actually picking up on his own thoughts. The letters he wrote felt like they were being dictated. On May 9, he spent a night plagued by nightmares and woke up determined to ride his motorcycle back to Paris to find the spies. He recounted his journey and the countless ideas he had along the way, his arrest, and his imprisonment in a cell filled with Hertzian waves that smelled of sulfur and poisoned bread—a necessary fate because of the spies.
On arrival at hospital, he had not known what was going forward. The nurses were giving him milk to destroy the taste of sulphur; the delirium then grew less and less. The room-mates were neutrals, war-weary; he seemed to be reading the newspapers before his mates, and they seemed to be talking of thought transference. May 20, the ward was changed. The new ward-mates did not believe in thought transference and laughed, causing the man to doubt.
Upon arriving at the hospital, he didn’t know what was happening. The nurses were giving him milk to wash away the taste of sulfur; slowly, the delirium faded. His roommates were neutral, worn out from the war; it felt like he was reading the newspapers to his friends, and they seemed to be discussing mind reading. On May 20, he was moved to a new ward. His new roommates didn’t believe in mind reading and laughed, which made him doubt himself.
June 2, the cure was in full process, and the ward was changed again; but in the new ward was a patient who had the same ideas of thought transference as the patient. At this time, the man’s autocritique saw through the delusion. He talked with his telepathic comrade and pretended to engage in a fake conversation about it. The delusions shortly disappeared, having lasted about six weeks.
June 2, the treatment was in full swing, and the ward was changed again; but in the new ward was a patient who shared the same thoughts about mind reading as the previous patient. At this point, the man’s self-critique recognized the delusion. He chatted with his telepathic companion and pretended to take part in a fake conversation about it. The delusions quickly vanished, having lasted about six weeks.
Ordinary gunner’s life; a few days’ feeling of moral and physical discomfort: Obsession leading to fugue.
Ordinary life as a gunner; a few days of moral and physical unease: Obsession leading to a state of disconnection.
Case 445. (Hammer, July, 1917.)
An artilleryman, 32, gave himself up a few kilometers back of the lines, three days after deserting his post. The man was a very good gunner and had never been punished once. Moreover, the battery was not under any special bombardment, and he had been in the same place a number of weeks.
An artilleryman, 32, surrendered a few kilometers behind the lines, three days after leaving his post. He was an excellent gunner and had never been disciplined. Plus, the battery wasn't facing any specific bombardment, and he had been stationed in the same spot for several weeks.
He explained that he had gotten tired during the last few days. Everything was well at home and in the regiment, but he felt sad, his head felt bad, and he couldn’t sleep. Something drew him to leave, but then “sang froid came back to me, and I gave myself up.” He had lived the three days without eating and without sleeping. He was very emotional over what he had done, but he began to work and asked that he be sent back.
He explained that he had grown tired over the past few days. Everything was fine at home and with the regiment, but he felt sad, had a headache, and couldn’t sleep. Something compelled him to leave, but then “sang froid came back to me, and I gave myself up.” He had gone three days without eating or sleeping. He was very emotional about what he had done, but he started to work and requested to be sent back.
His mother had been very nervous. There was a marked facial asymmetry and faulty arrangement of teeth. The man was not alcoholic.
His mom had been really anxious. There was a noticeable imbalance in his facial features and his teeth were misaligned. The guy wasn't an alcoholic.
According to Mallet, in these cases of fugue, and in other cases of absolute delirium of apparently sudden onset, there is a feeling of moral and physical discomfort for some days before the outbreak. The outbreak itself is sudden on the occasion of some idea, either an obsession or a hallucination. Of all the prodromal signs, headache is the most striking. According to Mallet, such fugues are the expression of a mental imbalance allied to the onirism of Régis.
According to Mallet, in cases of fugue and other instances of severe delirium that seem to come on suddenly, there is often a sense of moral and physical unease for several days leading up to the event. The actual outbreak happens suddenly, triggered by an idea, whether it's an obsession or a hallucination. Out of all the early warning signs, headaches are the most noticeable. Mallet suggests that these fugues reflect a mental imbalance related to Régis's concept of onirism.
Aprosexia and bird-like movements.
Aprosexia and birdlike movements.
Case 446. (Chavigny, October, 1915.)
A soldier of the dragoons, 25, entered Chavigny’s service May 30, 1915. He acted like a mechanical figure, requiring guidance. The face was without expression except for the mobile eyes, and sudden bird-like movements of the head, continually attracted to new noises and objects. An interlocutor was glanced at but not responded to. If an intense electrical shock was passed through his abdomen, for example, the man would look for a moment in that direction, but only the most fugitive defence reaction would be made, and the stimulus could be repeated with the same result, a moment later.
A 25-year-old soldier from the dragoons started working for Chavigny on May 30, 1915. He moved like a robot, needing direction. His face was expressionless except for his lively eyes, and his head made quick, bird-like movements, constantly drawn to new sounds and sights. He would glance at someone talking to him but wouldn’t respond. If, for instance, a strong electrical shock was applied to his abdomen, he would briefly look in that direction, but only show the slightest instinct to defend himself. The same stimulus could be applied again with the same reaction just a moment later.
After three days, this aprosexia began to clear, and in four or five days, answers to questions and ordinary associations set in. Memory reappeared. It seems that he had been in concealment in the loft of a barn, when he saw his commanding officer carried by, having lost an arm and a leg. He lost consciousness and fell three meters, through the trapdoor of the loft. There was thus a combination of trauma and emotional shock. No external lesion was produced in the fall. His memory showed a very sharply defined gap for the period of his aprosexia with the bird-like movements, of eight days, and his memory was perfectly good up to the time of the fall. This is one of five cases observed by Chavigny, who remarks that there is something in the attitude of the young child which recalls the aprosexia of these patients. (Perhaps the phrase of James, “buzzing, blooming confusion” might be used.) One must go back to a period in the child’s development when he is not yet able to smile or keep his glance fixed on a shining object. On the whole, the resemblance is closer to the attitude of certain caged birds.
After three days, this inability to focus started to improve, and within four or five days, he was able to respond to questions and make normal associations. His memory came back. It seems he had been hiding in the loft of a barn when he saw his commanding officer being carried past, having lost an arm and a leg. He lost consciousness and fell three meters through the loft's trapdoor. This resulted in a mix of trauma and emotional shock. There were no external injuries from the fall. His memory had a clear gap during the period of his inability to focus, lasting eight days, but his memory was completely intact up until the fall. This is one of five cases documented by Chavigny, who notes that there is something in the behavior of young children that resembles the inability to focus seen in these patients. (Perhaps the phrase from James, “buzzing, blooming confusion,” could be applied here.) We need to refer back to a stage in a child's development when they still can't smile or maintain their gaze on a shiny object. Overall, the similarity is more akin to the behavior of certain caged birds.
Shell-shock; unconsciousness (45 days): Mutism (monosymptomatic).
Shell shock; unconsciousness (45 days): Mutism (single symptom).
Case 447. (Liébault, 1916.)
A soldier, 32, had a large caliber shell burst one meter from him September 26, 1915, lost consciousness and remained comatose 45 days. He then got progressively better but did not recover speech. He was neither blind nor deaf. He was examined at the neurological center at Nantes and there Mirallié called him a case of hysterical mutism, finding no paralytic disorder of any sort and finding the patient able to write his story, to read and to understand what he read, but without much power of retention. He was placed in the phonetic reëducation service March 30, but made no progress. In the effort to speak the patient made strong generalized contractions, including contractions of his face and winking of his eyes, contractions of the jaw, and movements of the neck muscles. In fact, he seemed to be agitated by a sort of cervico-facial tic, and sometimes, although not always, he succeeded in getting out a loud voice sound, in which one could imagine the syllable that he was trying to utter.
A soldier, 32, had a large caliber shell explode one meter away from him on September 26, 1915. He lost consciousness and remained in a coma for 45 days. He then gradually improved but did not regain his ability to speak. He was neither blind nor deaf. He was evaluated at the neurological center in Nantes, where Mirallié called him a case of hysterical mutism, finding no signs of paralysis and noting that the patient could write his story, read, and comprehend what he read, but had limited retention. He was placed in a speech therapy program on March 30 but showed no progress. In his attempts to speak, the patient exhibited strong, generalized muscle contractions, including facial contractions and eye winking, jaw clenching, and neck muscle movements. In fact, he appeared to be affected by a kind of cervico-facial tic, and sometimes, though not always, he managed to produce loud vocal sounds, from which one could infer the syllable he was trying to pronounce.
In this case the mutism was evidently secondary to motor disorder. It is an example of functional dyskinesia (Benon). As long as this functional dyskinesia remains, the patient will not speak. The respiratory muscles are disordered, since the respiratory capacity does not go over 3 liters. This approaches the normal, however, and if the subject cannot speak it is because his diaphragm is subject to jerky or cramplike movements and because the lips and tongue do not execute the proper movements either for sounds, syllables or words. Such a patient cannot protrude the tongue or even bring it beyond the teeth.
In this case, the mutism was clearly due to a motor disorder. It’s an example of functional dyskinesia (Benon). As long as this functional dyskinesia is present, the patient will not speak. The respiratory muscles are affected, as the respiratory capacity doesn’t exceed 3 liters. This is close to normal, but if the person can’t speak, it’s because their diaphragm experiences jerky or cramp-like movements, and the lips and tongue aren’t moving correctly to produce sounds, syllables, or words. Such a patient cannot stick out their tongue or even extend it past their teeth.
Shell-explosion: Recurrent amnesia.
Shell explosion: Recurring amnesia.
Case 448. (Mairet and Piéron, April, 1917.)
A shock case of Mairet and Piéron had a disorder of memory. Association paths were open one day and closed the next. Subjected to shell-shock, September 18, 1915, he was found wandering in the woods a few days later, having completely lost his memory, even for his name. In November he recovered his surname but not his given name. On stimulation he was gotten to remember his city, his father, the street, and the like. Shortly he could get back his memories more quickly; after a week it took only 35 seconds to remember that he was born at Paris. However, his recollection of the Trocadero and of the Eiffel Tower, which had come back to him in November, 1915, was lost again in April, 1916, to return once more in August. December, 1915, he could not write to dictation, but copied writing as he would a design. He suddenly felt himself able to write in the Morse code (he was a telegrapher); then ordinary writing returned. February, 1916, however, he had forgotten what the Morse code was. In April, he was taught numbers. One day he would know left from right, but had forgotten it by evening.
A shocking case involving Mairet and Piéron showed a memory disorder. Association pathways were open one day and closed the next. After experiencing shell shock on September 18, 1915, he was found wandering in the woods a few days later, having completely lost his memory, even of his name. By November, he had recovered his last name but not his first name. With some stimulation, he was able to remember his city, his father, the street, and similar details. Soon, he could retrieve his memories more quickly; after a week, it only took him 35 seconds to remember he was born in Paris. However, his memories of the Trocadero and the Eiffel Tower, which had come back to him in November 1915, were lost again in April 1916, only to return once more in August. In December 1915, he couldn’t write from dictation but could copy writing like it was a drawing. Suddenly, he found he could write in Morse code (since he was a telegrapher); then regular writing returned. By February 1916, though, he had forgotten what Morse code was. In April, he was taught numbers. One day he would know left from right, but by evening he had forgotten.
Shell-explosion: Comrade killed: Amnesia.
Shell explosion: Comrade killed: Amnesia.
Case 449. (Gaupp, April, 1915.)
F. K., a 23-year old soldier, in civil life a turner, of Polish descent, and of a somewhat nervous and easily excitable disposition, early in August went from Strassburg into the Vosges and Lorraine. On the 26th a number of shells exploded near him. The troop was excited and took refuge in a cellar. K.’s best friend was torn to pieces by a shell. When his body was removed, K. felt sick and lost consciousness. He arrived at the clinic in Tübingen in a stuporous condition, by hospital train, on August 31, 1914. He walked weakly to his bed, supported by two men, and lay in the bed, apathetic and reacting to questions only with a stare. Things put in his mouth were swallowed. He remained motionless.
F. K., a 23-year-old soldier who worked as a turner in civilian life and is of Polish descent, has a somewhat nervous and easily excitable personality. Early in August, he left Strassburg for the Vosges and Lorraine. On the 26th, several shells exploded nearby. The troop panicked and took shelter in a cellar. K.'s best friend was killed by a shell. When his friend’s body was taken away, K. felt nauseous and lost consciousness. He arrived at the clinic in Tübingen in a dazed state by hospital train on August 31, 1914. He weakly walked to his bed, supported by two men, and lay there apathetically, responding to questions only with a blank stare. He swallowed whatever was placed in his mouth but remained completely still.
Next evening he answered a low Yes to a nurse’s question about eating. A little afterwards he said he supposed he was a prisoner in the enemy’s country. A little later he got properly oriented but still did not know how he had come. September 2, however, he was much clearer and said he had awakened out of a long dream. There was a complete amnesia, however, from the moment when he went to help remove the torn body of his friend up to September 1. Memories became clearer for the period before the shell explosion. The patient became very lively, talking vividly of war experiences, imitating shell hissing with an expression of intense anxiety, getting accustomed to battle scenes, saying that he was now seeing everything again as if real. He remained anxious for some days, complaining of weight on his chest and of feelings of internal restlessness and tension.
The next evening, he quietly replied "Yes" to a nurse's question about eating. A little while later, he mentioned that he thought he was a prisoner in enemy territory. Soon after, he managed to get his bearings but still didn’t know how he had ended up there. However, on September 2, he became much clearer and said he felt like he had just woken up from a long dream. He experienced complete amnesia from the moment he went to help remove the torn body of his friend until September 1. Memories from before the shell explosion started to come back more clearly. The patient became very animated, vividly discussing his war experiences, mimicking the sound of shells whistling with a look of intense anxiety, and saying that he was now seeing everything again as if it were real. He remained anxious for several days, complaining about a heavy feeling in his chest and sensations of internal restlessness and tension.
Amnesia for the period of August 26 to September 1 remained; all that K. could add to the story of those days was that he had been thrown sidewise for some distance by the air pressure of the shell.
Amnesia for the period from August 26 to September 1 remained; all that K. could add to the story of those days was that he had been thrown sideways for some distance by the air pressure of the shell.
From September 6 onwards, he grew calmer but he was still very labile, given to lively imaginings and emotion. By the middle of September he was well and discharged for garrison duty.
From September 6 onward, he became calmer, but he was still very unpredictable, prone to vivid daydreams and strong emotions. By the middle of September, he was doing well and was released for garrison duty.
Shell-explosion: Recurrent amnesia.
Shell explosion: Recurrent amnesia.
Case 450. (Mairet and Piéron, July, 1915.)
A man, 33, had suffered shell-shock early in December, 1914. His intervening history is not reported, but he showed on admission to the service of Mairet and Piéron, May 5, 1915, a remarkable amnesia. There was a complete cutaneous anesthesia, anosmia, and ageusia, and he was mute. He lived only in the specious present. His previous life was completely abolished for him. He could dress himself, eat, use a fork and spoon, and a glass. He understood ordinary words; such words as man, woman, day and night, however had no meaning. He was observed for 15 months and presented four phases.
A 33-year-old man had experienced shell shock in early December 1914. His history during the time is not documented, but when he was admitted to the care of Mairet and Piéron on May 5, 1915, he displayed significant amnesia. He had complete skin numbness, loss of smell, and loss of taste, and he was unable to speak. He existed only in the present moment. His past life was entirely erased for him. He was capable of dressing himself, eating, and using a fork, spoon, and glass. He could understand basic words; however, words like man, woman, day, and night held no meaning for him. He was observed for 15 months and went through four phases.
In phase one, there was a measure of success in reëducation, such that he grew able to recognize a few persons, to find his bed, and name objects. He was got to copy writing, to learn the alphabet, and to say a few words. He could not write from dictation, however. Less than two seconds after looking at an A, he had forgotten how it looked and could not trace it. This first phase lasted about two months.
In the first phase, there was some success in reeducation. He was able to recognize a few people, find his bed, and name certain objects. He could copy writing, learn the alphabet, and say a few words. However, he couldn't write from dictation. Less than two seconds after seeing an A, he had forgotten how it looked and couldn't trace it. This first phase lasted about two months.
The second phase began with fatigue, headaches, and the rather quick effacement of all he had relearned. If an errand was given him to do, he would run to do it before he should forget it; but if the trip required more than 4 or 5 seconds, he had to stop, not knowing what to do with the thing in his hands. He was still able to recognize 4 or 5 persons, but could add no more to his repertoire; and when one of them had been absent for a fortnight, he did not recognize him on his return. He could not remember the time for his meals.
The second phase started with tiredness, headaches, and quickly forgetting everything he had relearned. If he was given a task, he would rush to complete it before he forgot; but if the task took more than 4 or 5 seconds, he would have to stop, unsure of what to do with the item in his hands. He could still recognize 4 or 5 people, but he couldn’t add anyone new to that list; and if one of them was gone for two weeks, he wouldn’t recognize them when they came back. He couldn’t remember when it was time to eat.
The third phase was ushered in by improvement after vomiting; his speech came back in a feeble voice, November 16, 11 months after the shock. Reëducation could now be undertaken again. He easily relearned a number of things, feeling the greatest astonishment at his new acquirements as to the sun and the moon, the trees and the flowers, and the like. He expressed a curiosity to see his own home,[637] but when he went thither, he could recognize nothing. He wanted to get back home, namely to the hospital where he had lived all his life; where, in fact, he had been born from the psychic point of view.
The third phase started with improvement after vomiting; his speech returned in a weak voice on November 16, 11 months after the shock. He could now begin reeducation again. He quickly relearned a number of things, feeling the greatest amazement at his new understanding of the sun and the moon, the trees and the flowers, and similar things. He showed interest in seeing his own home,[637] but when he got there, he couldn't recognize anything. He wanted to return home, meaning the hospital where he had spent his entire life; where, in fact, he had been born from a psychological perspective.
At this time began the fourth phase, April, 1916—a phase of decline once more, in which a large portion of his acquisitions were again lost and he fell back to his condition in the second phase.
At this point, the fourth phase began, April 1916—a phase of decline again, where he lost a significant part of his gains and returned to his state from the second phase.
See discussion under Case 353 and under Case 367. Re confusional mental states, Roussy and Lhermitte, after distinguishing stuporous confusion from simple confusion, go on to differentiate what they call obtusion (see also discussion under Case 353). These authors say that Régis, in common with most psychiatrists, fails to distinguish the slow thinking and amnesia of true mental confusion from the temporal and the spatial disorientation that characterize the so-called obtusion. Of course, in all attacks of confusion, both attention and memory are affected, but there are special types in which attention defects and memory defects stand out in relief. The first of these types is the aprosexic type with birdlike movements, described by Chavigny (see for an example, Case 446). This aprosexia may be combined with mutism, deafness, or convulsions. The form of confusional disease in which amnesia is the out-standing feature is due to toxic or infectious disease, or is a Korsakow phenomenon, i.e., in the psychiatry of peace times; but the war has brought out amnestic confusion in other states than the toxic, infectious, and alcoholic states (Régis, Chavigny, Dumas, Roussy and Lhermitte). The amnesia may be incomplete, a sort of dysmnesia, or twilight memory, but as a rule, the amnesia is lacunar. The toxic and infectious amnestic confusions have a loss of memory for events following the onset, but these war cases of amnestic confusion have the loss of memory running back far into the patient’s past, slipping from the mind his name, his parentage, age, and vocation. Instead of being like the toxic confusional amnesia, an anterograde amnesia of fixation, the Shell-shock amnesia is apt to be antero-retrograde. These antero-retrograde amnesias, whether due to emotion or to[638] strong physical shock, may sometimes leave in sharp relief the recollection of the shock or event itself which initiated the amnesia. Meanwhile the patient does not forget automatic actions of dressing, reading, writing, and the like. The amnesia may be very selective, imitating aphasia, word blindness, letter blindness, agraphia, and the like. All this is part of the hallucinatory form of mental confusion which Régis describes as oniric delirium (see for oniric delirium, discussion under Case 333).
See discussion under Case 353 and under Case 367. Regarding confusional mental states, Roussy and Lhermitte, after distinguishing stuporous confusion from simple confusion, go on to differentiate what they call obtusion (see also discussion under Case 353). These authors argue that Régis, like most psychiatrists, does not distinguish the slow thinking and memory loss of true mental confusion from the time and space disorientation that defines the so-called obtusion. Of course, in all cases of confusion, both attention and memory are affected, but there are specific types in which attention defects and memory defects are particularly noticeable. The first of these types is the aprosexic type with birdlike movements, described by Chavigny (see for an example, Case 446). This aprosexia can be combined with mutism, deafness, or convulsions. The form of confusional disorder characterized by significant memory loss is usually due to toxic or infectious diseases, or is a Korsakow phenomenon, i.e., in the psychiatry of peacetime; however, the war has caused amnestic confusion in states beyond toxic, infectious, and alcoholic cases (Régis, Chavigny, Dumas, Roussy and Lhermitte). The amnesia may be incomplete, resembling dysmnesia or twilight memory, but typically, the amnesia is lacunar. The toxic and infectious amnestic confusions involve a memory loss for events following the onset, while these wartime cases of amnestic confusion experience memory loss that extends far back into the patient's past, erasing their name, parentage, age, and occupation. Unlike the toxic confusional amnesia, which is an anterograde amnesia of fixation, the shell-shock amnesia tends to be antero-retrograde. These antero-retrograde amnesias, whether caused by emotional distress or strong physical shock, may sometimes highlight the memory of the shock or event that triggered the amnesia. Meanwhile, the patient does not forget automatic activities like getting dressed, reading, writing, and similar tasks. The amnesia can be highly selective, mimicking aphasia, word blindness, letter blindness, agraphia, and so on. All of this is part of the hallucinatory form of mental confusion that Régis describes as oniric delirium (see for oniric delirium, discussion under Case 333).
Lépine distinguishes amongst the confusions, five forms as follows: Simple confusion, hallucinatory confusion, acute delirium, stuporous confusion (under which Lépine also considers the battle hypnosis of Milian, see Case 365, and Roussy’s narcolepsy), and amnestic confusion. All these phenomena from the clinical point of view are connected with an acute and fleeting insufficiency of the most delicate or, as it were, psychic portions of the cerebral cortex, the delirium, so to speak, being activity of the unconscious, whereas a confusion is due to a clouding of the centre O of Grasset’s polygon.
Lépine identifies five types of confusion: Simple confusion, hallucinatory confusion, acute delirium, stuporous confusion (which includes Milian's battle hypnosis, see Case 365, and Roussy’s narcolepsy), and amnestic confusion. From a clinical perspective, all these phenomena are linked to a temporary and acute deficiency in the most sensitive or, in a way, psychological areas of the cerebral cortex. Delirium can be seen as activity from the unconscious, while confusion arises from a clouding of the center O of Grasset’s polygon.
Soldier’s heart, both neurotic and organic.
Soldier's heart, both anxious and alive.
Case 451. (MacCurdy, July, 1917.)
A territorial, 19, who had enlisted in January 1914, reached France in September, 1916. He was of neurotic make-up (night terrors, fear of dark, giddiness in high places, fear of tunnels, enuresis until 10 years, worry about seminal emissions), and had always had a tendency to short wind. Enlisting at 16, he found it hard carrying his pack at first but soon grew stronger. The trench life was distasteful. He began to wish that he might be killed, or at all events removed from the trenches. Pains developed under the heart, with shortness of breath, palpitation, dizziness, and faint feelings. The man connected these heart symptoms with what he called his weakness of gall bladder (namely, enuresis). He was several times sent off duty for heart treatment. After three months in and out of hospital, he got trench foot, was sent to England, and transferred to a special heart hospital. Here the pulse test was positive, in that the rate did not diminish as it normally does after two minutes’ rest. After graduated exercises for several months, the pulse test had become negative and the heart had gradually improved from the organic standpoint. The patient, however, insisted that his heart trouble was as bad as ever, and was probably consciously hoping that his symptoms might persist.
A 19-year-old soldier, who enlisted in January 1914, arrived in France in September 1916. He had a neurotic personality (suffered from night terrors, was afraid of the dark, felt dizzy in high places, feared tunnels, dealt with bedwetting until he was 10, and worried about wet dreams) and had always struggled with shortness of breath. He enlisted at 16 and initially had a hard time carrying his pack but eventually got stronger. Life in the trenches was unpleasant. He started to wish he could be killed or, at the very least, taken out of the trenches. He developed chest pains, shortness of breath, heart palpitations, dizziness, and faint feelings. He connected these heart symptoms to what he referred to as his gallbladder issues (specifically, his bedwetting). He was sent off duty several times for heart treatment. After three months of being in and out of the hospital, he got trench foot and was sent to England, where he was transferred to a specialized heart hospital. There, the pulse test came back positive because his heart rate didn’t decrease as it usually does after two minutes of rest. After several months of graduated exercises, the pulse test became negative and his heart gradually improved from an organic perspective. However, the patient insisted that his heart problem was just as bad as ever and likely hoped that his symptoms would continue.
Re soldier’s heart, Abrahams classifies cases that come to the military surgeon for heart symptoms as (a) functional fatigue cases; (b) nicotine and drug cases; (c) organic heart disease and Graves’ disease; (d) the true soldier’s heart, occurring in men with a neurasthenic soil that lose control of the vasomotors and inhibitors of the heart.
Re soldier’s heart, Abrahams categorizes the cases that arrive at the military surgeon for heart symptoms as: (a) cases of functional fatigue; (b) cases related to nicotine and drugs; (c) cases of organic heart disease and Graves’ disease; and (d) true soldier’s heart, which occurs in men with a predisposition to neurasthenia that lose control of the heart's vasomotor functions and inhibitors.
Soldiers heart, neurotic.
Neurotic soldier's heart.
Case 452. (MacCurdy, July, 1917.)
An Australian gunner, 35, of a neurotic make-up (night terrors; horror of blood; fear of thunderstorms, high places, tunnels, horses; shy with both sexes), benefited by military training physically, but remained as neurotic as ever. On the way to his first service in Egypt, he feared shipwreck, and in Egypt was troubled by the weather and occasional palpitations and sinking feelings. He was transferred to the French front, May, 1916. He was terrified and depressed under shell fire, and horrified by blood. Peculiar sinking sensations or feelings that the soul was leaving the body came to him as he was going off to sleep; from which he woke at times with sudden starts. Later he had nightmares of things, mainly shells, falling on him. He worried, wanted death, and thought of suicide. In May, 1917, he was blown off his feet by a shell. Thereafter he began to feel that shells were being especially aimed at him, and four days later got a pain in the side, and began to tremble and breathe with difficulty, as if his throat were swelled up and he were going to choke. He ascribed this to gas. The bombardier finally sent him back to a hospital, where he grew weaker and screamed aloud on being awakened by his dreams. After six weeks in a special heart hospital, all the symptoms cleared up except the choking feelings and fear of instant death. Organically the man appeared normal. An initial pulse of 96 ran up to 168 after exercise, and down to 84 after two minutes’ rest.
An Australian gunner, 35, with a neurotic disposition (nightmares; fear of blood; anxiety around thunderstorms, heights, tunnels, and horses; awkward with both genders), gained physical benefits from military training, but remained just as neurotic as before. On his way to his first deployment in Egypt, he was anxious about shipwrecks, and while in Egypt, he struggled with the weather and experienced occasional heart palpitations and feelings of dread. He was moved to the French front in May 1916. There, he was terrified and depressed under shellfire and horrified by blood. He often felt a strange sinking sensation or the sense that his soul was leaving his body as he drifted off to sleep, waking suddenly at times. Later, he suffered nightmares about things, mostly shells, falling on him. He was anxious, wished for death, and had thoughts of suicide. In May 1917, a shell blast knocked him off his feet. Afterward, he began to feel that shells were being specifically targeted at him, and four days later, he developed a pain in his side, started trembling, and had difficulty breathing, feeling as if his throat was swollen and he might choke. He blamed this on gas. The bombardier eventually sent him back to a hospital, where he became weaker and screamed when awakened from his dreams. After six weeks in a specialized heart hospital, all symptoms cleared up except for the choking sensations and fear of imminent death. Physically, the man seemed normal. His initial pulse of 96 rose to 168 after exercise, then dropped to 84 after two minutes of rest.
Re soldier’s heart, Abrahams speaks of sundry hypotheses that he regards as erroneous. Soldier’s heart has been thought to be (a) athlete’s heart; others regard it as (b) a toxemic condition, possibly of bacterial origin; (c) hyperthyroidism (a larval form of Graves’ disease has been incriminated); (d) excessive cigarette smoking; and (e) deficiency of buffer salts in the blood, have been proposed by other authors.
Re soldier's heart, Abrahams discusses several theories that he believes are incorrect. Soldier's heart has been considered to be (a) athlete's heart; some see it as (b) a toxemic condition, possibly caused by bacteria; (c) hyperthyroidism (a preliminary stage of Graves’ disease has been blamed); (d) excessive cigarette smoking; and (e) a lack of buffer salts in the blood have been suggested by other authors.
Gallavardin has especially studied the tachycardial cases revealed by the war, cases in which auscultation is frequently unable to detect aught. These tachycardiacs are often hypertensive. Sedentary service should be found for them.
Gallavardin has particularly focused on the tachycardia cases exposed by the war, where listening with a stethoscope often fails to reveal anything significant. These patients with tachycardia are often also hypertensive. They should be assigned to sedentary roles.
Re pulse 168 after exercise, Gallavardin found 8 per cent of 500 non-organic and non-tuberculous cases to run up from 150 to 175 (125 to 150 in 27 per cent; 100 to 125 in 37 per cent; 75 to 100 in 26 per cent; 50 to 75 in 2 per cent).
Re pulse 168 after exercise, Gallavardin discovered that 8 percent of 500 cases that were non-organic and non-tuberculous increased from 150 to 175 (125 to 150 in 27 percent; 100 to 125 in 37 percent; 75 to 100 in 26 percent; 50 to 75 in 2 percent).
Re cardiac neuroses, Brasch points out that cardiac neuroses in the male in war time have found a strange new association with hyperesthesia of the skin. The patients showed dermatographia and hyperreflexia. The hyperesthetic zones of Head and Mackenzie were found by Brasch in all cases of organic cardiac disease, but also in two cases of cardiac neurosis in hysterics.
Re cardiac neuroses, Brasch notes that cardiac neuroses in men during wartime have developed an unusual connection with heightened sensitivity of the skin. The patients exhibited skin writing (dermatographia) and overreactive reflexes (hyperreflexia). Brasch discovered the hyperesthetic areas identified by Head and Mackenzie in all instances of organic heart disease, and also in two cases of cardiac neurosis in hysterical patients.
Moore calls attention to somewhat similar phenomena in the somatic group of nervous and depressed cases found in the war. These patients are fatigued, exhausted, sleepless, tremulous, vascular, and cardiac cases, with dermatographia, areas of paresthesia, and pains in the neighborhood of wound scars.
Moore points out somewhat similar issues in the group of nervous and depressed cases that emerged from the war. These patients are fatigued, worn out, sleepless, shaky, have vascular and cardiac problems, with skin writing, areas of unusual sensations, and pain near their wound scars.
War Strain; Shell-shock: Hysteria (question of malingering).
War Strain; Shell Shock: Hysteria (issue of faking).
Case 453. (Myers, March, 1916.)
A sergeant, 32, with 11 years’ service and eight months’ service in France, was admitted to a base hospital for inquiry as to possible malingering. It seems that he had taught in an army school for seven years before the war. He found heavy marches in France too much for him and fainted in the retreat from Mons and during the fighting on the Aisne, where he had reported sick for dysentery. The field ambulance where he was treated was near the shell fire, and a shell knocked him into a ditch. The ambulance had to move to a cave. Thereafter the patient suffered from tremor when spoken to or when watched. After discharge, he was employed as a dispatch rider on a motor cycle, but after three months lost his nerve for this work and took charge of fatigue parties. He found the work too much for him. He had been a total abstainer. Finally the malingering charge was brought up.
A 32-year-old sergeant with 11 years of service and 8 months in France was admitted to a base hospital for evaluation regarding possible malingering. He had taught at an army school for seven years before the war. He struggled with heavy marches in France, fainting during the retreat from Mons and while fighting on the Aisne, where he reported sick with dysentery. The field ambulance where he was treated was close to the shell fire, and a shell threw him into a ditch. The ambulance had to relocate to a cave. After that, the patient experienced tremors when spoken to or observed. After being discharged, he worked as a motorcycle dispatch rider, but after three months, he lost his confidence in that role and led fatigue parties instead. He found that work to be too demanding. He had always been a total abstainer. Eventually, the charge of malingering was raised.
The patient was nervous, delicate-looking, with widely dilated pupils, prominent eyeballs, tremor of right arm, and pulse of 102. The tremor was markedly lessened when he was alone, and was somewhat under control. He felt that his memory was defective, and tests demonstrated the defect.
The patient was anxious and looked fragile, with widely dilated pupils, bulging eyes, a tremor in his right arm, and a pulse of 102. The tremor significantly decreased when he was by himself and was somewhat manageable. He believed his memory was impaired, and tests confirmed the impairment.
In hospital patient slept better, the pupils grew smaller, the pulse rate diminished. There was a reduction in sensibility to pain over the right side of the head and body and over the right limbs. A prick of the right arm or leg was described as a finger touch. There was also almost complete hemi-anosmia and complete hemi-ageusia on the right side. Visual acuity was diminished on the right, and there was general limitation of right field; left-sided vision and field normal.
In the hospital, the patient slept better, the pupils got smaller, and the pulse rate slowed down. There was a decreased sensitivity to pain on the right side of the head and body as well as in the right limbs. A prick on the right arm or leg felt like just a light touch. There was also nearly complete loss of smell and complete loss of taste on the right side. Visual acuity was reduced on the right, and there was a general limitation in the right visual field; vision and field on the left side were normal.
After a month in hospital at home and two months’ leave, the patient was discharged no longer physically fit for service. He is now weak physically and mentally, subject to[643] severe headaches, and tremulous, especially in the right arm, when tired.
After a month in the hospital at home and two months off, the patient was discharged no longer fit for service. He is now weak both physically and mentally, experiencing[643] severe headaches and trembling, especially in his right arm, when he gets tired.
Re malingering, Sicard denies the existence of unconscious malingerers (presumably regarding this phrase as a figure of speech in relation to hysteria), and divides malingering into a creative and an acquired form. The simulateur de création assumes attitudes and symptoms to attract attention or pity; the simulateurs de fixation having been sick in the beginning, perpetuate their disease, in brief, crystallize their neuroses. The fixateur may be very realistic in all this, seeing that he has known from his own experience what a real disease is. The formula runs: The simulateur de création improvises; the simulateur de fixation repeats.
Re malingering, Sicard rejects the idea of unconscious malingerers (presumably viewing this phrase as a metaphor related to hysteria) and categorizes malingering into two types: creative and acquired. The simulateur de création adopts behaviors and symptoms to gain attention or sympathy; the simulateurs de fixation, having initially been genuinely ill, prolong their condition, essentially solidifying their neuroses. The fixateur can be very convincing in this, as he has firsthand knowledge of what a real illness feels like. The distinction is: The simulateur de création improvises; the simulateur de fixation repeats.
According to Mott, malingering in the form of an assumed Shell-shock is not uncommon amongst soldiers, and is rather hard to distinguish from a neurosis developing on the basis of an idée fixe.
According to Mott, pretending to have shell shock is not unusual among soldiers, and it's quite difficult to tell apart from a neurosis that develops based on a fixed idea.
Ballet’s definition of simulation is “a subjective or objective disorder which the patient invents with the idea of voluntarily and consciously misleading the observer.” Closely related to simulation is exaggeration or prolongation, conscious or intentional, of a real disorder. Babinski states that cases of genuine simulation are very rare, and that the subject under suspicion should be given the benefit of the doubt. Especially the word simulation, or similar words, should not be uttered in the presence of the patient. Practically speaking, psychotherapy applied as in cases of hysteria may often cure the simulator and the exaggerator.
Ballet defines simulation as "a subjective or objective disorder that the patient creates with the intention of voluntarily and consciously misleading the observer." Closely related to simulation is the exaggeration or prolongation, whether conscious or intentional, of a real disorder. Babinski notes that cases of genuine simulation are very rare, and that the person under suspicion should be given the benefit of the doubt. In particular, the word simulation, or similar terms, should not be mentioned in the patient's presence. In practice, psychotherapy, used in cases of hysteria, can often cure both the simulator and the exaggerator.
The officer who could not kick.
The officer who couldn't kick.
Case 454. (Mills, January, 1917.)
An officer had had a bullet in the right calf, of which nothing was evident months later but small scars of entrance and exit. Nevertheless he complained of pain, especially after walking, and of inability to dorsiflex the foot beyond a certain point. No wasting could be found and no impairment of sensation. The muscles were faradically normal. Mills thought the symptoms were exaggerated and so remarked to the officer.
An officer had a bullet wound in his right calf, which months later showed only small entrance and exit scars. However, he complained of pain, especially after walking, and couldn't lift his foot upwards past a certain point. There was no muscle wasting or loss of sensation. The muscles responded normally to electrical stimulation. Mills thought the officer was exaggerating his symptoms and mentioned this to him.
Under anesthesia, however, the dorsiflexion also proved to be impossible, and after exerting considerable force, Dr. Dunhill was able to rupture a massive fibrous band of adhesions that had prevented extension. The officer made a good recovery.
Under anesthesia, however, the ability to bend the foot upwards was also impossible, and after applying a lot of force, Dr. Dunhill managed to break a huge fibrous band of adhesions that had been blocking extension. The officer recovered well.
Dr. Mills confessed his error to the officer who had naturally resented the suggestion of malingering. The officer forgave him.
Dr. Mills admitted his mistake to the officer, who understandably took offense at the idea of faking illness. The officer forgave him.
Re malingering, Moore states that no diagnosis of malingering should be made without the most careful examination and consideration of the individual as such, on account of the fact that the erroneous diagnosis dejects the patient and postpones recovery. It is particularly unwise to term the trouble “imaginary,” or to talk about “suggestion” or use similar terms in the presence of the patient.
Re malingering, Moore says that no diagnosis of malingering should be made without thorough examination and consideration of the individual, because an incorrect diagnosis can discourage the patient and delay recovery. It's especially unwise to label the issue as “imaginary,” or to mention “suggestion” or similar terms in front of the patient.
Craig has found very few cases of actual malingering and states that tremors and paroxysms are often mistaken therefor. Bispham remarks that few malingerers are found among the patients of a doctor who is known to be a thorough examiner.
Craig has encountered very few instances of actual malingering and notes that tremors and sudden episodes are often confused with it. Bispham points out that there are typically few malingerers among patients of a doctor known for being a meticulous examiner.
Re orthopedic cases like Case 454, Gleboff remarks upon the simulation of joint affections and upon methods of surprising the malingerers into sudden movements made in obedience to request in the course of medical examination.
Re orthopedic cases like Case 454, Gleboff comments on the imitation of joint disorders and on techniques for catching malingering patients off guard with sudden movements prompted by requests during medical exams.
Doubtful accounts by patient concerning arm palsy: Incorrect diagnosis of simulation.
Doubtful accounts by the patient regarding arm paralysis: Incorrect diagnosis of a simulation.
Case 455. (Voss, November, 1916.)
A volunteer, 18, just before the war had a fall in which apparently he injured his skull. In December, 1914, he hurt his left forearm. About this injury he sometimes said he fell in a storming attack in a trench and broke his arm, and again he said his arm had been smashed by stones from a falling house. From that time forward there was paralysis of the left forearm with flexor contracture. May, 1915, slight hypesthesia could be demonstrated on the ulnar side of the arm, suggesting ulnaris injury. There were, however, no considerable electrical changes.
A volunteer, 18, had a fall just before the war that seemingly injured his skull. In December 1914, he hurt his left forearm. He sometimes mentioned that he fell during a storming attack in a trench and broke his arm, while at other times he claimed his arm was crushed by falling stones from a collapsing house. From then on, he experienced paralysis in his left forearm with flexor contracture. By May 1915, slight numbness was observed on the ulnar side of the arm, indicating possible ulnar nerve injury. However, there were no significant electrical changes.
Six months later the man was sent up with a suspicion of simulation. In the meantime the contracture had resolved and there was a typical hysterical paralysis with all signs of neurosis. Six months later he was well enough to be examined for military service.
Six months later, the man was sent up with a suspicion of faking. In the meantime, the contracture had resolved and he exhibited typical hysterical paralysis with all the signs of neurosis. Six months later, he was healthy enough to be examined for military service.
Here was a case in which the incorrect data offered by the patient himself as to the origin of his paralysis gave rise to the suspicion of simulation, whereas, as a matter of fact, the man was clearly hysterical.
Here was a situation where the wrong information provided by the patient about the cause of his paralysis raised suspicion of faking, while in reality, the man was obviously hysterical.
Re incorrect data supplied by the patient to his own disadvantage, Lumsden remarks on the great difficulty of diagnosis in cases where hysteria and malingering have been combined, and Morselli states that, if the doctor has really made up his mind that the man is shamming, he should send him back to the fighting line at once.
Re incorrect data provided by the patient to his own detriment, Lumsden notes the significant challenge of diagnosing cases where hysteria and feigning are mixed, and Morselli mentions that if the doctor is convinced the man is faking, he should immediately send him back to the front lines.
Forearm wound: Hysterical edema?
Forearm wound: Severe swelling?
Case 456. (Lebar, July, 1915.)
A corporal, 26, formerly a farmer, was struck in the forearm by a shell fragment on the mid-portion of the radial border. The wound was slight (the fragment entering and emerging hardly 2 cm. apart) but bled profusely, according to the patient, who was evacuated next day but one to a hospital in the interior. By this time the right hand was swollen, nor could any movement of hand or fingers be made. Massage, mechanotherapy, passive movements did no good.
A 26-year-old corporal, who was previously a farmer, was hit in the forearm by a shell fragment on the middle part of the radial side. The injury was minor (the fragment entered and exited less than 2 cm apart) but bled heavily, according to the patient, who was evacuated to a hospital inland the day after next. By then, the right hand was swollen, and he was unable to move his hand or fingers at all. Massage, mechanotherapy, and passive movements were ineffective.
The man entered the neurological center of the Eighth Region, July 7, 1915, when there were already a few skin changes with dorsal thinning and palmar thickening. There was cutaneous anesthesia not only of hand and fingers but of the forearm to the elbow, and this anesthesia included heat and cold. Position sense was preserved. There was no evidence of atrophy except for the skin changes. An electrical examination showed normal conditions.
The man arrived at the neurological center of the Eighth Region on July 7, 1915, when there were already some skin changes, including thinning on the back and thickening on the palms. He experienced loss of feeling in not just his hands and fingers, but also in his forearms up to his elbows, and this loss included sensitivity to temperature. His sense of position was intact. There were no signs of muscle wasting except for the skin changes. An electrical examination indicated normal conditions.
July 13, a sealed bandage was put on, but at the end of five days the hand looked as before. July 19, a new treatment was announced to the patient. With a hot needle a number of pricks were made on the dorsal surface of the hand and a few c.c. of fluid were withdrawn (containing a slight amount of albumin and a few lymphocytes), whereupon a dry bandage was put on. The next day a few finger and thumb flexion movements could be made and sensation had returned. Sensation completely returned July 21. The flexion movements were still incomplete, by reason of the edema and dryness of the skin. However, July 22, flexion was better and the swelling had gone down sixty per cent. Jacquet’s biokinetic treatment (active gymnastics of the hand and fingers) was given for four hours. July 25, the edema had greatly diminished and normal motion had returned.
On July 13, a sealed bandage was applied, but after five days, the hand looked the same. On July 19, a new treatment was proposed to the patient. A heated needle was used to make several pricks on the back of the hand, and a small amount of fluid was withdrawn (which contained a little albumin and some lymphocytes), after which a dry bandage was put on. The next day, a few movements of the fingers and thumb could be made, and sensation had come back. By July 21, sensation was fully restored. The flexion movements were still limited due to swelling and dry skin. However, by July 22, flexion improved, and the swelling had reduced by sixty percent. Jacquet’s biokinetic treatment (active exercise for the hand and fingers) was administered for four hours. By July 25, the swelling had significantly decreased, and normal movement had returned.
Examination excluded renal disease. There was no sign indicating phlegmon. Quincke’s disease had other features.[647] Fraudulent application of a bandage might be considered, but the course of the disease under sealed conditions seems to exclude this hypothesis also. May it, therefore, not be a case of hysterical edema?
Examination ruled out kidney disease. There were no signs pointing to phlegmon. Quincke’s disease presented different characteristics.[647] The possibility of a fraudulent bandage application could be considered, but the progression of the illness under controlled conditions also seems to eliminate this theory. Could it then be a case of hysterical edema?
Re hysterical edema, see remarks under Case 407. In the case above, of Lebar, Babinski calls attention to the fact that the edema and the contracture diminished though they did not entirely disappear after the scarifications. This physical treatment did not act, according to Babinski, wholly as a matter of suggestion, and he fears that some cases of so-called hysterical edema are really cases of physiopathic vasomotor disorder; in fact, three of the cases published (and amongst them, the present case of Lebar), were cases of edema associated with contracture and developing in an injured limb. To prove a case of anything to be hysterical is, of course, according to the Babinski school, to submit it to a therapeutic test and cure it by suggestion.
Re hysterical edema, see remarks under Case 407. In the case of Lebar, Babinski points out that the edema and the contracture lessened, even though they didn’t completely go away after the scarifications. According to Babinski, this physical treatment did not work solely through suggestion, and he worries that some instances of so-called hysterical edema are actually cases of physiopathic vasomotor disorder; in fact, three of the cases that were published (including the current case of Lebar) involved edema linked to contracture and occurring in an injured limb. According to the Babinski school, proving a case to be hysterical means putting it to a therapeutic test and treating it through suggestion.
Shell splinters in head: Suspicion of (a) simulation, (b) hysteria. Case actually surgical.
Shell fragments in the head: Suspected of (a) faking, (b) hysteria. The case is actually surgical.
Case 457. (Voss Water, November, 1916.)
A man, injured by shell fragments in the head and sustaining fracture of both arms and a thigh, got well of his wounds, but fell into a nervous state with headache and dizziness. He was given prolonged observation psychiatrically and then sent back to the front as fit for service, but was shortly returned to hospital and sent to Cologne under the suspicion of simulation.
A man who was hurt by shell fragments in the head and had fractures in both arms and a thigh recovered from his wounds but developed a nervous condition with headaches and dizziness. He underwent extended psychiatric observation and was then deemed fit for service and sent back to the front, but soon returned to the hospital and was sent to Cologne under suspicion of faking his condition.
The picture was of unilateral increase of tendon reflexes, accelerated pulse, disorder in the intake of ideas, difficulty in finding words and delayed associations. His gait suggested a psychogenic disorder. X-ray showed two shell fragments in the vault of the skull.
The image showed one-sided increases in tendon reflexes, a faster pulse, issues with processing ideas, trouble finding words, and delayed associations. His walking indicated a psychological disorder. X-rays revealed two shell fragments in the upper part of the skull.
According to Voss, it is a sad fact that victims of skull injuries are frequently charged with simulation or exaggeration. In the above instance, moreover, this charge was undoubtedly inaccurate.
According to Voss, it's unfortunate that people with skull injuries are often accused of faking or exaggerating their condition. In this case, in particular, that accusation was definitely wrong.
Re simulation, see remarks under Case 453. Re neurological cases, the Neurological Society of Paris sent to the War Ministry a special note pointing out how tardy was the reference of sundry neurological cases to the special neurological service. They pointed out how important it was to send to these special services all cases of bullet and shrapnel lesions.
Regarding simulation, see remarks under Case 453. Regarding neurological cases, the Neurological Society of Paris sent a special note to the War Ministry highlighting how delayed the referral of various neurological cases to the specialized neurological service was. They emphasized the importance of sending all cases of bullet and shrapnel injuries to these specialized services.
Re the malingering question, there is a wide divergence of opinion, even amongst experienced workers in the same city. The late Professor Dejerine said he had not seen a single case of malingering. In fact, he thought that malingering amongst soldiers and amongst injured industrial workers had been much exaggerated. Marie, however, working in the examination of many surgical cases, found malingering relatively common. Amongst forty of his cases, he regarded at least nine as malingerers or exaggerators.
Re the malingering question, there are a lot of differing opinions, even among experienced workers in the same city. The late Professor Dejerine mentioned that he hadn't seen a single case of malingering. In fact, he believed that malingering among soldiers and injured industrial workers had been greatly exaggerated. Marie, however, who examined many surgical cases, found malingering to be relatively common. Out of forty of his cases, he considered at least nine to be malingerers or exaggerators.
“Sciatica,” torticollis, stiff arm: The desire to avoid active service plus functional disease.
“Sciatica,” torticollis, stiff arm: The wish to dodge active duty along with a physical ailment.
Case 458. (Collie dog, January, 1916.)
A man enlisted September, 1914, went to France after six months’ training, immediately put himself on sick list, and was admitted to a base hospital: Diagnosis, sciatica. Later, he ceased complaining of sciatica and developed spastic torticollis. He was sent back to England, was treated with radiant heat and so on, and was eventually sent to the Royal Bath Hospital at Harrowgate.
A man signed up in September 1914, went to France after six months of training, immediately put himself on the sick list, and was admitted to a base hospital. The diagnosis was sciatica. Later, he stopped complaining about sciatica and developed spastic torticollis. He was sent back to England, treated with radiant heat and other methods, and was eventually sent to the Royal Bath Hospital in Harrogate.
He recovered from torticollis after six weeks’ treatment; but then developed a spasmodic contracture of the right shoulder and forearm. He was massaged for this and also given high frequency treatment. Then came two transfers (massage).
He recovered from torticollis after six weeks of treatment; but then developed a spasmodic contraction in his right shoulder and forearm. He received massages for this and was also given high-frequency treatment. Then came two transfers (massages).
Early in December, 1915, he came under Collie’s observation. He then showed right wrist bent at right angles to the forearm; hand tightly clenched, so firmly that it seemed as if the wrist were ankylosed. The case was obviously a functional one. The man refused to enter hospital at Collie’s suggestion. He was sent to the Maida Vale Hospital. Previously he tried to persuade the medical officer that further hospital treatment was unnecessary, stating that he was now able to straighten his arm and that he was applying a splint to keep it straight. He progressed slowly in the institution. Told, if he would recover within fourteen days, he would be classified “for home service only”—before the fourteen days were up, he had suspended his weight on a trapeze and pulled himself up to his chin on it; had also lifted a 28-lb. weight with his paralyzed hand. In short, he wholly recovered. He is now doing duty with his unit.
Early in December 1915, he came to Collie’s attention. He displayed a right wrist that was bent at a right angle to the forearm, with his hand tightly clenched, making it seem like the wrist was fused. It was clearly a functional issue. The man refused to go to the hospital at Collie’s suggestion and was sent to Maida Vale Hospital instead. He had previously tried to convince the medical officer that he didn’t need further hospital treatment, claiming he could now straighten his arm and was using a splint to keep it straight. He made slow progress at the hospital. He was told that if he recovered within fourteen days, he would be classified as “for home service only.” Before the fourteen days were up, he had suspended his weight on a trapeze and pulled himself up to his chin on it. He also lifted a 28-pound weight with his paralyzed hand. In short, he made a full recovery and is now serving with his unit.
Collie says this is not deliberate malingering but a mixture of functional disease and an obvious desire to avoid active service. When he appeared before the board for a final decision, there was a tendency to assume the old[650] paralyzed position until he was sharply called to order, when his arm assumed normal position.
Collie says this isn't intentional faking but a combination of real health issues and a clear wish to avoid active duty. When he showed up before the board for a final decision, he initially fell into his usual frozen posture until he was firmly directed to behave, at which point his arm returned to a normal position.
Conclusion: The direct personal treatment of his mental condition and an appeal to his lower instincts were immediately curative and of much more value than the radiant heat or high frequency treatment.
Conclusion: Direct personal attention to his mental state and appealing to his basic instincts were instantly effective and much more valuable than the radiant heat or high-frequency treatments.
Re Collie’s case, Russel finds surprisingly large numbers of malingerers; he found many at the time of the battles at Loos. It was particularly easy in cases of epilepsy to demonstrate a close relation between hysteria and malingering. In the psychogenesis of these conditions, Russel emphasizes the initial element of deception, which soon enormously increases either through the patient’s convictions of his ability to deceive or through a process of autosuggestion. Cases of semi-malingering are not uncommon. In England, Russel found more cases of a clearly psychogenic nature; yet in these, also, there was always primarily an element of deception.
Re Collie's case, Russel discovers surprisingly high numbers of people pretending to be ill; he found many during the battles at Loos. It was particularly easy to show a close connection between hysteria and feigning illness in cases of epilepsy. In understanding how these conditions develop, Russel highlights the initial factor of deception, which often grows significantly, either through the patient's belief in their ability to deceive or through a process of autosuggestion. Cases of mild malingering are fairly common. In England, Russel found more clearly psychogenic cases; however, in these instances as well, there was always primarily an element of deception.
Yes-No test of value re anesthesia.
Yes-No test of value for anesthesia.
Case 459. (Mills, January, 1917.)
The “Yes-No” test proved of special value in the case of an Australian private. Shortly after landing at Gallipoli this man had a bullet graze his ankle and fell some thirty feet over the bow of a ridge. He was picked up unable to move his legs and insensitive therein.
The “Yes-No” test turned out to be particularly useful for an Australian soldier. Soon after arriving at Gallipoli, this man was grazed by a bullet on his ankle and fell about thirty feet over the edge of a ridge. He was found unable to move his legs and felt no sensation in them.
The paraplegia and anesthesia lasted three months. “Fracture dislocation of the dorsal spine” was the diagnosis made, and laminectomy was even contemplated. The sphincter reflex was normal and there was no atrophy, no rigidity and no reflex disorder. Asked to say “no” when he could not feel a pin-prick and “yes” when he did feel it, he replied “no” to each prick to the anesthetic area and changed his reply to “yes” when the sensitive parts of the body were examined. At another time the answers were found not to correspond with those given before.
The paralysis and loss of feeling lasted three months. The diagnosis was “fracture dislocation of the dorsal spine,” and there was even talk of performing a laminectomy. The sphincter reflex was normal, and there was no muscle wasting, no stiffness, and no reflex issues. When asked to say “no” when he couldn't feel a pinprick and “yes” when he could, he responded “no” to each prick in the numb area and switched his answer to “yes” when sensitive parts of the body were tested. At another point, his answers were found to be inconsistent with those he had given earlier.
The soldier was assured that he would get well and that as soon as he could walk he would be boarded and returned to Australia.
The soldier was told he would recover and that as soon as he could walk, he would be put on a plane and sent back to Australia.
After a number of weeks he became able to walk.
After several weeks, he was able to walk.
Arabian fever.
Arabian craze.
Case 460. (Roussy, April, 1915.)
An Arab fell on his knee, one day in the trenches. A contracture of the left arm, with great pain, and a temperature of 38 to 40 degrees, with hemoptysis, developed. This man had been considered tuberculous. One day, however, the thermometer went up to 41 degrees. It was discovered that he took artificial means to push the mercury up, and that the spitting of blood was voluntary. All these phenomena disappeared after he was put in the guardhouse for 24 hours.
An Arab dropped to his knees one day in the trenches. He developed a cramp in his left arm, along with severe pain, and his temperature ranged from 100.4 to 104 degrees, accompanied by coughing up blood. This man had been thought to have tuberculosis. However, one day, his temperature shot up to 105.8 degrees. It was found that he was using tricks to raise the mercury, and that the coughing up blood was intentional. All these symptoms disappeared after he spent 24 hours in the guardhouse.
Shrapnel scratch of head: Hysterical amaurosis “?” On isolation in a dark room, the patient began to see light!
Shrapnel scratch of head: Hysterical amaurosis “?” In isolation in a dark room, the patient started to see light!
Case 461. (Briand and Cold, February, 1917.)
A man may seek to exaggerate an anomaly of his eye which had existed before the war, in order to live comfortably far from the front.
A man might try to amplify a problem with his eye that existed before the war, so he can comfortably stay away from the front lines.
A soldier sustained a slight scratch from a shrapnel bullet in front of the left ear, which scarred over in a few days. The soldier said, however, that the bullet had gone through his skull and a few hours after his wound said he could not see. Sent to the hospital he continued to say he was blind and finally brought up in an asylum for the blind near Lyons where he was taught to cane chairs and to write in Braille. This happened in July, 1915.
A soldier got a small scratch from a shrapnel bullet in front of his left ear, which healed in a few days. However, he claimed that the bullet had gone through his skull and a few hours after getting hurt, he said he couldn’t see. After being sent to the hospital, he kept insisting he was blind and was eventually placed in a blind asylum near Lyons, where he learned to weave chairs and write in Braille. This took place in July 1915.
In October he was sent to the Hospital at Quinze-Vingt where a diagnosis of hysterical amaurosis was made with a large interrogation point. He was then sent to Brequet where there was a section reserved for disciplinary cases and very nervous cases not wanting to get well, a service under the charge of Roubinowitch.
In October, he was sent to the Hospital at Quinze-Vingt, where they diagnosed him with hysterical amaurosis, leaving a lot of questions. He was then transferred to Brequet, which had a section specifically for disciplinary cases and very anxious patients who didn't want to get better, run by Roubinowitch.
The soldier escaped with a comrade and eventually reached Val-de-Grâce where the diagnosis of hysterical amaurosis was again made. Examinations several times showed that there was nothing abnormal about the eyes except that the eyelids presented habitual fibrillary movements (antebellum).
The soldier escaped with a buddy and eventually arrived at Val-de-Grâce, where they diagnosed him with hysterical amaurosis again. Multiple examinations revealed that there was nothing unusual about his eyes, except that his eyelids showed usual fibrillary movements (antebellum).
The eyelids passively opened, would remain open for a few minutes and then close. There was no winking of the eye to a light, yet the pupil preserved its reflex power.
The eyelids slowly opened, stayed open for a few minutes, and then closed. There was no blinking in response to the light, but the pupil still had its reflex response.
Vision was abolished, however, the soldier said. He was without any other motor or sensory disorder. Much sympathy was given to the poor blind soldier. People were much astonished when the chief of the ophthalmological service had the man isolated in a dark room. Three weeks later the man had begun to see the light a little. A week later[653] the eyes remained open without the necessity of having the lids raised by the fingers, and vision returned.
Vision was lost, however, the soldier said. He didn't have any other motor or sensory issues. A lot of sympathy was shown to the poor blind soldier. People were quite surprised when the head of the ophthalmology department had the man kept in a dark room. Three weeks later, he started to see light a bit. A week later[653] his eyes stayed open without needing to lift the lids with his fingers, and his vision returned.
Re amaurosis, Parsons explains the blindness which may remain after consciousness returns following Shell-shock, as a condition in which the lower visual paths are carrying on their functions normally. For example, the pupillary reactions are preserved. The condition is not unlike that found in amaurosis of uremia, and Parsons has found it in children with posterior basic meningitis. For Parsons, therefore, the block occurs in the higher centers above the thalamus, possibly in the synapses of the optic radiation fibers. Ormond states that the true cases of concussion blindness invariably pass through phases of great discomfort; whereas the malingerers are without such discomfort. Medical suggestion, also, has a powerful effect here, and may actually retard recovery.
Re amaurosis, Parsons describes the blindness that may persist after awareness returns following Shell-shock, as a condition where the lower visual pathways are functioning normally. For instance, the pupillary responses are intact. This condition is similar to what is seen in uremic amaurosis, and Parsons has observed it in children with posterior basic meningitis. Therefore, for Parsons, the blockage happens in the higher centers above the thalamus, possibly in the synapses of the optic radiation fibers. Ormond indicates that true cases of concussion-related blindness usually go through phases of significant discomfort; in contrast, those who are faking it do not experience such discomfort. Additionally, medical suggestion can have a strong impact here and may actually slow down recovery.
A newspaper cure.
A newspaper remedy.
Case 462. (Sicard, October, 1915.)
Sicard read in a French newspaper a story to the effect that, at two o’clock in the afternoon, a soldier had fallen on the sidewalk between Nos. 40 and 42 Boulevard de Liberté, in a nervous crisis. The people ran and picked him up. When he came to, he was very joyful, perceiving that the shock had given him back his speech, which he had lost the August previous. This soldier, the newspaper continued, became deafmute through the explosion of a bomb in a fight in Upper Alsace. “The brave soldier is most happy over the unexpected result.” The newspaper went on, “We congratulate him sincerely, as well as the people who assisted him.” He was the more contented that he had gotten well because, the soldier said, he would now be able to go back among his comrades to fight with the Boches!
Sicard read in a French newspaper a story stating that, at two o’clock in the afternoon, a soldier had collapsed on the sidewalk between Nos. 40 and 42 Boulevard de Liberté during a nervous breakdown. People rushed over and helped him up. When he regained consciousness, he was very happy to realize that the shock had restored his ability to speak, which he had lost the previous August. The newspaper continued, saying this soldier became deaf-mute due to a bomb explosion during a battle in Upper Alsace. “The brave soldier is extremely pleased with this unexpected outcome.” The newspaper added, “We sincerely congratulate him, as well as those who helped him.” He felt even happier about his recovery because, as the soldier said, he would now be able to return to his comrades and fight against the Germans!
Now, in point of fact, Sicard had dealt with this soldier the morning of the day in question. He had been simulating mutism for ten months, and finally told Sicard that he would like to leave that afternoon as he felt cure coming. Sometime after, he wrote a letter of profuse thanks for the benefits received, and said he did not deserve to avoid court-martial. He also said that he was going to do everything he could to justify himself. Incidentally, he kept his word and an officer in his regiment later gave him an enthusiastic recommendation.
Now, in fact, Sicard had spoken with this soldier the morning of the day in question. He had been pretending to be mute for ten months, and finally told Sicard that he wanted to leave that afternoon as he felt a recovery coming on. After some time, he wrote a letter expressing his gratitude for the help he received and mentioned that he didn’t think he deserved to avoid court-martial. He also stated that he would do everything he could to prove himself. By the way, he kept his promise, and an officer in his regiment later gave him a glowing recommendation.
Re malingering, see discussion concerning simulateurs de création and simulateurs de fixation under Case 453.
Re malingering, see the discussion about creation simulators and fixation simulators under Case 453.
Deafmutism: Explained by patient as malingering.
Deafmutism: Described by the patient as faking it.
Case 463. (Myers, September, 1916.)
A pure malingerer, of set purpose, initiates a quasipathological condition which he will discard when he has gained his end or when he is assured that he is unobserved. Malingering in the field of speech is rare. A private, 26, one year in service, three months in France, entered a base hospital, deafmute for nine weeks. He wrote: “I should be very happy if you can do anything for me. I cannot give a very clear account of what happened, as it is sometime since. I remember retiring from Hill —— with some more to some trenches, and in the open we were shelled and I lost touch with our chaps or else they were killed. I remember a great concussion and finding myself on the ground, and a soldier dragged me up and we ran for the trench. I was very thirsty and I ran down the trench to get some water. I met one of our chaps and tried to ask him for some, and I could not make him understand. He only smiled at me. The man who picked me up took me to an officer who was sitting on the edge of the trench and tried to make me understand, and then he sent me with this man to a dressing station, and from there I have been to different places, the names of which I do not know, except the last place, No. — Convalescent Camp. I have been there about two months——”
A complete faker, with a clear purpose, creates a nearly pathological condition that he will drop once he gets what he wants or is sure no one's watching. Faking in communication is uncommon. A private, 26, one year into his service, and three months in France, ended up in a base hospital, unable to speak or hear for nine weeks. He wrote: “I’d be really grateful if you could help me. I can’t give a clear account of what happened since it’s been a while. I remember retreating from Hill —— to some trenches, and out in the open, we were shelled, and I lost contact with my buddies or they were killed. I remember a loud blast and then found myself on the ground, and a soldier pulled me up and we ran to the trench. I was really thirsty and dashed down the trench to get some water. I ran into one of my guys and tried to ask him for some, but he didn’t understand me. He just smiled at me. The man who picked me up took me to an officer sitting on the trench's edge and tried to help me understand, and then sent me with this man to a medical station, and from there I’ve been to several places, which I don’t know the names of, except the last place, No. — Convalescent Camp. I’ve been there for about two months——”
He seemed anxious to get well. He could not understand what was said. Induced anesthesia caused no phase of excitement, and the patient failed to regain his speech. He was evacuated to England. Three months later the patient thence wrote the following confidential letter from a Convalescent Home.[656] “Sir,—I regret very much to inform you that I was imposing upon you.——I may state that I was physically unfit for the Front.——During the whole time of training my pay was chiefly spent in tonics and drugs, but I kept going as I was determined to see what it was like at the Front.——I have written this——that your ‘notes’ on cases will not suffer any detrimental effect through my imposture.——I have not got my discharge yet, but shall stick out for it. I ‘speak’ but do not ‘hear’ very well.—” He was in two hospitals for functional nervous disorders in England, but in neither institution was he regarded as a malingerer.
He seemed eager to recover. He couldn't understand what was being said. The anesthesia didn't cause any excitement, and the patient didn't regain his ability to speak. He was taken to England. Three months later, the patient wrote the following confidential letter from a rehabilitation center.[656] “Sir,—I regret to inform you that I’ve been deceiving you.——I may say that I was physically unfit for active duty.——Throughout my training, most of my pay went towards tonics and medications, but I kept pushing through because I was determined to experience what it was like at the front.——I’m writing this so that your ‘notes’ on cases won’t be negatively affected by my deception.——I haven’t received my discharge yet, but I’m going to fight for it. I can ‘speak’ but don’t ‘hear’ very well.—” He was in two hospitals for functional nervous disorders in England, but he wasn’t seen as a malingerer in either place.
Re hysteria explained by the patient as malingering, Chavigny discusses what he calls sursimulation. The physician must not fall into a permanent state of suspicion, and especially must not reveal his suspicions to the accused or to the bystanders. Chavigny quotes a French soldier whose letter to his wife was intercepted, stating that he was going to feign deafmutism to secure his discharge. Before he had succeeded in doing so, however, he suffered Shell-shock, and got a true hysterical deafmutism, which showed no signs of malingering whatever.
Re hysteria explained by the patient as faking, Chavigny discusses what he calls sursimulation. The physician must not become permanently suspicious, and especially should not disclose his suspicions to the accused or to observers. Chavigny quotes a French soldier whose letter to his wife was intercepted, in which he stated that he was going to pretend to be deaf and mute to get his discharge. However, before he managed to do so, he experienced Shell-shock and developed actual hysterical deafmutism, which showed no signs of faking at all.
Deafmutism: Appearance of malingering.
Deafmutism: Signs of faking it.
Case 464. (Myers, September, 1916.)
A stretcher bearer was seen by Lt.-Col. Myers two days after admission to a base hospital. Stolid looking and mute, he had nevertheless talked in his sleep, had written a few words about “shells coming over,” and understood what was said to him. Lt.-Col. Myers’ notes run, “He puts out his tongue and closes his eyes and holds out one hand when I ask him to do so, but gets stupid (as if sulky) when I ask for the other hand. He will not hear any more. Next day quite deaf, and the following day light anesthesia with ether caused a return of hearing and of speech, with repetition of syllables to request on the way to deeper anesthesia. On awaking he cried as he was induced to resume his speech, and complained of pains in the head.
A stretcher bearer was observed by Lt.-Col. Myers two days after being admitted to a base hospital. He appeared stoic and silent, yet he had spoken in his sleep, written a few words about “shells coming over,” and was aware of what was being said to him. Lt.-Col. Myers’ notes state, “He sticks out his tongue and closes his eyes while holding out one hand when I ask, but becomes unresponsive (almost sulky) when I request the other hand. He will not hear any more. The next day he was completely deaf, and the day after that, light anesthesia with ether allowed him to regain both hearing and speech, along with repeating syllables as requested on the way to deeper anesthesia. Upon waking, he cried as he was encouraged to speak again and complained of headaches.
“Two days later, he seemed normal and said that he could have spoken on the second day, but that his eyes and ears had begun to swim, that he had felt dizzy, and was afraid to talk. He did not want to be sent back to the trenches. There had been severe shelling. He had lost consciousness until he awoke in a hospital at Y—. He recalled, little by little, how he had been taken back by a corporal to a cellar. He said he wanted to go back, but wanted a rest first. He went back to his unit and was reported as having done well for four months.”
“Two days later, he seemed fine and said that he could have talked on the second day, but his eyes and ears started to feel fuzzy, he felt dizzy, and was scared to speak. He didn’t want to be sent back to the front lines. There had been heavy shelling. He had lost consciousness until he woke up in a hospital at Y—. He slowly remembered how a corporal had taken him back to a cellar. He said he wanted to return, but needed a break first. He went back to his unit and was reported to have performed well for four months.”
There was a certain suggestion of malingering about the admission of the lad that he could have spoken before he was induced to do so. According to Lt.-Col. Myers, a number of patients upon recovery of speech are apt falsely to believe that they have been malingering. Functional disorders may simulate malingering.
There was a hint of faking about the boy’s claim that he could have spoken before he was encouraged to do so. According to Lt.-Col. Myers, many patients who regain their speech often mistakenly think they were faking. Functional disorders can mimic faking.
Lannois and Chavanne warn against the suggestions given to malingerers and to hysterics by the statements on the tickets of admission borne by the patients for transfer, e.g. “incurable deafness.” These authors found 11 per cent malingerers amongst 262 cases of labyrinthine shock.
Lannois and Chavanne caution against the advice given to fakers and hysterics based on the information on the admission tickets carried by patients for transfer, e.g. “incurable deafness.” These authors discovered that 11 percent were fakers among 262 cases of labyrinthine shock.
Simulation of deafmutism.
Simulation of deaf-muteness.
Case 465. (Gradenigo, March, 1917.)
A soldier in the mountain artillery acted like a deafmute. He was unable to read or write. It was reported that he had been wounded, but no evidence of wound could be found. The man had a low forehead and a furtive glance, his whole impression being that of a criminal.
A soldier in the mountain artillery acted like he couldn’t hear or speak. He couldn’t read or write. It was said that he had been injured, but there was no sign of any injury. The man had a low forehead and a shifty look, giving off an overall impression of a criminal.
The only evidence of disease found was inflammation with perforation of the tympanic membrane of the left ear. Deep in the left auditory meatus was found a grain of crushed oats! The man’s speech difficulty was of a stuttering nature, but he stuttered in a different way at every test. He was unwilling to be narcotized. Finally by a process of scolding and cajoling, the man was made to confess that he could both hear and speak well. The peculiar stuttering early led to the diagnosis of simulation, but the fact that the tympanic membrane was not anesthetic, and that there was no anesthetic zone in the body strengthened the suspicion—to say nothing of the refusal of narcosis and the general behavior of the somewhat criminal-looking soldier.
The only sign of illness found was inflammation along with a tear in the eardrum of the left ear. Deep in the left ear canal was discovered a grain of crushed oats! The man had a speech problem that was characterized by stuttering, but his stutter varied with each test. He was reluctant to be sedated. Eventually, through a mix of scolding and persuading, the man admitted that he could hear and speak normally. The unusual stuttering initially suggested that he was faking, but the fact that the eardrum wasn’t numb and there was no numb area in the body added to the suspicion—especially considering his refusal of sedation and his overall behavior, which made him seem somewhat suspicious.
A lame rascal.
An annoying troublemaker.
Case 466. (Gilles, April, 1917.)
An infantryman, 28, had an equinovarus, for which he was evacuated, hospitalized, given treatment, sent home for convalescence, and declared unfit for service. He was, however, sent back to the front, and on arrival, went lame; whereupon the regimental surgeon sent him to a nerve center. The equinovarus was there but it was nothing but a simple contracture without pain, atrophy, sensory, reflex, electrical, or X-ray disorders.
An infantryman, 28, had a clubfoot, which led to his evacuation, hospitalization, treatment, and a period of recovery at home before being declared unfit for service. However, he was sent back to the front, and upon arrival, he became lame; as a result, the regimental surgeon referred him to a nerve center. The clubfoot was still present, but it was just a simple contracture without any pain, muscle wasting, sensory, reflex, electrical, or X-ray issues.
The abductor muscles were stimulated by electricity and the foot straightened. He was kept under observation for a time, was lame no longer, and was sent back to his regiment.
The abductor muscles were stimulated with electricity and the foot straightened. He was monitored for a while, was no longer lame, and was sent back to his regiment.
However, sometime later he was evacuated again to the same neurological center, stating that he did not know why. There was no longer any varus or anything abnormal. The rascal had enjoyed the game of going lame and had prevailed upon his officers to evacuate him. He then saw that he was found out and pretended that he had been forcibly evacuated.
However, sometime later he was evacuated again to the same neurological center, claiming that he didn’t know why. There was no longer any varus or anything abnormal. The troublemaker had enjoyed pretending to be lame and had convinced his officers to evacuate him. He then realized he had been caught and pretended that he had been forcibly evacuated.
Mother love and jaundice.
Mother's love and jaundice.
Case 467. (Briand and Haury, January, 1916.)
A soldier, 19½, entered the central psychiatric service at Val-de-Grâce, having been evacuated from a hospital in Paris, suspect of having brought about a picric acid jaundice. He had been undergoing treatment in this hospital, when the physician who had isolated him found that he was getting picric acid in packages secreted in his képi.
A 19½-year-old soldier was admitted to the central psychiatric service at Val-de-Grâce after being evacuated from a hospital in Paris, suspected of causing picric acid jaundice. He had been receiving treatment in this hospital when the doctor who was monitoring him discovered that he had picric acid hidden in packages inside his képi.
It seems that the soldier lived with his mother, and enlisted when he was not yet 18. He proved to be as good a soldier as he was workman, and came through the campaign without wound or disease. Accordingly, in December, 1915, he got a six-day leave. His mother, who loved him well, and of whom he was the sole support, had much regretted his enlisting. She was sick with some stomach disease and, after he enlisted, she told everybody that she was going to die and that it was his fault. So, when he came on leave the next day, she asked him to take a powder so he might stay a fortnight. She did not tell him the name of the drug; only told him how to take it in a small paper, swallowing it with a little water. She said he would become yellow and that he would get a supplementary leave. Three days after his return to the front, the boy took three of the ten powders; took the same number three or four days later; and the others five or six days later. He soon had jaundice with colic and diarrhea, and apparently was exempted from service for a few days. He had returned to the front hardly a month when his mother died and the boy got another six-day leave for the funeral. He took ten fresh doses of picric acid while at Paris, and was put into hospital by a physician without suspicion. His relatives thought he was suffering from a recurrent jaundice. When the story was told, the boy confessed to the family, and said that he had taken the drug in the first place only to please his mother. It is harder to explain the second trial, since he talked about the compassion and sense of obedience he felt to his dead mother. It is probable that he simply wanted a prolonged leave at Paris.
The soldier lived with his mother and joined the army before he turned 18. He turned out to be as skilled a soldier as he was a worker and got through the campaign without any injuries or illnesses. So, in December 1915, he received a six-day leave. His mother, who loved him dearly and depended on him for support, had deeply regretted his decision to enlist. She suffered from a stomach illness and, after he joined, she told everyone she was going to die and that it was his fault. When he came home on leave the next day, she asked him to take a powder so he could stay for two weeks. She didn’t tell him what the drug was called; she just explained how to take it in a small paper, swallowing it with some water. She said it would make him jaundiced and that he would get an extra leave. Three days after returning to the front, he took three of the ten powders; he took the same amount again three or four days later, and the rest five or six days after that. He soon developed jaundice along with colic and diarrhea, and he was apparently excused from service for a few days. He had barely been back at the front for a month when his mother passed away, and the boy received another six-day leave for the funeral. While in Paris, he took ten new doses of picric acid and was admitted to a hospital by a doctor who had no suspicions. His relatives thought he was dealing with recurring jaundice. When the story came out, the boy confessed to his family, saying he had taken the drug initially to please his mother. It’s harder to explain the second time he did it, as he talked about the compassion and sense of duty he felt toward his deceased mother. It’s likely that he just wanted an extended leave in Paris.
Re malingering, Blum speaks of fictitious jaundice as having received the name of La Carotte (the carrot) from the soldiers. Blum gives a partial list of instances of simulation as follows:
Re malingering, Blum talks about fake jaundice being called La Carotte (the carrot) by the soldiers. Blum provides a partial list of examples of simulation as follows:
SIMULATION
SIMULATION
(Blum, December, 1916)
Blum, December 1916
False angina, from irritating solution.
Fake angina, from irritating solution.
Gastric disorder. Oil and tobacco (with tachycardia or jaundice) (use ipecac).
Gastric disorder. Oil and tobacco (with rapid heartbeat or yellowing of the skin) (use ipecac).
Diarrhea. (Isolate.)
Diarrhea. (Isolate.)
Diarrheal stools imitated by a mixture of urine and water.
Diarrhea looked like a mix of urine and water.
Dysenteric stools imitated by the addition of fat pork and bits of raw meat.
Dysentery-like stools created by adding fatty pork and pieces of raw meat.
Appendicitis. Complaint of pain at the well-known McBurney point.
Appendicitis. Complaint of pain at the famous McBurney point.
Tape worm. Carriers supply others.
Tapeworm. Carriers infect others.
Jaundice. (Smoke mixture of antipyrin and tobacco; drink tobacco juice. Ingest picric acid.)
Jaundice. (Smoke a mix of antipyrin and tobacco; drink tobacco juice. Take picric acid.)
Hemoptysis. Irritation of throat surfaces with a needle.
Hemoptysis. Irritation of throat surfaces with a needle.
Albuminuria. Eat kitchen salt to excess in a bowl of milk. Edema and albumin disappear on surveillance. Albumin injected into bladder.
Albuminuria. Consume too much table salt in a bowl of milk. Swelling and albumin clear up after monitoring. Albumin is injected into the bladder.
Diabetes. Phloridzin, or oxalate of ammonia. Glucose added to urine.
Diabetes. Phloridzin, or ammonia oxalate. Glucose added to urine.
Incontinence. (Difficult to prove fraudulent. True incontinence in middle of night. Simulated, just before waking.)
Incontinence. (Hard to prove fraud. Real incontinence happens in the middle of the night. Simulated, just before waking.)
Skin diseases:
Skin conditions:
Erythema. Herbs.
Redness. Herbs.
Eruptions. Mercury, arsenic, iodine, bromide.
Eruptions. Mercury, arsenic, iodine, bromine.
Herpes. Euphorbiacae.
Herpes. Euphorbiaceae.
Eczema. Rubbing with slightly warmed thapsia. Rubbing excoriated skin with acids, Croton oil, bark of garou, sulphur, oil of cade, mercurial pomade.
Eczema. Rubbing with slightly warmed thapsia. Rubbing irritated skin with acids, Croton oil, garou bark, sulfur, cade oil, and mercurial ointment.
Impetigo. With cantharides plaster and pomade stibiée.
Impetigo. With cantharides plaster and stibnite ointment.
Intertrigo. (In the infantry.)
Intertrigo. (In the military.)
Hyperidrosis of feet. Prolonged hot baths. Hot foot baths with excoriation, followed by scratching and covering with linen soaked in urine.
Hyperhidrosis of feet. Long hot baths. Hot foot baths with skin irritation, followed by scratching and covering with linen soaked in urine.
Edema of legs. Constriction.
Swollen legs. Tightness.
(In Lombardy, cases due to introduction of equisetum arvense, an astringent herb, by fingers and toes, followed by energetic rubbing.)
(In Lombardy, cases caused by the introduction of equisetum arvense, astringent herb, through fingers and toes, followed by vigorous rubbing.)
Recurrent wounds. (Cover with wax sealed bandages.)
Recurring injuries. (Cover with wax-sealed bandages.)
Abscesses. Introduction of septic material. A thread soiled with tartar from teeth is drawn through the skin. Characteristic odor of resulting abscess.
Abscesses. Introduction of infected material. A thread dirty with plaque from teeth is passed through the skin. Distinctive smell of the resulting abscess.
Phlegmons. Subcutaneous introduction of turpentine or petrol.
Phlegmons. Injecting turpentine or petrol under the skin.
Paraffine tumors. (Apply heat.)
Paraffin tumors. (Apply heat.)
Sprain. A stopper is put under the heel; or compress the leg with bandages to stop circulation and knock below repeatedly and forcibly. Edema and ecchymosis follow.
Sprain. A stopper is placed under the heel, or wrap the leg with bandages to restrict circulation and hit below repeatedly and forcefully. Swelling and bruising follow.
Conjunctivitis. Ipecac, pepper, septic or fecal materials. Pupillary dilatation has been produced by introduction of a belladonna grain under the eyelid daily.
Conjunctivitis. Ipecac, pepper, septic or fecal materials. Pupillary dilation has been achieved by placing a belladonna grain under the eyelid every day.
Ears. Running at the ears produced by placing urine or chemical product in the ear.
Ears. Putting urine or a chemical product in the ear can cause ear problems.
Emaciation and pallor. Ingestion of a large amount of vinegar. Abuse of strong tobacco.
Extreme thinness and paleness. Consuming a lot of vinegar. Misuse of heavy tobacco.
Muscular weakness. Arsenious acid in eggs. Voluntary lead and mercurial intoxications.
Muscle weakness. Arsenic acid in eggs. Intentional lead and mercury poisoning.
Epilepsy. Absence of pupillary reflex to light and pupillary dilatation, insensibility of nasal mucosa and modifications of pulse persistent after the attack is over cannot be imitated.
Epilepsy. Lack of pupillary response to light and dilated pupils, numbness of the nasal mucosa, and changes in pulse that continue after the attack has ended cannot be faked.
Fever. Striking elbows against walls to elevate the mercury in the thermometer. Take temperature by rectum.
Fever. Banging elbows against walls to raise the mercury in the thermometer. Check temperature rectally.
Bites. One simulator had a fork with twisted teeth to produce the effect.
Bites. One simulator had a fork with twisted prongs to create the effect.
Intra-abdominal projectiles. Bullet swallowed.
Intra-abdominal projectiles. Swallowed bullet.
Swelling of hand and forearm, seven months.
Swelling of the hand and forearm for seven months.
Case 468. (Léri and Roger, September, 1915.)
A soldier was wounded September 22, 1914, at Charleroi by a bullet in the forearm. He came under observation May 14, 1915, with a huge edema of forearm and hand, suddenly stopping at the elbow, an elastic edema, especially marked in the palm, which was restored to its smooth contour very quickly after being compressed by the fingers, and very like an elephantiasis. The hand was in a position of moderate extension on the forearm, with fist clenched. There was a linear ecchymotic line at the upper edge of the zone of edema, especially on the antero-internal face.
A soldier was injured on September 22, 1914, at Charleroi by a bullet in the forearm. He was observed on May 14, 1915, with a large swelling in his forearm and hand that suddenly stopped at the elbow, a soft swelling that was particularly noticeable in the palm and quickly returned to a smooth shape after being pressed by the fingers, resembling elephantiasis. The hand was moderately extended on the forearm, with the fist clenched. There was a linear bruise along the upper edge of the swollen area, especially on the front inner side.
According to the soldier’s own story, the swelling had begun a fortnight after the injury. He said that a very tight moist dressing had been applied during the first few days.
According to the soldier’s own account, the swelling started two weeks after the injury. He mentioned that a very tight, wet bandage had been put on in the first few days.
The patient was cared for by massage, and then by local baths. He was anesthetized in December and several drains were inserted; no result. In January he was chloroformed again and two long incisions were made along the internal border of the supinator longus and along the ulnar border of the forearm. He was better for two weeks after this second operation, but then grew worse.
The patient received treatment through massage and local baths. In December, he was put under anesthesia and several drains were placed, but there was no improvement. In January, he was anesthetized again, and two long cuts were made along the inner edge of the supinator longus and along the ulnar side of the forearm. He felt better for two weeks after this second surgery, but then his condition declined again.
The diagnosis of syringomyelia was now made, based upon the appearance of the arm and upon some ill-defined hypesthesia. This diagnosis was not entertained by Léri and Roger who, when they obtained the patient, put him into a plaster cast up to the shoulder. The edema went down rapidly to normal. In short, it was here a question of a simulator, who was even willing to undergo surgical operations with general anesthesia.
The diagnosis of syringomyelia was now confirmed based on the appearance of the arm and some vague loss of sensation. Léri and Roger didn't accept this diagnosis. When they got the patient, they put him in a plaster cast up to the shoulder. The swelling quickly returned to normal. In short, this was a case of someone faking their condition, who was even willing to go through surgery under general anesthesia.
Re evading service, Gleboff’s classification is as follows: 1. False assertion of disease of (a) internal organs, (b) vision, (c) hearing, (d) joints. 2. Simulation of temporary disease of organs. 3. Mutilation of limbs.
Re evading service, Gleboff’s classification is as follows: 1. False claims of illness regarding (a) internal organs, (b) vision, (c) hearing, (d) joints. 2. Pretending to have a temporary illness of organs. 3. Injury to limbs.
A German shell-shy.
A German scared of shells.
Case 469. (Gaupp, April, 1915.)
Gaupp’s simulator had not been under shell fire. He said to his captain that he wanted to see his badly wounded brother (he had in fact no brother), and got a furlough on this ground. He then fled as far as possible from the front, into the interior, roved about for some days, falsely asserting that he was under dentist’s treatment.
Gaupp's simulator hadn’t been under artillery fire. He told his captain that he wanted to see his seriously injured brother (he actually didn't have a brother) and got a leave of absence on that basis. He then ran as far away from the front lines as he could, wandered around for a few days, and lied about being under dental treatment.
He was brought to Tübingen on the ground of mental derangement, on a hospital train, and was delivered to the clinic as a case of Shell-shock. This man’s state of excitement soon ended. As Gaupp could not make out his case clinically, he applied to the regiment and received in return court-martial papers. The man confessed that he had made false statements and fled because he was afraid of shells. Reproached with simulation, he preserved a shameful silence.
He was taken to Tübingen on the basis of mental instability, on a hospital train, and was handed over to the clinic as a case of shell shock. This man’s state of agitation quickly subsided. Since Gaupp couldn't understand his case clinically, he reached out to the regiment and received court-martial papers in response. The man admitted that he had lied and ran away because he was scared of the shells. When accused of faking his condition, he remained shamefully silent.
A fair exchange no robbery: France gets a simulator in an exchange with Germany of prisoners “unfit for service.”
A fair trade isn't stealing: France receives a simulator in a prisoner swap with Germany for those "unfit for service."
Case 470. (Marie, April, 1915.)
A French soldier arrived in France from Germany in a reciprocal exchange of prisoners supposed to be incapable of bearing arms. The man showed a paraplegia with clonic movements of exaggerated degree. He was rapidly “cured” after being placed in a military hospital, and disciplined. He proved to be a vulgar simulator.
A French soldier returned to France from Germany as part of a prisoner exchange program for those thought to be unfit for combat. The man had paralysis and severe involuntary movements. He was quickly “cured” after being admitted to a military hospital and receiving discipline. It turned out he was just pretending.
It was clear that the German physicians had made a gross error in diagnosis; but what, asks Marie, should be done with such a man, since he evidently should not be given a convalescent leave or a retirement? Should he be sent back to his dépôt?
It was obvious that the German doctors had made a serious mistake in their diagnosis; but what, Marie wonders, should be done with a man like that, since clearly, he shouldn't be granted a convalescent leave or retirement? Should he be sent back to his depot?
If a year’s treatment yields no results, Grasset suggests discharge with suitable gratuity.
If a year's treatment doesn't produce results, Grasset recommends discharging with an appropriate gratuity.
SIMULATION: Question of Quincke’s disease.
SIMULATION: Question about Quincke's disease.
Case 471. (Lewitus, May, 1915.)
An infantryman was brought to the eye department of the Wieden Hospital early in May, 1915, with a diagnosis (from the internists) of Quincke’s disease.
An infantryman was taken to the eye department of the Wieden Hospital early in May 1915, diagnosed (by the internists) with Quincke’s disease.
Under the conjunctiva of each globus oculi were countless small air vesicles. There was not the slightest emphysema of the eyelids or of the skin about the eyes. The skin in the neighborhood of the zygoma was thick, red and swollen; but no air could be demonstrated in the subcutaneous tissues on palpation. Next day the skin swelling and the conjunctival emphysema had disappeared. No communication of the orbits with the air spaces of the skull could be demonstrated nor was it possible to push air into the conjunctiva by nose-blowing. The fundi were both normal and vision was normal. Special rhinological examination showed the nose to be normal. It was the skin swelling of the orbital region that had given rise to the diagnosis of Quincke’s disease. The man had been then referred to the internists who could, however, find no evidence of disease whatever.
Under the conjunctiva of each eye were countless small air bubbles. There wasn’t the slightest sign of emphysema in the eyelids or the skin around the eyes. The skin around the cheekbone was thick, red, and swollen; however, no air could be felt in the subcutaneous tissue when pressed. The next day, the skin swelling and the conjunctival emphysema had disappeared. There was no connection between the eye sockets and the air spaces in the skull, nor could air be pushed into the conjunctiva by blowing the nose. The back of the eyes appeared normal, and vision was fine. A special examination of the nose showed it to be normal. It was the swelling of the skin around the eyes that had led to the diagnosis of Quincke’s disease. The man was then referred to internists, who found no evidence of any disease at all.
During the three months’ stay of the patient in the eye department, once more swelling of the left orbital region and air under the conjunctiva of the left globus oculi suddenly appeared one day, but disappeared over night. At this time small subconjunctival ecchymoses were found.
During the three-month stay of the patient in the eye department, swelling in the left orbital area and air beneath the conjunctiva of the left eye suddenly showed up one day but disappeared overnight. At that time, small subconjunctival bruises were observed.
This case must be regarded as one of simulation but produced in a manner unknown.
This case should be seen as a simulation, but it was created in a way that is not understood.
Bruises of head and back, not severe: “A case of pensionitis, a self-made neurasthenic for medicolegal purposes.”
Bruises on the head and back, not serious: “A case of pensionitis, a self-created neurasthenic for legal reasons.”
Case 472. (Collie dog, May, 1915.)
Sir John Collie remarks that sometimes one has to recommend a pension knowing that what amounts to a fraud is being perpetrated. A seaman, 25, got newspaper notoriety after receiving some not very serious bruises of head and back. Two months later, when seen by Sir John Collie, he was a victim of bent back. He was finally able to remove his clothes and put them on with some alacrity, although at first he declared he could not. Woebegone during examination, he was noted to laugh and gossip with strangers outside. A physician had diagnosticated it as an obscure spinal lesion, but as he was fit to work, he was sent back.
Sir John Collie notes that sometimes you have to recommend a pension even when you know it’s kind of a scam. A 25-year-old seaman got some media attention after suffering some minor bumps on his head and back. Two months later, when Sir John Collie saw him, he had a noticeably bent back. He eventually managed to take off his clothes and put them on fairly quickly, even though he initially claimed he couldn’t. Looking miserable during the examination, he was also seen laughing and chatting with strangers outside. A doctor had diagnosed him with a rare spinal issue, but since he was fit to work, he was sent back.
Forty-one days later he put himself on the sick-list again. Pluck and nerve were gone beyond recall, according to his physician. In hospital his appetite was good, he slept well, and he had no troubles except an hysterical loss of sensation. There followed 33 days in hospital, three weeks in a convalescent home, and return to work for a month. Unable to stoop or kneel for pain, he was thought organic.
Forty-one days later, he put himself on the sick list again. His doctor said his determination and strength were gone for good. In the hospital, he had a good appetite, slept well, and had no issues except for a hysterical loss of sensation. This led to 33 days in the hospital, three weeks in a recovery home, and then he went back to work for a month. Unable to bend or kneel because of pain, he was thought to have an organic issue.
Sir John found him without desire to get well, hysterical, and suffering “from pensionitis, a self-made neurasthenic for medico-legal purposes.” He was placed for four months in a nerve hospital. On leaving this hospital he was still in the bent-back position, and went into a pantomime display when asked to touch his toes. Four weeks in the convalescent home found the following: The attending physician now suggested locomotor ataxia as the correct diagnosis! Sir John Collie was asked to report finally as to the fitness for work. Well assured that the patient was really a malingerer, Sir John nevertheless certified him as permanently unfit for further service as a case of traumatic neurasthenia, venturing to predict that after receiving the pension, he would be at work within six months. He received the pension (25 s. a[667] week for life), and Sir John Collie’s ability at prediction was justified by his return to work, at the end of exactly six months.
Sir John found him with no desire to get better, hysterical, and suffering from "pensionitis," a self-imposed issue for legal reasons. He spent four months in a nerve hospital. When he left, he was still hunched over and put on a dramatic show when asked to touch his toes. After four weeks in the recovery home, the doctor suggested that he actually had locomotor ataxia! Sir John Collie was asked to give a final report on his fitness for work. Confident that the patient was just faking, Sir John nevertheless stated that he was permanently unfit for further service due to traumatic neurasthenia, boldly predicting that after getting the pension, he would return to work within six months. He received the pension (25 shillings a[667] week for life), and Sir John Collie's prediction was proven right when he went back to work exactly six months later.
Re malingerers, Glueck remarks that a malingerer, besides being a malingerer, is a worthless sort of person in any event, and calls attention to the fact that special stresses may reduce men to lower cultural levels, to which lying and deceit may be more appropriate. Glueck remarks that the lay mind does not readily appreciate that a man with mental disease may at the same time be a malingerer of additional mental symptoms. It may be added that the professional mind is sometimes equally slow to appreciate the fact.
Re malingerers, Glueck notes that a malingerer, apart from being a malingerer, is generally an undesirable person, and highlights that extreme stress can push individuals to lower cultural standards, where lying and deceit may seem more fitting. Glueck also mentions that people without specialized knowledge often struggle to understand that someone with a mental illness can also be faking additional mental symptoms. It can further be said that professionals are sometimes just as slow to recognize this reality.
Chart 14
SHELL-SHOCK
- GROUP I. EXHAUSTION
- (Alcoholism disrupts treatment)
- GROUP II. HEREDITY
- (Certain underprivileged recruits)
- GROUP III. MARTIAL MISFITS
- (Negative mindset)
After Farquhar Buzzard
After Farquhar Buzzard
Chart 15
NEUROSES AND PSYCHOSES OF WAR
- 1. NEUROSES
- Motor
- Sensory Experience
- 2. NEUROSES
- Sensory Experience
- Talk
- 3. NEURASTHENIA
- Hemichorea
- Graves' disease
- Trench Spine
- 4. PSYCHOSES
- Minor
- Gun-shy, Insomnia, Dreams, Phobias, Psychasthenia, Hypochondria
- Stupor, Fatigue, Severe Dementia
- Psychotic disorders (Civilian Forms)
After A. W. Campbell
After A.W. Campbell
D. TREATMENT AND RESULTS OF SHELL-SHOCK.
In previous sections we have already become acquainted with many therapeutic successes and failures: indeed it was almost necessary to detail treatment in certain cases to show the nature of the disease in hand or the correctness of a given diagnosis. In the present Section we approach the question more systematically.
In previous sections, we've already learned about various therapeutic successes and failures. In fact, it was almost essential to outline treatment in some cases to illustrate the nature of the disease at hand or the accuracy of a specific diagnosis. In this section, we will tackle the question more systematically.
After presenting a few examples of various spontaneous and non-medical recoveries, we bring into contrast the types of medical recovery that may be termed rapid (or miracle) cures and those that fall under the general head of reëducation. Admixed are cases of failure as well as of success: if it be remarked that the case method puts forward the best foot, it is probable that the same is true of almost any therapeutics as reported in early articles. As we go to press, trench reports indicate that at least one part of the profession is far more hopeful of successful psychotherapy even in the physiopathic group of disorders than their expounder, Babinski, could concede. The true statistical evaluation of the results must come years later.
After sharing a few examples of different spontaneous and non-medical recoveries, we contrast the types of medical recovery that can be called rapid (or miracle) cures with those that are generally categorized as re-education. Included are cases of both failure and success: while it's noted that the case method showcases the best outcomes, it's likely that this holds true for nearly any therapeutic approach as reflected in early articles. As we go to press, updates suggest that at least part of the profession is much more optimistic about successful psychotherapy, even in the physiopathic group of disorders, than Babinski, its leading proponent, would admit. The true statistical evaluation of the results will take years to emerge.
Some neuropsychiatrists have been fond of saying that there is nothing new in Shell-shock, that specialists have long been familiar with the psychoneuroses, etc. Yet in the past, specialists have not learned overmuch about the true inwardness of the psychoneuroses. Even a casual inspection of the various therapeutic efforts here described shows how much novelty of observation and ingenuity of plan must eternally be shown in these ever-so-simple psychoneuroses!
Some neuropsychiatrists have often claimed that there's nothing new about Shell-shock, and that specialists have long understood psychoneuroses, etc. However, in the past, specialists haven't really grasped the true complexities of these conditions. Even a brief look at the different treatment approaches described here reveals how much fresh insight and creative planning must always be applied to these seemingly straightforward psychoneuroses!
Shell-shock: Deafmutism. Spontaneous cure.
Shell shock: Deaf-mute. Spontaneous recovery.
Case 473. (Mott, January, 1916.)
A British soldier, 25, a coal miner, had had a bicycle accident five years before, after which he was unconscious for 2½ hours, and gave up work for five weeks, with headaches, fainting-fits, and nervousness ever after and with a tendency to imagine he could see things when there was nothing to be seen.
A 25-year-old British soldier, who worked as a coal miner, had a bicycle accident five years ago. After the accident, he was unconscious for 2½ hours and took five weeks off work. Since then, he has suffered from headaches, fainting spells, nervousness, and a tendency to imagine he sees things that aren’t there.
September 19, 1915, he was under shell fire in trench and dugout. A sergeant and three men working with him were killed by an explosion, and he remembers his cap being lifted off his head. He came to in 46 Rest Camp, some time later, unable to see clearly, or to hear or speak, and with headache and insomnia. He brought a paper from a hospital in France, saying, “Doctor, I had an awful dream last night again; I was dreaming that I was in the trenches; I could see the men falling and the great big shells exploding. I could see the light from the bursting of the shells very plain. They fairly lighted all the place up. I woke up very anxious I can tell you. I wish I could give over dreaming, and I keep having pains in my head right across my eyes.”
September 19, 1915, he was under heavy shell fire in the trench and dugout. A sergeant and three guys working with him were killed by an explosion, and he remembers his cap being blown off his head. He later woke up in 46 Rest Camp, unable to see clearly, or hear or speak, and suffering from a headache and insomnia. He brought back a note from a hospital in France that said, “Doctor, I had another awful dream last night; I dreamed I was in the trenches; I could see the men falling and the huge shells exploding. I could see the light from the bursts of the shells very clearly. They really lit up the whole place. I woke up very anxious, I can tell you. I wish I could stop dreaming, and I keep having these pains in my head right across my eyes.”
October 15, while sitting by himself outdoors, he felt a slight crackling in his head, noticed that he could hear sounds faintly, and in a few minutes he could hear fairly well.
October 15, while sitting alone outside, he felt a slight crackling in his head, noticed that he could hear sounds faintly, and within a few minutes, he could hear fairly well.
October 17, he was heard making inarticulate noises in his sleep. The corporal next him told him about the noises in his half drowsy state; he tried to speak and said, “Mother.” He then felt queer all over, with pain in his head, and afterward became able to talk very well with slight hesitation.
October 17, he was heard making strange sounds in his sleep. The corporal next to him mentioned the noises while he was still half asleep; he tried to respond and said, “Mother.” He then felt strange all over, with pain in his head, and later was able to talk quite clearly with just a bit of hesitation.
Re spontaneous cures, Elliot Smith and Pear cite the cure of two mutes on hearing that Roumania had entered the war, and the cure of another by seeing Charlie Chaplin’s antics. Some workers (for example, Aimé), treat the functional mutes by simply leaving them to themselves, and maintain that they secure numerous spontaneous recoveries, regarding these as superior to cures by isolation, psychotherapeutic treatment, and the like.
Regarding spontaneous cures, Elliot Smith and Pear mention the recovery of two mute individuals upon hearing that Romania had entered the war, and another person who was cured after watching Charlie Chaplin’s antics. Some practitioners (like Aimé) handle functional mutes by allowing them to be on their own, claiming that this approach leads to many spontaneous recoveries, which they believe are better than cures achieved through isolation, psychotherapy, and similar methods.
Chart 16
METHODS OF PSYCHOTHERAPY
- HYPNOSIS
- Verbal Prompt
- Focus
- Interest
- Various
- SUGGESTION (WAKING)
- Spoken
- Substance
- Equipment
- AUTOSUGGESTION
- DISTRACTION
- TERRORISM
- INFLICTION OF PAIN
- PERSUASION
- WILL TRAINING
- OCCUPATION THERAPY
- ISOLATION
- PSYCHOANALYSIS
Re mutism spontaneously or non-medically cured, see also cases 476, 480, 481, 482. For various medical methods of treatment, see, e.g., cases 516, 518, 520, 526, 544, 579.
Re mutism that was spontaneously or non-medically cured, see also cases 476, 480, 481, 482. For different medical treatment methods, see, e.g., cases 516, 518, 520, 526, 544, 579.
Mott had a case which had been mute more than six months, unable to whistle, phonate in coughing, or blow out a candle, though heard to shout in his sleep: This patient recovered his speech when pitched out of a punt on New Year’s Eve. The condition was in one sense physical enough, as the X-ray showed that the man’s diaphragm hardly moved even with the greatest effort. Mott regarded the inhibition of the breathing movements, especially the phonation, as caused by fear. Mott speaks of a case that recovered on being told by a comrade that he had talked in his sleep. The man was so astonished by this statement that he said, “I don’t believe it.” Other instances of cure under quasi natural conditions are related by Mott: In the presence of a functional mute, Mott speaks loudly to the patient’s sister so that the patient may hear: “This man must be kept on a No. 1 diet, and when he can ask loud enough for you to hear, he can have a bottle of stout and a mutton-chop.” Several mutes are reported to have gotten well the next day under this treatment.
Mott had a patient who hadn’t spoken in over six months, unable to whistle, cough, or blow out a candle, though he could be heard shouting in his sleep. This patient regained his speech after being thrown out of a boat on New Year’s Eve. The issue was quite physical, as X-rays indicated that the man's diaphragm barely moved even with significant effort. Mott believed that the lack of breathing movements, especially when it came to speaking, was due to fear. He mentions a case where a patient recovered after being told by a friend that he had talked in his sleep. The man was so surprised by this that he said, “I don’t believe it.” Mott recounts other instances of recovery under nearly natural conditions: when he was with a silent patient, he spoke loudly to the patient’s sister so the patient could hear: “This man needs to stick to a No. 1 diet, and when he can ask loudly enough for you to hear, he can have a bottle of stout and a mutton chop.” Several silent patients reportedly recovered the next day following this treatment.
These effects shade imperceptibly over into the manifestly suggestive, and probably no sharp line can be drawn between the effects of medical suggestion, non-medical heterosuggestion, and even autosuggestion. Adrian and Yealland rather decry the Micawber line of waiting for something to turn up. Zeehandelaar, a Dutch professor, studied Berlin methods (Lewandowsky), and found numerous cases (both of mutism and of deafness, paralyses, contractures, and tremors) lying about without special treatment. According to this observer, the expectant treatment was sometimes successful, and sometimes not; if unsuccessful, the soldier was sent home, and re-examined a year later; whereupon he might be found to have profited by this long waiting and to have gotten well enough to return to army duty.
These effects gradually blend into clearly suggestive ones, and it's likely that no definitive line can be drawn between the effects of medical suggestion, non-medical suggestion from others, and even self-suggestion. Adrian and Yealland criticize the Micawber approach of just waiting for something good to happen. Zeehandelaar, a Dutch professor, looked into the methods used in Berlin (Lewandowsky) and found many cases (including those of mutism and deafness, paralysis, contractures, and tremors) that were left untreated. According to this researcher, sometimes the wait-and-see approach worked, and sometimes it didn't; if it didn't work, the soldier was sent home and re-evaluated a year later, at which point he might have benefited from the long wait and could be well enough to return to army service.
A decorated officer, evacuated for Shell-shock on the third day of the Aisne, after four days returns to the front. Evacuated a second time, after weeks returns to the front without relapse.
A decorated officer, evacuated for shell shock on the third day of the Aisne, returns to the front after four days. Evacuated a second time, he returns to the front again after weeks without any relapse.
Case 474. (Gilles, 1916.)
A young officer, with many decorations for brilliant Colonial service, was in the battle of the Marne, under six consecutive days’ shell fire, smoked phlegmatically a cigarette no matter whether walls were crashing or horses disemboweled beside him, and was uniformly able to stimulate his men to the heavy work by humor or heroic phrases.
A young officer, decorated for outstanding service in the Colonies, was in the battle of the Marne, enduring six days of continuous shellfire. He calmly smoked a cigarette, regardless of the walls collapsing or horses being ripped open nearby, and consistently motivated his men for the tough tasks ahead with humor or inspiring words.
A week later, on the third day of the Aisne, he had to be evacuated. He was another man—wild-eyed, shivering, jumping at the least noise, unable to eat or sleep, given to battle dreams. He had to be carried away from the battle zone and put in a bed in a town in the rear and given chloral. The nightmares continued. On being awakened he would ask where he was. He was kept in bed, given strychnine cacodylate, and dieted. He went back to the front in four days. Two days later he had to be evacuated a second time. After some weeks more in the rear, however, he went back to the front, and thereafter had not relapsed (April, 1916.)
A week later, on the third day of the Aisne, he had to be evacuated. He was a different man—wide-eyed, shivering, flinching at the slightest sound, unable to eat or sleep, haunted by combat nightmares. He had to be carried away from the battlefield and put in a bed in a town farther back, where he was given chloral. The nightmares kept coming. When he woke up, he would ask where he was. He was kept in bed, given strychnine cacodylate, and put on a special diet. He returned to the front after four days. Two days later, he had to be evacuated again. After a few more weeks in the rear, he went back to the front, and from then on, he didn’t have a relapse (April, 1916.)
Re relapses, Wiltshire thinks their causes and frequency prove the psychogenic nature of Shell-shock. Ballard states that a severe case lasting six months does not recover in the army. Many that are said to recover in hospital break down at dépôts, often with symptoms quite unlike those which they originally presented, and it will be remembered that Ballard has an epileptic theory of the nature of Shell-shock. See Cases 82, 83, and 84 in Section A, III, Epileptoses. But another portion of Ballard’s contentions relates to a causation through fear suppressions released by perturbing events. According to Ballard, if the man endeavors to re-suppress the released fear, the fits occur. Ballet and DeFursac note the frequency of relapses—fewer after treatment at the front.
Re relapses, Wiltshire thinks their causes and frequency show the psychological nature of Shell-shock. Ballard mentions that a severe case lasting six months doesn’t recover in the army. Many who are said to recover in the hospital breakdown at dépôts, often with symptoms quite different from those they initially had, and it should be noted that Ballard has an epileptic theory about Shell-shock. See Cases 82, 83, and 84 in Section A, III, Epileptoses. Another part of Ballard’s arguments relates to a cause through fear suppressions that are released by distressing events. According to Ballard, if a person tries to re-suppress the released fear, the seizures happen. Ballet and DeFursac note the frequency of relapses—fewer after treatment at the front.
Vicissitudes in fifteen months of a Shell-shock case with mutism and amnesia. Attacks of mania. Hyperthyroidism?
Vicissitudes in fifteen months of a shell shock case with mutism and amnesia. Episodes of mania. Hyperthyroidism?
Case 475. (Chief Purser, October, 1917.)
An Englishman, 21, in a rifle regiment, arrived in May, 1915, at the Dublin University V. A. D. Hospital, being dumb, impaired as to vision and hearing, having dilated pupils, tremors, restlessness and weakness, and giving the impression of visual hallucinations. Although suspicious, he was treated kindly for a few days, recovered his hearing, and wrote the few things that he remembered about home and the war, now and then tremulously and perspiringly writing down, “Asylum; do not lock up; I am not mad.”
A 21-year-old Englishman in a rifle regiment arrived at the Dublin University V.A.D. Hospital in May 1915. He was mute, had impaired vision and hearing, dilated pupils, tremors, restlessness, and weakness, and appeared to be experiencing visual hallucinations. Even though he seemed suspicious, the staff treated him kindly for a few days. He gradually regained his hearing and wrote down the few things he could remember about home and the war, occasionally writing nervously and sweating, “Asylum; do not lock up; I am not mad.”
With the idea of hypnosis, his bed was surrounded by screens, whereupon he grew so perturbed that the attempted hypnosis could not be executed. He learned the letters PP, TT, SSS, A-OOO, and finally AA-SS, AA-TT, T-OO, and after many weeks SS-SST-R and B-TT-R. His father visited him and probably was recognized.
With the concept of hypnosis, his bed was surrounded by screens, which made him so anxious that the hypnosis couldn’t proceed. He learned the letters PP, TT, SSS, A-OOO, and finally AA-SS, AA-TT, T-OO, and after many weeks SS-SST-R and B-TT-R. His father visited him and he was likely recognized.
At the end of September another dumb Shell-shock case recovered speech upon being given ether. Maj. Purser asked the sister to arrange for a like treatment for the first case, explaining that an examination of his throat might be painful. The cure of the second case by anesthesia got into the papers and before he was treated the account was possibly seen by the hitherto gentle rifleman. At any rate, he was seized with a sort of spasm, became furious and could only see Germans coming and carrying off his machine gun. He shouted for help. A half grain of morphine was given him and when it began to take effect the fighting spirit gave way to despair. He trembled over the loss of the gun, and remained in this state of despair for three days, remembering his regiment number and the like, but amnestic for his life during the past few months. He could not read now because print was indistinct. Words, when he had spelled them out, conveyed no meaning. He had a functional alexia.[677] When he saw a picture of a bunch of flowers in a notebook of his, he had another spell of excitement and regained his power of speech, remembering about his experiences only that he had been locked up. He had now completely forgotten his father, who came to call.
At the end of September, another case of Shell shock managed to speak again after being given ether. Major Purser asked the nurse to arrange a similar treatment for the first case, explaining that examining his throat might be painful. The recovery of the second case through anesthesia made the news, and before he was treated, the article might have been seen by the previously gentle rifleman. At any rate, he became agitated, furious, and could only envision Germans coming to steal his machine gun. He called for help. A half grain of morphine was administered, and as it started to take effect, his fighting spirit shifted to despair. He was distraught over the loss of the gun and remained in this state of despair for three days, recalling his regiment number and similar details, but unable to remember anything from the past few months. He couldn't read because the print was blurry. Words, when he managed to spell them, held no meaning. He had a functional alexia.[677] When he saw a picture of a bunch of flowers in one of his notebooks, he had another episode of excitement and regained his ability to speak, remembering only that he had been locked up. He had now completely forgotten about his father, who had come to visit.
By the end of October he was stronger, but his horizon was still limited to the hospital surroundings and a little newspaper reading. Headaches and impaired vision persisted. Sight temporarily left him early in November, and there was a suggestion of an epileptic fit one day early in that month. Tonic and sedative drugs and suggestive remedies were of no avail. Hypnotism made him worse, and psychanalysis was, perforce, ineffective through the amnesia. At the end of November depression and suicidal thoughts set in, with an elevation of blood pressure to 178 m.m., pulse 80 to 90. Maj. Dawson then thought he was a suicidal melancholic. Rest in bed and thyroid extract were given, but the latter threw up his pulse on the fifth day to 140. He grew better mentally on the treatment, however, and his blood pressure fell to 140 in three weeks. He was now over-emotional, unable to stand or walk or feed himself or to pull on his socks.
By the end of October, he was feeling stronger, but his world was still limited to the hospital environment and some reading of newspapers. He continued to suffer from headaches and blurred vision. His sight temporarily left him in early November, and there was a hint of an epileptic seizure one day during that month. Tonic and sedative medications, as well as suggestive therapies, didn’t help. Hypnotism actually made him worse, and psychoanalysis couldn’t be effective due to his memory loss. By the end of November, he started experiencing depression and suicidal thoughts, with his blood pressure rising to 178 mm and his pulse ranging from 80 to 90. Maj. Dawson then concluded that he was a suicidal melancholic. He was prescribed bed rest and thyroid extract, but the latter spiked his pulse to 140 by the fifth day. However, he began to improve mentally with the treatment, and his blood pressure dropped to 140 in three weeks. At this point, he became overly emotional and was unable to stand, walk, feed himself, or even put on his socks.
For change of scene he was transferred to Mercer’s Hospital in February, 1916. He suffered from astasia-abasia. The tremor became jerky, coarse and persistent. The thyroid gland grew a good deal in size during the spring and the pulse went up to 120 per minute. There was also well-marked dermographia and there was a suggestion of the clinical picture of Graves’ disease. Even a quarter grain of morphine had little or no effect upon an ineradicable insomnia.
For a change of scenery, he was moved to Mercer’s Hospital in February 1916. He was dealing with astasia-abasia. The tremor became shaky, rough, and constant. The thyroid gland enlarged significantly during the spring, and his pulse rose to 120 beats per minute. There was also noticeable dermographia, and there were signs suggesting the clinical picture of Graves’ disease. Even a quarter grain of morphine had little to no effect on his unrelenting insomnia.
Maj. Purser gave the case up as a bad job and the man was discharged and sent home September 2, 1916. During the next two months at home he improved in steadiness, though he flushed if dealing with strangers, and improved as to memory. He began to be able to read better. He had begun to be able to get about on his feet without so much support. The ultimate outcome could not be reported by Maj. Purser.
Maj. Purser considered the case hopeless, and the man was released and sent home on September 2, 1916. Over the next two months at home, he became more stable, though he blushed when interacting with strangers, and his memory improved. He started to read better and was also able to move around on his own with less support. Maj. Purser could not provide a final assessment of the situation.
Shell-shock: Mutism. Cure after killing a snake.
Shell-shock: Silence. Recovery after killing a snake.
Case 476. (Jones, 1915.)
An Australian soldier of 20 went to Egypt, thence to Gallipoli where, on July 29, 1915, he was almost completely buried by earth from the bursting of a high explosive shell. He was admitted to hospital August 5 and transferred to Malta, where he did not speak, stared into space and sometimes made, impulsively, attempts to get away. About September 17 he began to assist the orderlies and played draughts.
An Australian soldier who was 20 went to Egypt and then to Gallipoli, where, on July 29, 1915, he was nearly buried alive by dirt from a exploding shell. He was taken to the hospital on August 5 and moved to Malta, where he didn’t talk, gazed into space, and occasionally tried to escape impulsively. Around September 17, he started helping the orderlies and played checkers.
The diagnosis there was cerebral concussion. He was sent back to Australia by transport and had to be put in a padded cell on November 1, having become violent, noisy and destructive. He would assault anyone who beat him at the game of draughts and threw anything he could lay his hands on out of the porthole. Hyoscine he resented and threatened the givers by signs. He was at times restrained. He threatened to throw himself overboard. Diagnosis: Melancholia.
The diagnosis was a concussion. He was transported back to Australia and had to be put in a padded cell on November 1, after becoming violent, loud, and destructive. He would attack anyone who won against him in draughts and threw anything he could grab out of the porthole. He hated hyoscine and signaled threats to those who administered it. At times, he was restrained. He even threatened to jump overboard. Diagnosis: depression.
At Melbourne he was found in good physical shape, but dazed, mute, apparently deaf, indicating his wants by signs. With pencil and paper he would draw a ship or a gun and would copy any question put to him in writing. He played draughts intelligently and made friends with one of his shipmates. In four days’ time he began to communicate in writing, answering simple questions correctly. Asked to put a question, he wrote “Do you think I am mad?” On the appropriate answer he shook hands with the physician heartily.
At Melbourne, he was found to be in good physical condition, but he seemed dazed, unable to speak, and apparently deaf, expressing his needs through gestures. Using a pencil and paper, he would draw a ship or a gun and would copy any questions asked of him in writing. He played checkers intelligently and made friends with one of his shipmates. After four days, he started to communicate in writing, correctly answering simple questions. When asked to write a question, he wrote, “Do you think I am mad?” Upon receiving the appropriate answer, he shook hands with the doctor enthusiastically.
He was then sent to a military convalescent home at Highton. Here he communicated often in writing, and had an appreciation of sounds without distinguishing words. At a picnic on December 4 he killed a snake. While returning in the dark he began to whistle a song the rest of the party were singing. At the end of the song he clapped his hands and said, “What is the next item on the program?” Thereafter he was able to hear and speak. Seen four days later he asked to join the officers’ training school. However, he was discharged as permanently unfit for the service.
He was sent to a military recovery center in Highton. There, he often communicated by writing and could appreciate sounds without understanding the words. At a picnic on December 4, he killed a snake. On the way back in the dark, he started whistling a song that the rest of the group were singing. When the song ended, he clapped his hands and said, “What’s next on the agenda?” After that, he was able to hear and speak. When he was seen four days later, he asked to join the officers' training school. However, he was discharged as permanently unfit for service.
Course in hospital of an oniric delirium.
Course in hospital of a dreamlike delirium.
Case 477. (Buscaino and Coppola, January, 1916.)
An Italian gun-maker, 27 (father neurotic; grandmother and mother, alcoholic; patient excessive onanist), was called to arms June 14, 1915, and went into artillery service in the Tolmino, early in September. Some time later, a shell burst about 30 meters away and killed his lieutenant. The patient, however, was not hurt and did not even fall. He became mute and inaccessible, and was sent to a military hospital, and thence to an asylum in Udine, where he was restless and hallucinatory. October 2, he was sent to Florence on two months’ leave for convalescence. He was still hallucinated, always seeing his dead lieutenant. He spoke rarely, slept little, and his conduct became more and more queer. Now and again, he would act exactly as if he were at the front. November 5, he started off to find his brother, but was met by a hospital attendant, who promptly took him to a clinic. Here he was inaccessible and lived in a hallucinatory way a soldier’s life at the front: in continual movement, shielding his eyes with his hands as if looking far into the distance, bending down to turn an imaginary lever, apparently taking part of his aim, crouching in a corner, clapping his ears with his palms, and obeying hallucinatory commands: “Ready,” “Fire,” and the like. As to his interpretation of the actual surroundings, he would give a military salute at the entrance of the physician, as if he were the lieutenant. Another patient near by was interpreted as a spy. Hypodermic injections, November 6, were interpreted as military antityphoid injections. On succeeding days he piled dry horse-chestnut leaves for a parapet, which became the scene of battle. November 12 he had become a little more lucid. November 14, he evidently heard whistling and made the leaves ready as a bed for horses. November 15, he rolled up his blanket in a military fashion and hid in a cell corner. He explained, November 16, that he was a sentinel and had not been relieved by the corporal. He had saved everybody’s lives by signaling from a tree the presence[680] of four airplanes. He could not be convinced he was in an institution for the insane. November 20, he was virtually recovered but amnestic for what he had done since commitment. Headaches and dizziness. November 21, he remembered some of his dreams, especially one of being blinded and another of being tied by a German to a tree. By November 29 he had become lucid and oriented, but there was an amnestic gap for his stay at the clinic. Early in December the fields of vision were contracted; polyopia and a glaring and burning sensation before the eyes (after each test conjunctival and tear duct inflammation).
An Italian gunmaker, 27 (father was neurotic; grandmother and mother were alcoholics; patient was an excessive masturbator), was drafted on June 14, 1915, and started serving in artillery in Tolmino by early September. Some time later, a shell exploded about 30 meters away, killing his lieutenant. The patient, however, wasn’t injured and didn’t even fall. He became mute and withdrawn, and was sent to a military hospital, then to an asylum in Udine, where he was restless and hallucinating. On October 2, he was sent to Florence for a two-month leave to recover. He was still hallucinating, constantly seeing his dead lieutenant. He spoke rarely, slept little, and his behavior became increasingly odd. Occasionally, he would act as if he were still at the front. On November 5, he set off to find his brother, but was intercepted by a hospital attendant, who immediately took him to a clinic. There, he was uncommunicative and lived out a hallucinated soldier’s life at the front: constantly moving, shielding his eyes with his hands as if looking far away, bending down to turn an imaginary lever, aiming as if a target were there, crouching in a corner, covering his ears with his palms, and following hallucinatory commands: “Ready,” “Fire,” and so on. In terms of interpreting his actual surroundings, he would salute the doctor at the entrance, treating him like the lieutenant. Another patient nearby was seen as a spy. Hypodermic injections on November 6 were interpreted as military antityphoid shots. In the following days, he piled dry horse chestnut leaves to build a parapet, which became a scene of battle. By November 12, he was slightly more aware. On November 14, he seemed to hear whistling and prepared the leaves as a bed for horses. On November 15, he rolled up his blanket in a military style and hid in a corner of his cell. On November 16, he claimed to be a sentinel who hadn’t been relieved by the corporal, asserting he had saved everyone by signaling the presence of four airplanes from a tree. He couldn’t be persuaded he was in a mental institution. By November 20, he had almost fully recovered but had no memory of what happened since he was committed. He experienced headaches and dizziness. On November 21, he recalled some of his dreams, particularly one of being blinded and another of being tied to a tree by a German. By November 29, he was lucid and oriented, but there was a memory gap concerning his time at the clinic. Early in December, his vision fields had narrowed; he experienced polyopia and a glaring, burning sensation in his eyes (after each test, he had conjunctival and tear duct inflammation).
December 21, discharged well.
Discharged well on December 21.
Re the nature of oniric delirium, see discussion under Cases 333 and 450, Chavigny had but two cases out of 260 in which a rapid curability was noted (90 per cent finally curable). Chavigny’s treatment consists of rest in bed, quiet, purgation if necessary, and warm or cold shower baths. Chavigny remarks upon the extraordinary transformation from apathy to lucidity in the course of a few minutes, brought about by arranging a slight but definite emotional shock to the patient, namely, by mentioning in his presence something about home or family. One bit of technic was to get the patient to write or dictate a letter home.
Regarding the nature of dream-related delirium, see discussion under Cases 333 and 450. Chavigny found only two cases out of 260 where quick recovery was observed (90 percent ultimately curable). Chavigny’s treatment involves bed rest, quiet, purging if necessary, and warm or cold showers. Chavigny notes the remarkable shift from apathy to clarity that can happen in just a few minutes, triggered by introducing a slight but distinct emotional shock to the patient, such as mentioning home or family. One technique was to have the patient write or dictate a letter home.
Régis remarks that battle dreams of this nature occasionally affect alcoholics in garrison or at home. The victim ought not to be hastily committed to an asylum, but should be treated in a military neuropsychiatric service with isolation chambers and open wards. Régis organized early in the war at Bordeaux a central psychiatric service along these modern lines. He remarks that the central service ought to receive not only patients from the military hospitals, but also patients from the temporary auxiliary hospitals of the city and district round about. A pooling of the military and civilian issue upon rational lines is here indicated.
Régis points out that combat-related nightmares like this sometimes impact alcoholics, whether they are in the military or at home. The person affected shouldn't be rushed into a psychiatric hospital; instead, they should be treated at a military neuropsychiatric facility that includes isolation rooms and open wards. Early in the war, Régis set up a central psychiatric service in Bordeaux based on these modern principles. He notes that this central service should receive not only patients from military hospitals but also those from the temporary auxiliary hospitals in the city and surrounding areas. This suggests a sensible approach to combining military and civilian care.
Régis and others have remarked upon the necessity of differentiating these battle deliria from toxic and infectious psychoses.
Régis and others have pointed out the importance of distinguishing these battle deliria from toxic and infectious psychoses.
Shell explosion: Deafmutism, recovery of speech with electrical treatment; deafness cured by suggestion in writing.
Shell explosion: Deaf-muteness, recovery of speech through electrical treatment; deafness cured by suggestion in writing.
Case 478. (Buscaino and Coppola, January, 1916.)
A fusileer, 20 (mother neurotic, brother hemiparetic from infantile disease; patient had extreme otorrhea from an early otitis media), entered the army January 15, 1915. He was sent to the Isonzo in May and was slightly injured in the nape of the neck and the left calf by fragments of a shell that exploded near by. He was picked up unconscious and taken to the hospital at Servignano. There he was given electric treatment, and in a period of 18 days recovered his speech, passing through a phase of stammering. He was sent to a special hospital in Florence, still deaf, and passed into a state of mental excitement with visual hallucinations of soldiers. He was given chloral and bromide. He insisted that he was incurably deaf. August 22, he was admitted to Buscaino’s clinic, completely deaf, slightly stuporous, somewhat indifferent, and innocent of any effort to make himself understood (contrary to the habits of an organically deaf person). Simulation could be excluded. It was possible to awaken the patient during sleep by auditory stimuli, whereupon he opened his eyes but could not hear. He talked well and spontaneously, telling about his accident, reading and answering by signs. He was assured,—always in writing,—that upon the following Sunday his hearing would be restored. Upon that day, during the visit of a lady,—one of the patient’s friends,—hearing was suddenly and almost completely restored in the left ear. The patient was so moved by this that he cried when the physician came. Upon the following day, he gradually began to hear with his right ear. A slight diminution of hearing in the right ear persisted, however, until September 24, and was associated with headache and pains in the left ear—pains which the patient compared to his ear pains in childhood (remains of otitis with retraction of the tympanic membrane).
A fusilier, 20 (mother had anxiety issues, brother had partial paralysis from a childhood illness; the patient experienced severe ear discharge from early ear infections), joined the army on January 15, 1915. He was sent to the Isonzo in May and sustained minor injuries to the back of his neck and left calf from shell fragments that exploded nearby. He was found unconscious and taken to the hospital in Servignano. There, he underwent electric treatment and, over 18 days, regained his speech, going through a stuttering phase. He was then transferred to a specialized hospital in Florence, where he remained deaf and experienced episodes of mental agitation with visual hallucinations of soldiers. He was treated with chloral and bromide. He maintained that he was permanently deaf. On August 22, he was admitted to Buscaino’s clinic, completely deaf, somewhat dazed, and indifferent, showing no effort to communicate (which is unusual for someone who is actually deaf). Simulation was ruled out. It was possible to wake him from sleep with sound stimuli, at which point he would open his eyes but remained unable to hear. He communicated well and spontaneously, recounting his accident, reading, and answering with gestures. He was repeatedly assured—in writing—that his hearing would be restored the following Sunday. On that day, during a visit from a friend, his hearing was suddenly and almost completely restored in his left ear. He was so overwhelmed that he cried when the doctor arrived. The next day, he gradually started to hear with his right ear as well. However, a slight reduction in hearing in the right ear continued until September 24, accompanied by headaches and pain in the left ear—pains he described as similar to his childhood earaches (residual effects of ear infections leading to retraction of the eardrum).
Paraplegia: Cured by administration of Iron Cross.
Paraplegia: Treated with Iron Cross.
Case 479. (Nonne, December, 1915.)
After heavy shelling a soldier fell for two days into a clouded state from which he waked with complete paraplegia of the lower extremities, and total anesthesia from the pelvis downward (reflexes and electric excitability normal).
After heavy shelling, a soldier fell into a dazed state for two days, waking up to find he had complete paralysis in his lower limbs and total numbness from the pelvis down (reflexes and electric responsiveness were normal).
On the third day after his reception in Nonne’s wards, he was about to be hypnotized when news came that he had been promoted to a lieutenantcy and had received the Iron Cross. He fell forthwith into hysterical convulsions, in the midst of which the hitherto paralyzed legs worked perfectly well! Even after the hysterical attack was over, the man could still move his legs in bed normally, but had absolute astasia-abasia. Next day, with deep hypnosis, markedly improved. After eight more days of hypnosis the new lieutenant got back his normal gait.
On the third day after he was admitted to Nonne’s wards, he was about to be hypnotized when he got the news that he had been promoted to lieutenant and had received the Iron Cross. He immediately fell into hysterical convulsions, during which his previously paralyzed legs worked perfectly! Even after the hysterical episode ended, he could still move his legs normally in bed but had complete inability to stand or walk. The next day, after deep hypnosis, he showed significant improvement. After eight more days of hypnosis, the new lieutenant regained his normal gait.
Shell-shock, burial: Mutism. Cure by getting drunk.
Shell shock, burial: Silence. Cure by drinking.
Case 480. (Proctor, October, 1915.)
A patient, 25, nine years in the service, was buried in a dugout by an explosive shell at Ypres, June 17, was taken out unconscious, and eventually reached the hospital at Versailles. Consciousness had returned a few days after the injury. There was ringing in the ears, difficulty in hearing, and inability to speak. He arrived at the Duchess of Connaught’s Hospital at Taplow, July 12, when, aside from the above-mentioned symptoms and a rapid heart action (108 at rest), he seemed perfectly well. About August 14, he began occasionally to refuse solid nourishment and remained in bed, eyelids closed but twitching at times, especially when spoken to. He resisted having his eyelids opened.
A 25-year-old patient, who had served for nine years, was buried in a dugout by an explosive shell at Ypres on June 17. He was rescued unconscious and eventually taken to the hospital in Versailles. He regained consciousness a few days after the injury. He experienced ringing in his ears, difficulty hearing, and an inability to speak. He arrived at the Duchess of Connaught’s Hospital in Taplow on July 12. Aside from the symptoms mentioned above and a rapid heart rate (108 at rest), he seemed perfectly fine. Around August 14, he started occasionally refusing solid food and stayed in bed with his eyelids closed, twitching at times, especially when spoken to. He resisted having his eyelids opened.
August 27, he was allowed to go to the village with companions, and got drunk, found his voice, for two days talked and sang incessantly. Discharged September 9, cured.
August 27, he was allowed to go to the village with friends, got drunk, found his voice, and for two days talked and sang nonstop. Discharged September 9, he was cured.
Shell-shock and burial: Mutism. Cure by work in a vineyard with wine to drink.
Shell shock and burial: Mutism. Treatment through working in a vineyard with wine to enjoy.
Case 481. (Anonymous, May, 1916.)
A correspondent of the British Medical Journal reports a case of cure of emotional mutism. This robust young soldier at Verdun was buried by the explosion of a shell and was thereafter found unable to speak. A week later he arrived at the ambulance in the interior, and was still mute. He could understand what was said to him without difficulty, and was able to reply by signs. He did not even move the lips when requested to pronounce such words as mamma and papa, but was eventually induced to whisper these words.
A reporter for the British Medical Journal shares a case of someone recovering from emotional mutism. This strong young soldier at Verdun was trapped after a shell explosion and was found unable to speak afterward. A week later, he was taken to a medical center and remained silent. He understood everything said to him easily and could respond with gestures. He didn’t even move his lips when asked to say words like mamma and papa, but eventually he was encouraged to whisper those words.
The laryngoscope showed complete paralysis of the vocal cords, which were in extreme abduction (it was possible to see several tracheal rings). There was no reaction on the part of the pharyngeal mucosa upon stimulation.
The laryngoscope showed total paralysis of the vocal cords, which were fully spread apart (several tracheal rings were visible). There was no response from the pharyngeal mucosa when stimulated.
A fortnight passed without restoration of speech, though at one time, not having bolted the closet door, the patient was startled when a nurse rushed in, and he said, “Oh, pardon, Madam.” The mutism persisted. He was then given work in the vineyard, plenty of wine to drink, and hard work. After a time (not specified) speech suddenly returned. According to this correspondent, “this indeed is a universal experience, namely, that hard manual work is the best remedy for such functional incapacities of traumatic origin.”
Two weeks went by without the patient speaking again, although there was one moment when he startled a nurse who came in after he hadn't locked the closet door, and he said, "Oh, excuse me, Ma'am." The silence continued. He was then assigned work in the vineyard, given plenty of wine to drink, and made to do hard labor. After an unspecified amount of time, he suddenly began to speak again. According to this correspondent, "this is truly a common experience, that hard physical work is the best cure for such functional issues caused by trauma."
Re gradual cures as opposed to sudden ones, Dundas Grant deprecates violent measures in the treatment of mutism during the period of exhaustion after Shell-shock. However, Dundas Grant does not advocate an expectant treatment, but employs a gradual reëducation of the voice through imitation of the teacher. The voice is sometimes restored at a sitting, sometimes gradually; see, for example, Case 578 of Briand and Philippe, and Case 586 of MacCurdy.
Re gradual cures compared to sudden ones, Dundas Grant criticizes harsh methods in treating mutism during the recovery period after Shell-shock. However, Dundas Grant doesn't support a wait-and-see approach; instead, he uses a gradual re-education of the voice through imitating the teacher. The voice can sometimes be restored in one session, and other times it takes longer; see, for instance, Case 578 of Briand and Philippe, and Case 586 of MacCurdy.
Shell-shock, unconsciousness: Deafmutism: Spontaneous recovery of speech and gradual recovery (several months’ isolation) of hearing.
Shell shock, unconsciousness: Deaf-muteness: Spontaneous recovery of speech and gradual recovery (after several months of isolation) of hearing.
Case 482. (Singer, July, 1915.)
A musketeer was deafened and stunned by a near-by shell explosion. On coming to, he found no wound, but was deaf and dumb.
A musketeer was shocked and disoriented by a nearby shell explosion. When he came to, he found no injuries, but he was left deaf and mute.
Speech returned after ten days, and hearing partially, but there was a tonic stuttering. He had to hunt anxiously for words, talked like a child in infinitives and telegram style, although he could express himself in writing perfectly well.
Speech returned after ten days, and hearing was partially restored, but there was a noticeable stutter. He had to search anxiously for words and spoke like a child, using simple phrases and a choppy style, even though he could write perfectly well.
Hearing improved on the right side very quickly, but on the left side conditions varied from total deafness to subtotal deafness. There was a general hyperesthesia of the skin, pain on pressure on the temples, exaggeration of skin and tendon reflexes, marked tremor in both hands. The man was anxious, depressed, and irritable. During caloric tests of the vestibular apparatus in the course of the next few weeks, the man had an hysterical attack of crying twice, following which all the phenomena got worse.
Hearing improved quickly on the right side, but on the left side, it ranged from complete deafness to partial deafness. There was an overall sensitivity of the skin, pain when pressure was applied to the temples, heightened skin and tendon reflexes, and noticeable tremors in both hands. The man felt anxious, depressed, and irritable. During heat tests of the vestibular system over the next few weeks, he experienced two hysterical crying episodes, after which all his symptoms worsened.
Rest and isolation from all such influences procured an almost complete recovery in several months.
Rest and being away from all those influences led to an almost complete recovery in a few months.
Re differential recoveries, see also Case 585 of Liébault, in which speech was recovered by suggestion and reëducation, and hearing by a process of reëducation alone.
Re differential recoveries, see also Case 585 of Liébault, where speech was regained through suggestion and reeducation, and hearing through a method of reeducation only.
Re isolation, Roussy and Lhermitte remark that in all the psychoneuroses of war, isolation is a valuable and indeed an indispensable aid to psychotherapy. The application of this old classical method of Weir Mitchell reinforces the persuasive talk of the doctor on the day of admission, allows the man to think over the promises made to the doctor, and permits longer observation. It depends on the case, whether rigorous isolation on limited diet shall be employed. See below a general discussion of the psycho-electric and reëducative method employed in French centres.
Re isolation, Roussy and Lhermitte note that in all the war-related psychoneuroses, isolation is a valuable and even essential aid to psychotherapy. Using this traditional method from Weir Mitchell supports the doctor's convincing conversation on the day of admission, gives the patient time to reflect on the commitments made, and allows for longer observation. Whether strict isolation with a restricted diet should be used depends on the individual case. See below for a general discussion of the psycho-electric and reëducative methods used in French centers.
Marches; battles; slight shell wound of left upper arm: Hysterical anesthesia of the arm and tremors (NO paresis). Causes slight—disease obstinate (partly explained by furloughs among sympathetic friends).
Marches; battles; minor shrapnel wound in the left upper arm: Hysterical numbness in the arm and tremors (no weakness). Causes slight—condition stubborn (partly explained by time off among supportive friends).
Case 483. (Binswanger, July, 1915.)
A soldier, 26, without heredity, always well, in long marches and several battles early in the war, August 23 sustained slight shell wounds of thighs and left upper arm. He was unconscious about five minutes. In eight days, the wounds were healed, and all movements were free.
A 26-year-old soldier, with no family history of issues, was always fit. During long marches and battles early in the war, on August 23, he received minor shell wounds to his thighs and left upper arm. He was unconscious for about five minutes. Within eight days, the wounds had healed, and he could move freely.
Immediately after the trauma the arms trembled, and at times the legs. Treatment was instituted (baths, drugs, massage, electricity), but without result. After a month’s treatment and a furlough at home, the patient was sent, January 3, 1915, to the Jena Nerve Hospital. He was a powerful man of middle size, with some small movable scars on the left upper arm, remains of the shell injury; two similar scars of the gluteus maximus. The deep reflexes were slightly exaggerated, as were the skin reflexes. The touch and pain sense in the left arm was absent as far as the shoulder in typical segmental fashion. Arm movements were free; there was an occasional tremor in both arms, especially the left. This tremor would pronouncedly increase upon intentional movements and with emotion.
Immediately after the trauma, his arms shook, and sometimes his legs did too. Treatment was started (baths, medication, massage, electricity), but it didn’t help. After a month of treatment and a break at home, the patient was sent to the Jena Nerve Hospital on January 3, 1915. He was a strong man of average height, with a few small movable scars on his left upper arm, remnants of the shell injury; there were two similar scars on his gluteus maximus. His deep reflexes were a bit exaggerated, as were his skin reflexes. He had lost the sense of touch and pain in his left arm up to the shoulder in a typical segmental pattern. His arm movements were free; however, there was an occasional tremor in both arms, especially the left one. This tremor would noticeably increase during intentional movements and in response to emotions.
He said that about two weeks before, at home, he had waked up in the night and lain down on the floor beside his bed, feeling giddy in his head. In a week the tremors had diminished, leaving only a very slight tremor of the left hand. The patient went to considerable pains to conceal his tremor, holding his hand in a military position at the seam of the trousers, on the medical visit. Sometimes he would succeed in making the tremor quite disappear. February 5, he was busy about the ward work, going errands and carrying trays. He would intentionally spare his left hand in this work. Upon trying gymnastic exercises, the[686] tremors of the left hand and also of the right reappeared. After a few days these tremors again disappeared, only to come back on the 12th, when there was a constant tremor also when the patient was at rest. He had been affected when observing another patient (8[7]). Accordingly, he was separated from this patient and put in a psychiatric ward. The tremor remained of varying intensity, sometimes being absent for hours together.
He mentioned that about two weeks ago, at home, he had woken up in the night and lay down on the floor next to his bed, feeling dizzy. Within a week, the tremors had lessened, leaving just a slight tremor in his left hand. The patient went to great lengths to hide his tremor, holding his hand in a stiff position at the seam of his trousers during the medical visit. Sometimes he managed to make the tremor completely disappear. On February 5, he was busy with ward tasks, running errands and carrying trays. He would intentionally avoid using his left hand while doing this work. When trying some exercise routines, the tremors in both his left and right hand came back. After a few days, these tremors went away again, only to return on the 12th, when there was a continuous tremor even at rest. He seemed to be affected when watching another patient (8[7]). As a result, he was separated from that patient and admitted to a psychiatric ward. The tremor varied in intensity, sometimes being absent for hours at a time.
Request for furlough at the beginning of March was refused with the statement that it would be granted when cure was complete. The patient was inaccessible to psychotherapeutic influence. He was always of a friendly, modest demeanor, sleeping well, and performing all bodily functions properly. On any exertion the pulse ran to 134. The heart was normal. There were outbreaks of perspiration.
Request for leave at the beginning of March was denied with the explanation that it would be approved once the recovery was complete. The patient couldn’t be reached through psychotherapy. He always had a friendly, humble attitude, was sleeping well, and was functioning normally in all bodily aspects. Any physical effort caused his pulse to reach 134. The heart was normal. There were episodes of sweating.
March 26, he renewed his request for leave, desiring his Easter furlough. He was told he might expect it. March 31, the tremor was found to have quite disappeared. Upon his return, April 12, there was a marked tremor of the left arm, especially of the wrist joint, which again disappeared after some days. The middle of June he was released as capable of garrison duty with the recruits.
March 26, he asked again for leave, wanting his Easter break. He was told he could expect it. By March 31, the tremor had completely gone. When he returned on April 12, there was a noticeable tremor in his left arm, particularly at the wrist, which also went away after a few days. In mid-June, he was declared fit for garrison duty with the recruits.
If there was a mechanical factor in this case, it must have been the shaking-up of the body by the shell explosion. His skin lesions were slight. The main factor was doubtless the emotional shock. The tremor supervened upon a very brief period of unconsciousness. It is hard, according to Binswanger, to explain the localization of the cutaneous anesthesia without the development of a corresponding paresis. May it be, inquires Binswanger, that the wound of the left upper arm at the moment of the setting-in of unconsciousness, or perhaps at the moment of waking from unconsciousness, directed the mind forthwith upon the left arm and in this way produced localized disorder of sensation? If so, why did the wound of the gluteal region not produce corresponding disorders of feeling and sensation of an hysterical nature? The obstinacy of the disease stands in striking disproportion[687] to the slightness of the causative factors at work.
If there was a mechanical factor in this case, it must have been the jolt of the body from the shell explosion. His skin lesions were minor. The main factor was likely the emotional shock. The tremor followed a very brief episode of unconsciousness. According to Binswanger, it’s difficult to explain the specific areas of numbness without a corresponding weakness. Binswanger wonders if the injury to the left upper arm at the moment of losing consciousness, or possibly when waking up, caused the mind to immediately focus on the left arm, leading to specific sensory issues? If that’s the case, why didn’t the injury to the lower back cause similar sensory problems? The stubbornness of the condition seems surprisingly out of proportion to the minor causes at play.[687]
According to Binswanger, this is perhaps due to the long furlough which the patient had. According to Binswanger’s experience, as that of many others, home works badly for these hysterical patients; their friends sympathize with them too much.
According to Binswanger, this might be because the patient had a long break. Based on Binswanger's experience, like many others, being at home isn’t helpful for these hysterical patients; their friends are too sympathetic toward them.
Re furloughs, Ballard states that severe Shell-shock cases should get analogous treatment to that of civilian psychoneurotics, namely, a complete removal from the environment in which the illness began. He advocates three months’ leave, after which the man is to be sent to a convalescent home, and thence to a command dépôt. He states that if a relapse then occurs, such a patient will never be a soldier. Ballard would allow the men to walk about with their “pals (not with escorts).” Cimbal remarks that German data show that home furloughs should be avoided in every instance where possible. Fiessinger remarks, on the basis of English experience, that a Shell-shock patient treated by rest, suggestion, and manual occupation may go back to the line “and on a subsequent occasion prove a hero.” (See Case 474 of Gilles.) But Forsyth remarks that it is probably injudicious to send any cases of Shell-shock, with few exceptions, back to the firing line, because their fighting value has been permanently deteriorated, and because, if the fear of return to the trenches is removed, recovery is more rapid. The experience here is not unlike that of industrial accident board cases with rapid recovery after the decree of compensation.
Re furloughs, Ballard says that severe cases of Shell-shock should be treated similarly to civilian psychological disorders, meaning a total break from the environment where the illness started. He recommends three months off, after which the person should be sent to a recovery home, and then to a command depot. He points out that if a relapse happens, that patient will never be able to serve as a soldier again. Ballard would let the men hang out with their “buddies (not with escorts).” Cimbal notes that German data indicates home furloughs should be avoided whenever possible. Fiessinger mentions, based on English experiences, that a Shell-shock patient treated with rest, reassurance, and hands-on activities may return to active duty and later prove to be a hero. (See Case 474 of Gilles.) However, Forsyth argues that it’s likely unwise to send any Shell-shock cases, with few exceptions, back to the front line, as their combat effectiveness has been permanently diminished and removing the fear of returning to the trenches leads to a quicker recovery. This experience is similar to cases of industrial accidents where rapid recovery follows the granting of compensation.
War stress in a volunteer banker: Hysterical seizures. Treatment by hydrotherapy.
War stress in a volunteer banker: Hysterical seizures. Treatment through hydrotherapy.
Case 484. (Hirschfeld, February, 1915.)
A banker, a volunteer (articular rheumatism at three years; at 18, some form of lung and tracheal inflammation; tendency to fainting spells on cold days—heart disease was said to have been found), as a result of the strain and excitement of the war had hysterical attacks during a fortnight before observation in hospital, consisting of sensations suddenly developing in the region of the heart, stiffness of the whole body, disorders of movement, without loss of consciousness.
A banker who had a history of health issues (arthritis at three years old; at 18, some kind of lung and trachea inflammation; and a tendency to faint on cold days—rumors of heart disease had been mentioned) experienced hysterical attacks for two weeks prior to being observed in the hospital. These attacks included sudden sensations in the heart area, stiffness throughout the body, and movement disorders, but he did not lose consciousness.
November 23, 1914, he was examined in bed in the dorsal position, with the muscles of the legs, back, and neck in a state of tonic contraction. He was unable to answer questions. The pupil reactions were normal in the seizure. The attack ceased in two minutes, as the result of hitting heavy blows on the chest with a moist handkerchief and the threat of a strong and painful application of the electric current. The patient then got out of bed at request, walked about a little incoördinately for a time, but after a few minutes was able to walk perfectly and to talk once more.
On November 23, 1914, he was examined in bed lying on his back, with the muscles in his legs, back, and neck tensed. He couldn't respond to questions. His pupil reactions were normal during the seizure. The attack stopped after two minutes due to firm pats on his chest with a moist handkerchief and the warning of a strong and painful electric shock. After that, he got out of bed when asked, walked around a bit unsteadily at first, but after a few minutes, he was able to walk perfectly and talk again.
Examined, November 25, he was found to be pale, fairly well nourished, with a somewhat accelerated pulse, and a melancholy, slightly apathetic expression. A systolic murmur at the right apex; accentuation of secondary pulmonary sound; increased knee-jerks; trembling of the lids (Rosenbach).
Examined on November 25, he was found to be pale, fairly well-nourished, with a somewhat quickened pulse, and a sad, slightly indifferent expression. There was a systolic murmur at the right apex; an intensification of secondary pulmonary sounds; increased knee-jerk reflexes; and trembling of the eyelids (Rosenbach).
By December 12, the patient was completely well. The seizures had not recurred. The treatment was by hydrotherapy. A preliminary treatment is advocated by Hirschfeld, to insure peripheral circulation, either by light baths, hot douches, or packs. More important than this preliminary treatment is the cooling off process by means of tepid douches or partial baths. These partial baths are given at 28°C. for the intense effect of the cold. Sometimes[689] this treatment can be concluded with a dry pack. The patients are treated by Hirschfeld three times a week with both the warming and the cooling procedure.
By December 12, the patient was completely better. The seizures hadn't happened again. The treatment involved hydrotherapy. Hirschfeld recommends a preliminary treatment to improve blood flow, using light baths, hot showers, or packs. More crucial than this preliminary treatment is the cooling process with tepid showers or partial baths. These partial baths are taken at 28°C for the strong effect of the cold. Sometimes[689] this treatment wraps up with a dry pack. Hirschfeld treats the patients three times a week with both the warming and cooling methods.
Re hydrotherapy, Mott has found the continuous warm bath of great value in Shell-shock cases coming back from France. He keeps the patient in the water from a quarter to three-quarters of an hour, or longer. A warm bath and a drink of warm milk at bedtime may permit a man to get on without hypnotics, or to get on with lesser amounts of hypnotics. The effect of these baths is doubtless largely somatic. Some writers stress the suggestive value of hydrotherapy as well as of electricity, radiant heat baths, and the like (Ballard). A neuropsychiatric center properly equipped with a hydrotherapeutic plant can do therapeutic work by means of the suggestion afforded by a cold shower, which may act quasi miraculously, like electricity (Roussy and Boisseau). In fatigue and exhaustion cases, along with adrenalin and strychnin, Aimé gives mild hydrotherapy without other sedatives. Laehr’s free sanatorium at Schönow treats the arrhythmia and tachycardia cases with rest and hydrotherapy.
Re hydrotherapy, Mott has found that a continuous warm bath is really helpful for Shell-shock cases returning from France. He keeps the patient in the water for anywhere from a quarter to three-quarters of an hour or even longer. A warm bath and a drink of warm milk at bedtime might allow someone to manage without hypnotics or to use a smaller amount of them. The effects of these baths are likely mostly physical. Some writers highlight the suggestive benefits of hydrotherapy, as well as treatments like electricity and radiant heat baths (Ballard). A neuropsychiatric center that is properly equipped with hydrotherapy facilities can provide therapeutic benefits from the suggestion offered by a cold shower, which may work almost like a miracle, similar to electricity (Roussy and Boisseau). In cases of fatigue and exhaustion, along with adrenalin and strychnin, Aimé provides mild hydrotherapy without other sedatives. Laehr’s free sanatorium at Schönow treats arrhythmia and tachycardia cases with rest and hydrotherapy.
Brasch reports rather poor results with hydrotherapy in the cardiac neuroses. Weichardt has used the continuous bath as a form of psychotherapy and permits the symptoms of psychoneurosis to subside therein.
Brasch reports rather poor results with hydrotherapy in the cardiac neuroses. Weichardt has used the continuous bath as a form of psychotherapy and allows the symptoms of psychoneurosis to reduce while there.
Shell-shock: low blood pressure: Pituitrin.
Shell shock: low blood pressure: Pituitrin.
Case 485. (Green, September, 1917.)
A lance corporal of the Expeditionary Force, 26, went to France feeling very fit, February, 1916. He was blown up by a shell July 1, and faintly remembered crawling out of some water. He came to in a dugout, dumb and partially deaf, and was blind for a few minutes. August 17, he was admitted to Mott’s wards at Maudsley, mute but with hearing normal. The hands were dusky, sweating, cold, and slightly tremulous. He was given to battle dreams and used to wake in a sweat and terror after a pantomime of bomb-throwing. He had headache and was depressed. He complained of feeling cold and the surface temperature was subnormal. The blood pressure was also subnormal (according to Green, nightmares are most marked in cases with low blood pressure; these are, in fact, severer cases of Shell-shock than cases with high blood pressure; only 10 of 27 cases with blood pressure above 120 showed nightmares).
A lance corporal of the Expeditionary Force, 26, went to France feeling really fit in February 1916. He was blown up by a shell on July 1 and vaguely remembered crawling out of some water. He came to in a dugout, unable to speak and partially deaf, and was blind for a few minutes. On August 17, he was admitted to Mott’s wards at Maudsley, mute but with normal hearing. His hands were dark, sweaty, cold, and slightly shaky. He was plagued by nightmares and often woke up in a sweat and panic after dreaming about throwing bombs. He had headaches and felt depressed. He complained of feeling cold, and his surface temperature was below normal. His blood pressure was also low (according to Green, nightmares are most common in cases with low blood pressure; these are actually more severe cases of Shell-shock than those with high blood pressure; only 10 out of 27 cases with blood pressure above 120 experienced nightmares).
September 25, he was able to speak in a whisper. The dreams had become less terrifying. The other symptoms had been slowly improving.
September 25, he could talk in a whisper. The dreams had become less scary. The other symptoms had been gradually getting better.
November 25-28, all of the symptoms returned upon hearing the death of his brother in action.
November 25-28, all the symptoms came back when he heard about his brother's death in action.
The man was now put on extract of pituitrin gr. 2, t.d.s. (better results are claimed by Green from pituitrin extract than from pituitary fluid injections, as these sometimes cause dizziness, of which no case treated with extract complained). As in other cases, the extract was immediately followed by an increase in blood pressure, a general improvement and a diminution of headache and depression. The bomb-throwing pantomimes still persisted, but the patient was less weak on waking. The treatment was continued for seven days, whereupon the surface temperature began to rise and the patient himself felt that he was much warmer. The pituitrin was discontinued after a month’s treatment, yet the improvement persisted. The man was boarded out of the army and in March, 1917, wrote that he was still feeling better.
The man was now given an extract of pituitrin, 2 grains, three times a day. (Green claims better results from the pituitrin extract than from injections of pituitary fluid, which sometimes cause dizziness—none of the cases treated with the extract reported that issue). As in other cases, the extract immediately led to an increase in blood pressure, a general improvement, and a reduction in headache and depression. The bomb-throwing behaviors continued, but the patient felt less weak upon waking. The treatment lasted for seven days, after which the surface temperature began to rise, and the patient himself noticed he felt much warmer. The pituitrin was stopped after a month of treatment, yet the improvement continued. The man was discharged from the army and wrote in March 1917 that he was still feeling better.
SHELL-SHOCK, PITUITRIN, AND BLOOD PRESSURE (EDITH GREEN)
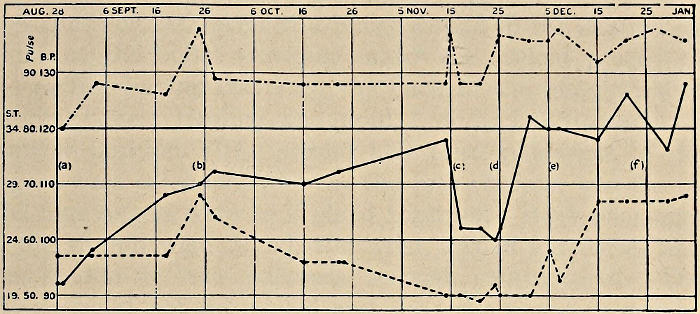
Blood pressure, surface temperature, and pulse in a case of functional mutism. (a) On admission, troubled by nightmare. (b) Able to speak in a whisper. (c) Much depressed after bad news. (d) Put on pituitrin. (e) Marked general improvement. (f) Taken off pituitrin.
Blood pressure, surface temperature, and pulse in a case of functional mutism. (a) Upon admission, troubled by nightmares. (b) Able to speak in a whisper. (c) Very depressed after receiving bad news. (d) Administered pituitrin. (e) Notable overall improvement. (f) Discontinued pituitrin.
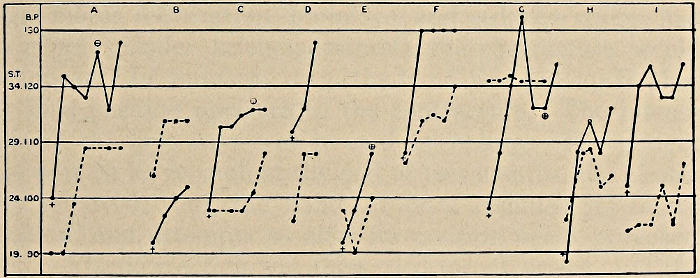
A-1 Showing the effect of pituitrin on the blood pressure and surface temperature. Each dot is one week’s interval. + is the pressure when the first dose was given. 𐌈 is the point at which the pituitrin was discontinued.
A-1 Showing the effect of pituitrin on blood pressure and surface temperature. Each dot represents a one-week interval. + indicates the pressure when the first dose was given. 𐌈 marks the point at which pituitrin was stopped.
Various treatments of a contracture of hand.
Various treatments for a hand contracture.
Case 486. (Duvernay, November, 1915.)
A chasseur, 22, received a bullet wound in the anatomical snuffbox, the bullet emerging under the styloid process of the radius, having traversed the back of the hand without striking bone. Healing was rapid, but the hand assumed a peculiar position. The second and third phalanges of the fingers were extended, whereas the first phalanx was flexed. The four fingers were as if glued together. Both phalanges of the thumb were flexed, the wrist was in extension, and the tendon of the palmaris seemed contractured. The fingers could not be moved and the wrist was very mobile. There was pain on attempts to move the hand passively, and small clonic contractions were made by the fingers. There were no sensory disorders, but there was a maceration of the interdigital spaces.
A soldier, 22, got shot in the anatomical snuffbox, with the bullet coming out below the styloid process of the radius after passing through the back of the hand without hitting any bones. Healing was quick, but the hand ended up in a strange position. The second and third phalanges of the fingers were straight, while the first phalanx was bent. The four fingers seemed stuck together. Both phalanges of the thumb were bent, the wrist was extended, and the tendon of the palmaris looked contracted. The fingers couldn't move, but the wrist had a lot of mobility. There was pain when trying to move the hand gently, and there were small involuntary contractions in the fingers. There were no sensory issues, but the spaces between the fingers were swollen.
Mechanotherapy accelerated the contracture, and massage, motor reëducation, bromides, and sedative drugs, had no effect. Under kelene-anesthesia the contracture would disappear. In January, 1915, the hand was put up in plaster in a position opposite to the contracture. The intense pain of the first days was treated by opium. The patient was sent on leave, and, at the end of two months, the plaster was removed; but the hand at once resumed its faulty position, and attempts to alter its position again provoked pain. Elastic traction was then tried for six weeks, and the bad position was somewhat modified but not improved by hyperextending the second phalanx on the first, and putting the third in slight flexion on the second. Hot compresses were unsuccessful also. May 14, 1915, the position was still irreducible; there was no R. D. or electrical hyperexcitability. This was not a question of radial paralysis, since finger extension was distinct; nor a paralysis of the median, since the thumb was flexed. The contracture, in fact, does not affect a special nerve territory, and the disorder is in the ulnar, radial, and median territories.
Mechanotherapy sped up the contracture, and massage, motor re-education, bromides, and sedative drugs had no effect. Under kelene anesthesia, the contracture would disappear. In January 1915, the hand was placed in a plaster cast in a position opposite to the contracture. The intense pain in the first few days was treated with opium. The patient was given leave, and after two months, the plaster was removed; however, the hand immediately returned to its faulty position, and attempts to reposition it caused pain again. Elastic traction was then tried for six weeks, and while the bad position was somewhat modified, it was not improved by hyperextending the second phalanx on the first and putting the third in slight flexion on the second. Hot compresses were also unsuccessful. As of May 14, 1915, the position was still unchangeable; there was no R. D. or electrical hyperexcitability. This was not a case of radial paralysis since finger extension was intact, nor was it median paralysis since the thumb was flexed. The contracture does not affect a specific nerve territory, and the disorder involves the ulnar, radial, and median territories.
Orthopedic case.
Orthopedic issue.
Case 487. (Sollier, November, 1916.)
A patient suffered from a rupture of the peroneal nerve in its lower part, September, 1915, and had operation scars before and behind the external malleolus. He was immobilized for 45 days at first, and then for 30 days, with the foot in extension on account of the pain produced in the endeavor to put it into normal position. A 6 cm. atrophy was then found to affect the calf, and there was a fibrous retraction of the tendo Achillis and of the calf muscles. There was no anesthesia, the toes moved easily, the foot was fixed in equinus, with about 7 cm. of the heel above the ground. He was placed in various orthopedic institutions and was treated with mechanotherapy, but without result.
A patient experienced a rupture of the peroneal nerve in the lower part of his leg in September 1915, and had surgical scars both in front of and behind the outer ankle bone. He was initially immobilized for 45 days, followed by another 30 days, with his foot extended due to the pain when trying to move it to a normal position. A 6 cm atrophy was observed in the calf, along with a fibrous retraction of the Achilles tendon and calf muscles. There was no loss of sensation, the toes moved freely, and the foot was positioned in equinus, with about 7 cm of the heel off the ground. He was treated at various orthopedic facilities with mechanotherapy, but there was no improvement.
At the neurological center, however, in six weeks, he was got to walk, with his heel on the ground, by means of massage and manual mobilization. The atrophy diminished a centimeter and the foot became mobile in all directions.
At the neurological center, though, in six weeks, he was able to walk with his heel on the ground, thanks to massage and manual mobilization. The atrophy decreased by a centimeter, and the foot became flexible in all directions.
According to Sollier, mechanotherapy by means of apparatus is apt to be ineffective, especially in contractures, because its action ceases the moment it ought to commence, namely, when the patient is beginning to react a little painfully after recovery from anesthesia. In cases of retraction, mechanotherapy with apparatus does not allow the proper combination of massage with progressive mobilization.
According to Sollier, using machines for mechanotherapy often doesn't work, particularly for contractures, because it stops being effective as soon as it should start, specifically when the patient begins to feel some pain after waking up from anesthesia. In cases of tightness, machine-based mechanotherapy doesn’t enable the right combination of massage and progressive movement.
Re orthopedic cases, Jones classes the conditions that create an orthopedic case under four heads (note especially the fourth):
Regarding orthopedic cases, Jones categorizes the conditions that create an orthopedic case into four categories (pay special attention to the fourth one):
1. Mechanical injury to bone, joint, muscle, or nerve.
1. Physical damage to bone, joint, muscle, or nerve.
2. Atrophy and disease of these structures primarily due to the injury.
2. Atrophy and disease of these structures mainly result from the injury.
3. Incoördination of movement due to disease of the brain—a result of atrophy and disease of peripheral structures.
3. Loss of coordination in movement caused by brain disease—a result of degeneration and illness in surrounding structures.
4. Psychological conditions which can be overcome by reëducational processes.
4. Psychological conditions that can be overcome through re-educational processes.
MECHANOTHERAPY (COLOLIAN)
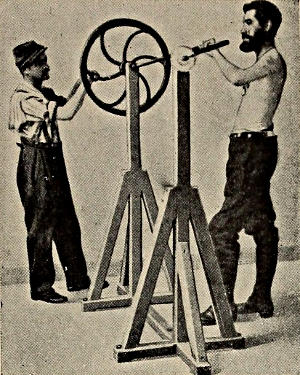
ROTATION OF SHOULDER
Shoulder rotation
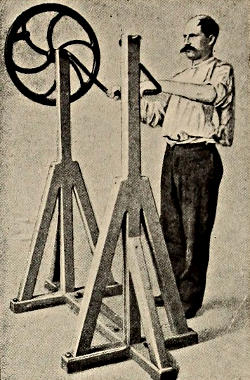
ROTATION OF SHOULDER
Shoulder rotation
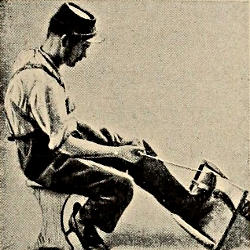
ANKLE EXTENSION
ANKLE EXTENSION
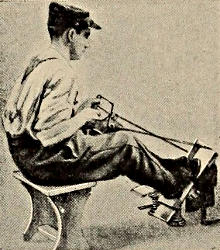
ANKLE EXTENSION
Ankle extension
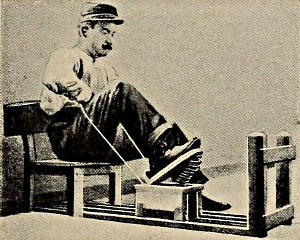
FLEXION AND EXTENSION
Flex and extend
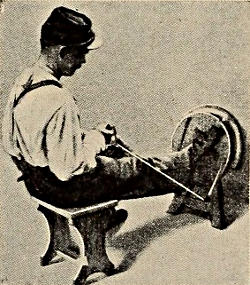
ROTATION OF HIP
Hip Rotation
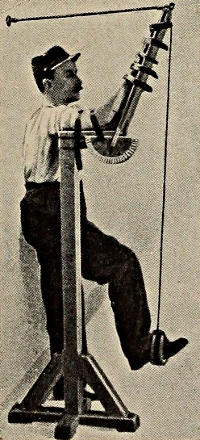
ELBOW FLEXION AND EXTENSION
Elbow bending and straightening
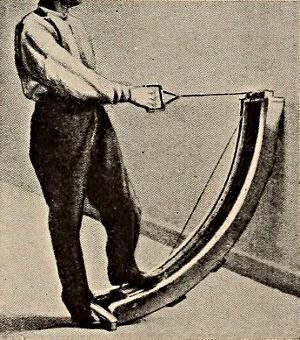
CIRCUMDUCTION OF THIGH
Thigh circumduction
Favorable effects of lumbar puncture.
Benefits of lumbar puncture.
Case 488. (Ravaut, August, 1915.)
An accountant, 20, in the 135th infantry sustained shock from mine explosion near his trench, March 6. He was kept two days at the relief station. March 8, at the ambulance, he did not appear to understand questions and had a fixed stare. He complained of a violent headache and kept pressing his head between his hands. He kept looking about him anxiously, and the slightest noise made him jump. He would mutter a few incomprehensible words, and in reply to a question would give only the last phrase which he happened to have been saying. Lumbar puncture showed a very slight excess of albumin. Next day, he answered his name. March 12, he could speak in monosyllables, and he began to understand what was said. After the lumbar puncture, the headache disappeared and did not set in again. March 13, he began to be able to write and say short phrases. March 16, expression was good though hesitant, and the patient wrote a letter to his parents, telling about his shock. Lumbar puncture showed that the albumin was now normal. From the rear, April 5, the patient sent Ravaut a postcard in perfect form, telling how he was ready to go back to the front.
An accountant, 20, in the 135th infantry experienced shock from a mine explosion near his trench on March 6. He was kept at the relief station for two days. By March 8, at the ambulance, he seemed confused and had a blank stare. He complained of a severe headache and kept pressing his head between his hands. He looked around anxiously, and even the slightest noise startled him. He would mumble a few nonsensical words, and when asked a question, he would only respond with the last phrase he had just said. A lumbar puncture indicated a very slight excess of albumin. The next day, he recognized his name. By March 12, he could respond in short words and began to comprehend what was being said. After the lumbar puncture, the headache vanished and didn’t return. On March 13, he started to write and express short phrases. By March 16, his expression was good though hesitant, and he wrote a letter to his parents about his shock. The lumbar puncture showed that the albumin levels were now normal. From the rear, on April 5, the patient sent Ravaut a postcard in perfect form, saying he was ready to return to the front.
Re lumbar puncture, Imboden quotes Podmanizky as having used lumbar puncture as a method of suggestion for the cure of abasia. See also cases 560 and 561, in which Claude cured two cases of dysbasia by the device of stovaine anesthesia of the spinal cord. Pastine also has a case in which a slight improvement was produced on removal of cerebrospinal fluid, and a sudden and complete cure was brought about by the second puncture, a very painful tap. Pastine’s case is thought by him (1916) to be in part at least organic.
Re lumbar puncture, Imboden cites Podmanizky as having used lumbar puncture as a method of suggestion for the treatment of abasia. See also cases 560 and 561, in which Claude successfully treated two cases of dysbasia using stovaine anesthesia of the spinal cord. Pastine also mentions a case where a slight improvement occurred after the removal of cerebrospinal fluid, and a sudden and complete cure was achieved by the second puncture, which was very painful. Pastine believes this case (1916) to be at least partially organic.
Bullet wound of forearm: Hysterical clenching of fist. Recovery by fatiguing the flexors.
Bullet wound of forearm: Hysterical clenching of fist. Recovery by exhausting the flexors.
Case 489. (Reeve, September, 1917.)
A soldier, 28, was thrice wounded between August 18, 1914, and July 14, 1916. The third time, a bullet passed through the fleshy part of the forearm, whereupon the hand became clenched and remained so after the wound was surgically healed. As a case of war neurosis, the man was treated by electricity, massage, passive movements, and fixation in a straight splint during a period of nine months, without result. He was admitted to Maghull Military Hospital, April 18, 1917.
A 28-year-old soldier was wounded three times between August 18, 1914, and July 14, 1916. The third injury involved a bullet passing through the soft part of his forearm, causing his hand to clench and remain that way even after the wound was surgically treated. Classified as a case of war neurosis, he underwent treatments involving electricity, massage, passive movements, and immobilization in a straight splint for nine months, but nothing worked. He was admitted to Maghull Military Hospital on April 18, 1917.
Two days after admission a treatment was given whose principle consists in producing a condition of fatigue in the muscles responsible for contracture. This fatigue is produced by continuous passive movements in a direction opposed to the normal action of the muscles in question. Many hours of forcible movement are sometimes necessary in the case of the more powerful muscles before the limp, toneless fatigue condition is brought about. Relays of men are told off for this purpose. Patients are got to assist in the work, particularly such as have been cured by the treatment. Also, the patient is himself told about the nature of spasms and the relief which the method will bring. This patient was told that after the flexor muscles were fatigued they would no longer be able to pull the fingers into the clenched position, whereupon the antagonistic muscles on the back of the forearm would begin to work.
Two days after admission, a treatment was administered that aims to create a state of fatigue in the muscles responsible for the contracture. This fatigue is achieved through continuous passive movements that go against the normal action of the muscles involved. For some of the stronger muscles, several hours of forced movement may be required to induce a limp, relaxed fatigue state. Teams of people are assigned for this task. Patients are encouraged to help with the process, especially those who have already benefited from the treatment. Additionally, the patient is informed about the nature of the spasms and how this method will provide relief. This patient was told that once the flexor muscles are fatigued, they would no longer be able to pull the fingers into a clenched position, allowing the opposing muscles on the back of the forearm to begin working.
The fingers were forcibly opened without interruption for six hours, in each case as soon as the fingers closed into the palm. In a few hours they began to return more slowly, and at the end of the six hours remained extended. The extended position was still found the following morning. The extensor muscles were feeble in action, but improved day by day. The spasm did not return. The patient was discharged July 2, 1917, about two and a half months after admission to Maghull. The hand was now strong and useful.
The fingers were forcibly opened continuously for six hours, each time as soon as they closed into the palm. After a few hours, they started to come back more slowly, and by the end of the six hours, they remained extended. The extended position was still observed the next morning. The extensor muscles were weak but improved each day. The spasm didn't come back. The patient was discharged on July 2, 1917, about two and a half months after being admitted to Maghull. The hand was now strong and functional.
Bullet through shoulder girdle: Hysterical adduction of arm. Treatment by induced fatigue.
Bullet through shoulder girdle: Extreme inward movement of the arm. Treatment through induced fatigue.
Case 490. (Reeve, September, 1917.)
A man, 29, was in hospital more than two years before the Reeve fatigue treatment was applied to a functional contracture. This man had a bullet pass through the right scapula and out the pectoralis major, June 4, 1915, was (according to patient’s story) operated two months later, then further operated for drainage of septic wounds, and from August, 1915, had his arm fixed to the side, going into spasm at any attempt to move it passively. The elbow was extended and at first the fingers were tightly flexed and wrist extended. The finger flexion and wrist flexion cleared in March, 1917, and recurred in May. Electrical massage in June, 1917, yielded free movement, but the spasm returned.
A 29-year-old man spent more than two years in the hospital before receiving the Reeve fatigue treatment for a functional contracture. He had a bullet pass through his right shoulder blade and exit out of his chest muscle on June 4, 1915. According to his account, he underwent surgery two months later, followed by another operation to drain infected wounds. Starting in August 1915, his arm was fixed to his side and went into spasms whenever anyone tried to move it. His elbow was straightened, and initially, his fingers were tightly curled and his wrist was extended. The curling of his fingers and wrist improved in March 1917 but returned in May. Electrical massage in June 1917 allowed for free movement, but the spasms came back.
The man was admitted to Maghull, June 12, 1917, that is, a little over two years after his injury. The arm sprang back to the side like a clasp knife on being released. The wrist and fingers were moved freely. Three days after admission the elbow was forcibly flexed for some hours, whereupon the spasm disappeared. Next day the arm was forcibly abducted and reabducted: for four or five hours the arm could be voluntarily abducted. Two assistants were necessary, such was the force of the adductor contraction. At the end of a week the patient was found able to lift his hand to the back of his head. There was no longer spasm.
The man was admitted to Maghull on June 12, 1917, which was just over two years after his injury. His arm snapped back to his side like a pocket knife when opened. His wrist and fingers moved freely. Three days after being admitted, his elbow was forcefully bent for several hours, and then the spasm went away. The next day, his arm was forcefully moved away from his body and then back again: for four or five hours, he could voluntarily lift his arm away from his body. Two assistants were needed due to the strength of the muscle contraction pulling his arm inward. By the end of the week, the patient could lift his hand to the back of his head. There was no longer any spasm.
Re abrupt treatments, amongst which Reeve’s treatment by induced fatigue may be counted, Babinski and Froment consider that abrupt treatment is far superior to slower psychotherapy combined with isolation, whether or not we are dealing with a recent or an old disease. So far as psychotherapy goes, Babinski wants to obtain a definite improvement, if not a cure, on the first application of treatment. According to Babinski, the patient’s faith in his physician’s power to cure him is most active at this first meeting, whose emotionality favors the cure.
Regarding sudden treatments, including Reeve’s treatment through induced fatigue, Babinski and Froment believe that abrupt treatment is much better than slower psychotherapy combined with isolation, regardless of whether the condition is new or longstanding. When it comes to psychotherapy, Babinski aims to achieve a clear improvement, if not a complete cure, during the first session. According to Babinski, the patient's belief in their doctor's ability to heal them is strongest during this initial encounter, and the emotional intensity of that moment enhances the chances of recovery.
Burial and bruises of back: Hysterical cross-legs. Treatment by induced fatigue of contractured muscles.
Burial and bruises on the back: Hysterical crossed legs. Treatment through induced fatigue of contracted muscles.
Case 491. (Reeve, September, 1917.)
A man, 32, was buried by a shell and bruised about the back, August 2, 1916. He was bedfast until February, 1917. Every attempt to move the legs brought on tremors. He was then allowed up; but the attempt to walk caused one foot to knock the other, and his ankles became bruised, necessitating cotton wool pads for feet.
A 32-year-old man was buried by a shell and injured on his back on August 2, 1916. He was confined to bed until February 1917. Every time he tried to move his legs, it caused shaking. He was then allowed to get up, but when he tried to walk, one foot hit the other, bruising his ankles and requiring cotton wool pads for his feet.
He was admitted to Maghull, June 12, with one leg crossed over the other and the thigh adductors spastic, especially on the right.
He was admitted to Maghull on June 12, with one leg crossed over the other and his right thigh muscles being overly tight, especially.
The fatigue treatment was carried out in dorsal decubitus, each leg being pulled by a man, and the separation repeated when necessary. Four hours a day for three days of this work finally reduced the spasm so that the patient was able to walk with assistance. On the sixth day he walked a mile without assistance. The spasm has not returned.
The fatigue treatment was done while lying on his back, with a person pulling each leg, and the separation repeated as needed. After four hours a day of this for three days, the spasm was reduced enough for the patient to walk with help. By the sixth day, he was able to walk a mile on his own. The spasm hasn't come back.
Re leg contractures, Bérard got successful results by continuous extension combined with injections of 1 per cent novocain into the sciatic nerve trunk and the contractured muscles. According to Babinski and Froment, there ought to be an almost certain cure of any genuine hysterical state. They quote the observations of Souques, Meige, Albert Charpentier, Clovis Vincent, Roussy, and Léri as proving this claim.
Re leg contractures, Bérard achieved successful results through continuous stretching along with injections of 1 percent novocain into the sciatic nerve trunk and the contracted muscles. Babinski and Froment assert that there should be an almost guaranteed cure for any genuine hysterical condition. They reference the observations of Souques, Meige, Albert Charpentier, Clovis Vincent, Roussy, and Léri as evidence supporting this claim.
The Reeve method, so far as it is psychotherapeutic, bears a resemblance to Clovis Vincent’s first stage of what the poilu calls torpillage, namely, the stage of crisis and of intensive reëducation. But Clovis Vincent uses in his direct and forcible reëducation the galvanic current.
The Reeve method, at least in its therapeutic aspect, is similar to Clovis Vincent’s initial stage of what the poilu refers to as torpillage, which is the crisis stage and intensive re-education phase. However, Clovis Vincent employs the galvanic current in his direct and forceful re-education.
Bullet wound of neck: Hysterical torticollis. Treatment by induced fatigue.
Bullet wound to the neck: Hysterical torticollis. Treatment through induced fatigue.
Case 492. (Reeve, September, 1917.)
A soldier, 20, had a bullet pass through the back of the neck, July 10, 1916, and returned to his dépôt surgically well October 1. A fortnight later a Zeppelin raid turned his troop out in the middle of the night, and on the morrow the man’s neck was twisted around and inclined upon the left shoulder.
A 20-year-old soldier had a bullet go through the back of his neck on July 10, 1916, and returned to his base after surgery on October 1. Two weeks later, a Zeppelin raid got his troop up in the middle of the night, and by the next day, the man's neck was twisted and leaning to the left shoulder.
Treatment followed in various hospitals, with fixation in the corrected position by plaster of Paris but without result. The patient was admitted to Maghull, April 18, 1917, with spasm of left trapezius and right sternomastoid muscles. Under hypnosis the deformity could be easily corrected. Unfortunately, it returned.
Treatment took place in different hospitals, using plaster casts to hold the corrected position but without success. The patient was admitted to Maghull on April 18, 1917, with spasms in the left trapezius and right sternomastoid muscles. The deformity could easily be corrected under hypnosis. Unfortunately, it came back.
The fatigue treatment described by Reeve was started a week after admission to Maghull. The neck was forcibly straightened and restraightened upon return to its twist. In a few hours the contracting muscles had become fatigued; the neck was straight.
The fatigue treatment described by Reeve began a week after he was admitted to Maghull. The neck was forcibly straightened and redone when it twisted back. In a few hours, the contracting muscles became tired; the neck was straight.
The next day the deformity returned slightly. The fatigue treatment was repeated. The patient was discharged well, July 2.
The next day, the deformity returned a bit. The fatigue treatment was repeated. The patient was discharged in good condition on July 2.
Burial by shell explosion: Abasia, tremors. Claw foot persistent two years cured by induced fatigue.
Burial from shell explosions: Abasia, tremors. Claw foot that lasted two years was cured through induced fatigue.
Case 493. (Reeve, September, 1917.)
A man, 24, buried by a shell, February, 1915, had had a functional “claw foot” for more than two years, cured by the Reeve fatigue treatment in less than a week. According to Reeve, claw foot is perhaps the most common of the war contractures, particularly intractable, and often seen out of hospital with an “inside splint.”
A 24-year-old man, buried by a shell in February 1915, had suffered from a functional “claw foot” for over two years, but was cured by the Reeve fatigue treatment in less than a week. Reeve noted that claw foot is probably the most common war-related contracture, particularly stubborn, and is often treated outside of hospitals with an “inside splint.”
After his burial this man could not walk, had tremors, was in bed for four months and on getting up showed strongly inverted foot. Three months’ splint treatment, strong faradic currents, massage, passive movements, special boots with leather wedges to tilt the foot over, were methods of treatment tried, but unsuccessful. At Maghull from November 18, 1916, he was treated by exercises, passive movements, suggestive and reëducative measures, and after a few months got about without sticks.
After his burial, this man couldn't walk, experienced tremors, and was in bed for four months. When he finally got up, he had a pronounced inverted foot. They tried various treatments, including three months of splint therapy, strong electrical currents, massage, passive movements, and special boots with leather wedges to adjust the foot, but none were successful. Starting November 18, 1916, he received treatment in Maghull that included exercises, passive movements, suggestive methods, and rehabilitation techniques, and after a few months, he was able to walk without support.
The claw foot continued. Toward the end of June, 1917, the feet were forcibly flexed and everted for eight hours. The deformity disappeared, but returned slightly next day. Further fatigue treatment for eight hours caused the spasm to cease permanently. He was discharged quite normal, July 20, 1917. Reeve remarks that this fatigue method might be applicable to certain hysterical contractures in civil practice.
The claw foot continued. By the end of June 1917, the feet were forcibly flexed and turned outwards for eight hours. The deformity went away, but came back a bit the next day. Additional fatigue treatment for eight hours made the spasm stop permanently. He was discharged completely normal on July 20, 1917. Reeve notes that this fatigue method might be useful for certain hysterical contractures in regular medical practice.
Skull trauma over right eye: Delirium, febrile? post-traumatic? exhaustive? Operation: Epileptiform excitement. Later, explosive diathesis: Operation: Euphoria. Seizures and slight mental change.
Skull injury above the right eye: Delirium, fever? Post-traumatic? Exhausted? Surgery: Epileptiform excitement. Later, explosive tendency: Surgery: Euphoria. Seizures and slight mental changes.
Case 494. (Binswanger, October, 1917.)
A soldier (brother choreic, sister infantile palsy) had had measles at 13 and in his fever climbed out of bed upon a couch, fell from the couch and was found by his mother lying on the floor. He was of moderate intellectual grade, of an emotional, passionate Saxon nature and had now and then been intoxicated.
A soldier (brother with a speech impediment, sister with cerebral palsy) had measles when he was 13, and during his fever, he got out of bed and climbed onto a couch, fell off the couch, and was found by his mother lying on the floor. He had average intelligence, an emotional, passionate Saxon nature, and had occasionally been drunk.
In September, 1914, he was wounded over the right eye. He did not lose consciousness but concluded that he could not get back to his own lines on account of the enemy fire. Using a knapsack to cover his head, he lay down for twenty-four hours, until rescued by a passing body of the sanitary corps who were about to leave him for dead when he called loudly to them.
In September 1914, he got injured above his right eye. He didn't pass out but realized he couldn't return to his own side because of the enemy fire. Covering his head with a knapsack, he stayed down for twenty-four hours until a passing medical unit found him. They were about to leave him for dead when he shouted out to them.
He was very weak in hospital and, towards the evening of the day after receiving his injury, he must have fallen into some sort of psychotic state lasting ten days. For this he remained quite amnestic, although he was told by comrades that he had hallucinations and had scolded and yelled, hearing voices. Apparently there were situation-deliria—the call to go over the top. Temperature, which had run to 38.8, after ten days sank to normal, and consciousness cleared up.
He was very weak in the hospital and, by the evening of the day after his injury, he must have fallen into some kind of psychotic state that lasted ten days. During this time, he couldn't remember anything, even though his comrades told him he had hallucinations and had been shouting and yelling, hearing voices. Apparently, there were situation-related delusions—the call to go over the top. His temperature, which had been as high as 38.8, finally dropped to normal after ten days, and his mind became clear again.
Was this a case of protracted febrile delirium? Or of psychosis due to commotio cerebri, that is, an effect of heightened intracranial pressure? Or was it exhaustion-delirium following loss of blood, sleep and food?
Was this a case of prolonged fever-induced confusion? Or was it psychosis caused by commotio cerebri, which is the result of increased pressure in the skull? Or was it delirium from exhaustion after losing blood, sleep, and food?
But this was not the end. The wound suppurated, and in May, 1915, eight months after the injury, operation was performed to relieve this abscess. Temperature immediately rose to from 38.4 to 38.6, the fever lasting three days, and a second psychotic phase with complete amnesia entered.[700] He went into this phase immediately after recovering from the operative narcosis, looking wildly about and cursing the sister. The patient was violently excited and was put in a straight jacket on the second day. This phase may be regarded as one of epileptiform excitement with delirium. The operation may have played a part in the psychosis.
But this was not the end. The wound became infected, and in May 1915, eight months after the injury, surgery was performed to drain the abscess. His temperature immediately rose from 38.4 to 38.6, with the fever lasting three days, and he entered a second psychotic phase with complete amnesia.[700] He entered this phase right after waking up from the anesthesia, looking around wildly and cursing the nurse. The patient was extremely agitated and was restrained in a straightjacket on the second day. This phase can be seen as one of epileptiform excitement with delirium. The surgery may have contributed to the psychosis.
There were no further psychotic phenomena which could be attributed in any way to commotio. There were, however, attacks of cortical origin and emotional seizures. The patient became emotionally excitable and lost all inhibitions against expression of emotion, such as crying. Once he actually tried to suppress his emotion with a noose about his throat. He became seclusive and withdrew within himself—a victim of Kaplan’s explosive diathesis, or of Bonhoeffer’s emotional hyperesthetic defect condition.
There were no additional psychotic symptoms that could be linked to commotio. However, there were episodes originating from the cortex and emotional seizures. The patient became emotionally volatile and lost all inhibitions against expressing emotions, like crying. At one point, he even attempted to suppress his emotions with a noose around his neck. He became reclusive and retreated into himself—a casualty of Kaplan’s explosive diathesis or Bonhoeffer’s condition of emotional hypersensitivity.
A second operation was performed in September, 1916, to loosen the brain scar, and a large splinter of bone was removed. During the operation, under local anesthesia, there was a severe cortical seizure with complete disappearance of the reflexes. Ether was then administered. Later, in the same day, there were several minor cortical attacks.
A second surgery took place in September 1916 to loosen the brain scar, and a large piece of bone was removed. During the surgery, under local anesthesia, there was a severe seizure in the cortex, resulting in the complete loss of reflexes. Ether was then given. Later that same day, there were several minor seizures in the cortex.
After this operation the man’s emotional status changed; he was no longer irritable or exclusive, but became slightly euphoric and contented. He received during the next two weeks four tablets of Sedobrol and for a long time thereafter two tablets daily. There were never any phenomena of bromidism or any suggestive effects of the bromides.
After this procedure, the man’s emotional state changed; he was no longer irritable or standoffish, but instead became a bit euphoric and satisfied. Over the next two weeks, he took four tablets of Sedobrol and for a long time after that, he took two tablets daily. There were never any signs of bromism or any noticeable effects from the bromides.
The first attack after the second operation came in November, 1916, and was followed by slight dysarthria. Repeated attacks followed which were attributed to contractions in the scar. Accordingly, a third operation was performed and an attempt was made to bridge over a defect in the right frontal bone. The man’s emotional status remained good after the operation, but further attacks appeared six weeks later and there were spells of dizziness. Occasionally, in process of thinking, he said something stuck in between his thoughts. Sometimes thinking broke off sharply as if he had cut through a wire with an electrical current in it. There was a slight reduction in attention and a slightly increased fatiguability.
The first attack after the second surgery occurred in November 1916, which was followed by mild speech difficulties. More attacks happened that were linked to tightness in the scar tissue. As a result, a third surgery was performed to fix a defect in the right frontal bone. The man's emotional state stayed stable after the operation, but more attacks came six weeks later along with episodes of dizziness. Occasionally, while thinking, he mentioned feeling like something was stuck between his thoughts. Sometimes, his thoughts would abruptly stop, as if he had severed a wire carrying an electrical current. There was a slight decrease in his attention span and a minor increase in his fatigue.
Hard service; shell explosion with loss of teeth: Vomiting. Cure by restoration of self-confidence.
Hard service; shell explosion with loss of teeth: Vomiting. Cure by rebuilding self-confidence.
Case 495. (McDowell, January, 1917.)
A married reservist was called up at the outbreak of the war and went through Mons, the Marne, and the Aisne and was finally blown up by a shell at Ypres. Early in November, 1914, he lost his speech but got it back in time to get home for Christmas. A number of teeth had been lost in the injury. Vomiting began first in England. While on leave at home he vomited at every meal. Asked whether it was his food or his thoughts, he said, “You are quite correct, Sir, you know I have always been with thinking.”
A married reservist was called up when the war started and fought at Mons, the Marne, and the Aisne, but was eventually blown up by a shell at Ypres. Early in November 1914, he lost his ability to speak but regained it just in time to make it home for Christmas. He had lost several teeth in the blast. The vomiting started while he was back in England. While on leave at home, he threw up at every meal. When asked if it was the food or his thoughts causing it, he replied, “You’re absolutely right, Sir, you know I’ve always been deep in thought.”
Under medical care, June, 1915, he was found suffering from hesitating speech, general tremulousness and emotionality. He worried a great deal on account of money matters at home. He lay awake thinking. A child became ill and died, and all the while he got worse, “thinking all the time.”
Under medical care, June 1915, he was found to be struggling with speech issues, general shakiness, and heightened emotions. He was very worried about financial problems at home. He lay awake, lost in thought. A child fell ill and passed away, and during this time, he continued to deteriorate, "thinking all the time."
It was explained to him that the vomiting was a matter of emotions. The lost teeth were replaced by false ones. As he began to get control of his emotions, he vomited less and increased in weight. Finally he was boarded for discharge and was sick again on the day of the meeting. A fortnight later when sent to sign discharge papers he vomited once more.
It was explained to him that the vomiting was linked to his emotions. His lost teeth were replaced with fake ones. As he started to manage his feelings better, he vomited less and gained weight. Eventually, he was cleared for discharge, but he got sick again on the day of the meeting. Two weeks later, when he went in to sign the discharge papers, he vomited again.
According to McDowell, the vagus may possibly be incriminated as a cause of these gastric disturbances. Practically, the vomiting is a result of emotional stress. The cure is to produce insight on the part of the patient, the removal of worry and the restoration of self-confidence.
According to McDowell, the vagus nerve might be linked to these stomach issues. Essentially, vomiting comes from emotional stress. The solution is to help the patient gain insight, eliminate worry, and restore their self-confidence.
Michell Clarke cured such cases with milk diet.
Michell Clarke treated such cases with a milk diet.
Roussy and Lhermitte find hysterical vomiting to be relatively common and as a rule without difficulty in diagnosis; but they remark that there is often some underlying organic condition to be sought for and treated after the neuropathic element has vanished. They remark, also, that there is no tendency to spontaneous cure of the disease. They advocate a strict dietetic régime and psychotherapy.
Roussy and Lhermitte consider hysterical vomiting to be fairly common and generally easy to diagnose; however, they note that there is often an underlying organic condition that needs to be identified and treated once the neuropathic element has subsided. They also point out that there is no tendency for the condition to resolve on its own. They recommend a strict diet regimen and psychotherapy.
Cure of self-accusatory (“started retreat from Mons”) and other delusions by “autognosis.”
Cure for self-blame ("began withdrawal from Mons") and other delusions through "self-knowledge."
Case 496. (Brown, January, 1916.)
Capt. William Brown, in the discussion at the Section of Psychiatry of the Royal Society of Medicine, January 25, 1916, speaks of a method of treatment which he calls autognosis—a method of giving the patient self-knowledge, by revealing to the patient through his own confessions the cause of mental change leading to his symptoms. One of Brown’s examples is that of a sergeant in the firing-line during the retreat from Mons. He was admitted to Maghull with the delusion that people thought he had given the signal for the retreat from Mons on a silver whistle, a shooting prize of his. German officers used silver whistles that made a note like his own. In fact, he had other like delusions, such as that people thought him responsible for an Edinburgh railroad accident in connection with his troop-train. A German spy might have heard this.
Capt. William Brown, during the discussion at the Section of Psychiatry of the Royal Society of Medicine on January 25, 1916, talks about a treatment method he calls autognosis—a way to help patients gain self-awareness by uncovering the reasons behind their mental changes through their own admissions, leading to their symptoms. One of Brown’s examples involves a sergeant on the front lines during the retreat from Mons. He was admitted to Maghull with the delusion that people believed he had signaled the retreat from Mons using a silver whistle, which was a shooting prize of his. German officers used silver whistles that produced a note similar to his. In reality, he had other similar delusions, like thinking that people blamed him for a railroad accident in Edinburgh related to his troop train. A German spy might have overheard this.
In the process of procuring autognosis, Capt. Brown found that at the age of 12 this man had been falsely accused of stealing pork pies from a shop, and had been brought before a magistrate. In point of fact, he proved an alibi, but he was greatly worried by the charge. According to Capt. Brown, this incident of the insistence of the false accusation was the beginning of his tendency to delusions. In two months’ time there was a remarkable improvement.
In the process of gaining self-knowledge, Capt. Brown discovered that when this man was 12 years old, he was wrongly accused of stealing pork pies from a shop and was taken before a magistrate. In reality, he proved his innocence with an alibi, but the accusation troubled him a lot. According to Capt. Brown, this incident of being falsely accused marked the start of his tendency towards delusions. Within two months, there was a significant improvement.
Re psychoanalysis, autognosis and various modifications, Forsyth remarks that when the acute stage is passed, the Shell-shock case becomes an everyday neurosis in which war experiences are merely the latest phases in the patient’s life, and that psychoanalysis may then become necessary. Eder regards the “mechanisms” of what he terms “war shock” as the Freudian mechanisms of hysteria, and has commended psychoanalysis for a few cases, preferring hypnotism for acute cases. Adrian and Yealland decry psychoanalysis on the score of time limitations.
Re psychoanalysis, self-knowledge, and various changes, Forsyth points out that once the acute stage has passed, the Shell-shock case turns into a common neurosis where war experiences are just the latest events in the patient’s life, and that psychoanalysis might then become necessary. Eder sees the "mechanisms" of what he calls "war shock" as the Freudian mechanisms of hysteria and has praised psychoanalysis for a few cases, while favoring hypnotism for acute cases. Adrian and Yealland criticize psychoanalysis because of the time constraints involved.
Deafmutism in three men shell-shocked at one time.
Deaf-mute condition in three men who were shell-shocked at the same time.
Cases 497, 498, 499. (Roussy, April, 1915.)
There were three Zouaves in a first-line trench north of Arras, January 14, 1915, who were blown up by a bomb thrown from the enemy trench some hundreds of meters away, by a mortar, a crapouillaud. This projectile burst with a great noise, louder than that of a bomb, and made a very strong windage. A dozen men were blown under the trench wall, just after entering the trench; two were killed; and the others, most of whom had been buried to the neck, were pulled out and carried, trembling, to the nearest relief post. Two of the three Zouaves were bleeding at nose and ears, and all three were absolutely deaf and mute. Evacuated to an ambulance, and thence to Paris, they arrived at Val-de-Grâce, January 17, that is to say, three days after the shell burst. They communicated with the attendants by signs; one got hold of paper and wrote several hours in the day rapid notes about the accident. However, hysteria or pure simulation was suspected in these three Zouaves, and they were placed in small separate rooms. They were informed through the physician’s remarks to his staff that these were cases of nothing but simple nervous shock such as we had often observed, and the claim was made that they would be completely well either on the morrow or the day after.
There were three Zouaves in a front-line trench north of Arras on January 14, 1915, who were blown up by a bomb thrown from the enemy trench hundreds of meters away, from a mortar, a crapouillaud. This projectile exploded with a loud noise, even louder than a bomb, and created a strong blast. A dozen men were thrown under the trench wall just after entering; two were killed, and the others, most of whom were buried up to their necks, were pulled out and carried, shaking, to the nearest medical post. Two of the three Zouaves were bleeding from their noses and ears, and all three were completely deaf and mute. Evacuated to an ambulance, and then to Paris, they arrived at Val-de-Grâce on January 17, three days after the shell exploded. They communicated with the staff using gestures; one managed to get some paper and wrote quick notes about the incident for several hours throughout the day. However, there were suspicions of hysteria or pure feigning with these three Zouaves, and they were placed in small separate rooms. They were informed through the doctor’s comments to his staff that these cases were just examples of simple nervous shock, which had been observed often, and it was claimed that they would be completely better either the next day or the day after.
On the morrow, two of them partially recovered hearing and got back their voices. They became loquacious and began to tell about the battle. The day after, the third patient began to speak. Two of them showed traces of auricular hemorrhage, and in fact, actual ear lesions were found in all three. One had a suppurative right middle ear, with perforation; another had both drums perforated and a suppurative middle ear, also on both sides. The third, who recovered his speech after the others, had perforation of the left tympanum with a little suppuration of the right ear tympanum and a slight tear of the right tympanum. In April, 1915, the hearing was cured.
The next day, two of them started to regain their hearing and got their voices back. They became talkative and began sharing stories about the battle. The following day, the third patient started to talk. Two of them showed signs of ear bleeding, and in fact, actual ear damage was found in all three. One had a severe infection in the right middle ear, with a hole; another had both eardrums perforated and an infected middle ear on both sides. The third, who recovered his speech after the others, had a hole in the left eardrum along with a minor infection in the right eardrum and a slight tear in the right eardrum. By April 1915, their hearing had fully recovered.
These men had been under fire several months, and had taken part in the battle of the Marne. It was not a question of their first baptism of fire, and in fact, each of them had been previously wounded. According to Roussy, the story is, that the shell-burst produces by displacement of air tympanic perforation, and at the same time a violent nerve shock with loss of consciousness for a few minutes. The men come to, but the ear lesion, probably exaggerated by the nervous status of its bearer, creates a complete bilateral deafness. This deafness produces an absolute hysterical mutism.
These men had been under fire for several months and had fought in the battle of the Marne. This wasn’t their first time in combat; in fact, each of them had been wounded before. According to Roussy, the story goes that a shell explosion causes an air displacement that leads to eardrum perforation and simultaneously creates a severe nerve shock, resulting in a loss of consciousness for a few minutes. The men come to, but the ear injury, likely worsened by their anxious state, results in complete deafness in both ears. This deafness leads to total hysterical mutism.
Re case groups of war neurosis, several writers speak of dangers of contagion, but also emphasize the values of contact of patients with one another in the securing of therapeutic results. What Mott has termed the atmosphere of cure was no doubt present in the three instances of Roussy just cited. The cure of one may act heterosuggestively to produce the cure of a second, and so on. Functional deafmutes are somewhat refractory as a rule. H. Campbell states that there is some danger attached to allowing large numbers of functional cases to consort together too closely. He suggests making use of small wards and screens, and a process of sorting out patients so that they shall not affect one another injuriously. Steiner especially stresses the value of individual rooms in preventing psychic infection, of which, he says, the danger is large in open dormitories. The psychic contagion is as a rule that of hysterical seizures and tremors; but complaints about faulty hospital arrangements are also readily spread. Steiner advocates never questioning a nervous patient concerning his troubles in the presence of other soldiers. To reach 60 to 70 patients, Steiner had one examining and treatment room. Roussy’s institution at Salins in 1917 had a service limited to traumatic hysteria, from which, in three months’ time, 200 subjects had been discharged cured (see Boschi).
Re case groups of war neurosis, several writers discuss the risks of contagion, but they also highlight the benefits of patients interacting with each other to achieve therapeutic outcomes. What Mott referred to as the atmosphere of cure was likely present in the three cases of Roussy mentioned earlier. The recovery of one patient might positively influence the recovery of another, and so on. Functional deaf-mutes are typically quite resistant. H. Campbell notes that there are risks associated with letting large groups of functional cases interact too closely. He suggests using smaller wards and partitions, and a method for sorting patients to prevent them from negatively affecting each other. Steiner particularly emphasizes the importance of individual rooms in avoiding psychic infection, which he claims is a significant risk in open dormitories. The typical psychic contagion involves hysterical seizures and tremors; however, complaints about poor hospital conditions also tend to spread quickly. Steiner recommends never asking a nervous patient about their issues in front of other soldiers. To accommodate 60 to 70 patients, Steiner had one examination and treatment room. Roussy’s facility at Salins in 1917 had a service focused solely on traumatic hysteria, from which 200 patients were discharged cured within three months (see Boschi).
Dysentery: Milk diet persisted in: Vomiting, incontinence, inability to walk. Cure by persuasion.
Dysentery: Continued with a milk diet: Vomiting, loss of control, inability to walk. Treated through encouragement.
Case 500. (McDowell, December, 1916.)
A soldier, 25, a low menial when war broke out, developed “dysentery and gastritis” at the Dardanelles, although even before the dysentery his nerves had gone bad. He had diarrhoea and vomiting, was sick every day, found himself unable to walk, and found himself always wet with urine dribbling day and night. Arriving in England and treated in a hospital, he still had vomiting. He had lived on milk and custard and been kept in bed.
A 25-year-old soldier, who was just a low-ranking worker when the war started, developed "dysentery and gastritis" at the Dardanelles. Even before the dysentery, he had severe anxiety. He dealt with diarrhea and vomiting, felt sick every day, couldn’t walk, and was constantly wet from urine dribbling day and night. After arriving in England and being treated in a hospital, he still experienced vomiting. His diet consisted of milk and custard, and he was kept in bed.
Capt. McDowell convinced the patient that his legs were not as weak as he supposed. He was encouraged to walk, put upon light diet and then upon ordinary diet. He became an active worker in the ward, later going for five-mile route marches. Two months later he went back to duty in good health, weighing seven pounds more than before. This man was weakminded and, when his dysentery was cured, did not dare to start eating ordinary food. He was a victim of hospital régime. Individual attention would have obviated much of the subsequent state.
Capt. McDowell convinced the patient that his legs weren't as weak as he thought. He was encouraged to walk, placed on a light diet, and then transitioned to a regular diet. He became an active worker in the ward and later went on five-mile route marches. Two months later, he returned to duty in good health, weighing seven pounds more than before. This man was easily influenced, and once his dysentery was treated, he was hesitant to eat regular food. He was a victim of the hospital routine. Individual attention could have prevented much of his later issues.
Re vomiting, see remarks under another case of McDowell (Case 495).
Re vomiting, check the notes in another McDowell case (Case 495).
Re incontinence, see Case 384, of Guillain and Barré.
Re incontinence, see Case 384, of Guillain and Barré.
Officer dies in convulsions: Servant develops hysterical convulsions, which vanish on being explained as such.
Officer dies in convulsions: Servant has hysterical convulsions that disappear once they are explained as such.
Case 501. (Hurst, March, 1917.)
An officer and his servant were blown up by a shell. The servant ran to fetch a stretcher for the officer, to whom he was much attached, but on his return the officer made a few convulsive movements and died. Immediately after, the servant had a fit. During the next two months he had eleven more. Hurst made a diagnosis of hysterical fits resulting from emotion, explained his idea of their origin and nature to the servant, and the convulsions then ceased completely.
An officer and his servant were killed by a shell explosion. The servant rushed to get a stretcher for the officer, with whom he was very close, but when he got back, the officer had a few convulsive movements and died. Right after that, the servant had a seizure. Over the next two months, he experienced eleven more. Hurst diagnosed the episodes as hysterical fits caused by strong emotions, explained his thoughts on their origin and nature to the servant, and then the convulsions completely stopped.
Re hysterical convulsions, see remarks under Case 443.
Re seizures, see remarks under __A_TAG_PLACEHOLDER_0__.
Course of a case with crises of trembling.
Course of a case with episodes of shaking.
Case 502. (Roussy, April, 1915.)
A soldier in the artillery, who had been in the lines from August as a kitchenman, looking after the food of the first line trenches, with which his shelter was connected by communication trenches, 800 meters away, was on January 17, 1915, with three other men placed in the shelter kitchen of the trenches but a short distance away from the French artillery. The firing passed over the heads of these men but they could feel the windage, which obliged them to lie down each time. The evening of that day, several hours after firing had ceased, the kitchenman had a shivering spell, with trembling that lasted all night; after which these crises came on every day. He had finally to be evacuated to the rear.
A soldier in the artillery, who had been serving as a cook for the front-line trenches since August, staying connected to his shelter through communication trenches 800 meters away, was on January 17, 1915, assigned to the shelter kitchen of the trenches, which was just a short distance from the French artillery. The shells flew over their heads, but they could feel the wind from the blasts, forcing them to lie down each time. That evening, hours after the firing stopped, the cook experienced severe shivering and trembling that lasted all night; after that, these episodes happened daily. He eventually had to be evacuated to the rear.
According to Roussy, such patients always have neuropathic taint and a history of previous crises. Such a patient ought to be handled with rather severe discipline. In this way, according to Roussy, the reappearance of a severe attack of convulsions can be prevented. But these patients cannot go back to the front.
According to Roussy, these patients always show signs of nerve damage and have a history of past episodes. Such a patient should be managed with strict discipline. This way, Roussy suggests, the chances of a severe seizure attack recurring can be minimized. However, these patients cannot return to the front lines.
Re tremors, see Cases __A_TAG_PLACEHOLDER_0__ and __A_TAG_PLACEHOLDER_1__.
Two cases of lameness cured by persuasion: Russel.
Two cases of lameness cured by persuasion: Russel.
Case 503. (Russell, August, 1917.)
A man on crutches, paralyzed completely in the right leg, partially in the left, developed paralysis in the right arm from the use of the crutch. There were marked vasomotor changes in the right leg and arm together with anesthesia to pinprick. Assured that he could move the legs perfectly he said that he had tried and failed. After a persuasive talk in private he began to use the arm, and to walk perfectly. It seems that in the trenches he had a sharp pain in the right knee, after which he did not use the leg and it gradually became more and more useless. It had been paralyzed for three months. The reason he did not use this leg was not on his own account, but on account of his mother at home. He seemed really grateful for the cure.
A man on crutches, completely paralyzed in his right leg and partially in his left, developed paralysis in his right arm from using the crutch. There were noticeable changes in circulation in his right leg and arm, along with loss of sensation to pinprick. He insisted he could move his legs just fine, but said he had tried and failed. After a convincing conversation in private, he started using his arm and was able to walk perfectly. It turns out that in the trenches, he experienced a sharp pain in his right knee, after which he stopped using the leg, and it gradually became more and more useless. It had been paralyzed for three months. His reason for not using the leg wasn't for himself, but because of his mother back home. He seemed genuinely grateful for the recovery.
Case 504. (Russell, August, 1917.)
A sergeant in hospital for a year for shell-shock still had a marked shaking of the right leg whenever he raised it from the ground. He walked in leaning on a silver headed cane. The functional nature of his shaking was explained to him by Russel, whereupon he walked out normally saying he could do without his cane. Russel suggested that crutches and sticks thus given up were often donated to the shrine. The sergeant whose cane must have cost at least three pounds beat a hasty retreat carrying the cane in front of him.
A sergeant who spent a year in the hospital for shell shock still had a noticeable tremor in his right leg whenever he lifted it off the ground. He walked while leaning on a silver-tipped cane. Russel explained the functional nature of his shaking to him, and after that, he walked out normally, stating he could manage without his cane. Russel mentioned that crutches and sticks that people overcame were often donated to the shrine. The sergeant, whose cane must have cost at least three pounds, quickly retreated while holding the cane in front of him.
Re Russel’s general point of view concerning malingerers and psychogenic cases, see under Case 458.
Re Russel’s general perspective on fakers and psychological cases, see under Case 458.
Hard patrol work: Delirium; head tremor augmented by excitement: Virtual recovery on bandaging neck, isolation, open air, to-and-fro transfers to mental and nervous wards.
Hard patrol work: Delirium; head tremor increased by excitement: Virtual recovery while bandaging the neck, isolation, fresh air, back-and-forth transfers to mental and nervous wards.
Case 505. (Binswanger, July, 1915.)
A metal moulder in civil life, 29, in military service 1907 to 1909 (no hereditary taint, moderately good scholar), became unconscious for a half hour after taking a cold drink following a somewhat long practice march, at some time during his first year of military service.
A metal molder in civilian life, 29 years old, served in the military from 1907 to 1909 (no family history of issues, moderately good student). He lost consciousness for half an hour after having a cold drink following a long practice march sometime during his first year of military service.
He was in several skirmishes in Belgium and Northern France early in the war, being once surrounded in patrol work (November 11) by Turcoes and Zouaves. There was a lively exchange of shots, in the course of which five of the eight men on patrol fell. The three survivors hid themselves for three days in a quarry, and on the fourth were found by the advancing troops, and immediately went into battle.
He was involved in several skirmishes in Belgium and Northern France early in the war, and once got surrounded while on patrol (November 11) by Turkish soldiers and Zouaves. There was an intense exchange of gunfire, during which five of the eight men on patrol were hit. The three survivors managed to hide for three days in a quarry, and on the fourth day, they were found by the advancing troops and immediately went into battle.
But during a pause while on the point of taking coffee, the man suddenly fell sick, tried to carry on, but lost consciousness and apparently remained unconscious for about three-quarters of an hour. It seems that he raved and shouted and tried to bite his fingers, being held with great difficulty by several comrades. He was removed to a dressing-station three km. distant.
But during a break while about to have coffee, the man suddenly got sick, tried to push through, but lost consciousness and seemed to be out for about forty-five minutes. He appeared to be delirious and yelled, even trying to bite his fingers, while being held down with a lot of effort by several comrades. He was taken to a medical station three kilometers away.
At the dressing-station, his head began to shake, although he was unaware of this until his attention was called to it by his comrades. He said that he felt restless and that his head ached almost continually. He was carried to the reserve hospital, and from thence, December 9, 1914, to the nerve hospital at Jena, where he was unaware of the shaking of his head (which had now lasted for three weeks), and said that he felt a thick fog in his head (to say nothing of headaches), and was only free and clear in his head while standing in the open air.
At the dressing station, his head started to shake, but he didn’t realize it until his buddies pointed it out. He mentioned that he felt restless and that his head was hurting almost all the time. He was taken to the reserve hospital, and from there, on December 9, 1914, he was moved to the nerve hospital in Jena, where he wasn’t aware of the head shaking (which had been going on for three weeks by then) and said that it felt like there was a thick fog in his head (not to mention the headaches), and he only felt clear-headed when he was outside in the fresh air.
His sleep was restless and poor; there were war dreams almost every night. In the process of getting to sleep, his arms and legs frequently twitched. He would soon tire and feel weak. Also since his dangerous experience, he had noticed a change in his speech: always fluent before, it was now hard for him to speak because one had to exert one’s head so much in speaking.
His sleep was fitful and unsatisfying; he had nightmares about war almost every night. While trying to fall asleep, his arms and legs often jerked. He would quickly become exhausted and feel weak. Since his traumatic experience, he had also noticed a change in his speech: he had always been fluent before, but now it was difficult for him to talk because he had to concentrate so much to speak.
This head tremor was in fact the most marked symptom of his illness. It would increase on every active motion of the head, but ceased almost entirely when attention was diverted. The head would then be held bent to the right.
This head tremor was actually the most noticeable symptom of his illness. It would get worse with any movement of the head, but almost completely stopped when his attention was focused elsewhere. During that time, his head would be tilted to the right.
During emotional excitement, the shaking spasm would spread over the entire upper part of the body, but would remain more severe upon the right than upon the left side. The forearms would fall into a lively shaking movement of pronation and supination. The hands and fingers would be attacked by a less marked tremor. After calm had set in, a fine tremor of the right hand would remain plainly noticeable. The musculature of facial expression would frequently fall into spasmodic movement, the left corner of the mouth twitching, the lips set for whistling, or the upper lip making movements as if snuffing spasmodically.
During emotional excitement, the shaking spasm would spread across the entire upper body, but it would be more intense on the right side than the left. The forearms would start to shake vigorously with movements of pronation and supination. The hands and fingers would show a less noticeable tremor. Once things calmed down, a noticeable fine tremor would remain in the right hand. The facial muscles would often go into spasmodic movements, with the left corner of the mouth twitching, the lips pursed as if to whistle, or the upper lip moving as if spasmodically sniffing.
Physically the man was of medium height, strongly built, with adherent lobules, and a somewhat pointed skull. The teeth were defective and irregularly placed. Both deep and skin reflexes were increased. Marked dermatographia and mechanical excitability of the muscles: periosteal reflexes strongly developed; numerous pressure points in the head. The right temple and back of the head were painful on percussion. The patient showed no disturbance in touch and pain sensibility. Outstretched tongue showed marked fibrillary twitching; speech was difficult, being slow, awkward, stumbling, and sometimes hesitating (suggesting the speech of general paresis). At other times, the speech was of a peculiar sighing, tremulous nature, reminding one of the speech of children complaining or asking for pity. Rest was secured by injections of salt solution. A few days later, the treatment was continued by a bandage about the neck. After this the tremor grew slighter and would even remain[710] absent for some hours. The patient was told to rest in bed and not to speak much; being “seriously ill,” he was kept alone. He was often irritated, querulous, and subject to outbursts of profanity. He took food well and slept well, receiving sodium bicarbonate.
The man was of average height, well-built, had attached earlobes, and a slightly pointed head. His teeth were not in good shape and were uneven. Both deep and skin reflexes were heightened. He had noticeable skin reactions and was easily excitable in his muscles; his periosteal reflexes were very strong, and there were many pressure points on his head. The right side of his head and the back were tender to touch. The patient did not have any issues with his sense of touch or pain. When he stuck out his tongue, there was noticeable twitching; his speech was slow, clumsy, and hesitant at times, reminiscent of someone with general paresis. At other times, his speech was strange, whiny, and shaky, similar to how children sound when they’re complaining or asking for sympathy. He was given salt solution injections to help him rest. A few days later, the treatment continued with a neck bandage. After that, the tremors decreased and sometimes disappeared for hours. The patient was instructed to stay in bed and limit his talking; since he was "seriously ill," he was kept isolated. He often felt irritated, complained a lot, and had fits of cursing. He ate and slept well, receiving sodium bicarbonate.
The bandage was changed after five days. The tremor was very marked. The patient was furious because visitors were refused to him. He was especially angry with his nearest relatives and his betrothed, and wrote defiant letters to all of them. He became one of the most troublesome patients in the psychiatric division of the hospital. He complained sometimes of anxiety and feelings of unrest. He received treatment by pantopon. He continued to be a very disagreeable patient, feeling himself opposed and not properly considered. He thought himself seriously ill, behaved much like a spoiled child, and was of the opinion that he would not get well in the hospital because they were grieving him so. His appetite became bad; he complained of pains in the loins and of rheumatism in the legs. A cord was found hidden in the bed. The patient expressed suicidal thoughts at various times.
The bandage was changed after five days. The tremor was quite pronounced. The patient was furious because he was denied visitors. He was especially angry with his close relatives and his fiancée, and he wrote confrontational letters to all of them. He became one of the most difficult patients in the psychiatric ward of the hospital. Sometimes he complained of anxiety and a sense of unease. He was treated with pantopon. He remained a very unpleasant patient, feeling misunderstood and neglected. He believed he was seriously ill, acted like a spoiled child, and thought he wouldn't recover in the hospital because they were upsetting him so much. His appetite worsened; he complained of pain in his lower back and rheumatism in his legs. A cord was found hidden in the bed. The patient expressed suicidal thoughts on several occasions.
At the beginning of January there was marked improvement. The headshaking ceased almost entirely; the patient walked in the garden some hours daily. However, in the middle of January, on refusal of furlough, the head-shaking began again markedly. At his request a bandage was placed on the head again for a few days. He seemed emotionally very tender; his head would shake at the sight of a dead rabbit.
At the beginning of January, there was a noticeable improvement. The head shaking stopped almost completely, and the patient spent several hours walking in the garden each day. However, in the middle of January, after being denied a leave of absence, the head shaking started up again significantly. At his request, a bandage was put back on his head for a few days. He seemed emotionally very sensitive; his head would shake at the sight of a dead rabbit.
He was transferred to the nerve division of the psychiatric clinic at the end of January. He had recently begun to complain of flickering before the eyes. The ophthalmologists established an existence of a choroiditis disseminata. The eye examination had a markedly depressing effect upon the patient, and the shaking spasm of the head appeared again. Upon being told that he would have to be sent back to the psychiatric section of the clinic, the shaking immediately disappeared (24 hours after it had begun).
He was moved to the nerve department of the psychiatric clinic at the end of January. He had recently started complaining about seeing flickering lights. The eye doctors found that he had choroiditis disseminata. The eye exam had a noticeably distressing effect on him, and the shaking spasms of his head returned. When he was told he would have to go back to the psychiatric section of the clinic, the shaking immediately stopped (24 hours after it had started).
Thereafter slow improvement followed. He stayed in the open a great deal and walked. March 2, he showed a vehement[711] outburst of anger, quarreling and using violence with a comrade. He was brought back to the psychiatric section, and in transit had a severe hysterical attack with unconsciousness, crying fits, and stepping movements of the extremities. He was promptly taken to a section for those seriously ill. The next day, upon his assurance that he could control himself, he was put in a more quiet division. He began to take part in gymnastic exercises, worked as a coachman, and then as an experiment was sent to a gentleman’s estate for recreation. At last accounts he was feeling well except that he occasionally had headaches during work. He could not work so hard as before on account of the rapid onset of fatigue, especially when working in the sun. The head-shaking recurred but seldom and lasted for a few hours only when the patient became angry or when there was much noise about.
After that, gradual improvement began. He spent a lot of time outdoors and walked around. On March 2, he had a strong outburst of anger, arguing and being violent with a buddy. He was brought back to the psychiatric unit, and during the transfer, he had a severe hysterical attack with unconsciousness, crying spells, and unusual movements in his limbs. He was quickly taken to a facility for people who were seriously ill. The next day, after he assured them that he could control himself, he was moved to a quieter area. He started participating in gym exercises, worked as a coachman, and then as an experiment, he was sent to a gentleman’s estate for some leisure time. As of the latest updates, he was feeling good, except that he occasionally experienced headaches while working. He couldn't handle the workload as he did before due to getting tired quickly, especially when working in the sun. The head-shaking happened infrequently and lasted only a few hours when he got angry or when there was a lot of noise around him.
Rationalization of war memories: Returned to duty.
Rationalizing war memories: Back on duty.
Case 506. (Rivers, February, 1918.)
A young English officer was wounded just as he was extricating himself from burial in a mass of earth. He became nervous and sleepless and lost his appetite. After the wound had healed, he was sent home on leave, which had to be extended as he got worse. An out-patient in London for a time, he was finally sent to a convalescent home, still troubled with insomnia, battle dreams and concern about his recovery. He made light of his condition and was on the point of being returned to duty by the medical board, when his sleeplessness led to his being sent to Craighlochart War Hospital.
A young English officer was injured just as he was digging himself out from under a pile of dirt. He became anxious, couldn’t sleep, and lost his appetite. After the wound healed, he went home on leave, which had to be extended because he got worse. He was an outpatient in London for a while and was eventually sent to a recovery home, still struggling with insomnia, nightmares about battle, and worries about getting better. He downplayed his situation and was close to being sent back to duty by the medical board when his inability to sleep resulted in him being sent to Craighlochart War Hospital.
He could not sleep without a light in the room, else every sound attracted his attention. He tried hard all day long to banish all unpleasant and disturbing thoughts, but at night it took him a long time to get to sleep and then came vivid dreams of warfare. He did not, himself, feel that he could ever forget the war scenes.
He couldn't sleep without a light in the room; otherwise, every noise caught his attention. He spent the whole day trying to push away all the unpleasant and disturbing thoughts, but at night it took him a long time to fall asleep, and then he had vivid dreams about war. He didn't feel like he could ever forget the war scenes.
Rivers, in general believing that the attempt to banish such experiences absolutely from the mind is poor psychotherapy, narrated his views to the patient. Rivers advised him no longer to try to banish the memories, but to try to transform them into tolerable, if not pleasant, companions. The war experiences and anxieties were talked over. That night the man had the best night he had had for five months, and during the following week the sleeplessness was no longer so painful and distressing. If unpleasant thoughts came, they had to do rather with home life than with the war. General health improved; insomnia diminished. He was at last able to return to duty.
Rivers, believing that trying to completely erase such experiences from the mind is ineffective therapy, shared his thoughts with the patient. He encouraged him not to suppress the memories any longer, but to work on transforming them into manageable, if not entirely pleasant, companions. They discussed the war experiences and anxieties. That night, the man had the best sleep he had enjoyed in five months, and over the following week, his sleeplessness became less painful and distressing. If unpleasant thoughts arose, they were more related to his home life than the war. His overall health improved, and his insomnia decreased. He was finally able to return to duty.
Rationalization of war memories.
Justifying war memories.
Case 507. (Rivers, February, 1918.)
An English officer was buried by shell explosion and developed severe headache, vomiting and disorder of micturition, yet remained on duty for more than two months. Collapse came when he went out to seek a fellow officer and found the body blown to pieces, with head and limbs severed from the trunk. This vision haunted him in dreams. Sometimes the officer appeared as on the battlefield; again as leprous. The officer would come nearer and nearer in the dream, until the patient woke pouring with sweat and in utmost terror. Accordingly, he was afraid to go to sleep, and spent all day thinking painfully about the night to come. Advice to keep all thoughts of war out of mind merely brought the memories in sleep upon him with redoubled force and horror.
An English officer was buried by a shell explosion and developed severe headaches, vomiting, and problems with urination, yet he stayed on duty for over two months. He collapsed when he went out to find a fellow officer and discovered the body blown to pieces, with the head and limbs detached from the torso. This image haunted him in his dreams. Sometimes the officer appeared as he did on the battlefield; other times he looked like he had leprosy. The officer would come closer and closer in the dream until the patient woke up drenched in sweat and filled with fear. As a result, he was scared to go to sleep and spent all day anxiously thinking about the coming night. Advice to keep all thoughts of war out of his mind only made the memories return in his sleep with even more intensity and horror.
Rivers’ therapy was to draw attention to the fact that the terrible mangling proved conclusively that the officer had been killed outright and without pain. The officer said he would now no longer attempt to banish the thoughts and memories of his friend, but would concentrate on the pain and suffering his friend had been spared. No dreams at all came for several nights, but one night in his dream he went out into No-Man’s-Land and saw the mangled body, but without horror. He knelt down, as he had in the original experience, and woke as he was taking off the Sam Browne belt to send to the relatives. A few nights later came another dream in which he talked with his friend. There was but one more dream in which horror occurred.
Rivers’ therapy was meant to highlight that the terrible injuries clearly showed that the officer had been killed instantly and without pain. The officer said he would no longer try to push away the thoughts and memories of his friend, but would instead focus on the pain and suffering his friend had avoided. For several nights, he didn’t have any dreams, but one night he found himself in a dream where he went into No-Man’s-Land and saw the mangled body, but without feeling horror. He knelt down like he had during the original event, and woke up as he was about to take off the Sam Browne belt to send to the family. A few nights later, he had another dream where he spoke with his friend. There was only one more dream in which he felt horror.
Rationalization of war memories: Eventually unfitted for military service.
Rationalizing war memories: Ultimately unfit for military service.
Case 508. (Rivers, February, 1918.)
A young English officer, after doing well for a period, was rendered unconscious by shell explosion. The first thing he remembered was being led by his servant towards his base, thoroughly broken down. He had headaches, sleeplessness, war dreams and spells of terrible depression appearing with absolute suddenness, unlike ordinary “blues.” For ten days in hospital no such attack appeared, but one evening he came to Rivers pale and anxious. A few minutes before, he had been writing a letter in his usual mood, when this causeless depression came on. In the afternoon he had walked about on some neighboring hills. The letter dealt with no depressing matter. In ten minutes the depression vanished. Nine days later another came as he was standing idly looking out of a window. The attack lasted for several hours, as no physician was present to meet the issue. If he had had a revolver he would have shot himself.
A young British officer, after performing well for a while, was knocked unconscious by a shell explosion. The first thing he remembered was being escorted by his servant back to his base, feeling completely broken. He experienced headaches, insomnia, nightmares about the war, and intense spells of depression that came on suddenly, unlike regular "blues." He spent ten days in the hospital without any such episode, but one evening he approached Rivers looking pale and anxious. Just minutes before, he had been writing a letter in his usual mood when this unexplained depression hit him. Earlier that afternoon, he had taken a walk on some nearby hills. The letter didn't touch on any depressing topics. Within ten minutes, the depression faded away. Nine days later, another episode struck while he was idly staring out a window. This attack lasted for several hours, as no doctor was available to help. If he had had a gun, he would have shot himself.
Rivers was inclined to interpret these gusts of depression as due to a forgotten but active experience. As there was no definite tendency to dissociation, Rivers hesitated to plunge in with the hypnotic method, nothing short of which, however, served to recall the incident. The man was gravely apprehensive about fitness for further service, and was repressing his fear, as he thought it either was cowardice or would be called cowardice. The patient, by his discussions with Rivers, had already become familiar with the idea that the gusts of depression might be due to a submerged experience. Perhaps, however, there had been no experience, and the patient was advised that possibly the thing repressed was the idea about fitness for service. Accordingly, the patient agreed to face the situation. One transient attack of morbid depression occurred, after an operation. Then the man fell into a state of anxiety neurosis such that he was passed by a medical board as unfit for military service.
Rivers thought these episodes of depression might be linked to a forgotten but still active experience. Since there wasn't any clear sign of dissociation, Rivers was hesitant to use hypnosis, which was the only method that could potentially bring back the incident. The man was seriously worried about being fit for further service and was hiding his fear, believing it might either be cowardice or be seen as such. Through discussions with Rivers, the patient had already started to understand that his depression might be connected to a buried experience. However, it was possible that there hadn't been any specific experience, and the patient was advised that what he was actually repressing was his concerns about being fit for service. As a result, the patient agreed to confront the situation. After an operation, he experienced a brief episode of severe depression. Then, he developed such a level of anxiety neurosis that a medical board declared him unfit for military service.
Rationalization of war memories: Commission relinquished.
Rationalization of war memories: Commission given up.
Case 509. (Rivers, February, 1918.)
An oldish English officer lost consciousness while looking at the havoc wrought by shell explosion. Probably there was a second shell that sent him off. He was eventually admitted to an English hospital with paresis and anesthesia of legs, severe headache, sleeplessness and terrifying dreams. Hypnotic drugs and advice neither to read nor to talk about the war were the measures adopted and after two months in hospital he was given three months leave. He buried himself in the heart of the country, away from relatives, with aspirin and bromides. He began to sleep better and had less headache. When the president of the medical board asked a question about trenches at the end of his period of leave, however, he broke down and wept. He again repaired to the country for two months’ leave, for the chosen treatment by isolation and repression.
An older English officer passed out while witnessing the destruction caused by a shell explosion. There was likely a second shell that knocked him out. He was eventually admitted to an English hospital with leg paralysis and numbness, severe headaches, insomnia, and terrifying dreams. They prescribed hypnotic drugs and advised him not to read or talk about the war. After two months in the hospital, he was granted a three-month leave. He secluded himself in the countryside, far from family, taking aspirin and bromides. He started sleeping better and experienced fewer headaches. However, when the president of the medical board asked him about trenches at the end of his leave, he broke down and cried. He returned to the countryside for another two months’ leave, continuing with the chosen treatment of isolation and repression.
An order was then given that all officers must be either in hospital or on duty. He was sent to an inland watering place and treated by baths, electricity and massage, whereupon he rapidly became worse, especially as to sleep. He was transferred to Craiglochart in an emaciated state, with an expression of anxiety and dread, paresis of legs, sleeplessness and war dreams.
An order was then given that all officers had to be either in the hospital or on duty. He was sent to a spa in the countryside and treated with baths, electricity, and massage, but he quickly got worse, particularly regarding his sleep. He was moved to Craiglochart in a very thin state, showing signs of anxiety and fear, weakness in his legs, insomnia, and nightmares about the war.
He was now advised to give up repressing, to read and talk a little about the war, and to accustom himself to thinking about war experiences. He did this but half-heartedly, as he thought the ideal treatment was what he had so long followed. Nevertheless, he got distinctly better and the content of the war dreams was altered to home scenes. He was still loath to acknowledge his improvement and thought that he would have recovered if he had not been taken from his retreat and sent to hospital. As it was obvious that he would be of no further use in the army, he was allowed to relinquish his commission.
He was now advised to stop holding back, to read and talk a bit about the war, and to get used to thinking about his war experiences. He did this but not very enthusiastically, as he believed the best approach was what he had been following all along. Still, he definitely felt better, and the content of his war dreams shifted to scenes from home. He was still reluctant to admit he was improving and thought he would have fully recovered if he hadn't been pulled from his retreat and sent to the hospital. Since it was clear he wouldn't be of any further use in the army, he was allowed to give up his commission.
Rationalization of war memories, without redeeming feature as nucleus.
Rationalizing war memories, without any redeeming qualities at the core.
Case 510. (Rivers, February, 1918.)
An English officer was flung by shell explosion so that his face struck the ruptured and distended abdomen of a dead German. The officer did not immediately lose consciousness and got distinct impressions of taste and smell and an idea of their source. After a period of unconsciousness he came to, vomiting and much shaken. He carried on several days, still troubled by vomiting and haunted by taste and smell images. Several months later he was observed by Rivers suffering from horrible dreams, in which the battle experience was faithfully reproduced. He got no relief except when he went into the country, far from every suggestion of war. Rivers’ psychotherapeutic plan of finding a redeeming feature in the experience, upon which the patient might concentrate, failed because there was no redeeming feature. Accordingly, it was thought best that the man should leave the army and seek the conditions that had given him slight relief.
An English officer was thrown by a shell explosion so that his face hit the torn and swollen abdomen of a dead German. The officer didn’t lose consciousness right away and had clear impressions of taste and smell, along with an idea of where they came from. After a period of unconsciousness, he woke up, vomiting and very shaken. He struggled for several days, still bothered by vomiting and haunted by images of taste and smell. A few months later, Rivers observed him suffering from terrible dreams, in which his battle experience was vividly recreated. He found no relief except when he went out to the countryside, far from any reminders of war. Rivers’ plan to help him find a positive aspect of his experience to focus on didn’t work because there was no positive aspect. Therefore, it was decided that the man should leave the army and seek the conditions that had given him some small relief.
Re psychoanalysis and its modifications, see remarks under Case 496, under which several favorable opinions were mentioned. Boschi in his report on French conditions gives no reference concerning psychoanalysis or hypnosis. Bruce has found blended with the war dreams many episodes quite alien to the war, and considers that the patient’s ante-bellum history is of importance, since ante-bellum emotions may be revivified by the war. Craig states that he has not been impressed favorably by the results of psychoanalytic treatment. Arinstein from Russian experience gives preference to Dubois’ psychotherapy over hypnosis and psychoanalysis. Nonne states that the data of the war prove that hysteria is neither a degenerative disease according to classical theory, nor a disease based upon Freudian principles.
Re psychoanalysis and its updates, see remarks under Case 496, where several positive opinions were mentioned. Boschi, in his report on the situation in France, makes no reference to psychoanalysis or hypnosis. Bruce found that many dream episodes related to the war were mixed with those completely unrelated, and he believes the patient’s pre-war history matters since pre-war emotions might resurface because of the war. Craig says he hasn’t been impressed with the outcomes of psychoanalytic treatment. Arinstein, based on Russian experience, prefers Dubois’ psychotherapy to hypnosis and psychoanalysis. Nonne claims that war data show hysteria is neither a degenerative disease according to classical theory nor a condition based on Freudian principles.
Post rheumatic “paraplegia” (or abulia?) cured by removal of crutches, after question of discharge “unfit” had been raised.
Post rheumatic "paraplegia" (or abulia?) cured by taking away the crutches, after the issue of being discharged as "unfit" was brought up.
Case 511. (Veal, November, 1917.)
A soldier, 23, had fever with swelling of several joints and temperature in 1915, and was furloughed to England. He complained of pains in the limbs and shortness of breath, and was put in hospital. As he did not improve, he was sent to a special hospital for baths and electricity. There he remained from August, 1915, to March, 1916, with D’Arsonval baths, cataphoresis, electric treatment and massage.
A 23-year-old soldier had a fever and joint swelling in 1915 and was sent on leave to England. He reported experiencing pain in his limbs and shortness of breath, which led to his hospitalization. When he didn't get better, he was transferred to a specialized hospital for baths and electrical treatments. He stayed there from August 1915 to March 1916, receiving D’Arsonval baths, cataphoresis, electric therapy, and massage.
He was now sent to the second Northern General Hospital to see whether he should be discharged permanently unfit. Here he shuffled along on two crutches, very tremulous, and sweating, and suffering from palpitation on exertion. He wanted to take poison if he could not be cured.
He was now sent to the second Northern General Hospital to see if he should be permanently discharged as unfit. Here, he shuffled along on two crutches, very shaky, sweating, and experiencing a rapid heartbeat with any effort. He wanted to take poison if he couldn't be cured.
The crutches were taken away. He was asked to walk up and down. He had to be supported at first and fell several times. The exercises were continued. Massage and drugging were stopped. The next day he was able to stand alone. In twenty-four hours he walked by himself. The other patients in the ward encouraged him on account of the genuine exertions he was making to get well. April 7, he returned to duty, smart and well set up.
The crutches were taken away. He was asked to walk back and forth. He needed support at first and fell several times. The exercises continued. Massage and medication were stopped. The next day, he could stand on his own. In twenty-four hours, he walked by himself. The other patients in the ward cheered him on because of the real effort he was putting in to recover. On April 7, he returned to duty, looking sharp and fit.
Babinski and Froment always give the suspected subject the benefit of the doubt, never uttering the word simulation in the presence of the soldier, and proceed to psychotherapy; for psychotherapy will act to cure simulation or exaggeration just as it acts to cure hysteria. They say that in their experience, all these disorders of doubtful nature—that is, that lie diagnostically between hysteria, exaggeration, and simulation—are as a rule cured by resort to psychotherapy provided that the due amount of energy, tact, and perseverance is employed. See also remarks under Case 453. Veale’s case (511) never showed mauvaise volonté, and nothing more than aboulia.
Babinski and Froment always give the suspected subject the benefit of the doubt, never using the word simulation in front of the soldier, and move forward with psychotherapy; because psychotherapy can help resolve both simulation and exaggeration just like it helps with hysteria. They mention that in their experience, all these conditions that are uncertain—that is, those that fall diagnostically between hysteria, exaggeration, and simulation—are usually resolved through psychotherapy, provided the right amount of energy, tact, and persistence is applied. See also remarks under Case 453. Veale’s case (511) never displayed mauvaise volonté, and showed nothing more than aboulia.
“Trench foot,” “neuritis,” a year of astasia-abasia or at least of complaint of inability to stand or walk. Treatment by a “cruel though justifiable” process.
“Trench foot,” “neuritis,” a year of not being able to stand or walk or at least complaining about it. Treatment through a “harsh but necessary” method.
Case 512. (Veale, November, 1917.)
A regular army man, 38, well built and muscular, in Flanders the first winter, returned to England in January, 1915, with “trench foot.” “Neuritis” then developed, with loss of power to walk. Baths, electricity, massage, sympathetic wheeling about in a chair by women, all failed.
A regular army guy, 38, fit and muscular, spent the first winter in Flanders, and came back to England in January 1915 with "trench foot." Then he developed "neuritis," which left him unable to walk. Baths, electrical treatments, massages, and being pushed around in a chair by women all didn’t help.
January 11, 1916, he still complained of inability to walk or stand. The reflexes were exaggerated. He was able to get into a wheel chair from bed by jerks, associated with palpitation, tremors, flushing and sweating.
January 11, 1916, he still complained about not being able to walk or stand. His reflexes were overactive. He could get into a wheelchair from bed in a jerky manner, accompanied by rapid heartbeat, shaking, flushing, and sweating.
He was told that he had now recovered from the neuritis. Crutches, sticks and wheelchair were removed. He flopped about and then lay on the bed exhausted. In a few days he began to shuffle about and was put on the stationary bicycle. January 29, he left the hospital well, remarking that though the treatment at first seemed cruel, it was fully justified.
He was informed that he had now recovered from the neuritis. Crutches, canes, and the wheelchair were taken away. He flopped around and then collapsed onto the bed, exhausted. In a few days, he started to shuffle around and was put on the stationary bike. On January 29, he left the hospital feeling good, noting that although the treatment initially felt harsh, it was completely justified.
Re genuine polyneuritis, Mann gives German experience regarding neuritis as somewhat frequent and affecting a special form which he terms polyneuritis neurasthenica. He states that the commonest instances of mononeuritis developing in the war are the sciatic and trigeminal. The neuritis often outlasts the other symptoms. The treatment was rest, tepid baths, and electricity. Naturally, alcohol and syphilis must be excluded in the diagnosis.
Re genuine polyneuritis, Mann shares insights from Germany about neuritis, mentioning it's relatively common and takes a specific form he calls polyneuritis neurasthenica. He notes that the most frequent cases of mononeuritis seen during the war are the sciatic and trigeminal types. The neuritis often persists longer than the other symptoms. The treatment included rest, warm baths, and electrical therapy. Naturally, alcohol and syphilis need to be ruled out in the diagnosis.
Nonne also described non-alcoholic, non-syphilitic, and non-infectious polyneuritis in neurasthenics, which he, however, finds most common in the ulnar, median, radial, anterior crural and posterior tibial nerves.
Nonne also described non-alcoholic, non-syphilitic, and non-infectious polyneuritis in people with neurasthenia, which he finds most often in the ulnar, median, radial, anterior crural, and posterior tibial nerves.
Re “spa” treatment, Turner thinks there may be easily too much massage, electricity, bathing. He prefers segregation in special hospitals to “spa” measures in general hospitals, prefers occupation to rest, and calls attention to the stimulating value of the gratuity to be paid on leaving the hospital.
Re “spa” treatment, Turner thinks there might be way too much massage, electricity, and bathing. He prefers separate hospitals for treatment instead of “spa” options in general hospitals, favors activity over rest, and highlights the motivating factor of the tip that patients are expected to pay when they leave the hospital.
Shell-shock paraplegia: Treatment by bed, cigarettes and chocolates altered to isolation, no tobacco, no visitors, faradization. Recovery.
Shell-shock paraplegia: Treatment by bed rest, cigarettes, and chocolates changed to isolation, no tobacco, no visitors, faradization. Recovery.
Case 513. (Buzzard, December, 1916.)
Early in the war, a lad, 19, was blown up by a shell. He was sent home paralyzed from waist down, and was seen by Capt. Buzzard after he had spent ten months in various hospitals, “carefully nursed, on the water bed, constantly using a bed urinal, smoking innumerable cigarettes, and eating countless chocolates.” He could not move his legs. They were wasted and flaccid. The knee-jerks could be got with difficulty. Plantar reflexes flexor. Complete anesthesia from umbilicus downwards, but preservation of abdominal reflexes. The navel did not shift downwards when the patient attempted to sit up. The incontinence was not real; urine was passed into the urinal at appropriate intervals.
Early in the war, a 19-year-old boy was blown up by a shell. He came home paralyzed from the waist down and was seen by Capt. Buzzard after spending ten months in different hospitals, “carefully nursed, on the water bed, constantly using a bed urinal, smoking countless cigarettes, and eating endless chocolates.” He couldn't move his legs. They were weak and limp. The knee-jerk reflexs were difficult to elicit. Plantar reflexes were flexor. He had complete numbness from the belly button down, but abdominal reflexes were intact. The navel didn't move downwards when the patient tried to sit up. The incontinence wasn't genuine; urine was passed into the urinal at appropriate intervals.
Buzzard directed treatment “not to his spinal cord but to his mind; isolation; the stoppage of tobacco and all visits; the assurance that he would rapidly get well, together with some suggestive faradization of his legs.” This brought about a cure in a very short period. The atrophied legs eventually grew strong enough to walk.
Buzzard focused his treatment “not on his spinal cord but on his mind; isolating him; stopping tobacco use and all visits; reassuring him that he would recover quickly, along with some suggestive electrical stimulation of his legs.” This led to a cure in a very short time. His weakened legs eventually became strong enough for him to walk.
Re cigarettes in Shell-shock, Mott decries the over-liberal gifts of cigarettes that induced cigarette habits in both officers and men. Of course, the cigarettes are still more detrimental to cases of soldier’s heart than to other cases of neurosis. Mott remarks how over-frequent are the social tea-parties, joy rides and drives given by well-meaning ladies for the “poor dears,” actually perpetuating neuroses.
Re cigarettes in Shell-shock, Mott criticizes the excessive distribution of cigarettes that led to smoking habits among both officers and soldiers. Naturally, the cigarettes are even more harmful to cases of soldier’s heart than to other types of neurosis. Mott points out how common the social tea parties, joy rides, and drives organized by well-meaning women are for the “poor dears,” which actually continue to sustain neuroses.
Re atrophy, Babinski and Froment again bring up the question whether muscular atrophy can be brought about by a hysterical motor disorder. In point of fact, Charcot and Babinski were the first to describe the true hysterical amyotrophy, but this hysterical amyotrophy is exceptional in hysterical paralysis, and is slight when it occurs.
Re atrophy, Babinski and Froment again raise the question of whether muscle atrophy can be caused by a hysterical motor disorder. In fact, Charcot and Babinski were the first to describe true hysterical amyotrophy, but this hysterical amyotrophy is rare in cases of hysterical paralysis and is mild when it occurs.
Shell-shock blindness, mutism, deafness: Blindness spontaneously vanished, 24 hours. Mutism, 2-3 months. Deafness cured by “small operation.”
Shell-shock blindness, mutism, deafness: Blindness spontaneously disappeared after 24 hours. Mutism lasted 2-3 months. Deafness was fixed by a "minor surgery."
Case 514. (Hurst, September, 1917.)
A lance corporal, 26, became blind, deaf and dumb, though without losing consciousness, when blown up by a shell, August 29, 1916. His sight returned next day. On reaching England he talked in his sleep. Encouragement, electricity, etherization failed to effect improvement. One night in November he woke up and asked the sister for a drink; thereafter he talked normally.
A 26-year-old lance corporal became blind, deaf, and mute, but remained conscious, after being hit by a shell on August 29, 1916. His sight came back the next day. Once he got to England, he spoke in his sleep. Attempts at encouragement, electric treatment, and anesthesia didn’t help. One night in November, he woke up and asked the nurse for a drink; after that, he spoke normally.
Seven months after the shell explosion he was transferred to the neurological section at Netley, March 21, 1917. Deaf to air and bone conduction, a loud noise behind him caused a slight tremor of hands, with blinking and dilatation of pupils; but further stimuli of the same sort failed to produce such reactions. Normal nystagmus and giddiness on functional tests of vestibular nerve and canals. The internal ear was then probably free from organic changes. Since shell-shock mutism is always hysterical, it was probable that the deafness was hysterical. Under hypnosis (staring at lines for fifteen seconds) he showed no change. During natural sleep, also, a shout of “Fire” and metallic noises failed to wake the patient or to produce contraction of eyelids. Electric suggestion (despite the patient’s belief in electricity) and reëducation failed.
Seven months after the shell explosion, he was transferred to the neurological section at Netley on March 21, 1917. He was deaf to air and bone conduction; a loud noise behind him caused a slight tremor in his hands, along with blinking and dilated pupils. However, further similar stimuli didn’t produce those reactions. He showed normal nystagmus and dizziness on functional tests of the vestibular nerve and canals. The inner ear was likely free from any organic changes. Since shell-shock mutism is always hysterical, it was likely that the deafness was hysterical as well. Under hypnosis (by staring at lines for fifteen seconds), he showed no change. Similarly, during natural sleep, a shout of “Fire” and metallic noises didn’t wake him or cause any eyelid contraction. Electric suggestion (despite the patient’s belief in electricity) and reeducation were unsuccessful.
April 16, he was told that a small operation would have to be done April 20. To this he readily consented. Two small incisions were made behind the ear under light ether and suture was inserted. A loud noise was made during the “operation”; he heard this noise and jumped from the table. To his intense delight normal hearing returned in a few minutes. Next day hearing was tested and found normal to air and bone conduction. He was discharged to duty three weeks later and on his way to France, June 29, demonstrated his normal hearing to the physicians.
On April 16, he was informed that a minor surgery would be necessary on April 20. He quickly agreed to this. Two small cuts were made behind his ear under light anesthesia, and stitches were put in. There was a loud noise during the “surgery”; he heard it and jumped off the table. To his great joy, his normal hearing came back within a few minutes. The next day, his hearing was tested and found to be normal for both air and bone conduction. He was cleared to return to duty three weeks later, and on his way to France on June 29, he demonstrated his normal hearing to the doctors.
Deafness: cure by stimulating vestibular apparatus.
Deafness: treat by stimulating the vestibular system.
Case 515. (O'Malley, May, 1916.)
A private, 20 years of age, lost speech and hearing after the battle of Neuve Chapelle. Eight days later he came under the care of the laryngologist in a very excited state, pointing to lips and ears and carrying a note with information concerning his deafmutism.
A private, 20 years old, lost his speech and hearing after the battle of Neuve Chapelle. Eight days later, he came under the care of the laryngologist in a very agitated state, pointing to his lips and ears and carrying a note with information about his deafness and mutism.
Dr. O’Malley wrote on a piece of paper that he would restore the patient’s speech and hearing. Dr. O’Malley then used the mirror until the point of retching, and wrote, “You can speak now; count up to ten loudly.” He did.
Dr. O’Malley wrote on a piece of paper that he would restore the patient’s speech and hearing. Dr. O’Malley then used the mirror until he felt nauseous and wrote, “You can speak now; count up to ten loudly.” He did.
Dr. O’Malley next used the cold water douche to the right ear to the point of giddiness, then shouting through a speaking-tube (see description below). The patient then found he could hear and the tears streamed down his face. Thereafter he was able to converse freely. Dr. O’Malley writes:
Dr. O’Malley next used a cold water spray on the right ear until the patient felt dizzy, then shouted through a speaking tube (see description below). The patient then realized he could hear, and tears streamed down his face. After that, he was able to talk freely. Dr. O’Malley writes:
The treatment of functional deafness consists in exciting the vestibular apparatus as follows. Cold or hot water is allowed to flow in a steady stream into and out of the external auditory meatus by means of a tube attached to a receptacle placed about one and a half to two feet above the patient’s head and continued until he becomes very giddy and an active nystagmus is produced. A speaking-tube three feet long is then used by placing the ear-piece in the ear so treated, and the surgeon shouts into the mouth-piece the assertion, “You hear now,” and the answer, “Yes” comes promptly. The tube is now dropped and a conversation held as if no deafness ever existed. So far I have found the treatment of one ear sufficient. The patient is usually very emotional, as the disturbed vestibular function, which in these cases responds easily and markedly, causes him to feel as uncomfortable as a bad sailor on a stormy voyage. This feeling, however, rapidly gives way to one of pleasure at the return of his hearing. Where functional deafness and mutism co-exist it does not appear to be material which is treated first. In two cases of this kind under my care I treated the loss of voice first.
The treatment for functional deafness involves stimulating the vestibular system in the following way. Cold or hot water is allowed to flow steadily in and out of the ear canal using a tube connected to a container positioned about one and a half to two feet above the patient's head, and this continues until the patient feels very dizzy and active nystagmus occurs. A three-foot speaking tube is then used by placing the ear piece in the treated ear, and the surgeon loudly states, “You hear now,” to which the response, “Yes,” comes promptly. The tube is then put aside, and a conversation is carried out as if no deafness ever existed. So far, I have found treating just one ear to be sufficient. The patient usually feels quite emotional, as the disrupted vestibular function, which reacts easily and noticeably in these cases, makes them feel as uncomfortable as a bad sailor during a rough sea journey. However, this discomfort quickly turns into pleasure at the return of their hearing. When functional deafness and mutism occur together, it doesn't seem to matter which condition is treated first. In two cases of this nature that I've handled, I addressed the loss of voice first.
Bullet through mouth; Hysterical mutism. Treatment by operative manipulation.
Bullet through mouth; Hysterical mutism. Treatment by surgery.
Case 516. (Morestin, January, 1915.)
A Colonial infantryman, 32, was wounded December 17, 1914, at the Boisselle, being struck by a bullet which entered on the right side in the upper part of the neck and came out behind the left side of the mouth, having traversed the tongue, broken two teeth, and caused a good deal of hemorrhage by mouth. The patient felt his tongue swell, and from this time on he could not pronounce a word. He was sent to the ambulance, then to Mien, then to Saint Germain, and finally to Morestin’s surgical service. With wounds by this time healed, the patient found it hard to open his mouth. There was no trace of fracture of the lower jaw. The tongue could be only incompletely examined. The man swallowed liquids easily but could take no solid food. He tried hard to speak, made pantomime movements, grew emotional and lachrymose.
A Colonial infantryman, 32, was injured on December 17, 1914, at Boisselle, hit by a bullet that entered on the right side of his upper neck and exited behind the left side of his mouth, having gone through his tongue, broken two teeth, and caused significant bleeding from his mouth. The patient felt his tongue swelling, and from that point on, he couldn’t pronounce a word. He was taken to an ambulance, then to Mien, then to Saint Germain, and finally to Morestin’s surgical service. By the time his wounds had healed, he found it difficult to open his mouth. There was no sign of a fracture in his lower jaw. The tongue could only be partially examined. He swallowed liquids easily but couldn’t eat solid food. He struggled to speak, made gestures, and became emotional and tearful.
On the whole, however, it seemed that his inability to articulate sound could not be due directly to the lesion. There must be either simulation or hysteria. For four days he was attentively watched, and not once did he pronounce a word. He grew more and more stricken and humiliated by his plight. Rigorous diet did not cause his mutism to cease. Isolation and ennui did not decide him to talk. Accordingly, it was announced, in the man’s hearing, that an operation was to be done to restore speech. January 9, 1915, his face was copiously washed with alcohol and ether. Cocaine was injected to secure anesthesia and resolution of the muscles of mastication. Six c.c. of a 1-100 solution on each side. Shortly the surgeon began to open the jaws, against decreasing resistance. The tongue, which was not spastic, was seized with a tractor and rhythmic movements were executed with it. After a few of these movements, joy was painted on the features of the patient. He said that he wanted to speak and that he was about to speak. He shook[723] the surgeon’s hands effusively and said, “Merci.” Although the first words came hard, little by little speech became free and a perfectly sincere elation at having recovered speech set in.
Overall, though, it seemed that his inability to speak wasn’t directly caused by the injury. There had to be either faking or hysteria involved. For four days, he was closely monitored, and not once did he say a word. He grew increasingly distressed and embarrassed by his situation. A strict diet didn’t make his silence go away. Being alone and bored didn’t motivate him to talk. So, it was announced for him to hear that an operation would be performed to restore his speech. On January 9, 1915, his face was thoroughly cleaned with alcohol and ether. Cocaine was injected to ensure anesthesia and relaxation of the chewing muscles. Six cc of a 1-100 solution was administered on each side. Shortly after, the surgeon began to open his jaws against lessening resistance. His tongue, which wasn’t spastic, was gripped with a device, and rhythmic movements were applied to it. After a few of these movements, joy appeared on the patient’s face. He expressed his desire to speak and said he was about to do so. He enthusiastically shook the surgeon’s hands and said, “Merci.” Although the first words were difficult to say, gradually his speech flowed freely, and he felt a genuine happiness at having regained the ability to talk.
This man was neuropathic, having always been a rather strange, irritable and restless person, and given to nervous crises in anger, in which he lost consciousness entirely.
This man had nerve issues, always being a bit strange, irritable, and restless, and prone to episodes of anger where he completely lost consciousness.
Re pseudo operations as forms of disguised persuasion, almost countless methods have been used. See Cases 514, 515, 518, 519, especially 521, 560, 561. Sham injections under ethyl chloride have been made (Goldstein). See also under Case 484, re continuous bath, and under Case 488, re lumbar puncture. Very close to these methods are the methods of torpillage of Vincent and the methods employed by Yealland in England and Kaufmann in Germany. See under Cases 574, 563, and 564, and 570.
Re pseudo operations as forms of disguised persuasion, countless methods have been utilized. See Cases 514, 515, 518, 519, especially 521, 560, 561. Fake injections under ethyl chloride have been performed (Goldstein). Also, check under Case 484, re continuous bath, and under Case 488, re lumbar puncture. Very similar to these methods are the techniques of torpillage by Vincent and the approaches used by Yealland in England and Kaufmann in Germany. See under Cases 574, 563, 564, and 570.
Léri quotes Babinski as saying, “We cannot fight hysteria in trench warfare; manoeuvres are necessary.”
Léri quotes Babinski as saying, “We can't tackle hysteria in trench warfare; we need to use maneuvers.”
Re treatment of mutism, Chavigny remarks that the principle of treatment for mutism is quite different from the principles of treatment of paralysis. The reëducation of mutism is psychic. Chavigny claims probably absolute success in the treatment of mutism through faradism to the larynx region simultaneously with a signal given to the patient to make an effort to pronounce the letter A. Garel modifies the treatment (in case the faradic apparatus is not at hand), by a vigorous and sudden blow to the patient’s epigastrium simultaneously with the patient’s endeavor to imitate the movement of the doctor’s lips.
Re treatment of mutism, Chavigny notes that the method for treating mutism is quite different from the methods for treating paralysis. The rehabilitation of mutism is psychological. Chavigny asserts that there is likely a high success rate in treating mutism using faradism directed at the larynx area, while simultaneously instructing the patient to make an effort to pronounce the letter A. Garel modifies the treatment (in case the faradic device is unavailable) by delivering a strong, sudden blow to the patient’s epigastrium while the patient tries to mimic the movement of the doctor’s lips.
Shell-shock: Impairment of vision (even commanded men to fire on kindred troops!) Improvement by verbal suggestion, faradization, injections.
Shell-shock: Vision impairment (even ordered troops to fire on each other!) Improvement through verbal suggestion, faradization, injections.
Case 517. (Mills, October, 1915.)
A sergeant-major, 29, in private life a bookkeeper, said that shrapnel struck the ground in front of him and burst as it struck. Unconscious for a moment, the sergeant-major thereafter saw everything imperfectly, led his men in the wrong direction, and even commanded them to fire in the direction of his own troops.
A 29-year-old sergeant major, who was a bookkeeper before the war, said that shrapnel hit the ground in front of him and exploded on impact. He was briefly knocked out, and after that, he saw everything hazily, led his men the wrong way, and even ordered them to fire toward his own soldiers.
Seven days afterwards the eyes looked normal, fundi were normal, vision was reduced to the perception of hand movements; with a plus 10 sphere the right eye could count fingers at 5 c.m. and with a plus 8 sphere the left eye could count fingers at 3 c.m. There was a right frontal analgesia.
Seven days later, the eyes looked normal, the fundi were normal, and vision had decreased to just being able to see hand movements; with a +10 sphere, the right eye could count fingers at 5 cm, and with a +8 sphere, the left eye could count fingers at 3 cm. There was a lack of sensation in the right frontal area.
Treatment: Sweating; rest in bed for several weeks; assurance of complete recovery. There was a slow but constant improvement, aided by faradization and injections of strychnine sulphate into the temporal region, but the prospect of a return to the front retarded the improvement.
Treatment: Sweating; resting in bed for several weeks; reassurance of complete recovery. There was a gradual but steady improvement, supported by faradization and injections of strychnine sulfate into the temple area, but the possibility of returning to the front slowed down the improvement.
Re injections into the temple, see also Case 521 of Bruce. Re cure of blindness, Grasset has a case of a blind deafmute who was cured by a nurse. She put a pencil in his hand and guided the pencil while she wrote a question. The patient replied in very good MSS. In blind deafmutes sight is described as returning first, hearing next, and speech last.
Regarding injections into the temple, see also Case 521 of Bruce. Regarding the cure of blindness, Grasset has a case of a blind deafmute who was treated by a nurse. She placed a pencil in his hand and guided it while she wrote a question. The patient responded in very good handwriting. In cases of blind deafmutes, sight is noted to return first, followed by hearing, and then speech.
For other cases of blindness, see especially under Section C, Cases 433 to 438, with discussions thereunder.
For other cases of blindness, see especially under Section C, Cases 433 to 438, with discussions below.
Re retardation of improvement by the prospect of further military service, Lewandowski has insisted upon the strong factor of the wish in all such functional conditions. Lewandowski wants all functional cases, however, to be sent to duty in the rear or to be discharged as unfit.
Re delay in progress due to the possibility of more military service, Lewandowski has emphasized the significant role of desire in all such functional situations. Lewandowski wants all functional cases, however, to be assigned to rear duty or discharged as unfit.
Aphonia: manipulation in larynx.
Aphonia: larynx manipulation.
Case 518. (O'Malley, May, 1916.)
A corporal, 28, had a bullet pass through his neck from a point in the middle line at the upper border of the thyroid cartilage to a point behind the right sternomastoid muscle, two inches below the point of entry. The corporal lost his voice at the time of injury, spat up a teaspoonful of blood, and thereafter was able to whisper only. The laryngoscopic examination betrayed no intralaryngeal lesion. Treatment as described below enabled the patient to speak. O’Malley describes his technique as follows:
A 28-year-old corporal had a bullet pass through his neck, starting from the center at the top edge of the thyroid cartilage and ending two inches below that point behind the right sternomastoid muscle. He lost his voice immediately after the injury, coughed up a teaspoon of blood, and could only whisper afterward. A laryngoscopy showed no problems inside the larynx. The treatment outlined below helped the patient regain his ability to speak. O’Malley describes his technique like this:
The patient is placed in the common position for the examination of the larynx, the tip of the tongue being seized in a piece of linen by the left hand fingers and the laryngeal mirror introduced with the right hand. The patient is then requested to say “e” or cough, and if the cords do not approximate, they can be made to do so by using moderate friction on the fauces and pharynx with the mirror to excite secretion. The latter begins to drop into the larynx, and acting as a foreign body, a protective reflex is at once excited which adducts the cords to prevent the secretion from entering the trachea. At the same time an involuntary cough is produced to expel the mucus, and if the friction and flow of secretion are maintained and the patient is urged to cough vigorously, voluntary coughing and a tendency to retching with forced laryngeal notes will rapidly follow. It is usually best to persist until retching occurs, as the cords are then forced together to protect the larynx and trachea from the possible entrance of regurgitated stomach contents. Involuntary laryngeal sounds are thus produced and the patient is conscious of laryngeal effort. Some of these cases are at the moment very shallow breathers, which can be demonstrated by X-ray screening, but the act of retching causes a wide excursion of the diaphragm with a more pronounced expiratory blast, to be rapidly followed by deeper inspirations. This method of treatment is best carried out just before a meal, as the stomach is then practically empty and the unpleasant effects of the sudden regurgitation of food are avoided. When the[726] explosive sounds accompanying retching have occurred two or three times the mirror is withdrawn, the tongue released, and the patient is requested to swallow, take a deep breath, and cough, and then urged to count up to ten, directing his voice to a certain point on the ceiling. This method has given me uniformly good results, and was rapidly effective in all cases coming under treatment soon after the onset of the neurosis.
The patient is positioned in the standard way for examining the larynx, with the tip of the tongue held by the left hand using a piece of cloth, while the laryngeal mirror is inserted with the right hand. The patient is then asked to say “e” or to cough. If the vocal cords don’t come together, they can be encouraged to do so by gently rubbing the back of the throat and pharynx with the mirror to stimulate secretion. This secretion starts to trickle into the larynx, and acting like a foreign object, it triggers a protective reflex that brings the cords together to stop the secretion from entering the trachea. At the same time, an involuntary cough is triggered to expel the mucus. If the rubbing and secretion continue, and the patient is encouraged to cough forcefully, voluntary coughing and a feeling of nausea with involuntary laryngeal sounds will quickly follow. It’s usually best to continue until the patient feels nauseous, as this forces the cords together to protect the larynx and trachea from any potential regurgitated stomach contents. Involuntary sounds from the larynx are produced, and the patient is aware of the effort in the larynx. Some of these patients are currently shallow breathers, as shown by X-ray screening, but the act of retching causes the diaphragm to move widely with a strong exhalation, quickly followed by deeper breaths. This treatment method works best just before a meal, as the stomach is likely empty, avoiding the unpleasant effects of sudden food regurgitation. When the[726] explosive sounds from the retching have happened two or three times, the mirror is taken out, the tongue is released, and the patient is asked to swallow, take a deep breath, cough, and then count to ten, directing their voice at a specific spot on the ceiling. This method has consistently provided good results and has been quickly effective in all cases treated soon after the onset of the condition.
Re methods for curing aphonia, Muck has a method called the “ball” method. A ball is put into the larynx to cause a temporary suffocation, which produces a reflex that starts the adductors. He would apply the method as soon as the man was well over the shock that produced aphonia. Muck states that he has applied the ball method, not only to cases of aphonia, but to cases of mutism and deafness, with success.
Re methods for treating aphonia, Muck has a technique called the “ball” method. A ball is placed in the larynx to induce temporary suffocation, triggering a reflex that activates the adductors. He would use this method as soon as the individual had recovered from the shock that caused the aphonia. Muck claims that he has used the ball method not only for aphonia but also for cases of mutism and deafness, with positive results.
Tilly mentions a case in which the patient refused to open his mouth, so the device was adopted of passing an electrode through the left nostril so that it finally reached the larynx. A spasm was produced, which was carried to the point of considerable cyanosis, but the aphonia was relieved and for the first time in three months the man spoke. Incidentally he began to hear also.
Tilly talks about a situation where a patient wouldn’t open his mouth, so they decided to insert an electrode through his left nostril until it reached the larynx. This caused a spasm that led to significant cyanosis, but it relieved his aphonia, and for the first time in three months, the man spoke. Interestingly, he also started to hear again.
Re treatment of aphonia, Schultz has used the electric current externally over the larynx, all the while carrying on a laryngoscopy. Schultz remarks upon the fatigue that may come during the first few sittings. Roussy and Lhermitte remark that, although aphonia sometimes exists from the outset of shock, it is often a phase in recovery from mutism.
Re treatment of aphonia, Schultz has applied electric current externally to the larynx while conducting a laryngoscopy. Schultz notes that fatigue may occur during the first few sessions. Roussy and Lhermitte point out that although aphonia can sometimes be present from the beginning of the shock, it is often a stage in the recovery from mutism.
Liébault notes that, not only cases of true nervous aphonia but cases of laryngitis, apparently of infectious origin, and cases of true voice strain, may also turn up for treatment. Some men have been improperly discharged from the army for aphonia actually due to voice strain.
Liébault points out that not only true cases of nervous aphonia but also cases of laryngitis, seemingly caused by an infection, and cases of actual voice strain can also appear for treatment. Some men have been wrongly discharged from the army for aphonia that is actually due to voice strain.
Hysterical aphonia in a mechanician (war time contributory?). Cure by suggestive manipulation of larynx.
Hysterical aphonia in a mechanic (could it be related to wartime experience?). Treated with suggestive manipulation of the larynx.
Case 519. (Vlasto, January, 1917.)
A mechanician was refitting an engine valve, when steam was suddenly put on and the drains were opened out. Some of the steam entered the throat of the mechanician, who rushed up, gasping, unable to speak. Oedema of the larynx was thought of; but there was no complaint except the inability to speak.
A mechanic was adjusting an engine valve when steam was suddenly applied and the drains were opened. Some of the steam got into the mechanic's throat, causing him to rush up, gasping and unable to speak. They suspected laryngeal edema, but the only issue reported was the inability to speak.
A month later he was discharged to the hospital ship at Plassy, where he got faradic treatment, the effect of which was to cause him pain without recovery of voice. The man could whisper well enough and cough fairly loudly. The vocal cords of the larynx appeared normal on laryngoscopic examination, but adduction of the cords was not be properly effected. He was now given rest and constant assurances that he would get well.
A month later, he was sent to the hospital ship at Plassy, where he received faradic treatment, which caused him pain without restoring his voice. He could whisper just fine and cough relatively loudly. The vocal cords in his larynx looked normal during the laryngoscopy, but the cords weren’t coming together properly. He was now given rest and constant reassurance that he would recover.
Ten days later, another laryngoscopic examination was made, with mild mechanical stimulation of the air passage. The patient remarked that he had never been so near being able to speak since his dumbness came on. The patient was now informed that his muscle of talking was going to be replaced and that the success of the operation depended upon his help, so that he was to shout out as soon as he became conscious of the physician’s working inside his throat. The patient was given ether lightly, into the second stage. When consciousness was about to return, the laryngeal mirror was placed lightly on the larynx. The patient was commanded and encouraged to count out loud and shout. Speech returned permanently.
Ten days later, another exam using the laryngoscope was done, along with some mild mechanical stimulation of the airway. The patient noted that he had never been this close to being able to speak since he lost his voice. He was now informed that his speech muscle would be replaced and that the success of the surgery relied on his cooperation, so he needed to shout as soon as he felt the doctor working inside his throat. The patient was lightly put under ether, reaching the second stage of anesthesia. As consciousness was about to return, the laryngeal mirror was gently placed on the larynx. The patient was instructed and encouraged to count out loud and shout. His ability to speak returned permanently.
It is to be noted that there was no specific war effect underlying the phenomena, unless we regard the fact of its being war time as contributory to the shock produced by an incident in every day engine room duties.
It should be noted that there was no specific war effect underlying the phenomena, unless we consider the fact that it was wartime as contributing to the shock caused by an incident during everyday engine room duties.
Gradual onset of mutism and amnesia without special occasion. Faradism. Dream.
Gradual onset of mutism and amnesia without any special event. Faradism. Dream.
Case 520. (Smyly, April, 1917.)
A soldier was slightly wounded in the arm and returned to the trenches. Later he found himself in hospital at Boulogne, unable to speak and unable to remember what had happened to him from the time he was in the trenches. It appears that his voice and memory had gradually disappeared, according to what was told him by his comrades.
A soldier was lightly injured in the arm and went back to the trenches. Later, he found himself in a hospital in Boulogne, unable to speak and unable to remember what had happened to him since he was in the trenches. It seems that his voice and memory had slowly faded away, as his comrades told him.
A month afterward, in a London hospital, the patient was roused suddenly from sleep, and then proved able to speak, although there was great difficulty in getting each word out. Two months later, he went to bed, feeling indisposed, in the night had a kind of fit, and remained unconscious until the following night; the next morning, his voice was again lost. The aphonia persisted for a fortnight, and the patient could hear only loud shouting when close to his ear. He was anxious to get well and requested electricity from the physician, Dr. Smyly, having heard probably of another case cured thereby. Dr. Smyly applied faradic current to the larynx externally, instructing the patient to blow at the same time. At first the patient spoke so low that he could not hear himself speak, but on suggestion succeeded in speaking up loudly enough. He was shortly able to speak and hearing improved. The climax arrived with a bad dream one night, from which the patient awoke in a fright and found himself able to hear and speak perfectly.
A month later, in a London hospital, the patient was suddenly woken from sleep and was able to speak, although it was very hard to get each word out. Two months later, he went to bed feeling unwell, had some kind of seizure during the night, and remained unconscious until the next night; when he woke up, he had lost his voice again. The loss of voice lasted for two weeks, and he could only hear loud shouting when someone was close to his ear. He was eager to get better and asked Dr. Smyly, the physician, for electricity treatment, likely having heard about another case that was cured this way. Dr. Smyly used a faradic current on the larynx from the outside, instructing the patient to blow at the same time. At first, the patient spoke so quietly that he couldn’t hear himself, but with encouragement, he succeeded in speaking loudly enough. Soon he was able to speak, and his hearing improved. The turning point came one night after a bad dream, from which he awoke in a panic and found that he could hear and speak perfectly.
Re nocturnal spontaneous cures, see observations by Mott under Case 473. Note also in this case the presence of what Mott has termed “the atmosphere of cure.”
Re spontaneous nighttime remedies, check Mott's observations under Case 473. Also, note the presence of what Mott refers to as “the atmosphere of cure.”
Re relapses, see Case 476 as well as remarks under Case 474. Re special cases of mutism, Goldstein has insisted upon a greater individualization of treatment for functional mutes than even for other neurotics, and advocates the establishment of schools within the hospitals and aftercare institutions. He thinks the problem very serious.
Re relapses, see Case 476 as well as remarks under Case 474. Re special cases of mutism, Goldstein has emphasized the need for a more personalized approach to treatment for functional mutes than for other neurotics, and supports the creation of schools within hospitals and aftercare facilities. He believes the issue is quite serious.
Shell-shock blindness: Cure by a course of injections in the temple.
Shell-shock blindness: Treated with a series of injections in the temple.
Case 521. (Bruce, May, 1916.)
A soldier from Gallipoli was admitted to the Royal Victoria Hospital at Edinburgh, blind. He had been at Gallipoli from May 1, 1915, until August 12, when a shell explosion blew in his trench and buried him. He was dug out nervous and tremulous. Shortly afterwards there was the bright flash of a second shell, and amnesia set in until he found himself in hospital. He could not see at all with the left eye and the sight of the other was poor. He arrived in Scotland, October 9. He was nervous, excitable and now somewhat depressed, complaining of blindness and pain in the left eye, and headache. The left eyelid drooped. The fundus was normal. He had not been given an anesthetic.
A soldier from Gallipoli was admitted to the Royal Victoria Hospital in Edinburgh, blind. He had been at Gallipoli from May 1, 1915, until August 12, when a shell explosion hit his trench and buried him. He was dug out feeling anxious and shaky. Shortly after that, there was a bright flash from a second shell, and he experienced memory loss until he found himself in the hospital. He couldn't see at all from his left eye, and the vision in the right eye was poor. He arrived in Scotland on October 9. He was anxious, easily agitated, and somewhat depressed, complaining of blindness and pain in his left eye, along with a headache. The left eyelid was drooping. The retina appeared normal. He had not been given any anesthetic.
It was explained to him that the eye had not been injured; that it had become weak from the explosion; that he would be given a series of injections into the left temple of a strong drug which would restore the sight of the eye.
He was told that the eye wasn't damaged; it had become weak from the explosion. They mentioned that he would receive a series of injections in the left temple of a powerful drug that would restore his eyesight.
Gradually increasing quantities of normal saline solution were given every morning. After four days he said that the treatment was doing him good. A week later he said that the eye was much stronger. After the fifteenth injection he could not sleep. The headache was worse, and there was “moving about inside his head.” Early in the morning he went to sleep after a period of restlessness. He awoke at eight o’clock able to see perfectly, and was overjoyed at the result. There was some blurring and four days later he said he was becoming blind again. More normal saline was injected, causing pain. After that there was no relapse, and the man was sent back to his unit.
Gradually increasing amounts of normal saline solution were given every morning. After four days, he said that the treatment was helping him. A week later, he mentioned that his eye felt much stronger. After the fifteenth injection, he couldn't sleep. His headache was worse, and he felt like there was “moving around inside his head.” Early in the morning, he finally fell asleep after a restless night. He woke up at eight o’clock able to see perfectly and was thrilled with the result. There was some blurring, and four days later he said he was starting to go blind again. More normal saline was injected, which caused pain. After that, there was no further decline, and the man was sent back to his unit.
Re Shell-shock blindness, Ormond and Hurst recommend a light hypnosis; taking the functionally blind man into a dark room and requesting him to make his mind a blank. Some cases are refractory. An anesthetic may be used with suggestion in the semi-conscious stage.
Re Shell-shock blindness, Ormond and Hurst recommend a light form of hypnosis; taking the functionally blind person into a dark room and asking them to clear their mind. Some cases are stubborn. An anesthetic may be used along with suggestions during the semi-conscious stage.
Deafness, cured by suggestion in writing.
Deafness, treated with written prompts.
Case 522. (Buscaino and Coppola, 1916.)
L. G., 20 years old; fusileer. (Mother of neuropathic constitution. Father died in 50th year of heart disease. One brother had hemiparesis from infantile cerebropathia.) The patient suffered from infantile otitis media bilateralis, which was followed by abundant chronic otorrhea from his fifteenth year. He relates that for a long time he was obliged to wear a very large handkerchief on his shoulders to receive the pus, which came from an ear. No sex disease. Nothing of importance in the physical anamnesis.
L. G., 20 years old; fusilier. (Mother had a neuropathic condition. Father died at 50 from heart disease. One brother had hemiparesis due to infantile cerebral pathology.) The patient experienced bilateral childhood otitis media, which led to significant chronic ear discharge starting at age fifteen. He reports that for a long time, he had to wear a large handkerchief on his shoulders to catch the pus that drained from an ear. No sexually transmitted diseases. No significant findings in the physical history.
Patient entered the army, Jan. 15, 1915. In May, he was sent to the front (Basso Isonzo). Towards the end of July, while he was in the trench, a grenade exploded a short distance from him, causing slight abrasions at the nape of the neck and in the fleshy part of the left calf. He was picked up in an unconscious state, and taken to the hospital at Cervignano, where he was admitted as a deafmute and was given electric treatments. After 18 days or so, first stammering and then pronouncing with difficulty a few words, he finally regained his speech entirely. Deafness continued, however.
Patient joined the army on January 15, 1915. In May, he was sent to the front lines (Basso Isonzo). Towards the end of July, while he was in the trench, a grenade exploded nearby, causing minor abrasions on the back of his neck and in the fleshy part of his left calf. He was found unconscious and taken to the hospital in Cervignano, where he was admitted as a deaf-mute and given electric treatments. After about 18 days, he began to stammer and then was able to pronounce a few words with difficulty, eventually regaining his speech completely. However, he continued to experience deafness.
Being transported to a special hospital in Florence, he was in a state of psychic excitement for several days, showing also visual hallucinations—saw “many soldiers,” saw “many soldiers all about him.” He was treated with chloral and bromide. The suspicions of several physicians were aroused by the obstinate declaration by the patient that he was incurably deaf.
Being taken to a special hospital in Florence, he experienced intense emotional agitation for several days, also showing visual hallucinations—he saw “many soldiers” and “many soldiers all around him.” He was treated with chloral and bromide. The persistent claim by the patient that he was incurably deaf raised suspicions among several physicians.
On being admitted to the clinic on August 22, he showed complete deafness in addition to a slight degree of stupor; he remained impassive to the glance of his questioner without showing signs of worry about his condition, nor did he make any effort to make himself understood by making lip-movements (which is in contrast to another patient affected by organic deafness, who on the contrary made great efforts to[731] understand anything said to him, clearly showing his great grief over his incapacity).
On being admitted to the clinic on August 22, he was completely deaf and also slightly stuporous; he remained expressionless in response to his questioner’s gaze, showing no signs of concern about his condition, nor did he try to communicate through lip movements (unlike another patient with organic deafness, who made considerable efforts to understand anything said to him, clearly showing his deep distress over his inability).
He failed to respond to auditory stimuli either by air or by bone conduction. It was possible from the beginning to exclude suspicion of simulation; during the day, indeed, it was not possible by any of the repeated attempts to awaken surprise in the patient by means of an acoustic stimulus. At night, while the patient slept, it was possible, however, to awaken him by calling his name, or by making a fairly loud sound; the patient would then open his eyes but was quite unable to hear. Neither confusion nor hallucinations were in evidence.
He didn't respond to sounds through the air or through bone conduction. From the start, there was no reason to think he was pretending; during the day, all attempts to surprise him with a sound failed. At night, while he was sleeping, we could wake him by calling his name or making a loud noise; he would open his eyes but couldn't hear anything. There were no signs of confusion or hallucinations.
He was able to converse very well and spontaneously (he remembers having lost consciousness at the explosion of the grenade and not coming to until after his arrival at the hospital at Cervignano); he read correctly both mentally and aloud, and answered by signs the questions put to him in writing. Being face to face with hysterical traumatic deafness, notwithstanding no other hysterical phenomena were noticed, a successful attempt was made with suggestive therapy, the patient being emphatically assured (always in writing) that the following Sunday his hearing would be restored without doubt. The following Sunday, in fact, during the visit of a lady (one of his friends), hearing in his left ear was suddenly and almost completely restored to the patient. He was in profound emotion on account of this, and upon the appearance of the physician he had a hard weeping spell. During the following day, he began slowly to hear with the right ear.
He was able to talk quite well and freely (he remembers losing consciousness during the explosion of the grenade and not waking up until he got to the hospital in Cervignano); he read accurately both mentally and out loud, and responded with gestures to the written questions he was asked. Faced with hysterical traumatic deafness, and despite not showing any other hysterical symptoms, a successful attempt was made with suggestive therapy, where the patient was strongly assured (always in writing) that his hearing would definitely be restored by the following Sunday. Indeed, that Sunday, during a visit from a lady (one of his friends), his hearing in the left ear suddenly and almost fully returned. He was deeply emotional about this and broke down in tears when the physician arrived. The next day, he started to slowly regain hearing in his right ear.
During the latter part of his stay at the clinic, however (until September 24, 1915), a slight hypo-acusia in the right ear persisted, along with severe headaches and pains in the left ear (which the patient compared to the suffering as a child with otitis).
During the later part of his time at the clinic, however (until September 24, 1915), a slight hearing loss in the right ear continued, along with severe headaches and pain in the left ear (which the patient compared to the pain he felt as a child with an ear infection).
At the otoscopic examination by a specialist, only residuals of the old catarrhal otitis with retraction of the tympanic membrane were found.
At the ear exam by a specialist, only traces of the old cold-related ear infection with a retraction of the eardrum were found.
Shell-shock story reproduced in hypnosis. Recovery.
Shell-shock story shared through hypnosis. Recovery.
Case 523. (Myers, January, 1916.)
A private had been found wandering in a village, in shirt and socks, unable to give name, regiment, or number. He was admitted at a field ambulance, and seen by Major Myers three days later. No Christian name seemed familiar to him. The past was a blank. He was depressed. There was numbness over the occiput. The legs, hands and tongue were tremulous. The left arm and leg and the left side of the face, chest and abdomen were hypalgesic. The knee-jerks were exaggerated; pseudo-clonus of left knee and right ankle. There had been a nightmare of bombs thrown into trenches—one thrown by a German hit him in the neck and woke him up in a cold sweat.
A private had been found wandering in a village, in just his shirt and socks, unable to remember his name, regiment, or number. He was taken to a field ambulance and seen by Major Myers three days later. No first name seemed familiar to him. The past was a blank. He felt depressed. There was numbness at the back of his head. His legs, hands, and tongue were shaky. The left arm and leg, as well as the left side of his face, chest, and abdomen, had reduced sensitivity. The knee reflexes were exaggerated; there was pseudo-clonus in his left knee and right ankle. He had a nightmare about bombs being dropped into trenches—one thrown by a German hit him in the neck and woke him up in a cold sweat.
In hypnosis the dream was repeated, and points about his previous life were dragged out piecemeal. Next, the names of village and near-by town, and finally his own name, regiment and number were elicited. After the bomb-throwing, he said, “I must have gone off my head and run away. I must have taken off my clothes in a field. I spent the first night under a hedge. I spent the next two nights in a wood. I ate nothing. The next night I was walking along a road on the outskirts of a village and I was taken to a house by two men.” On waking, he proved unable to remember these things and was promptly rehypnotized, whereupon the memories became clearer and more ample. More powerful suggestion was given, and complete recovery of memory followed the second period of hypnotism. The pupils became larger. The despondency disappeared, together with the occipital numbness and the left-sided hypalgesia. He was transferred to a base hospital, and thence after three weeks to a hospital in England, made an uninterrupted recovery, and rejoined his regiment.
In hypnosis, the dream was repeated, and details about his past life were slowly pulled out. Then, they uncovered the names of his village and a nearby town, and finally, his own name, regiment, and number. After the bomb-throwing incident, he said, “I must have lost my mind and run away. I must have taken off my clothes in a field. I spent the first night under a hedge. I spent the next two nights in a forest. I didn’t eat anything. The next night, I was walking along a road on the edge of a village, and two men took me to a house.” When he woke up, he couldn’t remember these things and was quickly put back under hypnosis, where the memories became clearer and more detailed. Stronger suggestions were given, and after the second hypnosis session, he completely recovered his memories. His pupils got larger. The sadness went away, along with the numbness in the back of his head and the reduced sensitivity on his left side. He was moved to a base hospital, and then after three weeks, to a hospital in England, where he made a full recovery and rejoined his regiment.
Shell-shock story reproduced in hypnosis. Recovery.
Shell-shock story recreated in hypnosis. Recovery.
Case 524. (Myers, January, 1916.)
Private, 29, seen by Major Myers in a base hospital the day after entrance, was in a stupor from which he had to be repeatedly roused to answer questions. He could recall neither name, regiment nor age, and was unable to write or read except a few letters in very large type. Twice he said the words war and comrade, and made a gesture as if following. He agreed that a shell came and intimated that he had pains in the forehead. He could not hold his hands out for many seconds without dropping them. Knee-jerks brisk.
Private, 29, was seen by Major Myers in a base hospital the day after he arrived. He was in a daze and had to be repeatedly shaken awake to answer questions. He couldn't remember his name, regiment, or age, and could only read or write a few letters in very large print. Twice, he mentioned the words war and comrade, and gestured as if he were following something. He acknowledged that a shell had exploded and hinted that he had pain in his forehead. He couldn't hold his hands out for more than a few seconds without dropping them. His knee-jerks were brisk.
Four days later he was very little better, never having spoken voluntarily, but replying yes to the utterance of his name, and was able with great effort to write his name. He still intimated his severe headache. The next day the names of his two children were given. He could not read aloud the figure 2 but held up two fingers. Next day, he gave syllable by syllable his wife’s name from her photograph.
Four days later, he was still not much better. He hadn’t spoken on his own but responded with yes when his name was called, and with a lot of effort, he managed to write his name. He still mentioned that he had a bad headache. The following day, they told him the names of his two kids. He couldn't read the number 2 out loud but held up two fingers instead. The next day, he spelled out his wife’s name, one syllable at a time, from her photograph.
A week from admission he was hypnotized and persuaded to talk about the events that preceded his disorder, breathing excitedly, gesturing, and evidently visualizing the scenes. He had been in the trenches, had been sent to draw water at a camp, and had been knocked down when two or three shells burst over him. He carried out post-hypnotic suggestions.
A week after he was admitted, he was hypnotized and encouraged to discuss the events leading up to his disorder. He breathed quickly, gestured, and clearly visualized the scenes. He had been in the trenches, was sent to get water at a camp, and was knocked down when two or three shells exploded near him. He followed post-hypnotic suggestions.
He was hypnotized again, two days later, and now described how, after shelling, he had lain on the ground, dazed; had risen, picked up the water bottle, returned to the trenches, and then lost all sense and reason. He recalled how his mates had told him he was silly, but had lost all intervening memories. But the full details were elicited by persuasion. Next day he complained that he still wrote with difficulty. Under hypnosis, his speech and writing were restored to normal. He was discharged two days later to an English hospital.
He was hypnotized again two days later and now explained how, after the shelling, he had lain on the ground, feeling dazed; got up, grabbed the water bottle, returned to the trenches, and then completely lost his mind. He remembered his friends telling him he was being foolish, but he couldn't recall any of the memories in between. However, with some coaxing, the full details came out. The next day, he noted that he still had trouble writing. Under hypnosis, his speech and writing returned to normal. He was discharged two days later to an English hospital.
He was then passed for foreign service, being prevented from active service in the field by occasional severe headaches.
He was then cleared for foreign service, but he was kept from active duty in the field by occasional severe headaches.
Burial after explosion of a “coal box”: Automatism, amnesia, deafmutism: Recovery by hypnosis.
Burial after the explosion of a “coal box”: Automatism, amnesia, deaf-muteness: Recovery through hypnosis.
Case 525. (Myers, September, 1916.)
A sergeant, 18, with nineteen months service in the army, 11 months in France, was seen by Lt. Col. Myers at a clearing station to which he had been transferred after three days in another clearing station, with a note “Found in the streets of B——, asking his way to the fire trench; could not be got to speak on admission nor since; seems deaf, but now writes rationally.”
A sergeant, 18, with nineteen months of service in the army and 11 months in France, was seen by Lt. Col. Myers at a clearing station to which he had been transferred after three days in another clearing station, with a note that said, “Found in the streets of B——, asking for directions to the fire trench; could not be made to speak upon admission nor since; seems deaf, but now writes clearly.”
Mute and very deaf at the second C. C. S., he regained a good deal of his hearing with encouraging talk and also became able to cough and utter P, B, F and S, finally whispering name, regimental number, and the like. At the same time he could write fluently. After being buried he had lost himself until he had asked his way of a military policeman at the crossroads in B——. There was amnesia again until he had been 48 hours in the clearing station at B——. The throat hurt as if it were pulled down when he tried to speak, and his head ached when he tried to remember. There was much tremor, especially of right arm. In a quiet room adjoining, the tremors increased and there was much agitation. Lt. Col. Myers suggested cure and encouraged the man, finally inducing a mild hypnotic state in which he spoke aloud, at first hesitatingly, later fluently.
Mute and mostly deaf at the second C.C.S., he regained a lot of his hearing through positive conversation and was also able to cough and make sounds like P, B, F, and S, eventually whispering his name, regimental number, and similar details. At the same time, he could write fluently. After being buried, he had lost track of himself until he asked a military policeman for directions at the crossroads in B——. Then he experienced amnesia again until he spent 48 hours at the clearing station in B——. His throat felt like it was being pulled down when he tried to speak, and his head throbbed when he attempted to remember. There was a lot of shaking, especially in his right arm. In a quiet room next door, the shaking worsened, and he became very agitated. Lt. Col. Myers proposed a treatment and encouraged the man, eventually putting him in a mild hypnotic state where he began to speak out loud, initially hesitantly, then more fluently.
The man eventually remembered what had happened after he had extricated himself. He had run, as he thought, towards the fire trench, taken a wrong direction, and met a Frenchman who gave him eggs and bread, allowed him to sleep on a couch, put him on a cart and drove him to B——. He was then very giddy and asked his way of the policeman. The shell by which he was “terribly shaken” was a “coal box.” Posthypnotic suggestion that the headache would not recur and that he would shake hands with the orderly was successful. He now talked in a proper voice, at first hesitatingly. He looked another man as his clay-colored face resumed a[735] normal aspect. After a good night’s sleep he was evacuated to a base hospital, thence to an English hospital, whence he wrote six days later in gratitude for the successful treatment, stating that he was now nearly well and hoped to be fit for light duty.
The man eventually recalled what had happened after he managed to free himself. He had run, as he thought, toward the fire trench, taken a wrong turn, and met a Frenchman who gave him eggs and bread, let him sleep on a couch, put him on a cart, and drove him to B——. He was feeling very dizzy and asked a policeman for directions. The shell that had "terribly shaken" him was a "coal box." The posthypnotic suggestion that the headache wouldn’t come back and that he would shake hands with the orderly worked. He was now speaking properly, at first a bit hesitantly. He looked like a different man as his pale face returned to a[735] normal appearance. After a good night’s sleep, he was evacuated to a base hospital, then to an English hospital, from where he wrote six days later to express his gratitude for the effective treatment, saying that he was now almost well and hoped to be ready for light duty.
Six weeks later he wrote that he was still dizzy. He also remembered certain further details of his experience; how he had wandered into a listening sap in front of the Huns’ barbed wire and had had a tussle with three Huns, after which he was buried during the heavy shelling.
Six weeks later, he wrote that he was still feeling dizzy. He also recalled some more details of his experience; how he had stumbled into a listening sap in front of the Huns' barbed wire and had a scuffle with three Huns, after which he was buried during the intense shelling.
This case belongs in the group termed by Myers “A Group,” namely, the physical group, in which the patient has been lifted, buried or knocked over by a shell or otherwise felt physical or chemical effects of an explosion (in contrast with the B Group, or psychical group, in which fear of the noise or emotional response to the mutilation of companions is the exciting cause). Predisposing affections occur as often in the physical group as in the psychical group. The average age of mutism cases seen by Lt. Col. Myers is twenty-five. Mutism is rare among commissioned officers. Lt. Col. Myers has heard of but one or two cases.
This situation fits into what Myers calls “A Group,” which refers to the physical group where the patient has been physically impacted, like being lifted, buried, or knocked down by a shell, or has experienced physical or chemical effects from an explosion. This is in contrast to the B Group, or psychical group, where fear of the noise or emotional reactions to seeing friends injured are the main triggers. Pre-existing conditions are seen as frequently in the physical group as in the psychical group. The typical age of mutism cases observed by Lt. Col. Myers is twenty-five. Mutism is uncommon among commissioned officers, with Lt. Col. Myers only knowing of one or two cases.
With respect to the technique of getting these men to utter sounds, Lt. Col. Myers states that he first assures the patient that he has already cured many cases of loss of speech by the method about to be employed. The patient is next asked to copy his teacher as the sounds (not the vowels) B, D, finally V, S and K are made. The patient is, as a rule, shortly induced to make the necessary movements of lips, tongue or throat. “You see you are beginning to talk. Now let me hear you cough.” The patient coughs. “You see you are able to make a noise. I want you next to cough out an A (Continental pronunciation).” After a time the patient adds this vowel to the cough. Other vowels are now taught him. Eventually a consonant is prefixed to the vowel instead of the cough. The patient is now delighted with his progress and can shortly repeat surname and regimental number.
Regarding the technique for getting these men to make sounds, Lt. Col. Myers says that he first reassures the patient that he has successfully treated many cases of speech loss using this method. The patient is then asked to imitate the teacher as the sounds (excluding the vowels) B, D, and later V, S, and K are produced. Generally, the patient is quickly encouraged to make the necessary movements of the lips, tongue, or throat. "You see, you're starting to talk. Now let me hear you cough." The patient coughs. "You see, you're capable of making a sound. Next, I want you to cough out an A (with a Continental pronunciation)." After a while, the patient adds this vowel to the cough. Other vowels are then introduced. Eventually, a consonant is added to the vowel instead of the cough. The patient is now thrilled with his progress and can soon repeat his surname and regimental number.
Mutism: Recovery by hypnosis.
Mutism: Healing through hypnosis.
Case 526. (Hurst, 1917.)
A transport driver, 31, was run over by a loaded wagon at Gallipoli in May, 1915, and fractured his pelvis. He remained perfectly conscious but unable to speak for three days. At the beginning of August, when he was admitted to the war hospital, he still spoke with great difficulty and with contortions of his face. Even when he did not speak, he had facial contortions and that mental condition characteristic of tic, namely: although he was able to control the contortions by will, he felt uncomfortable during the control and finally gave way to the irresistible impulse.
A 31-year-old transport driver got run over by a loaded wagon in Gallipoli in May 1915 and broke his pelvis. He stayed fully conscious but couldn’t speak for three days. By early August, when he was admitted to the war hospital, he still struggled to talk and had facial spasms. Even when he wasn’t speaking, his face would contort, showing signs of a tic: while he could control the spasms with effort, he felt uneasy during that control and ultimately succumbed to the overwhelming urge.
Under hypnotism, it was suggested to him that he would be able to speak without difficulty and would no longer have the contractions of the face. When he came out of hypnosis he was able to talk quite normally, sang next evening at a concert, and a few days later he took part in a play. The facial contortions persisted in hypnosis and even afterwards, but vanished after a second hypnosis.
Under hypnosis, it was suggested to him that he would be able to speak easily and wouldn’t have any facial contractions. When he came out of hypnosis, he was able to speak normally, sang at a concert the next evening, and a few days later he performed in a play. The facial twitches continued during hypnosis and even after, but disappeared after a second session of hypnosis.
Re hypnosis as treatment of mutism, Ballard remarks that a genuine return of speech and a merely hypnotic speech must be distinguished.
Re hypnosis as treatment of mutism, Ballard points out that it's important to differentiate between a true return of speech and speech that is just a result of hypnosis.
Nonne is the great exponent of the use of hypnotism in treatment of the war hysterias. He got as good results from high as from lower classes of men. He remarks that the hypnosis does not protect against recurrence if the patient again falls under the original conditions that brought about the first attack. Hypnosis may be used also as a diagnostic measure between functional and organic cases. Even tics and tremors have been at times cured.
Nonne is a leading advocate for using hypnotism to treat war-related hysteria. He achieved similar results with both high and low-class individuals. He notes that hypnosis doesn’t prevent a relapse if the patient is exposed to the same conditions that triggered the initial episode. Hypnosis can also serve as a diagnostic tool to distinguish between functional and organic cases. Even tics and tremors have been cured at times.
Re employment of hypnotism, Hurst suggests that it may well be used, not only in mutism, but in hysterical deafness, blindness, and occasionally in psychasthenia. It is not a cure-all for the war hysterias, but is to be used as a not infrequent form of treatment. Nonne claims cures of 51 out of 63 cases of hysteria major (28 rapidly, 23 more gradually). Ten of his 63 proved refractory to hypnosis altogether.
Re employment of hypnotism, Hurst suggests that it may be used not only for mutism but also for hysterical deafness, blindness, and sometimes in psychasthenia. It's not a universal solution for war-related hysteria, but it should be considered as a relatively common treatment option. Nonne reports cures in 51 out of 63 cases of major hysteria (28 quickly, 23 more gradually). Ten of his 63 cases did not respond to hypnosis at all.
Stammering: Cured by hypnosis.
Stuttering: Cured by hypnosis.
Case 527. (Hurst, 1917.)
An Australian, 22, wrote the following, August 21, 1916:
An Australian, 22, wrote the following on August 21, 1916:
“You may be a little surprised to hear that I am in the Hos. suffering from shell-shock, which has taken away my speech and hearing. It is some sixteen days now since it happened.… We were in the trenches and going for dear life, when two of us spotted a German machine gunner in a hole, so we made up our minds to have him. We made a charge at him, and I just remember getting to him when a high-explosive shell burst at my head; it seemed as if it burst inside my head; everything went black. I tried to call out and couldn’t, and I could not hear my mates—only just a terrible bursting in my head all the time. I never remembered anything more until I came to on the boat. The Drs. have told me that I will get alright in time. I saw a good deal of France.… There is not a young man there who is not in the Army. The girls and women work in the fie——”
"You might be a bit shocked to hear that I'm in the hospital, suffering from shell shock, which has taken away my ability to speak and hear. It's been about sixteen days since it happened... We were in the trenches fighting for our lives when two of us spotted a German machine gunner in a hole, so we decided to take him out. We charged at him, and I just remember reaching him when a high-explosive shell exploded near my head; it felt like it burst inside my head; everything went dark. I tried to shout out but couldn't, and I couldn’t hear my buddies—just a constant deafening burst in my head. I don't remember anything else until I woke up on the boat. The doctors have told me that I’ll be okay in time. I saw quite a bit of France... There isn't a young man there who isn't in the Army. The girls and women work in the fields..."
The abrupt ending of the letter was due to the entrance of Major Hurst. The patient had been hypnotized but his deafness had persisted during the hypnotic sleep, so that suggestions could not be effectively taken. He heard nothing whatever during a very heavy thunderstorm, was unable to make any sign whatever, and could not even cough.
The sudden end of the letter was caused by Major Hurst's arrival. The patient had been hypnotized, but his deafness continued even during hypnosis, making it impossible for him to respond to suggestions. He heard nothing at all during a loud thunderstorm, couldn't signal in any way, and wasn't even able to cough.
He was now told in writing that his speech and hearing would be restored when ether was given. After a few whiffs, he struggled and before he was under began to repeat the word “Mother.” Etherization was discontinued before his limbs had even become relaxed. As he was coming to, he was requested to repeat various words, and when the anesthetic had passed, he was talking normally and had completely recovered hearing.
He was now informed in writing that his speech and hearing would return once he was given ether. After a few breaths, he struggled and started to say the word “Mother” before he was fully out. The ether was stopped before his limbs had even relaxed. As he was coming to, he was asked to repeat different words, and once the anesthetic wore off, he was speaking normally and had completely regained his hearing.
Now, however, his memory had become a complete blank. From a short time before his shell-shock up to the moment of his regaining consciousness after etherization, he remembered nothing of his loss of speech or hearing, nothing about the events in his letter, and nothing about Major Hurst, whom he[738] felt he had not previously seen. According to Hurst, this patient had become (a) speechless from fright at the time of the shell explosion, (b) deaf from the noise of the explosion, and (c) unconscious from the windage. After he came to at the time of the explosion, an autosuggestion to the effect that he had lost his power of speech and hearing occurred. Ether broke down this inhibition of speech and hearing by interfering with the control of the high over lower cerebral centers.
Now, however, his memory was completely blank. From just before his shell shock to the moment he regained consciousness after being given ether, he remembered nothing about losing his ability to speak or hear, nothing about the events in his letter, and nothing about Major Hurst, whom he felt he had never seen before. According to Hurst, this patient had become (a) speechless from fear at the time of the shell explosion, (b) deaf from the noise of the explosion, and (c) unconscious from the blast. After he came to at the time of the explosion, he experienced autosuggestion that he had lost his ability to speak and hear. The ether broke down this inhibition of speech and hearing by interfering with the control of the higher over lower brain centers.
Re emotional stammering, Chavigny treats by voice gymnastics, rhythmical breathing movements, sounds spoken by metronome with simultaneous movements of arms or trunk, and by singing. Re hysterical stuttering, Roussy and Lhermitte remark that the symptoms are always very pronounced, come on suddenly, and cease just as suddenly under the influence of electrical treatment. The history will differentiate hysterical stuttering. The effects of treatment will also help. Genuine non-hysterical stammering may, of course, be increased through emotion or shock. Dundas Grant aids the stutterer by having him twist a button or carry out some other muscular movement simultaneously with the attempt to speak. He also has the patient endeavor to expand the lower part of his chest during the effort.
Regarding emotional stammering, Chavigny addresses it through voice exercises, rhythmic breathing movements, sounds produced in sync with a metronome along with arm or trunk movements, and by singing. As for hysterical stuttering, Roussy and Lhermitte note that the symptoms are always quite severe, arise suddenly, and disappear just as quickly with electrical treatment. The patient's history will help differentiate hysterical stuttering. The outcomes of treatment will also provide insight. True non-hysterical stammering can certainly be worsened by emotions or shock. Dundas Grant assists the person who stutters by having them twist a button or perform another physical action while attempting to talk. He also encourages the patient to try to expand the lower part of their chest during the effort.
MacMahon notes that Shell-shock stammering is chiefly a difficulty with vowel sounds and voiced consonants, and amounts to a speech inhibition, accompanied sometimes by amnesia for words and suggesting a form of aphasia. Mild cases of such stammering are cured simultaneously. MacMahon relies in part upon especially regulated breathing movements and the attendant sense of repose. The cases of old cured stammering that have come back under Shell-shock are harder to treat.
MacMahon points out that shell shock stuttering is mainly a struggle with vowel sounds and voiced consonants. It's a type of speech blockage that can sometimes be linked to a loss of memory for words, resembling a form of aphasia. Mild instances of this stuttering can be treated at the same time. MacMahon also focuses on specially controlled breathing techniques and the calming effect they have. However, cases of previously treated stuttering that have returned due to shell shock are more challenging to address.
Two burials; shell-shock: Mutism and amnesia. Recovery aided by hypnosis.
Two burials; shell shock: mute and forgetful. Recovery helped by hypnosis.
Case 528. (Myers, January, 1916.)
Major C. S. Myers recites hypnotic cure in a case of mutism. He remarks that malingering is sometimes suspected in these cases. There was, however, in this case a severe constipation which lasted five days from the shock, and a retention of urine with catheterization during the same period. This private, 32 years, came to a base hospital, mute but able to read and write as follows:
Major C. S. Myers presents a hypnotic cure in a case of mutism. He notes that faking illness is sometimes suspected in these cases. However, in this situation, there was a severe constipation that lasted five days after the shock, along with urinary retention that required catheterization during the same timeframe. This private, 32 years old, arrived at a base hospital, mute but able to read and write as follows:
“I was buried alive on —— and again on —— [5 months and 4½ months respectively before admission], and then I had the misfortune to have two shells burst over me on —— [four days before admission]. There was shelling for about 20 minutes and then two bursted over my head. I did not remember any more until you came to see me, but I am still living in hopes to regain my speech back.”
“I was buried alive on —— and again on —— [5 months and 4½ months respectively before admission], and then I had the bad luck of having two shells explode above me on —— [four days before admission]. There was shelling for about 20 minutes, and then two burst right over my head. I don’t remember anything else until you came to see me, but I’m still hoping to get my speech back.”
It seems that he had wandered off with a lance-corporal for three days after the first burial, and neither he nor his comrade were able to find their regiment.
It looks like he had drifted away with a lance-corporal for three days after the first burial, and neither he nor his buddy could locate their regiment.
Understanding was slow and look vacant. There were jerky movements of the arms and a snoring sound from the nasopharynx. Voluntary movements were restricted, weak, slowly executed, jerky, and incoördinated, but not tremulous. Station was unsteady; failure in finger-to-nose test. He could imitate the sound ah, and the consonants s and p.
Understanding was limited and the expression was blank. There were shaky arm movements and a snoring sound from the throat. Voluntary movements were restricted, weak, slow, jerky, and uncoordinated, but not shaky. His balance was unsteady; he failed the finger-to-nose test. He could imitate the sound ah and the consonants s and p.
Knee-jerks exaggerated; plantars flexor; abdominal reflexes absent; pupils reacted; eye movements normal; moderate restriction of visual fields on temporal side; watch not heard even in contact with ear; heard better by air than by bone conduction.
Knee-jerk responses were exaggerated; plantar flexor reflex was absent; abdominal reflexes were absent; pupils were reactive; eye movements were normal; moderate restriction of visual fields on the temporal side; watch was not heard even when in contact with the ear; heard better through air conduction than bone conduction.
In the next two days, the patient became brighter and movements became better. On the seventh day stupor and ataxia had disappeared. Familiar names could be repeated and the next day could be given on request. The patient would sweat profusely in giving replies. There was no spontaneous speech. A week later speech had improved.
In the next two days, the patient became more alert and their movements improved. By the seventh day, stupor and unsteady movements had disappeared. They could repeat familiar names and could state the next day when asked. The patient would sweat heavily while answering. There was no spontaneous speech. A week later, speech had gotten better.
Under hypnosis he spoke more fluently though feebly, and became emotional upon being questioned as to trench life, waking up suddenly from hypnosis and wiping the sweat from his chest.
Under hypnosis, he spoke more clearly, though weakly, and got emotional when asked about life in the trenches, suddenly waking up from the hypnosis and wiping the sweat from his chest.
The next day, forgotten events of the second burial were recalled together with what followed. Post-hypnotic suggestion of the performance of eccentric actions was successful.
The next day, the forgotten events of the second burial were remembered along with what happened after. The post-hypnotic suggestion to perform unusual actions worked well.
Next day his memory had returned save in reference to the two days’ wandering after the first burial; and under hypnosis the events of those two days were recalled. He was then transferred to an English hospital.
The next day, his memory came back except for the two days he wandered after the first burial; and under hypnosis, he recalled the events of those two days. He was then moved to an English hospital.
Re hypnosis for “war shock,” Eder remarks that the usual objections to hypnosis cannot apply because the majority of cases have no neuropathic antecedents. Eder, as psychoanalyst, endeavors to level hypnotic suggestion against the so-called “complexes.” Elliot Smith and Pear commend Lt.-Col. Myers’ results, but regard the results of hypnotic treatment as brilliant but erratic. Colin Russel, regarding hypnotism as an induced hysteria, remarks that a true hysteria can hardly be cured by adding more, although he has sometimes used the treatment with apparent success. Podiapolsky notes that some 17 per cent of his functional cases will, at a word, drop off into an artificial deep slumber. He thinks chloroform should not be given to these subjects without an attempt to secure this artificial deep slumber first. Chavigny, highly commending suggestion, notes that the use of hypnotism is prohibited in military hospitals in France. A remark of Smirnow indicates that the Russian authorities also look with disfavor upon hypnosis, but he notes certain patients whom he cured by hypnosis, so that apparently Russia did not absolutely forbid the use of hypnosis in war cases. Another Russian, Arinstein, prefers the Dubois method to hypnosis.
Re hypnosis for “war shock,” Eder notes that the typical objections to hypnosis don't really apply because most cases don't have any neuropathic background. Eder, as a psychoanalyst, tries to use hypnotic suggestion to address the so-called “complexes.” Elliot Smith and Pear acknowledge Lt.-Col. Myers’ results but see the outcomes of hypnotic treatment as impressive yet inconsistent. Colin Russel, viewing hypnotism as a form of induced hysteria, points out that real hysteria can hardly be treated by introducing more, although he has sometimes had success with the method. Podiapolsky observes that about 17 percent of his functional cases will, at a cue, fall into an artificial deep sleep. He believes chloroform shouldn’t be administered to these patients without first trying to induce this artificial deep sleep. Chavigny, who strongly supports suggestion, mentions that the use of hypnotism is banned in military hospitals in France. A statement from Smirnow suggests that the Russian authorities also disapprove of hypnosis, but he points out certain patients he successfully treated with hypnosis, indicating that Russia didn’t completely outlaw its use in war situations. Another Russian, Arinstein, prefers the Dubois method over hypnosis.
Roussy and Lhermitte definitely state that the psychotherapy of Dejerine, Dubois, and Babinski beneficially replaces hypnotic suggestion, “which ought definitely to be rejected.” However, if the conclusions of Bernheim are sound, there can be no theoretical claim of distinction between hypnosis and other forms of suggestion.
Roussy and Lhermitte definitely say that the psychotherapy of Dejerine, Dubois, and Babinski is a better alternative to hypnotic suggestion, “which should definitely be rejected.” However, if Bernheim’s conclusions are valid, there’s no theoretical basis to differentiate between hypnosis and other forms of suggestion.
Fifteen bayonet wounds; recommendation for Victoria Cross: Hysterical contracture of hand, revealed by hypnosis as the bayonet clutch.
Fifteen bayonet wounds; recommended for the Victoria Cross: Hysterical hand contraction, uncovered by hypnosis as the bayonet grip.
Case 529. (Eder, August, 1916.)
A left-handed Irishman, 23, on December 22, 1915, got 15 bayonet wounds, 14 of which were on the right side of the body. He was in the trenches with 23 men, when they were attacked by about 200 Turks. He and a sergeant leaped out of the trench into a bayonet attack with Turks.
A 23-year-old left-handed Irishman received 15 bayonet wounds on December 22, 1915, 14 of which were on the right side of his body. He was in the trenches with 23 other men when they were attacked by around 200 Turks. He and a sergeant jumped out of the trench to face the Turkish bayonet attack.
He was admitted to the hospital January 26, 1916, for a hysterical contracture of the right hand. The fingers were semi-flexed and could not be passively extended. Col. Purves Stewart noted that there was an anesthesia and analgesia to pin-pricks and cotton wool on the whole of the right arm. “At the beginning of the examination, the patient felt pin-pricks at the wrist; as examination continued, the boundary of anesthesia steadily increased until it reached the shoulder, by which time the previously sensitive spots were now anesthetic.” Later there was a complete right hemianesthesia.
He was admitted to the hospital on January 26, 1916, for a hysterical contracture of his right hand. The fingers were semi-flexed and couldn’t be passively straightened. Col. Purves Stewart observed that there was a loss of sensation and pain relief from pin-pricks and cotton wool across the entire right arm. “At the start of the examination, the patient felt pin-pricks at the wrist; as the examination went on, the area of numbness steadily expanded until it reached the shoulder, at which point the previously sensitive areas were now numb.” Later, there was complete numbness on the entire right side.
In telling his story, this soldier repeatedly emphasized that “You must clutch your rifle very firmly and never let it up, guarding yourself all the time.” This was the explanation of the contracture. According to Eder, in the unconscious, he was still clutching the rifle, fighting the good fight, and symbolizing the desire by the grasping hand. In hypnosis, suggestion was made that the fight was over and the rifle could be let go, whereupon the hand was immediately relaxed.
In sharing his story, this soldier repeatedly stressed that “You have to hold your rifle really tightly and never let it go, protecting yourself all the time.” This was the explanation for the contraction. According to Eder, in his unconscious mind, he was still holding onto the rifle, continuing the fight, and representing his desire with his clenched hand. During hypnosis, it was suggested that the fight was over and that he could release the rifle, at which point his hand immediately relaxed.
The analgesia, thinks Eder, was present during the fight and passed away subsequently. In fact, the soldier said that he felt no pain during the fight and did not know that he was wounded until his attention was called to the fact that blood was flowing from him. According to Eder, the unconscious mind refused to feel pain. At Col. Stewart’s first prick or two “the unconscious took no notice, but as the pricks continued, the former memory was revived and the unconscious became on guard.” He had been recommended for the V. C.
The pain relief, Eder thinks, was there during the fight and faded away afterward. In fact, the soldier mentioned that he felt no pain during the battle and didn't realize he was injured until someone pointed out that blood was running from him. According to Eder, the unconscious mind just didn't acknowledge the pain. At Col. Stewart’s first couple of pricks, “the unconscious didn't register it, but as the pricks went on, the earlier memory came back, and the unconscious became alert.” He had been recommended for the V. C.
Gunshot of forearm: Hysterical contracture, wrist and fingers: Cure by hypnosis, “indecently quick.”
Gunshot to the forearm: Hysterical contraction of the wrist and fingers: Treatment through hypnosis, “surprisingly fast.”
Case 530. (Nuns, December, 1915.)
An infantryman, without special hereditary taint and previously well, was shot September, 1914, in the right forearm. A paralysis of the hand and fingers persisted after the wound had healed. Several reserve hospitals failed to cure the paralysis.
An infantryman, without any special hereditary issues and who had previously been well, was shot in the right forearm in September 1914. Paralysis of the hand and fingers continued even after the wound had healed. Several reserve hospitals were unable to cure the paralysis.
Eight months after the injury he arrived at Nonne’s clinic at Eppendorf, with a flexor contracture of the right wrist joint as well as of the fingers (exclusive of thumb). The finger tips were deeply sunk in the flesh of the palm. Extension could only be brought about against strong resistance. There was a total anesthesia for all sensations in the hand and fingers. No contraction of visual fields.
Eight months after the injury, he arrived at Nonne’s clinic at Eppendorf with a flexor contracture of his right wrist and fingers (not including the thumb). The fingertips were deeply embedded in the palm. Extension could only be achieved against significant resistance. There was complete loss of sensation in the hand and fingers. No contraction of visual fields.
The patient, upon suggestion, fell immediately into hypnosis. At first the contracture was released with some difficulty; then, with greater ease, and then without any resistance whatever. During the same hypnotic séance the patient finally became able to extend actively both fingers and wrist; and next day, after the patient had convinced himself of his cure, he was able voluntarily to stretch the hand and fingers with normal amplitude and power. The disturbance of sensibility had spontaneously disappeared.
The patient, following a suggestion, quickly fell into hypnosis. Initially, the muscle tightness was released with some difficulty; then it became easier, and finally, there was no resistance at all. During that same hypnotic session, the patient was able to actively move both the fingers and wrist. The next day, after the patient realized he was cured, he could voluntarily stretch his hand and fingers with normal range and strength. The sensitivity issue had resolved on its own.
This cure was, from the patient’s point of view, indecently quick. He said everybody must feel he was a malingerer, and in fact he felt so himself. He went back into service, where he had been for several months at the date of Nonne’s report.
This treatment was, from the patient’s perspective, unreasonably fast. He thought everyone must see him as a phony, and honestly, he felt that way too. He returned to duty, where he had been for several months by the time Nonne provided his report.
Re Nonne’s enthusiasm for hypnosis, see under Case 526. Nonne, contrary to Babinski and Froment, would regard even the severe and obstinate vasomotor disturbances as purely functional and as not even “sub-organic.” The basis of this belief is that hypnosis cures these phenomena as well as various tics and pertinacious tremors. French observers consider that these tics and tremors may even be organic in their nature, basing their ideas upon the non-success of[743] suggestion. (It may be noted [see under Case 528] that the French military authorities do not allow the use of hypnotism in the army.) With respect to the present case (530), of course, the French observers would not deny the power of hypnotism to produce the cure. Babinski and Froment’s Postscript to the English edition of their work on hysteria, remarks that, though Roussy and Lhermitte state that vasomotor symptoms may disappear along with the psychotherapeutic cure of paralyses and contractures, yet Roussy and Boisseau later admitted that improvement in thermal and vasomotor control is at best an exceedingly slow one.
Re Nonne’s interest in hypnosis can be found under Case 526. Nonne, unlike Babinski and Froment, believes that even severe and stubborn vasomotor issues are purely functional and not even “sub-organic.” He holds this view because hypnosis appears to treat these issues as well as various tics and persistent tremors. French observers think these tics and tremors could even have an organic basis, supporting their opinion with the lack of success from suggestion. (It’s worth noting [see under Case 528] that French military authorities do not permit the use of hypnosis in the army.) Regarding the current case (530), the French observers would not dispute hypnosis's ability to effect a cure. Babinski and Froment’s Postscript to the English edition of their work on hysteria mentions that while Roussy and Lhermitte claim vasomotor symptoms can vanish with the psychotherapeutic treatment of paralysis and contractures, Roussy and Boisseau later conceded that improvement in thermal and vasomotor control is, at best, a very slow process.
More recent personal communications indicate that there is still room for some question as to the curability by suggestion of such disorders as tic, tremor, vasomotor imbalance, and the like. In short, the true scope of the “pithiatic” or suggestion-curable diseases is still somewhat a matter of controversy.
More recent personal communications suggest that there is still some debate about whether disorders like tic, tremor, and vasomotor imbalance can be cured through suggestion. In short, the true range of “pithiatic” or suggestion-curable diseases remains a bit controversial.
Shell-shock: “Doll’s head” anesthesia, mutism: Hypnosis.
Shell shock: "Doll's head" anesthesia, mutism: Hypnosis.
Case 531. (Nuns, December, 1915.)
An officer, mute for five months following shell-shock, had been for four months treated in a succession of hospitals—field hospital, war hospital, two reserve hospitals.
An officer, silent for five months due to shell shock, had spent four months being treated in a series of hospitals—field hospital, war hospital, and two reserve hospitals.
He had no acquired or hereditary neuropathic taint, but even in the period before the critical shock he had been under tremendous physical and mental strain. The explosion produced a total anesthesia of the skin of the head, face, neck and shoulder region—in short, what Charcot called the “doll’s head” form of sensory disorder. Moreover, there was a marked contraction of the visual fields.
He had no genetic or inherited nerve damage, but even before the critical shock, he had been under immense physical and mental stress. The explosion caused complete numbness of the skin on his head, face, neck, and shoulders—in short, what Charcot referred to as the “doll’s head” type of sensory disorder. Additionally, there was a noticeable narrowing of his visual fields.
The patient, when treatment was given, fell at once into a deep hypnosis and began to intone, and then to speak isolated words, and finally to speak complete sentences. All that was left of his mutism was a slight over-fatiguability of the speech organs. This also cleared up in the next few days. He was discharged well, and had already been—December, 1915—some months in the field.
The patient, after receiving treatment, quickly entered a deep hypnosis and started to intone, then to say single words, and finally to form complete sentences. The only remnant of his mutism was a slight fatigue in his speech muscles. This also resolved in the following days. He was discharged in good condition and had already spent several months in the field by December 1915.
Case 531, though an officer, responded to hypnosis well, and Nonne remarks that hypnotizability is independent of the presence of any neuropathic tendencies, or of any loss of resistance through exhaustion. One trouble with the hypnotic method, according to Nonne, is the fatigue of the hypnotizer and his inability to rely upon assistants.
Case 531, even though he was an officer, responded well to hypnosis, and Nonne notes that how easily someone can be hypnotized doesn't depend on any neurological issues or exhaustion. Nonne mentions that one problem with the hypnotic method is the tiredness of the hypnotist and their inability to depend on helpers.
Re Charcot, Nonne remarks that the work of Charcot on hysteria is not sufficiently well-known, especially as civilian practitioners in peace times had few cases. Re taint, Nonne found such tendencies absent in more than half of his cases with careful anamneses. The absence of adequate psychogenic cause is a not uncommon experience according to Nonne. Nonne, finding 26 cases of pure neurosis amongst 1800 cases of war injury, had a considerable number of odd erroneous diagnoses in the group. Not only were cerebrospinal paralyses wrongly diagnosticated, but ischemic paralysis, plexus paralysis, arthritis deformans and synovitis.
Re Charcot, Nonne points out that Charcot's work on hysteria isn't very well-known, especially since civilian doctors in peacetime encountered few cases. Re taint, Nonne discovered that such tendencies were absent in more than half of his cases after thorough histories were taken. The lack of a proper psychogenic cause is a common finding, according to Nonne. After identifying 26 cases of pure neurosis among 1800 cases of war injuries, Nonne noted that there were quite a few misdiagnoses in that group. Not only were cerebrospinal paralysis cases incorrectly diagnosed, but also ischemic paralysis, plexus paralysis, rheumatoid arthritis, and synovitis.
A soldier is put in the Landsturm at 22 and later called “unfit” by reason of tremors after mine-explosion (history of tremors at 14 after a fall), but is cured by hypnosis.
A soldier is placed in the Landsturm at 22 and later labeled as "unfit" due to tremors after a mine explosion (he had a history of tremors at 14 after a fall), but he is cured through hypnosis.
Case 532. (Grünbaum, November, 1916.)
A Landsturm soldier, 22 (father excitable, family otherwise normal), had a history of being the best scholar in the class and well up to his fourteenth year. At 16 he fell from a tree and though he apparently sustained no injury his head and arm began to tremble. He became unable to learn and gave up his preparations to be a teacher. The tremor, however, disappeared in six months and he went into some technical work. At 16½ years he went as cabin-boy, but in a fortnight he was sent home by the physician. He then began to breed carrier pigeons and got first prizes at international exhibitions. He also went into foundry work and did well as an apprentice. He worked well at home and busied himself with setting up small electrical and other machines. He had never been interested in women and loved his pigeons best, and therefore was regarded by people who knew him as not quite right. He was also non-alcoholic.
A Landsturm soldier, 22 (excitable father, otherwise normal family), had a reputation for being the top student in his class up until he was fourteen. At 16, he fell out of a tree and although he didn’t seem to hurt himself, his head and arm started shaking. He became unable to learn and gave up his plans to become a teacher. However, the tremors went away after six months, and he moved on to some technical work. At 16½, he worked as a cabin boy, but within two weeks, a doctor sent him home. He then started breeding carrier pigeons and won first prizes at international shows. He also worked in a foundry and did well as an apprentice. He was productive at home, tinkering with small electrical and other machines. He had never been interested in women and preferred his pigeons, leading those who knew him to see him as a bit odd. He also didn’t drink alcohol.
After mobilization he was sent back twice but finally was put into a Jäger Battalion. After reaching the front he had to have a hernia operation and on getting well went back to his place and a few days later a mine exploded near him. He was much frightened and fell down unconscious. On regaining consciousness he felt a “running” in the legs and tremors in the hands. The latter grew stronger and began to affect the arms.
After mobilization, he was sent back twice but was finally assigned to a Jäger Battalion. Once he reached the front, he needed a hernia operation, and after recovering, he returned to his unit. A few days later, a mine exploded nearby. He was extremely frightened and collapsed unconscious. When he regained consciousness, he felt a “running” sensation in his legs and tremors in his hands. The tremors intensified and started to affect his arms.
After two months in hospital he went to garrison unrecovered, was placed in the Landsturm and did four months station duty in Russia. The tremors persisted and when his comrades played a bad practical joke on him the tremors got so bad that he was sent back home as unfit for service.
After two months in the hospital, he went to the garrison without fully recovering, was assigned to the Landsturm, and spent four months on station duty in Russia. The tremors continued, and when his fellow soldiers pulled a cruel prank on him, the tremors worsened so much that he was sent back home as unfit for service.
He was a stocky looking, well-nourished man of middle height, without visceral disease or sign of organic nervous disorder.[746] The shaking tremor grew much more powerful in any state of excitement but always paused sufficiently to permit the execution of any particular movement. The head movements were continuous, slight rotations. There were a few regions of anesthesia to touch, but these areas differed at different examinations. There was a general hyperesthesia. Conjunctival, corneal and pharyngeal reflexes were absent. The man was slightly excitable, apprehensive, depressed, complained of sleeping badly, did not want to sit or stand and felt as if he wanted to run away, no matter where. In dropping off to sleep he would fall out of bed and talked aloud in his sleep. He thought he was incurably sick. Intelligence and school knowledge were very good.
He was a stocky, healthy-looking man of average height, without any signs of internal disease or organic nervous issues.[746] The tremors intensified significantly during times of excitement but always paused enough to allow him to carry out specific movements. His head movements were continuous and involved slight rotations. There were a few areas of numbness to the touch, but these zones changed with different examinations. He experienced overall heightened sensitivity. Conjunctival, corneal, and pharyngeal reflexes were absent. The man was somewhat excitable, anxious, and depressed, complained about poor sleep, and did not want to sit or stand, feeling an urge to escape, regardless of where. As he was falling asleep, he would sometimes fall out of bed and talk in his sleep. He believed he was terminally ill. His intelligence and academic knowledge were very good.
He was hypnotized eight times for periods of about five minutes each. Hypnosis was extremely easy to accomplish. At the second trial the manual tremor disappeared. After the third trial there was an essential improvement in the shaking tremor. Moreover, his emotional state had become happier. He began to sleep well. He was now free from disease and regained confidence and looked upon himself as well and fit for work. Undoubtedly without hypnotism this man would have been released from service after a few months of inconsequential hospital care without pension.
He was hypnotized eight times, with each session lasting about five minutes. Getting him into a hypnotic state was very easy. By the second session, his manual tremor was gone. After the third session, there was a significant improvement in his shaking. Plus, he felt much happier emotionally. He started sleeping well. He was now free from illness, gained confidence, and saw himself as healthy and ready to work. Without hypnosis, this man would have likely been discharged from service after a few months of pointless hospital treatment without a pension.
Re tremors, see remarks under Case 308, concerning the possibly organic nature of many of the so-called Shell-shock tremors; an opinion apparently shared in by Meige and by Guillain. Babinski also found that these tremors were not influencible by psychotherapy. Yet here is an instance in which tremors are reported cured by hypnosis, and moreover, tremors that were recurrent from an ante-bellum attack at 14. See remarks under Case 530.
Re tremors, see comments under Case 308, regarding the potentially organic nature of many of the so-called Shell-shock tremors; an opinion seemingly supported by Meige and Guillain. Babinski also discovered that these tremors were not affected by psychotherapy. However, here is a case where tremors are reported to be cured by hypnosis, and furthermore, tremors that were recurring from a pre-war attack at age 14. See comments under Case 530.
Shell-shock, slight injury, unconsciousness: Astasia-abasia: Recovery under hypnosis, two séances.
Shell shock, minor injury, unconsciousness: Astasia-abasia: Recovery through hypnosis, two sessions.
Case 533. (None, December, 1915.)
A musketeer, without neuropathic taint and without nervous symptoms before the war (parents both dead of tuberculosis, eleven brothers and sisters died young), saw four comrades killed by a shell October 27, 1914. The musketeer himself was slightly injured superficially in the back. He remained unconscious for three hours and on coming out showed general tremor of the body, felt pressure in the head, was lachrymose and unable to walk or stand. He was subject to insomnia. He was in four different hospitals, finally reaching Eppendorf. Diagnosis rendered at the first hospital and carried on through the others was hemorrhage into the spinal canal.
A musketeer, who had no nerve damage or symptoms before the war (both parents died of tuberculosis, and eleven siblings passed away young), witnessed four comrades killed by a shell on October 27, 1914. The musketeer himself suffered a minor injury to his back. He was unconscious for three hours, and when he woke up, he experienced shaking all over, felt pressure in his head, was tearful, and couldn't walk or stand. He also dealt with insomnia. He stayed in four different hospitals, eventually reaching Eppendorf. The diagnosis made at the first hospital and continued through the others was bleeding into the spinal canal.
For two months at Eppendorf he lay in extension. He was then examined by Nonne, who found general neuropathic habitus, pronounced “cramp neurosis” in the lower extremities, psychogenic astasia-abasia, hyperidrosis of the lower extremities, marked cyanosis of feet and lower legs, increased tendon and skin reflexes, pseudoclonus, no Babinski or Oppenheim reflexes. The man complained of pressure in the head, sleeplessness, a feeling of depression and hopelessness. Pulse 120-130.
For two months at Eppendorf, he lay flat. He was then examined by Nonne, who found general neuropathic traits, severe “cramp neurosis” in the legs, psychogenic inability to stand or walk, excessive sweating in the lower legs, significant blueness in the feet and lower legs, heightened tendon and skin reflexes, pseudoclonus, and no Babinski or Oppenheim reflexes. The man complained of pressure in his head, insomnia, and feelings of depression and hopelessness. His pulse was 120-130.
Hypnosis proved easy. After the first treatment the man stood and walked and showed no tremor. The next day the hypnosis was repeated and the cyanosis of the legs disappeared. Sleep on the second night was good. Appetite returned and the man fell into a good emotional state. Thereafter the patient was intentionally ignored by the physicians and could soon not be distinguished in any respect from the other non-nervous convalescents.
Hypnosis was simple. After the first session, the man stood up, walked, and showed no signs of trembling. The next day, the hypnosis was done again, and the blue discoloration in his legs went away. He slept well on the second night. His appetite came back, and he felt emotionally stable. From then on, the doctors intentionally overlooked the patient, and soon he was indistinguishable from the other non-anxious patients recovering.
This case is expressly stated by Nonne to resemble in all respects those formerly described by Oppenheim as[748] “traumatic neurosis.”
This case is specifically described by Nonne as being similar in every way to those previously mentioned by Oppenheim as[748] “traumatic neurosis.”
Crural monoplegia: Cured by hypnosis.
Leg paralysis: Cured by hypnosis.
Case 534. (Hurst, 1917.)
A Belgian soldier fell into mud on the collapse of a roof from which he was observing the enemy. It was an hour before he got his left leg out of the mud, and found it fixed in extension. He was sent to England, where for three months the leg remained stiff. The spastic paralysis did not seem organic as the leg was dragged behind. The knee and ankle could be bent only by using much force. The entire leg was in all ways anesthetic. Babinski sign gave additional proof that the condition was hysterical: when the patient lay with arms folded and legs apart and then tried to sit up, the normal leg was lifted and the paralyzed leg remained flat.
A Belgian soldier fell into mud when a roof collapsed while he was watching the enemy. It took him an hour to free his left leg from the mud, and he found it stuck straight out. He was sent to England, where his leg stayed stiff for three months. The spastic paralysis didn’t seem organic since the leg was being dragged behind him. The knee and ankle could only be bent with a lot of force. The entire leg was completely numb. The Babinski sign further indicated that the issue was hysterical: when the patient lay with his arms crossed and legs apart, then tried to sit up, the normal leg lifted while the paralyzed leg stayed flat.
According to Hurst, the paralysis and stiffness were due to an autosuggestion from the legs being embedded in mud. The anesthesia was probably a matter of medical suggestion produced in the course of examination during the three months of disability. According to Hurst, Babinski is right in supposing that hysterical anesthesia is almost invariably produced by the observer.
According to Hurst, the paralysis and stiffness were caused by the legs being stuck in mud due to autosuggestion. The numbness was likely a result of medical suggestion that occurred during the examination throughout the three months of disability. Hurst believes that Babinski is correct in suggesting that hysterical numbness is almost always created by the observer.
Accordingly a strong faradic current was passed through the leg, and he was assured that sensation and power would be restored. However, he could still walk only with difficulty.
Accordingly, a strong faradic current was passed through the leg, and he was assured that sensation and strength would be restored. However, he could still walk only with difficulty.
Hypnosis was therefore resorted to and repeated on several occasions. He went back to duty in three weeks, although he still held the leg somewhat stiff when he walked.
Hypnosis was used on multiple occasions. He returned to duty in three weeks, although he still walked with a bit of stiffness in his leg.
Re recurrences after hypnotism, see remarks of Nonne under Case 530. Howland also notes that cases treated by hypnotism must be followed up to prevent relapse. In the above case of Hurst’s, it will be noted that the hypnotic treatment was several times repeated.
Re recurrences after hypnotism, see remarks of Nonne under Case 530. Howland also points out that cases treated with hypnotism need follow-ups to avoid relapse. In the case of Hurst mentioned above, it’s important to note that the hypnotic treatment was repeated several times.
Shell-shock, emotional (slight trauma): Tremors and sensory impairment: Cure by hypnosis, thrice repeated.
Shell shock, emotional (mild trauma): Tremors and sensory issues: Treated with hypnosis, three times repeated.
Case 535. (Nonne, December, 1915.)
A reservist, always well, not neuropathic (mother had had seizures, possibly epileptic, for many years) was wounded in the left calf by a shell fragment, about the middle of December, 1914. He was at the same time, as a result of the shell explosions near by, afflicted with a tremor of the whole body; this tremor gradually increased and proved refractory to all treatment for nine months.
A reservist, who was always in good health and not neuropathic (his mother had experienced seizures, possibly epileptic, for many years), was injured in his left calf by a shell fragment around mid-December 1914. At the same time, due to the nearby shell explosions, he developed a full-body tremor; this tremor gradually worsened and resisted all treatment for nine months.
At the beginning of September, 1915, the patient reached Nonne’s wards, showing tremor of head, arms and legs, with pronounced hypalgesia of the whole body, abolition of frontal and conjunctival reflexes, and contraction of the visual fields.
At the start of September 1915, the patient arrived at Nonne's wards, displaying tremors in the head, arms, and legs, along with significant reduced sensitivity throughout the body, loss of frontal and conjunctival reflexes, and narrowing of the visual fields.
The tremor of the head was completely removed at the first hypnotic treatment. There was a slight recurrence of this tremor two days later, and traces of it could be observed for nine days. A third hypnotic treatment swept away this tremor, which did not return.
The head tremor was completely eliminated after the first hypnotic session. There was a slight return of the tremor two days later, and remnants of it could be seen for nine days. A third hypnotic session got rid of this tremor, which did not come back.
The patient was discharged after about four weeks, suitable for garrison duty.
The patient was released after about four weeks, fit for garrison duty.
Re traumatic neurosis, Nonne dislikes this term of Oppenheim, because such a term rather tends to connote unfavorable prognosis. As quoted under Case 530, Nonne holds that the war data show that hysteria is neither a form of degeneration nor an affair built on the Freudian schema.
Re traumatic neurosis, Nonne dislikes this term from Oppenheim, as it tends to suggest a negative prognosis. As quoted under Case 530, Nonne believes that the war data indicates hysteria is neither a form of degeneration nor something based on the Freudian model.
Nonne in fact maintains that the hysterical syndrome may occasionally occur with much greater ease in a normal person than ever has been known before. It is precisely in these cases of normals getting hysterical that Nonne gets especially good results with hypnosis. If the development of the hysterical syndrome had extended over days or weeks, then the hypnotic cure was a slower one. The above reservist developed his Shell-shock gradually and required three[750] hypnotic treatments. But although the number of doses of hypnotism required may be said roughly to depend upon the time which the condition took to come to a head, yet there is no similar rule re duration. A miracle cure may be brought about even in cases that have lasted over a year. This result, if confirmed, would signify that the hysterical condition once fixated did not especially increase in its tenacity.
Nonne argues that the hysterical syndrome can sometimes occur more easily in a normal person than ever seen before. It’s in these cases of normal individuals becoming hysterical that Nonne sees particularly good results with hypnosis. If the development of the hysterical syndrome has taken days or weeks, then the hypnotic treatment is a slower process. The reservist developed his Shell-shock gradually and needed three[750] hypnotic sessions. While the number of hypnosis sessions required generally depends on how long the condition took to develop, there isn’t a similar rule regarding the duration. A miraculous recovery may happen even in cases that have lasted over a year. If this result is confirmed, it would mean that once the hysterical condition is established, it doesn’t necessarily become more stubborn.
Re hypnosis in Germany, it should be noted that Nonne is the chief protagonist for hypnosis, at least among the well-known neurologists. Psychoelectric cures, which the Germans term Kaufmann’s cure, are also greatly in vogue in German clinics. Despite the well-based claims of Lt.-Col. Myers and of Eder, some English observers appear to condemn hypnosis as inadequate, or even as dangerous.
Regarding hypnosis in Germany, it's important to highlight that Nonne is the main advocate for hypnosis, at least among the prominent neurologists. Psychoelectric treatments, which Germans refer to as Kaufmann’s cure, are also very popular in German clinics. Despite the well-founded claims of Lt.-Col. Myers and Eder, some English observers seem to dismiss hypnosis as insufficient or even risky.
A series of relatively successful cases like those here mentioned might yield a wrong impression of the value of hypnosis (see Feiling’s unsuccessful case 369).
A number of relatively successful cases like the ones mentioned here might give a misleading impression of the effectiveness of hypnosis (see Feiling’s unsuccessful case 369).
Hysterical paraplegia of gradual development: recovery only under repeated hypnosis.
Hysterical paraplegia that develops slowly: recovery only through repeated hypnosis.
Case 536. (None, December, 1915.)
A volunteer, of nervous parents, had for four years suffered from attacks of uncertain (hysterical or epileptic) nature. These attacks came on again after strenuous marching in the campaign in Belgium and France. Released from service at the front and detailed for guide duty, he proved unsuitable for this work, too, and was sent back to a hospital at home. Here there gradually developed a paralysis of the lower extremities. Treatment proved ineffective.
A volunteer, with anxious parents, had suffered for four years from episodes of an uncertain nature (hysterical or epileptic). These episodes returned after intense marching during the campaign in Belgium and France. After being released from front-line service and assigned to guide duty, he was found unsuitable for that role as well and was sent back to a hospital at home. There, he gradually developed paralysis in his lower limbs. Treatment was ineffective.
At the end of January, 1915, he came to Nonne’s wards at Eppendorf with a paralysis that had lasted six months. There was a total paraplegia inferior, with anesthesia for all sensation from the knees downward. The lower legs and feet were cyanotic and cold. The tendon and skin reflexes were lively. There was a moderate contraction of the visual fields on both sides.
At the end of January 1915, he arrived at Nonne's wards in Eppendorf with paralysis that had lasted six months. He had complete paralysis below the waist, with no sensation from the knees down. His lower legs and feet were blue and cold. The reflexes in his tendons and skin were active. There was a slight narrowing of his visual fields on both sides.
Under hypnosis, the patient proved able to move both joints somewhat, but very weakly and slowly. The patient was hypnotized daily for a week, and made slow progress. Only after another week did it prove possible to get him to stand. After four weeks, his gait had so improved as to look like that of a tired old man. Three weeks more of treatment permitted the patient to walk, run and hop normally. Repeated waking suggestion had failed to accomplish anything in this case. The improvement followed only hypnosis. It seems to be a general principle that in cases of gradual development, the recovery by hypnosis will also be gradual.
Under hypnosis, the patient was able to move both joints a little, but very weakly and slowly. The patient was hypnotized daily for a week and made slow progress. It wasn't until another week that he was able to stand. After four weeks, his walking had improved enough to resemble that of a tired old man. Three more weeks of treatment allowed the patient to walk, run, and hop normally. Repeated waking suggestion hadn’t done anything in this case. The improvement only came from hypnosis. It seems to be a general principle that in cases of gradual development, recovery through hypnosis will also be gradual.
Re repeated hypnosis for cases of gradual development, see remarks under the preceding case (535).
Re repeated hypnosis for situations of gradual development, refer to comments in the previous case (535).
Struck by rifle butt: blindness of an eye already poor. Shell-shock: dysbasia. Hypnosis.
Struck by a rifle butt: blindness in an already weak eye. Shell shock: difficulty walking. Hypnosis.
Case 537. (Ormond, May, 1915.)
A lieutenant, 20 years, managed to get into the army despite the fact that he had never been able to use his left eye, owing to hypermetropia and amblyopia. He was hit on the left side of the head by a rifle butt, and knocked unconscious, in June. On recovering, he found he could not see at all with his left eye, which he had never been in the habit of using. August 10, he was wounded slightly in the left thigh. August 23, while still on duty, with the wound not completely healed, he was blown up by a shell. He regained consciousness on a stretcher. Feeling the pain in his old wound, he thought he should be unable to walk.
A 20-year-old lieutenant managed to join the army even though he had never been able to use his left eye, due to farsightedness and a lazy eye. In June, he was struck on the left side of the head by a rifle butt and knocked out. When he woke up, he realized he couldn’t see at all with his left eye, which he had never really used. On August 10, he was slightly wounded in his left thigh. On August 23, while still on duty and with the wound not fully healed, he was blown up by a shell. He came to on a stretcher. Feeling pain from his old wound, he thought he wouldn’t be able to walk.
On shipboard, he found that he actually could not walk. He kept his left eye covered by a shade on account of headache that would follow exposure to light. He was much excited and had bad nightmares.
On the ship, he realized that he couldn't actually walk. He kept his left eye covered with a shade because of a headache that would come after being exposed to light. He felt very anxious and had terrible nightmares.
After the journey home from the Dardanelles, it was found that the left eye was normal except for the hypermetropia, despite the fact that he was quite unable to see with the eye.
After the trip home from the Dardanelles, it was discovered that the left eye was normal except for the farsightedness, even though he still couldn't see out of that eye.
He was hypnotized four times, losing the nightmares and much of the headache after the first treatment; the eye pain on exposure to light, after the second treatment; and the blindness, after the third treatment. He was now able to see with his left eye as well as before he was struck. He was still unable to walk without crutches. Hypnotized the fourth time, he was told he could walk, and did so.
He was hypnotized four times, losing the nightmares and most of the headache after the first session; the eye pain when exposed to light, after the second session; and his blindness, after the third session. He was now able to see with his left eye just as well as before the accident. He still couldn’t walk without crutches. During the fourth hypnosis, he was told he could walk, and he did.
For hypnotic treatment of blindness, see under Case 521. Re blindness of eye already poor, see Cases 294-301 (296 and 297 eye cases). Ormond states that in the treatment of Shell-shock blindness, he first tried rest, tonics, cutting off tobacco, confinement in bed, isolation, persuasion, encouragement, counter-irritation; but that all these measures failed. Suggestion and hypnosis succeeded.
For the hypnotic treatment of blindness, see under Case 521. Regarding blindness in an already damaged eye, refer to Cases 294-301 (296 and 297 eye cases). Ormond mentions that when treating shell-shock blindness, he initially tried rest, tonics, cutting out tobacco, bed confinement, isolation, persuasion, encouragement, and counter-irritation; however, all these methods failed. Suggestion and hypnosis worked.
Shell explosion; concussion; retinal hemorrhage: Blindness. Cure by hypnosis.
Shell explosion; concussion; retinal hemorrhage: Blindness. Cure through hypnosis.
Case 538. (Hurst, November, 1916.)
An English private, 22, was looking over a parapet, July 18, 1915. He afterward remembered sand thrown in his eyes and a fall backward, hitting his head, after a shell had struck the sandbags in front of him. He was unconscious 24 hours. Upon recovery, he found himself completely blind, save that he could just tell light from darkness with the left eye. His eyes were sore and eyelids blackened; there was also severe headache and partial deafness.
An English private, 22, was peering over a parapet on July 18, 1915. He later recalled feeling sand thrown in his eyes and then falling backward, hitting his head after a shell exploded near the sandbags in front of him. He was unconscious for 24 hours. When he came to, he discovered he was completely blind, but could barely distinguish light from darkness with his left eye. His eyes were sore and his eyelids were bruised; he also had a severe headache and partial deafness.
Hearing returned and the headache improved shortly; but the condition of the eye seemed more permanent. On forcibly opening the eyes, September 14, they were turned far upwards so that the iris could scarcely be seen. Some sand grains were buried in the conjunctiva, not in the cornea. There was no inflammation about the sand grains.
Hearing came back and the headache got better soon after; however, the situation with the eye appeared to be more lasting. When forcibly opening the eyes on September 14, they were turned so far upward that the iris was barely visible. A few grains of sand were stuck in the conjunctiva, not in the cornea. There was no inflammation around the sand grains.
In hypnosis, he was told that he would see on waking. The moment he woke, this suggestion was repeated forcibly and his eyes were held open. He cried out that he could see; tears ran down his cheeks; he fell on his knees in gratitude. Three days later, he said he was able to see as well as he had ever seen. There was, however, an opacity of the vitreous of the left eye, the result of a retinal hemorrhage: doubtless the result of injury at the time of the explosion. September 30, he had perfect vision in the right eye and 6/36 in his left.
In hypnosis, he was told that he would be able to see when he woke up. As soon as he opened his eyes, this suggestion was strongly repeated, and his eyelids were kept open. He shouted that he could see; tears streamed down his face; he dropped to his knees in gratitude. Three days later, he claimed he could see as well as he ever could. However, there was some clouding in the vitreous of his left eye, likely due to a retinal hemorrhage from the injury sustained during the explosion. By September 30, he had perfect vision in his right eye and 6/36 vision in his left.
Re results of hypnotic treatment, Lt.-Col. Myers, summarizing 23 cases of Shell-shock, got apparently complete cures in 26 per cent, and distinct improvement in another 26 per cent. He failed to hypnotize 35 per cent, and got no improvement after hypnosis in 13 per cent. Is the recovery after hypnosis complete and permanent? Lt.-Col. Myers believes that it may be, but others remark the tendency to relapse (see Case 534). Similar objections may be made to the psychoelectric treatment as used by Vincent, Yealland, or Kaufmann. See under Case 535.
Re the results of hypnotic treatment, Lt.-Col. Myers, summarizing 23 cases of shell shock, achieved what seemed like complete cures in 26 percent and noticeable improvement in another 26 percent. He was unable to hypnotize 35 percent of the cases, and there was no improvement after hypnosis in 13 percent. Is recovery after hypnosis totally and permanently effective? Lt.-Col. Myers thinks it might be, but others point out the tendency for patients to relapse (see Case 534). Similar criticisms can be made regarding the psychoelectric treatment used by Vincent, Yealland, or Kaufmann. See under Case 535.
Appendix operation: Post-operative retention of urine. Relief by hypnosis.
Appendix surgery: After the operation, difficulty with urination. Relief through hypnosis.
Case 539. (Podiapolsky, August, 1917.)
A soldier, 32, operated for appendicitis, had a post-operative retention of urine. Hypnotic suggestion was requested to reëstablish excretion of urine before resort should be had to the catheter.
A 32-year-old soldier who had surgery for appendicitis experienced urinary retention after the operation. Hypnotic suggestion was requested to help him urinate again before having to use a catheter.
Somnambulistic amnesia was obtained at once and without questioning him P. suggested to him directly that he must feel the need of micturition. The suggestion was unsuccessful. However, bearing in mind psychogenic obstacles of an unknown nature, P. questioned the patient as to sensations and learned that in the operation the skin had been burned about the urinary passage and that the patient feared micturition. Besides this, micturition was painful on account of the wound above the appendix. The patient also feared that the sutures would yield.
Somnambulistic amnesia was established right away, and without hesitation, P. directly suggested to him that he must feel the urge to urinate. The suggestion did not work. However, considering the psychological barriers of an unknown kind, P. asked the patient about his sensations and discovered that during the procedure, the skin around the urinary passage had been burned and that the patient was anxious about urination. Additionally, urination was painful due to the wound above the appendix. The patient was also worried that the stitches might come apart.
Accordingly assurance was given that the burned parts would be insensible and that the bladder could be emptied without effort and without endangering the sutures. Analgesia was produced by a few passages of the hand upon the bed clothes. Complying with post-hypnotic suggestion the patient urinated after a quarter of an hour of sleep, and in thirty-six hours retention was relieved.
Accordingly, reassurance was given that the burned areas would be numb and that the bladder could be emptied easily without risking the stitches. Pain relief was achieved by lightly rubbing the bedclothes. Following the post-hypnotic suggestion, the patient urinated after about fifteen minutes of sleep, and in thirty-six hours, the retention was resolved.
With respect to frequency of immediate somnambulism for the first trial, P. states that, although authorities set the percentage of successful immediate somnambulisms at 17-20 per cent, war conditions yield three or four times as high a percentage. The war has produced a suitable soil for hypnotism. Hypnosis is impossible in from 1½ to 2 per cent of cases.
Regarding the frequency of immediate sleepwalking in the first trial, P. mentions that while experts estimate the success rate of immediate sleepwalking at 17-20 percent, war conditions result in three to four times that percentage. The war has created a favorable environment for hypnosis. Hypnosis is ineffective in about 1.5 to 2 percent of cases.
Wound of sciatic nerve: Pains after operation. Relief by hypnosis.
Wound of sciatic nerve: Pain after surgery. Relief through hypnosis.
Case 540. (Podiapolsky, August, 1917.)
A German prisoner, 33, was admitted to a Russian Hospital, November 11, 1916, with “a bad wound of upper right thigh, marked pains in right sciatic nerve especially affecting feet.” Morphine and pantopon did not abolish the pain. Insomnia. November 13, the sciatic nerve was surgically freed from a scar and laid in the midst of the femoral biceps. Every evening pantopon was injected; but the pains and insomnia persisted nevertheless.
A 33-year-old German prisoner was admitted to a Russian hospital on November 11, 1916, with a severe wound in his upper right thigh and significant pain in his right sciatic nerve, particularly affecting his feet. Morphine and pantopon didn’t relieve the pain. He had insomnia. On November 13, surgeons freed the sciatic nerve from a scar and positioned it amid the femoral biceps. Every evening, pantopon was injected; however, the pain and insomnia continued.
November 19, he was hypnotized. The pain stopped. He had an excellent night, and the next day felt only a slight pain in the toes.
November 19, he was hypnotized. The pain stopped. He had a great night, and the next day felt just a little pain in his toes.
Curiously enough, while giving him suggestion in the German language, P. had said fingers instead of toes (inadvertently, since the Russian language uses the same term for both). He slept well to November 29 but still felt a slight pain in the toes. On November 29 another hypnotic sitting was given, and the toes this time were named correctly. The next day the patient said, “You have relieved me of all the rest of my pain.” He had no pain thereafter and the morphine and pantopon were dispensed with. Sleep returned.
Curiously, while suggesting in German, P. accidentally said "fingers" instead of "toes" (since the same word is used for both in Russian). He slept well until November 29 but still felt a bit of pain in his toes. On November 29, he had another hypnotic session, and this time, the toes were named correctly. The next day, the patient said, “You’ve taken away all my other pain.” He felt no pain after that, and they stopped the morphine and pantopon. Sleep came back.
Incidentally, this patient had his hair grow white in a few months of war.
Incidentally, this patient had his hair turn white within a few months of the war.
Ship blown up by mine: Stereotyped explosion dream by survivor: Cure by hypnosis (also of antebellum habitual headache).
Ship blown up by a mine: Typical explosion dream by survivor: Treatment by hypnosis (also for pre-war chronic headache).
Case 541. (Riggall, April, 1917.)
A survivor of H.M.S. T.B. II, blown up by a mine off Harwich, was admitted to the naval hospital at Chatham, March 3, 1916, a well-nourished, nervous looking lad, aged 20. After the accident, he began to dream, always the same dream, of the explosion, waking up with the cry of the ship mates, and then unable to sleep the rest of the night. The knee and ankle-jerks were somewhat exaggerated.
A survivor of H.M.S. T.B. II, which was blown up by a mine off Harwich, was admitted to the naval hospital in Chatham on March 3, 1916. He was a well-nourished, nervous-looking young man, 20 years old. After the accident, he started having the same dream repeatedly about the explosion, waking up to the cries of his shipmates, and then he couldn’t sleep for the rest of the night. His knee and ankle reflexes were somewhat exaggerated.
April 15, when there had been no improvement, he was hypnotized. The patient was told to lie back in an arm chair, make himself comfortable and allow muscles to relax. He was told to fix his eyes and concentrate his attention on an electric lamp. The suggestion of sleep was made, and he was repeatedly told in a monotonous voice that he was becoming more and more sleepy. Then in an emphatic voice he was told that the treatment would completely cure him. He had no more dreams after this first sitting.
April 15, when there had been no improvement, he was hypnotized. The patient was instructed to lie back in an armchair, get comfortable, and let his muscles relax. He was asked to fix his eyes and focus on an electric lamp. The suggestion of sleep was given, and he was repeatedly told in a monotone voice that he was becoming more and more sleepy. Then, in a firm voice, he was told that the treatment would completely cure him. He didn’t have any more dreams after this first session.
Hypnosis was continued every other day until April 20, when he was discharged cured. After the first sitting hypnosis was induced by simply telling the patient to go to sleep, which he would immediately do on entering the room, while still standing up. At subsequent sittings, he was made to write twenty times such phrases as: “I feel much better”; “I shall have no more bad dreams.”
Hypnosis was carried on every other day until April 20, when he was discharged as cured. After the first session, hypnosis was triggered by simply telling the patient to go to sleep, which he would immediately do upon entering the room, while still standing up. In the following sessions, he was instructed to write twenty times phrases like: “I feel much better”; “I won’t have any more bad dreams.”
Once when a tooth was to be pulled a post-hypnotic suggestion that no more pain would be felt was given, nor was any pain felt. Headache persisted after the first two or three sittings. Accordingly, during hypnosis a pencil was pressed to the forehead with the suggestion that it would burn and that after waking there would be an itching pain for half an hour, followed by recovery from headache. Curiously enough, a distinct erythema of the skin was observed over the point of pressure. Toothache and headache vanished.
Once, when a tooth was about to be pulled, a post-hypnotic suggestion was given that no pain would be felt, and indeed, no pain was experienced. The headache continued after the first two or three sessions. So, during hypnosis, a pencil was pressed to the forehead with the suggestion that it would burn and that after waking, there would be an itching pain for half an hour, followed by relief from the headache. Interestingly, a noticeable redness of the skin was observed at the point of pressure. Both the toothache and headache disappeared.
Shell-shock from air-craft bomb: Amnesia: Recovery under hypnosis (also removal of a headache dating from childhood).
Shell shock from an aircraft bomb: Amnesia: Recovery under hypnosis (also relief from a headache that goes back to childhood).
Case 542. (Burmiston, January, 1917.)
May 22, 1916, a stoker, 26, was found on shipboard in a workshop behind oil drums, refusing to come out, looking dazed, not recognizing messmates, suspicious and complaining of headache. He reached the Royal Naval Hospital at St. Malo, May 24, answering questions “Don’t know,” and physically normal except for diminished knee-jerks. At the end of two or three weeks he would answer questions about his stay at the hospital, but complained of headache or weight in the head. Wassermann reaction, negative.
On May 22, 1916, a 26-year-old stoker was found on board a ship in a workshop behind some oil drums. He was refusing to come out, appearing dazed, not recognizing his shipmates, and was suspicious while complaining of a headache. He arrived at the Royal Naval Hospital in St. Malo on May 24, responding to questions with "Don’t know," and was physically normal except for reduced knee-jerk reflexes. After two or three weeks, he began to answer questions about his time in the hospital but continued to complain of headaches or a heavy feeling in his head. The Wassermann test came back negative.
Special examination on May 26, showed an amnesia for everything up to his arrival at St. Malo. For example, he did not know the name or use of a hammer or a pressure gauge, though he knew the pressure gauge was made of brass and glass, having seen brass and glass in the hospital wards. He had no idea of the nature of a ship. He was sent to the sick bay at the Royal Naval Barracks at Chatham, July 7, carrying a recommendation that he be retrained as a stoker.
A special exam on May 26 revealed that he couldn't remember anything before arriving at St. Malo. For instance, he didn’t recognize the name or function of a hammer or a pressure gauge, even though he knew a pressure gauge was made of brass and glass because he had seen those materials in the hospital wards. He had no concept of what a ship was. He was sent to the sick bay at the Royal Naval Barracks in Chatham on July 7, with a recommendation for retraining as a stoker.
He was put under hypnosis, induced by gazing at the brass knob of a paper weight. He went off easily, was told there was nothing to worry about, taken back to the beginning of his illness, and asked what happened. He told about a bomb explosion from aircraft, and how he had lost his memory after a nearby explosion. He told how he was married and had a child 21 months old. During the narrative about bombs falling, his worry was such that he was put in a deeper hypnotic sleep, and was told that he would remember all that had happened. Upon being ordered to wake up, he remained dazed for a few moments, and then said that he was all right. Asked about his marriage, he replied that of course he was married and had a child.
He was put under hypnosis by focusing on the brass knob of a paperweight. He relaxed easily, was reassured that there was nothing to worry about, taken back to the start of his illness, and asked what had happened. He talked about a bomb exploding from an aircraft and how he lost his memory after a nearby blast. He shared that he was married and had a 21-month-old child. During his recounting of the falling bombs, he became so anxious that he was placed in a deeper hypnotic state, and was told he would remember everything that had happened. When he was instructed to wake up, he felt dazed for a few moments, then said he was fine. When asked about his marriage, he replied that, of course, he was married and had a child.
After four days leave, he returned, July 13, without trouble except a headache, from which it appeared that he had suffered[758] ever since a fall when a child. He was again put into a hypnotic state and asked to remember the accident that caused the headache. He was conducted back through the years, and finally described a white house in India, his fall in the area, the black people in white clothes, the cut bleeding head. He was told that he would have no more of such headaches. On being wakened, he said that his headache was gone, and retold the story of the accident. August 2, he said he had never felt better in his life. September 1, he was drafted to a seagoing ship.
After four days off, he returned on July 13, with nothing wrong except a headache, which he seemed to have had since he fell as a child. He was placed in a hypnotic state again and asked to recall the accident that caused the headache. He was taken back through the years and eventually described a white house in India, his fall in that area, the people in white clothes, and his bleeding cut on the head. He was informed that he would not experience any more headaches. When he woke up, he said his headache was gone and repeated the story of the accident. On August 2, he mentioned that he had never felt better in his life. On September 1, he was drafted to a seagoing ship.
Shell-shock, unconsciousness: Convulsions (recollection of childhood convulsions): Cure by hypnosis.
Shell shock, unconsciousness: convulsions (remembering childhood convulsions): treatment through hypnosis.
Case 543. (Hurst, March, 1917.)
A New Zealander was rendered unconscious for a few minutes following concussion from a high explosive shell. Convulsions developed, occurring at least once and often several times a day.
A New Zealander was knocked out for a few minutes due to a concussion from a high-explosive shell. He experienced convulsions, happening at least once and often several times a day.
As to the origin of these convulsions, it appeared that the soldier had had a few convulsions after falling on his head at the age of 8. According to Hurst, recollection of these childhood convulsions probably led by a process of autosuggestion to the Shell-shock convulsions.
As for the cause of these convulsions, it seemed that the soldier had experienced a few after injuring his head when he was 8. According to Hurst, remembering those childhood convulsions likely triggered the Shell-shock convulsions through a process of autosuggestion.
Captain Crabtree hypnotized the man, suggesting recovery. The fits immediately ceased and did not recur.
Captain Crabtree hypnotized the man, suggesting that he would recover. The seizures immediately stopped and didn’t happen again.
Recurrent hysterical mutism. Spontaneous recovery in (a) 18 months (antebellum incident). (b) Hypnotic recovery in a few minutes.
Recurrent hysterical mutism. Spontaneous recovery in (a) 18 months (pre-war incident). (b) Hypnotic recovery in a few minutes.
Case 544. (Eder, August, 1916.)
A soldier in a mine accident eight years before the war, lost his speech when his brother was killed, and then recovered his speech spontaneously after 18 months.
A soldier in a mining accident eight years before the war lost his ability to speak when his brother died, but he regained his speech on his own after 18 months.
After a shell explosion in Gallipoli, he was again struck speechless and also deaf.
After a shell explosion in Gallipoli, he was once again left speechless and deaf.
Six weeks later, he came to Dr. Eder and objected in writing to treatment, saying that he believed in nature’s methods. God had taken his voice away before and had restored it. Eder replied in writing “rather irreverently” that God had taken 18 months, but he could do it in a few minutes. The patient afterward consented to treatment, and speech and hearing were duly restored in the time promised, whereupon Dr. Eder told him that in point of fact his physician was merely the instrument of Providence.
Six weeks later, he went to Dr. Eder and formally opposed the treatment, stating that he believed in natural healing. He mentioned that God had previously taken away his voice and then given it back. Eder responded in writing “somewhat disrespectfully” that God had taken 18 months to do it, but he could achieve it in just a few minutes. The patient later agreed to the treatment, and his speech and hearing were successfully restored within the promised time, after which Dr. Eder told him that in reality, his physician was just a tool of Providence.
Neurasthenic symptoms: Cured by repeated hypnosis.
Neurasthenic symptoms: Healed through repeated hypnosis.
Case 545. (Tombleson, September, 1917.)
A private, 24, was admitted to hospital with diagnosis neurasthenia, March 11, 1916. He suffered from vertical headache; general analgesia, more definite on the right side (patient left-handed); loss of smell and taste, also more definite on the right side; paresis of right leg, with dragging of foot (old trench foot); and sleeplessness.
A 24-year-old private was admitted to the hospital with a diagnosis of neurasthenia on March 11, 1916. He experienced severe headaches; overall pain sensitivity, more pronounced on the right side (the patient is left-handed); loss of smell and taste, also more pronounced on the right side; weakness in the right leg, with foot dragging (previous trench foot); and insomnia.
The next day Tombleson put him in a hypnotic state, third stage, and again, March 13, but without results.
The next day, Tombleson put him in a hypnotic state, third stage, on March 13 again, but it didn't work.
March 14, the somnambulistic stage was reached in hypnosis, and next day the man’s headache was much relieved as a result of the suggestion offered. He was again hypnotized and the following day, March 16, the headache had vanished and the man was in general much improved. In somnambulism the disappearance of the analgesia was suggested, and it proved possible to make the man walk about without limp and without dragging the right foot. Next day the analgesia was much relieved. In somnambulism the suggestions were repeated.
March 14, the sleepwalking stage of hypnosis was reached, and the next day the man's headache was greatly relieved due to the suggestion made. He was hypnotized again, and the following day, March 16, the headache was gone, and the man was overall much better. During sleepwalking, it was suggested that the pain would disappear, and it became possible to have the man walk around without a limp and without dragging his right foot. The next day, the pain was significantly reduced. In sleepwalking, the suggestions were repeated.
March 18, the man said he was quite well, and proved to be so on examination, except that he could not yet taste with absolute normality on the right side. In somnambulism it was further suggested that the cure was a perfect one and included the sense of taste. However, March 25, the expected improvement had not yet occurred in the taste, whereupon further suggestions were given in hypnotic somnambulism, re taste. Next day taste had become normal.
March 18, the man stated he was feeling fine, and an examination confirmed this, except he still couldn't taste normally on the right side. During a session of sleepwalking, it was suggested that the cure was complete and included the sense of taste. However, by March 25, there had been no improvement in his tasting ability, leading to more suggestions in hypnotic sleepwalking regarding taste. The next day, his taste was completely normal.
Re hypnosis, Tombleson says that the most successful cases of hypnosis are those of Shell-shock psychasthenia, but that he gets very good results with hyperthyroidism and with neurasthenia also. He goes so far as to say that practically all cases of war neurasthenia and psychasthenia can be cured and sent back to work if treatment by hypnotic suggestion is used in a reasonable time.
Regarding hypnosis, Tombleson states that the most successful cases of hypnosis are those involving Shell-shock psychasthenia, but he also achieves very good results with hyperthyroidism and neurasthenia. He even claims that nearly all cases of war neurasthenia and psychasthenia can be treated effectively and returned to work if hypnotic suggestion is applied within a reasonable timeframe.
Neurotic symptoms: Improvement under repeated hypnosis.
Neurotic symptoms: Improvement with repeated hypnosis.
Case 546. (Tombleson, September, 1917.)
A private, 32, was admitted, April 15, 1916, to Tombleson’s ward from the Cottonera Mental Ward with the diagnosis: psychasthenia with paresis of right arm. The man was very suspicious of the medical profession, melancholy, morose and prone to tears. He had been kicked by a horse four years before and showed a depressed and very tender scar in the right parietal region. The right side of the body since that injury had been getting weaker, but the arm was much weaker than the leg. Anesthesia was practically complete on the right side. There was a wasting of the muscles of the right arm and the skin of the hand and fingers was thin and shiny.
A private, 32, was admitted on April 15, 1916, to Tombleson’s ward from the Cottonera Mental Ward with the diagnosis: psychasthenia with weakness in the right arm. The man was very distrustful of doctors, sad, grumpy, and prone to crying. He had been kicked by a horse four years earlier and had a depressed and very sensitive scar on the right side of his head. Since that injury, the right side of his body had been getting weaker, but the arm was much weaker than the leg. Sensation was almost completely lost on the right side. The muscles in his right arm were wasting away, and the skin on his hand and fingers was thin and shiny.
Before his transfer the man was placed in the somnambulistic state, with suggestions of happiness and confidence in the coming cure. He arrived at Valletta, April 16, in a cheerful frame of mind, stating that there was nothing now the matter but weakness. Under somnambulism the loss of symptoms was suggested and, April 17, the patient was well except for the loss of power in the arm and leg. Daily training under somnambulism was given for a period of seven days, with suggestions especially leveled at the paretic muscles. He was then so far recovered that hypnotic treatment was stopped. The patient went to England, May 12, 1916, well.
Before his transfer, the man was put into a sleep-like state, with suggestions of happiness and confidence in the upcoming recovery. He arrived in Valletta on April 16, feeling cheerful and saying that he only felt weak. During his sleep-like state, it was suggested that his symptoms would go away, and by April 17, he was doing well except for some weakness in his arm and leg. He received daily training in this state for seven days, focusing specifically on the weak muscles. He improved so much that the hypnotic treatment was stopped. The patient went to England on May 12, 1916, feeling healthy.
Convulsions, “Jacksonian,” and dysbasia: Cure by hypnosis.
Convulsions, "Jacksonian," and trouble walking: Treatment through hypnosis.
Case 547. (Tombleson, September, 1917.)
A private, 18, was admitted to hospital, March 22, 1916, with the diagnosis Jacksonian epilepsy, with marked functional gait. He had just had several fits—two March 20, two March 21, and several earlier. He was tremulous and could not stand. Much pain. Knee-jerks brisk.
A private, 18, was admitted to the hospital on March 22, 1916, with a diagnosis of Jacksonian epilepsy and significant functional gait issues. He had just experienced several seizures—two on March 20, two on March 21, and several prior to that. He was shaky and unable to stand. He was in a lot of pain. His knee-jerk reflexes were brisk.
There was a history of a fall into a harbor at seven, followed by bleeding from nose and ears and unconsciousness for a week. Convulsions, involving the face, arm and leg, and attended by unconsciousness, kept recurring until twelve. Five months before admission there had been cerebrospinal meningitis. In February at Salonica he had had pneumonia.
There was a history of falling into a harbor at seven, followed by bleeding from the nose and ears and being unconscious for a week. Convulsions that affected the face, arm, and leg, and were accompanied by unconsciousness, kept happening until age twelve. Five months before being admitted, he had cerebrospinal meningitis. In February, he had pneumonia in Salonica.
March 23-24 the soldier was hypnotized to the third stage, but he had two fits. A “funny feeling in the right big toe” was brought out and suggested away. March 26-27 the patient was able to walk with a typical functional disorder. Under somnambulism the suggestions were repeated, but on the evening of March 27 two more convulsions appeared. In somnambulism he explained that he “had got round” the inhibition of the aura.
March 23-24, the soldier was hypnotized to the third stage, but he had two seizures. A “weird feeling in the right big toe” was brought up and suggested away. March 26-27, the patient was able to walk, though he had a typical functional disorder. While in a somnambulistic state, the suggestions were repeated, but on the evening of March 27, two more convulsions occurred. In his somnambulistic state, he explained that he “had gotten around” the inhibition of the aura.
The night of April 2 occurred two convulsions. April 5, the man was placed in the somnambulistic stage to last three days. During the night of April 6 he was observed to be restless for an hour, with some twitching of the right face, yet no fit followed. The morning of April 8 the patient woke feeling well. He was again placed in somnambulism to last two days. Two hours later, however, a fit started. It was stopped at once by suggestion, but the patient woke. He was left awake the rest of the day. April 9, somnambulism: suggestions repeated; sleep to last for two days. That evening there was a slight beginning of a fit, which was stopped at once by suggestion, the patient waking April 11 in another beginning of a fit, stopped by suggestion.
On the night of April 2, there were two seizures. On April 5, the man was put into a sleepwalking state that lasted for three days. During the night of April 6, he was restless for about an hour and had some twitching on the right side of his face, but he didn't have a seizure. By the morning of April 8, the patient woke up feeling fine. He was put back into a sleepwalking state for two days. However, two hours later, he started having a seizure. It was immediately stopped with suggestion, but the patient woke up. He stayed awake for the rest of that day. On April 9, he was placed back in sleepwalking: suggestions were repeated; the sleep was set to last for two days. That evening, a slight onset of a seizure began, which was quickly stopped by suggestion, and the patient woke up on April 11 during another onset of a seizure, which was also stopped by suggestion.
Thereafter no more fits recurred at all. May 12, 1916, well.
Thereafter, no more seizures occurred at all. May 12, 1916, good.
Agoraphobia: Cure by hypnosis.
Agoraphobia: Treated with hypnosis.
Case 548. (Hurst, 1917.)
A captain was (with one lieutenant) the sole survivor among his battalion officers at Ypres. The captain received the D. S. O. for his gallant conduct in saving the remnant of his battalion. He now felt he could never face responsibility again and that he would disgrace himself if he ever got into danger. He developed a terrible dread of open places and became more and more depressed. When he heard that there was going to be an attack at Neuve Chapelle, he broke down but managed to get through the first day of the battle. He was worse off than ever in the evening, felt that he could not face another day’s fighting, was invalided home, and arrived in a condition of exhaustion and feeling of disgrace. He had bad dreams at night. Rest was insufficient to restore confidence. Hypnosis was followed by rapid improvement, and the man was soon able to get back to duty.
A captain, along with one lieutenant, was the only survivor among his battalion officers at Ypres. He was awarded the D.S.O. for his brave actions in saving what was left of his battalion. He now felt he could never handle responsibility again and that he would shame himself if he ever faced danger again. He developed a terrible fear of open spaces and became increasingly depressed. When he learned there was going to be an attack at Neuve Chapelle, he broke down but managed to get through the first day of the battle. He felt worse than ever in the evening, convinced he couldn’t face another day of fighting, and was sent home, exhausted and feeling ashamed. He had bad dreams at night. Rest couldn’t restore his confidence. Hypnosis led to quick improvement, and he was soon able to return to duty.
Stress on Eastern front; cardiac seizures; cellulitis: In convalescence, manual tremors. Treatment eventually by forcing and isolation.
Stress on the Eastern front; heart attacks; cellulitis: In recovery, manual tremors. Treatment eventually through forced rest and isolation.
Case 549. (Binswanger, July, 1915.)
A subaltern officer, 24, in civil life a student of mathematics, had serious hereditary taint on both sides (father, alcoholic; maternal grandfather, victim of “severe nervous disease”). As a boy he developed normally, and was a good student. He served as volunteer in 1911 to 1912, but in drill in 1913 he had had to be released from service on account of nervous heart and difficulty with respiration.
A 24-year-old junior officer, who was a math student in civilian life, had a significant hereditary background of health issues on both sides (his father was an alcoholic, and his maternal grandfather suffered from a "severe nervous disease"). As a child, he developed normally and was an excellent student. He volunteered from 1911 to 1912, but during training in 1913, he had to be discharged due to a nervous heart condition and trouble breathing.
However, he was called to the colors at the outbreak of the war, and was subjected to tremendous strain in the eastern campaign; and he was put in the pack train at the end of November for cardiac seizures. He had a cellulitis with furunculosis following, and at the beginning of December there was suppuration of the whole right tibia. He was treated in hospital and slowly recovered.
However, he was drafted when the war started and faced immense strain during the eastern campaign; by the end of November, he was assigned to the supply train due to heart problems. He developed cellulitis and then a rash with boils, and at the beginning of December, there was pus buildup in his entire right tibia. He was treated in the hospital and gradually recovered.
At the beginning of March, 1915, without obvious external cause, while sitting in a café, the convalescent officer felt a cramp in his right hand, and strong movements of the hand to right and left followed. He was treated with bromides, but unsuccessfully. The tremors became more marked and then again from time to time grew weaker. Electric treatment increased the shaking to a maximal degree. April 27, the patient was brought to the nerve hospital at Jena.
At the start of March 1915, for no clear reason, while sitting in a café, the recovering officer felt a cramp in his right hand, and strong movements of the hand to the right and left followed. He was treated with bromides, but it didn’t work. The shaking became more pronounced and then occasionally lessened. Electric treatment made the shaking much worse. On April 27, the patient was taken to the nerve hospital in Jena.
The patient was a fat and muscular man, of average size, with very small ears and poorly-developed, adherent lobules, and syndactylism of the second and third toes of both feet; reflexes increased; marked dermatographia; a static fine tremor with rapid oscillations. The tremor became a positive tonus if the arm and hand were stretched out horizontally. Face and chest reddened easily.
The patient was a stocky and muscular man of average height, with very small ears and underdeveloped, attached earlobes, and webbing between the second and third toes on both feet; his reflexes were heightened; he had noticeable dermatographia; and a mild fine tremor with quick oscillations. The tremor turned into a strong tension when the arm and hand were extended horizontally. His face and chest flushed easily.
Whenever any other voluntary movement was carried out (even slight finger movements of the left hand or of the right or left foot while lying in bed) this right-sided convulsive[765] tremor immediately disappeared. The movements could also be made to disappear by slight turning movements of the head or of the tongue. Moreover, when the mind was diverted, as in reading, the tremors ceased. When the patient thought intensely of some mathematical problem, he could bring his shaking to a stop. The left grip was stronger than the right. In the Romberg position there was a marked swaying to the left and backwards.
Whenever any other voluntary movement was done (even slight finger movements of the left hand or the right hand or left foot while lying in bed), this right-sided convulsive tremor immediately disappeared. The tremors could also be made to stop by slight turning movements of the head or the tongue. Additionally, when the mind was distracted, such as when reading, the tremors ceased. When the patient concentrated intensely on a mathematical problem, he could stop the shaking. The grip with the left hand was stronger than the right. In the Romberg position, there was noticeable swaying to the left and backward.
Subjectively, the patient complained of nothing but a circumscribed headache in the left parietal region and of sleep interrupted by frightful dreams. At first the condition remained unchanged. There was much insomnia, and the slightest noise caused fright. Headaches in the daytime also were produced by any noise, and these headaches were localized in the left parietal region. The tremors of the right hand persisted except as he caused them to stop as above mentioned. He could write well with his left hand. He would drum with his left hand on the table until the tremor of his right hand disappeared. He could play on the piano, playing first with the left hand until the right had become quiet. He was a very irritable man, passing into anger and extreme profanity at the slightest occasion, and it was very difficult to bring him to any kind of orderly activity or persistence in therapeutic measures. These consisted of baths, massage, and gymnastics, but they proved quite unavailing.
Subjectively, the patient reported nothing but a specific headache in the left side of his head and sleep interrupted by terrifying dreams. Initially, his condition stayed the same. He experienced a lot of insomnia, and even the slightest noise startled him. Daytime headaches were also triggered by any sound, and these headaches were focused in the left side of his head. The tremors in his right hand continued, unless he managed to make them stop as mentioned earlier. He could write easily with his left hand. He would tap his left hand on the table until the tremors in his right hand faded away. He was able to play the piano, starting with his left hand until his right hand calmed down. He was a very irritable person, quickly becoming angry and using extreme profanity at the smallest provocation, and it was very challenging to get him to engage in any kind of structured activity or stick to therapeutic measures. These measures included baths, massage, and exercise, but they ended up being quite ineffective.
As the fellow got more and more intolerable, and as upon May 27 at about 9 o’clock in the evening, he disturbed the quiet of the entire hospital by a severe paroxysm of scolding, he was placed in a single room in the psychiatric department. He was placed in bed, cut off from all communication with others, and forced to carry out his exercises.
As the guy became more and more unbearable, and on May 27 at around 9 o’clock in the evening, he disrupted the entire hospital with a loud outburst of anger, he was put in a private room in the psychiatric department. He was put in bed, isolated from everyone, and required to do his exercises.
For two days he was surly, crabbed and obstinate, but then changed his demeanor completely; he became friendly and obedient. The tremor completely disappeared.
For two days, he was grumpy, moody, and stubborn, but then his attitude changed completely; he became friendly and compliant. The tension completely vanished.
Five days later he was able to carry out all active gymnastic exercises with great energy and without the slightest disturbance in the right arm. At date of report he was busy in the garden.
Five days later, he could perform all active gym exercises with great energy and without any issues in his right arm. As of the report, he was working in the garden.
Five weeks’ field service: Loss of speech. Cure by verbal and electric suggestion in three weeks.
Five weeks of field service: Loss of speech. Recovery through verbal and electric suggestion in three weeks.
Case 550. (Scholz, December, 1916.)
A grenadier, 21, of healthy stock, physique, and habits, lost his speech, April 15, 1916, five weeks after going into the field. May 5, examination showed him a well-nourished healthy man (lively reflexes and slight dermatographia), able to communicate only by signs and writing. The laryngoscope showed almost complete immobility of the two vocal cords, which lay in the cadaveric position, as in paralysis of the recurrent nerves. In endeavoring to pronounce the vowels ā and ee the cords trembled but failed to move toward each other. The patient’s effort to speak was such that his head soon got deep red and sweat streamed from the forehead.
A 21-year-old grenadier, in good health and shape, lost his ability to speak on April 15, 1916, just five weeks after being deployed. An examination on May 5 revealed he was a well-nourished, healthy man (with lively reflexes and slight skin sensitivity), who could only communicate through gestures and writing. The laryngoscope indicated that the two vocal cords were almost completely immobile, positioned like they were in a cadaver, similar to paralysis of the recurrent nerves. When he tried to pronounce the vowels "ā" and "ee," the cords trembled but did not move toward each other. His efforts to speak were so intense that his head turned deep red and sweat poured down his forehead.
Speech exercises were started by passing the electric current through the larynx during the processes of laryngoscopy. The patient was meantime assured that his larynx was healthy and that he would soon learn to speak again. At the first sitting, the patient felt himself able to cough aloud.
Speech exercises began with an electric current being passed through the larynx during laryngoscopy. The patient was reassured that his larynx was healthy and that he would soon be able to speak again. At the first session, the patient felt capable of coughing loudly.
After a few days, the patient was able to speak the separate vowels tolerably well, and was then made to go on with such words as Anna, Otto, Hurrah. The vocal cords began to move better. Fatigue was a feature of the first treatments, of such a degree that words that could be pronounced during the first part of the sitting were lost toward the close.
After a few days, the patient was able to pronounce the individual vowels fairly well and then was encouraged to proceed with words like Anna, Otto, and Hurrah. The vocal cords started to function better. Fatigue was a notable aspect of the initial treatments, to the extent that words that could be spoken at the beginning of the session were forgotten by the end.
The grenadier assiduously set himself to say over and over again the words that he had learned, and would come to the sister radiant with joy at his success. In ten days he was able to speak again perfectly, though giving the impression of a slight stuttering. After three weeks hospital stay he was discharged cured and fit for service.
The grenadier diligently repeated the words he had learned and would come to the sister beaming with joy at his success. In ten days, he was able to speak perfectly again, although he had a slight stutter. After three weeks in the hospital, he was discharged, cured and ready for service.
Struck by a rifle butt on right side of head; old wound of right thigh: Hysterical right hemiplegia and deafmutism. Treatment by faradization: Return of speech and improvement of hearing. Full recovery by suggestion. Hysterical CONVULSIONS developed BY HETEROSUGGESTION from convulsive neighbor.
Struck on the right side of the head with a rifle butt; old wound on the right thigh: Hysterical paralysis on the right side and deafness. Treated with faradization: Speech returned and hearing improved. Full recovery through suggestion. Hysterical convulsions developed from suggestion by a convulsing neighbor.
Case 551. (Arinstein, 1915.)
A Russian corporal, 21, was knocked unconscious, September 13, 1915, by a butt of a rifle which struck the right side of his head. He came to in a short time. He was examined in hospital, early in October, and besides a small skin wound of the head, there was evidence of a wound on the anterior aspect of the thigh. There was paralysis of both right arm and right leg, and anesthesia of the entire right side of the body, face and even of the tongue. There were also pains over the whole right side of the body. The abdominal reflexes were present on both sides; the tendon reflexes were in excess on the hemiplegic side; there were no pathological reflexes of any sort. The patient’s hearing was diminished, and he could not speak at all although he could understand the speech of others perfectly.
A 21-year-old Russian corporal was knocked out on September 13, 1915, when a rifle butt hit the right side of his head. He regained consciousness shortly after. He was examined in the hospital in early October, and apart from a small skin wound on his head, there was evidence of a wound on the front of his thigh. He experienced paralysis in both his right arm and right leg, along with numbness on his entire right side, including his face and tongue. He also had pain all over his right side. The abdominal reflexes were normal on both sides, while the tendon reflexes were heightened on the paralyzed side; there were no abnormal reflexes. The patient had reduced hearing and was completely unable to speak, though he could understand others perfectly.
Speech returned after a single séance of suggestion with faradism to the throat. Hearing began to improve. The patient’s suggestibility was a favorable factor in his cure, but there were some unfavorable features. One day, he saw a neighbor go into convulsions and proceeded to develop convulsions himself. These hysterical convulsions continued. According to Arinstein, such undesirable complications appear under conditions of extreme crowding of hospital patients suffering from shell-shock. Progressive séances of psychotherapy caused the disappearance of all the signs of paralysis, and at the time of the report, there was no disability, except that the full use of the hand had not yet been regained.
Speech returned after just one session of suggestion with faradism to the throat. Hearing began to improve. The patient’s suggestibility was a positive factor in his recovery, but there were some negative aspects. One day, he witnessed a neighbor have convulsions and then began to have convulsions himself. These hysterical convulsions continued. According to Arinstein, such unwanted complications occur in situations where there is severe overcrowding of hospital patients dealing with shell shock. Continued sessions of psychotherapy resulted in the disappearance of all signs of paralysis, and by the time of the report, there was no disability, except that the full use of the hand had not yet been regained.
Shell-shock and burial; labyrinthine disease on one side: DEAFMUTISM. Cures, relapses and eventual cure by general anesthesia, more than four months after shock.
Shell shock and burial; a complicated illness on one side: DEAFMUTISM. Treatments, setbacks, and eventual recovery through general anesthesia, more than four months after the shock.
Case 552. (Dawson, February, 1916.)
A private, 30, had been 12 years in the service. July 8, 1915, he was partially buried by a shell which killed two companions.
A private, 30, had been in the service for 12 years. On July 8, 1915, he was partially buried by a shell that killed two of his companions.
On admission to hospital he spoke a few sentences but was deaf, and next morning could neither speak nor read, nor did he take food for 36 hours thereafter.
On being admitted to the hospital, he managed to say a few sentences, but he was deaf. The next morning, he couldn't speak or read, and he also didn't eat for 36 hours after that.
Admitted to the King George Hospital, July 18, he was found stuporous, but started violently if touched, made signs indicating his wants, took no interest in surroundings, and resisted efforts to arouse him. He was without signs of organic disease. It seems that he had been a nervous child, with nightmares and fits.
Admitted to King George Hospital on July 18, he was found in a stupor but would startle violently when touched, gestured to indicate his needs, showed no interest in his surroundings, and resisted attempts to wake him up. There were no signs of any organic disease. It appears that he had been a nervous child, experiencing nightmares and seizures.
July 24, he was given gas for dental extraction, partly in the hope that he would recover speech; but though he struggled violently, he made no sound. He had by this time become rather intelligent in a childlike manner, being pleased to see his small boy, but taking no notice of his wife. It transpired afterward that he did not recognize her.
July 24, he was given gas for a dental extraction, partly hoping it would help him regain his speech; but even though he fought hard, he couldn't make a sound. By this point, he had become somewhat aware in a childlike way, happy to see his little boy but completely ignoring his wife. It later turned out that he didn't recognize her.
Phonation in whisper now began. There was then a relapse, and for a week or more no food was taken. Such relapses with irritation and hypobulia and an obstinate constipation recurred; but improvement came on slowly. He became able to read short printed words, and later handwriting.
Phonation in whisper began now. Then there was a setback, and for a week or more no food was eaten. These setbacks, along with agitation, lack of motivation, and stubborn constipation, kept happening; but progress came slowly. He became able to read short printed words and later handwriting.
For another month there was no improvement and he lost heart and the will to get well, brightening up only when offered a motor drive or something else pleasant. He was transferred to an auxiliary hospital, against his will, September 18.
For another month, there was no improvement, and he lost hope and the motivation to get better, only showing some joy when offered a motor drive or something enjoyable. He was transferred to an auxiliary hospital, against his will, on September 18.
November 1, he was brought back to the King George Hospital, excited, shouting, struggling and evidently drunk. On[769] a day’s leave from the convalescent hospital he had come up to London, and in alcoholic elation began to laugh and talk. Morphia did not reduce his violence. He insisted on seeing the physician, to tell him the good news. Hearing was still diminished, though if attention were diverted, direct answers were given to some questions. Sleep followed.
November 1, he was brought back to King George Hospital, excited, shouting, struggling, and clearly drunk. On[769] a day off from the recovery hospital, he had come up to London, and in a drunken high, he started laughing and talking. Morphine didn’t calm him down. He insisted on seeing the doctor to share the good news. His hearing was still limited, but if he was distracted, he answered some questions directly. Then he fell asleep.
The next day he spoke perfectly but could hear nothing. There was no further progress for three weeks, though he occasionally caught sounds. He now became bright and pleasant and had lost all irritability and sulkiness. Galvanic and faradic current had no effect on the ears.
The next day he spoke clearly but couldn’t hear anything. There was no further progress for three weeks, although he occasionally picked up on sounds. He became cheerful and friendly, having lost all irritability and moodiness. Galvanic and faradic currents had no impact on his hearing.
November 27, after elaborate preparation to heighten the suggestive effect, the patient was kept in bed and given gas and ether up to the abolition of the corneal reflex. As he was coming round, the doctor shouted that he could now hear well. He was overcome with joy and had hysterical convulsions. He could hear, but with the right ear only. In point of fact, the left ear on examination showed signs of labyrinthine deafness. He was placed on home service.
November 27, after thorough preparation to enhance the suggestive effect, the patient was kept in bed and was given gas and ether until the corneal reflex was completely gone. As he started to regain consciousness, the doctor shouted that he could now hear well. He was filled with joy and had hysterical convulsions. He could hear, but only with his right ear. In fact, an examination of the left ear showed signs of labyrinthine deafness. He was put on home service.
Re etherization for functional deafness and mutism, Ninian Bruce maintains that ether is more satisfactory than chloroform. The loss of consciousness in cases of deafness and mutism ought to be a relatively slight one, and the patient should be suddenly roused to the realization that he is speaking. Recovery from chloroform anesthesia is, according to Ninian Bruce, too slow to allow the patient to catch the point that he is now speaking and hearing when he was formerly dumb or deaf. A failure with the method is a bad thing for the patient, as he loses confidence in the method, whereupon some other method must be resorted to.
Re etherization for functional deafness and mutism, Ninian Bruce asserts that ether works better than chloroform. The loss of consciousness in cases of deafness and mutism should be minimal, and the patient should be quickly brought back to the realization that they are speaking. Recovery from chloroform anesthesia is, according to Ninian Bruce, too slow for the patient to notice that they are now speaking and hearing after being unable to before. A failure of this method can be detrimental for the patient, as it diminishes their confidence in the approach, leading to the need for an alternative method.
Re etherization for deafmutism, see technic of Ninian Bruce under Case 553. Penhallow has a case in which during primary etherization the patient reviewed in a loud voice the whole story of his speech loss. He was found to have recovered speech and hearing after coming out of ether.
Re etherization for deafmutism, see the technique of Ninian Bruce under Case 553. Penhallow has a case where, during primary etherization, the patient loudly recounted the entire story of his speech loss. It was found that he had regained both speech and hearing after coming out of ether.
Re anesthesia by gas, Abrahams has used nitrous oxide for cure of hysterical paraplegia. Proctor also reports the use of light ether anesthesia for bringing out the voice of functional mutes.
Re anesthesia by gas, Abrahams has used nitrous oxide to treat hysterical paraplegia. Proctor also mentions using light ether anesthesia to help functional mutes speak.
Shell-shock functional deafness (five months). Yes-No test. Cure by suggestion on emerging from ether anesthesia.
Shell-shock functional deafness (five months). Yes-No test. Treatment through suggestion after waking from ether anesthesia.
Case 553. (Bruce, May, 1916.)
A soldier was admitted to the Royal Victoria Hospital, Edinburgh, completely deaf in the left ear. He had been under shell fire a number of times in France and was eventually thrown down and made unconscious by a shell explosion on his left. He did not remember the noise of the explosion or anything until he found himself in hospital. After the explosion he had begun to stutter, and the stuttering had grown worse. Examination of the ear indicated that the deafness was functional. He was given ether and when just under was asked if he could hear anything spoken in his right ear. He said, “Yes.” With the right ear closed he was asked if he could hear when his left ear was spoken into. He said, “No.” This test was repeated several times. After covering his right ear, he gave his name, regiment, etc., in reply to questions whispered into his left (previously deaf) ear. The incongruity was pointed out. He was now suddenly wakened. He laughed hysterically with joy over his recovery.
A soldier was admitted to the Royal Victoria Hospital, Edinburgh, completely deaf in his left ear. He had been under shell fire several times in France and was eventually thrown down and knocked unconscious by a shell explosion on his left. He couldn’t remember the sound of the explosion or anything until he found himself in the hospital. After the explosion, he started to stutter, and the stuttering had gotten worse. An examination of the ear showed that the deafness was functional. He was given ether, and while just under, he was asked if he could hear anything spoken into his right ear. He said, “Yes.” With his right ear covered, he was asked if he could hear when someone spoke into his left (previously deaf) ear. He said, “No.” This test was repeated several times. After covering his right ear, he gave his name, regiment, etc., in response to questions whispered into his left ear. The contradiction was pointed out. He was suddenly woken up. He laughed hysterically with joy over his recovery.
But the next morning he was again stone deaf in the left ear. Blistering and electricity failed to produce benefit. He was, however, puzzled about himself.
But the next morning he was once again completely deaf in his left ear. Blistering and electrical treatments didn't help at all. He was, however, confused about what was going on with himself.
After a fortnight he was again given ether and a little chloroform was added. The yes-no test was again positive. He was allowed to recover gradually from the chloroform, but he had now lost recollection of what had happened. The left ear remained deaf. Ether was again given. He was asked to close his right ear with his finger. While answering questions addressed to his left ear, he was suddenly awakened and immediately said that his hearing had come back. This return proved permanent. He returned to his dépôt. In the conversations under ether there was no stuttering. He had been totally deaf in the left ear for five months.
After two weeks, he was given ether again, with a bit of chloroform added. The yes-no test was positive once more. He was allowed to slowly recover from the chloroform, but he had lost any memory of what had happened. His left ear remained deaf. Ether was administered again. He was instructed to close his right ear with his finger. While answering questions directed to his left ear, he was suddenly startled awake and immediately stated that his hearing had returned. This improvement turned out to be permanent. He went back to his station. During the conversations while under ether, there was no stuttering. He had been completely deaf in his left ear for five months.
Blow in neck by rifle butt: aphasia, right hemiplegia and hemianesthesia, and especially (here MEDICAL suggestion) trismus: Recovery by anesthetic and suggestion.
Blow to the neck from a rifle butt: loss of speech, paralysis on the right side, and lack of sensation on the right side, and especially (here MEDICAL suggestion) jaw lock: Recovery through anesthesia and suggestion.
Case 554. (Arinstein, September, 1915.)
A Russian soldier was struck in the head and neck by a rifle butt, and developed paralysis of right arm and leg with loss of speech. After the excitement experienced by the patient when exhibited to the students by the late Prof. M. N. Szukowsky in the neurological clinic of the Military Medical Academy, trismus developed.
A Russian soldier was hit in the head and neck by a rifle butt and ended up with paralysis in his right arm and leg along with losing his ability to speak. After the excitement he experienced when presented to the students by the late Prof. M. N. Szukowsky in the neurological clinic of the Military Medical Academy, he developed trismus.
The patient spent a year in various hospitals, the most diverse methods of treatment by drug therapy, electricity, and suggestion yielding no results. The patient had to be fed chiefly by nose and rectum, though small quantities of fluids were fed through the mouth through an opening formed by the falling out of one tooth in the upper jaw. The patient became greatly emaciated and weak and was, October 29, 1915, brought into the nervous wards of the hospital.
The patient spent a year in different hospitals, undergoing various treatment methods like medication, electrical therapy, and suggestion, but nothing worked. The patient had to be fed mainly through a tube in the nose and rectum, although small amounts of fluids were given through the mouth via an opening created by a lost upper tooth. The patient became very thin and weak and was admitted to the nervous wards of the hospital on October 29, 1915.
He showed flaccid paralysis of left arm and leg, together with anesthesia, analgesia and thermanesthesia over the whole left side of the head, extreme general atrophy of muscles, somewhat more marked on the palsied side. The temperature of the paralyzed half of the body was not lowered. No knee or Achilles reflex obtained upon either the affected or the healthy side (general exhaustion?). Abdominal and testicular reflexes lively. The pupils responded well to light. Corneal reflexes lively. The neck was held awry to the left, and the head was inclined somewhat downwards and leftwards; hearing on left side impaired. The jaws could not be opened even with the greatest effort. Wassermann reaction negative.
He displayed weakness and lack of movement in his left arm and leg, along with loss of sensation, pain relief, and temperature sensitivity on the entire left side of his head. There was significant muscle wasting, more pronounced on the affected side. The temperature on the paralyzed side of the body wasn’t reduced. There was no knee or Achilles reflex detected on either the affected or healthy side (possibly due to overall fatigue?). The abdominal and testicular reflexes were active. The pupils reacted well to light. Corneal reflexes were active. His neck was tilted to the left, and his head was slightly bent downwards and to the left; hearing was impaired on the left side. He was unable to open his jaws even with great effort. The Wassermann test was negative.
Patient thought himself incurable. Purves Stewart’s case, in which chloroform and oxide of nitrogen were used, was the basis of Arinstein’s treatment. It was suggested to the patient that he submit to narcosis with the proviso that he[772] would not be operated upon. His consent was secured; with the coöperation of others, the chloroform was administered November 6. The stage of excitability was not well marked. 8 gr. of chloroform was used altogether, by the drop system. Nevertheless, even with the weak initial excitability, the patient became capable of some movements with paralyzed hand and foot. On opening mouth, the patient yawned yet uttered no sound. Between the jaws was put a rubber insertion and upon awakening the patient was let see with his own eyes that his jaws were open and that therefore food might be introduced through the mouth. Upon repetition of the narcosis, 5 gr. of chloroform was used altogether, and the stage of excitability was this time better marked. To strengthen movements in the paralyzed extremities, the device of pricking the patient with a pin on the unaffected half of the body, with the unaffected hand and leg held horizontal by assistants, was adopted. The patient then made reflex defensive movements in the paralyzed extremities, especially the hand. At this point the narcosis was suspended, and the irritation with the pin was continued until consciousness returned. At this moment, the patient’s attention was called to the disappearance of the paralysis and his restored ability to move the paralyzed extremities.
The patient believed he was incurable. Purves Stewart’s case, which involved the use of chloroform and nitrous oxide, served as the foundation for Arinstein’s treatment. It was suggested to the patient that he undergo narcosis on the condition that he would not be operated on. He agreed; with the help of others, the chloroform was administered on November 6. The stage of excitability was not very pronounced. A total of 8 grams of chloroform was used with a drop method. However, even with the weak initial excitability, the patient was able to make some movements with his paralyzed hand and foot. When his mouth was opened, the patient yawned but didn’t make any sounds. A rubber insertion was placed between his jaws, and upon waking, the patient was shown that his jaws were open and that food could be introduced through his mouth. During a repeat of the narcosis, a total of 5 grams of chloroform was used, and this time the stage of excitability was more noticeable. To encourage movement in the paralyzed limbs, the method of pricking the patient with a pin on the unaffected side of the body was used, while assistants held the unaffected hand and leg horizontal. The patient then made reflexive defensive movements in the paralyzed limbs, especially the hand. At this point, the narcosis was paused, and the pin irritation continued until he regained consciousness. At that moment, the patient was made aware of the disappearance of the paralysis and his regained ability to move the previously paralyzed limbs.
From that time on, the patient’s condition underwent a sharp transition. Artificial feeding became unnecessary. The patient ate by mouth; the mouth was opened by the leverage of a small stick held by the patient between his teeth. Speech returned gradually. In reading aloud the patient aided the movements of his lips with his hands. At the time of report the patient spoke well, ate normally, had gained in weight, and with some effort could sit down and even stand and walk. All this was attained in a relatively short time after a whole year of paralysis.
From that point on, the patient's condition changed dramatically. Artificial feeding was no longer needed. The patient started eating by mouth; his mouth was opened using a small stick that he held between his teeth. Speech returned gradually. While reading aloud, the patient helped move his lips with his hands. At the time of the report, the patient spoke fluently, ate normally, had gained weight, and with some effort could sit down and even stand and walk. All of this was achieved in a relatively short time after a whole year of paralysis.
The author felt that the success attained in this case gave him the right to use the same method where the cause was not a contusion.
The author believed that the success achieved in this case granted him the privilege to apply the same method even when the cause wasn't a bruise.
Ten months’ field service; severe FEBRILE DISEASE: Afterward hysterical TRIPLEGIA, MUTISM, “JUMPING-JACK” reactions to stimulation of feet. Cure by anesthesia, verbal suggestion, faradism to palate.
Ten months of field service; serious fever illness: Later hysterical triplegia, mutism, “Jumping-jack” reactions to stimulation of feet. Treatment with anesthesia, verbal suggestion, faradism to the palate.
Case 555. (Arinstein, September, 1915.)
A Russian private, 30, brought to a field reserve hospital, June 20, 1915, was in a grave condition diagnosed typhoid. By the end of June the general condition had improved and the temperature had fallen.
A 30-year-old Russian private was taken to a field reserve hospital on June 20, 1915, in serious condition with a diagnosis of typhoid. By the end of June, his overall condition had improved and his temperature had dropped.
July 9, worse; happening to be in the company of a sanitary in a privy, he was observed suddenly to fall unconscious, with both feet and left arm paralyzed. Soon afterward he lost the power of speech. From September 30 to October 19, he lay in field hospital; but was then transferred to the nerve hospital with diagnosis: convulsive paralysis and aphasia. At entrance, complete paralysis of both legs and left hand; loss of speech and aphonia (speech understood). Upon touching a foot, strong convulsions developed with legs rapidly drawn apart and drawn together much in the manner of dancing toys. The mouth was twisted to the left. Though he silently opened his mouth and made rapid movements with the lower jaw, he could not utter a single sound, either vowel or consonant. Left hypalgesia. Hypesthesia of skin of hand and mucosa of tongue. Knee-jerks absent because of the strain of the muscles of the legs. Wassermann negative.
July 9, things got worse; while he was with a sanitary officer in a restroom, he suddenly collapsed, with both legs and his left arm paralyzed. Shortly after, he lost the ability to speak. From September 30 to October 19, he was in a field hospital, but then he was moved to a nerve hospital with a diagnosis of convulsive paralysis and aphasia. Upon admission, he had complete paralysis of both legs and his left hand; he had lost the ability to speak and could only understand speech. When his foot was touched, he experienced strong convulsions, with his legs moving apart and together like dancing toys. His mouth was twisted to the left. Although he opened his mouth silently and moved his lower jaw quickly, he couldn’t make a single sound, neither vowels nor consonants. He had reduced sensitivity on the left side. There was diminished sensation in the skin of his hand and the mucosa of his tongue. Knee-jerk reflexes were absent due to muscle strain in his legs. Wassermann test was negative.
The history showed that the speech of the patient had been incorrect and indistinct from childhood. Moreover, in 1908, in chopping wood in the forest he had fallen under a sleigh and hurt his left hand, which had not since fully recovered. He had volunteered for the war.
The history showed that the patient's speech had been incorrect and unclear since childhood. Moreover, in 1908, while chopping wood in the forest, he had fallen under a sleigh and injured his left hand, which had never fully healed. He had volunteered for the war.
The psychogenic character of the disease seemed clear. Suggestion was followed by ether narcosis, during which, on pricks of the healthy side with a pin, the patient made defensive movements with the paralyzed hands, and also[774] moved both legs. Speech was not regained either during or immediately after the narcosis, although the patient gave forth indefinite sounds. Speech was restored on the same day, September 7, with verbal suggestion and faradic brush applied to palate. The patient at once began to speak clearly and distinctly, read his prayer book, and described distinctly and in detail how he went to war. From that moment the convulsive movements in the feet disappeared, the region of anesthesia on the left side narrowed, speech was permanently reëstablished, and the patient began to move with his feet and finally began to walk after six months of paralysis. Before that time no medical treatment had had the slightest effect. The effort to stop mechanically the jerks even temporarily by means of plaster casts had been unsuccessful. In sleep the twitches ceased, but upon reawakening, even before full consciousness returned, the jerkings would resume. It is curious to note that upon falling asleep under the anesthetic the patient would issue always one and same kind of yells—“Help, there goes the German! They are shooting! Russians, do not yield!”
The psychological nature of the disease was evident. After suggestion, the patient was put under ether anesthesia. While they pricked the healthy side with a pin, the patient showed defensive movements with the paralyzed hands and also[774] moved both legs. Speech didn't return during or right after the anesthesia, though the patient made indistinct sounds. Speech was restored later that same day, September 7, through verbal suggestion and a faradic brush applied to the palate. The patient immediately began to speak clearly, read from their prayer book, and vividly described their experiences in the war. From that point on, the jerky movements in the feet vanished, the numb area on the left side reduced, speech was permanently restored, and the patient started to move their feet and eventually walked again after six months of paralysis. Until that moment, no medical treatment had any effect. Attempts to stop the jerks mechanically with plaster casts had failed. The twitches stopped during sleep, but resumed upon waking, even before full awareness returned. Interestingly, when falling asleep under anesthesia, the patient consistently yelled the same phrases—“Help, there goes the German! They are shooting! Russians, do not yield!”
Re chloroform anesthesia, Milligan remarks that the treatment should be carried out in a quiet, single room, with the chloroform slowly administered and the suggestions made by the anesthetist during the optimal phase for suggestion,—just before the stage of involuntary struggling.
Re chloroform anesthesia, Milligan notes that the procedure should take place in a calm, private room, with the chloroform administered gradually and the anesthetist providing suggestions during the best time for influence—right before the stage of involuntary struggling.
Shell-shock; unconsciousness: Mutism and musical alexia. Cure by anesthesia.
Shell shock; unconsciousness: Mutism and musical alexia. Treated with anesthesia.
Case 556. (Proctor, October, 1915.)
A private, 23, was admitted to the Duchess of Connaught’s Hospital at Taplow from Gallipoli, September 10, 1915. A shell had exploded behind this man. He had been picked up, unconscious, and remained so about a day. He recovered without the power of speech. Cerebration was slow at first but improved steadily.
A private, 23, was admitted to the Duchess of Connaught’s Hospital in Taplow from Gallipoli on September 10, 1915. A shell had exploded behind him. He was found unconscious and stayed that way for about a day. He recovered but was unable to speak. His thinking was slow at first but steadily got better.
The man had been a professional musician. Curiously enough, though his ability to read ordinary print was as good as ever, his reading of music was lost with the speech.
The man had been a professional musician. Interestingly, even though his ability to read regular print was just as good as always, he had lost his ability to read music along with his speech.
September 20, he was etherized, but being of a phlegmatic type, he was not readily excited and took the anesthesia very quietly. After perseverance, however, he was induced to talk. The ability to read music returned with the voice. He was discharged, October 4, 1915.
September 20, he was put under anesthesia, but since he was pretty calm by nature, he didn't get too worked up and handled the anesthesia well. After some persistence, though, he started to open up and talk. He found that he could read music again once he started speaking. He was released on October 4, 1915.
Re the use of anesthetics for curing deafmutism, Colin Russel rather disapproves of this method on the ground that no attempt is made to get at the genuine pathogenesis of the case and that accordingly there may be a tendency to recurrence.
Re the use of anesthetics for treating deafmutism, Colin Russel disapproves of this method because it doesn’t address the actual underlying cause of the condition, which could lead to it coming back.
Re the peculiar musical alexia, see discussion under Cases 353 and 450 of confusion and amnesia. The most highly selective amnesias have been found in confusional cases. However, Case 556 had been a professional musician and the effect may have been a highly specialized suggestion. See also Case 369 of Feiling for differentiated musical disorder. Mott has used the retained knowledge of tones as an avenue of approach in certain mute cases.
Re the unusual musical alexia, refer to the discussion under Cases 353 and 450 regarding confusion and amnesia. The most selective amnesias have been observed in confusional cases. However, Case 556 was a professional musician, and the effect might have been a very specialized suggestion. Also, see Case 369 of Feiling for differentiated musical disorder. Mott has utilized the retained knowledge of tones as a way to approach certain mute cases.
Shell-shock; burial (24 hours?); unconsciousness, 13 days: Deafmutism. Chloroform narcosis cured the deafness (!), not the mutism.
Shell shock; burial (24 hours?); unconsciousness, 13 days: deaf-mute. Chloroform anesthesia cured the deafness (!), but not the mutism.
Case 557. (Gradenigo, March, 1917.)
An Italian infantryman was buried under Mt. Zebio after shell explosion. After 24 hours he was found and dug out. He remained unconscious for 13 days and came out absolutely deaf and mute.
An Italian soldier was buried under Mt. Zebio after a shell exploded. After 24 hours, he was located and rescued. He stayed unconscious for 13 days and emerged completely deaf and mute.
At hospital he was markedly depressed and cried very readily on being spoken to. The tympanic membrane had lost its sensitiveness to pain. As for the speech mechanism, the larynx proved negative. All the movements of the soft palate, tongue and vocal cords could be normally performed. The tongue was anesthetic to touch, but the taste function was perfectly preserved. The cheeks and various parts of the face were also anesthetic to touch, and the lobules of the ears could even be pierced with large pins without reaction by the patient.
At the hospital, he was clearly depressed and would start crying easily when someone talked to him. The eardrum had lost its sensitivity to pain. Regarding his speech mechanism, the larynx showed no issues. All the movements of the soft palate, tongue, and vocal cords worked normally. The tongue was numb to touch, but he could still taste things perfectly. The cheeks and different areas of his face were also numb to touch, and even large pins could be pushed through the earlobes without him reacting.
He tried to pronounce labials, opening and closing the lips rapidly; but the expiratory movement was too weak, and not a single sound was made.
He attempted to pronounce labials, quickly opening and closing his lips; but his breath was too weak, and not a single sound came out.
At the patient’s request, he was chloroformed. During a very violent excited phase, he did emit groaning sounds. The narcosis, however, did not put an entire stop to the mutism, since only a few inarticulate sounds could be emitted, and those only after great efforts. Curiously enough, however, the chloroform narcosis had caused the deafness to disappear entirely. Another narcosis upon the patient’s insistent request was given but remained without results, and at the time of report, the patient though cheerful and intelligent-looking, was still mute.
At the patient’s request, he was given chloroform. During a very intense, agitated phase, he made groaning sounds. However, the sedation didn’t completely stop the mutism, as he could only produce a few inarticulate sounds, and those required a lot of effort. Interestingly, though, the chloroform sedation completely removed the deafness. Another sedation was administered at the patient’s strong request, but it had no effect, and at the time of the report, the patient, although looking cheerful and intelligent, was still mute.
Cases 558 and 559. (Smyly, April, 1917.)
A soldier was out with a bombing party when a shell burst. He came to in a casualty clearing station, and was sent on to Salonica, deaf, dumb and jumpy. Two months later, an attempt at hypnosis failed; faradism of vocal cords failed.
A soldier was out with a bombing crew when a shell exploded. He regained consciousness in a casualty clearing station and was sent on to Salonica, deaf, mute, and jittery. Two months later, an attempt at hypnosis didn't work; electrical stimulation of the vocal cords didn't succeed either.
The patient dreamed one night that if he vomited he could speak. Ipecac produced vomiting without speech. The patient, however, wanted a second dose, and while waiting for it, uttered an exclamation, which he did not himself hear, however. In the meantime, Dr. Smyly had been trying to hypnotize a second soldier, dumb but not deaf. This man’s dug-out had been blown in on him seven months before, whereupon the patient became very shaky, but did not become sick for a week. He was then sent to hospital, and his voice gradually disappeared. He suffered from violent headache and spasmodic movements of the arms and legs. Suggestion seemed powerless, and ether was unexpectedly given to the patient. While going under the ether, he said, “Oh dear, oh dear” several times indistinctly. It seems that another physician had already tried to cure the patient of dumbness by removing teeth without an anesthetic.
The patient dreamed one night that if he vomited, he would be able to speak. Ipecac made him throw up but didn’t help him talk. Nevertheless, the patient wanted a second dose, and while waiting, he exclaimed something he didn’t hear himself. Meanwhile, Dr. Smyly was attempting to hypnotize a second soldier, who was mute but not deaf. This soldier’s dugout had collapsed on him seven months earlier, which made him very shaky, but he didn’t feel sick for a week. He was then sent to the hospital, and his voice slowly faded away. He experienced intense headaches and involuntary movements in his arms and legs. Suggestions didn’t seem to work, and unexpectedly, ether was administered to the patient. As he was going under the ether, he muttered, “Oh dear, oh dear,” several times indistinctly. It appears that another doctor had already tried to treat the patient’s muteness by extracting teeth without anesthesia.
While this therapy was proceeding with the dumb man, the deaf-and-dumb man disappeared. It seems that the smell of the gas had caused him to take refuge on an outhouse-roof. The next day he had recovered voice and hearing completely, partly from shock and partly through suggestion.
While this therapy was going on with the mute man, the deaf-mute man vanished. It appears that the smell of the gas made him take shelter on a roof of an outhouse. The following day, he had fully regained his voice and hearing, partly due to shock and partly through suggestion.
The etherized patient did not recover voice but lost the spasmodic movements and his insomnia. A week later ether was again administered, and the patient was strapped down; as he was coming to, faradism was applied to the head and face. The patient then quickly recovered his voice and still retains it.
The patient who was under ether anesthesia didn't regain his voice but stopped the involuntary movements and his insomnia. A week later, ether was administered again, and the patient was strapped down; as he was waking up, electrical stimulation was applied to his head and face. The patient then quickly regained his voice and continues to have it.
Shell wound: Hysterical dysbasia from contracture. Many methods of treatment fail. Success with “a new measure,” e.g. stovaine.
Shell wound: Hysterical dysbasia from contracture. Many treatment methods fail. Success with “a new measure,” e.g. stovaine.
Case 560. (Claude, March, 1917.)
A sergeant was struck in the suprapubic region, December 15, 1915, by a shell fragment and got a large hematoma in the perineal region (shell fragment visible on X-ray). The man was treated a year in a center for physiotherapy and was then treated in a neurological center, where a faulty position of the right thigh maintained in extensor rotation and abduction was found. The patient walked on crutches, legs wide apart, balancing with body.
A sergeant was hit in the lower abdomen on December 15, 1915, by a shell fragment and developed a large hematoma in the perineal area (shell fragment visible on X-ray). He received treatment for a year at a physiotherapy center and was then treated at a neurological center, where it was found that his right thigh was in a faulty position, kept in an extended rotation and abduction. The patient walked on crutches, with his legs wide apart, balancing his body.
Upon transfer to Bourges, an intraspinal injection of stovaine (after withdrawal of 2-3 cc. fluid, 1 cc. stovaine, 0.07 to the cc., mixed with cerebrospinal fluid) was made. This reduced the contracture and permitted the patient to place his legs parallel. They were then bandaged in the parallel position. The bandages were removed two days later and the limbs did not reassume their faulty position. The man was shortly able to walk with a cane; progress was rapid. This man was very desirous of cure and refused to be invalided, believing he was to be cured, and had received medal and war cross. Simple motor reëducation in competent hands had been without effect. A new kind of measure, such as stovaine, proved successful.
Upon being transferred to Bourges, an intraspinal injection of stovaine (after removing 2-3 cc. of fluid, 1 cc. of stovaine, 0.07 per cc., mixed with cerebrospinal fluid) was administered. This eased the contracture and allowed the patient to place his legs parallel. They were then bandaged in that position. The bandages were taken off two days later, and the limbs didn’t revert to their incorrect position. The man was soon able to walk with a cane; progress was quick. He was very eager to recover and refused to be classified as an invalid, believing he would be cured and had received a medal and a war cross. Basic motor re-education in skilled hands had been ineffective. A new treatment, like stovaine, proved successful.
Burial: Hysterical dysbasia. Treatment by stovaine anesthesia.
Burial: Hysterical dysbasia. Treatment with stovaine anesthesia.
Case 561. (Claude, March, 1917.)
A chasseur, buried June 24, 1916, had a number of general symptoms, apparently got well and was given seven days’ leave at home. On the way he felt abdominal pain which he thought due to the jolting of the car. Suddenly he felt his legs trembling on extension. He left the train and went into a hospital where a diagnosis of radicular and spinal lesions was made. Two months later he was sent to Claude who found that he could walk only with knees flexed. If he was requested to stand up and extend his legs on the thigh, a trembling set in suggestive of an epileptoid trepidation. Even in the horizontal position the same clonic trepidation occurred which only stopped if the patient flexed his legs on the thighs.
A soldier, buried on June 24, 1916, had several general symptoms, seemed to recover, and was granted a week’s leave at home. On the way, he experienced abdominal pain, which he thought was due to the jolting of the car. Suddenly, he felt his legs shaking when he tried to extend them. He got off the train and went to a hospital where they diagnosed him with radicular and spinal issues. Two months later, he was sent to Claude, who found that he could only walk with his knees bent. When asked to stand up and straighten his legs, he started shaking in a way that resembled an epileptic tremor. Even when lying down, the same clonic shaking happened, which only stopped when the patient bent his legs at the hips.
However, no sign of organic lesion could be found. There was an analgesia limited to the ankles. Psycho-physiotherapeutic treatment was unavailing. January 28, 1917, the stovaine injection method was tried. After anesthesia had set in, it was found possible still to produce the spastic state by extending the legs; but a half hour after injection the spastic state could no longer be produced. The patient was shown that the trepidation was abolished. During the period of return of sensibility, the legs were constantly moved and the patient constantly told to make movements himself. He was convinced of his power. There was no longer any clonus. The patient remained all day in bed without epileptiform movements. Next day he complained merely of weakness in the legs and was got to walk without having convulsive tremors. During the next few days he began to walk with a cane, later without support, and there were no more contractions except transiently in the left leg if the patient walked a little too long. He left the hospital cured.
However, no signs of any organic damage could be found. There was limited numbness in the ankles. Psychotherapy and physical therapy were not effective. On January 28, 1917, the stovaine injection method was attempted. Once the anesthesia took effect, it was still possible to induce the spasm by extending the legs; however, a half hour after the injection, the spasms could no longer be triggered. The patient was shown that the tremors had disappeared. During the return of feeling, the legs were constantly moved, and the patient was encouraged to move them himself. He became confident in his ability. There was no more clonus. The patient stayed in bed all day without any seizure-like movements. The next day, he only complained of weakness in his legs and was able to walk without experiencing convulsive shaking. Over the next few days, he started to walk with a cane, and eventually without any support, and there were no more contractions, except briefly in the left leg if he walked for too long. He left the hospital fully recovered.
Shell-shock deafmutism: Psychic treatment.
Shell-shock deaf-muteness: Mental health treatment.
Case 562. (Bellin and Vernet, January, 1917.)
A soldier in a colonial regiment was sent, August 14, 1916, to an evacuation post with a diagnosis “deafness following shell-shock, unfit for service.” The patient asked that he be spoken to very loud because he could not hear, and he himself spoke in whispers. He kept watching his interlocutors’ lips and moved his own as if to pronounce the words.
A soldier in a colonial regiment was sent, August 14, 1916, to an evacuation post with a diagnosis “deafness following shell-shock, unfit for service.” The patient asked to be spoken to very loudly because he couldn’t hear, and he spoke in whispers. He kept watching his conversation partners’ lips and moved his own as if trying to pronounce the words.
A shell had burst nearby fourteen months before in June, 1915. After being in several hospitals, he was sent to an oto-rhino-laryngological service where he had his hearing reëducated and was taught lip reading. It was soon perceived that he could hear without lip reading and he was assured that he could be cured at once, but naturally he was not convinced. He produced a carefully filed paper stating “atrophic ozenous rhinitis, deafness from labyrinthine shock following shell explosion, hearing diminished 60 per cent right, 30 per cent left.”
A shell had exploded nearby fourteen months earlier in June 1915. After being in several hospitals, he was sent to an ENT service where he had his hearing retrained and learned lip reading. It quickly became clear that he could hear without lip reading, and he was told that he could be cured immediately, but of course, he wasn’t convinced. He presented a carefully organized document stating “atrophic ozenous rhinitis, deafness from labyrinthine shock following shell explosion, hearing reduced 60 percent right, 30 percent left.”
However, energetic psychotherapy was started and in the absence of electricity, subcutaneous injections of ether were given. Such patients had always been cured, and a drug injected under the skin, not dangerous but extremely painful would cure him! This treatment was carried out in a dugout near enough to the lines to be daily “potted.” The patient was left for a space to reflect, and he finally accepted the chance of cure. He was exhorted to stand courageously the pain and to breathe deeply and to repeat a word more and more loudly. Finally he was made to speak normally and eventually to cry out loudly. He now felt much astonished, and in his astonishment forgot his deafness. He said that he had never spoken or heard since the accident, that he had been a deafmute from the first month of his illness, and that for the last three months he had been able to speak only in a whispered voice.
However, energetic psychotherapy was initiated, and in the absence of electricity, patients received subcutaneous injections of ether. Such patients had always been cured, and a drug injected under the skin, while not dangerous, was extremely painful and would heal him! This treatment took place in a dugout close enough to the lines to be "potted" daily. The patient was left alone for a while to reflect, and he ultimately accepted the chance of being cured. He was encouraged to bravely endure the pain, breathe deeply, and repeat a word increasingly louder. Eventually, he was able to speak normally and ultimately cry out loudly. He felt quite astonished and, in his amazement, forgot about his deafness. He mentioned that he hadn’t spoken or heard since the accident, that he had been a deaf-mute since the first month of his illness, and that for the last three months, he could only speak in a whisper.
He should have been watched a few days to confirm the cure. This was impossible in the crowded dugout and no[781] risk could be run of his escaping. Kept over night he was found next day unable to hear and talking in the same voice as before.
He should have been kept under observation for a few days to confirm the cure. This was impossible in the crowded dugout, and no[781] risk could be taken of him escaping. After being kept overnight, he was found the next day unable to hear and speaking in the same voice as before.
He was now found to be either an exaggerator or a simulator. He was given a half hour to exercise his voice in and told that he must succeed unless he was a simulator. At the end of half an hour it was found that he had skipped. He was sent back by the division surgeon with orders to send him to the otological service for inquiry. The otological service found an atrophic ozenous rhinitis, a normal larynx, perfect audition. He was given a psychic X-raying and a few electric sparks were also drawn from his neck. He then began to talk in a loud voice and to hear normally. August 30, he was sent out completely cured and rejoined his regiment.
He was now seen as either someone who exaggerates or someone who fakes it. He was given half an hour to warm up his voice and was told that he had to succeed unless he was faking. By the end of the half hour, it turned out that he had skipped out. The division surgeon sent him back with orders to refer him to the ear, nose, and throat service for evaluation. The ENT service found he had a type of chronic nasal condition, a normal larynx, and perfect hearing. He underwent a psychological evaluation and received a few electric shocks to his neck. After that, he started speaking loudly and hearing normally. On August 30, he was discharged completely cured and rejoined his regiment.
Brachial monoplegia. Cure by electrical suggestion (physician bored-looking, brief, and authoritative).
Brachial monoplegia. Treatment through electrical suggestion (physician appears uninterested, succinct, and assertive).
Case 563. (Adrian and Yealland, June, 1917.)
Adrian and Yealland had occasion to treat an officer with a persistent functional paralysis of the arm, which had successfully withstood hypnotism, psychoanalysis, rest, massage, anesthesia with ether, and painful electrical treatment.
Adrian and Yealland had the opportunity to treat an officer with a stubborn functional paralysis of the arm, which had effectively resisted hypnotism, psychoanalysis, rest, massage, ether anesthesia, and painful electrical treatments.
This patient knew something of the functions of the brain and was prepared to discuss his condition exhaustively. He was told, however, that he had come to be cured and that the nature of his cure would be explained to him afterwards. Without further discussion, the motor areas of the cortex were mapped out rapidly. The measurements were repeated aloud to impress and mystify the patient. He was assured that as soon as the shoulder area of the cortex was stimulated faradically, he would be able to raise his shoulder, and that then the rest of his arm would recover. An exceedingly mild faradic current was then applied to the scalp for a few moments and he was then ordered to move his shoulder. He did so at once. In a few minutes, all of the paralysis had vanished and the patient could raise 30 pounds. Adrian and Yealland believe that the success here was largely due to the fact that the patient was not allowed to discuss the case or criticize the treatment beforehand.
This patient understood a bit about how the brain works and was ready to talk in detail about his condition. He was told, though, that he had come to be treated and that the details of his treatment would be explained later. Without any further discussion, the motor areas of the cortex were quickly mapped out. The measurements were repeated out loud to impress and confuse the patient. He was assured that as soon as the shoulder area of the cortex was stimulated with a mild electrical current, he would be able to lift his shoulder, and then the rest of his arm would recover. A very mild electrical current was applied to the scalp for a few moments, and then he was instructed to move his shoulder. He did so immediately. Within a few minutes, all of the paralysis disappeared, and the patient could lift 30 pounds. Adrian and Yealland believe that the success here was mainly because the patient was not allowed to discuss the case or criticize the treatment beforehand.
It is essential that the patient should be convinced that the physicians understand the case and can cure him. No physical sign should be examined as if it were interesting or obscure. An attitude of “mild boredom bred of perfect familiarity with the patient’s disorder” is cultivated. If the case is exhibited it should be exhibited “as a perfect example” of the type of case that is cured in five minutes by appropriate treatment. “Rapidity and an authoritative manner are the chief factors in the reëducative process.”
It’s crucial that the patient feels confident that the doctors understand the situation and can help him. No physical symptom should be looked at as if it’s intriguing or mysterious. An attitude of “mild boredom from being completely familiar with the patient’s issue” is developed. If the case is shown, it should be presented “as a perfect example” of a case that can be resolved in five minutes with the right treatment. “Speed and a confident approach are the main elements in the recovery process.”
Re psychoelectric treatment, see Yealland’s book, published while this compilation was going to press, Hysterical Disorders of Warfare, 1918.
Re psychoelectric treatment, see Yealland’s book, published while this compilation was going to press, Hysterical Disorders of Warfare, 1918.
Brachial monoplegia following use of sling after bruise or wound. Technique of electrical suggestion and rapid reëducation.
Brachial monoplegia after using a sling due to a bruise or injury. Method of electrical stimulation and quick rehabilitation.
Case 564. (Adrian and Yealland, June, 1917.)
Adrian and Yealland give the following typical case of paralysis of the arm as a very frequent and very curable form of war neurosis, occurring as a rule after a slight wound or bruise necessitating the use of a sling. The patient, having received a slight wound of the forearm, for months had a useless arm, which he could move but slightly at the shoulder on exerting a superhuman effort. Occasionally he could flex the fingers through a small angle. There was complete anesthesia of the hand and arm of long-glove type. This anesthesia was not complained of, and might not be noticed until suggested to the patient by the physician. It is well to elicit the anesthesia, however, in view of the treatment to be applied. There was no wasting of muscles; the sensory loss was typical of hysterical anesthesia; nor could the whole arm have been involved by an injury that did not affect the upper arm and shoulder.
Adrian and Yealland describe a typical case of arm paralysis as a common and highly treatable form of war-related nerve trauma, usually happening after a minor injury or bruise that requires using a sling. The patient, who had a small wound on the forearm, experienced a useless arm for months, managing only slight movement at the shoulder with incredible effort. Occasionally, he could bend his fingers slightly. The hand and arm had complete numbness, resembling a long-glove pattern. The patient didn’t mention the numbness, and it might not be noticed until a doctor points it out. It’s important to identify the numbness for treatment purposes. There was no muscle wasting; the sensory loss was typical of hysterical numbness, and it wouldn't be possible for the entire arm to be affected by an injury that didn't involve the upper arm and shoulder.
The patient was told that he was very lucky to have come off with such a slight injury; his arm was to be set right in five minutes by the application of a special form of electricity. He was then made to sit on a large pad electrode connected with an induction coil; the other terminal is connected with a wire brush. The first effect, he was told, would be the return of feeling in the forearm; power would return with the feeling. The wire brush with a fairly strong current was drawn downwards over the forearm from elbow to wrist. He was told that he could now feel as far as the wrist, and a pin was used to convince him that he could thus feel. If he had not felt the pinprick, the current would have been increased in strength until he could feel. The hand was now treated in the same way.
The patient was informed that he was very fortunate to have suffered such a minor injury; his arm would be fixed in five minutes using a special type of electricity. He was then seated on a large pad electrode linked to an induction coil; the other end was connected to a wire brush. He was told that the first sensation he would experience would be a return of feeling in his forearm, and strength would come back along with the feeling. The wire brush, with a fairly strong current, was moved downward over his forearm from elbow to wrist. He was told that he could now feel all the way to his wrist, and a pin was used to prove that he could indeed feel. If he hadn't felt the pinprick, the current would have been increased until he could. His hand was treated in the same manner.
He was now told that, as feeling had returned to the arm, the power of movement would be restored shortly. Adrian[784] and Yealland remark that laymen seem to consider that loss of power and loss of feeling are inseparably connected. The electrode was now used to produce contraction in the muscles. Under these circumstances, the arm will be used hesitatingly, with an appearance of great effort; but the patient is nevertheless convinced that power is returning.
He was now told that, since feeling had come back to the arm, the ability to move it would be restored soon. Adrian[784] and Yealland note that people without medical training seem to believe that loss of movement and loss of feeling are always linked. The electrode was now used to stimulate contraction in the muscles. In this situation, the arm is used cautiously, appearing to require a lot of effort; however, the patient is still convinced that strength is coming back.
“Rapid reëducation follows at once. He is given no time to think, but urged to move the arm more and more strongly, to grip the physician’s hand, to flex and extend the elbow, etc., and the pressure is not relaxed until the whole arm has returned to its normal vigor. If recovery is stationary, faradization is repeated with stronger and stronger currents. If it seems as though he might relapse on leaving the hospital, he is told that this is very unlikely, but that if it should occur, he should report sick at once and come back for treatment with a current far stronger than that already used.”
“Rapid rehabilitation starts right away. He doesn't get a moment to think; instead, he's encouraged to move his arm more vigorously, to grip the doctor's hand, to bend and straighten his elbow, and the pressure continues until his arm regains its normal strength. If his recovery stalls, faradization is done again with increasingly stronger currents. If it looks like he might have a setback after leaving the hospital, he’s told that this is very unlikely, but if it does happen, he should report feeling unwell immediately and come back for treatment with a much stronger current than what was used before.”
Adrian and Yealland claim that they have applied their combination of suggestion and reëducation in more than 250 cases (including 82 cases of mutism, 34 of deafness, 18 of aphonia, 37 brachial or crural monoplegia, 46 paraplegia, 16 hemiplegia, and 18 of non-organic gait disturbance), and that although a majority of the cases have been of several months’ standing, treatment has been almost immediately successful in at least 95 per cent of the cases.
Adrian and Yealland state that they have used their mix of suggestion and re-education in over 250 cases (including 82 cases of mutism, 34 of deafness, 18 of loss of voice, 37 cases of one-sided weakness in an arm or leg, 46 cases of paraplegia, 16 hemiplegia, and 18 cases of non-organic walking issues), and that even though most of these cases have lasted several months, treatment has been almost immediately effective in at least 95 percent of the cases.
Exposure in the retreat from Mons: Persistent hysterical sciatica. Treatment by faradism and verbal suggestion.
Exposure in the retreat from Mons: Ongoing hysterical sciatica. Treatment through faradism and verbal suggestion.
Case 565. (Harris, 1915.)
A soldier developed pains about the hips and down the right thigh after getting wet through in the retreat from Mons, August, 1914. He was treated for a period of nine months in various convalescent homes and military hospitals, incidentally receiving forty baths at Droitwich. He hobbled on a stick, leaning upon the left leg and dragging the right stiffly. The thigh was tender and hyperesthetic.
A soldier started experiencing pain in his hips and down his right thigh after getting soaked during the retreat from Mons in August 1914. He received treatment for nine months in different recovery homes and military hospitals, including having forty baths at Droitwich. He hobbled with a cane, leaning on his left leg and dragging his right leg stiffly. His thigh was sensitive and overly sensitive to touch.
The proper treatment of cases of hysteria, according to Harris, is strong faradism, applied by a small electrode or wire brush to the moistened skin. The stimulus is made powerful enough to force the patient to admit that he feels. The theory is that the powerful stimulation “breaks down the psychical auto-inhibition which produces the hysterical anesthesia.”
The right way to treat cases of hysteria, according to Harris, is strong faradism, applied with a small electrode or wire brush on damp skin. The stimulation is intense enough to make the patient acknowledge that they can feel. The idea is that the strong stimulation “breaks down the psychical auto-inhibition that causes the hysterical numbness.”
Faradism is only the first phase of the treatment. Verbal suggestion follows. Building on the basis of the feeling produced by the faradism or on the basis of the ocular evidence of motion in the hitherto paralyzed muscles, the patient is informed that the electricity will now be more and more strongly felt and that he will be cured in a few minutes.
Faradism is just the first step of the treatment. Next comes verbal suggestion. Building on the feeling created by the faradism or the visible movement in the previously paralyzed muscles, the patient is told that they will soon feel the electricity more intensely and that they will be cured in a few minutes.
The two elements in the therapy, then, are: encouraging verbal suggestion and the suggestion afforded by the paraphernalia of a complex looking, noisy machine. The knowledge on the part of the patient that a powerful and mysterious stimulus, namely, electricity, is being employed is a third element of suggestion.
The two elements in the therapy, then, are: encouraging verbal suggestion and the suggestion provided by the complicated, noisy machine. The patient's awareness that a powerful and mysterious stimulus, specifically electricity, is being used is a third element of suggestion.
Persistent hysterical sciatica, such as that of the present case, may require prolonged treatment. In this instance, the man was completely cured in five minutes, so that he was made able to run across the room. He said he would now be able to go back to the front, and wondered why he could not have been cured before.
Persistent hysterical sciatica, like in this case, might need long-term treatment. In this situation, the man was completely cured in five minutes, allowing him to run across the room. He mentioned that he could now return to the front and questioned why he couldn't have been healed earlier.
Prognosis of intensive reëducation in reflex (physiopathic) disorder—complete recovery (except for the hysterical fraction of the disease) not expected.
Prognosis of intensive rehabilitation in reflex (physiopathic) disorder—complete recovery (except for the hysterical part of the condition) is not anticipated.
Case 566. (Vinny, 1916.)
A young soldier was superficially wounded in the left knee, in August, 1914. A year later, he showed amyotrophy of the left calf, which measured 2.5 cm. less than the right, a weak slow Achilles reflex on the left side, cyanosis and hypothermia of the left foot, weakness and limitation of movements in the left foot, with slight contracture in flexion of leg upon thigh.
A young soldier received a superficial wound to his left knee in August 1914. A year later, he displayed muscle wasting in his left calf, which was 2.5 cm smaller than his right calf. He had a weak and slow Achilles reflex on the left side, along with a blueish discoloration and lower temperature in the left foot. There was weakness and restricted movement in the left foot, along with slight bending of the leg at the thigh.
Thenceforward and for eight months, this soldier was submitted at the Tours Centre to intensive reëducation. For two hours every day upon prescription he walked, ran, and hopped upon the left leg. In September, 1916, after twelve month’s training, there was a certain improvement in his disorder. The leg was now completely extended upon the thigh, and the amplitude in the movement of the foot was almost normal; but the amyotrophy, vasomotor disorder and certain electrical disturbances remained quite unchanged. The man himself recognized that his status was greatly improved, but he could not walk more than four or five kilometers without great fatigue.
From then on, for eight months, this soldier underwent intensive rehabilitation at the Tours Centre. For two hours each day as prescribed, he walked, ran, and hopped on his left leg. In September 1916, after a year of training, there was some improvement in his condition. The leg was now fully extended on the thigh, and the movement of the foot was nearly normal. However, the muscle wasting, circulation issues, and some electrical disturbances remained unchanged. The soldier acknowledged that his condition had significantly improved, but he still couldn't walk more than four or five kilometers without feeling very tired.
In view of the inferior results of reëducation in some of these cases, should any attempt at all be made to reëducate? Vincent thinks that that should be; but that it should be borne in mind that sometimes no results may be obtained. If the reflex disorder (in the Babinski sense) is minimal and the chief difficulty is hysterical, then sometimes the man may go back to service after reëducation; but in intense examples of reflex (physiopathic) disorder, invaliding has often proved necessary.
In light of the poor outcomes of rehabilitation in some of these cases, should we even try to rehabilitate? Vincent believes we should, but we need to remember that sometimes no results can be achieved. If the reflex issue (in the Babinski sense) is minimal and the main problem is psychological, then sometimes the person may return to work after rehabilitation; however, in severe cases of reflex (physiological) disorder, being declared unfit for duty has often been necessary.
Re values of intensive reëducation, Vincent’s technique and results have logical resemblances to those of Yealland and of Kaufmann. Vincent established in the 9th district neurological center a method of intensive reëducation which[787] is particularly suited to old hysterical cases. He divides the treatment into three stages: First, the stage called by the poilu by the picturesque name of torpillage; secondly, the stage of fixation; thirdly, the stage of training. According to Roussy and Lhermitte, there are few cases at the front suitable for the treatment of Clovis Vincent, which is especially devised for the old cases. See under Case 574 for further details of Vincent’s treatment.
Re values of intensive reëducation, Vincent’s technique and outcomes have clear similarities to those of Yealland and Kaufmann. Vincent developed a method of intensive reëducation at the 9th district neurological center that is especially effective for old hysterical cases. He breaks the treatment into three stages: First, a stage referred to by the poilu with the vivid name of torpillage; second, the fixation stage; and third, the training stage. According to Roussy and Lhermitte, there are few cases at the front that are suitable for Clovis Vincent's treatment, which is particularly designed for old cases. See under Case 574 for further details on Vincent’s treatment.
Re prognosis of the physiopathic disorder, there has been some controversy in France. See discussion under Case 530. Re suitable treatment for physiopathic disorders, Babinski and Froment suggested the application of heat. The warm bath test is also of value in diagnosis. Babinski and Froment claim progressive improvements with hot baths, hot air douches, and light baths—but counsel great prudence. The improvement is never rapid.
Regarding the prognosis of the physiopathic disorder, there has been some debate in France. See discussion under Case 530. As for suitable treatment for physiopathic disorders, Babinski and Froment recommended the use of heat. The warm bath test is also helpful in diagnosis. Babinski and Froment report gradual improvements with hot baths, hot air treatments, and light baths—but advise caution. The improvement is never quick.
Wound of calf; operations: hysterical contracture with “physiopathic” features. “Brutally conquered” by reëducation.
Wound of calf; operations: hysterical contracture with “physiopathic” features. “Brutally conquered” by reeducation.
Case 567. (Ferrand, March, 1917.)
A French infantryman, class of 1912, was wounded, May 12, 1915, in the upper third of the right calf. His posterior tibial artery had to be ligated. In a few weeks the wound was healed, but he began to walk badly, presenting a contracture of the calf with retraction of the tendo Achillis.
A French infantryman, class of 1912, was wounded on May 12, 1915, in the upper part of his right calf. His posterior tibial artery had to be tied off. In a few weeks, the wound healed, but he started to walk poorly, showing a contracture of the calf with tightness in the Achilles tendon.
Toward the last of 1915 a surgeon under the impression that the disease was organic cut the tendo Achillis but the soldier could not walk any better. As he could not take the position of equinism, he semiflexed his knee and walked upon a crutch.
Toward the end of 1915, a surgeon, believing the condition was physical, cut the Achilles tendon, but the soldier still couldn't walk any better. Since he couldn't achieve the position of equinism, he bent his knee slightly and walked with a crutch.
Another surgeon was now found to perform a tenotomy on the flexors of the leg and put the patient in a plaster cast to correct the flexion and immobilize in extension. This second operation was in July, 1916. The patient now walked without a crutch.
Another surgeon was found to perform a tenotomy on the leg's flexors and put the patient in a plaster cast to straighten it out and keep it immobilized. This second surgery took place in July 1916. The patient was now able to walk without crutches.
He was then sent to a neurological center, Dec. 8, 1916, walking on two canes, right leg in forced extension on thigh, in permanent and absolute contracture. All movements except leg flexion could be executed, though slowly and weakly; but positive movements were impossible, except flexion of the knees. There was no sensory disorder. Reflexes were normal save that the leg reflexes were a little stronger on the affected side, and the patellar reflex on that side was nullified by the contracture. Electrical reactions proved normal. There were marked trophic disturbances of the right foot and of the lower third of the lower leg. There was a certain amount of edema, cyanosis, coldness and thickening of skin; marked muscular over-excitability of the distal extremity of the leg. In short, Ferrand was here dealing with a case of Babinski’s group of the so-called physiopathic cases. The[789] man was somewhat feeble-minded, and anxious and a trembling suppliant for cure.
He was then sent to a neurological center on December 8, 1916, walking with two canes, his right leg forcibly extended at the thigh in a constant and complete contracture. He could perform all movements except for bending his leg, although it was slow and weak; however, any active movements were impossible, except for bending his knees. There were no sensory issues. Reflexes were normal except that the leg reflexes were slightly stronger on the affected side, and the patellar reflex on that side was absent due to the contracture. Electrical reactions were normal. There were noticeable trophic changes in the right foot and the lower third of the lower leg, including some edema, cyanosis, coldness, and thickening of the skin; marked muscular over-excitability was observed in the distal part of the leg. In short, Ferrand was dealing with a case from Babinski’s group of so-called physiopathic cases. The[789] man was somewhat mentally impaired, anxious, and a trembling supplicant for a cure.
He was put, December 15, in a reëducation room and by means of fatigue, induced by violent physical exercises, was (Ferrand states) “brutally conquered.” The contracture after a half hour of physical movement of flexion and extension of the leg ceased. The patient was shown how he could himself both flex and extend the limb himself; he was then caused to do this spontaneously. These active movements were aided and at times provoked by somewhat painful galvanic discharges. The patient then walked slowly, and flexed both knees to the maximum. He was cured after a treatment of 2½ hours. There were, of course, some (surgical) intra-articular adhesions in the knee and it was necessary for the patient to break these adhesions. An X-ray had shown the bone to be intact. A slight hydrarthrosis developed the next day, but a few days later he was able to walk as well as anyone. For five weeks he followed a training platoon in the reëducation work and was evacuated, January 23, 1917, to his station, though he had entered the neurological center with the idea that he was to be invalided with a pension.
He was placed in a rehabilitation room on December 15, and through intense physical exercises that caused exhaustion, was (according to Ferrand) “brutally conquered.” After half an hour of leg flexion and extension exercises, the muscle tightness stopped. The patient was shown how to flex and extend his leg on his own, and then encouraged to do this naturally. These movements were supported and occasionally triggered by somewhat painful electric shocks. The patient then walked slowly and flexed both knees fully. He was healed after 2½ hours of treatment. There were some (surgical) adhesions in the knee joint, and it was necessary for the patient to break these adhesions. An X-ray confirmed that the bone was intact. A slight buildup of fluid in the joint occurred the next day, but a few days later, he was able to walk as well as anyone else. For five weeks, he participated in a training platoon for rehabilitation, and on January 23, 1917, he was sent back to his unit, even though he had arrived at the neurological center believing he would be discharged with a disability pension.
He had a few relics of physiomotor disorder when he left, including the abnormal delicacy of skin and muscular over-excitability above mentioned. On the basis of this and similar cases Ferrand believes that, although the physiopathic group of Babinski exists, it does not signify a separate clinical syndrome and the occurrence of physiopathic symptoms does not contraindicate psychotherapy.
He had a few signs of a physical movement disorder when he left, including the unusual sensitivity of his skin and muscle overactivity mentioned earlier. Based on this and similar cases, Ferrand believes that, although the physiopathic group of Babinski exists, it doesn't represent a distinct clinical syndrome, and the presence of physiopathic symptoms doesn't rule out psychotherapy.
Re this controversy, see remarks under Case 530.
About this controversy, see remarks under __A_TAG_PLACEHOLDER_0__.
Shell-shock: Paraparesis. Cure by electricity.
Shell shock: Paraparesis. Cure with electricity.
Case 568. (Turrell, January, 1915.)
Turrell, in a paper on electrotherapy at a base hospital, narrates a case of spinal concussion which rapidly yielded to the persuasive influence of Bergonié’s machine for electrically provoked exercises. Turrell grants that such a rapid cure would probably be attributed to suggestion, but thinks that the term demonstration might be preferred on account of the vigor and amplitude of the muscular contractions excited.
Turrell, in a paper on electrotherapy at a base hospital, tells the story of a spinal concussion that quickly responded to the effective use of Bergonié’s machine for electrically induced exercises. Turrell acknowledges that this fast recovery might be seen as due to suggestion, but believes that the term demonstration would be more fitting because of the strength and intensity of the muscle contractions produced.
This soldier was driving an ammunition wagon at the front, when a shell exploded under the wagon, killing one horse and severely wounding the other. The patient himself was blown into the air, fell, dragged himself to a trench where he lay all night, and found himself in the morning unable to walk or stand. He recalls that pins were stuck into his legs by the examining medical officer and that they produced no sensation. When he was finally brought to the Third Southern Medical Hospital, he was unable to draw up or move his legs, or to stand up (yet neurologically normal).
This soldier was driving an ammo wagon at the front when a shell exploded underneath it, killing one horse and seriously injuring the other. He was thrown into the air, fell, and managed to crawl to a trench where he lay all night, only to discover in the morning that he couldn't walk or stand. He remembers that the examining doctor stuck pins into his legs and that he didn't feel a thing. When he was finally taken to the Third Southern Medical Hospital, he couldn't bend or move his legs, nor could he stand, even though his neurological status was normal.
After a few days’ rest in bed, he found himself able to walk a few steps with assistance, and was then transferred to the Radcliffe Infirmary for electrical treatment. This treatment consisted in electrically provoked exercises to the back (positive) and seat and thighs (negative). He was able to walk back to his ward, leaning on a wheelchair. Next day he walked to the electrical department with sticks, and after the exercises were repeated, he was found able to walk without assistance. On the third day, the Morton wave current was applied to the back, to clear up any persistent stiffness. The patient was then discharged on sick furlough.
After a few days of resting in bed, he found he could walk a few steps with help and was then moved to the Radcliffe Infirmary for electrical treatment. This treatment involved electrical exercises on his back (positive) and buttocks and thighs (negative). He managed to walk back to his ward, using a wheelchair for support. The next day, he walked to the electrical department with crutches, and after repeating the exercises, he was able to walk on his own. On the third day, the Morton wave current was applied to his back to relieve any lingering stiffness. The patient was then discharged on sick leave.
Re the Morton wave and similar applications of electricity, Zeehandelaar speaks of a high frequency hall fitted up at Berlin. Touching the walls of the hall with the finger elicited a powerful spark. The scheme appeared to be on a commercial basis, and it was proposed to start similar institutions for poor metabolism and neuroses in other cities.
Re the Morton wave and similar uses of electricity, Zeehandelaar mentions a high-frequency hall set up in Berlin. Touching the walls of the hall with your finger produced a strong spark. The setup seemed to be commercially viable, and there were plans to establish similar facilities for poor metabolism and neuroses in other cities.
A year’s field service, gunshot; typhoid fever: Astasia-abasia: Lourdes-like cure: Residual amnesia.
A year of doing fieldwork, got shot; typhoid fever: Astasia-abasia: a miraculous cure like Lourdes: lingering amnesia.
Case 569. (Voss, November, 1916.)
A soldier in service from the outbreak of war, shot in September, 1915, afterward suffering from fainting spells, was treated in several hospitals. He developed a typhoid fever at Lindau, which was at first taken for hysterical fever. Eventually he came to the observation of Voss, unable to stand and falling hysteria-wise if compelled to walk.
A soldier who served since the beginning of the war, was shot in September 1915 and later experienced fainting spells. He received treatment in several hospitals. While at Lindau, he developed typhoid fever, which was initially mistaken for hysteria. Eventually, he was observed by Voss, unable to stand and collapsing in a hysterical manner if he had to walk.
Thorough examination was made. It was emphatically explained to him that there could be no reason why he should not stand or walk.
A thorough examination was conducted. It was clearly explained to him that there was no reason he shouldn't be able to stand or walk.
A miracle occurred. From the second day of his hospital stay he not only walked about but began to polish doors and windows with inexhaustible strength.
A miracle happened. From the second day of his hospital stay, he not only walked around but also started polishing doors and windows with endless energy.
But when he was about to be told that he must now be looked upon as well, the miracle was not so manifest. It now transpired that he had serious gaps of memory and disorders in recognition, a sphincter disorder and ever since his typhoid incontinence with fluid feces.
But just when he was about to be told that he had to be regarded in a different light, the miracle wasn’t so obvious. It turned out that he had serious memory gaps and issues with recognition, a bowel disorder, and ever since his typhoid, he had been dealing with incontinence and fluid feces.
In short, waking suggestion had caused a very prominent symptom to disappear, but the total personality remained sick. According to Voss, the procedures of Kaufmann are dubious just because they cannot stand the test of time. Yet so far as the cure of this man’s astasia-abasia was concerned, it was not at all unlike the cures wrought at Lourdes.
In short, waking suggestion made a significant symptom go away, but the overall personality was still unwell. According to Voss, Kaufmann's methods are questionable because they don’t hold up over time. However, when it comes to curing this man’s astasia-abasia, it was really similar to the cures happening at Lourdes.
Re miracles of this sort, see cases of Colin Russel (503 and 504) as well as those of Veale (511 and 512). Voss’ arguments run parallel with the contentions of various persons that the miracle cures (such as those by anesthesia, electric suggestion, and hypnosis), do not get sufficiently to the bottom of the affections in question. Buzzard, in the preface to Yealland’s book on the Hysterical Disorders of Warfare, remarks that the question of the ultimate prognosis in cases thus suddenly cured must be left unanswered.
For miracles like these, refer to the cases of Colin Russel (503 and 504) as well as those of Veale (511 and 512). Voss’ arguments align with the opinions of various individuals who believe that miraculous cures (such as those achieved through anesthesia, electrical suggestion, and hypnosis) do not fully address the underlying issues. Buzzard, in the preface to Yealland’s book on the Hysterical Disorders of Warfare, notes that the question of the ultimate prognosis in cases that are suddenly cured remains unanswered.
Dysbasia after a fall: “Kaufmann” cure in six weeks.
Dysbasia after a fall: “Kaufmann” treatment in six weeks.
Case 570. (Schultze, August, 1916.)
Severe dysbasia, due to monoplegia of the right leg of sudden origin (a fall), was variously treated 64 weeks without effect.
Severe difficulty walking, caused by sudden weakness in the right leg (from a fall), was treated in different ways for 64 weeks without any results.
July 15, 1916, the patient walked in on a stick, and fell down on trying to walk without. August 1, 1916, at 9 o’clock, he was rapidly examined: Anesthesia to pain and temperature; inability to lift right foot; the right knee could be lifted about a hand-breadth above the body if the foot was supported.
July 15, 1916, the patient came in using a cane and collapsed when trying to walk without it. August 1, 1916, at 9 o’clock, he was quickly examined: No pain or temperature sensitivity; unable to lift the right foot; the right knee could be elevated about a hand’s width above the body if the foot was supported.
At 9:10, a small electrode was applied: sensibility became normal at once. Second application: leg raised much better. The man was told that he was better and that his hand could be put under the heel. Third application: Leg raised 8 cm. The patient showed pleasure at the advance. Fourth application (slightly increased strength): Patient able to stand and to lift knee with flexion at 135° while standing. Walking exercises under direction. At 9:30, five minutes recess was given for fatigue, whereupon the exercises were taken up again and transition made from stationary running to walking without aid as well as a variety of other associated acts (grasping handkerchief instead of physician’s hand, and the like). The patient became exhausted after 8 or 9 minutes running about, and another pause was given.
At 9:10, a small electrode was applied: sensitivity returned to normal immediately. Second application: the leg was raised much better. The man was informed that he was improving and that his hand could be placed under his heel. Third application: the leg was raised 8 cm. The patient showed pleasure at this progress. Fourth application (slightly increased strength): the patient was able to stand and lift his knee with a bend of 135° while standing. Walking exercises were done under supervision. At 9:30, a five-minute break was given for fatigue, after which the exercises continued, transitioning from stationary running to walking without assistance, along with various other related actions (like picking up a handkerchief instead of the physician’s hand). The patient became exhausted after 8 or 9 minutes of running around, and another break was taken.
The large brush electrode with stronger current was now given to the back and to the back of the right leg. Practice in slow walking, lifting knee, and holding hip joint firm. The patient became tired, but remained very willing. Exercises in pulling on stockings, in climbing stairs—the whole concluded at 10 o’clock, whereupon it was found that the patient could walk alone for a distance of 50 meters. The patient was a very suggestible one. It was striking that the patient in the time between 9:35 and 9:40 minutes could[793] walk better on the right (that is, the previously affected leg) than upon the left. Rest in bed and phenacetine were ordered, with the suggestion that in the morning he would walk much better. He became irritated after the treatment but grew quieter in the afternoon.
The large brush electrode with a stronger current was now applied to the back and the back of the right leg. They practiced slow walking, lifting the knee, and keeping the hip joint stable. The patient got tired but stayed very willing. They did exercises in pulling on stockings and climbing stairs—the whole session wrapped up at 10 o’clock, and it was noted that the patient could walk on their own for a distance of 50 meters. The patient was very suggestible. It was noticeable that between 9:35 and 9:40 minutes, the patient could walk better on the right (the previously affected leg) than on the left. Rest in bed and phenacetin were prescribed, along with the suggestion that in the morning, they would walk much better. The patient became irritated after the treatment but calmed down in the afternoon.
On August 3, he was found able to walk well, better when not observed than when observed. August 5, he complained that his leg was worse and used a cane, without permission. He was roundly scolded by the physician and threatened with being sent to bed if he did not practice earnestly. August 7, he was better, and confessed that he could not walk as well on command as he could alone; the exercises were nothing but a fraud and he could go out and beat everything up (alles zerschlagen) if he did not have to carry out such exercises.
On August 3, he was found to be walking well, and he did better when he thought no one was watching. On August 5, he complained that his leg was worse and used a cane without permission. The doctor scolded him harshly and warned him he would be sent to bed if he didn't take his practice seriously. By August 7, he felt better and admitted that he couldn't walk as well when he was being watched as he could when he was alone; he thought the exercises were pointless and claimed he could go out and smash everything up (alles zerschlagen) if he didn't have to do those exercises.
August 15, he was much better, quiet, and satisfied. The lameness was practically gone. August 30, there was no sign of lameness, even when he was observed. According to Schultze, the Kaufmann method is not merely an Erb tradition, and rather special measures need to be taken in executing it.
August 15, he felt much better, calm, and content. The lameness was almost completely gone. By August 30, there was no indication of lameness, even when he was being watched. According to Schultze, the Kaufmann method isn't just a family tradition; specific steps need to be followed to carry it out properly.
Re Kaufmann’s cure, Imboden sums up this “highly logical and brutal method” as a method in which powerful electric shocks and loud military orders to perform certain exercises secure results. Imboden suggests that relapses may follow, sometimes on the slightest provocation. Mann states that Kaufmann’s method of suggestion and electric shock forms very good treatment; yet Mann states there have been two deaths under this treatment: in both instances there was an enlarged thymus at autopsy. A better technique, especially the use of the faradic current alone, might have avoided these deaths. Mann himself prefers to Kaufmann’s Ueberrumpelung milder methods, such as rest. Kaufmann keeps up the sitting until the man is cured, even if it takes two hours of electricity and staccato commands. For similar persistance, see the treatment by induced fatigue of Reeve (Cases 489-493).
Re Kaufmann’s treatment, Imboden describes this “highly logical and brutal method” as one where intense electric shocks and loud military orders to complete certain exercises ensure results. Imboden suggests that relapses can occur, sometimes with the slightest trigger. Mann notes that Kaufmann’s approach of suggestion and electric shock provides very effective treatment; however, Mann also mentions that there have been two fatalities during this treatment: in both cases, an enlarged thymus was found during autopsy. A better technique, particularly the exclusive use of the faradic current, might have prevented these deaths. Mann himself prefers Kaufmann’s Ueberrumpelung to gentler methods, like rest. Kaufmann continues the sessions until the patient is cured, even if it requires two hours of electric shocks and rapid-fire commands. For similar persistence, see the treatment through induced fatigue by Reeve (Cases 489-493).
Wound of shoulder: Heterosuggestion of BRACHIAL paresis. Electrical suggestion of muscular power. Recovery in five days.
Wound on shoulder: Heterosuggestion of BRACHIAL paresis. Electrical suggestion of muscle strength. Recovery in five days.
Case 571. (Hewat, March, 1917.)
A reënlisted soldier arrived at the Royal Victoria Hospital, as a case of ulnar paralysis. He had been wounded in France six months before by a bullet which passed through the fleshy part of the shoulder, above the middle third of the clavicle. Power in the right arm gradually diminished; yet two months after the wound he seemed fit enough to be sent to Egypt. The paresis developed, and in a month’s time he was invalided home. He had been unable to use a rifle for months.
A re-enlisted soldier arrived at the Royal Victoria Hospital with ulnar paralysis. He had been wounded in France six months earlier by a bullet that went through the meaty part of his shoulder, above the middle third of his collarbone. Strength in his right arm gradually decreased; however, two months after the injury, he seemed fit enough to be sent to Egypt. The weakness developed, and within a month, he was sent back home. He had been unable to use a rifle for months.
The healed bullet wounds were found about the region of the brachial plexus. The patient was sure the bullet had damaged the nerves in that region. The right arm and hand were limp and over-inclined to blueness, and the muscles were flabby. Active movements of all sorts could be carried out with the arm but not against resistance. There was a definite anesthesia and analgesia throughout, and responses to touch and pain stimuli were irregular.
The healed bullet wounds were located around the area of the brachial plexus. The patient believed the bullet had harmed the nerves there. The right arm and hand were weak and had a bluish tint, with flabby muscles. The patient could perform all kinds of movements with the arm but not against any resistance. There was noticeable numbness and lack of pain sensation throughout, and responses to touch and pain were inconsistent.
By way of treatment, the patient had the muscles of the paretic arm stimulated electrically, and at the same time he was told that no nerve of the neck had been injured. He was greatly surprised to see his palsied arm move vigorously.
Through treatment, the patient had the muscles of his weak arm stimulated with electricity, and at the same time, he was informed that none of the neck nerves had been damaged. He was very surprised to see his paralyzed arm move actively.
A milk isolation treatment in bed behind screens was adopted, whereat the patient was angry, looking upon the Weir-Mitchell treatment as punishment.
A milk isolation treatment was carried out in bed behind screens, during which the patient was upset, viewing the Weir-Mitchell treatment as a form of punishment.
On the next day, another electrical application secured complete power in the arm and abolished sensory disturbance. Three days later the man went back to full duty. According to Fergus Hewat, someone doubtless had suggested to this patient that he had received a nerve injury. He had become obsessed thereby and developed a typical functional paralysis. This was a “cortical misinterpretation,” which disappeared upon forcible demonstration of the error.
The next day, another electrical treatment restored full power in the arm and eliminated any sensory disturbance. Three days later, the man returned to full duty. According to Fergus Hewat, someone must have told this patient that he had sustained a nerve injury. He became fixated on this idea and developed a typical functional paralysis. This was a “cortical misinterpretation,” which vanished when the error was forcefully demonstrated.
Exposure; intestinal disorder in weakminded neuropath: Camptocormia and hysterical paraplegia: Cure by psycho-electric treatment.
Exposure; intestinal disorder in weak-minded neuropath: Camptocormia and hysterical paraplegia: Cure by psycho-electric treatment.
Case 572. (Roussy and Lhermitte, 1917.)
A French territorial, 45, was observed at the Centre Neurologique, August 28, 1916. He was a victim of hysterical paraplegia with tripod gait. There was a stiffness of the lumbar vertebral column which had lasted six months. This paraplegia had begun spontaneously after cold and an attack of diarrhoea followed by constipation. The camptocormia and disorder of gait had come on gradually in the ambulance. He came on a stretcher. He was found to be able to walk with great difficulty by leaning both hands on a cane. The two legs were tremulous in a pseudospastic gait. The next day, after a single psycho-electric treatment, cure was complete. This patient was mentally somewhat weak and a constitutional neuropath. He was discharged, cured, October 20, 1916.
A 45-year-old French patient was seen at the Neurological Center on August 28, 1916. He was suffering from hysteria-induced paraplegia and had a tripod gait. There was stiffness in his lower back that had lasted for six months. This paraplegia started suddenly after he experienced cold weather and a bout of diarrhea, followed by constipation. The curvature of his spine and gait disorder developed gradually while he was in the ambulance. He arrived on a stretcher but was found to be able to walk with great difficulty by leaning on a cane with both hands. His legs trembled in a pseudo-spastic manner as he walked. The next day, after just one psycho-electric treatment, he was completely cured. This patient was mentally somewhat weak and had a predisposition to neuropathy. He was discharged, fully recovered, on October 20, 1916.
Brachial monoplegia, hysterical (or feigned?). Found able to descend ladder with arms only.
Brachial monoplegia, hysterical (or faked?). Found able to climb down the ladder using only arms.
Case 573. (Claude, July, 1916.)
Claude had a case of a soldier with right-sided brachial monoplegia, which had lasted for 18 months and defied efforts to cure. There was a question of simulation, and Claude handed the case over to Vincent.
Claude had a case involving a soldier with right-sided arm paralysis that had lasted for 18 months and resisted all attempts at treatment. There were suspicions of faking, so Claude passed the case on to Vincent.
The case came on service, June 20, and was seen June 21. He was then treated and found able to descend a ladder applied to a wall with the help of his arms only. On June 24, he was found able to lift a weight of 10 kilos, and could now write with the right hand, although he had been writing only with his left. This man had looked like a simulator to many physicians. He may have been a simulator or an hysteric. In any case, he was cured.
The case was brought in on June 20 and examined on June 21. He was treated and found capable of climbing down a ladder against a wall using only his arms. By June 24, he could lift a weight of 10 kilos and was able to write with his right hand, even though he had previously only used his left. Many doctors had thought he was faking. He might have been pretending or had a hysterical condition. Regardless, he was cured.
Vicissitudes of treatment of hysterical brachial monoparesis (shell burial).
Vicissitudes of treatment of hysterical arm weakness (shell burial).
Case 574. (Vinny, July, 1917.)
A French private was buried in a trench upon the explosion of a large shell, November, 1914. He said he had had a “fracture of the occiput” and had fainted away without regaining consciousness for several hours.
A French soldier was buried in a trench after a large shell exploded in November 1914. He mentioned that he had a “fracture of the occiput” and had passed out, not regaining consciousness for several hours.
He was evacuated to Dunkirk, then Saint Nasire, and then to Sables-d’Olonne. He showed no paralysis or paresis of limbs. During the first month, he had violent pains in the head, spells and vomiting. There was a slight aphasic disorder. He was treated by cupping upon the head and by applications of ice.
He was evacuated to Dunkirk, then Saint Nasire, and then to Sables-d’Olonne. He showed no paralysis or weakness in his limbs. During the first month, he experienced severe headaches, episodes of dizziness, and vomiting. There was a slight speech disorder. He received treatment that included cupping on his head and ice applications.
After the visit of the inspector general, he was sent to Nantes to be trephined. Dr. Mathieu regarded an operation as useless. He was treated with bromides and the faradic current by Miraillé, applied to the right arm, which had become paretic.
After the inspector general's visit, he was sent to Nantes for surgery to relieve pressure on the brain. Dr. Mathieu thought the operation was unnecessary. He was treated with bromides and electrical stimulation by Miraillé, applied to his right arm, which had become weak.
June, 1915, he started on a three-months convalescent leave in Paris.
June 1915, he began a three-month recovery leave in Paris.
From October to December, he had electric treatment at the Grand-Palais.
From October to December, he received electric treatment at the Grand Palais.
December, 1915, he went to the Salpêtrière under P. Marie, where he was given electric treatment.
December 1915, he went to the Salpêtrière under P. Marie, where he received electric treatment.
January 1916, he went to Maison-Blanche under Laignel-Lavastine, where he was given electricity 4½ months.
January 1916, he went to Maison-Blanche under Laignel-Lavastine, where he received electrical treatment for 4½ months.
April 4 he went back to his dépôt.
April 4, he returned to his depot.
Presented to the invaliding board, May 11, at Decize, he was sent to the neurological center at Bourges. He was there given massage and movements. Upon entrance he had a functional inactivity of the right arm. He should have been cured a long time before by the therapeutics employed. He was then sent to Vincent at the neurological center at Tours for special motor reëducation. Vincent found almost complete functional incapacity of the right arm, without atrophy, with normal reactions, no R. D., and normal arterial[797] pressure. June 26, 1916, the patient was able to write, although slowly. He could sign a letter, and could lift a weight of 10 kilos.
Presented to the disability board on May 11 in Decize, he was sent to the neurological center in Bourges. There, he received massage and physical therapy. Upon arrival, he had no function in his right arm. He should have been treated effectively much earlier with the therapies used. He was then referred to Vincent at the neurological center in Tours for specialized motor rehabilitation. Vincent found that his right arm had nearly no function, but there was no muscle wasting, normal reflexes, no deep tendon reflexes, and normal blood pressure. By June 26, 1916, the patient was able to write, albeit slowly. He could sign his name and lift a weight of 10 kilograms.
The details of Vincent’s method mentioned under Case 566 are pursued, to use his own words, with methodical ruthlessness. This form of reëducation consists in manoeuvres that make the patients yield despite themselves. The galvanic current is used to force a man to react voluntarily or automatically. See, for example, Claude’s case of a hysterical brachial monoplegic (Case 574) found able to descend a ladder with the use of his arms only. After the physician’s victory is secured, then a sort of consolidation must be obtained by means of the execution of certain movements on the part of the patient for an hour or two. As another factor in the situation set up by Clovis Vincent, is the enthusiasm generated in the moral atmosphere in which the cure takes place. Mott has also insisted upon this atmosphere of cure, which Mott believes is in part responsible for the good results of Adrian and Yealland. Roussy and Boisseau, at Salins, started out with a process similar to that of Vincent, with a preliminary period of isolation. Roussy also uses the faradic current instead of the galvanic (see remarks of Mann concerning deaths with the Kaufmann method in Germany, under Case 570). Vincent’s three stages are given in Chart 19, page 897.
The details of Vincent’s method mentioned under Case 566 are followed, to use his own words, with methodical ruthlessness. This type of reeducation involves maneuvers that make the patients comply against their will. The galvanic current is used to compel a person to react either voluntarily or automatically. Take, for instance, Claude’s case of a hysterical brachial monoplegic (Case 574) who was able to descend a ladder using only his arms. Once the physician's victory is secured, a kind of consolidation must be achieved through the execution of specific movements by the patient for an hour or two. Another important aspect of the situation established by Clovis Vincent is the enthusiasm generated in the positive environment where the treatment occurs. Mott has also emphasized this healing atmosphere, which he believes partially accounts for the successful outcomes of Adrian and Yealland. Roussy and Boisseau, at Salins, began with a process similar to Vincent’s, starting with a preliminary isolation period. Roussy also employs the faradic current instead of the galvanic (see Mann's comments about deaths related to the Kaufmann method in Germany, under Case 570). Vincent’s three stages are outlined in Chart 19, page 897.
Struck by shell fragment; run over by shell; paresis and regionary sense disorder. Treatment by reëducation.
Struck by shell fragment; run over by shell; weakness and localized sensory disorder. Treatment through reeducation.
Case 575. (Binswanger, July, 1915.)
A German subaltern officer, 27, was wounded September 25, 1914, in a battle in France. He gave the following account:
A 27-year-old German junior officer was wounded on September 25, 1914, in a battle in France. He provided the following account:
“We had been firing without interruption four days, and then were sent back. While going back from cover we were under shell fire. Three or four horses fell. I got a glancing blow from a shell fragment in the back of the head, and fell down. I was not quite unconscious. I tried several times to get up, but I could not, for I had very bad pains in the head and a confused feeling in it, too. I remember also that a wheel ran over my foot, and that I got a sharp blow in the chest. Then I was unconscious for about an hour. When I awoke, there were two comrades busy over me and they pulled me back of the firing-line. Then I got to a field hospital.”
“We had been firing continuously for four days, and then we were ordered to fall back. While retreating from cover, we were under shell fire. Three or four horses went down. I took a glancing hit from a shell fragment at the back of my head and fell to the ground. I wasn’t completely unconscious. I tried several times to get up, but I couldn’t because of the severe pain in my head and a feeling of confusion. I also remember feeling a wheel run over my foot and getting a sharp hit in my chest. Then I lost consciousness for about an hour. When I came to, two comrades were working over me and they pulled me back from the front line. After that, I was taken to a field hospital.”
The man arrived at the nerve hospital (Jena), October 8, 1914, with insomnia, respiratory disturbance, sudden perspiration, feelings of cold in the right foot, and poor appetite. He had had nausea for a few days. Lungs and heart proved normal. X-ray of the right foot showed normal relations. The man was a small, powerfully-built man, well nourished, with lively reflexes, especially the knee reflexes, of which the right was greater than the left; slight patellar clonus, right; left plantar reflex greater than right; segmental disorder of touch and pain sense in the right foot and lower leg, a zone of analgesia lying above the zone of total anesthesia. Gait was lame on account of inability to move the right ankle joint. In walking, the right foot was trailed.
The man arrived at the nerve hospital in Jena on October 8, 1914, with insomnia, breathing problems, sudden sweating, a cold sensation in his right foot, and a poor appetite. He had been feeling nauseous for a few days. His lungs and heart were normal. An X-ray of his right foot showed normal alignment. The man was small but strongly built, well-nourished, and had quick reflexes, especially in his knees, with the right one being more responsive than the left; there was slight clonus in the right patella; the left plantar reflex was stronger than the right; he experienced a sensory disorder affecting touch and pain in his right foot and lower leg, with a zone of reduced sensitivity situated above an area of complete numbness. His gait was limping due to the inability to move the right ankle joint, and as he walked, the right foot dragged behind.
Treatment was suggestive and supported by active gymnastic exercises, breathing exercises, exercises in moving the right leg, massage, faradism and local hydrotherapy. The gait gradually improved, the cold feeling disappeared[799] from the right leg, disturbances of pain and touch sense disappeared. The patient was released on the 2d of February, 1915, capable of garrison duty.
Treatment involved suggestions along with active gym exercises, breathing exercises, exercises for moving the right leg, massage, faradism, and local hydrotherapy. The patient's gait gradually improved, the cold sensation in the right leg went away[799], and issues with pain and touch perception disappeared. The patient was discharged on February 2, 1915, ready for garrison duty.
With respect to this man, who was married, he was from a healthy family and had healthy children. He is said, however, to have suffered from convulsions for a long time in early life, but thereafter had never been sick in any way. He was a good student and had been a post-office official since 1908. After two years’ military service, he became, in 1910, Unteroffizier-Aspirant. Later he was advanced to his subaltern position in the reserve.
Regarding this man, who was married, he came from a healthy family and had healthy kids. It's said that he suffered from convulsions for a long time in his early years, but after that, he never got sick. He was a good student and had been a postal worker since 1908. After two years of military service, he became a Unteroffizier-Aspirant in 1910. Later, he was promoted to his reserve officer position.
This case seems to be a characteristic example of segmental disorder of sensations of both touch and pain, combined with a paresis in the same region. Mechanical and mental factors seem to have been present, and the case belongs in what Binswanger calls the “hysterosomatic” group.
This case appears to be a typical example of a localized disorder affecting sensations of both touch and pain, along with weakness in the same area. Both physical and psychological factors seem to have played a role, and this case fits into what Binswanger refers to as the “hysterosomatic” category.
Re Binswanger’s so-called hysterosomatic group, he defines the cases as having emotional, mechanical, and toxic (gas) factors. On the whole, they are best classified as a kind of psychoneurosis. Binswanger finds all physical and drug treatment without result except as supportives. He has used hydrotherapy and electrotherapy with the perfectly clear conception that the procedures were of suggestive value only. In fact, Binswanger had before defined such procedures as Realsuggestionen or material suggestions. Common verbal suggestion, says Binswanger, will work sometimes only when aided by these material suggestions. See also under Case 576.
Re Binswanger’s so-called hysterosomatic group defines these cases as having emotional, mechanical, and toxic (gas) factors. Overall, they are best categorized as a type of psychoneurosis. Binswanger finds that all physical treatments and medications are ineffective except as supportive measures. He has utilized hydrotherapy and electrotherapy, clearly understanding that these procedures are only suggestive in nature. In fact, Binswanger previously defined such procedures as Realsuggestionen or material suggestions. Common verbal suggestions, according to Binswanger, will occasionally work only when complemented by these material suggestions. See also under Case 576.
Post-traumatic (ANTEBELLUM) seizures with unconsciousness: Further seizures, astasia-abasia, anesthesias, following no special period of stress in field service. Recovery by reëducation.
Post-traumatic (ANTE-BELLUM) seizures with unconsciousness: Further seizures, inability to walk or stand, numbness, happening without a specific period of stress in field service. Recovery through rehabilitation.
Case 576. (Binswanger, July, 1915.)
O. F., 26, healthy, of a healthy family, in military service, 1908-1910, a miner in October, 1912, had fallen into a shaft from a considerable height, and is said to have been unconscious for three days and two nights and to have had some sort of attack a short time after waking. Later he had another attack, beginning with violent headaches, running from the back to the fore part of the head, then dizziness, then a fall with unconsciousness. The whole attack lasted about four minutes and was followed by feelings of extreme fatigue.
O. F., 26, healthy, from a healthy family, served in the military from 1908 to 1910. In October 1912, he fell into a mine shaft from a significant height and is reported to have been unconscious for three days and two nights, experiencing some kind of attack shortly after waking up. Later, he had another episode that started with intense headaches, moving from the back to the front of his head, followed by dizziness, and then collapsing with unconsciousness. This entire episode lasted about four minutes and was followed by extreme fatigue.
It seems that in the spring of 1913 these attacks had begun to repeat themselves two or three times a week. In the spring of 1914 there had again been two attacks at an interval of two weeks. They had occurred on the way to work and had been introduced by the same symptoms as before. They lasted about half an hour.
It seems that in the spring of 1913, these attacks started happening two or three times a week. In the spring of 1914, there were again two attacks spaced two weeks apart. They occurred on the way to work and began with the same symptoms as before. They lasted about half an hour.
He was in the war in France from August 6, 1914. While he was cooking, one day, in the middle of September, he had an attack and this without special occasion. The next attack occurred a little while afterwards, at the time of an assault. He said that he fell down and lost his senses. When he came to his senses again, he found he could not move his legs.
He was in the war in France starting August 6, 1914. One day in mid-September, while he was cooking, he had an attack for no particular reason. The next attack happened soon after, during an assault. He noted that he collapsed and lost consciousness. When he came to, he realized he couldn't move his legs.
He was taken to a reserve hospital in Germany, and while there had several attacks with unconsciousness and spasmodic convulsions—the last on December 7, 1914. He was transferred to the Jena Hospital on the 11th.
He was taken to a military hospital in Germany, where he experienced several episodes of unconsciousness and convulsive spasms—the last one occurring on December 7, 1914. He was moved to Jena Hospital on the 11th.
The Jena examination had the benefit of an inquiry concerning the case. It seems that he had left the field hospital in the enemy’s country, in a half-conscious condition, and rode away therefrom aimlessly. It was only in Germany[801] that he, on his own story, found his bearings again. However, upon admission the disturbance in walking was very noticeable, since the patient came hobbling through the garden of the clinic with the upper part of his body bent forward, and with the support of two canes. The legs were moved with difficulty; he seemed to take short, tripping steps, with the toes dragging on the ground. His inability to walk he explained through the violent pains which he would feel in the joints of the legs and an extraordinary weakness in his legs.
The Jena examination benefited from an investigation into the case. It turns out that he had left the field hospital in enemy territory in a half-conscious state and rode away aimlessly. It wasn't until he got to Germany[801] that, according to his own account, he started to regain his bearings. However, when he was admitted, it was very noticeable that he had trouble walking, as he came hobbling through the clinic's garden with his upper body bent forward and using two canes for support. He struggled to move his legs; his steps were short and unsteady, with his toes dragging on the ground. He attributed his difficulty walking to severe pain in the joints of his legs and an unusual weakness in them.
Physically, the man was a tall, strongly built and well-nourished subject. Neurologically, the knee-jerks were somewhat decreased and weaker on the right side than on the left; the Achilles reflexes were lively. The plantar reflex was not obtainable on the left side; decreased on the right. The abdominal reflexes were absent on both sides.
Physically, the man was tall, muscular, and well-fed. Neurologically, his knee-jerk reactions were somewhat reduced and weaker on the right side compared to the left; the Achilles reflexes were active. The plantar reflex couldn't be elicited on the left side and was diminished on the right. The abdominal reflexes were absent on both sides.
Most remarkable was the general diminution in sensitiveness of the skin to touch and pain, involving the whole body, up to the neck, where the sensory impairment abruptly ceased in a sharp line. The anesthesia was not everywhere complete. In a few places pencil strokes were successfully localized and recognized. Deep pin-pricks were everywhere recognized as itching. When the trunk was everywhere examined on both sides symmetrically, a strong pressure with a pin-head was felt as a strong pressure on the right side, but was felt not at all on the left side. Anesthesia and analgesia were total in the legs. Deep folds of skin could be punctured by needles without reaction.
The most notable change was the overall decrease in sensitivity of the skin to touch and pain, affecting the entire body up to the neck, where the loss of sensation suddenly stopped along a clear line. The numbness wasn't complete everywhere. In some areas, strokes from a pencil were still felt and identified. Deep pinpricks were always perceived as itching. When the torso was examined symmetrically on both sides, a strong pressure from a pinhead was felt intensely on the right side, but not at all on the left. Numbness and lack of pain were complete in the legs, where deep folds of skin could be pierced by needles without any response.
The legs could be moved freely upon urgent request with the patient in dorsal decubitus. Still these movements were slow and difficult, as explained by the patient, on account of violent pains in the joints. If put on his feet, he would begin to sway greatly and permit himself to slide down to the ground, stating that he was quite incapable of standing or walking without aid. With two canes, however, he could move freely about in the ward and in the garden, and even with considerable speed, in a peculiar, dragging, shuffling way; in the execution he gave no sign of pain, contentedly smoking a cigar or a pipe.
The legs could be moved freely upon urgent request with the patient lying on his back. Still, these movements were slow and difficult, as the patient described, due to severe pain in the joints. When he was put on his feet, he would start to sway a lot and would allow himself to slide down to the ground, saying that he was completely unable to stand or walk without help. However, with two canes, he could move freely around the ward and in the garden, even quite quickly, in a unique, dragging, shuffling manner; during this, he showed no sign of pain, happily smoking a cigar or a pipe.
While his status was being taken on admission, he became suddenly dull and irresponsive, with a staring look. He could not state his age or his birthplace. However, he became clear shortly, upon urging, and explained the spell by saying that the blood had risen to his head. A few days later, he was transferred to the psychiatric division. He was given strict rest in bed, smoking was forbidden, prolonged baths were used, and the legs were massaged. He felt very comfortable in the prolonged baths and could then move his legs without pain.
While they were taking his status on admission, he suddenly became dull and unresponsive, with a blank stare. He couldn’t say how old he was or where he was born. However, he came back to clarity shortly after, with some prompting, and explained that he felt lightheaded. A few days later, he was moved to the psychiatric division. He was ordered to rest quietly in bed, smoking was banned, he was given long baths, and his legs were massaged. He felt really comfortable in the long baths and was then able to move his legs without pain.
A few days later he was taken out of bed several times a day, the canes being removed immediately, and he was led about the day-room with the light support of two nurses. Being promised a cigar as a reward, he proved able to walk through the day-room supported by but one nurse. A week later the pains in walking exercises had disappeared. He had become able to walk alone, supporting himself lightly along the wall with one hand. Walking was still uncertain and slow.
A few days later, he was helped out of bed several times a day, with the canes taken away right away, and he was guided around the day room with the gentle support of two nurses. After being promised a cigar as a reward, he managed to walk through the day room with just one nurse’s assistance. A week later, the pain he felt during walking exercises was gone. He was able to walk on his own, lightly holding onto the wall with one hand. His walking was still unsure and slow.
December 20, the patient could stand free without support, swaying slightly; improvement became rapid. He could shortly stand and walk without support though his walk was still awkward and on a wide base with knees pressed in and body bent forward, soles were kept applied to the ground. December 22, the patient could walk in the garden without aid.
December 20, the patient could stand on his own, swaying slightly; the improvement was quick. He could soon stand and walk unaided, though his gait was still awkward with a wide stance, knees pushed in, and body leaning forward, keeping his feet flat on the ground. By December 22, the patient was able to walk in the garden without assistance.
December 23, there was a spell of great weariness and complaint of being sick. The patient lay down on the bed, cried aloud, and had rhythmic twitchings and sudden movements with arms and legs. He scratched the right half of his face with his right hand. This spell lasted about a minute. It was repeated in the same way twice within the half hour.
December 23, there was a period of extreme fatigue and complaints of feeling unwell. The patient lay down on the bed, cried out, and had rhythmic twitches and sudden movements of his arms and legs. He scratched the right side of his face with his right hand. This episode lasted about a minute. It happened in the same way two more times within the half hour.
He had complete amnesia for these attacks. The pupillary reactions were entirely normal in the attacks. He had been in bad spirits that day because a Christmas furlough had been refused. The attacks provoked no bad consequences and his gait improved. He was on furlough from the 30th to January 3; on the 4th he was transferred to the nerve department, but on the 12th of January he was reprimanded for a breach of discipline, whereupon at 9:15 he had[803] an hysterical attack with the same coördinate rhythmic motions as before. This attack lasted about 20 minutes. Two hours before the attack he had complained of weariness and a boiling-hot feeling in the body. Long walks were taken. On February 15 he began to feel very happy. He was informed that the charge against him for leaving his troop had been dropped. He complained of sudden weariness and headache and was markedly depressed, but he had no hysterical attack.
He had complete amnesia regarding these episodes. The pupil reactions were completely normal during the episodes. He had been feeling down that day because his request for a Christmas break was denied. The episodes caused no negative effects, and his walking improved. He was on leave from the 30th to January 3; on the 4th, he was moved to the nerve department, but on January 12, he was reprimanded for a disciplinary issue, and at 9:15, he had[803] a hysterical episode with the same coordinated rhythmic movements as before. This episode lasted about 20 minutes. Two hours before the episode, he complained of fatigue and a boiling-hot feeling in his body. He went on long walks. On February 15, he started feeling very happy. He was told that the charges against him for leaving his troop had been dropped. He complained of sudden fatigue and a headache and was noticeably depressed, but he did not have a hysterical episode.
After February 23 he took part regularly in gymnastics, executing the movements with joy and without special weariness. He wanted to be discharged. He was discharged as fit for garrison duty and he has since gone back to field service.
After February 23, he participated regularly in gymnastics, performing the exercises joyfully and without much fatigue. He wanted to be released. He was released as fit for garrison duty, and he has since returned to field service.
Re gymnastics, Binswanger holds that they have a special value in overcoming inner psychic resistances and weak-willed persons. The Realsuggestionen (see under preceding case, 575), such as hydrotherapy and electrotherapy, serve to concentrate the person’s attention on certain regions. These regional suggestions then smooth the way for the curative suggestion, namely, the constant and monotonously repeated assurance that recovery is advancing. At the next stage, according to Binswanger, gymnastic exercises may be brought in to overcome hopelessness, indifference, or exaggeration of morbid feelings. Binswanger sets methodical tasks for the attention and the will (a so-called Uebungstherapie). If these gymnastics lead to manifest improvement, then a proper educational therapy is prescribed, which is no longer a merely exercise therapy, but consists of actions of actual value in hospital routine. The convalescents are gradually led to carry on housework, food service, gardening (the latter under supervision). Hospital clerical work is a suitable occupation. Re supervision over gardening, mentioned by Binswanger, Canadian experience indicates that the idea of supervision may be greatly extended. Particularly is this true in vocational reëducation. Kidner describes the functions of a vocational counsellor, who has to have an expert knowledge of industry and methods of industrial training, as well as an acquaintance with the varying[804] demands for workers, a knowledge of the seasonal variations in employment, and a knowledge of occupational diseases. Re occupational therapy, Todd estimates that from 0.5 to 1 per cent of wounded men in France will require vocational reëducation. Occupational therapy is the proper vestibule to vocational training. He lists the following forms of treatment used in institutions for vocational reëducation:
Regarding gymnastics, Binswanger believes they have a unique value in overcoming inner psychological barriers and helping individuals who are weak-willed. The Realsuggestionen (see under preceding case, 575), such as hydrotherapy and electrotherapy, aim to focus a person’s attention on specific areas. These regional suggestions then pave the way for the therapeutic suggestion, which is the ongoing and monotonous reassurance that recovery is progressing. At the next stage, based on Binswanger’s view, gymnastic exercises can be introduced to combat feelings of hopelessness, indifference, or exaggerated negative emotions. Binswanger assigns methodical tasks for attention and will (this is referred to as Uebungstherapie). If these exercises lead to noticeable improvement, then a proper educational therapy is recommended, which goes beyond mere exercise therapy to include meaningful activities within hospital routines. Patients are gradually encouraged to engage in housework, food service, and gardening (the latter under supervision). Hospital clerical work is also an appropriate activity. Regarding gardening supervision, as noted by Binswanger, Canadian experience suggests that the notion of supervision can be significantly broadened. This is especially true in vocational retraining. Kidner outlines the role of a vocational counselor, indicating that they should possess expert knowledge of industry and training methods, as well as familiarity with the varying demands for workers, seasonal employment changes, and knowledge of occupational diseases. Concerning occupational therapy, Todd estimates that 0.5 to 1 percent of wounded soldiers in France will need vocational retraining. Occupational therapy serves as a proper introduction to vocational training. He lists the following forms of treatment used in institutions for vocational retraining:
- Active mechanotherapy.
- Passive mechanotherapy.
- Galvanic, static, and faradic electricity.
- Vibration.
- Hot air baths and blasts.
- Water baths.
- Colored light.
- Massage.
- Gymnastics.
Central specialized institutions such as those developed in France are necessary, and such centres should be large rather than small, according to Todd, and should contain not less than 200 beds. Todd insists that work is, after all, the most important measure of reëducation; and Turner, speaking of the home for neurasthenics at Golders Green, says that during a period of three months (the number of the patients is limited to 100, and three months is the limit of stay), the vast majority, even of the most obstinate cases, get well through the effects of sympathy and insistance upon work. Near Golders Green is the Maida Vale Hospital for nervous cases, so that in case of need the physicians there may treat the patients. Salmon gives a list of the occupations which are suitable for these cases.
Central specialized institutions like those established in France are essential, and these centers should be larger rather than smaller, according to Todd, and should have at least 200 beds. Todd emphasizes that work is, ultimately, the most crucial factor in rehabilitation; and Turner, referring to the home for neurasthenics at Golders Green, notes that during a three-month period (the number of patients is limited to 100, and three months is the maximum stay), the vast majority, even among the most stubborn cases, recover due to the effects of support and a focus on work. Nearby Golders Green is the Maida Vale Hospital for nervous cases, so that in an emergency, the doctors there can provide care for the patients. Salmon provides a list of occupations that are suitable for these cases.
Blown up by shell; wounds, right side, distention and bloody urine: Paresis of right foot and spasticity of hip; later rectal and bladder incontinence.
Blown up by shell; wounds on the right side, swelling and bloody urine: Weakness in the right foot and stiffness in the hip; later developed rectal and bladder incontinence.
Case 577. (Binswanger, July, 1915.)
A Russian from the Ukraine was received at the nerve hospital, Jena, December 12, 1914. Through an interpreter it was established that he was a peasant, had been under shell fire in a skirmish at the beginning of November, and had been hurled (so he said) 1¼ meters into the air without loss of consciousness. There was a wound of the right shoulder and also, he thought, of the legs, from the air pressure. Becoming a German prisoner, he had been treated in various hospitals.
A Russian from Ukraine arrived at the nerve hospital in Jena on December 12, 1914. An interpreter confirmed that he was a farmer, had been exposed to shell fire during a skirmish at the start of November, and claimed to have been thrown 1¼ meters into the air without losing consciousness. He had an injury to his right shoulder and also thought there was an injury to his legs due to the air pressure. After becoming a German prisoner, he had been treated in several hospitals.
He was a strong man of medium height, with a healthy complexion. There were two healed wounds of the right shoulder, and near the twelfth spinous process a third similar scar. There were a number of ulcers and furuncles over the os sacrum.
He was a strong man of average height, with a healthy complexion. He had two healed wounds on his right shoulder, and near the twelfth spinous process was a similar scar. There were several ulcers and boils on his tailbone.
Neurologically, the knee-jerks and Achilles jerks could not be obtained, and the plantar reflex, extinct on the left, was weak on the right. Sensitiveness to pain on both sides was lost from the knee downwards but there was hyperalgesia in the thigh. Inaccurate statements in response to tactile tests were made, apparently on account of lack of understanding. In lying down, there was a slight restriction in the movements of the legs, and active movements of the joints of the foot on the right side were impossible. Gait was ataxic-paretic, more markedly so right than left. He could walk only with two canes, and during walking the musculature of the thigh fell into a spastic tension. The tongue deviated to the left. There were severe rheumatic pains in the thighs.
Neurologically, the knee-jerk and Achilles reflexes were absent, and the plantar reflex was nonexistent on the left side and weak on the right. Sensitivity to pain was lost from the knees down, but there was increased sensitivity in the thigh. The responses to tactile tests were inaccurate, likely due to a lack of comprehension. When lying down, there was a slight limitation in the movement of the legs, and active movement of the right foot joints was not possible. The gait was unsteady and weak, more so on the right than the left. He could only walk with the help of two canes, and while walking, the thigh muscles tensed up spastically. The tongue shifted to the left, and he experienced severe pain in the thighs due to rheumatism.
It appears that some weeks before, this Russian soldier had suffered from severe rheumatic pains in both sides and was at that time absolutely unable to walk or stand. At that time, however, there was no question of a crural paraplegia of organic origin, since the man could move his legs[806] well enough when in dorsal decubitus. There were no signs of paralysis of the rectum or bladder at that time.
It seems that a few weeks earlier, this Russian soldier had been experiencing intense rheumatic pain on both sides and was completely unable to walk or stand. However, at that time, there was no indication of an organic crural paraplegia, as he could move his legs fairly well while lying on his back. There were no signs of paralysis in the rectum or bladder at that moment.
Treatment at Jena consisted in regular walking exercises with support at the shoulders. The lower legs and feet remained weak and paretic. The decubital ulcers disappeared.
Treatment at Jena involved regular walking exercises with support at the shoulders. The lower legs and feet stayed weak and partly paralyzed. The bedsores went away.
About the middle of December rectal incontinence began, the stool being discharged without the patient’s noticing it while being led to the bath. Later there was incontinence of feces in bed. Pains in the legs were constantly complained of. Nevertheless improvement in walking was maintained. The toes were dragged at every step and the knee-joints were thrown outward in walking. The musculature of the lower legs was weak. Knee-jerks could not be elicited more than before. He constantly complained of pains in the knees and right hip. The rectal disorder did not again occur during January.
About mid-December, the patient started experiencing rectal incontinence, with stool being released without their notice while being taken to the bathroom. Later, there was fecal incontinence in bed. The patient frequently complained of leg pain. However, there was still some improvement in walking. The toes were dragged with every step, and the knees were positioned outward when walking. The muscles in the lower legs were weak. Knee reflexes could not be triggered more than before. The patient continuously reported pain in the knees and right hip. The rectal issue did not reappear in January.
Toward the close of January, the patient’s right lower leg and left foot would occasionally feel asleep; both legs felt cold and itched. In a general way, however, the pains had become less marked than they were at first. It seemed that he had no sensations at stool, and consequently had to resort to the closet at a definite time. Moreover, urine was discharged irregularly and involuntarily when he coughed. It appears that a few days after receiving his wounds in battle, there had been pains on micturition as well as blood in the urine, and it appears that he had been catheterized. It is probable that he had suffered from distention, as he described his abdomen, thighs and sex organs as swollen.
Toward the end of January, the patient’s right lower leg and left foot would occasionally feel numb; both legs felt cold and itchy. Overall, however, the pain was less severe than it had been initially. He seemed to have no sensation during bowel movements and had to go to the bathroom at specific times. Additionally, urine was discharged irregularly and involuntarily when he coughed. It appears that a few days after getting wounded in battle, he experienced pain while urinating as well as blood in the urine, and it seems he had to be catheterized. It’s likely that he suffered from swelling, as he described his abdomen, thighs, and genital area as enlarged.
In February he began to be able to move alone with two canes through the ward, but he moved his legs from the knee downward very little, and dragged them after the rest of the body. Upon galvanic examination, the peroneal and tibial nerve trunks were found normally excitable. At this time the sensibility situation had changed somewhat, since complete analgesia was present only in the foot, and hypalgesia had developed upon the anterior surfaces of the lower legs. Pin-pricks were described as touches. The posterior surface of the left lower leg was normally sensitive. There was an oblong stripe about 3 cm. long, beginning in the popliteal[807] space and stretching downward on the left side. The right lower leg was entirely insensitive. The posterior surfaces of both thighs as far as the gluteal folds were completely insensible to pain. The Wassermann reaction of the blood was negative. In this condition the patient was transferred to a prison camp hospital.
In February, he started to be able to move independently with two canes around the ward, but he hardly moved his legs from the knee down and dragged them after the rest of his body. During a galvanic examination, the peroneal and tibial nerve trunks were found to be normally excitable. At this point, the sensitivity situation had changed somewhat, as complete numbness was only present in the foot, and reduced sensitivity had developed on the front surfaces of the lower legs. Pin pricks felt like touches. The back of the left lower leg was normally sensitive. There was a long stripe about 3 cm. long, starting in the popliteal[807] space and extending downward on the left side. The right lower leg was entirely numb. The backs of both thighs, up to the gluteal folds, were completely insensible to pain. The Wassermann reaction of the blood was negative. In this condition, the patient was transferred to a prison camp hospital.
Re bloody urine, see Section B, Case 202. Re rectal incontinence, it might be inquired whether this was possibly functional. Roussy and Lhermitte devote a chapter to visceral disorders. They do not list rectal incontinence amongst the disorders noted in this war, nor have any cases of hysterical anorexia or disorders of sensation in the intestinal tract been seen during the war despite the occurrence of these latter disorders in the civilian group. The main digestive disorder that the war cases show is vomiting (see Cases 495 and 500).
Regarding bloody urine, see Section B, Case 202. Regarding rectal incontinence, it may be worth asking if this was possibly functional. Roussy and Lhermitte focus a chapter on visceral disorders. They do not mention rectal incontinence among the disorders noted in this war, nor have there been any cases of hysterical anorexia or sensory disorders in the intestinal tract during the war, even though these latter disorders have been seen in the civilian group. The main digestive disorder observed in war cases is vomiting (see Cases 495 and 500).
Emotionality: Shell explosion; mutism. Recovery by reëducation.
Emotionality: Shell explosion; silence. Recovery through re-education.
Case 578. (Briand and Philippe, September, 1916.)
A plumber, 27, went into the infantry. He was very emotional and was but a short time in the trenches when the explosion of shells threw him into a state of mutism. Deafness, rather curiously, did not manifest itself for several days. He had to go back on horseback, and, as he was a poor horseman, slipped off the horse, giving himself a bad fright. When he got up, he had lost his hearing.
A 27-year-old plumber joined the infantry. He was very emotional and had only been in the trenches for a short time when a shell explosion left him mute. Interestingly, he didn't lose his hearing for several days. He had to return on horseback, and since he wasn't a good rider, he fell off the horse, which scared him badly. When he got up, he realized he had lost his hearing.
He was sent to several hospitals and finally to Val-de-Grâce, in July, 1915. He recovered hearing in fifteen days, but the mutism persisted several months. According to Briand and Philippe, this is a typical case, except for the duration of the mutism. The first treatment was given this patient August 6. His respiration was examined and tracing was taken. August 15, on the morning visit, he was found able to whistle very distinctly the first bars of “Au Clair de la Lune,” and then began to sing the first verses, articulating distinctly, but stammering a little. He was now left to his own resources, without special exercises, from August 15 to September 26, and completely lost the benefit of his previous exercises. A week of special treatment allowed him to recover speech again, enough to take up every day life. The patient went out well.
He was sent to several hospitals and finally to Val-de-Grâce in July 1915. He regained his hearing in fifteen days, but the inability to speak lasted several months. According to Briand and Philippe, this is a typical case, except for how long the mutism lasted. The first treatment for this patient was given on August 6. His breathing was examined and a tracing was taken. On the morning visit of August 15, he was found able to clearly whistle the first notes of "Au Clair de la Lune," and then began to sing the first verses, articulating clearly but stammering a bit. From August 15 to September 26, he was left to his own devices, without special exercises, and completely lost the benefits of the previous exercises. A week of special treatment allowed him to regain his speech enough to resume daily life. The patient left in good spirits.
The general lines of the examination in this case took up attitude in abdominal respiration and the question of respiratory pauses, especially pauses in abdominal respiration, which, in the above case, were exaggerated. Expiration was deficient and disordered. The normal adaptations that had been established during his childhood learning of speech had failed, and the patient would not have been able by himself to regain proper balance of respiration for speech.
The main points of the examination in this case focused on the way the patient breathed using their abdomen and the issue of breathing pauses, particularly those in abdominal breathing, which were excessive in this situation. The exhalation was insufficient and irregular. The normal adjustments that had formed during his childhood speech development were not working, and the patient wouldn't have been able to restore proper respiratory balance for speech on his own.
The examination was continued to learn the difficulties of innervation of the muscles of phonation whose proper delicacy had been lost. Such a patient is a kind of bad gymnast,[809] executing an exercise known to be hard by contracting all the muscles of the region, both the antagonist and the agonist muscles. Reëducation must, therefore, endeavor to sweep away the contractions that block sound. Then the patient must be made to perform the contractions necessary in phonation and articulation unconsciously. The methods used for teaching children might here be employed, but more elaborate and designed methods can be used with the adult, e.g.,
The examination continued to explore the issues with the nerve connections of the vocal muscles, which had lost their proper sensitivity. Such a patient is like a poor gymnast, [809], trying a difficult routine by tensing all the muscles in the area, both the opposing and the primary muscles. Rehabilitation must, therefore, aim to eliminate the tension that hinders sound production. Then, the patient needs to practice the necessary muscle contractions for speaking and articulation without being aware of it. Techniques used to teach children could be applied here, but more advanced and tailored methods can be utilized for adults, e.g.,
1. Breathing exercises, especially with the idea of making respiration complete.
1. Breathing exercises, especially with the goal of making breathing complete.
2. Blowing exercises.
2. Breathing exercises.
3. Whistling.
Whistling.
4. Vowel sounding.
4. Vowel pronunciation.
Séguin and Rouma, on the other hand, counsel beginning exercises with consonants in stammerers and dyslalics.
Séguin and Rouma, on the other hand, recommend starting exercises with consonants for people who stutter and have speech sound disorders.
Re tests for functional deafness, Ranjard states that on account of the complexity of Shell-shock deafness, exact diagnosis needs to be made. Examination of the hearing by speech alone, or by the watch-tick, yielded poor results; and an accurate mathematical acoumeter (Sirène à voyelles, Marage) is recommended. See especially chapter on the functional examination of audition in Bourgeois and Sourdille’s War Otitis and War Deafness, a work translated and highly recommended by the English otologist, Dundas Grant.
Re tests for functional deafness, Ranjard states that due to the complexity of Shell-shock deafness, a precise diagnosis is necessary. Testing hearing through speech alone or by listening to a ticking watch produced unsatisfactory results; therefore, an accurate mathematical acoumeter (Sirène à voyelles, Marage) is suggested. See especially the chapter on the functional examination of hearing in Bourgeois and Sourdille’s War Otitis and War Deafness, a work that has been translated and is highly recommended by the English otologist, Dundas Grant.
Three days’ skirmish on East front: Unconsciousness, later delirium, still later (six weeks) stammering, hysterical stigmata: Recovery by isolation and reëducation.
Three days of fighting on the East front: Unconsciousness, then delirium, later (six weeks) stuttering, hysterical symptoms: Recovery through isolation and re-education.
Case 579. (Binswanger, July, 1915.)
A traveling salesman in civil life, 36, as a non-commissioned officer took part in severe fighting in the East shortly after the outbreak of the war. He was under violent shell fire at one time for five hours at a stretch. In the middle of November, after a skirmish in the woods which had lasted for three days, he was found unconscious. According to his own story, he was awakened from this unconsciousness about a week later in a hospital. He described himself as quite unable to say anything about what had gone on during that week.
A traveling salesman in civilian life, 36, served as a non-commissioned officer and took part in intense fighting in the East shortly after the war began. At one point, he endured heavy shelling for five hours straight. In mid-November, after a three-day skirmish in the woods, he was discovered unconscious. According to his account, he woke up about a week later in a hospital and said he couldn't remember anything about what happened during that week.
The medical report on the case stated that he arrived at the hospital, November 18, in a dormant state of mind. He had appeared markedly excited and kept incessantly talking about military matters, such as the placing of machine guns, the occupation of the edge of the woods by his company, addressing the nurse as “Captain,” and the sister as “Mrs. Captain,” making as it were an official report to them. He showed shyness, and always an extreme excitement. His hands and legs were in constant motion; he complained of headaches and itching finger-tips. Sleep could be achieved only by drugs. This mental state lasted till November 26, when he became oriented. Sleep improved, but he complained of pains in the back of the head.
The medical report on the case noted that he arrived at the hospital on November 18, in a mentally dormant state. He had seemed extremely agitated and was constantly talking about military topics, like positioning machine guns, the occupation of the edge of the woods by his unit, addressing the nurse as “Captain,” and the sister as “Mrs. Captain,” almost as if he were giving them an official report. He exhibited shyness and a high level of excitement. His hands and legs were always in motion; he reported headaches and itching fingertips. Sleep could only be achieved with medication. This mental state lasted until November 26, when he became oriented. Sleep improved, but he continued to complain of pain in the back of his head.
Upon transfer to a convalescent home, December 5, he was still occasionally excited and sometimes sleepless. On December 30, the patient began to stammer; his speech had before this been somewhat difficult, but the stammering began suddenly; speech was indistinct and slow; syllables failed to follow one another at like intervals. The headache at this time radiated from the middle of the top of the head to the side of the neck. There was a complaint of[811] vibrating pains on the two sides of the vertebral column, and a feeling of weakness and unsteadiness in walking. The patient would sway with eyes closed and turn sidewise. The heart action was tumultuous, the pulse irregular and uneven.
Upon moving to a rehabilitation center on December 5, he was still occasionally agitated and had trouble sleeping. By December 30, the patient started to stutter; his speech had previously been somewhat difficult, but the stuttering appeared suddenly; his speech was unclear and slow, with syllables not following one another at regular intervals. At this time, his headache radiated from the center of the top of his head to the side of his neck. He complained of[811] vibrating pain on both sides of his spine, along with feelings of weakness and unsteadiness while walking. He would sway with his eyes closed and turn sideways. His heart was racing, and his pulse was irregular and uneven.
The patient was transferred back to the reserve hospital on January 2, 1915, whereupon the stammering became worse, sleep restless, and arms and legs subject to spasmodic pains and twitching. On January 25, he was removed to the Jena Hospital. He remarked that at the convalescent home he became very much excited at the Christmas celebration and had to cry, whereupon his speech became more and more difficult; he could not find the beginnings of words and had to stammer. Upon admission he also complained of sharp pains in the soles of the feet and in the finger-tips.
The patient was transferred back to the reserve hospital on January 2, 1915, where his stammering worsened, sleep became restless, and he experienced spasms and twitching in his arms and legs. On January 25, he was moved to the Jena Hospital. He mentioned that during his time at the convalescent home, he became very excited during the Christmas celebration and started to cry, which made his speech increasingly difficult; he struggled to find the beginnings of words and began to stammer. Upon admission, he also complained of sharp pains in the soles of his feet and in his fingertips.
Neurologically, there was marked dermatographia, the deep reflexes were increased, abdominal reflexes were absent; there were points of pain on pressure in both supra-orbital regions, and there was a general hypalgesia with the exception of the head, the lower legs, the feet, the scrotum, the penis and the anal region. Pin-pricks were recognized on the right side only, when the patient was tested bilaterally. They could be recognized on both sides when the patient was examined on one side at a time. There was a static tremor on both sides (?). He could move his arms, but in dorsal decubitus he could move his legs only jerkily and uncertainly. His gait was waddling with dragging of toes.
Neurologically, there was significant skin writing, the deep reflexes were heightened, and abdominal reflexes were absent; there were painful spots on both supra-orbital areas, and there was overall reduced sensitivity except in the head, lower legs, feet, scrotum, penis, and anal area. Pin-prick sensations were felt on the right side only when the patient was tested on both sides. However, he could feel them on both sides when examined one side at a time. There was a noticeable tremor on both sides (?). He could move his arms, but when lying on his back, he could only move his legs in a jerky and unsteady manner. His gait was unsteady with a toe-dragging motion.
There was a marked photophobia. The palatal and swallowing reflexes were in excess; speech was hesitant and stammering. The first letters of words, especially initial consonants, could be pronounced with difficulty, explosively with cheeks blown up, after several attempts. The consonant would be repeated several times before the vowel could be added. The patient’s name was Singer, and he would pronounce it: S … S … S … Si … n … n … ger; the last syllable (ger) being brought out with a strong accentuation. The whole process took five seconds. The word Flanelllatten took 14 seconds. It seems that the patient had already suffered (in 1907) from nasal catarrh and disturbance of hearing from stoppage of the Eustachian tubes. Another[812] attack in 1908 had been accompanied by an irritating cough, and there seems to have been catarrh on the right in 1913, as well as cerumen on the left side.
There was a noticeable sensitivity to light. The reflexes for swallowing and the roof of the mouth were overactive; speech was slow and stuttered. The first letters of words, especially the initial consonants, were difficult to pronounce, often resulting in explosive sounds with puffed cheeks after multiple attempts. The consonant would be repeated several times before a vowel could be added. The patient's name was Singer, and he would say it: S … S … S … Si … n … n … ger; with the last syllable (ger) emphasized strongly. The entire process took five seconds. The word Flanelllatten took 14 seconds. It appears that the patient had already experienced (in 1907) nasal congestion and hearing issues due to blocked Eustachian tubes. Another[812] attack in 1908 was marked by an annoying cough, and there seems to have been congestion on the right side in 1913, along with earwax on the left side.
Treatment: The patient was isolated; in the next few days there was improvement in the headache. The patient complained of muscular twitchings, which would occur suddenly in different parts of the body. On February 1 there was a subjective feeling of happiness since all pains had disappeared.
Treatment: The patient was isolated; in the next few days, the headache improved. The patient complained of muscle twitches that would suddenly happen in different parts of the body. On February 1, there was a sense of happiness since all pain had gone away.
The patient was given regular exercises in speaking and there was gradual improvement in speech. Body-weight increased, regular walks were taken, and the patient occupied himself with garden work.
The patient was given regular speech exercises, and there was gradual improvement in their speech. Their body weight increased, they took regular walks, and the patient kept busy with gardening.
By June, 1915, he had still further remarkably improved, working now all day long, partly in the garden, partly in the hospital office. Disturbance of speech was not noticed except for hesitation before the last syllables of long words during comparatively long conversations. All trace of difficulty in walking had disappeared. In this patient no hereditary taint could be proved. He appears to have been of normal development, serving in the army from 1901 to 1903. In his life as a traveling salesman, there was frequently catarrh of the throat, and in 1912 there was a marked swelling of the vocal cords with extreme hoarseness and inability to speak, which condition was cured after local treatment.
By June 1915, he had made remarkable improvements, now working all day, partly in the garden and partly in the hospital office. There was no noticeable speech disturbance except for some hesitation before the last syllables of long words during relatively long conversations. All signs of difficulty in walking had vanished. In this patient, no hereditary issues could be proven. He appeared to have developed normally, serving in the army from 1901 to 1903. In his life as a traveling salesman, he often had throat issues, and in 1912, he experienced significant swelling of the vocal cords, leading to extreme hoarseness and loss of speech, which was resolved after local treatment.
Re hysterical speech and voice disorders, Binswanger has found them amongst the most obstinate conditions, often persisting when all other hysterical phenomena have dropped away. He states that apparently the cure of some of these cases must be postponed until the end of the war.
Re hysterical speech and voice disorders, Binswanger has found them to be among the most stubborn conditions, often continuing even after all other hysterical symptoms have disappeared. He notes that it seems the treatment for some of these cases will have to wait until after the war ends.
Re general results of the therapeutic treatment of the war hysterias, Binswanger states that he has been able to send some cases back to the front that have successfully stayed there. He has had failures, however, even amongst men who have had no mauvaise volonté and have themselves desired to be sent back to the front.
Re general results of the therapeutic treatment of war hysterias, Binswanger states that he has been able to send some cases back to the front that have successfully stayed there. He has had failures, however, even among men who have had no mauvaise volonté and have themselves desired to be sent back to the front.
Gordon Wilson observed 250 cases of Shell-shock at the Ypres salient and on the Somme. Fifty of these cases complained of deafness, and 17 of the 50 were found to have[813] actual nerve deafness. Wilson treated “fixed idea” cases by hypnotism, and sometimes by cold water run into the ear. He, in general, divides the cases in to (a) cases of nerve deafness, (b) fixed idea cases, and (c) malingerers.
Gordon Wilson observed 250 cases of shell shock at the Ypres salient and on the Somme. Fifty of these cases reported deafness, and 17 of the 50 were found to have[813]actual nerve deafness. Wilson treated "fixed idea" cases through hypnotism and sometimes by using cold water poured into the ear. He generally categorizes the cases into (a) nerve deafness cases, (b) fixed idea cases, and (c) malingerers.
Marage states that frequent exposure to the noise of shells for long periods may produce a permanent deafness, as has long been known in naval gun-makers and boiler-makers in peace times. He advocates obturators, a good form being plasticine wrapped in gauze moulded to the shape of the internal meatus. Celluloid plugs, sometimes used, have been known to be set afire by the flash of a shell. Cerumen sometimes protects against deafness, but Mott speaks of the driving of the wax into the tympanum as a dangerous effect in certain shock cases.
Marage says that being exposed to the noise of shells for long periods can lead to permanent hearing loss, a fact that's been well-known among naval gun-makers and boiler-makers during peacetime. He recommends using obturators, with one effective type being plasticine wrapped in gauze shaped to fit the ear canal. Celluloid plugs, which are sometimes used, have been known to catch fire from the flash of a shell. Earwax can sometimes protect against hearing loss, but Mott warns that in certain shock cases, the wax can be pushed into the eardrum, which is dangerous.
BURIAL by shell explosion: DEAFMUTISM. Treatment: phonetic reëducation.
BURIAL by shell explosion: DEAFMUTISM. Treatment: phonetic re-education.
Case 580. (Liébault, 1916.)
A machine gunner, 26, was buried at Rheims, January 5, 1915, by the explosion of a large shell bursting over the dugout. He was unconscious three days and deafmute on coming to, without amnesia but with a feeling of constriction in the throat.
A 26-year-old machine gunner was buried at Rheims on January 5, 1915, when a large shell exploded above the dugout. He was unconscious for three days and was deaf and mute when he came to, without memory loss but with a tight feeling in his throat.
After fifteen days in the ambulance he was sent for four months to the Maritime Hospital at Brest, and treated by hypnotism. Seven or eight sittings had no other result than to fatigue him. There were then three months of convalescence. Returned to Vannes, September 20, 1915, he was put into the auxiliaries. As he could not work much he was sent, December, 1915, to the Hôtel-Dieu at Nantes. Here electric vibratory massage was given, which secured a few hoarse sounds.
After fifteen days in the ambulance, he was sent to the Maritime Hospital in Brest for four months and treated with hypnosis. Seven or eight sessions only managed to tire him out. Then there were three months of recovery. He returned to Vannes on September 20, 1915, and was placed in the auxiliaries. Since he couldn't do much work, he was sent to the Hôtel-Dieu in Nantes in December 1915. There, he received electric vibratory massage, which produced a few hoarse sounds.
Phonetic reëducation was then undertaken at Prés-à-goutrière, May 10, and his respiratory capacity increased from 170 the first week to 250 and 300 the following weeks. His blowing strength was raised from 15 to 20 to 25 at the same time. In a few weeks he was much improved and June 27 passed on to his auditory reëducation. The respiratory capacity in this man was insufficient. He could not speak, but his respiratory movements were good and he learned again to speak in a voice as good as ever.
Phonetic re-education was then started at Prés-à-goutrière on May 10, and his breathing capacity increased from 170 in the first week to 250 and then 300 in the following weeks. His blowing strength improved from 15 to 20 to 25 during the same time. In just a few weeks, he showed significant improvement and on June 27, he moved on to his auditory re-education. This man’s breathing capacity was insufficient. He couldn’t speak, but his breathing movements were strong, and he learned to speak again in a voice just as good as ever.
According to Liébault, it is a general principle that, if the respiratory capacity is increased, the voice will clear or become better; but, if the respiratory capacity remains stationary, the voice will not improve. It is the same with normal persons. A subject with a very subnormal respiratory capacity cannot speak loudly, but, if his respiratory capacity approaches normal, he can speak normally. According to Liébault, all cases of this sort have had some respiratory anomaly and each case must be systematically examined with the aid of anthropometric tables, including[815] weight, height and chest capacity. The vocal disorder is proportionate to the degree of functioning of the phonating apparatus taken as a whole. It is not merely that the larynx should be examined, but the motor side of the apparatus, the respiratory muscles, the resonating apparatus, the lips, the mouth, the nasal fossæ and the pharynx.
According to Liébault, a general rule is that if someone's lung capacity increases, their voice will become clearer or improve; however, if their lung capacity stays the same, their voice won’t get better. This applies to normal people too. A person with significantly low lung capacity can’t speak loudly, but as their lung capacity gets closer to normal, they can speak normally. Liébault states that all cases like this have some respiratory issue, and each case needs to be thoroughly examined using anthropometric tables, which include weight, height, and chest capacity. The vocal problem relates to how well the entire phonation system works. It’s not just about checking the larynx; the muscles that help with breathing, the resonating system, the lips, the mouth, the nasal passages, and the throat also need to be evaluated.
Re curability of different types of war deafmute, Roussy and Boisseau maintain that the type (a) that comes gesticulating, pointing to the ears, and desirous of writing, is the type that responds most rapidly to psychotherapy. There are two other types less responsive: (b) is an apathetic type, with impassive and stupid facies, lies immobile in bed, or sits in a chair in mental confusion; type (c) shows a facies of terror, looks haggard and anxious, confused, disoriented, and possibly delirious.
Re curability of different types of war deafmute, Roussy and Boisseau argue that the type (a) that comes gesticulating, pointing to the ears, and eager to write is the type that responds most quickly to psychotherapy. There are two other types that are less responsive: (b) is an apathetic type, with an indifferent and blank expression, lying motionless in bed or sitting in a chair in mental confusion; type (c) has a look of terror, appears haggard and anxious, confused, disoriented, and possibly delirious.
Re general treatment of deaf cases, Zange suggests that emotion should not be aroused by intense auditory impressions, that he should not be reminded of his shock, and should be kept as cheerful as possible. Zange states that he found the static electric current of service, and got good results in hysterical deafness of sudden development by applying a strong faradic current.
Re general treatment of deaf cases, Zange suggests that intense sounds shouldn't provoke strong emotions, that reminders of his shock should be avoided, and that he should be kept as upbeat as possible. Zange mentions that he found static electric current helpful and achieved good results in cases of sudden hysterical deafness by applying a strong faradic current.
A year’s service; leave: Hysterical aphonia developed at home. Respiratory gymnastics.
A year of service; leave: Hysterical voice loss started at home. Breathing exercises.
Case 581. (Garel, April, 1916.)
A soldier, 35, went on leave August, 1915. Arriving at his farm, he had a violent feeling of moral perturbation and suddenly lost his voice. When he returned from leave he seemed stupid, spoke very few words and seemed to look about in a vague and undecided way. He was several months in this state and sent January, 1916, to Saint-Luc.
A 35-year-old soldier went on leave in August 1915. When he got to his farm, he experienced a strong sense of moral confusion and suddenly lost his voice. Upon returning from leave, he seemed dull, spoke very few words, and looked around in a vague, uncertain manner. He remained in this state for several months and, in January 1916, was sent to Saint-Luc.
The vocal cords were there found of a normal color and without paralysis. “It was, therefore,” remarks Garel, “a nervous aphonia susceptible of instantaneous cure.” The patient was made to make a sound in the lowest tone possible. While he was making this attempt, sharp pressure was exerted upon the lower part of the sternum, to provoke expiratory reinforcement. The sound emitted was loud, to the great astonishment of the patient, who, thus aided by suggestion, shortly began to talk aloud.
The vocal cords were found to be a normal color and without paralysis. “It was, therefore,” notes Garel, “a nervous aphonia that could be instantly cured.” The patient was asked to make a sound at the lowest tone possible. While he attempted this, firm pressure was applied to the lower part of the sternum to encourage expiratory support. The sound produced was loud, to the great surprise of the patient, who, with this encouragement, soon began to speak out loud.
In this particular patient a temporary return of voice was readily obtained, but not maintained. Special exercises had to be instituted, whereupon the patient immediately fell back into a complete aphonia. He was then made to scan words, syllable by syllable, executing with his arms classical movements of respiratory gymnastics, or sometimes with the utterance of every syllable the epigastrium was manually compressed or the shoulders suddenly lowered. The patient could now read a book in a jerky manner, and after a few lines he could read without his shoulders being pressed.
In this particular patient, a temporary return of voice was easily achieved, but it wasn’t sustained. Specific exercises had to be started, and right away, the patient completely lost his voice again. He was then instructed to sound out words, syllable by syllable, while performing classical breathing exercises with his arms, or sometimes, as he pronounced each syllable, his stomach was manually pressed or his shoulders were suddenly lowered. The patient could now read a book in a choppy way, and after a few lines, he was able to read without his shoulders being pressed.
Another plan was to have the man read or talk while walking. As soon as he was stopped and accosted, however, he lost his voice again. Up to the time of report it was impossible to secure a definite return of voice, as the patient was not willing to associate words with peculiar movements. It might make him ridiculous. Accordingly, the nurses were requested not to fulfil requests unless they were made aloud. Recovery was to be hoped for from this measure.
Another plan was to have the man read or talk while walking. However, as soon as he was stopped and approached, he lost his voice again. Up until the time of the report, it was impossible to get a clear return of his voice because the patient didn't want to connect words with specific movements. It might make him look silly. So, the nurses were asked not to fulfill requests unless they were made out loud. Recovery was hoped for from this approach.
Wounded: Recurrent stammering: Reëducation.
Wounded: Ongoing stammering: Reeducation.
Case 582. (MacMahon, August, 1917.)
A young English officer, previously cured of stammering while a boy, fell to stammering again after being twice wounded. The impediment was of the laryngeal type. When spoken to he was often quite speechless. In Shell-shock stammering, the chief difficulty according to MacMahon is in the production of voice consonants and vowel sounds. In mild cases the trouble is best left alone.
A young English officer, who had been cured of his stammer as a child, started stammering again after being injured twice. The issue was related to his larynx. When someone talked to him, he often found himself completely unable to speak. According to MacMahon, in cases of stammering caused by shell shock, the main problem lies in producing consonant and vowel sounds. In mild cases, it's usually best to just leave it alone.
This officer was anxious to pass into the regular army from the reserve to which he was attached. The stammering prevented this. He was treated nine months and improved rapidly. He passed through the trying ordeal of the medical board successfully and went to his regiment.
This officer was eager to move from the reserve army to the regular army. His stutter held him back. After nine months of treatment, he made significant progress. He successfully faced the challenging medical board and joined his regiment.
In severe cases the patient is taught how to fill his lungs properly. He is taught to acquire an inferior lateral costal expansion in inspiration. During expiration the abdominal muscles are trained to contract slowly and strongly, pressing the diaphragm upwards and drawing the lower ribs downwards and inwards. This steady breathing produces a sensation of repose in the stammerer. He is not to raise the upper chest and not to tense the throat, tongue or jaws.
In severe cases, the patient is taught how to properly fill their lungs. They learn to achieve a lower side expansion during inhalation. During exhalation, the abdominal muscles are trained to contract slowly and strongly, pushing the diaphragm upwards while pulling the lower ribs down and in. This steady breathing creates a sense of calm for the person who stutters. They should avoid raising their upper chest and tensing the throat, tongue, or jaw.
The main vowel sounds are now taught. The main vowel sounds are oo, oh, au, ah, a and ee. They combine in six ways, oh and oo in the word wound, ah and ee make the long i, au and ee in boy, oh and oo in road, a and ee in rain and fair, ee and oo in new and you. There are also words in which no main vowel or compound sounds appear, which may be placed either on the open ah position or the closed ee position. Such words as long, abbot, among, which are on the position of ah and such words as it, sister, minister which are in the position of ee. The voice consonants are b, d, g, j, l, m, n, r, v, w, y, z, w being oo sound and y the ee sound. The breathed consonants are c, f, h, k, p, q, s, t.
The main vowel sounds are now being taught. The key vowel sounds are oo, oh, au, ah, a, and ee. They combine in six ways: oh and oo in the word “wound,” ah and ee create the long i, au and ee in “boy,” oh and oo in “road,” a and ee in “rain” and “fair,” and ee and oo in “new” and “you.” There are also words that don’t contain any main vowel or compound sounds, which can be placed either in the open ah position or the closed ee position. Examples include words like “long,” “abbot,” and “among,” which use the ah position, and words like “it,” “sister,” and “minister,” which are in the ee position. The voiced consonants are b, d, g, j, l, m, n, r, v, w, y, z, with w representing the oo sound and y the ee sound. The unvoiced consonants are c, f, h, k, p, q, s, t.
The treatment of stammering intensified by Shell-shock is more difficult than that of Shell-shock stammering de novo.
The treatment of stammering caused by Shell shock is more challenging than treating stammering that arises independently from Shell shock.
Wound of face: Speech disorder. Recovery by reëducation in two months.
Wound to the face: Speech issue. Recovery through rehabilitation in two months.
Case 583. (MacMahon, August, 1917.)
An officer was wounded under his left eye, October 7, 1916. His speech was affected only five days later in a casualty clearing station. Observed by MacMahon, November 5, he was found to speak with great difficulty and became exhausted after a few words. He was tensing all the muscles in attempting to speak. Breathing advice was given and counsel how to relax in the abnormal efforts.
An officer was injured under his left eye on October 7, 1916. He only started having speech problems five days later at a casualty clearing station. On November 5, MacMahon observed him and found that he struggled to speak and became tired after just a few words. He was tensing all his muscles while trying to talk. They provided breathing tips and advice on how to relax during his unusual efforts.
November 12, the officer, who was at Number One London General Hospital, began to speak with more freedom. “I am getting a bit better. I feel I must keep quiet, and it comes after a bit. I think far quicker than I speak.” He said that the breathing exercises had helped him most.
November 12, the officer at Number One London General Hospital started to express himself more freely. “I’m improving a little. I know I need to stay quiet, and it happens gradually. I think much faster than I can speak.” He mentioned that the breathing exercises had been the most beneficial for him.
November 15, he still spoke in a rather staccato way; but the words did not check as they had. In a week further there had been so much improvement that he was discharged with a prognosis of complete recovery.
November 15, he still spoke in a somewhat choppy way; but the words didn’t stumble like they used to. A week later, there had been so much progress that he was released with an outlook of full recovery.
January, 1917, he had recovered.
January 1917, he had recovered.
Shell wound and burial: Camptocormia (psychoelectric treatment successful in one séance) and lameness (long reëducative treatment successful).
Shell wound and burial: Camptocormia (successful psychoelectric treatment in one session) and lameness (long rehabilitative treatment successful).
Case 584. (Roussy and Lhermitte, 1917.)
At a Neuropsychiatric Center, September 2, 1916, arrived a chasseur, 29, showing lameness of a pseudocoxalgic type on the left side, combined with an anterior camptocormia. The whole situation had lasted a year. The chasseur had been wounded by shell explosion on the left side and was buried on July 29, 1915. He lost consciousness and had respiratory trouble and mutism. His arched walk and lameness began August 20, 1915.
At a Neuropsychiatric Center on September 2, 1916, a 29-year-old soldier arrived, showing a limp resembling pseudocoxalgia on his left side, along with an anterior curving of the spine. This condition had persisted for a year. The soldier had been injured by a shell explosion on his left side and was buried on July 29, 1915. He lost consciousness, experienced breathing difficulties, and was unable to speak. His arched walking style and limp started on August 20, 1915.
He had a number of terms in hospital and six months at the dépôt. He was sent back to the front, June 20, 1916, being proposed for auxiliary work. There was some mental weakness. After one séance of electric treatment, the improper attitude of the trunk was corrected. The lameness, however, persisted and required long daily reëducation.
He spent some time in the hospital and six months at the depot. He was sent back to the front on June 20, 1916, after being recommended for auxiliary work. There were signs of mental weakness. After one session of electric treatment, the improper posture of his body was corrected. However, the lameness continued and needed long daily rehabilitation.
The patient was discharged cured, October 20, 1916, without lameness or camptocormia. There were a few persistent lumbar pains.
The patient was discharged healthy on October 20, 1916, without any lameness or camptocormia. There were a few lingering lower back pains.
Re treatment of war psychoneuroses, Roussy and Lhermitte recommend rational and persuasive psychotherapy after the manner of Dejerine, Dubois, Babinski, and others. Hypnosis, they say, should definitely be rejected. Mental contagion must be staved off, and Roussy and Lhermitte believe that almost all cases are curable and should be sent back as competents.
Re treatment of war psychoneuroses, Roussy and Lhermitte recommend rational and persuasive psychotherapy similar to that of Dejerine, Dubois, Babinski, and others. They advocate for definitely rejecting hypnosis. It's essential to prevent mental contagion, and Roussy and Lhermitte believe that nearly all cases are treatable and should be returned as competent individuals.
They maintain that the medical officer himself plays the leading part. Many patients are “cured” when they find “good masters”; this mastery of the combined confessor and educator is greatly aided by prestige. He must speak with authority, with “iron in the velvet glove”; but with patience and persistence. If a long sitting fails, postpone work on the pretext of resting the patient. The patient must not be early threatened with discipline. Even exaggerators[820] and malingerers must be talked to as if neuropathic.
They argue that the medical officer plays a crucial role. Many patients feel “cured” when they find “good mentors”; this combination of confessor and educator is strongly supported by their authority. He needs to speak with confidence, using “an iron fist in a velvet glove,” while also showing patience and determination. If a long session doesn’t work out, take a break under the guise of allowing the patient to rest. The patient shouldn’t be threatened with discipline too soon. Even those who exaggerate or fake symptoms should be treated as if they’re experiencing neuropathic issues.[820]
A careful medical examination, besides correcting false diagnoses and demonstrating hystero-organic associations, will give the patient confidence in his physician.
A thorough medical exam, in addition to correcting inaccurate diagnoses and showing psychophysical connections, will help the patient trust their doctor.
A new patient is more easily cured than an old one. In general, patients should be treated as soon as possible after the shock. Contractures are habitually more persistent than paralysis; tremors and tic are more pertinacious than deafmutism; ante-bellum psychoneuroses are less easy to treat than cases developed by the war alone.
A new patient is easier to cure than an old one. In general, patients should be treated as soon as possible after the shock. Contractures tend to be more persistent than paralysis; tremors and tics are more stubborn than being deaf and mute; pre-war psychoneuroses are harder to treat than cases that developed solely due to the war.
The neurological centers near the front, with their discipline, inaccessibility to friends, and nearness to the front, present a situation which yields easier and quicker cures than the interior; but after the two-years’ experience which proved this fact, according to Roussy and Lhermitte, many cases still get sent back into the interior for many months,—cases that ought to be cured near the front. Cases having convulsive attacks get confinement in separate rooms; chronic neuropaths are kept in bed on a milk diet.
The neurological centers near the front, with their strict discipline, isolation from friends, and proximity to the front line, create a scenario that leads to faster and easier treatments than those done deeper in the facility. However, after two years of experience that confirmed this, as noted by Roussy and Lhermitte, many cases are still sent back to the interior for several months—cases that should be treated near the front. Patients with convulsive episodes are placed in separate rooms, while chronic neuropathies are confined to bed on a milk-only diet.
The general features of the treatment of psychoneuroses commended by Roussy and Lhermitte are summed up in what they call the psychoelectric and reëducative method, divided into four stages: A stage (a) of persuasive conversation; (b) isolation; (c) faradization; and (d) physical and psychical reëducation. Roussy and Lhermitte got during six months in one of the army neurological centers, 98 to 99 per cent of recoveries. Clovis Vincent, in a special interior hospital (see for Clovis Vincent’s treatment, a summary under Case 575). Re the first stage of persuasive conversations, Roussy and Lhermitte discuss on the day of admission the general nature of the patient’s condition, and place him in the atmosphere of cure, in contact with recovered patients. The conversation takes place in the physician’s consulting room. The patient is gotten to promise on oath that he will submit to any methods of treatment. Although one may pass from the first stage to the third or electrical stage, forthwith, Roussy and Lhermitte recommend several days of isolation. The patient is placed in a separate room, and[821] kept in bed on a milk diet. This isolation treatment of Weir Mitchell allows reinforcement of the suggestion by talks on the medical rounds, allows the patient, perhaps, to beg for the electrical treatment, which he may have refused at first, and lengthens the period of observation. According to Roussy and Lhermitte, spontaneous recovery not infrequently takes place during this phase of isolation. Lameness of long standing, tremors, and deafmutism disappear.
The general features of the treatment for psychoneuroses recommended by Roussy and Lhermitte are summarized in what they refer to as the psychoelectric and reeducative method, which is divided into four stages: (a) a stage of persuasive conversation; (b) isolation; (c) faradization; and (d) physical and psychological reeducation. Roussy and Lhermitte achieved a recovery rate of 98 to 99 percent over six months at one of the army neurological centers. Clovis Vincent had results in a special interior hospital (see Clovis Vincent’s treatment summary under Case 575). In the first stage of persuasive conversations, Roussy and Lhermitte discuss the general nature of the patient’s condition on the day of admission and create a healing atmosphere by connecting the patient with those who have recovered. The conversation takes place in the physician’s consulting room, where the patient is asked to promise on oath that he will follow any treatment methods. Although it's possible to move directly from the first stage to the third or electrical stage, Roussy and Lhermitte recommend several days of isolation. The patient is placed in a separate room and kept in bed on a milk diet. This isolation treatment from Weir Mitchell enhances the effectiveness of suggestions through discussions during medical rounds, allows the patient to potentially request the electrical treatment that he may have initially declined, and extends the observation period. According to Roussy and Lhermitte, spontaneous recovery often occurs during this isolation phase, with long-standing lameness, tremors, and deaf-mutism disappearing.
The third stage is that of faradization, executed by the physician with only such attendants as may be necessary to support the patient. At first, the man lies nude upon the bed, but later may be treated while sitting, standing, walking, or running. Feeble currents are used at first; later stronger ones. The poles are applied to the affected parts, and sometimes to especially sensitive parts of the skin, such as the ears, neck, lips, soles, perineum, and scrotum. Energetic treatment by the rapid method is indicated in the vast majority of cases, especially at the front. If a case is seen early, the rapid energetic treatment almost always cures at once. The success of the method depends upon the production of a crisis, which ought to be produced at the first sitting. Sometimes this sitting has to be continued for hours. Some patients require two or three sittings; some, still more. Instead of faradism, a cold jet of water, or even painful subcutaneous injections of ether, may be used.
The third stage is faradization, performed by the doctor with only a few assistants needed to help the patient. At first, the person lies naked on the bed, but later can be treated while sitting, standing, walking, or running. Weak currents are used initially; then stronger ones follow. The electrodes are placed on the affected areas and sometimes on particularly sensitive parts of the skin, like the ears, neck, lips, soles, perineum, and scrotum. Energetic treatment using the rapid method is recommended in most cases, especially in acute situations. If a case is addressed early, the rapid energetic treatment almost always provides immediate results. The effectiveness of the method relies on inducing a crisis, which should happen during the first session. Sometimes this session needs to last for hours. Some patients may need two or three sessions; others may need even more. Instead of faradization, a cold jet of water or even painful subcutaneous ether injections may be used.
The fourth stage is that of physical and psychical reëducation, important in long-standing cases. The various forms of physiotherapy are carried out by special assistants or head nurses, accompanied by psychotherapy, and if necessary by electricity. According to Roussy and Lhermitte, these reëducative methods used alone, without previous faradic treatment, are not successful. Relapse follows premature transference from the front to hospitals in the interior, and too early sick leave.
The fourth stage involves physical and mental rehabilitation, which is important for long-term cases. Different types of physiotherapy are carried out by specialized assistants or head nurses, along with psychotherapy, and if needed, electrical therapy. According to Roussy and Lhermitte, these rehabilitation methods used on their own, without prior faradic treatment, are not effective. A relapse occurs when there is a premature transfer from the front lines to hospitals inland, as well as too early of a sick leave.
Shell-shock deafmutism. Speech recovered by suggestion and reëducation; hearing by reëducation.
Shell shock deafness. Speech restored through suggestion and reeducation; hearing through reeducation.
Case 585. (Liébault, October, 1916.)
A corporal, 20, was exposed to the shock of an aerial torpedo, January 18, 1916, at Souchez. The torpedo fell a meter away. There was no loss of consciousness, but the patient was agitated for several hours, not knowing what he was doing. Evacuated to hospital, he remained several days in a stupid state. He was completely deaf and remembered poorly what had happened. He made every effort to speak, but could not. His head felt on fire. He could not open his mouth well and his lower jaw was almost in a state of contracture. He felt that his tongue could not move easily. In this status he remained until February, always trying to talk, but not succeeding.
A 20-year-old corporal was exposed to the shock of an aerial torpedo on January 18, 1916, in Souchez. The torpedo landed a meter away. He didn't lose consciousness, but he was agitated for several hours, not aware of what he was doing. After being evacuated to the hospital, he spent several days in a dazed state. He was completely deaf and struggled to remember what had happened. He tried hard to speak but couldn't. His head felt like it was on fire. He had difficulty opening his mouth, and his lower jaw was almost locked. He felt like his tongue couldn't move easily. He remained in this condition until February, continually trying to talk but unable to.
He then arrived at Hôtel-Dieu. The mouth was now opening better and he was in a better general status, though always feeling fatigued. Vibratory massage was given to the laryngeal region. He was gradually got to emit a few sounds in a low voice. He was sent, April 26, to Prés-à-goutrière. He was now somewhat vocal, but at times would become completely aphonic once more. The voice during the first few weeks of treatment became better, and the respiratory capacity was increased from 450 the first week to 460 and 500 in the next two weeks.
He then arrived at Hôtel-Dieu. His mouth was now opening better, and he was feeling generally better, although he still felt tired. They gave him vibratory massage in the laryngeal area. He gradually started to produce a few sounds in a low voice. On April 26, he was sent to Prés-à-goutrière. He was somewhat able to speak, but at times he would completely lose his voice again. Over the first few weeks of treatment, his voice improved, and his respiratory capacity increased from 450 in the first week to 460 and then 500 in the next two weeks.
May 12, he suddenly lost his voice again and wanted to commit suicide. However, in three more days he was able to speak normally again and has had no relapse. He was then put under auditory reëducation and at the time of report his hearing had slightly improved.
May 12, he suddenly lost his voice again and felt like taking his life. However, in three more days, he was able to speak normally again and hadn’t had any relapses. He was then placed under auditory reeducation, and at the time of the report, his hearing had slightly improved.
Liébault remarks that during the time when the patient could not speak his jaw muscles were contracted and his tongue could not mobilize well. He could think words but could not articulate them. It was accordingly important to cultivate the normal functioning of these muscles.
Liébault notes that when the patient couldn't speak, his jaw muscles were tense and his tongue was not able to move properly. He could form thoughts but couldn't express them. Therefore, it was crucial to nurture the normal functioning of these muscles.
Gassing; tracheitis; crash from airplane; unconsciousness: mutism; stammering. Reëducation; hypnosis.
Gassing; tracheitis; plane crash; unconsciousness: mute; stuttering. Rehabilitation; hypnosis.
Case 586. (MacCurdy, July, 1917.)
A lieutenant in the Royal Flying Corps, 23, described as “unusually normal,” a successful business man, athletic, socially popular, had been for a year in the Infantry. He was caught suddenly in a gas attack, and, though he recovered after a few days in bed, had a severe tracheitis and laryngitis. The lieutenant had been very proud of his voice and its carrying power. He went to a laryngologist in London, who said that he would never be able to sing again—a matter of some worry.
A 23-year-old lieutenant in the Royal Flying Corps, described as "unusually normal," was a successful businessman, athletic, and socially popular. He had spent a year in the Infantry before being caught off guard in a gas attack. Although he recovered after a few days of bed rest, he developed severe tracheitis and laryngitis. The lieutenant had taken great pride in his voice and its projection. He visited a laryngologist in London, who told him that he would never be able to sing again, which was quite troubling for him.
He soon became an expert airman. In the spring of 1917 he was shot at by antiaircraft guns in a trip over the enemy’s lines. One of the wings was hit and so weakened that in landing the lieutenant crashed to the ground. He was unconscious for three hours and on coming to tried to shout to his servant in the distance, who, on arrival, found the lieutenant quite unable to speak.
He quickly became a skilled pilot. In the spring of 1917, he was fired at by anti-aircraft guns during a flight over enemy territory. One of the wings was hit and became so damaged that when he landed, the lieutenant crashed to the ground. He was unconscious for three hours, and when he came to, he tried to call out to his servant in the distance. When his servant arrived, he found the lieutenant completely unable to speak.
According to MacCurdy, there was here a conversion hysteria with regression to the tracheitis that followed the gassing. The mutism MacCurdy regards as a pathological degree of an effort of protection for his voice. In hospital three weeks later he learned to whisper a few words, though with great mental effort. He regained the voiced sounds by coughing and then saying “ah.” Stammering now developed. Not more than one or two words could be said at a breath. Training to say two, three, four and then five letters in one expiration yielded improvement in the stammering. Under mild hypnosis, to the degree merely of distraction, normal speech was re-attained. There was no relapse. Singing was then practiced and in a period of six weeks the singing voice was virtually as good as it ever had been.
According to MacCurdy, there was a wave of conversion hysteria along with a regression to the tracheitis that followed the gassing. MacCurdy sees the mutism as an extreme protective mechanism for his voice. In the hospital three weeks later, he learned to whisper a few words, although it took a lot of mental effort. He regained the ability to make vocal sounds by coughing and then saying “ah.” Stammering then developed. He could only say one or two words at a time. Training to say two, three, four, and then five letters in one breath led to improvement in the stammering. Under mild hypnosis, just enough to provide distraction, he regained normal speech. There was no relapse. Singing was then practiced, and within six weeks, his singing voice was almost as good as it had ever been.
Shell-shock: Loss of consciousness, possibly hemorrhage from head: Spontaneous gradual recovery from anesthesias in three months: Recovery from paralysis by reëducation in a few more weeks.
Shell shock: Loss of consciousness, possibly bleeding from the head: Spontaneous gradual recovery from anesthesia in three months: Recovery from paralysis through rehabilitation in a few more weeks.
Case 587. (Binswanger, July, 1915.)
A German youth of 19 volunteered at the outset of the war as a motor cycle rider. About the end of October, he was hurled from his wheel by a shell which struck close beside him and exploded, knocking his back against a pile of beams. He lost consciousness. There may have been hemorrhage.
A 19-year-old German guy volunteered to be a motorcycle rider at the beginning of the war. Around the end of October, he was thrown off his bike by a shell that hit nearby and exploded, slamming his back against a stack of beams. He lost consciousness. There might have been bleeding.
He came to, two hours later, in the dressing station, hardly able to move his limbs. Such movements as he could make were painful. There was an evident contusion of the back. He had a fainting fit after his bath in the field hospital and then could get to bed only with support. Severe pains in the legs, especially in the knee.
He woke up two hours later in the medical station, barely able to move his limbs. Any movement he could manage was painful. There was a noticeable bruise on his back. He had fainted after his shower in the field hospital and could only get to bed with help. He experienced severe pain in his legs, particularly in his knees.
In the reserve hospital, there was a second similar fainting spell, followed by buzzing in the head, feelings of pressure in the chest and an irregular pulse; all of which phenomena disappeared the morning after the fit.
In the reserve hospital, there was a second similar fainting spell, followed by a buzzing in the head, feelings of pressure in the chest, and an irregular pulse; all of these symptoms disappeared the morning after the episode.
A careful examination about the middle of November showed the persistence of a severe paresis of the left arm, and a less marked motor weakness of the right arm. Both legs were paretic, and there were no spontaneous movements of the leg. This paresis of the legs was combined with complete anesthesia and analgesia. Sensory impairment was found only in the right arm and trunk, and there was no evidence of sensory impairment in the left arm. Both motor and sensory disturbances of the arm disappeared rapidly.
A close look around mid-November revealed that there was a noticeable weakness in the left arm, along with a less severe weakness in the right arm. Both legs were weak, and there were no spontaneous movements in the legs. The weakness in the legs was accompanied by total loss of feeling and pain sensitivity. Sensory loss was only found in the right arm and trunk, with no sensory issues in the left arm. Both the motor and sensory issues in the arm disappeared quickly.
However, at the beginning of December, 1914, the complete insensibility of the lower extremities up to the groin still persisted. The anesthesia then began to retreat, so that four days later, the upper limit of anesthesia was somewhat below the groin. There could be found a circumscribed area of anesthetic skin over the os sacrum up as far as the second[825] vertebra of the os sacrum; but the skin around this area, as well as over each tuber ischii, gave normal sensation.
However, at the beginning of December 1914, there was still complete numbness in the lower extremities up to the groin. Then, the numbness began to fade, so that four days later, the upper limit of numbness was slightly below the groin. There was a defined area of numb skin over the sacrum up to the second vertebra of the sacrum; however, the skin around this area, as well as over each ischial tuberosity, felt normal.
The anesthesia continued to retreat: to the middle of the thigh at the middle of December; to a level 3 cm. above the knee-cap at the end of December; to the upper end of the knee-cap on the right side and the middle of the left knee-cap, January 1. January 11, the anesthesia had retreated to a level 10 cm. below both right and left patella. February 8, sensibility in the legs had entirely returned.
The anesthesia kept fading: by mid-December it was at the middle of the thigh; by the end of December, it was 3 cm above the kneecap; on January 1, it was at the top of the right kneecap and the middle of the left kneecap. By January 11, the anesthesia had faded to 10 cm below both the right and left kneecaps. By February 8, feeling in the legs had completely returned.
While the anesthesia was pursuing this favorable course, the motor symptoms failed to improve to any marked extent, although active motion of the legs with the patient in dorsal decubitus had gradually returned to a limited degree.
While the anesthesia was going smoothly, the motor symptoms didn’t show much improvement, although the patient was gradually able to move their legs a little while lying on their back.
The diagnosis upon arrival at the Jena Nerve Hospital was “rheumatism of the left side of the body and dislocation of the spine.”
The diagnosis upon arrival at the Jena Nerve Hospital was “rheumatism of the left side of the body and dislocation of the spine.”
The treatment consisted at first of rest in bed and moist dressings of the legs, but the treatment had to depend greatly upon the diagnosis. The patient complained of difficult micturition; yet there were no other positive signs of organic disease, of spine or cord.
The treatment initially involved resting in bed and using moist dressings on the legs, but the approach needed to rely heavily on the diagnosis. The patient reported trouble urinating; however, there were no other clear signs of underlying disease in the spine or cord.
Hysteria was the diagnosis preferred to rheumatism, despite the fact that examination at the Jena Hospital failed to show any disorder in pain or tactile sense.
Hysteria was the diagnosis chosen over rheumatism, even though tests at the Jena Hospital showed no issues with pain or touch sensitivity.
The patient was a rather tall man of slender build, with a slightly accentuated second pulmonic sound, decidedly increased tendon reflexes, weak plantar reflexes, and many points painful on pressure in various parts of the head, over the spine, and in the sciatic regions. The vertebral sensibility to pressure was most acute in the region of the third, fourth, and fifth thoracic vertebrae. There was a marked dermatographia. There was no other sensory disorder and no motor disorder of the arms, though the left hand-grasp was weak. All passive movements could be successfully carried out with the legs. Upon bending at the hip, there were subjective feelings of tension in the posterior parts of the thighs. In active motion there was a marked limitation in leg movements, which appeared to be executed with great difficulty with but small excursion and with considerable[826] trembling. The knee-joint could be flexed only when the sole of the foot had support. The lower leg could not be extended. The excursion in the joints of the feet and toes was slight. Muscular strength was in general decreased. There were no feelings of pain in muscular action but merely feelings of great effort. Gait was slow, shuffling, unsteady, hesitating and only possible with support. Fatigue set in after a few steps. In walking, the legs could hardly be bent at the knee. The soles of the feet dragged on the ground. The patient was unable to stand upright, and when placed upon his feet, anxiously and stiffly clung to some support. Without support, he fell over backwards. When supported he could move his legs at the hip and lift the feet from their base by bending the knee-joints. The patient could not sit in a chair or in bed except with support; otherwise he would fall to the right side. In dorsal decubitus he complained of pain in the loins.
The patient was a tall, slender man with a slightly exaggerated second pulmonary sound, significantly increased tendon reflexes, weak plantar reflexes, and many painful spots when pressed in different areas of his head, over his spine, and in the sciatic regions. He had heightened sensitivity to pressure around the third, fourth, and fifth thoracic vertebrae. There was noticeable skin writing (dermatographia). No other sensory or motor disorders were present in the arms, although the grip in his left hand was weak. All passive movements in his legs could be performed successfully. Bending at the hip caused subjective tension in the back of his thighs. Active leg movements were greatly limited, and he executed them with difficulty, minimal range, and significant trembling. He could only bend his knee when the sole of his foot was supported, and he couldn't extend his lower leg. The movement in his foot and toe joints was slight. Overall muscular strength was reduced. He didn’t experience pain during muscular activity, just a sense of great effort. His gait was slow, shuffling, unsteady, hesitant, and he could only walk with support. Fatigue set in after taking a few steps. His legs barely bent at the knees while walking, and the soles of his feet dragged on the ground. The patient couldn't stand up straight and, when placed on his feet, anxiously and stiffly held onto something for support. Without support, he would fall backward. When supported, he could move his legs at the hip and lift his feet off the ground by bending his knees. He couldn’t sit in a chair or in bed without support; otherwise, he would fall to the right side. While lying on his back, he complained of pain in his lower back.
With this hysterical picture, treatment of a psychotherapeutic nature was carried out. The patient was given methodical exercises in walking and standing, during which affirmative suggestions about his new capacity to walk and stand were given with monotonous repetition.
With this dramatic image, psychotherapy was performed. The patient was given structured exercises for walking and standing, during which positive suggestions about his newfound ability to walk and stand were repeated in a monotonous way.
For the first fortnight he walked with the support of two nurses for a half hour every day. He was very industrious and willing to execute this treatment; and later began to exercise with a cane. Two days later, he omitted the cane and found himself able to walk about without support. He was shortly able to stand without swaying, although for some time the walk was upon a rather wide base and somewhat slow and suggestive of spastic paresis.
For the first two weeks, he walked with the help of two nurses for half an hour every day. He was very committed and eager to follow this treatment, and eventually started to practice walking with a cane. Two days later, he ditched the cane and discovered he could walk without support. Soon, he was able to stand without swaying, though for a while, his walk was wide and a bit slow, resembling mild muscle weakness.
The general condition of this patient remained good. His appetite and sleep were good. After the middle of March, 1915, there were no more peculiarities in walking, and the patient was able to take somewhat long walks in the city and vicinity. He applied for work in the airship division, for which he already possessed some experience.
The overall condition of this patient was stable. His appetite and sleep were good. After mid-March 1915, he no longer had any unusual walking patterns, and he was able to take longer walks around the city and nearby areas. He applied for a job in the airship division, where he already had some experience.
The youth appears to have been of a normal mental and bodily development, though his mother is said to have been nervous and a sister died of convulsions in childhood.
The young man seems to have had normal mental and physical development, although his mother is reported to have been anxious and a sister passed away from convulsions during childhood.
Shell-shock with loss of consciousness: Deafmutism, rhythmic head movements, anesthesia, asymmetrical areflexia. Recovery by suggestion with faradism, massage and reëducation.
Shell shock with loss of consciousness: Deafness, rhythmic head movements, numbness, uneven reflexes. Recovery through suggestion using electrical stimulation, massage, and rehabilitation.
Case 588. (Arinstein, September, 1916.)
A Russian private, 30, literate, lost consciousness upon the explosion of a large shell, November 10, 1915. He was brought to hospital, November 14, completely deaf and dumb, and with his head rhythmically swaying sidewise 60 to 70 times per minute. The swaying ceased during sleep. The head was carried inclined to the right; there was complaint of headache. The left leg, the trunk and the hairy part of the head were anesthetic. The knee-jerks were obtained with difficulty, the Achilles jerks were lively; the throat and conjunctival reflexes were absent; the abdominal and cremasteric reflexes were lively. The right plantar reflex was absent; the left normal. The vision of the right eye was impaired, and there was a monocular diplopia of this eye. The drum membranes were pulled in, and the disorder of hearing was explained on the basis of labyrinthine shock.
A 30-year-old Russian private who could read and write lost consciousness when a large shell exploded on November 10, 1915. He was taken to the hospital on November 14, completely deaf and mute, with his head rhythmically swaying side to side 60 to 70 times per minute. The swaying stopped when he slept. His head tilted to the right, and he complained of a headache. The left leg, torso, and hairy part of the head felt numb. Knee-jerk responses were difficult to elicit, but Achilles reflexes were strong; the throat and conjunctival reflexes were absent, while the abdominal and cremasteric reflexes were strong. The right plantar reflex was absent, but the left was normal. The vision in his right eye was impaired, and he experienced double vision in that eye. The eardrums were retracted, and the hearing disorder was attributed to labyrinthine shock.
After a séance of written suggestion with faradism to neck and small palate and vibratory massage to throat, speech returned. November 26, the patient read in a loud voice a written phrase. He did not speak again independently until early in December, when he read aloud written matter. The return of spontaneous speech was gradual. Hearing returned December 5, when he was able to hear in the right ear by means of a tube. In the sitting posture there was less swaying of the head. If the patient lay down, rhythmic movements of the head became stronger and more rapid (120).
After a session of written suggestion combined with faradism to the neck and soft palate, along with vibratory massage to the throat, the patient was able to speak again. On November 26, he read a written phrase out loud. He didn't talk independently again until early December, when he read some written material aloud. The return of his spontaneous speech happened slowly. His hearing came back on December 5, when he was able to hear in his right ear using a tube. When sitting, there was less swaying of his head. However, when the patient lay down, the rhythmic movements of his head became stronger and faster (120).
Shell explosion; unconsciousness: Amnesia; paralyses. Reëducation.
Shell explosion; unconsciousness: Amnesia; paralysis. Rehabilitation.
Case 589. (Batten down, January, 1916.)
A corporal in the Belgian army was mobilized when the war broke out, and was in action continuously in the retreat from Liège, in the siege of Antwerp, and finally on the Yser until October 27, 1914, when the explosion of large shells rendered him unconscious. He recovered consciousness only in hospital at Calais. Though he was able to see and hear well, he was dazed and remembered nothing of what had happened. In fact, he did not understand what was said to him.
A corporal in the Belgian army was called up when the war started and was actively engaged during the retreat from Liège, the siege of Antwerp, and finally at the Yser until October 27, 1914, when a series of big explosions knocked him out. He only regained consciousness in a hospital in Calais. Although he could see and hear well, he was confused and didn’t remember anything that had happened. In fact, he didn’t understand what people were saying to him.
In a week’s time, his memory and intelligence returned, save for periodic attacks in which he was dazed. From the very beginning he had been quite unable to move his legs, and at first the arms were weak. He had a series of attacks of violent struggling in November and December, 1914, which the corporal himself called fainting attacks, claiming that he did not move his legs in the attacks but only his arms. In fact, he claimed that he could move neither head, body, nor legs, but only the arms. He said, “Sometimes I try hard and set my teeth, but I do not know how to move my head and my legs; I try but they do not move.” Sphincter control was maintained. Although he could see, when he attempted to read, everything went black.
In a week, his memory and intelligence came back, except for occasional moments when he felt dazed. From the start, he couldn't move his legs, and his arms were weak at first. He experienced a series of intense struggles in November and December 1914, which he referred to as fainting spells, insisting that during these times, he couldn't move his legs, only his arms. In fact, he maintained that he could move neither his head, body, nor legs, just his arms. He said, “Sometimes I try really hard and grit my teeth, but I don’t know how to move my head and legs; I try, but they don’t budge.” He had control over his sphincter. Even though he was able to see, whenever he tried to read, everything turned black.
He was finally admitted to the National Hospital for the Paralyzed and Epileptic on July 8, 1915, on the service of Major Walshe. He was thin and wasted. He was firmly convinced, according to the notes of Major Walshe, that he was seriously paralyzed. He said he could not lift his head; when his body was lifted, his head fell back, or rather perhaps was definitely thrown back, lolling about alarmingly. However as he lay in bed he frequently lifted his head unconsciously and placed his hands under it. When asked to lift his head, the sternomastoids were strongly contracted, but at the same time the neck extensors also, so that the head was[829] stiffly and strongly held in an extended position. Despite the patient’s statement that he could not move the trunk muscles, he could turn over readily in bed, and when trying to move the head the trunk was fixed in a strong opisthotonos, and the abdominal walls were rigid. When requested to move his legs, he made no movement whatever, though during head movements the legs were strongly fixed in extension. On passive movements, there was no active muscular resistance. There was an indefinite blunting of all kinds of sensations. Reflexes were normal.
He was finally admitted to the National Hospital for the Paralyzed and Epileptic on July 8, 1915, under the care of Major Walshe. He was thin and emaciated. He was firmly convinced, according to Major Walshe's notes, that he was seriously paralyzed. He claimed he couldn't lift his head; when his body was lifted, his head fell back, or perhaps it was thrown back in a way that looked alarming. However, while lying in bed, he often lifted his head unconsciously and placed his hands under it. When asked to lift his head, his sternocleidomastoid muscles were strongly contracted, but at the same time, his neck extensors were also engaged, so the head was stiffly and strongly held in an extended position. Despite the patient’s claim that he couldn't move his trunk muscles, he could easily turn over in bed, and when he tried to move his head, his trunk was fixed in a strong opisthotonos, and his abdominal muscles were rigid. When asked to move his legs, he didn’t make any movement at all, although during head movements, his legs were firmly extended. During passive movements, there was no active muscular resistance. There was a vague dullness to all types of sensations. Reflexes were normal.
Major Walshe worked hard with the patient, inducing him first to lift his head from the pillow, and finally to move the legs. In three weeks’ time, the corporal could just sit up, and at the end of another month, he was able to stand in the walking machine. At the end of a third month, he was walking upon crutches, and at the end of another, he could walk upon two sticks with his feet wide apart, moving as if glued to the floor. To quote Batten,[830] “The corporal will eventually get well but not, I think, before the end of the war.”
Major Walshe worked hard with the patient, encouraging him first to lift his head from the pillow and finally to move his legs. In three weeks, the corporal could sit up a little, and by the end of another month, he was able to stand in the walking machine. After a third month, he was walking on crutches, and by the end of another month, he could walk with two sticks, his feet spread wide apart, moving as if stuck to the floor. To quote Batten,[830] “The corporal will eventually get well, but I don’t think it will be before the end of the war.”
E. EPICRISIS[8]
[8] Material is here drawn passim from the compiler’s Shattuck Lecture on Shell-shock and After, read before the Massachusetts Medical Society, Boston, June 18, 1918.
[8] This material is taken passim from the compiler's Shattuck Lecture on Shell-shock and After, presented to the Massachusetts Medical Society in Boston on June 18, 1918.
Terminology
1. Shell-shock, a lay term, usually refers to the medical entity or disease-group: functional neurosis, or more briefly, neurosis.
1. Shell shock, a common term, usually refers to the medical condition or group of disorders known as functional neurosis, or more simply, neurosis.
The history of the term Shell-shock will repeat that of Railway Spine in the last century; the term will fall into disuse when the cases subsumed thereunder get their exact medical diagnoses—which, statistically speaking, will prove to be as a rule psychoneuroses, either hysteria (pithiatism), neurasthenia (nervous exhaustion, “prostration”), or psychasthenia (obsessive neurosis).
The history of the term Shell-shock will mirror that of Railway Spine from the last century; it will fall out of use when the cases contained within it receive their precise medical diagnoses—which, statistically speaking, will typically turn out to be psychoneuroses, such as hysteria (pithiatism), neurasthenia (nervous exhaustion, “prostration”), or psychasthenia (obsessive neurosis).
2. But the laity cannot be got to use the term Shell-shock in this exact sense, because the laity cannot make exact diagnoses.
2. But regular people can't use the term Shell-shock in this specific way, because they can't make precise diagnoses.
In the post-bellum and reconstruction period the physician will need to guard against regarding all cases called Shell-shock as really neuroses, merely on the ground that Shell-shock is probably neurosis. Laymen will in the reconstruction period succumb to the lure of the 100 per cent and gossip about cures and failures in the same loose manner that is but too familiar in discussions of Lourdes, Christian Science, the Emmanuel Movement. It will be worth while to preserve a certain generality and comprehensiveness for the term Shell-shock, which will stand to medicine as the term weeds stands to botany.
In the post-war and reconstruction period, doctors need to be careful not to treat every case labeled as Shell-shock as if it’s definitely a neurosis, just because Shell-shock is likely a neurosis. During the reconstruction period, the public will fall for the idea of absolute cures and will talk freely about successes and failures in a way that’s all too common in discussions around Lourdes, Christian Science, and the Emmanuel Movement. It’s important to keep a broad and inclusive definition for the term Shell-shock, just like the term weeds is used in botany.
3. In short, keep the connotation but try not for any denotation of this lay term Shell-shock in the lay mind!
3. In short, maintain the meaning but avoid any literal interpretation of the term "Shell-shock" in the public's understanding!
The dangerous history of the term dementia praecox may be recalled. Neither dementia nor praecox is an exact term[832] except for the statistical majority of cases of schizophrenia. Yet does not the layman hearing the term dementia feel entitled to assume that a victim must be demented or become so?
The troubling history of the term dementia praecox might come to mind. Neither dementia nor praecox is a precise term[832] except for the majority of schizophrenia cases. Still, doesn't the average person hearing the term dementia feel justified in thinking that the person must be demented or will become so?
4. The term Shell-shock appears to be a perfect term for the ordinary man, as it means much and little, connotes enormously and denotes a minimum and casts the lay hearer back upon the expert.
4. The term Shell-shock seems to be the perfect phrase for the average person, as it carries a lot of meaning and yet very little, suggests a great deal and signifies only a small amount, and makes the general listener rely on the expert.
But confronted by the term Shell-shock, the ardent social worker or the ordinary man fails to get any incorrect notion about the nature, and especially about the prognosis, of the condition. If there is any suggestion of prognosis, it is the correct suggestion of curability possibly conveyed by the suddenness implied in the term shock; but I defy the ordinary man to get from the ordinary term Shell-shock very much that denotes anything in particular. All he gets is an enormous connotation. This connotation may run back for the race into tree stumps, savages brandishing spears, palatial decorations, the protrusion of animal spirits, the Leyden jar (sometimes familiarly known as the “shock bottle”), and the aspen shaking of the man in fear or its interior equivalent. But whether the slang runs back so far or no, and whether the shell is a shell of powder or a shell of fear, and whether the shock is of solid particles or in a moral sense, the problem is implicitly laid down in the slang (see historical discussion, Shattuck Lecture).
But when faced with the term Shell-shock, the passionate social worker or the average person doesn't really understand what it means, especially regarding the prognosis of the condition. If there’s any hint of a prognosis, it’s the accurate suggestion of treatability, possibly hinted at by the suddenness in the term shock; but I challenge the average person to derive any specific meaning from the term Shell-shock. What they get is a vast amount of implications. These implications may reach back through history to tree stumps, primitive people waving spears, grand decorations, a surge of animal instincts, the Leyden jar (often casually called the “shock bottle”), and the trembling of a person in fear or its internal equivalent. But whether the slang has roots that go back that far or not, and whether the shell refers to an explosive shell or a shell of fear, and whether the shock is made up of solid particles or is moral in nature, the issue is implicitly established in the slang (see historical discussion, Shattuck Lecture).
5. The terminological difficulties are clarified somewhat by the French distinction of états commotionnels and états émotionnels in the Shell-shock group.
5. The terminology issues are somewhat clarified by the French distinction between états commotionnels and états émotionnels within the Shell-shock group.
The French very neatly distinguish what they term états commotionnels from états émotionnels. They think of the états commotionnels or commotional states much as we think of commotio cerebri, that is, of a physico-chemical happening in the brain of an essentially curable (or reversible) nature; that is, of something that falls short of being, as they say, lésionnel, namely, as bringing about a structural lesion. That is, they distinguish a brain with a visible focal lesion from one which has sustained a physical jar or commotion, and they distinguish the effects of both of these from the états émotionnels[833] or emotional effects of an injury. The nomenclature here brings out one of the most fundamental difficulties in the whole field of so-called Shell-shock, namely, the distinction between structural conditions, microscopic or macroscopic, on the one hand, and functional conditions of a psychopathic nature, on the other. The commotion would affect the neurones themselves in some perhaps invisible but still genuine physico-chemical way, whereas the emotion would affect these neurones merely after the manner of the normal emotional life, except that the neurones would perhaps deliver an excessive stream of impulses.
The French clearly differentiate between what they call états commotionnels and états émotionnels. They view états commotionnels, or commotional states, similarly to how we understand commotio cerebri, meaning it's a physical-chemical event in the brain that is essentially curable (or reversible); in other words, it doesn’t lead to what they refer to as lésionnel, which means it doesn’t create a structural lesion. They distinguish between a brain with a visible focal lesion and one that has experienced a physical jolt or commotion, and they also separate the effects of both from the états émotionnels[833], or emotional effects of an injury. This terminology highlights one of the main challenges in the entire area of so-called Shell-shock, specifically the difference between structural conditions, whether microscopic or macroscopic, and functional conditions that are psychopathic in nature. The commotion would impact the neurones in a possibly invisible but still real physico-chemical way, while the emotion would influence these neurones in the usual manner of emotional life, except that the neurones might produce an excessive flow of impulses.
6. Terminology, especially in the matter of explanations to laymen (Americans demand monosyllabic explanations as a preliminary to taking suggestions!), is not always assisted to clearness by physicians on account of the old ontological fallacy that Charcot insisted on.
6. Terminology, especially when it comes to explaining things to the average person (Americans expect simple, one-syllable explanations before considering any suggestions!), isn't always made clear by doctors because of the outdated ontological mistake that Charcot emphasized.
Would that the medical profession understood neuroses at their true value! Only too frequent is the impression on the part of the profession that imaginary symptoms are by the same token non-existent! I have even heard a physician well-trained in somatic lines say that Shell-shock did not exist because Shell-shock was nothing but neurosis, and neuroses were characterized by imaginary symptoms,—accordingly neuroses, being imaginary, do not exist! All of which reminds us that many of the profession were entirely skeptical when Charcot made his original observations. Some men here in America felt that, whereas hysteria might occur in Paris, it did not occur to any extent in America. The Shell-shock data of this war will abundantly prove to the profession the existence of the neuroses, and I feel that physicians will have to brush up their ontology to the extent of conceding that a symptom may be in a sense imaginary and yet not in any sense non-existent.
I wish the medical field understood neuroses for what they really are! Too often, professionals assume that imaginary symptoms are therefore non-existent! I've even heard a well-trained doctor in physical medicine claim that Shell-shock didn’t exist because Shell-shock was just neurosis, and neuroses were defined by imaginary symptoms—so, since neuroses are imaginary, they don’t exist! This brings to mind that many in the field were completely skeptical when Charcot first made his observations. Some people here in America believed that while hysteria might happen in Paris, it didn't really occur in the U.S. The data on Shell-shock from this war will definitely demonstrate the reality of neuroses, and I think doctors will need to revise their thinking to acknowledge that a symptom may be in a way imaginary and yet not in any sense non-existent.
7. Babinski points out a case of hysterical paralysis of a leg which led the patient to lean so heavily upon his arm as to produce an organic crutch paralysis. It would be to no point to argue that the hysterical paralysis was here non-existent. Of course we shall have to meet the false analogies drawn from methods of cure. If a paralysis can be cured in a[834] few minutes by the electric brush, or by hypnosis, or on emergence from chloroform, or by some other modern miracle.
7. Babinski describes a case of hysterical paralysis in a leg that caused the patient to lean so heavily on his arm that it resulted in an organic crutch paralysis. It wouldn't make sense to argue that the hysterical paralysis wasn't real in this case. Of course, we will need to address the misleading comparisons drawn from different treatment methods. If a paralysis can be resolved in a [834] matter of minutes using the electric brush, hypnosis, recovery from chloroform, or some other modern treatment miracle.
8. Is it too much to ask the profession not ever to say that this rapid and seemingly miraculous cure was brought about because the disease was non-existent?
8. Is it too much to ask the profession to avoid claiming that this quick and seemingly miraculous cure happened because the disease wasn’t real?
Diagnostic Boundary Issue
9. The delimitation problem, taken up in Section A, is not identical with the differentiation problem, taken up especially in Section C but passim in Sections B and D; by delimitation we may refer to the process of localizing the diagnostic battle through exclusion of the other great groups of mental diseases that à priori ought not to come in question, but do come in question sometimes, before we slice down to the question.
9. The delimitation problem, discussed in Section A, is not the same as the differentiation problem, which is particularly covered in Section C but also appears in Sections B and D; by delimitation, we mean the process of identifying the specific diagnostic issues by excluding other major categories of mental illnesses that à priori shouldn't be considered, but sometimes are, before we get to the main question.
10. Is there or is there not evidence of destructive lesion in the nervous system of this so-called Shell-shocker? Is this man a victim of organic or of functional neurosis? This latter is what may be termed the differentiation problem.
10. Is there evidence of damaging lesions in the nervous system of this so-called Shell-shocker, or isn’t there? Is this man experiencing organic or functional neurosis? This is what could be called the differentiation problem.
Confining ourselves now to the delimitation problem, what are the major groups of mental diseases that might come in question?
Confining ourselves now to the delimitation problem, what are the major groups of mental diseases that might come into play?
I shall enumerate these. We think of mental diseases as I, syphilitic; II, hypophrenic (that is, feeble-minded in some of its phases, including even slight degrees of subnormality not entitled to be called feeble-minded in the ordinary sense); III, epileptic; IV, alcoholic (or due perhaps to some drug or poison); V, encephalopathic (in the sense of some focal brain disease); VI, symptomatic (in the sense of some somatic disease); VII, senile (or presenile). The seven groups so far enumerated, I believe, the general profession is pretty well equipped to consider, at least roughly to diagnosticate and to handle with due respect to the interests of the patient and of the community. I am bound to say that some of my colleagues would not go so far as to the competence of physicians in general in these fields, and one is aware that a plenty of mistakes have occurred even in these groups through the bad judgment of practitioners. Nevertheless, I hold to the conception that our profession is reasonably well equipped to[835] handle these greater groups, having in mind all the while the appropriate temporary calling-in of the specialist. But there are two more groups, in addition to these seven, in which I am not so sure that the general profession knows as much as it should. I refer to VIII, the schizophrenic group, commonly known as the dementia praecox group; and IX, the cyclothymic group, sometimes termed the manic-depressive group. It is the victims of the diseases that constitute these latter groups that ought unconditionally to be excluded with few exceptions from the army; and it is the study of these conditions which ought to be carried out as a part of every man’s post-graduate training, not merely for his work on draft boards, but for his work in civilian and reconstruction practice. There is another group of, X, psychoneuroses, with which the profession regards itself as familiar, and with which it doubtless is familiar, in what might be called blooming examples of hysteria, neurasthenia, and psychasthenia. But the nub of the situation lies in the fact that the diagnosis of instances which are not such blooming examples is difficult, and hence it was that I qualified my statement as to the competence of the practitioner in this tenth group. It is, of course, the tenth group, of psychoneuroses, into which the majority of the Shell-shock cases fall.
I will list these. We think of mental illnesses as I, syphilitic; II, hypophrenic (which means feeble-minded in some phases, including even slight degrees of subnormality that aren’t usually called feeble-minded); III, epileptic; IV, alcoholic (or perhaps caused by some drug or poison); V, encephalopathic (referring to some focal brain disease); VI, symptomatic (related to some bodily disease); VII, senile (or presenile). I believe the medical profession is generally equipped to at least roughly diagnose and manage these seven groups, keeping the patient's and community's best interests in mind. I must admit that some of my colleagues may not agree about the general competence of physicians in these areas, and it's clear that many mistakes have happened even within these groups due to poor judgment from practitioners. Still, I believe our profession is reasonably capable of[835] handling these major groups, while also considering the need to call in specialists when appropriate. However, there are two more groups beyond these seven, where I'm not so confident that the general profession has enough knowledge. I’m referring to VIII, the schizophrenic group, commonly known as the dementia praecox group; and IX, the cyclothymic group, sometimes called the manic-depressive group. People affected by these latter conditions should generally be excluded from the army, with few exceptions; and studying these conditions should be a part of every physician’s post-graduate training, not just for work on draft boards but also for civilian and reconstruction practice. There is another group, X, psychoneuroses, which the profession considers itself familiar with, and indeed it is, in what might be termed blooming examples of hysteria, neurasthenia, and psychasthenia. However, the issue lies in the fact that diagnosing cases that aren’t such clear examples is difficult, which is why I was cautious in stating how competent practitioners are in this tenth group. This tenth group of psychoneuroses is where the majority of Shell-shock cases fall.
11. Now a study of the literature of the belligerents having Shell-shock in mind as its special topic and aim proves to require a study of war literature in all of these groups. There are cases of so-called Shell-shock which even well-prepared medical men have placed in the neurosis group, when they should have been placed in one or other of the groups mentioned.
11. A study of the literature from the warring sides, focusing specifically on Shell-shock, shows that it requires an examination of war literature across all these groups. There are instances of so-called Shell-shock that even experienced medical professionals have categorized as neuroses when they should have been classified in one of the other groups mentioned.
12. In short, whereas the Shell-shock delimitation problem deals with groups, I, II, III, IV, VI, VIII, IX and (as our compilation shows) especially with groups I, III and VI, on the other hand the shell-shock differentiation problem deals primarily with groups V and X.
12. In short, while the Shell-shock delimitation problem focuses on groups I, II, III, IV, VI, VIII, IX, and (as our compilation shows) especially on groups I, III, and VI, the shell-shock differentiation problem mainly concerns groups V and X.
To clear the decks for action re the differentiation problem, let us dismiss the major troubles of the delimitation problem as shown in groups I (syphilitic), III (epileptic), VI (somatic) and thereafter very briefly refer to the residue of the delimitation[836] problem. For convenience of reference, a few out-standing remarks concerning the general relations of these divisions to war and peace conditions are inserted here. We dealt in the diagnostic order of exclusion with 190 cases, distributed as in the table below (bear in mind that the method of this book precludes attaching great statistical weight to the comparative figures, since the various authors published their cases for their special rather than their typical interest).
To prepare for action regarding the differentiation problem, let’s set aside the major issues of the delimitation problem as seen in groups I (syphilitic), III (epileptic), and VI (somatic), and then briefly touch on the remaining aspects of the delimitation problem. For easy reference, some key comments about the overall relationships of these divisions to conditions of war and peace are included here. We looked at 190 cases in the diagnostic order of exclusion, distributed as shown in the table below (keep in mind that the method of this book does not allow us to place significant statistical importance on the comparative figures since the various authors presented their cases based on their specific interests rather than typical patterns).
| I. | Syphilopsychoses | 34 | |
| II. | Hypophrenoses (feeble-mindedness and imbecility) | 18 | |
| III. | Epileptoses | 33 | |
| VI. | Pharmacopsychoses (alcohol; morphine) | 17 | |
| V. | Encephalopsychoses (focal brain lesion cases) | 15 | [9] |
| VI. | Somatopsychoses | 29 | |
| VII. | Geriopsychoses (senile—a null class) | 0 | |
| VIII. | Schizophrenoses | 16 | |
| IX. | Cyclothymoses | 7 | |
| X. | Psychoneuroses | 12 | [9] |
| XI. | Psychopathoses | 15 | |
| 196 |
13. The neuropsychiatric side of syphilis in the war is presented in 34 cases (Cases 1 to 34). The syphilitic basis of sundry military difficulties, quite unsuspected by the laity and probably not too well understood by service men, is suggested by Case 1, a case of desertion by a French officer of high rank. Nor is Case 2, in which visions of submarines proved syphilitic, without its warning. Such cases point only too obvious a moral:
13. The neuropsychiatric aspects of syphilis during the war are illustrated through 34 cases (Cases 1 to 34). The connection between syphilis and various military issues, often overlooked by the general public and likely not fully understood by military personnel, is highlighted by Case 1, a case involving the desertion of a high-ranking French officer. Similarly, Case 2, where visions of submarines were linked to syphilis, serves as a cautionary example. These cases clearly point to an important lesson:
14. Neurosyphilitics have no place in the army or navy.
14. People with neurosyphilis have no place in the army or navy.
Eight cases (Cases 3-10) follow in which the aggravation or acceleration or liberation of neurosyphilis has come about under the conditions of war. Some of these cases suggest the gravity of the problems of compensation, allowance and pension that may arise. We might ask,
Eight cases (Cases 3-10) follow where the worsening, speeding up, or release of neurosyphilis occurred due to wartime conditions. Some of these cases highlight the seriousness of the issues related to compensation, benefits, and pensions that may come up. We might wonder,
15. Should not a government which enlists a syphilitic pay full allowances to him when under war conditions he becomes a neurosyphilitic?
15. Shouldn’t a government that recruits someone with syphilis provide full benefits when, due to wartime conditions, that person develops neurosyphilis?
For the government was theoretically able to learn at the start (within a small margin of error by means of the serum test) whether the man was syphilitic. If a one-eyed man loses his remaining eye in an industrial accident in civil life, his damages are often fixed at damages for total blindness; for the industrial firm should not have employed a one-eyed man in an industry dangerous to eyes. The principle cannot differ with a man hired in a spirochete-bearing state: The company has hired a man who may under traumatic conditions become an incompetent neurosyphilitic, and should pay damages accordingly when the aggravation begins.
The government could theoretically find out at the start (within a small margin of error using a serum test) whether a person had syphilis. If a one-eyed man loses his remaining eye in a workplace accident, his compensation is often set at what he would receive for total blindness because the company shouldn’t have hired a one-eyed person for a job that puts his eyes at risk. The same principle applies to someone hired who has syphilis: the company has employed a person who could potentially become severely ill and should provide compensation accordingly when that condition worsens.
16. What are the responsibilities of government if the neurosyphilis is due to a syphilis acquired during the war?
16. What are the government's responsibilities if the neurosyphilis is caused by syphilis contracted during the war?
Often such infection may be due to a tragical form of “negligence.” But, as pointed out in a work on Neurosyphilis, 1917, I believe that any form of licensing system, official or virtual, which would permit the purchase of syphilis in or near military zones, abolishes the argument of “negligence.” A man acquiring syphilis under the connivance of government ought to stand as well as a syphilitic hired by the government, when it shall come to the question of compensation for incapacity. Yet, it may be argued, the man might have remained continent after all. The point is left to the mercy of jurists.
Often such infections may be attributed to a tragic form of “negligence.” However, as noted in a study on Neurosyphilis from 1917, I believe that any licensing system, whether official or unofficial, that allows for the purchase of syphilis in or around military zones eliminates the argument of “negligence.” A person who contracts syphilis with the government’s tacit approval should be treated the same as a syphilitic individual hired by the government when it comes to compensation for inability to work. However, one might argue that the person could have remained celibate anyway. This matter is left to the discretion of legal experts.
17. The share of neurosyphilis in the “crimes” and disciplinary problems of the army is intimated in three cases (Cases 11 to 13).
17. The role of neurosyphilis in the “crimes” and disciplinary issues within the army is suggested in three cases (Cases 11 to 13).
18. The latter part of the series (Cases 14 to 31) embraces problems of a more medical nature, touching traumatic paresis and “Shell-shock paresis.” Unusual, these cases may be readily conceded to be; but their infrequency is not such as to put them out of the field of consideration in the “Shell-shock” group.
18. The latter part of the series (Cases 14 to 31) includes issues that are more medical, involving traumatic paresis and “Shell-shock paresis.” While these cases are indeed unusual, their rarity doesn’t exclude them from being considered in the “Shell-shock” group.
Case 28, in which shell-shock (the physical event) apparently caused recurrence of a syphilitic (!) hemiplegia, is particularly instructive and might better belong with the[838] series (under Section B: Nature and Causes, Cases 286-301) in which ante-bellum weak spots were picked out by shell-shock and war conditions. But Case 28 is placed here for its syphilitic interest.
Case 28, where shell shock (the physical event) seemingly triggered a return of a syphilitic (!) hemiplegia, is especially informative and might fit better with the[838] series (under Section B: Nature and Causes, Cases 286-301) where before the war vulnerabilities were highlighted by shell shock and wartime conditions. However, Case 28 is included here for its relevance to syphilis.
Case 29 stands out as a warning example not to crowd the hypothesis and try to make syphilis sponsor for everything, even when it plainly is at work.
Case 29 serves as a cautionary example not to overload the hypothesis and assume syphilis is the cause of everything, even when it’s clearly involved.
Cases 32-34 are cases in which syphilis played a part, though possibly a minor part, in certain peculiar mental reactions.
Cases 32-34 are cases where syphilis was involved, though perhaps only to a small extent, in some unusual mental reactions.
To sum up the part played by syphilopsychoses and syphiloneuroses in the war, we find, that
To sum up the role of syphilopsychoses and syphiloneuroses in the war, we find that
19. Syphilis may have occasionally a serious military effect, as in the case of desertion by a French officer of high rank.
19. Syphilis can sometimes have a serious impact on military operations, as demonstrated by the desertion of a high-ranking French officer.
20. Important problems of pension, retirement, and compensation are brought out, and as no previous war has had the benefit of the Wassermann reaction and other exact tests bearing upon the nature, progress, and curability of neurosyphilis, we may hope for a far more scientific determination of these questions by review boards during and after the war.
20. Key issues regarding pensions, retirement, and compensation are highlighted, and since no previous war has utilized the Wassermann reaction and other precise tests related to the nature, progression, and treatability of neurosyphilis, we can expect a much more scientific evaluation of these matters by review boards during and after the war.
21. We find a few instances in which neurosyphilis has played a part in the discipline of troops. According to one author (Thibierge, 1917), syphilis has become a genuine epidemic among French soldiers and mobilized munition workers. In Germany, also, it may be remembered that Hecht has claimed that no less than an equivalent of sixty army divisions has been temporarily withdrawn from fighting on the Teutonic side for venereal diseases. In this connection, Neisser had recommended the giving of salvarsan and mercury in the trenches. According to Hecht, the appearance of syphilis should be a signal for sending a man to the front. Hecht also made the somewhat bizarre suggestion that special companies of syphilitics should be formed, for convenience of treatment, on the firing line.
21. There are a few cases where neurosyphilis has influenced the discipline of troops. One author (Thibierge, 1917) notes that syphilis has become a real epidemic among French soldiers and mobilized munitions workers. In Germany, Hecht has pointed out that around the equivalent of sixty army divisions has been temporarily pulled from combat on the Teutonic side due to venereal diseases. In this context, Neisser suggested administering salvarsan and mercury in the trenches. According to Hecht, the onset of syphilis should trigger sending a person to the front lines. Hecht also made the rather unusual proposal to form special companies of syphilitics for easier treatment on the battlefield.
22. A more solid foundation is laid for the theory that general paresis may be evoked by trauma—a conclusion already fairly well established by civilian cases, notably those of industrial accident.
22. A stronger basis is forming for the idea that general paresis can be triggered by trauma—a conclusion that's already been reasonably established through civilian cases, especially those involving industrial accidents.
23. The question whether shell-shock (the physical event) can produce general paresis is probably to be settled in the affirmative, for it may always prove difficult to show that the physical shell-shock did not actually produce mechanical molar lesions of the brain, permitting the rapid advance of spirochetes. It is perhaps easier to prove that shell explosion may precipitate neurosyphilis in the form of tabes dorsalis (take, for example, Cases 21 and 22). The cases of most importance in the question of traumatic neurosyphilis and traumatic paresis are cases 20, 21, 22, 24 and 25.
23. The issue of whether shell shock (the physical event) can lead to general paresis is likely to be answered positively, as it may always be difficult to demonstrate that the physical shell shock didn't actually cause mechanical damage to the brain, allowing for the rapid spread of spirochetes. It might be simpler to show that a shell explosion can trigger neurosyphilis in the form of tabes dorsalis (for example, look at Cases 21 and 22). The most significant cases concerning traumatic neurosyphilis and traumatic paresis are cases 20, 21, 22, 24, and 25.
26. It must be said that presumably there will be, unless our authorities are more successful than in the past, a considerable increase in venereal disease as the result of army life in wartime. There will be a certain number of cases of neurosyphilis a number of years after discharge from the army caused by infection acquired during service. (Germany is said to have got its crop of neurosyphilis after the War of 1870, in the early eighties of the last century.) The names of all soldiers acquiring syphilis and not considered cured at the time of discharge should, under ideal conditions, be given to health organizations in their home states so that they may be accorded proper care and treatment.
26. It should be noted that there will likely be, unless our authorities do better than before, a significant increase in sexually transmitted diseases due to military life during wartime. A certain number of cases of neurosyphilis will emerge several years after soldiers are discharged, caused by infections contracted during their service. (It's said that Germany faced a rise in neurosyphilis after the War of 1870, in the early 1880s.) Ideally, the names of all soldiers who contract syphilis and are not considered cured at the time of their discharge should be forwarded to health organizations in their home states so that they can receive appropriate care and treatment.
27. Shell-shock and epilepsy. The authorities have been somewhat surprised by the number of epileptics that have gotten by the draft boards. The statistics are not yet ripe, but certainly the enlistment of an epileptic is not a rarity. There are some singular instances in the war literature showing how hard it sometimes is to bring out epilepsy. There is the English case, for example, of a man, an epileptic’s son, who had himself been epileptic from 11-18, who entered the Expeditionary Force at the outbreak of hostilities, went[840] through the retreat from Mons and through two years of active warfare without having a single epileptic convulsion. In fact, in September, 1916, he was put in charge of eight men on guard duty. Apparently the new responsibilities worried him, and two months later he had become epileptic to the extent of petit mal.
27. Shell-shock and epilepsy. The authorities have been somewhat surprised by the number of people with epilepsy that have passed through the draft boards. The statistics are still coming in, but it's clear that enlisting someone with epilepsy isn't uncommon. There are some unique cases in wartime literature that show how difficult it can be to identify epilepsy. For instance, there's the English case of a man, the son of an epileptic, who himself had epilepsy from ages 11 to 18. He joined the Expeditionary Force at the start of the war, went[840] through the retreat from Mons, and participated in two years of active combat without experiencing a single epileptic seizure. In fact, in September 1916, he was given responsibility for eight men on guard duty. It seems that the new responsibilities stressed him out, and two months later he began experiencing seizures, including petit mal.
Another man who had never been epileptic (though his sisters had been) was wounded four times, was never worried by shell fire, got somewhat depressed after the death of his father and five brothers in the service, but did not become epileptic until finally he was blown up and buried three times in one day, and it was a whole month later when he became epileptic, although treatment by rest and bromides apparently resolved the affair.
Another man who had never had epilepsy (although his sisters did) was injured four times, was never scared by gunfire, became somewhat depressed after the death of his father and five brothers in the military, but didn’t develop epilepsy until he was blown up and buried three times in one day. It was a full month later when he developed epilepsy, although treatment with rest and bromides seemed to resolve the issue.
Other cases seem to show that war experiences can bring out epilepsy, although in most instances it would appear that there was an epileptic or otherwise neuropathic heredity in these cases.
Other cases suggest that war experiences can trigger epilepsy, although in most instances, it appears that there was an existing hereditary predisposition to epilepsy or other neurological issues in these cases.
28. There is one author, Ballard, who has actually propounded a theory of Shell-shock as epileptic, pointing out the occurrence of epilepsy long after the early symptoms of Shell-shock have disappeared.[10] There does not appear to[841] have been any increase in epileptics as the result of the war, either from the standpoint of Shell-shock or from the standpoint of brain injury, so far as the records of the National Hospital for the Paralyzed and Epileptic in London are able to show.
28. One author, Ballard, has actually proposed a theory that shell shock can be seen as epilepsy, noting that epilepsy can occur long after the initial symptoms of shell shock have faded.[10] It seems that[841] there hasn't been any increase in epilepsy cases resulting from the war, whether from shell shock or brain injuries, based on records from the National Hospital for the Paralyzed and Epileptic in London.
[10] In one instance, fugue and other minor symptoms were later replaced by epilepsy; in another, an epileptic confusion developed eight months after an explosion, and in a third, a case of mine explosion, stammering resolved into mutism and mutism finally into epilepsy. Of course there is a so-called general resemblance among all forms of hyperkinesis or irritative discharge of the nervous system. If we term epileptic all the things that various authors have termed epileptoid, we may be doing nothing more than to say that we believe these cases all subject to epileptic hyperkinesis. In that direction, of course, it has long been said that dipsomania was really a form of epilepsy. Whether Shell-shock is ordinarily subject to recurrence in such wise as to imitate the recurrence of attacks of dipsomania, of manic-depressive psychosis or of epilepsy, is, to say the least, doubtful at this time.
[10] In one case, symptoms like fugue and others eventually turned into epilepsy; in another, an epileptic episode occurred eight months after an explosion, and in a third case of a mine explosion, stammering changed to mutism and then mutism eventually became epilepsy. Clearly, there’s a general similarity among all types of hyperkinesis or irritative discharges of the nervous system. If we label everything that various authors have called epileptoid as epileptic, we might just be stating that we believe all these cases are subject to epileptic hyperkinesis. It has long been suggested that dipsomania is actually a form of epilepsy. Whether Shell-shock typically recurs in a way that mimics the recurrence of dipsomania, manic-depressive psychosis, or epilepsy is, at the very least, uncertain at this time.
29. As in all other instances of mental or nervous disease, when an epileptic returns from the war, whether or not he was potentially or actually an epileptic before the war, his relatives are bound to term him a case of Shell-shock. I am familiar with a case in a hospital in a certain Atlantic port, a case of pronounced and obvious epilepsy. In the wards he is treated as the hero of every occasion. Not only the nurses and attendants, but the other patients and often the physicians can hardly resist thinking of him as somehow a case of Shell-shock. It is a comment upon the status of mental hygiene in general that this self-same epileptic, had there been no war, would have been, as it were, a common or garden epileptic, mute and inglorious on some sunny hillside.
29. Just like in all other cases of mental or nervous illness, when an epileptic returns from the war, whether he had the condition before the war or not, his family tends to label him as a case of Shell-shock. I know of a case in a hospital at a certain Atlantic port, involving a clear and obvious epilepsy. In the wards, he is treated as a hero in every situation. Not just the nurses and staff, but also the other patients and often the doctors struggle to see him as anything other than a case of Shell-shock. It highlights the state of mental health care that this same epileptic, if there had been no war, would have been seen as just another ordinary epileptic, quietly living out his life on some sunny hillside.
30. In passing I may note how many instances in the medicolegal part of the war literature there are of epileptics who come up for courtmartial or for medical examination pending courtmartial. We may suspect that many a case of epileptic fugue has been regarded as a case of desertion. There is the case of an epileptic who left camp one morning and got drunk. Investigation showed that he left camp before anything epileptoid had happened. He developed in his drunkenness a pretty clearly epileptic crisis with great violence, for which he had a complete loss of memory. The French Council condemned him to five years of labor, not admitting in this instance that responsibility was diminished by reason of the man’s being epileptic. In short, from the military point of view, he should, so to say, have known enough not to have gotten drunk, and so have avoided getting his epileptic crisis. Of course the decision was here very close, and a like decision would not always be rendered. To add to the complication of this particular case, the very first epileptoid crisis which caused it to be known that the man fell into the epileptic group was due to Shell-shock, or at least developed immediately after the bursting of a shell[842] nearby. On the whole, however, the relation between epilepsy and Shell-shock is not a close one.
30. It's worth mentioning how many instances in the medicolegal sections of wartime literature feature epileptics facing court-martial or undergoing medical evaluations due to pending court-martial. We can suspect that many cases of epileptic fugue have been misinterpreted as desertion. Take, for example, the case of an epileptic who left his camp one morning and got drunk. Investigations revealed that he had left camp before any epileptic episodes occurred. He experienced a very clear epileptic crisis in his drunken state, marked by intense violence, resulting in complete memory loss. The French Council sentenced him to five years of hard labor, not acknowledging that his accountability was lessened due to his epilepsy. Essentially, from a military perspective, he should have known better than to get drunk, thus avoiding his epileptic episode. Obviously, the decision was very nuanced, and such a ruling wouldn't always be made in similar cases. To complicate matters, the very first epileptoid episode that identified him as part of the epileptic group was triggered by Shell shock, or at least manifested right after a shell[842] exploded nearby. Overall, however, the connection between epilepsy and Shell shock isn’t a strong one.
31. The question of epilepsy in the war is considered in a series of 33 cases (Cases 53-85). The considerations range from banal cases developing quite incidentally, up to cases regarded by one author (Ballard) as illustrating a theory of Shell-shock as epileptic (Cases 82-84). First are considered two cases actually syphilitic. In the first (Case 53), the diagnosis had to be revised from epilepsy to neurosyphilis (the convulsions of this neurosyphilitic were brought out by alcohol, and the reporter, Hewat, remarks that the serum of any patient developing epileptiform seizures between 35 and 50 years of age should be subject to test). In Case 54, the soldier got his syphilis in wartime and the syphilis acted to bring out an epilepsy with which the patient was hereditarily tainted (epilepsy syphilogenic, i.e., reactive to syphilis).
31. The question of epilepsy in the war is examined through a series of 33 cases (Cases 53-85). The observations range from straightforward cases that developed incidentally to cases that one author (Ballard) argues illustrate a connection between shell shock and epilepsy (Cases 82-84). First, two syphilitic cases are discussed. In the first case (Case 53), the diagnosis was changed from epilepsy to neurosyphilis (the convulsions in this neurosyphilis patient were triggered by alcohol, and the reporter, Hewat, notes that the serum of any patient experiencing epileptiform seizures between the ages of 35 and 50 should be tested). In Case 54, the soldier contracted syphilis during wartime, and the syphilis triggered an epilepsy of hereditary origin (syphilogenic epilepsy, i.e., reactive to syphilis).
Case 55 might perhaps better have been considered in the group of hypophrenoses, as he was epileptic and imbecile. He was at first condemned by court martial to five years’ imprisonment for leaving his post in the presence of the enemy.
Case 55 might have been better classified within the group of hypophrenoses, as he was epileptic and had an intellectual disability. He was initially sentenced by a military court to five years in prison for abandoning his post during combat.
Another mixed case is Case 57, in which another feeble-minded subject showed seizures of a psychogenic nature, which he was able eventually to stop by clenching his teeth.
Another mixed case is Case 57, in which another intellectually challenged subject experienced psychogenic seizures, which he was eventually able to stop by clenching his teeth.
Seven cases (Cases 58-64) are cases of a disciplinary nature, amongst which attention may be called to Case 62, the “specialist in escapes.” The medicolegal questions of responsibility in the drunken epileptic (Case 58) are particularly perplexing.
Seven cases (Cases 58-64) involve disciplinary issues, including Case 62, the “escape expert.” The legal questions surrounding responsibility in the case of the drunken epileptic (Case 58) are especially complicated.
32. Case 64 is one of epilepsy following antityphoid inoculation one-half hour. There were five attacks during a fortnight and then no others. The antityphoid inoculation came eight weeks after a shell wound of the thigh, which had not served to bring out the epilepsy in this patient. Bonhoeffer had three other instances of the sort: one in a severely tainted subject, and the others in alcoholics.
32. Case 64 is one of epilepsy following antityphoid inoculation one-half hour. There were five seizures over a two-week period, and then no more. The antityphoid inoculation happened eight weeks after a shell wound to the thigh, which did not trigger the epilepsy in this patient. Bonhoeffer had three other similar cases: one in a severely affected individual and the others in people with alcohol dependency.
33. The next group of cases, 66-77, yields a series of the most interesting medical problems, some of which scarcely[843] belong in an account of psychoses incidental in the war. Case 66 is one with recovery from Jacksonian seizures after decompression of the upper Rolandic region, which was edematous following an (apparently very slight) scalp wound and shell-shock.
33. The next group of cases, 66-77, presents a series of the most intriguing medical issues, some of which hardly[843] fit in a discussion about psychoses related to the war. Case 66 is one case where the patient recovered from Jacksonian seizures after decompressing the upper Rolandic region, which had swelling due to an (seemingly very minor) scalp injury and shell shock.
35. The theoretical implications of Case 69 are striking: The case was one of musculo-cutaneous neuritis (gross enlargement), in association with which Brown-Séquard’s epilepsy developed, waxing and waning with the disease of the nerve. Another case of possible reactive epilepsy is Case 70, and a case of epilepsia tarda brings up the same issue (Case 71). Cases 72-74 are cases with strong psychogenic components, of which Case 74 is particularly instructive on account of the gradual building up of a remarkable visual aura of an approaching fire-wheel, this aura developing after scotoma from looking at the sun. Cases 75 and 76 are cases of somewhat doubtful epilepsy, one of fugue and the other of a solitary epileptic episode following 38 artillery battles in two months.
35. The theoretical implications of Case 69 are striking: The case involved musculo-cutaneous neuritis (notable swelling), which was associated with the development of Brown-Séquard’s epilepsy, fluctuating alongside the nerve condition. Another instance of potential reactive epilepsy is Case 70, and a case of epilepsia tarda raises the same concern (Case 71). Cases 72-74 includes cases with significant psychogenic components, particularly Case 74, which is noteworthy due to the gradual emergence of an incredible visual aura resembling a fire-wheel, developing after experiencing a scotoma from staring at the sun. Cases 75 and 76 involve somewhat questionable epilepsy, one related to fugue and the other to a singular epileptic episode occurring after 38 artillery battles in two months.
36. Friedmann discusses narcoleptic seizures, regarded as due to the brain fag of trench life (Case 77). Sham fits and epileptoid attacks controllable by will appear in Cases 78 and 79 respectively. Case 80 is a striking case of a man with epileptic taint, which two years’ service, four wounds, the death of a father and five brothers, and eventually Shell-shock and burial thrice in one day, served at last to bring out.
36. Friedmann talks about narcoleptic seizures, which are seen as a result of the mental fatigue from trench life (Case 77). Fake seizures and seizures that can be controlled by willpower show up in Cases 78 and 79 respectively. Case 80 is a notable example of a man with a genetic predisposition to epilepsy, which two years of service, four wounds, the death of a father and five brothers, and eventually Shell-shock and being buried three times in one day ultimately revealed.
37. Shell-shock and bodily disease. In civilian psychopathic hospital practice, if a case is not syphilitic, not feeble-minded, not epileptic, not alcoholic, and without signs of intracranial pressure or disorder of reflexes, then we, as specialists, must consider whether the disease in question is not due to some form of bodily disorder outside the nervous system; for example, we think in practice of infectious psychoses, of exhaustive states such as the puerperium, of toxic states[844] such as may be found in cardiorenal cases, and of glandular phenomena such as we are familiar with in the thyroid disorders.
37. Shell-shock and bodily disease. In civilian psychiatric hospitals, if a case isn’t related to syphilis, isn’t affected by mental disability, isn’t epileptic, isn’t alcohol-related, and shows no signs of intracranial pressure or reflex issues, then we, as specialists, must consider whether the illness might be linked to some form of physical disorder outside the nervous system. For instance, we think about infectious psychoses, exhausting conditions like those that occur post childbirth, toxic conditions such as those found in heart and kidney cases, and glandular issues like those we see in thyroid disorders.[844]
Under the war conditions, it might be thought that these somatic disorders yielding the so-called symptomatic mental diseases would be frequently found.
Under wartime conditions, one might think that these physical disorders leading to what's known as symptomatic mental illnesses would be common.
Aside from these rarities in puzzling diagnosis, we find more commonly in the literature evidence of
Aside from these rare and puzzling diagnoses, we more often find evidence of
38. The soldier’s heart, the so-called “D.A.H.,” or disordered action of the heart, of the English army reports. This soldier’s heart is sometimes associated with hyperthyroidism, and sometimes hyperthyroidism is found alone, with symptoms suggesting those of a sort of diffuse Shell-shock.
38. The soldier’s heart, known as “D.A.H.” or disordered action of the heart, is reported in the English army. This soldier’s heart is sometimes linked to hyperthyroidism, and at other times, hyperthyroidism occurs on its own, with symptoms that resemble a kind of widespread Shell-shock.
One author claims rapid cures of hyperthyroidism by the relatively simple process of hypnosis. Perhaps this is not too unlikely in view of the still obscure relations between mind and hormones. A little more surprising, perhaps, is the assertion met with that psoriasis is sometimes a Shell-shock phenomenon.
One author suggests quick fixes for hyperthyroidism through the fairly straightforward method of hypnosis. This might not be too surprising considering the still unclear connections between the mind and hormones. What’s maybe more surprising is the claim that psoriasis can sometimes be a result of Shell shock.
The literature clearly shows, however, that, as in most special problems, the internist is still in demand. I recall how one internist was misled on the witness stand into stating that he was a “general specialist.” This is what we would all need to be, were we to solve the problems of Shell-shock in the time allotted to us by the war.
The literature clearly shows, however, that, like in most specialized issues, the internist is still needed. I remember how one internist was misled on the witness stand into saying he was a “general specialist.” This is what we would all need to be if we were to solve the problems of Shell-shock in the time given to us by the war.
39. Following are special cases to show how near the somatic (“symptomatic”) may be to Shell-shock.
39. Here are special cases that demonstrate how close the somatic (“symptomatic”) can be to Shell-shock.
The somatic group of psychoses, sometimes termed symptomatic, is illustrated in 29 cases (Cases 118-146), and comprises cases ranging all the way from rabic phenomena to those of hyperthyroidism. Possibly the first two cases (Cases 118 and 119) might better be placed among the encephalopsychoses. Case 118, one of rabies, was that of a farmer without history of having been bitten by a dog, who eventually came to autopsy and received the Pasteur Institute diagnosis of rabies. A diagnosis of angina was at first made. When the symptoms became more serious and masseter spasm developed, a question of tetanus arose. Later[845] the diagnosis of meningitis was suggested. At this point, the symptoms became predominantly psychotic.
The somatic group of psychoses, sometimes called symptomatic, is shown in 29 cases (Cases 118-146) and includes cases from rabid episodes to those of hyperthyroidism. The first two cases (Cases 118 and 119) might be better categorized under encephalopsychoses. Case 118, which involved rabies, was that of a farmer who had no history of being bitten by a dog and ultimately underwent an autopsy, receiving a diagnosis of rabies from the Pasteur Institute. Initially, he was diagnosed with angina. However, as his symptoms worsened and he developed masseter spasm, tetanus became a possible diagnosis. Later, the possibility of meningitis was raised. At this point, his symptoms were primarily psychotic.
Case 119 was one of seven cases reported by Lumière and Astier, in which delirium and hallucinations appeared as a complication of tetanus. The case in question had been given anti-tetanic serum. (Another case showed identical symptoms without having been given anti-tetanic serum.)
Case 119 was one of seven cases highlighted by Lumière and Astier, where delirium and hallucinations were complications of tetanus. The specific case had received anti-tetanic serum. (Another case displayed the same symptoms without receiving anti-tetanic serum.)
That a local tetanus could be mistaken for hysteria might seem à priori unlikely, but Cases 120 and 121 indicate as much; and Case 121 is interesting on account of the officer’s own description of his local tetanus and its treatment. A psychosis apparently related with dysentery occurred in Case 122. Hysteria followed typhoid fever in Case 123. Another form of typhoid fever complication is perhaps shown in Case 124, wherein the diagnostic question lay between dementia praecox and a post-typhoid encephalitis.
That a local tetanus could be confused with hysteria might seem unlikely, but Cases 120 and 121 suggest otherwise; and Case 121 is noteworthy because of the officer’s own description of his local tetanus and its treatment. A psychosis seemingly linked to dysentery occurred in Case 122. Hysteria followed typhoid fever in Case 123. Another type of typhoid fever complication is possibly shown in Case 124, where the diagnostic question was between dementia praecox and a post-typhoid encephalitis.
Diphtheria was also represented in the matter of nervous and mental symptoms in Cases 127 and 128. In Case 127 the nervous symptoms appeared eight days after evacuation for diphtheria. There were a few sensory symptoms (hypalgesia, hypoacusia, and peculiar bone sensations) in this subject. The phenomenon in Case 128 was apparently one of hysterical paraparesis; nor does it appear in this case that the hysterical paralysis was preceded by polyneuritis.
Diphtheria was also reflected in the nervous and mental symptoms in Cases 127 and 128. In Case 127, the nervous symptoms showed up eight days after treatment for diphtheria. This subject experienced a few sensory symptoms (reduced sensitivity, decreased hearing, and unusual bone sensations). The situation in Case 128 seemed to be a case of hysterical leg weakness; it also doesn't seem that this case had hysterical paralysis that was preceded by polyneuritis.
Malarial effects are present in three cases (Cases 129-131), of which Case 129 showed an amnesia, Case 130 a Korsakow syndrome, and Case 131 anterior horn symptoms. Case 132 exemplifies 15 instances of acroparesthetic disorders in so-called trench foot. This case, like several others, is inserted in this group, not because the symptoms are psychotic, but because they might cause diagnostic difficulty as against hysterical phenomena.
Malarial effects are observed in three cases (Cases 129-131), of which Case 129 demonstrated amnesia, Case 130 exhibited Korsakow syndrome, and Case 131 showed anterior horn symptoms. Case 132 highlights 15 instances of acroparesthetic disorders in what's known as trench foot. This case, like several others, is included in this group not because the symptoms are psychotic, but because they may lead to diagnostic challenges compared to hysterical phenomena.
Case 133 is an autopsied case of bronchopneumonia following bullet injury of the spine. Microscopic examination of the spinal cord showed small cavities in the first and fourth[846] dorsal segments. This myelomalacia was doubtless related with the bullet injury of the spine, although the spinal cord was not itself directly touched by the bullet. Case 134 might be regarded perhaps as one of Shell-shock and should be considered in relation with the cases at the head of Section B (Cases 197-209). The case might be regarded as functional, except for a decubitus that developed. Despite this decubitus, there was recovery. The case is placed in the somatic group on account of pulmonary phenomena which it seemed well to relate with those of Case 133. Compare also Case 136, in which reflex phenomena are associated with a bullet wound of the pleura. Case 135 is a many-sided case, with ante-bellum hysteria and certain Shell-shock phenomena. While under observation, the patient caught typhoid fever and then developed neuritis. This neuritis was very probably not post-typhoidal so much as hysterical. Accordingly, the case should be considered in connection with the ante-bellum weak spot series, Section B (Cases 286-301). There was in this case a cure by reëducation.
Case 133 is a case of bronchopneumonia that occurred after a bullet injury to the spine. Microscopic examination of the spinal cord showed small cavities in the first and fourth[846] dorsal segments. This myelomalacia was likely related to the bullet injury of the spine, even though the bullet didn't directly impact the spinal cord. Case 134 could be seen as a form of Shell-shock and should be evaluated in relation to the cases at the head of Section B (Cases 197-209). The case might be viewed as functional, except for a pressure sore that developed. Despite this sore, there was recovery. The case is classified in the somatic group due to pulmonary phenomena that appeared to be connected with those of Case 133. Also refer to Case 136, where reflex phenomena are linked to a bullet wound of the pleura. Case 135 presents a complex situation, involving pre-war hysteria and certain Shell-shock symptoms. While being observed, the patient contracted typhoid fever and then developed neuritis. This neuritis was likely not post-typhoidal but rather hysterical. Therefore, the case should be considered in connection with the pre-war weak spot series, Section B (Cases 286-301). In this case, there was recovery through re-education.
The reflex hemiplegia with double ulnar syndrome in Case 136 seemed to have followed a bullet wound of the pleura. According to the authors, Phocas and Gutmann, there is considerable literature upon nerve complications of pleura trauma, including syncope, epilepsy, and (more rarely) hemiplegia.
The reflex hemiplegia with double ulnar syndrome in Case 136 appeared to have come after a bullet wound of the pleura. The authors, Phocas and Gutmann, noted that there is a significant amount of literature on nerve complications from pleural trauma, including fainting, epilepsy, and (less commonly) hemiplegia.
Heart cases are illustrated by Cases 137-139: the first one of hysterical tachypnoea, and the others of the so-called soldiers’ heart.
Heart cases are illustrated by Cases 137-139: the first one of hysterical rapid breathing, and the others of what's known as soldiers’ heart.
Diabetes mellitus seems to have followed war strain and shell wound in Case 140.
Diabetes mellitus seems to have come after war injuries and shell wounds in Case 140.
It is doubtful whether shell-shock and burial had anything to do with the appearance ten days later of lipomata, which proved to be the initial phenomenon in a pronounced Dercum’s disease. (Case 141).
It’s uncertain if shell shock and burial were related to the emergence of lipomata ten days later, which turned out to be the first sign of a clear case of Dercum’s disease. (Case 141).
Hyperthyroidism is illustrated in four cases (Cases 142-144). The first (Case 142) appears to have been cured by inducing deep somnambulism (Tombleson claims cures by suggestion in eight cases of hyperthyroidism). Neurasthenia or questionable Graves’ disease (Case 145) followed Shell-shock. That[847] of Case 144 followed 10 months’ service, at times under protracted shell fire. A forme fruste of Graves’ disease is shown in Case 145, in which the phenomena followed gassing and shelling.
Hyperthyroidism is illustrated in four cases (Cases 142-144). The first (Case 142) seems to have been cured by inducing deep sleepwalking (Tombleson reports cures through suggestion in eight cases of hyperthyroidism). Neurasthenia or questionable Graves’ disease (Case 145) followed Shell-shock. That[847] of Case 144 came after 10 months of service, sometimes under prolonged shell fire. A forme fruste of Graves’ disease is shown in Case 145, in which the symptoms followed exposure to gas and shelling.
A somewhat curious somatic complication in a case of Shell-shock hysteria was the finding of a needle in the left upper arm, which was then extracted. (Case 146).
A somewhat curious somatic complication in a case of shell shock hysteria was the discovery of a needle in the left upper arm, which was then removed. (Case 146).
The Nature of War Trauma
40. Regarding our rough delimitation of the Shell-shock group as well in hand, having put upon one side three of the most disturbing groups (save one) in our process of demarcation, we must proceed to the Shell-shock material itself: a material now definable as assuredly non-syphilitic, non-epileptic, non-somatic,[11] as beyond question without narrow relations with feeble-mindedness, alcohol and drug states, schizophrenia and cyclothymia, and as probably of the general nature of the psychoneuroses.
40. Now that we have a rough outline of the Shell-shock group, having set aside three of the most troubling categories (except for one) in our classification, we need to focus on the Shell-shock material itself: a category that is clearly non-syphilitic, non-epileptic, and non-somatic,[11] and definitely not closely related to issues like intellectual disability, substance abuse, schizophrenia, or cyclothymia, and is likely part of the broader category of psychoneuroses.
Note that in this epicrisis I have designedly not followed the order of presentation of the text materials. The process of diagnosis per exclusionem in ordine which I find most serviceable in civilian psychopathic hospital practice is the elimination of possibilities in the order presented in Chart 1 or in Paragraph 10 of this epicrisis. Because this book will find its greatest use in peace times as a kind of illustrative commentary on the peace material that presents itself in general practice or in psychopathic hospital voluntary, temporary-care, and out-patient practice, I chose to arrange the delimiting material according to the order of the practical key devised for civilian practice. We may now profitably change our order of consideration and consider whether
Note that in this epicrisis, I've intentionally not followed the order in which the text materials are presented. The process of diagnosis per exclusionem in ordine, which I find most helpful in civilian psychopathic hospital practice, involves eliminating possibilities in the order presented in Chart 1 or Paragraph 10 of this epicrisis. Since this book will be most useful during peacetime as a type of illustrative commentary on the peace material that comes up in general practice or in voluntary, temporary-care, and outpatient practice at psychopathic hospitals, I decided to organize the delimiting material according to the practical key created for civilian practice. Now we can beneficially change our order of consideration and examine whether
41. The most practical key or sequence of consideration in the endeavor to delimit Shell-shock neuroses is probably: Exclude (1) syphilis, (2) epilepsy, (3) somatic disease (of a sort able to produce “symptomatic” effects somewhat like those of Shell-shock).
41. The most practical key or sequence of consideration in figuring out Shell-shock neuroses is probably: Exclude (1) syphilis, (2) epilepsy, (3) physical illnesses (that could produce “symptomatic” effects similar to those of Shell-shock).
Below I shall still permit myself some general words concerning the other more easily excluded groups because of the light which feeble-mindedness, alcoholism, schizophrenia, cyclothymia, and even old age can theoretically throw on the nature of Shell-shock.
Below I will still allow myself to share some general thoughts about the other groups that are often excluded, as they can, in theory, shed light on the nature of Shell-shock, such as those with intellectual disabilities, alcoholism, schizophrenia, cyclothymia, and even old age.
42. Suppose then that syphilis, epilepsy, and somatic (non-nervous) disease are out of the running, we come practically down to the psychoneuroses, knowing that knotty problems are at hand in telling them from structural traumatic effects: But, after all, what are functional neuroses? What do we really know about the neuroses other than to say that they are not distinguished by the existence of the structural lesions which characterize organic disease of the nervous system? Is not the definition of neurosis purely by negatives? However true this definition by negatives may be from the genetic and general pathological viewpoint, the work of Charcot and in particular of Babinski has yielded a number of positive features from the clinical viewpoint, which to some degree make up for the lack of anything positive in the neurones themselves as studied post-mortem. An eminent German has recently declared that the data of this war itself go far to prove some of the long dubious contentions of the Frenchman, Charcot; and the work of Babinski during the war has strengthened and developed the conceptions of his master, Charcot, as well as the ante-bellum conceptions of Babinski himself.
42. Let’s assume that syphilis, epilepsy, and physical (non-nervous) illness are not the issues, we are left mainly with psychoneuroses, knowing that there are complex challenges in distinguishing them from structural traumatic effects: But really, what exactly are functional neuroses? What do we actually know about neuroses besides the fact that they are not identified by the structural damage that defines organic diseases of the nervous system? Isn’t the definition of neurosis mainly based on what it isn’t? Although this negative definition may hold true from a genetic and general pathological perspective, the work of Charcot and especially Babinski has provided several positive characteristics from a clinical perspective, which somewhat compensates for the lack of concrete findings in the neurons themselves as studied after death. A prominent German has recently claimed that the data from this war significantly support some of the long-debated arguments of the Frenchman, Charcot; and Babinski's work during the war has reinforced and advanced the ideas of his mentor, Charcot, as well as Babinski’s own pre-war concepts.
43. Let me insist that the problem is practical enough: Organic versus functional neurosis. The point I want to make is that, when so much theoretical doubt concerning organic and functional neuropathy holds sway, the practical doubts in the individual case under the varying conditions of civilian practice and in the upheavals of military practice, must be still more in evidence. Case after case described in the literature of every belligerent has passed from pillar to post and from post to pillar before diagnostic resolution and therapeutic success. Colleagues meeting, for example, at the Paris Neurological Society, find themselves reporting the same case from different standpoints,—the one announcing a semi-miraculous cure of a case which another had[849] months before claimed only as a diagnostic curiosity. In the midst of such discussions and controversies, there must inevitably be a renaissance in neurology.
43. Let me emphasize that the issue is quite practical: Organic versus functional neurosis. What I want to highlight is that, with so much theoretical uncertainty surrounding organic and functional neuropathy, the practical doubts in individual cases—given the varying conditions of civilian practice and the changes in military practice—are even more significant. Case after case described in the literature of each warring nation has gone back and forth without clear diagnostic or therapeutic resolution. Colleagues meeting, for example, at the Paris Neurological Society, often find themselves discussing the same case from different perspectives—the one reporting a somewhat miraculous recovery of a case that another had[849] months earlier only identified as a diagnostic oddity. In the midst of such discussions and debates, a revival in neurology is bound to emerge.
44. In cases of alleged Shell-shock, the hypothesis of focal structural damage to the nervous system or its membranes has to be raised.
44. In cases of reported Shell-shock, we need to consider the possibility of localized structural damage to the nervous system or its membranes.
Shell bursts and other detonations can produce hemorrhage in the nervous system and in various organs without external injury. Thus a man died from having both his lungs burst from the effects of a shell exploding a meter away. Hemorrhage into the urinary bladder has been identically produced. Lumbar puncture yields blood in sundry cases of shell explosion without external wound, and Babinski has a case of hematomyelia produced while the victim was lying down, so that the factor of direct violence through fall can be excluded. In sundry cases, not only blood but also lymphocytes have been found, sometimes in a hypertensive puncture fluid.
Shell explosions and other blasts can cause bleeding in the nervous system and in various organs without any visible injuries. For example, a man died because both of his lungs ruptured from the effects of a shell detonating just a meter away. Similar bleeding has occurred in the urinary bladder. A lumbar puncture can show blood in several cases of shell explosions even with no external wounds, and Babinski documented a case of hematomyelia that occurred while the victim was lying down, eliminating the possibility of direct injury from a fall. In various cases, not only blood but also lymphocytes have been found, sometimes in a fluid under pressure.
45. Moreover, in cases of alleged Shell-shock there may be a combination of structural and functional disease.
45. Additionally, in cases of claimed Shell-shock, there might be a mix of both structural and functional issues.
A herpes or the graying-out of hair overnight can suggest organic changes. A case may combine lost knee-jerks (suggesting organic disease) with urinary retention (suggesting functional disorder).
A herpes outbreak or suddenly graying hair can indicate physical changes. A situation might include lost knee-jerk reflexes (which suggest a physical illness) along with urinary retention (which points to a functional issue).
46. Again, there is a group of war neuroses, especially clearly brought out in cases of ear injury, in which the functional disorder surrounds the organic as a nucleus. But these “periorganic” neuroses are no proof that the neuroses in question are organic in nature. Hysterical anesthesia, paralysis, or contracture may occur on the side of the body which has received a wound: the process of such a peritraumatic disorder is, nevertheless, a functional process.
46. Again, there is a group of war-related psychological disorders, especially evident in cases of ear injuries, where the functional disorder revolves around the organic injury as its core. However, these “periorganic” disorders do not prove that the neuroses are of an organic nature. Hysterical numbness, paralysis, or muscle tightening can occur on the side of the body that has been wounded: the nature of such a peritraumatic disorder is, nonetheless, a functional issue.
47. But, when the problem is statistically taken, the majority of cases of alleged Shell-shock without external wound prove to be functional, as indicated by their clinical pictures. Thus, after a mine explosion, a man was hemiplegic, tremulous and mute. After sundry vicissitudes, the tremors were hypnotized away. Then the mutism vanished, to be supplanted by stuttering. Finally the hemiplegia remained. So far as[850] the mutism and the tremors went, this man might belong in the majority group of Shell-shock cases, namely, the functional group. Assuming the hemiplegia to be really organic, we should regard this man as a mixed case, organic and functional.
47. However, when analyzing the issue statistically, most cases of reported Shell-shock without any visible injury turn out to be functional, as shown by their clinical presentations. For instance, after a mine explosion, a man became paralyzed on one side, shaky, and unable to speak. After various treatments, the shaking was resolved through hypnosis. Then, he began to speak again, but with stuttering. Ultimately, the paralysis on one side remained. In terms of[850] his inability to speak and the shaking, he could be categorized as part of the majority group of Shell-shock cases, which is the functional group. Assuming the paralysis is truly organic, we should consider this man a mixed case, combining both organic and functional elements.
48. But do we not know all we need to know or all we are likely to know about the neuroses already from old civilian studies? There are some cases without very close relations to the war: Thus, we conceive of (a) psychoneuroses incidental to the war and such that they might very probably have developed without the entrance of war factors; and on the other hand, we conceive of (b) psychoneuroses (to be dealt with in extenso later) in which war factors (either physical Shell-shock or other factors) forcibly enter. There are in this group of incidental psychoneuroses 12 cases. The first, described as a constitutional intimiste, a psychasthenic en herbe, was one in which a hallucination was developed in the field, and in which three phases of a psychopathic nature—(a) over-emotionality, (b) obsessions, (c) loss of feeling of reality—developed. In this case the war work at first seemed to better the man’s general condition, and he gave two years of effective service. This officer in effect invented his own Shell-shock equivalent in a hallucination of Germans appearing in his trench. The case may be compared with one described in Section B, namely, Case 347: that of a Russian soldier who developed perfectly characteristic war dreams, though his entire service had been rendered in the rear and he had not had experiences in action.
48. But don’t we already know everything we need to know or all we’re likely to know about neuroses from past civilian studies? There are some cases that aren't very closely related to the war: First, we think of (a) psychoneuroses related to the war that probably would have developed even without the war factors; on the other hand, we consider (b) psychoneuroses (which will be discussed in extenso later) where war factors (like physical shell-shock or other influences) play a significant role. In this group of incidental psychoneuroses, there are 12 cases. The first, described as a constitutional intimiste, a psychasthenic en herbe, experienced a hallucination in the field, leading to three phases of a psychopathic nature—(a) heightened emotions, (b) obsessions, (c) loss of the sense of reality. In this case, the war service initially seemed to improve the man's overall condition, and he served effectively for two years. This officer essentially created his own version of Shell-shock through a hallucination of Germans appearing in his trench. This case can be compared to one described in Section B, namely, Case 347: that of a Russian soldier who had classic war dreams, even though his entire service was in the rear and he had not experienced combat.
Possibly Case 171, that of hysterical fugue, might be regarded as one of Shell-shock, since two shells burst near him prior to his fugue. The man had had analogous crises, certified by Régis, in adolescence, and had received the diagnosis hysteria. In this instance, we are dealing merely with an habitual somnambulist who has a characteristic fugue following explosion of two shells. The war is in a sense responsible for the fugue, yet not directly, and the fugue would, without the stress and strain of war, probably never have developed (see sundry cases in the group in which ante-bellum phenomena are newly evoked in war: Cases 286-301).
Possibly Case 171, the condition of hysterical fugue, could be seen as a type of Shell-shock, given that two shells exploded near him before he experienced the fugue. The man had gone through similar crises, as noted by Régis, during his teenage years and had been diagnosed with hysteria. In this case, we are simply looking at a habitual sleepwalker who shows a typical fugue after the explosion of two shells. The war is somewhat responsible for the fugue, although not in a direct way, and without the stress and strain of war, the fugue likely would never have occurred (see various cases in the group where pre-war issues are brought back during war: Cases 286-301).
The hysterical psychosis of an Adventist (Case 172) might be regarded as liberated by military service; the terrible fear of the guns shown by the psychoneurotic (Case 173) proceeded to the point of fugue. A Shell-shock victim whose war bride was pregnant, developed fugue with amnesia and mutism (Case 174). Under hypnosis, it appeared that his fugue began with his running away from shells. Case 175 was that of a neurasthenic who volunteered and had to be sent back from the front after three months. In this case, war dreams were supplanted by sex dreams, and the fear of insanity became ingrained. The phenomena here were largely ante-bellum and the war brought them out once more, as might other disturbing experiences.
The extreme mental breakdown of an Adventist (Case 172) might be seen as a release through military service; the intense fear of gunfire displayed by the person with psychoneurosis (Case 173) escalated to the point of fugue. A shell-shock victim whose war bride was pregnant developed fugue along with amnesia and mutism (Case 174). During hypnosis, it became clear that his fugue started when he ran away from explosions. Case 175 was a neurasthenic who volunteered but had to be sent back from the front after three months. In this instance, battle dreams were replaced by sexual dreams, and the fear of going insane became deeply rooted. The phenomena observed here were mostly pre-war, and the war triggered them again, similar to other disturbing experiences.
Case 176 is here introduced to show that neurasthenia may develop in a man without hereditary taint or acquired soil. There was a very slight shrapnel injury of the skull, which somewhat clouds the diagnosis in the case. Five months’ war experience brought out the neurasthenia. Case 177 deals with a point in the diagnosis of psychasthenia, which, according to Crouzon, shows arterial hypotension, a condition important to distinguish from that of pulmonary tuberculosis and of Addison’s disease. Compare this case with Case 169: a case of depression treated by pituitrin. Case 178 is a case of psychasthenia following several months’ service by a man who probably should never have entered military service.
Case 176 is introduced here to highlight that neurasthenia can occur in a person without a hereditary background or prior susceptibility. There was a minor shrapnel injury to the skull, which makes the diagnosis somewhat unclear in this case. After five months of war experience, neurasthenia became apparent. Case 177 addresses a diagnostic point in psychasthenia, which, according to Crouzon, is marked by low blood pressure, a condition that needs to be differentiated from pulmonary tuberculosis and Addison’s disease. Compare this case with Case 169: a case of depression treated with pituitrin. Case 178 involves a case of psychasthenia following several months of service by a man who likely should never have joined the military.
Another case of ante-bellum origin is Case 179. Antityphoid inoculation appears to have been the initial factor in the case of neurasthenia No. 180. Compare Case 65, epilepsy after antityphoid inoculation. Case 181 was that of a non-commissioned reserve German officer whose neurasthenia was distinguished by sympathy with the enemy. He did not want to let his men shoot at the enemy because the idea came forcibly to him that the enemy soldiers had wives and children. This symptom of sympathy with the enemy was also shown by another German (Case 229). Compare the sentiments of a Russian under narcosis (Case 555).
Another case from before the war is Case 179. Antityphoid inoculation seems to have been the main factor in the case of neurasthenia No. 180. Compare Case 65, epilepsy following antityphoid inoculation. Case 181 was a non-commissioned reserve German officer whose neurasthenia was marked by sympathy with the enemy. He couldn't bring himself to let his men shoot at the enemy because he felt strongly that the enemy soldiers had families. This symptom of sympathy for the enemy was also observed in another German (Case 229). Compare this with the feelings of a Russian under narcosis (Case 555).
To sum up concerning the small group of psychoneuroses presented in the section on Psychoses Incidental in the War,[852] we are dealing with cases in which the phenomena are either continuous with ante-bellum phenomena, or are of such a nature that they might well have been brought out by other factors than those of war. These cases by the design of their choice throw little or no light upon the relation of physical shell-shock or its equivalent to the psychoneuroses, though in a few instances the factor of shell explosion is not entirely to be excluded, and in one instance (Case 170) a hallucination may be regarded as a virtual equivalent of an emotional shock of great compelling power.
To summarize the small group of psychoneuroses discussed in the section on Psychoses Incidental in the War,[852] we're looking at cases where the symptoms either continue from pre-war issues or arise from factors unrelated to war. These cases, by their very nature, provide little or no insight into how physical shell-shock or similar experiences relate to psychoneuroses, although in a few situations, the impact of a shell explosion can't be completely ruled out. In one instance (Case 170), a hallucination can be considered a strong equivalent to a significant emotional shock.
49. Let us now contrast with these specified ante-bellum or non-war cases the situation which will face us in the war group.
49. Now let's compare these specific pre-war or non-war cases to the situation we will encounter in the war group.
Section B contains 174 cases (Cases 197-370). Autopsied cases (Cases 197-201) are put first and are followed by cases in which lumbar puncture data are available (Cases 202-207). A third group of cases is that in which so-called organic symptoms are much in evidence, either independently or in association with functional symptoms (Cases 208-219). There follows a small group of three cases with shrapnel wound (Cases 220-222), in which hysterical symptoms were prominent, as against the prevalent and correct conception that wounded cases are not so prone to psychoneurosis as non-wounded cases. Three cases specially marked by tremors (Cases 223-225) follow, the last of which gives the victim’s (a French artist) own account of his feelings. The next two cases (Cases 226 and 227) give respectively a German and a British soldier’s account of Shell-shock symptoms.
Section B includes 174 cases (Cases 197-370). Autopsied cases (Cases 197-201) are listed first, followed by cases where lumbar puncture data is available (Cases 202-207). A third group includes cases where organic symptoms are prominent, either on their own or along with functional symptoms (Cases 208-219). Next is a small group of three cases with shrapnel wounds (Cases 220-222), where hysterical symptoms were significant, contrary to the common belief that wounded cases are less likely to develop psychoneurosis than those who aren't wounded. After that, there are three cases specifically noted for tremors (Cases 223-225), with the last one featuring the victim’s (a French artist) own account of his experiences. The following two cases (Cases 226 and 227) present accounts of Shell-shock symptoms from a German soldier and a British soldier, respectively.
There then follows a great group of cases (Cases 228-273) arranged according to the part of the body chiefly affected by hysterical symptoms. The arrangement is one of toe to top, or as one might more technically say, cephalad. This cephalad arrangement naturally begins with cases with symptoms affecting one leg or foot (Cases 228-235). Then follow cases of paraplegia (Cases 236-241). As we proceed cephalad then follow four cases of the so-called hysterical[853] bent back, or camptocormia (Souques). Then come walking disorders (Cases 246-248). Still proceeding cephalad, disorders of one arm and hand are considered in a series of six cases (Cases 249-254). Bilateral phenomena, symmetrical or asymmetrical, follow in Cases 255-258. Now reaching the head, we deal with cases of deafness (Cases 259-260), of deafmutism (Cases 261-263), of speech disorder (Cases 264 and 265), with two special cases (Cases 266 and 267). Eye symptoms are dealt with in a series of cases (Cases 268-272), and Case 273 deals with cranial nerve disorder supposed to be due to shell windage without explosion.
There follows a large group of cases (Cases 228-273) sorted by the part of the body most affected by hysterical symptoms. The sorting goes from the toe to the top, or more technically, cephalad. This cephalad arrangement starts with cases showing symptoms affecting one leg or foot (Cases 228-235). Next, we move on to cases of paraplegia (Cases 236-241). Continuing cephalad, we reach four cases of the so-called hysterical bent back, or camptocormia (Souques). Then we examine walking disorders (Cases 246-248). Moving further cephalad, we look at disorders affecting one arm and hand in a series of six cases (Cases 249-254). Bilateral phenomena, whether symmetrical or asymmetrical, come next in Cases 255-258. When we reach the head, we address cases of deafness (Cases 259-260), deafmutism (Cases 261-263), and speech disorders (Cases 264 and 265), along with two special cases (Cases 266 and 267). Eye symptoms are covered in a series of cases (Cases 268-272), and Case 273 addresses cranial nerve disorders believed to be caused by shell windage without an explosion.
The idea of the above arrangement of 46 cases (Cases 228-273) is that the reader dealing with cases of hysterical disorder due to physical shell-shock, or some equivalent thereof, may inspect the data in a few analogous cases described more or less fully in the literature. By reference to the index, the reader will be able to find still further cases to illustrate the symptom in question.
The setup of the 46 cases (Cases 228-273) is designed so that readers facing cases of hysterical disorder from physical shell-shock or something similar can look through the information in a handful of similar cases discussed in the literature. By checking the index, readers can find additional cases that highlight the symptoms being examined.
The next series of cases (Cases 274-281) are to illustrate the contentions of Babinski concerning the elective exaggeration of reflexes under chloroform, and the conception of reflex or physiopathic disorders based thereon—a topic to which return is made in Section C on Diagnosis, and elsewhere. A small group of cases (Cases 282-285) illustrate the delay of Shell-shock and kindred symptoms in certain instances, cases that suggest a refractory period of greater length than usual, or the interposition of some unusual factor.
The following series of cases (Cases 274-281) are meant to demonstrate Babinski's ideas about the selective enhancement of reflexes under chloroform, and the concept of reflex or physiopathic disorders that stem from this—an issue that's revisited in Section C on Diagnosis, and other sections. A small group of cases (Cases 282-285) illustrates the delay of Shell-shock and similar symptoms in some situations, suggesting a refractory period that's longer than usual, or the involvement of some unique factor.
The next group of cases (Cases 286-301) is of special note, bringing out what is discussed below, namely, the emphasis, reminiscence, or repetition of antebellum phenomena, and the picking out of weak spots in the organism by Shell-shock. Possibly Cases 302-303 belong in the same group of illustrations of the driving in of ante-bellum effects. Cases 304 and 305 are definitively cases in which hereditary instability is a factor, whereas Cases 306 and 307 form a foil to these, in that the phenomena develop in subjects confidently stated to be without hereditary or acquired psychopathic tendency.
The next group of cases (Cases 286-301) is particularly important, highlighting what is mentioned below, specifically, the emphasis, memory, or repetition of pre-Civil War phenomena, and how Shell-shock reveals vulnerabilities in the system. Possibly Cases 302-303 belongs in the same category of examples illustrating the impact of pre-war effects. Cases 304 and 305 clearly involve hereditary instability, while Cases 306 and 307 contrast with these, as the phenomena manifest in subjects who are confidently asserted to be free from hereditary or acquired psychopathic tendencies.
The next series of cases (Cases 308-320) shows peculiar phenomena; e.g., monocular diplopia, shell-shock psoriasis,[854] synesthesia, puerilism, and the like. Shell-shock equivalents of various sorts are placed in a group of cases (Cases 321-325). The next series of cases (Cases 326 to the end of this Section: 370) show tendencies to general neurasthenic, psychasthenic, and other psychopathic phenomena, rather than the more definite phenomena discussed in the early part of this section in the series arranged “cephalad.”
The next set of cases (Cases 308-320) showcases strange phenomena; e.g., monocular diplopia, shell-shock psoriasis, [854] synesthesia, puerilism, and similar conditions. Different types of shell-shock equivalents are grouped together in a set of cases (Cases 321-325). The following set of cases (Cases 326 to the end of this Section: 370) displays tendencies toward general neurasthenic, psychasthenic, and other psychopathic phenomena, rather than the more specific phenomena discussed in the earlier part of this section organized “cephalad.”
50. Rehearsing more briefly these findings, what is the nature of these disorders? The literature is practically unanimous on the point: We have to do merely with the classical problem of the neuroses, and when all the data are some day united, we shall doubtless know a great deal more about the neuroses.
50. Summarizing these findings briefly, what are these disorders all about? The literature generally agrees on this: We are dealing with the classic issue of neuroses, and when all the data is eventually combined, we will likely understand much more about neuroses.
51. Locus minoris resistentiae. That the process, whatever else it does, is rather apt to pick out pre-existent weak spots in the patient (the habitual gastropath becoming subject to vomiting; the old stammerer stammering once more or even becoming mute; the man always “hit in the legs” by exertion, now becoming paraplegic) is obvious. The striking instances in which an old cured syphilitic monoplegia, or an old hysterical hemichorea, comes back under the influence of shell explosion in precisely the limits and with precisely the appearance of the former disease, indicate how various a factor may be the locus minoris resistentiae.
51. Area of Least Resistance. It's clear that the process tends to highlight existing weak spots in the patient (like a person with a history of stomach issues becoming prone to vomiting; an old stutterer starting to stutter again or even becoming mute; or someone who has always struggled with leg pain now becoming paralyzed). The striking cases where an old cured syphilitic condition or an old hysterical movement disorder returns after a shell explosion, matching the previous symptoms exactly, show just how varied the area of least resistance can be.
52. But, without weak spot, without acquired soil, without heredity, we must now erect the hypothesis that, the classical neuroses may in some, though certainly a minority of cases, afflict normal men. Under the war conditions of investigation touching the family and personal histories of the men, perhaps we should not be too sure of this hypothesis; but the army records will after the war allow us to make or break the point forever and thereby throw the clearest light upon the vexing problems of industrial medicine, wherein progress in general has been so slow on account of the partisanship of the corporation and plaintiff’s attorneys.
52. However, without a weak spot, without inherited factors, without the influence of upbringing, we must now propose the idea that classical neuroses may affect normal individuals in some cases, although this is likely a minority. Given the wartime conditions of our investigation into the family and personal backgrounds of these men, we shouldn’t be overly confident in this hypothesis; however, the army records after the war will provide us the opportunity to confirm or dismiss this point once and for all, shedding light on the complicated issues in industrial medicine, where overall progress has been slow due to the bias from corporations and plaintiff attorneys.
53. Purely psychogenic war cases exist: Though Shell-shock denotes, to say the least, shocks and shells—yet we know Shell-shock sans any shock and sans any shell, nay sans either shell or shock.
53. Purely psychogenic war cases exist: Although Shell-shock refers, at the very least, to shocks and shells—we also know that Shell-shock can occur without any shock and without any shell, in fact, without either shell or shock.
The fact that a soldier may get war dreams though he has never been in the fighting zone and never by any chance observed the circumstance of war, or the fact that a man can become mute on the second day after a shell explosion because the night before he had dreamed of some hysterically mute patients in his ward—these facts again, although they argue a psychogenic origin for the phenomena of so-called “Shell-shock,” do not at all mean that actual physical explosion in other cases may not be tremendously important.
The fact that a soldier can have war dreams even though he’s never been in a combat zone or seen anything related to war, or that a man can go mute the day after a shell explosion because the night before he dreamed about some extremely mute patients in his ward—these points, while suggesting a psychological cause for what’s known as “Shell-shock,” don’t imply that real physical explosions in other cases aren’t incredibly significant.
54. This is shown by the exceedingly interesting phenomena of localization or determination of symptoms to a given region under the special local influence of the explosion. Thus, in the schematic case, an explosion to the left of the soldier produces anesthesia and paralysis on the left or exposed side. Now and again a case will show such anesthetic and paralytic phenomena upon the side exposed to the explosion and some hypertonic, irritative phenomena upon the other side. One gets the figure in one’s mind of an organism fixed, immobile and numb, on the spot by the explosion—and the other half of the body, as it were, attempting to run away from the situation. One side of the body, as it were, plays ’possum, the other tends to flight.
54. This is highlighted by the really interesting phenomenon of localization or determination of symptoms to a specific area due to the local impact of the explosion. In a typical case, an explosion to the left of a soldier causes numbness and paralysis on the left or exposed side. Occasionally, a case will show these numbness and paralysis effects on the side facing the explosion, while some heightened, irritative symptoms appear on the other side. You can picture an organism that is fixed, motionless, and numb where the explosion occurred—while the other half of the body seems to be trying to escape the situation. One side of the body plays dead, while the other tends to flee.
55. Of course these physical phenomena should not blind us to the emotional ones. Now and then the multiple causes of a case may be analyzed, as, for example, one of blindness in which a series of factors emerged, such as excitement, blinding flashes, fear, disgust and fatigue. I cannot here go further into these details, and I need no longer insist upon the fact that surrounding the problem of Shell-shock means surrounding the problem of nervous and mental diseases as a whole, and that thus to be a Shell-shock analyst means to be a neuropsychiatrist.
55. Of course, these physical phenomena shouldn't distract us from the emotional ones. Occasionally, we can analyze the multiple causes of a case, such as in a situation of blindness where a series of factors came into play, including excitement, blinding flashes, fear, disgust, and fatigue. I can't go into more detail here, and I no longer need to emphasize that addressing the issue of Shell-shock involves dealing with the problem of nervous and mental illnesses overall, meaning that to be a Shell-shock analyst is equivalent to being a neuropsychiatrist.
56. The organic problems of the nervous system are brought up constantly in differential diagnosis, but the functional problems divide themselves up in a perturbing manner into a fraction properly termed the “psychopathic” (that is, after the manner of hysteria), and “non-psychopathic” (that is, after the manner of reflex disorders of Charcot, newly named “physiopathic” by Babinski).
56. The physical issues of the nervous system are frequently discussed in differential diagnosis, but the functional issues split in a confusing way into two categories: the "psychopathic" (like hysteria) and "non-psychopathic" (like Charcot's reflex disorders, recently labeled "physiopathic" by Babinski).
57. For the moment we are not discussing differential diagnosis, but are merely trying to circumscribe the features we wish to call Shell-shock features: We have concluded to call them functional—but what is it to be functional?
57. Right now, we're not talking about differential diagnosis; we're just trying to outline the characteristics we want to refer to as Shell-shock features. We've decided to call them functional—but what does it mean to be functional?
Too simple is the reply:
Too simple is the response:
Functional = Non-Organic.
Functional = Non-Organic.
Inaccurate and misleading is the reply
Inaccurate and misleading is the response
Functional = Psychic.
Functional = Psychic.
We may more correctly express the situation, pathologically speaking, in the following categories (see chart, page 870):
We can more accurately describe the situation, in medical terms, using the following categories (see chart, page 870):
ORGANOPATHIC (Lesional, destructive):
ORGANOPATHIC (Lesional, damaging):
(a) gross, or (b) microscopic, or perhaps (c) chemical.
(a) gross, or (b) microscopic, or maybe (c) chemical.
DYNAMOPATHIC (functional, irritative, inhibitory,—but reversible ad originem):
DYNAMOPATHIC (functional, irritative, inhibitory—but reversible ad originem):
(a) psychopathic; (b) physiopathic (“reflex”).
(a) psychopathic; (b) physiopathic (“reflex”).
58. As to the high psychic functions, we had thought of them as split in hysteria, in dissociation of personality. And we had roughly distinguished these conditions as psychopathic from conditions we called neuropathic, regarding the latter neuropathic disorders as on the model of the effects of cutting off or destroying certain necessary neurons. However clear or unclear we were as to the nature of the neuropathic, it does not here matter. Babinski’s point is that there is another kind of dynamic disease that operates, not after the manner of hysteria, but after a manner reminding one of the forgotten “reflex” disorders of Charcot—disorders that fitted the textbooks so poorly that the textbooks dropped them out. In short, what you might call the dynamopathic or functional in nervous disease has been shown to fall into two parts—a psychopathic fraction and a non-psychopathic fraction. Babinski calls this non-psychopathic fraction physiopathic or reflex. And these reflex or physiopathic disorders have a different order of curability from that of hysterical or psychopathic disorders. By what simple device did Babinski prove this? By chloroforming the patient. Under chloroform, when all the other reflexes were stilled, Babinski could bring out, in relief as it were, certain reflexes, or even hypertonuses, that were in the waking[857] life wholly concealed,—yet at the same time consciousness, in the usual sense of that term, had vanished. Accordingly, the proof of a new type of functional disease, at times concealed by the overlay of higher neurones, was now plain. Does not this offer new leads of the greatest value in that most intricate of fields, psychopathology? Is not the model here offered of diseased nervous functions, non-psychic in nature (in the ordinary sense of psychic) but of almost equally complex nature:
58. Regarding the higher mental functions, we used to think of them as disrupted in hysteria and in dissociated personalities. We generally distinguished these conditions as psychopathic, separate from those we labeled as neuropathic, viewing the latter neuropathic disorders as similar to the effects of removing or damaging certain essential neurons. Regardless of how clearly or unclearly we understood the neuropathic aspect, that's not the focus here. Babinski pointed out that there is another type of dynamic disorder that doesn't function like hysteria, but rather resembles the overlooked “reflex” disorders identified by Charcot—disorders that were inadequately represented in textbooks and subsequently omitted. In essence, what could be termed the dynamopathic or functional aspect of nervous diseases has been shown to divide into two categories—one psychopathic and the other non-psychopathic. Babinski refers to this non-psychopathic category as physiopathic or reflex. These reflex or physiopathic disorders have a different potential for recovery compared to hysterical or psychopathic disorders. How did Babinski demonstrate this so simply? By using chloroform on the patient. While under chloroform, when all other reflexes were suppressed, Babinski could reveal certain reflexes, or even heightened muscle tone, that were completely hidden in the patient's conscious waking life—yet simultaneously, consciousness in the typical sense of the word was absent. Therefore, the evidence of this new type of functional disorder, sometimes masked by the dominance of higher neurons, became clear. Doesn’t this provide valuable new insights in the complex field of psychopathology? Isn’t this model of diseased nervous functions, which is non-psychic in the traditional sense of the term, but equally intricate:
Whoever wins the great war from the military point of view, there can be no doubt as to what writers contributed most from the war data concerning the doctrine of hysteria, especially concerning the theoretical delimitation of hysteria from other forms of functional nervous disease: There can be no other answer than that, in theoretical neurology at least, the French have already won the war, if only by means of the remarkable concept set up by Babinski of the so-called physiopathic (that is, non-neuropathic and non-psychopathic).
Whoever wins the great war from a military perspective, there’s no doubt about which writers added the most to our understanding of hysteria based on war data, particularly in distinguishing hysteria from other types of functional nervous disorders. The conclusion is clear: at least in theoretical neurology, the French have already won the war, largely due to Babinski's impressive idea of the so-called physiopathic (meaning, non-neuropathic and non-psychopathic).
But how has this splitting of functional neuroses into psychopathic and physiopathic been rendered certain? By the tremendous modern sharpening of differential diagnosis dating from, e.g., the discovery of the Babinski reflex. This brings us to the brink of considerations concerning the differential diagnostic problem.
But how has this division of functional neuroses into psychopathic and physiopathic been confirmed? By the significant advancement in differential diagnosis that has developed since, e.g., the discovery of the Babinski reflex. This leads us to the edge of discussions about the differential diagnostic issue.
First it may be well to regard the whole problem in the light of those mental diseases that we slid over when we were delimiting Shell-shock as against syphilis, epilepsy and somatic disease.
First, it might be useful to look at the whole issue in the context of those mental illnesses that we briefly touched on when differentiating Shell-shock from syphilis, epilepsy, and physical illness.
59. Why do some authors think of Shell-shock as an “officer’s disease”? It is clear that they cannot be thinking so much of the physiopathic cases as of the psychopathic ones. But psychopathic conditions are obviously more readily brought about in complex and labile apparatus. This point comes out strongly in relation with the comparative stability of the feeble-minded, at least of most feeble-minded, that get into war relations.
59. Why do some authors see Shell-shock as an “officer’s disease”? It's clear that they are likely focusing more on the psychopathic cases rather than the physiopathic ones. However, psychopathic conditions can obviously develop more easily in complex and unstable situations. This point is particularly evident when compared to the relative stability of the feeble-minded, at least for most feeble-minded individuals, who find themselves in wartime situations.
The possible relations of Shell-shock to feeble-mindedness are of some interest. We know that Shell-shock picks out[858] certain nervous and mental weaklings and indeed that one author claims as high a percentage as 74 for war neuroses having a hereditary or acquired neuropathic basis. How far does feeble-mindedness itself count among these supposedly susceptible nervous and mental weaklings? Is a feeble-minded person especially in condition for Shell-shock?
The possible connections between Shell-shock and mental weakness are quite intriguing. We know that Shell-shock tends to affect certain vulnerable individuals with nervous and mental issues, and one author even suggests that up to 74% of war neuroses may stem from genetic or acquired neuropathic factors. To what extent does mental weakness play a role among these supposedly vulnerable individuals? Is a person with mental weakness more likely to experience Shell-shock?
There are rumors of experiments to show that if in an aquarium containing some jelly fish alongside bony fishes, you explode a substance, the jelly fish ride through unscathed whereas the bony fishes are killed by the shock. The jelly fish presumably had too simple an organization.
There are rumors of experiments suggesting that if you explode a substance in an aquarium with jellyfish and bony fish, the jellyfish come through unharmed while the bony fish are killed by the shock. The jellyfish presumably have such a simple structure.
There is something to be said for the idea that in man also the higher and more complex specimens are more susceptible to Shell-shock, that is, to the neuroses of war, than are the lower and more simple combatants. Some statistics indicate that officers, who are in the main of a higher and more complex organization than the private soldiers, are much more susceptible than are private soldiers to the neuroses of war. Doubtless we shall not be able to verify these statistics until long after the war and, so far as I know, no very inclusive statistics have been presented.
There’s something to consider about the idea that higher and more complex individuals are more prone to Shell-shock, or the psychological effects of war, than simpler combatants. Some statistics suggest that officers, who typically have a more advanced and layered role than regular soldiers, are significantly more vulnerable to war-related neuroses. We probably won’t be able to confirm these statistics until long after the war, and to my knowledge, no comprehensive statistics have been published.
On the whole, I judge from the case history literature that the feeble-minded, unless they be of that very high level sometimes called subnormal, are not particularly susceptible to the neuroses. It is obvious that idiots and, for the most part, imbeciles, do not get into military service. As for what the English term the feeble-minded or what we in America are now terming morons, it may well be that our draft boards do not always exclude. High French authorities have specifically determined in certain instances that the high-grade feeble-minded would be perfectly suitable for certain branches of the service. There is the case, for example, of a sandwich man of Paris who somehow got into the French army and was being perpetually sent to look for the squad’s umbrella and the key to the drill ground, but sang and swung his gun with joy as he went to the front, and apparently did very well there. This man had been a state ward and, as you know, well-trained state wards are frequently exceedingly good at elementary forms of drill.
Overall, from what I gather from the case history literature, people with intellectual disabilities, unless they are at a very high level sometimes referred to as subnormal, are not particularly prone to neuroses. It's clear that idiots and, for the most part, imbeciles do not enter military service. As for what the English call feeble-minded or what we in America currently refer to as morons, it seems our draft boards don’t always exclude them. High-ranking French officials have determined in some cases that those with high-grade intellectual disabilities would be perfectly suitable for certain branches of the military. Take, for instance, the case of a sandwich man from Paris who somehow joined the French army and was constantly sent to look for the squad’s umbrella and the key to the drill ground, but cheerfully sang and swung his gun as he went to the front, doing surprisingly well there. This man had been a state ward, and as you know, well-trained state wards are often very good at basic forms of drill.
Then there is another case of an obvious imbecile who was quite without any idea of military rank and often got punished for treating his superiors like his comrades and was the butt of his section, but on the firing-line remained cool, careless of danger—a magnificent example to his comrades—at last surrounded and taken prisoner. Here the story might have ended and the folly of enlisting imbeciles in the army might have seemed perfectly plain, except that our imbecile forthwith escaped from the Germans, swam the Meuse and got back to his regiment!
Then there's another case of a complete fool who had no clue about military ranks and often got punished for treating his superiors like his buddies. He was the laughingstock of his section, but when it came to the front lines, he stayed calm and didn't care about danger—a great example for his comrades. Eventually, he got surrounded and taken prisoner. The story could have ended there, making the foolishness of enlisting fools in the army seem crystal clear. But then our fool managed to escape from the Germans, swam across the Meuse, and made his way back to his regiment!
Here then are cases in which the slight degree of hypophrenia—it seems unwise to give it the opprobrious title “feeble-mindedness”—would have been entirely inconsistent with the development of Shell-shock. Such men are, perhaps, too simple to develop neuroses. On the other hand, it would appear that certain of the slight degrees of hypophrenia, such as we might find in so-called subnormal or stupid persons, would prove capable of “catching Shell-shock” as it were, and then find themselves entirely incapable of rationalizing the situation. In short, there may be a group of psychic weaklings, just complex enough to fall into the zone of potential neurotics, but just simple enough to render the processes of rationalization (or what one author terms autognosis) and of psychotherapy in general entirely unavailing.
Here are cases where a slight degree of hypophrenia—it seems unwise to label it “feeble-mindedness”—would completely contradict the onset of Shell-shock. Such individuals are perhaps too straightforward to develop neuroses. On the flip side, it seems that certain mild forms of hypophrenia, like those we might see in people considered subnormal or unintelligent, could be susceptible to “catching Shell-shock” and then struggle to rationalize the situation. In summary, there might be a group of psychologically weak individuals, just complex enough to fall into the realm of potential neurotics, but simple enough to make the processes of rationalization (or what one author refers to as autognosis) and psychotherapy in general completely ineffective.
After the war we may be confronted with a number of persons with their edges dulled by the war experiences. One has met even brave officers who, after months of furlough, still maintain that they will never get back to their normal will and initiative. Whether these hypoboulic persons have not been reduced to subnormality so as to resemble the slighter degrees of hypophrenia or feeble-mindedness can hardly be determined now. They will form important problems in mental reconstruction, for with the best will in the world, the occupation-therapeutist with all her technic, may be unable to force or coax the will of such hypoboulics into proper action. Nor will the ordinary environment of home and neighborhood turn the trick properly. Expert social work in adjustment, both of the returned soldier to his environment and of the environment to the returned soldier,[860] may be necessary. I speak of this problem here not because these persons are hypophrenic or feeble-minded in the ordinary sense, but we must constantly bear in mind our experience in the teaching of hypophrenics (both in the schools for the feeble-minded and in the community) when we are facing problems of mental reconstruction.
After the war, we might encounter a number of people whose edges have been softened by their experiences. I've even met courageous officers who, after months of leave, insist they will never return to their normal drive and initiative. It's hard to say whether these hypoboulic individuals have been lowered to a level resembling mild hypophrenia or mental weakness. They will create significant challenges in mental reconstruction, because even the most skilled occupational therapist may struggle to motivate these hypoboulics into taking the right actions. The usual home and neighborhood environment won’t do the trick either. Expert social work in adjusting both the returning soldier to his surroundings and the surroundings to the returning soldier,[860] may be essential. I'm discussing this issue here not because these individuals are hypophrenic or mentally weak in the traditional sense, but we must always remember our experiences teaching hypophrenics (both in special schools and in the community) when addressing mental reconstruction challenges.
60. As for alcoholism, Lépine’s figures bespeak its importance as a hospital-filler and a good deal of prime interest surrounding alcoholism has been developed in the war; but on the whole, so far as I can determine from the war case literature, there is little or no direct relation between alcoholism and Shell-shock, despite the fact that in a number of instances alcohol has complicated the issue and very possibly helped in a general demoralization of the victim. However, the alcoholic amnesias and particularly a few instances of the so-called pathological intoxication have exhibited a certain medicolegal interest, recalling what was just said above about the responsibility of a drunken epileptic. Alcohol remains, I should say, pending exact monographic work upon this topic, purely a contributory factor for the war neuroses.
60. When it comes to alcoholism, Lépine’s statistics highlight its significance as a major reason for hospital admissions, and there's been considerable attention paid to alcoholism during the war. However, based on my review of the war-related literature, there seems to be little to no direct connection between alcoholism and Shell-shock, even though, in some cases, alcohol has complicated the situation and may have contributed to the victim's overall demoralization. Nevertheless, the instances of alcoholic amnesias and some cases of the so-called pathological intoxication have raised certain legal and medical interests, echoing the previous discussion about the responsibility of a drunk person with epilepsy. For now, I would argue, pending detailed studies on this subject, that alcohol is merely a contributing factor in war-related neuroses.
It must be that the exigencies of the war have prevented full reports of alcoholic cases; or perhaps they are regarded as of such every-day occurrence as not to demand case reports. The alcohol and drug group is represented by 17 cases (Cases 86-102).
It seems that the demands of the war have stopped complete reports of alcohol-related cases; or maybe they’re seen as so common that detailed reports aren’t necessary. The alcohol and drug group includes 17 cases (Cases 86-102).
The so-called pathological intoxication is illustrated in Cases 86 and 87. Case 86 was entirely amnestic for an attack of hallucinations in which he tried to transfix comrades with a bayonet. Cases 87-97 are cases of disciplinary nature,—the majority from a German writer, Kastan. Case 88 illustrates desertion in alcoholic fugue, and Cases 90-92 are three further cases of desertion in alcoholism.
The so-called pathological intoxication is shown in Cases 86 and 87. Case 86 had no memory of an episode where he attempted to stab his comrades with a bayonet while experiencing hallucinations. Cases 87-97 are disciplinary cases,—mostly from a German writer, Kastan. Case 88 shows desertion during an alcoholic fugue, and Cases 90-92 are three additional cases of desertion related to alcoholism.
Cases 94 and 95 give a partial explanation of some German atrocities. At least, here are cases in which the atrocities, with attempted murder and rape, are described more or less fully in transcripts of medicolegal reports. Case 98 throws a curious cross-light upon the war, in that a drunken soldier got an unmerited long leave after paying 100 sous for an injection of petrol in his hand. Cases 99-102 are cases of[861] morphinism, illustrating the effects of the war upon the fate of morphinists.
Cases 94 and 95 provide a partial explanation of some German atrocities. At the very least, these cases involve accounts of the atrocities, including attempted murder and rape, which are detailed to some extent in the transcripts of medicolegal reports. Case 98 offers an interesting perspective on the war, where a drunken soldier received an undeserved long leave after paying 100 sous for an injection of petrol in his hand. Cases 99-102 are cases of[861] morphinism, showcasing the impact of the war on the lives of morphine addicts.
61. That war makes nobody go mad in the asylum or lay sense of the term has been abundantly proved by the data of this war—and this conclusion is of value in our medical endeavors to establish a proper lay conception of the nature of Shell-shock. Consider first schizophrenia (dementia praecox).
61. The idea that war drives nobody insane in the asylum or casual sense has been clearly demonstrated by the evidence from this war—and this conclusion is important for our medical efforts to develop an accurate understanding of Shell-shock. First, let’s consider schizophrenia (dementia praecox).
That the causes of dementia præcox, still unknown as they are, lodge more in the interior of the body or in special individual reactions of the victim’s mind, seems to be shown by the phenomena of this war, since there seems to be no great number of dementia præcox cases therein produced. To be sure, some schizophrenic subjects do get into the service, and sometimes their delusions and hallucinations get their content and coloring from the war. Thus a Russian, wounded in the army, developed delusions concerning currents running from his arm to the German lines and felt that he was, so to say, the Jonah of the Russian front, as he could determine shell fire to the spot where he was by the arm currents.
The causes of dementia præcox, still unknown today, seem to be more rooted in the body's interior or in the specific individual reactions of the affected person's mind. This appears to be supported by the phenomena of this war, as there don't seem to be many new cases of dementia præcox arising from it. Of course, some people with schizophrenia do join the military, and sometimes their delusions and hallucinations are influenced by their experiences in the war. For example, a Russian soldier who was wounded in battle developed delusions about currents flowing from his arm to the German lines and believed that he was, in a way, the Jonah of the Russian front, as he thought he could direct shellfire to the place where he was based on these arm currents.
Now and then a case shows a scientifically beautiful admixture of ordinary dementia præcox phenomena with the effects of shell wound or shock. A picturesque case from the standpoint of German psychiatric diagnosis is one of a soldier who boxed the ear of a kindly sister who tried to steer him from a room where the examination of another patient, a woman, was going on. On the whole, the eminent German psychiatrist who examined him felt that the case was really one of psychopathic constitution, as he had shown somewhat similar irascibility on a slight occasion before. However, much to the astonishment of all, the patient developed further symptoms. His ego got terribly swollen. At last he was fain to utter a denunciation of the entire Junkertum and of the Kaiser: he said in fact that he was an Inhabitant of the World and not of Prussia merely. Over here we allow such persons to edit newspapers and write books with impunity, but the eminent German psychiatrist, before mentioned, was constrained to alter his diagnosis of this cosmopolite from psychopathic constitution to dementia praecox!
Now and then, a case presents a striking combination of typical symptoms of schizophrenia with the effects of shell shock or trauma. A noteworthy case from the perspective of German psychiatric diagnosis involves a soldier who slapped a kind nurse trying to guide him away from a room where an examination of another patient, a woman, was taking place. Overall, the distinguished German psychiatrist who evaluated him believed the case was truly one of psychopathic personality, as the soldier had shown similar irritability on a minor occasion earlier. However, much to everyone's surprise, the patient developed additional symptoms. His ego became excessively inflated. Eventually, he boldly condemned all of the aristocracy and the Kaiser, stating that he considered himself a citizen of the world and not just of Prussia. Here, we allow such individuals to run newspapers and write books without consequence, but the aforementioned eminent German psychiatrist felt compelled to change his diagnosis of this cosmopolitan from psychopathic personality to schizophrenia!
The group is represented by 16 cases (Cases 147-162).
The group is represented by 16 cases (Cases 147-162).
62. There are four cases (Cases 148-151) of a disciplinary nature. The first (Case 148) was actually arrested as a spy because he was making drawings near a petroleum tank. Of two cases of desertion, one was due to a fugue of catatonic nature (Case 149), and the other (Case 150) was one of desertion with behavior suggesting schizophrenia. However, this man was determined to be responsible for his act, and condemned to 20 years in prison. This latter case might be considered also in connection with Group III (the epilepsies), Group IV (the pharmacopsychoses), and possibly Group XI (the unresolved psychopathias).
62. There are four cases (Cases 148-151) that involve disciplinary actions. The first (Case 148) was actually arrested as a spy for drawing near a petroleum tank. Out of the two desertion cases, one was due to a catatonic episode (Case 149), and the other (Case 150) involved desertion with behaviors indicating schizophrenia. However, this man was found to be responsible for his actions and sentenced to 20 years in prison. This latter case might also be considered alongside Group III (the epilepsies), Group IV (the pharmacopsychoses), and possibly Group XI (the unresolved psychopathias).
Case 151 was likewise alcoholic and disciplinary: the man went so far as to keep a cigar in his mouth while the captain was rebuking him and was, in fact, an old sanatorium case, afflicted with some sort of degenerative disease, presumably dementia praecox.
Case 151 was also an alcoholic and faced discipline: the guy even kept a cigar in his mouth while the captain was scolding him, and he was, in fact, a long-term patient from a sanatorium, suffering from some kind of degenerative disease, probably early-onset dementia.
63. That schizophrenic symptoms may be aggravated by service is shown likewise in the case that follows, namely, Case 152, a man who had been hearing false voices for some two years, had heard his own thoughts, and felt his personality changing. The military board decided that the mental disease had been aggravated by service. Case 153 might offhand be regarded as a malingerer, as he shot himself in the hand. Upon military review, a delusional state set in, and in the course of no very long time a state of schizophrenic apathy. In point of fact, however, this man had already been in several hospitals for previous examination, and had served in the army in relatively normal intervals. Case 154 is that of a dementia praecox who volunteered for three years in French infantry but forthwith gave indications of mental deterioration. This case of a dementia praecox volunteer may be compared with Case 36: that of a superbrave imbecile who swam the Meuse, back from a German prison; with Case 47, that of the feeble-minded person with an insubordinate desire to remain at the front; with Case 163, a maniacal volunteer; and Case 175, a neurasthenic volunteer.
63. The fact that schizophrenic symptoms can be worsened by military service is demonstrated in the following case, Case 152, a man who had been hearing voices for about two years, was hearing his own thoughts, and felt his personality changing. The military board concluded that his mental illness had been aggravated by service. While Case 153 may initially seem like a malingerer for shooting himself in the hand, further military evaluation revealed a delusional state, which quickly led to a state of schizophrenic apathy. However, this man had already been hospitalized multiple times for prior assessments and had served in the army during relatively stable periods. Case 154 refers to a case of dementia praecox in a volunteer who served three years in the French infantry but soon began showing signs of mental decline. This case of the dementia praecox volunteer can be compared to Case 36: that of a superbrave imbecile who swam across the Meuse to escape from a German prison; with Case 47, that of a feeble-minded person who stubbornly wanted to stay at the front; with Case 163, a maniacal volunteer; and Case 175, a neurasthenic volunteer.
64. Diagnostic questions are brought up by Cases 155-166, in the former of which Bonhoeffer made at first a[863] diagnosis of some form of psychogenic disease, possibly hysterical, but had eventually to alter the diagnosis to hebephrenia or catatonia. Case 156 was possibly one of Shell-shock, though the man remained on duty for a month with but one symptom, trembling of the arm. For nine months he showed a variety of symptoms apparently consistent with the diagnosis hysteria, but then developed catatonic and paranoic symptoms clearly warranting the diagnosis dementia praecox.
64. Diagnostic questions are raised by Cases 155-166, where initially Bonhoeffer diagnosed a type of psychogenic illness, possibly hysterical, but later had to change the diagnosis to hebephrenia or catatonia. Case 156 might have been a case of Shell-shock, even though the man was able to serve for a month with only one symptom: trembling in his arm. For nine months, he exhibited various symptoms that seemed to match the hysteria diagnosis, but then he developed catatonic and paranoid symptoms that clearly required the diagnosis of dementia praecox.
65. Schizophrenia may not only be aggravated by service, but as Case 157 shows, war experience may have a definite effect upon the content of hallucinations and delusions. Thus, a man wounded in the left shoulder built up the idea of currents running from his left arm to the Germans, such that if anything were touched by the arm, bombardment of the Russians would at once start up. The arm, in short, was charmed.
65. Schizophrenia might not only get worse because of service, but as Case 157 shows, experiencing war can definitely influence the nature of hallucinations and delusions. For example, a man wounded in the left shoulder developed the belief that currents flowed from his left arm to the Germans, so that if anything touched his arm, Russian bombardment would immediately begin. In short, his arm was enchanted.
66. Psychopathic bravery is not shown in the feeble-minded only: Case 158 is that of an Iron Cross winner who, after an hysterical-looking attack with hallucinatory reminiscences of a Gurkha whom he had bayoneted, turned out to be hebephrenic. Case 159 might at first sight have been placed among the encephalopsychoses on account of the trauma to the occiput, and in fact the mystical hallucinations shown were of a visual nature (a rainbow-colored bird with the face of the Holy Virgin). In point of fact, there was probably no causal relation between the mystical delusions and the brain injury.
66. Psychopathic bravery isn't just found in the intellectually disabled: Case 158 is that of an Iron Cross winner who, after a dramatic episode filled with hallucinations of a Gurkha he had stabbed, turned out to be hebephrenic. Case 159 might initially have been categorized among the encephalopsychoses due to the head trauma, and indeed, the mystical hallucinations he experienced were visual (a rainbow-colored bird with the face of the Holy Virgin). In reality, there was likely no direct connection between the mystical delusions and the brain injury.
67. Case 156, above mentioned, might perhaps be interpreted as one of Shell-shock dementia praecox, but the interval of nine months, though filled with hysterical symptoms, is decidedly long in which to suppose that shell-shock factors could be in process of causing dementia praecox. Cases 160 and 161 are more suspicious. Six German soldiers were killed by a German shell within the zone of German fire, two steps away from the subaltern officer (Case 160), who carried on for some hours, made his report duly, but thereafter developed tremors and lost consciousness. According to Weygandt, the case is one suggestive of dementia praecox, but[864] very possibly should be regarded as one of psychoneurosis. At all events, it would be dangerous to found a doctrine to the effect that dementia praecox can be initiated by shell-shock upon such a case as 160. Case 161 is similarly doubtful. There are a number of symptoms in this man (the sole survivor of an explosion in a blockhouse) consistent with the diagnosis Shell-shock, and a number of others which hardly can be given any other interpretation than that of catatonic dementia praecox. But the available medical data do not begin until five months after the shell explosion. We must conclude here also that no definite evidence exists that dementia praecox can be initiated by the physical factor shell-shock. Case 162 is one in which there are shell-shock factors and fatigue factors in a man who had once ante-bellum shown signs of mental disorder, and who developed delusions subsequent to a fugue following shell-shock. The most one could make of this case would be to say that a latent schizophrenia had been liberated by shell-shock.
67. Case 156, mentioned earlier, could possibly be seen as a case of shell-shock dementia praecox, but the nine-month gap, although marked by hysterical symptoms, is definitely too long to think that shell-shock factors could lead to dementia praecox. Cases 160 and 161 raise more doubts. Six German soldiers were killed by a German shell within the German fire zone, just two steps from the subaltern officer (Case 160), who continued operating for several hours, filed his report, but later developed tremors and lost consciousness. According to Weygandt, this case suggests dementia praecox but[864] might actually be a case of psychoneurosis. In any case, it would be risky to base a theory that shell-shock can cause dementia praecox on a case like 160. Case 161 is similarly questionable. This man's symptoms (the only survivor of an explosion in a blockhouse) align with a shell-shock diagnosis, but there are also symptoms that can only really be interpreted as catatonic dementia praecox. However, the medical records only start five months after the shell explosion. We must conclude that there is no clear evidence that dementia praecox can be triggered by the physical factor of shell-shock. Case 162 involves shell-shock and fatigue factors in a man who had previously shown signs of mental disorder before the war and who experienced delusions after a fugue following shell-shock. The most that can be said about this case is that a latent schizophrenia may have been triggered by shell-shock.
68. To sum up concerning the schizophrenias (dementia praecox group), there are cases of great disciplinary interest in which alleged espionage and desertion turn out actually to be schizophrenic phenomena. Again, there are interesting diagnostic problems in the differential diagnosis of hysteria and catatonia. There is evidence that experience in the war may be woven into the hallucinatory and delusional contents of cases of pre-existent psychosis.
68. In summary regarding the schizophrenias (dementia praecox group), there are cases of significant disciplinary interest where supposed espionage and desertion actually turn out to be symptoms of schizophrenia. Additionally, there are intriguing diagnostic challenges in distinguishing between hysteria and catatonia. There is evidence that experiences from the war may be integrated into the hallucinatory and delusional aspects of cases with pre-existing psychosis.
69. As to the important question whether shell-shock can initiate dementia praecox, the evidence from these reported cases is against the hypothesis; but if the query be, whether Shell-shock might not aggravate dementia praecox, it may be stated that a military board has decided that dementia praecox may be aggravated by some forms of military service. There is no reason to suppose that shell-shock factors might not operate in this way. Cases 152 and 162 will be of service in the proof of this contention; and Case 162 seems to be definitely one in which a latent schizophrenia, showing itself in one ante-bellum attack, was liberated once more after shell-shock. Of course, the plan of this book and the method of choice of its cases precludes any statistical conclusions[865] of great weight from the relative number of cases found in the different groups; and it might well happen that psychiatrists would not report cases of an everyday and commonplace nature which might yet be very frequent. On the whole, however, it would not appear that dementia praecox is at all a frequent phenomenon in the war.
69. Regarding the important question of whether shell shock can lead to dementia praecox, the evidence from these reported cases goes against that idea. However, if we ask whether shell shock could worsen dementia praecox, it can be said that a military board has concluded that some types of military service may aggravate dementia praecox. There’s no reason to believe that shell shock factors couldn’t act in this way. Cases 152 and 162 will help support this claim; and Case 162 appears to be a clear instance where a latent schizophrenia, which was evident in one pre-war episode, was triggered again after shell shock. Of course, the structure of this book and the method for selecting its cases prevent any strong statistical conclusions from the relative number of cases found in the different groups; it’s also possible that psychiatrists may not report cases that are common and ordinary, even if they are very frequent. Overall, however, dementia praecox does not seem to be a common issue during the war.
70. Nor can the cyclothymias (manic-depressive psychoses) be charged up to war factors to any important extent.
70. The cyclothymias (manic-depressive disorders) cannot be primarily attributed to war factors to any significant degree.
On account of the somewhat close resemblance between the phenomenon of manic-depressive psychosis and what we ordinarily feel ourselves—a logical situation reflecting merely the fact that the phenomena of over-activity (mania) and of under-activity (depression) are merely quantitative variations from the normal—it might be supposed that the war life and its shock and strain would start up the cyclothymias in some numbers. Why should not a shell explosion start up a mania or throw a man into a depression? In point of fact the literature somehow does not agree with this presupposition.
Because of the similarity between manic-depressive psychosis and our everyday feelings—a straightforward situation that highlights that over-activity (mania) and under-activity (depression) are just different levels of the norm—it could be assumed that the stresses of war would trigger cyclothymia in many people. Why wouldn’t the blast from a shell cause someone to go into a mania or plunge into a depression? However, the existing literature does not support this assumption.
Some years ago in Massachusetts a brief investigation was made of the assigned causes of the successive attacks in a great number of cyclothymic (manic-depressive) cases, and it was found that each successive attack progressively had less of the physical in the previous history. Something like 45% of all the first attacks had a pretty obvious cause in the soma, such as a kidney disease, a heart disease, a puerperal condition and the like, but the second attacks failed to show even 20% of such obvious somatic causes, and the third attacks even less than 10%, and so on.
Some years ago in Massachusetts, a brief investigation was conducted into the causes of repeated attacks in a large number of cyclothymic (manic-depressive) cases. It was found that each successive attack had fewer physical causes in the individual’s previous history. About 45% of all the first attacks had a pretty clear physical cause, like kidney disease, heart disease, or a condition related to childbirth. However, the second attacks showed these obvious physical causes in less than 20% of cases, and the third attacks showed them in fewer than 10%, and so on.
Now war conditions and even the shell explosions themselves have apparently not set up any such conditions as those of mania or of depression. Most of the instances of cyclothymia are instances of men who are cyclothymic before they enter the army. These experiences, when after the war we can sift them all out, may allow us to form better ideas as to the etiology of many of the psychoses, and the great war may thus prove a gigantic experimental reagent which will aid in solving some of the major problems of mental hygiene.
Now, the conditions of war and even the explosions from shells don't seem to create situations that lead to mania or depression. Most cases of cyclothymia are found in men who were already cyclothymic before they joined the army. When we look back at these experiences after the war, we might be able to understand better the causes of various psychoses, and the great war might turn out to be a massive experimental factor that helps us tackle some of the main issues in mental health.
71. The cyclothymic or manic-depressive group is represented in strikingly few cases, seven in number (Cases 163-169).[866] One of the ideas in the literature concerning the manic-depressive group has been that it is very possibly remotely allied to Graves’ disease, a hypothesis upheld by Stransky in Aschaffenburg’s Handbook. Hyperthyroidism itself has been, of course, a rather striking feature in the foreground or background of many sick patients in the war. However, war factors have proved able to bring out very few instances of cyclothymic (manic-depressive) disease. Amongst our seven cases, the first (Case 163) was that of a maniacal Alsatian of 59 years, who volunteered because of his hypomania. Case 165, the case of a German who pelted French trenches with apples from an appletree in No Man’s Land, was another case in which the war had little or nothing to do with the development of the mania. One of fugue (Case 164) was a case of melancholia and anxiety not closely related with war experience. In three further cases trench life and war stress may be thought to have liberated the cyclothymic phenomena. Case 166 was that of a man of 38, previously referred to, who developed arteriosclerosis and whose depression and hallucinations had followed four months of trench life devoid of battles or injury. It is possible that this case should be regarded rather as syphilitic or of some unknown organic origin. At all events, it is not clear that it could be made to bear a heavy weight of hypothesis concerning the genesis of cyclothymic psychoses. Case 167, a naval officer who distinguished himself greatly by work on land in Belgium, was regarded by its reporter as one of manic-depressive psychosis with the fatigue of war as its base. It might be queried whether the man’s distinguished work was not due to an early phase of hypomania, after which the cyclothymic effects began. In Case 168 there was some evidence of the effect of war stress, as certain hallucinations grew more intense after the bombardment of Dunkirk; but in point of fact, this man had shown a predisposition and indeed a period of so-called neurasthenia ante-bellum. It is doubtful, therefore, whether there is any case here abstracted which can be used to support the hypothesis that the manic-depressive (cyclothymic) group of mental diseases has had or is likely to have its genesis in war stress. The remaining[867] case (Case 169) is one illustrating a method of treating low blood pressure in depression.
71. The cyclothymic or manic-depressive group is seen in very few cases, totaling seven (Cases 163-169).[866] One idea in the literature about the manic-depressive group suggests it might be somewhat related to Graves’ disease, a theory supported by Stransky in Aschaffenburg’s Handbook. Hyperthyroidism has, of course, been a noticeable feature in many patients during the war, whether in the foreground or background. However, wartime factors have revealed very few cases of cyclothymic (manic-depressive) disorders. Among our seven cases, the first (Case 163) involved a maniacal 59-year-old from Alsace who volunteered due to his hypomania. Case 165, the case of a German man who threw apples from an apple tree into French trenches in No Man’s Land, showed that the war had little to do with the onset of his mania. One case of fugue (Case 164) involved melancholia and anxiety that weren't closely connected to war experiences. In three other cases, life in the trenches and the stress of war may have triggered the cyclothymic symptoms. Case 166 involved a 38-year-old man, previously mentioned, who developed arteriosclerosis, with his depression and hallucinations following four months of trench life marked by no battles or injuries. This case might actually be better classified as syphilitic or from some other unknown organic cause. Regardless, it’s unclear whether it can carry significant weight in supporting any theories about the origins of cyclothymic psychoses. Case 167, a naval officer who excelled in his land duties in Belgium, was seen by the reporter as having manic-depressive psychosis with war fatigue as a contributing factor. It raises the question of whether his notable performance stemmed from an early phase of hypomania, after which the cyclothymic symptoms emerged. In Case 168, there was some indication of war-related stress affecting him, as his hallucinations intensified following the bombardment of Dunkirk; however, this individual had previously shown a predisposition and went through a period of what was termed neurasthenia before the war. Thus, it’s questionable whether any of these cases can substantiate the idea that the manic-depressive (cyclothymic) category of mental illnesses originates or is likely to originate from war stress. The last case (Case 169) demonstrates a method for treating low blood pressure in depression.
To sum up concerning the cyclothymias: War stress seems to have had singularly little effect in the production of fresh attacks, and so far as we are aware, no effect in starting up a manic-depressive diathesis, unless Case 167,—that of the naval officer who distinguished himself in land battles,—looks in that direction. It is, of course, to be conceded that hypomania might readily be overlooked under war conditions, and that suicidal melancholias, belonging in this group, might be interpreted as natural war-made depressions. Very possibly, therefore, this result (running to the effect that the cyclothymic forms of mental disease are rare in military life) may need revision.
To summarize about cyclothymias: War stress seems to have had surprisingly little impact on causing new episodes, and as far as we know, it hasn’t triggered a manic-depressive tendency, unless Case 167,—the naval officer who stood out in land battles,—suggests otherwise. It’s important to acknowledge that hypomania could easily go unnoticed during wartime, and that suicidal depression, which falls into this category, might be seen as simply normal war-related depression. Therefore, it's quite possible that this outcome (indicating that cyclothymic mental disorders are rare in military settings) might need to be reevaluated.
72. Summary of general considerations concerning the nature of the Shell-shock neuroses (paragraphs 40-71).
72. Summary of general considerations regarding the nature of Shell-shock neuroses (paragraphs 40-71).
Having (a) roughly delimited the Shell-shock neuroses from syphilis, epilepsy, and somatic disease, we inquired
After (a) roughly distinguishing the Shell-shock neuroses from syphilis, epilepsy, and physical illness, we asked
(b) What, after all, are functional neuroses? We remained dissatisfied with a definition by negatives. But we found that
(b) What, really, are functional neuroses? We were still not happy with a definition that only explained what they are not. But we found that
(c) practically the problem seemed to reduce to telling the organic apart from the functional and we found that
(c) essentially, the problem boiled down to distinguishing the organic from the functional and we found that
(d) in almost all cases we have to raise the hypothesis of the organic. Also that
(d) in almost all cases we need to consider the hypothesis of the organic. Also that
(e) the absence of external injury is no guarantee against the existence of internal injury. Also that
(e) just because there are no visible injuries doesn't mean there aren't any internal injuries. Also that
(f) cases are frequent enough in which organic and functional phenomena are combined. Also that
(f) there are enough cases where organic and functional phenomena come together. Also that
(g) essentially functional cases may be peritraumatic or metatraumatic (in the sense of Charcot’s hysterotraumatism). But
(g) functional cases are primarily peritraumatic or metatraumatic (referring to Charcot’s concept of hysterotraumatism). But
(h) the statistical majority of cases remains essentially functional.
(h) the statistical majority of cases is still mostly functional.
(i) We then looked over a series of cases developing incidentally in the war and
(i) We then reviewed several cases that emerged incidentally during the war and
(j) we compared these with the war cases, the latter arranged cephalad.
(j) we compared these with the war cases, which were arranged towards the head.
Chart 17
DIAGNOSTIC ALLIANCES OF THE SHELL-SHOCK
NEUROSES
CYCLOTHYMIA
MORONITY
ALCOHOLISM
SHOCK
NEUROSES
EPILEPSY
SOMATOPATHY
Note arrow lengths: Practically we find shell-shock neuroses very different from certain functional (or but mildly organic) disorders and not so different from certain seriously organic disorders.
Note arrow lengths: Basically we see that shell-shock neuroses are quite different from some functional (or only slightly organic) disorders and not so different from some serious organic disorders.
CYCLOTHYMIA
MORONITY
ALCOHOLISM
SHOCK
NEUROSES
EPILEPSY
SOMATOPATHY
Note arrow lengths: Theoretically, shell-shock neuroses, being presumably in large part functional, ought to ally themselves more closely with the left-hand group than with the right-hand group. But they do not!
Note arrow lengths: Theoretically, shell-shock neuroses, which are likely mostly functional, should connect more with the left-hand group than with the right-hand group. But they don't!
In short, these functional diseases are not so hard to distinguish from various other functional diseases as they are from certain organic diseases. The most serious diagnostic problem is between the war neuroses and organic brain disorders.
In short, these functional diseases are not too difficult to tell apart from other functional diseases, but they are more challenging to differentiate from specific organic diseases. The biggest diagnostic challenge lies between war neuroses and organic brain disorders.
Chart 18
LOGICAL PLACE OF THE “REFLEX” DISORDERS
(OF BABINSKI-FROMENT)
| e.g. neurosyphilis paretica ORGANO- PSYCHOPATHIC |
Hysteria e.g. DYNAMO- PSYCHOPATH |
| ORGANO-NEUROPATHIC e.g. neurosyphilis tabetica |
DYNAMO- NEUROPATHY Babinski’s “reflex” or physiopathic disorders e.g. |
A frequent error of neurologists has been to identify “functional” with “psychic” when it came to a question of the classical functional neuroses. The above diagram indicates that “functional” contains more than “psychic.” Doubtless much that goes under the name “unconscious” belongs in the right lower quadrant of this diagram. See discussion in text.
A common mistake made by neurologists has been to equate "functional" with "psychic" when discussing classical functional neuroses. The diagram above shows that "functional" encompasses more than just "psychic." Undoubtedly, a lot of what is referred to as "unconscious" fits into the lower right quadrant of this diagram. See discussion in text.
(k) We found many war cases showing emphasis, reminiscence, or repetition of ante-bellum phenomena (weak spots, locus minoris resistentiae, imitation), but
(k) We found many war cases highlighting emphasis, memories, or repetition of pre-war phenomena (weak spots, locus minoris resistentiae, imitation), but
(l) we also found that perfectly sound untainted men could succumb to Shell-shock neurosis.
(l) we also found that completely healthy, unblemished men could fall victim to Shell-shock neurosis.
(m) We found a few purely psychogenic cases without sign or suspicion of physical shock.
(m) We found a few cases that were purely psychological with no signs or indications of physical trauma.
(n) We studied the localization (traumatotropic) group.
We studied the localization (traumatotropic) group.
(o) We arrived, with the aid of Babinski, at the necessity of splitting functional cases into psychopathic and physiopathic.
(o) We arrived, with Babinski's help, at the need to divide functional cases into psychopathic and physiopathic.
73. Summary of general considerations: continued.
73. Summary of general considerations: ongoing.
We found ourselves looking on the Shell-shock neuroses as, like other functional neuroses, in a sense mental diseases. Perhaps we would better say (to get rid of all suspicion of medicolegal “insanity”) that the Shell-shock neuroses seemed to us in some sense psychopathic. But, though the Shell-shock neuroses looked psychopathic and were presumably more functional than organic in nature, it was a curious thing that, practically speaking, the Shell-shock neuroses proved to be farther away from the more functional of the psychoses than from certain organic psychosis.
We viewed the Shell-shock neuroses as, similar to other functional neuroses, a type of mental disorder. It might be more accurate to say (to avoid any implications of medico-legal “insanity”) that the Shell-shock neuroses appeared to be somewhat psychopathic. However, although the Shell-shock neuroses seemed psychopathic and were likely more functional than organic in nature, it was interesting that, in practical terms, the Shell-shock neuroses were actually more distant from the more functional types of psychoses than from certain organic psychoses.
In particular, we found reliable authors insisting on the practical diagnostic necessity of excluding syphilis, epilepsy, somatic disease—whereas the nature and causes of the Shell-shock neurosis seemed theoretically to withdraw them most remotely from that triad of mainly organic disorders. By the same token, theoretically one might have supposed these Shell-shock neuroses to draw very near to those far less organic disorders (schizophrenia, cyclothymia, feeble-mindedness (i.e., the slighter degrees likely to be found in military service, alcoholism))—yet practically few large diagnostic problems came to light as between the Shell-shock neuroses and the tetrad of dynamic or lightly organic diseases above listed.
We found that reliable authors emphasized the need to rule out syphilis, epilepsy, and physical illnesses as part of the diagnosis. However, the nature and causes of Shell-shock neuroses seemed to be quite distant from that specific group of primarily physical disorders. Similarly, one might think that these Shell-shock neuroses could be closely related to those much less physical disorders (like schizophrenia, cyclothymia, or mild mental disabilities—such as the lesser degrees often seen in military service or alcoholism)—yet in practice, there were not many significant diagnostic issues that emerged between Shell-shock neuroses and the previously mentioned lighter physical or dynamic diseases.
74. Diagrammatically this situation is presented in Chart 17.
74. This situation is shown in __A_TAG_PLACEHOLDER_0__.
(a) Organic mental (cortical), e.g., general paresis.
(a) Organic mental (cortical), e.g., general paresis.
(b) Functional mental (cortical), e.g., hysteria.
Functional mental (cortical), e.g., hysteria.
(c) Organic neural (subcortical), e.g., tabes dorsalis.
(c) Organic neural (subcortical), e.g., tabes dorsalis.
(d) Functional neural (subcortical), e.g., “reflex” disorders.
(d) Functional neural (subcortical), e.g., “reflex” disorders.
Diagnosis Differentiation Issue
75. Having disposed of the problem of the rougher Delimitation of the Shell-shock neuroses, we approach the problem of their finer Differentiation. For the sake of the present argument we propose to regard the Shell-shock neuroses as essentially Dynamopathic, i.e., functional whether in the ordinary mind-born (psychogenic) sense of classical hysteria or in the modern nerve-born (neurogenic) sense of Babinski. The problem of this differentiation will accordingly be that between the dynamopathic and the organopathic.
75. After addressing the rough aspects of the Defining boundaries of shell shock neuroses, we now turn to the issue of their more subtle Differentiation. For this discussion, we will consider the shell shock neuroses as fundamentally Dynamopathic, i.e., functional in the traditional psychological sense of classical hysteria or in the contemporary neurological sense of Babinski. The challenge of this differentiation will therefore be between the dynamopathic and the organopathic.
In the orderly diagnosis of mental disease, from the standpoint of the major orders or groups, we ordinarily come at this point to the focal brain diseases. In analyzing the neuro-psychiatric problem of a so-called Shell-shocker, it is, of course, our bounden duty to exclude syphilis. Even though the percentage of syphilitic victims of Shell-shock is not high, yet these cases promise so much from treatment that they deserve to get their diagnosis as early as possible, and the English workers who have worked most in the syphilitic field insist upon this point.
In the systematic diagnosis of mental illness, when we consider the main categories or groups, we typically arrive at the primary brain diseases. When examining the neuro-psychiatric issues of someone labeled as a Shell-shocker, it is essential that we rule out syphilis. Although the number of syphilitic victims of Shell-shock isn't significant, these cases show considerable potential for treatment, which means they should receive a diagnosis as soon as possible. The English researchers who have focused extensively on syphilis stress the importance of this.
We next proceed, as above indicated, to the elimination of hypophrenia with all the various grades of feeble-mindedness. Thirdly, we try to exclude the various forms of epilepsy; and fourthly, the effects of alcohol, drugs and poisons.
We will now move on, as mentioned earlier, to the exclusion of hypophrenia along with all the different levels of intellectual disability. Thirdly, we will aim to rule out the various types of epilepsy; and fourthly, the impacts of alcohol, drugs, and toxins.
In ordinary civilian practice, such as that at the Psychopathic Hospital, the orderly elimination for diagnostic purposes of the great groups of the syphilitic, hypophrenic (feeble-minded), epileptic and alcoholic, leaves us with cases in which there either is or is not important evidence of organic[872] nervous-system disease, such as that shown in cases with heightened intracranial pressure or in cases with asymmetry of reflexes and other forms of parareflexia. In military practice these logical questions of prior elimination of syphilis, feeble-mindedness, epilepsy, and alcoholism must go a-glimmering at first, unless their signs are so obvious as to permit diagnosis by inspection.
In everyday civilian settings, like the Psychopathic Hospital, the careful screening for diagnostic purposes of major groups such as syphilitics, those with intellectual disabilities, epileptics, and alcoholics, leaves us with cases where there is either significant evidence of organic nervous system disease or there isn't. This includes cases with increased pressure inside the skull or those showing uneven reflexes and other types of abnormal reflexes. In military settings, these logical questions about previously eliminating syphilis, intellectual disabilities, epilepsy, and alcoholism are often ignored initially, unless their signs are so clear that they can be diagnosed just by looking.
76. But the nervous and mental cases almost one and all give rise to the suspicion at least of organic disease, possibly traumatic in origin. Even when a man falls to the ground without a scratch upon his skin, there is some question whether in his fall he has not sustained some slight intracranial hemorrhage which the lumbar puncture fluid might show. Add to this that the signs of hysteria are very often unilateral, and it will readily be conceived how much like an organic case an hysteric in the casualty clearing station may look. Rapid decision may be necessary in order to get immediate effects in psychotherapy a few minutes or hours after the shell explosion, and one may need to choose between applying a possibly unsuccessful psychotherapy forthwith and making a thorough neurological examination. As Babinski has pointed out, making a thorough neurological examination gives opportunity for all sorts of medical suggestion to be conveyed to the patient. It would appear that many an hysterical anesthesia has been given to a patient by the very suggestion of the physician testing sensation. Here one does not refer to malingering in the conscious and designed sense of the term, but to the operation of some genuinely psychopathic, that is to say, hysterical process.
76. However, most of the cases related to nervous and mental issues raise at least suspicion of underlying illness, possibly due to trauma. Even if a person falls to the ground without any visible injuries, there’s still a chance that they could have experienced a minor intracranial hemorrhage that a lumbar puncture could detect. Additionally, the symptoms of hysteria are often one-sided, making it easy to see how a hysterical patient in the emergency room might closely resemble someone with an organic condition. Quick decisions may be necessary to achieve immediate results from psychotherapy a few minutes or hours after the explosion, which may force a choice between starting potentially ineffective psychotherapy right away or conducting a thorough neurological exam. As Babinski noted, performing a full neurological examination allows for various medical suggestions to be communicated to the patient. It seems that many cases of hysterical anesthesia have been induced simply through the physician’s suggestion while testing sensation. This isn't about feigning illness in a deliberate way, but rather about the effects of a genuinely psychopathic, or hysterical, process.
77. In the case of head injury, naturally the majority of nerve phenomena will ordinarily be upon the opposite side of the body to the side of the head that is injured. The reverse situation holds for hysterical cases, wherein it would appear that the bursting of a shell, let us say upon the left side of the body, seems to determine contractures, paralyses and anesthesias to that same left side of the body; now and then complicated cases appear which put the neurologist through his best paces. Such a case is that of a man who was wounded on the left side of the head and promptly developed[873] a hemiplegia on the same (left) side, with aphasia. Now aphasia ought to be the result of a lesion on the left side of the brain in the common run of cases, whereas left-sided hemiplegia ought to be the result of lesion on the right side of the brain. In point of fact, the analyst of this case felt that he was dealing with a direct injury on the left side of the brain, leading to aphasia, and a lesion by contrecoup on the right side of the brain, leading to a left-sided hemiplegia.
77. In cases of head injury, typically most nerve issues will be found on the side of the body opposite to where the head was injured. In contrast, with hysterical cases, it seems that an explosion, for example on the left side of the body, can cause contractures, paralysis, and loss of sensation on that same left side. Occasionally, there are complicated cases that really challenge neurologists. One such case involved a man who was injured on the left side of his head and quickly developed [873] a hemiplegia on the same (left) side, with aphasia. Usually, aphasia is expected from damage on the left side of the brain, while left-sided hemiplegia is typically caused by damage on the right side. However, the analyst for this case believed he was dealing with a direct injury to the left side of the brain causing the aphasia, along with a secondary injury (contrecoup) on the right side of the brain, resulting in left-sided hemiplegia.
It is not only at the casualty clearing stations and along the lines of communication that the difficulties in telling Shell-shock in the neurotic sense from traumatic psychosis and the effects of focal brain lesions are found, since the literature amply shows that diagnostic problems remain open for weeks or months in the various institutions of the interior, to which all the belligerents have been forced to send their cases.
It’s not just at the casualty clearing stations and along the supply lines where it’s hard to distinguish shell shock in the neurotic sense from traumatic psychosis and the effects of focal brain injuries. The literature clearly indicates that diagnostic issues persist for weeks or months in various facilities inland, to which all the warring sides have had to send their patients.
78. A glance at the differential tables that have been developed, for example, by the French neurologists, will show how fine the diagnosis betwixt a hysterical and an organic disease may be, especially when we consider how often there are admixtures of the two. The rule holds for the vast majority of cases that absolute bullet wounds or shrapnel wounds do not produce Shell-shock; and the statistical story is so clear that one might almost think of the wounds as in some sense protective against shock, that is, against Shell-shock, not against traumatic or surgical shock. Nevertheless, by some process whose nature is obscure, the hysteric is apt to pick up some slight wound and, as it were, surround this wound with hysterical anesthesia, hyperesthesia, paralysis or contractures.
78. A look at the differential tables created by French neurologists will reveal how subtle the distinction is between hysterical and organic diseases, especially since these conditions often overlap. In most cases, it’s true that actual bullet or shrapnel wounds do not lead to Shell-shock; the statistics are so clear that one could almost consider these wounds protective against shock, specifically against Shell-shock, not against traumatic or surgical shock. However, through a process that isn’t entirely understood, a hysterical person may sustain a minor injury and, in a way, encase this injury with hysterical anesthesia, heightened sensitivity, paralysis, or muscle contractions.
The chances are, if we should collect all our civilian cases of Railway Spine and of industrial accident with traumatic neuroses, we should be able to prove this same strange relation between slight wound in a particular part of the body and the local determination of hysterical symptoms to that region. Of course, the determination follows no known laws of nerve distribution to skin or muscles, and the effect is apparently a psychopathic or, at all events, a dynamic process without clear relations to the accepted landmarks.
If we were to gather all our civilian cases of Railway Spine and industrial accidents involving traumatic neuroses, we could likely demonstrate this same strange connection between a minor injury to a specific part of the body and the localized development of hysterical symptoms in that area. Naturally, this connection doesn't adhere to any known patterns of nerve distribution to the skin or muscles, and the outcome seems to be a psychopathic or, at the very least, a dynamic process that doesn't have obvious links to the established reference points.
I do not mean to suggest, that aside from the hurry of war, the differential diagnoses here are more difficult than those in civilian practice; but the difficulties are at least as great as those that have faced the civilian practitioner. What needs emphasis is that just because we have concluded that the statistical majority of the cases of so-called Shell-shock belongs in the division of the neuroses, we should not feel too cock-sure that a given case of alleged Shell-shock appearing in the war zone or behind it is necessarily a case of neurosis.
I don't want to imply that, aside from the rush of war, the different diagnoses here are more challenging than those in civilian medical practice; but the challenges are at least as significant as those faced by civilian doctors. It’s important to highlight that just because we've determined that most cases of so-called Shell-shock are classified as neuroses, we should not be too confident that a particular case of alleged Shell-shock occurring in or around the war zone is definitely a case of neurosis.
After the early “period of election” for psychotherapy in the war zone has passed, there can be no excuse except general war conditions for not according to every case of alleged Shell-shock a complete neuropsychiatric examination, having due regard to the ideas of Babinski concerning medical suggestion of new increments and appendices to the original hysteria, developed in battle or shortly thereafter.
After the initial "election period" for psychotherapy in the war zone has ended, there’s really no reason—other than the overall conditions of war—for not giving every case of reported Shell-shock a thorough neuropsychiatric examination. This should take into account Babinski's ideas about how medical suggestions can lead to new developments and additions to the original hysteria that emerged during or immediately after battle.
We have, however, been able to find in the literature good instances of puzzling diagnosis in which such conditions are in evidence as acute meningitis of various forms, hydrophobia, tetanus, and the like.
We have, however, been able to find in the literature good instances of puzzling diagnosis in which such conditions are in evidence as acute meningitis of various forms, hydrophobia, tetanus, and the like.
Especially in the diagnosis against Shell-shock hysterias we may need to think of the abnormal forms of tetanus, to which an entire book in the Collection Horizon has been devoted. The differential diagnostic tables here draw up distinctions between local tetanus, involving, let us say, the contracture of one arm, as against a hysterical monoplegia.
Especially in diagnosing shell shock hysteria, we might need to consider the unusual types of tetanus, which an entire book in the Collection Horizon discusses. The differential diagnostic tables presented here outline the differences between local tetanus, which could, for example, involve the contraction of one arm, and hysterical monoplegia.
79. The focal brain group of psychoses here termed encephalopsychoses, is illustrated by a comparatively short series of cases, 16 in number (Cases 103-117). Many more cases of this group are presented in Section B, On the Nature and Causes of Shell-shock. The motive here is to show sundry effects of focal brain lesions produced in the war and not related with shell-shock. Case 103 was the curious case (see above) of aphasia with hemiplegia—not upon the right side, but upon the left side. There had been a wound in the left parietal region, and the aphasia was presumably consequent upon a direct affection of the left hemisphere. On the other hand, the left-sided hemiplegia may probably be regarded as due to lesions on the right side of the brain produced[875] by contrecoup. The case not only has surgical implications and suggestions of importance, but also it throws some light on the possibilities in concussion of minor degree. As the cases in Section B (On the Nature and Causes of Shell-shock) show, shell-shock, the physical factor, is apt to produce anesthesia and paralysis or contracture on the side exposed to the shell-shock. The means by which these symptoms ipsilateral with the shock are produced is commonly thought to be the “hysterical mechanism,” whatever that may be. Lhermitte, however, suggests that in some cases such phenomena might be due to an actual brain jarring with contrecoup effects. However, it must be granted that Case 103 did not come to autopsy.
79. The main brain group of psychoses, called encephalopsychoses, is demonstrated by a relatively short series of 16 cases (Cases 103-117). Many more cases in this category are discussed in Section B, On the Nature and Causes of Shell-shock. The aim here is to highlight various effects of focal brain injuries resulting from the war that are not related to shell shock. Case 103 was the interesting case (see above) of aphasia with hemiplegia—not on the right side, but on the left side. There was an injury in the left parietal area, and the aphasia was likely due to direct damage to the left hemisphere. On the other hand, the left-sided hemiplegia may be attributed to injuries on the right side of the brain caused by contrecoup. This case not only has surgical implications and important suggestions but also sheds light on the potential effects of minor concussions. As the cases in Section B (On the Nature and Causes of Shell-shock) illustrate, shell shock, as the physical factor, tends to result in anesthesia and paralysis or contracture on the side that faced the shock. The way these symptoms occur on the same side as the shock is usually believed to be related to the so-called “hysterical mechanism,” whatever that might mean. Lhermitte, however, proposes that in some instances, these phenomena could stem from an actual brain jarring with contrecoup effects. Nonetheless, it must be acknowledged that Case 103 did not undergo autopsy.
80. Case 104 might perhaps better be considered in the section on alcoholism, since a gun-shot wound of the head may be regarded as having produced intolerance of alcohol in the classical manner, similar to that described in Case 97, wherein, however, the trauma was ante-bellum. Peculiar crises associated with cortical blindness, vertigo, and hallucinations, characterized a case of brain trauma by bullet (Case 105). Case 106 is that of a Tunisian, who before the war had had a number of theopathic traits with mystical hallucinations, but after a gun-shot wound of the occiput developed lilliputian hallucinations and micromegalopsia.
80. Case 104 might be better discussed in the section on alcoholism because a gunshot wound to the head can cause alcohol intolerance in a classic way, similar to what's described in Case 97, although that trauma occurred before the war. Unique crises related to cortical blindness, dizziness, and hallucinations were noted in a case of brain trauma caused by a bullet (Case 105). Case 106 refers to a Tunisian who had experienced several mystically-related traits with hallucinations before the war, but after a gunshot wound to the back of the head, he developed tiny hallucinations and changes in perception of size.
81. Cases 107-112 are cases of infection or probable infection. Cases 107 and 108 are instances of meningococcus meningitis, the second of which appears to have followed shell-shock (?). Case 107 led to psychosis with dementia. Case 109 developed a meningitic syndrome, which followed shell explosion a metre away, the syndrome lasting 14 months. The spinal puncture fluid was several times found to contain blood. There was apparently no infection of the fluid as in Case 112. Possibly Case 109 should be set down as an unusual example of shell-shock psychosis, chiefly dependent upon meningeal hemorrhage.
81. Cases 107-112 are cases of infection or likely infection. Cases 107 and 108 are examples of meningococcus meningitis, the second of which seems to have followed shell shock (?). Case 107 resulted in psychosis with dementia. Case 109 developed a meningitic syndrome after a shell explosion just a meter away, with the syndrome lasting 14 months. The spinal puncture fluid was found to contain blood several times. There was apparently no infection in the fluid as in Case 112. Possibly Case 109 should be noted as an unusual case of shell shock psychosis, primarily due to meningeal bleeding.
82. A syphilitic (Case 110) in which appropriate tests were made and found positive, showed at autopsy a yellowish abscess or area of softening in the right hemisphere. The curious point about this case was that the only neurological[876] phenomenon in the case was the absence of knee-jerks in the early part of the day; later in the day, they would appear once more. Possibly Case 111, a case of somewhat doubtful nature but presumably of organic hemiplegia, ought to be aligned more with the group of cases illustrating the nature and causes of Shell-shock. The case was not one with the physical factor shell-shock, since the phenomena began ten days after a serene convalescence following an operation for chronic appendicitis. Perhaps the case was one of organic lesion grafted upon a neurosis.
82. A syphilitic (Case 110) in which appropriate tests were performed and came back positive, showed at autopsy a yellowish abscess or area of softening in the right hemisphere. The interesting aspect of this case was that the only neurological[876] symptom observed was the absence of knee-jerks earlier in the day; later in the day, they would return. Perhaps Case 111, a case of somewhat questionable nature but likely of organic hemiplegia, should be categorized more with the group of cases that illustrate the nature and causes of Shell-shock. This case did not involve the physical factor of shell-shock, since the symptoms began ten days after a smooth recovery from surgery for chronic appendicitis. It is possible that this case involved an organic lesion layered on top of a neurosis.
83. Case 112 is the one noted above of infection of the spinal fluid. It is the only case of infected meningeal hemorrhage observed by Guillain and Barré in a wide experience. As a rule, these hemorrhages remain aseptic and have a favorable prognosis. The organism cultivated from the spinal fluid proved to be the pneumococcus. Case 113 yielded a somewhat remarkable phenomenon and perhaps would be more logically considered in relation with the series of cases in Section B that show the picking up of ante-bellum weak spots (Cases 287-301); for this subject had had two serious affections of the brain ante-bellum. He had had a poliomyelitis at five, affecting the left leg, and he had had a right hemiplegia with aphasia following pneumonia, at 20. He was struck (but apparently not wounded) by shrapnel on the right shoulder, and developed athetotic movements of the right hand, as well as a general weakness of the left leg. In this case, according to Batten, the stress had been sufficient to bring into prominence symptoms due to an old cerebral lesion. Whether the mechanism in this case is hysterical is doubtful.
83. Case 112 refers to the infection of the spinal fluid mentioned earlier. It's the only instance of infected meningeal hemorrhage documented by Guillain and Barré in their extensive experience. Typically, these hemorrhages are aseptic and have a good prognosis. The bacteria grown from the spinal fluid turned out to be the pneumococcus. Case 113 revealed a somewhat notable phenomenon and might be better understood in connection with the cases in Section B that indicate previous weak spots from before the war (Cases 287-301); this subject had experienced two serious brain issues prior to the war. He had poliomyelitis at five, which affected his left leg, and he had a right hemiplegia with aphasia following pneumonia at the age of 20. He was hit (but apparently not injured) by shrapnel on his right shoulder and began exhibiting athetotic movements in his right hand, along with a general weakness in his left leg. In this situation, according to Batten, the stress was enough to highlight symptoms from an old brain injury. It’s uncertain if the mechanism in this case is hysterical.
84. That not every case of hemianesthesia is hysterical is suggested by Case 114, in which the diagnosis of hysteria was actually made; but the diagnosis was soon rendered doubtful by the fact that there was no evidence of autosuggestion or heterosuggestion. Other phenomena make a diagnosis of thalamic hemianesthesia more likely.
84. The fact that not every instance of hemianesthesia is hysterical is indicated by Case 114, where hysteria was actually diagnosed; however, this diagnosis quickly became questionable because there was no sign of autosuggestion or heterosuggestion. Other symptoms make a diagnosis of thalamic hemianesthesia more probable.
85. Although Shell-shock is not the subject of this section, yet a case of syndrome strongly suggesting multiple sclerosis is here inserted, following shell-shock (Case 115). The[877] co-existence of hysterical and organic symptoms is illustrated in Case 116, one of mine explosion, and Case 117, one of injury to back. Case 116 somewhat resembled another case of Smyly (Case 219).
85. While shell shock isn't the focus of this section, a case of a syndrome that strongly resembles multiple sclerosis is included here, following shell shock (Case 115). The[877] presence of both hysterical and physical symptoms is demonstrated in Case 116, which involves a mine explosion, and Case 117, which involves a back injury. Case 116 was somewhat similar to another case of Smyly (Case 219).
86. Differential Diagnosis between Organic and Hysteric Hemiplegia. Babinski, 1900.
86. Differential Diagnosis between Organic and Hysterical Hemiplegia. Babinski, 1900.
| Organic Hemiplegia | Hysterical Hemiplegia |
|---|---|
| 1. Paralysis unilateral. | 1. Paralysis not always unilateral; especially facial paralysis, usually bilateral. |
| 2. Paralysis not symptomatic., e.g., in unilateral facial paresis, the paresis occurs also when bilateral synergic movements are being performed. | 2. Paralysis sometimes symptomatic; facial paralysis almost always symptomatic. With complete unilateral paralysis, the muscles of the paralyzed side may function normally during the performance of bilateral synergic movements. |
| 3. Paralysis affects voluntary, conscious, and unconscious or sub-conscious movements; hence, (a) platysma sign,[12] (b) sign of combined flexion of thigh and trunk, and (c) absence of active balancing arm movements in walking contrasted with exaggeration of passive balancing movements (limb inert on sudden turn of body). | 3. Voluntary, unconscious, or sub-conscious movements not disordered. Absence of platysma sign and combined flexion of thigh and trunk. The active balance movements of arm may be lacking but there is no exaggeration of passive balance movements. |
| 4. Tongue usually slightly deviated to the paralyzed side. | 4. Tongue sometimes slightly deviated to the paralyzed side; but sometimes contralateral deviation. |
| 5. Hypertonicity of muscles, especially at first. The buccal commissure may be lowered, the eyebrow lowered; there may be exaggerated flexion of the forearm, and the sign of pronation may occur (hand left to itself lies in pronation). | 5. No hypertonicity of muscles. If facial asymmetry exists, it is due to spasm. No exaggerated flexion of forearm, and no pronation sign. |
| 6. Tendon and bone reflexes often disturbed at the beginning, either absent, weakened, or exaggerated (almost always exaggerated.) In many cases, there is epileptoid trepidation of the foot. | 6. No alteration of tendon or bone reflexes. No trepidation of the foot.[878] |
| 7. Skin reflexes usually disordered. Abdominal and cremasteric reflexes, especially at first, weakened or abolished. On stimulation of sole, toes, and especially the great toe, are extended on the metatarsals. Babinski toe reflex. Extension of great toe often associated with abduction of other toes (fan sign). Sometimes exaggeration of reflexes of defence. | 7. No disturbance of skin reflexes. Abdominal and cremasteric reflexes normal. Babinski toe reflex and fan sign absent. Defense reflexes not exaggerated. |
| 8. Contracture characteristic and non-reproducible by voluntary contractions. The hand-grip yields a sensation of elastic resistance, automatically accentuated on passive extension of the hand. | 8. The contracture can be reproduced by voluntary contractions. |
| 9. Evolution of diseased regular contracture follows flaccidity. When regression of disorder occurs, it is progressive. Paralysis not subject to ups and downs (motor defect fixed). |
9. Evolution of disease capricious. Paralysis may remain indefinitely flaccid or may be spastic from the beginning.
Spastic phenomena may sometimes be associated (particularly in the face) with characteristic phenomena. The disorder may get better and worse alternately several times, alter rapidly in intensity, and present transitory remissions which may last even but a few moments (motor defect variable). |
87. Differential between Reflex (Physiopathic) Contracture and Paralysis, and Hysterical Contracture and Paralysis. Babinski, 1917.
87. Difference between Reflex (Physiopathic) Contracture and Paralysis, and Hysterical Contracture and Paralysis. Babinski, 1917.
| Reflex | Hysterical |
|---|---|
| 1. Paralysis usually limited but severe and obstinate even when methodically treated. | 1. Paralysis usually extensive but superficial and transient if treated. |
| 2. In the hypertonic forms attitude of the limb does not correspond to any natural attitude. | 2. The hysterical contracture as a rule resembles a natural attitude fixed. |
| 3. Amyotrophy marked and of rapid development. | 3. Amyotrophy, as a rule, absent, even when the paralysis is of long standing. If existent, it is not marked. |
| 4. Vasomotor and thermic disorder often very marked, accompanied by an often very pronounced reduction in amplitude of oscillations measured by oscillometer. | 4. There may be thermo-asymmetry but it is slight. There are no very characteristic vasomotor disorders nor modifications in amplitude of oscillations.[879] |
| 5. Sometimes very marked hyperidrosis. | 5. No sharply defined hyperidrosis. |
| 6. Tendon reflexes often exaggerated. | 6. No modifications of tendon reflexes. |
| 7. Hypotonia sometimes very well marked, and in arm paralysis main ballante. | 7. Hypotonia absent. |
| 8. Mechanical over excitability of muscles, often accompanied by slow response (?). | 8. Over-excitability of muscles absent. |
| 9. Fibrotendinous retractions of rapid development except in the rare completely flaccid forms. | 9. No retractions even if paralysis is of long duration. |
| 10. Trophic disorders of bone, decalcification of the hairs and of the phanères. | 10. No trophic disorders. |
88. The section on Shell-shock diagnosis contains 102 cases (Cases 371-472). These cases differ in no respect from those of Section B except that many of them are more puzzling and dubious and have been presented by their reporters more from the standpoint of diagnosis than from that of etiology or therapeutics. In general arrangement, the cases roughly correspond to those of Section B. First are four cases illustrating the value of lumbar puncture data (Cases 371-374). There follow cases with either a mixture of organic and functional symptoms, or such a constellation of symptoms as might readily lead to erroneous diagnosis (Cases 375-381). Retention and incontinence of urine after shell-shock are illustrated in Cases 382-384. Crural monoplegia, monocontractures, and other affections of one leg are shown in Cases 385-392; but these monocrural cases are in many respects peculiar or even unique as compared with the monocrural cases of Section B. Peculiar paraplegias or spasms affecting both legs are found in the series 393-395. Then follow (Cases 396-400) other cases of doubtful spinal cord lesion or shock, including several with dysbasia. Camptocormia, astasia-abasia and abdominothoracic contracture are found respectively in 401, 402, and 403. Affections of one arm follow (Cases 404-409). An assortment of peculiar cases in which the differentiation between hysteria and[880] structural disease is in question, is found in Cases 410-415. Peripheral nerve injuries of a sort which might be confused with Shell-shock phenomena, including one of light tetanus, are considered in Cases 416-419. A variety of cases bearing upon the question of the reflex or physiopathic disorders of Babinski is found in the series of Cases 420-432. Peculiar eye phenomena are presented by Cases 433-438; and cases of otological interest are 439 and 440. Epileptoid, obsessive, fugue, and amnestic phenomena follow in Cases 441-450; 451 and 452 are cases of soldier’s heart. The simulation question is presented in a series of 20 cases (Cases 453-472).
88. The section on Shell-shock diagnosis includes 102 cases (Cases 371-472). These cases are no different from those of Section B except that many are more confusing and questionable, and their reporters have presented them from a diagnostic perspective rather than focusing on etiology or therapy. In terms of overall organization, the cases roughly align with those of Section B. First, there are four cases that highlight the value of lumbar puncture data (Cases 371-374). Next are cases featuring either a mix of organic and functional symptoms, or a combination of symptoms that could easily lead to misdiagnosis (Cases 375-381). Retention and incontinence of urine following shell shock are illustrated in Cases 382-384. Crural monoplegia, monocontractures, and other issues affecting one leg are shown in Cases 385-392; however, these monocrural cases are quite peculiar or even unique compared to the monocrural cases of Section B. Unusual paraplegias or spasms affecting both legs are included in the series 393-395. There are also (Cases 396-400) other cases that raise doubts about spinal cord lesions or shock, including several with dysbasia. Camptocormia, astasia-abasia, and abdominothoracic contracture are noted respectively in 401, 402, and 403. Issues affecting one arm follow (Cases 404-409). A range of unusual cases where the distinction between hysteria and[880] structural disease is questioned can be found in Cases 410-415. Peripheral nerve injuries that might be mistaken for Shell-shock phenomena, including a case of mild tetanus, are discussed in Cases 416-419. A variety of cases related to reflex or physiopathic disorders of Babinski are included in the series of Cases 420-432. Unusual eye phenomena are presented by Cases 433-438; and cases of otological interest are found in 439 and 440. Epileptoid, obsessive, fugue, and amnestic phenomena follow in Cases 441-450; 451 and 452 are cases of soldier’s heart. The simulation question is discussed in a series of 20 cases (Cases 453-472).
General Nature of PTSD
89. We are now ready to consider in how far Shell-shock[13] is a distinctive disease. The physical event, shell-shock[13] we have seen at work in most of the major groups of mental disease and in some groups of nervous disease. Shell-shock, the physical event, has started up a “Shell-shock” paresis, a “Shell-shock” epilepsy, a “Shell-shock” Graves’ disease, a “Shell-shock” dementia praecox, wherein the term “Shell-shock” is merely a more specific term than the term “traumatic.” The physical event, shell-shock, has in special ways also changed the responses of the feeble-minded, the alcoholic, the cyclothymic, and the psychopathic person of whatever ill-defined sort may get into military service.
89. We are now ready to examine how Shell-shock[13] is a unique condition. The physical event of shell-shock[13] has been observed in many major mental disorders and some nervous disorders. Shell-shock, as a physical event, has given rise to a “Shell-shock” paresis, a “Shell-shock” epilepsy, a “Shell-shock” Graves’ disease, and a “Shell-shock” dementia praecox, where “Shell-shock” serves as a more specific term compared to “traumatic.” This physical event, shell-shock, has also altered the responses of individuals who are feeble-minded, alcoholic, cyclothymic, or psychopathic, regardless of their unclear classification, who may enlist in the military.
[13] I capitalize Shell-shock here (as elsewhere) to indicate the name of a supposed disease entity and leave shell-shock without an initial capital to indicate the physical event.
[13] I capitalize Shell-shock here (and in other instances) to signify the name of a supposed disease and leave shell-shock in lowercase to refer to the physical event.
The physical event, shell-shock, has likewise caused focal irritative and destructive brain disease, spinal cord disease, peripheral nerve disease; and many well-recognized species of the so-called “organic” diseases of the nervous system have been produced. Shell-shock “organic” diseases have proved as difficult to tell from all sorts of Shell-shock “functional” diseases as ever have been the organic and functional analogues of these diseases in peace practice.
The physical event of shell shock has also led to specific irritating and damaging brain conditions, spinal cord diseases, and peripheral nerve issues; many well-known types of the so-called "organic" diseases of the nervous system have emerged. Shell shock "organic" diseases have proven to be just as challenging to distinguish from various shell shock "functional" diseases as the organic and functional equivalents of these diseases have been in regular medical practice.
But, besides (a) sharing in the cause of mental and nervous disease (in the sense of “Shell-shock” general paresis and “Shell-shock” tabes, wherein at least one other factor, viz. the spirochete, is known to be at work) and (b) producing mental and nervous disease by killing or weakening or sensitizing neurones in the classical manner of the “focal” lesion, the physical event, Shell-shock, (c) appears able to bring out the subtler diseases and dispositions of mind which we term psychoneuroses, that is, hysteria, neurasthenia, psychasthenia. Just as we have for years spoken of “traumatic” psychoneuroses, so we may now speak of “Shell-shock” psychoneuroses—nor should anyone believe we cheat ourselves with the idea that the adjective “Shell-shock” has helped us more re genesis than the adjective “traumatic.” “Shell-shock hysteria” and “traumatic hysteria” are on precisely the same—slippery—footing in the matter of their origin. The physics and chemistry of the psychoneuroses remain in Egyptian darkness.
But besides (a) being involved in mental and nervous disorders (like “Shell-shock” general paresis and “Shell-shock” tabes, where at least one other factor, viz. the spirochete, is known to play a role) and (b) causing mental and nervous disorders by killing, weakening, or sensitizing neurons in the classic way of the “focal” lesion, the physical event, Shell-shock, (c) also seems capable of revealing the subtler mental disorders and tendencies we call psychoneuroses, such as hysteria, neurasthenia, and psychasthenia. Just as we've talked about “traumatic” psychoneuroses for years, we can now talk about “Shell-shock” psychoneuroses— and no one should think we're fooling ourselves by assuming that the term “Shell-shock” has given us more re genesis than the term “traumatic.” “Shell-shock hysteria” and “traumatic hysteria” are on the exact same—slippery—ground regarding their origins. The physics and chemistry of psychoneuroses are still shrouded in mystery.
The physical event, shell-shock, then, as the common man might say, affects body, brain, and mind in a great number of familiar ways; and these familiar ways remain as plain or as blind as the neuropathology and the psychopathology of today leave them. If thunderstorms and earthquakes got suddenly more frequent, we should have numbers of “lightning neuroses” and “earthquake hysterias,” neither of which would render the physics and chemistry of the psychoneuroses immediately a whit clearer.
The physical event, shell shock, as an everyday person might put it, impacts the body, brain, and mind in a lot of familiar ways; and these familiar ways stay as obvious or as unclear as the current understanding of neuropathology and psychopathology allows. If thunderstorms and earthquakes suddenly became more common, we'd end up with many cases of "lightning neuroses" and "earthquake hysteria," but that wouldn't make the physics and chemistry of psychoneuroses any clearer.
When the common man speaks of some one as suffering from lightning stroke or earthquake, he is entitled to be met halfway by his hearer, who readily understands that the victim is suffering some sort of transient or permanent effects of the stroke or quake. In a like common sense should the term shell-shock be taken. Stroke, quake, or shock, each physical event is recognized as a factor in the situation. An event has become a factor. A condition for which the noun “shell-shock” was descriptive, in the present tense of some event, has passed into history; and the adjective “shell-shock” is now explanatory of the past cause, or one of the past causes, of a new situation. Shell-shock, the physical[882] event, takes part in a great number of pathological events and as such lapses from noun to adjective.
When an everyday person talks about someone suffering from a lightning strike or an earthquake, they expect their listener to understand that the person is experiencing some kind of temporary or lasting effects from the strike or quake. Similarly, we should interpret the term shell-shock with the same common sense. Each of these physical events—stroke, quake, or shock—is recognized as a contributing factor to the situation. An event has become a factor. The condition described by the term “shell-shock,” which referred to the immediate effects of an event, is now part of history; and the adjective “shell-shock” now explains the past cause, or one of the past causes, of a new situation. Shell-shock, as a physical [882] event, plays a role in many pathological events and therefore shifts from being a noun to an adjective.
But what are these pathological events, viz., the conditions of disease, that supervene? So far, in our consideration of psychoses incidental in the war, we have found Shell-shock varieties, perhaps, of mental disease; again, possibly a few Shell-shock species, using both these terms, variety and species, in a quasi botanical or zoölogical sense. But in either instance we do not rise, under the ordinary principles of nomenclature, beyond the adjective: Is there any evidence that shell-shock, the physical happening, has issued in a pathological event of greater dignity, namely, a genus of disease? Can shell-shock rise to the dignity of a proper noun, Shell-shock, so that we might think of e.g., a new genus of the psychoneuroses, something coördinate with hysteria, neurasthenia, psychasthenia? None, I believe, has the hardihood to propose a new genus of mental or nervous disease for Shell-shock regarded as a pathological event. A fortiori, it is unheard-of to think of Shell-shock, the pathological event, as representing a new order of such events, coördinate with the psychoneuroses or the epilepsies, for example.
But what are these pathological events, namely, the conditions of disease that occur? So far, in our discussion of the psychoses related to the war, we have identified different types of Shell-shock, perhaps as varieties of mental illness; again, possibly a few distinct forms of Shell-shock, using both terms, variety and species, in a somewhat botanical or zoological sense. However, in either case, we don’t categorize it beyond the descriptive level: Is there any evidence that Shell-shock, as a physical event, has led to a more significant pathological occurrence, namely, a type of disease? Can Shell-shock be elevated to the status of a proper noun, Shell-shock, so that we might consider, for example, a new category of psychoneuroses, something alongside hysteria, neurasthenia, and psychasthenia? I believe no one has the audacity to suggest a new category of mental or nervous disease for Shell-shock viewed as a pathological event. Furthermore, it is simply unheard of to think of Shell-shock, the pathological event, as representing a new class of such events, comparable to the psychoneuroses or epilepsies, for instance.
Shell-shock, the pathological event, we conclude, is a variety or a species, hardly a genus or an order of mental or nervous diseases. If we can keep in mind the obvious distinction between shell-shock, the physical event, and Shell-shock, the pathological event, we shall save ourselves much trouble. And if we can apply the ordinary criteria for the differentiation of the great groups (or orders) and the lesser groups (or genera) of mental and nervous disease to the given concrete case, we shall not go far wrong therapeutically in any case of so-called Shell-shock. For Shell-shock, the pathological event, becomes a humble variety or species of disease whose therapeutic indications are in larger part those of higher and comparatively well-recognized genera of disease, e.g., hysteria, neurasthenia, psychasthenia.
Shell shock, as a psychological condition, is really a specific type of mental or nervous disorder, not a broad category. If we can clearly differentiate between shell shock as a physical occurrence and shell shock as a psychological condition, we'll avoid a lot of confusion. Furthermore, if we use the usual methods for classifying major groups and subgroups of mental and nervous diseases when examining any individual case of so-called shell shock, we are likely to be correct in our treatment approach. The psychological aspect of shell shock is a straightforward type of disorder, and its treatment largely aligns with those of more recognized categories of mental illness, such as hysteria, neurasthenia, and psychasthenia.
A shock is not a smash, a crush, a breach. A shock literally shakes. The shaken thing stays, for a time at least. Shaken up or down, the victim of shock is not at first thought[883] of as done for. The spirit of the language is against the thought of shock as destruction or even as permanent irritation. Shock ought to be a “functional” rather than an “organic” thing, as medicine bandies these terms about. Shell-shock or Surgical Shock, it is all one to the logic of shock, which is thought of as a physical or chemical disturbance of mechanisms and arrangements that are, or ought to be readjustable. The one character which the late Professor Royce told me (in conversation) he could find in the term “functional” was the idea “reversible.” Shock is or ought to be, as a pathological event, reversible.
A shock isn’t a smash, a crush, or a break. A shock literally shakes things up. What’s shaken usually stays that way for a while. When someone experiences shock, they’re not immediately considered done for. The essence of the language opposes the idea that shock leads to destruction or even lasting distress. Shock should be seen as a “functional” rather than an “organic” issue, as medicine often describes these concepts. Whether it’s shell-shock or surgical shock, it all aligns with the reasoning of shock, viewed as a physical or chemical disruption of systems and structures that can or should be adjusted. The only aspect that the late Professor Royce mentioned to me (in conversation) he could associate with the term “functional” was the concept of “reversible.” Shock is, or should be, a reversible pathological event.
If this thought is in the backs of our minds as we think of Shell-shock, it can readily be seen why the “organic,” that is, non-reversible diseases, do not take kindly to the term Shell-shock. Shell-shock, the pathological event, prefers to be an item in the pathology of function. Can we further specify? The pathology of function, neuropsychically taken, considers such great groups as the psychoneuroses; (so far as we know) the cyclothymias; some of the symptomatic psychoses; a portion of the alcohol and drug group; some of the epilepsies; perhaps the dementia præcox group; not to mention various unresolved psychopathias. The psychoneuroses are the group most innocent of every “organic” taint: the machinery is assumed to be most normal in them and presumably the effects of disorder most reversible.
If we keep this thought in mind while considering Shell-shock, it's easy to see why "organic," or non-reversible, diseases are resistant to the term Shell-shock. Shell-shock, as a pathological event, is more comfortable being listed under functional pathology. Can we be more specific? Functional pathology, from a neuropsychological perspective, includes significant groups like psychoneuroses; (as far as we know) cyclothymias; some symptomatic psychoses; parts of the alcohol and drug-related issues; some epilepsies; and possibly the dementia præcox group; not to mention various unresolved psychopathologies. The psychoneuroses are the group most free from any "organic" implications: their mechanisms are assumed to be mostly normal, and the effects of any disorder are likely to be reversible.
Shall we not therefore accept the psychoneuroses as the group in which to place those pathological happenings called Shell-shock? It will do no harm to make this choice if we do it humbly in the spirit of acknowledgment that we know next to nothing about the psychoneuroses. The psychoneuroses should fall on their knees to Shell-shock rather than that Shell-shock make obeisance to the psychoneuroses. For what is a psychoneurosis? It is a functional disease of the nervous system in which the mind plays an important part—it is also probably much else. But the “much else” is as likely to be found in Shell-shock as anywhere else during these particular years.
Should we then consider psychoneuroses as the category for those pathological events known as Shell-shock? It wouldn't hurt to make this decision if we do so with humility, recognizing that we understand very little about psychoneuroses. Psychoneuroses should bow to Shell-shock rather than the other way around. So, what exactly is a psychoneurosis? It's a functional disorder of the nervous system where the mind plays a significant role—it’s likely much more than that. But this “much more” could be just as easily found in Shell-shock as in any other area during these years.
Thus, rehearsing in a broad way the case arrangement of Section B, we find, first, autopsied cases and cases with lumbar[884] puncture data; then cases with prominent admixture of organic phenomena; a few cases to illustrate the victims’ own impressions of their disease; the long toe to top, or “cephalad” series (crural monoplegias and paraplegias, campto-cormias, astasia-abasias, brachial monoplegias, brachial paraplegias, deafmutism, blindness); the series to illustrate the idea of reflex or physiopathic disorders; the series of delayed Shell-shock phenomena; the series to show the picking out by Shell-shock of ante-bellum weak spots and tendencies in the organism; cases touching the hereditary question; peculiar and unique cases; examples of Shell-shock equivalents; and cases of a psychopathic rather than local hystero-traumatic trend.
So, looking broadly at the case arrangement of Section B, we start with the autopsied cases and those with lumbar[884] puncture data. Then we have cases with a notable mix of organic phenomena, a few examples highlighting the patients’ personal impressions of their illness, the long toe to top, or “cephalad” series (which includes crural monoplegias and paraplegias, campto-cormias, astasia-abasias, brachial monoplegias, brachial paraplegias, deaf-mutism, and blindness). There are also series illustrating reflex or physiopathic disorders, as well as the delayed Shell-shock phenomena. We’ll look at how Shell-shock revealed pre-existing weaknesses and tendencies in individuals, cases relevant to the hereditary aspect, some peculiar and unique cases, examples of Shell-shock equivalents, and instances emphasizing a psychopathic rather than purely local hystero-traumatic tendency.
90. At the outset of Section B (Shell-shock: Nature and Causes), we face the question of the possibly organic nature of Shell-shock. It is safe to say that the vast majority of cases of Shell-shock do not die of Shell-shock, and the collection of material from true Shell-shock cases that are killed by accident or intercurrent disease has proved a matter of great difficulty under military conditions. Of course, it is possible to answer the question à priori, by agreeing that any case with structural lesion of whatever sort, is by the same token not a case of Shell-shock.
90. At the beginning of Section B (Shell-shock: Nature and Causes), we encounter the question of whether Shell-shock might have an organic basis. It's safe to say that the vast majority of Shell-shock cases do not die from Shell-shock itself, and gathering information on true Shell-shock cases that are killed accidentally or by other illnesses has proven to be very challenging in military settings. Of course, we can address the question à priori by agreeing that any case with a structural injury of any kind is therefore not classified as Shell-shock.
91. Apparently the most informatory case yet presented is that of Mott (Case 197). In this case, death came in 24 hours, and the immediate cause of death was doubtless a small hemorrhage of the spinal bulb. There was a congestion of veins in the bulb, as well as a congestion of the pia mater over all other parts of the brain. Nor was the bulbar hemorrhage unique, for there were a number of superficial punctate hemorrhages. In short, the brain was not even grossly normal, such as one might desire in a case of true Shell-shock as conceived by à priori workers. Yet, according to Mott, there are microscopic changes of an intimate nature that lie nearer to the microscopic possibilities in true Shell-shock. For example, in the bulb itself there was a distinct and photographable change of nerve cells: the vago-accessorius nucleus had cells in a state of chromatolysis. The internal alterations of these cells, with dissolution of chromatic material, may[885] possibly indeed have been the direct cause of death or an indicator of its direct cause. Here again, to accord full justice to Mott’s contention, we are dealing perhaps more with a phenomenon of the cause of death than with a Shell-shock phenomenon. According to Mott, the Shell-shock symptoms themselves are due to capillary anemia and to nerve cell changes such as he found in various regions. These nerve cell lesions were of the nature of chromatolysis and identical with those of the vago-accessorius nucleus. In this connection, one thinks of the ideas of Crile concerning exhaustion and its effect upon certain nerve cells and other cells, and indeed the whole conception runs back to the early years of discussion of the meaning of chromatin deposits in nerve cells, and to the work on fatigue of such cells. It may well be that Mott’s suggestion is sound, and that changes of the order of chromatolysis are what subtend some, if not most, of the phenomena of Shell-shock. On account of the myriad interconnections of neurones and the remote effects upon normal neurones of disturbances of a microchemical or microphysical nature in a few neurones, it would not do to throw out of court forthwith such a contention as that of Mott by triumphantly pointing to the miracle cures of certain Shell-shock phenomena; for it will not necessarily be the chromatolytic (or otherwise microchemically or physically altered) cells that will be directly responsible for the symptoms in question. Cells whose activity is but temporarily in abeyance (perhaps by phenomena akin to diaschisis) might be reached from an unusual source in the process of “miracle cure,” whereupon the newly opened paths of energy might conceivably remain open. Nevertheless, it cannot be denied that there are considerable stretches of speculation in the thread of this hypothesis.
91. The most informative case so far is that of Mott (Case 197). In this case, death occurred within 24 hours, and the immediate cause was likely a small hemorrhage in the spinal bulb. There was a congestion of veins in the bulb, as well as congestion of the pia mater across other parts of the brain. The bulbar hemorrhage was not alone; there were also several superficial punctate hemorrhages. In short, the brain was not even grossly normal, which one would expect in a true Shell-shock case as theorized by à priori researchers. However, according to Mott, there are intimate microscopic changes that are more aligned with the microscopic possibilities in true Shell-shock. For instance, in the bulb itself, there was a distinct and photographable change in nerve cells: the vago-accessorius nucleus had cells in a state of chromatolysis. The internal changes in these cells, characterized by the breakdown of chromatic material, may[885] actually have been the direct cause of death or at least an indicator of it. To fully appreciate Mott’s argument, we might be looking more at a phenomenon related to the cause of death than a Shell-shock issue. Mott claims that the Shell-shock symptoms themselves result from capillary anemia and changes in nerve cells similar to those he observed in various regions. These nerve cell lesions were of the chromatolysis type, identical to those in the vago-accessorius nucleus. This reminds one of Crile's ideas on exhaustion and its effect on certain nerve cells and others, tying back to early discussions on the meaning of chromatin deposits in nerve cells and research on their fatigue. Mott’s suggestion may indeed be valid, implying that changes like chromatolysis could underlie some, if not most, of the Shell-shock phenomena. Given the vast interconnections of neurons and the distant effects on normal neurons from microchemical or microphysical disturbances in a few neurons, it's premature to dismiss Mott’s argument by pointing to miraculous cures of certain Shell-shock symptoms; it may not necessarily be the chromatolytic (or otherwise microchemically or physically altered) cells that directly cause the symptoms. Cells whose activity is only temporarily suppressed (perhaps from phenomena similar to diaschisis) might reactivate from an unusual source during a "miracle cure," allowing new paths of energy to remain open. Nevertheless, it's undeniable that there's a considerable amount of speculation in this hypothesis.
92. Particularly important is the question, how frequently such hemorrhages as those found by Mott in Case 197 occur. Cases are given in the text which show such hemorrhages.
92. An important question is how often the hemorrhages identified by Mott in Case 197 occur. The text provides cases that illustrate these types of hemorrhages.
Rather often quoted in this relation is Case 201, a case of Sencert, in which a shell exploded one metre away from a soldier and injured him so that he died that night through the bursting of the pleura of both lungs within a thoracic[886] cage which was quite intact. This sort of finding reminds one of cases in which the inner partitions of houses are burst by explosion when the outer walls remain intact. In particular, one thinks of the physical changes within an aneroid barometer, which have been shown to come about when something is exploded near by. If such an event may happen as the bursting of the lungs within an otherwise intact body, so also is there evidence that a similar event occurs in the nervous system. Clinical evidence of this is obtained in the hemorrhage and pleocytosis of spinal fluid obtained early in the clinical examination of certain cases. In fact, in Case 205 (one of Souques), there is a pleocytosis of the fluid as late as a month after shell-shock. When there is no pleocytosis or hemorrhage, there may be a hypertension of the fluid,—a finding sometimes attributed to Dejerine (see, for example, Case 207, of Leriche). It might be inquired whether the fall sustained by the patient as a result of the shell explosion could not be responsible for the hemorrhage, and this may indeed be the fact in certain instances. Babinski has offered in Case 209, an instance in which hematomyelia (with later partial recovery) was produced in a subject who was lying prone in the performance of machine-gun duty (the phenomena in this case were well described by the victim himself, a veterinary student who was six months a captive in Germany). Doubtless, it would not be difficult to produce a complete series of cases with and without trauma to the tissues investing the nervous system, with definite clinical or autopsy evidence of organic lesions of the nervous system, whether by mechanical impact, by the concussion (windage) of the air, or even by the effects of muscular contractions.
Often cited in this context is Case 201, a case involving Sencert, where a shell exploded one meter away from a soldier, injuring him to the point that he died that night due to the rupture of the pleura in both lungs, even though his rib cage was completely intact. This type of finding is reminiscent of cases where the inner walls of houses are blown out by an explosion while the outer walls remain undamaged. Specifically, one thinks of the physical changes that occur within an aneroid barometer when something explodes nearby. If such an event can lead to lung rupture within an otherwise intact body, there’s also evidence to suggest that a similar phenomenon occurs in the nervous system. Clinical evidence of this is reflected in the hemorrhage and pleocytosis of spinal fluid collected early during the clinical examination of certain cases. In fact, in Case 205 (one case from Souques), there was pleocytosis of the fluid even a month after the shell shock. When there is no pleocytosis or hemorrhage, there may still be hypertension of the fluid—a finding sometimes attributed to Dejerine (see, for instance, Case 207, from Leriche). One might wonder if the fall sustained by the patient due to the shell explosion could account for the hemorrhage, and this may indeed be true in some cases. Babinski describes in Case 209 an instance where hematomyelia (with subsequent partial recovery) occurred in a subject who was lying face down while operating a machine gun (the events in this case were well described by the victim himself, a veterinary student who was held captive in Germany for six months). Certainly, it would not be difficult to compile a comprehensive series of cases with and without trauma to the tissues surrounding the nervous system, providing clear clinical or autopsy evidence of organic lesions in the nervous system, whether from mechanical impact, the concussive force of air, or even the effects of muscle contractions.
93. A case of Chavigny’s (Case 198), in which there was an extremely careful autopsy, showed a strongly blood-stained cerebrospinal fluid; in fact, there was an intradural hemorrhage, though of minor degree and possibly not the cause of death; and throughout the brain substance there were slight hemorrhagic points. But there was no sign whatever of fracture of the cranial vault or base. Another case of similar meningeal hemorrhage but sharply localized, was Case 199, an instance of minor explosion in which neither skin nor muscles,[887] bone or viscera showed any lesion; and the death, which occurred in seven days, seemed hardly explicable on the basis of hemorrhage itself. In fact, this case would require the sort of microscopic examination performed by Mott in Case 197 for a proof of the cause of death, which was thought by the reporters themselves (Roussy and Boisseau) to be within the field of histology.
93. A case of Chavigny’s (Case 198) involved a very thorough autopsy that revealed highly blood-stained cerebrospinal fluid; there was indeed an intradural hemorrhage, although it was minor and likely not the cause of death. Throughout the brain tissue, there were small hemorrhagic spots. However, there were no signs of fracture in the skull or base. Another case with similar meningeal hemorrhage, but distinctly localized, was Case 199, which resulted from a minor explosion where neither skin nor muscles, bones, or internal organs showed any damage. The death, which happened seven days later, seemed difficult to explain solely by the hemorrhage. In fact, this case would need the kind of microscopic examination conducted by Mott in Case 197 to determine the cause of death, which the reporters (Roussy and Boisseau) believed fell within the scope of histology.
94. Case 200 seems to bring proof that there may be areas of gross softening within the spinal cord produced by the concussion of the cord from shell-burst, although there had been no fracture of the spine itself and no penetration of splinters of shell or of bone into the spinal canal or the substance of the cord itself. The argument here is that the tissues that lie between the agent of violence and the interior of the spinal cord are affected en bloc by the impact, the resultant gross or molar lesions being several millimetres or centimetres from the point reached by the impinging body or force. How complicated such a situation might be, we may recall from a case previously studied, namely, Case 103 (Lhermitte), wherein a missile struck the left side of the skull and produced lesions beneath its point of impact, but at the same time apparently caused a contre-coup effect upon the opposite hemisphere. That particular case did not come to autopsy, but Lhermitte’s explanation of its queer association of aphasia with ipsilateral hemiplegia seems sound enough. In fine, what with the mechanical trauma to which many victims of shell explosion are subject, what with the findings in sundry autopsies, and what with the determination of hemorrhage in the spinal fluid early after the shock, it might be conceived that the majority of cases of Shell-shock are actually cases of mechanical injury to the brain or spinal cord in which hemorrhage or laceration and overriding of neuronic tissues would be found. Nor would such a hypothesis be prima facie absurd with the evidence afforded by certain cases of Shell-shock having an admixture of reflex phenomena and other symptoms proved by the older neurologists to be beyond peradventure organic. (Compare, for example, such a case as that of Case 210, with herpes zoster and segmentary symptoms.) It should be remembered, however,[888] that Mott in the case cited above (Case 197) sharply distinguishes between the hemorrhages (especially the bulbar hemorrhage which caused death) and the nerve cell chromatolysis which he regarded as possibly at the basis of Shell-shock symptoms. It is decidedly doubtful whether the hypothesis of microscopic or larger hemorrhages, or of local areas of destruction of neurones will suffice for the explanation of true Shell-shock. This is not to say that in the diagnosis of true Shell-shock (that is, roughly speaking, the psychoneurosis), we shall not need to concede and consider in every case the possibility of traumatic focal brain disease. This will always need to be faithfully excluded in all cases unless the initial set-up of symptoms is so suggestive of immediately curable psychoneurosis that without further ado miracle-therapy is undertaken and executed. But in virtually all the slower cases, an exclusion of organic brain and cord disease is undertaken. Admixtures of organic and focal phenomena are quite in the order of everyday occurrence.
94. Case 200 seems to provide evidence that there may be significant softening in certain areas of the spinal cord caused by concussion from shell explosions, even though there was no fracture of the spine itself and no splinters from the shell or bone penetrating the spinal canal or the cord tissue. The argument here is that the tissues between the source of the violence and the spinal cord are affected as a whole by the impact, with the resulting large lesions appearing several millimeters or centimeters away from the point of contact with the impacting object or force. The complexity of such a situation can be illustrated by a previously studied case, namely, Case 103 (Lhermitte), in which a projectile struck the left side of the skull and created lesions directly beneath the impact site, while also seemingly causing a counter-coup effect on the opposite side of the brain. That particular case didn't undergo autopsy, but Lhermitte’s explanation of the unusual combination of aphasia with ipsilateral hemiplegia seems quite plausible. Ultimately, given the mechanical trauma experienced by many victims of shell explosions, along with findings from various autopsies and the discovery of hemorrhage in the spinal fluid shortly after the shock, it could be understood that most cases of Shell-shock are actually instances of mechanical injury to the brain or spinal cord where hemorrhage or laceration and damage to neuronal tissues would be present. This hypothesis isn't prima facie absurd, especially when considering certain cases of Shell-shock that exhibit a mix of reflex phenomena and other symptoms proven by earlier neurologists to be undoubtedly organic. (For instance, compare the case of Case 210, which had herpes zoster and segmental symptoms.) However, it’s important to remember that Mott, in the aforementioned case (Case 197), clearly differentiates between the hemorrhages (particularly the bulbar hemorrhage that caused death) and the nerve cell chromatolysis, which he viewed as possibly underlying Shell-shock symptoms. It remains quite uncertain whether the hypothesis of microscopic or larger hemorrhages, or local areas of neuronal destruction, can adequately explain true Shell-shock. This doesn't imply that in diagnosing true Shell-shock (roughly defined as psychoneurosis), we shouldn't acknowledge and evaluate the possibility of traumatic focal brain disease in every case. This must always be thoroughly ruled out unless the initial symptom setup strongly suggests an immediately treatable psychoneurosis, prompting an urgent implementation of miracle therapy. However, in nearly all slower cases, an assessment to exclude organic brain and spinal cord disease is conducted. Combinations of organic and focal phenomena are quite common.
95. Especially good instances of this co-existence of functional and organic symptoms are found in ear cases; and it may be suspected that when, after the war, all these data can be suitably gathered and compared, it will be from the field of otology that some of the most fruitful hypotheses will be developed. In the cases of Shell-shock deafness, mechanical peripheral factors are admixed with central factors in phenomena admitting in some ways more exact diagnosis than in other fields. We may await the correlation of these data by some worker, equally skilled in otology and neurology, with the profoundest interest. Analogous results may be hoped from a correlation of neurological and ophthalmological conceptions.
95. Some of the best examples of the coexistence of functional and organic symptoms can be found in ear cases. It’s likely that after the war, when all this data can be collected and analyzed, otology will produce some of the most productive theories. In cases of deafness from shell shock, mechanical peripheral factors mix with central factors, allowing for diagnoses that are often more precise than in other areas. We can look forward to a skilled researcher, proficient in both otology and neurology, correlating this data with great interest. Similar outcomes might be expected from linking neurological and ophthalmological concepts.
96. Suffice it to say that the differentiation of organic and functional phenomena has long been possible on the basis of what we know concerning various reflexes (e.g., the Babinski reflex and its congeners); and the net result of this work is that the majority of Shell-shock cases,—that is, cases in which the physical factor shell-shock has entered,—are probably not cases in which a coarse organic disease could be[889] proved to exist, or assumed with any color of likelihood to exist. Even limiting ourselves to cases in which the physical factor shell-shock or some sort of impact with or without an external wound occurred, we shall find cases enough of a truly functional nature, as indicated by their reflexes, to render it quite impossible to assert that they are in the classical sense “organic” cases. Putting these cases with the physical shell-shock factors together with the other large series of cases in which precisely similar symptoms occur without the presence of the physical shell-shock factor, we shall find ourselves convinced that classical Shell-shock phenomena are by and large what is called functional. We shall arrive at the hypothesis that they are cases of hysteria or other form of psychoneurosis, entitled to the diagnosis of traumatic hysteria (or hysterotraumatism, in the sense of Charcot), or not, according to whether the physical factor shell-shock was in evidence. What now underlies the concept functional, as we use it in Charcot’s sense of hysterotraumatism, or in the more modern phrase traumatic hysteria? Do we perhaps mean some microchemical or microphysical change of a reversible nature, similar to that described by Mott, e.g., in Case 197? It is not possible to answer this question at this time.
96. It’s enough to say that we’ve been able to distinguish between organic and functional phenomena for a long time based on what we know about various reflexes (e.g., the Babinski reflex and similar ones); and the outcome of this research is that most cases of shell shock—meaning cases where the physical aspect of shell shock has played a role—likely aren't cases where a serious organic illness can be proven to exist or reasonably assumed to exist. Even if we only consider cases where shell shock or some kind of trauma with or without an external wound occurred, we’ll find enough truly functional cases, as shown by their reflexes, to make it impossible to claim that they are "organic" in the classical sense. By combining these cases with the physical shell shock factors with a large number of other cases displaying similar symptoms without the presence of the physical shell shock factor, we'll be convinced that classical shell shock phenomena are largely functional. We’ll come to the hypothesis that they are instances of hysteria or another form of psychoneurosis, deserving the diagnosis of traumatic hysteria (or hysterotraumatism, in Charcot's terms), or not, depending on whether the physical aspect of shell shock was present. What exactly is meant by the term functional, as we use it in Charcot's sense of hysterotraumatism, or in the more contemporary term traumatic hysteria? Could it refer to some reversible microchemical or microphysical change, similar to what Mott described, e.g., in Case 197? It’s not possible to answer that question at this time.
97. But if we give up the hypothesis of organic disease of the nervous system (that is, the hypothesis of coarse lesions, small or large, conceived to be the direct effect of mechanical impact), can we incriminate any other factor? Chemical factors from the gas of bursting shells may be thought of; yet in abundant cases there is no evidence that these have been in play. They and a variety of other special causes may be found working in a few instances but have nothing to do with the moot question.
97. But if we dismiss the idea of organic disease of the nervous system (meaning, the idea of significant damage, whether small or large, thought to be caused directly by mechanical impact), can we blame any other factor? We might consider chemical factors from the gas of exploding shells; however, in many cases, there is no proof that these were involved. They, along with various other specific causes, may appear in a few instances but have nothing to do with the debated issue.
98. Upon giving up the organic hypothesis, the modern functionalist is very apt to run directly into the embrace of hysteria. If a thing is not physical, it must be psychical in its genesis, so runs the argument. What, after all, is a neurosis? We mean ordinarily by neurosis, something functional rather than structural. We often mean something psychical rather than peripheral. Accordingly, as we have seen, many[890] writers rush to the hypothesis that Shell-shock effects, except in a few unusual instances of organic disease, are functional; and not only are they functional but psychic, and maintained by some of the so-called “mechanisms” which abound in modern speculative writing.
98. When giving up the organic hypothesis, the modern functionalist often quickly resorts to hysteria. The argument goes that if something isn't physical, it must originate from the mind. So, what exactly is a neurosis? We usually refer to neurosis as something functional rather than structural. We often mean it's something psychological rather than peripheral. As we've seen, many[890] writers jump to the conclusion that the effects of Shell shock, except for a few rare cases of physical disease, are functional; and not only are they functional but also psychological, sustained by some of the so-called “mechanisms” that are prevalent in contemporary speculative writing.
99. Case 253, a case of Tinel, may serve to illustrate this point. Tinel’s patient was not subject to shell-shock at all, but was wounded in the arm. Three weeks later, he was able to flex his forearm only by means of the supinator longus. It was found that the biceps was soft and flaccid, though the electrical reactions of the biceps were normal. Now, since flexion of the forearm is normally produced by a synergic contraction of the biceps and supinator longus, the situation in Tinel’s case was striking in that the functions of the biceps and supinator longus had been separated out by a process which could not be hysterica. The hypothesis is that in hysteria it has always been found impossible to split the synergic action of these two muscles. What has happened? In Tinel’s picturesque phrase, the biceps muscle has been stupefied by a process which involved no destruction of a nerve trunk or any important nerve elements. This process of stupefaction passed away with a few weeks’ massage and rhythmic faradism. But what is this process of stupefaction, as Tinel calls it? No definite answer can be given. But is not the process analogous to what may happen in a variety of cases of shell explosion in which, for one reason or another, sundry neurones are, as it were, stupefied, stunned, anesthetized, or thrown out of gear by some internal physico-chemical readjustment of unknown nature? Perhaps that readjustment, though in Tinel’s case it probably took place within the tissues of the arm itself, is analogous to the chromatolytic process in nerve-cell bodies suspected by Mott to be at the bottom of certain Shell-shock symptoms as in Case 197.
99. Case 253, a case described by Tinel, illustrates this point. Tinel’s patient didn’t suffer from shell shock at all but was injured in the arm. Three weeks later, he could only flex his forearm using the supinator longus. It was found that the biceps was soft and weak, even though the electrical reactions of the biceps were normal. Normally, flexion of the forearm is caused by a coordinated contraction of the biceps and supinator longus. In Tinel’s case, it was notable that the functions of the biceps and supinator longus had been divided by a process that could not be hysterical. The hypothesis is that, in hysteria, it has always been impossible to separate the synergistic action of these two muscles. What happened? In Tinel’s vivid description, the biceps muscle has been stupefied by a process that involved no damage to a nerve trunk or any significant nerve elements. This process of stupefaction faded away after a few weeks of massage and rhythmic faradism. But what is this process of stupefaction, as Tinel puts it? No clear answer can be provided. Yet, isn’t this process similar to what might occur in various cases of shell explosion where, for different reasons, certain neurons are metaphorically stupefied, stunned, anesthetized, or disrupted by some internal physical-chemical adjustment of an unknown nature? Perhaps that adjustment, although in Tinel’s case likely occurred within the tissues of the arm itself, is comparable to the chromatolytic process in nerve-cell bodies that Mott suspected to be involved in certain shell-shock symptoms as seen in Case 197.
100. Are there, then, phenomena of peripheral nerve shock analogous to the phenomena of spinal cord and brain shock which we find in so many cases? But if so, it is clearly unnecessary, and indeed injurious for us to conceive that cases proved not to be organic must necessarily be hysterical.[891] Several authors have called a halt upon this undue extension of the concept of hysteria to include all the non-organic phenomena. Take, for example, the case of the Victoria Cross winner (Case 529), reported by Eder, in which a contracture was shown by hypnosis to be a representation of the patient’s clutch upon his bayonet (he had been at Gallipoli and was wounded in fourteen places during a bayonet fight with Turks). It would not be possible—in fact, it would seem almost impolite—to refuse to entertain the hypothesis of a kind of symbolism in the bayonet-clutch contracture of Eder’s case; but it would, on the contrary, be far from exact to consider all cases of contracture to be even probably or possibly symbolic in the manner of the bayonet-clutch. There are, many workers feel, many functional phenomena that are non-hysterical, and as it were infra-hysterical in the sense that the “mechanisms” (to use that over-worked term) are in neurones below the level of complexity required by hysteria. This theoretical possibility (that the functional should be divided into the psychical and the infrapsychical) has been given a new status by the work of Babinski and his associates. That work seems to show that the older doctrines of Charcot concerning the existence of “reflex” disorders, are perfectly sound.
100. Are there, then, instances of peripheral nerve shock similar to the spinal cord and brain shock phenomena we see in many cases? If that's the case, it’s clearly unnecessary—and even harmful—to assume that instances which are proven not to be organic must automatically be hysterical.[891] Several authors have called for an end to this excessive extension of the hysteria concept to encompass all non-organic phenomena. Take, for example, the case of the Victoria Cross winner (Case 529), reported by Eder, where a contracture was revealed through hypnosis to be a reflection of the patient’s grip on his bayonet (he had fought at Gallipoli and sustained wounds in fourteen places during a bayonet fight with the Turks). It wouldn’t be possible—and it might seem rather rude—to disregard the idea of a kind of symbolism in the bayonet-clutch contracture from Eder’s case; however, it would be quite inaccurate to assume that all contracture cases are likely or possibly symbolic in the same way as the bayonet-clutch. Many professionals believe there are numerous functional phenomena that are non-hysterical and, in a sense, infrapsychical, indicating that the “mechanisms” (to use that overused term) are present in neurons below the level of complexity needed for hysteria. This theoretical possibility—that functional issues could be divided into the psychological and infrapsychological—has gained new relevance thanks to the work of Babinski and his colleagues. Their research seems to support the older views of Charcot concerning the existence of “reflex” disorders, demonstrating that they are indeed valid.
101. Babinski has been able to bring into the light of observation the morbid operation of certain of these reflex arcs. Even in cases where in the waking life the central nervous system is able to overpower the reflex arcs in question and permit the limb or limbs to work reasonably well and smoothly, the process of chloroform anesthesia will quickly bring out an odd and unsuspected interior situation. The chloroform suspends the operation of numerous neurones, including those that have to do with the downflow of cerebral inhibitions, those silent streams of impulse that serve to keep the knee-jerks, for example, in leash. Now at a time when all the other muscles of the body are relaxed, the withdrawal of the cerebral inhibitions by chloroform anesthesia may cause a phenomenon to appear in certain reflex arcs that argues an excess of activity; thus in the leg, for example, an ankle-clonus, or a patella-clonus, or a degree of contracture,[892] may be brought about early in chloroform anesthesia, though there had been little or no suspicion of such a tendency in the waking life. The cerebral inhibitions in the waking life have been enough to dampen the ardor of the reflex arc in question. It must be remarked that these cases of reflex, or, as Babinski termed them, physiopathic disorders, as a rule occur in cases locally wounded. It is the locally wounded limb that develops functional excess of contained reflex arcs. Does this occur by a process of neuritis, or by some other unknown process? Whatever the answer to this question, Babinski and his associates appear to have shown the existence of a group of physiopathic or reflex disorders; disorders below the level of the psyche and below the theatre of operations of hysteria.
101. Babinski has been able to highlight the abnormal functioning of certain reflex arcs. Even in cases where the central nervous system can control these reflex arcs and allow the limb or limbs to move appropriately and smoothly in everyday life, chloroform anesthesia quickly reveals an unusual and hidden internal condition. The chloroform halts the activity of many neurons, including those related to the transmission of cerebral inhibitions, which are the silent pathways of impulses that help keep knee-jerks in check, for example. Now, when all the other muscles in the body are relaxed, the removal of cerebral inhibitions due to chloroform anesthesia may trigger an observable phenomenon in certain reflex arcs, indicating an overactivity; for instance, in the leg, this could manifest as ankle clonus, patellar clonus, or a degree of stiffness, potentially occurring early in chloroform anesthesia, even though there was little or no indication of such a tendency while awake. The cerebral inhibitions in waking life have been sufficient to suppress the activity of the relevant reflex arc. It should be noted that these cases of reflex, or as Babinski called them, physiopathic disorders, typically happen in cases of local injury. It is the injured limb that shows an excess of functional activity in these reflex arcs. Is this due to neuritis, or some other unknown process? Whatever the answer might be, Babinski and his colleagues seem to have demonstrated the presence of a group of physiopathic or reflex disorders; disorders operating beneath the level of consciousness and outside the realm of hysteria.[892]
102. Practically speaking, also, it is important not to consider every functional situation hysterical, since the non-hysterical functional changes may be extremely obstinate to treatment. Both physician and patient suffer if the patient is treated along psychotherapeutic lines for hysterical symptoms, some of which turn out on investigation to be functional enough but non-psychic. The peculiar configuration of symptoms shown in cases with the physical shell-shock or its equivalent, is perhaps dependent upon what neurones are locally affected. If there has been good evidence of near-by explosion or of wound, it will be especially important to learn just what parts of the nervous system and just what synergic neurones and other structures were affected. Whether the process within these neurones be one analogous to the dissolution of chromatin, or whether the process is more like one of narcosis, or narcosis and stupefaction, or whether the process is more like that of a stun, or like the plight of the nerves in a foot for a long time “asleep,” it may be impossible to say; but it is entirely unnecessary to soar directly to the higher mental process, unnecessary in short, to assume a hysterical dissociation when the dissociation may be far lower down in the nervous system.
102. Practically speaking, it's also important not to label every functional situation as hysterical, since non-hysterical functional changes can be really tough to treat. Both the doctor and the patient can struggle if the patient is treated with psychotherapeutic methods for hysterical symptoms, some of which, upon investigation, turn out to be functional but not psychological. The unique pattern of symptoms seen in cases of physical shell shock or its equivalent may depend on which neurons are affected. If there’s compelling evidence of a nearby explosion or wound, it becomes especially crucial to determine which parts of the nervous system and which synergistic neurons and other structures were impacted. Whether the process occurring within these neurons is similar to the breakdown of chromatin, or more like narcosis, or a combination of narcosis and stupor, or resembles a stun, or is akin to how a foot feels after being "asleep" for a long time, may be hard to determine; however, it’s completely unnecessary to immediately jump to higher mental processes, or to assume a hysterical dissociation when the dissociation may actually occur much lower in the nervous system.
Treating Shell-Shock Neuroses
103. We have pictured the practical situation in which the neuroses of the war find themselves—a situation bristling with diagnostic difficulties. The great proposition deducible therefrom is,
103. We have illustrated the practical situation in which the war-related neuroses exist—a scenario filled with diagnostic challenges. The key takeaway from this is,
The diagnostic problem in Shell-shock is the diagnostic problem of neuropsychiatry at large.
The diagnostic issue in Shell shock is the diagnostic issue of neuropsychiatry overall.
The neuroses of war have this in common with the neuroses of peace—that they need to be distinguished from all other nervous and mental diseases. One cannot be a specialist in Shell-shock unless one is a neuropsychiatric specialist; even the neuropsychiatrist has much to learn from the internist, the orthopedist, the neurosurgeon, as well as from the psychologist.
The psychological issues from war have this in common with those from peace—they need to be separated from all other nervous and mental illnesses. You can't be an expert in Shell shock unless you're a neuropsychiatric specialist; even the neuropsychiatrist still has a lot to learn from the internist, the orthopedist, the neurosurgeon, and the psychologist.
But however wide the diagnostic field for Shell-shock, the therapeutic field is wider still. For the neuropsychiatric reconstructionist has to face the peculiarities of the military status of his ward, the difficulties of demobilization into civilian life (a canal system with very precise technic for the opening and closing of locks), the choice and timing of the proper measures of bedside occupation, of occupation therapy in a broader sense, of prevocational and vocational training—the whole complicated by the character changes that may have set in to bowl over all one’s preconceptions. The nub of the matter, after the era of the manière forte, the brusque psychotherapy, the rough jarring of the man back into approximate normality is, perhaps, this potentiality of subtle character changes defying possibly anybody’s analysis, but stimulating us all to our best endeavor, whether we are physicians, psychologists, occupation-workers, social workers, or nurses. Now that all sorts of reconstruction programs are in the air, each claiming its share, or more than its share, of attention, let us not forget that no one can stake out in any small plot the measures of refitting, readjustment, readaptation, rehabilitation—all these terms with slightly differing denotation have been used—especially when we take into account that not only must the patient be refitted to his entourage,[894] but also not seldom the entourage to its returned Shell-shocker.
But no matter how broad the diagnostic field for Shell shock is, the therapeutic field is even broader. The neuropsychiatric therapist has to deal with the unique challenges of the military background of their patient, the difficulties of transitioning back to civilian life (like a canal system with specific techniques for opening and closing locks), the selection and timing of appropriate bedside activities, broader occupational therapy, and vocational training— all complicated by the personality changes that may have occurred, which can challenge all preconceived notions. The core issue, after the era of the manière forte, the harsh psychotherapy, and the jarring return to near-normalcy, is perhaps this potential for subtle personality changes that might resist anyone’s full analysis, while pushing all of us—physicians, psychologists, occupational therapists, social workers, or nurses—to do our best. With various reconstruction programs emerging, each trying to claim attention, we must remember that no one can limit the measures of refitting, readjustment, readaptation, rehabilitation—all these terms with slightly different meanings—especially considering that not only must the patient be readapted to their environment,[894] but often the environment must also adjust to the returning Shell shock survivor.
104. It is proper to place these general considerations first because the slow, patient, prosaic measures of reëducation are apt to be forgotten in our enthusiasm for the lightning-like cures of the hypnotic, the psychoelectric, the pseudo-operative, and other psychotherapeutic forms. Psychotherapy in all its forms has come into its own in Shell-shock. Miracles or their equivalents are daily wrought by men who are not prophets. Lourdes and Christian Science have their unassuming rivals. Let us remember, however, that even Lourdes and Christian Science never solved 100% of the problems placed before them, even though the votaries have the best will in the world to be cured. If the will itself is disordered, what can be done save investigate? And the mauvaise volonté is by no means absent from some of our prospective patients; witness one man, a Frenchman, who so resented being cured by torpillage, i.e., by the electric brush, that he carried his case against Clovis Vincent, who cured him of his hysteria, clear to the Academy! And, even after we have cured our cases by these modern miracles, let us not be too proud of ourselves! One soldier sent back to Australia, hysterically mute for months, got his voice back after killing a snake—a peculiar instance of occupation-therapy, not enumerated in courses on reconstruction. And remember the man who jumped the wall and got drunk, breaking back into the hospital to show his doctor how his refractory voice had at last come back. Thus there are cures and cures (even a newspaper cure of mutism by a moving picture vision of the antics of Charlie Chaplin), and spontaneous non-medical cures as well as medical ones, and slow cures due to vis medicatrix, as well as to shrewd reëducation measures.
104. It's important to address these general ideas first because the slow, careful, straightforward methods of reeducation tend to be overlooked in our excitement for the quick fixes offered by hypnosis, electric therapies, pseudo-surgery, and other forms of psychotherapy. Psychotherapy in all its varieties has taken center stage in dealing with shell shock. Miracles, or something akin to them, are performed daily by people who aren’t necessarily experts. Lourdes and Christian Science have their humble competitors. However, let’s keep in mind that even Lourdes and Christian Science never resolved 100% of the issues presented to them, despite the sincere intentions of those seeking healing. If the will itself is disordered, what can we do except investigate? And there is certainly some mauvaise volonté among some of our potential patients; for instance, there was a Frenchman who was so upset about being treated with torpillage, meaning the electric brush, that he took his complaint against Clovis Vincent, who cured him of his hysteria, all the way to the Academy! Moreover, even after we use these modern miracles to treat our cases, we shouldn’t be too self-satisfied! One soldier, sent back to Australia after being hysterically mute for months, regained his voice after he killed a snake—a unique example of occupation therapy not covered in rehabilitation courses. And don’t forget the man who jumped over the wall and got drunk, only to break back into the hospital to show his doctor how his stubborn voice had finally returned. There are different types of cures (including a newspaper cure for mutism triggered by watching Charlie Chaplin’s antics), along with spontaneous non-medical cures as well as medical ones, and slow recoveries due to vis medicatrix, as well as clever reeducation strategies.
105. I shall not attempt to cover systematically the topic of Shell-shock therapy in this epicrisis. The reader must go through the treated cases, especially in Section D but passim elsewhere, if he is to obtain a proper conception of all the methods so far employed—and at the end he cannot know the ultimate outcome of the cases. Patrons of the miracle[895] cures and the manière forte are having their day: on the whole, the law of sudden onset, sudden ending has much to say for itself in the hysterical (pithiatic) group. Forebodings of relapse in these torpedoed cases may indeed have some foundation: but figures are yet lacking, and relapses may be as expectantly predicted in the slow-onset, slow-cure group. The decision must be post-bellum. Nor must the fact that a few absolutely normal subjects have succumbed de novo to Shell-shock blind us to the fact that, statistically speaking, most cases are ab ovo psychopaths in whom relapses, recurrences, or new instances of neurosis may be confidently expected. For these ab ovo psychopaths, what can suffice but (a) removal of the disease by the vis medicatrix naturae; or (b) reëducation, intellectual or (c) moral (as the case may be); or else (d) some plan of environmental shielding from new occasions of disease?
105. I won’t try to systematically cover the topic of Shell-shock therapy in this summary. The reader needs to go through the cases discussed, especially in Section D but passim elsewhere, if they want to grasp all the methods that have been used so far—and even then, they won't know the final outcome of the cases. Supporters of miracle[895] cures and the manière forte are having their moment: overall, the principle of sudden onset, sudden ending has a lot of validity within the hysterical (pithiatic) group. Concerns about relapse in these torpedoed cases may indeed have some basis: but we still lack concrete data, and relapses might be just as predictably found in the slow-onset, slow-cure group. The decision must be made after the war. We also shouldn't let the fact that a few completely normal individuals have fallen de novo to Shell-shock distract us from the reality that, statistically speaking, most cases involve ab ovo psychopaths where relapses, recurrences, or new neuroses can be confidently expected. For these ab ovo psychopaths, what can be enough but (a) the removal of the disease by the vis medicatrix naturae; or (b) re-education, whether intellectual or (c) moral (depending on the individual); or else (d) some strategy for protecting them from new sources of illness?
106. I shall content myself with a brief survey (insisting that the details be read of at least the leading cases in each treatment subgroup) of the cases offered in Section D (Shell-shock: Treatment and Results), consisting of 117 cases (Cases 473-589). The cases are in general arranged with the spontaneous and quasi-natural cures at the outset,—a series of 11 cases (Cases 473-483). The remainder of the section deals with cures under medical conditions, although many cases naturally show an interplay of non-medical factors in the cure or persistence of one or more symptoms.
106. I will stick to a brief overview (emphasizing that the details should be read for at least the main cases in each treatment group) of the cases presented in Section D (Shell-shock: Treatment and Results), which includes 117 cases (Cases 473-589). The cases are generally organized with the spontaneous and quasi-natural cures first—a series of 11 cases (Cases 473-483). The rest of the section focuses on cures under medical conditions, although many cases naturally reveal a mix of non-medical factors in the cure or the persistence of one or more symptoms.
A few cases illustrative of the physical value of hydrotherapy, mechanical therapy, and drugs are given in a short series (Cases 484-489). A treatment of hysterical contractures by induced fatigue is dealt with in Cases 489-493; and the occasional value of surgery is shown by Case 494.
A few examples that highlight the physical benefits of hydrotherapy, mechanical therapy, and medications are presented in a brief series (Cases 484-489). The treatment of hysterical contractures through induced fatigue is discussed in Cases 489-493; and the occasional benefits of surgery are illustrated by Case 494.
The simpler methods of persuasion and explanation follow in a series of 19 cases (Cases 495-513).
The simpler methods of persuasion and explanation follow in a series of 19 cases (Cases 495-513).
Pseudo-operations and suggestive operative manipulation of avail in the treatment of certain local hysterical phenomena are considered in a series of eight cases (Cases 514-521). The comparatively long hypnotic series follows: 27 cases (Cases 522-548). The above-mentioned cures by pseudo-operation and by hypnosis may be classified with those that follow, i.e.,[896] mainly rapid cures by psychoelectric methods and by suggestion on emergence from anesthesia (Cases 549-574), as modern miracles. These cases of modern miracle are followed by a briefer set of reëducative cases (Cases 575-589).
Pseudo-operations and suggestive operative manipulation useful in treating certain local hysterical phenomena are discussed in a series of eight cases (Cases 514-521). The relatively long hypnotic series follows: 27 cases (Cases 522-548). The previously mentioned cures through pseudo-operation and hypnosis can be categorized along with those that follow, i.e.,[896] primarily rapid cures by psychoelectric methods and by suggestion on awakening from anesthesia (Cases 549-574), regarded as modern miracles. These cases of modern miracles are succeeded by a shorter set of reëducative cases (Cases 575-589).
Throughout the treatment section are scattered instances in which, not a cure, but merely a modification or even a persistence of symptoms was the outcome. It is useful to bear in mind, while reading cases in the etiological and diagnostic sections, these main divisions of treatment into what might be called (1) spontaneous, (2) rapid (or “miraculous”) and (3) slow or reëducative.
Throughout the treatment section, there are several instances where the outcome was not a cure, but simply a change or even a continuation of symptoms. It's helpful to keep in mind, while reading through the cases in the etiological and diagnostic sections, these main categories of treatment that could be called (1) spontaneous, (2) rapid (or “miraculous”), and (3) slow or re-educative.
107. It is beyond the scope of this book to deal systematically with the hospital and administrative side of these questions. Especially the zone question is of practical importance, that is, the question of arrangements at the front, on evacuation lines, and in the interior. Roussy and Lhermitte have particularly discussed these matters.
107. This book doesn't aim to systematically cover the hospital and administrative aspects of these issues. The zone question, in particular, is practically important, meaning the arrangements at the front, along evacuation routes, and within the interior. Roussy and Lhermitte have especially addressed these topics.
After thirty months’ experience in the psychiatric centers of two armies, Damaye suggested an organization of psychiatric centers in two parts,—First, a service draining patients from the firing line, rapidly give them first care and evacuate them, in charge of special attendants, to: Second, a psychiatric or neurological center in the communication zone (étapes) without danger of bombardment and at a distance from the guns. The more serious cases will then be evacuated, thirdly, into the interior from these centers along communication lines. But most will have gotten well at the front.
After thirty months of working in the psychiatric centers of two armies, Damaye proposed a structure for psychiatric centers in two parts: First, a service that would quickly remove patients from the firing line, provide them with immediate care, and transport them with the help of special attendants to: Second, a psychiatric or neurological center in the communication zone (étapes) that is safe from bombings and away from the artillery. The more serious cases will then be moved, thirdly, to the interior from these centers along communication lines. However, most patients will have recovered by the time they reach the rear.
108. By orthopedists and mechanotherapeutists too much stress may indeed be laid on non-psychiatric measures, as Duprat hints. Yet perhaps neuropsychiatrists may need as much coaching in the opposite direction. One must remember the non-psychopathic fraction of these Shell-shock disorders and their need of diathermy (Babinski). Duprat says that the centers for physiotherapy cannot effectively do the work of all Shell-shock therapy, as the physiotherapists have their aims fixed on nerves and muscles rather than the mind. Each case requiring psychotherapy ought to be studied in an experimental psychological laboratory from a number of points of view such as mechano-motor capacity, the sensibility, emotional and intellectual sides, memory, impulses and the like. Testing apparatus should be available together with dynamometers, sphygmometers, chronoscopes, ergographs, pneumographs, cardiographs and recording apparatus.
108. Orthopedists and mechanotherapeutists often put too much emphasis on non-psychiatric measures, as Duprat points out. However, neuropsychiatrists might need just as much guidance in the opposite direction. It's important to keep in mind the non-psychopathic aspects of these Shell-shock disorders and their need for diathermy (Babinski). Duprat notes that physiotherapy centers can't effectively handle all Shell-shock therapy since physiotherapists focus more on nerves and muscles than on the mind. Each case that requires psychotherapy should be examined in an experimental psychological laboratory from multiple angles, like mechano-motor skills, sensitivity, emotional and intellectual aspects, memory, impulses, and more. Testing equipment should include dynamometers, sphygmometers, chronoscopes, ergographs, pneumographs, cardiographs, and recording devices.
Chart 19
PSYCHOELECTRIC AND REËDUCATIVE TREATMENT
| Stage | I. | PERSUASIVE TALK IN CONSULTING ROOM |
| Stage | II. | ISOLATION, REST IN BED, MILK DIET (a few days) |
| Stage | III. | FARADIZATION |
| Stage | IV. | REËDUCATION (Physiotherapy and Psychotherapy) |
| Stage | V. | AFTER-CARE |
Curing a psychoneuropath means victory in a moral battle!
Curing a mental illness means winning a moral struggle!
After Roussy and Lhermitte
After Roussy and Lhermitte
Chart 20
TREATMENT FOR INVETERATE HYSTERICS
| Stage | I. | “TORPILLAGE” AND INTENSIVE REËDUCATION |
| Stage | II. | FIXATION OF PROGRESS BY EXERCISES |
| Phase | III. | PROLONGED SPECIAL TRAINING |
After Clovis Vincent
After Clovis Vincent
Specialists for consultation should be available, including ophthalmologists, otologists, laryngologists and electrical specialists. The tests over, the patient should be examined as it were, in a free state and his habits and character noted. Hypnosis may be tried but it should not be prolonged. Psychic contagion is to be avoided especially in the case of subjects with epileptoid crises.
Specialists for consultation should be available, including ophthalmologists, ear specialists, throat specialists, and electrical experts. Once the tests are complete, the patient should be examined, so to speak, in an unrestricted state, and their habits and character should be observed. Hypnosis can be attempted, but it should not be extended. Psychic contagion should be avoided, especially in cases involving individuals with epileptoid seizures.
It would be well to establish for the cases regarded as susceptible to psychotherapy, reëducation centers like those for the re-adaptation of the tuberculous. The improved tuberculous are sent to health centers under the Ministry of the Interior for three months at the maximum and emerge much better able to support the exigencies of life. According to Duprat, there ought to be psychotherapy centers which should not in any sense recall asylums for the insane. Set in the country but not far from the city, managed by the psychological physicians and “médecins psychologues, plus éducateurs que médecins.” The personnel should consist of students going into psychiatry and of teachers whose pedagogical practice ought to enable them to second the efforts of the psychiatrists. In this way we might avoid the perpetuation of some of the psychopathies of war.
It would be beneficial to create centers for cases considered amenable to psychotherapy, re-education centers similar to those for the rehabilitation of tuberculosis patients. Improved tuberculosis patients are sent to health centers run by the Ministry of the Interior for up to three months and come out much better equipped to handle life's demands. According to Duprat, there should be psychotherapy centers that don’t resemble asylums for the mentally ill in any way. These centers would be located in the countryside, but not too far from the city, managed by psychological doctors and “psychologists more as educators than as doctors.” The staff should include students training in psychiatry and teachers whose educational experience would support the efforts of the psychiatrists. This approach could help prevent the continuation of some war-related mental health issues.
109. Possibly “putting forward the best foot” may yield a wrong impression of the proportion of what I have termed “miracle cures.” Other devices of a slower nature are mentioned throughout the book. Perhaps much depends on the temperament of the psychotherapeutist, as e.g., Laignel-Lavastine has remarked about the method of psychotherapy by means of conversation: that one might easily remain in a honeymoon state in military psychotherapy. When hundreds and thousands of functional nervous cases pass through one’s hands it is necessary to remember that behind the conversation there stands the imposing finger of material force.
109. Perhaps saying “putting your best foot forward” may give the wrong impression about the extent of what I’ve called “miracle cures.” Other, more gradual methods are mentioned throughout the book. A lot might depend on the therapist’s personality, as e.g., Laignel-Lavastine pointed out regarding the method of psychotherapy through conversation: that one might easily stay in a honeymoon phase in military psychotherapy. When countless functional nervous cases come through your hands, it’s important to remember that behind the conversation lies the significant influence of material force.
Compare the work of Clovis Vincent, Yealland, Kaufmann.
Compare the work of Clovis Vincent, Yealland, and Kaufmann.
110. On the other hand, Rows points out that shock is a term that does not explain at all adequately the great variety of mental illnesses occurring in the soldiers at the front. The term is popularly used for cases which recover quickly, but in the majority of cases there is a residuum after the shock has disappeared. Accordingly Rows’ work has dealt chiefly with underlying causes, conditions, and factors. Here we may consider
110. On the other hand, Rows emphasizes that "shock" doesn't really capture the wide range of mental illnesses affecting soldiers at the front. People often use the term for cases that heal quickly, but in most cases, there’s still something left behind after the shock wears off. Therefore, Rows' work has mainly focused on the deeper causes, conditions, and factors. Here we may consider
(a) The war strain before breakdown;
The war stress before collapse;
(b) Special causes of shock, such as death of comrades near by, near-by shell explosions and blowing up of trenches;
(b) Special causes of shock, like the death of nearby comrades, explosions from nearby shells, and the destruction of trenches;
(c) Fatigue and exhaustion with lowered capacity of resistance.
(c) Tiredness and burnout with decreased ability to resist.
The men themselves find that they have
The men themselves find that they have
(d) undergone a change of character, having become irascible, unable to sustain interest and attention; solitary and morose, and less capable of self-control. Anxiety, worry and a state of morbid expectancy set in. Everyday trifles are exaggerated.
(d) undergone a change of character, becoming irritable, unable to maintain interest and focus; lonely and gloomy, and less able to control oneself. Anxiety, worry, and a sense of constant unease take over. Everyday annoyances become overblown.
But below these cases are still deeper ones, such as
But beneath these cases are even deeper ones, such as
(e) revival of horrible memories and terrifying dreams of war scenes, together with memories of incidents of past life.
(e) revival of awful memories and frightening dreams about war scenes, along with memories of past experiences.
(Rows attributes to Dejerine the idea that the cause of all cases of hysteria and neurasthenia must be sought in antecedent emotion.)
(Rows attributes to Dejerine the idea that the cause of all cases of hysteria and neurasthenia must be sought in antecedent emotion.)
Emotion compels attention, and to such a degree in some cases that the memories and attendant fears and anxieties cannot be expelled. Hallucinations and delusions may then develop. The patient is largely incapable of reasoning about his status; he lacks[901] “insight into the nature and mode of origin of his mental illness. This insight can be provided by explaining to him in plain language the mechanism of simple mental processes, by enabling him to understand that every incident is accompanied by its own special emotional state, and that this emotional state can be re-awakened by the revival of the incident in memory.” The patient and the physician now “begin to realize that they have some ground in common.… The mystery of the illness will be swept away and the physician will be able to … show him how he can educate himself to regain that which was lost.” “The patient can be induced to face the trouble.” “The excessive emotional tone will thus be stripped away and the patient will thus become able to appreciate the real value of the incident.” “The reëducation must vary with each case in order to overcome the difficulties connected with the specific cause which has been discovered.”
Emotion draws attention, sometimes so intensely that memories and the related fears and anxieties can't be pushed away. This can lead to hallucinations and delusions. The patient often struggles to think logically about their situation; they lack[901] "insight into the nature and origin of their mental illness. This insight can be gained by explaining to them in straightforward terms how basic mental processes work, helping them understand that every event comes with its own specific emotional response, and that this emotional response can be triggered again by recalling the event." The patient and the doctor will now "start to see that they have some common ground.… The mystery of the illness will be cleared up, and the doctor will be able to … show the patient how to train themselves to reclaim what was lost." "The patient can be encouraged to confront the issues." "The overwhelming emotional intensity will be removed, allowing the patient to better recognize the true significance of the event." "The retraining must adapt to each individual case to address the challenges linked to the particular cause that has been identified."
Rows’ work has been done at the Red Cross Hospital at Maghull, and several of the Maghull cases have been reported in Elliot Smith and T. H. Pear’s book on Shell-shock. A somewhat similar point of view has been maintained by Wm. Brown, who has suggested the neat term autognosis for psychoanalysis. W. A. Turner speaks of the Maghull point of view as one of modified psychoanalysis.
Rows’ work has been conducted at the Red Cross Hospital in Maghull, and several cases from Maghull have been documented in Elliot Smith and T. H. Pear’s book on shell shock. A somewhat similar perspective has been put forth by Wm. Brown, who has coined the term autognosis for psychoanalysis. W. A. Turner refers to the Maghull perspective as a type of modified psychoanalysis.
111. Or again a species of combination of the manière forte and the manière douce (operations, shall we say with William James, of the “tough-minded” and the “tender-minded” respectively?) may be used as in the formula
111. Alternatively, a mix of the manière forte and the manière douce (operations, let's say with William James, of the “tough-minded” and the “tender-minded” respectively?) might be employed as in the formula
SYMPATHY + FIRMNESS (Mott).
Sympathy and firmness (Mott).
112. More special devices, suggesting faintly the methods of animal training, may be used, as described in the following account of a new isolation and psychotherapeutic service established in May, 1915, at the Salpêtrière for soldiers with functional nervous diseases. The basic idea has long been held by Dejerine,—the avoidance of heterosuggestion by other patients, imitation, ill effects of visits from members of the family. The functional additions that come from near-by organic patients are among the disadvantages of the ordinary treatment. The isolation service of the neurological center is composed of 34 beds, arranged in two halls, with three extra rooms. Each bed is isolated. The régime in one of the rooms is more rigorous than in the other, and it is an advance for a patient to be moved from the first to the second room. The patient on wakening has no right to leave his box or communicate[902] with his neighbors. He leaves only to be treated by hydrotherapy or electrotherapy. He takes his meals in isolation, receives no calls, and has no leave to go out. The physician sees the patient twice a day and carries on psychotherapy and motor reëducation, as well as special treatments.
112. More specialized techniques, somewhat resembling methods used in animal training, may be applied, as described in the following account of a new isolation and psychotherapeutic service initiated in May 1915 at the Salpêtrière for soldiers suffering from functional nervous disorders. The central concept, long advocated by Dejerine, is to avoid heterosuggestion from other patients, imitation, and negative effects from visits by family members. The functional complications that arise from nearby organic patients are some of the drawbacks of conventional treatment. The isolation service at the neurological center consists of 34 beds arranged in two halls, along with three additional rooms. Each bed is isolated. The regimen in one of the rooms is more stringent than in the other, and it is considered an improvement for a patient to be transferred from the first room to the second. Upon waking, the patient is not allowed to leave their space or interact with neighboring patients. They only leave for hydrotherapy or electrotherapy treatments. Meals are taken in isolation, no visitors are permitted, and they are not allowed to go outside. The physician examines the patient twice a day and conducts psychotherapy, motor reeducation, and specific treatments.
Women nurses care for the patients. A system of control and of progressive rewards has been installed, being a sort of metric evaluation of the process of cure. As the cure proceeds the patient’s lot is progressively mitigated, or if he gets worse the regime is clamped down. Suppose a man a victim of paralysis of leg—the height to which he can lift his leg is measured in centimeters daily as well as the time during which he can hold the leg in air; or, the progress of an ankle, or of the forearm or the arm in a case of arm contracture, is measured. The grade obtained by our scholar in psychotherapy is inscribed upon a slate. Finally, walks, concerts, visits and eventually permission to go out into the town are granted.
Women nurses care for the patients. A control system and a system of progressive rewards have been set up, acting as a sort of metric evaluation for the healing process. As the healing progresses, the patient's situation gradually improves, or if their condition worsens, the restrictions are tightened. For example, if a man is suffering from leg paralysis, the height to which he can lift his leg is measured in centimeters daily, along with the time he can hold it in the air; similarly, the progress of an ankle or the forearm/arm in cases of arm contracture is monitored. The grade earned by our scholar in psychotherapy is noted on a slate. Eventually, walks, concerts, visits, and ultimately the permission to go out into the town are granted.
113. Can Shell-shock neuroses be prevented, other than by stopping or modifying the war or by weeding out Shell-shock candidates as they volunteer or are drafted? Morton Prince offers points of some suggestive value. The very various proportions of neurosis observed in different units and arms of the service suggest that various degrees of preparedness may have played a part. Bernheim says suggestion is an idea accepted. Aside from a possible increase of simulation, much might depend on what idea administered really got accepted! Morton Prince’s plan is that the prevention must be based upon the education of the mind. This therapeutic education should be based, however, on a preliminary systematic study by a board of specialists in the psychoneuroses of (a) the mental attitude of minds generally toward shell fire, and (b) clinical varieties of this “shock” neurosis as it occurs in trench warfare, (c) its frequency and disabling incidence, and (d) the state of mind previous to the trauma of those suffering from it.
113. Can shell-shock neuroses be prevented, other than by stopping or changing the war or by screening out shell-shock candidates as they volunteer or are drafted? Morton Prince provides some insightful points. The different rates of neurosis seen in various military units suggest that different levels of preparedness may have influenced this. Bernheim states that suggestion is an accepted idea. Aside from a possible rise in simulation, much might depend on which idea was actually accepted! Morton Prince believes that prevention should focus on educating the mind. However, this therapeutic education should be based on a systematic study conducted by a board of specialists in psychoneuroses regarding (a) the general mental attitude towards shell fire, (b) the clinical variations of this “shock” neurosis as it appears in trench warfare, (c) its frequency and disabling impact, and (d) the state of mind before the trauma for those affected.
On the basis of the findings of such a study, first, the regimental surgeon through lectures and clinical demonstrations would be instructed systematically in the symptoms and[903] pathology of the disease and the methods of psychotherapy for its prevention.
Based on the findings of this study, first, the regimental surgeon would be systematically taught through lectures and clinical demonstrations about the symptoms and pathology of the disease, as well as the psychotherapy methods for its prevention.
Second, soldiers, including officers, could then, in units of say 100, in turn be instructed in the nature of the disease through lectures by regimental surgeons. Shell-shock, they should be told, is a form of hysteria caused by mental factors. The work of the instruction should be done in France in the atmosphere of the war, wherein would be formed an attitude of healthy mental preparedness instead of an attitude of fear and mystery. Has mental hygiene this great scope? Is morale merely education?
Second, soldiers, including officers, could then be taught about the disease in groups of around 100 through lectures by regimental surgeons. They should be informed that shell shock is a type of hysteria triggered by psychological factors. This instruction should take place in France, in the context of the war, to foster a mindset of healthy mental readiness instead of one of fear and uncertainty. Can mental hygiene really cover this vast scope? Is morale just education?
114. What after all, is Morale? We hope to learn a little about it from this war for use hereafter, when we can say with the Florentine
114. What, after all, is Morale? We hope to learn a bit about it from this war for future use, when we can say with the Florentine
BIBLIOGRAPHY
These references were collected in the main by Sergeant Norman Fenton both before and after his entering the army, in connection with preparations for the work of one of the Neuropsychiatric Training Schools (that at Boston), established by the Division of Neurology and Psychiatry of the Surgeon-General’s Office, U. S. Army. The work, through the year 1917, at least, is not a mere vernis de bibliographe, but is based on a first-hand search through journals available in the Boston Medical Library and the New York Academy of Medicine (to whose officers thanks are due for very special privileges accorded). After Sergeant Fenton’s departure for service in the war neurosis hospital, 117, American E. F., France, the work was finished by the writer in considerable haste by skimming the current indexes and gathering the more prominent titles for 1918 (some for 1919). The titles, be it noted, go beyond the scope of the case-material in the body of the book and cover also a variety of reconstructional, reëducational, clinical-neurological, neurosurgical, and other topics bearing indirectly on neuropsychiatry. These auxiliary subjects are by no means completely covered, but it was thought the titles might help other inquirers. Under the war conditions numerous errors have no doubt crept into the references, which errors we hope will not, by reason of the short space of time covered by the bibliography, prove particularly misleading. The auxiliary topics can be referred to in the Index under page-numbers after the word “Bib.”
These references were mainly collected by Sergeant Norman Fenton both before and after he joined the army, in connection with preparations for the work of one of the Neuropsychiatric Training Schools (specifically the one in Boston), established by the Division of Neurology and Psychiatry of the Surgeon General’s Office, U.S. Army. The work, at least through 1917, is not just a simple vernis de bibliographe, but is based on a firsthand search through journals available in the Boston Medical Library and the New York Academy of Medicine (to whose officials thanks are due for the special privileges granted). After Sergeant Fenton’s departure for service in the war neurosis hospital, 117, American E.F., France, the work was completed by the writer in considerable haste by reviewing the current indexes and gathering the more notable titles for 1918 (some for 1919). It should be noted that the titles go beyond the scope of the case material in the body of the book and also cover a variety of reconstruction, re-education, clinical neurology, neurosurgery, and other topics related to neuropsychiatry. These additional subjects are not fully covered, but it was thought that the titles might assist other researchers. Due to the wartime conditions, numerous errors have likely slipped into the references, which we hope will not, because of the brief timeframe of the bibliography, prove particularly misleading. The additional topics can be found in the Index under page numbers following the word “Bib.”
E. E. S.
E.E.S.
Abadie. La neuro-psychiatrie d’urgence aux armées. Presse Méd., Par., 1915, v. 23, p. 46.
Abadie. Emergency neuro-psychiatry in the military. Medical Press, Paris, 1915, v. 23, p. 46.
Abrahams, Adolphe. A case of hysterical paraplegia. Lancet, Lond., 1915, v. ii, p. 178.
Abrahams, Adolphe. A case of hysterical paraplegia. Lancet, London, 1915, v. ii, p. 178.
Abrahams, A. “Soldier’s Heart.” Lancet, Lond., 1917, i, 442.
Abrahams, A. “Soldier’s Heart.” Lancet, London, 1917, i, 442.
Absence of neuroses in war. N. York M. J., 1916, v. 103, p. 1178.
Absence of neuroses in war. N. York M. J., 1916, v. 103, p. 1178.
Ackerley, R. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-1918, v. 10 (sect. Balneol.), pp. 37-38.
Ackerley, R. Treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-1918, v. 10 (sect. Balneol.), pp. 37-38.
Aconi, A. Le nevrosi di cuore e la guerra. Riforma med., Napoli, 1916, v. 32, pp. 501-505.
Aconi, A. Heart neuroses and war. Medical Reform, Naples, 1916, vol. 32, pp. 501-505.
Addinsell, A. W. Head injuries in war. Brit. Med. Jour., 1916, ii, 99.
Addinsell, A. W. Head injuries in war. Brit. Med. Jour., 1916, ii, 99.
Adler, H. M. The broader psychiatry and the war. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 364-370.
Adler, H. M. The wider field of psychiatry and the war. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 364-370.
Adrian, E. D. and Yealland, L. R. The treatment of some common war neuroses. Lancet, Lond., 1917, i, 667.
Adrian, E. D. and Yealland, L. R. The treatment of some common war neuroses. Lancet, London, 1917, i, 667.
Adrian and Yealland. The treatment of some common war neuroses. Lancet, Lond., 1917, i, pp. 867-872.
Adrian and Yealland. The treatment of some common war neuroses. Lancet, Lond., 1917, i, pp. 867-872.
After care of nerve injuries. Rev. of War Surg. & Med., 1918, i, no. 3, 49.
After care of nerve injuries. Rev. of War Surg. & Med., 1918, i, no. 3, 49.
Agostini, C. Sulla utilizazione degli epilettici in zona di guerra. Gior. di med. mil., Roma, 1918, lxvi, 24-33.
Agostini, C. On the Use of Epileptics in War Zones. Journal of Military Medicine, Rome, 1918, lxvi, 24-33.
Agnus, A. Le cloquement de la balle et de l’obus. Rev. Scient., Paris, 1915, li, pp. 358-363.
Agnus, A. The sound of the bullet and the shell. Sci. Rev., Paris, 1915, li, pp. 358-363.
Agudo Avilla, A. La guerra y las enfermedades mentales. Prensa med. argentina, Buenos Aires, 1916-1917, v. 3, pp. 129-131.
Agudo Avilla, A. War and Mental Illnesses. Argentine Medical Press, Buenos Aires, 1916-1917, vol. 3, pp. 129-131.
Aimé, Henri. De la variété et de l’évolution des troubles nerveux et psychiques d’origine commotionnelle pendant la guerre. Presse Méd., Par., 1917, v. 25, pp. 113-114.
Aimé, Henri. On the Variety and Evolution of Nervous and Psychotic Disorders from Concussions During the War. Medical Press, Paris, 1917, vol. 25, pp. 113-114.
Aimé, H. et Perrin, E. Considerations sur un cas d’épilepsie partielle guérie après extraction du projectile intra-cérébral. Progrès Méd., Par., 1916, v. 3, pp. 187-189.
Aimé, H. and Perrin, E. Considerations on a case of partial epilepsy cured after the removal of an intracerebral projectile. Progrès Méd., Paris, 1916, v. 3, pp. 187-189.
Aitkin, D. M. Orthopaedic methods in military surgery. Lancet, Lond., 1917, v. 1, pp. 10-16.
Aitkin, D. M. Orthopaedic techniques in military surgery. Lancet, Lond., 1917, v. 1, pp. 10-16.
Albert-Weil, E. Physiothérapie et blessés de guerre. Paris Méd., 1914-1915, (Part. Méd.), v. 15, p. 405.
Albert-Weil, E. Physical Therapy and War Injuries. Paris Med., 1914-1915, (Part. Méd.), v. 15, p. 405.
Alberti, A. I servizi psichiatrici di guerra. Riv. ospedal., Roma, 1917, v. 7, pp. 233-245.
Alberti, A. War psychiatric services. Hosp. Rev., Rome, 1917, vol. 7, pp. 233-245.
Alienée arrosé des passants avec de l’esprit de sel. Ann. méd.-psychol., Par., 1914-1915, v. 6, p. 524.
Alienée sprayed passersby with salt spirit. Ann. méd.-psychol., Par., 1914-1915, v. 6, p. 524.
Allbutt, T. C. Investigation of the significance of disorders and diseases of the heart in soldiers. Brit. Med. Jour., 1917, ii, 139.
Allbutt, T. C. Study on the importance of heart disorders and diseases in soldiers. Brit. Med. Jour., 1917, ii, 139.
Alquier, L. Sur les troubles nerveux par engorgements lymphatiques. Rev. neurol., Par., 1917, v. 24, pp. 8-13.
Alquier, L. On nerve disorders caused by lymphatic congestion. Neurol. Rev., Paris, 1917, vol. 24, pp. 8-13.
Alquier, Paul and Tanton, J. L’appareillage dans les fractures de guerre. Collection Horizon, Masson et Cie, Paris, 1916; also trans. Engl. in Military Medical Manuals, Univ. Lond. Press, and in Medical and Surgical Therapy, D. Appleton, N. Y.
Alquier, Paul and Tanton, J. Equipment for War Fractures. Horizon Collection, Masson et Cie, Paris, 1916; also translated into English in Military Medical Manuals, Univ. Lond. Press, and in Medical and Surgical Therapy, D. Appleton, N. Y.
Alt, Konrad. Psychische Störungen im Kriege. (D. Oester. Sanat., Wien, 1915, v. 12, p. 2). Aerztl. Central Ztschr., Wien, 1915, also v. 10, pp. 1-2; and 1915, v. 9, p. 2.
Alt, Konrad. Psychological Disorders in War. (D. Oester. Sanat., Vienna, 1915, v. 12, p. 2). Medical Central Journal, Vienna, 1915, also v. 10, pp. 1-2; and 1915, v. 9, p. 2.
Alt, Konrad. Im Deutschen Heere während des Krieges aufgetretende psychische Störungen und ihre Behandlung. Ztschr. f. ärztl. Fortbild., Jena, 1915, No. 11, pp. 331-333.
Alt, Konrad. Psychological disorders that occurred in the German army during the war and their treatment. Journal of Medical Continuing Education, Jena, 1915, No. 11, pp. 331-333.
Alt, Konrad. Ueber die Kur- u. Badefürsorge f. nervenkranken Krieger, mit besonderer Berücksichtigung der sogen. Kriegsneurotiker. Wien. Klin. Wchnschr. Nr. 18, 1918.
Alt, Konrad. On the care and treatment of mentally ill veterans, with special attention to so-called war neurotics. Vienna. Clinical Weekly, No. 18, 1918.
Alter, W. Zur Erkenntnis abwegger und krankhafter Geisteszustände bei Schulrekruten. Psychiat.-neurol. Wchnschr., Halle a. S., 1914-1915, v. 16, pp. 327-330; 339-341; 351-356.
Alter, W. On the understanding of deviant and pathological mental states in school recruits. Psychiat.-neurol. Weekly, Halle a. S., 1914-1915, v. 16, pp. 327-330; 339-341; 351-356.
Amar, Jules. Le moteur humain. Dunod et Piénat, Paris, 1914.
Amar, Jules. The Human Engine. Dunod and Piénat, Paris, 1914.
Amar, J. Principes de rééducation professionnelle. Compt. rend. acad. d. sc., Par., 1915, v. 160, pp. 559-562.
Amar, J. Principles of Vocational Rehabilitation. Compt. rend. acad. d. sc., Par., 1915, v. 160, pp. 559-562.
Amar, J. La rééducation des blessés et mutilés de la guerre. Rev. scient., 1915, v. 53, pp. 363-367.
Amar, J. The rehabilitation of war injuries and amputees. Sci. Rev., 1915, v. 53, pp. 363-367.
Amar, J. La rééducation professionnelle des blessés et des mutilés de la guerre. J. de physiol. et de path. gen., 1915, p. 820; p. 837; p. 855.
Amar, J. The vocational rehabilitation of war injured and disabled individuals. J. of physiology and general pathology, 1915, p. 820; p. 837; p. 855.
Amar, J. Technique d’éducation sensitive pour amputés et aveugles. Compt. rend. Acad. d. sc., Par., 1916, v. 163, pp. 335-338.
Amar, J. Sensitive education techniques for amputees and blind individuals. Compt. rend. Acad. d. sc., Par., 1916, v. 163, pp. 335-338.
Amar, J. Organization of vocational training for war cripples. Am. J. Care Cripples, N. Y., 1916, v. 3, pp. 176-183, 12 pl.
Amar, J. Organization of job training for veterans with disabilities. Am. J. Care Cripples, N. Y., 1916, v. 3, pp. 176-183, 12 pl.
Amar, J. La rééducation professionnelle des mutilés de guerre. Paris, 1917, P. Renouard, 33 p., 8o.
Amar, J. The vocational rehabilitation of war veterans. Paris, 1917, P. Renouard, 33 p., 8o.
Amélie, A. C. L. Contribution à l’étude des complications cardiovasculaires mentales de la méningite cérébrospinal de l’adulte. Thèses de Paris, 1915-1916, v. 13.
Amélie, A. C. L. Contribution to the study of cardiovascular and mental complications of adult cerebrospinal meningitis. Paris Theses, 1915-1916, v. 13.
Amenitski, D. A. The insane at the front. Sovrem. Psikhiat., Mosk., 1915, v. 9, pp. 325-333.
Amenitski, D. A. The Insane at the Front. Modern Psychiatry, Moscow, 1915, vol. 9, pp. 325-333.
Ancherson, Maria. (Psychosis following gunshot wound of the brain.) Ugeskr. f. Laeger, Kbenh., 1917, v. 79, pp. 1039-1046.
Ancherson, Maria. (Psychosis after a gunshot wound to the brain.) Ugeskr. f. Laeger, Kbenh., 1917, v. 79, pp. 1039-1046.
Anderson, H. M. and Noel, H. L. C. Case of shrapnel injury to right parietal cortex, showing paresis of left lower extremity, together with cortical sensory loss and thalamic over-response. Lancet, Lon., 1916, i, 79.
Anderson, H. M. and Noel, H. L. C. Case of shrapnel injury to the right parietal cortex, showing weakness in the left leg, along with loss of cortical sensation and increased response from the thalamus. Lancet, Lon., 1916, i, 79.
André-Thomas. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 473.
André-Thomas. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 473.
André-Thomas. Le tonus du poignet dans la paralysie du nerf cubital. Paris méd., 1917, No. 49, pp. 473-476.
André-Thomas. The tone of the wrist in ulnar nerve paralysis. Paris med., 1917, No. 49, pp. 473-476.
Angelucci, A. La protezione degli occhi dei soldati e la rieducazione dei ciechi di guerra. Arch. di ottal., Napoli, 1916, v. 23, pp. 177-205.
Angelucci, A. The Protection of Soldiers' Eyes and the Rehabilitation of War Blindness. Arch. di ottal., Naples, 1916, vol. 23, pp. 177-205.
Anglade. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 471.
Anglade. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 471.
Ankle-jerk. Brit. M. J., Lond., 1917, i, p. 556.
Ankle-jerk. Brit. M. J., Lond., 1917, i, p. 556.
Anton, G. Über psychische Folgen von Kopfverletzungen mit und ohne Gehirnerschütterung. Psychiat.-neurol. Wchnschr., Halle a. S., 1914-1915, v. 16, pp. 365-370.
Anton, G. On the Psychological Effects of Head Injuries with and without Concussion. Psychiat.-neurol. Weekly Journal, Halle a. S., 1914-1915, vol. 16, pp. 365-370.
Anton, G. Geistige Wechselwirkung im menschlichen Verkehr und Psychologie der Masse. Neurol. Centralbl., 37, Nr. 12, 1918.
Anton, G. Mental Interaction in Human Relations and the Psychology of the Masses. Neurol. Centralbl., 37, No. 12, 1918.
Antonini, G. (Mental symptoms of returning disabled soldiers.) Pensiero med., Milano, 1915, v. 5, No. 50.
Antonini, G. (Mental symptoms of returning disabled soldiers.) Pensiero med., Milan, 1915, v. 5, No. 50.
À propos d’alcoolisme. J. de méd. et chir. prat., Par., 1916, v. 87, pp. 149-153.
About alcoholism. J. de méd. et chir. prat., Par., 1916, v. 87, pp. 149-153.
Arinstein, L. S. (Neuropathological observations on those suffering from wind contusion.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 85-88.
Arinstein, L. S. (Neuropathological observations on people suffering from wind contusion.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 85-88.
Arinstein, L. S. (Hysteria and organic troubles of commotional origin.) Novoye v. Med., Petrog., 1915, v. 9, No. 9 and 10.
Arinstein, L. S. (Hysteria and physical issues caused by trauma.) New in Medicine, Petrograd, 1915, v. 9, No. 9 and 10.
Arinstein, L. S. (War and psychiatry.) Russk. Vrach, Petrogr., 1916, v. 15, p. 950.
Arinstein, L. S. (War and psychiatry.) Russk. Vrach, Petrogr., 1916, v. 15, p. 950.
Armstrong-Jones, R. Psychology of fear. Effects of panic fear in wartime. Hospital, Lon., 1917, lxi, 493.
Armstrong-Jones, R. Psychology of fear. Effects of panic fear during wartime. Hospital, Lon., 1917, lxi, 493.
Armstrong-Jones, R. Relation of alcohol to mental states, particularly in regard to the war. Practitioner, 1918, c, 201.
Armstrong-Jones, R. The relationship between alcohol and mental states, especially concerning the war. Practitioner, 1918, c, 201.
Armstrong-Jones, R. Mental states and the war; in particular the psychological effect of fear. St. Barth. Hosp. J., Lond., 1916-1917, v. 24, pp. 95-103.
Armstrong-Jones, R. Mental states and the war; especially the psychological impact of fear. St. Barth. Hosp. J., Lond., 1916-1917, v. 24, pp. 95-103.
Arnoux. La mort par décompression. La Nature, 18 Dec., 1915.
Arnoux. Death by decompression. Nature, Dec 18, 1915.
Ascarelli, A. Una nuova forma di autolesione (noduli sclerotici sottocutanei da iniezione di sostanze inassorbibili). Policlin., Roma, 1917, xxiv, sez. prat., 1407-1410.
Ascarelli, A. A new form of self-harm (subcutaneous sclerotic nodules from the injection of non-absorbable substances). Policlin., Rome, 1917, xxiv, prat. sect., 1407-1410.
Aschaffenburg, G. Über das Zusammenvorkommen organischer und nicht organischer Nervenstörungen. Neurol. Central bl., Leipz., 1915, v. 34, pp. 926-928.
Aschaffenburg, G. On the Co-occurrence of Organic and Inorganic Nerve Disorders. Neurol. Central Bl., Leipzig, 1915, v. 34, pp. 926-928.
Aschaffenburg, G. Winke zur Beurteilung von nerven- und psychisch-nervösen Erkrankungen. München. Med. Wchnschr., 1915, v. 622, pp. 931-932.
Aschaffenburg, G. Tips for Assessing Nerve and Psychoneurotic Disorders. Munich. Med. Weekly, 1915, v. 622, pp. 931-932.
Aschaffenburg, G. Lokalisierte und allgemeine Ausfallserscheinungen nach Hirnverletzung. Die Methode zur Feststellung und ihre Bedeutung für die soziale Brauchbarkeit der Geschädigten. Berl. klin. Wchnschr., 1916, v. 53, p. 127.
Aschaffenburg, G. Localized and general symptoms following brain injury. The method for diagnosis and its significance for the social usability of the affected individuals. Berl. klin. Wchnschr., 1916, v. 53, p. 127.
Ash, Edwin Lancelot. Nerves in war-time. Lond., 1914, Mills and Boon. 126 p., 8o.
Ash, Edwin Lancelot. Nerves in wartime. London, 1914, Mills and Boon. 126 pages, 8o.
Astvatsturoff, M. L. (Critique of the study of reflex epilepsy, based on observations on wounded.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 185-190.
Astvatsturoff, M. L. (Critique of the study of reflex epilepsy, based on observations on injuries.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 185-190.
Athanassio-Benisty, Mme. Formes cliniques des nerfs. Paris, 1917, Masson and Cie, 12o; also transl. Engl. in Medical and Surgical Therapy, D. Appleton, 1918; and in Military Med. Manuals, Univ. Lond. Press, 1918.[14]
Athanassio-Benisty, Mme. Clinical Forms of Nerves. Paris, 1917, Masson and Cie, 12o; also translated into English in Medical and Surgical Therapy, D. Appleton, 1918; and in Military Medicine Manuals, University of London Press, 1918.[14]
Aubaret. L’héméralopie des tranchées. Bull. Acad, de méd., Par., 1917, v. 77, p. 552.
Aubaret. The Night Blindness of the Trenches. Bull. Acad, de méd., Par., 1917, v. 77, p. 552.
Aubertin. Les tachycardies de guerre. Presse méd., 24 Jan., 1918.
Aubertin. War tachycardias. Med Press, Jan 24, 1918.
Audibert, Victor. La simulation dans l’armée. Paris méd., 1916, v. 19, pp. 103-106.
Audibert, Victor. Simulation in the Army. Paris méd., 1916, v. 19, pp. 103-106.
Auer, E. M. Phenomena resultant upon fatigue and shock of the central nervous system observed at the front in France. Med. Rec., N. Y., 1916, v. 89, pp. 641-644.
Auer, E. M. Effects of fatigue and shock on the central nervous system observed at the front in France. Med. Rec., N. Y., 1916, v. 89, pp. 641-644.
Auer, E. M. Some of the nervous and mental conditions arising in the present war. Mental Hyg., Concord, N. H., 1917, i. 383-388.
Auer, E. M. Some of the nervous and mental conditions that have emerged during the current war. Mental Hyg., Concord, N. H., 1917, i. 383-388.
Auerbach, F. Der Nachweis der Simulation von Schwerhörigkeit mittels einfacher Gehörprüfung. Deutsche med. Wchnschr., 1916, v. 52, pp. 1600-1601.
Auerbach, F. The detection of simulated hearing loss using simple hearing tests. German Med. Weekly, 1916, v. 52, pp. 1600-1601.
Auerbach, F. Zur Erkennung der Simulation von Schwerhörigkeit und Taubheit. Deutsche mil. ärztl. Ztschr., Berl., 1917, 46, 412-17.
Auerbach, F. On the Detection of the Simulation of Hearing Loss and Deafness. German Military Medical Journal, Berlin, 1917, 46, 412-17.
Axenfeld, T. Hemianopische Gesichtsfeldstörungen nach Schädelschüssen. Klin. Monatsbl. Augenh., Stuttg., 1915, n. F., v. 20, pp. 126-143.
Axenfeld, T. Hemianopic visual field disturbances after gunshot wounds. Klin. Monatsbl. Augenh., Stuttg., 1915, n. F., v. 20, pp. 126-143.
Axhausen. Die Behandlung der Schädelschüsse. Die Behandlung von Kriegsverletzungen und Kriegskrankheiten in den Heimatlazaretten. Erster Teil, p. 128. Jena, Fischer, 1915.
Axhausen. The Treatment of Gunshot Wounds to the Skull. The Treatment of War Injuries and War Diseases in Home Hospitals. Part One, p. 128. Jena, Fischer, 1915.
Babcock, H. L. Bárány tests as applied to aviators. Bos. M. and S. J., 1917, clxxvii, 840.
Babcock, H. L. Bárány tests for pilots. Bos. M. and S. J., 1917, clxxvii, 840.
Babinoff, Y. K. (Characteristics of diseases of the nervous system during the present war.) Mosk. Vrech., Petrogr., 1915, pp. 503-514.
Babinoff, Y. K. (Characteristics of diseases of the nervous system during the current war.) Mosk. Vrech., Petrogr., 1915, pp. 503-514.
Babinski, J. De la paralysie radiale due à la compression du nerf par des béquilles (Association organo-hystérique.) Rev. neurol., 1914-15, v. 22, pp. 408-409.
Babinski, J. On radial paralysis caused by nerve compression from crutches (Hysterical organ association.) Neurological Review, 1914-15, vol. 22, pp. 408-409.
Babinski, J. Lésion spinale par éclatement d’obus à proximité sans blessure ni contusion. Rev. neurol., Par., 1914-15, v. 22, pp. 581-583.
Babinski, J. Spinal injury from shell explosion nearby without injury or bruise. Rev. neurol., Par., 1914-15, v. 22, pp. 581-583.
Babinski, J. Les caractères des troubles moteurs (paralysies, contractures, etc.), dits “fonctionnels” et la conduite à tenir à leur égard. Rev. neurol., Par., 1916, v. 23, pp. 404; 521-534.
Babinski, J. The characteristics of motor disorders (paralyses, contractures, etc.), known as "functional," and the appropriate approach to take regarding them. Rev. neurol., Par., 1916, v. 23, pp. 404; 521-534.
Babinski, J. Réformes, incapacités, gratifications dans les névroses. Rev. neurol., Par., 1916, v. 23, pp. 753-756.
Babinski, J. Reforms, disabilities, rewards in neuroses. Rev. neurol., Paris, 1916, v. 23, pp. 753-756.
Babinski, J. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 464.
Babinski, J. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, v. 29, p. 464.
Babinski, J. et Froment, J. Contributions à l’étude des troubles nerveux d’ordre réflexe. Examen pendant l’anesthésie chloroformique. Rev. neurol., Par., 1914-15, v. 22, pp. 925-933.
Babinski, J. and Froment, J. Contributions to the study of nerve disorders of reflex origin. Examination during chloroform anesthesia. Rev. neurol., Paris, 1914-15, vol. 22, pp. 925-933.
Babinski, J. et Froment, J. Sur une forme de contracture organique d’origine périphérique et sans exaggération des réflexes. Rev. neurol., Par., 1914-15, v. 222, p. 1276.
Babinski, J. and Froment, J. On a form of organic contraction of peripheral origin without exaggeration of reflexes. Rev. neurol., Paris, 1914-15, v. 222, p. 1276.
Babinski, J. et Froment, J. Les modifications des réflexes tendineux pendant le sommeil chloroformique et leur valeur en sémiologie. Lyon Méd., 1915, v. 124, pp. 347-361. Also, Bull. Acad, de Méd., Par., 1915, v. 74, pp. 439-452.
Babinski, J. and Froment, J. Changes in tendon reflexes during chloroform sleep and their significance in symptomatology. Lyon Méd., 1915, v. 124, pp. 347-361. Also, Bull. Acad. de Méd., Paris, 1915, v. 74, pp. 439-452.
Babinski, J. and Froment, J. Hysteria or Pithiatism and Reflex Nervous Disorders. Military Medical Manuals, Univ. of London Press, 1918.
Babinski, J. and Froment, J. Hysteria or Pithiatism and Reflex Nervous Disorders. Military Medical Manuals, Univ. of London Press, 1918.
Babinski, J. and Froment, J. Service de neurologie militarisé de la Pitié. Rev. neurol., Par., 1916, v. 23, pp. 638-645.
Babinski, J. and Froment, J. Military Neurology Department of Pitié. Rev. neurol., Par., 1916, v. 23, pp. 638-645.
Babinski, J. et Froment, J. Troubles nerveux d’ordre réflexe ou syndrome d’immobilisation. Rev. neurol., Par., 1916, v. 29, pp. 914-918.
Babinski, J. and Froment, J. Reflex nerve disorders or immobilization syndrome. Neurol. Rev., Paris, 1916, vol. 29, pp. 914-918.
Babinski, J. et Froment, J. Abolition du réflexe cutané plantaire, anesthésie, associées à des troubles vaso moteurs et à l’hypothermie d’ordre réflexe. Rev. neurol., Par., 1916, v. 29, pp. 918-921.
Babinski, J. and Froment, J. Abolition of the plantar cutaneous reflex, anesthesia, associated with vasomotor disturbances and reflex-induced hypothermia. Rev. neurol., Paris, 1916, vol. 29, pp. 918-921.
Babinski, J. et Froment, J. Paralysie et hypotonie réflexes avec surexcitabilité mécanique, voltaique et faradique des muscles. Bull. Acad, de méd., Par., 1916, p. 40.
Babinski, J. and Froment, J. Paralysis and reflex hypotonia with mechanical, voltage, and faradic overexcitability of the muscles. Bull. Acad, de méd., Par., 1916, p. 40.
Babinski, J. et Froment, J. Contractures et paralysies traumatiques d’ordre réflexe. Presse méd., Par., 1916, v. 24, pp. 81-83.
Babinski, J. and Froment, J. Reflexive traumatic contractures and paralysis. Medical Press, Paris, 1916, vol. 24, pp. 81-83.
Babinski, J. et Froment, J. Troubles physiopathiques d’ordre réflexe. Association avec l’hysterie. Evolution de mesures médico-militaires. Presse Méd., Par., 1917, v. 25, pp. 385-386.
Babinski, J. and Froment, J. Reflex-related physiopathological issues. Association with hysteria. Evolution of medical-military measures. Medical Press, Paris, 1917, vol. 25, pp. 385-386.
Babinski, J. et Froment, J. Hystérie, pithiatisme et troubles nerveux d’ordre réflexe en neurologie de guerre. Paris, 1916, Masson and Cie., 12o; also transl. Engl. in Medical and Surgical Therapy, D. Appleton, 1918, and in Military Med. Manuals, Univ. London Press, 1917.
Babinski, J. and Froment, J. Hysteria, pithiatisme, and reflex nerve disorders in wartime neurology. Paris, 1916, Masson and Cie., 12o; also translated into English in Medical and Surgical Therapy, D. Appleton, 1918, and in Military Med. Manuals, Univ. London Press, 1917.
Babinski, J. et Froment, J. A propos de la communication de Roussy et Boisseau sur le pronostic et le traitement des troubles physiopathiques. Rev. neurol., Par., 1917, v. 24, pp. 527-537.
Babinski, J. and Froment, J. Regarding the communication by Roussy and Boisseau on the prognosis and treatment of pathophysiological disorders. Neurology Review, Paris, 1917, vol. 24, pp. 527-537.
Babinski, J., Froment, J., et Heitz, J. Des troubles vasomoteurs et thermiques dans les paralysies et les contractures d’ordre réflexe. Ann. de Méd., Par., 1916, v. 3, pp. 461-497.
Babinski, J., Froment, J., and Heitz, J. Vasomotor and thermal disorders in reflex-related paralysis and contractures. Ann. de Méd., Par., 1916, v. 3, pp. 461-497.
Babonneix et Célos. Deux cas de goitre exophtalmique survenus à la suite d’une commotion nerveuse. Bull. et mém. Soc. méd. d. hôp. de Par., 1917, v. 33, pp. 738-739.
Babonneix and Célos. Two cases of exophthalmic goiter following a nervous shock. Bull. et mém. Soc. méd. d. hôp. de Par., 1917, v. 33, pp. 738-739.
Babonneix, L. et David, H. Traumatismes cérébraux et syphilis. Rev. neurol., Par., 1917, v. 23, pp. 277-281.
Babonneix, L. and David, H. Brain injuries and syphilis. Neurology Review, Paris, 1917, vol. 23, pp. 277-281.
Babonneix et David. Monoplégie hystérique de membre supérieur gauche durant depuis deux ans et guéri en deux jours par la suggestion. J. de méd. et de chir. prat., Par., 1917, v. 88, Oct. 10.
Babonneix and David. Hysterical monoplegia of the left upper limb lasting for two years and cured in two days by suggestion. J. of Med. and Surg. Pract., Paris, 1917, v. 88, Oct. 10.
Bailey, Pearce. Neuropsychiatry and the mobilization. N. Y. Med. Jour., 1918, cvii, 794.
Bailey, Pearce. Neuropsychiatry and the mobilization. N. Y. Med. Jour., 1918, cvii, 794.
Bailey, Pearce. The care of disabled returned soldiers. Pacific M. J., San Francisco, 1917, lx, 608-615.
Bailey, Pearce. The care of disabled veterans. Pacific M. J., San Francisco, 1917, lx, 608-615.
Bailey, Pearce. The care of disabled returned soldiers. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 345-353.
Bailey, Pearce. The care of disabled veterans. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 345-353.
Bailey, Pearce. Psychiatry and the army. Harper’s monthly mag., 1917, v. 135, pp. 251-257.
Bailey, Pearce. Psychiatry and the army. Harper’s monthly magazine, 1917, vol. 135, pp. 251-257.
Bailey, Pearce. War and mental diseases. Am. Jour. Pub. Health, 1918, viii, 1.
Bailey, Pearce. War and mental illnesses. Am. Jour. Pub. Health, 1918, v. 8, no. 1.
Baldi, Felice. Le subconscient dans la génèse des phénomènes traumato-névrosiques. Contribution à la connaissance de la névrose traumatique. Annali di Neurologia, an XXXII, fasc. 4, pp. 147-178, 1914.
Baldi, Felice. The subconscious in the development of traumatic neurosis phenomena. Contribution to the understanding of traumatic neurosis. Annals of Neurology, vol. XXXII, issue 4, pp. 147-178, 1914.
Ballard, E. Fryer. An epitome of mental disorders. 1917, Blakiston, pp. 145-165.
Ballard, E. Fryer. A summary of mental disorders. 1917, Blakiston, pp. 145-165.
Ballet, Gilbert. Oedème blanc associé aux contractures d’origine psychique. Rev. neurol., Par., 1914-15, v. 222, pp. 705-707.
Ballet, Gilbert. White edema associated with psychological contractures. Rev. neurol., Par., 1914-15, v. 222, pp. 705-707.
Ballet, G. Bourdonnements et sifflements d’oreille dus à un trouble du représentation mentale. Rev. neurol., Par., 1914-15, v. 222, pp. 707-708.
Ballet, G. Tinnitus and ear buzzing or whistling caused by a disturbance in mental representation. Rev. neurol., Par., 1914-15, v. 222, pp. 707-708.
Ballet, G. Syndrome de Brown-Séquard par suite de commotion par éclatement d’obus, sans plaie extérieure (hématomyélie vraisemblable). Rev. neurol., Par., 1914-15, v. 222, pp. 768-769.
Ballet, G. Brown-Séquard syndrome due to concussion from shrapnel, without external injury (likely hematomyelia). Rev. neurol., Paris, 1914-15, vol. 222, pp. 768-769.
Ballet, G. Note sur la relation des tremblements et des états émotionnels. Rev. neurol., Par. 1914-15, v. 221, pp. 934-936.
Ballet, G. Note on the relationship between tremors and emotional states. Rev. neurol., Par. 1914-15, v. 221, pp. 934-936.
Ballet, G. L’insomnie à crises intermittentes. Presse méd. Par., 1916, v. 24, pp. 73-74.
Ballet, G. Intermittent insomnia. Med. Press Paris, 1916, vol. 24, pp. 73-74.
Ballet, G. Persistance des contractures d’origine psychique pendant le sommeil. Société de Neurol. 29 juillet 1915.
Ballet, G. Persistence of psychogenic contractures during sleep. Neurology Society. July 29, 1915.
Ballet, G. et Rogues de Fursac, J. Les psychoses “commotionnelles.” Paris méd., 1916, v. 19, pp. 2-8.
Ballet, G. and Rogues de Fursac, J. The "Commotion" Psychoses. Paris Med., 1916, vol. 19, pp. 2-8.
Ballet, Sicard, Dejerine, etc. Examens où l’on peut suspecter simulation chez les “blessés nerveux.” Rev. neurol., Par., 1914-15, v. 22, pp. 1245-1247.
Ballet, Sicard, Dejerine, etc. Exams where one might suspect faking among the "nervous injuries." Rev. neurol., Par., 1914-15, v. 22, pp. 1245-1247.
Bannard, W. The mechanics of convalescence: methods of hastening the cure of German wounded soldiers. Scient. Am., N. Y., 1915, v. 112, p. 404.
Bannard, W. The mechanics of recovery: ways to speed up the healing of German soldiers. Scient. Am., N. Y., 1915, v. 112, p. 404.
Barat, L. Une fugue confusionnelle en temps de guerre. J. de psychol., norm. et path., Par., 1914, v. 2, pp. 455-463.
Barat, L. A Confused Fugue During Wartime. J. of Psychol., Norm. and Path., Paris, 1914, vol. 2, pp. 455-463.
Barker, L. F. War and the nervous system. J. Nerv. and Ment. Dis., N. Y., 1916, v. 44, pp. 1-10.
Barker, L. F. War and the Nervous System. J. Nerv. and Ment. Dis., N. Y., 1916, v. 44, pp. 1-10.
Barr, J., Sir. The “Soldier’s Heart” and its relation to thyroidism. Brit. Med. Jour., 1916, i, 544.
Barr, J., Sir. The “Soldier’s Heart” and its link to thyroid issues. Brit. Med. Jour., 1916, i, 544.
Barron, Netterville. Physical training with especial reference to the training of convalescents. J. Roy. Army Med. Corps, Lond., 1916, v. 27, pp. 460-476.
Barron, Netterville. Physical training with a special focus on the training of patients recovering from illness. J. Roy. Army Med. Corps, Lond., 1916, v. 27, pp. 460-476.
Barth, E. Ueber organische und funktionelle Kehlkopfstörungen bei Kriegsverletzungen. Berl. klin. Wchschr., 1916, No. 5, pp. 120-121.
Barth, E. On organic and functional laryngeal disorders from war injuries. Berl. klin. Wchschr., 1916, No. 5, pp. 120-121.
Basset, A. Plaies des nerfs des membres par projectiles de guerre. Rev. de Chir., 1916, li, 609.
Basset, A. Nerve injuries in the limbs caused by war projectiles. Rev. de Chir., 1916, li, 609.
Batten, F. E. Some functional nervous affections produced by the war. Quart. J. Med., Oxford, 1915-1916, ii, pp. 13-38.
Batten, F. E. Some functional nervous disorders caused by the war. Quart. J. Med., Oxford, 1915-1916, ii, pp. 13-38.
Batten, F. E. Two cases of post-central injury of cortex shown for the purpose of eliciting evidence on—(i) the appreciation of vibration, (ii) Recovery, (iii) Segmental Representation of the Cortex. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (neurol. sect.), pp. 67-68.
Batten, F. E. Two cases of post-central cortex injury presented to gather evidence on—(i) the perception of vibration, (ii) recovery, (iii) the segmental representation of the cortex. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (neurol. sect.), pp. 67-68.
Baudisson and Marie (A.). Sur la spondylothérapie des troubles asthéniques et vasomoteurs post-traumatiques ou commotionnels. Comp. rend. Acad. d. sc., Par., 1917, clxv, 479.
Baudisson and Marie (A.). On the spondylotherapy of asthenic and vasomotor disorders following trauma or concussion. Comp. rend. Acad. d. sc., Par., 1917, clxv, 479.
Bauer, J. Kombinationen organischer mit funktionellen Nervenstörungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 175-176.
Bauer, J. Combinations of organic and functional nerve disorders. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 175-176.
Bauer, J. Einige Bemerkungen über die Beurteilung und Behandlung der Kriegsneurosen. Wien. klin. Wchschr., 1916, v. 29, pp. 951-953.
Bauer, J. Some Remarks on the Assessment and Treatment of War Neuroses. Wien. klin. Wchschr., 1916, v. 29, pp. 951-953.
Bauer, J. Der Báránysche Zeigeversuch und andere zerebellare Symptome bei traumatischen Neurosen. Wien. klin. Wchschr., 1916, v. 29, pp. 1136-1144.
Bauer, J. The Barányi Test and Other Cerebellar Symptoms in Traumatic Neuroses. Vienna Clinical Weekly, 1916, vol. 29, pp. 1136-1144.
Baumel, J. La ponction lombaire dans les commotions nerveuses et les traumatismes du crâne par projectiles de guerre. Lyon chirurg., 1915, v. 12, pp. 271-292.
Baumel, J. Spinal taps in nerve concussions and skull injuries from war projectiles. Lyon surg., 1915, v. 12, pp. 271-292.
Baumel, J. et Lardennois, G. Diplégie faciale. N. iconog. de la Salpêtrière, Par., 1916-17, No. 4, pp. 272-381.
Baumel, J. and Lardennois, G. Facial diplegia. N. iconog. de la Salpêtrière, Par., 1916-17, No. 4, pp. 272-381.
Bayliss, Wm. M. Intravenous injection in wound shock. Longmans, Green & Co., 1918.
Bayliss, Wm. M. Intravenous injection in wound shock. Longmans, Green & Co., 1918.
Bayliss, W. M. On the origin of electro-currents led off from the human body, especially in relation to “Nerve-leaks.” Proc. Roy. Soc. Med., Lond., 1917 (sect. of electro-therap.), v. 10, No. 7, p. 11.
Bayliss, W. M. On the origin of electric currents emitted from the human body, particularly in relation to “Nerve-leaks.” Proc. Roy. Soc. Med., Lond., 1917 (sect. of electro-therap.), v. 10, No. 7, p. 11.
Beaton, T. Some Observations on Mental Conditions among a Ship’s Company in War-time. J. Roy. Nav. M. Serv., Lond., 1916, No. 1; pp. 447-452.
Beaton, T. Some Observations on Mental Conditions among a Ship’s Company in War-time. J. Roy. Nav. M. Serv., Lond., 1916, No. 1; pp. 447-452.
Beauchant, R. Morichau. Le signe de l’atrophie musculaire et de l’hyperesthésie profonde dans la tuberculose fibreuse du sommet. Paris Méd., 1916 (Part. Méd.), v. 19, pp. 589-592.
Beauchant, R. Morichau. The sign of muscle atrophy and deep hypersensitivity in fibrous tuberculosis of the apex. Paris Méd., 1916 (Part. Méd.), v. 19, pp. 589-592.
Bechterew, W. M. (War and psychoses.) Novoye v. Med., Petrogr., 1915, v. 9, No. 7, No. 8.
Bechterew, W. M. (War and psychoses.) New in Medicine, Petrograd, 1915, v. 9, No. 7, No. 8.
Beck, O. Das Romberg-Phänomen bei traumatischer Neurose (Schrapnellneurose). Monatschr f. Ohrenhk., Berl. u. Wien., 1915, v. 49, pp. 209-210.
Beck, O. The Romberg Phenomenon in Traumatic Neurosis (Shrapnel Neurosis). Monthly Journal of Otology, Berlin and Vienna, 1915, vol. 49, pp. 209-210.
Becker, Wern. H. Kriegspsychosen. Psychiat.-neurol. Wchschr., 1914-15, v. 16, pp. 295-298.
Becker, Wern. H. War Psychoses. Psychiatric and Neurological Weekly, 1914-15, vol. 16, pp. 295-298.
Belenki. Les symptomes sensitifs dans les sections anatomiques et physiologiques des nerfs périphériques. Presse Méd. Feb. 17, 1916.
Belenki. The sensory symptoms in the anatomical and physiological sections of peripheral nerves. Méd. Press. Feb. 17, 1916.
Bellin et Vernet. Sur une forme nouvelle de syndrome bulbaire inférieur avec ataxie du larynx. Bull. et mém. Soc. méd. d’. hôp. de Par., 1917, v. 33, pp. 83-89.
Bellin and Vernet. On a new form of lower bulbar syndrome with laryngeal ataxia. Bull. et mém. Soc. méd. d’. hôp. de Par., 1917, v. 33, pp. 83-89.
Benassi, G. Malattie vere e malattie simulate in rapporto al servizio militaire. Quaderni di med. leg., Milano, 1917, i. 196; 217-252.
Benassi, G. Real illnesses and feigned illnesses in relation to military service. Medical Law Notebooks, Milan, 1917, i. 196; 217-252.
Benedikt. Der Epileptiker bei der Musterung. Wien. klin. Wchschr., 1915, v. 28, pp. 592-593.
Benedikt. The epileptic during the medical examination. Wien. klin. Wchschr., 1915, v. 28, pp. 592-593.
Benedikt. Der Epileptiker bei der Musterung. Med. klin., Berl. u. Wien., 1915, v. 22, p. 762.
Benedikt. The epileptic during the examination. Med. clin., Berl. and Wien., 1915, v. 22, p. 762.
Benisty-Athanassio. Clinical Forms of Nerve Lesions. Military Medical Manuals, Univ. of London Press, 1918.
Benisty-Athanassio. Clinical Forms of Nerve Injuries. Military Medical Manuals, Univ. of London Press, 1918.
Benisty-Athanassio. The Treatment and Repair of Nerve Lesions. Military Medical Manuals, Univ. of London Press, 1918.
Benisty-Athanassio. The Treatment and Repair of Nerve Lesions. Military Medical Manuals, University of London Press, 1918.
Benisty-Athanassio. Traitement et restoration de lésions des nerfs. Collection Horizon, Masson et Cie, Paris, 1917.
Benisty-Athanassio. Treatment and restoration of nerve injuries. Collection Horizon, Masson et Cie, Paris, 1917.
Bennati, Nando. La etiologia determinante nella nevrosi traumatica di guerra. Rev. sper. di freniat., Reggio-Emilia, 1916, v. 42, pp. 49-84.
Bennati, Nando. The Determining Etiology in War Trauma Neurosis. Rev. sper. di freniat., Reggio-Emilia, 1916, v. 42, pp. 49-84.
Bennett, Wm. L. Psychasthenia. J. Roy Army Med. Corps, Lond., 1917, v. 28, p. 614.
Bennett, Wm. L. Psychasthenia. J. Roy Army Med. Corps, Lond., 1917, v. 28, p. 614.
Benon, R. Au sujet des névroses traumatiques, Réunion de la IIe armée 17 juillet, 1915.
Benon, R. On the subject of traumatic neuroses, Meeting of the IIe army July 17, 1915.
Benon, R. Les maladies mentales et nerveuses et la guerre. Rev. neurol., Par., 1916, 4. 23, pp. 210-215.
Benon, R. Mental and Nervous Illnesses and War. Neurological Review, Paris, 1916, 4. 23, pp. 210-215.
Benon, R. Les maladies mentales et nerveuses et la pratique des réformes No. 1. Rev. neurol., Par., 1917, v. 24, pp. 306-309.
Benon, R. Mental and Nervous Disorders and the Practice of Reforms No. 1. Rev. neurol., Paris, 1917, vol. 24, pp. 306-309.
Benon, R. La guerre et les pensions pour maladies mentales et nerveuse. Rev. neurol., Par., 1916, v. 24, pp. 320-323.
Benon, R. War and pensions for mental and nervous illnesses. Neurological Review, Paris, 1916, v. 24, pp. 320-323.
Bérard. Alcoolisme et anesthésie. Lyon Méd., 1917, v. 126, pp. 282-285.
Bérard. Alcoholism and Anesthesia. Lyon Med., 1917, v. 126, pp. 282-285.
Bergonzoli, G. Stati ansiosi nelle malattie mentali. Voghers: Art Grafiche, 1915, pp. 186.
Bergonzoli, G. Anxious States in Mental Illness. Voghers: Art Grafiche, 1915, pp. 186.
Berlung, Richard. Organische Erkrankungen mit hysterische Pseudodemenz. Monatschr. f. Psychiat. u. Neurol., Berl., 1916, v. 39, No. 5; p. 268.
Berlung, Richard. Organic Diseases with Hysterical Pseudodementia. Monthly Journal of Psychiatry and Neurology, Berlin, 1916, vol. 39, No. 5; p. 268.
Bernhard, L. I. Business organization of the workshops connected with the Royal Orthopedic Reserve Hospital at Nürnberg. Am. J. Care Cripples, N. Y., 1917, v. 4, pp. 197-200.
Bernhard, L. I. Business organization of the workshops associated with the Royal Orthopedic Reserve Hospital in Nürnberg. Am. J. Care Cripples, N. Y., 1917, v. 4, pp. 197-200.
Bernheim. Le courage. Rev. gén. de clin. et de thérap., Par., 1915, v. 29, pp. 495-498.
Bernheim. Courage. General Review of Clinical and Therapy, Paris, 1915, vol. 29, pp. 495-498.
Bernheim. Amaurose simulée et amaurose psychique. Simulation et autosuggestion. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 609-610.
Bernheim. Simulated blindness and psychic blindness. Simulation and self-suggestion. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 609-610.
Bernheim. Psychonévroses, psychothérapie. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 739-741.
Bernheim. Psychoneuroses, psychotherapy. Gen. Rev. of Clin. and Ther., Paris, 1916, vol. 30, pp. 739-741.
Bernheim. Psychonévroses rebelles. Procédés divers associés à la suggestion. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 820-823.
Bernheim. Resilient Psychoneuroses. Various methods associated with suggestion. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 820-823.
Bernheim. Névroses, psychonévroses, hystérie. Progrès méd., Par., 1917, v. 43, pp. 355-357.
Bernheim. Neuroses, psychoneuroses, hysteria. Progress Med., Paris, 1917, vol. 43, pp. 355-357.
Bernheim. Y-a-t-il des aphasies sensorielles?—Surdité et cécité verbales. Rev. gén. de clin. et de thérap., Par., 1917, v. 31, pp. 518-520.
Bernheim. Are there sensory aphasias?—Verbal deafness and blindness. Rev. gén. de clin. et de thérap., Par., 1917, v. 31, pp. 518-520.
Berruyer. Un cas de surdi-mutité simulée datant de cinq mois. Caducée, Par., 1916, v. 16, pp. 129-130.
Berruyer. A case of faked deaf-muteness dating back five months. Caducée, Par., 1916, v. 16, pp. 129-130.
Berruyer. Surdité de guerre. Rééducation de l’ouïe. Caducée, Par., 1917, v. 17, pp. 17-21; also pp. 1-3.
Berruyer. War deafness. Hearing rehabilitation. Caducée, Paris, 1917, vol. 17, pp. 17-21; also pp. 1-3.
Berruyer. Un cas de surdi-mutité simulée datant de cinq mois. J. de Méd. de Par., 1917, v. 36, p. 34.
Berruyer. A case of faked deaf-muteness from five months ago. J. de Méd. de Par., 1917, v. 36, p. 34.
Bertein et Nimmer. Les premières heures du blessé de guerre du trou d’obus au poste de secours. Collection Horizon, Masson et Cie., 1918.
Bertein et Nimmer. The first hours of the war wounded from the shell hole at the first aid station. Horizon Collection, Masson et Cie., 1918.
Besson. Au sujet des névroses traumatiques. Rev. gén. de clin. et de thérap., Par., 1915, v. 29, p. 527.
Besson. On traumatic neuroses. Gen. Rev. of Clin. and Therapy, Paris, 1915, vol. 29, p. 527.
Besson. Au sujet des névroses traumatiques. Presse Méd., Par., 1915, v. 23, p. 316.
Besson. On traumatic neuroses. Med. Press, Paris, 1915, vol. 23, p. 316.
Best, F. Über Nachtblindheit im Felde. München Med. Wchschr., 1915, v. 622, pp. 1121-1124.
Best, F. On Night Blindness in the Field. Munich Med. Wkly., 1915, v. 622, pp. 1121-1124.
Beutenmüller. Über Nachtblindheit im Felde. München med. Wchnschr., 1915, v. 622, p. 1207.
Beutenmüller. On Night Blindness in the Field. Munich Medical Weekly, 1915, v. 622, p. 1207.
Beyer, Ernest. Über die Bedeutung der Rentenhöhe bei der Entstehung der Rentenneurose. Aerztl. Sachverst. Ztg., 1915, v. 21, pp. 242-244.
Beyer, Ernest. On the Significance of Pension Amounts in the Development of Pension Neurosis. Medical Expert Journal, 1915, v. 21, pp. 242-244.
Bianchi, V. Le nevrosi nell’ esercito in rapporto alla guerra. Med. e chir. d. med. prat., Napoli, 1917, v. 1, No. 5, pp. 1-16.
Bianchi, V. The neuroses in the army in relation to war. Med. and chir. d. med. prat., Naples, 1917, vol. 1, No. 5, pp. 1-16.
Bianchi, V. Le nevrosi nell’ esercito in rapporto alla guerra. Ann. di. nevrol., Napoli, 1917, v. 34, pp. 1-20.
Bianchi, V. The neuroses in the army in relation to war. Ann. of neurology, Napoli, 1917, v. 34, pp. 1-20.
Bianchi, V. Neuropsichiatria di guerra. Ann. di nevrol., Napoli, 1917, v. 34, pp. 21-38.
Bianchi, V. War Psychiatry. Ann. of Neurology, Naples, 1917, vol. 34, pp. 21-38.
Bickel, Heinrich. Zur pathogenese der im Krieg auftretenden psychischen Störungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 117-121.
Bickel, Heinrich. On the Pathogenesis of Psychological Disorders Occurring in War. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 117-121.
Bielschowsky, A. Sehstörungen im Kriege ohne objektiven Augenbefund, München med. Wchnschr., 1914, v. 61, pp. 2443-2445.
Bielschowsky, A. Vision problems in war without any objective eye findings, Munich med. Wchnschr., 1914, v. 61, pp. 2443-2445.
Bielschowsky, A. Die Forderung des akademischen Blindenbildungswesens im Kriege. Stuttgart, Enke, 1917.
Bielschowsky, A. The Demand for Academic Education for the Blind During the War. Stuttgart, Enke, 1917.
Bikhovski, S. (Diagnosis of epilepsy in the clinic and in army medical practice.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 300-306.
Bikhovski, S. (Diagnosis of epilepsy in the clinic and in army medical practice.) Psychiatry Gazette, St. Petersburg, 1916, vol. 3, pp. 300-306.
Bilancioni, G. Di un metodo sicuro per svelare la simulazione della sordita bilaterale. Arch. ital. di otol. (etc.), Torino, 1916, xxvii, 516-524. Also: Policlin, Roma, 1917, xxiv, sez. prat., 743-745.
Bilancioni, G. On a Reliable Method to Reveal the Simulation of Bilateral Deafness. Arch. ital. di otol. (etc.), Turin, 1916, xxvii, 516-524. Also: Policlin, Rome, 1917, xxiv, prat. sect., 743-745.
Bing, Robert. Pathogenese, Prophylaxe und Begutachtung psychoneurotischer Unfallfolgen. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, pp. 903.
Bing, Robert. Pathogenesis, Prevention, and Assessment of Psychoneurotic Accident Consequences. German Medical Weekly, Berlin and Leipzig, 1915, v. 412, pp. 903.
Binswanger, Otto. Kriegsneurologische Krankenvorstellungen. München med. Wchnschr., 1915, v. 631, p. 1651.
Binswanger, Otto. War Neurology Patient Presentations. Munich Medical Weekly, 1915, v. 631, p. 1651.
Binswanger, Otto. Hystero-somatische Krankheitsserscheinungen bei der Kriegshysterie. Monatschr. f. Psychiat. u. Neurol., Berl., 1915, v. 38, pp. 1-60.
Binswanger, Otto. Hysterical physical symptoms in war hysteria. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, vol. 38, pp. 1-60.
Binswanger, Otto. Über Kommotionspsychosen und Verwandtes. Cor. Bl. f. Schweiz. Aerzte., 1917, v. 47, pp. 1401-1412.
Binswanger, Otto. On Psychotic Disturbances and Related Topics. Cor. Bl. f. Schweiz. Ärzte., 1917, v. 47, pp. 1401-1412.
Bird, Charles. From home to the charge; a psychological study of the soldier. Am. J. Psychol., 1917, v. 28, pp. 315-348.
Bird, Charles. From home to the frontlines; a psychological study of the soldier. Am. J. Psychol., 1917, v. 28, pp. 315-348.
Birkett. Special discussion on warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), p. 90.
Birkett. Special discussion on injuries and mental health issues from warfare. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), p. 90.
Birnbaum, Karl. Geistesstörungen im Kriege. Umschau, 1914, No. 43.
Birnbaum, Karl. Mental Disorders in War. Outlook, 1914, No. 43.
Birnbaum, Karl. Kriegsneurosen und psychosen auf Grund der gegenwärtigen Kriegsbeobachtungen. Ztschr. f. d. ges. neurol. u. psychiat., Berl. u. Leipz., 1914-1915, v. 11 (Ref.), pp. 321-369.
Birnbaum, Karl. War neuroses and psychoses based on current war observations. Journal of General Neurology and Psychiatry, Berlin and Leipzig, 1914-1915, vol. 11 (Ref.), pp. 321-369.
Birch-Hirschfeld. Ueber Nachtblindheit im Kriege. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, p. 1306.
Birch-Hirschfeld. On Night Blindness in War. German Medical Weekly, Leipzig and Berlin, 1916, v. 42, p. 1306.
Bittorf, A. Zur Behandlung der nach Granatexplosionen auftretenden Neurosen. Med. klin., Berl. u. Wien, 1915, v. 112, pp. 897-898.
Bittorf, A. Treatment of Neuroses Following Grenade Explosions. Med. clin., Berl. u. Wien, 1915, v. 112, pp. 897-898.
Bittorf, A. Zur Behandlung der nach Granatexplosionen auftretenden Neurosen. München med. Woch., 1915, v. 62, pp. 1029-1031.
Bittorf, A. On the Treatment of Neuroses Following Grenade Explosions. Munich Medical Weekly, 1915, v. 62, pp. 1029-1031.
Black. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-1918, v. 10 (sect. Balneol.), pp. 24-30.
Black. Physical treatment for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-1918, v. 10 (sect. Balneol.), pp. 24-30.
Blanc, Jean. La dysthyroïdie, facteur de névroses. Le réflexe oculocardiaque régulateur de l’opotherapie thyroïdienne. Progrès méd., Par., 1917, No. 12, pp. 95-98.
Blanc, Jean. Dysthyroidism, a factor in neuroses. The oculocardiac reflex regulating thyroid therapy. Med Progress, Paris, 1917, No. 12, pp. 95-98.
Blässig. Funktionelle Stimmbandlähmung. München med. Wchnschr., 1915, v. 62, p. 835.
Blässig. Functional vocal cord paralysis. Munich Med. Weekly, 1915, vol. 62, p. 835.
Blin and Kernéis. Un cas de paralysie générale spinale antérieure. Caducée, Par., 1916, v. 16, pp. 111-113.
Blin and Kernéis. A case of anterior general spinal paralysis. Caducée, Par., 1916, v. 16, pp. 111-113.
Blum, E. De la simulation: Étude des qualités que doit posséder le médecin militaire expert. Gaz. hebd. d. sc. méd. de Bordeaux, 1916, 27 août, pp. 124-125, also 1916, 10 Sept., pp. 129-132.
Blum, E. On Simulation: A Study of the Qualities Required of an Expert Military Doctor. Weekly Gazette of Medical Science in Bordeaux, 1916, August 27, pp. 124-125, also 1916, September 10, pp. 129-132.
Blum, E. De la simulation “La carotte.” J. de méd. de Bordeaux, 1915-16, v. 45, pp. 274-280.
Blum, E. On the simulation “The Carrot.” J. de méd. de Bordeaux, 1915-16, v. 45, pp. 274-280.
Blum, E. and Dimier, G. De la simulation; ses causes, son traitement. Gaz. hebd. d. sc. méd. d. Bordeaux, 1916, xxxvii, 76; 84; 93.
Blum, E. and Dimier, G. On simulation; its causes, its treatment. Weekly Gazette of Medical Sciences in Bordeaux, 1916, xxxvii, 76; 84; 93.
Blum, E. La dissimulation. Gaz. hebd. d. sc. med. de Bordeaux, 1917, v. 38, pp. 57-61, and pp. 67-68.
Blum, E. The Concealment. Weekly Gazette of Medical Sciences of Bordeaux, 1917, vol. 38, pp. 57-61, and pp. 67-68.
Blumenau, L. V. (Organization of medical aid to neurotic soldiers at the front.) Psikhiat. Gaz., Petrogr., 1915, v. 2, p. 5.
Blumenau, L. V. (Organization of medical support for neurotic soldiers at the front.) Psychiatric Gazette, St. Petersburg, 1915, Vol. 2, p. 5.
Boeckel, J. À quels accidents tardifs sont exposés les blessés du crâne? Bull. et mém. Soc. de chir. de Par., 1916, v. 42, pp. 1575-1593.
Boeckel, J. What late complications are skull injury victims at risk for? Bull. et mém. Soc. de chir. de Par., 1916, v. 42, pp. 1575-1593.
Boeckel, J. Les blessures du crâne. Lyon chir., 1916, 13, pp. 903-911.
Boeckel, J. Skull injuries. Lyon surgery, 1916, 13, pp. 903-911.
Boisseau, J. Quelques exemples de différents modes de suggestion déterminant des accidents hystériques. Presse méd., Par., 1915, v. 23, pp. 47-48.
Boisseau, J. Some examples of different modes of suggestion leading to hysterical accidents. Med. Press, Paris, 1915, vol. 23, pp. 47-48.
Bonhoeffer, K. Die Dienstbeschädigungsfrage in der Psychopathologie. Die militärärztliche Sachsverständigentätigkeit auf dem Gebiete des Ersatzwesens und der militärischen Versorgung. Erste Teil, pp. 86-115. Jena, Fischer, 1917.
Bonhoeffer, K. The Issue of Service Damage in Psychopathology. The military medical expert activity in the field of compensation and military supply. Part One, pp. 86-115. Jena, Fischer, 1917.
Bonhoeffer, K. Psychiatrisches zum Kriege. Monatschr. f. Psychiat. un Neurol., Berl., 1914, v. 36, pp. 435-448.
Bonhoeffer, K. Psychiatric Perspectives on War. Monthly Journal of Psychiatry and Neurology, Berlin, 1914, v. 36, pp. 435-448.
Bonhoeffer, K. Psychiatrie und Krieg. Deutsche med. Wchnschr., 1914, v. 40, pp. 1777-1779.
Bonhoeffer, K. Psychiatry and War. German Med. Weekly, 1914, vol. 40, pp. 1777-1779.
Bonhoeffer, K. Die Dienstbeschädigungsfrage in der Psychopathologie. Mil. ärtzl. Sachvest-Tatigk., Jena, 1917, i, 86-114.
Bonhoeffer, K. The Issue of Service Damage in Psychopathology. Mil. Medical Expert Report, Jena, 1917, i, 86-114.
Bonhoeffer, K. Ueber Fälle von hysterischer Granatexplosionslahmung. Berl. klin. Wchnschr., 1915, lii, 166-168.
Bonhoeffer, K. On Cases of Hysterical Grenade Explosion Paralysis. Berl. klin. Wchnschr., 1915, lii, 166-168.
Bonhoeffer, K. Über die Abnahme des Alkoholismus während des Krieges. Monatschr. f. Psychiat. u. Neurolog., 1917, 41, 382-5.
Bonhoeffer, K. On the Decrease of Alcoholism During the War. Monthly Journal of Psychiatry and Neurology, 1917, 41, 382-5.
Bonhoeffer, K. Die Differentialdiagnose der Hysterie und psychopathischen Konstitution gegenüber der Hebephrenie im Felde. Med. Klin., Berl. u. Wien, 1915, v. 11, pp. 877-881.
Bonhoeffer, K. The differential diagnosis of hysteria and psychopathic constitution in relation to hebephrenia in the field. Med. Klin., Berl. u. Wien, 1915, v. 11, pp. 877-881.
Bonhoeffer, K. Erfahrungen über Epilepsie und Verwandtes im Feldzüge. Monatschr. f. Psychiat. u. Neurol., Berl., 1915, v. 38, p. 61.
Bonhoeffer, K. Experiences with Epilepsy and Related Conditions in Campaigns. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, vol. 38, p. 61.
Bonhoeffer, K. Hysterischer Granatexplosionslähmung. Berl. klin. Wchnschr., 1915, v. 521, pp. 166-168.
Bonhoeffer, K. Hysterical Grenade Explosion Paralysis. Berl. Clin. Wkly, 1915, v. 521, pp. 166-168.
Bonhoeffer, K. Über meningeale Scheincysten am Rückenmark. Berl. klin. Wchnschr., 1915, v. 522, pp. 1015-1018.
Bonhoeffer, K. On meningeal pseudocysts in the spinal cord. Berl. klin. Wchnschr., 1915, v. 522, pp. 1015-1018.
Bonhoeffer, K. Psychiatrisches zum Krieg. Ztschr. f. Ärtzl. Fortbild., Jena, 1915, c. 12, pp. 1-9.
Bonhoeffer, K. Psychiatric Insights on the War. Journal of Medical Continuing Education, Jena, 1915, c. 12, pp. 1-9.
Bonhoeffer, K. Fälle von sogenannter Granatexplosionslähmung. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 73-74.
Bonhoeffer, K. Cases of so-called granatexplosion paralysis. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 73-74.
Bonhoeffer, K. Die Bedeutung der Kriegsbeschädigungen in der Psychopathologie unter besonderer Berücksichtigung der D.-B.-Frage. Med. Klin., Berl., 1916, v. 12, pp. 1301; also Deutsche med. Wchnschr., Berl. u. Leipz., 1916, v. 42, pp. 1466.
Bonhoeffer, K. The Significance of War Injuries in Psychopathology with Special Consideration of the D.-B. Question. Med. Klin., Berl., 1916, v. 12, pp. 1301; also Deutsche med. Wchnschr., Berl. u. Leipz., 1916, v. 42, pp. 1466.
Bonhoeffer, K. Erfahrungen aus dem Kriege über die Aetiologie psychopathischer Zustände. München med. Wchnschr., 1916, v. 63, pp. 1557-1558.
Bonhoeffer, K. Experiences from the war regarding the causes of psychopathic conditions. Munich Medical Weekly, 1916, v. 63, pp. 1557-1558.
Bonhoeffer, K. Fälle von hysterischer Granatexplosionslähmung. Arch. f. Psychiat., Berl., 1916, v. 56, pp. 701-702.
Bonhoeffer, K. Cases of Hysterical Granade Explosion Paralysis. Arch. f. Psychiatry, Berl., 1916, v. 56, pp. 701-702.
Bonhomme. Un cas de puérilisme mental post commotionnel. Ann. méd. psychol., Par., 1917, v. 73, pp. 384-390.
Bonhomme. A case of childishness due to post-concussion syndrome. Ann. méd. psychol., Par., 1917, v. 73, pp. 384-390.
Bonhomme et Nordmann. Caractères essentiels de la commotion cérébrospinale. Progrès méd., Par., 1916, pp. 194-196.
Bonhomme and Nordmann. Essential characteristics of cerebrospinal disturbance. Progrès méd., Paris, 1916, pp. 194-196.
Bonhomme et Nordmann. Caractères essentiels de la commotion cérébrospinale. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 530-540.
Bonhomme and Nordmann. Essential characteristics of cerebrospinal shock. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 530-540.
Bonhomme et Nordmann. Note sur deux cas de déments précoces à l’armée. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 546-549.
Bonhomme and Nordmann. Note on two cases of early dementia in the army. Ann. méd. psychol., Paris, 1916-17, v. 7, pp. 546-549.
Bonhomme et Nordmann. Un cas d’hallucinose. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 549-554.
Bonhomme and Nordmann. A case of hallucinosis. Ann. méd. psychol., Paris, 1916-17, v. 7, pp. 549-554.
Bonnier, P. L’état de guerre et les pannes nerveuses. Compt. rend. Soc. de Biol., Par., 1916, v. 75, pp. 216-218; Presse méd., Par., 1916, v. 24, p. 140.
Bonnier, P. The state of war and nervous breakdowns. Compt. rend. Soc. de Biol., Paris, 1916, vol. 75, pp. 216-218; Presse méd., Paris, 1916, vol. 24, p. 140.
Bonnier, P. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 5-6.
Bonnier, P. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, pp. 5-6.
Bonnus, G. La radiothérapie dans les affections spasmodiques de la moelle par blessures de guerre. Paris méd., 1916, (Part. Méd.), v. 19, pp. 32-35.
Bonnus, G. Radiation therapy in spasmodic conditions of the spinal cord due to war injuries. Paris méd., 1916, (Part. Méd.), v. 19, pp. 32-35.
Bonnus, Chartier et Rose. Résultats de la radiothérapie dans les traumatisme cranio-cérébraux. Lyon méd., 1917, v. 126, pp. 233-234.
Bonnus, Chartier and Rose. Results of radiotherapy in cranio-cerebral trauma. Lyon Med., 1917, v. 126, pp. 233-234.
Bonola, F. La sindrome commozionale da scoppio di projettile. Bull. d. sc. med. di Bologna, 1917, 9. s., v. 282-288. Also: Gazz. med. lomb., Milano, 1917, lxxiv, 189-192.
Bonola, F. The explosion-induced concussion syndrome. Bull. d. sc. med. di Bologna, 1917, 9. s., v. 282-288. Also: Gazz. med. lomb., Milano, 1917, lxxiv, 189-192.
Bonola, F. I disturbi psico-nervosi dei combattenti. Quaderni di psichiat., Genova, 1917, v. 4, pp. 141-156.
Bonola, F. The psychological and nerve disorders of fighters. Psychiatric notebooks, Genoa, 1917, vol. 4, pp. 141-156.
Bonola, F. Contributo allo studio delle psiconevrosi di guerra. Gior. di med. mil., Roma, 1915, lxiii, 837-841.
Bonola, F. Contribution to the study of war psychoneuroses. Mil. Med. Journal, Rome, 1915, lxiii, 837-841.
Bonola, F. (Psychoneuroses of War. A case of psychic deafness.) Gior. di med., Mil., 1915, v. 63 (Nov.).
Bonola, F. (Psychoneuroses of War. A case of psychic deafness.) Gior. di med., Mil., 1915, v. 63 (Nov.).
Borchard, A. Spätapoplexien nach Gehirnschüssen und Schadelplastiken. Centralbl. f. Chir., Leipz., 1917, 44, 650.
Borchard, A. Late apoplexies after brain injuries and skull surgeries. Centralbl. f. Chir., Leipzig, 1917, 44, 650.
Bordier, H., et Gérard, M. Ce que peut donner la radiothérapie dans les lésions nerveuses par blessures de guerre. Presse méd., Par., 1917, v. 25, pp. 453-455.
Bordier, H., and Gérard, M. What radiotherapy can provide for nerve injuries from war wounds. Méd. Press, Paris, 1917, v. 25, pp. 453-455.
Borishpolski, Ye. S. (Role of the motor area of the brain cortex in the development of epileptic attacks, based on observations on wounded.) Psikhiat. Gaz., Petrogr., 1916, v. 3, p. 119.
Borishpolski, Ye. S. (The role of the motor area of the brain cortex in the development of epileptic seizures, based on observations of injuries.) Psikhiat. Gaz., Petrogr., 1916, v. 3, p. 119.
Borne. De la rééducation et de la réadaptation au travail des blessés et des mutilés de la guerre. Rev. d’hyg., Par., 1915, v. 37, p. 81; p. 159.
Borne. On rehabilitation and reintegration into work for war casualties and amputees. Rev. d’hyg., Par., 1915, v. 37, p. 81; p. 159.
Borne. De l’assistance et de la réadaptation des malades de la guerre. Rev. d’hyg., Par., 1915, v. 37, pp. 833-849.
Borne. On the support and rehabilitation of war patients. Hyg. Rev., Par., 1915, v. 37, pp. 833-849.
Borne. De la réadaptation et de la rééducation au travail des blessés et des mutilés de la guerre. Paris méd., 1915-16, v. 17, pp. 293-298.
Borne. On rehabilitation and job retraining for wounded soldiers and war victims. Paris méd., 1915-16, v. 17, pp. 293-298.
Borovikoff, I. V. (Prisoners and those under test for insanity, and insane, in the psychiatric ward of the Riga military hospital.) Voyenno-Med. J., St. Petersb., 1914, ccxxxix, med.-spec. pt., 221-240.
Borovikoff, I. V. (Prisoners and those being evaluated for insanity, as well as those who are insane, in the psychiatric ward of the Riga military hospital.) Voyenno-Med. J., St. Petersb., 1914, ccxxxix, med.-spec. pt., 221-240.
Boschi, G. La neuropsychiatrie et la guerre. Rev. neurol., Par., 1917, v. 24, p. 474.
Boschi, G. Neuropsychiatry and War. Rev. neurol., Paris, 1917, vol. 24, p. 474.
Boschi, G. L’assistenza feminile nei reparti maschili dei manicomi durante la guerra. Atti Accad. d. sc. med. e nat. di Ferrara (1914-15), 1915-16, lxxxix, No. 2, 3-7.
Boschi, G. Women's assistance in male wards of asylums during the war. Proceedings of the Academy of Medical and Natural Sciences of Ferrara (1914-15), 1915-16, lxxxix, No. 2, 3-7.
Boschi, G. (Provision for the Care of War Neuroses and Psychoses in France.) Gior. di med., Mil., 1917, v. 65, Nov. 30.
Boschi, G. (Support for Dealing with Combat-Related Mental Health Issues in France.) Gior. di med., Mil., 1917, v. 65, Nov. 30.
Bossi, P. Il padiglione di meccanoterapia F. Ponti. Osp. Maggiore, Milano, 1916, 2 s., v. 4, pp. 144-153.
Bossi, P. The pavilion of mechanotherapy F. Ponti. Osp. Maggiore, Milan, 1916, 2 s., v. 4, pp. 144-153.
Bostroem, A. Zur Psychologie u. Klinik der psychogenen Hörstörungen. Ztschr. f. d. ges. Neurol. u. Psychiat., 40, 1918.
Bostroem, A. On the Psychology and Clinic of Psychogenic Hearing Disorders. Journal of General Neurology and Psychiatry, 40, 1918.
Bott, E. A. Rehabilitation of wounded Canadian soldiers. Mod. Hosp., 1917, ix, 365.
Bott, E. A. Rehabilitation of injured Canadian soldiers. Mod. Hosp., 1917, ix, 365.
Boucherot, F. M. A. Maladies mentales dans l’armée en temps de guerre. Thèses de Paris., 1915-16, No. 37, v. 2.
Boucherot, F. M. A. Mental illnesses in the army during wartime. Thesis from Paris., 1915-16, No. 37, v. 2.
Bouquet, Henri. La rééducation des mutilés de la guerre. Bull. gén. de thérap., Par., 1916, v. 85, pp. 156-181; pp. 193-213.
Bouquet, Henri. The Rehabilitation of War Injured. Gen. Bull. of Therapy, Par., 1916, v. 85, pp. 156-181; pp. 193-213.
Bouquet. Deux cas de tétanos localisé tardif. Bull. gén. de thérap., Par., 1916, v. 168, pp. 814-817.
Bouquet. Two cases of late localized tetanus. Bull. gén. de thérap., Paris, 1916, v. 168, pp. 814-817.
Bourgeois, H. and Sourdille. Otites et surdités de guerre. Collection Horizon, Masson et Cie., Paris, 1917.
Bourgeois, H. and Sourdille. War-related Ear Infections and Deafness. Horizon Collection, Masson et Cie., Paris, 1917.
Bourgeois, H. and Sourdille. War Otitis and War Deafness. Military Medical Manuals, Univ. of London Press, 1918.
Bourgeois, H. and Sourdille. War Otitis and War Deafness. Military Medical Manuals, University of London Press, 1918.
Bourgeois, A. Traumatismes graves de l’oeil par blessures de guerre dans lésions immédiatement apparentes. Arch. d’ophth., Par., 1914-15, v. 34, pp. 766-769.
Bourgeois, A. Serious eye trauma from war injuries with immediate visible damage. Arch. d’ophth., Par., 1914-15, v. 34, pp. 766-769.
Bourillon. Comment rééduquer nos invalides de la guerre: l’assistance aux estropiés et aux inutilés en Danemark, Suède, et Norvège. Collection Horizon, Masson et Cie, 1916.
Bourillon. How to rehabilitate our war invalids: assistance for the disabled and the unfit in Denmark, Sweden, and Norway. Horizon Collection, Masson et Cie, 1916.
Bourillon. Functional readaptation and professional reëducation of the disabled victims of the war. Amer. Jour. Care for Crip., 1916, iii, 23.
Bourillon. Functional readaptation and professional reeducation of disabled victims of the war. Amer. Jour. Care for Crip., 1916, iii, 23.
Bourillon. The vocational re-education of disabled soldiers. Mil. Hosp. Com. Canada, Spec. Bull., Ottawa, 1916, pp. 77-89.
Bourillon. The vocational retraining of disabled soldiers. Mil. Hosp. Com. Canada, Spec. Bull., Ottawa, 1916, pp. 77-89.
Boven. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 4-5.
Boven. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 4-5.
Boveri, P. Di alcune questioni medico-legali in rapporto alla guerra; le nevrosi. Riv. crit. in materia di infortuni (etc.), Roma, 1916, v. 5, pp. 33-35.
Boveri, P. On some medico-legal issues related to the war; neuroses. Crit. Rev. on injury matters (etc.), Rome, 1916, vol. 5, pp. 33-35.
Brackenbury, H. B. Discharged disabled soldiers and sailors. Brit. M. J., Lond., 1917, v. 2, p. 437.
Brackenbury, H. B. Discharged disabled soldiers and sailors. Brit. M. J., Lond., 1917, v. 2, p. 437.
Braquehaye. Section du nerf médian droit. Suture immédiate du nerf. Retour partiel des fonctions. Reunion med. de la VI armée, Nov.-Dec. 1915.
Braquehaye. Right median nerve section. Immediate nerve suture. Partial return of functions. Medical reunion of the VI army, Nov.-Dec. 1915.
Brasch. Herzneurosen mit Hauthyperästhesie. Med. klin., Berl. u. Wien., 1915, v. 111, pp. 627.
Brasch. Heart neuroses with skin hypersensitivity. Med. klin., Berlin and Vienna, 1915, v. 111, pp. 627.
Braunschweig. Kurze Mitteilungen über die epidemische Hemeralopie im Felde. Med. Klin., Berl. u. Wien., 1915, v. 111, pp. 313-314.
Braunschweig. Brief communications on the epidemic hemeralopia in the field. Med. Klin., Berl. u. Wien., 1915, v. 111, pp. 313-314.
Bresler. Schädel- und Gehirnverletzungen (Bib.) C. Marhold, Halle, 1917.
Bresler. Skull and brain injuries (Bib.) C. Marhold, Halle, 1917.
Briand, Marcel. Les toxicomanes et la mobilisation. Presse méd., Par., 1914, v. 22, pp. 751-752.
Briand, Marcel. Addicts and Mobilization. Medical Press, Paris, 1914, v. 22, pp. 751-752.
Briand, Marcel. Les fugueurs à l’armée. Soc. de méd. lég. de France, Bull., Par., 1915, v. 12, pp. 42-63.
Briand, Marcel. The Evaders in the Army. Soc. de méd. lég. de France, Bull., Paris, 1915, vol. 12, pp. 42-63.
Briand, Marcel. Les comitiaux à l’armée. Soc. de méd. lég. de France, Bull., Par., 1915, v. 12, pp. 196-202.
Briand, Marcel. The Committees in the Army. Soc. de méd. lég. de France, Bull., Par., 1915, v. 12, pp. 196-202.
Briand, Marcel. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 470.
Briand, Marcel. Discussion on how to approach skull injuries—by P. Marie. Neurological Review, Paris, 1916, vol. 29, p. 470.
Briand, Marcel. Troubles organiques d’origine fonctionnelle chez les militaires commotionnés. Ann. méd.-psychol., Par., 1917, v. 73, pp. 577-582.
Briand, Marcel. Functional Organic Disorders in Concussed Soldiers. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 577-582.
Briand, Marcel et Delmas. Sur la liquidation des indemnités aux militaires “persévérateurs” atteints de troubles fonctionnels hystériques. Soc. méd. lég. de France, Par., 1917, v. 14, pp. 223-233.
Briand, Marcel and Delmas. On the Settlement of Compensation for Military "Perseverators" Experiencing Hysterical Functional Disorders. Med. Leg. Soc. of France, Paris, 1917, v. 14, pp. 223-233.
Briand et Haury. Rôle de la complicité dans la simulation ou la provocation des maladies. Soc. de méd. lég. de France, Bull., Par., 1916, v. 13, pp. 51-59.
Briand and Haury. The role of complicity in simulating or provoking diseases. Soc. of legal medicine of France, Bull., Paris, 1916, vol. 13, pp. 51-59.
Briand et Kalt. Maladies simulées et maladies provoquées dans l’armée. Soc. de méd. lég. de France, Bull., Par., 1917, v. 14, pp. 42-48.
Briand and Kalt. Simulated illnesses and induced illnesses in the military. Soc. de méd. lég. de France, Bull., Paris, 1917, vol. 14, pp. 42-48.
Briand, Marcel et Philippe, Jean. L’audi-mutité rebelle, d’origine émotionelle. Progrès Méd., Par., 1916, No. 17, pp. 145-148.
Briand, Marcel and Philippe, Jean. The Rebellious Audi-Muteness, of Emotional Origin. Progress Med., Paris, 1916, No. 17, pp. 145-148.
Brickley, C. W. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-1918, v. 10 (sect. Balneol.), pp. 36-37.
Brickley, C. W. Treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-1918, v. 10 (sect. Balneol.), pp. 36-37.
Briggs, L. V. A plea for more psychiatrists and neurologists for war service. Proc. Alienists and Neurol. Am., Chicago, 1917, v. 6, p. 31.
Briggs, L. V. A request for additional psychiatrists and neurologists for military service. Proc. Alienists and Neurol. Am., Chicago, 1917, v. 6, p. 31.
Broca, Aug. Troubles locomoteurs consécutifs aux plaies de guerre. Collection Horizon, Masson et Cie, Paris, 1918.
Broca, Aug. Consequences of War Injuries on Movement Disorders. Collection Horizon, Masson et Cie, Paris, 1918.
Broca, A. et Ducsoquet. La prothèse des amputés en chirurgie de guerre. 1917, Paris, Masson and Cie.
Broca, A. and Ducsoquet. The Prosthesis for Amputees in War Surgery. 1917, Paris, Masson and Cie.
Brock, A. J. The war neurasthenic. Lancet, Lon., 1918, i, 436.
Brock, A. J. The war neurasthenic. Lancet, Lon., 1918, i, 436.
Brock, L. G. Reëducation of the disabled. Amer. Jour. Care for Crip., 1917, iv, 19.
Brock, L. G. Reeducation of the disabled. Amer. Jour. Care for Crip., 1917, iv, 19.
Brocq. Influence de la guerre sur les affections cutanées. Bull. méd., 1916, No. 3.
Brocq. Influence of war on skin conditions. Med Bull, 1916, No. 3.
Brodman, K. Zur Neurologie der Stirnhirnschüsse. München med. Wchnschr., 1915, v. 622, p. 1120.
Brodman, K. On the Neurology of Frontal Lobe Injuries. Munich Med. Weekly, 1915, v. 622, p. 1120.
Brousses, J. Une mécanothérapie de fortune à l’hôpital complémentaire No. 31 de Toulouse. Arch. de méd. et pharm. mil., Par., 1914-15, v. 64, pp. 177-185.
Brousses, J. A makeshift mechanotherapy at the complementary hospital No. 31 in Toulouse. Arch. de méd. et pharm. mil., Par., 1914-15, v. 64, pp. 177-185.
Brovchinski, A. V. (Case of nervous symptom complex due to wind contusion.) Psikhiat. Gaz., Petrogr., 1916, pp. 237-240.
Brovchinski, A. V. (Case of nervous symptom complex due to wind injury.) Psychiatric Journal, St. Petersburg, 1916, pp. 237-240.
Brovchinski, A. V. (Paraplegia in atmospheric contusion.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 394-398.
Brovchinski, A. V. (Paraplegia from atmospheric contusion.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 394-398.
Brown, H. E. Head, abdominal and joint injuries; notes on cases. Lancet, Lon., 1916, i, 1082.
Brown, H. E. Head, abdominal, and joint injuries; notes on cases. Lancet, Lon., 1916, i, 1082.
Brown, Mabel W. and Williams, Frankwood E. Neuropsychiatry and the War, 1918.
Brown, Mabel W. and Williams, Frankwood E. Neuropsychiatry and the War, 1918.
Brown, Mabel W. and Williams, F. E. Neuropsychiatry and the War; a bibliography with abstracts. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 409-474.
Brown, Mabel W. and Williams, F. E. Neuropsychiatry and the War; a bibliography with summaries. Mental Hygiene, Concord, NH, 1917, vol. 1, pp. 409-474.
Brown, William. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-1916 (sect. Psychiat.), pp. 301-32.
Brown, William. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-1916 (sect. Psychiat.), pp. 301-32.
Bruce, Ninian. The Treatment of Functional Blindness and Functional Loss of Voice. Rev. Neurol. and Psychiat., Edinb., 1916, v. 14, pp. 195-198.
Bruce, Ninian. The Treatment of Functional Blindness and Functional Loss of Voice. Rev. Neurol. and Psychiat., Edinb., 1916, v. 14, pp. 195-198.
Brunig, F. Ueber grosse lufthaltige Gehirncyste nach Schussverletzung. Bruns’ Kriegschir. Hefte d. Beitr. z. klin. Chir., Tübing., 1917, 107, 432.
Brunig, F. About large air-filled brain cysts after gunshot wounds. Bruns’ War Surgery. Contributions to Clinical Surgery, Tübingen, 1917, 107, 432.
Bruns, L. Kriegsneurologische Beobachtungen und Betrachtungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 12-15.
Bruns, L. Observations and Reflections on War Neurology. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 12-15.
Bucky. Diathermia in den Lazaretten. Deut. Med. Woch., 1915, xli, 467.
Bucky. Diathermy in the hospitals. Deut. Med. Woch., 1915, xli, 467.
Bulletins. Federal Board for Vocational Education. Nos. 1-10, 1917-1918. Washington Government Printing Office.
Bulletins. Federal Board for Vocational Education. Nos. 1-10, 1917-1918. Washington Government Printing Office.
Bunnemann. Zur traumatische Neurose im Kriege. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 888-898.
Bunnemann. On traumatic neurosis in war. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 888-898.
Bunnemann. Die Neurosenfrage und das biologische Grundgesetz. Neurol. Centralbl., Leipz., 1916, v. 35, pp. 178-187.
Bunnemann. The Neurosis Question and the Biological Fundamental Law. Neurol. Centralbl., Leipzig, 1916, v. 35, pp. 178-187.
Bunse, P. Die reaktiven Dämmerzustände u. verwandte Störungen in ihrer Bedeutung als Kriegspsychosen. Ztschr. f. d. ges. Neurol. u. Psych., 40, 1918.
Bunse, P. The Reactive Twilight States and Related Disorders in Their Significance as War Psychoses. Journal of General Neurology and Psychology, 40, 1918.
Burke, Noel H. M. Electrotherapy in Military Hospitals. Arch. Radial. and Elec., Lond., 1917, Oct., pp. 130-135.
Burke, Noel H. M. Electrotherapy in Military Hospitals. Arch. Radial. and Elec., Lond., 1917, Oct., pp. 130-135.
Burniston, Hugh S. Notes on a successful case of treatment by suggestion. J. Roy. Nav. M. Serv., Lond., 1917, v. 3, pp. 116-117.
Burniston, Hugh S. Notes on a successful case of treatment through suggestion. J. Roy. Nav. M. Serv., Lond., 1917, v. 3, pp. 116-117.
Burton-Fanning, F. W. Neurasthenia in soldiers of the home forces. Lancet, Lond., 1917, v. 1, pp. 907-911.
Burton-Fanning, F. W. Neurasthenia in soldiers of the home forces. Lancet, Lond., 1917, v. 1, pp. 907-911.
Burton-Fanning, F. W. Neurasthenia in soldiers of the home forces. Lancet, Lon., 1917, i, 907.
Burton-Fanning, F. W. Neurasthenia in soldiers of the home forces. Lancet, Lon., 1917, i, 907.
Bury, J. S. Distant effects of rifle bullets, with special reference to the spinal cord. Brit. Med. Jour., 1916, ii, 212.
Bury, J. S. Distant effects of rifle bullets, with special reference to the spinal cord. Brit. Med. Jour., 1916, ii, 212.
Busacchi, A. Edemi pseudo-traumatici della man. Bull. d. sc. med. di Bologna, 1917, 9. s., v. 345-355.
Busacchi, A. Pseudo-traumatic injuries of the hand. Bull. d. sc. med. di Bologna, 1917, 9. s., v. 345-355.
Buscaino, V. M. and Coppola, A. Disturbi mentale in tempo di guerra. Riv. di patol. nerv., Firenze, 1916, v. 21, pp. 1-103; also pp. 135-182.
Buscaino, V. M. and Coppola, A. Mental Disorders in Wartime. Riv. di patol. nerv., Florence, 1916, vol. 21, pp. 1-103; also pp. 135-182.
Buschan, Georg. Über Kriegspsychosen. Med. Klin., Berl. u. Wien, 1914, v. 102, pp. 1588-1591.
Buschan, Georg. On War Psychoses. Med. Klin., Berlin and Vienna, 1914, v. 102, pp. 1588-1591.
Butenko, A. A. (The War and Mental Diseases in Women.) Obozr. Psikhiat., Neurol. (etc.), Petrogr., 1914-1915, v. 19, pp. 521-542.
Butenko, A. A. (The War and Mental Diseases in Women.) Obozr. Psikhiat., Neurol. (etc.), Petrogr., 1914-1915, v. 19, pp. 521-542.
Butt, A. P. Destruction of the spinal cord by molecular vibration. Surg., Gynec. and Obst., Chicago, 1915, xx, 486.
Butt, A. P. Destruction of the spinal cord by molecular vibration. Surg., Gynec. and Obst., Chicago, 1915, xx, 486.
Buttersack. Zur Casuistik der Kriegsneurosen. Med. Cor.-Bl. d. würtemb. ärztl. Landesver., Stuttg., 1916, v. 86, pp. 1-5.
Buttersack. On the Case Studies of War Neuroses. Med. Cor.-Bl. d. würtemb. ärztl. Landesver., Stuttg., 1916, v. 86, pp. 1-5.
Buzzard, E. Farquhar. “Warfare on the Brain.” Lancet, Lond., 1916, ii, pp. 1095-1099.
Buzzard, E. Farquhar. “Warfare on the Brain.” Lancet, London, 1916, ii, pp. 1095-1099.
Call, Annie P. Nerves and the war. 1918.
Call, Annie P. Nerves and the War. 1918.
Calot, F. Orthopédie de guerre; appareil pour fractures, etc. Paris, 1916, A. Maloine et fils, p. 100, 8o.
Calot, F. War Orthopedics; Device for Fractures, etc. Paris, 1916, A. Maloine et fils, p. 100, 8o.
Cadenat, F. M. Le pronostic des fractures du crâne par projectiles. Paris méd., 1915 (Part. Méd.), v. 17, pp. 437-44.
Cadenat, F. M. The prognosis of skull fractures from projectiles. Paris med., 1915 (Part. Med.), v. 17, pp. 437-44.
Campbell, A. W. Remarks on some neuroses and psychoses in war. M. J. Australia, Sydney, 1916, i, pp. 319-323.
Campbell, A. W. Comments on certain neuroses and psychoses related to war. M. J. Australia, Sydney, 1916, i, pp. 319-323.
Campbell, Harry. War neuroses. Practitioner, Lond., 1916, v. 96, pp. 501-509.
Campbell, Harry. War neuroses. Practitioner, London, 1916, vol. 96, pp. 501-509.
Camus, J. L’évaluation des incapacités fonctionnelles. Paris méd., 1916-17, (Part. Méd.), v. 21, pp. 289-297.
Camus, J. The Evaluation of Functional Disabilities. Paris Med., 1916-17, (Part. Med.), v. 21, pp. 289-297.
Camus, J. Le corps de rééducation physique du Grand-palais. (Dépot de physiothérapie). Arch. de méd. et pharm., mil., Par., 1916, v. 65, pp. 365-410.
Camus, J. The Physical Rehabilitation Body of the Grand Palace. (Physiotherapy Depot). Arch. de méd. et pharm., mil., Par., 1916, v. 65, pp. 365-410.
Camus, J. Les sourds, leur placement, leurs intérèts economiques et sociaux. Presse méd., Par., 1917, v. 25, pp. 309.
Camus, J. The deaf, their placement, their economic and social interests. Med Press, Paris, 1917, v. 25, pp. 309.
Camus, J. La rééducation des aveugles de guerre. Presse méd., Par., 1917, v. 25, p. 309.
Camus, J. The Rehabilitation of War Blind. Medical Press, Paris, 1917, v. 25, p. 309.
Camus, J. Placement et rééducation des grands infirmes par lésions des centres nerveux. Paris méd., 1917, No. 27, pp. 1-5.
Camus, J. Placement and rehabilitation of severely disabled individuals due to nervous system injuries. Paris Med., 1917, No. 27, pp. 1-5.
Camus, J. et Nepper. Recherches sur les réactions psychomotrices et émotives des anciens trépanés. Rev. neurol., Par., 1916, v. 29, pp. 923-924.
Camus, J. and Nepper. Research on the psychomotor and emotional reactions of ancient trepanned individuals. Neurology Review, Paris, 1916, vol. 29, pp. 923-924.
Capelle, W. Über Prognose und Therapie der Schädelchüsse. München. Med. Wchnschr., 1917, 64, Nr. 8.
Capelle, W. On the Prognosis and Treatment of Skull Fractures. Munich. Med. Wchnschr., 1917, 64, No. 8.
Capgras, Juquelier et Bonhomme. La confusion mentale de guerre. J. de méd. de Bordeaux, 1917, v. 88, pp. 164-165. Rev. Progrès méd., Par., 1917, v. 43, p. 355.
Capgras, Juquelier and Bonhomme. The mental confusion of war. J. de méd. de Bordeaux, 1917, vol. 88, pp. 164-165. Rev. Progrès méd., Paris, 1917, vol. 43, p. 355.
Cardgill, L. V. Recent work on ophthalmology. Practitioner, Lond., 1916, v. 97, p. 44.
Cardgill, L. V. Recent work on ophthalmology. Practitioner, London, 1916, vol. 97, p. 44.
Carle, M. Vocational schools for war cripples in France. Amer. Jour., Care for Crip., 1917, v, 165.
Carle, M. Vocational schools for war veterans with disabilities in France. Amer. Jour., Care for Crip., 1917, v, 165.
Carle, M. Les écoles professionnelles de blessés à Lyon. Par., 1915, p. 132, 8o.
Carle, M. The vocational schools for the injured in Lyon. Par., 1915, p. 132, 8o.
Carlill, Hildred. The diagnostic importance of ankle-jerk. J. Roy. Nav. Med. Serv., Lond., 1916, ii, pp. 180-190.
Carlill, Hildred. The diagnostic importance of ankle-jerk. J. Roy. Nav. Med. Serv., Lond., 1916, ii, pp. 180-190.
Carlill, Hildred. Korsakow’s psychosis in association with malaria. Lancet, Lond., 1917, i, v. 192, pp. 648-650.
Carlill, Hildred. Korsakow’s psychosis linked to malaria. Lancet, Lond., 1917, i, v. 192, pp. 648-650.
Carlill, Fildes and Baker. A report on cases of syphilis of the central nervous system observed in the Neurological Department of Royal Naval Hospital, Haslar, during twelve months. J. Roy. Nav. Med. Serv., Lond., 1917, v. 3, pp. 397-427.
Carlill, Fildes, and Baker. A report on cases of syphilis affecting the central nervous system observed in the Neurological Department of the Royal Naval Hospital, Haslar, over twelve months. J. Roy. Nav. Med. Serv., Lond., 1917, v. 3, pp. 397-427.
Cas remarquable de protection crânienne par le casque. Lyon méd., 1916, v. 125, pp. 259-261.
Remarkable case of skull protection by helmet. Lyon méd., 1916, v. 125, pp. 259-261.
Case of Emotional Mutism. Brit. M. J., Lond., 1916, i, p. 769.
Case of Emotional Mutism. Brit. M. J., Lond., 1916, i, p. 769.
Cases of neurasthenia and mental shock. Mod. Hosp., St. Louis, 1917, ix, 368.
Cases of neurasthenia and mental shock. Mod. Hosp., St. Louis, 1917, ix, 368.
Caspari, J. Klinische Beiträge zur Differentialdiagnose zwischen Epilepsie und Hysterie aus den Erfahrungen des gegenwärtigen Krieges. Inaug-Dissert., Berlin, 1916.
Caspari, J. Clinical Contributions to the Differential Diagnosis between Epilepsy and Hysteria Based on Experiences from the Current War. Inaugural Dissertation, Berlin, 1916.
Cassirer. Demonstration eines Falles von Erythromelalgie. Berl. klin. Wchnschr., 1915, v. 421, p. 168.
Cassirer. Demonstration of a case of erythromelalgia. Berl. klin. Wchnschr., 1915, v. 421, p. 168.
Cassirer. Demonstration von Verwundeten mit erfolgreicher Nervennaht. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 284-287.
Cassirer. Demonstration of wounded individuals with successful nerve suturing. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 284-287.
Cassirer. Über Kombination funktioneller und organischer Symptome bei Kriegsverletzungen. Ztschr. f. d. ges. Neurol. Psychiat., Berl. u. Leipz., 1916, v. 30, p. 229.
Cassirer. On the combination of functional and organic symptoms in war injuries. Journal of General Neurology and Psychiatry, Berlin and Leipzig, 1916, vol. 30, p. 229.
Castex, André. Surdités de guerre. Bull. acad. de méd., Par., 1915, v. 74, pp. 547-548.
Castex, André. War Deafness. Bull. acad. de méd., Paris, 1915, vol. 74, pp. 547-548.
Castex, André. La rééducation des sourds de guerre. (Présentation de militaires rééduqués.) Bull. Acad, de méd., Par., 1917, v. 77, p. 817.
Castex, André. The Rehabilitation of War Veterans with Hearing Loss. (Introduction of rehabilitated soldiers.) Bull. Acad, de méd., Par., 1917, v. 77, p. 817.
Catalepsie “post mortem.” Caducée, Par., 1916, v. 16, p. 101.
Post-mortem Catalepsy. Caducée, Paris, 1916, vol. 16, p. 101.
Cathelin, F. Classifications des troubles sphinctériens avec les blessures ou commotions de la région lombo-sacrée. Paris méd., 1917, No. 42, pp. 319-323.
Cathelin, F. Classifications of sphincter disorders with injuries or concussions of the lumbosacral region. Paris méd., 1917, No. 42, pp. 319-323.
Catola, G. Neuropatologia di guerra; le ferite dei nervi periferici. Riv. di patol. nerv., Firenze, 1915, v. 20, pp. 533-554.
Catola, G. Neuropathology of War; Injuries to Peripheral Nerves. J. of Nerv. Pathol., Florence, 1915, vol. 20, pp. 533-554.
Catola, G. A proposito di alcune sindromi nervose funzionali di guerra con considerazioni in rapporti alla simulazione nelle sue varie forme. Riv. di patol. nerv., Firenze, 1916, v. 21, pp. 662-675.
Catola, G. Regarding some functional nerve syndromes of war with considerations on simulation in its various forms. Rev. of nerve pathology, Florence, 1916, v. 21, pp. 662-675.
Cestan. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 465-466.
Cestan. Discussion on how to deal with skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, pp. 465-466.
Cestan; Descomps, Paul; et Sauvage, Roger. Les troubles de l’équilibre dans les commotions crâniennes. Paris méd., 1916 (Part. Méd.), v. 19, pp. 518-525.
Cestan; Descomps, Paul; and Sauvage, Roger. Balance disorders in concussions. Paris Med., 1916 (Med. Part.), v. 19, pp. 518-525.
Cestan, R.; Descomps, Paul; Euzière, J. Les empreintes digitales dans les lésions nerveuses du membre supérieur. Leur application au diagnostic des névrites traumatiques. Presse méd., Par., 1916, v. 24, pp. 258-262.
Cestan, R.; Descomps, Paul; Euzière, J. Fingerprints in Nerve Injuries of the Upper Limb. Their Application to the Diagnosis of Traumatic Neuritis. Med. Press, Paris, 1916, v. 24, pp. 258-262.
Cestan, Descomps, P., et al. “La marche sous courant galvanique” chez les commotionnés et les traumatismes du crâne. Bull. et mém. Soc. méd. d’hôp. de Par., 1916, v. 32, pp. 1730-1747.
Cestan, Descomps, P., et al. “Walking under galvanic current” in individuals with concussions and skull injuries. Bull. et mém. Soc. méd. d’hôp. de Par., 1916, v. 32, pp. 1730-1747.
Cestan, Descomps P., Euzière, J. et Sauvage, R. Troubles de la sensibilité d’origine corticale à disposition pseudo-radiculaire en épilepsie Jacksonnienne. Rev. neurol., Par., 1917, v. 24, pp. 235-242.
Cestan, Descomps P., Euzière, J. and Sauvage, R. Cortical sensitivity disorders with pseudo-radicular symptoms in Jacksonian epilepsy. Rev. neurol., Paris, 1917, vol. 24, pp. 235-242.
Cestan, Descomps, P., et Sauvage, R. Sur une nouvelle méthode d’exploration du sens de l’orientation et de l’équilibre chez les traumatismes du crâne. La[917] sensibilisation à l’épreuve de Babinski-Weill. (Rev. Neurol., Par., 1917, p. 368) Bull. et mém. Soc. méd. d’hôp. de Par., 1916, v. 32, pp. 1381-1403.
Cestan, Descomps, P., and Sauvage, R. On a new method for exploring orientation and balance in cases of head trauma. The[917] sensitization in the Babinski-Weill test. (Rev. Neurol., Paris, 1917, p. 368) Bull. and mém. Soc. méd. d’hôp. de Paris, 1916, vol. 32, pp. 1381-1403.
Chalier, A. et Chalier, J. Des phlegmons provoqués chez les soldats. Rev. internat. de méd. et de chir., Par., 1914-16, v. 25, pp. 277-281.
Chalier, A. and Chalier, J. On the cellulitis caused in soldiers. Int. Rev. of Med. and Surgery, Paris, 1914-16, vol. 25, pp. 277-281.
Chalier, A. and Glénard, R. Grandes blessures de guerre. Rev. de Chir., 1916, li, 210.
Chalier, A. and Glénard, R. Major War Injuries. Rev. de Chir., 1916, li, 210.
Chamberlin, J. W. Injuries in modern warfare. Boston M. and S. J., 1917, i, p. 113; also p. 116.
Chamberlin, J. W. Injuries in modern warfare. Boston M. and S. J., 1917, i, p. 113; also p. 116.
Chapin, F. Stuart. The training school of psychiatric social work at Smith College. IV. A scientific basis for training social workers. Mental Hygiene, II, October, 1918.
Chapin, F. Stuart. The training school for psychiatric social work at Smith College. IV. A scientific basis for training social workers. Mental Hygiene, II, October, 1918.
Charon, R. Psychopathologie de guerre. Progrès méd., Par., 1914, v. 30, pp. 425-428.
Charon, R. War Psychopathology. Med Progress, Paris, 1914, vol. 30, pp. 425-428.
Charon, R. et Halberstadt, G. Puérilisme mental au cours d’une psychose postcommotionnelle. Rev. neurol., Par., 1916, v. 24, pp. 316-319.
Charon, R. and Halberstadt, G. Mental infantilism during post-concussion psychosis. Rev. neurol., Paris, 1916, v. 24, pp. 316-319.
Charon, R. et Halberstadt, G. Les troubles psychiques des commotionnés. Paris méd., 1917, No. 27, pp. 23-32.
Charon, R. and Halberstadt, G. The psychological issues of concussed individuals. Paris méd., 1917, No. 27, pp. 23-32.
Charpentier, R. Un cas de puérilisme mental au cours des opérations de guerre. Rev. neurol., Par., 1917, v. 24, pp. 296-306.
Charpentier, R. A case of mental childlike behavior during wartime operations. Rev. neurol., Par., 1917, v. 24, pp. 296-306.
Chartier, M. Un cas de paralysie hystérique persistant chez un sujet en danger de mort par immersion. Rev. neurol., Par., 1914-15, v. 222, pp. 1241-1245.
Chartier, M. A case of persistent hysterical paralysis in a person at risk of drowning. Rev. neurol., Par., 1914-15, v. 222, pp. 1241-1245.
Chatelin and de Martel. Blessures du crâne et du cerveau. (Collection Horizon), Paris, 1917.
Chatelin and de Martel. Skull and brain injuries. (Horizon Collection), Paris, 1917.
Chatelin, C. and De Martel, T. Wounds of the Skull and Brain. Military Medical Manuals, Univ. of London Press, 1918.
Chatelin, C. and De Martel, T. Wounds of the Skull and Brain. Military Medical Manuals, Univ. of London Press, 1918.
Chauvin, H. et Heiser. À propos d’un cas de tétanos monoplégique. Rev. neurol., Par., 1917, v. 24, p. 445.
Chauvin, H. and Heiser. Regarding a case of monoplegic tetanus. Neurol. Rev., Paris, 1917, vol. 24, p. 445.
Chavanne, F. Les sourds, leur placement, leurs intérêts économiques et sociaux. Presse méd., Par., 1917, v. 25, p. 309.
Chavanne, F. The Deaf, Their Placement, and Their Economic and Social Interests. Medical Press, Paris, 1917, vol. 25, p. 309.
Chavigny, P. Étude médico-légale sur les mutilations volontaires par coup de feu. Soc. de méd. légal de France, Bull., Par., 1915, v. 12, pp. 209-222.
Chavigny, P. Medical-Legal Study on Intentional Mutilation by Gunshot. Society of Forensic Medicine of France, Bulletin, Paris, 1915, vol. 12, pp. 209-222.
Chavigny, P. Les réformes et l’aptitude au service militaire. Soc. de méd. lég. de France, Bull., Par., 1915, v. 12, pp. 253-260.
Chavigny, P. Reforms and Military Service Readiness. Society of Legal Medicine of France, Bulletin, Paris, 1915, vol. 12, pp. 253-260.
Chavigny, P. Phlegmons provoqués par injection sous-cutanée d’essence de térébenthine, de pétrole ou d’essence de pétrole. Soc. de méd. lég. de France, Bull., Par., 1915, v. 12, pp. 274-284.
Chavigny, P. Phlegmons caused by subcutaneous injection of turpentine, petroleum, or gasoline. Soc. de méd. lég. de France, Bull., Par., 1915, v. 12, pp. 274-284.
Chavigny, P. Psychiatrie et médecine légale aux armées. Paris méd., 1915, (part. méd.), v. 17, pp. 184-189.
Chavigny, P. Psychiatry and Forensic Medicine in the Military. Paris Med., 1915, (Med. Part.), vol. 17, pp. 184-189.
Chavigny, P. À propos des mutilations volontaires doit-on le dire? Paris méd., 1915 (part. méd.), v. 17, pp. 384-387.
Chavigny, P. On the subject of voluntary mutilations, should we say it? Paris méd., 1915 (part. méd.), v. 17, pp. 384-387.
Chavigny, P. Psychiatrie des armées. Paris méd., 1915 (part. méd.) v. 17, pp. 415-423.
Chavigny, P. Military Psychiatry. Paris méd., 1915 (part. méd.) v. 17, pp. 415-423.
Chavigny, P. Étude médico-légale sur les mutilations volontaires par coup de feu. Ann. d’hyg., Par., 1915, v. 24, pp. 5-21.
Chavigny, P. Medical-Legal Study on Intentional Mutilations by Gunshot. Ann. d’hyg., Par., 1915, v. 24, pp. 5-21.
Chavigny, P. Psychiatrie aux armées. Thérapeutique et médecine légale. Paris méd., 1916 (part. méd.), v. 19, pp. 8-13.
Chavigny, P. Military Psychiatry. Therapeutics and Forensic Medicine. Paris Med., 1916 (med. part), vol. 19, pp. 8-13.
Chavigny, P. Les maladies méconnues. Anesthésies et analgésies hystériques. Paris méd., 1916 (part. méd.), v. 19, pp. 214-215.
Chavigny, P. Unknown Diseases. Anesthesias and Hysterical Analgesias. Paris Méd., 1916 (Part. Méd.), Vol. 19, pp. 214-215.
Chavigny, P. Maladies provoquées ou simulées en temps de guerre. Paris méd., 1916 (part. méd.), v. 21, pp. 150-153.
Chavigny, P. Diseases Caused or Faked During Wartime. Paris Med., 1916 (part. med.), v. 21, pp. 150-153.
Chavigny, P. Les explosions des champs de bataille. Ann. d’hyg., Par., 1916, v. 25, pp. 5-25.
Chavigny, P. The Explosions of the Battlefields. Ann. d’hyg., Paris, 1916, v. 25, pp. 5-25.
Chavigny, P. La complicité dans la simulation et la provocation des maladies. Soc. de méd. lég. de France, Bull., Par., 1916, v. 13, pp. 74-76.
Chavigny, P. The complicity in simulating and provoking illnesses. Soc. de méd. lég. de France, Bull., Par., 1916, v. 13, pp. 74-76.
Chavigny, P. Présentation d’un blessé atteint de monoplégie hystérique. Presse méd., Par., 1917, v. 25, p. 193.
Chavigny, P. Presentation of a patient with hysteria-related monoplegia. Med Press, Paris, 1917, v. 25, p. 193.
Chavigny, P. Un fugueur pendant la guerre. Presse méd., Par., 1917, No. 31, P 326.
Chavigny, P. A runaway during the war. Medical Press, Paris, 1917, No. 31, P 326.
Chavigny, P. Un cas de dipsomanie. Presse méd., Par., 1917, v. 25, p. 502.
Chavigny, P. A Case of Dipsomania. Medical Press, Paris, 1917, v. 25, p. 502.
Chavigny, P. Les maladies rares et le diagnostic de la simulation. Un cas de “tic de la marche.” Caducée, Par., 1917, v. 17, pp. 45-49.
Chavigny, P. Rare diseases and the diagnosis of simulation. A case of “gait tic.” Caducée, Paris, 1917, vol. 17, pp. 45-49.
Chavigny et Laurens. Un fugueur pendant la guerre. Rev. neurol., Par., 1917, v. 24, p. 486.
Chavigny and Laurens. A runaway during the war. Rev. neurol., Paris, 1917, v. 24, p. 486.
Chavigny et Spillman, L. Un cas de hystéro-traumatisme revu 15 ans après les accidents initiaux. Paris méd., 1916 (part. méd.) v. 19, pp. 525-527.
Chavigny et Spillman, L. A case of hystero-trauma reviewed 15 years after the initial incidents. Paris méd., 1916 (med. part) v. 19, pp. 525-527.
Chevallier. Installation et résultats du service de rééducation physique et massage au cantonnement de Villetaneuse occupé par le Ne régiment de Zouaves. Arch, de méd. et pharm. mil., Par., 1916, v. 65, pp. 411-433.
Chevallier. Setup and outcomes of the physical rehabilitation and massage service at the Villetaneuse camp occupied by the 5th Zouave Regiment. Arch, de méd. et pharm. mil., Paris, 1916, vol. 65, pp. 411-433.
Chevallier, Paul. Traitement pratique de la blennorragie chez l’homme. Presse méd., Par., 1917, v. 25, pp. 573-574.
Chevallier, Paul. Practical Treatment of Gonorrhea in Men. Med Press, Paris, 1917, vol. 25, pp. 573-574.
Chevalier-Lavaure. A propos de la réforme des militaires aliénés. Montpel. méd., 1916, n.s., v. 39, pp. 418-427.
Chevalier-Lavaure. Regarding the reform of mentally ill soldiers. Montpel. méd., 1916, n.s., v. 39, pp. 418-427.
Chevassu, M. Les traumatismes cranio-cérébraux dans la zone de l’avant. Montpel. méd., 1916, v. 39, p. 29.
Chevassu, M. Head injuries in the front area. Montpel. méd., 1916, v. 39, p. 29.
Cheyrou. Réactions immédiates observées à la suite d’éclatements à proximité de projectiles de guerre. Caducée. Par., 1917, xvii, 31-33.
Cheyrou. Immediate reactions observed following explosions near war projectiles. Caduceus. Par., 1917, xvii, 31-33.
Chiari, H. Zur Pathogenese der Meningitis bei Schussverletzungen des Gehirns. Münch. med. Wchnschr., 1915, v. 621, pp. 596-598.
Chiari, H. On the Pathogenesis of Meningitis from Gunshot Injuries to the Brain. Münch. med. Wchnschr., 1915, v. 621, pp. 596-598.
Chiray. Centre neurologique de la 10e région (Rennes). Rev. neurol., Par., 1916, v. 23, pp. 672-686.
Chiray. Neurological Center of the 10th Region (Rennes). Rev. neurol., Par., 1916, v. 23, pp. 672-686.
Chiray. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 472.
Chiray. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 472.
Chiray, J., Bourguignon, G. et Dagnan-Bouvert. Interprétation des discordances entre les réactions électriques et les signes cliniques, dans les lésions nerveuses périphériques. Paris méd., 1916 (part. méd.) v. 21, pp. 220-224.
Chiray, J., Bourguignon, G. and Dagnan-Bouvert. Interpretation of discrepancies between electrical reactions and clinical signs in peripheral nerve injuries. Paris méd., 1916 (med. part) vol. 21, pp. 220-224.
Cimbal. Psychosen und Psychoneurosen im IX. Armeekorps seit der Mobilmachung. Berl. klin. Wchnschr., 1915, v. 52, p. 304.
Cimbal. Psychoses and Psychoneuroses in the IX Army Corps since Mobilization. Berl. klin. Wchnschr., 1915, v. 52, p. 304.
Cimbal. Die seelischen und nervosen Erkrankungen, seit der Mobilmachung. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 411-415.
Cimbal. The psychological and nerve-related illnesses since the mobilization. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 411-415.
Clarke, C. K. Psychiatric treatment. Mil. Hosp. Com. Canada, Spec. Bull., Ottawa, 1916, p. 101.
Clarke, C. K. Psychiatric treatment. Mil. Hosp. Com. Canada, Spec. Bull., Ottawa, 1916, p. 101.
Clark, D. A. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 12-18.
Clark, D. A. Treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 12-18.
Clark, E. Eyesight and the war. Med. Press and Circ., Lond., 1916, ii, pp. 72-74. Also: Nature, Lond., 1916, v. 96, pp. 552-555.
Clark, E. Vision and the war. Medical Press and Circular, London, 1916, vol. 2, pp. 72-74. Also: Nature, London, 1916, vol. 96, pp. 552-555.
Clark, E. Clinical lecture on eyesight and the war. Med. Press and Circ., Lond., 1916, v. 102, p. 72.
Clark, E. Clinical lecture on vision and the war. Med. Press and Circ., Lond., 1916, v. 102, p. 72.
Clarke, J. Mitchel. Some neuroses of the war. Bristol. M. Chir. J., 1916, v. 34, p. 130. Rev. J. Nerv. and Ment. Dis., N. Y., 1917, i, p. 119.
Clarke, J. Mitchel. Some neuroses of the war. Bristol. M. Chir. J., 1916, v. 34, p. 130. Rev. J. Nerv. and Ment. Dis., N. Y., 1917, i, p. 119.
Claude, Henri. Les états névropathiques (Rev. neurol., Par., 1914-15), v. 222, p. 1162.
Claude, Henri. The Neurotic States (Rev. neurol., Paris, 1914-15), vol. 222, p. 1162.
Claude, H. L’organisation et le fonctionnement des centres neurologiques régionaux. Paris méd., 1915 (part. méd.), v. 17, pp. 61-65.
Claude, H. The organization and operation of regional neurological centers. Paris méd., 1915 (part. méd.), v. 17, pp. 61-65.
Claude, H. Discussion de accidents nerveux par la déflagration des explosifs. Rev. neurol., Par., 1916, v. 23, pp. 587-590.
Claude, H. Discussion of nerve accidents caused by the explosion of explosives. Rev. neurol., Paris, 1916, v. 23, pp. 587-590.
Claude, H. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 460-462.
Claude, H. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, v. 29, pp. 460-462.
Claude, H. Discussion de Vincent. Rev. neurol., Par., 1916, v. 29, p. 587.
Claude, H. Discussion of Vincent. Neurological Review, Paris, 1916, vol. 29, p. 587.
Claude, H. De l’évolution des incapacités dans les attitudes vicieuses sans rapport avec des lésions organiques appréciables. Paris Medical, octobre 1916.
Claude, H. On the evolution of disabilities in bad attitudes unrelated to noticeable organic lesions. Paris Medical, October 1916.
Claude, H. War neurology; traumatic lesions of nerves by projectiles. Med. Press, and Circ., Lond., 1916, v. 102, p. 72, and p. 469.
Claude, H. War neurology; traumatic nerve damage caused by projectiles. Med. Press, and Circ., Lond., 1916, v. 102, p. 72, and p. 469.
Claude, H. L’évaluation des incapacités dans les attitudes vicieuses sans rapport avec des lésions organiques appréciables. Paris méd., 1916-17, v. 21, pp. 300-305.
Claude, H. The assessment of disabilities in harmful attitudes unrelated to noticeable organic lesions. Paris méd., 1916-17, v. 21, pp. 300-305.
Claude, H. L’anesthésie régionale associée aux méthodes psychophysiothérapiques dans le traitement des attitudes vicieuses et des tremblements des membres inférieurs d’ordre fonctionnel. Bull. et. Soc. méd. d’hôp. de Par., 1917, v. 33, pp. 424-430.
Claude, H. Regional anesthesia combined with psychophysiotherapeutic methods in the treatment of dysfunctional attitudes and tremors in the lower limbs. Bull. et. Soc. méd. d’hôp. de Par., 1917, v. 33, pp. 424-430.
Claude et Chauvet. Sémiologie réelle des sections totales des nerfs mixtes périphériques. Paris, 1901.
Claude and Chauvet. Real semiology of the total sections of mixed peripheral nerves. Paris, 1901.
Claude, H., Dide, M., et Lejonne, P. Psychoses hystéro-émotives de la guerre. Paris méd., 1916, v. 21, pp. 181-185.
Claude, H., Dide, M., and Lejonne, P. Hysterical-emotional psychoses of the war. Paris méd., 1916, vol. 21, pp. 181-185.
Claude, Henri, et Lhermitte, J. Étude clinique et anatomo-pathologique de la commotion médullaire directe par projectiles de guerre. Ann. de méd., Par., 1914-15, v. 2, pp. 479-506.
Claude, Henri, and Lhermitte, J. Clinical and Anatomopathological Study of Direct Medullary Concussion from War Projectiles. Ann. de méd., Paris, 1914-15, vol. 2, pp. 479-506.
Claude, Henri, et Lhermitte, J. Le tétanos fruste à évolution lente et incubation prolongée. Étude des réactions électriques. Presse méd., 1915, 14 oct., p. 406.
Claude, Henri, and Lhermitte, J. Slow-progressing incomplete tetanus with prolonged incubation. Study of electrical reactions. Medical Press, 1915, Oct 14, p. 406.
Claude, Henri, et Lhermitte, J. Les réflexes tendineux et cutanés, les mouvements de défense et d’automatisme dans la section totale de la moelle d’après une observation anatomo-clinique. Ann. de méd., Par., 1916, v. 3, pp. 407-430.
Claude, Henri, and Lhermitte, J. Tendon and skin reflexes, defensive movements, and automatic responses in total spinal cord section based on an anatomical-clinical observation. Ann. de méd., Par., 1916, v. 3, pp. 407-430.
Claude, Henri, et Lhermitte, J. Les paraplégies cérébello-spasmodiques et ataxo-cérébello-spasmodiques consécutives aux lésions bilatérales des lobules paracentraux par projectiles de guerre. Soc. méd. d’hôp. de Par., 1916, 26 mai.
Claude, Henri, and Lhermitte, J. Cerebellar-spastic and ataxic-cerebellar-spastic paraplegia resulting from bilateral lesions of the paracentral lobules due to war projectiles. Med. Soc. Hosp. Paris, 1916, May 26.
Claude, Henri, et Lhermitte, J. La glycosurie dans les lésions traumatiques du cerveau. Soc. méd. d. hôp. de Par., 1916, 26 mai.
Claude, Henri, and Lhermitte, J. Glycosuria in traumatic brain injuries. Med. Soc. of Hosp. of Paris, 1916, May 26.
Claude, Henri, et Lhermitte, J. Les contractures du tétanos tardif à évolution prolongée et leur diagnostic avec les contractures organiques ou “fonctionnelles.” Progrès méd., Par., 1916, pp. 185-187.
Claude, Henri, and Lhermitte, J. The contractures of late tetanus with prolonged evolution and their diagnosis alongside organic or “functional” contractures. Progress Med., Paris, 1916, pp. 185-187.
Claude, Henri, et Lhermitte, J. Troubles médullaires dans les commotions directes mais à distance de la colonne vertébrale. Paris méd., 1917, No. 27, pp. 11-14.
Claude, Henri, and Lhermitte, J. Spinal issues from direct concussions but distant from the spine. Paris méd., 1917, No. 27, pp. 11-14.
Claude, H., et Lhermitte, J. Formes cliniques de la commotion de la moelle cervicale par projectiles de guerre. Rev. de méd. Par., 1916, 35, 535-554.
Claude, H., and Lhermitte, J. Clinical Forms of Spinal Cord Concussion from War Projectiles. Med. Rev. Paris, 1916, 35, 535-554.
Claude, Henri, et Lhermitte, J. Le syndrome infundibulaire dans un cas de tumeur du troisième ventricule. Presse méd., Par., 1917, v. 25, pp. 417-418.
Claude, Henri, and Lhermitte, J. The infundibular syndrome in a case of a tumor in the third ventricle. Med Press, Paris, 1917, vol. 25, pp. 417-418.
Claude, H., et Lhermitte, J. Les modifications dynamogéniques des centres nerveux inférieurs dans les paralysies ou dans les contractures fonctionnels. Presse méd., 1918, No. 1.
Claude, H., and Lhermitte, J. The dynamic modifications of the lower nerve centers in paralysis or functional contractures. Med. Press, 1918, No. 1.
Claude, Henri, et Porak, R. De la décalcification osseuse dans les paralysies des membres organiques ou névropathiques. Paris méd., 1915, v. 17 (part. méd.), pp. 321-328.
Claude, Henri, and Porak, R. On bone demineralization in organic or neuropathic limb paralysis. Paris méd., 1915, vol. 17 (med. part), pp. 321-328.
Claude, Henri, et Porak, R. Les troubles de la motilité dans les psychonévroses du type hystérique. Progrès méd., Par., 1914-15, v. 23, p. 486 and p. 512. Rev. Paris méd., 1915, v. 17 (part. méd.), p. 540.
Claude, Henri, and Porak, R. The motility disorders in psychoneuroses of the hysterical type. Progrès méd., Paris, 1914-15, v. 23, p. 486 and p. 512. Rev. Paris méd., 1915, v. 17 (part. méd.), p. 540.
Claude, Henri, et Lhermitte, J. et Loyes, Mlle. M. Étude histologique d’un cas de commotion médullaire par éclatement d’obus. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 680-687.
Claude, Henri, and Lhermitte, J. and Loyes, Mlle. M. Histological study of a case of spinal concussion due to shell explosion. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 680-687.
Claude, Henri, Lhermitte, J., et Vigouroux, A. Délire mystique chez un blessé de l’encéphale. Ann. méd.-psychol., Par., 1917, v. 73, pp. 560-568.
Claude, Henri, Lhermitte, J., and Vigouroux, A. Mystical Delirium in a Brain-Injured Patient. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 560-568.
Claude, Henri, Loyes, Mlle. M., et Lhermitte, J. Étude clinique et anatomique de la commotion médullaire par éclatement d’obus. Rev. Paris Méd., 1915, v. 17 (part. méd.), p. 370.
Claude, Henri, Loyes, Mlle. M., and Lhermitte, J. Clinical and anatomical study of spinal concussion caused by shell explosions. Rev. Paris Méd., 1915, v. 17 (part. méd.), p. 370.
Claude, Vigouroux, et Dumas. Étude anatomique de cent cas de lésions traumatiques des nerfs des membres. Presse Méd., March 4, 1915.
Claude, Vigouroux, and Dumas. Anatomical study of one hundred cases of traumatic nerve injuries in the limbs. Medical Press, March 4, 1915.
Clerici, A. Disturbi psichici nei soldati combattenti. Riv. di. psicol. applic., Bologna, 1915, v. 11, pp. 112-117.
Clerici, A. Mental disorders in combat soldiers. Journal of Applied Psychology, Bologna, 1915, vol. 11, pp. 112-117.
Clinical aspects of hemilesions of the cord. N. Y. Med. Jour., 1917, cvi, 1189.
Clinical aspects of hemilesions of the cord. N. Y. Med. Jour., 1917, cvi, 1189.
Clunet, Jean. Les effets immédiats de l’émotion sur le système nerveux, en dehors de toute commotion. Rev. neurol., Par., 1917, v. 24, pp. 48-51.
Clunet, Jean. The immediate effects of emotion on the nervous system, aside from any concussion. Rev. neurol., Par., 1917, v. 24, pp. 48-51.
Cluzet. Paralysie du plexus brachial avec troubles trophiques de la main, sans blessure ni contusion apparente, provoquée par l’explosion d’un obus. Lyon méd., 1916, v. 125, p. 20.
Cluzet. Brachial plexus paralysis with trophic disorders of the hand, without any visible injury or bruise, caused by the explosion of a shell. Lyon méd., 1916, v. 125, p. 20.
Cohn, Toby. (Discussing Lewandowsky)—“Kriegsverletzungen des Nervensystems.” Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 89 and p. 149.
Cohn, Toby. (Discussing Lewandowsky)—“War Injuries of the Nervous System.” German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, p. 89 and p. 149.
Cohn, Toby. Zur Frage der psychogenen Komponente bei Motilitätdefekten infolge von Schussverletzungen. Neurol. Zbl., Leipz., 1916, v. 35, No. 6.
Cohn, Toby. On the Question of the Psychogenic Component in Mobility Defects Due to Gunshot Injuries. Neurol. Zbl., Leipzig, 1916, vol. 35, No. 6.
Cohn, Toby, Kron, H., and Hansemann, etc. Ueber Kriegsverletzungen des Nervensystems. Discussion before Referat of Lewandowsky. Berl. klin. Wchnschr., 1915, v. 521, pp. 88-91.
Cohn, Toby, Kron, H., and Hansemann, etc. On War Injuries of the Nervous System. Discussion before the Presentation of Lewandowsky. Berl. klin. Wchnschr., 1915, v. 521, pp. 88-91.
Colella, R. Arteriosclerosi e neurosi posttraumatiche. Gazz. med. sicil. Catania, 1916, xix, 121-128.
Colella, R. Arteriosclerosis and post-traumatic neuroses. Sicilian Medical Gazette, Catania, 1916, xix, 121-128.
Colin, H. De l’envoi en congé de convalescence des alienés militaires guéris et fortunés en cas de refus du certificat d’hébergement. Soc. de méd. lég. de France, Bull., Par., 1916, v. 13, pp. 136-146.
Colin, H. On the Leave of Absence for Recovered Military Patients in Cases of Denial of Accommodation Certificate. Legal Medicine Society of France, Bulletin, Paris, 1916, vol. 13, pp. 136-146.
Colin, H. et Lautier, J. De la valeur émotionnelle des maladies vénériennes dans l’étiologie et l’évolution des psychoses. Ann. méd.-psychol., Par., 1917, v. 73, pp. 357-373.
Colin, H. and Lautier, J. The Emotional Value of Venereal Diseases in the Etiology and Evolution of Psychoses. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 357-373.
Colin, H., Lautier, et Magnac. Les imbéciles à l’armée. Ann. méd.-psychol., Par., 1916-17, v. 7, pp. 540-546.
Colin, H., Lautier, and Magnac. The Fools in the Army. Ann. méd.-psychol., Par., 1916-17, v. 7, pp. 540-546.
Collie, Sir John. Fraudulent and neurasthenic cases. Tr. Med.-Leg. Soc., Lond., 1914-15, v. 12, pp. 25-67.
Collie, Sir John. Fraudulent and neurasthenic cases. Tr. Med.-Leg. Soc., Lond., 1914-15, v. 12, pp. 25-67.
Collie, Sir John. Fraudulent and neurasthenic cases. J. Roy. Army Med. Corps, Lond., 1915, v. 24, pp. 653-682; also Practitioner, Lond., 1915, v. 44, pp. 653-682.
Collie, Sir John. Fraudulent and neurasthenic cases. J. Roy. Army Med. Corps, Lond., 1915, v. 24, pp. 653-682; also Practitioner, Lond., 1915, v. 44, pp. 653-682.
Collie, Sir John. Fraud and skin eruptions. Lancet, Lond., 1916, ii, pp. 1007-1010.
Collie, Sir John. Fraud and skin eruptions. Lancet, London, 1916, II, pp. 1007-1010.
Collie, Sir John. Neurasthenia; what it costs the State. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 525-544.
Collie, Sir John. Neurasthenia; its cost to the State. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 525-544.
Collie, Sir John. Tests for simulated defective vision or for blindness of one eye. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 800-812.
Collie, Sir John. Tests for simulated defective vision or for blindness of one eye. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 800-812.
Collie, Sir John. Jaundice and malingering. Birmingh. M. Rev., 1916, v. 80, pp. 93-94.
Collie, Sir John. Jaundice and Malingering. Birmingham Medical Review, 1916, vol. 80, pp. 93-94.
Collie, Sir John. Malingering: examination of the upper extremities. J. Roy. Army Med. Corps, Lond., 1916, v. 27, pp. 85-91.
Collie, Sir John. Faking illness: examination of the upper limbs. J. Roy. Army Med. Corps, Lond., 1916, v. 27, pp. 85-91.
Collie, Sir John. Malingering and feigned sickness. 2nd. ed., 1917.
Collie, Sir John. Faking illness and pretending to be sick. 2nd ed., 1917.
Collie, Sir John. La simulazione dei dolori di schiena. Gazz. med. lomb., Milano, 1917, xxiv, 129-132.
Collie, Sir John. The Simulation of Back Pain. Gazz. med. lomb., Milan, 1917, xxiv, 129-132.
Collie, Sir John. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18 (sect. Balneol.), v. 10, pp. 21-24.
Collie, Sir John. Treatment for mental disabilities caused by the war through physical methods. Proc. Roy. Soc. Med., Lond., 1917-18 (sect. Balneol.), v. 10, pp. 21-24.
Collie, Sir John. The management of neurasthenia and allied disorders contracted in the Army. With report of remarks made by Lt. Col. Aldren Turner. “Recalled to Life,” 1917, Sept., No. 2, pp. 234-250.
Collie, Sir John. The management of neurasthenia and related disorders acquired in the Army. With a report of comments made by Lt. Col. Aldren Turner. “Recalled to Life,” September 1917, No. 2, pp. 234-250.
Collier, James. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., 1915-16, v. 9 (sect. Psychiat.), pp. 34-35.
Collier, James. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., 1915-16, v. 9 (sect. Psychiat.), pp. 34-35.
Collier, James. Gunshot wounds and injuries of the spinal cord. Lancet, Lond., 1916, i, pp. 711-716. Also Tr. M. Soc., Lond., 1915-16, v. 39, pp. 227-256.
Collier, James. Gunshot wounds and spinal cord injuries. Lancet, Lond., 1916, i, pp. 711-716. Also Tr. M. Soc., Lond., 1915-16, v. 39, pp. 227-256.
Collins, J. and Craig, C. B. Injuries to spinal cord produced by modern warfare. J. Nerv. and Ment. Dis., N. Y., 1916, v. 44, pp. 527-528.
Collins, J. and Craig, C. B. Injuries to the spinal cord caused by modern warfare. J. Nerv. and Ment. Dis., N. Y., 1916, v. 44, pp. 527-528.
Colmers, F. Ueber Schädelschüsse. Deutsche med. Wchnschr., 1917, 43, 741.
Colmers, F. On Skull Shots. German Medical Weekly, 1917, 43, 741.
Cololian. La mécanothérapie de guerre avec les appareils de fortune. Arch. de méd. et pharm. mil., Par., 1914-15, v. 64, pp. 155-176; also pp. 658-695.
Cololian. War mechanotherapy with makeshift devices. Arch. of med. and pharm. mil., Par., 1914-15, v. 64, pp. 155-176; also pp. 658-695.
Commotion des centres nerveux par explosion. Lyon méd., 1916, v. 125, pp. 181-182.
Commotion of the nerve centers due to explosion. Lyon méd., 1916, v. 125, pp. 181-182.
Commotionnés vrais. Caducée, Par., 1916, v. 16, p. 172.
Genuinely shaken. Caducée, Par., 1916, v. 16, p. 172.
Condorelli-Francaviglia, M. Congiuntivite catarrhale acuta in un militare, provocata mediante l’uso di semi di ricino. Policlin., Roma, 1917, xxiv, sez. prat., 735-739.
Condorelli-Francaviglia, M. Acute catarrhal conjunctivitis in a soldier, caused by the use of castor seeds. Policlin., Rome, 1917, xxiv, prat. sect., 735-739.
Conférence interalliée pour l’étude de la rééducation professionelle et des questions qui intéressent les invalides de la guerre. Grand-Palais, Paris, May 8-12, 1917. Proc. Roy. Soc. Méd., Lond., 1917-1918 (Sect. Balneul. and Climatol.), v. 10, pp. 81-95.
Allied Conference on the Study of Vocational Rehabilitation and Issues Affecting War Veterans. Grand Palais, Paris, May 8-12, 1917. Proc. Roy. Soc. Méd., Lond., 1917-1918 (Sect. Balneul. and Climatol.), v. 10, pp. 81-95.
Cone, S. M. Pathological findings in nerves in following war injuries; preliminary report. Brit. Med. Jour., 1917, ii, 615.
Cone, S. M. Pathological findings in nerves after war injuries; preliminary report. Brit. Med. Jour., 1917, ii, 615.
Cone, Sydney M. Some of the results of work on the pathology of peripheral nerve injuries. Amer. Jour. Orthop. Surg., 1918, xvi, 319.
Cone, Sydney M. Some of the results of work on the pathology of peripheral nerve injuries. Am. J. Orthop. Surg., 1918, 16, 319.
Cone, Sydney M. Surgical pathology of the peripheral nerves. Brit. Jour. of Surg., 1918, vi, 524.
Cone, Sydney M. Surgical pathology of the peripheral nerves. Brit. Jour. of Surg., 1918, vi, 524.
Congrès interallié de rééducation des mutilés. Presse méd. Par., 1917, v. 25, pp. 301-303.
Allied Congress on Rehabilitation of the Disabled. Med. Press. Par., 1917, v. 25, pp. 301-303.
Consiglio, P. Studii di psichiatria militare. Riv. sper. di freniat., Reggio-Emilia, 1912, v. 38, p. 370; 1913, v. 39, p. 792; 1914, v. 40, p. 881; 1915, v. 41, p. 35.
Consiglio, P. Studies in Military Psychiatry. Experimental Journal of Psychiatry, Reggio-Emilia, 1912, vol. 38, p. 370; 1913, vol. 39, p. 792; 1914, vol. 40, p. 881; 1915, vol. 41, p. 35.
Consiglio, P. Delle psicosi e delle nevrosi e specialmente della criminalità in guerra. Ann. di med., nav., Roma, 1915, ii, pp. 408-417.
Consiglio, P. On psychosis and neurosis, especially regarding crime in wartime. Ann. di med., nav., Roma, 1915, ii, pp. 408-417.
Consiglio, P. Psicosi, nevrosi e criminalita nell’ ambiente militare in tempo di pace. Ann. di med., nav., Roma, 1915, ii, pp. 418-422.
Consiglio, P. Psychosis, neurosis, and crime in the military environment during peacetime. Ann. di med., nav., Rome, 1915, ii, pp. 418-422.
Consiglio, P. Nevrosi e psicosi in guerra. (Nota 2) Gior. di med. mil., Roma, 1915, v. 63, pp. 665-703.
Consiglio, P. Neurosis and Psychosis in War. (Note 2) Journal of Military Medicine, Rome, 1915, vol. 63, pp. 665-703.
Consiglio, P. Studien über Militär-psychiatrie und Kriminologie. Ztschr. f. d. Ges. Neurol. u. Psychiat., Berl. u. Leipz., 1915, v. 128, pp. 384-444.
Consiglio, P. Studies on Military Psychiatry and Criminology. Journal of General Neurology and Psychiatry, Berlin and Leipzig, 1915, vol. 128, pp. 384-444.
Consiglio, P. Psicosi nevrosi e criminalita nei militari in guerra. Arch. di antrop. crim., etc., Torino, 1916, v. 8, pp. 258-268.
Consiglio, P. Psychosis, neurosis, and criminal behavior in soldiers at war. Archives of Criminal Anthropology, etc., Turin, 1916, vol. 8, pp. 258-268.
Consiglio, P. L’Anomalie de carattere dei militari in guerra. Riv. sper. di freniat., Reggio-Emilia, 1916, v. 42, pp. 131-172.
Consiglio, P. The Character Anomalies of Soldiers in War. Riv. sper. di freniat., Reggio-Emilia, 1916, v. 42, pp. 131-172.
Consiglio, P. Disturbi nervosi e mentale nei militari in guerre. Gior. di méd. mil., 1917, v. 65, pp. 607-616.
Consiglio, P. Nervous and mental disorders in soldiers during wars. Military Medical Journal, 1917, vol. 65, pp. 607-616.
Cooper, George. Contractures and allied disorders: their cause and treatment. Brit. M. J., Lond., 1917, i, pp. 109-114.
Cooper, George. Contractures and related disorders: their cause and treatment. Brit. M. J., Lond., 1917, i, pp. 109-114.
Cooper, P. R. (Discussion of Milligan’s paper.) Brit. M. J., Lond., 1916, ii, p. 73; also p. 201.
Cooper, P. R. (Discussion of Milligan’s paper.) Brit. M. J., Lond., 1916, ii, p. 73; also p. 201.
Cooper, J. W. A. Use of alcohol on the battlefield and elsewhere. Lancet, Lon., 1914, ii, 1168.
Cooper, J. W. A. The use of alcohol on the battlefield and beyond. Lancet, Lon., 1914, ii, 1168.
Cooper, P. R. Treatment of “shell shock,” Brit. M. J., Lond., 1916, ii, 201.
Cooper, P. R. Treatment of “shell shock,” Brit. M. J., Lond., 1916, ii, 201.
Cordier, Charles Albert. Les états psychasthéniques frustes et la guerre. Thèse de Lyon, 1916. Rev. neurol., Par., 1917, v. 22, p. 471.
Cordier, Charles Albert. The Incomplete Psychasthenic States and War. Thesis from Lyon, 1916. Rev. neurol., Paris, 1917, vol. 22, p. 471.
Core, Donald E. The “Instinct-distortion,” or “war neurosis.” Bos. M. and S. J., 1918, clxxix, 448.
Core, Donald E. The “Instinct-distortion,” or “war neurosis.” Bos. M. and S. J., 1918, clxxix, 448.
Core, Donald E. “Instinct-distortion,” or “war-neurosis.” Lancet, Lon., 1918, ii, 168.
Core, Donald E. "Instinct distortion," or "war neurosis." Lancet, London, 1918, ii, 168.
Cornet. L’auto-mutilation. Rev. gén. de clin. et de thérap., Par., 1915, v. 29, pp. 649-653; and pp. 683-686.
Cornet. Self-mutilation. Gen. Rev. of Clin. and Therapy, Paris, 1915, vol. 29, pp. 649-653; and pp. 683-686.
Costello, C. A. Principal defects found in persons examined for service in the United States Navy. Amer. Jour. Pub. Health, 1917, vii, 489.
Costello, C. A. Main issues found in individuals examined for service in the United States Navy. Amer. Jour. Pub. Health, 1917, vii, 489.
Cottet, J. Troubles objectifs de la sensibilité cutanée dans les gelures des pieds: l’acrotrophodynie paresthésique des tranchées. Paris méd., 1917, No. 11, pp. 222-27.
Cottet, J. Objective Issues of Skin Sensitivity in Foot Frostbite: Trench Paresthetic Acrotrophodynia. Paris Med., 1917, No. 11, pp. 222-27.
Cottet, J. Syndrome d’aéro-paresthésie a frigore et gelures des pieds. Presse méd., Par., 1917, v. 25, pp. 517-518.
Cottet, J. Aero-paresthesia syndrome due to cold and frostbite of the feet. Med. Press, Paris, 1917, v. 25, pp. 517-518.
Courtois, Suffit M. et Giroux, R. Les formes anormales du tétanos. 1916, Paris, Masson et Cie.
Courtois, Suffit M. and Giroux, R. The Abnormal Forms of Tetanus. 1916, Paris, Masson et Cie.
Craig, C. B. Injuries to the peripheral nerves produced by modern warfare. Am. Jour. Med. Jour., 1916, clii, 368.
Craig, C. B. Injuries to the peripheral nerves caused by modern warfare. Am. Jour. Med. Jour., 1916, clii, 368.
Craig, Maurice. Psychological medicine. 1917, 3rd ed., Blakiston, pp. 300-311.
Craig, Maurice. Psychological medicine. 1917, 3rd ed., Blakiston, pp. 300-311.
Crile, G. W. The Kinetic Drive. W. B. Saunders, 1916.
Crile, G. W. The Kinetic Drive. W. B. Saunders, 1916.
Crile, G. W. A mechanistic view of war and peace. Macmillan, 1916.
Crile, G. W. A mechanistic view of war and peace. Macmillan, 1916.
Crile, G. W. Man: An adaptive mechanism. Macmillan, 1916.
Crile, G. W. Man: An Adaptive Mechanism. Macmillan, 1916.
Crile, G. W. Notes on Base Hospital No. 4, U. S. A., on Active Service. J. Am. M. Asso., Chicago, 1917, v. lxix, p. 206.
Crile, G. W. Notes on Base Hospital No. 4, U. S. A., on Active Service. J. Am. M. Assoc., Chicago, 1917, v. 69, p. 206.
Crile, G. W. The Fallacy of the German State Philosophy. Doubleday, Page, 1918.
Crile, G. W. The Fallacy of the German State Philosophy. Doubleday, Page, 1918.
Crinon, J. Les éclopés psychiques. (Méd. légale.) Caducée, Par., 1916, v. 16, pp. 115-116.
Crinon, J. Psychological Relics. (Forensic Medicine.) Caducée, Paris, 1916, v. 16, pp. 115-116.
Crinon, J. Les centres psychiatriques de l’avant. Progrès méd., Par., 1917, v. 43, pp. 364-365.
Crinon, J. The Psychiatric Centers of the Past. Med Progress, Paris, 1917, v. 43, pp. 364-365.
Cristiani, A. Note practiche (psichiatriche militari). Riv. ital. di neuropat. (etc.), Catania, 1917. x 265-272.
Cristiani, A. Military Psychiatric Practice Notes. Ital. J. Neuropath. (etc.), Catania, 1917. x 265-272.
Crouzon, O. Cécité temporaire provoquée par l’éclatement d’obus à proximité. Bull. et mém. soc. d’hôp. de Par., 1915, v. 39.
Crouzon, O. Temporary blindness caused by nearby shell explosions. Bull. et mém. soc. d’hôp. de Par., 1915, v. 39.
Crouzon, O. Les pseudo-maux de Pott au conseil de révision. La spondylite traumatique. Bull. et mém. soc. méd. de Par., 1915, v. 39, pp. 111-113.
Crouzon, O. The pseudo-symptoms of Pott at the review board. Traumatic spondylitis. Bull. and mem. soc. méd. de Par., 1915, v. 39, pp. 111-113.
Crouzon, O. Hémorrhagies naso-pharyngiennes profuse et répétées après commotion par éclatement d’obus chez un sujet atteint d’hypertension artérielle. Bull. et mém. Soc. méd. d’hôp. de Par., 1916, 3. s. xl, 1376-1378.
Crouzon, O. Profuse and repeated nasal-pharyngeal hemorrhages after concussion from shell explosion in a patient with high blood pressure. Bull. et mém. Soc. méd. d’hôp. de Par., 1916, 3. s. xl, 1376-1378.
Crouzon, O. De la valeur de l’hypotension artérielle comme signe objectif de la psychasthénie. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 234-237.
Crouzon, O. The value of low blood pressure as an objective sign of psychasthenia. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 234-237.
Cruchet, R. Calmettes et Bertrand. Épilepsie Jacksonienne grave. Trépanation et application de sac herniaire. Cessation des crises. Disparition des troubles subjectifs. Rev. neurol., Par., 1917, v. 24, pp. 510-511.
Cruchet, R. Calmettes et Bertrand. Severe Jacksonian Epilepsy. Trepanation and Hernia Sack Application. Stopping of Seizures. Disappearance of Subjective Disturbances. Rev. neurol., Par., 1917, v. 24, pp. 510-511.
Cruchet, R. Calmettes et Bertrand. Fracture du crâne méconnue. Commotion cérébrale. Crises d’hystéro-epilepsie avec état obsenant. Trépanation tardive. Guérison. Rev. neurol., Par., 1917, v. 24, pp. 511-513.
Cruchet, R. Calmettes and Bertrand. Undiagnosed skull fracture. Concussion. Hysterical-epileptic episodes with a state of unresponsiveness. Late trepanation. Recovery. Rev. neurol., Paris, 1917, vol. 24, pp. 511-513.
Culpin, M. Practical hints on functional disorders. Brit. M. J., Lond., ii, pp. 548-549.
Culpin, M. Practical tips on functional disorders. Brit. M. J., Lond., ii, pp. 548-549.
Cumberbatch, E. P. A criticism on the reaction testing of muscles and the interpretation of the results with reference to electrical examination of nerve injury in war. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Electro.-therap. sect.), pp. 23-38.
Cumberbatch, E. P. A critique of muscle reaction tests and how to interpret the results, focusing on the electrical assessment of nerve injuries sustained during wartime. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Electro.-therap. sect.), pp. 23-38.
Curschmann. Bemerkungen zur Behandlung hysterischer Stimmstörungen. München med. Wohnschr., 1916, v. 63, pp. 1644-1645.
Curschmann. Comments on the Treatment of Hysterical Speech Disorders. Munich Medical Journal, 1916, vol. 63, pp. 1644-1645.
Cutler, E. C. Neurological surgery in a war hospital. Boston M. and S. J., 1916, v. 174, pp. 305-309.
Cutler, E. C. Neurological surgery in a war hospital. Boston M. and S. J., 1916, v. 174, pp. 305-309.
Cygielstrejch, Adam. La psychologie de la panique pendant le guerre. Ann. med.-psychol., Par., 1916-17, v. 7, pp. 172-192.
Cygielstrejch, Adam. The psychology of panic during war. Ann. med.-psychol., Paris, 1916-17, vol. 7, pp. 172-192.
D’Abundo, G. Alterazioni nel sistema nervoso centrale consecutive a particolari commozioni traumatiche. Riv. ital. di neuropat., Catania, 1916, v. 9, pp. 145-171.
D’Abundo, G. Changes in the central nervous system following specific traumatic concussions. Ital. Rev. of Neuropath., Catania, 1916, vol. 9, pp. 145-171.
D’Abundo, G. Considerazioni cliniche sui traumi di guerra a capo. Riv. ital. di neuropat. psichiatr., ed elettroter., 1917, v. 10, 357-76.
D’Abundo, G. Clinical considerations on head injuries from war. Ital. J. Neuropath. Psychiatry, and Electrother., 1917, vol. 10, 357-76.
D’Abundo, G. Reparto neuropatologico militarizzato della clinica delle malattie nervose e mentale della R. Universita di Catania. Riv. ital. di neuropat., Catania, 1917, v. 10, pp. 22-24.
D’Abundo, G. Militarized neuropathological department of the clinic for nervous and mental diseases at the R. University of Catania. Ital. J. of Neuropath., Catania, 1917, vol. 10, pp. 22-24.
Dacco, E. Autolesioni cutanee nei militari. Gior. ital. d. mal. ven., Milano, 1917, lii, 340, 370.
Dacco, E. Skin self-harm in soldiers. Ital. J. Ven. Dis., Milan, 1917, lii, 340, 370.
Dal Collo, M. E. Contributo casuistico alle dermatosi simulate di guerra. Quaderni di med. leg., Milano, 1917, i, 24-29.
Dal Collo, M. E. A case study contribution on war simulated dermatoses. Medical Legal Notebooks, Milan, 1917, i, 24-29.
Damaye, H. Organisation et fonctionnement d’un service de neuropsychiatrie, d’armée. Presse méd., Par., 1916, v. 24, p. 24.
Damaye, H. Organization and operation of an army neuropsychiatry service. Medical Press, Paris, 1916, vol. 24, p. 24.
Damaye, H. Étude sur les affections mentales et neuropathiques occasionnées par les commotions de la guerre. Progrès méd., Par., 1917, 3. s., xxxii, 441-443.
Damaye, H. Study on mental and neuropathic conditions caused by war injuries. Med. Progress, Paris, 1917, 3rd series, xxxii, 441-443.
Damaye, H. Organisation des centres psychiatriques. Caducée, Par., 1917, v. 126, p. 147.
Damaye, H. Organization of psychiatric centers. Caducée, Par., 1917, v. 126, p. 147.
Damaye, H. Considérations cliniques sur les commotions de la guerre. Progrès méd., Par., 1917, 3. s., xxxii, 332-334.
Damaye, H. Clinical considerations on war concussions. Med. Prog., Paris, 1917, 3rd series, xxxii, 332-334.
Damaye, H. Aperçu général sur les fonctions d’un service de psychiatrie d’armée. Progrès méd., Par., 1917, v. 43, pp. 362-364.
Damaye, H. General Overview of the Functions of a Military Psychiatry Service. Med. Progress, Paris, 1917, v. 43, pp. 362-364.
Dames de la Croix-Rouge et la simulation. Caducée, Par., 1916, v. 16, p. 94.
Women of the Red Cross and the Simulation. Caducée, Par., 1916, v. 16, p. 94.
Darkshevich, L. O. (Nomenclature of disturbances in the region of the nervous system, following traumatism.) Russk. Vrach., Petrogr., 1916, v. 15, p. 97.
Darkshevich, L. O. (Nomenclature of disturbances in the nervous system after trauma.) Russk. Vrach., Petrogr., 1916, v. 15, p. 97.
Daude. Contribution a l’étude de la psychopathologie de guerre. Fonctionnement d’un centre psychiatrique de l’avant. Thèse de Bordeaux, 1916.
Daude. Contribution to the Study of War Psychopathology. Operation of a Frontline Psychiatric Center. Bordeaux Thesis, 1916.
Daussant. L’assistance aux invalides et mutilés de la guerre (appareillage, rééducation professionelle, placement). Arch. de méd. et pharm. mil., Par., 1916, v. 65, pp. 733-759.
Daussant. Support for war invalids and disabled individuals (prosthetics, vocational rehabilitation, employment placement). Arch. de méd. et pharm. mil., Paris, 1916, v. 65, pp. 733-759.
Davidenkoff, S. N. (Acute psychoses in time of war.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 321-325.
Davidenkoff, S. N. (Acute psychoses during wartime.) Psikhiat. Gaz., Petrograd, 1915, v. 2, pp. 321-325.
Davidenkoff, S. N. (Dysarthria and mutism following wind contusions.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 190-194.
Davidenkoff, S. N. (Speech difficulties and inability to speak after head injuries.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 190-194.
Davidenkoff, S. N. Acute traumatic psychoses; retroanterograde amnesia after traumatism of the skull. Ibid., 341-347.
Davidenkoff, S. N. Acute traumatic psychoses; retroanterograde amnesia after head trauma. Ibid., 341-347.
Davidenkoff, S. N. (Case of hysterical psychosis developed during battle.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 211-213.
Davidenkoff, S. N. (Case of hysterical psychosis developed during battle.) Psychiatry Journal, St. Petersburg, 1916, vol. 3, pp. 211-213.
Davidenkoff, S. N. (Nature of speech disturbances in the contused.) Sovrem. Psikhiat., Mosk., 1916, v. 10, pp. 292-373.
Davidenkoff, S. N. (Nature of speech disturbances in the contused.) Modern Psychiatry, Moscow, 1916, vol. 10, pp. 292-373.
Davidson, J. M. and Lockhart-Mummery, P. Fragment of shell embedded in the internal popliteal nerve: illustrating the value of accurate localization. Lancet, Lon., 1917, i, 719.
Davidson, J. M. and Lockhart-Mummery, P. A piece of shell found in the internal popliteal nerve: highlighting the importance of precise localization. Lancet, Lon., 1917, i, 719.
Dawson, G. H. A case of shell concussion: treatment by general anaesthesia. Lancet, Lond., 1916, i, p. 463.
Dawson, G. H. A case of shell shock: treatment with general anesthesia. Lancet, Lond., 1916, i, p. 463.
De Boer, J. Desertie en vagabondage. Mill.-geneesk. Tijdschr., Haarlem, 1917, v. 21, pp. 149-167.
De Boer, J. Desertion and Vagabondage. Mil.-Med. Journal, Haarlem, 1917, v. 21, pp. 149-167.
De Brun, H. L’amnésie paludienne, Presse méd., Par., 1917, v. 25, pp. 625-627.
De Brun, H. Malaria-related amnesia, Med. Press, Paris, 1917, vol. 25, pp. 625-627.
Dedor, V. P. (Skull-brain wounds, according to the data of the evacuational hospital No. 88.) Russk. Vrach., Petrogr., 1917, v. 17, pp. 429-431, and pp. 450-454.
Dedor, V. P. (Skull-brain injuries based on data from evacuation hospital No. 88.) Russk. Vrach., Petrogr., 1917, v. 17, pp. 429-431, and pp. 450-454.
DeFleury, Maurice. Un moyen de délassement pour les troupes en marche. Bull. de Acad, de méd., Par., 1914, v. 72, pp. 442-443.
DeFleury, Maurice. A way for troops on the march to relax. Bull. de Acad, de méd., Par., 1914, v. 72, pp. 442-443.
Dejerine, J. Deux cas de paraplégie fonctionnelle d’origine émotive observée chez des militaires. Rev. neurol., Paris, 1915.
Dejerine, J. Two cases of functional paraplegia of emotional origin observed in military personnel. Rev. neurol., Paris, 1915.
Dejerine, J. Sur l’abolition de réflexe cutané plantaire dans certains cas de paralysies fonctionnelles, accompagnées d’anesthésie (hystéro-traumatisme). Rev. neurol., Paris, 1914-15, v. 221, pp. 521-529.
Dejerine, J. On the abolition of the plantar skin reflex in certain cases of functional paralysis accompanied by anesthesia (hystero-trauma). Rev. neurol., Paris, 1914-15, v. 221, pp. 521-529.
Dejerine, J. Deux cas de paralysie fonctionnelle d’origine émotive observés chez les militaires. Rev. neurol., Par., 1914-15, v. 222, pp. 421-424.
Dejerine, J. Two cases of emotional functional paralysis observed in soldiers. Rev. neurol., Par., 1914-15, v. 222, pp. 421-424.
Dejerine et Gascuel. Tachycardie d’origine émotive permanente. Rev. neurol., Par., 1914-15, v. 222, pp. 211-214.
Dejerine et Gascuel. Permanent emotional tachycardia. Rev. neurol., Par., 1914-15, v. 222, pp. 211-214.
Dejerine, J. et Gauckler, E. Le traitement par l’isolement et la psychothérapie des militaires atteints de troubles fonctionnels du système nerveux. Presse méd., Par., 1915, v. 23, pp. 521-522.
Dejerine, J. and Gauckler, E. Treatment through isolation and psychotherapy for soldiers suffering from functional disorders of the nervous system. Med. Press, Paris, 1915, vol. 23, pp. 521-522.
Dejerine, Marie, Babinski, Claude, Léri, Sollier, Sicard. Travaux des centres neurologiques. Rev. neurol., Par., 1915, p. 1136.
Dejerine, Marie, Babinski, Claude, Léri, Sollier, Sicard. Work of the Neurological Centers. Rev. neurol., Paris, 1915, p. 1136.
Dejerine et Mouzon. Deux cas de syndrôme sensitif cortical. Rev. neurol., Par., 1914-15, v. 222, p. 388.
Dejerine and Mouzon. Two cases of cortical sensory syndrome. Rev. neurol., Paris, 1914-15, v. 222, p. 388.
Dejerine et Mouzon. Les lésions des gros troncs nerveux par projectiles de guerre. Les différents syndrômes cliniques et les indications opératoires, Presse méd., May 10, July 8, Aug. 30, 1915.
Dejerine and Mouzon. Injuries to major nerve trunks from war projectiles. The various clinical syndromes and surgical indications, Med Press, May 10, July 8, Aug. 30, 1915.
Dejerine et Mouzon. Un nouveau type de syndrôme sensitif cortical dans un cas de monoplégie corticale dissociée. Rev. neurol., Par., 1914-15, v. 222, pp. 1265-1273.
Dejerine and Mouzon. A new type of cortical sensory syndrome in a case of dissociated cortical monoplegia. J. Neurol., Paris, 1914-15, vol. 222, pp. 1265-1273.
Dejerine et Mouzon. Le diagnostic de l’interruption complète des gros troncs nerveux de membres. Presse méd., Par., 1916, v. 24, pp. 97-101.
Dejerine and Mouzon. The diagnosis of complete interruption of the major nerve trunks in limbs. Med. Press, Paris, 1916, vol. 24, pp. 97-101.
Dejerine, M. and Mme. and Mouzon. Troubles trophiques articulaires analogues à ceux du rhumatisme subaigu et semblant consécutif à un tiraillement des racines des plexus brachiaux chez un soldat atteint de paraplégie traumatique. Rev. neurol., Paris, 1915.
Dejerine, M. and Mme. and Mouzon. Joint trophic disorders similar to those of subacute rheumatism, seeming to follow a pulling of the roots of the brachial plexus in a soldier with traumatic paraplegia. Rev. neurol., Paris, 1915.
Dejerine et Schwartz. Déformations articulaires analogues à celles du rhumatisme chronique, avec troubles trophiques, cutanées et hyperidrose relevant d’une lésion irritative du nerf médian. Rev. neurol., Paris, 1915.
Dejerine et Schwartz. Joint deformities similar to those of chronic rheumatism, with trophic disorders, skin issues, and excessive sweating due to an irritative lesion of the median nerve. Rev. neurol., Paris, 1915.
De la Motte. Demonstration zweier forensischer Fälle. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 590-591.
De la Motte. Demonstration of two forensic cases. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 590-591.
De Lapersonne. La rééducation des aveugles de guerre. Presse méd., Par., 1917, v. 25, p. 309.
De Lapersonne. Rehabilitation of war-blind individuals. Medical Press, Paris, 1917, vol. 25, p. 309.
Del Greco, Francesco. Gli ansioso emotivi. Riv. ital. di neuropat. (Psichiat. ed elettro.) Catania, 1917, v. 10, pp. 169-183.
Del Greco, Francesco. The Anxious Emotional. Ital. J. of Neuropath. (Psychiat. and Electro.) Catania, 1917, v. 10, pp. 169-183.
Delherm, L. Note sur les contractures et les paralysies traumatiques d’ordre réflexe. J. de radiol. et d’électrol., Par., 1916, v. 2, pp. 292-300.
Delherm, L. Note on reflex trauma-related contractures and paralysis. J. de radiol. et d’électrol., Par., 1916, v. 2, pp. 292-300.
Delherm, L. Le traitement des phénomènes hystériques par la rééducation intensive d’après Cl. Vincent. J. de radiol. et d’électrol., Par., 1917, v. 2, pp. 531-532.
Delherm, L. Treatment of hysterical phenomena through intensive rehabilitation according to Cl. Vincent. J. of radiology and electrology, Paris, 1917, vol. 2, pp. 531-532.
Delherm and Py. De l’importance de bien différencier les manifestations organiques et les manifestations psychiques chez les blessés de guerre. J. de radiol. d’électrol., Par., 1914-15, i, 625-628.
Delherm and Py. On the importance of clearly distinguishing between organic manifestations and psychological manifestations in war injuries. J. de radiol. d’électrol., Paris, 1914-15, i, 625-628.
Delinquent children and the war. Brit. M. J., Lond., 1917, i, p. 231.
Delinquent children and the war. Brit. M. J., Lond., 1917, i, p. 231.
Délire raisonnant d’invention. Ann. méd.-psychol., Par., 1917, v. 73, pp. 589-594.
Reasoned Delirium of Invention. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 589-594.
De Lisi, L. Ricerche sperimentali sulle alterazioni nervose centrali degli annuali sottoposti a commozione cerebrale. Riv. sper. di freniat., Reggio-Emilia, 1915, v. 41, pp. 249-312.
De Lisi, L. Experimental research on central nervous system changes in annuals subjected to concussion. Riv. sper. di freniat., Reggio-Emilia, 1915, v. 41, pp. 249-312.
Delorme, Edmond. Sur la fréquence des troubles des organes des sens, et en particulier de la vision, dans les blessures de la tête par les projectiles. Bull. Acad, de méd., Par., 1915, v. 73, p. 397.
Delorme, Edmond. On the frequency of sensory organ disorders, particularly vision, in head injuries caused by projectiles. Bull. Acad, de méd., Par., 1915, v. 73, p. 397.
DeMartel, T. Blessures du crâne. Collection Horizon, Masson et Cie, Paris, 1917.
DeMartel, T. Skull Injuries. Horizon Collection, Masson and Co., Paris, 1917.
De Massary, E., et Du Souich, P. Syndrôme choréiforme hystérique et paralysie générale incipiens. Rev. neurol., Par., 1917, v. 24, pp. 219-221.
De Massary, E., and Du Souich, P. Hysterical choreiform syndrome and early general paralysis. Rev. neurol., Paris, 1917, vol. 24, pp. 219-221.
De Massary, E., et Tockmann. Un cas de paludisme avec réaction meningée violente simulant la méningite cérébrospinale. Bull. et mem. Soc. méd. d’hôp. de Paris, 1917, 3 ser. 41, 1195-9.
De Massary, E., and Tockmann. A case of malaria with severe meningeal reaction mimicking cerebrospinal meningitis. Bull. et mem. Soc. méd. d’hôp. de Paris, 1917, 3 ser. 41, 1195-9.
Deny, G. La neuropsychopathologie française pendant une année de guerre (août 1914-août 1915). Encéphale, Par., 1914-15, ii, pp. 153-174.
Deny, G. French Neuropsychopathology During a Year of War (August 1914-August 1915). Encéphale, Paris, 1914-15, vol. ii, pp. 153-174.
Deny, G. Sur trois cas d’hystéro-traumatisme (monoplégie brachiale, contracture dorso-lumbaire, météorisme). Rev. neurol., Par., 1914-15, v. 221, pp. 559-560.
Deny, G. On three cases of hysterical trauma (brachial monoplegia, dorsolumbar contracture, meteorism). Neurology Review, Paris, 1914-15, vol. 221, pp. 559-560.
De Paeuw, Leon. The Vocational Reëducation of Maimed Soldiers. Princeton Univ. Press, 1918.
De Paeuw, Leon. The Vocational Reeducation of Maimed Soldiers. Princeton Univ. Press, 1918.
De Parrel, G. Surdité de guerre et méthode orale. Rev. de laryngol., etc., Par., 1911, v. 1, pp. 401-425.
De Parrel, G. War Deafness and Oral Method. Rev. de laryngol., etc., Paris, 1911, vol. 1, pp. 401-425.
De Sanctis, S. L’isterismo di guerra. Riv. ospedal., Roma., 1917, vii, 405-409.
De Sanctis, S. The War Hysteria. Hospital Review, Rome, 1917, vii, 405-409.
De Sandro, D. Il mutismo funzionale da scoppo di granata e quello degli isterici; loro cura con l’eterizzazione. Riv. di patol. nerv., Firenze, 1917, v. 22, pp. 9-31.
De Sandro, D. Functional mutism caused by grenade explosions and that of hysterics; their treatment with etherization. Riv. di patol. nerv., Florence, 1917, v. 22, pp. 9-31.
Deschamps, Albert. Un symptôme fonctionnel de la fatigue. L’inversion de la sensation de fatigue. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 262-264.
Deschamps, Albert. A Functional Symptom of Fatigue. The Reversal of the Fatigue Sensation. Gen. Rev. Clin. and Therap., Paris, 1916, v. 30, pp. 262-264.
Déserteur ambulatoire. Ann. méd. psychol., Par., 1914-15, p. 527.
Ambulatory Deserter. Ann. méd. psychol., Par., 1914-15, p. 527.
Descoust, Paul. Attitudes vicieuses du pied d’origine névropathique dans les traumatismes du membre inférieur. Presse méd., Par., 1917, v. 25, pp. 330-331.
Descoust, Paul. Maladaptive foot attitudes of neuropathic origin in lower limb injuries. Med Press, Paris, 1917, vol. 25, pp. 330-331.
Desplates, R., and Buquet, A. Oblitération des artères des membres et troubles circulatoires des nerfs. L’ischémie nerveuse des blessés de guerre. Rev. de méd., Par., 1916, 25, 578-619 (Published in February, 1918).
Desplates, R., and Buquet, A. Blockage of the arteries in the limbs and circulatory issues in the nerves. Nerve ischemia in wounded soldiers. Rev. de méd., Par., 1916, 25, 578-619 (Published in February, 1918).
Dessoir, M. Kriegspsychologische Betrachtungen. Leipz., 1916, S. Hirzel, 47 p. 8o.
Dessoir, M. Psychological Reflections on War. Leipzig, 1916, S. Hirzel, 47 pages. 8o.
De Tarnowsky, George. Military Surgery of the Advanced Zone. No. 7, Medical Manual War Series. Lea and Febiger.
De Tarnowsky, George. Military Surgery of the Advanced Zone. No. 7, Medical Manual War Series. Lea and Febiger.
Detecting the pretense of deafness; tests adopted in France to reveal the tricks of slackers. Scient. Am. Suppl., N. Y., 1917, lxxxiii, 372.
Detecting the act of being deaf; methods used in France to expose the tricks of slouches. Scient. Am. Suppl., N. Y., 1917, lxxxiii, 372.
Devaux et Logue. Les délires guerriers dans la fièvre typhoide. Presse méd., Par., 1915, v. 23, pp. 363-364.
Devaux and Logue. War delusions in typhoid fever. Medical Press, Paris, 1915, vol. 23, pp. 363-364.
Devaux et Logue. Les anxieux. 1917, Paris, Masson et Cie., pp. 283-300.
Devaux and Logue. The Anxious. 1917, Paris, Masson et Cie., pp. 283-300.
Dide, W. et Lhermitte, J. La diplégie brachiale spasmodique consécutive aux blessures par coup de feu de la région cervicale. Progrès méd., Par., 1917, No. 1, pp. 1-3.
Dide, W. and Lhermitte, J. Spastic diplegia in the arms following gunshot injuries to the neck. Med. Progress, Paris, 1917, No. 1, pp. 1-3.
Diederich-Schwalbe. Discussion, Everth, E. Von der Stelle des Soldats im Felde. Rev. in Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, p. 1351.
Diederich-Schwalbe. Discussion, Everth, E. Regarding the role of the soldier in the field. Rev. in Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, p. 1351.
Die behauptete Zunahme geistiger Erkrankungen bei Beginn des Krieges in der Zivilvölkerung Deutschlands. Psychiat.-neurol. Wchnschr., Halle a. S., 1915-16, v. 17, No. 29-30, 131-132.
The alleged increase in mental illnesses at the start of the war among the civilian population of Germany. Psychiat.-neurol. Wchnschr., Halle a. S., 1915-16, v. 17, No. 29-30, 131-132.
Di Pietro, S. Pneumotorace curativo o pneumotorace practicato a scopo di simulazione per esenzione dal servisio militare. Ann. di clin. med., Palermo, 1916, vii, 43-63.
Di Pietro, S. Therapeutic pneumothorax or pneumothorax performed for simulation purposes to avoid military service. Ann. of Clin. Med., Palermo, 1916, vii, 43-63.
Discussion of Functional Cases. Proc. Roy. Soc. Med. Lond., 1914-15, v. 8, (sect. laryngol.), pp. 117-120.
Discussion of Functional Cases. Proc. Roy. Soc. Med. Lond., 1914-15, v. 8, (sect. laryngol.), pp. 117-120.
Discussion on Shell Shock. Lancet, Lond., 1916, i, p. 306.
Discussion on Shell Shock. The Lancet, London, 1916, i, p. 306.
Discussion on the treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 1-44.
Discussion on the treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 1-44.
Discussion sur les troubles nerveux dits fonctionnels observés pendant la guerre. Rev. neurol., Par., 1914, xxii, 447-452.
Discussion on the so-called functional nervous disorders observed during the war. Rev. neurol., Par., 1914, xxii, 447-452.
Disordered action of the heart among soldiers. Jour. Lab. and Clin. Med., 1917, iii, 134.
Disordered action of the heart among soldiers. Jour. Lab. and Clin. Med., 1917, iii, 134.
Disqué. Behandlung der Kriegsneurosen durch Hypnose, Wachsuggestion und suggestive elektrische Anwendungen. Therapie der Gegenwart, May, 1918.
Disqué. Treatment of war neuroses through hypnosis, suggestion, and suggestive electrical applications. Therapy of the Present, May, 1918.
Dölger, R. Hysterische Erkrankungen des inneren Ohres neben allgem. Hysterie nach Granatenschlag u. Verschüssung. Münch. med. Wchnschr., nr. 16, 1918.
Dölger, R. Hysterical disorders of the inner ear alongside general hysteria following grenade wounds and closure. Münch. med. Wchnschr., no. 16, 1918.
D’Oelsnitz. L’adaptation organique des territoriaux à la guerre actuelle. Bull. et mém. soc. méd. d’hôp. de Par., 1915-16, v. 40, pp. 1935-44.
D’Oelsnitz. The organic adaptation of the territorial forces to the current war. Bull. et mém. soc. méd. d’hôp. de Par., 1915-16, v. 40, pp. 1935-44.
D’Oelsnitz, M. et Boisseau, J. Note sur les résultats des recherches oscillo-métriques pratiquées dans 100 cas de mains figées et 27 cas de pieds bots psychonévrosiques. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 1147-1149.
D’Oelsnitz, M. and Boisseau, J. Note on the results of oscillo-metric research conducted in 100 cases of frozen hands and 27 cases of psychoneurotic club feet. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 1147-1149.
Donald-Smith, Helen. War distress and war help; short catalogue of the leading war help societies. Lond. 1917, John Murray, 38 p. 16o.
Donald-Smith, Helen. War distress and war assistance; brief catalog of the main war aid organizations. London, 1917, John Murray, 38 pages. 16o.
Donath, J. Beiträge zu den Kriegsverletzungen und Erkrankungen des Nervensystems. Wien. klin. Wchnschr., 1915, v. 28, pp. 725-730, and pp. 763-766.
Donath, J. Contributions to War Injuries and Diseases of the Nervous System. Vienna Clinical Weekly, 1915, vol. 28, pp. 725-730, and pp. 763-766.
Donath, J. Schwere Polyneuritis rheumatica der Plexus brachiales bei einem Kriegsteilnehmer. Wien. klin. Wchnschr., Nr. 41, S. 1291.
Donath, J. Severe brachial plexus polyneuritis in a war participant. Wien. klin. Wchnschr., No. 41, p. 1291.
Droiin. Plaie du crâne par éclat d’obus. Epilepsie Jacksonnienne et hémiparésie. Cranioplastie par transplant cartilagineux. Résultats. Jour. de méd. de Bordeaux, 1915-16, v. 45, pp. 241-242.
Droiin. Skull wound from shell fragment. Jacksonian epilepsy and hemiparesis. Cranioplasty with cartilage graft. Results. Journal of Medicine of Bordeaux, 1915-16, v. 45, pp. 241-242.
Drouot, E. Pour les sourds de la guerre; rééducation auditive, lecture sur les lèvres, orthophonie. Rev. scient., Par., 1915, i, pp. 363-367.
Drouot, E. For the deaf from the war; auditory rehabilitation, lip reading, speech therapy. Sci. Rev., Paris, 1915, i, pp. 363-367.
Drug Habit and Mobilization in France. Lancet, Lond., 1915, i, p. 161.
Drug Habit and Mobilization in France. Lancet, London, 1915, 1, p. 161.
Dub. Heilung psychogenen Taubheit und Stummheit. Deutsche med. Wchnschr., Berl. u. Leipz., 1916, No. 52, pp. 1601-1602.
Dub. Healing psychogenic deafness and mutism. German medical weekly, Berlin and Leipzig, 1916, No. 52, pp. 1601-1602.
Dubois, Laumonier, Bouquet, Fiessinger, Pardel. Sur l’angoisse de guerre. Bull. gén. de thérap., Par., 1915-16, v. 168, pp. 821-828.
Dubois, Laumonier, Bouquet, Fiessinger, Pardel. On the Anxiety of War. Bull. gén. de thérap., Paris, 1915-16, vol. 168, pp. 821-828.
Duco, A. and Blum, E. Guide pratique du médecin dans les expertises médico-légales militaires. Collection Horizon, Masson et Cie, Paris, 1917.
Duco, A. and Blum, E. Practical Guide for Physicians in Military Forensic Evaluations. Horizon Collection, Masson et Cie, Paris, 1917.
Ducoste. Les contractures dans les lésions nerveuses périphériques. Compt. rend. Soc. de biol., Par., 1915, No. 14, p. 435.
Ducoste. Contractures in peripheral nerve injuries. Compt. rend. Soc. de biol., Paris, 1915, No. 14, p. 435.
Ducroquet. L’ankylose tibio-tarsienne et les troubles fonctionnels consécutifs. Presse méd., Par., 1917, v. 25, pp. 561-564.
Ducroquet. The ankle joint fusion and the resulting functional disorders. Medical Press, Paris, 1917, vol. 25, pp. 561-564.
Ducroquet. Les troubles fonctionnels dans les raideurs et les ankyloses douloureuses de l’articulation tibio-tarsienne. Presse méd., Par., 1917, v. 25, pp. 597-599.
Ducroquet. Functional issues in stiffness and painful ankylosis of the tibio-tarsal joint. Med. Press, Paris, 1917, vol. 25, pp. 597-599.
Dufour, Henri. De l’origine infectieuse de certaines hémiplégies par hémorrhagie et ramollissement cérébral. Rev. neurol., Par., 1917, v. 24, pp. 505-507.
Dufour, Henri. On the Infectious Origin of Certain Hemiplegias from Hemorrhage and Cerebral Softening. Neurological Review, Paris, 1917, v. 24, pp. 505-507.
Dufour, Henri, et Livy. Neurasthénie avec troubles de la nutrition décelée par l’examen du sang. Presse méd., Par., 1917, v. 25, p. 323.
Dufour, Henri, and Livy. Neurasthenia with nutrition issues detected through blood examination. Med Press, Paris, 1917, vol. 25, p. 323.
Duken, John. Ueber zwei Fälle von intrakranieller Pneumatocele nach Schussverletzung. Münch. med. Wchnschr., 1915, v. 621, pp. 598-599.
Duken, John. On Two Cases of Intracranial Pneumatocele Following Gunshot Injury. Münch. med. Wchnschr., 1915, v. 621, pp. 598-599.
Dumas. Sur les accidents nerveux determinés par la déflagration de fortes charges d’explosifs. Rev. neurol., Par., 1916, v. 29, pp. 593-595.
Dumas. On the nervous accidents caused by the explosion of large amounts of explosives. Neurology Review, Paris, 1916, vol. 29, pp. 593-595.
Dumas, R. Libération des nerfs et recupération fonctionnelle. Bulletins et Memoires de la Soc. de chirurgie de Paris, Feb. 8, 1916.
Dumas, R. Release of Nerves and Functional Recovery. Bulletins and Records of the Society of Surgery of Paris, Feb. 8, 1916.
Dumas, G. et Aimé, H. Les troubles mentaux et nerveux dans les armées Austro-Allemandes. J. de psychol. norm. et path., Par., 1915, v. 2, pp. 329-347.
Dumas, G. and Aimé, H. Mental and Nervous Disorders in the Austro-German Armies. J. of Norm. and Path. Psychol., Paris, 1915, vol. 2, pp. 329-347.
Dumas, G. and Delmas. Les confusions mentales d’origine commotionnelle chez les blessés. Arch. de méd. et pharm. mil., Par., 1917, lxvii, 69-77.
Dumas, G. and Delmas. Mental Confusions from Concussions in Injured Individuals. Arch. de méd. et pharm. mil., Paris, 1917, lxvii, 69-77.
Dumesnil, Marius A. Délires de guerre. Thèses de Paris, 1915-16, v. 5, No. 62.
Dumesnil, Marius A. War Deliriums. Paris Theses, 1915-16, v. 5, No. 62.
Dumesnil, Marius A. Délires de guerre. (Review.) Ann. d’hyg., Par., 1916, v. 26, p. 183.
Dumesnil, Marius A. War Deliriums. (Review.) Ann. d’hyg., Paris, 1916, v. 26, p. 183.
Dumolard, Rebierre et Quellien. Inhibition, variabilité, instabilité des réflexes tendineux. Rev. neurol., Par., 1916, v. 23, pp. 139-142.
Dumolard, Rebierre, and Quellien. Inhibition, variability, instability of tendon reflexes. Neurology Review, Paris, 1916, vol. 23, pp. 139-142.
Dumolard, Rebierre et Quellien. Réflexes tendineux variables. Seule manifestation clinique objective d’un état asthénique grave. Paris méd., 1916, v. 21 (part. méd.), pp. 286-288.
Dumolard, Rebierre, and Quellien. Variable tendon reflexes. The only objective clinical manifestation of a serious asthenic condition. Paris Méd., 1916, v. 21 (part. méd.), pp. 286-288.
Dumoz, A. G. The simulation of disease; drugs, chemicals, and septic materials used therefor. Pub. Health Rep., Wash., 1917, xxxii, 1887-1892.
Dumoz, A. G. The simulation of disease; drugs, chemicals, and septic materials used for that purpose. Pub. Health Rep., Wash., 1917, xxxii, 1887-1892.
Dunlap, Knight. Psychologic observations and methods. Jour. A. M. A., 1918, lxxi, 1392.
Dunlap, Knight. Psychological observations and methods. Journal of the American Medical Association, 1918, 71, 1392.
Dunn, Naughton. Treatment of lesions of the musculo-spiral nerve in military surgery. Amer. Jour. Orthop. Surg., 1918, xvi, 258.
Dunn, Naughton. Treatment of injuries to the musculo-spiral nerve in military surgery. Amer. Jour. Orthop. Surg., 1918, xvi, 258.
Duplant, A. G. Blessure du crâne datant de vingt mois. Abcès du cerveau à méningocoques. Meningite cérébrospinale. Presse méd., Par., v. 24, p. 366.
Duplant, A. G. Skull injury from twenty months ago. Brain abscess due to meningococci. Cerebrospinal meningitis. Presse méd., Par., v. 24, p. 366.
Dupont, J. et Troisier, Jean. Plaie perforante du crâne dans la région occipitale. Polyurie, dysphagie, tachycardie et zona cervical. Guérison. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 21-28.
Dupont, J. and Troisier, Jean. Penetrating skull wound in the occipital region. Increased urination, difficulty swallowing, rapid heartbeat, and cervical shingles. Recovery. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 21-28.
Dupouy, Roger. Notes statistiques et cliniques sur les troubles neuro-psychiques dans l’armée en temps de guerre. Ann. méd.-psychol., Par., 1914-15, v. 6, pp. 444-451.
Dupouy, Roger. Statistical and clinical notes on neuro-psychic disorders in the army during wartime. Ann. méd.-psychol., Par., 1914-15, v. 6, pp. 444-451.
Dupouy, R. Note sur les commotions cérébro-médullaires par l’explosion d’obus sans blessure extérieure. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 926-930.
Dupouy, R. Note on cerebral and spinal shock from shell explosions without external injuries. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 926-930.
Dupouy, R. Commotion cérébro-médullaire par éclatement rapproché. Presse méd., Par., 1916, v. 24, p. 52.
Dupouy, R. Close-range cerebral-medullary commotion. Médical Press, Paris, 1916, v. 24, p. 52.
Dupouy et Bosc. Troubles cérébro-médullaires par explosion de mine. Presse méd., Par., 1915, v. 23, p. 330.
Dupouy and Bosc. Cerebrospinal issues from mine explosions. Medical Press, Paris, 1915, vol. 23, p. 330.
Duprat, G. L. La psychothérapie en temps de guerre. Progrès méd., Par., 1917, No. 13, also No. 15, pp. 123-125.
Duprat, G. L. Psychotherapy in Wartime. Med. Progress, Par., 1917, No. 13, also No. 15, pp. 123-125.
Duprat, G. L. Rôle des complexus idéo-affectifs et de l’onirisme dans les syndrômes émotionnels. Progrès méd., Par., 1917, v. 43, pp. 357-360.
Duprat, G. L. The Role of Ideo-Affective Complexes and Dreaming in Emotional Syndromes. Med. Progress, Paris, 1917, v. 43, pp. 357-360.
Dupré. The emotions and the war. War Med., 1918, ii, 31.
Dupré. The emotions and the war. War Med., 1918, ii, 31.
Dupré, E. Recherches sur les symptômes homolatéraux dans les perforations du crâne et de l’encéphale par projectiles de guerre. Presse méd., Par., 1916, v. 24, p. 174.
Dupré, E. Studies on ipsilateral symptoms in skull and brain perforations caused by war projectiles. Medical Press, Paris, 1916, v. 24, p. 174.
Dupré, E. Réformes, incapacités, gratifications dans les états psychopathiques de guerre. Rev. neurol., Par., 1916, v. 23, pp. 790-799.
Dupré, E. Reforms, disabilities, rewards in psychopathic conditions of war. Neurology Review, Paris, 1916, vol. 23, pp. 790-799.
Dupré, E. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 471.
Dupré, E. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 471.
Dupré et Grimbert. La psychonévrose émotive constitutionelle et acquise. Rev. neurol., Par., 1917, v. 24, pp. 45-48.
Dupré et Grimbert. Constitutional and Acquired Emotional Psychoneurosis. Rev. neurol., Paris, 1917, v. 24, pp. 45-48.
Dupré, E., et LeFur. Paraplégie spasmodique par traumatisme du vertex. Rev. neurol., Par., 1914-15, v. 222, p. 406.
Dupré, E., and LeFur. Spastic paraplegia due to vertex trauma. Rev. neurol., Paris, 1914-15, v. 222, p. 406.
Dupré et Rist. Hémiplégie hystérique chez un cuirassier. Rev. neurol., Par., 1914-15, v. 22, p. 200.
Dupré and Rist. Hysterical hemiplegia in a cuirassier. Neurology Review, Paris, 1914-15, vol. 22, p. 200.
DuRoselle et Oberthür. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol., Par., 1916, v. 23, pp. 598-605.
DuRoselle and Oberthür. On nerve accidents caused by the detonation of large amounts of explosives. Neurological Review, Paris, 1916, v. 23, pp. 598-605.
Duroux, E. and Couvreur, E. Résultats éloignés expérimentaux et cliniques des sutures nerveuses. Rev. de Chir., 1917, liii, 401.
Duroux, E. and Couvreur, E. Experimental and Clinical Distant Results of Nerve Sutures. Rev. de Chir., 1917, liii, 401.
Dutheillet De Lamothe, G. Étude sur les troubles laryngés moteurs dans le paludisme. Thèses de Paris, 1916-17, Nr. 87.
Dutheillet De Lamothe, G. Study on motor laryngeal disorders in malaria. Paris Theses, 1916-17, No. 87.
Dutton, A. S. Beards in warfare. Med. Press and Circ., Lond., 1915, v. 100, p. 520.
Dutton, A. S. Beards in warfare. Med. Press and Circ., Lond., 1915, v. 100, p. 520.
Duvernay, L. Contractures post-traumatiques en chirurgie de guerre. Paris méd., 1915, v. 17 (part. méd.), pp. 429-437.
Duvernay, L. Post-traumatic contractures in wartime surgery. Paris méd., 1915, v. 17 (part. méd.), pp. 429-437.
Dyakonoff, P. P. (Cases of self-inflicted injury to avoid military service.) Vestnik Obshtsh. Hig., Sudeb. i Prakt. Med., Petrogr., 1916, v. 52, pp. 1080-1082.
Dyakonoff, P. P. (Cases of self-inflicted injury to avoid military service.) Vestnik Obshtsh. Hig., Sudeb. i Prakt. Med., Petrogr., 1916, v. 52, pp. 1080-1082.
Eager, E. War psychoses occurring in cases with a definite history of shell shock. Brit. Med. Jour., 1918, i, 422.
Eager, E. War psychoses happening in cases with a clear history of shell shock. Brit. Med. Jour., 1918, i, 422.
Ebel, S. Einige Bemerkungen über physikalische Therapie der Kriegskrankheiten. Ztschr. f. Phys. u. Diätet. Therapie, Leipzig. 1915, v. 19, pp. 182-190.
Ebel, S. Some Remarks on the Physical Therapy of War Injuries. Journal of Physical and Dietary Therapy, Leipzig. 1915, v. 19, pp. 182-190.
Ebers, E. M. Functional Reëducation and Vocational Training of Soldiers disabled in War. Canad. M. Ass. J., 1917, No. 3, pp. 193-200.
Ebers, E. M. Functional Rehabilitation and Job Training for Soldiers Disabled in War. Canad. M. Ass. J., 1917, No. 3, pp. 193-200.
Edel. Psycho-analytische Behandlung der Hysterie im Lazarett. Psychiat.-neurol. Wchnschr., Halle a. S., 1916, v. 17, No. 2. Rev. Aerztl. Rundschau, München, 1916, v. 26, pp. 128-130.
Edel. Psychoanalytic treatment of hysteria in the hospital. Psychiatric and Neurological Weekly, Halle a. S., 1916, v. 17, No. 2. Review Medical Roundup, Munich, 1916, v. 26, pp. 128-130.
Edel, K. Krieg und Geisteskranken. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 590.
Edel, K. War and Mental Illness. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 590.
Edel, M. Neurosen und Psychosen. Deutsche med. Wchnschr., 1915, v. 411, p. 30.
Edel, M. Neuroses and Psychoses. German Medical Weekly, 1915, v. 411, p. 30.
Eder, M. D. The psychopathology of the war neuroses, Lancet, Lond., 1916; ii, pp. 264-268.
Eder, M. D. The mental health issues related to war trauma, Lancet, London, 1916; ii, pp. 264-268.
Eder, M. D. War Shock. Philadelphia, Blakiston Son & Co. and Wm. Heinemann, 1917.
Eder, M. D. War Shock. Philadelphia, Blakiston Son & Co. and Wm. Heinemann, 1917.
Effects of high explosives. Jour. A. M. A., 1917, lxviii, 1182.
Effects of high explosives. Jour. A. M. A., 1917, lxviii, 1182.
Effect (The) of the war upon psychiatry in England. Lancet, Lond., 1917, ii, 352.
The Effect of the War on Psychiatry in England. Lancet, London, 1917, ii, 352.
Ehrmann. Notiz über die Herztätigkeit während Granatfeuers. Ztschr. f. Phys. u. Diätet. Therap., Leipz., 1915, v. 19, p. 52.
Ehrmann. Note on heart activity during shelling. Journal of Physical and Dietary Therapy, Leipzig, 1915, vol. 19, p. 52.
Elliott, T. R. Transient paraplegia from shell explosions. Brit. M. J., Lond., 1914, ii, pp. 1005-1006.
Elliott, T. R. Temporary paralysis from shell explosions. Brit. M. J., Lond., 1914, ii, pp. 1005-1006.
Emerson, E. B. Mental states responsible for malingering. Med. Press, Lond., 1917, n. s., civ, 433-436.
Emerson, E. B. Mental states responsible for faking illness. Medical Press, London, 1917, n.s., civ, 433-436.
Emslie, Isabel. The war and psychiatry. Edinb. M. J., 1915, v. 14, p. 359.
Emslie, Isabel. The war and psychiatry. Edinb. M. J., 1915, v. 14, p. 359.
Engelen. Beurteilung der Persuasion (Unter Bezugnahme auf die Kriegsneurosen und Unfallsneurosen). Aerztl. sachv. Ztg., Berl., 1915, v. 2, pp. 157-163, and pp. 171-175.
Engelen. Evaluation of Persuasion (Regarding War and Accident Neuroses). Medical Expert Journal, Berlin, 1915, vol. 2, pp. 157-163, and pp. 171-175.
Engelen and Rangette. Nachweis von Simulation durch das Assoziations-Experiment. Aerztl. Sachverst.-Ztg., Berl., 1916, v. 22, pp. 37-40.
Engelen and Rangette. Evidence of simulation through the association experiment. Medical Expert Report Journal, Berlin, 1916, vol. 22, pp. 37-40.
Epstein, L. (The war and psychoses.) Gyógyászat, Budapest, 1915, v. 55, pp. 40-43.
Epstein, L. (The war and psychoses.) Medicine, Budapest, 1915, v. 55, pp. 40-43.
Erben, S. Ueber die motorischen Reizerscheinungen bei Kriegsteilnehmern. Wien. klin. Wchnschr., 1916, v. 29, pp. 1129-1134.
Erben, S. On the Motor Reaction Phenomena in War Participants. Wien. klin. Wchnschr., 1916, v. 29, pp. 1129-1134.
Erving, William G. Orthopedic treatment of nerve lesions. Amer. Jour. Orth. Surg., 1918, xvi, 346.
Erving, William G. Orthopedic treatment of nerve injuries. Amer. Jour. Orth. Surg., 1918, xvi, 346.
Escat, E. Epreuve des diapasons unisonnants appliquée, au diagnostic de la surdité unilatérale simulée. Presse Méd., Par., 1916, v. 24, pp. 562-563.
Escat, E. Test of unison tuning forks applied to the diagnosis of simulated unilateral deafness. Med. Press, Paris, 1916, vol. 24, pp. 562-563.
Eschbach, H. et Lacaze, H. Méningite cérébrospinale débutant par des troubles mentaux. Bull. et mém. Soc. Méd. d’Hôp. de Par., 1915, v. 39, pp. 1024-1029.
Eschbach, H. and Lacaze, H. Cerebrospinal meningitis starting with mental disturbances. Bull. and mém. Soc. Méd. d’Hôp. de Par., 1915, v. 39, pp. 1024-1029.
Estève. La nostalgie des militaires. Gaz. méd. de Par., 1916, v. 87, pp. 122-123.
Estève. The nostalgia of soldiers. Gaz. méd. de Par., 1916, v. 87, pp. 122-123.
États anxieux. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 89-90.
Anxious States. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 89-90.
Eugène, V. Paralysie radiale par section complète du nerf, avec perte de substance de 3 centimetres suture; guérison avec recuperation des fonctions motrices du nerf. Lyon Méd., 1916, v. 125, pp. 192-194.
Eugène, V. Complete radial paralysis due to a full cut of the nerve, with a loss of substance of 3 centimeters; healed with recovery of the nerve's motor functions. Lyon Méd., 1916, v. 125, pp. 192-194.
Evans, J. J. Organic Lesions from Shell Concussion. Brit. M. J., Lond., 1915, ii, pp. 848.
Evans, J. J. Organic Injuries from Shell Shock. Brit. M. J., Lond., 1915, ii, pp. 848.
Evans, Jameson. The Peripheral Lesions of Shell Concussion. Brit. M. J., Lond., 1916, i, pp. 721.
Evans, Jameson. The Peripheral Lesions of Shell Concussion. British Medical Journal, London, 1916, vol. 1, pp. 721.
Everidge, John. Mental symptoms complicating a case of acute tetanus during treatment by carbolic injections. Brit. M. J., Lond., 1916, i, pp. 443-444.
Everidge, John. Mental symptoms complicating a case of acute tetanus during treatment with carbolic injections. Brit. M. J., Lond., 1916, i, pp. 443-444.
Everth, E. Von der Seele des Soldaten im Felde. Jena, 1915. Rev.-Deutsche Med. Wchnschr., Berl. u. Leipz., 1915, v. 412, p. 1351.
Everth, E. On the Soul of the Soldier in the Field. Jena, 1915. Rev.-German Med. Weekly, Berlin and Leipzig, 1915, vol. 412, p. 1351.
Farrar, Clarence B. Neuroses among returned soldiers; types and indications. Bos. M. & S. J., 1918, clxxix, 583, 615.
Farrar, Clarence B. Neuroses among returning soldiers; types and signs. Bos. M. & S. J., 1918, clxxix, 583, 615.
Farrar, C. B. War and neurosis, with some observations of the Canadian Expeditionary Force. Am. J. Insan., Balt., 1917, v. 73, pp. 693-719.
Farrar, C. B. War and neurosis, with some observations of the Canadian Expeditionary Force. Am. J. Insan., Balt., 1917, v. 73, pp. 693-719.
Farrar, C. B. The problem of mental disease in the Canadian Army. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 389-391.
Farrar, C. B. The issue of mental illness in the Canadian Army. Mental Hyg., Concord, N. H., 1917, v. 1, pp. 389-391.
Farrar, Clarence B. War neuroses and psychoses. Amer. Jour. Med. Sc., 1918, clv, 425.
Farrar, Clarence B. War neuroses and psychoses. Amer. Jour. Med. Sc., 1918, clv, 425.
Fauntleroy. Military organization and equipment in the present war. U. States Nav. M. Bull., Wash., 1916, v. 10, pp. 34-61.
Fauntleroy. Military organization and equipment in the current war. U. States Nav. M. Bull., Wash., 1916, v. 10, pp. 34-61.
Faure, J. L. Sur les tumeurs provoquées par l’huile camphorée. Bull. et mém. Soc. de chir. de Par., 1917, n. s., xliii, 525.
Faure, J. L. On tumors caused by camphor oil. Bull. et mém. Soc. de chir. de Par., 1917, n. s., xliii, 525.
Faure, Maurice. La rééducation motrice des blessés et infirmes de la guerre. Bull. gén. de Thérap., Par., 1916, v. 168, pp. 40-46.
Faure, Maurice. The Motor Rehabilitation of War Injured and Disabled Individuals. Bull. gén. de Thérap., Par., 1916, v. 168, pp. 40-46.
Fauser, A. Über dysglanduläre Psychosen. Deutsche med. Wchnschr., Berl. u. Leipz., 1916, No. 2, pp. 47-49.
Fauser, A. On Dysglandular Psychoses. German Medical Weekly, Berlin and Leipzig, 1916, No. 2, pp. 47-49.
Fazio, F. La cura del mutismo psicoisterico dei militari combattenti. Med. prat., Napoli, 1916, v. 1, pp. 371-373.
Fazio, F. The treatment of psychogenic mutism in combat soldiers. Med. prat., Naples, 1916, vol. 1, pp. 371-373.
Fearnsides. Wassermann reaction in shell shock. Proc. Roy. Soc. Med., London., (Sec. of Neurol.), 1915-16, v. 9, pp. 39-41.
Fearnsides. Wassermann reaction in shell shock. Proc. Roy. Soc. Med., London., (Sec. of Neurol.), 1915-16, v. 9, pp. 39-41.
Feilchenfeld, Hugo. Ein objektives Symptom zur Prüfung der Nachtblindheit. Berl. Klin. Wchnschr., 1916, No. 44, pp. 1195-1196.
Feilchenfeld, Hugo. An objective symptom for testing night blindness. Berl. Klin. Wchnschr., 1916, No. 44, pp. 1195-1196.
Feilchenfeld und Bauer. Kriegsblinden Fürsorge. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, pp. 1324.
Feilchenfeld and Bauer. Care for War Blinded. German Medical Weekly, Leipzig and Berlin, 1916, vol. 42, pp. 1324.
Feiling, Anthony. Loss of personality from shell shock. Lancet, Lond., 1915, ii, pp. 63.
Feiling, Anthony. Loss of personality from shell shock. Lancet, London, 1915, ii, pp. 63.
Fellner, B. Fall von echter Katatonie (Mähren). Wien. med. Wchnschr., 1915, No. 30, pp. 1155.
Fellner, B. Case of genuine catatonia (Moravia). Wien. med. Wchnschr., 1915, No. 30, pp. 1155.
Felzmann. (War psychoses). J. Neuropath. i. Psikhiat., Korsakova, Mosk., 1915, v. 15, No. 4.
Felzmann. (War psychoses). J. Neuropath. i. Psikhiat., Korsakova, Mosk., 1915, v. 15, No. 4.
Fenwick, P. C. C. Entero-spasm following shell shock. Practitioner, Lond., 1917, s. xviii, 391.
Fenwick, P. C. C. Entero-spasm after shell shock. Practitioner, London, 1917, s. xviii, 391.
Fernández Sanz. Contribución á la psiquiatria de la guerra; comentarios al determinismo causal y á la sintomatología de la psicosis de origen belico. Rev. clin. de Madrid, 1915, v. 13, pp. 121-131.
Fernández Sanz. Contribution to the psychiatry of war; comments on causal determinism and the symptoms of war-induced psychosis. Clin. Rev. of Madrid, 1915, v. 13, pp. 121-131.
Fernet, Charles. De la surdité et de son traitement par l’activité fonctionelle. J. de Méd. et de chir., 1915, v. 86, Apr.
Fernet, Charles. On Deafness and Its Treatment Through Functional Activity. J. de Méd. et de chir., 1915, v. 86, Apr.
Fernet, Charles. De la gymnastique oculaire et de son application à l’éducation de la vue et au traitement de la myopie et de la presbyopie. J. de Méd. et chir. prst., Par., 1916, v. 87, pp. 153-157.
Fernet, Charles. On Eye Gymnastics and Its Application to Vision Education and the Treatment of Myopia and Presbyopia. J. de Méd. et chir. prst., Paris, 1916, vol. 87, pp. 153-157.
Ferrand, J. Réflexions médicochirurgicales sur la pratique neurologique en temps de guerre. J. de radiol. et d’électrol., Par., 1914-15, i, pp. 629-639.
Ferrand, J. Medical and Surgical Reflections on Neurological Practice in Times of War. J. of Radiology and Electrology, Paris, 1914-15, i, pp. 629-639.
Ferrand, Jean. Aphasie avec hémiplegie gauche par ligature de la carotide primitive droite. Paris Méd., 1916 (Part. Méd.), v. 19, pp. 537-540.
Ferrand, Jean. Aphasia with left hemiplegia due to ligation of the right common carotid artery. Paris Méd., 1916 (Med. Part.), vol. 19, pp. 537-540.
Ferrand, J. Y-a-t-il des hystéro-traumatismes différents en temps de paix et en temps de guerre? Rev. de méd., Par., 1916, v. 35, pp. 239-275; and pp. 293-313.
Ferrand, J. Are there different hystero-traumas in peacetime and wartime? Rev. de méd., Par., 1916, v. 35, pp. 239-275; and pp. 293-313.
Ferrand, Jean. Y-a-t-il des hystéro-traumatismes différents en temps de paix et en temps de guerre? Rev. de méd., mai-juin, 1917, Rev. Progrès méd., Par., 1917, v. 43, pp. 356-357.
Ferrand, Jean. Are there different hystero-traumas in times of peace compared to times of war? Med. Rev., May-June, 1917, Progrès Méd. Rev., Paris, 1917, vol. 43, pp. 356-357.
Ferrand, Jean. Hystéro-traumatismes avec syndrôme dit “physiopathique” guéri par la rééducation. Progrès méd., Par., 1917, No. 10, pp. 81-83.
Ferrand, Jean. Hystero-traumas with what is called "physiopathological" syndrome treated by rehabilitation. Progrès méd., Par., 1917, No. 10, pp. 81-83.
Ferrand, Jean. De l’unité clinique et pathogénique de tous les hystéro-traumatismes. Paris méd., 1917, No. 24, pp. 509-512.
Ferrand, Jean. On the Clinical and Pathogenic Unity of All Hystero-Traumas. Paris méd., 1917, No. 24, pp. 509-512.
Ferrannini, L. La rieducazione professionale degli invalidi della guerra. Riforma, med., Napoli, 1917, v. 33, pp. 347-349.
Ferrannini, L. The professional rehabilitation of war invalids. Reform, med., Naples, 1917, vol. 33, pp. 347-349.
Ferrie, Jean L. Contribution à l’étude des voyages pathologiques chez les alienés militaires. Thèses de Paris, 1915, v. 5.
Ferrie, Jean L. Contribution to the study of pathological travels in military personnel. Paris Theses, 1915, v. 5.
Feuillade. Sur les accidents nerveux determinés par la déflagration de fortes charges d’explosifs. Rev. neurol. Par., 1916, v. 29, pp. 591-592.
Feuillade. On the nerve accidents caused by the explosion of large amounts of explosives. Rev. neurol. Par., 1916, v. 29, pp. 591-592.
Fiessinger, Ch. Le rôle psychologique du vin. Bull. Acad. de méd., Par., No. 8, fer. 1916. Paris Méd., 1916 (Part. Méd.), v. 19, p. 210.
Fiessinger, Ch. The psychological role of wine. Bull. Acad. de méd., Par., No. 8, fer. 1916. Paris Méd., 1916 (Part. Méd.), v. 19, p. 210.
Fiessinger, Noel. Choc emotionnel par explosion d’obus de gros calibre. Rev. gén. de clin. et de thérap., 1915, v. 29, pp. 99-100.
Fiessinger, Noel. Emotional shock from a large-caliber shell explosion. Gen. Rev. of Clin. and Therap., 1915, v. 29, pp. 99-100.
Fiessinger, Noel. Emotional Shock. Med. Press and Circ., Lond., 1915, v. 99, p. 563.
Fiessinger, Noel. Emotional Shock. Med. Press and Circ., Lond., 1915, v. 99, p. 563.
Fischer, H. Six months of war surgery in a base hospital in Germany. Am. J. Surg., N. Y., 1917, v. 31, pp. 4-10.
Fischer, H. Six months of war surgery in a base hospital in Germany. Am. J. Surg., N. Y., 1917, v. 31, pp. 4-10.
Fischer, H. Gunshot injuries of the peripheral nerves and their treatment. Ann. of Surg., 1917, lxv, 56.
Fischer, H. Gunshot injuries to the peripheral nerves and how to treat them. Ann. of Surg., 1917, lxv, 56.
Fischer, M. Die Erwerbsfürsorge für Kriegsinvalide an unseren Heil- und Pflegeanstalten. Psych.-neurol. Wchnschr., Halle a. S., 1915, v. 16, p. 420.
Fischer, M. The welfare support for disabled war veterans at our healing and care facilities. Psych.-neurol. Wchnschr., Halle a. S., 1915, v. 16, p. 420.
Flesch, J. Ueber sogen. funktionelle Nervenerkrankungen. Psychiatr.-neurol. Wchnschr., 20, 1918-9.
Flesch, J. On so-called functional nerve diseases. Psychiatr.-neurol. Wchnschr., 20, 1918-9.
de Flines, E. W. Doofheid, simulatie en dissimulatie. Mil.-geneesk. Tijdschr., Haarlem, 1917, xxi, 124-133.
de Flines, E. W. Deafness, Simulation, and Dissimulation. Mil.-med. J., Haarlem, 1917, xxi, 124-133.
Flusser, E. Über Psychosen beim Kriegstyphus. Wien. med. Wchnschr., 1915, v. 65, No. 297.
Flusser, E. On Psychoses in War Typhus. Wien. med. Wchnschr., 1915, v. 65, No. 297.
Foix, Ch. Contribution à l’étude de l’apraxie idéo-motrice, de son anatomie pathologique et de ses rapports avec les syndrômes qui ordinairement l’accompagnent. Rev. neurol., Par., 1916, v. 29, p. 283.
Foix, Ch. Contribution to the study of ideomotor apraxia, its pathological anatomy, and its relationship with the syndromes that usually accompany it. Rev. neurol., Paris, 1916, v. 29, p. 283.
Folgezustände. Über durch der Krieg bedrohte Folgezustände am Nervensystem. Berl. klin. Wchnschr., 1915, v. 42, p. 277.
Consequences. On the consequences for the nervous system threatened by war. Berl. klin. Wchnschr., 1915, v. 42, p. 277.
Forgues. Maladies simulées. Caducée, Par., 1915, v. 15, pp. 132-133.
Forgues. Faked Illnesses. Caducée, Paris, 1915, vol. 15, pp. 132-133.
Forster. Der Krieg und die traumatischen Neurosen. Monatschr. f. Psychiat. u. Neurol., Berl., 1915, v. 37, pp. 72-75.
Forster. The War and Traumatic Neuroses. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, vol. 37, pp. 72-75.
Forster, Frederick C. Management of neurasthenia, psychasthenia, shell-shock, and allied conditions. Practitioner, 1918, c. 85.
Forster, Frederick C. Management of neurasthenia, psychasthenia, shell shock, and related conditions. Practitioner, 1918, c. 85.
Forsyth, David. Functional nervous disease and the shock of battle: a study of the so-called traumatic neuroses arising in connection with the war. Lancet, Lond., 1915, ii, pp. 1399. (See also Mercier, Lancet, Lond., 1916, i, P. 154.)
Forsyth, David. Functional nervous disease and the shock of battle: a study of the so-called traumatic neuroses related to the war. Lancet, Lond., 1915, ii, pp. 1399. (See also Mercier, Lancet, Lond., 1916, i, P. 154.)
Fortineau, Louis. Quelques cas de délire onirique observés au cours de la fièvre typhoïde. Presse Méd., Par., 1915, v. 23, p. 225.
Fortineau, Louis. A few cases of dream-like delirium observed during typhoid fever. Medical Press, Paris, 1915, vol. 23, p. 225.
Foucault, Prof. Expériences sur la fatigue mentale. Rev. phil., Par., 1915, v. 79. pp. 505-526.
Foucault, Prof. Experiments on Mental Fatigue. Rev. Phil., Paris, 1915, vol. 79, pp. 505-526.
Fox, R. Fortescue. Model hydrotherapeutic installation for soldiers with ground plan. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 660-664. Also, The “sedative pool bath”—Lancet, Lond., 1916, v. ii, p. 302.
Fox, R. Fortescue. Model hydrotherapy setup for soldiers with floor plan. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 660-664. Also, The “calming pool bath”—Lancet, Lond., 1916, v. ii, p. 302.
Fox, R. Fortescue. Physical remedies for disabled soldiers. Lond., 1917, Bailliere, p. 287, 8o.
Fox, R. Fortescue. Physical treatments for injured soldiers. London, 1917, Bailliere, p. 287, 8o.
Frank. Krieg und ärztliche Sachverständigentätigkeit. Ärztl. Sachverst. Ztg., Berl., 1914, No. 23, pp. 434-436.
Frank. War and Medical Expert Activity. Medical Expert Journal, Berlin, 1914, No. 23, pp. 434-436.
Fraser, J. S. War Injuries of the Ear. Edinb. M. J., 1917, p. 107.
Fraser, J. S. War Injuries of the Ear. Edinb. M. J., 1917, p. 107.
Fraser, J. S. and John. The Morbid Anatomy of War Injuries of the Ear. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (see Otol.), pp. 56-90.
Fraser, J. S. and John. The Morbid Anatomy of War Injuries of the Ear. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (see Otol.), pp. 56-90.
French wounded from some early actions. Brit. M. J., Lond., 1914, ii, p. 853-854.
French wounded from some early actions. Brit. M. J., Lond., 1914, ii, p. 853-854.
Frenkel, H. L’héméralopie chez les mobilisés de l’intérieur. Arch. d’opht., Par., 1917, v. 35, pp. 577-579.
Frenkel, H. Night blindness in mobilized individuals from within. Arch. d’opht., Par., 1917, v. 35, pp. 577-579.
Freud, Sigmund. Zeitgemässes über Krieg und Tod. Imago, Leipz. and Wien., 1915, v. 4, pp. 1-21.
Freud, Sigmund. Contemporary Views on War and Death. Imago, Leipzig and Vienna, 1915, v. 4, pp. 1-21.
Frey, Hugo and Selye, Hugo. Beiträge zur Chirurgie der Schussverletzungen des Gehirns. Wien. klin. Wchnschr., 1915, v. 28, pp. 722-724.
Frey, Hugo and Selye, Hugo. Contributions to the Surgery of Gunshot Wounds of the Brain. Vienna. Clinical Weekly, 1915, v. 28, pp. 722-724.
Friedländer, A. Nerven- und Geisteskrankheiten im Felde und im Lazarett. Wiesb., 1914 (J. J. Bergmann), p. 39, 8o.
Friedländer, A. Nervous and Mental Illnesses in the Field and in the Hospital. Wiesb., 1914 (J. J. Bergmann), p. 39, 8o.
Friedländer, R. Julius. Zerebellare Symptomenkomplexe nach Kriegsverletzungen. Neurol. Centralbl., Leipz., 1915, v. 34, p. 813.
Friedländer, R. Julius. Cerebellar symptom complexes after war injuries. Neurol. Centralbl., Leipzig, 1915, vol. 34, p. 813.
Friedmann. Zur Auffassung die gehäuftigten kleinen Anfälle. Monatschr. f. Psychiat. u. Neurol., Berl., 1915, v. 38, p. 76.
Friedmann. On the view of frequent minor seizures. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, v. 38, p. 76.
Fröderström, H. (Neurological impressions (May, 1916) from a travel report to the chief of the naval medical department.) Tidskr. i mil. Hälsov., Stockholm, 1917, v. 42, pp. 137-149.
Fröderström, H. (Neurological impressions (May, 1916) from a travel report to the head of the naval medical department.) Tidskr. i mil. Hälsov., Stockholm, 1917, v. 42, pp. 137-149.
Froment, J. Paraplégie par déflagration d’obus. Rev. neurol., Par., 1914, v. 22, pp. 754-755, and pp. 1205-1214.
Froment, J. Paraplegia from shell explosion. Neurological Review, Paris, 1914, vol. 22, pp. 754-755, and pp. 1205-1214.
Froment, J. Du pronostic de l’aphasie traumatique consécutive aux plaies du crâne par armes à feu. Lyon chirurg., 1916, v. 13, pp. 434-447.
Froment, J. On the prognosis of traumatic aphasia resulting from gunshot wounds to the skull. Lyon surgeon, 1916, vol. 13, pp. 434-447.
Froment. La préhension dans les paralysies du nerf cubital et le signe du pouce. Presse méd., Oct. 21, 1915.
Froment. Grasping in ulnar nerve paralysis and the thumb sign. Medical Press, Oct. 21, 1915.
Fuchs, W. Mobilmachungspsychosen. Aerztl. Sachverst.-Ztg., Berl., 1915, xxi, 25-29.
Fuchs, W. Mobilization Psychoses. Medical Expert Report Journal, Berlin, 1915, xxi, 25-29.
Functional cardiac disorders in soldiers. J. Am. M. Ass., Chicago, 1917, v. 69, p. 202.
Functional cardiac disorders in soldiers. J. Am. M. Ass., Chicago, 1917, v. 69, p. 202.
Furbush, Edith M. Mental disease, suicides and homicides in the United States Army and Navy, 1897-1915, prepared from the Annual Reports of the Surgeons-General. Mental Hyg., Concord, N. H., 1917, i, 406-408.
Furbush, Edith M. Mental illness, suicides, and homicides in the United States Army and Navy, 1897-1915, compiled from the Annual Reports of the Surgeons General. Mental Hyg., Concord, N. H., 1917, i, 406-408.
Further Extension of Second Eastern General Hospital, Brighton. Brit. M. J., Lond., 1915, i, p. 908.
Further Extension of Second Eastern General Hospital, Brighton. Brit. M. J., Lond., 1915, i, p. 908.
Gaillard. Tachypnée hystérique chez un militaire. Bulletins de la Société Médicale des Hôpitaux de Paris, 30 décembre 1915.
Gaillard. Hysterical tachypnea in a soldier. Reports of the Medical Society of the Hospitals of Paris, December 30, 1915.
Garbo. A propos du choc gazeux causé par l’explosion des obus. Wien. Klin. Woch., No. 4, 1915.
Garbo. Regarding the gas shock caused by the explosion of shells. Wien. Klin. Woch., No. 4, 1915.
Garrod, A. E. War heart, which calls for treatment by complete rest. Lancet, Lon., 1917, i, 985.
Garrod, A. E. War heart, which needs treatment through complete rest. Lancet, Lon., 1917, i, 985.
Garton, W. Shell shock and its treatment by cerebrospinal galvanism. Brit. Med. Jour., 1916, ii, 584.
Garton, W. Shell shock and its treatment with cerebrospinal galvanism. Brit. Med. Jour., 1916, ii, 584.
Garton, Wilfrid. Shell shock and its treatment by cerebrospinal galvanism. Brit. M. J., 1916, v. ii, pp. 584-586.
Garton, Wilfrid. Shell shock and its treatment with cerebrospinal galvanism. Brit. M. J., 1916, v. ii, pp. 584-586.
Gaté, J. et M. Dechosal. Méningite cérébro-spinale à pseudoméningocoque. Lyon Méd., 1916, v. 125, pp. 349-352.
Gaté, J. and M. Dechosal. Cerebrospinal Meningitis due to Pseudomeningococcus. Lyon Méd., 1916, v. 125, pp. 349-352.
Gaucher et Renée Klein. Le psoriasis émotif et traumatique. Paris méd., 1916, (Part. Méd.), v. 18, pp. 428-430.
Gaucher and Renée Klein. Emotional and Traumatic Psoriasis. Paris Med., 1916, (Part. Med.), v. 18, pp. 428-430.
Gaupp, R. Granatkontusion. Bruns. Beitr. 96 H. 3. Rev. Deutsche med. Wchnschr., 1915, v. 412, pp. 811-812.
Gaupp, R. Granatkontusion. Bruns. Beitr. 96 H. 3. Rev. Deutsche med. Wchnschr., 1915, v. 412, pp. 811-812.
Gaupp, R. Hysterie und Kriegsdienst. Münch. med. Wchnschr., 1915, v. 62, pp. 361-363.
Gaupp, R. Hysteria and Military Service. Munich Medical Weekly, 1915, v. 62, pp. 361-363.
Gaupp, R. Ungewöhnliche Formen der Hysterie bei Soldaten. Münch. med. Wchnschr., 1915, v. 33, p. 1119.
Gaupp, R. Unusual Forms of Hysteria in Soldiers. Münch. med. Wchnschr., 1915, v. 33, p. 1119.
Gaupp, R. Ungewöhnliche Formen der Hysterie bei Soldaten. Psychiat. Neurol. Wchnschr., Halle a. S., 1915-16, v. 17, p. 256.
Gaupp, R. Unusual Forms of Hysteria in Soldiers. Psychiat. Neurol. Wchnschr., Halle a. S., 1915-16, v. 17, p. 256.
Gaupp, R. Die Granatkontusion. Beitr. z. klin. Chir., Tübing., 1915, v. 96B, pp. 277-294.
Gaupp, R. The Grenade Contusion. Contributions to Clinical Surgery, Tübingen, 1915, vol. 96B, pp. 277-294.
Gaupp, R. Die Granatkontusion. Centralbl. f. Chir., Leipz., 1915, v. 421, pp. 429-430.
Gaupp, R. The Grenade Contusion. Central Journal of Surgery, Leipzig, 1915, vol. 421, pp. 429-430.
Gaupp, R. Die Diensbrauchbarkeit der Epileptiker und Psychopathen. Die militärärztliche Sachsverständigentatigkeit auf dem Gebiete des Ersatzwesens und der militärischen Versorgung. Erste Teil., pp. 115-139. Jean Fischer, 1917.
Gaupp, R. The Usability of Epileptics and Psychopaths. The military medical expert activity in the field of replacement services and military supply. First part, pp. 115-139. Jean Fischer, 1917.
Gautrelet, J. Les bases scientifiques de l’éducation professionnelle des mutilés. Bull. Acad, de Méd., Par., 1915, v. 73, pp. 663-668.
Gautrelet, J. The Scientific Foundations of Vocational Education for the Disabled. Bull. Acad, de Méd., Par., 1915, v. 73, pp. 663-668.
Geigel. Nervöses Herz und Herzneurosen. Münch. Med. Wchnschr., 1917, No. 1, pp. 30-32.
Geigel. Nervous heart and heart neuroses. Münch. Med. Wchnschr., 1917, No. 1, pp. 30-32.
Gennerich, W. Die Ursachen von Tabes und Paralyse. Monatschr. f. Psychiat. u. Neurol., Berl., 1916, v. 39, No. 6, p. 341.
Gennerich, W. The Causes of Tabes and Paralysis. Monthly Journal of Psychiatry and Neurology, Berlin, 1916, vol. 39, no. 6, p. 341.
Gerhardt. Uber Herzstörungen im Kriege. Münch. med. Wchnschr., 1915, v. 342, p. 1174.
Gerhardt. On Heart Disorders in War. Munich Medical Weekly, 1915, v. 342, p. 1174.
Gerhardt. Hysterische Paraplegie. Münch. med. Wchnschr., 1915, v. 342, pp. 1763.
Gerhardt. Hysterical Paraplegia. Münch. med. Wchnschr., 1915, v. 342, pp. 1763.
Gerstmann. Hemianopie durch Contrecoup nach Schussverletzung. Klin. therap. Wchnschr., Wien. u. Berl., 1916, v. 332, p. 29.
Gerstmann. Hemianopsia due to contrecoup from a gunshot injury. Clin. Ther. Wchnschr., Vienna and Berlin, 1916, v. 332, p. 29.
Gerver, A. V. (A study of statistics of mental diseases in the army in time of war.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 158-165.
Gerver, A. V. (A study of statistics on mental illnesses in the military during wartime.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 158-165.
Gerver, A. V. (Mental diseases in the theatre of war.) Russk. Vrach., Petrogr., 1915, v. 14, p. 793; p. 817; p. 841.
Gerver, A. V. (Mental illnesses in wartime.) Russk. Vrach., Petrograd, 1915, v. 14, p. 793; p. 817; p. 841.
Gerver, A. V. (Traumatic neuroses among soldiers). Russk. Vrach., Petrogr., 1915, v. 14, pp. 937-944; and pp. 967-972.
Gerver, A. V. (Traumatic neuroses in soldiers). Russk. Vrach., Petrogr., 1915, v. 14, pp. 937-944; and pp. 967-972.
Gerver, A. V. (Neurasthenia and influence of the war on its symptomatology.) Russk. Vrach., Petrogr., 1916, v. 15, p. 220; p. 241.
Gerver, A. V. (Neurasthenia and the impact of the war on its symptoms.) Russk. Vrach., Petrogr., 1916, v. 15, p. 220; p. 241.
Giachetti, C. I caratteri e la guerra. Riv. di psicol., Bologna, 1916, v. 12, pp. 301-316.
Giachetti, C. Characters and War. Journal of Psychology, Bologna, 1916, vol. 12, pp. 301-316.
Giannelli, A. Le malattie mentali e nervosi in guerra. Riv. ospedal., Roma, 1915, v. 5, pp. 322-331.
Giannelli, A. Mental illnesses and nerve disorders in war. Hospital Review, Rome, 1915, vol. 5, pp. 322-331.
Giannuli, F. Le syndrome Korsakoff et la commotion cérébrale. Rivista sperimentale di Freniatria, vol. XL, fasc. 2, 30 juin 1914.
Giannuli, F. The Korsakoff Syndrome and Brain Concussion. Experimental Journal of Psychiatry, vol. XL, no. 2, June 30, 1914.
Gibt es eine “Kriegspsychose?” Psychiat. Neurol. Wchnschr., Halle a. S., 1914-1915, v. 6, pp. 356-357.
Is there a “war psychosis?” Psychiat. Neurol. Wchnschr., Halle a. S., 1914-1915, v. 6, pp. 356-357.
Gilbreth, F. B. The problem of the crippled soldier; how to put him on the payroll. Scient. Am. Suppl., N. Y., 1917, v. 83, p. 260.
Gilbreth, F. B. The challenge of getting injured soldiers onto the payroll. Scient. Am. Suppl., N. Y., 1917, v. 83, p. 260.
Gilbreth, F. B. and Gilbreth, Lillian M. The conservation of the world’s teeth; a new occupation for crippled soldiers. Trained nurse (etc.), N. Y., 1917, v. 59, pp. 5-11.
Gilbreth, F. B. and Gilbreth, Lillian M. The conservation of the world’s teeth; a new job for disabled soldiers. Trained nurse (etc.), N. Y., 1917, v. 59, pp. 5-11.
Gilchrist, Norman S. Analysis of causes of breakdown in flying: with notes on the nervous mechanism of the flying man. (Ref. lost.)
Gilchrist, Norman S. Analysis of the reasons for failure in flight: with notes on the nervous system of the flying individual. (Ref. lost.)
Gilles, André. Étude sur certains cas de neurasthénie. Ann. méd.-psychol., Par., 1916, 1917; v. 73, pp. 209-229; and pp. 333-364.
Gilles, André. Study on certain cases of neurasthenia. Ann. méd.-psychol., Paris, 1916, 1917; v. 73, pp. 209-229; and pp. 333-364.
Gilles, André. L’hystérie et la guerre troubles fonctionnels par commotion. Leur traitement par le torpillage. Ann. méd. psychol., Par., 1917, v. 73, pp. 207-227.
Gilles, André. Hysteria and war functional disorders caused by concussion. Their treatment through torpedo therapy. Ann. méd. psychol., Paris, 1917, vol. 73, pp. 207-227.
Gillet, H. et Boyé, G. Les insuffisants cardiaques. Paris méd., 1916, v. 21, pp. 30-33.
Gillet, H. and Boyé, G. Heart Failure Patients. Paris Méd., 1916, v. 21, pp. 30-33.
Gilyarovski, V. A. (The war and the care of the insane in time of peace.) Sovrem. Psikhiat., Mosk., 1915, v. 9, pp. 287-297.
Gilyarovski, V. A. (The war and the care of the mentally ill in peacetime.) Sovrem. Psikhiat., Mosk., 1915, v. 9, pp. 287-297.
Gilyarovski, V. A. (Nature of alterations in the neuropsychic sphere after war contusions.) Sovrem. Psikhiat., Mosk., 1916, v. 10, pp. 403-433.
Gilyarovski, V. A. (Nature of changes in the mental state after war injuries.) Modern Psychiatry, Moscow, 1916, v. 10, pp. 403-433.
Ginestous, E. L’indice visuel d’aptitude au service militaire. Arch. de méd. et pharm. mil., Par., 1914-15, v. 64, pp. 718-24.
Ginestous, E. The visual index of military service aptitude. Arch. de méd. et pharm. mil., Par., 1914-15, v. 64, pp. 718-24.
Ginestous, Etienne. Blépharospasme tonique hystéro-traumatique. Gaz. méd. de Par., 1915, v. 14, pp. 61-62.
Ginestous, Etienne. Hystero-traumatic tonic blepharospasm. Gaz. méd. de Par., 1915, v. 14, pp. 61-62.
Ginestous, E. L’armée française perd 20,000 astigmates. Caducée, Par., 1915, v. 15, p. 99.
Ginestous, E. The French army loses 20,000 astigmatics. Caducée, Par., 1915, v. 15, p. 99.
Ginestous, E. Hémianopsie en quadrant. Progrès méd., Par., 1916, v. 31, pp. 3-4.
Ginestous, E. Quadrant Hemianopsia. Progrès méd., Paris, 1916, vol. 31, pp. 3-4.
Gino, S. and Stefano, B. Mutismo isterico consecutivo a scoppio di granata in sogetto istero-epilettico. Gazz. d. osp., Milano, 1917, v. 38, pp. 308-310.
Gino, S. and Stefano, B. Hysterical mutism following a grenade explosion in an hysterical-epileptic subject. Gazz. d. osp., Milan, 1917, v. 38, pp. 308-310.
Giroux. Hémiplégie consécutive à une intoxication par les gaz asphyxiants. Rev. Paris méd., 1916. (Part. Méd.), v. 21, p. 436.
Giroux. Hemiplegia resulting from poisoning by asphyxiating gases. Rev. Paris méd., 1916. (Part. Méd.), v. 21, p. 436.
Glaser, W. Diphtheriebazillen als Meningitiserregen. München. med. Wchnschr., 1917, 64, 856-57.
Glaser, W. Diphtheria bacilli as causes of meningitis. Munich. Med. Wkly, 1917, 64, 856-57.
Glieboff, D. A. (Malingering by recruits.) Sibirsk. Vrach., Tomsk, 1915, i, 4, 49, 62.
Glieboff, D. A. (Faking illness among recruits.) Sibirsk. Vrach., Tomsk, 1915, i, 4, 49, 62.
Goddard, H. H. The place of intelligence in modern warfare. U. S. Nav. M. Bull., Wash., 1917, v. 9, pp. 283-289.
Goddard, H. H. The role of intelligence in modern warfare. U. S. Nav. M. Bull., Wash., 1917, v. 9, pp. 283-289.
Goetjes. Ueber Gehirnverletzungen durch Granatsplitter. Münch. med. Wchnschr., 1915, v. 62, pp. 897-898.
Goetjes. On brain injuries caused by shell fragments. Munich Med. Weekly, 1915, v. 62, pp. 897-898.
Goissard, Liébault. Les aphones pendant la guerre. Archiv. de Méd. et de Pha. Mil., 1916, v. 66, No. 1 or No. 3; p. 169.
Goissard, Liébault. The voiceless during the war. Archives of Medicine and Pharmacy Military, 1916, vol. 66, No. 1 or No. 3; p. 169.
Golant, R. Ya. (Neurotic symptoms in soldiers). Obozr. Psikhiat., Nevrol., Petrogr., 1916, v. 20, pp. 63-66.
Golant, R. Ya. (Neurotic symptoms in soldiers). Obozr. Psikhiat., Nevrol., Petrogr., 1916, v. 20, pp. 63-66.
Goldscheider. Zur Frage der traumatischen Neurose. Deutsche med. Wchnschr., Berl. u. Leipz., 1916, v. 42, No. 46.
Goldscheider. On the issue of traumatic neurosis. German med. Wchnschr., Berlin and Leipzig, 1916, v. 42, No. 46.
Goldsmith. Special Discussion on Warfare Injuries and Neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Octol.), pp. 119-122.
Goldsmith. Special Discussion on Warfare Injuries and Stress Disorders. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Octol.), pp. 119-122.
Goldstein, K. Die militärische Sachsverständigentatigkeit auf dem Gebiete des Ersatzwesens und der militärischen Versorgung bei de Hirnverletzungen. Erste Teil, pp. 194-232. Jena, Fischer, 1917.
Goldstein, K. The Military Expertise on Replacements and Military Supply in Cases of Brain Injuries. Part One, pp. 194-232. Jena, Fischer, 1917.
Goldstein. Beobachtungen an Schussverletzungen des Gehirns und Rückenmarks. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 215-217.
Goldstein. Observations on gunshot injuries to the brain and spinal cord. German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, pp. 215-217.
Goldstein. Die Suggestionstherapie der funktionellen neurosen im Feldlazarett. Therapie der Gegenwart, Sept., 1917.
Goldstein. The suggestion therapy for functional neuroses in the field hospital. Modern Therapy, Sept., 1917.
Goldthwaite, J. E. The place of orthopedic surgery in war. Am. J. Orthop. Surg., Bost., 1917, v. 15, pp. 679-686.
Goldthwaite, J. E. The role of orthopedic surgery in wartime. Am. J. Orthop. Surg., Bost., 1917, v. 15, pp. 679-686.
Gonda, Viktor. Rasche Heilung der Symptome der im Kriege entstandenen traumatischen Neurosen. Wien. klin. Wchnschr., 1916, v. 29, No. 30.
Gonda, Viktor. Quick Healing of the Symptoms of Traumatic Neuroses Developed During the War. Vienna. Clinical Weekly, 1916, vol. 29, No. 30.
Goodwin, T. H. No. 2, Notes for Army Medical War Officers. Medical Manual War Series. Lea and Febiger, 1917.
Goodwin, T. H. No. 2, Notes for Army Medical War Officers. Medical Manual War Series. Lea and Febiger, 1917.
Gordon, W., Sunderland, S. (et al). Physical treatment for disabled soldiers. Lancet, Lond., 1917, v. 1, p. 348.
Gordon, W., Sunderland, S. (et al). Physical treatment for disabled soldiers. Lancet, Lond., 1917, v. 1, p. 348.
Goria, C. Alcune considerazioni attomo al mutismo psichico nei militari alla sua genesi emozionale e commozionale. Riform. med., Napoli, 1916, v. 32, pp. 725 and 756.
Goria, C. Some considerations about psychic mutism in soldiers regarding its emotional and affective origins. Riform. med., Naples, 1916, vol. 32, pp. 725 and 756.
Gosset, H. Contribution à l’étude expérimentale du contrôle auditif. Progrès méd., Par., 1916, No. 1, pp. 21-22.
Gosset, H. Contribution to the Experimental Study of Auditory Control. Med. Progress, Paris, 1916, No. 1, pp. 21-22.
Gosset, H. Traitement des impotences consécutives aux blessures de guerre par la rééducation psycho-motrice. Progrès Méd., Par., 1916, No. 3, pp. 35-38.
Gosset, H. Treatment of disabilities resulting from war injuries through psycho-motor rehabilitation. Medical Progress, Paris, 1916, No. 3, pp. 35-38.
Gosset, H. La rééducation de l’appareil locomoteur. Progrès Méd., Par., 1916, No. 3, pp. 65-70.
Gosset, H. Rehabilitation of the Locomotor System. Medical Advances, Paris, 1916, No. 3, pp. 65-70.
Gosset, H. Expériences relatives au contrôle auditif. Progrès Méd., Par., 1917, No. 2, pp. 9-10.
Gosset, H. Experiences Related to Auditory Control. Med. Progress, Paris, 1917
Gouget, A. La bradycardie de fatigue. Bull. Acad. de Méd., Par., 1915, v. 74, pp. 810-812.
Gouget, A. Fatigue-induced bradycardia. Bull. Acad. de Méd., Par., 1915, v. 74, pp. 810-812.
Gouget. Un cas de neuro-fibromatose. Presse Méd., 1916, v. 24, p. 309.
Gouget. A case of neurofibromatosis. Médical Press, 1916, vol. 24, p. 309.
Gougerot, H. and Charpentier, Albert. Paralysies réflexes troubles trophiques réflexes consécutifs aux blessures des extrémités. Ann. de méd., Par., 1916, v. 3, pp. 269-297.
Gougerot, H. and Charpentier, Albert. Reflex paralysis and trophic disorders resulting from injuries to the extremities. Ann. de méd., Par., 1916, v. 3, pp. 269-297.
Grace, J. J. A note on the electrical treatment of disabilities due to wounds. Brit. M. J., Lond., 1915, ii, p. 812.
Grace, J. J. A note on the electrical treatment of disabilities caused by wounds. Brit. M. J., Lond., 1915, ii, p. 812.
Gradenigo, G. Esagerazione e simulazione della sordita nei militari. Arch. ital. di otol. Torino, 1916, v. 27, pp. 139-147.
Gradenigo, G. Exaggeration and simulation of deafness in soldiers. Ital. Arch. of Otol. Turin, 1916, v. 27, pp. 139-147.
Gradenigo. Mutismo, afonia, sordita nei militari: di origine psichica, de cause organiche: simulazioni e criteri differenziedi obiettive. Riv. di patol. nerv. Firenze, 1917 (March).
Gradenigo. Muteness, aphonia, deafness in soldiers: of psychological origin, from organic causes: simulations and different criteria of objectives. Riv. di patol. nerv. Firenze, 1917 (March).
Graham, W. War and the incidence of insanity. Med. Officer, Lond., 1916, v. 16, p. 453.
Graham, W. War and the occurrence of mental illness. Medical Officer, London, 1916, v. 16, p. 453.
Granjux. La faillite de l’instruction sur l’aptitude physique au service militaire. J. de méd. et chir. prat., Par., 1915, v. 86, pp. 849-853.
Granjux. The failure of the assessment of physical fitness for military service. J. de méd. et chir. prat., Par., 1915, v. 86, pp. 849-853.
Granjux. De la nécessité des services de psychiatrie et de médecine légale aux armées. Caducée. Par., 1916, xvi, 43-45.
Granjux. On the necessity of psychiatric and forensic medicine services for the armies. Caducée. Paris, 1916, xvi, 43-45.
Granjux. Les conditions dans lesquelles seront pratiquées les expertises en matière d’accidents du travail dont seront victimes les mutilés de la guerre. Soc. méd. lég. de France, Bull., Par., 1917, v. 14, pp. 221-222.
Granjux. The conditions under which assessments related to workplace accidents affecting war victims will be carried out. Soc. méd. lég. de France, Bull., Par., 1917, v. 14, pp. 221-222.
Grant, Dundas. Mutism, stammering, psychical deafness. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sect. Psychiat.), pp. 37-38.
Grant, Dundas. Mutism, stuttering, psychological deafness. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sect. Psychiat.), pp. 37-38.
Grant, D. Special discussion on warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 93-96.
Grant, D. Special discussion on injuries and psychological issues from war. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 93-96.
Grasset. Clinical lectures on the psychoneuroses of war. (2 papers). Med. Press and Circ., Lond., 1915, i, v. 99, pp. 560-563; and pp. 586-587.
Grasset. Clinical lectures on the psychological effects of war-related neuroses. (2 papers). Med. Press and Circ., Lond., 1915, i, v. 99, pp. 560-563; and pp. 586-587.
Grasset. Le traitement des psychonévroses de guerre. Presse méd., Par., 1915, v. 23, pp. 105-108; and p. 425.
Grasset. Treating war-related psychoneuroses. Med. Press, Paris, 1915, vol. 23, pp. 105-108; and p. 425.
Grasset. Les psychonévroses de guerre. Presse médicale, 1 avril, 1915.
Grasset. The war-related psychoneuroses. Medical Press, April 1, 1915.
Grasset. Les névroses et psychonévroses de guerre; conduite à tenir à leur égard. Rev. neurol., Par., 1916, xxiii, 767-774. (Discussion) 774-788.
Grasset. The war neuroses and psychoneuroses: how to deal with them. Rev. neurol., Paris, 1916, xxiii, 767-774. (Discussion) 774-788.
Grasset. Les symptômes atypiques à développement tardif dans les traumatismes crânio-cérébraux. Montpel. méd., 1916, v. 39, p. 19.
Grasset. Atypical late-developing symptoms in cranio-cerebral traumas. Montpel. méd., 1916, v. 39, p. 19.
Grasset. Les maladies de guerre du système nerveux et les conseils de réforme. Presse méd. Par., 1916, v. 24, pp. 1-2.
Grasset. The war-related diseases of the nervous system and reform recommendations. Medical Press. Paris, 1916, vol. 24, pp. 1-2.
Grasset. Les grandes types cliniques des psychonévroses de guerre. Rev. neurol. Par. 1917, v. 24, p. 471.
Grasset. The major clinical types of war psychoneuroses. Neurological Review, Paris. 1917, vol. 24, p. 471.
Grasset. Les grandes types cliniques de psychonévroses de guerre. Montpel. méd., 1917, n. s., v. 39, pp. 607-628.
Grasset. The major clinical types of war psychoneuroses. Montpel. méd., 1917, n. s., v. 39, pp. 607-628.
Grasset et Maurice Villaret. À propos de pronostic tardif des traumatismes crânio-cérébraux. Rev. neurol., Par., 1916, v. 29, pp. 833-834.
Grasset and Maurice Villaret. Regarding late prognosis of cranio-cerebral injuries. Rev. neurol., Paris, 1916, vol. 29, pp. 833-834.
Gray, H. M. W. Gunshot wounds of the head. Brit. Med. Jour., 1916, i, 261.
Gray, H. M. W. Gunshot wounds to the head. Brit. Med. Jour., 1916, i, 261.
Green, Edith M. N. Blood pressure and surface temperature in 110 cases of shell shock. Lancet, Lond., 1917, ii, pp. 456-457.
Green, Edith M. N. Blood pressure and surface temperature in 110 cases of shell shock. Lancet, Lond., 1917, ii, pp. 456-457.
Greenlees, T. D. The war; impressions, neuro- and psychological. Med. Press and Circ., Lond., 1916, n. s., v. 101, pp. 101-103; also Caledon., M. J., Glasg., 1915-16, No. 10, pp. 183-187.
Greenlees, T. D. The war; impressions, neuro- and psychological. Med. Press and Circ., Lond., 1916, n. s., v. 101, pp. 101-103; also Caledon., M. J., Glasg., 1915-16, No. 10, pp. 183-187.
Gregor. Granatenkontusion mit ausgedehntem amnestichen Defekt. Münch. med. Wchnschr., 1915, v. 622, p. 1055.
Gregor. Grenade contusion with extensive amnesic defect. Münch. med. Wchnschr., 1915, v. 622, p. 1055.
Grenier de Cardenal, Legrand, Benoit. Trois nouveaux cas de rage chez l’homme. Presse méd., Par., 1917, v. 25, pp. 564-566.
Grenier de Cardenal, Legrand, Benoit. Three new cases of rabies in humans. Méd. Press, Paris, 1917, vol. 25, pp. 564-566.
Griffith, A. D. Injuries of the eye and orbit. Lancet, Lon., 1916, i, 1245.
Griffith, A. D. Eye and orbital injuries. Lancet, Lon., 1916, i, 1245.
Grivot, M. Appareil auditif et traumatismes de guerre. Paris méd., 1915, v. 17, pp. 359-365.
Grivot, M. Hearing devices and war injuries. Paris Med., 1915, v. 17, pp. 359-365.
Grober. Die Krankheiten der Kreislauforgane und der Krieg. Munch. med. Wchnschr., 1914, ii, v. 61, pp. 2388-2390.
Grober. The Diseases of the Circulatory Organs and War. Munch. med. Wchnschr., 1914, ii, v. 61, pp. 2388-2390.
Gross, C. Nervöse Kriegsdienstschädigungen. Wien klin. Wchnschr., 1916, xxix, 1577.
Gross, C. Nervous war service injuries. Wien klin. Wchnschr., 1916, xxix, 1577.
Grünbaum, F. Hysterie und Kriegsdienstbeschädigung. Deutsche med. Wchnschr., Berl. u. Leipz., 1916, v. 42, pp. 1452-1453.
Grünbaum, F. Hysteria and War Service Injury. German Med. Weekly, Berlin and Leipzig, 1916, vol. 42, pp. 1452-1453.
Grünwald. Schussverletzungen der pneumatischen Schädelhöhlen. München [933]med. Wchnschr. 1915, v. 621, pp. 823-825.
Grünwald. Gunshot wounds of the pneumatic skull cavities. Munich [933]med. Wchnschr. 1915, v. 621, pp. 823-825.
Grutzhaendler-Indelson. Troubles sensitivo-moteurs hystérotraumatiques observés a l’occasion de la guerre 1914-1915. Thèse de Paris, 1915.
Grutzhaendler-Indelson. Hysterical sensory-motor issues observed during the 1914-1915 war. Thesis from Paris, 1915.
Gudden. Beginnende Behandlung psychischer Erkrankungen im Felde. München med. Wchnschr., 1915, v. 62, pp. 1730.
Gudden. Initial treatment of mental illnesses in the field. Munich med. Wchnschr., 1915, v. 62, pp. 1730.
Guépin, A. Dix cas de chirurgie cérébrale. Caducée, Par., 1916, v. 16, pp. 74-77.
Guépin, A. Ten Cases of Brain Surgery. Caducée, Paris, 1916, vol. 16, pp. 74-77.
Guerre et les éclopés psychiques. Ann. d’Hyg., Par., 1917, v. 25, pp. 252-254.
War and Psychological Injuries. Ann. d’Hyg., Paris, 1917, vol. 25, pp. 252-254.
Guilbert, Charles and Maucurier, G. Guide de rééducation physique en groupe. Méthode de gymnastique rééducative pour les blessés militaires. Par., 1916, J. B. Baillière et fils. 128 pp., 12o.
Guilbert, Charles and Maucurier, G. Guide to Group Physical Rehabilitation. Rehabilitative Gymnastics Method for Military Injuries. Par., 1916, J. B. Baillière et fils. 128 pp., 12o.
Guild, S. R. War deafness and its prevention; a critical review. J. Lab. and Clin. M., St. Louis, 1916-17, v. 2, pp. 849-861.
Guild, S. R. Hearing loss from war and how to prevent it; a critical review. J. Lab. and Clin. M., St. Louis, 1916-17, v. 2, pp. 849-861.
Guillain, G. Un cas de contractures généralisées avec symptômes méningés consécutive à l’éclatement d’un projectile sans plaie extérieure. Presse Méd., Par., 1915, v. 23, p. 181.
Guillain, G. A case of generalized contractions with meningitis symptoms following the explosion of a projectile without external wounds. Medical Press, Paris, 1915, v. 23, p. 181.
Guillain, G. Les crises épileptiques consécutives à l’explosion des projectiles sans plaie extérieure. Presse méd., Par., 1915, v. 23, pp. 181.
Guillain, G. Epileptic seizures resulting from projectile explosions without external wounds. Med. Press, Paris, 1915, v. 23, pp. 181.
Guillain, G. Sur un cas de mutisme consécutif à l’éclatement d’un projectile. Presse Méd., Par., 1915, v. 23, p. 182.
Guillain, G. On a case of mutism following a projectile explosion. Presse Méd., Par., 1915, v. 23, p. 182.
Guillain, G. Un cas de tremblement pseudo-parkinsonien consécutif à l’éclatement d’un projectile sans plaie extérieure. Presse Méd., Par., 1915, v. 23, p. 182.
Guillain, G. A case of pseudo-parkinsonian tremor following the explosion of a projectile with no external wound. Medical Press, Paris, 1915, v. 23, p. 182.
Guillain, G. Les syndrômes paralytiques consécutifs à l’éclatement des projectiles sans plaie extérieure. Presse méd. Par., 1915, v. 23, pp. 225-226.
Guillain, G. The paralyzing syndromes resulting from the bursting of projectiles without external wounds. Med. Press, Paris, 1915, v. 23, pp. 225-226.
Guillain, G. Le syndrôme cérébelleux à type de sclérose en placques consécutif à l’éclatement des projectiles sans plaie extérieure. Presse méd., Par., 1915, v. 23, p. 226.
Guillain, G. The cerebellar syndrome resembling multiple sclerosis following projectile blasts without external wounds. Med. Press, Paris, 1915, vol. 23, p. 226.
Guillain, G. Sur un état de stupeur avec catatonie, hypothermie, bradycardie et hypopnée consécutif à l’éclatement d’un projectile sans plaie extérieure. Presse méd., Par., 1915, v. 23, p. 226.
Guillain, G. On a state of stupor with catatonia, hypothermia, bradycardia, and hypopnea following the detonation of a projectile without any external injury. Méd. Press, Paris, 1915, v. 23, p. 226.
Guillain, G. Les névrites irradiantes et les contractures et paralysies traumatiques d’ordre réflexe. Soc. méd. des Hôpitaux, 26 mai 1916.
Guillain, G. Radiant neuritis and traumatic reflex contractures and paralysis. Med. Society of Hospitals, May 26, 1916.
Guillain, G. Sur un syndrôme choréiforme consécutif à l’éclatement d’un projectile sans plaie extérieure. Presse méd., Par., 1915, v. 23, p. 225.
Guillain, G. On a choreiform syndrome following the explosion of a projectile without an external wound. Med. Press, Paris, 1915, vol. 23, p. 225.
Guillain, G. Hémiplegie organique consécutive à un éclatement d’obus sans plaie extérieure. Presse méd., Par., 1915, v. 23, p. 429.
Guillain, G. Organic hemiplegia following a shell explosion without external injury. Med Press, Paris, 1915, v. 23, p. 429.
Guillain, G. Influence sur le système nerveux des éclatements d’obus de gros calibre. Rev. gén. de clin. et de theráp., Par., 1915, v. 29, p. 736.
Guillain, G. Influence on the nervous system from large-caliber shell explosions. Gen. Rev. of Clin. and Ther., Paris, 1915, vol. 29, p. 736.
Guillain, G. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol. Par., 1916, v. 29, pp. 576-577.
Guillain, G. On nerve accidents caused by the explosion of large amounts of explosives. Rev. neurol. Par., 1916, v. 29, pp. 576-577.
Guillain, G. Un syndrôme consécutif à l’éclatement des gros projectiles sans plaie extérieure. Arch. de méd. et pharm. mil., Par., 1916-17. lxvi, 542.
Guillain, G. A syndrome resulting from the explosion of large projectiles without external wounds. Arch. de méd. et pharm. mil., Par., 1916-17. lxvi, 542.
Guillain, G. et Barré, A. Inversion du réflexe achilléen et du réflexe médio-plantaire dans un cas de lésion du nerf sciatique poplité interne. Presse méd., Par., 1917, v. 25, p. 448.
Guillain, G. and Barré, A. Inversion of the Achilles reflex and the mid-plantar reflex in a case of injury to the internal popliteal sciatic nerve. Medical Press, Paris, 1917, vol. 25, p. 448.
Guillain et Barré. Hémorragie méningée consécutive à une commotion par éclatement d’obus sans plaie extérieure. Méningite à pneumocoques mortelle secondaire. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 898-900.
Guillain and Barré. Meningeal hemorrhage resulting from a concussion caused by a shell explosion without an external wound. Fatal pneumococcal meningitis secondary. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 898-900.
Guillain and Barré. Les troubles sphinctériens transitoires dans les commotions par éclatement de gros projectiles sans plaies extérieures. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 22, pp. 1114-1118.
Guillain and Barré. Temporary sphincter issues in concussions caused by large projectiles without external wounds. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 22, pp. 1114-1118.
Guillain and Barré. Les troubles des réactions pupillaires dans les commotions par éclatement de gros projectiles sans plaie extérieure. Bull. Acad. de méd., Par., 1917, v. 78, pp. 158-159.
Guillain and Barré. Disorders of pupillary reactions in concussions caused by the impact of large projectiles without external wounds. Bull. Acad. de méd., Par., 1917, v. 78, pp. 158-159.
Guillain et Barré. Troubles pyramidaux organiques consécutifs à l’éclatement d’un projectile sans plaie extérieure. Soc. méd. d’hôp. Par., 1916, 26 mai.
Guillain and Barré. Organic pyramidal disorders following the explosion of a projectile without external wounds. Méd. Soc. d’hôp. Paris, 1916, May 26.
Guillain et Barré. Soc. méd. d’hôp. Par., 1916, 21 janvier.
Guillain and Barré. Med. Soc. of Hosp. Par., 1916, January 21.
Guillain et Barré. Soc. méd. d’hôp. Par., 1916, 7 avril.
Guillain and Barré. Med. Soc. of Hosp. Par., 1916, April 7.
Guillain et Barré. Les contractures ischémiques. Réunion Méd. de la VI armée, Jan. 12, 1916.
Guillain and Barré. Ischemic contractions. Medical meeting of the VI army, Jan. 12, 1916.
Guillain. Les névrites irradiantes et les contractures et paralysies traumatiques d’ordre réflexe. Soc. Méd. des Hôpitaux, May 26, 1916.
Guillain. Radiating neuritis and reflexive traumatic contractures and paralysis. Medical Society of Hospitals, May 26, 1916.
Guillain et Barré. Forme clinique de la névrite ascendante. Presse méd. 3 avril 1916.
Guillain and Barré. Clinical form of ascending neuritis. Med Press. April 3, 1916.
Guillain and Barré. (Lesions with external wounds.) Bull. et mem. soc. méd. hôp. d Par., 1916, v. 40, p. 834.
Guillain and Barré. (Injuries with external wounds.) Bull. et mem. soc. méd. hôp. d Par., 1916, v. 40, p. 834.
Guillain and Barré. Deux cas d’astasie-abasie avec troubles du nerf vestibulaire chez les syphilitiques anciens. Ann. de méd. Par., v. 3, 1916, pp. 431-436.
Guillain and Barré. Two cases of astasia-abasia with vestibular nerve disorders in patients with old syphilis. Ann. de méd. Par., v. 3, 1916, pp. 431-436.
Guillain and Barré. A propos d’un cas d’astasie-abasie trépidante. Presse méd., Par., 1916, v. 24, pp. 119-120.
Guillain and Barré. About a case of tremulous astasia-abasia. Med. Press, Par., 1916, v. 24, pp. 119-120.
Guillain and Barré. Apoplexie tardive consécutive à une commotion par éclatement d’obus sans plaie extérieure. Ibid., 1473-74.
Guillain and Barré. Delayed stroke resulting from a concussion due to shell explosion without external injury. Ibid., 1473-74.
Guillain et Barré. Hémiplégies par blessures de guerre. Diagnostic topographique du siège des lésions. Presse méd., Par., 1916, v. 24, pp. 121-122.
Guillain and Barré. Hemiplegias from war injuries. Topographical diagnosis of the site of lesions. Med. Press, Paris, 1916, v. 24, pp. 121-122.
Guillain et Barré. Syndrôme d’avellis bilatéral, manifestation de syphilis nerveuse. Presse méd., Par., 1916, v. 24, p. 150.
Guillain and Barré. Bilateral Avellis syndrome, a manifestation of nervous syphilis. Presse méd., Par., 1916, v. 24, p. 150.
Guillain et Barré. Deux cas d’hémiplégie organique consécutifs à la déflagration de fortes charges d’explosifs, sans plaie extérieure. Paris méd., 1916 (Part. Méd.), v. 21, p. 420.
Guillain and Barré. Two cases of organic hemiplegia resulting from the explosion of large amounts of explosives, without external wounds. Paris méd., 1916 (Part. Méd.), v. 21, p. 420.
Guillain Barré and Strohl. Étude graphique des réflexes tendineux abolis à l’examen clinique dans un cas de commotion par éclatement d’obus sans plaie extérieure. Bull. et mém. Soc. méd. d’hôp. de Par., 1917, 3. s, xii, 313-315.
Guillain Barré and Strohl. A graphic study of the absent tendon reflexes observed during a clinical exam in a case of shell shock without external wounds. Bull. et mém. Soc. méd. d’hôp. de Par., 1917, 3. s, xii, 313-315.
Gumpertz. Beiträge z. Kenntniss d. Nervenschädigungen des Kriegs. Aus dem Kriegslazarett. Berl., J. Goldschmidt.
Gumpertz. Contributions to the Understanding of Nerve Damage from the War. From the War Hospital. Berlin, J. Goldschmidt.
Gunson, E. B. Cardiac symptoms following dysentery among soldiers. Lancet, Lon., ii, 146.
Gunson, E. B. Heart issues after dysentery in soldiers. Lancet, Lon., ii, 146.
Gutzmann, H. Stimm- und Sprachstörungen im Kriege und ihre Behandlung. Berl. klin. Wchnschr., 1916, v. 53, pp. 154-158.
Gutzmann, H. Voice and Speech Disorders in War and Their Treatment. Berl. klin. Wchnschr., 1916, v. 53, pp. 154-158.
Haas. Sur quelques blessures oculaires occasionnées par les engins à forte charge d’explosif. Presse méd., Par., 1916, v. 24, p. 52.
Haas. On some eye injuries caused by high-explosive devices. Méd. Press, Paris, 1916, vol. 24, p. 52.
Haberer, H. v. Beitrag zu den Schädelverletzungen im Kriege. Wien. klin. Wchnschr., 1914, v. 27, pp. 1590-1593.
Haberer, H. v. Contribution to Skull Injuries in War. Vienna. Clinical Weekly, 1914, vol. 27, pp. 1590-1593.
Hadfield, J. A. Influence of hypnotic suggestion on inflammatory conditions. Lancet, Lond., 1917, v. ii, p. 678.
Hadfield, J. A. The impact of hypnotic suggestion on inflammatory conditions. Lancet, Lond., 1917, v. ii, p. 678.
Haddon, John. Shell-shock: its cause and proper treatment by diet. Domin. Med. Mon., 1918, i, 33.
Haddon, John. Shell-shock: its cause and proper treatment through diet. Domin. Med. Mon., 1918, i, 33.
Haddon, J. Shell shock; its cause and proper treatment by diet. Med. Press. Lond., 1917, n. s., civ, 409-411.
Haddon, J. Shell shock; its cause and proper treatment by diet. Med. Press. Lond., 1917, n. s., civ, 409-411.
Hagedorn. Abnorme Selbstbeschädigungen. Deutsche Zeitschr. f. Chir., Leipz., 1916, v. 137, pp. 1-46.
Hagedorn. Abnormal Self-harm. German Journal of Surgery, Leipzig, 1916, vol. 137, pp. 1-46.
Hahn. Kriegspsychosen. Med. Klin. Berl. u. Wien., 1915, v. 3, pp. 114-115.
Hahn. War Psychoses. Med. Clin. Berlin and Vienna, 1915, vol. 3, pp. 114-115.
Hahn. Uber Kriegspsychosen. München med., Wchnschr., 1915, v. 621, p. 268.
Hahn. On War Psychoses. Munich Medical Weekly, 1915, vol. 621, p. 268.
Hakkebusch, V. M. (What is caused by wind contusion: neurosis, or organic injury of the nervous system.) Sovrem, Psikhiat., Mosk., 1915, v. 9, pp. 389-405.
Hakkebusch, V. M. (What is caused by wind contusion: neurosis, or organic injury of the nervous system.) Sovrem, Psikhiat., Mosk., 1915, v. 9, pp. 389-405.
Hakkebusch, V. M. (Nervous diseases in connection with wind contusion.) Sovrem. Psikhiat., Mosk., 1916, v. 10, pp. 226-249.
Hakkebusch, V. M. (Nervous diseases related to impacts from wind.) Modern Psychiatry, Moscow, 1916, vol. 10, pp. 226-249.
Halipré, A. Test de guérison de la paralysie radiale (signe des fléchisseurs) Rev. neurol., Par., 1917, v. 24, pp. 87-89.
Halipré, A. Test for the healing of radial paralysis (flexor sign) Rev. neurol., Par., 1917, v. 24, pp. 87-89.
Hamburger, Franz. Uber simulierte und aggravierte Bronchitis. Militärarzt Wien. med. Wchnschr., 1915, v. 49, No. 35.
Hamburger, Franz. About simulated and aggravated bronchitis. Military doctor Vienna. med. Wchnschr., 1915, v. 49, No. 35.
Hamilton, Allan McLane. Tests for the perception efficiency of recruits. Med. Rec., N. Y., 1918, v. 93, pp. 285-286.
Hamilton, Allan McLane. Tests for the perception efficiency of recruits. Med. Rec., N. Y., 1918, v. 93, pp. 285-286.
Hamilton, Allan McLane. Psychopathology of the war. Med. Rec., N. Y., 1915, v. 87, p. 110.
Hamilton, Allan McLane. The mental health effects of the war. Medical Record, New York, 1915, vol. 87, p. 110.
Hammesfahr. Vorstellung zweier Patienten mit Gehirnschüssen. (Abstract.) Deutsche med. Wchnschr., 1915, Berl. u. Leipz., v. 41, p. 575.
Hammesfahr. Presentation of two patients with gunshot wounds to the head. (Abstract.) German Medical Weekly, 1915, Berlin and Leipzig, vol. 41, p. 575.
Hammond, T. E. Involvement of the external and internal popliteal nerves in lesions of the sciatic nerve. Brit. Med. Jour., 1918, i, 397.
Hammond, T. E. Involvement of the external and internal popliteal nerves in lesions of the sciatic nerve. Brit. Med. Jour., 1918, i, 397.
Harford, C. F. Visual neuroses of miners in their relation to military service. Brit. M. J., Lond., 1916, i, pp. 340-342.
Harford, C. F. Visual neuroses of miners and their connection to military service. Brit. M. J., Lond., 1916, i, pp. 340-342.
Harris, W. Abnormal median and ulnar nerve-supply in the hand. Lancet, London, 1917, ii, 710.
Harris, W. Unusual median and ulnar nerve supply in the hand. Lancet, London, 1917, ii, 710.
Harris, Wilfred. Nerve Injuries and Shock. 1915, London, Henry Frowde.
Harris, Wilfred. Nerve Injuries and Shock. 1915, London, Henry Frowde.
Harris, Wilfred. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., 1915-16 (Sec. Psychiat.), pp. 33-34.
Harris, Wilfred. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., 1915-16 (Sec. Psychiat.), pp. 33-34.
Harrower, H. R. Shell shock and the internal secretions; with suggestions as to treatment. Prescriber, Edinb., 1916, x, 203-209.
Harrower, H. R. Shell shock and the hormonal imbalances; with recommendations for treatment. Prescriber, Edinburgh, 1916, x, 203-209.
Harwood, T. E. Nature and treatment of concussion. Lancet, Lond., 1916, i, p. 551.
Harwood, T. E. The nature and treatment of concussion. Lancet, London, 1916, i, p. 551.
Harwood, T. E. Shell shock. Lancet, Lond., 1916, i, 698.
Harwood, T. E. Shell shock. Lancet, London, 1916, 1, 698.
Harwood, T. E. Three cases illustrating the functional consequences of head injuries. Lancet, Lond., 1916, ii, v. 191, p. 431.
Harwood, T. E. Three cases showing the functional effects of head injuries. Lancet, Lond., 1916, ii, v. 191, p. 431.
Harwood, T. E. Functional conditions in head injuries. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 699-707.
Harwood, T. E. Functional conditions in head injuries. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 699-707.
Harzbecker. Ueber die Aetiologie der Granatkontusionsverletzungen. Deutsche med. Wchnschr., Berl., u. Leipz., 1914, v. 402, p. 1985.
Harzbecker. On the Etiology of Grenade Blast Injuries. German Medical Weekly, Berlin, and Leipzig, 1914, vol. 402, p. 1985.
Hauptmann, A. Kriegsneurosen und traumatische Neurose. Monatschr. f. Psychiat. u. Neurol., Berl., 1916, v. 38, pp. 20-32.
Hauptmann, A. War Neuroses and Traumatic Neurosis. Monthly Journal of Psychiatry and Neurology, Berlin, 1916, vol. 38, pp. 20-32.
Haury. Un dément précoce engagé volontaire. Rev. de méd., Par., 1914-15, v. 24, pp. 591-593.
Haury. A precocious madman who volunteered. Rev. de méd., Par., 1914-15, v. 24, pp. 591-593.
Haury. Un cas de “folie minime” chez un débile. Presse Méd., Par., 1915, v. 23, p. 429.
Haury. A case of “minor insanity” in a mentally disabled person. Presse Méd., Par., 1915, v. 23, p. 429.
Haury. Un autre déserteur pathologique. Presse Méd., 1915, v. 23, p. 429.
Haury. Another pathological deserter. Presse Méd., 1915, v. 23, p. 429.
Haury. Les retentissements psycho-organiques de la vie de guerre. Presse Méd., Par., 1915, v. 23, pp. 458-459.
Haury. The psycho-organic effects of wartime life. Med. Press, Paris, 1915, v. 23, pp. 458-459.
Haury. De l’utilisation des indisciplinés en temps de guerre. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 525-530.
Haury. On the use of undisciplined individuals in wartime. Ann. méd. psychol., Paris, 1916-17, vol. 7, pp. 525-530.
Hayward, E. Beitrag zur Klinik der Schädelschüsse, nach den Erfahrungen im Heimatlazarett. Berl. klin. Wchnschr., 1915, v. 52, pp. 1186-1200; and pp. 1212-1218.
Hayward, E. Contribution to the Treatment of Gunshot Wounds to the Head, Based on Experiences in a Local Hospital. Berl. klin. Wchnschr., 1915, v. 52, pp. 1186-1200; and pp. 1212-1218.
Hecht, V. Leitfaden den physikalisch-therapeutischer Nachbehandlung Kriegsverwundeten. W. Braumüller, Wien. u. Leipz., 1916. Rev. Deutsch. med. Wchnschr., 1916, No. 39, p. 1207.
Hecht, V. Guide for the Physical and Therapeutic Rehabilitation of War Injuries. W. Braumüller, Vienna and Leipzig, 1916. Rev. German Med. Weekly, 1916, No. 39, p. 1207.
Heilig and Sick, P. Uber Schussverletzungen des Gehirns. München med. Wchnschr., 1915, v. 621, pp. 172-173.
Heilig and Sick, P. On Gunshot Wounds of the Brain. Munich Med. Wkly., 1915, v. 621, pp. 172-173.
Heimanovich, A. I. (Public psychiatric hospitals and the war.) Kharkov. M. J., 1915, v. 20, pp. 371-376.
Heimanovich, A. I. (Public psychiatric hospitals and the war.) Kharkov. M. J., 1915, v. 20, pp. 371-376.
Heimanovich, A. I. (Mental diseases of war time.) Kharkov. M. J., 1915, v. 20, pp. 377-395.
Heimanovich, A. I. (Mental illnesses during wartime.) Kharkov. M. J., 1915, v. 20, pp. 377-395.
Heimanovich, A. I. (Institutes of functional reëstablishment.) Kharkov. M. J., 1916, v. 22, pp. 243-252.
Heimanovich, A. I. (Institutes of Functional Reestablishment.) Kharkov. M. J., 1916, v. 22, pp. 243-252.
Heitz, Jean. Cinq cas de paraplégie organique consécutive à des éclatements d’obus sans plaie extérieure. Paris Méd. (Part. Méd.), 1915, v. 17, pp. 78-85.
Heitz, Jean. Five cases of organic paraplegia following shell explosions without external wounds. Paris Méd. (Part. Méd.), 1915, v. 17, pp. 78-85.
Helys, M. The reëducation and placement of war cripples. Am. J. Care Cripples, N. Y., 1917, v. 4, pp. 168-178.
Helys, M. The reeducation and placement of war cripples. Am. J. Care Cripples, N. Y., 1917, v. 4, pp. 168-178.
Helys, M. Reëducation and placement of war cripples. Amer. Jour., Care for Crip., 1917, iv, 168.
Helys, M. Rehabilitation and placement of war veterans with disabilities. American Journal of Care for the Disabled, 1917, iv, 168.
Henderson, D. K. A case of pathological lying occurring in a soldier. Rev. Neurol. and Psychiat., Edinb., 1917, v. 15, pp. 223-232.
Henderson, D. K. A case of pathological lying in a soldier. Rev. Neurol. and Psychiat., Edinb., 1917, v. 15, pp. 223-232.
Henderson, Yandell and Seibert, E. G. Organization and objects of the Medical Research Board, Air Service, U. S. Army. Jour. A. M. A., 1918, lxxi, 1398.
Henderson, Yandell and Seibert, E. G. Organization and objects of the Medical Research Board, Air Service, U.S. Army. Journal of the American Medical Association, 1918, 71, 1398.
Hertz, A. F. (See also Hurst.) Paresis and involuntary movements following commotion produced by the bursting of a large shell. Proc. Roy. Soc., Méd., Lond., (sec. Neurol.), 1914-15, v. 8, pp. 83-84.
Hertz, A. F. (See also Hurst.) Weakness and uncontrollable movements after the shock from a large shell explosion. Proc. Roy. Soc., Méd., Lond., (sec. Neurol.), 1914-15, v. 8, pp. 83-84.
Hertz, A. F. Nerves and the War. Guy’s Hosp. Gaz., Lond., 1915, v. 29, pp. 169-173; and pp. 335-339.
Hertz, A. F. Nerves and the War. Guy's Hosp. Gaz., London, 1915, vol. 29, pp. 169-173; and pp. 335-339.
Hertz, A. F. Concussion Blindness. Lancet, 1916, i, p. 15.
Hertz, A. F. Concussion Blindness. Lancet, 1916, i, p. 15.
Hertz, A. F. Medical diseases of the war. Lond., 1917, G. Arnold, pp. 151, 8o.
Hertz, A. F. Medical diseases of the war. London, 1917, G. Arnold, pp. 151, 8o.
Hertz, A. F. and Ormond, A. W. The treatment of concussion blindness. Lancet, Lond., 1916, i, 15-17.
Hertz, A. F. and Ormond, A. W. The treatment of concussion blindness. Lancet, London, 1916, i, 15-17.
Hesnard, A. Le traitement local et la radiothérapie locale des blessures des troncs nerveux. Arch. d’électric. méd., Bordeaux, 1916, v. 26, pp. 5-9.
Hesnard, A. Local treatment and local radiotherapy for nerve trunk injuries. Arch. d’électric. méd., Bordeaux, 1916, v. 26, pp. 5-9.
Hesnard, A. Note sur la radiothérapie des blessures des troncs nerveux. Paris méd., 1916 (Par. Méd), v. 19, p. 302.
Hesnard, A. Note on the radiotherapy of nerve trunk injuries. Paris méd., 1916 (Par. Méd), v. 19, p. 302.
Hesnard, A. Un nouvel élément de la réaction de dégénérescence—l’hyperexcitabilité galvanotonique des muscles. Par. méd., 1917, No. 46, pp. 410-415.
Hesnard, A. A new factor in the degeneration reaction—the galvanotonic hyperexcitability of muscles. Med. J., 1917, No. 46, pp. 410-415.
Hesnard, A. Un cas d’hémiplégie glosso-pharyngo-cervico-laryngée par syndrôme des quatres dernières paires crâniennes. Arch. de méd. et pharm. nav., Par., 1917, v. 103, pp. 370-377.
Hesnard, A. A case of glossopharyngeal-cervical-laryngeal hemiplegia due to syndrome of the last four cranial nerves. Arch. de méd. et pharm. nav., Paris, 1917, vol. 103, pp. 370-377.
Hesnard, A. Un cas de psychose post-onirique chez un aliéné militaire. Caducée, Par., 1914, xiv, 202.
Hesnard, A. A Case of Post-Dream Psychosis in a Military Patient. Caducée, Paris, 1914, xiv, 202.
Hesse, W. Ueber Spättetanus, chronischen Tetanus und Tetanusrezidiv. Deutsches Archiv. f. klin. Med., Leipz., 1917, 124, p. 284.
Hesse, W. On Late Tetanus, Chronic Tetanus, and Tetanus Recurrence. German Archives of Clinical Medicine, Leipzig, 1917, 124, p. 284.
Hewat, A. Fergus. Clinical cases from Medical Division, Royal Victoria Hospital, Netley. Edinb. M. J., 1917, v. 18, pp. 210-215.
Hewat, A. Fergus. Clinical cases from the Medical Division, Royal Victoria Hospital, Netley. Edinb. M. J., 1917, v. 18, pp. 210-215.
Hezel. Eine im Felde vorkommende Beschäftigungsneuritis. Neurol. Centralbl., 37, Nr. 15, 1918.
Hezel. An occupational neuritis occurring in the field. Neurol. Centralbl., 37, No. 15, 1918.
Hill, David Spence. Valid uses of psychology in the rehabilitation of war victims. Mental Hygiene, II, October, 1918.
Hill, David Spence. Appropriate applications of psychology in helping war victims recover. Mental Hygiene, II, October, 1918.
Hill, L. Death from high explosives without wounds. Brit. M. J., Lond., 1917, v. 1, p. 665.
Hill, L. Death from high explosives without wounds. Brit. M. J., Lond., 1917, v. 1, p. 665.
Hine, M. L. The recovery of fields of vision in concussion injuries of the occipital cortex. Brit. J. Ophth., Lond., 1918, v. 2, pp. 12-25.
Hine, M. L. The recovery of fields of vision in concussion injuries of the occipital cortex. Brit. J. Ophth., Lond., 1918, v. 2, pp. 12-25.
Hinsdale, G. Hydrotherapeutics in the war. N. Y. Med. Jour., 1917, cvi, 893.
Hinsdale, G. Hydrotherapeutics in the war. N. Y. Med. Jour., 1917, cvi, 893.
Hirschfeld, Arthur. Die hydrotherapeutische Behandlung der im Kriege erworbene Neurasthenie und Hysterie. Zerb. f. Phys. u. Diätet., Ther., Leipz., 1915, v. 19, pp. 59-62.
Hirschfeld, Arthur. The Hydrotherapy Treatment of Neurasthenia and Hysteria Acquired in War. Zerb. f. Phys. u. Diätet., Ther., Leipzig, 1915, v. 19, pp. 59-62.
Hirtz, E. J. Le traitement des impotences fonctionnelles consecutives aux blessures de guerre. Presse Méd., Par., 1915, v. 23, pp. 139-141.
Hirtz, E. J. Treatment of Functional Impotence Following War Injuries. Med Press, Paris, 1915, vol. 23, pp. 139-141.
His, W. Ermüdungsherzen im Felde. Med. Klin. Berl. u. Wien., 1915, v. ii1, pp. 293-298.
His, W. Exhaustion Hearts in the Field. Med. Klin. Berl. u. Wien., 1915, v. ii1, pp. 293-298.
Hoch, August. Recommendations for the observation of mental disorders incident to the War. Psychiat. Bull. Utica, 1917, v. 2, No. 3, pp. 377-385.
Hoch, August. Recommendations for observing mental disorders related to the War. Psychiat. Bull. Utica, 1917, v. 2, No. 3, pp. 377-385.
Hoche. Krieg und Seelenleben, 1915, Speyer and Kaerner, Freiburg.
Hoche. War and the Soul, 1915, Speyer and Kaerner, Freiburg.
Hoche. Die Versorgung der funktionellen Kriegsneurosen. Münch. med. Wchnschr., 1916, v. 63, p. 1782.
Hoche. The Treatment of Functional War Neuroses. Münch. med. Wchnschr., 1916, v. 63, p. 1782.
Holland, C. T. Two years’ experience of war radiography in a base hospital. Amer. Jour. Elec. and Radiol., 1917, xxvi, 448.
Holland, C. T. Two years of experience in war radiography at a base hospital. Amer. Jour. Elec. and Radiol., 1917, xxvi, 448.
Hollande, Lepeytre et Gate, J. Simulation d’albuminurie par injection intravésicale d’ovalbumine. Lyon méd., 1916, v. 125, pp. 194-196.
Hollande, Lepeytre et Gate, J. Simulation of albuminuria by intravesical injection of ovalbumin. Lyon méd., 1916, v. 125, pp. 194-196.
Hollande et Marchand. A propos d’un cas de maladie de Derkum. Lyon med., 1917, v. 126, pp. 362-365.
Hollande and Marchand. Regarding a case of Derkum's disease. Lyon med., 1917, v. 126, pp. 362-365.
Holmes. G. and Lister, W. T. Disturbances of vision from cerebral lesions, with special reference to the cortical representation of the macula. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sec. Ophth.), pp. 57-96.
Holmes, G. and Lister, W. T. Vision disturbances due to brain lesions, focusing on how the macula is represented in the cortex. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sec. Ophth.), pp. 57-96.
Holmes, Gordon and Smith, S. Case of bilateral motor apraxia with disturbance of visual orientation. Jr. Roy. Army Med. Corps, Lond., 1917, i, pp. 78-91.
Holmes, Gordon and Smith, S. Case of bilateral motor apraxia with disturbance of visual orientation. Jr. Roy. Army Med. Corps, Lond., 1917, i, pp. 78-91.
Horder, Thomas J. Cerebro-spinal fever. Lond., 1915, Henry Frowde.
Horder, Thomas J. Meningococcal meningitis. London, 1915, Henry Frowde.
Horn, P. Zur Begutachtung nervöser Unfallfolgen. München. méd. Wchnschr., 1915, v. 62, pp. 1745-48.
Horn, P. Evaluation of Nervous Accident Consequences. Munich. Medical Weekly, 1915, v. 62, pp. 1745-48.
Horn, P. Zur Nützbarmachung erhaltener und wiedergewonnener Arbeitskraft bei Unfallsneurosen. Aerztl. sachverst. Ztg., Berl., 1915, v. 21, pp. 253-257; and pp. 279-282.
Horn, P. On the Utilization of Preserved and Regained Workforce in Accident Neuroses. Medical Expert Journal, Berlin, 1915, vol. 21, pp. 253-257; and pp. 279-282.
Horn, P. Uber Sonnenstich mit organische Symptomen. Zentralbl. Nervenk. u. Psychiat., Coblenz. u. Leipz., 1915, v. 51, No. 4. Berl. Klin, Wchnschr. 1916, i, No. 2, p. 44.
Horn, P. On sunstroke with organic symptoms. Zentralbl. Nervenk. u. Psychiat., Coblenz. u. Leipz., 1915, v. 51, No. 4. Berl. Klin, Wchnschr. 1916, i, No. 2, p. 44.
Horn, P. Zur Aetiologie und klinischen Stellung der Unfall- und Kriegsneurosen. Neurol. Zentralbl. Leipz., 1917, v. 36, No. 3, and No. 7.
Horn, P. On the Etiology and Clinical Position of Accident and War Neuroses. Neurol. Central Journal. Leipzig, 1917, vol. 36, No. 3, and No. 7.
Horsfall, W. N. Malingering in the services. Med. J. Australia, Sydney, 1916, iii, 54.
Horsfall, W. N. Faking illness in the military. Med. J. Australia, Sydney, 1916, iii, 54.
Horsley, Sir Victor. Address on gun-shot wounds of the head; Lancet, Lond., 1915, i, pp. 359-362.
Horsley, Sir Victor. Speech on gunshot wounds to the head; Lancet, London, 1915, i, pp. 359-362.
Horstmann. Zur traumatischen Neurose. Arztl. Sachverst. Ztg., Berl., 1914, v. 22, Nov. 5; Rev. Psychiat. neurol. Wchnschr., Halle, a. S., 1914-15; v. 16; p. 346.
Horstmann. On traumatic neurosis. Medical Expert Journal, Berlin, 1914, vol. 22, Nov. 5; Review of Psychiatry and Neurology Weekly, Halle, a. S., 1914-15; vol. 16; p. 346.
Horstmann. Traumatische Neurose. Arztl. Centr. Ztg., v. 27, p. 53, also p. 76.
Horstmann. Traumatic Neurosis. Medical Central Journal, vol. 27, p. 53, also p. 76.
Hotz. Über Kriegsverletzen des Nervensystems. München med Wchnschr., 1914, No. 45, pp. 2219-2221; and pp. 2264-2266.
Hotz. On war injuries of the nervous system. Munich Med Weekly, 1914, No. 45, pp. 2219-2221; and pp. 2264-2266.
Hotz. Über Kriegsverletzungen des Nervensystems. Zentralbl. f. Chir., Leipz., 1915, v. 421, pp. 6-7.
Hotz. On War Injuries of the Nervous System. Central Journal for Surgery, Leipzig, 1915, vol. 421, pp. 6-7.
Hoven. Les maladies mentales et la guerre. Presse Méd., 1917, v. 53, p. 559.
Hoven. Mental illnesses and war. Medical Press, 1917, v. 53, p. 559.
How to Avoid Damage to Auditory Apparatus by Explosions. Monde méd., 1918, v. 28, pp. 61-63.
How to Avoid Damage to Hearing from Explosions. Monde méd., 1918, v. 28, pp. 61-63.
Howard, W. L. Psychology of War. N. Y. M. J., 1915, v. 101, p. 15.
Howard, W. L. Psychology of War. New York: M. J., 1915, vol. 101, p. 15.
Howland, G. W. Neurosis in returned soldiers. Med. Fortnightly, St. Louis, 1917, v. 49, pp. 97-100.
Howland, G. W. Neurosis in veterans. Med. Fortnightly, St. Louis, 1917, v. 49, pp. 97-100.
Howland, G. W. The neuroses of returned soldiers. Am. Med., Burlington, Vt., 1917, v. 23, pp. 313-319.
Howland, G. W. The psychological issues of returning soldiers. Am. Med., Burlington, Vt., 1917, v. 23, pp. 313-319.
Hrdlicka, Ales. Suggestions relating to the new National Army by the Anthropology Committee of the National Research Council. (Wash., 1917), p. 4, 8o.
Hrdlicka, Ales. Recommendations for the new National Army by the Anthropology Committee of the National Research Council. (Wash., 1917), p. 4, 8o.
Hunt, J. R. Exhaustion pseudoparesis; a fatigue syndrome simulating early paresis, developing under intensive military training. Jour. A. M. A., lxx, 11.
Hunt, J. R. Exhaustion pseudoparesis; a fatigue syndrome that mimics early paresis, occurring during intense military training. Jour. A. M. A., lxx, 11.
Huntington, P. W. The present and proposed Roentgenologic Service of the United States Army. Am. J. Roentgenol., Detroit, 1917, v. 4, pp. 597-601.
Huntington, P. W. The current and suggested Roentgenologic Service of the United States Army. Am. J. Roentgenol., Detroit, 1917, v. 4, pp. 597-601.
Hurst, A. F. (See also Hertz.) Nerves and the war. Guy’s Hosp. Gaz., 1915, v. 29, pp. 169-173.
Hurst, A. F. (See also Hertz.) Nerves and the war. Guy's Hosp. Gaz., 1915, v. 29, pp. 169-173.
Hurst, A. F. Case of deaf-mutism followed by partial amnesia. Guy’s Hosp. Gaz., Lond., 1916, v. 30, p. 279; also pp. 410-412.
Hurst, A. F. Case of deaf-mutism followed by partial amnesia. Guy’s Hosp. Gaz., Lond., 1916, v. 30, p. 279; also pp. 410-412.
Hurst, A. F. Medical diseases of the war. Lond., 1917, Arnold, p. 151, 8o.
Hurst, A. F. Medical diseases of the war. London, 1917, Arnold, p. 151, 8o.
Hurst, A. F. Observations on the etiology and treatment of war neuroses. Brit. M. J., Lond., 1917, ii, pp. 409-414.
Hurst, A. F. Observations on the causes and treatment of war-related psychological conditions. Brit. M. J., Lond., 1917, ii, pp. 409-414.
Hurst, A. F. (Nervous Affections.)
Hurst, A. F. (Anxiety Disorders.)
Hurst, A. F. War epilepsy. Guy’s Hosp. Gaz., Lond., 1917, pp. 209-213.
Hurst, A. F. War epilepsy. Guy's Hosp. Gaz., London, 1917, pp. 209-213.
Hurst, A. F. Classification of war neuroses. Guy’s Hosp. Gaz., Lond., 1917, xxi, 109. Also: Alienist and Neurol., St. Louis, 1917, xxxviii, 458.
Hurst, A. F. Classification of war neuroses. Guy’s Hosp. Gaz., London, 1917, xxi, 109. Also: Alienist and Neurol., St. Louis, 1917, xxxviii, 458.
Hurst, A. F. Etiology and treatment of war neuroses. Brit. Med. Jour., 1917, ii, 409.
Hurst, A. F. Causes and treatment of war-related psychological issues. Brit. Med. Jour., 1917, ii, 409.
Hurst, A. F. Psycho-analysis and war neuroses. Guy’s Hosp. Gaz., Lond., 1917, pp. 308-309.
Hurst, A. F. Psychoanalysis and war neuroses. Guy’s Hospital Gazette, London, 1917, pp. 308-309.
Hurst, A. F. Syphilis of the nervous system in soldiers. Guy’s Hosp. Gaz., Lond., 1917, pp. 365-368.
Hurst, A. F. Syphilis of the nervous system in soldiers. Guy’s Hosp. Gaz., Lond., 1917, pp. 365-368.
Hurst, A. F. Warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sec. otol.), pp. 115-118.
Hurst, A. F. Warfare injuries and mental health issues. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sec. otol.), pp. 115-118.
Hurst, Arthur F. Medical diseases of the war; a record of personal experiences. Hospital, Lon., 1918, lxv, 9.
Hurst, Arthur F. Medical diseases of the war; a record of personal experiences. Hospital, Lon., 1918, lxv, 9.
Hurst, A. F. and Peters, E. A. The pathology, diagnosis and treatment of absolute hysterical deafness in soldiers. Lancet, Lond., 1917, v. ii, pp. 517-519.
Hurst, A. F. and Peters, E. A. The causes, diagnosis, and treatment of total hysterical deafness in soldiers. Lancet, Lond., 1917, v. ii, pp. 517-519.
Hurst, A. F. and Peters, E. A. Pathology, diagnosis, and treatment of absolute hysterical deafness in soldiers. Lancet, Lon., 1917, ii, 517.
Hurst, A. F. and Peters, E. A. The pathology, diagnosis, and treatment of complete hysterical deafness in soldiers. Lancet, Lon., 1917, ii, 517.
Hurst, A. F. and Peters, E. A. Nerve-shattered soldiers and their treatment; Dr. Lumsden’s excellent scheme. Hospital, Lon., 1917, lxii, 487.
Hurst, A. F. and Peters, E. A. Soldiers with nerve damage and their treatment; Dr. Lumsden’s outstanding plan. Hospital, Lon., 1917, lxii, 487.
Hurst, A. F. and Syms, J. L. M. Rapid cure of hysterical symptoms in soldiers. Lancet, Lon., 1918, ii, 139.
Hurst, A. F. and Syms, J. L. M. Quick recovery from hysterical symptoms in soldiers. Lancet, Lon., 1918, ii, 139.
Hutt, C. W. Education of the left hand of disabled sailors and soldiers. Lancet, Lond., 1917, v. 1, pp. 642-646.
Hutt, C. W. Training for the left hand of disabled sailors and soldiers. Lancet, Lond., 1917, v. 1, pp. 642-646.
Hutt, C. W. The future of the disabled soldier. Wm. Wood, 1917.
Hutt, C. W. The Future of the Disabled Soldier. Wm. Wood, 1917.
Hypertension des névroses tachycardiques. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 185-186.
Hypertension from tachycardic neuroses. Gen. Rev. of Clin. and Therapy, Paris, 1916, vol. 30, pp. 185-186.
Hyslop, T. B. The psychology of warfare. West Lond., M. J., 1917, v. 22, pp. 2-12.
Hyslop, T. B. The Psychology of Warfare. West London, M. J., 1917, v. 22, pp. 2-12.
Imbert, Léon. Accidents du travail et blessures de guerre. Une nouvelle loi. Presse Méd., Par., 1917, v. 25, pp. 591-592.
Imbert, Léon. Work Accidents and War Injuries. A New Law. Medical Press, Paris, 1917, vol. 25, pp. 591-592.
Imbert, Léon, et Réal, Pierre. La constriction des machoires, par blessure de guerre. Presse méd., Par., 1916, v. 24, pp. 372-373.
Imbert, Léon, and Réal, Pierre. The Constriction of the Jaw from War Injury. Medical Press, Paris, 1916, vol. 24, pp. 372-373.
Imboden, K. Das Neurosenproblem im Lichte der Kriegsneurologie. Cor. Bl. f. Schweiz. Aerzte., 1917, No. 34, pp. 1098-1109.
Imboden, K. The Neurosis Issue in Light of War Neurology. Cor. Bl. f. Schweiz. Aerzte., 1917, No. 34, pp. 1098-1109.
Isolation and Psychotherapy for soldiers suffering from functional disturbances of the nervous system. Monde méd., Par., 1917, v. 27, pp. 113-115.
Isolation and Psychotherapy for soldiers experiencing functional issues with their nervous system. Monde méd., Par., 1917, v. 27, pp. 113-115.
Isserlin. Kriegspsychiatrische Erfahrungen. Berlin. klin. Wchnschr., 1916, v. 53, p. 295.
Isserlin. Military Psychiatric Experiences. Berlin. Clinical Weekly, 1916, v. 53, p. 295.
Jackson, J. A. A report of the clinical and pathological findings in a case of hystero-epilepsia and hystero-epileptoid. Alienist and Neurol., St. Louis, 1915, xxxvi, 231-235.
Jackson, J. A. A report on the clinical and pathological findings in a case of hystero-epilepsia and hystero-epileptoid. Alienist and Neurol., St. Louis, 1915, xxxvi, 231-235.
Jacob, O. Tumeurs consécutives à l’injection d’huile camphorée preparée avec de l’huile de vaseline. Compt. rend. Soc. de biol., Par., 1917, lxxx, 371, 487.
Jacob, O. Tumors resulting from the injection of camphor oil prepared with petroleum jelly. Compt. rend. Soc. de biol., Paris, 1917, lxxx, 371, 487.
Jacobson, L. Krieg und Nervensystem. Therap. d. Gegenw., Berl., 1915, v. 56, pp. 22-29.
Jacobson, L. War and the Nervous System. Therapy of the Present, Berlin, 1915, vol. 56, pp. 22-29.
Jacobson, L. Krieg und Nervensystem. Med. Klin., Berl. u. Wien., 1915, v. 111, p. 110.
Jacobson, L. War and Nervous System. Med. Klin., Berlin and Vienna, 1915, vol. 111, p. 110.
Jacquetty, G., Bergonié, J. Le travail agricole médicalement prescrit et surveillé comme traitement des séquelles de blessures de guerre. Arch. d’elec. méd. et physiothérap., Par., 1917, No. 148, pp. 297-317.
Jacquetty, G., Bergonié, J. Agricultural work that is medically prescribed and supervised as a treatment for the effects of war injuries. Arch. d’elec. méd. et physiothérap., Par., 1917, No. 148, pp. 297-317.
Jahrmärker. Ueber psychische u. nervöse Störungen bei Kriegern. München med. Wchnschr., 1915, No. 33, p. 1118.
Jahrmärker. On psychological and nervous disorders in soldiers. Munich med. Wchnschr., 1915, No. 33, p. 1118.
Jarrett, Mary C. The Training School of Psychiatric Social Work at Smith College. V. An Emergency Course in a New Branch of Social Work. Mental Hygiene, II, October, 1918.
Jarrett, Mary C. The Training School of Psychiatric Social Work at Smith College. V. An Emergency Course in a New Branch of Social Work. Mental Hygiene, II, October, 1918.
Jeanselme et Huet. Syndrome jacksonien de nature hystérotraumatique. Rev. neurol., Par., 1914-15, v. 222, pp. 723-726.
Jeanselme et Huet. Jacksonian syndrome of hysterotraumatic nature. Rev. neurol., Paris, 1914-15, v. 222, pp. 723-726.
Jeanselme et Huet. Myotonie acquise. Rev. neurol., Par., 1916, v. 29. pp. 414-418.
Jeanselme and Huet. Acquired myotonia. Neurology Review, Paris, 1916, vol. 29, pp. 414-418.
Jelliffe, Smith Ely. Nervous and mental disturbances of influenza. N. Y. Med. Jour., 1918, cviii, 725, 755, 807.
Jelliffe, Smith Ely. Nervous and mental disturbances of influenza. N. Y. Med. Jour., 1918, 108, 725, 755, 807.
Jelliffe, S. E. War (The) and the nervous system. I. Peripheral nerve injuries. N. Y. Med. Jour., 1917, cvi, 17.
Jelliffe, S. E. War and the Nervous System. I. Peripheral Nerve Injuries. N. Y. Med. Jour., 1917, cvi, 17.
Jellinek, S. Zur militärärztlichen Konstatierung der Epilepsie. Wien. klin. Wchnschr., 1915, v. 28, pp. 1021-1025.
Jellinek, S. On the Military Medical Diagnosis of Epilepsy. Wien. klin. Wchnschr., 1915, v. 28, pp. 1021-1025.
Jellinek, S. Zur militärärztlichen Konstatierung der Kriegsneurosen. Wien. klin. Wchnschr., 1916, v. 29, pp. 189-193.
Jellinek, S. On the Military Medical Diagnosis of War Neuroses. Vienna. klin. Wchnschr., 1916, v. 29, pp. 189-193.
Jendrassik, E. Einige Bemerkungen zur Kriegsneurose. Neurol. Centralbl., Leipz., 1916, v. 35, No. 12.
Jendrassik, E. Some Remarks on War Neurosis. Neurol. Centralbl., Leipzig, 1916, v. 35, No. 12.
Jendrassik. E. Zur Discussion über die Neurosenfrage. Theorie der Hysterie und der Neurasthenie. Neurol. Centralbl., Leipz., 1917, 36, 962.
Jendrassik. E. On the discussion regarding the issue of neuroses. Theory of hysteria and neurasthenia. Neurol. Centralbl., Leipzig, 1917, 36, 962.
Jessop, Walter, H. H. Discussion on ophthalmic injuries in warfare. Tr. Ophth. Soc. U. Kingdom, Lond., 1914-15, v. 35, pp. 1-68.
Jessop, Walter, H. H. Discussion on eye injuries in warfare. Tr. Ophth. Soc. U. Kingdom, Lond., 1914-15, v. 35, pp. 1-68.
Jessop, Walter H. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sec. Psychiat.), p. 36.
Jessop, Walter H. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sec. Psychiat.), p. 36.
Jobson, T. B. Normal gun-deafness. Lancet, Lon., 1917, ii, 566.
Jobson, T. B. Typical gun-related hearing loss. Lancet, London, 1917, ii, 566.
Johnstone, E. K. Shell Shock; notes. Mil. Surg., 1918, xlii, 531.
Johnstone, E. K. Shell Shock; notes. Mil. Surg., 1918, xlii, 531.
Jolly. Uber die Dienstfähigkeit und Rentenfrage bei nervenkranken Soldaten. München med. Wchnschr., 1915, v. 34, pp. 1714-1719.
Jolly. On the ability to work and pension issues for soldiers with mental illness. Munich Medical Weekly, 1915, v. 34, pp. 1714-1719.
Jolly, Ph. Arbeitstherapie für nervenkranken Soldaten. Deutsche med. Wchnschr., 1916, v. 42, p. 1514.
Jolly, Ph. Occupational therapy for soldiers with mental health issues. German Med. Weekly, 1916, v. 42, p. 1514.
Jolly, P. Uber Kriegsneurosen. Arch. f. Psychiat., Berl., 1916, v. 56, pp. 385-444.
Jolly, P. On War Neuroses. Archives of Psychiatry, Berlin, 1916, vol. 56, pp. 385-444.
Joltrain, E. Camptocormie et paraplégie consécutives à un ensevelissement par éclatement d’obus. Presse méd., Par., 1917, v. 25, pp. 194-195.
Joltrain, E. Camptocormy and paraplegia following burial due to shell explosions. Méd. Press, Paris, 1917, v. 25, pp. 194-195.
Joltrain, E. Camptocormie et paraplégie consécutives à un ensevelissement par éclatement d’obus; considerations sur l’action due choc émotif. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 41, pp. 431-436.
Joltrain, E. Camptocormia and paraplegia resulting from being buried by exploding shells; considerations on the effects of emotional shock. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 41, pp. 431-436.
Jones, A. B. and Llewellyn, J. L. Malingering, or the Simulation of Disease. Lond., 1917, Wm. Heinemann.
Jones, A. B. and Llewellyn, J. L. Faking Illness, or Pretending to be Sick. Lond., 1917, Wm. Heinemann.
Jones, I. H. Ear (The) and aviation. Jour. M. M. A., 1917, lxix, 1607.
Jones, I. H. Ear and aviation. Journal of the Medical Military Association, 1917, 69, 1607.
Jones, Robert. Notes on Military Orthopedics. Cassell and Co., 1917.
Jones, Robert. Notes on Military Orthopedics. Cassell and Co., 1917.
Jones, Robert. Orthopedic surgery in its relation to the war. Amer. Jour. Care for Crip., 1917, vi, 119.
Jones, Robert. Orthopedic surgery and its connection to the war. Am. Jor. Care for Crip., 1917, vi, 119.
Jones, Robert. The Psychology of Fear and the Effects of Panic Fear in War Times. J. Ment. Sc., Lond., 1917, v. 63, pp. 346-389.
Jones, Robert. The Psychology of Fear and the Effects of Panic Fear in War Times. J. Ment. Sc., Lond., 1917, v. 63, pp. 346-389.
Jones, Robert. Notes on military orthopaedics. Lond., N. Y., etc., 1917, Cassell and Co., p. 132, 8o.
Jones, Robert. Notes on military orthopedics. London, New York, etc., 1917, Cassell and Co., p. 132, 8o.
Jones, Robert. The orthopaedic outlook in Military Surgery. Brit. M. J., Lond., 1918, i, pp. 41-45.
Jones, Robert. The orthopedic perspective in Military Surgery. Brit. M. J., Lond., 1918, i, pp. 41-45.
Jones, W. E. Case of Shell Shock. M. J. Australia, Sydney, 1916, v. 1, pp. 203-204.
Jones, W. E. Case of Shell Shock. M. J. Australia, Sydney, 1916, v. 1, pp. 203-204.
Jones-Phillipson, C. E. Special Discussion on Warfare Injuries and Neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 96-110.
Jones-Phillipson, C. E. Special Discussion on Warfare Injuries and Neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 96-110.
Jörger, J. Mobilmachung als krankheitsauslösendes Trauma bei Dementia Praecox. Cor.-Bl. f. Schweiz., Aerzte, 1914, v. 442, No. 50, pp. 1553-1570.
Jörger, J. Mobilization as a Cause of Trauma in Dementia Praecox. Cor.-Bl. f. Schweiz., Ärzte, 1914, v. 442, No. 50, pp. 1553-1570.
Joseph, E. Einige Erfahrungen über Schädelschüsse, besonders über die Bedeutung des Röntgenbildes für die Schädelchirurgie. Münch. Med. Woch., 1915, lxii, 1197.
Joseph, E. Some experiences regarding skull shots, especially the significance of X-rays for skull surgery. Münch. Med. Woch., 1915, lxii, 1197.
Joubert, Camille. Note sur un cas de paraplégie organique consécutive à la déflagration d’un obus de gros calibre sans plaie extérieure. Paris méd., 1915 (Part. Méd.), v. 17, pp. 444-446.
Joubert, Camille. Note on a case of organic paraplegia resulting from the explosion of a large-caliber shell without any external wounds. Paris méd., 1915 (Part. Méd.), v. 17, pp. 444-446.
Jourdan. Un cas d’oedème provoqué du membre inférieur. Montpel. méd., 1916, xxxix, 446-449.
Jourdan. A case of edema in the lower limb. Montpel. méd., 1916, xxxix, 446-449.
Jourdan and Sicard. Étude macroscopique et microscopique des lésions des nerfs par blessure de guerre. Presse méd., July 29, 1915.
Jourdan and Sicard. Macroscopic and microscopic study of nerve injuries from war wounds. Medical Press, July 29, 1915.
Jourdran, Maurice-Louise-Marie. Crises nerveuses chez les blessés de guerre crâniocérébraux. (Épilepsie généralisée, hystérie, hystéro-épilepsie). Bordeaux, 1917, 88 pp., 8, + No. 1.
Jourdran, Maurice-Louise-Marie. Nervous Crises in War Injuries to the Cranio-Cerebral Area (Generalized Epilepsy, Hysteria, Hystero-Epilepsy). Bordeaux, 1917, 88 pages, 8, + No. 1.
Jourdran et Marchand, L. De la rage chez l’homme. Presse Méd., Par., 1917, v. 25, pp. 371-373.
Jourdran et Marchand, L. On Rabies in Humans. Medical Press, Paris, 1917, v. 25, pp. 371-373.
Juliusburger, O. Zur Kenntnis der Kriegsneurosen. Monatschr. f. Psychiat. u. Neurol., Berl., 1915, v. 38, pp. 305-318.
Juliusburger, O. On the Understanding of War Neuroses. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, vol. 38, pp. 305-318.
Jumentié. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 463.
Jumentié. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 463.
Jumentié. Contraction neuro-musculaire et réflexes tendineux dans certains états d’impotence dits fonctionnels et à caractères psychonévrosiques. Étude par la méthode graphique. Rev. neurol., Par., 1916, No. 6, p. 960.
Jumentié. Neuromuscular contractions and tendon reflexes in certain states of functional impairment with psychoneurotic characteristics. Study using graphic method. Rev. neurol., Par., 1916, No. 6, p. 960.
Jumentié. Deux cas d’hémiatrophie linguale associée à d’autres paralysies des nerfs crâniens et rachidiens chez des commotionnés. Montpel. med., 1917, xxxix, 1006-1009.
Jumentié. Two cases of hemihypertrophy of the tongue associated with other cranial and spinal nerve paralysis in individuals with concussions. Montpel. med., 1917, xxxix, 1006-1009.
Juquelier, P. Un cas complexe d’appréciation de la résponsabilité pénale chez un épileptique. J. de méd. de Par., 1917, v. 36, pp. 47-48.
Juquelier, P. A complex case regarding the assessment of criminal responsibility in an epileptic. J. de méd. de Par., 1917, v. 36, pp. 47-48.
Juquelier, P., et Quellien, P. Épilepsie larvée par traumatisme de guerre (commotion cérébrale). Ann. méd. psychol. Par., 1917, v. 73, pp. 536-546.
Juquelier, P., and Quellien, P. Epilepsy triggered by war trauma (concussion). Ann. méd. psychol. Par., 1917, v. 73, pp. 536-546.
Kafka, V. Fortschritte der für die Psychiatrie wichtigen biologischen, insbesondere serologischen Forschungsgebiete. Jahresb. f. Ärztl. Fortbild., München, 1915, v. 5, pp. 51-54.
Kafka, V. Advances in the Biological Research Areas Important for Psychiatry, Especially Serological Research. Annual Report for Medical Continuing Education, Munich, 1915, vol. 5, pp. 51-54.
Kafka. Schreckneurose. (Ärztl. Verein Hamburg, 26, Jan., 1915.) München. med. Wchnschr., 1915, v. 62, p. 198.
Kafka. Schreckneurose. (Medical Association Hamburg, Jan. 26, 1915.) Munich. Medical Weekly, 1915, vol. 62, p. 198.
Kahne, Max. Über die Anwendung der physikalischen Heilmethoden bei Kriegskrankheiten. Wien. med. Wchnschr., 1914, v. 64, pp. 540-547.
Kahne, Max. On the Application of Physical Healing Methods for War-Related Illnesses. Vienna Medical Weekly, 1914, v. 64, pp. 540-547.
Kahne, Max. Vorschläge zur Organisation der spezialärztlichen Dienstleistung in Kriegszeiten. Wien. klin. Wchnschr., 1914, ii, pp. 1262-1263.
Kahne, Max. Suggestions for the Organization of Specialist Medical Services in Wartime. Vienna. Clinical Weekly, 1914, ii, pp. 1262-1263.
Kahne, Max. Über Hyperthyreoidismus vom Standpunkte der Kriegsmedizin. Wien. klin. Wchnschr., 1915, v. 281, pp. 148-153.
Kahne, Max. On Hyperthyroidism from the Perspective of Military Medicine. Vienna Clinical Weekly, 1915, v. 281, pp. 148-153.
Kalhof. Operierte Schädelschüsse. Ther. Monatschr., Berl., 1915, v. 29, pp. 450-453.
Kalhof. Operative head injuries. Ther. Monatschr., Berlin, 1915, vol. 29, pp. 450-453.
Kalt. Rapport sur les maladies simulées et les maladies provoquées. Clin. Ophth., Par., 1916, v. 21, pp. 500-504.
Kalt. Report on feigned illnesses and induced diseases. Clin. Ophth., Paris, 1916, vol. 21, pp. 500-504.
Karplus, I. P. Ueber Erkrankungen nach Granatexplosionen. Wien. klin. Wchnschr., 1915, v. 28, pp. 145-148.
Karplus, I. P. About Illnesses Following Grenade Explosions. Vienna. Clinical Weekly, 1915, v. 28, pp. 145-148.
Karplus, I. P. Ueber eine ungewöhnliche zerebrale Erkrankung nach Schrapnellverletzung. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 456-462.
Karplus, I. P. About an unusual brain condition following a shrapnel injury. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 456-462.
Kashtshenko, P. P. (Statistics of the movement of insane soldiers, according to data obtained by an inquiry.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 199-203.
Kashtshenko, P. P. (Statistics on the movement of mentally ill soldiers, based on data from an inquiry.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 199-203.
Kashtshenko, P. P. (History of development of measures for the care of insane soldiers and those participating in military events.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 151-156.
Kashtshenko, P. P. (History of development of measures for the care of mentally ill soldiers and those involved in military events.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 151-156.
Kashtshenko, P. P. (À propos of M. B. Krol’s article, “Statistics of the movement of insane soldiers, etc.”) Ibid., 1916, iii, 22, 43.
Kashtshenko, P. P. (Regarding M. B. Krol’s article, “Statistics of the Movement of Insane Soldiers, etc.”) Ibid., 1916, iii, 22, 43.
Kashtshenko, P. P. (Certain data concerning insane warriors, prepared by the combined Statistico-Psychiatrical Bureau of the Unions of Zemstvos and Municipalities.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 353-377.
Kashtshenko, P. P. (Some information about mentally ill soldiers, compiled by the joint Statistical-Psychiatric Bureau of the Unions of Zemstvos and Municipalities.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 353-377.
Kastan, Max. Forensisch-psychiatrische Beobachtungen an Angehörigendes Feldheeres. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 734-737.
Kastan, Max. Forensic psychiatric observations on members of the field army. German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, pp. 734-737.
Kastan, Max. Die strafbaren Handlungen psychischkranker Angehöriger des Feldheeres. Archiv. f. Psychiat., Berl., 1916, pp. 573-631.
Kastan, Max. The Criminal Acts of Mentally Ill Members of the Field Army. Archives of Psychiatry, Berlin, 1916, pp. 573-631.
Kaufmann, Fritz. Die planmässige Heilung komplizierter psychogener Bewegungsstörungen bei Soldaten in einer Sitzung. Münch. med. Wchnschr., 1916, v. 631, pp. 802-804.
Kaufmann, Fritz. Systematic Treatment of Complex Psychogenic Movement Disorders in Soldiers in One Session. Münch. med. Wchnschr., 1916, v. 631, pp. 802-804.
Keiper, G. F. Pretended blindness and deafness and their detection. J. Indiana M. Ass., Fort Wayne, 1917, x, 422-426.
Keiper, G. F. Faking blindness and deafness and how to detect it. J. Indiana M. Ass., Fort Wayne, 1917, x, 422-426.
Keith, John R. Vasodilators in the treatment of hysterical aphonia. Brit. M. J., Lond., 1915, i, p. 847.
Keith, John R. Vasodilators in the treatment of hysterical aphonia. Brit. M. J., Lond., 1915, i, p. 847.
Kennedy, F. Clinical observations on shell shock. Med. Rec., N. Y., 1916, v. 89, p. 388.
Kennedy, F. Clinical observations on shell shock. Med. Rec., N. Y., 1916, v. 89, p. 388.
Kennedy, Foster. Nature of nervousness in soldiers. Jour. A. M. A., 1918, lxxi, 17.
Kennedy, Foster. The nature of nervousness in soldiers. Journal of the American Medical Association, 1918, 71, 17.
Kenyon, E. L. The stammerer and army service. J. Am. M. Ass., Chicago, 1917, v. 69, p. 664.
Kenyon, E. L. The Stutterer and Military Service. J. Am. M. Ass., Chicago, 1917, v. 69, p. 664.
Khoroshko, V. K. (Psychiatric impressions and observations in the regions of the active army.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 377-383.
Khoroshko, V. K. (Psychiatric impressions and observations in the areas of the active army.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 377-383.
Khoroshko, V. K. (Mental disturbances following physical and mental shock in the war; traumatic psychoses in the active army.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 3-10.
Khoroshko, V. K. (Mental disturbances after physical and mental shock in the war; traumatic psychoses in the active army.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 3-10.
Khoroshko, V. K. (Organization of aid to warriors with wounded or diseased nervous system.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 398-401.
Khoroshko, V. K. (Helping warriors with injured or affected nervous systems.) Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 398-401.
Kidner, E. B. The vocational reëducation of the disabled soldier. Am. Med., Burlington, Vt., 1917, v. 23, pp. 405-408.
Kidner, E. B. The vocational reeducation of the disabled soldier. Am. Med., Burlington, Vt., 1917, v. 23, pp. 405-408.
Kinberg, O. (Psychoneuroses in soldiers at the front.) Hygiea, Stockholm, 1916, v. 78, pp. 97-126.
Kinberg, O. (Psychoneuroses in soldiers at the front.) Hygiea, Stockholm, 1916, v. 78, pp. 97-126.
Kindlmann. Entlarvung von Taubheit und Schwerhörigkeit Simulierenden. Wien. klin. Wchnschr., 1915, v. 28, p. 1069.
Kindlmann. Unmasking Those Pretending to be Deaf and Hard of Hearing. Vienna. Clinical Weekly, 1915, v. 28, p. 1069.
Kirmsze, M. Geistesschwäche als Helden. Ztschr. f. d. Behndl., Schwachsinn. u. Epilept., Dresd., 1915, No. 9, pp. 134-141.
Kirmsze, M. Mental Weakness as Heroes. Journal for Treatment, Weakness, and Epilepsy, Dresden, 1915, No. 9, pp. 134-141.
Kleist. Schreckpsychosen. Neurol. Centralbl., 37, Nr. 16, 1918.
Kleist. Schreckpsychosen. Neurol. Centralbl., 37, No. 16, 1918.
Kluge, O. Hysterische Seh- und Hröstörungen bei Soldaten; (Inaug. Dissert., Berl., 1914). Rev. Neurol. Centralbl., Leipz., 1915, v. 34, p. 735.
Kluge, O. Hysterical vision and hearing disorders in soldiers; (Inaug. Dissert., Berl., 1914). Rev. Neurol. Centralbl., Leipz., 1915, v. 34, p. 735.
Knapp, Paul. Kriegschädigungen der Sehorgane. Cor.-Bl. f. Schweizer Aerztl., 1916, Nr. 38, pp. 1185-1201.
Knapp, Paul. Damage to the Visual Organs from War. Cor.-Bl. f. Schweizer Aerztl., 1916, No. 38, pp. 1185-1201.
Koblylinsky, M. La psichiatria e la guerra. Quaderni di psichiat., Genova, 1914, i, pp. 337-341.
Koblylinsky, M. Psychiatry and War. Psychiatric Notebooks, Genoa, 1914, vol. i, pp. 337-341.
Kofler. Fall von hysterischer Gehstörung nach Schussverletzung des Unterschenkels. Wien. med. Wchnschr., 1915, No. 1, p. 39.
Kofler. Case of hysterical walking disturbance following a gunshot wound to the lower leg. Vienna. Med. Weekly, 1915, No. 1, p. 39.
Kouindjy, P. Le massage méthodique chez les blessés de guerre. Presse méd., Par., 1914, v. 22, pp. 610-611.
Kouindjy, P. Systematic Massage for War Injuries. Medical Press, Paris, 1914, vol. 22, pp. 610-611.
Kouindjy, P. La rééducation chez les blessés de la guerre et le rôle de la suppléance. Bull. Acad. de méd., Par., 1915, 3 s., v. 74, pp. 105-108.
Kouindjy, P. Rehabilitation for War Injuries and the Role of Substitution. Bull. Acad. de méd., Par., 1915, 3 s., v. 74, pp. 105-108.
Kouindjy, P. La rééducation des mouvements chez les blessés de guerre. Paris méd., 1915-16, v. 17, pp. 298-302.
Kouindjy, P. Rehabilitation of Movement in War Injuries. Paris Med., 1915-16, v. 17, pp. 298-302.
Kouindjy, P. La kinésithérapie de guerre. Paris, 1916, A. Maloine and Fils.
Kouindjy, P. The Physiotherapy of War. Paris, 1916, A. Maloine and Sons.
Krebs. Ohrbeschädigungen im Felde. Münch. med. Wchnschr., 1915, v. 62, pp. 347-349.
Krebs. Hearing damage in the field. Münch. med. Wchnschr., 1915, v. 62, pp. 347-349.
Kreuser, D. Zur Frage der Kriegspsychosen. Allg. Ztschr. Psychiat., 74, 1918.
Kreuser, D. On the Question of War Psychoses. General Journal of Psychiatry, 74, 1918.
Krieg und Wahnsinn. Psychiat. Neurol. Wchnschr., Halle a. S., 1914-15, v. 16, p. 298.
War and Madness. Psychiat. Neurol. Wchnschr., Halle a. S., 1914-15, v. 16, p. 298.
Krol, M. B. (Statistics of the movement of insane soldiers; Apropos of P. B. Kashtshenko’s article: “Statistics of the movement of insane soldiers, etc.,”) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 287-291.
Krol, M. B. (Statistics on the movement of mentally ill soldiers; Related to P. B. Kashtshenko’s article: “Statistics on the movement of mentally ill soldiers, etc.,”) Psikhiat. Gaz., Petrograd, 1915, v. 2, pp. 287-291.
Krüche, A. Zur medico-mechanischen Nachbehandlung der verwundeten Krieger. Aerztl. Centralbl. Ztg., Wien., 1915, v. 27, pp. 43-45.
Krüche, A. On the medical-mechanical aftercare of wounded soldiers. Medical Central Bulletin, Vienna, 1915, vol. 27, pp. 43-45.
Krückmann, E. Ueber Kriegsblindenfürsorge. Deutsche med. Wchnschr., Leipz. u. Berl., 1915, v. 41, p. 725; p. 763; p. 788.
Krückmann, E. On the Care of War Blinded Individuals. German Medical Weekly, Leipzig and Berlin, 1915, v. 41, p. 725; p. 763; p. 788.
Krüll. M. Die Strafrechtliche Begutachtung der Soldaten im Felde. Berl. klin. Wchnschr., Nr. 24, 1918.
Krüll. M. The Criminal Assessment of Soldiers in the Field. Berl. klin. Wchnschr., No. 24, 1918.
Kuehn, A. Ueber functionelle Erkrankungen des Nervensystems bei Kriegsteilnehmern. Ztschr. f. Med. Beamte, Berl., 1917, 30, 497.
Kuehn, A. On functional disorders of the nervous system in war participants. Ztschr. f. Med. Beamte, Berl., 1917, 30, 497.
Laborderie, J. La mécanothérapie dans les formations sanitaires. Rev. gén. de clin. et de thérap., Par., 1915, v. 29, p. 327.
Laborderie, J. Mechanotherapy in Health Facilities. Gen. Rev. of Clinic and Therapy, Paris, 1915, vol. 29, p. 327.
Lagrange. Des désordres oculaires médiats ou indirects par les armes à feu. Bull. Acad. de méd., Par., 1915, v. 73, pp. 591-601.
Lagrange. Eye disorders caused directly or indirectly by firearms. Bull. Acad. de méd., Par., 1915, v. 73, pp. 591-601.
Lagrange, Félix. Les fractures de l’orbite. Paris, 1917, Masson and Cie.
Lagrange, Félix. The fractures of the orbit. Paris, 1917, Masson and Company.
Lahy, J. M. Sur la psycho-physiologie du soldat mitrailleur. Compt. rend. Acad. d. sc., Par., 1916, v. 163, pp. 33-35.
Lahy, J. M. On the Psychophysiology of the Machine Gunner. Compt. rend. Acad. d. sc., Paris, 1916, v. 163, pp. 33-35.
Laignel-Lavastine. Diagnosis and treatment of war psychoneuroses, especially with reference to cases of convulsions and asthenia. War Med., 1918, ii, 44.
Laignel-Lavastine. Diagnosis and treatment of war-related mental health issues, particularly concerning cases of convulsions and fatigue. War Med., 1918, ii, 44.
Laignel-Lavastine. Rapport sur le centre neurologique de la Ire région. Rev. neurol., Par., 1914-15, v. 222, p. 1165.
Laignel-Lavastine. Report on the neurological center of the 1st region. Rev. neurol., Paris, 1914-15, v. 222, p. 1165.
Laignel-Lavastine. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 472.
Laignel-Lavastine. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 472.
Laignel-Lavastine. Sur les accidents nerveux determinés par la déflagration de fortes charges d’explosifs. Rev. neurol. Par., 1916, v. 29, pp. 595-596.
Laignel-Lavastine. On nervous accidents caused by the explosion of large amounts of explosives. Rev. neurol. Par., 1916, v. 29, pp. 595-596.
Laignel-Lavastine. Sur la relative fréquence des cas de peur invincible, chez les combattants. Ann. med.-psychol., Par., 1917, v. 73, pp. 380-384.
Laignel-Lavastine. On the relative frequency of cases of overwhelming fear among combatants. Ann. med.-psychol., Paris, 1917, vol. 73, pp. 380-384.
Laignel-Lavastine. Centre des psychonévroses du gouvernement militaire de Paris. Rev. neurol., Par., 1916, xxiii, 649-656.
Laignel-Lavastine. Center for Psychoneuroses of the Military Government of Paris. Rev. neurol., Paris, 1916, xxiii, 649-656.
Laignel-Lavastine et Ballet, V. “Pseudo-ptosis hystérique” avec synergie fonctionnelle oculo-palpébrale. Rev. neurol., Par., 1916, v. 29, pp. 179-181.
Laignel-Lavastine and Ballet, V. “Hysterical Pseudo-ptosis” with Functional Oculo-palpable Synergy. Rev. neurol., Paris, 1916, v. 29, pp. 179-181.
Laignel-Lavastine et Ballet, Victor. Maniérisme puéril post-confusionnel. Ann. méd.-psychol., Par., 1917, v. 23, pp. 232-240.
Laignel-Lavastine and Ballet, Victor. Childish mannerism after confusion. Ann. méd.-psychol., Paris, 1917, vol. 23, pp. 232-240.
Laignel-Lavastine et Courbon, Paul. Camptodactylie, causalgie et inversion du reflexe tricipital par lesion de la VII paire cervicle. Rev. neurol., Par., 1916, v. 29, pp. 927-932.
Laignel-Lavastine and Courbon, Paul. Camptodactyly, causalgia, and inversion of the triceps reflex due to damage to the 7th cervical nerve. Neurol. Rev., Paris, 1916, vol. 29, pp. 927-932.
Laignel-Lavastine et Courbon, Paul. Amaurose par éclatement d’obus avec meningite syphilitique. (Présentation de malade.) Rev. neurol., Par., 1916, v. 24, pp. 402-405.
Laignel-Lavastine and Courbon, Paul. Amaurosis caused by shell explosions with syphilitic meningitis. (Patient presentation.) Neurology Review, Paris, 1916, vol. 24, pp. 402-405.
Laignel-Lavastine et Courbon, Paul. Les déviations de la colonne vertébrale: le Campto-Rachis. Rev. gén. de pathol. de guerre, Par., 1916, No. 1, pp. 1-18.
Laignel-Lavastine and Courbon, Paul. Spinal Deviations: Campto-Rachis. Gen. Rev. of War Pathology, Paris, 1916, No. 1, pp. 1-18.
Laignel-Lavastine et Courbon, Paul. Les troubles de la marche consécutives aux émotions et commotions de la guerre. Paris méd., 1916, v. 21, pp. 194-203.
Laignel-Lavastine and Courbon, Paul. The walking disorders resulting from the emotions and shocks of war. Paris méd., 1916, v. 21, pp. 194-203.
Laignel-Lavastine et Courbon, P. Stéréotypies de la marche, de l’attitude et de la mimique avec représentation mentale professionnelle de l’ouie consécutives aux émotions du champ de bataille. Ann. méd.-psychol., Par., 1916-17, v. 7, pp. 498-505.
Laignel-Lavastine and Courbon, P. Stereotypies of walking, posture, and facial expression with professional mental representation of hearing resulting from emotions on the battlefield. Ann. méd.-psychol., Paris, 1916-17, vol. 7, pp. 498-505.
Laignel-Lavastine et Courbon, P. De la simulation des troubles fonctionnels du système nerveux par les débiles mentaux. Ann. méd.-psychol., Par., 1916-17, v. 7, pp. 512-519.
Laignel-Lavastine and Courbon, P. On the simulation of functional disorders of the nervous system by individuals with cognitive disabilities. Ann. méd.-psychol., Paris, 1916-17, vol. 7, pp. 512-519.
Laignel-Lavastine et Courbon, P. Trois dysbasies différentes consécutives à des blessures de la région du tenseur du fascia lata (Essai de physiologie pathologique neuro-musculaire). Rev. neurol., Par., 1917, v. 24, pp. 221-224.
Laignel-Lavastine and Courbon, P. Three different forms of dysbasia resulting from injuries to the area of the tensor fascia lata (Essay on neuro-muscular pathological physiology). Rev. neurol., Paris, 1917, vol. 24, pp. 221-224.
Laignel-Lavastine et Courbon, P. Syndrôme sympathique cervical oculaire de paralysie avec hémianidrose cervico-faciale et aphonie hystérique par blessure cervicale droite. Rev. neurol., Par., 1917, v. 24, p. 509.
Laignel-Lavastine and Courbon, P. Cervical sympathetic eye syndrome from paralysis with hemidryness of the neck and face and hysterical aphonia due to right cervical injury. Neurology Review, Paris, 1917, v. 24, p. 509.
Laignel-Lavastine et Courbon, P. Féminisme post-ourlien (microrchidie et gynécomastie consécutives à une orchite double). Presse méd., Par., 1917, v. 25, p. 492.
Laignel-Lavastine and Courbon, P. Post-ourlian feminism (micropenis and gynecomastia following a double orchitis). Med. Press, Paris, 1917, v. 25, p. 492.
Laignel-Lavastine et Courbon, P. Essai sur l’insincérité chez les accidentés de la guerre. Paris méd., 1917, No. 27, pp. 14-19.
Laignel-Lavastine and Courbon, P. Essay on Insincerity Among War Accident Victims. Paris Med., 1917, No. 27, pp. 14-19.
Laignel-Lavastine et Courbon, P. Prophylaxie et traitement de l’insincérité chez les accidentés de la guerre. Paris méd., 1917, No. 46, pp. 407-410.
Laignel-Lavastine and Courbon, P. Prevention and treatment of dishonesty in war casualties. Paris med., 1917, No. 46, pp. 407-410.
Laignel-Lavastine et Courbon, P. Syndrôme psychasthénique consécutif aux émotions de guerre. Ann. méd.-psychol., Par., 1917, v. 73, pp. 391-403.
Laignel-Lavastine and Courbon, P. Psychasthenic syndrome following war emotions. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 391-403.
Laignel-Lavastine et Courbon, P. États seconds cataleptiformes post-confusionnels par émotion-choc de guerre. Ann. méd.-psychol., Par., 1917, v. 73, pp. 411-422.
Laignel-Lavastine and Courbon, P. Secondary cataleptiform states following post-confusion shock from war trauma. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 411-422.
Laignel-Lavastine et Courbon, P. Psychasthénie acquise. Ann. méd.-psychol., Par., 1917, v. 73, pp. 582-588.
Laignel-Lavastine et Courbon, P. Acquired Psychasthenia. Ann. méd.-psychol., Paris, 1917, v. 73, pp. 582-588.
Laignel-Lavastine et Fay, H. M. Psychogénèse d’une crise hystérique. Ann. méd.-psychol., Par., 1917, v. 73, pp. 422-425.
Laignel-Lavastine and Fay, H. M. Psychogenesis of a Hysterical Crisis. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 422-425.
Landau. Le principe de l’isolement psychique dans le traitement des troubles nerveux fonctionnels. Presse méd., Par., 1916, v. 25, p. 312.
Landau. The principle of psychological isolation in the treatment of functional nervous disorders. Med. Press, Paris, 1916, v. 25, p. 312.
Landau. Le principe de l’isolement psychique dans le traitement des “troubles nerveux fonctionnels” de guerre. Bull. Acad. de méd. de Par., 20 juin 1917, v. 31, p. 236, No. 23.
Landau. The principle of psychological isolation in the treatment of "functional nervous disorders" from war. Bull. Acad. de méd. de Par., June 20, 1917, vol. 31, p. 236, No. 23.
Lande, P. et Marguery, F. Contribution à l’étude expérimentale de l’ictère simulé picrique. J. de méd. de Bordeaux, 1917, v. 88, pp. 277-280.
Lande, P. and Marguery, F. Contribution to the experimental study of simulated picric jaundice. J. de méd. de Bordeaux, 1917, v. 88, pp. 277-280.
Landolt, Marc. Les troubles de la vision nocturne chez les soldats. Arch. d’ophth., Par., 1917, v. 35, pp. 580-605.
Landolt, Marc. Night vision disorders in soldiers. Arch. d’ophth., Paris, 1917, vol. 35, pp. 580-605.
Lannois (avec M. Chavanne). Des surdités totales par éclatement d’obus. Bull. Acad. de Méd., Par., 1915, v. 73, pp. 105-108.
Lannois (with M. Chavanne). Total hearing loss from shell explosions. Bull. Acad. de Méd., Paris, 1915, v. 73, pp. 105-108.
Lannois et Chavanne. Des surdités totales par éclatement d’obus. J. méd. et de chir., 1915, v. 86.
Lannois and Chavanne. Total deafness from shell explosion. J. méd. et de chir., 1915, v. 86.
Lannois et Chavanne, F. Le pronostic des surdités de guerre (d’après 1000 cas). Rev. Paris, méd. (Part. méd.), v. 19, p. 36.
Lannois et Chavanne, F. The Prognosis of War-Related Hearing Loss (Based on 1,000 Cases). Rev. Paris, méd. (Part. méd.), v. 19, p. 36.
Lannois, M. et Chavanne, F. Le pronostic des surdités de guerre (d’après 1000 cas.). Lyon méd., 1916, v. 125, pp. 35-40.
Lannois, M. and Chavanne, F. The prognosis of war-related hearing losses (based on 1000 cases). Lyon med., 1916, v. 125, pp. 35-40.
Lannois et Chavanne, F. La surdité de guerre bilatérale totale. Rééducation auditive ou lecture sur les lèvres? Lyon méd., 1916, v. 125, pp. 479-487.
Lannois et Chavanne, F. Total bilateral war deafness. Auditory rehabilitation or lip reading? Lyon méd., 1916, v. 125, pp. 479-487.
Lannois et Chavanne. Rééducation auditive ou lecture sur les lèvres dans la surdité bilatorale totale. J. d. méd. Par., 1917, pp. 114-115.
Lannois and Chavanne. Auditory rehabilitation or lip reading in total bilateral deafness. J. d. méd. Par., 1917, pp. 114-115.
Laquerrière, A. Notes sur l’électro-diagnostic de guerre. J. de radiol. et d’électrol., Par., 1916, v. 2, pp. 19-30.
Laquerrière, A. Notes on War Electrodiagnostics. J. of Radiology and Electrology, Paris, 1916, vol. 2, pp. 19-30.
Laquerrière, A. L’électricité dans la rééducation des troubles névropathiques des blessés de guerre. J. de radiol. et d’électrol., Par., 1917, v. 2, pp. 459-467.
Laquerrière, A. Electricity in the Rehabilitation of Neuropathic Disorders of War Injuries. J. de radiol. et d’électrol., Paris, 1917, vol. 2, pp. 459-467.
Laquerrière et Peyre. La physiothérapie préventive dans les blessures de guerre. J. de méd. et de chir., 1915, v. 86. June.
Laquerrière and Peyre. Preventive physiotherapy in war injuries. J. of Med. and Surg., 1915, vol. 86. June.
Larat et Billiard. L’électrothérapie pendant la rééducation professionnelle. Arch. d’élect. méd. et de physiothérap., Par., 1917, No. 418, pp. 335-336.
Larat and Billiard. Electrotherapy during occupational rehabilitation. Arch. d’élect. méd. et de physiothérap., Par., 1917, No. 418, pp. 335-336.
Larat, J. et Billiard, A. Électricité médicale et rééducation professionnelle. Paris méd., 1917, No. 43, pp. 344-347.
Larat, J. and Billiard, A. Medical Electricity and Professional Rehabilitation. Paris Med., 1917, No. 43, pp. 344-347.
Larat, J. et Lehmann, P. Traitement électrique simplifié des accidents nerveux consécutifs aux blessures de guerre. Presse méd., Par., 1915, v. 23, pp. 35-37.
Larat, J. and Lehmann, P. Simplified electrical treatment of nerve injuries resulting from war wounds. Med Press, Paris, 1915, vol. 23, pp. 35-37.
Lattes, L. I semi-alienati in medicina legale militare e il concetto di pericolosità. Riv. di méd. leg., Pisa, 1917, vii, iv, 49.
Lattes, L. Semi-alienation in military legal medicine and the concept of dangerousness. Riv. di méd. leg., Pisa, 1917, vii, iv, 49.
Laudenheimer. Die Anamnese der sogenannten Kriegspsychoneurosen. München. med. Wchnschr., 1915, v. 62, pp. 1302-1304.
Laudenheimer. The history of the so-called war psychoneuroses. Munich. med. Weekly, 1915, v. 62, pp. 1302-1304.
Laurent, O. Accidents nerveux produits à distance par les projectiles de guerre. Compt. rend. acad. d. sc., Par., 1914, v. 158, pp. 1211-1213.
Laurent, O. Nervous accidents caused remotely by war projectiles. Compt. rend. acad. d. sc., Paris, 1914, v. 158, pp. 1211-1213.
Lautier-Jean, H. M. A. Contribution à l’étude des maladies mentales dans l’armée. Peut-on utiliser les imbéciles? Thèses de Paris, 1915-1916, v. 8.
Lautier-Jean, H. M. A. Contribution to the study of mental illnesses in the army. Can we utilize the mentally challenged? Paris theses, 1915-1916, v. 8.
Lautier, J. Médecine mentale de guerre. Presse méd., 1917, v. 25, p. 492.
Lautier, J. Mental Medicine of War. Medical Press, 1917, vol. 25, p. 492.
Lautier. J. Un cas de délire mystique chez un Musulman. Ann. méd.-psychol., Par., 1917, v. 73, pp. 404-411.
Lautier. J. A case of mystical delirium in a Muslim. Ann. méd.-psychol., Paris, 1917, vol. 73, pp. 404-411.
Lattes, Leone, e Goria, Carlo. Alcune considerazioni attorno alle psiconeurosi d’origine bellica. Arch. di antrop. crim. (etc.), Torino, 1917, v. 38, pp. 97-117.
Lattes, Leone, and Goria, Carlo. Some thoughts on war-related psychosomatic disorders. Arch. di antrop. crim. (etc.), Turin, 1917, vol. 38, pp. 97-117.
Laval, E. Des abcès par injection de pétrole. Bull. et mém. Soc. de chir. de Par., 1915, n. s., xli, 2378-2382. Also: Bull. méd., Par., 1916, xxx, 94-96.
Laval, E. On abscesses caused by oil injections. Bull. et mém. Soc. de chir. de Par., 1915, n. s., xli, 2378-2382. Also: Bull. méd., Par., 1916, xxx, 94-96.
Lawson, A. Blinded sailors and soldiers; remarks on the training at St. Dunstan’s. Lancet, Lond., 1917, v. 1, p. 223.
Lawson, A. Blinded sailors and soldiers; comments on the training at St. Dunstan’s. Lancet, Lond., 1917, v. 1, p. 223.
Lawson, A. How blinded soldiers are cared for. Hospital, Lon., lxi, 319.
Lawson, A. How blinded soldiers are cared for. Hospital, Lon., lxi, 319.
Lawson, A. Making the unfit into serviceable recruits. Hospital, Lon., lix, 390.
Lawson, A. Turning unfit individuals into usable recruits. Hospital, Lon., lix, 390.
Lebar. Sur un cas de canitie rapide. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 439-443.
Lebar. On a case of rapid graying. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 439-443.
Lebar. Sur l’oedème hystérique. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 757-760.
Lebar. On hysterical edema. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 757-760.
L’école de rééducation professionelle et les œuvres d’assistance pour les mutilés à Bordeaux. J. de méd. de Bordeaux, 1915-1916, v. 45, pp. 139-141.
The professional rehabilitation school and support services for the handicapped in Bordeaux. J. de méd. de Bordeaux, 1915-1916, v. 45, pp. 139-141.
LeClerc et Tixier. Un cas de paralysie totale du plexus brachial droit compliquée de paraplégie spasmodique produite par le même-projectile. Lyon méd., 1916, v. 125, pp. 196-199.
LeClerc and Tixier. A case of total paralysis of the right brachial plexus complicated by spastic paraplegia caused by the same projectile. Lyon méd., 1916, v. 125, pp. 196-199.
Le Damany, P. La paralysie du facial supérieur dans l’hémiplégie cérébrale. Presse méd. Par., 1917, v. 25, pp. 1-3.
Le Damany, P. The paralysis of the upper facial nerve in cerebral hemiplegia. Med. Press. Paris, 1917, vol. 25, pp. 1-3.
Le Dantec. Rééducation et auto-rééducation des blessés de guerre. J. de méd. de Bordeaux, 1917, v. 88, pp. 219-224.
Le Dantec. Rehabilitation and self-rehabilitation of war injuries. J. de méd. de Bordeaux, 1917, v. 88, pp. 219-224.
Ledoux-Lebard, R., Chabaneix, Dessane. L’importance des variations du squelette dans le diagnostic radiologique des blessures de guerre. J. de radiol. et électrol., 1914-15, v. 1, pp. 689-693.
Ledoux-Lebard, R., Chabaneix, Dessane. The importance of skeletal variations in the radiological diagnosis of war injuries. J. of Radiology and Electrology, 1914-15, v. 1, pp. 689-693.
Lee, John R. A case of gunshot wound of the head with a piece of shrapnel in the brain; value of the use of an electric magnet and x-ray screen for removal. J. Roy. Army Med. Corps, London, 1916, v. 26, pp. 105-106.
Lee, John R. A case of a gunshot wound to the head with a piece of shrapnel in the brain; the importance of using an electric magnet and x-ray screen for removal. J. Roy. Army Med. Corps, London, 1916, v. 26, pp. 105-106.
Leeson, C. The war and juvenile delinquency. Pub. for Howard Ass. of Lond., by P. S. King and Son, Ltd., 1917. (1 s. net.)
Leeson, C. The war and juvenile delinquency. Published for the Howard Association of London by P. S. King and Son, Ltd., 1917. (1 shilling net.)
Le Fur, René. Abcès du cerveau (lobe temporal), consécutif à une plaie par éclat d’obus en avant de l’oreille. Paris Chirur., 1916, v. 8, pp. 276-278.
Le Fur, René. Brain abscess (temporal lobe), following a shell fragment wound in front of the ear. Paris Chirur., 1916, v. 8, pp. 276-278.
Legros. L’électrothérapie de guerre. Paris, 1916, A. Maloine et fils.
Legros. War Electrotherapy. Paris, 1916, A. Maloine et fils.
Legueu, F. Battlefield urology; urinary and vesical psychoses in the fighting line. Med. Press and Circ., Lond., 1915, n. s., v. 100, p. 11.
Legueu, F. Battlefield urology; urinary and bladder psychoses in the front lines. Med. Press and Circ., Lond., 1915, n. s., v. 100, p. 11.
Legueu, F. De l’incontinence d’urine et des psychoses vésicales chez les combattants. Bull. Acad. de Méd., Par., 1915, v. 73, pp. 314-315.
Legueu, F. On urinary incontinence and bladder psychoses in soldiers. Bull. Acad. de Méd., Par., 1915, v. 73, pp. 314-315.
Leitner, P. Wien. klin. Wchnschr., 1917, 30, 1327-28.
Leitner, P. Wien. klin. Wchnschr., 1917, 30, 1327-28.
Lelong, Marcel. Quelques formes de la fatigue à l’avant. Paris méd., 1917, No. 3, pp. 66-68.
Lelong, Marcel. Some Forms of Fatigue in the Frontline. Paris Med., 1917, No. 3, pp. 66-68.
Lemon, Felix. Functional cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-15 (Sect. Laryncol.), v. 8, p. 117.
Lemon, Felix. Functional cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-15 (Sect. Laryngol.), v. 8, p. 117.
Lenoir, R. Contribution à l’étude des phénomènes psychologiques et physiologiques observés pendant la narcose. Rev. neurol., 1914-15, v. 2211, p. 1310.
Lenoir, R. Contribution to the study of psychological and physiological phenomena observed during narcosis. Rev. neurol., 1914-15, v. 2211, p. 1310.
Lents, A. (The war and hysterical stigmata.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 152-155.
Lents, A. (The war and hysterical stigmata.) Psychiatr. Gaz., St. Petersburg, 1915, v. 2, pp. 152-155.
Lenz. La guerre et les stigmates hystériques. Gazette psychiatrique (russe), 1915.
Lenz. War and Hysterical Stigmas. Psychiatric Gazette (Russian), 1915.
Lépine, Jean. Troubles mentaux de guerre. Collection Horizon, Masson et Cie, Paris, 1918.
Lépine, Jean. Mental Health Issues from War. Horizon Collection, Masson & Co., Paris, 1918.
Lépine, Jean. Commotions nerveuses à la suite d’explosions. Rev. Paris méd. (Part. méd.), 1916, v. 21, p. 67.
Lépine, Jean. Nervous disturbances following explosions. Rev. Paris méd. (Part. méd.), 1916, v. 21, p. 67.
Lépine, J. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 473.
Lépine, J. Discussion on how to deal with skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 473.
Lépine, J. Centre de psychiatrie de la 14e région. (Lyon). Rev. neurol., Par., 1916, xxiii, 698-701.
Lépine, J. Center for Psychiatry of the 14e Region. (Lyon). Rev. neurol., Par., 1916, xxiii, 698-701.
Lépine, J. La commotion des centres nerveux par explosion. Bull. acad. de méd. de Par., 1916, v. 75, pp. 9-11.
Lépine, J. The impact of explosive blasts on the nervous system. Bull. acad. de méd. de Par., 1916, v. 75, pp. 9-11.
Lépine J. La commotion des centres nerveux par explosion. Lyon méd., 1916, v. 125, pp. 181-182.
Lépine J. The impact of explosions on the nervous system. Lyon méd., 1916, vol. 125, pp. 181-182.
Lépine, J. Réformes, incapacités, gratifications dans les psychoses. Ibid., 803-809.
Lépine, J. Reforms, disabilities, rewards in psychoses. Ibid., 803-809.
Lépine J. Troubles mentaux de guerre. Les solutions militaires. Presse méd., Par., 1917, v. 25, pp. 659-663.
Lépine J. Mental health issues from war. Military solutions. Medical Press, Paris, 1917, vol. 25, pp. 659-663.
Leplat, Georges. Note sur un cas de troubles oculaires produits à distance par une explosion. Arch. méd. Belges, Brux., 1917, v. 47, pp. 412-415.
Leplat, Georges. Note on a case of eye disorders caused from a distance by an explosion. Arch. méd. Belges, Brux., 1917, v. 47, pp. 412-415.
Leppmann. Psychiatrische und nervenärztliche Sachverständigentatigkeit im Krieg. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 209.
Leppmann. Psychiatric and neurological expert activities in the war. German medical weekly, Berlin and Leipzig, 1915, vol. 41, p. 209.
Lerda, G. Contributo alla conoscenza delle suppurazioni da benzina. Gior. di med. mil., Roma, 1916, lxiv, 586-590.
Lerda, G. Contribution to the understanding of gasoline suppurations. Journal of Military Medicine, Rome, 1916, lxiv, 586-590.
Lereboullet. Spasmes consécutifs à la paralysie faciale. Rev. gén. de clin. et de thérap., Par., 1917, v. 31, p. 294.
Lereboullet. Spasms resulting from facial paralysis. Gen. Rev. of Clin. and Therapy, Paris, 1917, vol. 31, p. 294.
Lereboullet, P. et Mouzon, J. Hallucinations de la vue et crises jacksoniennes dans un cas de lésion du cortex visuel. Paris méd., 1917, No. 27, pp. 19-23.
Lereboullet, P. and Mouzon, J. Visual hallucinations and Jacksonian seizures in a case of damage to the visual cortex. Paris méd., 1917, No. 27, pp. 19-23.
Leredu. Réponse du ministre de la guerre au sujet de l’envoi en convalescence des aliénés militaires guéris et fortunes en cas de refus par leur famille de les recevoir. Soc. de méd. Lég. de France, Bull. Par., 1916, v. 13, pp. 179-180.
Leredu. Response from the Minister of War regarding the sending of recovered military personnel to convalescence and their circumstances in case their families refuse to take them in. Soc. de méd. Lég. de France, Bull. Par., 1916, v. 13, pp. 179-180.
Léri, André. Commotions et Émotions de guerre. Collection Horizon, Masson et Cie, Paris, 1917.
Léri, André. Commotions and War Emotions. Horizon Collection, Masson et Cie, Paris, 1917.
Léri, André. Sur les pseudo-commotions ou contusions médullaires d’origine fonctionelle. Rev. neurol., Par., 1914-15, v. 222, pp. 433-436.
Léri, André. On pseudo-concussions or functional spinal contusions. Rev. neurol., Paris, 1914-15, v. 222, pp. 433-436.
Léri, A. L’électrisation directe des troncs nerveux au cours des interventions pour blessures des nerfs, ses données pratiques. Paris méd., 1915 (Part. Méd.), v. 17, pp. 134-138.
Léri, A. Direct electrification of nerve trunks during interventions for nerve injuries, its practical data. Paris méd., 1915 (Part. Méd.), v. 17, pp. 134-138.
Léri, A. Hémorragie de la couche optique par commotion pure. Hémiplégie avec hémianesthésie à type cérébral. Soc. méd. d’hôp., Par., 26 mai, 1916.
Léri, A. Hemorrhage of the optical layer from pure concussion. Hemiplegia with hemisensory loss of cerebral type. Med. Soc. of Hospitals, Paris, May 26, 1916.
Léri, A. Hémorragie de l’épicone médullaire par commotion (éclatement d’obus à proximité). Rev. neurol., Par., 1916, v. 23, pp. 133-135.
Léri, A. Spinal cord hemorrhage from concussion (nearby shell explosion). Neurol. Rev., Paris, 1916, vol. 23, pp. 133-135.
Léri, A. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 466-469.
Léri, A. Discussion on how to deal with skull injuries—by P. Marie. Neurological Review, Paris, 1916, vol. 29, pp. 466-469.
Léri, A. Sur les accidents nerveux determinés par la deflagration de fortes charges d’explosifs. Rev. neurol. Par., 1916, v. 29, pp. 586-587.
Léri, A. On nerve accidents caused by the detonation of large explosive charges. Rev. neurol. Par., 1916, v. 29, pp. 586-587.
Léri, A. Réformes, incapacités, gratifications, dans les névroses de guerre. Rev. neurol., Par., 1916, xxiii, pp. 763-766.
Léri, A. Reforms, disabilities, rewards, in the war neuroses. Rev. neurol., Paris, 1916, xxiii, pp. 763-766.
Léri, A. A propos de l’hystérie. Sur un cas d’hémianesthesie organique presque pure. Paris méd., 1916 (Part méd.), v. 19, pp. 531-534.
Léri, A. About Hysteria. Regarding a case of almost pure organic hemianesthesia. Paris méd., 1916 (Part méd.), v. 19, pp. 531-534.
Léri, A. Les commotions des centres nerveux par éclatement d’obus. Rev. gén. de. path. de guerre, 1916, No. 2, pp. 169-212.
Léri, A. The impacts on the nervous system from shell explosions. Gen. Rev. of War Pathology, 1916, No. 2, pp. 169-212.
Léri, A. Épilepsie jacksonienne par “vent d’obus” (hémorragie corticale probable). Presse méd., Par., 1916, v. 24, p. 96.
Léri, A. Jacksonian epilepsy due to "shell shock" (likely cortical hemorrhage). Medical Press, Paris, 1916, vol. 24, p. 96.
Léri, A. Traumatisme du crâne; hémiparésie droite, grosse hémiatrophie post-hémiplégique avec hémiatrophie linguale homolatérale; syndrôme protubérantiel probable. Rev. neurol., Par., 1917, v. 24, pp. 561-563.
Léri, A. Skull trauma; right hemiparesis, significant post-hemiplegic hemiphyrophy with ipsilateral tongue atrophy; probable pontine syndrome. Rev. neurol., Par., 1917, v. 24, pp. 561-563.
Léri, A. Procédé bi-photographique pour mesurer l’évolution progressive ou régressive des paralysies et pour étudier les mouvements des membres. Rev. neurol., Par., 1917, v. 24, pp. 563-564.
Léri, A. Bi-photographic method for measuring the gradual or regressive evolution of paralysis and studying limb movements. Rev. neurol., Par., 1917, v. 24, pp. 563-564.
Léri, A. Émotions et commotions de guerre. Collection Horizon, Masson et Cie, 1918.
Léri, A. Emotions and War Shock. Horizon Collection, Masson and Co., 1918.
Léri, A. and Dagnan-Bouvert. Soc. de Neurol. May 6, 1915. Rev. Neurol., July, 1915.
Léri, A. and Dagnan-Bouvert. Soc. de Neurol. May 6, 1915. Rev. Neurol., July, 1915.
Léri, Froment et Mahar. Atrophie musculaire et déflagration d’obus sans traumatisme apparent. Rev. neurol., 1914-15, v. 222, p. 754.
Léri, Froment and Mahar. Muscle atrophy and shell explosion without apparent trauma. Rev. neurol., 1914-15, v. 222, p. 754.
Léri, A. et Roger, Édouard. Sur la pathogénie de certains oedèmes soi-disant traumatiques. Rev. neurol., Par., 1914-15, v. 222, pp. 756-759.
Léri, A. and Roger, Édouard. On the Pathogenesis of Certain So-Called Traumatic Edemas. Neurology Review, Paris, 1914-15, vol. 222, pp. 756-759.
Léri, A. et Roger, É. Sur quelques variétés de contractures post-traumatiques et sur leur traitement. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 885-8941.
Léri, A. and Roger, É. On some types of post-traumatic contractions and their treatment. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 885-8941.
Léri, A. et Schaeffer, H. Hématobulbie par commotion; survie; syndrôme bulbaire complexe. Soc. méd. d’hôp., Par., 1916, 26 mai.
Léri, A. and Schaeffer, H. Hematobulbia from concussion; survival; complex bulbous syndrome. Med. Soc. Hosp., Paris, 1916, May 26.
Léri et Schaeffer. Hémorragies du nevraxe par commotion. Presse méd., Par., 1916, v. 24, p. 351.
Léri and Schaeffer. Hemorrhages of the nervous system due to concussion. Med Press, Paris, 1916, vol. 24, p. 351.
Léri, A. et Schaeffer. Un cas de lésion bulbo-médullaire par commotion due à un éclatement d’obus hématobulbie probable survie avec syndrôme bulbaire complexe. Rev. neurol., Par., 1917, v. 24, pp. 1-8.
Léri, A. and Schaeffer. A case of bulbomedullary injury from concussion due to probable hematobulbic shell explosion, with complex bulbar syndrome survival. Rev. neurol., Paris, 1917, v. 24, pp. 1-8.
Lériche, René. De la causalgia envisagée comme une névrite du sympathique et de son traitement par la dénudation et l’ablation des plexus nerveux péri-artériels. Soc. de Neurol., 6 janvier 1916.
Lériche, René. On causalgia viewed as a neuritis of the sympathetic and its treatment through denervation and removal of the peri-arterial nerve plexuses. Soc. de Neurol., January 6, 1916.
Lériche, R. Des lésions cérébrales et médullaires produites par l’explosion à faible distance des obus de gros calibre. Lyon chirurg., 1915, v. 12, pp. 343-350.
Lériche, R. Brain and spinal cord injuries caused by explosions at close range from large caliber shells. Lyon chirurg., 1915, v. 12, pp. 343-350.
Lériche, R. Des petites plaies du crâne par éclates d’obus et de bombes sans pénétration du projectile et des lésions nerveuses que les accompagnent. Lyon chirurg., 1915, v. 12, pp. 293-342.
Lériche, R. About small head wounds from shrapnel and bombs without projectile penetration and the accompanying nerve damage. Lyon chirurg., 1915, v. 12, pp. 293-342.
Lériche, R. De la sympathectomie péri-artérielle et de ses résultats. Presse méd., Par., 1917, v. 25, pp. 513-515.
Lériche, R. On peri-arterial sympathectomy and its outcomes. Medical Press, Paris, 1917, vol. 25, pp. 513-515.
Lermoyez, Marcel. La surdité de guerre. Presse méd., Par., 1915, v. 23, pp. 57-59.
Lermoyez, Marcel. The Deafness of War. Medical Press, Paris, 1915, vol. 23, pp. 57-59.
Leroy. Sur les accidents nerveux determinés par la déflagration de fortes charges d’explosifs. Rev. neurol. Par., 1916, v. 29, pp. 595-597.
Leroy. On nervous accidents caused by the blast of large explosive charges. Rev. neurol. Par., 1916, v. 29, pp. 595-597.
Lesieur et Peuret, A. L’insomnie nerveuse dite essentielle et son traitement médicamenteux. Caducée, Par., 1917, v. 17, p. 96; Bull. méd., Par., 1917, v. 31, pp. 12-13.
Lesieur and Peuret, A. Essential nervous insomnia and its drug treatment. Caducée, Paris, 1917, vol. 17, p. 96; Bull. méd., Paris, 1917, vol. 31, pp. 12-13.
Lesions of peripheral nerves resulting from war injuries: Pathology and treatment. Brit. Med. Jour., 1918, i, 379, 408.
Injuries to peripheral nerves caused by war wounds: Pathology and treatment. Brit. Med. Jour., 1918, i, 379, 408.
Lévy, L. Note sur les renseignements cytologiques donnés par la ponction lombaire au cours de l’évolution des blessures du crâne. Lyon chirurg., 1916, v. 13, pp. 428-433.
Lévy, L. Note on the cytological information provided by lumbar puncture during the progression of skull injuries. Lyon surgery, 1916, v. 13, pp. 428-433.
Lévy, R. Ueber die Resultate der Kaufmann’schen Behandlung. Münch. med. Wchnschr., 1917, v. 64, No. 6.
Lévy, R. On the results of Kaufmann's treatment. Münch. med. Wchnschr., 1917, v. 64, No. 6.
Lévy-Valensi, J. Notes sur quelques faits cliniques. Presse méd., 1915, v. 23, pp. 179-181.
Lévy-Valensi, J. Notes on some clinical facts. Med Press, 1915, vol. 23, pp. 179-181.
Levy-Bing et Gerbay. Epilepsia syphilitica. Ann. d. mal. vén., Par., 1917, 12, 265-8.
Levy-Bing and Gerbay. Syphilitic Epilepsy. Ann. of Venereal Diseases, Paris, 1917, 12, 265-8.
Lewandowsky, M. Die Kriegsverletzungen des Nervensystems. Berl. klin. Wchnschr., 1914, v. 51, pp. 1929-1934.
Lewandowsky, M. The War Injuries of the Nervous System. Berl. klin. Wchnschr., 1914, v. 51, pp. 1929-1934.
Lewandowsky, M. Ueber Kriegsverletzungen des Nervensystems. 1. Gehirnschüsse. 2. Rückenmarksverletzungen. 4. Hysterie. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 47-48.
Lewandowsky, M. On War Injuries of the Nervous System. 1. Brain Injuries. 2. Spinal Cord Injuries. 4. Hysteria. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 47-48.
Lewandowsky, M. Kriegsverletzungen des Nervensystems. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 29.
Lewandowsky, M. War Injuries of the Nervous System. German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, pp. 29.
Lewandowsky, M. Erfahrungen über die Behandlung nervenverletzter und nervenkranker Soldaten. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 1565-1567.
Lewandowsky, M. Experiences in Treating Soldiers with Nerve Injuries and Nerve Disorders. German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, pp. 1565-1567.
Lewandowsky, M. Familiäre Kältelähmung. Berl. klin. Wchnschr., 1916, No. 5, pp. 120.
Lewandowsky, M. Familial Cold Paralysis. Berl. klin. Wchnschr., 1916, No. 5, pp. 120.
Lewandowsky, M. Ein Fall von Rindenepilepsie und Rindenschwäche. Aerztl. Sachvert. Ztg., Berl., 1916, No. 3. Rev. Berl. klin. Wchnschr., 1916, No. 12, p. 316.
Lewandowsky, M. A case of cortical epilepsy and cortical weakness. Medical Expert Journal, Berlin, 1916, No. 3. Review of Berlin Clinical Weekly, 1916, No. 12, p. 316.
Lewis, E. R. Influence of altitude on the hearing and the motion-sensing apparatus of the ear. Jour. A. M. A., 1918, lxxi, 1398.
Lewis, E. R. Impact of altitude on hearing and the motion-sensing system of the ear. Jour. A. M. A., 1918, lxxi, 1398.
Lewis, Thomas. Observations upon Prognosis: “Irritable heart of soldiers.” Lancet, Lond., 1918, i, pp. 181-183.
Lewis, Thomas. Observations on Prognosis: “Irritable Heart of Soldiers.” Lancet, London, 1918, i, pp. 181-183.
Lewis, Thomas. Tolerance of physical exertion, as shown by soldiers suffering from so-called “irritable heart.” Brit. Med. Jour., 1918, i, 363.
Lewis, Thomas. Tolerance of physical exertion, as demonstrated by soldiers experiencing what is known as “irritable heart.” Brit. Med. Jour., 1918, i, 363.
Lewitus. Ein seltener Simulationsfall. Wien. med. Wchnschr., 1915, No. 24, p. 925.
Lewitus. A rare simulation case. Wien. med. Wchnschr., 1915, No. 24, p. 925.
Lhermitte, J. Hémiplégie secondaire aux blessures du crâne. Rev. neurol., Par., 1916, v. 24, pp. 807-813.
Lhermitte, J. Hemiplegia secondary to head injuries. Neurology Review, Paris, 1916, vol. 24, pp. 807-813.
Liébault, G. Les troubles de la parole et les commotions de guerre. Rev. gén. de path. de guerre, 1916, No. 3, pp. 245-269.
Liébault, G. Speech disorders and war injuries. Gen. Rev. of war pathology, 1916, No. 3, pp. 245-269.
Liebers, M. Zur Behandlung der Zitterneurosen nach Granatschock. Neurol. Centralbl., Leipz., 1916, v. 35, No. 21.
Liebers, M. On the Treatment of Tremor Neurosis following Grenade Shock. Neurol. Centralbl., Leipzig, 1916, vol. 35, No. 21.
Liebl. Ein charakteristisches künstlich erzeugtes Geschwür. Wien. klin. Wchnschr., 1916, xxix, 1305.
Liebl. A distinctive artificially created ulcer. Vienna. clinical weekly, 1916, xxix, 1305.
Liepmann, H. Psychiatrisches aus dem Russ.-Jap. Feldzug. Deutsche med. Wchnschr., Berl. u. Leipz., 1914, v. 40, pp. 1823.
Liepmann, H. Psychiatry from the Russo-Japanese Campaign. German Medical Weekly, Berlin and Leipzig, 1914, vol. 40, pp. 1823.
Liepmann, H. Zur Fragestellung in dem Streit über die traumatische Neurose. Neurol. Centralbl., Leipz., 1916, v. 35, No. 6.
Liepmann, H. On the question raised in the debate about traumatic neurosis. Neurol. Centralbl., Leipz., 1916, v. 35, No. 6.
Loeper, M. et Carlotti, J. Pustule maligné des paupières a guérison rapide. Progrès méd., Par., 1916, No. 3, pp. 17-19.
Loeper, M. and Carlotti, J. Rapid healing of malignant pustule on the eyelids. Progrès méd., Paris, 1916, No. 3, pp. 17-19.
Loeper, M. and Verpy, G. Les troubles vasculaires et hématiqués de la commotion. Compt. rend. Soc. de biol., Par., 1916, lxxix, pp. 831-833.
Loeper, M. and Verpy, G. Vascular and hematological issues from concussion. Compt. rend. Soc. de biol., Paris, 1916, lxxix, pp. 831-833.
Loeper, M. et Verpy, G. La répercussion glandulaire et humorale des commotions. Progrès méd., Par., 1916, v. 21, pp. 202-205.
Loeper, M. and Verpy, G. The glandular and humoral effects of concussions. Medical Progress, Paris, 1916, vol. 21, pp. 202-205.
Logre, M. Début de paralysie générale avec tabes par des crises de poltronnerie avec incontinence d’urine. Presse méd., Par., 1917, v. 25, p. 395.
Logre, M. Beginning of general paralysis with tabes characterized by panic attacks and urinary incontinence. Medical Press, Paris, 1917, vol. 25, p. 395.
Lollet. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 470.
Lollet. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, v. 29, p. 470.
Lombard et Baldenweck. Traitement de quelques cas de mutité hystérotraumatique par le procédé de la suppression de contrôle auditif de la voix (méthode de Lombard). Presse méd., Par., 1915, v. 23, p. 338.
Lombard and Baldenweck. Treatment of a few cases of hysterical mutism through the method of suppressing auditory control of the voice (Lombard's method). Méd. Press, Paris, 1915, vol. 23, p. 338.
London War Hospitals. Boston M. and S. J., 1917, i, pp. 222-223.
London War Hospitals. Boston M. and S. J., 1917, i, pp. 222-223.
Long, E. Radiculite lombo-sacrée (sciatique radiculaire) d’origine syphilitique. Rev. neurol. Par., 1916, v. 29, pp. 298-300.
Long, E. Lumbosacral radiculitis (radicular sciatica) of syphilitic origin. Rev. neurol. Par., 1916, v. 29, pp. 298-300.
Loreta, U. Per l’applicazione di esami psicologici nell’ esercito. Policlin., Roma, 1915, c. 17, sez. prat., pp. 1298-1300.
Loreta, U. For the application of psychological tests in the army. Policlin., Rome, 1915, p. 17, practical section, pp. 1298-1300.
Lortat-Jacob. Le syndrôme des éboulés. Rev. neurol. Par., 1914-15, v. 222, pp. 1173.
Lortat-Jacob. The syndrome of collapses. Rev. neurol. Par., 1914-15, v. 222, pp. 1173.
Lortat-Jacob. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 470.
Lortat-Jacob. Discussion on how to handle head injuries—by P. Marie. Neurological Review, Paris, 1916, vol. 29, p. 470.
Lortat-Jacob. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol. Par., 1916, v. 29, pp. 590-591.
Lortat-Jacob. On nerve accidents caused by the explosion of large amounts of explosives. Neurology Review, Paris, 1916, v. 29, pp. 590-591.
Lortat-Jacob et Buvat, J. B. Sur un procédé de guérison des sourds-muets par commotion. Bull. et mém. de soc. méd. d’hôp. de Par., 1916, pp. 169-176; Rev. Paris méd., 1916 (Part. méd.), v. 19, p. 226.
Lortat-Jacob and Buvat, J. B. On a method of healing the deaf-mute through concussion. Bull. et mém. de soc. méd. d’hôp. de Par., 1916, pp. 169-176; Rev. Paris méd., 1916 (Part. méd.), v. 19, p. 226.
Lortat-Jacob et Sézary. Synesthésialgie et blessure du sciatique. Rev. neurol., 1914-15, v. 222, pp. 1277-1278.
Lortat-Jacob and Sézary. Synesthetic pain and sciatic injury. Neurology Review, 1914-15, v. 222, pp. 1277-1278.
Lortat-Jacob et Sézary. Maladie de Thomsen. Rev. neurol., Par., 1916, v. 23, pp. 15-18.
Lortat-Jacob and Sézary. Thomsen's Disease. Neurology Review, Paris, 1916, vol. 23, pp. 15-18.
Lortat-Jacob et Oppenheim, R. Hémiplegie post-scarlatineuse. Progrès méd., Par., 1916, pp. 213-215.
Lortat-Jacob and Oppenheim, R. Post-scarlet fever hemiplegia. Medical Progress, Paris, 1916, pp. 213-215.
Lortat, Jacob et Oppenheim, R. et Tournay, A. Topographie des modifications de la sensibilité au cours des troubles physiopathiques; constitution d’un syndrôme radiculo-sympathique réflexe. Progrès méd., Par., 1917, No. 10, pp. 77-81.
Lortat, Jacob, Oppenheim, R., and Tournay, A. Topography of changes in sensitivity during pathophysiological disorders; development of a reflex sympathetic radiculopathy syndrome. Progrès méd., Paris, 1917, No. 10, pp. 77-81.
Love, K. Hearing in the Army. J. Roy. Army Med. Corps, Lond., 1915, v. 27, pp. 652-654.
Love, K. Hearing in the Army. J. Roy. Army Med. Corps, Lond., 1915, v. 27, pp. 652-654.
Löwenfeld. Über den französischen Nationalcharakter und seine Auswüchse im gegenwärtigen Kriege (Psychopathia gallica). Allgem. Zeitschr. f. Psychiat., Wiesbaden, 1914.
Löwenfeld. On the French National Character and its Growths in the Current War (Psychopathia Gallica). General Journal of Psychiatry, Wiesbaden, 1914.
Löwenstein, Kurt. Zerebellare Symptomenkomplexe nach Kriegsverletzungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 626-637.
Löwenstein, Kurt. Cerebellar symptom complexes after war injuries. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 626-637.
Löwenstein, Sally. Zur traumatischen Entstehung chronischer Rückenmarksleiden. Neurol. Centralbl., 37, Nr. 16, 1918.
Löwenstein, Sally. On the traumatic origins of chronic spinal cord disorders. Neurol. Centralbl., 37, No. 16, 1918.
Löwy, Max. Neurologische und psychiatrische Mitteilungen aus dem Kriege. Monatschr. f. Psychiat. und Neurol., Berl., 1915, v. 37, pp. 380-388.
Löwy, Max. Neurological and psychiatric communications from the war. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, vol. 37, pp. 380-388.
Löwy, Julius. Über die Beeinflussung von Erkrankungen des Nervensystem durch den Apparat von Bergonié. Ztschr. f. Phys. u. Diätet. Therap., Leipz., 1915, No. 9, pp. 272-276.
Löwy, Julius. On the Influence of Nervous System Diseases from the Bergonié Apparatus. Journal of Physics and Diet Therapy, Leipzig, 1915, No. 9, pp. 272-276.
Lumière, Auguste et Astier. Cerebral troubles in tetanus. Monde Méd., Par., 1917, v. 27, pp. 101-105.
Lumière, Auguste and Astier. Mental issues in tetanus. Monde Méd., Paris, 1917, vol. 27, pp. 101-105.
Lumsden, T. The psychology of malingering and functional neuroses in peace and war. Lancet, Lond., 1916, ii, pp. 860-862. Rev. Boston M. and S. J., 1916, ii, p. 8.
Lumsden, T. The psychology of faking illness and functional neuroses in peace and war. Lancet, Lond., 1916, ii, pp. 860-862. Rev. Boston M. and S. J., 1916, ii, p. 8.
Lumsden, T. Treatment of war neuroses. Lancet, Lond., 1917, ii, p. 804.
Lumsden, T. Treatment of war neuroses. Lancet, London, 1917, 2, p. 804.
Lumsden, T. Shell Shock. (A letter.) Lancet, Lond., 1917, i, p. 34.
Lumsden, T. Shell Shock. (A letter.) Lancet, London, 1917, 1, p. 34.
Lumsden’s scheme for treatment of nerve-shattered soldiers. Hospital, Lond., 1917, v. 61, pp. 487-488.
Lumsden’s treatment plan for soldiers with nerve damage. Hospital, Lond., 1917, v. 61, pp. 487-488.
Lust, F. Kriegsneurosen und Kriegsgefangene. Münch, med. Wchnschr., 1916, v. 63, p. 1829.
Lust, F. War neuroses and prisoners of war. Münch, med. Wchnschr., 1916, v. 63, p. 1829.
Lyonnet. Un cas de paraplégie d’origine cérébrale. Lyon méd., 1915, v. 124, pp. 362-363.
Lyonnet. A case of paraplegia of cerebral origin. Lyon med., 1915, v. 124, pp. 362-363.
Lyle, H. H. M. Physiological treatment of bullet and shell wounds of the peripheral nerve trunks. S. G. O., 1916, xxii, 127.
Lyle, H. H. M. Physiological treatment of bullet and shell wounds of the peripheral nerve trunks. S. G. O., 1916, xxii, 127.
Lyristritski, V. V. (Psychical symptoms, difficult to simulate). Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 121-124.
Lyristritski, V. V. (Psychological symptoms that are hard to fake). Psychiatr. Gaz., St. Petersburg, 1915, v. 2, pp. 121-124.
MacAuliffe, Léon. Evolution de l’état commotionnel chez les blessés du crâne trépanés. Paris méd., 1917, No. 47, pp. 421-424.
MacAuliffe, Léon. Evolution of the state of concussion in patients with trepanned skulls. Paris méd., 1917, No. 47, pp. 421-424.
MacCurdy, John T. The Psychology of War. Wm. Heinemann, 1917.
MacCurdy, John T. The Psychology of War. Wm. Heinemann, 1917.
MacCurdy, John T. War Neuroses. Cambridge Univ. Press, 1918.
MacCurdy, John T. War Neuroses. Cambridge University Press, 1918.
MacCurdy, John T. War neuroses. Psychiat. Bull., Utica, 1917, v. 2, No. 3, pp. 243-254.
MacCurdy, John T. War neuroses. Psychiat. Bull., Utica, 1917, v. 2, No. 3, pp. 243-254.
Macdonald, W. M. Contractions of the hand after wounds of the upper limb. Brit. M. J., Lond., 1916, ii, pp. 209-212.
Macdonald, W. M. Hand contractions after injuries to the upper limb. Brit. M. J., Lond., 1916, ii, pp. 209-212.
MacDonald, W. M. Tinel’s sign in peripheral nerve lesions. Brit. Med. Jour., 1918, ii, 6.
MacDonald, W. M. Tinel's sign in peripheral nerve injuries. Brit. Med. Jour., 1918, ii, 6.
Mackenzie, W. C. Military orthopaedic hospitals. Brit. M. J., Lond., 1917, v. 1, pp. 669-678.
Mackenzie, W. C. Military orthopedic hospitals. Brit. M. J., Lond., 1917, v. 1, pp. 669-678.
MacKenzie, Kenneth A. J. Repair of large gaps in peripheral nerves by neuroplasty. Surg. Gynecol. and Obstet., 1918, xxvii, 355.
MacKenzie, Kenneth A. J. Fixing large gaps in peripheral nerves through neuroplasty. Surg. Gynecol. and Obstet., 1918, xxvii, 355.
MacLeod, Kenneth. Dreaming. Med. Press and Circ., Lond., 1916, v. 102, pp. 98-100.
MacLeod, Kenneth. Dreaming. Med. Press and Circ., London, 1916, vol. 102, pp. 98-100.
MacMahon, Cortlandt. Shell shock, stammering and other affections of voice and speech. J. Roy. Army Med. Corps, Lond., 1917, v. 39, pp. 192-201.
MacMahon, Cortlandt. Shell shock, stuttering, and other voice and speech disorders. J. Roy. Army Med. Corps, Lond., 1917, v. 39, pp. 192-201.
Madelung. Kriegsärztliche Erfahrungen im England und Frankreich. Münch. med. Wchnschr., v. 621, pp. 283-284.
Madelung. Experiences as a wartime doctor in England and France. Münch. med. Wchnschr., v. 621, pp. 283-284.
v. Maiendorf. Über Kriegsneurosen. Wien. klin. Wchnschr., 1915, v. 381, pp. 79-80.
v. Maiendorf. On War Neuroses. Wien. klin. Wchnschr., 1915, v. 381, pp. 79-80.
Mairet, A. et Durante, G. Contribution à l’étude expérimentale du syndrôme commotionnel. Rev. neurol., Par., 1917, v. 24, pp. 456-466.
Mairet, A. et Durante, G. Contribution to the experimental study of concussion syndrome. Rev. neurol., Paris, 1917, v. 24, pp. 456-466.
Mairet, A. et Durante, G. Étude expérimentale du syndrôme commotionnel. Presse méd., Par., 1917, v. 25, p. 478.
Mairet, A. et Durante, G. Experimental study of concussion syndrome. Méd. Press, Paris, 1917, v. 25, p. 478.
Mairet et Piéron. Les troubles de mémoire d’origine commotionnelle. J. de psychol. norm, et path., Par., 1915, v. No. 2, pp. 300-328.
Mairet and Piéron. Memory disorders resulting from concussion. J. of norm. and path. psychology, Paris, 1915, vol. No. 2, pp. 300-328.
Mairet et Piéron. Accès épileptiques determinés par une irritation nerveuse périphérique. Rev. Paris méd., 1916 (Part méd.), v. 19, p. 178.
Mairet and Piéron. Epileptic seizures triggered by peripheral nerve irritation. Rev. Paris méd., 1916 (Med. Part), v. 19, p. 178.
Mairet et Piéron. De la differenciation des symptômes “commotionnels” et des symptômes “atypiques” dans les traumatismes cranio-cérébraux. Montpel. méd., 1916, v. 39, p. 174.
Mairet and Piéron. On the differentiation between “concussive” symptoms and “atypical” symptoms in cranio-cerebral injuries. Montpel. méd., 1916, v. 39, p. 174.
Mairet et Piéron. De quelques problèmes posés par la neuropsychiatrie de guerre au point de vue des réformes. Montpel. méd., 1916, v. 39, pp. 387-402.
Mairet and Piéron. On some issues raised by the neuropsychiatry of war regarding reforms. Montpel. méd., 1916, v. 39, pp. 387-402.
Mairet, A. et Piéron, H. Syndrôme épileptique par irritation nerveuse périphérique ou “Epilepsie de Brown-Séquard.” Bull. acad. de méd., Par., 1916, v. 75, pp. 80-90.
Mairet, A. and Piéron, H. Epileptic syndrome from peripheral nerve irritation or "Brown-Séquard Epilepsy." Bulletin of the Academy of Medicine, Paris, 1916, vol. 75, pp. 80-90.
Mairet, A. et Piéron, H. De quelques problèmes posés par la neuropsychiatrie de guerre au point de vue des réformes. Paralysies générales, crises d’épilepsie apparues ou aggravées, accès de somnambulisme, accidents après vaccination antityphoidique. Rev. neurol., Par., 1917, v. 24, pp. 89-98.
Mairet, A. and Piéron, H. On some issues raised by wartime neuropsychiatry regarding reforms. General paralysis, epilepsy crises that emerged or worsened, episodes of sleepwalking, and accidents following anti-typhoid vaccination. Rev. neurol., Paris, 1917, vol. 24, pp. 89-98.
Mairet et Piéron. Le syndrôme émotionnel. Sa différenciation du syndrôme commotionnel. Rev. neurol., Par., 1917, v. 24, pp. 474-475.
Mairet and Piéron. The emotional syndrome. Its differentiation from the concussion syndrome. Rev. neurol., Paris, 1917, v. 24, pp. 474-475.
Mairet, A. and Piéron, H. Le syndrôme commotionnel. Ibid., p. 345.
Mairet, A. and Piéron, H. The concussion syndrome. Ibid., p. 345.
Mairet, A. et Piéron, H. Le syndrôme émotionnel; sa différenciation du syndrôme commotionnel. Montpel. méd., 1917, v. 39, pp. 581-599.
Mairet, A. and Piéron, H. The emotional syndrome; its differentiation from the concussion syndrome. Montpel. méd., 1917, vol. 39, pp. 581-599.
Mairet, A. et Piéron, H. Le syndrôme emotionnel: sa différenciation du syndrôme commotionnel. Ann. méd.-psychol., 1917, v. 73, pp. 183-206.
Mairet, A. and Piéron, H. The emotional syndrome: its differentiation from the concussion syndrome. Ann. méd.-psychol., 1917, v. 73, pp. 183-206.
Mairet, A. et Piéron, H. et Mme. Bouzansky. De l’existence d’un “syndrôme commotionnel” dans les traumatismes de guerre. Bull. de acad. de méd., Par., 1915, v. 73, pp. 654-661.
Mairet, A. and Piéron, H. and Mrs. Bouzansky. On the existence of a “concussion syndrome” in war-related injuries. Bull. de acad. de méd., Paris, 1915, v. 73, pp. 654-661.
Mairet, Piéron et Bouzansky. Des variations du “syndrôme commotionnel,” suivant la nature des traumatismes, et de son unité. Bull. de l’acad. de méd., Par., 1915, v. 73, pp. 690-700.
Mairet, Piéron, and Bouzansky. Variations of the "concussion syndrome," depending on the nature of the trauma, and its unity. Bull. de l’acad. de méd., Par., 1915, v. 73, pp. 690-700.
Mairet, Piéron et Bouzansky. Le “syndrome commotionnel” au point de vue du mécanisme pathogénique et de l’évolution. Bull. de acad. de méd., Par., 1915. v. 73, pp. 710-716.
Mairet, Piéron, and Bouzansky. The “concussion syndrome” in terms of pathogenic mechanisms and progression. Bull. de acad. de méd., Par., 1915. v. 73, pp. 710-716.
Mahomet. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10, (sect. Balneol.), p. 42.
Mahomet. Treatment through physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10, (sect. Balneol.), p. 42.
Maitland, T. J. Accumulated fatigue in warfare. (2nd int. rep., Brit. Ass. Comm.) Lancet, Lond., 1916, ii, pp. 955-956.
Maitland, T. J. Accumulated fatigue in warfare. (2nd int. rep., Brit. Ass. Comm.) Lancet, Lond., 1916, ii, pp. 955-956.
Malingering in the French Army. Brit. M. J., Lond., 1916, i, p. 64.
Malingering in the French Army. Brit. M. J., Lond., 1916, i, p. 64.
Malingering. Brit. M. J., Lond., 1917, ii, p. 117.
Malingering. Brit. M. J., Lond., 1917, ii, p. 117.
Malingering in the army. Monde méd., Paris, 1916. Eng. ed., xxvi, p. 147.
Malingering in the army. Medical World, Paris, 1916. English edition, xxvi, p. 147.
Mallet, R. À propos de quelques psychopathes. Presse méd., Par., 1915, v. 23, p. 390.
Mallet, R. About Some Psychopaths. Medical Press, Paris, 1915, vol. 23, p. 390.
Mallet, R. Troubles psychiques et hallucinations chez le combattant. Progrès méd., Par., 1916, No. 3, p. 16.
Mallet, R. Mental issues and hallucinations in soldiers. Medical Advances, Paris, 1916, No. 3, p. 16.
Mallet, R. Troubles psychiques et hallucinations chez le combattant. Rev. Paris méd., 1916 (Part, méd.), v. 19, p. 96.
Mallet, R. Psychological issues and hallucinations in soldiers. Rev. Paris méd., 1916 (Part, méd.), v. 19, p. 96.
Mallet, R. Troubles d’origine émotive chez le combattant. Presse méd., Par., 1916, v. 24, p. 95.
Mallet, R. Emotional Issues in Combatants. Medical Press, Paris, 1916, v. 24, p. 95.
Mallet, R. La confusion mentale chez le combattant. Presse méd., Par., 1916, v. 24, pp. 294-295.
Mallet, R. Mental Confusion in the Fighter. Medical Press, Paris, 1916, v. 24, pp. 294-295.
Mallet, R. Fugues des dégénérés. Presse méd., Par., v. 24, 1916, p. 493.
Mallet, R. Fugues of the Degenerates. Medical Press, Paris, vol. 24, 1916, p. 493.
Mallet, R. Discussion de Vincent. Rev. neurol. Par., Nos. 4-5, p. 597.
Mallet, R. Discussion of Vincent. Rev. neurol. Par., Nos. 4-5, p. 597.
Mallet, R. Fugues et délires aigus. Rev. neurol., 1917, v. 24, p. 486.
Mallet, R. Fugues and acute delusions. Neurology Review, 1917, vol. 24, p. 486.
Mallet, R. États du fatigue. Presse méd., Par., 1917, v. 25, p. 325.
Mallet, R. States of Fatigue. Medical Press, Paris, 1917, vol. 25, p. 325.
Mallet, R. États confusionnels et anxieux chez le combattant. Ann. méd. psychol., Par., 1917, v. 73, pp. 27-35.
Mallet, R. Confused and anxious states in soldiers. Ann. méd. psychol., Paris, 1917, v. 73, pp. 27-35.
Mallet, R. Fugue et délire. Contribution à l’étude des troubles psychiques de la guerre. Ann. méd. psychol., Par., 1917, v. 73, pp. 330-343.
Mallet, R. Fugue and Delirium. A Contribution to the Study of War-Related Mental Disorders. Ann. méd. psychol., Par., 1917, v. 73, pp. 330-343.
Mally and Corpechot. Monomyoplégies traumatiques; étude sur un groupe de lésions du système nerveux périphérique causées par les projectiles modernes. Rev. de Chir., 1917, lii, 281.
Mally and Corpechot. Traumatic monoplegies; study on a group of peripheral nervous system injuries caused by modern projectiles. Rev. de Chir., 1917, lii, 281.
Mann, G. Die traumatischen Neurosen, ihre Entstehungsweise und klinischen Formen bei Kriegsverletzten. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, p. 1563.
Mann, G. The traumatic neuroses, their development and clinical forms in war casualties. German Medical Weekly, Leipzig and Berlin, 1916, vol. 42, p. 1563.
Mann, G. Neue Gesichtspunkte und Methoden zur Behandlung der Kriegsneurosen. Med. Klin., Berl., 1916, v. 12, p. 1270.
Mann, G. New Perspectives and Methods for Treating War Neuroses. Med. Klin., Berl., 1916, v. 12, p. 1270.
Mann, L. Über Polyneuritis als Begleiterscheinung nervöser Erschöpfungszustände im Kriege. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 150-152.
Mann, L. On Polyneuritis as an Accompanying Symptom of Nervous Exhaustion States in War. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 150-152.
Mann, L. Über Granatexplosionsstörungen. Med. Klin., Berl. u. Wien., 1915, v. 11, pp. 963-964.
Mann, L. On Garnet Explosion Disturbances. Med. Klin., Berlin and Vienna, 1915, v. 11, pp. 963-964.
Mann, L. Neue Methoden und Gesichtspunkte zur Behandlung der Kriegsneurosen. Berl. klin. Wchnschr., 1916, No. 50, pp. 1333-1338.
Mann, L. New Methods and Perspectives for Treating War Neuroses. Berl. klin. Wchnschr., 1916, No. 50, pp. 1333-1338.
Mann, L. Die traumatischen Neurosen, ihre klinischen Formen und ihr Entstehungsmodus bei Kriegsverletzungen. Berl. klin. Wchnschr., 1916, v. 53, No. 37, and No. 38.
Mann, L. The traumatic neuroses, their clinical forms and how they arise from war injuries. Berl. klin. Wchnschr., 1916, v. 53, No. 37, and No. 38.
Mann, L. Zur Frage der traumatischen Neurosen. Wien. klin. Wchnschr., 1916, xxix, 1651.
Mann, L. On the Question of Traumatic Neuroses. Wien. klin. Wchnschr., 1916, xxix, 1651.
Mann, Lillienstein, etc. Discussion; Neurosen nach Kriegsverletzungen. Berl. klin. therap. Wchnschr., Wien u. Berl., 1916, v. 49-50, pp. 486-496.
Mann, Lillienstein, etc. Discussion; Neurological disorders after war injuries. Berl. klin. therap. Wchnschr., Wien u. Berl., 1916, v. 49-50, pp. 486-496.
Mannell, J. D. Reëducation in walking. Hospital, Lon., 1917, lxi, 383.
Mannell, J. D. Retraining in walking. Hospital, Lon., 1917, lxi, 383.
Marage. Les sourds-muets de guerre. Académie des Sciences, 25 avril 1915.
Marriage. The deaf-mute soldiers. Academy of Sciences, April 25, 1915.
Marage. Rééducation auditive des surdités consécutives à des blessures de guerre. Vigot frères, 1915.
Marriage. Auditory rehabilitation for hearing loss resulting from war injuries. Vigot brothers, 1915.
Marage. Contribution à l’étude des hypo-acousies consécutives à des blessures de guerre. Compt. rend. acad. d. sc., Par., 1915, v. 161, pp. 148-150.
Marage. Contribution to the study of hearing loss due to war injuries. Compt. rend. acad. d. sc., Paris, 1915, v. 161, pp. 148-150.
Marage. Traitement des hypo-acousies consécutives à des blessures de guerre. Compt. rend. acad. d. sc., Par., 1915, v. 161, pp. 319-322.
Marriage. Treatment of hearing loss resulting from war injuries. Compt. rend. acad. d. sc., Paris, 1915, vol. 161, pp. 319-322.
Marage. Les sourds-mutités vraies et simulées consécutives à des blessures de guerre. Compt. rend. acad. d. sc., Par., 1916, v. 162, pp. 651-654.
Marriage. The deaf-mutes, both genuine and feigned, resulting from war injuries. Compt. rend. acad. d. sc., Paris, 1916, v. 162, pp. 651-654.
Marage, M. Classement des soldats sourds d’àprès leur degré d’audition. Compt. rend. acad. d. sc., Par., 1916, v. 162, pp. 801-804.
Marage, M. Classification of deaf soldiers based on their hearing ability. Compt. rend. acad. d. sc., Paris, 1916, vol. 162, pp. 801-804.
Marage. Douze mois de rééducation auditive dans l’armée; résultats de 250 cas. Bull. acad. de méd., Par., 1916, v. 76, pp. 318-320.
Marage. Twelve months of auditory rehabilitation in the military; results from 250 cases. Bull. acad. de méd., Par., 1916, v. 76, pp. 318-320.
Marage. La rééducation des surdités consécutives à des blessures de guerre. Bull. gén. psychol., Par., 1916, v. 15, pp. 5-21.
Marriage. The rehabilitation of hearing loss resulting from war injuries. Bull. gén. psychol., Paris, 1916, v. 15, pp. 5-21.
Marage. Traitement de la surdité par commotion. Paris méd., 1916, (Part. méd.), v. 21, p. 419.
Marriage. Treatment of deafness through shock. Paris méd., 1916, (Part. méd.), v. 21, p. 419.
Marburg. Zur Frage der Beurteilung traumatischer Neurosen im Kriege. Wien. klin. Wchnschr., 1916, v. 29, pp. 281-282.
Marburg. On the Question of Assessing Traumatic Neuroses in War. Vienna. Klin. Wchnschr., 1916, v. 29, pp. 281-282.
Marburg, O. Nervöse Folgezustände von kriegerischen Ereignissen. Militärarzt, Wien, 1914, xlviii, pp. 402-404.
Marburg, O. Nervous aftereffects of war events. Military Doctor, Vienna, 1914, xlviii, pp. 402-404.
Marchal, R. Les lésions des nerfs périphériques. Arch. méd. belges., Paris, 1917, 70, 44.
Marchal, R. Peripheral Nerve Injuries. Belgian Medical Archives, Paris, 1917, 70, 44.
Marchand, L. Des troubles mentaux dans les blessures pénétrantes du crâne. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 192-208.
Marchand, L. Mental disorders in penetrating skull injuries. Ann. méd. psychol., Par., 1916-17, v. 7, pp. 192-208.
Marchand, L. Des paraplégies hystériques consécutives aux polyneurites diphtériques. Bull. et mém. Soc. méd. hôp. de Paris, 1917, 3 ser. 41, pp. 248-53.
Marchand, L. On hysterical paraplegia following diphtheritic polyneuritis. Bull. et mém. Soc. méd. hôp. de Paris, 1917, 3 ser. 41, pp. 248-53.
Maresch. Über Schädelschüsse. Wien. klin. Wchnschr., 1915, v. 28, pp. 1208-1231.
Maresch. On Skull Shots. Vienna Clinical Weekly, 1915, vol. 28, pp. 1208-1231.
Marguliés, A. Nervenerkrankungen im Kriege. Prag. med. Wchnschr., 1915, v. 40, pp. 299-301.
Marguliés, A. Nerve Diseases in War. Prague Med. Weekly, 1915, v. 40, pp. 299-301.
Marie, Pierre. A propos d’un prisonnier de guerre simulateur. Rev. neurol., Par., 1914-1915, v. 221, p. 492.
Marie, Pierre. About a prisoner of war faking it. Rev. neurol., Par., 1914-1915, v. 221, p. 492.
Marie, P. Sur la fréquence relative des amélioration dans les cas de quadriplégie par traumatisme médullaire, due à une blessure de guerre. Bull. acad. de méd., Par., 1915, v. 73, pp. 675-678.
Marie, P. On the Relative Frequency of Improvement in Cases of Quadriplegia from Spinal Cord Injury Due to War Wounds. Bull. acad. de méd., Par., 1915, v. 73, pp. 675-678.
Marie, P. La conduite à tenir vis-à-vis des blessés du crâne. Rev. neurol., Par., 1916, v. 29, pp. 453-457.
Marie, P. The approach to take regarding head injuries. Rev. neurol., Par., 1916, v. 29, pp. 453-457.
Marie, P. Tétanos tardif localisé à type abdominothoracique. Paris méd., 1916, v. 21, pp. 49-51.
Marie, P. Late localized tetanus of the abdominothoracic type. Paris méd., 1916, v. 21, pp. 49-51.
Marie, P. et Benisty, A. Troubles nerveux purement fonctionnels consécutifs à des blessures de guerre. Rev. neurol., Par., 1914-15, v. 221, pp. 424-425.
Marie, P. and Benisty, A. Purely functional nerve disorders following war injuries. Rev. neurol., Paris, 1914-15, vol. 221, pp. 424-425.
Marie et Benisty. Remarques cliniques sur quelques cas de lésions de la moelle cervicale par plaies de guerre. Rev. Paris méd., (Part. méd.), v. 17, p. 178.
Marie and Benisty. Clinical observations on some cases of spinal cord injuries from war wounds. Rev. Paris méd., (Part. méd.), v. 17, p. 178.
Marie et Benisty. Du retour de la contractilité faradique avant le rétablissement de la motilité volontaire dans les muscles paralysés, à la suite des lésions des nerfs périphériques. Soc. de Neurol. de Paris, 1915. Revue Neurol., May-June 1915, and July 1915.
Marie and Benisty. On the return of faradic contractility before the restoration of voluntary movement in paralyzed muscles following peripheral nerve injuries. Soc. de Neurol. de Paris, 1915. Revue Neurol., May-June 1915, and July 1915.
Marie and Benisty. Individualité clinique des nerfs périphériques. Soc. de Neurol. March 15, 1915. Revue neurol., May-June 1915.
Marie and Benisty. Clinical individuality of peripheral nerves. Neurology Society. March 15, 1915. Neurological Review, May-June 1915.
Marie and Benisty. Une forme douloureuse des lésions de nerf médian par plaie de guerre. Académie de Méd., Mar. 16, 1915.
Marie and Benisty. A painful form of median nerve injuries from war wounds. Académie de Méd., Mar. 16, 1915.
Marie, P. et Chatelin. Un cas d’hématomyélie par éclatement d’obus à distance. Rev. neurol., Par., 1914-15, v. 222, p. 777.
Marie, P. and Chatelin. A case of hematomyelia caused by distant shell explosion. Rev. neurol., Paris, 1914-15, v. 222, p. 777.
Marie, P. et Chatelin. Notes sur une variété de troubles de la parole (scansion) observée dans les blessures de la région frontale. Rev. neurol., Par., 1917, v. 24, pp. 135-136.
Marie, P. and Chatelin. Notes on a variety of speech disorders (scansion) observed in injuries to the frontal region. Neurological Review, Paris, 1917, vol. 24, pp. 135-136.
Marie, P., Chatelin et Patrikios. Paralysie générale progressive développée chez un jeune soldat pendant la guerre. Rev. neurol., Par., 1917, v. 24, p. 38.
Marie, P., Chatelin and Patrikios. Progressive general paralysis developed in a young soldier during the war. Rev. neurol., Par., 1917, v. 24, p. 38.
Marie, P., Dejerine, Ballet, G., Thomas, A., Dupré, Babinski, J., Meige, H. Discussion sur les troubles nerveux, dits fonctionnels, observés pendant la guerre. Rev. neurol., Par., 1914-15, v. 221, pp. 447-452.
Marie, P., Dejerine, Ballet, G., Thomas, A., Dupré, Babinski, J., Meige, H. Discussion on the so-called functional nerve disorders observed during the war. Rev. neurol., Par., 1914-15, v. 221, pp. 447-452.
Marie, P. et Foix. Sur une forme spéciale de parésie paratonique des muscles moteurs de la main. Soc. méd. d’hôp., 1916, 10 février.
Marie, P. and Foix. On a special form of paratonic weakness of the motor muscles of the hand. Med. Soc. Hosp., 1916, February 10.
Marie et Foix. Les syncinésies des hémiplégiques étude séméiologique et classification. Rev. neurol., Par., 1916, v. 23, pp. 2-27.
Marie and Foix. The Synkinesias of Hemiplegics: Semiology Study and Classification. Rev. neurol., Paris, 1916, v. 23, pp. 2-27.
Marie et Foix. Influence du froid et des troubles vasomoteurs sur les réactions électriques. Rev. neurol., Par., 1916, v. 29, pp. 921-923.
Marie and Foix. Influence of cold and vasomotor disorders on electrical reactions. Rev. neurol., Par., 1916, v. 29, pp. 921-923.
Marie et Foix. Indications opératoires fournies par l’examen histologique des nerfs lésés par plaies de guerre. Presse Méd., Jan. 31, 1916.
Marie and Foix. Surgical indications provided by the histological examination of nerves damaged by war wounds. Méd. Press, Jan. 31, 1916.
Marie et Meige. Appareils pour blessés nerveux. Académie de Médecine, 1915.
Marie and Meige. Devices for nerve injury patients. Academy of Medicine, 1915.
Marie, Meige, et Gosset. Les localisations motrices dans les nerfs périphériques. Académie de Médecine, Dec. 28, 1915.
Marie, Meige, and Gosset. Motor locations in the peripheral nerves. Academy of Medicine, Dec. 28, 1915.
Marie, P. et Foix. Les aphasies de guerre. Rev. neurol., Par., 1917, v. 24, pp. 53-87.
Marie, P. and Foix. War-related aphasias. Neurology Review, Paris, 1917, v. 24, pp. 53-87.
Marie, P. et Mlle. G. Lévy. Un cas d’hémiplégie organique par commotion sans blessure. Rev. neurol., Par., 1917, v. 24, pp. 44-45.
Marie, P. and Mlle. G. Lévy. A case of organic hemiplegia due to concussion without injury. Rev. neurol., Paris, 1917, vol. 24, pp. 44-45.
Marie, P., Meige, H., et Béhague, P. Necessité d’un examen neurologique des plicatures dorsaux (camptocormiques). Rev. neurol., Par., 1917, v. 24, pp. 129-130.
Marie, P., Meige, H., and Béhague, P. The need for a neurological examination of dorsal flexions (camptocormic). Neurology Review, Paris, 1917, vol. 24, pp. 129-130.
Marriage, H. J. Special discussion on warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10, (sect. Otol.), pp. 47-56.
Marriage, H. J. Special discussion on injuries and psychological effects from warfare. Proc. Roy. Soc. Med., Lond., 1917, v. 10, (sect. Otol.), pp. 47-56.
Marshall, W. H. Shell shock. J. Mich. M. Soc., Detroit, 1917, Sept., pp. 396-399.
Marshall, W. H. Shell shock. J. Mich. M. Soc., Detroit, 1917, Sept., pp. 396-399.
Martinet, Alfred. Guerre et névroses cardiaques. Presse méd., Par., 1915, v. 23, pp. 433-435.
Martinet, Alfred. War and Heart Neuroses. Medical Press, Paris, 1915, v. 23, pp. 433-435.
Martyn, King. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10, (sect. Balneol.), pp. 19-21.
Martyn, King. Treatment of mental disabilities caused by the war using physical methods. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10, (sect. Balneol.), pp. 19-21.
Marx, S. Über funktionelle Stimm- und Sprachstörungen und ihre Behandlung. München med. Wchnschr., 1916, No. 42, pp. 1502-1503.
Marx, S. On Functional Voice and Speech Disorders and Their Treatment. München Med. Wchnschr., 1916, No. 42, pp. 1502-1503.
Massachusetts committee for the State Care and Treatment of Soldiers Suffering from Nervous and Mental Diseases (letter). Bos. M. & S. J., 1917, clxxvi, 922.
Massachusetts committee for the State Care and Treatment of Soldiers Dealing with Nervous and Mental Health Issues (letter). Bos. M. & S. J., 1917, clxxvi, 922.
Mathieu, Albert. Cause psychique de vomissements excessifs après la chloroformisation et après la gastro-entérostomie. Presse méd., Par., 1917, v. 25, pp. 197.
Mathieu, Albert. Psychological cause of excessive vomiting after chloroform anesthesia and after gastroenterostomy. Medical Press, Paris, 1917, vol. 25, pp. 197.
Matiri, A. I disturbi mentali nella sclerosi laterale amiotrofica. Riv. crit. di clin. med., Firenze, 1916, v. 17, pp. 197, 209, 221, 233.
Matiri, A. Mental disorders in amyotrophic lateral sclerosis. Crit. Rev. Clin. Med., Florence, 1916, vol. 17, pp. 197, 209, 221, 233.
Mauclaire, Pl. Troubles moteurs d’origine psychiques chez les blessés militaires. Bull. et mém. soc. de chir. de Par., 1914, v. 40, p. 1290.
Mauclaire, Pl. Psychological motor troubles in military injuries. Bull. et mém. soc. de chir. de Par., 1914, v. 40, p. 1290.
Mauclaire, Pl. Commotion cérébrale intense avec mutisme et surdité psychiques. Bull. et mém. soc. de chir. de Par., 1916, v. 421, pp. 140-141.
Mauclaire, Pl. Severe concussion with mutism and psychological deafness. Bull. et mém. soc. de chir. de Par., 1916, v. 421, pp. 140-141.
Maude, A. Influenza and purulent bronchitis. Lancet, Lon., 1918, ii, 324.
Maude, A. Influenza and purulent bronchitis. Lancet, London, 1918, ii, 324.
Mayendorf. Über pathologische Zitterformen zur Kriegszeit. Münch. med. Wchnschr., 1916, v. 63, p. 323.
Mayendorf. On pathological tremors during wartime. Münch. med. Wchnschr., 1916, v. 63, p. 323.
Mayer, A. G. On the non-existence of nervous shell-shock in fishes and marine invertebrates. Proc. Nat. Acad. Sc., Balt., 1917, iii, p. 597.
Mayer, A. G. On the non-existence of nervous shell-shock in fish and marine invertebrates. Proc. Nat. Acad. Sc., Balt., 1917, iii, p. 597.
Mayer, C. Behandlung gekommenen Fälle von Kriegsverletzungen. Wien. med. Wchnschr., 1915, v. 65, p. 37.
Mayer, C. Treatment of cases of war injuries. Vienna. med. Wchnschr., 1915, v. 65, p. 37.
Mayer, C. Kriegsneurologische Erfahrungen. Med. Klin., Berl. u. Wien., 1915, v. 112, pp. 1017-1022.
Mayer, C. Experiences in War Neurology. Med. Klin., Berlin and Vienna, 1915, v. 112, pp. 1017-1022.
Mayer, Leo. Autoplastic nerve transplantation in the repair of gunshot injuries. Surg. Gynecol. and Obstet., 1918, xxvii, 530.
Mayer, Leo. Autoplastic nerve transplantation in the repair of gunshot injuries. Surg. Gynecol. and Obstet., 1918, xxvii, 530.
Mayer, L. Organization and aims of the Orthopedic Reconstruction Hospital. Amer. Jour., Care for Crip., 1917, 78.
Mayer, L. Organization and goals of the Orthopedic Reconstruction Hospital. Amer. Jour., Care for Crip., 1917, 78.
Maynard. Syndrôme psychique atypique chez les blessés cranio-cérébraux. Montpel. méd., 1916, v. 39, pp. 65-69.
Maynard. Atypical mental syndrome in brain-injured patients. Montpel. méd., 1916, v. 39, pp. 65-69.
Mayo-Robson, A. W. Treatment of paraplegia from gunshot or other injuries of the spinal cord. Brit. Med. Jour., 1917, ii, 853.
Mayo-Robson, A. W. Treatment of paraplegia caused by gunshot or other spinal cord injuries. Brit. Med. Jour., 1917, ii, 853.
McArdle, J. S. Joint troubles arising from nervous diseases. Practitioner, Lond., 1915, v. 95, pp. 174-180.
McArdle, J. S. Joint problems caused by nervous diseases. Practitioner, Lond., 1915, v. 95, pp. 174-180.
McClure, J. Campbell. The manipulation bath. Proc. Roy. Soc. Med., Lond., 1917, v. 10, No. 9 (Sect. of B. and Climatology), pp. 70-78.
McClure, J. Campbell. The manipulation bath. Proc. Roy. Soc. Med., Lond., 1917, v. 10, No. 9 (Sect. of B. and Climatology), pp. 70-78.
McClure, J. C. Gastric atony and war neurasthenia. Lancet, Lond., 1917, ii. 600-602.
McClure, J. C. Gastric atony and war neurasthenia. Lancet, London, 1917, ii. 600-602.
McDougall, W. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Sect. Psychiat.), pp. 25-26.
McDougall, W. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Sect. Psychiat.), pp. 25-26.
McDowall, Colin. Functional gastric disturbances in the soldier. J. Ment. Sc., Lond., 1917, v. 63, pp. 76-88.
McDowall, Colin. Functional gastric disturbances in soldiers. J. Ment. Sc., Lond., 1917, v. 63, pp. 76-88.
McDowall, Colin. Functional gastric disturbances in the soldier. Lancet, Lond., 1916, ii, pp. 944-45.
McDowall, Colin. Functional gastric issues in soldiers. Lancet, Lond., 1916, ii, pp. 944-45.
McEllroy, W. S. Acidosis in shock. Jour. A. M. A., 1918, lxx, 846.
McEllroy, W. S. Acidosis in shock. JAMA, 1918, 70, 846.
McKellar, H. R. Malingering. Mil. Surgeon, Wash., 1916, xxxix, 293-299.
McKellar, H. R. Faking Illness. Military Surgeon, Washington, 1916, vol. 39, pp. 293-299.
McKenzie, R. Tait. Functional reëducation of the wounded. N. Y. Med. Jour., 1918, cviii, 683.
McKenzie, R. Tait. Functional reeducation of the injured. N. Y. Med. Jour., 1918, cviii, 683.
McKenzie, R. Tait. Reclaiming the Maimed. Macmillan, 1918.
McKenzie, R. Tait. Reclaiming the Maimed. Macmillan, 1918.
McKenzie, R. Tait. Treatment of convalescent soldiers by physical means, Brit. M. J., Lond., 1916, ii, pp. 215-218; also Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Surg. Sect.), pp. 31-70.
McKenzie, R. Tait. Treatment of recovering soldiers using physical methods, Brit. M. J., Lond., 1916, ii, pp. 215-218; also Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Surg. Sect.), pp. 31-70.
McLaughlin, J. Loss of speech and shell shock. Lancet, Lond., 1916, i, 212.
McLaughlin, J. Loss of speech and shell shock. Lancet, London, 1916, 1, 212.
McMurtrie, Douglas C. The Disabled Soldier. Macmillan, 1919.
McMurtrie, Douglas C. The Disabled Soldier. Macmillan, 1919.
McMurtrie, D. C. Industrial training for war cripples. Illustrations of educational work in France and Germany. Am. J. Care Cripples, N. J., 1917, v. 4, p. 16.
McMurtrie, D. C. Industrial training for injured veterans. Examples of educational work in France and Germany. Am. J. Care Cripples, N. J., 1917, v. 4, p. 16.
McMurtrie, D. C. Reëducating German war cripples at Düsseldorf. Bos. M. & S. J., 1918, clxxviii, 182.
McMurtrie, D. C. Reeducating German war veterans at Düsseldorf. Bos. M. & S. J., 1918, clxxviii, 182.
McWalter, J. C. A note on commotio cerebri, or shell shock. Med. Press and Circ., Lond., 1916, v. 101, pp. 332-333.
McWalter, J. C. A note on commotio cerebri, or shell shock. Med. Press and Circ., Lond., 1916, v. 101, pp. 332-333.
McWalter, J. C. An experiment in enforced continence. Med. Press and Circ., Lond., 1916, v. 102, pp. 363-364.
McWalter, J. C. An experiment in enforced continence. Med. Press and Circ., Lond., 1916, v. 102, pp. 363-364.
Meakins, J. C. and Gunson, E. B. Occurrence of hyperalgesia in the “irritable heart of soldiers.” Heart, 1917, vi, 343.
Meakins, J. C. and Gunson, E. B. Occurrence of hyperalgesia in the “irritable heart of soldiers.” Heart, 1917, vi, 343.
Medea, E. Malattie nervose e malattie mentali in rapporto alla guerra. Osp. maggiore, Milano, 1915, 2 s., v. 3, pp. 399-408.
Medea, E. Nervous diseases and mental illnesses related to war. Major Hospital, Milan, 1915, 2 s., v. 3, pp. 399-408.
Medea, E. Neurologia di Guerra. Atti. d. Soc. lomb. di sc. Med. e Biol., Milano, 1915-16, v. 5, pp. 49-60.
Medea, E. Neurology of War. Proceedings of the Lombard Society of Medical and Biological Sciences, Milan, 1915-16, vol. 5, pp. 49-60.
Médication hypnotique par le dial. Progrès Méd., Par., 1916, v. 31, p. 56.
Hypnotic medication by the dial. Progrès Méd., Paris, 1916, v. 31, p. 56.
Médecin tiré par un aliéné qu’il soignait. Ann. Méd.-psychol., Par., 1916-17, p. 567.
Doctor pulled by a patient he was treating. Ann. Méd.-psychol., Par., 1916-17, p. 567.
Meige, Henri. De certaines boîteries observées chez les “blessés nerveux.” Rev. neurol., Par., 1914-15, v. 22, pp. 939-947.
Meige, Henri. On Certain Disorders Observed in “Nervous Wounded.” Rev. neurol., Par., 1914-15, v. 22, pp. 939-947.
Meige, H. Contractions convulsives des muscles peauciers du crâne à la suite d’une déflagration (Tic ou Spasme?) Rev. neurol., Par., 1916, v. 23, pp. 107-109.
Meige, H. Convulsive contractions of the muscles of the scalp following an explosion (Tic or Spasm?) Neurology Review, Paris, 1916, v. 23, pp. 107-109.
Meige, H. Les tremblements consécutifs aux explosions. Rev. neurol., Par., 1916, Nos. 4-5, p. 592.
Meige, H. The tremors following explosions. Neurological Review, Paris, 1916, Nos. 4-5, p. 592.
Meige, H. Torticolis convulsif survenu chez un blessé du crâne hémiplégique et jacksonien. Rev. neurol., Par., 1916, v. 23, pp. 571-574.
Meige, H. Convulsive torticollis in a skull-injured patient with hemiplegia and Jacksonian symptoms. Rev. neurol., Paris, 1916, vol. 23, pp. 571-574.
Meige, H. Réformes, incapacités, gratifications dans les tremblements, les tics et les spasmes. Rev. neurol., Par., 1916, v. 23, pp. 758-763.
Meige, H. Reforms, disabilities, rewards in tremors, tics, and spasms. Rev. neurol., Par., 1916, v. 23, pp. 758-763.
Meige, H. Torticolis convulsif survenu chez un blessé du crâne hémiplégique et jacksonien. Rev. neurol., Par., 1916. v. 24, pp. 571-574.
Meige, H. Convoluted torticollis occurred in a patient with a hemiplegic skull injury and Jacksonian seizures. Rev. neurol., Par., 1916. v. 24, pp. 571-574.
Meige, H. Tremblement, tressaillement, trémophobie consécutifs aux explosions. Rev. neurol., Par., 1916, v. 29, pp. 140-158.
Meige, H. Trembling, shivering, and fear of tremors following explosions. Rev. neurol., Par., 1916, v. 29, pp. 140-158.
Meige, H. Les tremblements consécutifs aux explosions (tremblement, tressaillement, trémophobie). Rev. neurol., Par., 1916, v. 29, pp. 201-209.
Meige, H. The tremors following explosions (tremor, twitching, tremophobia). Neurological Review, Paris, 1916, v. 29, pp. 201-209.
Meige, H. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol., Par., 1916, v. 29, pp. 592-593.
Meige, H. On nerve accidents caused by the explosion of large quantities of explosives. Neurology Review, Paris, 1916, vol. 29, pp. 592-593.
Meige, H. Appareil pour redresser les griffes cubitales (Appareil Gillot). Rev. neurol., Par., 1917, v. 24, pp. 264-265.
Meige, H. Device for correcting cubital claws (Gillot Device). Rev. neurol., Paris, 1917, v. 24, pp. 264-265.
Meige et Mme. Athanassio Benisty. De l’importance des lésions vasculaires associées aux lésions des nerfs périphériques dans les plaies de guerre. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 208-211.
Meige and Mrs. Athanassio Benisty. The importance of vascular injuries associated with peripheral nerve injuries in war wounds. Bull. et mém. soc. méd. d’hôp. de Par., 1915, v. 39, pp. 208-211.
Meige et Benisty. Les formes douloureuses des blessures des nerfs. Soc. de Neurol., July 1, 1915.
Meige and Benisty. The painful forms of nerve injuries. Neurology Society, July 1, 1915.
Meige et Benisty. Les signes cliniques des lésions de l’appareil sympathique et de l’appareil vasculaire dans les blessures des membres. Presse méd., Par., 1916, v. 24, pp. 153-156.
Meige and Benisty. The clinical signs of lesions in the sympathetic system and vascular system in limb injuries. Med. Press, Paris, 1916, vol. 24, pp. 153-156.
Meige, H., Benisty, A., et Lévy, G. Impotence de tous les mouvements de la main et des doigts, avec intégrité des réactions électriques (main figée). Rev. neurol., Par., 1914-15, v. 22, pp. 1273-1276.
Meige, H., Benisty, A., and Lévy, G. Impotence of all movements of the hand and fingers, with intact electrical reactions (frozen hand). Rev. neurol., Paris, 1914-15, v. 22, pp. 1273-1276.
Meige, Maré, T., etc. Discussion sur la camptocormie. Rev. neurol., Par., [952]1914-15, v. 222, p. 1250.
Meige, Maré, T., etc. Discussion on camptocormia. Rev. neurol., Par., [952]1914-15, v. 222, p. 1250.
Melocchi, F. Importanza dei centri fisiatrici di rieducazione funzionale per gli invalidi di guerra. Pensiero med., Milano, 1917, v. 7, p. 282.
Melocchi, F. The Importance of Physiotherapy Rehabilitation Centers for War Invalids. Medical Thought, Milan, 1917, vol. 7, p. 282.
Mendel, Kurt. Psychiatrisches und Neurologisches aus dem Felde. Neurol. Centralbl., Leipz., 1915, No. 1, p. 2. Rev. Med. Klin., Berl. u. Wien., 1915, v. 111, p. 575.
Mendel, Kurt. Psychiatry and Neurology from the Field. Neurol. Centralbl., Leipzig, 1915, No. 1, p. 2. Rev. Med. Klin., Berlin and Vienna, 1915, v. 111, p. 575.
Mendelssohn, Maurice. Deux cas de paraplégie de nature organique suivis de guérison. Rev. neurol., Par., 1916, v. 29, pp. 190-193.
Mendelssohn, Maurice. Two cases of organic paraplegia followed by recovery. Neurological Review, Paris, 1916, vol. 29, pp. 190-193.
Mental and nervous cases in the war. Alb. Med. Ann., 1917, xxxviii, 328.
Mental and nervous cases in the war. Alb. Med. Ann., 1917, xxxviii, 328.
Mental disabilities for war service. Lancet, Lond., 1916, v. 191, p. 234.
Mental disabilities from military service. Lancet, London, 1916, vol. 191, p. 234.
Mentality (fortitude) of Wounded. Brit. M. J., Lond., 1915, i. p. 980.
Mentality (fortitude) of Wounded. Brit. M. J., Lond., 1915, i. p. 980.
Menzel. Mobilisierung in ursächlichem Zusammenhange stehenden Neurosen der oberen Luftwege, beziehungsweise des Ohres vor Militärärzt. Wien. med. Wchnschr., 1915, No. 4, p. 163.
Menzel. Mobilization in relation to neuroses of the upper respiratory tract or the ear before military doctors. Wien. med. Wchnschr., 1915, No. 4, p. 163.
Menzel. Symptom des sogenannten labyrinthören Spontan-nystagmus. Militärärzt. Wien. med. Wchnschr., 1915, v. 65, p. 235.
Menzel. Symptom of what’s known as labyrinthine spontaneous nystagmus. Military doctor. Wien. med. Wchnschr., 1915, v. 65, p. 235.
Mériel. Deux cas de tétanos partiel. Soc. chir., 2 Feb., 1916.
Mériel. Two cases of partial tetanus. Surgical Society, Feb 2, 1916.
Merklen, P. Sur les déterminations psychiques des paratyphoides. Rev. Paris méd., 1916 (Part. méd.), v. 19, p. 96.
Merklen, P. On the Psychic Determinations of Paratyphoids. Rev. Paris méd., 1916 (Part. méd.), v. 19, p. 96.
Merklen. Sur les déterminations psychiques des paratyphoides. Paris méd., 1916, (Part. Méd.), v. 21, pp. 64-66.
Merklen. On the psychological determinations of paratyphoids. Paris med., 1916, (Part. Med.), v. 21, pp. 64-66.
Merklen. Sur les déterminations psychiques des paratyphoides. Presse méd., Par., 1916, v. 24, p. 6.
Merklen. On the psychological determinants of paratyphoids. Medical Press, Paris, 1916, vol. 24, p. 6.
Merklen. Note sur l’hypothermie chez les militaires. Bull. et mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 1008-1010.
Merklen. Note on hypothermia in the military. Bull. and mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 1008-1010.
Merle und Schaidler. Ausbildung und Berufstätigkeit der Kriegsblinden. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, p. 468.
Merle and Schaidler. Training and Employment of War Blind. German Medical Weekly, Leipzig and Berlin, 1916, v. 42, p. 468.
Mesnard. Tétanos monoplégique. Marseille méd., Par., 1917, pp. 363-365.
Mesnard. Monoplegic tetanus. Marseille méd., Par., 1917, pp. 363-365.
Metcalfe, F. A Red Cross “Plattsburg”; the U. S. Army Ambulance Corps’ Camp at Allentown, Pa. Red Cross Mag., Wash., 1917, v. 12, pp. 430-436.
Metcalfe, F. A Red Cross “Plattsburg”; the U.S. Army Ambulance Corps’ Camp at Allentown, PA. Red Cross Mag., Wash., 1917, v. 12, pp. 430-436.
Meyer, E. Psychosen und Neurosen in der Armee während des Krieges. Deutsche med. Wchnschr., Berl. u. Leipz., 1914, v. 402, pp. 2085-2088.
Meyer, E. Psychoses and neuroses in the army during the war. German medical weekly, Berlin and Leipzig, 1914, v. 402, pp. 2085-2088.
Meyer, E. Ueber die Frage der Dienstbeschädigung bei den Psychosen. München. med. Wchnschr., 1916, lxiii, 1558.
Meyer, E. On the Issue of Service Damage in Psychoses. Munich. Med. Weekly, 1916, lxiii, 1558.
Meyer, E. Der Einfluss des Krieges, insbesondere des Kriegsausbruch auf schon bestehende Psychosen. Archiv. f. Psych., Berl., 1915, v. 55, pp. 353-364.
Meyer, E. The Influence of War, Particularly the Outbreak of War on Existing Psychoses. Archiv. f. Psych., Berl., 1915, v. 55, pp. 353-364.
Meyer, E. Functionelle Nervenstörungen bei Kriegsteilnehmen nebst Bemerkungen zur traumatischen Neurose. Deutsche med. Wchnschr., Leipz. u. Berl., 1915, v. 41, pp. 1509-1511.
Meyer, E. Functional Nerve Disorders in War Participants along with Comments on Traumatic Neurosis. Deutsche med. Wchnschr., Leipzig and Berlin, 1915, v. 41, pp. 1509-1511.
Meyer, E. Beitrag zur Kenntnis des Einflusses kriegerischer Ereignisse auf die Entstehung geistiger Störungen in der Zivilbevölkerung und zu der physischen Infektion. Ibid., lvi, 247-279.
Meyer, E. Contribution to the Understanding of the Impact of War Events on the Development of Mental Disorders in the Civil Population and Physical Infection. Ibid., lvi, 247-279.
Meyer, E. Zwei Soldaten mit psychogenen Störungen. Berl. klin. Wchnschr., 1915, v. 521, p. 94.
Meyer, E. Two Soldiers with Psychogenic Disorders. Berl. klin. Wchnschr., 1915, v. 521, p. 94.
Meyer, E. Die Frage der Laminektomie von neurologischen Standpunkt. Berl. klin. Wchnschr., 1915, v. 521, pp. 282-283.
Meyer, E. The Issue of Laminectomy from a Neurological Perspective. Berl. klin. Wchnschr., 1915, v. 521, pp. 282-283.
med. Wchnschr., 1916, No. 44, p. 1558.
med. Wchnschr., 1916, No. 44, p. 1558.
Meyer, E. Bemerkungen zu der Differentialdiagnose der Psychosen. Reaktionen mit besonderer Berücksichtigung der im Kriege beobachteten psychischen Störungen. Archiv. f. Psychiat., 1916, v. 56, pp. 244-246.
Meyer, E. Comments on the differential diagnosis of psychoses. Reactions with particular attention to the psychological disturbances observed in wartime. Archiv. f. Psychiat., 1916, v. 56, pp. 244-246.
Meyer, E. Kriegshysterie. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, pp. 69-71.
Meyer, E. War Hysteria. German Medical Weekly, Leipzig and Berlin, 1916, v. 42, pp. 69-71.
Meyer, E. Funktionelle Nervenstörungen bei Kriegsteilnehmern nebst Bemerkungen zur traumatischen Neurose. Med. Klin., Berl., 1916, v. 12, p. 26.
Meyer, E. Functional nerve disorders in war participants along with remarks on traumatic neurosis. Med. Klin., Berl., 1916, v. 12, p. 26.
Meyer, E. Krankheitsanlagen und Krankheitsursachen im Gebiete der Psychosen und Neurosen. Berl. klin. Wchnschr., 1917, No. 3, Rev. Cor. bl. f. Schweize Arztr., 1917, No. 19, p. 620.
Meyer, E. Paths to Illness and Causes of Disease in the Area of Psychoses and Neuroses. Berl. klin. Wchnschr., 1917, No. 3, Rev. Cor. bl. f. Schweizer Arztr., 1917, No. 19, p. 620.
Meyer, E. Ueber die Frage der Dienstbeschädigung bei den Psychosen. Arch. f. Psychiat., Berl., 1917, 57, 208-220.
Meyer, E. On the Issue of Service Damage in Psychoses. Arch. f. Psychiatry, Berl., 1917, 57, 208-220.
Meyer, E. und Frida Reichmann. Über nervose Folgezustände nach Granatexplosionen. Arch. f. Psychiat., Berl., 1916, v. 56, No. 3.
Meyer, E. and Frida Reichmann. On Nervous Aftereffects Following Grenade Explosions. Arch. f. Psychiat., Berl., 1916, v. 56, No. 3.
Mézie, A. Troubles réflexes et insuffisance cérébrale. Gazette hebdomadaire des Sciences médicales de Bordeaux, 23 Sept. 1916.
Mézie, A. Reflex issues and brain insufficiency. Weekly Gazette of Medical Sciences of Bordeaux, September 23, 1916.
Michon, E. Impotence fonctionnelle du muscle trapèze à la suite d’une plaie par balle de la région sus-claviculaire. Bull. et mém. soc. de chir. de Par., 1915, v. 41, pp. 652-655.
Michon, E. Functional impairment of the trapezius muscle following a bullet wound to the supraclavicular region. Bull. et mém. soc. de chir. de Par., 1915, v. 41, pp. 652-655.
Midelton, W. J. Nerves and the war. Med. Times, Lond., 1914, v. 42, pp. 726, 742, 758, 776, 786, 802, 835.
Midelton, W. J. Nerves and the war. Med. Times, Lond., 1914, v. 42, pp. 726, 742, 758, 776, 786, 802, 835.
Mignard. Syndrôme psychique atopique chez les blessés crânio-cérébraux (Observé quelques mois après la blessure). Montpel. méd., 1916, v. 39, p. 65.
Mignard. Atopic psychological syndrome in patients with brain injuries (Observed a few months after the injury). Montpel. méd., 1916, v. 39, p. 65.
Mignard. Quelques considérations sur la résponsabilité des blessés crânio-cérébraux. Montpel. méd., 1916, v. 39, p. 127.
Mignard. A few considerations on the responsibility of individuals with cranial and cerebral injuries. Montpel. méd., 1916, v. 39, p. 127.
Mignot, Roger. L’évolution de la paralysie générale chez les officiers combattants. Presse méd., Par., 1917, v. 25, pp. 487-488.
Mignot, Roger. The development of general paralysis in combat officers. Medical Press, Paris, 1917, vol. 25, pp. 487-488.
Milian, G. Battle hypnosis. Med. Press and Circ., Lond., 1915, n.s., c, 486-488.
Milian, G. Battle hypnosis. Med. Press and Circ., Lond., 1915, n.s., c, 486-488.
Milian, G. Les aliénés dans l’armée. Paris méd., 1914-15, v. 15, (Part. méd.), p. 458.
Milian, G. The insane in the army. Paris méd., 1914-15, v. 15, (Part. méd.), p. 458.
Milian, G. L’hypnose des batailles. Paris méd., v. 15, 1914-15, pp. 265-270.
Milian, G. The Hypnosis of Battles. Paris méd., vol. 15, 1914-15, pp. 265-270.
Milian, G. Désertion ou fugue. Paris méd., (Part. méd.), 1915, v. 17, pp. 11-13.
Milian, G. Desertion or Escape. Paris Med., (Part. Med.), 1915, v. 17, pp. 11-13.
Milian, G. Les éruptions provoquées. Paris méd., 1917, xxi, 343-351.
Milian, G. Induced Eruptions. Paris Med., 1917, xxi, 343-351.
Milian, G. La fête au camp. Paris Méd., 1915, (Part. méd.), 1915, v. 17, pp. 11-13.
Milian, G. The Party at the Camp. Paris Méd., 1915, (Part. méd.), 1915, v. 17, pp. 11-13.
Military mental cases. Med. officer, Lond., 1915, v. 14, p. 150.
Military mental cases. Med. officer, Lond., 1915, v. 14, p. 150.
Military orthopaedics and the American unit. Brit. M. J., Lond., 1917, v. 1, p. 772.
Military orthopaedics and the American unit. Brit. M. J., Lond., 1917, v. 1, p. 772.
Military Orthopedic Surgery. No. 4, Medical Manual War Series. Lea and Febiger, 1918.
Military Orthopedic Surgery. No. 4, Medical Manual War Series. Lea and Febiger, 1918.
Military psychiatry. Bos. M. and S. J., 1918, clxxviii, 98.
Military psychiatry. Bos. M. and S. J., 1918, clxxviii, 98.
Milligan, E. T. C. Medical Experiences in the War Zone. M. J. Australia, Sydney, 1917, v. 1, pp. 201-203.
Milligan, E. T. C. Medical Experiences in the War Zone. M. J. Australia, Sydney, 1917, vol. 1, pp. 201-203.
Milligan, E. T. C. Method of treatment of “shell shock.” Brit. Med. Jour., 1916, ii, 73.
Milligan, E. T. C. Treatment method for “shell shock.” Brit. Med. Jour., 1916, ii, 73.
Milligan, E. C. Treatment of Shell Shock. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 272-273.
Milligan, E. C. Treatment of Shell Shock. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 272-273.
Milligan, W. Functional Cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-1915, (sect. laryngol.), v. 8, p. 118.
Milligan, W. Functional Cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-1915, (sect. laryngol.), v. 8, p. 118.
Milligan, W. Treatment of “Functional aphonia” in Soldiers from the Front. J. Laryngol., Lond., 1916, v. 31, pp. 299-300.
Milligan, W. Treatment of "Functional aphonia" in Soldiers from the Front. J. Laryngol., Lond., 1916, v. 31, pp. 299-300.
Milligan, W. Treatment of Shell Shock. Brit. M. J., Lond., 1916, ii, p. 73; also ii, p. 242.
Milligan, W. Treatment of Shell Shock. Brit. M. J., Lond., 1916, ii, p. 73; also ii, p. 242.
Milligan and Westmacott. Warfare injuries and neuroses. J. Laryngol., 1915, v. 30, p. 297.
Milligan and Westmacott. Injuries and mental health issues from warfare. J. Laryngol., 1915, v. 30, p. 297.
Mills, A. E. Some nerve injuries seen on active service. M. J. Australia, Sydney, 1917, v. 4, pp. 73-75.
Mills, A. E. Some nerve injuries observed during active duty. M. J. Australia, Sydney, 1917, v. 4, pp. 73-75.
Mills, Lloyd. Projectile Wounds of the Head. J. Am. M. Ass., Chicago, 1915, v. 65, pp. 1424-1427.
Mills, Lloyd. Projectile Wounds of the Head. J. Am. M. Ass., Chicago, 1915, v. 65, pp. 1424-1427.
Mingazzini, G. Sindromi nervose organiche consecutive a lesioni (da proiettili) del cervello. Policlin., Roma, 1916 (sez. med.), v. 23, p. 409.
Mingazzini, G. Organic nerve syndromes resulting from brain injuries (by bullets). Policlin., Rome, 1916 (med. section), vol. 23, p. 409.
Mingazzini, G. Neurologia di guerra (ferite da proiettile del cervello e midollo spinale). Policlinico, Roma, sez. prat., 1917, v. 24, pp. 22-23.
Mingazzini, G. War Neurology (bullet wounds of the brain and spinal cord). Policlinico, Rome, pract. sect., 1917, vol. 24, pp. 22-23.
Mingazzini, G. Osservazioni cliniche sulle lesioni del cervello e del midollo spinale da proiettili di guerra. Policlin., Roma, 1917, v. 24 (sez. med.), pp. 121, 178, 189.
Mingazzini, G. Clinical observations on brain and spinal cord injuries from war bullets. Policlin., Rome, 1917, vol. 24 (med. section), pp. 121, 178, 189.
Mirallié, M. Paralysies réflexes. Rev. gén. de path. de guerre, Par., 1916, No. 1, pp. 19-35.
Mirallié, M. Reflex Paralysis. Gen. Rev. of War Pathology, Paris, 1916, No. 1, pp. 19-35.
Mirc, J. Folies de guerre chez les civils. Caducée, Par., 1916, v. 16, p. 141.
Mirc, J. War Madness Among Civilians. Caducée, Paris, 1916, vol. 16, p. 141.
Mirc, J. Folies de guerre chez les civils. J. de méd. de Par., 1917, v. 36, p. 12.
Mirc, J. The Madness of War Among Civilians. J. of Med. of Paris, 1917, v. 36, p. 12.
Misch, W. Ueber Hemiplegie bei Diphtherie. Neurol. Centralbl., Leipz., 1916, v. 35, No. 22.
Misch, W. On Hemiplegia in Diphtheria. Neurol. Centralbl., Leipzig, 1916, v. 35, No. 22.
Mizie, A. Troubles réflexes et insuffisance cérébralles. Gaz. hebd. d. sc. méd., Par., 1916, v. 2, pp. 141-142.
Mizie, A. Reflex Troubles and Cerebral Insufficiency. Weekly Gazette of Medical Science, Paris, 1916, v. 2, pp. 141-142.
Mohr, F. Behandlung nervöser und depressiver Zustandsbilder bei Kriegsteilnehmer. n. Aerztl. Centralbl. Ztg., 1915, Wien, v. 32, p. 134.
Mohr, F. Treatment of nervous and depressive conditions in war participants. n. Medical Central Journal, 1915, Vienna, vol. 32, p. 134.
Mohr, F. Zur Entstehung, Vorhersage und Behandlung nervöser und depressiver Zustandsbilder bei Kriegsteilnehmern. Med. Klin., Berl., 1915, xi, 920.
Mohr, F. On the Origin, Prediction, and Treatment of Nervous and Depressive Conditions in War Participants. Med. Klin., Berl., 1915, xi, 920.
Mohr, F. Grundsätzliches zur Kriegsneurosenfrage. Med. Klin. Berl. u. Wien, 1916, v. 12, pp. 89-93. Rev. Aerztl. Rundschau, 1916, v. 26, pp. 40-41.
Mohr, F. Basics on the issue of war neuroses. Med. Klin. Berl. u. Wien, 1916, v. 12, pp. 89-93. Rev. Aerztl. Rundschau, 1916, v. 26, pp. 40-41.
Mohr, F. Behandlung der Kriegsneurosen. Therap. Monatschr., Berl., 1916, v. 30, No. 3.
Mohr, F. Treatment of Combat Neuroses. Therapy Monthly, Berlin, 1916, v. 30, No. 3.
Molhaut, M. Les troubles moteurs d’ordre réflexe. Arch. méd., Belges, Brux., 1917, v. 47, pp. 910-927.
Molhaut, M. Reflex Motor Disorders. Arch. méd., Belges, Brux., 1917, v. 47, pp. 910-927.
Moll, A. Ueber psychopathologische Erfahrungen vom westlichen Kriegsschauplatz. Berl. klin. Wchnschr., 1915, iii, 95.
Moll, A. On Psychopathological Experiences from the Western Front of War. Berl. klin. Wchnschr., 1915, iii, 95.
Moll, A. Kriegsärztlicher Abend, Berlin, Jan. 12, 1915. Psychiat.-Neurolog. Wchnschr., Halle, a. s., 1914-15, v. 16, p. 402.
Moll, A. Military Medical Evening, Berlin, Jan. 12, 1915. Psychiat.-Neurolog. Weekly Journal, Halle a. s., 1914-15, v. 16, p. 402.
Moll, A. Psychopathologische Erfahrungen vom westlichen Kriegsschauplatz. Med. Klin., Berl. u. Wien, 1915, v. 111, p. 710.
Moll, A. Psychopathological Experiences from the Western War Front. Med. Klin., Berl. u. Wien, 1915, v. 111, p. 710.
Moll, A. Psychopathologische Erfahrungen vom westlichen Kriegsschauplatz. Ztschr. f. ärtzl. Fortbild., 1915, No. 10, pp. 305-310; also No. 9, pp. 261-266.
Moll, A. Psychopathological Experiences from the Western Front. Journal of Medical Continuing Education, 1915, No. 10, pp. 305-310; also No. 9, pp. 261-266.
Moll, A. Psychopathologische Erfahrungen im Kriege. Aerzt. Central. Zeit., Wien, 1915, v. 27, p. 139.
Moll, A. Psychopathological Experiences in War. Physician's Central Journal, Vienna, 1915, v. 27, p. 139.
Moll, A. Psychopathologische Erfahrungen auf dem westlichen Kriegsschauplatz. Berl. klin. Wchsnchr., 1915, No. 4, p. 95.
Moll, A. Psychopathological experiences on the Western front. Berl. klin. Wchsnchr., 1915, No. 4, p. 95.
Mollison, W. M. Cases of deafness as a result of the war. Guy’s Hosp. Gaz., Lond., 1916, Feb., pp. 69-71.
Mollison, W. M. Cases of hearing loss due to the war. Guy’s Hosp. Gaz., Lond., 1916, Feb., pp. 69-71.
Monbrun, A. Les hémianopsies en quadrant et le centre cortical de la vision. Presse méd., Par., 1917, v. 25, pp. 607-609.
Monbrun, A. Quadrant Hemianopsia and the Cortical Center of Vision. Medical Press, Paris, 1917, vol. 25, pp. 607-609.
Monier-Vinard. Troubles physiopathiques médullaires post-tétaniques et latents décélés par l’anesthésie chloroformique. Rev. neurol. Par., 1917, v. 24, pp. 568-572.
Monier-Vinard. Post-tetanus spinal pathophysiological issues that were revealed by chloroform anesthesia. Rev. neurol. Par., 1917, v. 24, pp. 568-572.
Montier. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 469.
Montier. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 469.
Moravensic, von E. C. Die Rolle des Krieges im der Aetiologie nervöser insbesonders psychische Störungen. Neurol. Centralbl., Leipz., 1915, v. 34, p. 637.
Moravensic, von E. C. The Role of War in the Etiology of Nervous, Especially Psychological Disorders. Neurol. Centralbl., Leipzig, 1915, v. 34, p. 637.
Moravskaya, V. Ye. and Moravskaya, Yu. A. (The “Kokhanuvka” institution for the insane and the war). Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 311-333.
Moravskaya, V. Ye. and Moravskaya, Yu. A. (The “Kokhanuvka” institution for the mentally ill and the war). Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 311-333.
Morax, V. Notes cliniques et statistiques sur l’ophtalmie sympathique aux armées. Ann. d’ocul., Par., 1917, v. 144, pp. 706-722.
Morax, V. Clinical and statistical notes on sympathetic ophthalmia in the armies. Ann. d’ocul., Par., 1917, v. 144, pp. 706-722.
Morchen. Traumatische Neurosen und Kriegsgefangene. München. med. Wchnschr., 1916, v. 64, No. 32.
Morchen. Traumatic neuroses and prisoners of war. Munich. med. Wchnschr., 1916, v. 64, No. 32.
Morestin. Mutisme hystérique à l’occasion d’une blessure de la langue. J. de méd. et de chir., 1915, Jan., v. 86.
Morestin. Hysterical mutism following a tongue injury. J. of Med. and Surg., 1915, Jan., v. 86.
Morestin. Un cas de mutisme hystérique à l’occasion d’une blessure de la langue. Bull. et mém. soc. de chir. de Par., 1915, v. 41, pp. 98-100.
Morestin. A case of hysterical mutism following a tongue injury. Bull. et mém. soc. de chir. de Par., 1915, v. 41, pp. 98-100.
Morhardt, P. E. Cure de soleil et chirurgie de guerre. Paris méd., 1915-16, v. 17, pp. 315-317.
Morhardt, P. E. Sun Cure and War Surgery. Paris Med., 1915-16, v. 17, pp. 315-317.
Moricand, I. Note sur un cas de paralysie radiale bilatérale par compression, due à l’usage prolongé des béquilles chez un soldat atteint de monoplégie crurale hystérique. Société de Neurol., 1915.
Moricand, I. Note on a case of bilateral radial paralysis due to prolonged use of crutches in a soldier with hysterical crural monoplegia. Neurological Society, 1915.
Morcelli, Arturo. (Psychiatry of War.) Boll. d. r. Accad. med. di Genova, 1916, v. 31, p. 65.
Morcelli, Arturo. (Psychiatry of War.) Bull. d. r. Accad. med. di Genova, 1916, v. 31, p. 65.
Morselli, A. Sui fenomeni fisio-patologici da emozione massime in rapporto alla neurologia di guerra. Quaderni di psichiat., Genova, 1916, v. 3, pp. 206-214.
Morselli, A. On the physiological and pathological phenomena caused by extreme emotions in relation to war neurology. Psychiatric Notebooks, Genoa, 1916, vol. 3, pp. 206-214.
Morselli, A. Sugli stati confusionali psichici da guerra. Quaderna di psichiat., Genova, 1917, iv, 45-52.
Morselli, A. On War-Induced Confused Mental States. Psychiatric Notebook, Genoa, 1917, iv, 45-52.
Morselli, A. Sopra le sindromi emotive di guerra. Rev. di patol. nerv., Firenze, 1917, v. 22, pp. 329-336.
Morselli, A. On the Emotional Syndromes of War. Rev. of Nervous Pathology, Florence, 1917, v. 22, pp. 329-336.
Mosny, E. La rééducation professionelle et la réadaptation au travail. Ann. d’Hyg., Par., 1915, v. 23, pp. 317-339.
Mosny, E. Professional rehabilitation and work reintegration. Ann. d’Hyg., Par., 1915, v. 23, pp. 317-339.
Mosquet, P. et Schwartz, Anselme. The immediate treatment of head injuries from projectiles. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 278-283.
Mosquet, P. and Schwartz, Anselme. The immediate treatment of head injuries caused by projectiles. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 278-283.
Mott, F. W. The microscopic examination of the brains of two men dead of commotio cerebri (shell shock) without visible external injury, Ibid., 612-615, 1 pl.
Mott, F. W. The microscopic examination of the brains of two men who died from commotio cerebri (shell shock) without any visible external injuries, Ibid., 612-615, 1 pl.
Mott, F. W. Psychic mechanism of the voice in relation to the emotions. Brit. M. J. Lond., 1915, ii, pp. 845-847.
Mott, F. W. The psychological mechanism of the voice concerning emotions. Brit. M. J. Lond., 1915, ii, pp. 845-847.
Mott, F. W. Discussion on shell shock without visible signs of injury. Proc. Roy. Soc. Med. Lond., 1915-16, v. 9 (sec. psychiat. and neurol.), pp. 1-44.
Mott, F. W. Discussion on shell shock without visible signs of injury. Proc. Roy. Soc. Med. Lond., 1915-16, v. 9 (sec. psychiat. and neurol.), pp. 1-44.
Mott, F. W. The effects of high explosives upon the central nervous system. Tr. M. Soc. Lond., 1915-16, xxxix, 157-226, 11 pl. Also Lancet, Lond., 1916, i, 331, 545.
Mott, F. W. The impact of high explosives on the central nervous system. Tr. M. Soc. Lond., 1915-16, xxxix, 157-226, 11 pl. Also Lancet, Lond., 1916, i, 331, 545.
Mott, F. W. The Lettsomian lectures on the effects of high explosives upon the central nervous system. Lancet, Lond., 1916, i, v. 190, pp. 331-338, pp. 441-449, pp. 545-553; also Tr. Med. Soc. Lond., 1915-16, v. 39, pp. 157-226.
Mott, F. W. The Lettsomian lectures on the effects of high explosives on the central nervous system. Lancet, London, 1916, i, v. 190, pp. 331-338, pp. 441-449, pp. 545-553; also Transactions of the Medical Society of London, 1915-16, v. 39, pp. 157-226.
Mott, F. W. Mental hygiene in shell shock. J. M. Sc., Lond., 1917, v. 63, pp. 467-488.
Mott, F. W. Mental hygiene in shell shock. J. M. Sc., Lond., 1917, v. 63, pp. 467-488.
Mott, F. W. 1. On war psychoneurosis. 2. The psychology of soldiers’ dreams. Lancet, Lond., 1918, i, pp. 169-177.
Mott, F. W. 1. On war psychoneurosis. 2. The psychology of soldiers’ dreams. Lancet, Lond., 1918, i, pp. 169-177.
Mott, F. W. Punctiform hemorrhages of the brain in gas poisoning. Brit. Med. Jour., 1917, i, 637.
Mott, F. W. Small bleeding spots in the brain due to gas poisoning. Brit. Med. Jour., 1917, i, 637.
Mott, F. W. The Chadwick Lectures on mental hygiene and shell shock during and after the war. Brit. M. J., Lond., 1917, ii, 39-42.
Mott, F. W. The Chadwick Lectures on mental health and shell shock during and after the war. Brit. M. J., Lond., 1917, ii, 39-42.
Mott, F. W. War psychoneurosis. Lancet, Lon., 1918, i, 127, 177.
Mott, F. W. War psychoneurosis. Lancet, Lon., 1918, i, 127, 177.
Mougeot, A. and Duverger. Bradycardie et réflexe oculocardiaque dans les traumatismes oculaires, crâniens, encéphaliques. Presse méd., Par., 1917, v. 25, pp. 730-732.
Mougeot, A. and Duverger. Bradycardia and oculocardiac reflex in eye, skull, and brain injuries. Medical Press, Paris, 1917, vol. 25, pp. 730-732.
Moure, E. J. Paralysies faciales de la guerre. Presse méd., Par., 1916, v. 24, pp. 161-164.
Moure, E. J. Facial paralysis from the war. Med Press, Paris, 1916, v. 24, pp. 161-164.
Moure et Pietri. L’organe de l’audition pendant la guerre. Arch. de méd. et de pharm. mil., Par., 1916, v. 65, pp. 809-837; and 1916, v. 66, pp. 167-186.
Moure and Pietri. The organ of hearing during the war. Arch. de méd. et de pharm. mil., Paris, 1916, vol. 65, pp. 809-837; and 1916, vol. 66, pp. 167-186.
Mouriquand. Sur quelques maladies simulées. Vomissements pseudoporracés. Lyon méd., 1917, v. 126, pp. 276-278.
Mouriquand. On Some Faked Illnesses. Pseudopore-like Vomiting. Lyon méd., 1917, v. 126, pp. 276-278.
Moutier, François. Recherches sur les troubles labyrinthiques chez les commotionnés et blessés du crâne. Rev. neurol., Par., 1916, v. 23, pp. 9-15.
Moutier, François. Research on labyrinthine disorders in those who have suffered concussions and skull injuries. Neurol. Rev., Paris, 1916, vol. 23, pp. 9-15.
Moynihan, Berkley. On injuries to the peripheral nerves and their treatment. Brit. M. J., 1917, ii, pp. 571-574.
Moynihan, Berkley. On injuries to the peripheral nerves and their treatment. Brit. M. J., 1917, ii, pp. 571-574.
Moynihan, Berkley. Injuries to the peripheral nerves and their treatment. Brit. Med. Jour., 1917, ii, 571.
Moynihan, Berkley. Injuries to the peripheral nerves and their treatment. Brit. Med. Jour., 1917, ii, 571.
Muenzer, Arthur. Die Psyche des Verwundeten. Berl. klin. Wchnschr., 1915, v. 52, pp. 234-235.
Muenzer, Arthur. The Psyche of the Wounded. Berl. klin. Wchnschr., 1915, v. 52, pp. 234-235.
Muirhead, I. B. Shock and the soldier. Lancet, Lond., 1916, i, p. 1021.
Muirhead, I. B. Shock and the soldier. Lancet, London, 1916, 1, p. 1021.
Müller. Typhuspsychose. Deutsche med. Wchnschr., 1915, Berl. u. Leipz., v. 41, pp. 331-332.
Müller. Typhus psychosis. German medical weekly, 1915, Berlin and Leipzig, v. 41, pp. 331-332.
Myerhof, M. Night-blindness as a war disease. Am. J. Ophth., St. Louis, 1916, p. 139.
Myerhof, M. Night blindness as a war-related condition. Am. J. Ophth., St. Louis, 1916, p. 139.
Myers, Charles S. Contributions to the study of shell shock. Lancet, Lon., 1916, ii, 461.
Myers, Charles S. Contributions to the study of shell shock. Lancet, Lon., 1916, ii, 461.
Myers, Charles S. Shell shock. Three cases of loss of memory, vision, smell and taste. Lancet, Lond., 1915, i, pp. 316-320.
Myers, Charles S. Shell shock. Three cases of memory loss, and loss of vision, smell, and taste. Lancet, London, 1915, i, pp. 316-320.
Myers, Charles S. Shell shock. An account of certain cases treated by hypnosis. Lancet, Lond., 1916, i, pp. 65-69; also J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 642-655.
Myers, Charles S. Shell shock. A report on specific cases treated with hypnosis. Lancet, London, 1916, i, pp. 65-69; also J. Roy. Army Med. Corps, London, 1916, v. 26, pp. 642-655.
Myers, Charles S. Shell shock. Certain disorders of cutaneous sensibility. Lancet, Lond., 1916, i, pp. 608; also J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 782-797.
Myers, Charles S. Shell shock. Some disorders of skin sensitivity. Lancet, London, 1916, i, pp. 608; also Journal of the Royal Army Medical Corps, London, 1916, v. 26, pp. 782-797.
Myers, Charles S. Shell shock. Certain disorders of speech,—their causation and their relation to malingering. Lancet, Lond., 1916, ii, pp. 461-467; also J. Roy. Army Med. Corps, Lond., 1916, v. 27, pp. 561-582.
Myers, Charles S. Shell shock. Some speech disorders—their causes and connection to faking. Lancet, London, 1916, ii, pp. 461-467; also J. Roy. Army Med. Corps, London, 1916, v. 27, pp. 561-582.
Naccarati, Sante. Medical organization of the Italian army; the neuropsychiatric service. Jour. A. M. A., 1918, lxxi, 1477.
Naccarati, Sante. Medical organization of the Italian army; the neuropsychiatric service. JAMA, 1918, 71, 1477.
Nägeli, O. Ueber die Entschädigung der Kriegsneurosen. Med. Cor.-Bl. d. würtemb. ärztl. Landesver., Stuttg., 1916, v. 86, No. 5.
Nägeli, O. On the Compensation for War Neuroses. Med. Cor.-Bl. d. würtemb. ärztl. Landesver., Stuttg., 1916, v. 86, No. 5.
Nägeli, O. Zur Frage der traumatischen Kriegsneurosen im besonderer Berucksichtigung der Oppenheim’schen Auffassungen. Neurol. Centralbl., Leipz., 1916, v. 35, No. 12.
Nägeli, O. On the issue of traumatic war neuroses, with particular consideration of Oppenheim’s views. Neurol. Centralbl., Leipzig, 1916, v. 35, No. 12.
Nägeli, O. Schlussfolgerungen für die Art der Abfindung der Kriegsneurosen. Ztschr. f. ärztl. Fortbldg., Nr. 8, 1918.
Nägeli, O. Conclusions on the Compensation for War Neuroses. Journal of Medical Progress, No. 8, 1918.
Nageotte, J. Le processus de la cicatrisation des nerfs. Rev. Neurol., July, 1915.
Nageotte, J. The process of nerve healing. Rev. Neurol., July, 1915.
Nash, E. H. Education of the left hand of disabled sailors and soldiers. Lancet, Lond., 1917, v. 1, p. 964.
Nash, E. H. Training the left hand of disabled sailors and soldiers. Lancet, Lond., 1917, v. 1, p. 964.
Natalelli and Roger, H. Erythèmes de la face provoqués pour simuler un érysipèle. Arch. de méd. et pharm. mil., Par., 1916-17, lxvi, 547.
Natalelli and Roger, H. Facial rashes created to mimic erysipelas. Arch. de méd. et pharm. mil., Par., 1916-17, lxvi, 547.
Naville, F. Le traitement et la guérison des psychonévroses de guerre invétérés à l’hôpital Saint-André de Salins. Corr.-Bl. f. Schweizer Aerzte, Nr. 25, 1918.
Naville, F. The treatment and healing of chronic war psychoneuroses at Saint-André Hospital in Salins. Corr.-Bl. f. Schweizer Aerzte, No. 25, 1918.
Necessité de créer des établissements spéciaux destinés aux invalides nerveux. Rev. neurol. Par., 1916, v. 23, pp. 593-594.
Need to create special facilities for those with nervous disabilities. Rev. neurol. Par., 1916, v. 23, pp. 593-594.
Necessité des services de psychiatrie et de médecine légale aux armées. Caducée, Par., 1916, v. 16, pp. 43-45.
Need for psychiatric and forensic medicine services in the military. Caducée, Par., 1916, v. 16, pp. 43-45.
Necessité de traiter les plicatures vertébrales (camptocormies) dans les centres neurologiques. Rev. Neurol. Par., 1917, v. 24, p. 137.
Need to treat spinal flexures (camptocormies) in neurological centers. Rev. Neurol. Par., 1917, v. 24, p. 137.
Negro, C. Annotazione di neurologia di guerra. Gior. d. r. Accad. di med. di Torino, 1916, v. 22, pp. 377-389.
Negro, C. Annotation on War Neurology. Journal of the Royal Academy of Medicine of Turin, 1916, vol. 22, pp. 377-389.
Neiding, M. N. (Nervous phenomena accompanying poisoning by asphyxiating gases). Russk. Vrach., Petrogr., 1917, v. 16, p. 397.
Neiding, M. N. (Nervous phenomena that occur with poisoning from asphyxiating gases). Russk. Vrach., Petrogr., 1917, v. 16, p. 397.
Neilson, W. A. The Training School of Psychiatric Social Work at Smith College. I. Educational Significance of the Course. Mental Hygiene, II, October, 1918.
Neilson, W. A. The Training School of Psychiatric Social Work at Smith College. I. Educational Importance of the Course. Mental Hygiene, II, October, 1918.
Nepper et Vallée. Recherches comparatives sur les impotences fonctionnelles dues aux lésions osseuses et articulaires (ankyloses et résections) du membre supérieur. Paris méd., 1916 (Part. méd.), v. 21, pp. 86-92.
Nepper et Vallée. Comparative studies on functional disabilities caused by bone and joint lesions (ankyloses and resections) of the upper limb. Paris méd., 1916 (Part. méd.), v. 21, pp. 86-92.
Néri, V. Moyen pour découvrir la simulation de la sciatique. Presse méd., Par., 1917, v. 25, p. 64.
Néri, V. Method for discovering the simulation of sciatica. Medical Press, Paris, 1917, vol. 25, p. 64.
Néri, V. Les petits signes électriques de la sciatique. Presse méd., Par., 1917, v. 25, pp. 466-468.
Néri, V. The small electrical signs of sciatica. Medical Press, Paris, 1917, v. 25, pp. 466-468.
Nervöse Disposition. Med. Cor. Bl. d. Württemb. ärztl. Landesver., Stuttg., 1916, v. 86, p. 42.
Nervous disposition. Med. Cor. Bl. d. Württemb. ärztl. Landesver., Stuttg., 1916, v. 86, p. 42.
Nervous and mental disease among soldiers. N. Y. Med. Jour., 1917, cvi, 1043.
Nervous and mental illness in soldiers. N. Y. Med. Jour., 1917, cvi, 1043.
Nervous temperament in war. Brit. Med. Jour., 1918, i, 649.
Nervous temperament in war. Brit. Med. Jour., 1918, i, 649.
Netter, F. L’épilepsie généralisée consécutive aux traumatismes de guerre crânio-cérébraux. Thèses de Paris. 1917-8, No. 9.
Netter, F. Generalized epilepsy following cranio-cerebral war injuries. Paris Theses. 1917-8, No. 9.
Neumann, E. Psychologische Beobachtungen im Felde. Neurol. Centralbl., 1914, v. 33, pp. 1243-1245.
Neumann, E. Psychological Observations in the Field. Neurol. Centralbl., 1914, v. 33, pp. 1243-1245.
Neurasthenia and shell shock. Lancet, Lond., 1916, i, p. 627.
Neurasthenia and shell shock. Lancet, London, 1916, 1, p. 627.
Neurologie de Guerre. Presse Méd., Par., 1917, v. 25, pp. 217-221.
Neurology of War. Medical Press, Paris, 1917, vol. 25, pp. 217-221.
Neutra, W. Einige Bemerkungen über die Beurteilung und Behandlung der Kriegsneurosen. Wien. klin. Wchnschr., 1916, v. 29, p. 1253.
Neutra, W. Some Observations on the Assessment and Treatment of War Neuroses. Wien. klin. Wchnschr., 1916, v. 29, p. 1253.
Neutra, W. Wien. klin. Wchnschr., 1917, 30, 1198-9.
Neutra, W. Wien. klin. Wchnschr., 1917, 30, 1198-9.
Névrite irradiante et paralysies ou contractures d’ordre réflexe. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 457-460.
Radiant neuritis and reflex paralysis or contractions. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 457-460.
Nicolai, George F. Biology of War. Century Co., 1918.
Nicolai, George F. Biology of War. Century Co., 1918.
Niessl von Mayendorf. Ueber pathologische Zitterformen zur Kriegszeit. Münch. med. Wchnschr., 1916, v. 63, p. 323.
Niessl von Mayendorf. On pathological tremors during wartime. Münch. med. Wchnschr., 1916, v. 63, p. 323.
Nikitina-Pakhorzkaya, T. P. (Case of choreo-athetosis of war-traumatic origin). J. Nevropat. i Psikhiat.… Korsakova, Mosk., 1915-16, v. 15, pp. 436-444.
Nikitina-Pakhorzkaya, T. P. (Case of choreo-athetosis from war trauma). J. Nevropat. i Psikhiat.… Korsakova, Mosk., 1915-16, v. 15, pp. 436-444.
Nissl. Ueber den Stand der Hysterielehre mit besonderer Berücksichtigung der Kriegserfahrungen. Berl. klin. Wchnschr., 1916, v. 53, p. 232.
Nissl. On the Status of Hysteria Theory with Particular Attention to War Experiences. Berl. klin. Wchnschr., 1916, v. 53, p. 232.
Noehte. Nystagmus bei Verletzungen des Fusses der II. Stirnhirnwindung. Deut. Med. Woch., 1915, xli, 1217.
Noehte. Nystagmus with injuries to the foot of the II. frontal lobe. Deut. Med. Woch., 1915, xli, 1217.
Nöica, (de Bucarest.) Sur la contracture dans les paraplégies spasmodiques. Rev. neurol., Par., 1916, v. 23, pp. 257-263.
Nöica, (de Bucarest.) On contractures in spastic paraplegia. Rev. neurol., Par., 1916, v. 23, pp. 257-263.
Nonne, M. Soll man wieder “traumatische Neurose” bei Kriegsverletzten diagnostizieren? Med. Klin., Berl. u. Wien, 1915, v. 112, pp. 849-854; also pp. 948-949.
Nonne, M. Should we diagnose "traumatic neurosis" in war veterans again? Med. Klin., Berl. u. Wien, 1915, v. 112, pp. 849-854; also pp. 948-949.
Nonne, M. Zur therapeutischen Verwendung der Hypnose bei Fällen von Kriegshysterie. Med. Klin., Berl. u. Wien, 1915, v. 112, pp. 1391-1396.
Nonne, M. On the therapeutic use of hypnosis in cases of war hysteria. Med. Klin., Berlin and Vienna, 1915, vol. 112, pp. 1391-1396.
Nonne, M. Fälle von Kriegsverwundeten. Neurol. Centralbl., 1915, v. 34, pp. 41-46.
Nonne, M. Cases of War Injuries. Neurol. Centralbl., 1915, v. 34, pp. 41-46.
Nonne, M. Demonstration von Nervenkriegsverletzungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 317-321.
Nonne, M. Demonstration of Nerve War Injuries. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 317-321.
Nonne, M. Ueber Neurosen und Hysterie bei Soldaten. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 408-409.
Nonne, M. On Neuroses and Hysteria in Soldiers. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 408-409.
Nonne, M. Kriegsverletzungen. Ztschr. f. d. ges. Neurol. u. Psychiat., Berl. u. Leipz., 1914-15, v. 11, pp. 198-200.
Nonne, M. War Injuries. Journal of General Neurology and Psychiatry, Berlin and Leipzig, 1914-15, v. 11, pp. 198-200.
Nonne, M. Ueber Polyneuritis gemischter Nerven bei neurasthenischen Kriegsteilnehmern. Deutsche Ztschr. f. Nervenh., Leipz., 1915, v. 53, pp. 464-469.
Nonne, M. On polyneuritis of mixed nerves in neurasthenic war participants. German Journal of Neurology, Leipzig, 1915, v. 53, pp. 464-469.
Nonne, M. Hysterie bei Soldaten. Ztschr. f. d. ges. Neurol. u. Psychiat., Berl. u. Leipz., 1914-15, v. 11, pp. 421-422.
Nonne, M. Hysteria in Soldiers. Journal for General Neurology and Psychiatry, Berlin and Leipzig, 1914-15, vol. 11, pp. 421-422.
Nonne, M. Zur therapeutischen Werth der Hypnose bei Fällen im Kriegshysterie. München. med. Wchnschr., 1915, v. 62, p. 1579.
Nonne, M. On the therapeutic value of hypnosis in cases of war hysteria. Munich. Med. Weekly, 1915, v. 62, p. 1579.
Nonne, M. Nervenverletzungen und Erkrankungen im Kriege. (Abstract). Deutsche med. Wchnschr., Berl., u. Leipz., 1915, v. 41, pp. 573-574.
Nonne, M. Nerve Injuries and Diseases in War. (Abstract). German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, pp. 573-574.
Nonne, M. Nervenkriegsverletzungen. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 695.
Nonne, M. Nerve war injuries. German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, p. 695.
Nonne, M. Hypnose bei Kriegshysterie. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, pp. 1587-1588.
Nonne, M. Hypnosis in War Hysteria. German Medical Weekly, Berlin and Leipzig, 1915, v. 412, pp. 1587-1588.
Nordman, Charles. Psychose post-typhique chez un adulte avec évolution probable vers la démence précoce. Ann. méd.-psychol., Par., 1916-17, v. 7, pp. 493-498.
Nordman, Charles. Post-typhoid psychosis in an adult with a probable progression towards early dementia. Ann. méd.-psychol., Paris, 1916-17, vol. 7, pp. 493-498.
Nordmann et Bonhomme. De l’utilisation des indisciplinés en temps de guerre. Ann. méd. psychol., Par., 1916-17, v. 32, pp. 490-493; also pp. 519-524.
Nordmann and Bonhomme. On the use of the undisciplined during wartime. Ann. méd. psychol., Paris, 1916-17, vol. 32, pp. 490-493; also pp. 519-524.
Norman, Hubert J. Some neuroses of the war. Rev. of Clark., J. Ment. Sc., Lond., 1917, v. 63, pp. 119-121.
Norman, Hubert J. Some neuroses of the war. Rev. of Clark., J. Ment. Sc., Lond., 1917, v. 63, pp. 119-121.
Notes on British military medical arrangements; work in the restoration and reëducation of disabled soldiers; treatment of cases of heart disease; military orthopedic hospitals. Mod. Hosp., St. Louis, 1917, v. 9, p. 293.
Notes on British military medical arrangements; work in the recovery and rehabilitation of disabled soldiers; treatment of heart disease cases; military orthopedic hospitals. Mod. Hosp., St. Louis, 1917, v. 9, p. 293.
Notes on hydrological treatment for wounded soldiers and sailors; with a list of the British spas and health resorts and the disorders which they benefit. Lond., 1915, Adlard and Son, 20, p. 9.
Notes on water therapy for injured soldiers and sailors; including a list of British spas and health resorts and the conditions they help. Lond., 1915, Adlard and Son, 20, p. 9.
Nouvelle Jeanne d’Arc. Ann. méd. psychol., Par., 1914-1915, p. 422.
New Joan of Arc. Ann. méd. psychol., Paris, 1914-1915, p. 422.
Nuthall, A. W. Three cases of gunshot wound of the superior longitudinal sinus. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 235-240.
Nuthall, A. W. Three cases of gunshot wounds to the superior longitudinal sinus. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 235-240.
Nunneley, P. P. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (Sect. Balneol.), pp. 30-34.
Nunneley, P. P. Treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (Sect. Balneol.), pp. 30-34.
Nyns, Adrien. La rééducation professionnelle d’après les variétés d’impotence. Paris méd., 1916, v. 21, pp. 493-496.
Nyns, Adrien. Professional rehabilitation based on kinds of incapacity. Paris méd., 1916, v. 21, pp. 493-496.
Obendorf, C. P. Traumatic hysteria. N. Y. Med. Jour., 1917, cvi, 874.
Obendorf, C. P. Traumatic hysteria. N. Y. Med. Jour., 1917, cvi, 874.
Oloff. Bemerkenswerte Fälle von Verwundung des Sehorgans. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, pp. 1190-1192.
Oloff. Notable cases of injury to the eye. German Med. Weekly, Berlin and Leipzig, 1915, v. 412, pp. 1190-1192.
O’Malley, J. F. Functional aphonia. Proc. Roy. Soc. Med., Lond., 1914-15, v. 8 (Sect. Laryng.), p. 116.
O’Malley, J. F. Functional aphonia. Proc. Roy. Soc. Med., Lond., 1914-15, v. 8 (Sect. Laryng.), p. 116.
O’Malley, J. F. Warfare neuroses of the throat and ear. Lancet, Lond., 1916, i, 1080.
O’Malley, J. F. War-related mental health issues concerning the throat and ear. Lancet, London, 1916, i, 1080.
Ombredanne, L. and Ledoux-Lebard, R. Localisation et extraction des projectiles. 1917, Paris, Masson et Cie.
Ombredanne, L. and Ledoux-Lebard, R. Localization and extraction of projectiles. 1917, Paris, Masson et Cie.
Oppenheim, H. Zur Kriegsneurologie. Berl. klin. Wchnschr., 1914, No. 48, pp. 1853-1856.
Oppenheim, H. War Neurology. Berl. klin. Wchnschr., 1914, No. 48, pp. 1853-1856.
Oppenheim, H. Krankendemonstrationen zur Kriegsneurologie. Discussion Rothmann-Cohn, Toby. Berl. klin. Wchnschr., 1915, v. 421, p. 168.
Oppenheim, H. Demonstrations of Illness in War Neurology. Discussion Rothmann-Cohn, Toby. Berl. klin. Wchnschr., 1915, v. 421, p. 168.
Oppenheim, H. Der Krieg und die traumatischen Neurosen. Berl. klin. Wchnschr., 1915, v. 52, pp. 257-261.
Oppenheim, H. War and Traumatic Neuroses. Berl. klin. Wchnschr., 1915, v. 52, pp. 257-261.
Oppenheim, H. Kriegsneurosen. Med. Klin., Berl. u. Wien. 1915, v. 11, p. 147.
Oppenheim, H. War Neuroses. Med. Klin., Berlin and Vienna. 1915, vol. 11, p. 147.
Oppenheim, H. Bemerkung zu dem Aufsatze Nonnes: Soll man wieder traumatische Neurose bei Kriegsverletzten diagnostizieren? Med. Klin., Berl. [958]u. Wien, 1915, v. 112, pp. 920-921.
Oppenheim, H. Comment on Nonne's article: Should we diagnose traumatic neurosis in war casualties again? Med. Klin., Berl. [958]u. Wien, 1915, v. 112, pp. 920-921.
Oppenheim, H. Ueber Hemiplegia spinalis mit homolateraler Hemianästhesie. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 49-51.
Oppenheim, H. On spinal hemiplegia with homolateral hemianesthesia. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 49-51.
Oppenheim, H. Zur traumatischen Neurosen im Kriege. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 514-518.
Oppenheim, H. On Traumatic Neuroses in War. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 514-518.
Oppenheim, H. Die Neurosen nach Kriegsverletzungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 810-813.
Oppenheim, H. The Neuroses Following War Injuries. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 810-813.
Oppenheim, H. Der Krieg und die traumatischen Neurosen. 1915, Berlin, A. Herschwald.
Oppenheim, H. The War and Traumatic Neuroses. 1915, Berlin, A. Herschwald.
Oppenheim, H. Ueber Kriegsverletzungen des peripheren und zentralen Nervensystems. Ztschr. f. ärztl. Fortbild., Jena, 1915, No. 4, pp. 97-106.
Oppenheim, H. On War Injuries of the Peripheral and Central Nervous System. Journal of Medical Continuing Education, Jena, 1915, No. 4, pp. 97-106.
Oppenheim, H. (Discussion of Lewandowsky) Ueber Kriegsverletzungen des Nervensystems. Deutsche med. Wchnschr., 1915, v. 411, p. 89.
Oppenheim, H. (Discussion of Lewandowsky) On War Injuries of the Nervous System. German Medical Weekly, 1915, v. 411, p. 89.
Oppenheim, H. (Further discussion) Ueber die traumatischen Neurosen. Neurol. Centralbl., Leipz., 1916, v. 35, No. 13.
Oppenheim, H. (Further discussion) On Traumatic Neuroses. Neurol. Centralbl., Leipzig, 1916, vol. 35, No. 13.
Oppenheim, H. “Alloparalgie.” Neurol. Centralbl., Leipz., 1916, No. 21. Rev. Berl. klin. Wchnschr., 1916, No. 48, p. 1302.
Oppenheim, H. “Alloparalgie.” Neurological Central Journal, Leipzig, 1916, No. 21. Review of Berlin Clinical Weekly, 1916, No. 48, p. 1302.
Oppenheim, H. Zur Frage der traumatischen Neurosen. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, pp. 1567-1570.
Oppenheim, H. On the Question of Traumatic Neuroses. German Medical Weekly, Leipzig and Berlin, 1916, vol. 42, pp. 1567-1570.
Oppenheim, H. Die Neurosen infolge von Kriegsverletzungen. 1916, Berlin, S. Karger.
Oppenheim, H. The Neuroses Resulting from War Injuries. 1916, Berlin, S. Karger.
Oppenheim, H. (Aussprache zum Vortrag von Singer: Zitterer im Felde.) Neurol. Centralbl., 37, Nr. 12, 1918.
Oppenheim, H. (Speech on Singer's lecture: Quakers in the field.) Neurol. Centralbl., 37, No. 12, 1918.
Oppenheim, Nonne, Gaupp, etc. Neurosen nach Kriegsschädigungen. Münch. med. Wchnschr., 1916, No. 45, p. 1594.
Oppenheim, Nonne, Gaupp, etc. Neurosis after war injuries. Münch. med. Wchnschr., 1916, No. 45, p. 1594.
Oppenheim, R. L’amnésie traumatique chez les blessés. Progrès méd., Par., 1917, 3. s., xxxii, 189, 199.
Oppenheim, R. Traumatic amnesia in the injured. Med. Progress, Par., 1917, 3. s., xxxii, 189, 199.
Oppenheim, R. Le pouls, la tension artérielle et le réflexe oculocardiaque dans les suites éloignées des traumatismes crâniens. Progrès méd., Par., 1917, No. 7, pp. 53-55.
Oppenheim, R. The pulse, blood pressure, and oculocardiac reflex in the remote aftermath of head injuries. Med. Progress, Paris, 1917, No. 7, pp. 53-55.
Oppenheim, R. et Hallez, G. L. La diplégie faciale traumatique. Paris méd., 1917, v. 23, pp. 136-139.
Oppenheim, R. et Hallez, G. L. Traumatic facial diplegia. Paris méd., 1917, v. 23, pp. 136-139.
Organic lesions in shell shock. Bos. Med. and Surg. Jour., 1918, 24.
Organic lesions in shell shock. Bos. Med. and Surg. Jour., 1918, 24.
Organisation des asiles publics d’aliénés de la Seine après la guerre. Progrès méd., Par., 1917, v. 32, p. 366.
Organization of public asylums for the mentally ill in Seine after the war. Med. Progress, Paris, 1917, v. 32, p. 366.
Ormond, A. W. Short notes on 30 cases of blinded soldiers during the present war. Guy’s Hos. Gaz., Lond., 1915, May 22.
Ormond, A. W. Brief notes on 30 cases of blinded soldiers during the current war. Guy’s Hos. Gaz., Lond., 1915, May 22.
Ormond, A. W. Treatment of “concussion blindness.” Guy’s Hos. Gaz., Lond., 1915, v. 30, pp. 99-101.
Ormond, A. W. Treatment of “concussion blindness.” Guy’s Hospital Gazette, London, 1915, vol. 30, pp. 99-101.
Ormond, A. W. Treatment of “concussion blindness.” J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 43-49.
Ormond, A. W. Treatment of “concussion blindness.” J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 43-49.
Orth. Simulation. Dementia Praecox. Deutsche med. Wchnschr., 1915, v. 412, p. 936.
Orth. Simulation. Dementia Praecox. German Medical Weekly, 1915, v. 412, p. 936.
Osier, Sir William. Science and war. 1915, Oxford, Clarendon Press, 40 p., 8o.
Osier, Sir William. Science and War. 1915, Oxford, Clarendon Press, 40 p., 8o.
Osnos. (Case of nervous and mental disease during the war.) Nevropat. i Psikhiat., Korsakova, Mosk., 1915-16, v. 15, p. 143.
Osnos. (Case of nervous and mental illness during the war.) Nevropat. i Psikhiat., Korsakova, Mosk., 1915-16, v. 15, p. 143.
Oudet, L. Deux épreuves pratiques pour dépister les simulateurs de surdité. Presse méd., Par., 1917, xxv, annexes, 515.
Oudet, L. Two practical tests to identify those faking hearing loss. Medical Press, Paris, 1917, xxv, annexes, 515.
Overbeck-Wright, A. W. A case of malingering. Indian M. Gaz., Calcutta, 1915, v. 50, p. 334.
Overbeck-Wright, A. W. A case of faking illness. Indian M. Gaz., Calcutta, 1915, v. 50, p. 334.
Overbeek, H. J. Psychoses in war and wounds of the nervous system. Mil.-geneesk Tijdschr., Haarlem, 1915, xix, 209-216.
Overbeek, H. J. Psychoses in war and wounds of the nervous system. Mil.-geneesk Tijdschr., Haarlem, 1915, xix, 209-216.
Overbeek, H. J. Mobilisatie-neurosen en Psychosen. Nedrl. Tijdschr. v. Geneesk., Amst., 1917, v. 1, pp. 1617-1620.
Overbeek, H. J. Mobilization Neuroses and Psychoses. Dutch Journal of Medicine, Amsterdam, 1917, vol. 1, pp. 1617-1620.
Pachantoni, D. Paralysies multiples des nerfs crâniens par “vent d’obus.” Rev. méd. de la Suisse Rom., Genève, 1917, v. 37, pp. 226-229.
Pachantoni, D. Multiple cranial nerve palsies caused by “shell shock.” Rev. méd. de la Suisse Rom., Geneva, 1917, v. 37, pp. 226-229.
Pactet, M. La réforme des paralytiques généraux. J. de méd. de Bordeaux, 1917, v. 88, pp. 163-164.
Pactet, M. The Reform of General Paralysis. J. de méd. de Bordeaux, 1917, v. 88, pp. 163-164.
Pactet et Bonhomme. Deux observations de peur invincible chez des combattants. Ann. méd. psychol., Par., 1917, v. 73, pp. 375-380.
Pactet et Bonhomme. Two observations of an unstoppable fear in combatants. Ann. méd. psychol., Par., 1917, v. 73, pp. 375-380.
Padovani, E. Note e osservazioni dalle zone di guerra. Rassegna di studi psichiat., Siena, 1915, v. 5, pp. 342-346.
Padovani, E. Notes and Observations from War Zones. Psychiatric Review, Siena, 1915, v. 5, pp. 342-346.
Pangon, J. et Gate, J. Accidents syphilitiques et dermatoses simulés. Lyon méd., 1916, v. 125, pp. 216-219.
Pangon, J. and Gate, J. Syphilitic accidents and simulated dermatoses. Lyon méd., 1916, v. 125, pp. 216-219.
Pansky. Contribution à l’étude de la psychonévrose consécutive à la contusion et aux incidents des combats. Nouvelles médicales de Minsk, No. 3, 1915.
Pansky. Contribution to the Study of Psychoneurosis Following Concussions and Combat Incidents. Medical News from Minsk, No. 3, 1915.
Pansky. Contribution à la connaissance des névroses de contusion compliquées par des lésions organiques du système nerveux. Gazette médicale russe, No. 9, 1915.
Pansky. Contribution to the understanding of concussion neuroses complicated by organic lesions of the nervous system. Russian Medical Gazette, No. 9, 1915.
Parhon, C. J. et Vasiliu, Mme. Eug. Troubles sensitifs et moteurs (tremblement à type parkinsonien; phénomènes paralytiques) à topographie surtout cubitale, du côté droit, à la suite d’une lésion crânienne dans la région pariétale gauche. Rev. Neurol., Par., 1917, v. 24, pp. 156-162.
Parhon, C. J. and Vasiliu, Mme. Eug. Sensory and motor issues (tremors similar to Parkinson's; paralysis phenomena) primarily affecting the cubital area on the right side, following a cranial injury in the left parietal region. Rev. Neurol., Paris, 1917, vol. 24, pp. 156-162.
Parkinson. An inquiry into the cardiac disabilities in soldiers on active service. Lancet, Lond., 1916, ii, pp. 133-138.
Parkinson. A study on heart issues in soldiers on active duty. Lancet, Lond., 1916, ii, pp. 133-138.
Parkinson, J. Digitalis in soldiers with cardiac symptoms and a frequent pulse. Heart, 1917, vi, 321.
Parkinson, J. Digitalis in soldiers with heart issues and a rapid pulse. Heart, 1917, vi, 321.
Parkinson, J. and Drury, A. N. P-R interval before and after exercise in cases of “soldier’s heart.” Heart, 1917, vi, 337.
Parkinson, J. and Drury, A. N. P-R interval before and after exercise in cases of "soldier's heart." Heart, 1917, vi, 337.
Parkinson, J. Pulse rate on standing and on slight exertion in healthy men and in cases of “soldier’s heart.”
Parkinson, J. Heart rate when standing and during light exercise in healthy men and in cases of "soldier's heart."
Parkinson, J. and Koefod, H. Immediate effect of cigarette smoking on healthy men and on cases of “soldier’s heart.” Lancet, Lon., 1917, ii, 232.
Parkinson, J. and Koefod, H. Immediate impact of cigarette smoking on healthy men and on cases of “soldier’s heart.” Lancet, Lon., 1917, ii, 232.
Paris. Aliénation mentale et état de guerre, leurs rapports. Société de médecine de Nancy, 1915.
Paris. Mental alienation and the state of war, their connections. Medical Society of Nancy, 1915.
Pariset. Le massage chirurgical, méthode d’enseignement rapide à l’usage des infirmiers militaires. Presse méd., Par., 1915, v. 23, pp. 97-100.
Pariset. Surgical massage, a quick teaching method for military nurses. Med. Press, Par., 1915, v. 23, pp. 97-100.
Parsons, J. H. The psychology of traumatic amblyopia following explosions of shell. Proc. Roy. Soc. Med., Lond., 1914-15, v. 8, (neurol. sect.), pp. 55-68; also Lancet, Lond., 1915, i, p. 697.
Parsons, J. H. The psychology of traumatic amblyopia after shell explosions. Proc. Roy. Soc. Med., Lond., 1914-15, v. 8, (neurol. sect.), pp. 55-68; also Lancet, Lond., 1915, i, p. 697.
Pascha, Wieting. Leitsätze der funktionellen Nachbehandlung kriegschirurgischer Schäden. Samml. klin. Vortr. n. F., Leipz., 1915, pp. 123-165.
Pascha, Wieting. Guidelines for the Functional Aftercare of War-Surgery Injuries. Collection of Clinical Lectures n. F., Leipzig, 1915, pp. 123-165.
Pastini, C. Commozione dei centri nervosi da esplosione violenta a breve distanza. (Influenza del delore finio sullo stato psichico). Riv. di patol. neu., Firenze, 1916, v. 21, pp. 433-438.
Pastini, C. Nervous center disturbance from violent explosions at close range. (Influence of finite pain on the mental state). Journal of Neuropathology, Florence, 1916, v. 21, pp. 433-438.
Paton, Stewart. Mobilizing the brains of the nation. Mental Hyg., Concord, N. H., v. 1, pp. 334-344.
Paton, Stewart. Engaging the minds of the nation. Mental Hyg., Concord, N. H., v. 1, pp. 334-344.
Paton, Stewart. Effects of low oxygen pressure on the personality of the aviator. Jour. A. M. A., 1918, lxxi, 1399.
Paton, Stewart. Effects of low oxygen pressure on the personality of the aviator. Jour. A. M. A., 1918, lxxi, 1399.
Paton, Stewart, MacLake, William, Hamilton, Arthur S. Personality Studies and the Personal Equation of the Aviator. Mental Hygiene, II, October, 1918.
Paton, Stewart, MacLake, William, Hamilton, Arthur S. Personality Studies and the Personal Equation of the Aviator. Mental Hygiene, II, October, 1918.
Paul, B. Beobachtungen über Nachtblindheit im Felde. München med. Wchnschr., 1915, v. 62, pp. 1548-1550.
Paul, B. Observations on Night Blindness in the Field. Munich Med. Wkly., 1915, v. 62, pp. 1548-1550.
Paul, B. Zur Therapie der Nachtblindheit. Rev. München med. Wchnschr., 1915, v. 622, p. 1707.
Paul, B. On the Treatment of Night Blindness. Rev. Münch. Medizin Wochenschr., 1915, v. 622, p. 1707.
Paulian, Démétre. Hémiparaplégie fonctionnelle gauche avec troubles de la sensibilité et abolition du réflexe cutané plantaire. Rev. neurol., Par., 1914-15, v. 222, pp. 431-433.
Paulian, Démétre. Left functional hemiplegia with sensory disturbances and loss of plantar skin reflex. Rev. neurol., Par., 1914-15, v. 222, pp. 431-433.
Paulian. Sur quelques cas d’hémiplégie cérébelleuse. Rev. neurol., Par., 1916, v. 23, pp. 18-20.
Paulian. On some cases of cerebellar hemiplegia. Neurological Review, Paris, 1916, vol. 23, pp. 18-20.
Payne, Charles R. and Jelliffe, S. E. War neuroses and psychoneuroses. Jour. Nerv. and Ment. Dis., 1918, xlviii, 246, 325.
Payne, Charles R. and Jelliffe, S. E. War-related neuroses and psychoneuroses. Journal of Nervous and Mental Disease, 1918, volume 48, pages 246, 325.
Pegler, L. H. Case of nervous or functional aphonia. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sec. Laryngol.), pp. 118-120.
Pegler, L. H. Case of nervous or functional aphonia. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (sec. Laryngol.), pp. 118-120.
Pelissier, A. et Borel, P. Hémiplégie spinale avec troubles de la sensibilité homolatéraux. Rev. neurol., Par., 1914-15, v. 222, pp. 125-127.
Pelissier, A. and Borel, P. Spinal hemiplegia with sensory disturbances on the same side. Neurology Review, Paris, 1914-15, v. 222, pp. 125-127.
Pellacani, Giuseppe. Sulla nosografia di alcune neuropatie caratterizzati da sindromi accessuali epilettoidi. Riv. di patol. nerv., Firenze, 1917, v. 22, pp. 131-172.
Pellacani, Giuseppe. On the nosography of some neuropathies characterized by epileptoid accessory syndromes. Journal of Nervous Pathology, Florence, 1917, vol. 22, pp. 131-172.
Pelz. Ueber hysterische Aphonen. (Arch. f. Psych., 1916, v. 57, No. 2, pp. 445-465.) Rev. Berl. klin. Wchnschr., 1916, No. 6, p. 434.
Pelz. On Hysterical Aphonia. (Arch. for Psych., 1916, v. 57, No. 2, pp. 445-465.) Rev. Berl. Clin. Weekly, 1916, No. 6, p. 434.
Pemberton, Hugh S. The psychology of traumatic amblyopia following the explosion of shells. Lancet, Lond., 1915, i, p. 967.
Pemberton, Hugh S. The psychology of traumatic amblyopia after shell explosions. Lancet, Lond., 1915, i, p. 967.
Penhallow, Dunlap P. Mutism and deafness due to emotional shock and etherization. Boston M. and S. J., 1916, 174, p. 1311.
Penhallow, Dunlap P. Loss of speech and hearing from emotional trauma and anesthesia. Boston M. and S. J., 1916, 174, p. 1311.
Penhallow, Dunlap P. Military surgery. 1916, London, Henry Frowde, pp. 367-398.
Penhallow, Dunlap P. Military surgery. 1916, London, Henry Frowde, pp. 367-398.
Pensions for Mentally Incapacitated. Brit. M. J., Lond., 1915, i, p. 820.
Pensions for Mentally Incapacitated. Brit. M. J., Lond., 1915, i, p. 820.
Perls, W. Beitrag zur Symptomatologie und Therapie der Schädelschüsse (Nach Beobachtungen in den Heimatlazaretten). Bruns’ Kriegschir. Hefte d. Beitr. z. Klin. Chir., Tübing, 1917, 105, 435.
Perls, W. Contribution to the Symptomatology and Treatment of Skull Gunshot Wounds (Based on Observations in Local Military Hospitals). Bruns' War Surgery. Contributions to Clinical Surgery, Tübingen, 1917, 105, 435.
Peterson, Joseph and David, Quentin J. The psychology of handling men in the army. Perine Book Co., 1918.
Peterson, Joseph and David, Quentin J. The psychology of handling men in the army. Perine Book Co., 1918.
Pfersdorff. Ueber paranoide Erkrankungen im Felde. Neurol. Centralbl. Nr. 16, 1918.
Pfersdorff. On paranoid disorders in the field. Neurol. Centralbl. No. 16, 1918.
Pflugradt, R. Ueber Schädeldefekte. Ein Beitrag zur Behandlung der Schädelschüsse in den Heimatlazaretten. Bruns’ Kriegschir. Hefte d.
Pflugradt, R. On Skull Defects. A Contribution to the Treatment of Gunshot Wounds to the Skull in Military Hospitals. Bruns’ War Surgery. Issues of the
Pförringer. Psychische Erkrankungen nach Typhus (Abstract). Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 331.
Pförringer. Mental illnesses following typhus (Abstract). German medical journal, Berlin and Leipzig, 1915, v. 41, p. 331.
Phocas, D. Accident produit par l’éboulement. Bull. et mém. Soc. de chir. de Par., 1916, v. 42, pp. 2839-2840.
Phocas, D. Accident caused by a landslide. Bull. et mém. Soc. de chir. de Par., 1916, v. 42, pp. 2839-2840.
Phocas, et Gutman, R. A. L’hémiplégie pleurale traumatique. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 329-335.
Phocas, et Gutman, R. A. Traumatic pleural hemiplegia. Bull. et mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 329-335.
Physical qualities of aviators. Jour. A. M. A., 1918, lxiv, 37.
Physical qualities of aviators. Jour. A. M. A., 1918, lxiv, 37.
Physical tests for airmen are novel and exciting. N. Y. Med. Jour., 1918, cviii, 690.
Physical tests for pilots are new and exciting. N. Y. Med. Jour., 1918, cviii, 690.
Physical treatment for disabled soldiers. Lancet, Lond., 1916, i, pp. 691-694.
Physical therapy for injured soldiers. Lancet, Lond., 1916, i, pp. 691-694.
Pick, A. Der Krieg und die Reservekräfte des Nervenssystem. Samml. zwangl. Abhandl. a. d. Geb. d. Nerv. u. Geisteskr., Halle a. S., 1916, v. 11, No. 5, pp. 1-27.
Pick, A. The War and the Reserve Forces of the Nervous System. Collection of Compulsory Papers on the Field of Nervous and Mental Disorders, Halle a. S., 1916, v. 11, No. 5, pp. 1-27.
Pick, W. (Simulation of venereal disease.) Med. Klin., Berl. u. Wien, 1917, No. 6, pp. 148-151. Rev. J. Roy. Nav. M. Serv., Lond., 1917, Oct., pp. 497-498.
Pick, W. (Simulation of sexually transmitted diseases.) Med. Klin., Berl. u. Wien, 1917, No. 6, pp. 148-151. Rev. J. Roy. Nav. M. Serv., Lond., 1917, Oct., pp. 497-498.
Piéron, Henri. “Hyperesthésie” signifie toujours “Hyperalgésie.” Rev. neurol., Par., 1914-15, v. 221, pp. 947-951.
Piéron, Henri. “Hyperesthesia” always means “Hyperalgesia.” Rev. neurol., Par., 1914-15, v. 221, pp. 947-951.
Pierre-Robin, Dr. Mécanothérapie fonctionnelle. J. de méd. et de chir. prat., Par., 1916, v. 87, pp. 309-320.
Pierre-Robin, Dr. Functional Mechanotherapy. J. of Med. and Surgery Pract., Par., 1916, v. 87, pp. 309-320.
Pighini, G. Il servizio neuro-psichiatrico nella zona di guerra. Ann. di manic. prov. di Perugia (1915), 1917, v. 9, pp. 49-55.
Pighini, G. The neuro-psychiatric service in the war zone. Ann. di manic. prov. di Perugia (1915), 1917, v. 9, pp. 49-55.
Pighini, G. Contributo alla clinica e patogenesi delle psiconeurosi emotive osservate al fronte. Riv. sper. di freniat., Reggio-Emilia, 1916-17, xiii, 298-343.
Pighini, G. Contribution to the clinic and pathogenesis of emotional psychoneuroses observed at the front. Riv. sper. di freniat., Reggio-Emilia, 1916-17, xiii, 298-343.
Pilca, A. Zur Aetiologie und Behandlung der progressiven Analyse nebst einigen kriegspsychiatrischen Erfahrungen. Wien. klin. Wchnschr., 1915, v. 28, p. 633.
Pilca, A. On the Etiology and Treatment of Progressive Analysis Along with Some Wartime Psychiatric Experiences. Wien. klin. Wchnschr., 1915, v. 28, p. 633.
Piotrowski. Traumatische Neurosen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 591-592.
Piotrowski. Traumatic Neuroses. Neurol. Centralbl., Leipzig, 1915, vol. 34, pp. 591-592.
Pitres, A. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 470-471.
Pitres, A. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, pp. 470-471.
Pitres, A. Étude sur les principales causes d’erreurs de diagnostic dans les paralysies des membres consécutives aux blessures des nerfs. J. de méd. de Bordeaux, 1917, v. 88, pp. 239-247.
Pitres, A. Study on the main causes of diagnostic errors in limb paralysis due to nerve injuries. J. de méd. de Bordeaux, 1917, v. 88, pp. 239-247.
Pitres, A. La valeur des signes cliniques permettant de reconnaître dans les blessures des nerfs périphériques: A. La section complète du nerf; B. La restauration fonctionnelle. Soc. de Neurol. April 6, 1916. Revue Neurol. April-May, 1916.
Pitres, A. The significance of clinical signs that help identify peripheral nerve injuries: A. Complete nerve section; B. Functional restoration. Soc. de Neurol. April 6, 1916. Revue Neurol. April-May, 1916.
Pitres, A. Sur les processus histologiques qui president à la cicatrisation et à la restauration fonctionnelle des nerfs traumatisés. Journ. de Méd. de Bordeaux, Dec., 1915.
Pitres, A. On the histological processes involved in the healing and functional restoration of injured nerves. Journal of Medicine of Bordeaux, Dec., 1915.
Pitres, A. et Marchand, L. Quelques observations de syndrômes commotionnels simulant des affections organiques du système nerveux central (méningite, paralysie générale, lésions cérébelleuses, sclérose en plaques, tabes). Rev. neurol., Par., 1916, v. 23, pp. 298-311.
Pitres, A. and Marchand, L. Some observations of concussion syndromes that resemble organic diseases of the central nervous system (meningitis, general paralysis, cerebellar lesions, multiple sclerosis, tabes). Rev. neurol., Paris, 1916, v. 23, pp. 298-311.
Placido, C. Delinquenza militaire in pace ed in guerra. Ann. di manic. prov. di Perugia (1915), 1917, v. pp. 25-47.
Placido, C. Military delinquency in peace and war. Annals of provincial madness of Perugia (1915), 1917, v. pp. 25-47.
Plantier. Une application médicale de l’esperanto comme moyen de rééducation psychique. Paris méd. (Part. paraméd.), 1916, v. 22, pp. 195-197.
Plantier. A medical application of Esperanto as a means of mental rehabilitation. Paris méd. (Part. paraméd.), 1916, v. 22, pp. 195-197.
Podiapolsky. Application de la suggestion hypnotique dans la pratique des hôpitaux militaires. (Jour. de neurop. et psychiat. de S. S., Korsakoff, 1916, fasc. 2), Rev. neurol., Par., 1917, v. 24, pp. 477-478.
Podiapolsky. Application of hypnotic suggestion in the practice of military hospitals. (Journal of Neurology and Psychiatry of S. S., Korsakoff, 1916, issue 2), Rev. Neurol., Paris, 1917, vol. 24, pp. 477-478.
Podiapolsky, P. P. La suggestion hypnotique à l’hôpital de camp. Paris méd., 1917, No. 34, pp. 165-170.
Podiapolsky, P. P. Hypnotic suggestion at the field hospital. Paris méd., 1917, No. 34, pp. 165-170.
Podmaniczky, B. T. von. Die Lumbalpunktion als therapeutische Hilfsmittel bei gewissen Formen der Kriegshysterie. Wien. klin. Wchnschr. 1916, xxix, 1396.
Podmaniczky, B. T. von. The lumbar puncture as a therapeutic tool for certain types of war hysteria. Vienna. Clinical Weekly. 1916, xxix, 1396.
Podmaniczky, T. Einige interessante Fälle von Kriegsneurosen. Pest. med.-chir. Presse, Budapest, 1915, v. 51, p. 81.
Podmaniczky, T. Some Interesting Cases of War Neuroses. Pest. med.-chir. Press, Budapest, 1915, v. 51, p. 81.
Podmaniczky. Die Lumbalpunktion als therapeutische Hilfsmittel bei gewissen Formen von Kriegshysterie. Wien. klin. Wchnschr., 1916, v. 29, No. 44, p. 1396.
Podmaniczky. The lumbar puncture as a therapeutic tool for certain forms of war hysteria. Vienna. clinical weekly, 1916, v. 29, No. 44, p. 1396.
Pollosson et Collet. Epilepsie partielle continue d’origine traumatique. Trépanation. Guérison. Rev. neurol., Par., 1914-15, v. 222, pp. 291-295.
Pollosson and Collet. Ongoing partial epilepsy from trauma. Trepanation. Recovery. Rev. neurol., Paris, 1914-15, vol. 222, pp. 291-295.
Popoff, N. F. (Rare case of self injury to avoid military service). Voyenno Med. J., Petrogr., 1915, v. 242, med. spec. pt., pp. 288-292.
Popoff, N. F. (Uncommon case of self-harm to evade military service). Military Medicine Journal, Petrograd, 1915, vol. 242, medical special part, pp. 288-292.
Poppelreuter, Walter. Psychische Ausfallserscheinungen nach Hirnverletzungen. Aertzl. Centralbl. Zeit., 1915, v. 27, p. 152. Also München. med. Wchnschr., 1915, v. 62, pp. 489-491.
Poppelreuter, Walter. Psychological Symptoms Following Brain Injuries. Aertzl. Centralbl. Zeit., 1915, v. 27, p. 152. Also München. med. Wchnschr., 1915, v. 62, pp. 489-491.
Porak, René. Nouveaux signes physiologiques des psychonévroses de guerre. Compt. rend. Soc. de biol., Par., 1916, v. 792, pp. 630-634.
Porak, René. New Physiological Signs of War Psychoneuroses. Compt. rend. Soc. de biol., Paris, 1916, v. 792, pp. 630-634.
Porot, A. Les bases de l’expertise mentale dans les bataillons d’Afrique et les groupes spéciaux en temps de guerre. Rev. neurol., Par., 1916, v. 23, pp. 24-27.
Porot, A. The fundamentals of mental expertise in African battalions and special groups during wartime. Rev. neurol., Par., 1916, v. 23, pp. 24-27.
Porot, A. Les bases de l’expertise mentale dans les bataillons d’Afrique et des groupes spéciaux en temps de guerre. (Aptitude au service et responsabilité). Caducée, Par., 1916, v. 16, pp. 85-87.
Porot, A. The Foundations of Mental Expertise in African Battalions and Special Groups During Wartime. (Fitness for Service and Responsibility). Caducée, Par., 1916, v. 16, pp. 85-87.
Porot, A. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol., Par., 1916, v. 29, pp. 603-605.
Porot, A. On the nerve accidents caused by the detonation of large explosives. Neurology Review, Paris, 1916, vol. 29, pp. 603-605.
Porot and Gutmann, R. A. Centre neurologique de la 19e région (Alger). Rev. neurol., Par., 1916, v. 23, pp. 726-733.
Porot and Gutmann, R. A. Neurological Center of the 19e Region (Algiers). Rev. neurol., Paris, 1916, v. 23, pp. 726-733.
Porot et Gutmann. Les psychoses du paludisme. Paris méd., 1917, 7, 518-22.
Porot and Gutmann. The Psychoses of Malaria. Paris Méd., 1917, 7, 518-22.
Porter, W. T. and Emerson, E. Wound shock and the vasomotor center. Bos. M. and S. J., 1918, clxxix, 275.
Porter, W. T. and Emerson, E. Wound shock and the vasomotor center. Bos. M. and S. J., 1918, clxxix, 275.
Porter, William Townsend. Shock at the Front. Atlantic Monthly Press, 1918.
Porter, William Townsend. Shock at the Front. Atlantic Monthly Press, 1918.
Porter, W. T. Shock at the front. Boston M. and S. J., 1916, v. 175, pp. 854-858.
Porter, W. T. Shock at the front. Boston M. and S. J., 1916, v. 175, pp. 854-858.
Porter, William T. Traumatic shock. Bos. M. & S. J., 1918, clxxviii, 657.
Porter, William T. Traumatic shock. Bos. M. & S. J., 1918, 178, 657.
Porter, W. T. Further observations on shock at the front. Boston M. and S. J., 1917, v. 177, pp. 327-328.
Porter, W. T. Additional observations on shock at the front. Boston M. and S. J., 1917, v. 177, pp. 327-328.
Previously insane recruit. N. York M. J., 1916, v. 104, p. 857.
Previously insane recruit. N. York M. J., 1916, v. 104, p. 857.
Pribram, B. O. Erfolge und Misserfolge bei der operativen Behandlung der Schädelschüsse, besonders der Durchschüsse. Wien. klin. Wchnschr., 1915, v. 28, pp. 1025-1028.
Pribram, B. O. Successes and failures in the surgical treatment of skull wounds, especially penetrative injuries. Wien. klin. Wchnschr., 1915, v. 28, pp. 1025-1028.
Priest, E. Massage in the after-treatment of the wounded. Lancet, Lond., 1915, ii, p. 1052.
Priest, E. Massage in the aftercare of the wounded. Lancet, Lond., 1915, ii, p. 1052.
Prince, Morton. Prevention of so-called shell shock. J. Am. M. Ass., Chicago, 1917, v. 69, pp. 726-727.
Prince, Morton. Prevention of so-called shell shock. J. Am. M. Ass., Chicago, 1917, v. 69, pp. 726-727.
Privat, J. La mécanothérapie de guerre. Bull. Acad. de méd., Par., 1915, v. 73, pp. 411-416. Also Rev. gén. de clin. et de thérap., Par., 1915, v. 29, pp. 219, 234, 250, 266.
Privat, J. The mechanotherapy of war. Bull. Acad. de méd., Paris, 1915, vol. 73, pp. 411-416. Also in Rev. gén. de clin. et de thérap., Paris, 1915, vol. 29, pp. 219, 234, 250, 266.
Privat, J. La méchanothérapie de guerre. 1915, Paris, A. Maloine.
Privat, J. The War Mechanotherapy. 1915, Paris, A. Maloine.
Problem, (The) of the insane sailor and soldier. Lancet, Lond., 1917, ii, 612.
Problem of the Insane Sailor and Soldier. Lancet, London, 1917, ii, 612.
Proctor, A. P. Three cases of concussion aphasia: treatment by general anesthesia. Lancet, Lond., 1915, ii, p. 977.
Proctor, A. P. Three cases of concussion aphasia: treatment using general anesthesia. Lancet, Lond., 1915, ii, p. 977.
Prozoroff, L. A. (Organization of aid to insane soldiers). Psikhiat. Gaz., Petrogr., 1915, v. 2, p. 167.
Prozoroff, L. A. (Organization of support for mentally ill soldiers). Psychiatric Gazette, St. Petersburg, 1915, vol. 2, p. 167.
Prusenko, A. I. (Conditions of nervous and insane soldiers in the Caucasian front). Psikhiat., Mosk., 1915, v. 9, pp. 291-293.
Prusenko, A. I. (Conditions of nervous and insane soldiers on the Caucasian front). Psikhiat., Mosk., 1915, v. 9, pp. 291-293.
Pruvost, L. P. Les débiles mentaux à la guerre. Leur utilisation. Thèses de Paris, 1915-16, v. 10, No. 23.
Pruvost, L. P. The Mentally Disabled in War. Their Use. Theses of Paris, 1915-16, v. 10, No. 23.
Psyche und Kriegserfahrungen. Discussion von Bonhoeffer, Meyer. Berl. klin. Wchnschr., 1916, v. 532, pp. 1206-1207.
Mental Health and War Experiences. Discussion by Bonhoeffer, Meyer. Berl. klin. Wchnschr., 1916, v. 532, pp. 1206-1207.
Psychiatrie und Krieg. Psychiat. neurol. Wchnschr. Halle a. S., 1914-1915, v. 16, pp. 284-285.
Psychiatry and War. Psychiatr. neurol. Wchnschr. Halle a. S., 1914-1915, v. 16, pp. 284-285.
Psychological Examining in the Army. Amer. Jour. Med. Sc., 1918, clv, 128.
Psychological Examining in the Army. Am. J. Med. Sci., 1918, clv, 128.
Purser, F. C. Shell shock. Report of Section of Medicine of the Royal Academy of Medicine in Ireland. Brit. M. J., 1917, ii, p. 81.
Purser, F. C. Shell shock. Report of the Section of Medicine of the Royal Academy of Medicine in Ireland. Brit. M. J., 1917, ii, p. 81.
Purser, F. C. Shell shock. Dublin J. M. Sc., 1917, v. 144, p. 206.
Purser, F. C. Shell shock. Dublin J. M. Sc., 1917, v. 144, p. 206.
Quaet-Faslem. Die allgemeine nervöse Erschöpfung. Psychiat.-neurol. Wochnsch., 19, 1917-8.
Quaet-Faslem. General nervous exhaustion. Psychiat.-neurol. Weekly, 19, 1917-8.
Quidot, L. Deux épreuves pratiques pour dépister les simulateurs de surdité. Presse méd., Par., 1917, v. 25, p. 515.
Quidot, L. Two practical tests to identify fakers of hearing loss. Med. Press, Paris, 1917, vol. 25, p. 515.
Rablossky. (War hysteria, traumatic neuroses). Wien. klin. Wchnschr., 1916, v. 29, p. 1616.
Rablossky. (War hysteria, traumatic neuroses). Vienna Clinical Weekly, 1916, v. 29, p. 1616.
Radcliffe, Frank. Hydrotherapy as an agent in the treatment of convalescents. Brit. M. J., Lond., 1916, ii, p. 554.
Radcliffe, Frank. Hydrotherapy as a tool in the recovery of convalescents. Brit. M. J., Lond., 1916, ii, p. 554.
Raether, M. Neurosen-Heilungen nach der “Kaufmann-Methode.” Arch. f. Psychiat., Berl., 1917, 57, 489-518.
Raether, M. Neurotherapy using the “Kaufmann Method.” Arch. f. Psychiatry, Berl., 1917, 57, 489-518.
Raether, M. Ueber psychogene “Ischias-Rheumatismus” und “Wirbelsäulenerkrankungen.” Arch. f. Psychiat., Berl., 1917, 57, 772-791.
Raether, M. On psychogenic "sciatica-rheumatism" and "spinal diseases." Arch. f. Psychiat., Berl., 1917, 57, 772-791.
Raeuber. Die Beschäftigung und Arbeitverwendung der Kriegsbeschädigten auf Grund eigener Erfahrung. Ztschr. f. Med. Beamte, Berl., 1917, 30, 441.
Raeuber. The Employment and Work Utilization of War Veterans Based on Personal Experience. Journal of Medical Officials, Berlin, 1917, 30, 441.
Raffaele, R. Considerazioni su una centuria di casi di patomimia cutanea (durante un anno dell’attuale campagna, 1915-16). Gior. ital. d. mal. ven., Milano, 1916, li, 415-420.
Raffaele, R. Thoughts on a hundred cases of skin pathomimesis (during a year of the current campaign, 1915-16). Italian Journal of Venereal Diseases, Milan, 1916, li, 415-420.
Raffegeau, du Vésinet. Note sur un cas de séton du crâne par balle de mitrailleuse. Ann. méd.-psychol., Par., 1917, v. 73, pp. 101-104.
Raffegeau, du Vésinet. Note on a case of skull seton from a machine gun bullet. Ann. méd.-psychol., Par., 1917, v. 73, pp. 101-104.
Raimann, E. Ein Fall von “Kriegspsychose.” Wien. klin. Wchnschr., 1916, v. 29, pp. 42-47.
Raimann, E. A Case of "War Psychosis." Wien. klin. Wchnschr., 1916, v. 29, pp. 42-47.
Ramond et De la Grandière. Troubles de la sensibilité au cours de la diphthérie. L’hystérie diphthérique. Presse méd., Par., 1916, v. 24, p. 523.
Ramond and De la Grandière. Sensitivity issues during diphtheria. Diphtheric hysteria. Med. Press, Paris, 1916, vol. 24, p. 523.
Ramsay, A. M., Grant, Dundas, Whale, H. L., West, C. E. Injuries of eyes, nose, throat and ears. London, 1915, Oxford Press, 160 pp., 12o.
Ramsay, A. M., Grant, Dundas, Whale, H. L., West, C. E. Injuries of the eyes, nose, throat, and ears. London, 1915, Oxford Press, 160 pages, 12o.
Rautenberg, H. Wert der Abderhaldenschen Dialysieverfahrens für die Kriegspsychiatrie. Deutsche Mil. arztl. Ztschr., Berl., 1917, 46, 417-23.
Rautenberg, H. The value of the Abderhalden dialysis method for war psychiatry. German Military Medical Journal, Berlin, 1917, 46, 417-23.
Raujard, L. Les surdités par obusite. Bull. Acad. de méd. de Par., 1916, v. 75, pp. 195-198.
Raujard, L. Hearing Loss from Shell Shock. Bull. Acad. de méd. de Par., 1916, v. 75, pp. 195-198.
Ravaut, Paul. Les hémorragies internes produites par le choc vibratoire de l’explosif. Presse méd., Par., 1915, v. 23, p. 114.
Ravaut, Paul. Internal bleeding caused by the shock wave of explosives. Medical Press, Paris, 1915, vol. 23, p. 114.
Ravaut, Paul. Les blessures indirectes du système nerveux déterminés par le “vent de l’explosif.” Presse méd., Par., 1915, v. 23, pp. 313-315.
Ravaut, Paul. The indirect injuries of the nervous system caused by the "blast of the explosive." Medical Press, Paris, 1915, vol. 23, pp. 313-315.
Ravaut, Paul. Étude sur quelques manifestations nerveuses déterminés par le “vent de l’explosif.” Bull. Acad. de méd., Par., 1915, v. 73, pp. 717-720.
Ravaut, Paul. Study on some nerve manifestations caused by the "blast of the explosive." Bull. Acad. de méd., Par., 1915, v. 73, pp. 717-720.
Ravaut, P. et Reniac. Intoxication par les gaz asphyxiants; Diphthérie secondaire méconnue; Paralysie diphthérique généralisée avec réaction méningee. Bull. et mém. Soc. méd. des hôp. de Paris, 1917, 3 ser., 41, 1190-2.
Ravaut, P. and Reniac. Poisoning from asphyxiant gases; Secondary diphtheria not recognized; Widespread diphtheritic paralysis with meningeal reaction. Bull. et mém. Soc. méd. des hôp. de Paris, 1917, 3rd series, 41, 1190-2.
Rawling, L. Bathe. Surgery of the head. 1915, London, Henry Frowde.
Rawling, L. Bathe. Head Surgery. 1915, London, Henry Frowde.
Rawling, L. Bathe. Surgery of the Head. Oxford War Primers, 1915.
Rawling, L. Bathe. Surgery of the Head. Oxford War Primers, 1915.
Raynal, Albert J. L. La rééducation motrice chez les blessés de guerre. Thèses de la Faculté de Paris, 1915-16, v. 11.
Raynal, Albert J. L. Motor rehabilitation for war injuries. Theses from the Faculty of Paris, 1915-16, v. 11.
Raynaud. Contracture hystérique du membre supérieur droit avec oedème. Réunion médicale VI armée, 4 août, 1915, et Presse méd., 1915.
Raynaud. Hysterical contraction of the right upper limb with swelling. Medical meeting VI army, August 4, 1915, and Medical Press, 1915.
Raynier. Les états dépressifs et les états mélancoliques chez les militaires pendant la guerre. J. de méd. et de chir., 1915, Feb., v. 86.
Raynier. Depressive and melancholic states in soldiers during the war. J. of Med. and Surg., 1915, Feb., v. 86.
Raymond, Victor. Les déséquilibrés mentaux dans l’armée. Ann. d’hyg., Par., 1914, v. 22, pp. 305-330.
Raymond, Victor. The Mentally Imbalanced in the Army. Ann. d’hyg., Paris, 1914, v. 22, pp. 305-330.
Rebierre, Paul. Un centre psychiatrique d’armée. Arch. de méd. et pharm. mil., Par., 1916, v. 65, pp. 434-454.
Rebierre, Paul. A military psychiatric center. Arch. de méd. et pharm. mil., Par., 1916, v. 65, pp. 434-454.
Rebierre. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 473.
Rebierre. Discussion on how to deal with skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 473.
Rebierre. Sur les accidents nerveux determinés par la déflagration de fortes charges d’explosifs. Rev. neurol.. Par., 1916, v. 29, pp. 597-598.
Rebierre. On nerve accidents caused by the explosion of strong explosive charges. Neurology Review. Paris, 1916, v. 29, pp. 597-598.
Reconstruction hospitals and orthopedic surgery. Science, N. Y. and Lancaster, Pa., 1917, n. s., v. 46, p. 305.
Reconstruction hospitals and orthopedic surgery. Science, N. Y. and Lancaster, Pa., 1917, n. s., v. 46, p. 305.
Reconstruction Hospitals. Boston M. and S. J., 1917, i, p. 744.
Reconstruction Hospitals. Boston M. and S. J., 1917, i, p. 744.
Recherche de l’acide picrique dans les urines et dans les viscères. Soc. de méd. lég. de France, Bull., Par., 1916, v. 12, pp. 42-47.
Search for picric acid in urine and in the organs. Soc. de méd. lég. de France, Bull., Par., 1916, v. 12, pp. 42-47.
Redlich, Emil. Einige allgemeine Bemerkungen über den Krieg und unser Nervensystem. Med. Klin., Berl. u. Wien, 1915, v. 111, pp. 467-473.
Redlich, Emil. Some General Remarks on War and Our Nervous System. Med. Klin., Berl. and Wien, 1915, v. 111, pp. 467-473.
Redlich, Emil. Bemerkungen zur Aetiologie der Epilepsie mit besonderer Berücksichtigung der Frage einer “Kriegsepilepsie.” Wien. med. Wchnschr., Nr. 17, 1918.
Redlich, Emil. Remarks on the Etiology of Epilepsy with Special Consideration of the Question of “War Epilepsy.” Wien. med. Wchnschr., No. 17, 1918.
Rééducation fonctionnelle et rééducation professionnelle des blessés. (A symposium study), 1917, Paris, J. B. Baillière et Fils.
Functional rehabilitation and vocational rehabilitation of the injured. (A symposium study), 1917, Paris, J. B. Baillière et Fils.
Reeve, E. F. The treatment of functional contracture by fatigue. Lancet, Lond., 1917, ii, pp. 419-421.
Reeve, E. F. The treatment of functional contracture through fatigue. Lancet, Lond., 1917, ii, pp. 419-421.
Reformatski, N. N. (Care and evacuation of insane soldiers to the rear of the armies of the northwestern front). Russk. Vrach., Petrogr., 1915, v. 14, pp. 677-679.
Reformatski, N. N. (Care and evacuation of mentally ill soldiers to the rear of the armies of the northwestern front). Russk. Vrach., Petrogr., 1915, v. 14, pp. 677-679.
Reformatski, N. N. (Care and evacuation of insane soldiers from the active armies in the northwestern region). Russk. Vrach., Petrogr., 1916, v. 15, pp. 230-234.
Reformatski, N. N. (Care and evacuation of insane soldiers from the active armies in the northwestern region). Russk. Vrach., Petrograd, 1916, v. 15, pp. 230-234.
Reformatski, N. N. (Organization at the rear for the care and evacuation of insane soldiers in the northwestern front). Sovrem. Psikhiat., Mosk., 1915, v. 9, pp. 194-198.
Reformatski, N. N. (Organization at the back for the care and evacuation of mentally ill soldiers on the northwestern front). Modern Psychiatry, Moscow, 1915, vol. 9, pp. 194-198.
Reformatski, N. N. (Care and evacuation of insane warriors of the active army of the northwestern region). Sovrem. Psikhiat., Mosk., 1916, v. 10, pp. 118-128. Also Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 165-175.
Reformatski, N. N. (Care and evacuation of mentally ill soldiers in the active army of the northwestern region). Modern Psychiatry, Moscow, 1916, vol. 10, pp. 118-128. Also in Psychiatry Gazette, Petrograd, 1916, vol. 3, pp. 165-175.
Régis, E. Les troubles psychiques et neuro-psychiques de la guerre. Presse méd., Par., 1915, v. 23, pp. 177-179.
Régis, E. The Psychological and Neuropsychological Issues of War. Med Press, Paris, 1915, v. 23, pp. 177-179.
Régis, E. Psychic and neuro-psychic affections in war. Boston M. and S. J., 1916, v. 174, pp. 784-792.
Régis, E. Mental and neurological disorders in war. Boston M. and S. J., 1916, v. 174, pp. 784-792.
Régis, E. Les aliénés militaires internés du centre psychiatrique de Bordeaux. Statistique et commentaires. Caducée, Par., 1916, v. 16, pp. 55-59.
Régis, E. The military detainees in the psychiatric center of Bordeaux. Statistics and commentary. Caducée, Paris, 1916, vol. 16, pp. 55-59.
Régis et Hesnard. Un cas d’aphonie hystérique d’origine émotive. Le rôle pathogéne des émotions oniriques. Journal de Psychologie, mai-juin 1913.
Régis and Hesnard. A case of hysterical aphonia with an emotional origin. The pathogenic role of dream emotions. Journal of Psychology, May-June 1913.
Regnier, P. Organisation scientifique de la rééducation professionnelle des mutilés. Rev. scient., Par., 1916, v. 2, pp. 458-460.
Regnier, P. Scientific organization of vocational rehabilitation for the disabled. Sci. Rev., Paris, 1916, vol. 2, pp. 458-460.
Regnier, P. De la rééducation fonctionnelle des blessés. Rev. de chir., Par., 1916, 4. 35, pp. 668-696.
Regnier, P. On the functional rehabilitation of the injured. J. of Surgery, Paris, 1916, 4. 35, pp. 668-696.
Renaux, Jules. États confusionnels consécutifs aux commotions des batailles. (Thèse, Paris, 1915), Presse méd., Par., 1916, v. 24, p. 184.
Renaux, Jules. Confused states following battle concussions. (Thesis, Paris, 1915), Medical Press, Paris, 1916, v. 24, p. 184.
Renon, Louis. L’angoisse de guerre et son traitement. Bull. gén. de thérap., Par., 1915-16, v. 1681, pp. 785-791; also pp. 821-827.
Renon, Louis. The Anxiety of War and Its Treatment. Gen. Bull. of Therapy, Paris, 1915-16, v. 1681, pp. 785-791; also pp. 821-827.
Renon, Louis. L’angoisse de guerre et son traitement. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 41-43.
Renon, Louis. The Anxiety of War and Its Treatment. Gen. Rev. of Clin. and Therapy, Paris, 1916, vol. 30, pp. 41-43.
Repkewitz. Ueber die Simulation und Uebertreibung. Neurol. Centralbl., 37, Nr. 12, 1918.
Repkewitz. On Simulation and Exaggeration. Neurological Central Journal, 37, No. 12, 1918.
Report of Dr. Henry Carre. Glasgow District Mental Hospital, Brit. M. J., Lond., 1916, i, p. 148.
Report of Dr. Henry Carre. Glasgow District Mental Hospital, Brit. M. J., Lond., 1916, i, p. 148.
Report. War Disablement Committee. Use of Remedial Baths in connection with other physical methods in the treatment of disabled soldiers. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sec. Balneol.), pp. 78-80.
Report. War Disablement Committee. Use of Remedial Baths along with other physical therapies in the treatment of disabled soldiers. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sec. Balneol.), pp. 78-80.
Resch, H. Geisteskrankheiten und Krieg. Allg. Ztschr. f. Psychiat., Berl., 1915, v. 72, No. 2 and No. 3, pp. 121-133.
Resch, H. Mental Illness and War. Gen. J. Psychi., Berl., 1915, v. 72, No. 2 and No. 3, pp. 121-133.
Responsabilité des oeuvres de rééeducation des mutilés de guerre au point de vue des accidents. Ann. d’Hyg., Par., 1917, v. 25, pp. 190-192.
Responsibility for the rehabilitation of war mutilees in terms of accidents. Ann. d’Hyg., Paris, 1917, vol. 25, pp. 190-192.
Revault d’Allones, G. Le signe achilléen sensitif des affections du nerf sciatique. Press méd., Par., 1917, v. 25, pp. 351-352.
Revault d’Allones, G. The sensitive Achilles sign for affections of the sciatic nerve. Medical Press, Paris, 1917, vol. 25, pp. 351-352.
Richet, Ch. “Anesthésie” en dictionnaire de physiologie. Lyon méd., 1915, v. 124, p. 347.
Richet, Ch. “Anesthesia” in the dictionary of physiology. Lyon medical, 1915, v. 124, p. 347.
Richet, Ch. Le courage. Rev. sc., Par., 1916, ii, pp. 385-391.
Richet, Ch. Courage. Scientific Review, Paris, 1916, vol. 2, pp. 385-391.
Richet, Ch. Les évènements psychiques de la guerre. Un appel de M. Charles Richet aux soldats; avez-vous des pressentiments? Ann. d. sc. psych., Par., 1916, xxvi, 185-192.
Richet, Ch. The Psychic Events of War. A Call from Mr. Charles Richet to Soldiers; Do You Have Any Intuitions? Ann. d. sc. psych., Par., 1916, xxvi, 185-192.
Riddoch, George. Dissociation of visual perceptions due to occipital injuries with especial reference to appreciation of movement. Brain, Lond., 1917, v. 40, pp. 15-57.
Riddoch, George. Breakdown of visual perceptions from occipital injuries, focusing on the ability to perceive movement. Brain, Lond., 1917, v. 40, pp. 15-57.
Riddoch, George. On the relative perceptions of movement and a stationary object in certain visual disturbances due to occipital injuries. Proc. Roy. Soc. Med., Lond., 1917, v. 10, No. 3 (Sect. Neurol.), p. 13.
Riddoch, George. On how people perceive movement and stationary objects during specific visual disturbances caused by occipital injuries. Proc. Roy. Soc. Med., Lond., 1917, v. 10, No. 3 (Sect. Neurol.), p. 13.
Riebeth. Ueber Neurasthenie bei Kriegsteilnehmern. Psychiat.-neurol. Wchnschr., Halle a. S., 1915-16, v. 17, p. 71.
Riebeth. On Neurasthenia in War Participants. Psychiat.-neurol. Wchnschr., Halle a. S., 1915-16, v. 17, p. 71.
Rietschel, H. Die Kriegsenuresis. Münch. med. Wchnschr., Nr. 26, 1918.
Rietschel, H. The War Enuresis. Munich Medical Weekly, No. 26, 1918.
Riggall, Robert M. The treatment of neurasthenia by hypnotism. J. Roy. Nav. M. Serv., Lond., 1917, v. 3, pp. 190-194.
Riggall, Robert M. Treatment of neurasthenia with hypnotism. J. Roy. Nav. M. Serv., Lond., 1917, v. 3, pp. 190-194.
Rimbaud, L. À propos de la méthode de traitement des psychonévroses dite “du torpillage.” Marseille méd., 1916, v. 53, pp. 33-41.
Rimbaud, L. Regarding the method of treating psychoneuroses known as “torpedo therapy.” Marseille méd., 1916, v. 53, pp. 33-41.
Rimbaud, L. Le traitement des psychonévroses de guerre et des troubles nerveux dits “réflexes.” Marseille med., 1917, v. 54, pp. 817-829.
Rimbaud, L. The Treatment of War Psychoneuroses and So-Called "Reflex" Nervous Disorders. Marseille Med., 1917, v. 54, pp. 817-829.
Rimbaud, L. Les réflexes de percussion plantaire; leur valeur diagnostique. Presse méd., Par., 1917, v. 25, pp. 539-540.
Rimbaud, L. The reflexes of plantar percussion; their diagnostic value. Medical Press, Paris, 1917, vol. 25, pp. 539-540.
Rippon, T. S. Essential characteristics of successful and unsuccessful aviators. Lancet, Lon., 1918, ii, 411.
Rippon, T. S. Key traits of successful and unsuccessful pilots. Lancet, Lon., 1918, ii, 411.
Rivers, W. H. R. A case of claustrophobia. Lancet, Lond., 1917, v. 2, pp. 237-240.
Rivers, W. H. R. A case of claustrophobia. Lancet, London, 1917, vol. 2, pp. 237-240.
Rivers, W. H. R. Freud’s psychology of the unconscious. (Evidence afforded by the war.) Lancet, Lon., 1917, i, 912.
Rivers, W. H. R. Freud’s psychology of the unconscious. (Evidence provided by the war.) Lancet, Lon., 1917, i, 912.
Rivers, W. H. R. Repression of war experience. Proc., Roy. Soc. of Med., Lon., 1918, xi (Sec. of Psychiatry), 1.
Rivers, W. H. R. Repression of war experience. Proc., Roy. Soc. of Med., Lon., 1918, xi (Sec. of Psychiatry), 1.
Rivers, W. H. R. The repression of war experience. Lancet, Lond., 1918, i, pp. 173-177.
Rivers, W. H. R. The repression of war experience. Lancet, London, 1918, vol. 1, pp. 173-177.
Rivers, W. H. R. War neurosis and military training. Mental Hygiene, II, October, 1918.
Rivers, W. H. R. War trauma and military training. Mental Hygiene, II, October, 1918.
Roberts, John B. War surgery of the face. 1919.
Roberts, John B. Facial Surgery in War. 1919.
Robertson, George M. War and alcohol as exciting factors in the onset of insanity. Med. Officer, Lond., 1915, v. 14, pp. 283-284.
Robertson, George M. War and alcohol as thrilling contributors to the onset of mental illness. Med. Officer, Lond., 1915, v. 14, pp. 283-284.
Robin, Pierre. Méthode de prothèse fonctionelle. Caducée, Par., 1916, v. 16, pp. 35-40.
Robin, Pierre. Method of Functional Prosthesis. Caducée, Paris, 1916, vol. 16, pp. 35-40.
Roches, H. Louis. Extraction magnétique des projectiles intracérébraux. J. de Radiol. et d. electrol. Par., 1916, v. 2, pp. 165-172.
Roches, H. Louis. Magnetic extraction of intracerebral projectiles. J. de Radiol. et d. electrol. Par., 1916, v. 2, pp. 165-172.
Rochtein, I. D. Contribution à l’étude des soi-disant contusions de guerre et de leur traitement. Médecin russe pratique, No. 24, 1915.
Rochtein, I. D. Contribution to the study of so-called war contusions and their treatment. Practical Russian Medicine, No. 24, 1915.
Roemheld, L. Ueber homolaterale Hemiplegien nach Kopfverletzungen. München med. Wchnschr., 1915, v. 621, pp. 600-601.
Roemheld, L. On homolateral hemiplegia following head injuries. München medical weekly, 1915, vol. 621, pp. 600-601.
Roeper, E. Zur Prognose der Hirnschüsse. (Aus dem Marinelazarett Hamburg.) Münch. med. Wchnschr., 1917, 64. Feldartzl. Beil. 4 (Abstract in Centralbl. f. Chir., Leipz., 1917, 44, 1036).
Roeper, E. On the Prognosis of Brain Injuries. (From the Naval Hospital Hamburg.) Münch. med. Wchnschr., 1917, 64. Field Surgeon Supplement 4 (Abstract in Centralbl. f. Chir., Leipzig, 1917, 44, 1036).
Roger, H. Simulation des oreillons. Rev. gén. de clin. et de thérap., Par., 1916, xxx, 80.
Roger, H. Simulation of mumps. Gen. Rev. of Clin. and Therapy, Paris, 1916, xxx, 80.
Roger, H. Le choc nerveux. Presse méd., Par., 1916, v. 24, pp. 513-516.
Roger, H. Nervous Shock. Medical Press, Paris, 1916, vol. 24, pp. 513-516.
Roger, H. Les pseudo-érysipèles de la face provoqués. Marseille méd., 1916-17, liii, 785-800.
Roger, H. The pseudorhynochoses of the face caused. Marseille méd., 1916-17, liii, 785-800.
Roger, H. Deux cas de tétanos localisé post-sérique. Marseille méd., 1917, v. 54, pp. 353-363.
Roger, H. Two Cases of Localized Tetanus Post-Serum. Marseille Med., 1917, v. 54, pp. 353-363.
Rogues de Fursac, J. Un cas d’émotivité morbide chez un militaire. Rev. neurol., Par., 1914-15, v. 221, pp. 774-776.
Rogues de Fursac, J. A case of morbid emotionality in a soldier. Rev. neurol., Paris, 1914-15, v. 221, pp. 774-776.
Rôle de l’auto-intoxication dans la fatigue. Presse Méd., Par., 1917, v. 25, pp. 142-143 (or 102-103).
Role of self-poisoning in fatigue. Med Press, Paris, 1917, vol. 25, pp. 142-143 (or 102-103).
Romer, F. Mechano-therapy at the Corydon War Hospital. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 578-585.
Romer, F. Mechano-therapy at the Corydon War Hospital. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 578-585.
Roncoroni, L. Quattro casi di mutismo di guerra. Boll. d. Soc. med. in Parma, 1915, v. 8, pp. 114-117.
Roncoroni, L. Four Cases of War Mutism. Bulletin of the Medical Society of Parma, 1915, vol. 8, pp. 114-117.
Röper. Das Hamburger Marine-Lazarett. Neurol. Centralbl., Leipz., 1915, v. 34, 505-506.
Röper. The Hamburg Naval Hospital. Neurol. Centralbl., Leipzig, 1915, v. 34, 505-506.
Röper. Funktionelle Neurosen bei Kriegsnehmern. Deutsche mil.-ärtzl. Ztschr., Berl., 1915, Nos. 9-10, p. 752.
Röper. Functional neuroses in war veterans. German military medical journal, Berlin, 1915, Nos. 9-10, p. 752.
Roquette. Sur l’installation et le fonctionnement de l’hôpital-dépôt de convalescence Faucher. Arch. de méd. et pharm. mil., Par., 1914-15, v. 64, pp. 206-232.
Roquette. On the establishment and operation of the convalescent hospital depot Faucher. Arch. of military medicine and pharmacy, Paris, 1914-15, vol. 64, pp. 206-232.
Ross, T. A. Prevention of relapse of hysterical manifestations. Lancet, Lon., 1918, ii, 516.
Ross, T. A. Preventing the return of hysterical symptoms. Lancet, London, 1918, ii, 516.
Rosenbach. (Psychoses of war time.) Russk. Vrach., Petrogr., 1915, v. 14.
Rosenbach. (Psychoses of wartime.) Russian Doctor, Petrograd, 1915, vol. 14.
Rosanoff, A. J. First psychiatric experiences at the National Army Cantonment at Camp Upton, Long Island, N. Y. Med. Rec., N. Y., 1917, xcii, 877.
Rosanoff, A. J. First psychiatric experiences at the National Army Cantonment at Camp Upton, Long Island, N. Y. Med. Rec., N. Y., 1917, xcii, 877.
Rosanoff-Saloff, Mme. Considérations générales sur la camptocormie. N. Iconog. de la Salpêtrière, Par., 1916-17, v. 28, pp. 28-33.
Rosanoff-Saloff, Mme. General considerations on camptocormia. N. Iconog. de la Salpêtrière, Par., 1916-17, v. 28, pp. 28-33.
Rose, Felix. Le signe de fessier dans la névralgie sciatique. Presse méd., Par., 1917, v. 25, p. 319.
Rose, Felix. The Sign of the Buttock in Sciatic Neuralgia. Medical Press, Paris, 1917, vol. 25, p. 319.
Rose et Villandre. Cranioplastie cartilagineuse faite après trépanation pour épilepsie Jacksonienne. Lyon méd., 1916, v. 125, p. 348.
Rose et Villandre. Cartilaginous craniofacial surgery performed after trepanation for Jacksonian epilepsy. Lyon méd., 1916, v. 125, p. 348.
Rosenfeld. Ueber Kriegsneurosen, ihre Prognose und Behandlung. Arch. f. Psychiat., Berl., 1917, 57, 221-244.
Rosenfeld. On War Neuroses, Their Prognosis and Treatment. Archives of Psychiatry, Berlin, 1917, 57, 221-244.
Roth, E. Kriegsgefahr und Psyche. Aertztl. Sachverst.-Ztg., Berl., 1915, v. 21, pp. 1-3.
Roth, E. Danger of War and the Mind. Medical Expert Report, Berlin, 1915, vol. 21, pp. 1-3.
Rothacker, A. Einige Fälle von Hyperthyroidismus, darunter drei von akuten Basedow bei Kriegsteilnehmern zur Stutze der neurogenen Entstehung dieser Krankheit. Münch. med. Wchnschr., 1916, No. 3, pp. 99-101.
Rothacker, A. Some cases of hyperthyroidism, including three of acute Graves' disease in war participants as evidence for the neurogenic origins of this illness. Münch. med. Wchnschr., 1916, No. 3, pp. 99-101.
Rothmann, Max. Ueber isolierte Thermanalgesie eines Beines nach Schussverletzung des obersten Brustmarks. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 153-157.
Rothmann, Max. On Isolated Thermal Analgesia of a Leg After Gunshot Injury to the Upper Spinal Cord. Neurological Central Journal, Leipzig, 1915, vol. 34, pp. 153-157.
Rothmann, M. Zur Beseitigung psychogener Bewegungstörungen bei Soldaten in einer Sitzung. München med. Wchnschr., 1916, v. 64, No. 35.
Rothmann, M. On the Elimination of Psychogenic Movement Disorders in Soldiers in a Session. München med. Wchnschr., 1916, v. 64, No. 35.
Rottenstein. Les phlegmons provoqués. Marseille méd., 1916-17, lii, 801-807.
Rottenstein. The caused phlegmons. Marseille med., 1916-17, lii, 801-807.
Rouge, C. Influence de la guerre actuelle: (1) Sur le mouvement de la population de l’asile de Limoux du 2 août 1914 au 31 décembre 1915; (2) Sur les psychoses des aliénés internés pendant la même époque. Ann. méd.-psychol., Par., 1916, v. 7, p. 425.
Rouge, C. Influence of the current war: (1) On the movement of the population of the asylum in Limoux from August 2, 1914, to December 31, 1915; (2) On the psychoses of the mentally ill interned during the same period. Ann. méd.-psychol., Par., 1916, v. 7, p. 425.
Roussy, G. Accidents nerveux produits à distance par éclatement d’obus. Rev. neurol., Par., 1914-15, v. 222, pp. 216-217.
Roussy, G. Nervous accidents caused remotely by shell explosions. Rev. neurol., Par., 1914-15, v. 222, pp. 216-217.
Roussy, G. Boisseau, J. and d’Oelnitz, M. Emotions de guerre. Collection Horizon, Masson et Cie, Paris, 1918.
Roussy, G. Boisseau, J. and d’Oelnitz, M. War Emotions. Horizon Collection, Masson et Cie, Paris, 1918.
Roussy, Gustave. Complications of wounds of the spinal cord. War Med., Surg. and Hygiene, 1918, i, 602.
Roussy, Gustave. Complications of spinal cord injuries. War Med., Surg. and Hygiene, 1918, i, 602.
Roussy, G. Psycho-neurological disturbances affecting the limbs, observed during the war. War Med., 1918, ii, 37.
Roussy, G. Psycho-neurological issues affecting the limbs, observed during the war. War Med., 1918, ii, 37.
Roussy, G. Surdité-mutité par éclatement d’obus chez trois Zouaves compagnons d’armes. Rev. neurol., Par., 1914-15, v. 222, pp. 394-396.
Roussy, G. Hearing loss and mutism caused by shell explosions in three Zouaves comrades in arms. Rev. neurol., Par., 1914-15, v. 222, pp. 394-396.
Roussy, G. À propos de quelques troubles nerveux observés à l’occasion de la guerre (hystérie, hystérie-traumatisme, simulation). Rev. neurol., Par., 1914-15, v. 222, pp. 425-430. Also Presse méd., Par., 1915, v. 23, pp. 115-117.
Roussy, G. On some nervous disorders observed during the war (hysteria, traumatic hysteria, feigning). Rev. neurol., Paris, 1914-15, v. 222, pp. 425-430. Also Presse méd., Paris, 1915, v. 23, pp. 115-117.
Roussy, G. Troubles nerveux psychiques de guerre. Presse méd., Par., 1915, v. 23, p. 141.
Roussy, G. Psychological Nerve Disorders of War. Medical Press, Paris, 1915, v. 23, p. 141.
Roussy, G. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 472.
Roussy, G. Discussion on how to handle head injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 472.
Roussy, G. Sur la fréquence des complications pleuro-pulmonaires et leur rôle comme facteur de gravité chez les grands blessés nerveux. Bull. Acad. de méd., Par., 1916, v. 75, p. 722-725. Also Presse méd., Par., 1916, v. 24, p. 266.
Roussy, G. On the frequency of pleuropulmonary complications and their role as a severity factor in major nerve injuries. Bull. Acad. de méd., Par., 1916, v. 75, p. 722-725. Also Presse méd., Par., 1916, v. 24, p. 266.
Roussy, G. Un cas de tumeur de lobe frontal pris cliniquement pour une méningite tuberculeuse. Presse méd., Par., 1916, v. 24, p. 47.
Roussy, G. A case of a frontal lobe tumor clinically mistaken for tuberculous meningitis. Med. Press, Paris, 1916, vol. 24, p. 47.
Roussy, G. Des complications pleuro-pulmonaires comme facteur de gravité chez les blessés du crâne et de la moelle par plaie de guerre. Presse méd., Par., 1916, v. 24, p. 47.
Roussy, G. Complications in the lungs and pleura as a serious factor in skull and spinal injuries from war wounds. Medical Press, Paris, 1916, vol. 24, p. 47.
Roussy, G. Un cas de paraplégie hystérique datant de 21 mois avec gros troubles vaso-moteurs thermiques et sécrétoires des extrémités inférieures. Rev. neurol., Par., 1917, v. 24, pp. 253-256.
Roussy, G. A case of hysterical paraplegia lasting 21 months with significant thermal and secretory vaso-motor issues in the lower limbs. Rev. neurol., Par., 1917, v. 24, pp. 253-256.
Roussy et Boisseau. Fausse commotion cérébrale. Bégaiement hystérique. Presse méd., Par., 1915, v. 23, p. 391.
Roussy and Boisseau. False concussion. Hysterical stuttering. Medical Press, Paris, 1915, vol. 23, p. 391.
Roussy et Boisseau. Les sinistroses de guerre. Accidents nerveux par éclatement d’obus à distance. Presse méd., Par., 1915, v. 23, pp. 452-453.
Roussy and Boisseau. War casualties. Nerve injuries from shell explosions at a distance. Med. Press, Paris, 1915, vol. 23, pp. 452-453.
Roussy et Boisseau. Discussion des accidents nerveux par la déflagration explosifs. Rev. neurol., Par., 1916, v. 23, pp. 577-586.
Roussy and Boisseau. Discussion of nerve accidents caused by explosive detonations. Rev. neurol., Paris, 1916, vol. 23, pp. 577-586.
Roussy et Boisseau. Un centre de neurologie et de psychiatrie d’armée. Paris méd., 1916 (Part. méd.), v. 19, pp. 14-20.
Roussy and Boisseau. A military neurology and psychiatry center. Paris med., 1916 (Part. med.), v. 19, pp. 14-20.
Roussy et Boisseau. Les accidents nerveux déterminés par la déflagration des explosifs. Paris méd., 1916-17, v. 21, pp. 185-191.
Roussy and Boisseau. Nervous accidents caused by the explosion of explosives. Paris méd., 1916-17, v. 21, pp. 185-191.
Roussy et Boisseau. Sur le pronostic et le traitement des troubles nerveux dits réflexes. Rev. neurol., Par., 1917, v. 24, pp. 516-527.
Roussy and Boisseau. On the prognosis and treatment of so-called reflex neurological disorders. Neurological Review, Paris, 1917, vol. 24, pp. 516-527.
Roussy et Boisseau. Deux cas de soi-disante commotion labyrinthique par éclatement d’obus à distance. Presse méd., Par., 1917, v. 25, p. 323.
Roussy and Boisseau. Two cases of supposed labyrinthine concussion caused by distant shell explosions. Medical Press, Paris, 1917, v. 25, p. 323.
Roussy et Boisseau. Pronostic et traitement des troubles nerveux dits réflexes. Presse méd., Par., 1917, v. 25, p. 374.
Roussy and Boisseau. Prognosis and treatment of so-called reflex nerve disorders. Medical Press, Paris, 1917, vol. 25, p. 374.
Roussy et Boisseau. Deux cas de pseudo-commotion labyrinthique par éclatement d’obus à distance (commotion labyrinthique persévérée simulée ou suggestionnée). Bull. et. mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 671-676.
Roussy and Boisseau. Two cases of pseudo-labyrinthine concussion from distant shell explosions (persistent simulated labyrinthine concussion or suggested). Bull. et. mém. soc. méd. d’hôp. de Par., 1917, v. 33, pp. 671-676.
Roussy, Boisseau et Cornil, L. Pseudo-tympanites abdominales hystériques; les catiémophrénoses. Bull. et mém. Soc. méd. d’hôp. de Par., 1917, v. 41, pp. 665-670.
Roussy, Boisseau, and Cornil, L. Hysterical abdominal pseudo-tympanites; the catiémophrénoses. Bull. et mém. Soc. méd. d’hôp. de Par., 1917, v. 41, pp. 665-670.
Roussy, Boisseau et d’Oelsnitz. La station neurologique de Salins (Jéna) après trois mois de fonctionnement (Projections de films cinématographiques). Bull. et mém. Soc. méd. d’hôp. de Par., 1917, v. 33, pp. 643-644.
Roussy, Boisseau and d’Oelsnitz. The neurological station in Salins (Jena) after three months of operation (Film projections). Bull. et mém. Soc. méd. d’hôp. de Par., 1917, v. 33, pp. 643-644.
Roussy, Boisseau et d’Oelsnitz. Sur l’influence du facteur psychique dans la guérison des psychonévroses de guerre. Presse méd., Par., 1917, v. 25, pp. 413-414. Also Rev. neurol., Par., 1917, v. 24, pp. 545-553.
Roussy, Boisseau, and d’Oelsnitz. On the influence of psychological factors in the healing of war psychoneuroses. Med. Press, Paris, 1917, vol. 25, pp. 413-414. Also Neurol. Rev., Paris, 1917, vol. 24, pp. 545-553.
Roussy, Boisseau et d’Oelsnitz. Traitement des psychonévroses de guerre. Collection Horizon, Masson et Cie, 1918.
Roussy, Boisseau and d’Oelsnitz. Treatment of War Psychoneuroses. Collection Horizon, Masson and Co., 1918.
Roussy, Cornil et Leroux. Les manœuvres d’élongation du nerf dans le diagnostic des sciatiques. Presse méd., Par., 1917, v. 25, pp. 506-508.
Roussy, Cornil, and Leroux. The stretching maneuvers of the nerve in diagnosing sciatica. Medical Press, Paris, 1917, vol. 25, pp. 506-508.
Roussy, G., Lhermitte, J. The psychonevroses of war. Military Medical Manuals, Univ. of London Press, 1918.
Roussy, G., Lhermitte, J. The psychological traumas of war. Military Medical Manuals, University of London Press, 1918.
Roussy, G. and Lhermitte, J. Blessures de la moelle et la queue de cheval. Collection Horizon, Masson et Cie, Paris, 1917.
Roussy, G. and Lhermitte, J. Spinal cord injuries and cauda equina syndrome. Horizon Collection, Masson et Cie, Paris, 1917.
Roussy, G. and Lhermitte, J. Psychonévroses de guerre. Collection Horizon, Masson et Cie, Paris, 1917.
Roussy, G. and Lhermitte, J. War Psychoneuroses. Horizon Collection, Masson et Cie, Paris, 1917.
Roussy et Lhermitte. Les psychonévroses de guerre. Ann. de méd., Par., 1916, v. 3, pp. 525-563; also pp. 619-665.
Roussy and Lhermitte. War Psychoneuroses. Ann. de méd., Paris, 1916, v. 3, pp. 525-563; also pp. 619-665.
Roussy et Lhermitte, J. La forme hémiplégique de la commotion directe de la moelle cervicale avec lésion de la XIe paire crânienne. Ann. de méd., Par., 1917, v. 4, pp. 458-469.
Roussy and Lhermitte, J. The hemiplegic form of direct concussion of the cervical spinal cord with damage to the XIe cranial nerve. Ann. de méd., Paris, 1917, vol. 4, pp. 458-469.
Roussy et Ichlonski. Mouvements syncinésiques très prononcés chez un hémiplégique organique par blessure de guerre. Rev. neurol., Par., 1914-15, v. 222, pp. 492-494.
Roussy and Ichlonski. Very pronounced syncinetic movements in an organic hemiplegic due to a war injury. Rev. neurol., Paris, 1914-15, v. 222, pp. 492-494.
Routier. Notes à propos d’un certain nombre de cas de tétanos anormal. Bull. Acad. de méd., Par., 1915, v. 74, pp. 515-516; also pp. 600-611.
Routier. Notes on a number of cases of abnormal tetanus. Bull. Acad. de méd., Par., 1915, v. 74, pp. 515-516; also pp. 600-611.
Rows, R. G. Mental conditions following strain and nervous shock. Brit. M. J., Lond., 1916, i, pp. 441-443.
Rows, R. G. Mental health issues after stress and emotional trauma. British Medical Journal, London, 1916, i, pp. 441-443.
Rucker. Le service d’isolement et de psychothérapie à la Salpêtrière pour le traitement des militaires atteints de troubles fonctionnels du système nerveux. J. de méd. et de chir. prat., Par., 1916, v. 87, pp. 90-94.
Rucker. The isolation and psychotherapy service at Salpêtrière for the treatment of soldiers suffering from functional nervous system disorders. J. de méd. et de chir. prat., Par., 1916, v. 87, pp. 90-94.
Rusca, Franchino. Experimentelle Untersuchungen über die traumatischen Druckwirkung der Explosionen. Deutsche Ztschr. f. Chir., 1914-15, v. 132, pp. 315-374.
Rusca, Franchino. Experimental Studies on the Traumatic Pressure Effects of Explosions. German Journal of Surgery, 1914-15, v. 132, pp. 315-374.
Russel, Colin K. A study of certain psychogenetic conditions among soldiers. Canad. Med. Ass. J., Montreal, 1917, v. 7, No. 8, pp. 704-720.
Russel, Colin K. A study of specific psychological conditions among soldiers. Canad. Med. Ass. J., Montreal, 1917, v. 7, No. 8, pp. 704-720.
Ryan, E. A case of shell shock. Canad. Prac. and Rev., Toronto, 1916, v. 41, pp. 507-510. Also Canad. Med. Ass. J., Montreal, 1915, v. 6, pp. 1095-1099.
Ryan, E. A case of shell shock. Canadian Practice and Review, Toronto, 1916, v. 41, pp. 507-510. Also Canadian Medical Association Journal, Montreal, 1915, v. 6, pp. 1095-1099.
S. (C.) Le service d’isolement et de psychothérapie à la Salpêtrière pour le traitement des militaires atteints de troubles fonctionnels du système nerveux. J. de méd. et de chir. prat., 1916, lxxxvii, 90-94.
S. (C.) The isolation and psychotherapy service at Salpêtrière for treating soldiers with functional nervous system disorders. J. de méd. et de chir. prat., 1916, lxxxvii, 90-94.
S. (C.) Les blessures indirectes du système nerveux déterminées par le vent de l’explosif. J. de méd. et chir. prat., Par., 1916, lxxxvii, 436.
S. (C.) Indirect injuries to the nervous system caused by the blast of explosives. J. of Med. and surg. pract., Paris, 1916, lxxxvii, 436.
Saaler, B. Ueber nervöse und psychische Krankheiten in ihren Beziehungen zum Kriegsdienst. Berl. klin. Wchnschr., 1916, liii, 1389.
Saaler, B. On nervous and mental illnesses in relation to military service. Berl. klin. Wchnschr., 1916, liii, 1389.
Sabrazis. Simulation de méningite cérébro-spinale par les accidents nerveux du 1914, dans deux cas guérison. Gaz. hebd. d. sc. med. de Bordeaux, 1917, v. 38, pp. 134-135.
Sabrazis. Simulation of cerebrospinal meningitis caused by nerve accidents in 1914, with recovery in two cases. Weekly Gazette of Medical Sciences of Bordeaux, 1917, v. 38, pp. 134-135.
Sainsbury, H. Treatment of neuritis, with special reference to sciatica. Lancet, Lon., 1917, i, 911.
Sainsbury, H. Treatment of neuritis, with special focus on sciatica. Lancet, Lon., 1917, i, 911.
Salmon, Thomas W. Care and treatment of mental diseases of war neuroses (“shell shock”) in the British Army. Nat. Com. Ment. Hyg., 1917.
Salmon, Thomas W. Care and treatment of mental health issues from war neuroses (“shell shock”) in the British Army. Nat. Com. Ment. Hyg., 1917.
Salmon, T. W. Outline of American plans for dealing with war neuroses. War Med., 1918, ii, 34.
Salmon, T. W. Overview of American strategies for addressing war-related mental health issues. War Med., 1918, ii, 34.
Salmon, Thomas W. The care and treatment of mental diseases and war neuroses (“shell shock”) in the British Army. Ment. Hyg., Concord, N. H., 1917, v. 1, pp. 509-547.
Salmon, Thomas W. The care and treatment of mental illnesses and war-related stress injuries (“shell shock”) in the British Army. Ment. Hyg., Concord, N. H., 1917, v. 1, pp. 509-547.
Salmon, Thomas W. The use of institutions for the insane as military hospitals. Ment. Hyg., Concord, N. H., 1917, v. 7, pp. 806-812.
Salmon, Thomas W. The use of facilities for the mentally ill as military hospitals. Ment. Hyg., Concord, N. H., 1917, v. 7, pp. 806-812.
Salmon, Thomas W. Recommendations for the treatment of mental and nervous diseases in the United States Army. Psychiat. Bull., Utica, 1917, v. 2, No. 3, pp. 355-376.
Salmon, Thomas W. Recommendations for treating mental and nervous disorders in the United States Army. Psychiat. Bull., Utica, 1917, v. 2, No. 3, pp. 355-376.
Samuel. Neurologische Beobachtungen bei den Truppen. Berl. klin. Wchnschr. 1915, v. 521, pp. 140-141.
Samuel. Neurological Observations in the Troops. Berl. klin. Wchnschr. 1915, v. 521, pp. 140-141.
Sandberg. Zwei Fälle von traumatischer Hysterie nach Granatsplitterverletzung. Zentralbl. f. Chir., Leipz., 1915, v. 421, pp. 221-222.
Sandberg. Two cases of traumatic hysteria following grenade fragment injuries. Central Journal of Surgery, Leipzig, 1915, v. 421, pp. 221-222.
Sandoz, F. Le mécanothérapie des raideurs articulaires consécutifs aux blessures de guerre. Paris méd., 1914-15 (Part. méd.), v. 15, p. 408.
Sandoz, F. The mechanotherapy of joint stiffness following war injuries. Paris méd., 1914-15 (Part. méd.), v. 15, p. 408.
Sänger. Ueber die durch den Krieg bedingten Folgezustände im Nervensystem. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, ii, p. 815. Also Berl. klin. Wchnschr., 1915, v. 421, p. 277, and Neurol. Centralbl., Leipz., 1915, v. 34, pp. 364-366.
Sänger. On the effects of war-related conditions on the nervous system. German med. Wchnschr., Berlin and Leipzig, 1915, ii, p. 815. Also Berlin clin. Wchnschr., 1915, v. 421, p. 277, and Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 364-366.
Sänger and Cimbal. Nervöse Erkrankungen im Kriege. Deutsche med. Wchnschr., Leipz. u. Berl., 1915, v. 41, p. 902; also 933-935.
Sänger and Cimbal. Nervous Disorders in War. German Med. Weekly, Leipzig and Berlin, 1915, vol. 41, p. 902; also 933-935.
Sarbó, A. v. Ueber den sogennanten Nervenschock nach Granat- und Schrapnell-explosionen. Wien. klin. Wchnschr., 1915, v. 28, pp. 86-91. Also Psychiat.-Neurol. Wchnschr., Halle a. S., 1914-15, v. 16, pp. 429-431, and München. med. Wchnschr., 1915, v. 621, p. 230.
Sarbó, A. v. On the so-called nerve shock after grenade and shrapnel explosions. Vienna Clinical Weekly, 1915, vol. 28, pp. 86-91. Also in Psychiatric-Neurological Weekly, Halle a. S., 1914-15, vol. 16, pp. 429-431, and Munich Medical Weekly, 1915, vol. 621, p. 230.
Sarbó, A. Ueber die durch Granat- und Schrapnell-explosionen entstandenen Zustandsbilder. Ibid., 608-616.
Sarbó, A. On the state images created by grenade and shrapnel explosions. Ibid., 608-616.
Sarbó, A. v. (Nerve shock following grenade and shrapnel explosions). Orvosi hetil., Budapest, 1915, v. 59, pp. 45-48.
Sarbó, A. v. (Nerve shock after grenade and shrapnel explosions). Medical Weekly, Budapest, 1915, v. 59, pp. 45-48.
Sarbó, A. v. Durch Schrapnel- und Granatexplosion herbeigeführter sogenannter Nervenschock. Pest. med. chir. Presse, Budapest, 1915, v. 51, p. 21.
Sarbó, A. v. Nerve shock caused by shrapnel and grenade explosions. Pest. med. chir. Presse, Budapest, 1915, v. 51, p. 21.
Sargeant, P. and Holmes. Report of the later results of gunshot wounds of the head. J. Roy. Army Med. Corps, Lond., 1916, v. 57, pp. 300-311.
Sargeant, P. and Holmes. Report on the recent outcomes of gunshot wounds to the head. J. Roy. Army Med. Corps, Lond., 1916, v. 57, pp. 300-311.
Sauer, W. Enuresis und Hypnose im Felde. München med. Wchnschr., 1916, v. 63, pp. 102-103.
Sauer, W. Enuresis and Hypnosis in the Field. Munich Med. Weekly, 1916, v. 63, pp. 102-103.
Savage, George H. Mental disabilities for war service. J. Ment. Sc., Lond., 1916, ii, p. 42; also v. 62, pp. 653-657.
Savage, George H. Mental disabilities for military service. J. Ment. Sc., Lond., 1916, ii, p. 42; also v. 62, pp. 653-657.
Savage, George H., Sir. Mental war cripples. Practitioner, 1918, c. 1.
Savage, George H., Sir. Mental war cripples. Practitioner, 1918, c. 1.
Savariaud. À propos des phlegmons provoqués par les injections de pétrole. Bull. et mém. Soc. de chir. de Par., 1915, n. s., xli, 2364.
Savariaud. Regarding the abscesses caused by oil injections. Bull. et mém. Soc. de chir. de Par., 1915, n. s., xli, 2364.
Sawdon. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 42-44.
Sawdon. Treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 42-44.
Sayer, Ettie. The organization of electrotherapy in military hospitals. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Electro-therap. sect.), p. 39.
Sayer, Ettie. The setup of electrotherapy in military hospitals. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Electro-therap. sect.), p. 39.
Scarisbrick, W. Cardiac diseases in soldiers and recruits. Brit. Med. Jour., 1917, i, 254.
Scarisbrick, W. Heart diseases in soldiers and recruits. Brit. Med. Jour., 1917, i, 254.
Schermers, D. Oorlogsneurosen en Psychosen. Med. Weekbl., Amst., 1916-17, v. 23, pp. 109-112.
Schermers, D. War Neuroses and Psychoses. Med. Weekbl., Amst., 1916-17, v. 23, pp. 109-112.
Schier, A. R. A further study of mental tests in the examination of recruits. U. S. Nav. M. Bull., Wash., 1917, v. 9, pp. 325-333.
Schier, A. R. A further study of mental tests in the examination of recruits. U. S. Nav. M. Bull., Wash., 1917, v. 9, pp. 325-333.
Schiffbauer, H. E. Operative treatment of gunshot injuries to the peripheral nerves. S. G. O., 1916, xxii, 133.
Schiffbauer, H. E. Surgical treatment of gunshot injuries to peripheral nerves. S. G. O., 1916, xxii, 133.
Schlachter, J. Psychogener Stridor bei Soldaten. Ztschr. f. Ohrenheilh., 77, 1918.
Schlachter, J. Psychogenic Stridor in Soldiers. Journal of Ear Medicine, 77, 1918.
Schlayer. Vorschläge zur Versorgung der funktionellen Neurosen. München med. Wchnschr., 1916, No. 46, pp. 1645-1646.
Schlayer. Suggestions for the treatment of functional neuroses. Munich Med. Weekly, 1916, No. 46, pp. 1645-1646.
Schlayer. Die Versorgung der funktionellen Kriegsneurosen. München med. Wchnschr., 1917, No. 1, p. 39.
Schlayer. The treatment of functional war neuroses. Munich med. Wchnschr., 1917, No. 1, p. 39.
Schlendler, L. Schädelverletzungen. Bruns’ kriegschir. Hefte d. Beitr. z. klin. Chir., Tübing., 1916, 103, 500.
Schlendler, L. Skull Injuries. Bruns’ wartime surgery. Contributions to clinical surgery, Tübingen, 1916, 103, 500.
Schlesinger, H. Fall von hochgradiger retrograder Amnesie nach Gehirnverletzung. Wien. med. Wchnschr., 1915, No. 49, p. 1815.
Schlesinger, H. Case of severe retrograde amnesia after brain injury. Vienna Medical Weekly, 1915, No. 49, p. 1815.
Schlesinger, H. Hochgradige retrograde Amnesie nach Gehirnverletzung. Wien. klin. Wchnschr., 1915, xxviii, 1329.
Schlesinger, H. Severe retrograde amnesia after brain injury. Wien. klin. Wchnschr., 1915, xxviii, 1329.
Schlesinger, H. Epilepsie und Anfall Temperaturerhöhungen. Klin, therap. Wchnschr., Wien u. Berl., 1916, v. 332, p. 29.
Schlesinger, H. Epilepsy and Seizure Temperature Increases. Klin, therap. Wchnschr., Vienna and Berlin, 1916, vol. 332, p. 29.
Schmidt, G. B. Chirurgische Behandlung der Kriegsverletzungen peripherischer Nerven. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, pp. 1263-1264.
Schmidt, G. B. Surgical Treatment of War Injuries to Peripheral Nerves. German Medical Weekly, Berlin and Leipzig, 1915, vol. 412, pp. 1263-1264.
Schmidt, W. Die psychischen und nervösen Folgezustände nach Granatexplosionen und Minenverschüttungen. Ztschr. f. d. ges. Neurol. u. Psychiat., Berl. u. Leipz., 1915, v. 29, pp. 514-542.
Schmidt, W. The psychological and nerve-related aftermath of grenade explosions and mine collapses. Journal of General Neurology and Psychiatry, Berlin and Leipzig, 1915, vol. 29, pp. 514-542.
Schneider, E. Zur Klinik und Prognose der Kriegsneurosen. Wien. klin. Wchnschr., 1916, v. 29, pp. 1295-1303.
Schneider, E. On the Clinic and Prognosis of War Neuroses. Wien. klin. Wchnschr., 1916, v. 29, pp. 1295-1303.
Scholtz, W. Funktionelle Sprachlähmung im Felde. Med. Klin., Berl., 1915, v. 111, pp. 1423-1424.
Scholtz, W. Functional Speech Paralysis in the Field. Med. Klin., Berl., 1915, v. 111, pp. 1423-1424.
Schröder, P. Traumatische Psychosen. Monatschr. f. Psychiat. u. Neurol., Berl., 1915, No. 4, pp. 193-201.
Schröder, P. Traumatic Psychoses. Monthly Journal of Psychiatry and Neurology, Berlin, 1915, No. 4, pp. 193-201.
Schüller, A. Pulsus paradoxus respiratorius. Klin. therap. Wchnschr., Wien u. Berl., 1916, v. 32, pp. 28-29.
Schüller, A. Respiratory paradoxical pulse. Clin. Ther. Weekly, Vienna and Berlin, 1916, vol. 32, pp. 28-29.
Schüller, A. Hypertrichose bei Ischiadicusläsionen. Wiener med. Wchnschr., Nr. 46, 1917.
Schüller, A. Hypertrichosis in Sciatic Nerve Damage. Wiener Medical Weekly, No. 46, 1917.
Schultz, J. H. Einige Bemerkungen über Feindschaftsgefühle im Felde. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 373-378.
Schultz, J. H. Some Remarks on Feelings of Hostility in the Field. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 373-378.
Schultz, J. H. Wege und Ziele der Psychotherapie. Therap. Monatschr. Berl., 1915, No. 8, pp. 443-450.
Schultz, J. H. Paths and Goals of Psychotherapy. Ther. Monthly Journal Berlin, 1915, No. 8, pp. 443-450.
Schultz, J. H. Fünf neurologisch bemerkungswerte Hirnschüsse. Monatschr. f. Psychiat. u. Neurol., 1916, v. 39, No. 6, p. 319.
Schultz, J. H. Five neurologically significant brain injuries. Monthly Journal of Psychiatry and Neurology, 1916, v. 39, No. 6, p. 319.
Schultz, J. H. and Meyer, Robert. Zur klinischen Analyse der Granatschockwirkung. Med. Klin., Berl. u. Wien, 1916, v. 12, pp. 230-233.
Schultz, J. H. and Meyer, Robert. On the clinical analysis of grenade shock effect. Med. Klin., Berl. and Vienna, 1916, v. 12, pp. 230-233.
Schultze, Otto. Ueber die Kaufmanns’sche Behandlung hysterischen Bewegungsstörungen. Münch. med. Wchnschr., 1916, No. 38, pp. 1349-1353.
Schultze, Otto. On the Merchant's Approach to Hysterical Movement Disorders. Münch. med. Wchnschr., 1916, No. 38, pp. 1349-1353.
Schuster. Kriegsneurologische Demonstrationen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 1914-1916.
Schuster. War Neurology Demonstrations. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 1914-1916.
Schuster. Crampusneurose. Neurol. Centralbl., Leipz., 1915, v. 34, p. 72.
Schuster. Crampusneurose. Neurol. Centralbl., Leipzig, 1915, v. 34, p. 72.
Schuster. Entstehen der traumatischen Neurosen oder Psychosen? Neurol. Centralbl., Leipz., 1916, v. 35, No. 12.
Schuster. Do traumatic neuroses or psychoses develop? Neurol. Centralbl., Leipzig, 1916, v. 35, No. 12.
Schuster. Kriegsneurologische Demonstrationen. Berl. klin. Wchnschr., 1916, No. 1, pp. 24-25.
Schuster. War Neurology Demonstrations. Berl. klin. Wchnschr., 1916, No. 1, pp. 24-25.
Schuster, Bonhoeffer, Oppenheim. Diskussion—Zerebellare Symptomen-Komplexe nach Kriegsverletzungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 664-666.
Schuster, Bonhoeffer, Oppenheim. Discussion—Cerebellar Symptom Complexes after War Injuries. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 664-666.
Schuster. Der Mechanismus der hysterischen Skoliose. Neurol. Centralbl., Leipz., 37, Nr. 18, 1918.
Schuster. The Mechanism of Hysterical Scoliosis. Neurol. Centralbl., Leipzig, 37, No. 18, 1918.
Sebileau, Pierre. Monoplégie du membre inférieur, conséquence d’un coup de feu de la cuisse sans blessure apparente de l’appareil d’innervation. Bull. et mém. Soc. de chir. de Par., 1914-15, v. 40, pp. 1175-1177.
Sebileau, Pierre. Monoplegia of the lower limb, resulting from a gunshot wound to the thigh without any visible injury to the nerve apparatus. Bull. et mém. Soc. de chir. de Par., 1914-15, v. 40, pp. 1175-1177.
Seelert, H. Ueber Neurosen nach Unfällen mit besonderer Berücksichtigung von Erfahrungen im Kriege. Monatschr. f. Psychiat. u. Neurol., Berl., 195, v. 38, pp. 328-340.
Seelert, H. On Neuroses After Accidents With Special Consideration of Experiences in War. Monthly Journal of Psychiatry and Neurology, Berlin, 195, vol. 38, pp. 328-340.
Seelert, H. Differentialdiagnose der Hysterie und des progressiven Torsionspasmus. Arch. f. Psychiat., Berl., 1918, v. 56, pp. 684-688.
Seelert, H. Differential diagnosis of hysteria and progressive torsion spasm. Arch. f. Psychiat., Berl., 1918, v. 56, pp. 684-688.
Seeuwen, H. J. Heart and active service. Lancet, Lon., 1916, ii, 432.
Seeuwen, H. J. Heart and active service. Lancet, London, 1916, 2, 432.
Seeuwen, H. J. Treatment of the wounded by means of electricity. Arch. of Radiol. and Electrotherap., 1917, xxii, 136.
Seeuwen, H. J. Treatment of the injured using electricity. Arch. of Radiol. and Electrotherap., 1917, xxii, 136.
Segaloff, T. E. Contribution à l’étude des lésions organiques et fonctionnelles dans les contusions par éclatements d’obus. Psychiatrie contemporaine russe, 1015; Revue Neurol. 1914-15, II, p. 1081-1082.
Segaloff, T. E. Contribution to the study of organic and functional injuries in blast trauma from shell explosions. Contemporary Russian Psychiatry, 1015; Neurology Review. 1914-15, II, pp. 1081-1082.
Segaloff, T. E. Nature of contusions caused by artillery fire. Morbus decompressionis. Sovrem. Psikhiat., Mosk., 1915, ix, 103, 263, 405.
Segaloff, T. E. Nature of contusions caused by artillery fire. Morbus decompressionis. Sovrem. Psikhiat., Mosk., 1915, ix, 103, 263, 405.
Segaloff, T. E. (de Moscou.) Contribution à la connaissance de la nature des contusions par les obus actuels. Psychiatrie contemp. russe, 1915.
Segaloff, T. E. (from Moscow.) Contribution to the understanding of the nature of bruises caused by modern artillery. Contemporary Russian Psychiatry, 1915.
Self-mutilation by soldiers. Brit. M. J., Lond., 1915, i, p. 899.
Self-harm among soldiers. Brit. M. J., Lond., 1915, i, p. 899.
Sencert, L. Rupture des deux poumons par le “vent du boulet.” Bull. et mém. Soc. de chir. de Par., 1915, v. 41, pp. 79-82.
Sencert, L. Rupture of both lungs by “the cannon wind.” Bull. et mém. Soc. de chir. de Par., 1915, v. 41, pp. 79-82.
Sensory phenomena in head injuries. Brit. M. J., Lond., 1915, i, p. 738.
Sensory phenomena in head injuries. Brit. M. J., Lond., 1915, i, p. 738.
Seppilli, G. Guerra e psicopatie. Gazz. med. d. Marche, Ancona, 1915, v. 23, No. 6, p. 3.
Seppilli, G. War and Psychopathies. Gazz. Med. d. Marche, Ancona, 1915, v. 23, No. 6, p. 3.
Seppilli, G. I disturbi mentali nei militari in rapporto alla guerra. Riv. ital. di neuropat. etc., Catania, 1917, v. 10, pp. 105-114; also pp. 137-141.
Seppilli, G. Mental disorders in soldiers related to war. Ital. J. Neuropath. etc., Catania, 1917, vol. 10, pp. 105-114; also pp. 137-141.
Sereysky, M. J. (A contribution to the problem of poisoning by German asphyxiating gas: Their influence in the nervous psychic condition of the asphyxiated.) Russk. Vrach., Petrogr., 1917, v. 16, p. 401.
Sereysky, M. J. (A contribution to the issue of poisoning from German asphyxiating gas: Their impact on the mental state of those affected by asphyxiation.) Russk. Vrach., Petrogr., 1917, v. 16, p. 401.
Sérieux, P. et Laignel-Lavastine. Sur utilité de mesures spéciales pour les anormaux psychiques constitutionnels en temps de guerre. Bull. méd., Par., 1917, v. 31, pp. 11-12.
Sérieux, P. and Laignel-Lavastine. On the usefulness of special measurements for constitutional psychological anomalies during wartime. Med. Bull., Paris, 1917, vol. 31, pp. 11-12.
Serog. Zwei Fälle von krankhafter Selbstbesichtigung der Simulation. Med. Klin., Berl., 1916, xii, 1100-1102.
Serog. Two cases of pathological self-examination of the simulation. Med. Klin., Berl., 1916, xii, 1100-1102.
Serre, Biron and Brette. Tentative de fraude au moyen de l’ovoalbumine (simulation de l’albuminurie). Arch. de méd. et pharm. mil., Par., 1917, lxviii, 935-939.
Serre, Biron, and Brette. Attempt to commit fraud using ovoalbumin (simulating albuminuria). Arch. of Med. and Pharm. Mil., Paris, 1917, lxviii, 935-939.
Service d’isolement et de psychothérapie à la Salpêtrière pour le traitement des militaires atteints de troubles fonctionnels du système nerveux. J. de méd. et chir. prat., Par., 1916, v. 87, pp. 90-94.
Isolation and Psychotherapy Service at Salpêtrière for the treatment of military personnel suffering from functional nervous system disorders. J. de méd. et chir. prat., Par., 1916, v. 87, pp. 90-94.
Sforza, N. Le sindromi nervose di commozione da scoppio de granata. Med. nuova, Roma, 1916, v. 7, pp. 6-10.
Sforza, N. The nervous syndromes from grenade blast concussions. New Med., Rome, 1916, v. 7, pp. 6-10.
Sgobbo, F. P. La röntgenologia causa di turbamento psichico nei militari, ed utile mezzo per la diagnosi di alcuni male simulati. Radiol. med., Torino, 1916, v. 3, pp. 313-317.
Sgobbo, F. P. X-ray technology causing psychological disturbances in soldiers, and a useful tool for diagnosing certain feigned illnesses. Radiol. med., Turin, 1916, v. 3, pp. 313-317.
Shaikevich, M. O. (Neuro-mental disease in time of war and its prevention.) Sibirsk. Vrach., Tomsk, 1915, v. 2, pp. 35-39.
Shaikevich, M. O. (Neuro-mental illness during wartime and its prevention.) Sibirsk. Vrach., Tomsk, 1915, v. 2, pp. 35-39.
Shairp, L. V. The reëducation of disabled soldiers. Am. J. Care Cripples, N. Y., 1917, v. 4, pp. 201-211.
Shairp, L. V. The re-education of disabled soldiers. Am. J. Care Cripples, N. Y., 1917, v. 4, pp. 201-211.
Shangengberg, E. (War injuries affecting the voice and speech.) Hygiea, Stockholm, 1917, v. 79, p. 49.
Shangengberg, E. (War injuries affecting the voice and speech.) Hygiea, Stockholm, 1917, v. 79, p. 49.
Sheehan, R. Malingering in mental disease. U. S. Nav. M. Bull., Wash., 1916, x, 646-653.
Sheehan, R. Faking illness in mental health. U. S. Nav. M. Bull., Wash., 1916, x, 646-653.
Shell explosions and the special senses. Lancet, Lond., 1915, i, p. 663.
Shell explosions and the special senses. Lancet, London, 1915, 1, p. 663.
Shell shock and neurasthenia. Lancet, Lond., 1916, i, p. 627.
Shell shock and neurasthenia. Lancet, London, 1916, i, p. 627.
Shell shock. Am. med., Burlington, Vt., 1917, v. 23, pp. 606-607.
Shell shock. Am. med., Burlington, Vt., 1917, v. 23, pp. 606-607.
Shell shock among troops. Bos. M. and S. J., 1918, clxxviii, 133.
Shell shock among troops. Bos. M. and S. J., 1918, clxxviii, 133.
Shell shock patients in air raids. Brit. M. J., Lond., 1918, i, p. 90.
Shell shock patients during air raids. Brit. M. J., Lond., 1918, i, p. 90.
Shufflebotham, Frank. The effects of military training upon lead workers. Brit. M. J., Lond., 1915, i, p. 672.
Shufflebotham, Frank. The impact of military training on lead workers. Brit. M. J., Lond., 1915, i, p. 672.
Shumkoff, G. E. (Number of the insane in the war.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 363-366.
Shumkoff, G. E. (Number of people with mental illness during the war.) Psychiatric. Gaz., St. Petersburg, 1915, v. 2, pp. 363-366.
Shumkoff, G. E. (Rapid psychiatric aid in the war.) Psikhiat. Gaz., Petrograd, 1916, v. 3, pp. 281-288.
Shumkoff, G. E. (Quick psychiatric help during the war.) Psikhiat. Gaz., Petrograd, 1916, v. 3, pp. 281-288.
Shuttleworth, G. War and insanity. J. Ment. Sc., Lond., 1916, v. 62.
Shuttleworth, G. War and insanity. J. Ment. Sc., Lond., 1916, v. 62.
Sicard, J. A. Blessures de guerre. Traitement de certaines algies et acrocontractures rebelles par l’alcoolisation nerveuse locale. Soc. méd. des Hôpitaux, 17 decembre 1915.
Sicard, J. A. War Injuries. Treatment of Certain Pain Conditions and Rebellious Muscle Contractions through Local Nerve Alcoholization. Med. Society of Hospitals, December 17, 1915.
Sicard. Simulateurs de création et simulateurs de fixation. Simulateurs sourds-muets. Paris méd., 1915, v. 17 (Part. méd.), pp. 423-428.
Sicard. Creation simulators and fixation simulators. Deaf-mute simulators. Paris méd., 1915, v. 17 (Part. méd.), pp. 423-428.
Sicard. Traitement de la névrite douloureuse du médian par l’alcoolisation tronculaire sus-lésionnelle. Soc. Méd. de Hôp., July 9, 1915; Traitement de certaines algies et acrocontractures rebelles par l’alcoolisation nerveuse locale. Ibid., Dec. 17, 1915.
Sicard. Treatment of painful median neuritis through supralesional trunk alcoholization. Soc. Méd. de Hôp., July 9, 1915; Treatment of certain stubborn pain conditions and acrocontractures through local nerve alcoholization. Ibid., Dec. 17, 1915.
Sicard. Traitement des névrites douloureuses de guerre causalgies par l’alcoolisation nerveuse locale. Presse méd., juin, 1916.
Sicard. Treatment of painful war neuritis causalgia caused by local nerve alcoholization. Medical Press, June, 1916.
Sicard. Examen du liquide céphalo-rachidien au cours des commotions par “vent d’explosif.” Paris méd., 1915, v. 17, p. 556.
Sicard. Examination of cerebrospinal fluid during concussions caused by "explosive wind." Paris méd., 1915, v. 17, p. 556.
Sicard. Plicatures vertébrales par “vent d’obus.” Spondyloses et attitudes vertébrales antalgiques. Examen du liquide céphalo-rachidien. Soc. méd. des Hôpitaux, 9 juillet, 1915.
Sicard. Vertebral folds due to "shell blast." Spondylosis and antalgic spinal positions. Examination of cerebrospinal fluid. Medical Society of Hospitals, July 9, 1915.
Sicard. Spondylites par obusite ou vent d’obus. Attitudes vertébrales antalgiques. Bull. et mém. Soc. méd. d. hôp. de Paris, 1915, v. 39, p. 582.
Sicard. Shell shock or artillery wind. Antalgic spinal postures. Bull. et mém. Soc. méd. d. hôp. de Paris, 1915, v. 39, p. 582.
Sicard. À propos du procès-verbal et de la communication de MM. Souques, Mégévand et Donet sur l’examen du liquide céphalo-rachidien (séance du 29 octobre, 1915) au cours des commotions par vent d’explosif. Bull. et mém. Soc. méd. d. hôp. de Par., 1915, x. s. xxxix, 1034.
Sicard. Regarding the minutes and the report from Messrs. Souques, Mégévand, and Donet on the examination of cerebrospinal fluid (session of October 29, 1915) during explosive wind impacts. Bull. et mém. Soc. méd. d. hôp. de Par., 1915, x. s. xxxix, 1034.
Sicard. L’alcoolisation tronculaire au cours des acromyonties rebelles du membre supérieur. Paris méd., 1916, v. 19, 509-512.
Sicard. The use of alcohol in stubborn acromyonties of the upper limb. Paris méd., 1916, v. 19, 509-512.
Sicard. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. Neurol. Paris, 1916, v. 29, p. 462.
Sicard. Discussion on how to deal with skull injuries—by P. Marie. Rev. Neurol. Paris, 1916, v. 29, p. 462.
Sicard et Cantaloube. Les oedèmes de striction. Soc. méd. des Hôpitaux, 26 mai 1916.
Sicard and Cantaloube. Restrictive Edemas. Medical Society of Hospitals, May 26, 1916.
Sicard et Cantaloube. Les réflexes musculaires du pied et de la main (myo-diagnostic mécanique). Presse méd., Par., 1916, v. 24, pp. 145-147.
Sicard and Cantaloube. The muscle reflexes of the foot and hand (mechanical myo-diagnosis). Medical Press, Paris, 1916, vol. 24, pp. 145-147.
Sicard et Cantaloube. Réflexes musculaires pédo-dorsaux. Leur valeur diagnostique et pronostique. Soc. de Neurol. 3 février 1916.
Sicard and Cantaloube. Pedal-dorsal muscle reflexes. Their diagnostic and prognostic value. Neurology Society. February 3, 1916.
Sicard, J. A., Roger, H. and Rimbaud, L. Syncinésie d’effort; réactions syncinétiques par choc du liquide rachidien sur le faisceau pyramidal dégéneré. Ibid., 1917, 3. s, xli, 619-622.
Sicard, J. A., Roger, H. and Rimbaud, L. Syncinesis of effort; syncinetic reactions due to the impact of spinal fluid on the degenerated pyramidal tract. Ibid., 1917, 3. s, xli, 619-622.
Siciliano. Les tropho-névroses traumatiques. Rivista critica di clinica medica, Nos. 19, 20 et 21.
Siciliano. Traumatic trophoneuroses. Critical journal of clinical medicine, Nos. 19, 20, and 21.
Signorelli e Buscaino. Bradicardia e riflesso oculo-cardiaco nella dissenteria amoebica. Riv. di patol. nerv. e ment., 1917, 22, 487-90.
Signorelli and Buscaino. Bradycardia and ocular-cardiac reflex in amoebic dysentery. Rev. of Nervous and Mental Pathology, 1917, 22, 487-90.
Siege, Max. Typhuspsychosen im Felde. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 291-296.
Siege, Max. Typhus Psychoses in the Field. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 291-296.
Silberstein, Adolf. Kriegsenvalidenfürsorge und staatliche Unfallfürsorge. Würzb. Abhandl. a. d. Gesamt.-geb. d. prakt. Med., 1915, v. 15, pp. 119-130, and pp. 135-148.
Silberstein, Adolf. Support for wartime disabilities and state accident care. Würzb. Abhandl. a. d. Gesamt.-geb. d. prakt. Med., 1915, v. 15, pp. 119-130, and pp. 135-148.
Silberstein. The Royal Orthopedic Reserve Hospital at Nürnberg, Germany. Am. J. Cripples, N. Y., 1917, v. 4, pp. 188-191.
Silberstein. The Royal Orthopedic Reserve Hospital in Nürnberg, Germany. Am. J. Cripples, N. Y., 1917, v. 4, pp. 188-191.
Silex, P. Neue Wege in der Kriegsblindfürsorge. 2 Aufl., Berl., 1916, S. Karger, 8o.
Silex, P. New Approaches in War Blindness Care. 2nd ed., Berlin, 1916, S. Karger, 8o.
Silver, D. The function of orthopedic surgery in the present war. Am. J. Orthop. Surg., Bost., 1917, v. 15, pp. 509-511.
Silver, D. The role of orthopedic surgery in the current war. Am. J. Orthop. Surg., Bost., 1917, v. 15, pp. 509-511.
Similarity of War Neuroses to Accident Neuroses. Brit. M. J., Lond., 1915, i, p. 1072.
Similarity of War Neuroses to Accident Neuroses. Brit. M. J., Lond., 1915, i, p. 1072.
Simple method of detecting simulated deafness. Lancet, Lond., 1917, ii, 369.
Easy way to spot fake deafness. Lancet, Lond., 1917, ii, 369.
Singer, Kurt. Wesen und Bedeutung der Kriegspsychosen. Berl. klin. Wchnschr., 1915, v. 52, pp. 177-180.
Singer, Kurt. The Nature and Significance of War Psychoses. Berl. klin. Wchnschr., 1915, v. 52, pp. 177-180.
Sklyar, N. I. (The war and mental diseases). Sovrem. Psikhiat., Mosk., 1916, v. 10, p. 98, p. 157, p. 453.
Sklyar, N. I. (The war and mental illnesses). Modern Psychiatry, Moscow, 1916, v. 10, p. 98, p. 157, p. 453.
Small, C. P. Equilibrium tests for aviation recruits. Jour. A. M. A., 1917, lxix, 1078.
Small, C. P. Equilibrium tests for aviation recruits. Jour. A. M. A., 1917, lxix, 1078.
Smirkoff, D. Deux cas graves de névrose traumatique par contusion, guéris par la suggestion hypnotique. Jour. de neurop. et psychiat. de S. S. Korsakoff, 1916, fasc. 2, also Rev. neurol., Par., 1917, v. 24, p. 477.
Smirkoff, D. Two serious cases of traumatic neurosis from concussion, cured through hypnotic suggestion. Journal of Neurology and Psychiatry of S. S. Korsakoff, 1916, fasc. 2, also Neurological Review, Paris, 1917, v. 24, p. 477.
Smith, G. E. Shock and the soldier. Lancet, Lond., 1916, i, pp. 813-817, and pp. 853-857.
Smith, G. E. Shock and the soldier. Lancet, Lond., 1916, i, pp. 813-817, and pp. 853-857.
Smith, G. E. and Pear, T. H. Shell shock and its lessons. Nature, Lond., 1917, v. 100, pp. 64-66.
Smith, G. E. and Pear, T. H. Shell shock and its lessons. Nature, London, 1917, v. 100, pp. 64-66.
Smith, G. E. and Pear, T. H. Shell shock and its lessons. 1917, Manchester, University Press.
Smith, G. E. and Pear, T. H. Shell shock and its lessons. 1917, Manchester, University Press.
Smith, Percy. War and insanity. J. Ment. Sc., Lond., 1916, v. 62, pp. 815-817.
Smith, Percy. War and insanity. J. Ment. Sc., Lond., 1916, v. 62, pp. 815-817.
Smith, Percy. Civilian mental disease in wartime. Proc. Roy. Soc. Med., Lond., 1916, v. 10, pp. 1-20.
Smith, Percy. Mental health issues among civilians during wartime. Proc. Roy. Soc. Med., Lond., 1916, v. 10, pp. 1-20.
Smyly, C. P. Shell shock. Dublin, J. M. Sc., 1917, v. 142, pp. 247-256.
Smyly, C. P. Shell shock. Dublin, J. M. Sc., 1917, v. 142, pp. 247-256.
Sogenannten funktionellen Nervenerkrankungen der Kriegsteilnehmer. Jahresb. f. ärztl. Fortbild, München, 1915, v. 6, pp. 26-27.
So-called functional nervous disorders of war veterans. Ann. for medical training, Munich, 1915, vol. 6, pp. 26-27.
Soldats aveugles masseurs. Caducée, Par., 1917, v. 11, p. 12.
Blind soldier masseurs. Caducée, Par., 1917, v. 11, p. 12.
Soldat mendiant. Ann. méd. psychol., Par., 1914-1915, v. 6, p. 527.
Homeless soldier. Ann. méd. psychol., Paris, 1914-1915, vol. 6, p. 527.
Sollier, P. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 63-64. Also p. 473.
Sollier, P. Discussion on how to manage skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, pp. 63-64. Also p. 473.
Sollier. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol., Par., 1916, v. 29, pp. 575-576.
Sollier. On nerve accidents caused by powerful explosive detonations. Neurological Review, Paris, 1916, vol. 29, pp. 575-576.
Sollier. Troubles trophiques osseux dans un cas d’hémiplégie hystérique. Lyon méd., 1916, v. 125, pp. 20-21.
Sollier. Bone trophic issues in a case of hysterical hemiplegia. Lyon méd., 1916, v. 125, pp. 20-21.
Sollier. Impotence fonctionnelle d’origine nerveuse chez les blessés de guerre. Bull. Acad. de méd., Par., 1914, v. 72, pp. 346-347.
Sollier. Functional impotence of nerve origin in war injuries. Bull. Acad. de méd., Paris, 1914, v. 72, pp. 346-347.
Sollier. Trois cas d’hémiplégie hystérique consécutive à des lésions craniocérébrales. Lyon méd., 1915, v. 124, p. 334.
Sollier. Three cases of hysterical hemiplegia following cranial and cerebral injuries. Lyon méd., 1915, v. 124, p. 334.
Sollier. La neurologie de guerre: Décisions prises aux trois réunions des chefs des centres neurologiques. Lyon méd., 1916, v. 125, p. 339.
Sollier. The neurology of war: Decisions made at the three meetings of heads of neurological centers. Lyon méd., 1916, v. 125, p. 339.
Sollier. Un cas de canitie par commotion et émotion. Lyon méd., 1916, v. 125, p. 329.
Sollier. A case of graying hair due to shock and emotion. Lyon méd., 1916, v. 125, p. 329.
Sollier. Persistance des troubles fonctionnelles pendant le sommeil. Rev. neurol., Par., 1914-15, v. 222, p. 1240.
Sollier. Persistence of functional disorders during sleep. Rev. neurol., Paris, 1914-15, v. 222, p. 1240.
Sollier. Sur l’abolition du réflexe cutané plantaire dans les paralysies ou contractures fonctionnelles. Rev. neurol., Par., 1914-15, v. 222, pp. 1280-1283.
Sollier. On the abolition of the plantar cutaneous reflex in functional paralysis or contractions. Rev. neurol., Par., 1914-15, v. 222, pp. 1280-1283.
Sollier. Du diagnostic clinique de l’exagération et de la persévérance des troubles nerveux fonctionnelles. Presse méd., Par., 1915, v. 23, pp. 505-507.
Sollier. On the clinical diagnosis of the exaggeration and persistence of functional nerve disorders. Med. Press, Paris, 1915, v. 23, pp. 505-507.
Sollier. Statistique des cas de névrose dus à la guerre. Bull. Acad. de méd., Par., 1915, v. 73, pp. 682-684.
Sollier. Statistics on cases of neurosis caused by the war. Bull. Acad. de méd., Par., 1915, v. 73, pp. 682-684.
Sollier. Diagnostic des contractures hystéro-traumatiques et des rétractions. Lyon méd., 1917, v. 126, pp. 93-96.
Sollier. Diagnosis of hystero-traumatic contractions and retractions. Lyon méd., 1917, v. 126, pp. 93-96.
Sollier. Mécanothérapie et rééducation motrice au point de vue psycho-physiologique et moral. Paris méd., 1917, No. 38, pp. 246-249.
Sollier. Mechanotherapy and motor rehabilitation from a psycho-physiological and moral perspective. Paris méd., 1917, No. 38, pp. 246-249.
Sollier et Chartier. La commotion par explosifs et ses conséquences sur le système nerveux. Paris méd., 1915, v. 17, pp. 406-414.
Sollier and Chartier. The effects of explosives on the nervous system. Paris méd., 1915, v. 17, pp. 406-414.
Sollier and Jousset, Xavier. Névrites nitro-phénolées. Lyon méd., 1917, v. 126, pp. 187-192.
Sollier and Jousset, Xavier. Nitro-Phenol Neuritis. Lyon Med., 1917, v. 126, pp. 187-192.
Somen, H. La pratique du massage. Paris méd., 1915, v. 17, pp. 97-103.
Somen, H. The Practice of Massage. Medical Paris, 1915, vol. 17, pp. 97-103.
Somen, H. Memento de mécanothérapie. Paris, 1916, J. B. Ballière et fils, 96 p., 8o.
Somen, H. Memento of Mechanotherapy. Paris, 1916, J. B. Ballière et fils, 96 p., 8o.
Sommer, R. Krieg und Seelenleben—Einfluss des Krieges auf das normale Seelenleben. Wien. med. Wchnschr., 1915, No. 40, p. 1481.
Sommer, R. War and the Mind—The Impact of War on Normal Mental Life. Vienna. Med. Weekly, 1915, No. 40, p. 1481.
Soulié, A. Les nerfs. In Poirier, tome iii, fasc. 3.
Soulié, A. The nerves. In Poirier, volume iii, issue 3.
Souttar, H. S. Some points in nerve injuries. Brit. M. J., Lond., 1917, ii, pp. 817-820.
Souttar, H. S. Some points in nerve injuries. Brit. M. J., Lond., 1917, ii, pp. 817-820.
Soukhanoff, S. A. De la conviction délirante d’être prisonnier de guerre; contribution à l’étude des troubles mentaux provoqués par la guerre actuelle. Ann. méd.-psychol., Par., 1914-15. v. 6, pp. 549-557.
Soukhanoff, S. A. On the delusional belief of being a prisoner of war; contribution to the study of mental disorders caused by the current war. Ann. méd.-psychol., Par., 1914-15. v. 6, pp. 549-557.
Soukhanoff, S. A. Des psychonévroses traumatiques de guerre. Assemblée scientifique des médecins de l’hôpital de Notre-Dame-des-Affligés pour les alienés et de l’asile Novoznamenskaia, à Petrograd, avril 1915.
Soukhanoff, S. A. On the traumatic psychoneuroses of war. Scientific assembly of physicians from the Hospital of Our Lady of the Afflicted for the insane and the Novoznamenskaia asylum, in Petrograd, April 1915.
Soukhanoff, S. A. Psychopathy in time of war. Russk. Vrach., Petrogr., 1915, xiv, 800-804.
Soukhanoff, S. A. Psychopathy during wartime. Russk. Vrach., Petrogr., 1915, xiv, 800-804.
Soukhanoff, S. A. (Present condition of science concerning traumatic neurosis, questions of its study and treatment from the viewpoint of military medicine.) Voyenno-Med. J. Petrogr., 1916, ccxlv, med.-spec., 241-272.
Soukhanoff, S. A. (Current state of science on traumatic neurosis, issues surrounding its study and treatment from the perspective of military medicine.) Voyenno-Med. J. Petrogr., 1916, ccxlv, med.-spec., 241-272.
Soukhanoff, S. A. (Psychoneuroses of war time.) Russk. Vrach., Petrogr., 1915, xiv, 437-442.
Soukhanoff, S. A. (Psychoneuroses of wartime.) Russk. Vrach., Petrogr., 1915, xiv, 437-442.
Soukhanoff, S. A. Psychopathies de guerre. Assemblée scientifique de l’hôpital de Notre-Dame-des-Affligés et de l’asile psychiatrique Novoznamenskaia, 7 août, 1915.
Soukhanoff, S. A. War Psychopathies. Scientific Assembly of the Hospital of Our Lady of the Afflicted and the Novoznamenskaia Psychiatric Asylum, August 7, 1915.
Soukhanoff, S. A. Symptômes nerveux accompagnant l’abasourdissement par l’explosion des obus. Gazette médicale russe, 1915.
Soukhanoff, S. A. Nervous symptoms accompanying the shock of artillery shell explosions. Russian Medical Gazette, 1915.
Soukhanoff, S. A. (Psychoneuroses of wartime). Russk. Vrach., Petrogr., 1915, v. 14, pp. 437-442, pp. 800-804, pp. 841-843.
Soukhanoff, S. A. (Psychoneuroses of wartime). Russk. Vrach., Petrogr., 1915, v. 14, pp. 437-442, pp. 800-804, pp. 841-843.
Soukhanoff, S. A. (Influence of wind contusion on the central nervous system.) Russk. Vrach., Petrogr., 1915, v. 14, pp. 1010-1013.
Soukhanoff, S. A. (The effect of wind contusion on the central nervous system.) Russk. Vrach., Petrogr., 1915, v. 14, pp. 1010-1013.
Soukhanoff, S. A. (Data on the question of psychoses in time of war). Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 160, 165, 204, 271.
Soukhanoff, S. A. (Data on the issue of psychoses during wartime). Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 160, 165, 204, 271.
Soukhanoff, S. A. (Present condition of science concerning traumatic neurosis, questions of its study and treatment from the viewpoint of military medicine). Voyenno-Med. J., Petrogr., 1916, v. 245, med.-spec. pt., pp. 241-272.
Soukhanoff, S. A. (Current state of science on traumatic neurosis, issues related to its study and treatment from a military medicine perspective). Voyenno-Med. J., Petrogr., 1916, v. 245, med.-spec. pt., pp. 241-272.
Soulshow, H. Sur la névrose traumatique avec lésion du labyrinthe. Gaz. méd. russe, No. 35, 1915.
Soulshow, H. On traumatic neurosis with labyrinth injury. Russian Med. Gaz., No. 35, 1915.
Souques, A. Monoplégies hystéro-traumatiques chez les soldats. Rev. neurol., 1914-15, v. 222, pp. 403-405.
Souques, A. Hystero-traumatic monoplegies in soldiers. Neurology Review, 1914-15, v. 222, pp. 403-405.
Souques, A. Contractures ou pseudo-contractures hystéro-traumatiques. Rev. neurol., Par., 1914-15, v. 222, pp. 430-431.
Souques, A. Hysterical trauma contractures or pseudo-contractures. Rev. neurol., Par., 1914-15, v. 222, pp. 430-431.
Souques, A. A propos des contractures hystéro-traumatiques. Rev. neurol., Par., 1914-15, v. 222, p. 437.
Souques, A. About Hystero-Traumatic Contractures. Neurology Review, Paris, 1914-15, vol. 222, p. 437.
Souques, A. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, p. 471.
Souques, A. Discussion on how to handle skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, p. 471.
Souques, A. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Discussion de Vincent. Rev. neurol., Par., 1916, v. 29, pp. 585-586.
Souques, A. On nerve accidents caused by the explosion of large charges of explosives. Discussion by Vincent. Rev. neurol., Paris, 1916, vol. 29, pp. 585-586.
Souques, A. (Synaesthesialgia in certain forms of painful neuritis: its treatment by rubber gloves.) Soc. de Neurol., May 6, 1915. Rev. Neurol., July, 1915.
Souques, A. (Synaesthesialgia in some types of painful neuritis: treating it with rubber gloves.) Soc. de Neurol., May 6, 1915. Rev. Neurol., July, 1915.
Souques, A. Aréflexie généralisée chez un blessé du crâne. Rev. neurol., Par., 1917, v. 33, pp. 33-34.
Souques, A. Generalized arreflexia in a skull injury patient. Neurology Review, Paris, 1917, v. 33, pp. 33-34.
Souques, A. et Mégévand, J. Un cas de camptocormie ancienne traitée et guérie par l’électrothérapie persuasive. Rev. neurol., Par., 1917, v. 24, pp. 142-143.
Souques, A. and Mégévand, J. A case of ancient camptocormia treated and cured by persuasive electrotherapy. Rev. neurol., Paris, 1917, v. 24, pp. 142-143.
Souques, Mégévand et Donnet, V. Importance de l’analyse précoce du liquide céphalo-rachidien pour le diagnostic des syndrômes cérébromédullaires dûs au “vent de l’explosif.” Bull. et mém. soc. d’hôp. de Par., 1915, v. 39, pp. 917-926.
Souques, Mégévand and Donnet, V. Importance of early analysis of cerebrospinal fluid for the diagnosis of cerebromedullary syndromes caused by "explosive blasts." Bull. et mém. soc. d’hôp. de Par., 1915, v. 39, pp. 917-926.
Souques et Rosanoff-Saloff, Mme. La camptocormie. Rev. neurol., Par., 1914, 15, v. 221, pp. 937-939.
Souques and Rosanoff-Saloff, Mrs. Camptocormia. Neurology Review, Paris, 1914, 15, v. 221, pp. 937-939.
Southard, E. E. Shell Shock and After. (Shattuck Lecture.) Bos. M. & S. J., 1918, clxxix, 73.
Southard, E. E. Shell Shock and After. (Shattuck Lecture.) Bos. M. & S. J., 1918, 179, 73.
Southard, E. E. The Training School of Psychiatric Social Work at Smith College. II. A Lay Reaction to Psychiatry. Mental Hygiene, II, October, 1918.
Southard, E. E. The Training School of Psychiatric Social Work at Smith College. II. A Lay Reaction to Psychiatry. Mental Hygiene, II, October, 1918.
Southard, E. E. and Solomon, H. C. Neurosyphilis. Boston, 1917, pp. 398-425.
Southard, E. E. and Solomon, H. C. Neurosyphilis. Boston, 1917, pp. 398-425.
Souttar, H. S. Points arising in nerve injuries. Brit. Med. Jour., 1917, ii, 817.
Souttar, H. S. Issues Related to Nerve Injuries. Brit. Med. Jour., 1917, ii, 817.
Spaulding, Edith R. The Training School of Psychiatric Social Work at Smith College. III. The Course in Social Psychiatry. Mental Hygiene, II, October, 1918.
Spaulding, Edith R. The Training School for Psychiatric Social Work at Smith College. III. The Course in Social Psychiatry. Mental Hygiene, II, October, 1918.
Specht. Zur Psychopathologie der Fahnenflucht. Münch. med. Wchnschr., 1915, 4. 621, p. 267.
Specht. On the Psychopathology of Desertion. Münch. med. Wchnschr., 1915, 4. 621, p. 267.
Spielmeyer, W. Zur Behandlung “traumatischer” Epilepsie. Münch. med. Wchnschr., 1915, v. 62, pp. 342-344.
Spielmeyer, W. On the treatment of "traumatic" epilepsy. Münch. med. Wchnschr., 1915, v. 62, pp. 342-344.
Spielmeyer, W. Zur Behandlung “traumatischer Epilepsie” nach Hirnschüssverletzung. Med. Klin., Berl. u. Wien, v. 111, p. 344.
Spielmeyer, W. On the treatment of "traumatic epilepsy" after a head injury. Med. Klin., Berlin and Vienna, vol. 111, p. 344.
Spillmann. Travaux du centre neurologique de Nancy. Rev. neurol., Par., 1914-15, v. 22, p. 1191.
Spillmann. Work from the Neurological Center of Nancy. Neurology Review, Paris, 1914-15, vol. 22, p. 1191.
Spillman. Psychoses et psychonévroses de guerre. Société de Méd. de Nancy, 1915.
Spillman. War Psychoses and Psychoneuroses. Society of Medicine of Nancy, 1915.
Squire, J. Edward. Medical Hints. Oxford War Primers, 1915.
Squire, J. Edward. Medical Tips. Oxford War Primers, 1915.
Stasser, M. La rééducation professionnelle de mutilés de guerre. Arch. méd. Belges, 1917, v. 47, pp. 236-241.
Stasser, M. The vocational rehabilitation of war amputees. Arch. méd. Belges, 1917, v. 47, pp. 236-241.
Stankovic, R. Ueber tödlich verlaufende Tetanie. Wien. Klin. Wchnschr., 1917, 30, 1107-8.
Stankovic, R. About deadly tetany. Wien. Klin. Wchnschr., 1917, 30, 1107-8.
St. Clair-Thomson, W. Functional cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-15 (sect. Laryngol.), v. 8, pp. 118-119.
St. Clair-Thomson, W. Functional cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-15 (sect. Laryngol.), v. 8, pp. 118-119.
Stearns, A. W. The psychiatric examination of recruits. J. Am. M. A., Chicago, 1918, v. 70, pp. 229-231.
Stearns, A. W. The psychiatric evaluation of recruits. J. Am. M. A., Chicago, 1918, v. 70, pp. 229-231.
Steiner. Neurologie und Psychiatrie im Kriegslazarett. Ztschr. f. d. ges. Neurol. u. Psychiat., Berl., 1915, v. 30, pp. 305-318.
Steiner. Neurology and Psychiatry in the War Hospital. Journal of General Neurology and Psychiatry, Berlin, 1915, vol. 30, pp. 305-318.
Stelzner, H. Aktuelle Massensuggestionen. Arch. f. Psychiat., Berl., 1914-15, v. 55, No. 2, pp. 365-388.
Stelzner, H. Current Mass Suggestions. Arch. f. Psychiat., Berl., 1914-15, v. 55, No. 2, pp. 365-388.
Sterz. Neuritis im Gebiete des Plexus lumbo-sacralis und hysterische Abasie nach Typhus. Deutsche med. Wchnschr., Berl. u. Wien, 1915, v. 111, p. 331.
Sterz. Neuritis in the area of the lumbosacral plexus and hysterical ataxia after typhus. German Medical Weekly, Berlin and Vienna, 1915, v. 111, p. 331.
Stevenson, W. F. A note on “wind contusions” in war. Brit. M. J., Lond., 1915, ii, p. 338.
Stevenson, W. F. A note on “wind contusions” in war. Brit. M. J., Lond., 1915, ii, p. 338.
Stevenson, W. F. Note on the cause of death due to high explosive shells in unwounded men. Ibid., 450.
Stevenson, W. F. Note on the cause of death from high explosive shells in uninjured men. Ibid., 450.
Stewart, Purves. Diagnoses of nervous diseases (War neurology). 1916, E. B. Treat Co., New York.
Stewart, Purves. Diagnoses of Nervous Diseases (War Neurology). 1916, E. B. Treat Co., New York.
Stewart, P. and Evans, Arthur. Nerve injuries and treatment. 1916, Oxford Univ. Press.
Stewart, P. and Evans, Arthur. Nerve injuries and treatment. 1916, Oxford Univ. Press.
Steyerthal. Die Hysterie im Kriege. Neurol. Centralbl., 37, Nr. 16, 1918.
Steyerthal. The Hysteria in War. Neurol. Centralbl., 37, No. 16, 1918.
Stiefler, G. Ein Fall von genuinen Narkolepsie. Neurol. Centralbl., 37, Nr. 11, 1918.
Stiefler, G. A Case of Genuine Narcolepsy. Neurol. Centralbl., 37, No. 11, 1918.
Stier, E. Dienstbeschädigung und Rentenversorgung bei Psychopathen. Die militärärztliche Sachsverständigentätigkeit auf dem Gebiete des Ersatzwesens und der militärischen Versorgung. Erste Teil., pp. 140-174, Jena, Fischer, 1917.
Stier, E. Damage to Service and Pension Provision for Psychopaths. The military medical expert's work in the field of compensation and military support. First Part., pp. 140-174, Jena, Fischer, 1917.
Stier, E. Wie kann der Entstehung von Kriegsneurosen bei der Feldarmee vorgebeugt werden? Deutsche mil. ärztl. Ztschr., Berl., 1918, 47, 60-72.
Stier, E. How can we prevent the development of shell shock in the army? German Military Medical Journal, Berlin, 1918, 47, 60-72.
Stier, E. Zur militärischen Beurteilung nervöser Krankheitzustände, speziell der Epilepsie. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, pp. 1153 and 1190-1196.
Stier, E. On the military assessment of nervous disorders, particularly epilepsy. German Medical Weekly, Leipzig and Berlin, 1916, vol. 42, pp. 1153 and 1190-1196.
Stiles, Harold J. Operative treatment of nerve injuries. Amer. Jour. Orthop. Surg., 1918, xvi, 351.
Stiles, Harold J. Surgical treatment of nerve injuries. American Journal of Orthopedic Surgery, 1918, 16, 351.
Stivers, C. G. Testing the aviation candidate. So. Calif. Prac., 1917, xxxii, 169.
Stivers, C. G. Testing the aviation candidate. Southern California Practice, 1917, vol. 32, p. 169.
Stookey, Byron. Gunshot wounds of the peripheral nerves. Surg. Gynec. and Obst., Chic., 1916, v. 23, pp. 639-656.
Stookey, Byron. Gunshot wounds of the peripheral nerves. Surg. Gynec. and Obst., Chic., 1916, v. 23, pp. 639-656.
Stookey, B. Gunshot wounds of peripheral nerves. S. G. O., 1916, xxiii, 639.
Stookey, B. Gunshot wounds of peripheral nerves. S. G. O., 1916, xxiii, 639.
Stookey, B. Surgical considerations of peripheral nerve injuries. Surg. Gynecol. and Obstet., 1918, xxvii, 362.
Stookey, B. Surgical considerations of peripheral nerve injuries. Surg. Gynecol. and Obstet., 1918, xxvii, 362.
Stopford, John S. B. So-called functional symptoms in organic nerve injuries. Lancet, Lon., 1918, i, 795.
Stopford, John S. B. Functional symptoms in organic nerve injuries. Lancet, London, 1918, i, 795.
Stopford, John S. B. Pathological diagnosis in gunshot injuries of peripheral nerves. Lancet, Lon., 1918, ii, 445.
Stopford, John S. B. Pathological diagnosis in gunshot injuries of peripheral nerves. Lancet, Lon., 1918, ii, 445.
Stopford, John, S. B. Trophic disturbances in gunshot injuries of peripheral nerves. Lancet, Lon., 1918, i, 465.
Stopford, John, S. B. Trophic disturbances in gunshot injuries of peripheral nerves. Lancet, London, 1918, 1, 465.
Strain of War on the Nervous System. Hospital, Lond., 1917, v. 61, pp. 415-416.
Strain of War on the Nervous System. Hospital, Lond., 1917, v. 61, pp. 415-416.
Strain of war on the nervous system. Hospital, Lon., 1917, lxii, 415.
Effects of war on the nervous system. Hospital, Lon., 1917, lxii, 415.
Stransky, E. Einiges zur Psychiatrie und zur Psychologie im Kriege. Wien. med. Wchnschr., 1915, lxv., 1025-1030.
Stransky, E. Some Thoughts on Psychiatry and Psychology in War. Vienna. Med. Wchnschr., 1915, lxv., 1025-1030.
Strasser, Charlot. Ueber Unfall und Militärneurosen. Cor.-Bl. f. Schwerze Aerzt., 1917, No. 9, pp. 257-274.
Strasser, Charlot. On Accidents and Military Neuroses. Cor.-Bl. f. Schwerze Aerzt., 1917, No. 9, pp. 257-274.
Strauss, H. Die Balneotherapie als Heilfactor bei Kriegsverletzungen und Erkrankungen. Med. Klin., Berl. u. Wien, 1915, v. 111, p. 659, also Ztschr. f. ärtzl. Fortbild., Jena, 1915, v. 12, pp. 581-586.
Strauss, H. The Balneotherapy as a Healing Factor for War Injuries and Illnesses. Med. Klin., Berlin and Vienna, 1915, vol. 111, p. 659, also in Journal of Medical Education, Jena, 1915, vol. 12, pp. 581-586.
Strümpell, A. Ueber Wesen und Entstehung der hysterischen Krankheiterscheinungen. Deutsche Ztschr. f. Nervenh., Leipz., 1916, v. 55, No. 1-3.
Strümpell, A. On the Nature and Origin of Hysterical Illness Symptoms. German Journal of Neurology, Leipzig, 1916, vol. 55, No. 1-3.
Sudden turning grey of the hair. Lancet, Lond., 1915, ii, p. 613.
Sudden graying of the hair. Lancet, Lond., 1915, ii, p. 613.
Symonds, C. P. Some diseases which have become common among soldiers in this country. II. Hysteria. Guy’s Hosp. Gaz., Lond., 1916, xxx, 444-448.
Symonds, C. P. Some diseases that have become common among soldiers in this country. II. Hysteria. Guy’s Hosp. Gaz., Lond., 1916, xxx, 444-448.
Syms, J. L. M. Hysterics as seen at a base hospital. Practitioner, 1918, ci, 90.
Syms, J. L. M. Hysterics observed at a base hospital. Practitioner, 1918, ci, 90.
Syndrômes nerveux provoqués par l’éclatement des gros projectiles de guerre. Rev. gén. de clin. et de thérap., Par., 1915, v. 29, pp. 379-380.
Nerve syndromes caused by the explosion of large war projectiles. Rev. gén. de clin. et de thérap., Par., 1915, v. 29, pp. 379-380.
Syring. Zur Behandlung der Schädelschüsse im Felde. München med. Wchnschr., 1915, v. 621, pp. 592-593.
Syring. For the treatment of gunshot wounds to the head in the field. Munich Med. Wchnschr., 1915, v. 621, pp. 592-593.
Szasz, Pest T. Ueber funktionelle Hörstörungen. Wien. klin. Wchnschr., 1915, v. 622, p. 117, also pp. 818-819.
Szasz, Pest T. On Functional Hearing Disorders. Wien. klin. Wchnschr., 1915, v. 622, p. 117, also pp. 818-819.
Sztanojevits, L. Neurologisches während des Feldzunges. Med. Klin., Berl. u. Wien, 1915, v. 112, pp. 1155-1156.
Sztanojevits, L. Neurological issues during field service. Med. Klin., Berlin and Vienna, 1915, vol. 112, pp. 1155-1156.
Tanflyeff, P. I. Paraffin tumors, produced with a view of avoiding military service. Prakt. Vrach., S.-Peterb., 1914, xiii, 105, 120.
Tanflyeff, P. I. Paraffin tumors, created to avoid military service. Prakt. Vrach., S.-Peterb., 1914, xiii, 105, 120.
Taylor, J. Madison. Types of men as observed among recruits. Bos. M. & S. J., 1918, clxxix, 646.
Taylor, J. Madison. Types of men seen among recruits. Bos. M. & S. J., 1918, clxxix, 646.
Terrien, T. De quelques troubles visuels consécutives à l’éclatement des obus. Arch. d’ophth., Par., 1914-15. v. 34, pp. 633-650.
Terrien, T. On some visual disturbances following shell explosions. Arch. d’ophth., Par., 1914-15. v. 34, pp. 633-650.
Terrien, F. Remarques sur la rééducation des aveugles. Paris méd., 1916, v. 21, pp. 490-493.
Terrien, F. Comments on the rehabilitation of the blind. Paris méd., 1916, v. 21, pp. 490-493.
Tests for alleged deafness in exemption claims. N. Y. Med. Jour., 1917, cvi, 324.
Tests for alleged deafness in exemption claims. N. Y. Med. Jour., 1917, cvi, 324.
Tests for the Detection of Malingering. Lancet, Lond., 1916, ii, pp. 80-81.
Tests for the Detection of Malingering. Lancet, London, 1916, 2, pp. 80-81.
Terrien, F. et Vinsonneau. Hémianopsies d’origine corticale. Paris méd., 1916 (Part. méd.), v. 19, pp. 527-531.
Terrien, F. and Vinsonneau. Cortical hemianopsias. Paris méd., 1916 (Part. méd.), vol. 19, pp. 527-531.
Thibierge, G. La syphilis et l’armée. Paris, 1917, Masson et Cie.
Thibierge, G. Syphilis and the Army. Paris, 1917, Masson et Cie.
Thibierge, G. Syphilis and the Army. Military Medical Manuals, Univ. of London Press, 1918.
Thibierge, G. Syphilis and the Army. Military Medical Manuals, University of London Press, 1918.
Thiemann, H. Schädelschüsse. Münch. med. Wchnschr., 1915, v. 621, pp. 593-595.
Thiemann, H. Skull Shots. Munich Medical Weekly, 1915, vol. 621, pp. 593-595.
Thoma. Neurosen nach Kriegsverletzungen. Wien. klin. Wchnschr., 1916, xxix, 1412, 1509, 1541, 1574.
Thoma. Neuroses from war injuries. Vienna. Clin. Weekly, 1916, xxix, 1412, 1509, 1541, 1574.
Thomas, A. Hypertonie musculaire dans la paralysie radiale en voie d’amélioration. Sensations cutanées dans le domaine du nerf radial, provoquées par la pression de muscles qui reçoivent leur innervation du même nerf. Egarement des cylindraxes regénérés, destinés à la peau dans les nerfs musculaires. Soc. de Neurol., July 29, 1915. Revue Neurol., Aug.-Sept., 1915.
Thomas, A. Muscle hypertonicity in improving radial paralysis. Skin sensations in the area of the radial nerve, caused by pressure from muscles that are innervated by the same nerve. Misalignment of regenerated axons intended for the skin in muscle nerves. Soc. de Neurol., July 29, 1915. Revue Neurol., Aug.-Sept., 1915.
Thomas, A. La sensibilité douloureuse de la peau à la piqûre et au pincement dans la période de restauration des nerfs sectionnés après suture ou greffe. Soc. de Neur., Feb. 3, 1916. Revue Neurol., Feb., 1916.
Thomas, A. The painful sensitivity of the skin to pinching and pricking during the recovery period of severed nerves after stitching or grafting. Soc. de Neur., Feb. 3, 1916. Revue Neurol., Feb., 1916.
Thomas, A. (Multiple paralyses of the cranial nerves.) Soc. de Neurol., July 1, 1915.
Thomas, A. (Multiple paralysis of the cranial nerves.) Soc. de Neurol., July 1, 1915.
Thomas, André. Topoparesthésies cicatricielles: examen des troncs nerveux et des cicatrices dans les blessures des nerfs. Paris méd., 1916 (Part. méd.), v. 19, pp. 535-537.
Thomas, André. Topoparesthésies cicatricielles: examination of nerve trunks and scars in nerve injuries. Paris méd., 1916 (Part. méd.), v. 19, pp. 535-537.
Thomas, André. Hypermyotonie ou contracture secondaire dans les paralysies des nerfs périphériques par blessure de guerre. Paris méd., 1916, v. 21, pp. 203-209.
Thomas, André. Hypertonicity or secondary contraction in peripheral nerve paralysis due to war injuries. Paris med., 1916, v. 21, pp. 203-209.
Thomas, André et Ceillier, H. Hémianesthésie cérébrale par blessure de guerre. Rev. neurol., Par., 1917, v. 24, pp. 34-38.
Thomas, André et Ceillier, H. Brain hemianesthesia due to war injury. Rev. neurol., Par., 1917, v. 24, pp. 34-38.
Thomas, E. Troubles cardiaques et service militaire. Rev. méd. de la Suisse, Rom., Genève, 1917, v. 37, pp. 270-283.
Thomas, E. Heart Issues and Military Service. Swiss Medical Review, Rom., Geneva, 1917, vol. 37, pp. 270-283.
Thomas, J. J. Types of neurological cases seen at a base hospital. J. Nerv. and Ment. Dis., N. Y., 1916, v. 44, pp. 495-502.
Thomas, J. J. Types of neurological cases seen at a base hospital. J. Nerv. and Ment. Dis., N. Y., 1916, v. 44, pp. 495-502.
Thomas, J. Lynn. Peripheral shock and its central effects. Brit. M. J., Lond., 1916, ii, pp. 44-45.
Thomas, J. Lynn. Peripheral shock and its central effects. Brit. M. J., Lond., 1916, ii, pp. 44-45.
Thomas, J. L. Death from high explosives without wounds. Brit. M. J., Lond., 1917, v. 1, p. 599.
Thomas, J. L. Death from high explosives without injuries. Brit. M. J., Lond., 1917, v. 1, p. 599.
Thomson, Campbell. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Neurol. sect.), pp. 36-37.
Thomson, Campbell. Shell shock without visible signs of injury. Proc. Roy. Soc. Med., Lond., 1915-16, v. 9 (Neurol. sect.), pp. 36-37.
Thomson, D. G. A descriptive record of the conversion of a county asylum into a war hospital for sick and wounded soldiers in 1915. J. Ment. Sc., Lond., 1916, v. 62, pp. 109-135.
Thomson, D. G. A detailed account of turning a county asylum into a war hospital for sick and injured soldiers in 1915. J. Ment. Sc., Lond., 1916, v. 62, pp. 109-135.
Thorne, Bezly. Treatment by physical methods of mental disabilities induced by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 39-41.
Thorne, Bezly. Treatment using physical methods for mental disabilities caused by the war. Proc. Roy. Soc. Med., Lond., 1917-18, v. 10 (sect. Balneol.), pp. 39-41.
Thorne, W. B. The soldier’s heart. Practitioner, 1916, xcvi, 551.
Thorne, W. B. The soldier’s heart. Practitioner, 1916, 96, 551.
Three Cases of Head Injury. Guy’s Hosp. Gaz. Lond., 1916, v. 30, pp. 297-299.
Three Cases of Head Injury. Guy's Hosp. Gaz. Lond., 1916, v. 30, pp. 297-299.
Tilley, Herbert. Two cases of functional aphonia following bursting of a shell in close proximity. Proc. Roy. Soc. Med., Lond., 1915-16, v. 8 (Laryngol. sect.), p. 155.
Tilley, Herbert. Two cases of functional aphonia after a shell exploded nearby. Proc. Roy. Soc. Med., Lond., 1915-16, v. 8 (Laryngol. sect.), p. 155.
Timofieyeff, A. V. (Where do soldiers in the active army become insane?) Psikhiat. Gaz., Petrogr., 1915, v. 2, p. 261.
Timofieyeff, A. V. (Where do soldiers in the active army go insane?) Psychiatry Gazette, Petrograd, 1915, vol. 2, p. 261.
Timofieyeff, A. V. (Statistics of mental diseases in the active army in the present campaign.) Psikhiat. Gaz., Petrogr., 1915, v. 2, p. 341.
Timofieyeff, A. V. (Statistics on mental health issues in the active army in the current campaign.) Psikhiat. Gaz., Petrogr., 1915, v. 2, p. 341.
Timofieyeff, S. L. (Contractures of the fingers and toes in those who injure themselves to avoid military service.) Voyenno. Med. J., Petrogr., 1915, v. 242, pued. spec. pt., pp. 27-42.
Timofieyeff, S. L. (Contractures of the fingers and toes in individuals who harm themselves to evade military service.) Military Medical Journal, Petrograd, 1915, vol. 242, special publication, pp. 27-42.
Timofieyeff, S. L. (Self inflicted injuries and malingering among recruits under observation; according to data of the Kiyev military hospital for 1911.) Voyenno. Med. J., Petrogr., 1915, v. 243, pp. 591-630.
Timofieyeff, S. L. (Self-inflicted injuries and faking illness among recruits under observation; based on data from the Kyiv military hospital for 1911.) Voyenno. Med. J., Petrogr., 1915, v. 243, pp. 591-630.
Tinel, J. Les Blessures des Nerfs. Collection Horizon, Masson et Cie, Paris, 1917 (also trans. Engl., Phila.).
Tinel, J. The Injuries of Nerves. Horizon Collection, Masson and Co., Paris, 1917 (also translated into English, Philadelphia).
Tinel. Le signe du “fourmillement” dans les lésions des nerfs. Presse méd., Oct. 7, 1915.
Tinel. The sign of “tingling” in nerve lesions. Press Med., Oct. 7, 1915.
Tinel, J. Un cas de nystagmus fonctionnel. Rev. neurol., Par., 1914-15, v. 221, pp. 490-492.
Tinel, J. A case of functional nystagmus. Rev. neurol., Paris, 1914-15, v. 221, pp. 490-492.
Tinel, J. Paralysie fonctionnelle par stupeur musculaire. Rev. neurol., 1917, v. 24, pp. 500-501.
Tinel, J. Functional paralysis due to muscle shock. Rev. neurol., 1917, v. 24, pp. 500-501.
Tobias, E. Ergebnisse der bisherigen Kriegserfahrungen auf dem Gebiete des Nervensystems. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 62, p. 139.
Tobias, E. Results of Previous War Experiences in the Field of the Nervous System. German Medical Weekly, Leipzig and Berlin, 1916, v. 62, p. 139.
Todd, J. L. The retraining of disabled men. Am. Med., Burlington, Vt., 1917, v. 23, pp. 380-384.
Todd, J. L. The retraining of disabled men. Am. Med., Burlington, Vt., 1917, v. 23, pp. 380-384.
Tombleson, J. B. A series of military cases treated by hypnosis. Lancet, Lond., 1916, ii, pp. 709-710.
Tombleson, J. B. A series of military cases treated with hypnosis. Lancet, London, 1916, ii, pp. 709-710.
Tombleson, J. B. An account of twenty cases treated by hypnotic suggestion. J. Roy. Army Med. Corps, Lond., 1917, v. 29, pp. 340-346.
Tombleson, J. B. A report on twenty cases treated with hypnosis. J. Roy. Army Med. Corps, Lond., 1917, v. 29, pp. 340-346.
Tompkins, E. Stammering in connection with military service. Amer. Jour. Pub. Health, 1917, vii, 638.
Tompkins, E. Stuttering related to military service. Amer. Jour. Pub. Health, 1917, vii, 638.
Tooth, Howard H. Neurasthenia and psychasthenia. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 329-345.
Tooth, Howard H. Neurasthenia and psychasthenia. J. Roy. Army Med. Corps, Lond., 1917, v. 28, pp. 329-345.
Townsend, R. O. Two cases for comment. (I) Malingering or true neurosis. (II) Malingering or hysteria. Practitioner, Lond., 1917, xcix, 88-91.
Townsend, R. O. Two cases for discussion. (I) Malingering or genuine neurosis. (II) Malingering or hysteria. Practitioner, Lond., 1917, xcix, 88-91.
Traitement de l’anorexie mentale. J. de méd. et chir. prat., Par., 1916, v. 87, pp. 94-96.
Treatment of Anorexia Nervosa. J. de méd. et chir. prat., Par., 1916, v. 87, pp. 94-96.
Treatment of peripheral nerve injuries. Rev. of War Surg. & Med., 1918, i, No. 3, 40.
Treatment of peripheral nerve injuries. Rev. of War Surg. & Med., 1918, i, No. 3, 40.
Treatment of Shell Shock. N. Y. Med. Jour., 1917, cvi, 1142.
Treatment of Shell Shock. N. Y. Med. Jour., 1917, cvi, 1142.
Treatment of War Psychoses. Med. Press and Circ., Lond., 1916; pp. 507-508.
Treatment of War Psychoses. Med. Press and Circ., London, 1916; pp. 507-508.
Trombetta, E. Gli epilettici in zona di guerra. Gior. d. med. mil., Roma, 1918, lxvi, 54-58.
Trombetta, E. Epileptics in a War Zone. Military Medical Journal, Rome, 1918, lxvi, 54-58.
Trombetta, E. Gli inabili alle fatiche di guerra. Gior. di med. mil., Roma, 1917, lxv, 427-436.
Trombetta, E. Those unable for the hardships of war. Military Medical Journal, Rome, 1917, lxv, 427-436.
Trömner. Einen Fall von lokaler traumatischer Hysterie. Neurol. Centralbl., Leipz., 1915, p. 415.
Trömner. A case of local traumatic hysteria. Neurol. Centralbl., Leipzig, 1915, p. 415.
Trömner. Brown-Séquard-Lähmung durch Nackenschuss ohne Wirbelverletzung. Neurol. Centralbl., Leipz., 1915, p. 416.
Trömner. Brown-Séquard syndrome from a neck shot without vertebral injury. Neurol. Centralbl., Leipz., 1915, p. 416.
Trömner. (a) Lokale traumatische Hysterie. (b) Schuss durch den Hals. (c) Brown-Séquard-Lähmung durch Nackenschuss ohne Wirbelverletzung. (Abstract) Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 901-902.
Trömner. (a) Local traumatic hysteria. (b) Gunshot through the neck. (c) Brown-Séquard paralysis from a neck gunshot without spinal injury. (Abstract) Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 901-902.
Trömner. (a) Nachweis der Entartungsreaktion. (b) Mittlere Arm-Plexuslähmung. (c) Blutdruck- und Pulsanomalien bei organischen Nervenleiden. (d) Halsschüsse. (Abstract) Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 1021.
Trömner. (a) Evidence of degenerative reaction. (b) Average arm plexus paralysis. (c) Blood pressure and pulse anomalies in organic nerve diseases. (d) Neck injuries. (Abstract) German Medical Weekly, Berlin and Leipzig, 1915, v. 41, p. 1021.
Trotter, Robert H. Observations upon the condition known as D. A. H. Lancet, Lon., 1918, l, 371.
Trotter, Robert H. Observations on the condition known as D. A. H. Lancet, Lon., 1918, l, 371.
Troubles d’origine émotive chez le combattant. Progrès méd., Par., 1916, v. 31, p. 48.
Emotional issues in the soldier. Progrès méd., Par., 1916, v. 31, p. 48.
Truc, H. L’héméralopie dans l’armée. Montpel. méd., 1916, v. 39, pp. 269-273.
Truc, H. Night blindness in the army. Montpel. méd., 1916, v. 39, pp. 269-273.
Truelle, V., et Bouderlique, Mlle. Etat dépressif consécutif à une émotion de guerre. Ann. méd. psychol., Par., 1917, v. 73, pp. 595-602.
Truelle, V., and Bouderlique, Mlle. Depressive state following a war emotion. Ann. méd. psychol., Paris, 1917, v. 73, pp. 595-602.
Tsimken. (Experimental psychology in the nature of an objective means in the diagnosis of malingering.) Psikhiat. Gaz., Petrogr., 1915, v. 1, pp. 240-242.
Tsimken. (Experimental psychology as an objective method for diagnosing malingering.) Psikhiat. Gaz., Petrogr., 1915, v. 1, pp. 240-242.
Tsiplyayeff, P. I. (Simulation of fever, and measuring of the temperature in cadets.) Vestnik Obshtsh. Hig., Sudeb. i Prakt. Med., Petrogr., 1916, lii, 1277-1284.
Tsiplyayeff, P. I. (Simulating fever and measuring temperature in cadets.) Vestnik Obshtsh. Hig., Sudeb. i Prakt. Med., Petrogr., 1916, lii, 1277-1284.
Tubby, A. H. Cases of nerve concussion due to bullet and shell wounds. Brit. M. J., Lond., 1915, i, pp. 57-59.
Tubby, A. H. Cases of nerve concussion from bullet and shell wounds. Brit. M. J., Lond., 1915, i, pp. 57-59.
Tubby, A. H. Bullet wounds affecting the motor fibers of the external popliteal nerve. Brit. M. J., Lond., 1915, i. p. 333.
Tubby, A. H. Bullet wounds impacting the motor fibers of the external popliteal nerve. Brit. M. J., Lond., 1915, i. p. 333.
Tuke, Seymour. War and insanity. J. Ment. Sc., Lond., 1916, v. 62, pp. 818-819.
Tuke, Seymour. War and insanity. J. Ment. Sci., Lond., 1916, v. 62, pp. 818-819.
Tullidge, E. K. Shock neuroses et psychoses in present war. Penn. M. J., Athens, 1916, v. 19, pp. 778-782.
Tullidge, E. K. Shock neuroses and psychoses in the current war. Penn. M. J., Athens, 1916, v. 19, pp. 778-782.
Tulloch, A. B. Shell shock. Lancet, Lond., 1915, ii, p. 575.
Tulloch, A. B. Shell shock. The Lancet, London, 1915, ii, p. 575.
Tumiati, C. La guérison rapide du mutisme de guerre par la méthode de Lombard. Rev. neurol., Par., 1917, v. 24, p. 475.
Tumiati, C. The quick healing of war mutism using the Lombard method. Rev. neurol., Par., 1917, v. 24, p. 475.
Turck, Fenton, B. Wound and shell shock and their cure. N. Y. Med. Jour., 1918, cvii, 901.
Turck, Fenton, B. Wound and shell shock and their treatment. N. Y. Med. Jour., 1918, cvii, 901.
Türk, N. Ueber psychische Störungen bei Verschütteten nach ihrer Belebung. Wien. klin. Wchnschr., 1917, v. 29, pp. 910-913.
Türk, N. On psychological disorders in those trapped after their revival. Vienna Clinical Weekly, 1917, vol. 29, pp. 910-913.
Turlais. Vent d’obus. Arch. méd. d’Angers, 1915, xix, 113-117.
Turlais. Shell blast. Arch. méd. d’Angers, 1915, xix, 113-117.
Turner, W. A. Nervous and mental shock; arrangements for the care of cases coming from overseas. Lancet, Lon., 1916, i, 1073.
Turner, W. A. Nervous and mental shock; plans for taking care of cases coming from overseas. Lancet, Lon., 1916, i, 1073.
Turner, W. A. Remarks on cases of nervous and mental shock observed in the base hospitals in France. Brit. M. J., Lond., 1915, i, 833-835. Also J. Roy. Army Med. Corps, Lond., 1915, xxiv, 343-352.
Turner, W. A. Comments on instances of nervous and mental shock seen in the base hospitals in France. Brit. M. J., Lond., 1915, i, 833-835. Also J. Roy. Army Med. Corps, Lond., 1915, xxiv, 343-352.
Turner, W. A. Cases of nervous and mental shock. Brit. M. J., London, 1915, i, pp. 833-835.
Turner, W. A. Cases of nervous and mental shock. Brit. M. J., London, 1915, i, pp. 833-835.
Turner, W. A. Arrangements for the care of cases of nervous and mental shock coming from overseas. J. Roy. Army Med. Corps, Lond., 1916, v. 271, pp. 619-626; also Lancet, Lond., 1916, i, pp. 1073-1075.
Turner, W. A. Plans for handling cases of nervous and mental shock from overseas. J. Roy. Army Med. Corps, Lond., 1916, v. 271, pp. 619-626; also Lancet, Lond., 1916, i, pp. 1073-1075.
Turner, W. A. Remarks made on paper of Sir John Collie, “The management of neurasthenia and allied disorders contracted in the Army.” “Recalled to Life,” 1917, Sept., No. 2, pp. 251-252.
Turner, W. A. Comments on Sir John Collie's paper, “Managing neurasthenia and related disorders acquired in the Army.” “Recalled to Life,” Sept. 1917, No. 2, pp. 251-252.
Turrell, W. J. Electric treatment of trench foot and frost-bite. Pract., Lond., 1916, v. 96, pp. 52-61.
Turrell, W. J. Electric treatment of trench foot and frostbite. Pract., Lond., 1916, v. 96, pp. 52-61.
Turrell, W. J. Electrotherapy at a base hospital. Lancet, Lond., 1915, i, pp. 229-231.
Turrell, W. J. Electrotherapy at a base hospital. Lancet, Lond., 1915, i, pp. 229-231.
Turrell, Sibley, et al. Discussion of electrical treatment of wounds. Proc. Roy. Soc. Med., Lond., 1914-15 (Electro-therap. sect.), pp. 35-52.
Turrell, Sibley, et al. Discussion of electrical treatment for wounds. Proc. Roy. Soc. Med., Lond., 1914-15 (Electro-therap. sect.), pp. 35-52.
Turrell, W. J. The electrical treatment of the wounded. Lancet, Lond., 1916, ii, pp. 1005-1008; also Am. J. Electrotherap. and Radiol., N. Y., 1917, v. 35, 215-221.
Turrell, W. J. The electrical treatment of the wounded. Lancet, London, 1916, ii, pp. 1005-1008; also American Journal of Electrotherapy and Radiology, New York, 1917, v. 35, 215-221.
Uhthoff, W. Ueber Kriegsblinde und Kriegsblinden-Fürsorge. Berl. klin. Wchnschr., 1916, v. 53, pp. 78-81.
Uhthoff, W. On War Blindness and Care for the War Blind. Berl. klin. Wchnschr., 1916, v. 53, pp. 78-81.
Uhthoff. Augenärztliche Erfahrungen und Betrachtungen über Kriegsblinde. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, p. 1468.
Uhthoff. Ophthalmological experiences and observations on war blind. German medical weekly, Leipzig and Berlin, 1916, vol. 42, p. 1468.
U. S. War Dept., Surgeon General’s Office. War surgery of the nervous system; a digest of the important medical journals and books published during the European War. Wash., 1917, Gov. Print. Off., 360 p., 8o.
U. S. War Dept., Surgeon General’s Office. War surgery of the nervous system; a summary of the key medical journals and books published during the European War. Wash., 1917, Gov. Print. Off., 360 p., 8o.
Urbantschitsch, E. Rasche Heilung der Symptome der im Kriege entstandenen traumatischen Neurose. Wien. klin. Wchnschr., 1916, xxix, 1051.
Urbantschitsch, E. Quick healing of the symptoms of the traumatic neurosis caused by the war. Wien. klin. Wchnschr., 1916, xxix, 1051.
Urstein, M. S. (Mental diseases caused by the war, and mental disturbances caused by wounds of the brain.) Russk. Vrach., Petrogr., 1916, xv, 246-249.
Urstein, M. S. (Mental illnesses caused by the war, and mental issues caused by brain injuries.) Russk. Vrach., Petrogr., 1916, xv, 246-249.
Utilisation des indisciplinés en temps de guerre. Progrès Méd., Par., 1916, No. 3, pp. 70-72.
Using the Undisciplined During Wartime. Prog. Med., Par., 1916, No. 3, pp. 70-72.
Vachet, Pierre. Les troubles mentaux consécutifs au shock des explosifs modernes. Thèses de Paris, 1915-16, No. 15.
Vachet, Pierre. Mental disorders following the shock of modern explosives. Theses of Paris, 1915-16, No. 15.
Valobra, I. Sui disturbi nervosi detti di natura riflessa in neurologia di guerra. Policlin., Roma, 1917, xxiv, sez. med., 349-370.
Valobra, I. Reflex nerve disorders in war neurology. Policlin., Rome, 1917, xxiv, med. sect., 349-370.
Van Schevensteen, A. Considerations sur les conjonctivites provoquées. Clin. opht., Par., 1916, v. 21, pp. 595-603.
Van Schevensteen, A. Thoughts on provoked conjunctivitis. Clin. opht., Par., 1916, v. 21, pp. 595-603.
Vaquez, H. and Donzelot, E. L’aptitude fonctionnelle cardiaque du soldat. Ann. de méd., Par., 1917, v. 4, pp. 377-390.
Vaquez, H. and Donzelot, E. The cardiac functional capacity of the soldier. Ann. de méd., Par., 1917, v. 4, pp. 377-390.
Veale, Rawdon A. Some cases of so-called functional paresis arising out of the war and their treatment. J. Roy. Army Med. Corps, Lond., 1917, v. 29, pp. 607-614.
Veale, Rawdon A. Some cases of so-called functional weakness resulting from the war and their treatment. J. Roy. Army Med. Corps, Lond., 1917, v. 29, pp. 607-614.
Verdelet, Louis. Un cas de lésion nerveuse traumatique. Caducée, Par., 1916, v. 16, p. 118.
Verdelet, Louis. A case of traumatic nerve injury. Caducée, Par., 1916, v. 16, p. 118.
Verger, Henri. Abandon de poste en présence de l’ennemi dans une fugue épileptique. Jour. de méd. de Bordeaux, 1915-16, v. 45, pp. 63-65.
Verger, Henri. Abandon of post in the presence of the enemy during an epileptic episode. Journal of Medicine of Bordeaux, 1915-16, vol. 45, pp. 63-65.
Verger, H. La notion de consolidation dans les névroses traumatiques des sinistrés du travail et des blessés de guerre. Progrès méd., Par., 1916, v. 31, pp. 118-122.
Verger, H. The concept of consolidation in traumatic neuroses of work-related victims and war injuries. Progrès méd., Par., 1916, v. 31, pp. 118-122.
Verger, H. et Penaud, R. Les hémiplégies tardives consécutives aux blessures de la région cervicale. Rev. neurol., Par., 1917, v. 24, pp. 281-288.
Verger, H. et Penaud, R. Late hemiplegias following injuries to the cervical region. Neurology Rev., Paris, 1917, v. 24, pp. 281-288.
Viets, Henry. Shell shock. J. Am. M. Ass., Chicago, 1917, v. 69, pp. 1779-1786.
Viets, Henry. Shell shock. J. Am. M. Ass., Chicago, 1917, v. 69, pp. 1779-1786.
Viets, Henry. London war hospitals. Boston M. and S. J., 1917, v. 176, p. 222.
Viets, Henry. London War Hospitals. Boston M. and S. J., 1917, v. 176, p. 222.
Villaret, Maurice. Au sujet des séquelles nerveuses des traumatismes crânio-cérébraux de la guerre (une statistique de 250 cas). Bull. Acad. de méd., Par., 1916, v. 76, p. 420.
Villaret, Maurice. Regarding the nervous sequelae of cranio-cerebral trauma from the war (a statistic of 250 cases). Bull. Acad. de méd., Par., 1916, v. 76, p. 420.
Villaret, Maurice. Vingt-cinq cas d’astéréognosie reliquat de blessures crânio-cérébrales? Presse méd., Par., 1916, v. 241, p. 56.
Villaret, Maurice. Twenty-five cases of astereognosis resulting from cranio-cerebral injuries? Med. Press, Paris, 1916, v. 241, p. 56.
Villaret, Maurice. Discussion de la conduite à tenir vis-à-vis des blessures du crâne—par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 458-460; also p. 473.
Villaret, Maurice. Discussion on how to deal with skull injuries—by P. Marie. Rev. neurol., Paris, 1916, vol. 29, pp. 458-460; also p. 473.
Villaret, Maurice. Propositions de réforme, les évaluations d’invalidité et les décisions concernant les militaires atteints de lésions ou troubles du système nerveux. Montpel. méd., 1916, v. 39, pp. 372-386.
Villaret, Maurice. Reform proposals, disability assessments, and decisions concerning military personnel with injuries or disorders of the nervous system. Montpel. méd., 1916, v. 39, pp. 372-386.
Villaret, Maurice et Faure-Beaulieu, M. Les anesthésies corticales à topographie atypique dans les traumatismes crâniens. Paris méd., 1916, v. 19, pp. 514-518.
Villaret, Maurice and Faure-Beaulieu, M. Atypical cortical anesthesias in head injuries. Paris méd., 1916, v. 19, pp. 514-518.
Villaret, Maurice et Faure-Beaulieu, M. L’épilepsie tardive consécutive aux traumatismes de guerre crânio-cérébraux. Montpel. méd., 1916, v. 39, p. 61.
Villaret, Maurice and Faure-Beaulieu, M. Late epilepsy following cranio-cerebral war injuries. Montpel. méd., 1916, v. 39, p. 61.
Villaret, Maurice et Faure-Beaulieu, M. L’évolution des traumatismes de guerre crânio-cérébraux. Rev. neurol., Par., 1916, v. 24, pp. 832-833.
Villaret, Maurice and Faure-Beaulieu, M. The evolution of head and brain war injuries. Neurology Review, Paris, 1916, vol. 24, pp. 832-833.
Villaret, Maurice et Faure-Beaulieu, M. Les troubles nerveux tardifs consécutifs aux traumatismes crânio-cérébraux de guerre. Rev. gén. de path. de guerre, 1916, No. 3, pp. 213-245.
Villaret, Maurice and Faure-Beaulieu, M. Late nerve disorders following war-related head injuries. Gen. Rev. of War Pathology, 1916, No. 3, pp. 213-245.
Villaret, Maurice et Faure-Beaulieu, M. Le signe de la flexion du gros orteil par percussion du tendon achilléen. Presse méd., Par., 1917, v. 25, 531-532.
Villaret, Maurice and Faure-Beaulieu, M. The sign of the flexion of the big toe from percussion of the Achilles tendon. Med. Press, Paris, 1917, v. 25, 531-532.
Villaret, Maurice et Rives, A. L’hémianopsie en quadrant, reliquat isolé de certaines blessures crânio-cérébrales. Bull. et. mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 1234-1237.
Villaret, Maurice and Rives, A. Quadrant hemianopsia, an isolated remnant of certain cranio-cerebral injuries. Bull. et. mém. Soc. méd. d’hôp. de Par., 1915, v. 39, pp. 1234-1237.
Villaret, Maurice et Rives, A. L’hémianopsie bilatérale homonyme en quadrant seul reliquat de blessures graves du lobe occipital. Paris méd., 1916, v. 19 (part. méd.), pp. 20-23.
Villaret, Maurice and Rives, A. Homonymous bilateral hemianopsia in the quadrant as the only remaining effect of severe injuries to the occipital lobe. Paris méd., 1916, v. 19 (part. méd.), pp. 20-23.
Villaret, Maurice et Mignard, M. Le syndrôme psychique résiduel des traumatismes crânio-cérébraux de la guerre. Paris méd., 1916, (part. méd.), v. 21, pp. 209-214.
Villaret, Maurice and Mignard, M. The residual psychological syndrome of war-related cranio-cerebral trauma. Paris méd., 1916, (part. méd.), v. 21, pp. 209-214.
Vilvandre, G. Radiography in gunshot wounds of the skull. Arch. of Radiol. and Elec., 1916, 306.
Vilvandre, G. X-rays in gunshot wounds of the skull. Arch. of Radiol. and Elec., 1916, 306.
Vilvandre, G. and Morgan, J. D. Movements of foreign bodies in the brain. Arch. of Radiol. and Elec., 1916, xxi, 22.
Vilvandre, G. and Morgan, J. D. Movements of foreign bodies in the brain. Arch. of Radiol. and Elec., 1916, xxi, 22.
Vinaj, G. S. La terapia fisica in tempo di guerra. Idrol. e climat., Firenze, 1917, v. 28, pp. 30-45.
Vinaj, G. S. Physical therapy in wartime. Hydrology and climatology, Florence, 1917, v. 28, pp. 30-45.
Vincent, Armand et Wilhelm, André. Un cas curieux de blessure du crâne par éclat d’obus. Paris méd., 1915 (part. méd.) v. 17, pp. 118-119.
Vincent, Armand and Wilhelm, André. A curious case of skull injury from shell fragment. Paris méd., 1915 (med. part.) vol. 17, pp. 118-119.
Vincent, Cl. Du pronostic des troubles nerveux d’ordre réflexe. Persistance ou augmentation des troubles vasomoteurs et de l’amyotrophie malgré une mobilisation active et prolongée du membre malade. Soc. de Neurol., Nov. 1916.
Vincent, Cl. On the prognosis of reflex nervous disorders. Persistence or increase of vasomotor issues and muscle atrophy despite active and prolonged movement of the affected limb. Neurological Society, Nov. 1916.
Vincent, Cl. Note sur le traitement de certaines troubles fonctionnels. Rev. neurol., Par., 1916, v. 23, pp. 102-104.
Vincent, Cl. Note on the treatment of certain functional disorders. Rev. neurol., Paris, 1916, v. 23, pp. 102-104.
Vincent, Cl. Au sujet de l’hystérie et de la simulation. Rev. neurol., 1916, v. 23, pp. 104-107.
Vincent, Cl. About hysteria and simulation. Rev. neurol., 1916, v. 23, pp. 104-107.
Vincent, Cl. Discussion de la conduite à tenir vis-à-vis des blessures du crâne par P. Marie. Rev. neurol., Par., 1916, v. 29, pp. 471-472.
Vincent, Cl. Discussion on how to handle skull injuries by P. Marie. Rev. neurol., Paris, 1916, v. 29, pp. 471-472.
Vincent, Cl. Quelques rectifications à l’article de M. Rimbaud; Sur le traitement des psychonévroses de guerre. Marseille méd., 1916-17, liii, 936-940.
Vincent, Cl. A few corrections to Mr. Rimbaud's article; On the treatment of war psychoneuroses. Marseille méd., 1916-17, liii, 936-940.
Vincent, Cl. La rééducation intensive des hystériques invétérés. Bull. et mém. Soc. méd., d’ hôp. de Par., 1916, 21 juillet.
Vincent, Cl. The intensive rehabilitation of chronic hysterics. Bull. et mém. Soc. méd., d’ hôp. de Par., 1916, July 21.
Vincent, Cl. Sur les accidents nerveux déterminés par la déflagration de fortes charges d’explosifs. Rev. neurol., Par., 1916, v. 29, pp. 573-574.
Vincent, Cl. On nerve accidents caused by the explosion of large amounts of explosives. Neurological Review, Paris, 1916, vol. 29, pp. 573-574.
Vincent, Cl. Le traitement des phénomènes hystériques par la “rééducation intensive.” Arch. de méd. électr., Bordeaux, 1916, v. 24, pp. 405-416.
Vincent, Cl. Treating hysterical phenomena with "intensive rehabilitation." Arch. de méd. électr., Bordeaux, 1916, v. 24, pp. 405-416.
Vincent, Cl. Variations du réflexe achilléen chez certaines hommes atteints de troubles physiopathiques des membres inférieurs. Rev. neurol., Par., 1917, v. 24, pp. 224-231.
Vincent, Cl. Variations of the Achilles reflex in certain men with physiological and pathological disorders of the lower limbs. Neurological Review, Paris, 1917, v. 24, pp. 224-231.
Vincent, Cl. Sur le traitement et le pronostic des phénomènes physiopathiques. Rev. neurol., Par., 1917, v. 24, pp. 537-544.
Vincent, Cl. On the Treatment and Prognosis of Physiopathological Phenomena. Rev. neurol., Paris, 1917, vol. 24, pp. 537-544.
Vincent, W. Use of asylums as military hospitals. J. Ment. Sc., Lond., 1916, v. 62, pp. 174-178.
Vincent, W. Use of asylums as military hospitals. J. Ment. Sc., Lond., 1916, v. 62, pp. 174-178.
Viruboff, M. A. (Psychoses and psychoneuroses of the war.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 70-72.
Viruboff, M. A. (Psychoses and psychoneuroses of the war.) Psychiatric Gazette, Petrograd, 1915, vol. 2, pp. 70-72.
Viruboff, M. A. (Organization of aid to insane soldiers.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 168-171.
Viruboff, M. A. (Organization of support for mentally ill soldiers.) Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 168-171.
Viruboff, M. A. (Necessity for constructing hospitals for soldiers suffering from psychoneuroses.) Psikhiat. Gaz., Petrogr., 1916, v. 3, p. 194.
Viruboff, M. A. (Need to build hospitals for soldiers dealing with mental health issues.) Psikhiat. Gaz., Petrogr., 1916, v. 3, p. 194.
Viruboff, M. A. (Organization of the care of insane warriors.) Sovrem. Psikhiat., Mosk., 1916, v. 10, pp. 19-27.
Viruboff, M. A. (Organizing care for mentally ill soldiers.) Modern Psychiatr., Moscow, 1916, vol. 10, pp. 19-27.
Viry, H. L’instinct génésique et la guerre actuelle. Rev. gén. de clin. et de thérap., Par., 1916, v. 30, pp. 355-357.
Viry, H. The Reproductive Instinct and the Current War. Gen. Rev. of Clinical and Therapy, Paris, 1916, vol. 30, pp. 355-357.
Vitaut, L. Un cas d’œdème de striction. Rev. gén. de clin. et de thérap., Par., 1916, xxx, 551.
Vitaut, L. A case of striction edema. Rev. gén. de clin. et de thérap., Par., 1916, xxx, 551.
Vlasoff, Y. P. Cases of artificial phlegmons caused by injections of kerosene. Voyenno-Med. J., Petrogr., 1915, ccxlii, med.-spec. pt., 63-73.
Vlasoff, Y. P. Cases of artificial phlegmons caused by injections of kerosene. Voyenno-Med. J., Petrogr., 1915, ccxlii, med.-spec. pt., 63-73.
Vlasto, Michael. Two cases of functional aphonia. J. Roy. Nav. M. Serv., Lond., 1917, v. 3, pp. 113-115.
Vlasto, Michael. Two cases of functional aphonia. J. Roy. Nav. M. Serv., Lond., 1917, v. 3, pp. 113-115.
Vogt, H. Die Kriegsneurosen (in: Handbuch der Therapie der Nervenkrankheiten, Jena, Gustav Fischer, 1916).
Vogt, H. War Neuroses (in: Handbook of Therapy for Nervous Disorders, Jena, Gustav Fischer, 1916).
Vogt, H. Die Neurosen im Kriege (in: Die Kriegsbeschädigungen des Nervensystems, Wiesbaden, Bergmann, 1917).
Vogt, H. Neuroses in War (in: The War Damages of the Nervous System, Wiesbaden, Bergmann, 1917).
Von Eberts, E. M. Functional re-education and vocational training of soldiers disabled in war. Canad. M. Ass. J., Toronto, 1917, v. 7, pp. 193-200.
Von Eberts, E. M. Functional rehabilitation and job training for soldiers disabled in war. Canad. M. Ass. J., Toronto, 1917, v. 7, pp. 193-200.
Vorschläge zur Abfindung der Kriegsneurosen auf Grund dieser Erfahrungen. Med. Cor.-Bl. d. Württemb. ärztl. Landesver. Stuttg., 1916, v. 86, p. 42.
Suggestions for the settlement of war neuroses based on these experiences. Med. Cor.-Bl. d. Württemb. ärztl. Landesver. Stuttg., 1916, v. 86, p. 42.
Voskresenski, M. K. (Brief annual review of the activity of the psychiatric organization of the Russian Society of the Red Cross at the armies of the southwestern front.) Russk. Vrach., Petrogr., v. 15, pp. 12-16.
Voskresenski, M. K. (Brief annual review of the activities of the psychiatric organization of the Russian Society of the Red Cross at the armies of the southwestern front.) Russk. Vrach., Petrogr., v. 15, pp. 12-16.
Voss, G. Zur Frage der Simulation bei Soldaten. Deutsche med. Wchnschr., Berl. u. Leipz., 1916, No. 48, pp. 1476-1477.
Voss, G. On the issue of simulation in soldiers. German Med. Weekly, Berlin and Leipzig, 1916, No. 48, pp. 1476-1477.
Vvedenski, I. N. (Cases of wartime psychoses in children.) Sovrem. Psikhiat., Mosk., 1916, v. 10, pp. 1-8.
Vvedenski, I. N. (Cases of wartime psychoses in children.) Modern Psychiatry, Moscow, 1916, vol. 10, pp. 1-8.
Wagener. Arbeitstherapie und Rentenabschätzung bei Kriegsneurotiker. Neurol. Centralbl., 37, Nr. 16, 1918.
Wagener. Occupational therapy and pension assessment for war neurotics. Neurol. Centralbl., 37, No. 16, 1918.
Wagner. Ueberblick über die in der Heil- und Pflegeanstalt Giessen behandelten nerven und geisteskranken Soldaten. München med. Wchnschr., 1916, No. 15, pp. 548-550.
Wagner. Overview of the soldiers with nerve and mental disorders treated at the Giessen Healing and Care Institution. Munich Medical Weekly, 1916, No. 15, pp. 548-550.
Wagner, v. Jauregg. Nervöse Störungen nach eine oberflächliche Verletzung am Rücken durch Schrapnellschuss. Wien. klin. Wchnschr., 1915, v. 28, p. 190.
Wagner, v. Jauregg. Nerve issues following a superficial injury to the back from a shrapnel wound. Wien. klin. Wchnschr., 1915, v. 28, p. 190.
Wallace, Cuthbert C. Traumatic shock. Report of fourth session of Research Soc. of American Red Cross in France. Med. Bull., 1918, i, 417.
Wallace, Cuthbert C. Traumatic shock. Report of the fourth session of the Research Society of the American Red Cross in France. Med. Bull., 1918, i, 417.
Wallace, W. Methods of examining the vision of recruits and soldiers with special reference to assumed and real defects. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 471-489.
Wallace, W. Methods for assessing the vision of recruits and soldiers, focusing on both suspected and actual defects. J. Roy. Army Med. Corps, Lond., 1916, v. 26, pp. 471-489.
Waller, A. D. Galvanometric observation of the emotivity of a normal subject (English) during the German air raid of Whit-Sunday, May 19, 1918. Lancet, Lon., 1918, I, 916.
Waller, A. D. Galvanometric observation of the emotional response of a typical subject (English) during the German air raid on Whit-Sunday, May 19, 1918. Lancet, Lon., 1918, I, 916.
Walther, Ch. Traumatisme de la région scapulaire. Décollement de l’omoplate. Paralysie totale du membre supérieur d’origine psychique. Bull. et mém. soc. de chir. de Par., 1914, v. 40, pp. 1380-1382.
Walther, Ch. Trauma of the shoulder region. Separation of the scapula. Total paralysis of the upper limb of psychological origin. Bull. et mém. soc. de chir. de Par., 1914, v. 40, pp. 1380-1382.
War and Incidence of Insanity. Med. Officer, Lond., 1917, v. 16, Oct. 6.
War and Incidence of Insanity. Med. Officer, Lond., 1917, v. 16, Oct. 6.
War and the Incidence of Insanity. Pub. Health J., Toronto, 1917, v. 8, p. 30.
War and the Incidence of Insanity. Pub. Health J., Toronto, 1917, v. 8, p. 30.
War and Insanity. Med. Officer, Lond., 1916, v. 15, p. 43.
War and Insanity. Med. Officer, Lond., 1916, v. 15, p. 43.
War and Insanity. Hospital, Lond., 1917, v. 60, p. 5.
War and Insanity. Hospital, London, 1917, vol. 60, p. 5.
War and Mental Hospitals. Med. Officer, Lond., 1916, v. 15, p. 108.
War and Mental Hospitals. Med. Officer, Lond., 1916, v. 15, p. 108.
War and Nervous Breakdowns. Lancet, 1915, i, pp. 189-190.
War and Nervous Breakdowns. Lancet, 1915, i, pp. 189-190.
War and the Nervous System. M. J. Australia, Sydney, 1916, v. 1, p. 205.
War and the Nervous System. M. J. Australia, Sydney, 1916, vol. 1, p. 205.
War and Neuroses. J. Am. M. A., Chicago, 1917, v. 67, pp. 647-648.
War and Neuroses. J. Am. M. A., Chicago, 1917, v. 67, pp. 647-648.
War and Other Causes of Insanity. Brit. M. J., Lond., 1917, i, p. 301 (also 1917, i, p. 310).
War and Other Causes of Insanity. Brit. M. J., Lond., 1917, i, p. 301 (also 1917, i, p. 310).
War and Psychoanalysis. N. York M. J., 1916, v. 104, p. 1251.
War and Psychoanalysis. N. York M. J., 1916, v. 104, p. 1251.
War neuroses and psychoses. Mil. Surgeon, Wash., 1916, v. 38, pp. 320, 428, 545.
War neuroses and psychoses. Mil. Surgeon, Wash., 1916, v. 38, pp. 320, 428, 545.
War Surgery of the Nervous System. Pub. Office Surgeon General, 1917.
War Surgery of the Nervous System. Pub. Office Surgeon General, 1917.
Watson-Williams, P. Functional cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-15 (sect. Laryngol.), v. 8, p. 119.
Watson-Williams, P. Functional cases. Discussion. Proc. Roy. Soc. Med., Lond., 1914-15 (sect. Laryngol.), v. 8, p. 119.
Weber, L. W. Ueber Granatkontusion (Gaupp). Neurol. Centralbl., 1915, v. 34, p. 780.
Weber, L. W. On Grenade Contusion (Gaupp). Neurological Central Journal, 1915, v. 34, p. 780.
Weber, L. W. Zur Entstehung der Unfallsneurosen. München med. Wchnschr., 1915, v. 62, p. 400.
Weber, L. W. On the Development of Accident Neuroses. Munich Med. Weekly, 1915, v. 62, p. 400.
Weber, F. Parkes. Aspects of death and correlated aspects of life in art, epigram, and poetry. 3rd ed., London, 1918.
Weber, F. Parkes. Aspects of death and related aspects of life in art, epigrams, and poetry. 3rd ed., London, 1918.
Weekers, L. L’héméralopie chez les soldats. Arch. d’opht., Par., 1916, v. 35, pp. 73-88.
Weekers, L. Night blindness in soldiers. Arch. d’opht., Par., 1916, v. 35, pp. 73-88.
Weekers, L. Night Blindness (hemeralopia). Med. Press and Circ., Lond., 1916, v. 102, pp. 386-387.
Weekers, L. Night Blindness (hemeralopia). Medical Press and Circular, London, 1916, vol. 102, pp. 386-387.
Weichbrodt, R. Einige Bemerkungen zur Behandlung d. Kriegsneurotikern. Monatschr. f. Psych. u. Neurol., 43, 1918.
Weichbrodt, R. Some Comments on the Treatment of War Neurotics. Monthly Journal of Psychology and Neurology, 43, 1918.
Weil, Gaupp, Weintrand, Sänger, Lilienstein. Diskussion über Kriegserfahrungen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 956-960.
Weil, Gaupp, Weintrand, Sänger, Lilienstein. Discussion about war experiences. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 956-960.
Welch, W. H. Medical problems of the war. Johns Hopkins Hosp. Bull., Balt., 1917, Apr., p. 156.
Welch, W. H. Medical issues of the war. Johns Hopkins Hosp. Bull., Balt., 1917, Apr., p. 156.
Wessman, R. Die Beurteilung von Augensymptomen bei Hysterischen. Abhandl. a. d. Geb. d. Augenh., Halle a. S., 1916, v. 10, No. 1/2 also Cor. Bl. f. Schweize Aerzte, 1917, No. 6, p. 191.
Wessman, R. The Assessment of Ocular Symptoms in Hysterical Patients. Proceedings from the Field of Ophthalmology, Halle a. S., 1916, v. 10, No. 1/2 also Correspondence. Journal for Swiss Physicians, 1917, No. 6, p. 191.
West, C. E. Special discussion on warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 92-93.
West, C. E. Special discussion on warfare injuries and mental health issues. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 92-93.
Westphal, A. Hysterischen beziehungsweise psychogenen Hör- und Sprachstörungen bei Soldaten. Med. Klin., Berl. u. Wien, 1915, v. 112, p. 1303.
Westphal, A. Hysterical or psychogenic hearing and speech disorders in soldiers. Med. Klin., Berlin and Vienna, 1915, v. 112, p. 1303.
Westphal, A. Ueber Augensymptome in einem Falle von traumatischer Hysterie (mit Krankenvorstellung). (Abstract) Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 1202.
Westphal, A. About Eye Symptoms in a Case of Traumatic Hysteria (with Patient Presentation). (Abstract) German Medical Weekly, Berlin and Leipzig, 1915, vol. 41, p. 1202.
Westphal, A. (a) Hysterische Taubstummheit bei Kriegsteilnehmern. (b) Hörstummheit. Deutsche med. Wchnschr., Leipz. u. Berl., 1915, v. 412, pp. 1560-1561.
Westphal, A. (a) Hysterical Deaf-Muteness in War Participants. (b) Deafness. German Med. Weekly, Leipzig and Berlin, 1915, v. 412, pp. 1560-1561.
Westphal, A. und Hübner, A. H. Ueber nervöse und psychische Erkrankungen im Kriege. Med. Klin., Berl. u. Leipz., 1915, v. 111, pp. 381-383; also pp. 413-417.
Westphal, A. and Hübner, A. H. On Nervous and Psychological Disorders in War. Med. Klin., Berlin and Leipzig, 1915, vol. 111, pp. 381-383; also pp. 413-417.
Wexberg, Erwin. Indirekte Gehirnverletzung durch Schädelschuss. Wien. klin. Wchnschr., 1916, v. 29, pp. 418-419.
Wexberg, Erwin. Indirect brain injury from skull shot. Vienna. Clin. Wchnschr., 1916, v. 29, pp. 418-419.
Weyert. Militär-psychiatrische Beobachtungen und Erfahrungen. Samml. zwangl. Abhandl. u. d. Geb. d. Nerv. u. Geistesk., Halle a. S., 1915, v. 11, No. 2 to No. 4, pp. 1-145.
Weyert. Military-psychiatric Observations and Experiences. Collection of Coercive Treatises in the Field of Nervous and Mental Diseases, Halle a. S., 1915, vol. 11, No. 2 to No. 4, pp. 1-145.
Weygandt, W. Versorgung der Neurosen und Psychosen im Felde. Med. Klin., Berl. u. Wien, v. 102, pp. 1503-1505.
Weygandt, W. Treatment of neuroses and psychoses in the field. Med. Klin., Berl. u. Wien, v. 102, pp. 1503-1505.
Weygandt, W. Psychosen. Berl. klin. Wchnschr., 1914, v. 512, p. 1949.
Weygandt, W. Psychoses. Berl. klin. Wchnschr., 1914, v. 512, p. 1949.
Weygandt, W. Geisteskrankheiten im Kriege. München med. Wchnschr., 1914, ii, v. 61, pp. 2109-2112.
Weygandt, W. Mental Illness in War. Munich Med. Wchnschr., 1914, ii, v. 61, pp. 2109-2112.
Weygandt, W. Kriegspsychiatrische Begutachtungen. München. med. Wchnschr., 1915, v. 622, pp. 1257-1259; also Neurol. Centralbl. Leipz., 1915, v. 34, pp. 925-926.
Weygandt, W. War Psychiatry Assessments. Munich. Medical Weekly, 1915, v. 622, pp. 1257-1259; also Neurology Central Journal Leipzig, 1915, v. 34, pp. 925-926.
Weygandt, W. Kriegspsychosen. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 43-44.
Weygandt, W. War Psychoses. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 43-44.
Weygandt, W. Psychische Erkrankungen bei Soldaten. Deutsche med. Wchnschr., Leipz. u. Berl., 1915, xli, 540, 694.
Weygandt, W. Mental Illnesses in Soldiers. German Med. Weekly, Leipzig and Berlin, 1915, xli, 540, 694.
Weygandt, W. Psychose auf Grund von Hirntrauma. Deutsche med. Wchnschr., Leipz. u. Berl., 1915, v. 41, p. 1354.
Weygandt, W. Psychosis Due to Brain Trauma. German Medical Journal, Leipzig and Berlin, 1915, v. 41, p. 1354.
Weygandt, W. Kriegspsychiatrische Begutachtungen. Med. Klin., Berl. u. Wien, 1915, v. 112, p. 1084.
Weygandt, W. War Psychiatry Evaluations. Med. Clin., Berlin and Vienna, 1915, vol. 112, p. 1084.
Weygandt, W. Psychosen. Berl. klin. Wchnschr., 1915, v. 521, p. 224.
Weygandt, W. Psychoses. Berl. klin. Wchnschr., 1915, v. 521, p. 224.
Weygandt, W. Kriegseinflüsse und Psychiatrie. Jahresk. ärtzl. Fortbild., München, 1915, v. 5, pp. 15-50.
Weygandt, W. Effects of War and Psychiatry. Yearbook for Medical Training, Munich, 1915, vol. 5, pp. 15-50.
Weygandt, W. Kriegspsychiatrische Begutachtungen. Psychiat.-neurol. Wchnschr., Halle a. S., 1915-16, v. 17, pp. 215-217.
Weygandt, W. War Psychiatry Assessments. Psychiat.-neurol. Weekly, Halle a. S., 1915-16, v. 17, pp. 215-217.
Weygandt, W. Die Geisteskrankheiten im Kriege (in Die Kriegsbeschädigungen des Nervensystems. Wiesbaden, Bergmann, 1917).
Weygandt, W. Mental Illnesses in War (in The War Injuries of the Nervous System. Wiesbaden, Bergmann, 1917).
Whale, H. L. Functional aphonia. Proc. Roy. Soc. Med., Lond., 1914-15, (Laryngol. sec.), v. 8, p. 117.
Whale, H. L. Functional aphonia. Proc. Roy. Soc. Med., Lond., 1914-15, (Laryngol. sec.), v. 8, p. 117.
White, Ernest W. Shell shock and neurasthenia in the hospitals in the western command; observations. Brit. Med. Jour., 1918, i, 421.
White, Ernest W. Shell shock and neurasthenia in the hospitals in the western command; observations. Brit. Med. Jour., 1918, i, 421.
White, J. Renfrew. The extent and nature of the sensory loss in musculospiral paresis. J. Roy. Army Med. Corps, Lond., 1916, pp. 340-353.
White, J. Renfrew. The scope and characteristics of sensory loss in musculospiral paralysis. J. Roy. Army Med. Corps, Lond., 1916, pp. 340-353.
White, R. P. Effects of dinitrobenzine and other nitrosubstitution products of the aromatic series on the workmen employed in the manufacture of high explosives. (See Oliver’s “Dangerous Trades,” p. 475.)
White, R. P. Effects of dinitrobenzene and other nitrosubstitution products of the aromatic series on the workers engaged in the production of high explosives. (See Oliver’s “Dangerous Trades,” p. 475.)
White, S. E. Nerve-strain and war. Lancet, Lond., 1915, ii, 1317.
White, S. E. Nerve-strain and war. Lancet, London, 1915, ii, 1317.
White, W. A. The state hospital and the war. Mental Hyg., Concord, N. H., 1917, i, 377-382.
White, W. A. The state hospital and the war. Mental Hygiene, Concord, NH, 1917, 1, 377-382.
Wicart. Les mutilations de l’ouïe par les détonations. Comment elles guérrissent. Presse méd., Par., 1917, v. 25, p. 8.
Wicart. Hearing damage from explosions. How they heal. Presse méd., Par., 1917, v. 25, p. 8.
Wideroe, S. (Shell shock.) Norsk. Tidsskr. i mil., Hälsov., Kristiania, 1917, v. 21, pp. 77-90.
Wideroe, S. (Shell shock.) Norsk. Tidsskr. i mil., Hälsov., Kristiania, 1917, v. 21, pp. 77-90.
Wiener, E. Hitzschlag und Sonnenstich. Wien. med. Wchnschr., 1915, v. 28, pp. 721-722.
Wiener, E. Heat Stroke and Sunstroke. Wien. med. Wchnschr., 1915, v. 28, pp. 721-722.
Wietfeldt. Avitaminose als Ursache der Nachtblindheit im Felde. München med. Wchnschr., 1915, v. 622, p. 1743.
Wietfeldt. Vitamin deficiency as a cause of night blindness in the field. Munich med. Wchnschr., 1915, v. 622, p. 1743.
Wietung. Leitsätze der funktionellen Nachbehandlung kriegschirurgischer Schäden. Leipz., 1915, 43 p., 8o.
Wietung. Guidelines for the functional aftercare of war surgery injuries. Leipzig, 1915, 43 p., 8o.
Williams, Frankwood E. and Brown, Mabel W. Neuropsychiatry and the war, a bibliography with abstracts. Ment. Hyg., Concord, N. H., 1917, v. 1, pp. 409-474.
Williams, Frankwood E. and Brown, Mabel W. Neuropsychiatry and the war, a bibliography with summaries. Ment. Hyg., Concord, N. H., 1917, v. 1, pp. 409-474.
Williamson, R. T. Remarks on the treatment of neurasthenia and psychasthenia following shell shock. Brit. M. J., Lond., 1917, ii, 713-715.
Williamson, R. T. Comments on treating neurasthenia and psychasthenia after shell shock. Brit. M. J., Lond., 1917, ii, 713-715.
Williamson, R. T. Treatment of neurasthenia following shell shock. Brit. M. J., Lond., ii, pp. 713-715.
Williamson, R. T. Treatment of neurasthenia after shell shock. Brit. M. J., Lond., ii, pp. 713-715.
Wilmanns. Dienstbrauchbarkeit der Psychopathen. München med. Wchnschr. 1916, No. 44, p. 1558.
Wilmanns. Usefulness of psychopaths. Münchener medizinische Wochenschrift. 1916, No. 44, p. 1558.
Wilson, Gordon. Special discussion on warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 91-92.
Wilson, Gordon. Special discussion on warfare injuries and neuroses. Proc. Roy. Soc. Med., Lond., 1917, v. 10 (sec. Otol.), pp. 91-92.
Wilson, J. G. Effects of high explosives on the ear. Brit. Med. Jour., 1917, i, 353.
Wilson, J. G. Effects of high explosives on the ear. British Medical Journal, 1917, vol. 1, p. 353.
Wilson, J. G. Further report on the effects of high explosives on the ear. Brit. Med. Jour., 1917, i, 578.
Wilson, J. G. Additional report on the impact of high explosives on the ear. British Medical Journal, 1917, i, 578.
Wiltshire. A contribution to the etiology of shell shock. Lancet, Lond., 1916, i, 1207-1212.
Wiltshire. A contribution to the causes of shell shock. Lancet, London, 1916, i, 1207-1212.
Wind of the Cannon Ball. Monde méd., Par., 1915, v. 25, pp. 214-217.
Wind of the Cannon Ball. Medical World, Paris, 1915, vol. 25, pp. 214-217.
Wiszwianski. Demonstration von Kriegsneurosen und Neuralgien besonders Ischias. Fortsche. d. Med., Berl. u. Leipz., 1915-16, v. 2, p. 24.
Wiszwianski. Demonstration of war neuroses and neuralgias, especially sciatica. Fortschritte der Medizin, Berlin and Leipzig, 1915-16, vol. 2, p. 24.
Witry. Le centre neurologique et psychiatrique de la forteresse de Metz en 1914. Ann. méd. psychol., Par., 1916-17, v. 73, pp. 96-101.
Witry. The neurological and psychiatric center of the fortress of Metz in 1914. Ann. méd. psychol., Par., 1916-17, v. 73, pp. 96-101.
Wittermann, E. Kriegspsychiatrische Erfahrungen aus der Front. Wien. klin. Wchnschr., 1916, v. 29, p. 1315.
Wittermann, E. Experiences in War Psychiatry from the Front. Vienna. Clinical Weekly, 1916, v. 29, p. 1315.
Wittermann, E. Kriegspsychiatrische Erfahrungen aus der Front. Münch. med. Wchnschr., 1915, v. 62, pp. 1164-1166; also, Neurol. Centralbl., Leipz., 1915, v. 34, p. 928.
Wittermann, E. Military psychiatric experiences from the front. Münch. med. Wchnschr., 1915, v. 62, pp. 1164-1166; also, Neurol. Centralbl., Leipz., 1915, v. 34, p. 928.
Wohlwill. Aphasische Störungen infolge von Kopfschüssen. (Abstract) Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, p. 1603.
Wohlwill. Aphasia disorders resulting from gunshot wounds. (Abstract) German med. weekly, Berl. and Leipz., 1915, v. 41, p. 1603.
Wohlwill. Demonstration: 3 Patienten mit aphasischen Störungen infolge von Kopfschüssen. Berl. klin. Wchnschr., 1915, v. 511, pp. 168-169.
Wohlwill. Demonstration: 3 patients with aphasia due to gunshot wounds. Berl. klin. Wchnschr., 1915, v. 511, pp. 168-169.
Wohlwill. Sprachstörung nach Schussverletzung. Neurol. Centralbl., Leipz., 1915, v. 34, p. 46.
Wohlwill. Speech disorder following a gunshot wound. Neurol. Centralbl., Leipzig, 1915, v. 34, p. 46.
Woitachewsky. Contribution à l’étude de l’hystéro-traumatisme. Rev. Neurol., Par., 1917, v. 24, p. 476.
Woitachewsky. Contribution to the study of hysterical trauma. Rev. Neurol., Paris, 1917, vol. 24, p. 476.
Wolff. Erhebliche Sprachstörung nach Schussverletzung am Kopf. Deutsche med. Wchnschr., Berl. u. Leipz., 1916, No. 3, p. 92.
Wolff. Significant speech disorder after gunshot injury to the head. German med. Wchnschr., Berl. u. Leipz., 1916, No. 3, p. 92.
Wolfsohn, Julian M. The predisposing factors of war psychoneuroses. Lancet, Lond., 1918, i, pp. 177-180; also J. Am. M. A., Chicago, 1918, v. 70, pp. 303-308.
Wolfsohn, Julian M. The factors that lead to war-related mental health issues. Lancet, Lond., 1918, i, pp. 177-180; also J. Am. M. A., Chicago, 1918, v. 70, pp. 303-308.
Wollenberg, R. Lazarettbeschäftigung und Militärnervenheilstätte. Deut. Med. Woch., 1915, xli, 757.
Wollenberg, R. Hospital employment and military nerve sanatorium. Deut. Med. Woch., 1915, xli, 757.
Wollenberg. Psychisch-nervöse Störungen im Kriegszeiten. Deutsche med. Wchnschr., Berl. u. Leipz., 1914, v. 102, p. 1927.
Wollenberg. Psychological and Nervous Disorders in Wartime. German Medical Weekly, Berlin and Leipzig, 1914, v. 102, p. 1927.
Wollenberg. Nervöse Erkrankungen bei Kriegsteilnehmern. München med. Wchnschr., 1914, No. 44, pp. 2181-2183.
Wollenberg. Nervous disorders in war participants. Munich Med. Weekly, 1914, No. 44, pp. 2181-2183.
Wollenberg, R. Ueber die Wirkungen der Granatschütterung. Neurol. Centralbl., Leipz., 1915, v. 34, pp. 922-924.
Wollenberg, R. On the Effects of Shell Shock. Neurol. Centralbl., Leipzig, 1915, v. 34, pp. 922-924.
Wollenberg, R. Lazarettbeschäftigung und Militärnervenheilstätte. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 41, pp. 757-760.
Wollenberg, R. Hospital Work and Military Nerve Treatment Center. German Med. Weekly, Berlin and Leipzig, 1915, vol. 41, pp. 757-760.
Wollenberg, R. Weitere Erfahrungen mit der Heilbeschäftigung nervenkranker Soldaten. Deutsche med. Wchnschr., Leipz. u. Berl., 1916, v. 42, pp. 6-7.
Wollenberg, R. Further experiences with the therapeutic employment of soldiers with nerve disorders. German Medical Weekly, Leipzig and Berlin, 1916, vol. 42, pp. 6-7.
Wollenberg, R. Zur Lehre von den traumatischen Neurosen. Kriegsärztliche Erfahrungen. Beitr. z. klin. Chir., Tübing., 1916, ci (Kriegschir. Hefte V), 343-357.
Wollenberg, R. On the Theory of Traumatic Neuroses. Military Medical Experiences. Contributions to Clinical Surgery, Tübingen, 1916, ci (Military Surgery Notebooks V), 343-357.
Wollenberg. Zur Vorgeschichte du Kriegsneurotiker. Neurol. Centralbl., 37, Nr. 16, 1918.
Wollenberg. On the Background of War Neurotics. Neurological Central Journal, 37, No. 16, 1918.
Work in France and Germany (for the care of disabled soldiers). Recalled to Life, Lond., 1917, pp. 180-186, 3 pl.
Work in France and Germany (for the care of disabled soldiers). Recalled to Life, Lond., 1917, pp. 180-186, 3 pl.
Wright, Almroth E. (Sir) and Colebrook, Leonard. Acidosis of shock and suspended circulation. Lancet, Lon., 1918, i, 763.
Wright, Almroth E. (Sir) and Colebrook, Leonard. Acidosis of shock and suspended circulation. Lancet, Lon., 1918, i, 763.
Wright, H. P. Suggestions for a further classification of cases of so-called shell shock. Canad. M. Ass. J., Toronto, 1917, v. 7, pp. 629-635.
Wright, H. P. Suggestions for a further classification of cases of so-called shell shock. Canad. M. Ass. J., Toronto, 1917, v. 7, pp. 629-635.
Wyroubow, N. A. (Traumatic Psychoneuroses.) Moscow, 1915.
Wyroubow, N. A. (Traumatic Psychoneuroses.) Moscow, 1915.
Wyroubow, N. A. (Contribution à l’étude des psychoses et des psychonévroses, observées à la suite de la guerre.) Gaz. (russe) Psychiat. 1915, No. 5. (Rev. neurol., Par., 1917, v. 24, p. 468.)
Wyroubow, N. A. (Contribution to the study of psychoses and psychoneuroses observed after the war.) Gaz. (Russian) Psychiat. 1915, No. 5. (Rev. neurol., Paris, 1917, v. 24, p. 468.)
Wyroubow, N. A. Les altérations de la voix et de la parole dans la psychose ou psychonévrose par contusion. Rev. neurol., Par., 1916, v. 24, pp. 312-316.
Wyroubow, N. A. Changes in Voice and Speech in Psychosis or Psychoneurosis Caused by Concussion. Rev. neurol., Paris, 1916, vol. 24, pp. 312-316.
Yealland, Lewis R. Hysterical Disorders of Warfare. Macmillan, 1918.
Yealland, Lewis R. Hysterical Disorders of Warfare. Macmillan, 1918.
Yegiazaroff, I. N. (Psycho- and neuropathological observations on the wounded and contused in the present war; mutism and deaf-mutism in wounded and contused; demonstration in four cases.) Trudi, Protok. Imp. Kavkazsk. Med. Obsh., Tiflis, 1914-15, v. 51, pp. 81-83.
Yegiazaroff, I. N. (Psychological and neurological observations on the injured and bruised in the current war; mutism and deaf-mutism in the injured and bruised; case studies in four instances.) Proceedings, Protocol of the Imperial Caucasian Medical Society, Tiflis, 1914-15, v. 51, pp. 81-83.
Yerkes, R. M. The relation of psychology to military activities. Mental Hyg., Concord, N. H., i, pp. 371-376.
Yerkes, R. M. The connection between psychology and military operations. Mental Hygiene, Concord, N. H., i, pp. 371-376.
Yerkes, R. M. Psychology and national service. Psychol. Bull., Princeton, N. J., and Lancaster, Pa., 1917, v. 14, pp. 259-263; also Science, N. Y., and Lancaster, Pa., 1917, v. 46, pp. 101-103.
Yerkes, R. M. Psychology and national service. Psychol. Bull., Princeton, N. J., and Lancaster, Pa., 1917, v. 14, pp. 259-263; also Science, N. Y., and Lancaster, Pa., 1917, v. 46, pp. 101-103.
Yurman, N. A. (Neurasthenic psychoses in time of war). Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 139-142.
Yurman, N. A. (Neurasthenic Psychoses During War). Psychiatric Gazette, St. Petersburg, 1915, vol. 2, pp. 139-142.
Zade, M. Ueber Blendungserscheinungen im Felde. München med. Wchnschr., 1915, v. 62, pp. 1514-1515.
Zade, M. On Glare Phenomena in the Field. Munich Medical Weekly, 1915, v. 62, pp. 1514-1515.
Zadek, J. Lähmungen nach Typhus. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, pp. 1033-1034.
Zadek, J. Paralysis after Typhus. German Medical Weekly, Berlin and Leipzig, 1915, vol. 412, pp. 1033-1034.
Zakharschenko, M. A. Un nouveau syndrôme dans les contusions aériennes. Gaz. (russe) Psychiat., 1915, No. 4. Rev. neurol., Par., 1917, v. 24, p. 468.
Zakharschenko, M. A. A new syndrome in air contusions. Gaz. (Russian) Psychiat., 1915, No. 4. Rev. neurol., Par., 1917, v. 24, p. 468.
Zakharschenko, M. A. (New symptom in wind contusion). Psikhiat. Gaz., Petrogr., 1915, v. 2, pp. 56-59.
Zakharschenko, M. A. (New symptom in wind contusion). Psychiat. Gaz., Petrograd, 1915, vol. 2, pp. 56-59.
Zakharschenko, M. A. (The clinical picture of disturbances of speech in those suffering from contusion, in connection with the question of air contusions). Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 369-372.
Zakharschenko, M. A. (The clinical picture of speech disturbances in people with concussions, related to the issue of air concussions). Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 369-372.
Zalkind, A. B. (Nervous diseases of war time). Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 76-78.
Zalkind, A. B. (Nervous diseases of wartime). Psikhiat. Gaz., Petrogr., 1916, v. 3, pp. 76-78.
Zange, Johannes. Ueber hysterische (psychogene) Funktionsstörungen des nervosen Ohrapparats im Kriege. München med. Wchnschr., 1915, v. 622, pp. 957-961.
Zange, Johannes. On hysterical (psychogenic) dysfunctions of the auditory system in wartime. Munich Med. Weekly, 1915, v. 622, pp. 957-961.
Zange, Johannes. Hysterische Hörstörungen im Kriege. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, p. 843.
Zange, Johannes. Hysterical Hearing Disorders in War. German Medical Weekly, Berlin and Leipzig, 1915, v. 412, p. 843.
Zange, Johannes. Die organischen Schädigungen des nervösen Ohrapparates im Kriege. Deutsche med. Wchnschr., Berl. u. Leipz., 1915, v. 412, p. 994.
Zange, Johannes. Organic Damage to the Nervous Ear System in War. German Medical Weekly, Berlin and Leipzig, 1915, vol. 412, p. 994.
Zangger. Welche medizinischen Erfahrungen bei Katastrophen können im heutiger Kriege verwertet werden? Cor. Bl. f. Schweiz. Aerzte, 1915, v. 45, pp. 190-191.
Zangger. What medical experiences from disasters can be applied in today's wars? Cor. Bl. f. Schweiz. Aerzte, 1915, v. 45, pp. 190-191.
Zangger, H. Zur Frage der traumatischen Neurose. Zentralbl. f. Gewerbehyg., Berl., 1916, v. 4, p. 10; pp. 25-32.
Zangger, H. On the Issue of Traumatic Neurosis. Central Journal for Occupational Hygiene, Berlin, 1916, vol. 4, p. 10; pp. 25-32.
Zanietowski, J. Die moderne Elektromedizin in der Kriegstherapie. Wien. klin. Wchnschr., 1915, v. 28, p. 805, p. 810, p. 838.
Zanietowski, J. Modern Electromedicine in War Therapy. Vienna. Clin. Weekly, 1915, v. 28, p. 805, p. 810, p. 838.
Zimmern, A. Quels enseignements nous fournit la réaction de dégénérescence dans les blessures des nerfs. Presse méd., April 15, 1915.
Zimmern, A. What lessons can we learn from the degenerative reaction in nerve injuries. Médical Press, April 15, 1915.
Zimmern, A. et Logre, B. Sur le réflexe galvano-psychique. Rev. neurol., Par., 1917, v. 24, pp. 565-567; also Jour. de Radiol. et d’Electrol., v. 2, No. 10, 1917, juillet-août, p. 610.
Zimmern, A. and Logre, B. On the galvanic-psychic reflex. Neurology Review, Paris, 1917, vol. 24, pp. 565-567; also Journal of Radiology and Electrology, vol. 2, No. 10, 1917, July-August, p. 610.
Zimmern, A. et Logre, B. Sur le réflexe galvano-psychique. Presse méd., Par., 1917, v. 25, p. 414.
Zimmern, A. and Logre, B. On the galvanic-psychic reflex. Med Press, Paris, 1917, vol. 25, p. 414.
Zimmern et Perol. Electrodiagnostie de guerre. Collection Horizon, Masson et Cie, 1917.
Zimmern and Perol. Electrodiagnosis of War. Horizon Collection, Masson and Co., 1917.
Zoroastroff, A. V. (Malingering with a view to avoiding military service). Voyenno-Med. J., Petrogr., 1915, v. 243, pp. 473-475.
Zoroastroff, A. V. (Pretending to be ill to get out of military service). Voyenno-Med. J., Petrogr., 1915, v. 243, pp. 473-475.
Zuccari, G. Alcuni casi di psicosi da guerra. Riv. di psicol., Bologna, 1916, v. 12, pp. 129-140.
Zuccari, G. Some Cases of War Psychosis. Journal of Psychology, Bologna, 1916, v. 12, pp. 129-140.
Zunahme geistiger Erkrankungen, Die behauptete, bei Beginn des Kriegs in der Zivilbevölkern Deutschlands (Ergebnis einer Umfrage). Psychiat.-neurol. Wchnschr., Halle, 1915, v. 17, pp. 167-170.
Increase in Mental Illnesses, which stated that at the onset of the war among the civilian population of Germany (result of a survey). Psychiat.-neurol. Wchnschr., Halle, 1915, v. 17, pp. 167-170.
INDEX
- Abderhalden test, 219.
- Abdominothoracic tetanus, Case 403.
- Aboulia, 719.
- Abrahams, 639, 640, 769, Case 236.
- Accommodation paresis, 612.
- Acrocontracture, Cases 235, 428, 486, 489, 529 (bayonet clutch), 530.
- Acroparalysis, Cases 250, 428.
- Acroparesthesia, 845, Case 132.
- Acoumeter, 809.
- Addison’s disease, 239.
- Adiadochokinesis, 301.
- Adrenalin, 229, 239, 689.
- Adrian and Yealland, 674, 702, 797, Cases 563, 564.
- Ageusia, 375.
- Agoraphobia, 260, 763.
- Agraphia, Cases 220.
- Aimé, 672, 689.
- Albumin in spinal fluid, 280.
- Albuminuria, question of hysterical, 535.
- Alcoholism (see Pharmacopsychoses, dipsomania), 58, 113-130, 459, 589, 668, 768, 800, 874, Cases 86-97, Bib., 907, 910, 912, 964.
- Alcoholism, experimental, 118.
- Alexia, 161.
- Alquier, 196.
- Amaurosis (see Ophthalmology).
- Amblyopia, 374, 609-610. References., 959.
- Amentia, 360.
- Amnesia, 303, 392, 435, 441, 444, 453, 462, 467, 477, 487, 488, 492, 499, 634 (recurrent), 635, 676, 734, 739, 757, 828. Bib., 932, 955, 958, 968.
- Amnesia, in malaria, Case 129. Bib., 923.
- Amyotrophy, 719, 761.
- Analgesia, 252, 253, 483, 567.
- Anaphylaxis, 114, 329, 414, 464.
- Anemia, capillary, 265.
- Aneroid, 275.
- Anesthesia, 253, 262, 277, 292, 320, 452, 483, 498, 538, 544, 568, 575, 577, 685, 744, 771, 783, 800, 824, 827, 872. Bib., 918, 961.
- Anesthesia, corneal, in normal persons, 610.
- Anesthesia en lunettes, 610.
- Anesthesia, reëducation of, 568.
- Anesthesia, sexual parts, 531, 533.
- Ankle-jerk, 585. Bib., 906, 916.
- Ankylosis, Bib., 925.
- Anonymous, Case 481.
- Anorexia, Bib., 975.
- Anosmia, 301, 580.
- Antagonist muscles, 353, 355, 545.
- Antagonist muscles in contraction, 350.
- Antalgic reaction, 525.
- Anterior horn cell shock, 526.
- Antebellum experiences repeated in shell-shock hysteria, 876, Cases 286-301, 397, 532, 537, 576.
- Antityphoid inoculation, 842, Cases 65, 180, 303.
- Anuria, 535.
- Anxiety neurosis, 110, 260, 457. Bib., 910, 924, 925, 927, 963.
- Aphasia, 159-161, 874, Case 103, Bib., 910, 928, 929, 950, 961, 981.
- Aphasia, hysterical, non-existent, 454, 766.
- Aphonia, 370, 725, 727, 816. Bib., 931, 932, 940, 953, 957, 959, 963, 975, 978, 980.
- Apoplexy, Bibliography., 936.
- Apraxia, Bib., 928, 936.
- Aprosexia, 487, 632, 637.
- Argyll-Robertson sign inverted (Sollier), 612
- Arinstein, 716, 746. Cases 212, 249, 551, 554, 555, 588.
- Arnoux, 270.
- [4]Armstrong-Jones, 526.
- Arrangement of cases (see Shell-shock, general arrangement of cases).
- Arteriosclerosis, 225, 866. Bib., 919.
- Arthritics, 231.
- Arthritis, 325.
- Association-experiment, Bib., 927.
- Association of hysterical and other symptoms (see passim), 522, 523, especially 530-534.
- Association of hysteric, reflex, and organic conditions, 605.
- Astasia-abasia, 282, 312, 362, Cases 246, 247, 348, 402, 512, 533, 569, 576. Books., 934, 973.
- Asymmetry of reflexes, chloroform, 594.
- Athanassio-Benisty, 540, 556.
- Athetosis, 876, Case 113.
- “Atmosphere of cure,” 728.
- Atrocities, 860, Cases 94, 95.
- Atrophy, “reflex,” 545.
- Aura, 98, 626.
- Autobiographical statements of soldiers, Cases 121, 209, 216, 217, 226, 227, 341, 344, 361, 364, 463, 527, 528, 575.
- Autocritique, 63.
- Autofixity, 369.
- Autognosis, 702, 859, 901.
- Autokratow, 9, 469.
- Automatism, 431, 734.
- Autopsies, Cases 110, 118, 133, 197, 198, 199, 200, 201.
- Auto-suggestion, frontispiece, 95, 98, 109, 153, 395, 498, 543, 577, 674, 738, 748.
- Aviation (see also Otology), 275, 489, 823. Bib., 907, 930, 938, 945, 959, 960, 964, 970, 973.
- Babinski, 157, 395, 401, 454, 456, 469, 481, 491, 498, 535, 543, 544, 554, 563, 566, 568, 569, 576, 578, 603, 604, 605, 643, 647, 671, 723, 746, 748, 788, 819, 833, 848, 856, 857, 871, 874, 877, 878, 891, 896, Cases 871, 877, 878, 891, 896.
- Babinski reflex, 280.
- Babinski-Weil test, 621.
- Babinski and Froment, 389, 390, 585, 607, 608, 695, 696, 717, 719, 742, 787, Cases 274, 275, 276, 422-426.
- Babonneix and Célos, Case 145.
- Babonneix and David, Cases 16, 17, 30.
- “Bait” for hysteria, 544.
- Baldwin, 374.
- Ballard, 675, 689, 736, 840, Cases 82-84.
- Ballet, 465, 554, 643, Cases 267, 396, 407.
- Ballet and de Fursac, 404, 472, 675.
- Barany, 624. Bib., 907, 909.
- Barat, Case 75.
- Batten, Cases 113, 222, 227, 589.
- Battle hypnosis, 638.
- Beaton, 9, Case 5.
- Bechterew, 342.
- Beck, Case 439.
- “Bends,” 275.
- Benisty, 331.
- Bennati, 414, Cases 186, 221, 320, 336.
- Benon, 633.
- “Bent-back” (see Camptocormia).
- Bérard, 118, 696.
- Bergonié, 790.
- Bernheim, 95, 740, 902.
- “Big belly” (see Pregnancy, hysterical).
- Bilateral symptoms, 362.
- Binswanger, Cases 179, 217, 220, 229, 233, 239, 309, 327, 368, 483, 505, 549, 575, 576, 577, 579, 587.
- Biological principles and neuroses, Bib. 915.
- Birdlike movements, 487, 632, 637.
- Birnbaum, 222.
- Bispham, 644.
- Bladder, 276, 284, 294.
- Blässig, Case 264.
- Blepharospasm, Case 211. Bib. 931.
- Blepharospasm, 372, 374.
- Blin, Case 131.
- Blindness, Cases 29, 208-272, 296, 297, 433, 517, 521, 537, 538. Bib., 915, 921, 928, 935, 943, 952, 958, 974, 976.
- Blindness, cortical, Case 105.
- Block (see Inhibition).
- Blood, buffer salts, 640.
- Blood pressure high, 497. Bib. 232.
- Blood pressure low, 225, 228, 231, 239, 260, 690, 851. Bib. 232.
- Blum, 661.
- Bolshevist, 249.
- Bonhoeffer, 31, 82, 83, 222, 700, Cases 54, 55, 57, 65, 58, 70, 71, 76, 147, 155, 158, 340.
- [5]Bonnet’s sign, 452.
- Boschi, 704, 716.
- Boucherot, 36, Cases 6, 18, 86, 149, 163.
- Bouquet, Case 419.
- Bourgeois and Sourdille, 620, 623, 809.
- Brachial plexus palsy, 353, 566, 611.
- Brachial symptoms (see Monoplegia).
- Brain abscess, Case 110.
- “Brain fag,” 104.
- Brain injury, 67, 265, 270. Bib. 915.
- Brain tumor. References. 919 (third ventricle).
- Brasch, 41, 689.
- Bravery, psychopathic, 859, Case 36.
- Briand, Case 1, 40, 43, 99, 100, 101, 102.
- Briand and Haury, Cases 98, 467.
- Briand and Kalt, Case 461.
- Briand and Philippe, 683, Case 578.
- Broca, 160-161.
- Bronchopneumonia, 845.
- Brown, 412, 470, 901, Case 496.
- Brown-Séquard, 89, 528, 555, 843.
- Bruce, 716, 724, 769, Cases 521, 553.
- Bulbar syndrome, Bibliography. 910.
- Burial, 334, 349, 373, 393, 396, 405, 419, 435, 457, 499, 512, 573, 682, 696, 698, 768, 779, 796, 814, 819.
- Bury, 228.
- Buscaino and Coppola, 205, Cases 34, 188, 189, 190, 370.
- Butenko, 222.
- Buzzard, 668 (chart), 791, Cases 380, 381, 513.
- Caisson disease, 275.
- Campbell, A. W., 669.
- Campbell, H., 373, 704.
- Camptocormia, 525, 529, Cases 242-245, 322, 385, 401, 572, 584. Bib. 938, 950, 951, 956, 965, 972.
- Canities, Cases 211, 212, 540. Bib. 943, 971, 974.
- Cargill, Case 418.
- Carlill, Case 130.
- Carlill, Fildes, Baker, Case 2.
- Cassirer, Case 398.
- Catalepsy, local, 544, 551, 552. Bib. 916 (post mortem), 942.
- Catatonia, 485. Bib. 928.
- Catiemophrenosis, 479.
- Cauda equina, 533, 540.
- Causes (see Shell-shock, nature and causes).
- Cellulitis, 764.
- Celluloid obturators, 813.
- Central gyrus lesions, 160.
- Cephalad arrangement of Shell-shock cases, 852.
- Cephalea, 490.
- Cerebellar symptoms, Cases 375, 398.
- Cerebellum, 268, 296, 300.
- Cerebrospinal fluid (see Spinal fluid).
- Cerumen, 813.
- Cestex, 366.
- Chaplin, Charlie, 672, 894.
- Character (see also Psychology). Biblio. 921.
- Charcot, 348, 454, 531, 544, 545, 569, 572, 618, 719, especially 744 and 833, 848, 867, 891.
- Charon and Halberstadt, Case 318.
- Charpentier, 608, 696.
- Chartier, Case 257.
- Chavigny, 115, 223, 275, 460, 487, 568, 637, 656, 680, 723, 738, 740, 886, Cases 198, 400, 446.
- Chemical warfare, 321, 574, 799, 889, Cases 215, 216, 232, 284, 314, 318, 360, 367, 452, 586. Bib. 956, 962, 969, 980.
- Children (delinquent and the War). Bib. 923, 943.
- Chloroform (Babinski’s experiments), 380, 388, 545, 554, especially 592-597, 608.
- Chorea, 421, Cases 14, 224, 300. Bib. 924, 933.
- Chromatolysis of nerve-cells, 265, 884, 885.
- Cintrage (see Camptocormia).
- Civilians, psychiatry of, Bib. 915, 924, 952, 953, 965, 981, 982.
- Clarke, Cases 67, 394.
- Clarke, Michell, 701.
- Claude, 693, 979, Cases 560, 561, 573.
- Claude, Dide, and Lejonne, 509, Case 331.
- Claude and Lhermitte, 275, Cases 120, 200, 214, 375.
- Claude, Lhermitte, Vigouroux, Case 159.
- Claustrophobia, Case 182. Bib. 964.
- Clavus hystericus, 349.
- Claw foot, 698.
- [6]Clunet, 456.
- Colchicum, 239.
- Colin and Lautier, 260, Cases 32, 195.
- Colin, Lautier, Magnac, 46.
- Collie, Cases 458, 472.
- Commotio cerebri (see also Brain), 134, 260, 366, 490, 524, 699, 888.
- Commotio spinalis, 335, 528-534.
- Compensation (see also Simulation), 14, 28, 482, 666, 837, Cases 3, 7, 8, 22. Bib. 910, 911, 912.
- Concussion deafness, 364.
- Conditioned reflex, 445, 467, 495, 530, 613, 622.
- Confusion, 483, 484, 487, 492, 509, 637. Bib. 916, 925, 948, 954, 963.
- Consiglio, 36, Cases 63, 150, 180, 191, 367.
- Constriction edema (see also Edema), 569.
- Contracture, 282, 318, 525, 529, 545, 569, Cases 489-493 (Treatment by induced fatigue) and passim. Bib. 921, 926, 933, 939, 944, 947, 956, 962, 963, 971, 972.
- Contrecoup, 873, 887, Case 103.
- Conversion-hysteria, 405, 823.
- Convulsions, 706, 759, 762, 820 (see Hysteria, Epilepsy). Bib. 941.
- Convulsions after inoculation, Cases 63, 65.
- Corpse-contacts, 262, 375, 467, 476, 491, 716 (no redeeming feature).
- Cortical blindness, Case 105.
- Cottet, Case 132.
- Coughing, 425.
- Courtois-Suffit and Giroux, 164.
- Crabtree, 759.
- Craig, 644, 716.
- Crampusneurose, 409, 588. Bib. 968.
- Cranial nerves, 378.
- Crile, 269.
- Criminality (see also Medico-legal, Simulation, etc.). Bib. 920, 921.
- Crises (see Emotional crises), 548.
- Crouzon, 373, 851, Cases 177, 433.
- Crutch-paralysis, 324, 605, 833.
- Cyclothymoses (Manic-Depressive group), 865-867, Cases 163-169.
- D.A.H. (see Soldiers’ heart).
- Damaye, 153, 896.
- Dawson, Case 552.
- Deaf-mutism, 362, 405, 767, 815, Cases 497-499, 514, 515, 517, 552, 557, 558, 580, 585, 588. Bib. 911, 914, 937.
- Deafmutism, cure, 672, 681, 721, 734, 775, 776, 781. Bib. 925, 946, 948, 950, 960, 965.
- Deafness, 813, 888, Cases 259-267, 514, 515, 522. (See also Otology), Bib. 913, 915, 916, 917, 924, 927, 932, 933, 937, 942, 945, 954, 962, 974, 979.
- Death, delusion, 405.
- DeBrun, Case 129.
- Decubitus, 285, 527, 533.
- DeFursac, Case 302.
- Dejerine, 528, 538, 648, 740, 819, 886, 900, 901, Cases 288, 289, 412.
- Dejerine and Gascuel, Case 143.
- De la Motte, Cases 152, 234.
- Delherm, Cases 431, 432.
- Deliria (see also Oniric), 488. Bib. 919, 924, 925, 929, 942, 971.
- Delirium, oniric (see Oniric delirium).
- Delusions, influenced by war, 214, 702, 863.
- DeMassary and Du Sonich, Case 14.
- Dementia praecox (see Schizophrenoses), 861, Cases 147-162. Bib. 935, 939, 957, 958.
- Denechau and Matrais, 479.
- Dentistry (see teeth).
- Depressions (see also Cyclothymoses), 714.
- Dercum’s disease, 846, Case 141. Bib. 936.
- Dermatology, 331, 358, 361, 362, 535 (see also Hypertrichosis). Bib. 914, 921, 922.
- Desertion, Cases 1, 12, 45, 52, 56, 58, 88, 90, 92, 149, 150. Bib. 923, 924.
- Determination of symptoms to parts of body, 459, 359, 360, 362.
- Diabetes mellitus, 846, Case 140.
- Diagnosis, delimitation, 834-847.
- Diagnosis per exclusionem in ordine, 847, 871.
- Diagnosis, Shell-shock, differentiation, 871-880. Bib. 923.
- Diagnosis: Shell-shock, 2, 3, Cases 371-422 and passim. Bib. 942.
- Diathermia, 166, 607, 896.
- [7]Dichroism, spinal fluid, 283.
- Dide, 456.
- Dietotherapy, 476, 674, 675, 701.
- Dieulafoy, 373, 609.
- Diphtheria, 845, Cases 127, 128. Bib. 931, 953, 962.
- Diplegia, facial, Bib. 909, 958.
- Diplopia, monocular, 427, 613, 827.
- Dipsomania, Bib. 917.
- Disciplinary (see Medicolegal).
- Disgust (see also Corpse-contacts), 262, 375, 467, 476, 491, 519, 855.
- Dissociation of personality, Case 369.
- Dissociation of sensations, 570.
- “Doll’s head” anesthesia, 744.
- Donath, Cases 20, 306, 362.
- Dubois, 716, 740, 819.
- Dreams, hunger and thirst, 475.
- Dreams, smell, 476.
- Dreams (see also Oniric delirium), 470, 477, 503, 582, 713, 716, 728, 732, 756. Bib. 947, 955.
- Dromomania (see also Fugue), Case 191.
- Duco and Blum, Case 22.
- Dumas, 637.
- Dumesnil, Cases 167, 168, 185.
- Dumolard, Rebierre, Quellien, Case 110.
- Dupouy, Cases 161, 300, 377.
- Duprat, 896, 899, Cases 51, 346, 442, 443.
- Dupré, 437, 459.
- Duprés and Rist, Case 292.
- Duret and Michel, 273.
- Duvernay, 554, Case 486.
- Dynamopathic, 856, 871.
- Dysarthria, 159, 356.
- Dysbasia (see passim), 560, Cases 248, 278; especially 397-400; 537, 547, 560, 561. Bibliography. 941.
- Dysentery, 586, 705.
- Dysentery, psychosis, Case 122.
- Dyskinesia, 633.
- Dysmnesia, 637.
- Ear, injuries of (see also Otology), Bib. 929, 932, 937, 940, 943, 948, 949, 955, 957, 962, 981.
- “Earthquake hysterias,” 881.
- Ecmnesia, 438.
- Eczema, 429.
- Edema, hysterical, 535, 569, 646, 663. Bib. 909, 942, 943.
- Eder, 702, 740, 750, 891, Cases 178, 296, 359, 529, 544.
- Edinger, 414.
- “Effectives,” military, 56, 161.
- Elective exaggeration of reflexes, 380 (see Physiopathic).
- Electrotherapy (see also Treatment, psychoelectric), Bib. 916.
- Elliot, Cases 210, 237.
- Embolism (see Fat, Gas).
- Emotion, 266, 348, 413, 539, 559, 582, 589, 635, 679, 701, 706, 713, 735, (B group, emotional, Myers), 808, 900. Bib. 909, 919, 920, 923, 926, 939, 941, 944, 947, 948, 954, 955, 958, 963, 964, 965, 968, 976, 978.
- Emotion and epilepsy, 97, 413, Cases 85, 302.
- Emotional crises, 453, 455.
- Emotional factors absent, Case 239.
- Emotional shock, Cases 334-339, 343. References. 928.
- Encephalitis (alcoholic?), 459.
- Encephalopsychoses (focal brain group of mental diseases), 490, Cases 103-121.
- Enterospasm, Bib. 928.
- Enuresis, 70, 252, Cases 51, 61. Bib. 964, 967.
- Epilepsy, see Epileptoses.
- Epilepsy, “affect,” 97.
- Epilepsy, Brown-Séquard’s, Case 69. Bib. 947.
- Epilepsy, hysterical, treatment of, 628. Bib. 938.
- Epilepsy and inoculation (see Convulsions).
- Epilepsy, Jacksonian, 158, Cases 66, 105, 441 (hysterical), 547 (same). Bib. 916, 922, 925, 938, 944, 965.
- Epilepsy, larvata, 73, Case 81.
- Epilepsy, late, 93.
- Epilepsy, pleural, 187.
- Epilepsy, “reactive,” 70, 102, Cases 57, 70, 76. Book. 933.
- Epileptic equivalents, 112, 488, 490.
- Epileptoses (Epileptic Group), 675, 699, 839-843, Cases 53-85. Bib. 905, 910, 911, 937, 938, 939, 945, 947, 956, 961, 968, 972, 973, 975, 977.
- [8]Equilibrium-tests (see Otology).
- Erb’s palsy, 598.
- Ereutophobia, 432.
- Erichsen, 544.
- Erythromelalgia, Bib. 916.
- Eschars, 285.
- Eschbach and Lacaze, Case 108.
- Espionage, 126, 201.
- États commotionnels, 832.
- États émotionnels, 832.
- États seconds, 72, 108, 530.
- Etiology (see Shell-shock, Nature and causes).
- Ether versus chloroform, 769.
- “Excommunication” by inhibition, 369, 403.
- Exhaustion, 102, 228, 469, 482, 689, 699.
- Experimental work, 294.
- Explosive diathesis, 700.
- Explosives, high, 115, 266, 294, 295.
- Exposure, 519, Case 239.
- Eye (see also Ophthalmology), Bib. 932, 934, 940, 941, 962, 964.
- Eye, functional cases, Cases 432-437.
- Facial paralysis, 530.
- Facial spasm, Case 306.
- Facies, deafmutism, 815.
- Faradism (see Treatment, Shell-shock neuroses, Psychoelectric).
- Farrar, Case 8.
- Fat embolism, 24.
- Fatigue, 225, 231, 375, 448, 469, 498, 502, 557, 639, 689, 708, 855, 900. Bib. 907, 924, 929, 931, 937, 941, 943, 948, 964, 975.
- Fatigue, induced (see Treatment).
- Fauntleroy, 275.
- Fear, 64, 223, 258, 338, 375, 404, 425, 440, 441, 451, 466, 519, 675, 855. Bib. 907, 958.
- Fearnsides, 12.
- Feeblemindedness, 857, Cases 35-52.
- Feebleminded, of use in army, 48, Cases 35, 37, 41.
- Feiling, 750, 775, Case 369.
- Ferrand, 390, Case 567.
- Finger-prints, Bib. 916.
- First name extraordinary, Case 48.
- Fluorescein test, 372.
- Focal brain lesions with mental disease, Cases 103-121 (see also under Encephalopsychoses).
- Foix, 159.
- Formulae of Shell-shock, 4, 5, chart 2 (page 6), chart 3 (page 7).
- Forster, 348, 349.
- Forsyth, 702, Cases 286, 297.
- Foucault, 405, 561.
- Fractures, Bib. 906.
- Fraser, 364.
- Freud, 39, 702, 716.
- Friedmann, 843, Case 77.
- Friedreich’s disease, 551.
- Froment (see also Babinski and Froment), Case 203.
- Fugue à deux, 235.
- Fugue, alcoholic, 841, Case 88.
- Fugue, catatonic, 202, Case 149.
- Fugue, emotional, Cases 43, 52, 75.
- Fugue, epileptic, 72, 841, Cases 58, 61, 62, 75. Bib. 977.
- Fugue, hysterical, 850, Cases 171, 173, 368, 444.
- Fugue, melancholic, Case 164.
- Fugue, obsessive, Case 445.
- Fugue and oniric delirium, 471, 569. Bib. 914, 917, 948.
- Furloughs, 685. Bib. 919.
- Gaillard, Case 137.
- Gait disorder (see Astasia-abasia, Dysbasia).
- Gallavardin, 641.
- Galvanism, (see Treatment, Shell-shock, Neurosis, Psychoelectric).
- Ganser symptom, 212, 213.
- Garel, 723, Case 581.
- Gas embolism, 270.
- Gassing (see Chemical warfare).
- Gastroenterology (see Stomach).
- Gastropaths, 400.
- Gaucher and Klein, Case 313.
- Gault’s cochleopalpebral reflex, 624.
- Gaupp, Cases 226, 259, 317, 334, 353, 359, 449, 469.
- Gayet, 26.
- [9]General paresis, 9, 18, 223, Cases 2, 6, 9, 12, 15. Bib. 924, 946, 947, 949, 953, 958.
- Genito-urinary, 260.
- Genito-urinary disorder, see Urology.
- Geriopsychoses (senile-senescent group), 200, 225, 262.
- Gerver, 31, Cases 157, 166, 255, 257, 258, 347, 350, 351, 352.
- Giles, Cases 466, 474.
- Gilles de la Tourette, 18.
- Ginestous, Case 268.
- Gleboff, 644, 663.
- Glueck, 667.
- Glycosuria, Bib. 919.
- Goldstein, 723, 728.
- Gonorrhœa, 41, 260, 261.
- Gordon sign, 157.
- Gosset, 624.
- Gougerot and Charpentier, Cases 428, 429, 430.
- Gradenigo, Cases 465, 557.
- Grandclaude, 486.
- Grant, Dundas, 683, 738, 809.
- Grasset, 405, 501, 522, 523, 638, 724.
- Gray hair (see Canities).
- Green, Case 169.
- Greenlees, Case 269.
- Grenier de Cardenal, Legrand, Benoit, Case 118.
- Grünbaum, Case 532.
- Guillain, 281, 421, 746, Case 372.
- Guillain and Barré, Cases 31, 112, 382, 384, 402.
- Gunshot head wounds, see especially under Encephalopsychoses.
- Hahn, 222.
- Hair (see Canities, Hypertrichosis).
- Hallucinations. Bib. 944, 948.
- Hallucinations, auditory, 367, 371, 431, 484, 493. Bib. 913.
- Hallucinations, experimental, 460.
- Hallucinations, Lilliputian, Case 106.
- Hallucinations, pain and temperature, 452.
- Hallucinations, smell, 478.
- Hallucinations, tetanus, 164.
- Hallucinations, visual, 485, Case 159.
- Harris, 404, Case 565.
- Harwood, Case 436.
- Haury, Cases 46, 154.
- Head, Henry, 641.
- Headache, 255, 258, 524, 525, 526.
- Head injury (see also cases under Encephalopsychoses wounds), Bib. 905, 906, 907, 912, 913.
- Head sensations, 321, 490.
- Heart, neurosis, 35, 400, 477, 689, 764 (see also Soldiers’ heart, Precordial sensations). Bib. 909, 914, 927, 929, 930, 931, 934, 936, 937, 945, 950, 951, 959, 968, 969, 974, 975, 976, 977.
- Heat stroke, 447.
- Hecht, 838.
- Heilbronner’s sign, 157.
- Heitz, Case 134.
- Heliotherapy, Bib. 954.
- Helmet, Bib. 916.
- Hemeralopia (see night-blindness).
- Hematology (see Blood).
- Hematomyelia, 277, 284, 286, 555, 570.
- Hemeralopia, Bib. 907, 914, 927, 929.
- Hemiageusia, 476.
- Hemianosmia, 476.
- Hemianesthesia, 876, Cases 114, 218, 255, 376, 380, 554. Bib. 958.
- Hemianopsia, 428, 616. Bib. 930, 931, 953, 974, 977.
- Hemicontracture, 529.
- Hemichorea, 411.
- Hemiplegia, 282, 293, 302, 874, especially, 877, Cases 255, 256, 281, 291, 292, 372, 408, 412, 551, 554. Bib. 926, 931, 934, 936, 943, 945, 946, 949, 953, 958, 959, 960, 964, 966, 971, 977.
- Hemiplegia, organic, minor signs of, 157. Bib. 925, 933, 950.
- Hemorrhages of brain, 265, 270. Bib. 955.
- Hemorrhage, bladder, Case 202.
- Hemorrhages, meningeal, 270, 271, 372. Bib. 933.
- Hemorrhages, naso-pharyngeal. Bib. 921.
- Hemorrhages of skin, 358, 362.
- Hemorrhage, spinal, 888, Cases 202, 372.
- Henderson, Case 183.
- Heredity, 289, 401, 418, 419, 668, 812.
- Heredity and acquired soil absent in Shell-shock, 348, 349, 401, 418, 419.
- Herpes, 288.
- [10]Hesnard, 212.
- Heterosuggestion—frontispiece, 109, 153, 395, 674, 676, 767, 777, 794, 901.
- Hewat, Cases 53, 299, 571.
- Hippus, 87.
- Hirschfeld, Case 484.
- Histology, 265, 271, 272.
- Hollande and Marchand, Case 141.
- Homosexuality, 257.
- “Honeymoon” psychotherapy, 899.
- Hoover’s sign, 157.
- Horse (in the unconscious), Case 359.
- Hospital organization, 896. Bib. 907.
- Hoven, Cases 156, 183, 333.
- Howland, 748.
- Hunger dreams, 475.
- Hunter, John, 608.
- Hurst, 91, 736, Cases 4, 15, 24, 25, 64, 72, 78, 80, 238, 378, 399, 501, 514, 527, 538, 543, 548.
- Hydrophobia, Case 118.
- Hydrotherapy (see Treatment), Bib. 905, 906, 911, 929, 936.
- Hyperalbuminosis (see Spinal fluid), Cases 371, 373.
- Hyperalgesia, 288, 299, 579, 583. Bib. 951.
- Hyperacusis, 367.
- Hyperboulia, 859.
- Hyperesthesia, 267, 700, Cases 221, 223, 262, 383. Bib. 960.
- Hyperreflexia, hysterical, 535.
- Hypersensitive phase (see Anaphylaxis).
- Hypertension, spinal fluid, 282, 283.
- Hyperthyroidism, 361, 639, 640, 760, 844, 846, 866, Cases 142-145, 315, 326, 497. Bib. 939, 965.
- Hypertonus (see passim), 543, 545.
- Hypertrichosis, 89, 567.
- Hypnotism in blind, 377.
- Hypnotism, 96, 282, 509, 532, 554, 702, 729 (blind), 731 (deaf), 743 (not in French army), Cases 142, 174, 361, 369. Bib. 934, 951, 953, 955, 957, 964, 967.
- Hypnotism, spontaneous, 504-508.
- Hypochondria, 231, 260.
- Hypophrenoses (Feeble-mindednesses), Cases 35-52, 236. Bib. 920, 935, 940, 941, 942, 957, 962, 977.
- Hypotonia, 350, 592.
- Hysteria, 69, 152, 165, 211, 213, 253, Cases 67, 68, 123, 128, 137. Bib. 917, 924, 930, 932, 940, 942, 943, 944, 945, 952, 956, 957, 965, 973, 974, 975, 978, 979, 982.
- Hysterical symptoms in sleep, 554.
- Hysterical and organic symptoms, Cases 116, 117, 134, 214, 219, 230, 231, 399, 495. Bib. 924, 928, 933, 981.
- Hystero-emotive factors, 456, 509.
- Hystero-organic association, 605, 799.
- Hystero-reflex association, 605.
- Hystero-traumatism, 531, 544, 545, 560, 568, 571, 799. Bib. 918, 933.
- Imaginary symptoms, 833.
- Imboden, 288, 693, 793.
- Incontinence of urine (see Urology), Cases 384, 401, 500, 577.
- Indemnity-neurosis, 348.
- Industrial medicine, 854, 873.
- Infection (see also Somatopsychoses), 488, 509, 875.
- Inferno, passim.
- Inhibition, 355, 356, 369, 653, 891.
- Inoculation and convulsions (see Convulsions).
- Insomnia, 299. Bib. 945.
- Insular sclerosis (see Multiple Sclerosis).
- Intermediolateral tract shock, 526.
- Iron cross and psychopathy, 863, Case 158.
- Iron cross and psychotherapy, Case 479.
- Instinct (see Emotion, Psychology, etc.), Bib. 921, 934, 978.
- Insubordination, 77, Cases 47, 59, 60, 63, 93.
- Isolation, see Treatment.
- Jacquet’s biokinetic treatment, 646.
- James, 632, 901.
- Jeanselme and Huet, 538, Case 441.
- Jelly-fish not shocked, 858.
- Joint-disease, 539, 545, 562, 569, 608, 744, 789.
- Jolly, Cases 176, 349.
- Joltrain, Case 245.
- Jones, 692, Case 476.
- Joubert, Case 374.
- [11]Jousset, 609.
- Jumping-jack, Case 555.
- Jung, 240.
- Juquelier, Case 58.
- Juquelier and Quellien, 97, Case 81.
- Kaplan, 700.
- Karplus, 348, Cases 27, 140.
- Kastan, 860, Cases 11, 12, 13, 44, 45, 47, 49, 89, 90, 91, 92, 93, 94, 95, 96, 97, 104, 148, 151.
- Kaufmann’s Treatment (see Treatment, Shell-shock Neuroses, Psychoelectric), 723, 750, 753, 786, 791, 792, 793, 900. Bib. 940, 945, 962, 968.
- Khoroshko, 227.
- Kidner, 803.
- King, Edgar, 210.
- Klippel and Weil, 528.
- Knee-jerks, loss of (matutinal), Case 110.
- Kocher, 343.
- Korsakow syndrome, in malaria, Case 130. Bib. 916, 930.
- Kyphosis, 340.
- Labilizing factors, 329.
- Labyrinth disease, 366, 623, Case 211. Bib. 955, 966.
- La Carotte, 660.
- Laehr, 689.
- Laignel-Lavastine, 14, 570, 796, 899.
- Laignel-Lavastine and Ballet, Cases 38, 438.
- Laignel-Lavastine and Courbon, 560, Cases 29, 106, 170, 194, 314.
- Laignel-Lavastine and Fay, Case 74.
- Lannois and Chavanne, 657.
- Laryngology, 576, 683, 721, 723, 726, 727, 766, 823 (see also Treatment, Shell-shock neuroses, pseudo-operations). Biblio. 909, 912.
- Lasègue, 452, 483.
- Lattes, 257.
- Lattes and Goria, Cases 196, 266, 295, 319, 321, 322, 323.
- Lautier, 36, Cases 42, 48, 56.
- Lebar, 569, Cases 211, 456.
- Lépine, 18, 27, 30, 72, 73, 75, 81, 82, 91, 112, 113, 120, 126, 155, 202, 231, 260, 458, 473, 490, 638, 860.
- Lereboullet and Mouzon, Case 105.
- Lèri, 498, 696, 723, Cases 114, 228, 393.
- Lèri, Froment and Mahar, Case 411.
- Lèri and Roger, Cases 252, 468.
- Leriche, 886, Cases 66, 206, 207.
- Lévy, 331.
- Lewandowski, 348, 674, 724.
- Lewitus, Case 471.
- Lhermitte, 157, 874, 887, Case 103.
- Liébault, 726, Cases 261, 447, 580, 585.
- “Lightning neuroses,” 881.
- Lilliputian hallucinations, Case 106.
- Lipomatosis, 846, Case 141.
- Lloyd Morgan, 374.
- Localizing sense, 557.
- Localization of hysterical symptoms (see passim) 529, 855, 872, 873.
- Locus minoris resistentiae, Shell-shock hysteria, 36, 854, 876, Cases 286-301, 409-414.
- Loewy, Cases 87, 122, 310.
- Logre, Cases 21, 62, 88, 164, 235.
- Long, Case 10.
- Lortat-Jacob and Sézary, Case 316.
- Lumbar puncture (see Spinal fluid and Treatment).
- Lumière and Astier, Case 119.
- Lumsden, 645.
- Lungs, 846.
- Lust, 228.
- Lymphatics, Bib. 906.
- Lymphocytosis of spinal fluid (see Spinal fluid and Meningitis).
- MacCurdy, 683, Cases 193, 232, 293, 307, 332, 355, 415, 451, 452, 586.
- MacMahon, 738, Cases 582, 583.
- MacKenzie, 641.
- Main d’accoucheur, 593.
- Main figée, 593.
- Main succulent, 186.
- Mairet, 401.
- Mairet and Durante, 294.
- Mairet and Piéron, 92, Cases 28, 69, 448, 450.
- Mairet, Piéron, Bouzansky, 134, Case 330.
- Maitland, 225.
- Maixandeau, Case 107.
- [12]Malaria, 845, Cases 129-131. Citation. 923, 926, 961.
- Malingering (see Simulation, Medicolegal, etc.), 514, 554, 642, 643, 707, 717, Cases 453-472. Bib. 920, 927, 931, 936, 938, 940, 948, 950, 955, 958, 969, 974, 975, 976, 982.
- Mallet, 487, Cases 354, 444, 445.
- Mania, Cases 163, 165, 187, 188, 350, 351.
- Manic-depressive psychoses (Cyclothymoses), Cases 163-169.
- Manic-depressive (also see Cyclothymia), Case 16.
- Manière forte, 189, 893, 895, 901.
- Mann, 718, 793, 797, Cases 240, 265, 356.
- Mannkopf-Thomayer test, 415.
- Marage, 809, 813.
- Marchand, Cases 127, 128.
- Marie, 14, 159, 342, 648, 796, Cases 403, 470.
- Marie, Chatelin, Patrikios, Case 9.
- Marie-Foix sign, 157.
- Marie and Lévy, Case 213.
- Marie, Meige, Béhagne, Case 401.
- Marionette movements, 350.
- Marriage, H. J., Case 260.
- Martial misfit, 415, 668.
- Martinet, 231.
- Massage, 353, 529, 566. Bib. 918, 940, 959, 961, 971.
- Mathieu, 796.
- Maurice, 231.
- Mauvaise volonté, 717, 812, 894, Case 228.
- McDougall, 374.
- McDowell, Cases 495, 500.
- McWalter, 391.
- “Mechanisms,” 890, 891.
- Mechanotherapy (see also Treatment), Bib. 914.
- Medicolegal, 509 (see also Desertion, Fugue, Epilepsy, Simulation, etc.), 837, 838, 841, 862, 864, Cases 1, 3, 11. Bib. 914, 917, 920, 925, 926, 932, 935, 938, 940, 941, 942, 943, 944, 952, 953, 956, 960, 961, 973, 977.
- Medicolegal period in general paresis, 18.
- Meige, 331, 432, 465, 696, 746, Cases 224, 308, 413.
- Meiopragia, 592.
- Melancholia, Cases 164, 166, 168, 169.
- Memory (see Amnesia, Hypnosis, etc.).
- Mendel-Bechterew’s sign, 157.
- Mendelssohn, Cases 111, 208.
- Ménière’s disease, 623.
- Meninges (see also Hemorrhage), Bib. 912 (cysts).
- Meningitis, 875, Case 109. Bib. 927, 930, 967.
- Meningitis (Meningococcus). Cases 107, 108. Bib. 906.
- Meningitis (pneumococcus), Case 112.
- Mental disease (in war), 926, 936, 937, 963, 966, 967, 975, 980, 981, 982.
- Mental hygiene, Bib. 955.
- Mental symptoms, Bib. 917.
- Mériel, 548.
- Merklen, Cases 125, 126.
- Metatraumatic hysteria, 329.
- Meyer, 50, 208, 222.
- Meynert, 62, 226.
- Micawber, 674.
- Micromegalopsia, Case 106.
- Micro-organic changes, 572.
- Milian, 501, 638, Cases 171, 364, 365, 366.
- Military psychiatry (see War and Psychiatry).
- Milligan and Westmacott, 365.
- Milligan, 775.
- Mills, Cases 454, 459, 517.
- Mine-explosion, 492.
- “Miracle” cures (see Treatment, Shell-shock, rapid versus slow, and passim, 885).
- Mitchell, Weir, 821.
- Mobilization, neuropsychiatry of, Bib. 908, 929.
- Molecular changes, 572.
- Monier-Vinard, 388.
- Monoplegia, 282, 317, 318, 323, 539, 591 (diagnostic table), 595, 596, 605, 874, Cases (crural), 229-234, 286, 287, 385, 386, 388, 410, 428, 534, 575, 577, Cases (brachial), 249-254, 281, 404, 405, 409, 421, 426, 427, 429, 430, 563, 564, 571, 573. Bib. 954.
- Montembault, 222.
- Moore, 641, 644.
- Morale, 9, 257, 903.
- Mörchen, 228.
- Morestin, Case 516.
- [13]Morphinism, Cases 99-102.
- Morselli, 222, 226, 645.
- Mott, 158, 228, 476, 643, 689, 704, 719, 728, 775, 797, 813, 884, 885, 887, 888, 901, Cases 85, 197, 262, 328, 341, 344, 414, 473.
- Muck, 726.
- Multiple sclerosis, 309, 422, 530, 580, 876, Case 115.
- Musculospiral nerve, 540.
- Musical alexia, 775.
- Mutism, 282, 454, Cases 185, 219, 226, 227, 283, 330, 356, 365, 447, 473, 475, 476, 480, 516, 520, 526, 528, 531, 544, 550, 555, 556, 559, 578, 586. Bib. 916, 924, 927, 931, 932, 933, 946, 954, 964.
- Mutism, classification (Myers), 369.
- Mutism, treatment, 674 and passim. Bib. 915, 927, 976.
- Myelitis (see Spinal cord lesions).
- Myers, 355, 568, 579, 740, 750, Cases 174, 223, 263, 272, 287, 329, 360, 361, 395, 453, 463, 464, 523, 524, 525, 538.
- Myokymia, 361.
- Myopathy, question of Shell-shock, 574.
- Narcolepsy, 487, 843, Case 77.
- Narcosis (see Treatment, Narcosis).
- Naval Service, Bib. 910, 929, 965.
- Neiding, Case 215.
- Neisser, 838.
- Néri’s sign, 452.
- Nerve concussion, 354.
- Nerve leaks, Bib. 910.
- Nerve lesions, peripheral (see also Neuritis), Bib. 905, 909, 910, 916, 918, 920, 921, 925, 926, 928, 933, 934, 935, 936, 937, 938, 939, 941, 945, 947, 948, 949, 950, 951, 953, 955, 956, 957, 958, 959, 960, 963, 965, 967, 968, 970, 971, 972, 973, 975, 976, 977 (large nerve trunks), 923 (median), 914, 923 (electrical methods of diagnosis), 922.
- Nerve sutures, 916, 926.
- Nerves (and the War), 915, 953, 956.
- Nervous system, 922, 923, 925, 928, 933, 938, 940, 944, 945, 958, 959, 962, 963, 967, 971, 972, 973, 975, 978.
- Nervous temperament, 956.
- Neurasthenia, 231, 578, 639, 718, Cases 143, 175, 176, 177, 179, 284, 340, 349, 416, 420, 545. Bib. 914, 915, 916, 920, 925, 930, 950, 957, 964, 969, 975, 980.
- Neuritis, 89, 574, 583, 598, 843, 846, Cases 127, 128, 130, 131, 132, 135, 387, 417, 418, 512, 540. Bib. 907.
- Neuropsychiatry, Bib. 915, 922, 924, 926, 947, 951, 952, 955, 960, 963, 969, 976, 980.
- Neurological centers, Bib. 918, 923, 941, 956, 961, 966, 971, 972, 981.
- Neurologists in war, Bib. 914.
- Neurology (see War and neurology).
- Neuropotential, 268.
- Neurosis, definition, 831-834, 889. Bib. 926, 938, 939, 946, 947, 952, 957.
- Neurosyphilis, Cases 1-34, 53, 110. Bib. 916, 972.
- Neurosyphilis and exhaustion, 31.
- Neurosyphilis and trauma, 838.
- Night-blindness, Bib. 907, 911, 942, 959, 975, 979, 980.
- Nitrophenol, Case 434.
- Nitrous oxide anesthesia, 769.
- Noise, 308.
- Nonne, 282, 348, 716, 718, 736, 748, Cases 248, 479, 530, 531, 533, 535, 536.
- Nose, see Rhinology.
- Nosophobia, Case 261.
- Nostalgia, 440. Bib. 927.
- Nystagmus, 432, 489, 557. Bib. 952, 956, 975.
- Obsessions, 229, 466, 631.
- Obturators, aural, 813.
- Obtusion, 487, especially, 637.
- Occipital lesions, 159, 217.
- Officers’ susceptibility to Shell-shock, 735, 744, 857.
- Old age, 200, 225, 262.
- O’Malley, Cases 515, 518.
- Oniric delirium, 405, 437, 456, 477, 478, 628, Cases 50, 81, 295, 314, 319, 321, 331, 333, 444, 477, 579.
- Oniric delirium, treatment by prearranged emotional shock, 461.
- Ontological fallacy, 833.
- [14]Ophthalmology (see Vision, etc.), Cases 268-272, 433-438. Bib. 906, 907, 910, 911, 916, 918, 930, 931, 938, 941, 944, 954, 955, 970.
- Ophthalmoplegia, Case 19.
- Ophthalmoplegia externa, 613.
- Oppenheim, 157, 348, 361, 401, 747, 749, Cases 146, 256, 311, 326, 376, 379, 405, 420, 427.
- Organic neurology (see Encephalopsychoses, Trauma, and passim), 158-161, 489. Bib. 914.
- Organo-hysterical association, 605. Bib. 916.
- Organopathic, 856, 871.
- Orientation-sense (see Otology).
- Ormond, 653, Case 537.
- Ormond and Hurst, 729.
- Orthopedics, 356, 692. Bib. 906, 910, 915, 927, 931, 939, 947, 950, 953, 957, 963, 970.
- Otology (see Ear, Labyrinth, Vestibular, Deafness, Mutism, Aviation), 888, Cases 259-287, 370, 414, 439, 440, 497-499, 562, 578, 579, 588. Bib. 907, 913, 916 (Equilibrium, Orientation), 919, 925, 962.
- Over-reaction, 307.
- Over the top, 481, 699.
- Overwork, 11.
- Pachantoni, Case 273.
- Pactet and Bonhomme, Case 52.
- Pain, see Antalgic hallucinations.
- Panic (see Psychology, Emotion, etc.), Bib. 922.
- Paranoia, Case 185. Bib. 960.
- Paraphernalia, 785 (see Atmosphere of cure).
- Paralyses (see also Hemiplegia, Monoplegia, Paraplegia, etc.), (P. Brachialis), Bib. 919, 943;(traumatic), 923, 927, 933; (facial), 955; (functional), 977.
- Paraplegia, 282, 284, 541, 769, Cases 236-241, 279, 288, 374, 379, 387, 393, 394, 421, 479, 511, 536, 555, 568, 572. Bib. 919, 923, 926, 927, 929, 930, 935, 938, 939, 947, 949, 950, 952, 956, 966.
- Paratyphoid fever, psychosis, 845, Cases 125, 126. Bib. 952.
- Paresthesia, 357, 359.
- Parinaud, 618.
- Paris, 84.
- Parkinson, Cases 138, 139. Bib. 933, 958.
- Parkinson’s disease, 422.
- Parsons, 653, Case 270.
- Pastine, 693.
- Pathological intoxication, Cases 86, 87, 90, 96.
- Pathological lying, Case 183.
- Paulian, 576, Case 385.
- Pearson, 373.
- Pellacani, Case 59, 60, 187.
- Pemberton, Case 271.
- Penhallow, 769.
- “Pensionitis,” 666.
- Pensions (see Medicolegal), Bib. 914.
- Periorganic hysterical symptoms (see passim), 529-534, 544, 548 (tetanic), 563, 569, 849, 873.
- Personality disorder (see also passim and Psychopathoses), 493, 512. Bib. 927.
- Persuasion, 96. Bib. 927.
- Petrol-injection, Case 98.
- Pharmacopsychoses (Alcohol, Drug, and Poison group), Cases 86-102. Bib. 925.
- Phillipson, 364.
- Phobia (see Psychoneuroses, Psychasthenia), 627, 628.
- Phobias, 464.
- Phocas and Gutmann, 846, Case 136.
- Photophobia, 372, 511.
- Physiopathic decalcification, Case 429.
- Physiopathic disorder, 380, 521, 543, 544, 554, 585 (diagnostic table), Cases 274-281, 421-428; 591 (diagnostic table), 878, 892. Bib. 932, 953, 954, 956, 964, 966, 977, 978.
- Physiopathic electrodiagnostics, 608.
- Physiopathic disorder, cure, 387, 607, 671. References. 928.
- Physiotherapy, 821, 896, 897. Bibliography. 914, 918, 920, 926, 929, 931, 935, 939, 948, 950, 951, 957, 960, 967, 975, 978.
- Pick, Case 33.
- Pied figé, 330.
- Pitres and Marchand, 837, Cases 23, 109, 115, 218.
- Pitres and Régis, 423.
- Pituitrin, 228, 690.
- [15]Plantar reflex, question of absence, 537, 538, 575. Bib. 923.
- Pleocytosis (see Spinal fluid).
- Pleura, hemorrhage, Case 201.
- Pleura, reflex disorder, 186, 846.
- Plicature (see Camptocormia).
- Plumbism, 584.
- Pneumonia, Case 133.
- Podiapolsky, 740, Cases 539, 540.
- Podmanizky, 693.
- Poliencephalitis, 26.
- Poliomyelitis, 574, 598.
- Polyneuritis neurasthenica (Mann), 718. Bib. 925, 957.
- Poliomyelitis, residuals, Case 113.
- Pollakisuria, 347
- “Poor dears!”, 719.
- Popliteal nerve, 354, 540, 600.
- Post-diphtheritic symptoms, Case 127.
- Post mortem (see Autopsies).
- Post-oniric suggestion, 477, 628.
- Potain, 239.
- Pott’s disease, 343.
- Precordial sensations, 477, 526.
- Predisposition, 401 (see also frontispiece).
- Prefrontal lesions, 159.
- Pregnancy, hysterical, 387, Case 348. Bib. 966.
- Prestige, 819.
- Prevention of Shell-shock, 3, 902.
- Prince, Morton, 902.
- Prisoners, 228, 303. Bib. 913.
- Proctor, 769, Cases 480, 556.
- Pruvost, Cases 35, 36, 37, 39, 41.
- Pseudodementia, Bib. 910.
- Pseudologia phantastica, Case 183.
- Pseudocoxalgia, 323, 341, 819.
- Pseudohallucinations, 430.
- Pseudo multiple sclerosis, 155.
- Pseudoparesis, Case 26.
- Pseudoptosis of Charcot and Parinaud, 618.
- Pseudotabes, Case 23.
- Psoitis, 525.
- Psoriasis, Case 313. Bib. 930.
- Psychasthenia, Cases 170, 178, 194, 342, 347. Bibliography. 910, 921, 929, 942, 975, 980.
- Psychiatric social work, Bib. 917, 938, 956, 972.
- Psychiatrists in war, Bib. 914, 927, 950.
- Psychiatry in war (see War and psychiatry).
- Psychoanalysis, 361, 497, 582, 675, 677, 702, 712-716 (rationalization), 851, 901 (autognosis). Bib. 926, 937, 979.
- Psychoelectric treatment, 285, 313.
- Psychogenesis, 69, 83, 332, 337, 348, 351, 497, 744, 855, 871. Bib. 919.
- Psychological laboratory, 896.
- Psychology, passim, also Bib. 907, 911, 924, 925, 928, 931, 932, 934, 936, 937, 938, 941, 943, 946, 947, 952, 955, 956, 959, 960, 962, 963, 964, 968, 971, 873, 876, 982.
- Psychoneuroses, Cases 170-182. Bib. 926.
- Psychoneuroses of war, Charts 11 and 12, pages 522 and 523, 760, 761, 799. Bib. 932, 940, 941, 943, 955, 956, 959, 960, 961, 965, 966, 972, 973, 976, 978, 981.
- Psychopathic constitution, Case 147.
- Psychopathic hospitals, 3, 680, 871.
- Psychopathic inferiority, Case 186.
- Psychopathology of War, Bib. 917, 922, 926, 954, 971, 972.
- Psychopathoses (Psychopathias), Cases 183-196. Bib. 935, 948, 957, 960, 962, 969, 977, 980.
- Psychoses, 2-262, Chart 1 (page 2). Bib. 915, 918, 922 (acute), 926 (post-shell-shock), 927 (Dysglandular), 927, 928, 934, 936, 940, (vesical) 943, 952, 955, 957, 958, 962, 965, 968, 972, 973, 975, 976, 978, 979, 980, 982 (see also Mental diseases [in war]).
- Psychoses, treatment, Bib. 918.
- Psychotherapy (see Treatment); also chart 16 (page 673).
- Psychotic symptoms in hysterical cases, 327.
- Puerilism, Case 318. Bib. 912, 917, 941.
- Pulmonary phenomena, 846.
- Pupils in Shell-shock, 526. Bib. 933.
- Purser, Case 475.
- Quadriplegia, 528, 530, 551, 573.
- Quincke’s disease, 646, 665.
- Rabies, 844, Case 118.
- Radial paralysis, 350, 351.
- Radicular symptoms, Case 134.
- [16]Railway spine, 5, 348, 544, 831, 873.
- Raimiste, 528.
- Ranjard, 809.
- Rationalization (Rivers), Cases 506-510 (see also Treatment: Shell-shock neuroses), 237, 859.
- Ravaut, 275, 281, Cases 202, 373, 408, 488.
- Raynaud, 569.
- Reaction-psychosis, 304.
- Reactive idealization, 468.
- Realsuggestionen, 799, 803.
- Reconstruction, 831, 859, 893 (see Treatment, Shell-shock neuroses, Mechanotherapy, Reëducation, etc., etc., and passim). Bib. 908.
- Recovery (see Shell-shock).
- Recruits, possible elimination of defective (see also Hypophrenoses), 835, 858, Cases 42, 44, 49, 91. Bib. 906.
- Rectal incontinence, 807.
- Recurrence, Cases 286-301.
- Reëducation (see Treatment, Shell-shock neuroses, Reëducation), also Bib. 906, 914, 915, 916, 918, 920, 922, 923, 925, 926, 927, 928, 930, 931, 933, 935, 937, 938, 940, 942, 943, 948, 949, 950, 951, 952, 954, 956, 957, 961, 962, 963, 964, 969, 971, 978.
- Reëducation, respiratory, 808, 814-818.
- Reeve, 793, Cases 489, 490, 491, 492, 493.
- “Reflex” disorder (see Physiopathic).
- Reflexes, Bib. 919, 925, 934, 939, 953, 970, 971, 977, 978.
- Refrigeration, 424, 590.
- Régis, 62, 72, 233, 461, 478, 509, 631, 637, 638, 680, 850.
- Relapse (see also “Reminiscence” process in shell-shock), 403, 404, 457, 463, 495, 675.
- Religiosity, 256.
- “Reminiscence” process in Shell-shock hysteria, Cases 286-301, 314.
- Responsibility (see Desertion, Fugue, Insubordination, Pharmacopsychoses), 72, 100, 117, 171.
- Responsibility a psychogenic factor, 458.
- Retention of urine (see also Urology), Cases 111, 382, 383, 539 (Hypnotism).
- Retrobulbar neuritis, 609, Case 434.
- Retrocentral lesions, 160.
- Rhinology, 262, 321, 375, 476, 511, 665. Bib. 955.
- Riggall, Case 541.
- Rivers, 476, Cases 506-510.
- Rombergism, Shell-shock, 620.
- Romner, Case 406.
- Rontgenology (see X-Ray).
- Rosanoff-Saloff, Mme., 340.
- Roselle and Oberthur, 456.
- Rossolimo’s sign, 157.
- Rothacker, Case 144.
- Rouge, Cases 153, 162.
- Roussy, 281, 696, Cases 133, 279, 387, 460, 497, 498, 499, 502.
- Roussy and Boisseau, 275, 362, 404, 689, 743, 797, 815, 887, Cases 199, 440.
- Roussy, Boisseau, Cornil, Case 348.
- Roussy and Lhermitte, 466, 471, 476, 487, 509, 525, 560, 563, 578, 637, 701, 726, 738, 743, 787, 807, 896, Cases 230, 235, 243, 244, 246, 247, 250, 291, 572, 584.
- Routier, Case 409.
- Rows, 471, 478, 900, Cases 301, 335, 342, 343.
- Russca, 295.
- Russel, 404, 650, 740, 775, 781, Cases 79, 241, 503, 504.
- Saaler, 208.
- Salmon, 804.
- Sargent and Holmes, 158.
- Sartorius muscle, 553.
- Savage, 48, 83, 404.
- Schäfer’s sign, 151.
- Schizophrenia and typhoid fever, Case 124.
- Schizophrenoses (Dementia præcox group), 202, 223, 861-865, 864 (medicolegal), Cases 124, 147-162. Bib. 913.
- Scholz, Case 550.
- Schultz, 726.
- Schultzer, Case 570.
- Schuster, 343, 349, Cases 19, 234, 298.
- Sciatica, Cases 10, 565.
- Scotoma, 98, 374.
- Sebileau, Case 388.
- Secretory disorder, 387.
- [17]Séguin and Rouma, 809.
- Self-inflicted injury, Cases 153, 187, 193. Bib. 917, 921, 922, 926, 961, 969.
- Sencert, 885, Case 201.
- Senility (see Geriopsychoses), 200, 225, 262.
- Sensibility (see Dermatology, Ophthalmology, etc.). Bib. 923, 946, 955, 962, 969, 978, 980.
- Serbians, 102, 225, 228.
- Sereysky, 297.
- Serology (see Syphilopsychoses, also under Spinal fluid).
- Sexual continence, 459.
- Sex sensations, 259.
- Shell-shock: animal experimentation, 294, 295.
- “Shell-shock,” the term, 5.
- Shell-shock and croix de guerre, 430, 675.
- Shell-shock: Diagnosis, Cases 371-472 and passim. Biblio. 915, 922, 941.
- Shell-shock: Nature and Causes, Cases 197-370 and passim. Bib. 917, 918, 920, 926, 927, 928, 935, 937, 942, 958, 967, 977, 981.
- Shell-shock: Treatment and results, Cases 473-589 (and see special headings under Treatment, Shell-shock). Cited work. 967.
- “Shell-shock” diseases, 880.
- Shell-shock and epilepsy (Ballard’s Theory), Cases 82-84.
- Shell-shock and traumatic neurosis, Case 248.
- Shell-shock equivalent, 850.
- Shell-shock, general arrangement of cases, 852 et seq., 879-880, 883, 894 et seq.
- Shell-shock, nature in general, 847, 867, 880-892. Bib. 926, 931, 932, 934, 946, 950, 952, 953, 954, 955, 961, 962, 965, 967, 968, 971, 974.
- Shell-shock: organic hypotheses, 526, Cases 197-222. Bib. 927.
- Shell-shock, relapse, 391.
- Shell-shock, repeated, 299.
- Shell-shock (spelled with capital letter) versus shell-shock (spelled lower case), 880.
- Shell-shock, symptoms delayed, Cases 282-285.
- Shell-shock, terminology, 831-834.
- Shell-shock, treatment in general, 893, ad finem. Bib. 921, 923, 924, 929, 930, 934, 936, 937, 953, 954, 976, 978.
- “Shock” ought to be “functional,” 883.
- Shufflebotham, Case 417.
- Shunhoff, 228.
- Shuttleworth, 48.
- Sicard, 525, 544, 554, 643, Case 462.
- Simulateurs de création, de fixation, 643.
- Simulation (see malingering, medicolegal, etc.), 42, 91, 260, 569, 592, 605, especially 642-667, 661-662 (list of methods). Bib. 914, 916, 917, 922, 925, 927, 928, 932, 934, 936, 939, 940, 941, 942, 945, 946, 949, 953, 955, 956, 958, 959, 960, 962, 963, 964, 965, 967, 969, 970, 974, 975, 976, 977, 978.
- Simulation, Cases 33, 34, 39, 78, 79, 257. Bib. 907, 909, 910, 912, 917, 918, 920, 924, 946.
- Sirène à voyelles, 908.
- Situation-delirium, 699.
- Skin-lesions (see Dermatology).
- Skin reflexes, 538, 543.
- Skull, see Head and Wounds. Bib. 916 (Protection, etc.).
- Slang, 832.
- Sleep, deep, 70.
- Sleep, Shell-shock not produced in, 349.
- Sleep, hysterical symptoms persistent in, 553. Bib. 971.
- Smell (see Rhinology).
- Smirnow, 740.
- Smith, E., 471, Cases 175, 284.
- Smith, E., and Pear, T. H., 672, 740, 901.
- Smith, R. P., Case 192.
- Smyly, Cases 116, 117, 219, 283, 397, 520, 558, 559.
- Snake killed, 678.
- Social work (see also Social Psychiatry), 2, 859, 893.
- Soldier, Bib. 927; Mind of, in field, Bib. 927.
- Soldiers’ heart, 44, Cases 138, 139, 451, 452. Bib. 905, 924.
- Sollier, 538, 554, 603, Cases 389, 390, 487.
- Sollier and Chartier, 531.
- [18]Sollier and Jousset, Case 434.
- Somatopsychoses (“symptomatic” of bodily [non-nervous] disorder), 843-847, Cases 118-146.
- Somatopsychoses (Symptomatic, non-nervous group), Cases 122-146.
- Somnambulism, 70, 499, 502, 503, 504, 506, 508, 509.
- Soukhanoff, 120, Cases 50, 223.
- Souques, 91, 342, 345, 696, 886, Cases 242, 386.
- Souques and Donnet, Case 371.
- Souques and Mégevand, Case 401.
- Souques, Mégevand, Donnet, Case 205.
- “Spa” treatment, 718. Bib. 957.
- Spasms, 409, 548, 563, 571, 577, 588. Bib. 951.
- Spasm, facial, Cases 222, 309. Bib. 944.
- Spasm, glossolabial, 563, Case 309.
- Spasm, head, Cases 223, 413, 588.
- Spasticity, 427.
- Speech disorder, Cases 217, 219, 369, 377, 527 (see also Stuttering). Bib. 922, 932, 934, 940, 945, 947, 949, 950, 951, 955, 968, 969, 975, 979, 981.
- Specialists in escape, 81.
- Sphincter-disorder (see also Urology). Bib. 916, 933.
- Spinal cord lesions, 562, 887, Cases 111, 133, 372; especially Cases 375-381. Bib. 915, 919, 920, 945, 946, 950, 965, 978.
- Spinal fluid, 149; especially 276-283; 344, 398, 421, 506, 521; especially 524-527; 530, 535, 536, 539, 570, 576, Bib. 909, 951, 972.
- Spine (see under Camptocormia).
- Spondylitis, 342, 525, Bib. 921.
- Spondylotherapy, References. 909.
- Spontaneous cures in Shell-shock, Cases 283, 310, 357, 365.
- Spirometer, 366.
- Staircase test, 190, 533, 640.
- Stansfield, 220.
- Statistics, 222, 227, 228, 362, 753, 784, 812, 820, 831, 836, 839, 858, 864.
- Steiner, 704, 763, Cases 181, 182, 312, 437.
- Stereotyped movements, 430.
- “Sterno” sign of Dupuoy, Case 161.
- Sterz, Case 123.
- Stewart, 741, 771.
- Stier, 222.
- Stomach, 400, 476, 479, 533, 701, 705, 716, 807. Bib. 950, 951.
- Stokes, 268.
- Stovaine anesthesia, 778, 779.
- Stransky, 866.
- Stress, 226, 227, 867 (see also Exhaustion, Fatigue and passim).
- “Stupefaction” of muscle, 355, 542, 890.
- Stupor, 362, 369, 435, 462, 486, 503. Bib. 933.
- Stupor, “local” (peripheral), 542.
- Stuttering, 681, 638, 817, Cases 219, 527, 579, 586 (see also Speech disorder).
- Subconscious, Bib. 909.
- Suggestion (see also Auto-Heterosuggestion), frontispiece, 95, 318, 338, 476, 477, 438, 498, 653, 872. Bib. 910, 912, 915, 931, 961.
- Suicide, 257, 258, 261, 283, 351, 460, 468, 478.
- “Superposition” of hysterical symptoms, 531, 533, 545, Case 68.
- Supinator longus, 353, 355, 892.
- Surgery, 118, 158-161, Cases 66, 69, 146, 252 (see also Treatment, Shell-shock neuroses, pseudo-operations). Bib. 954, 960, 962, 964.
- Sursimulation, 656.
- Sympathetic nerve effect, 394.
- Sympathy, 718, 719, 901 (see also “Poor dears!”).
- Sympathy with enemy, 245, 258, 319, 851.
- Symptomatic psychoses (see Somatopsychoses).
- Syncope, pleural, 187.
- Syndesmitis, 525.
- Synesthesialgia, 433.
- Syphilopsychoses, 836-839, 875, Cases 1-34. Bib. 934, 937, 941.
- Syphilis and epilepsy, 66, 67, Cases 45, 55.
- Syphilis, in the army. Bib. 972, 974.
- Syphilis, danger of vaccination in, 85.
- Syphilis, in married women, 16.
- Syphilis, in munition-workers, 16, 838.
- Syphilophobia, 260.
- [19]Syringomyelia, 570, 663.
- Tabes dorsalis, Cases 4, 20, 21, 22, 23. Bib. 930.
- Tachycardia, 76, 103, 198, 260, 309, 359, 526, 529, 533, 641, 689. Bib. 907, 923.
- Tachypnoea, 526, 846, Case 137.
- Teeth, 701.
- Tension, arterial (see Blood pressure).
- Tétanos fruste, Case 120.
- Temperature changes in hysteria, 331.
- Tetanus, 845, 874, Cases 99, 119, 120, 121, 280, 392, 403, 409, 419. Bib. 913, 917, 919, 921, 927, 936, 946, 949, 952, 954, 964, 966, 973.
- Thalamus, optic, 653, 876, Case 114.
- Theopaths, 851, Case 106.
- Thermanesthesia, Case 380.
- Thermotherapy, 607.
- Thibierge, 16, 30, 838.
- Thirst dreams, 475.
- Thorax, 94.
- Thyroid disease, Case 186. Bib. 912.
- Thyroid extract, 228.
- Tic, 282, 401, 428, 432, 446, 559, 577, 627, 742. Bib. 917, 951.
- Tinel, 356, 890, Cases 253, 315.
- Tobacco, 639.
- Todd, 804, Case 7.
- Tombleson, 846, Cases 142, 545, 546, 547.
- Torpillage (see Treatment, Shell-shock neuroses, psychoelectric), 786, 895. Bib. 930, 964.
- Torpor, 487.
- Torticollis, 697. Bib. 951.
- Toxic psychosis (see Somatopsychoses), Bib. 914.
- Trauma and general paresis, Cases 15, 18, 20.
- Trauma and neurosyphilis (also see Trauma and general paresis), Cases 5, 16, 17, 19, 20, 24, 25, 27.
- Trauma, spinal, Cases 375-381.
- Traumatic neurosis, 347, 359, 749. Bib. 915, 929, 930, 931, 935, 937, 946, 948, 949, 952, 954, 956, 957, 958, 962, 967, 970, 971, 972, 976, 977, 981, 982.
- Traumatic psychoses (see also Encephalopsychoses), 490, 534, 872, 873. Bib. 940, 968.
- Traumatropism, see Localization.
- Treatment, physiopathic or reflex disorder, 671, 743, 787, 892, Cases 277-279.
- Treatment, psychoses, Bib. 918.
- Treatment, shell-shock neuroses; drugs, 675, 677, 689, 777.
- Treatment, Shell-shock neuroses, Hydrotherapy, 588, 680, Case 484. Bib. 962, 963, 973, 978.
- Treatment, Shell-shock neuroses, Hypnotism, 347, 367, 499, 515, 532, 676, 681 (in writing), 682, 697, 514, especially Cases 521-548. Bib. 970, 975.
- Treatment: Shell-shock neuroses by induced fatigue, 789, Cases 489-493.
- Treatment, Shell-shock neuroses, Isolation, 575, 672, 695, 708, 812, 820, 901. Bib. 929, 930, 937, 942, 966, 967, 969.
- Treatment, Shell-shock neuroses, Lumbar puncture, 693, 778, 779.
- Treatment, Shell-shock neuroses, Mechanotherapy, 318, 560, 566, 691, 692, 697, 698, 717, 718, 788, 821, 827. Bib. 913, 940, 941, 960, 961, 964, 967, 971.
- Treatment, Shell-shock neuroses: rapid versus slow methods, 683, 695, 749, 751, 782-797 (rapid or miracle cures), 791, 872, 895. Bib. 965.
- Treatment, Shell-shock neuroses, Narcosis, 318, 332, 532, 676, 682 (alcohol), 683 (alcohol), 737, 768 (alcohol), especially Cases 552-559, but passim; 560, 561 (stovaine).
- Treatment, Shell-shock neuroses, Occupation therapy, see passim, 683, 685, 711, 803, 859, 893. Bib. 938, 979.
- Treatment, Shell-shock neuroses, Pseudooperations, 344, 264, 267, 588, 609, 646, 821 especially Cases 514-521; 560 and 561 (stovaine); 562 (X-ray).
- Treatment, Shell-shock neuroses, Psychoelectric, 696, 815, 827, especially 897 and 898, Cases 230, 235, 250, 264, 401, 404, 418 (428), 478, 513, 514, 555, 559, especially 563-574, 584. Bib. 929, 930, 932, 942, 943, 948, 967, 976.
- [20]Treatment, Shell-shock neuroses: faith, rationalization, explanation, persuasion, “tracing back”, reassurance, etc., 463, 474, 580, 622, 695, 701, 706, 707, 820, 900, 901. Bib. 937, 967, 969.
- Treatment, Shell-shock neuroses, Reëducation, 568, 683, 692, 735, 899, 900, 901, Cases 230, 284, 293, 299, 387, 400, 404, 447, 514, 550, especially 575-589, 578 (respiratory). Bib. 913.
- Treatment, Shell-shock neuroses, Recovery without medical treatment, Cases 283, 310, 357, 364, 365, especially 473-477, 520.
- Treatment, Shell-shock neuroses, prearranged emotional shock (see Emotion), 680.
- Treatment, Shell-shock neuroses, relation to the front line, 675, 897.
- Treatment, Shell-shock neuroses, studied neglect, 672, Cases 67, 533.
- Treatment, Shell-shock neuroses, Psychotherapy undefined, 553, 554, 874, 899 (honeymoon type). Bib. 923, 926, 950, 966.
- Tremophobia, 465, Case 308.
- Tremor, 282, 466, 492, 551, 622, 742, Cases 224, 308, 325, 327, 337, 483, 502, 532, 535. Bib. 909, 945, 950, 951.
- Tremors, head, 292, 708.
- Trench-foot, 718, 760, Case 132.
- Trephining (see also Organic neurology), 490.
- Triad of Dieulafoy, 373, 609.
- Triplegia, 773.
- Trismus, 300, 771.
- Trophic changes, 603.
- Tubby, 354, Cases 254, 285.
- Tuberculosis, 239.
- Turner, 718, 804, 901.
- Turrell, Cases 121, 568.
- Tympanum, 300.
- Typhoid fever, Cases 123, 124, 135, 276. Bib. 229.
- Typhus (and war psychoses). Bib. 928, 955, 960, 970, 972.
- Ulnar syndrome, Case 136.
- Urology, Urine, 347, 377, 427, 476, 527, 533, especially 535-6, 805.
- Vago-accessorius nucleus, 265, 884.
- Vagus, 701.
- Vasomotors, labile, 260, 387, 428, 569, 639, 742 (also passim). Bib. 921 (arterial hypertension).
- Veale, Cases 511, 512.
- Venereal diseases (see Syphilis, Urology, etc.). Bib. 920.
- Verger, Case 61.
- Vertigo, Case 105.
- Vestibular symptoms, Cases 31, 368, 398, 439, 515.
- Vicissitudes of treatment, 796 and passim.
- Victoria cross, 741, 891.
- Vigouroux, 44.
- Vignolo-Nutati, 429.
- Vincent, 266, 696, 723, 753, 820, 894, 900, Cases 277, 278, 566, 564.
- Vincent’s treatment (see Treatment, Shell-shock neuroses, psychoelectric).
- Violence, 75, 76, 252-255.
- Vision (see also Ophthalmology), 490. Bib. 931, 934, 974.
- Visual fields, contracted, 253, 254, 374, 551. Bib. 936.
- Vlasto, Case 519.
- Vocational reëducation, 803. Bib. 915, 916, 917, 924, 926, 930, 940, 971, 973, 974, 975, 978.
- Voltaic vertigo, 621, 624.
- Vomiting (see Stomach).
- Von Sarbo, 348, Case 410.
- Voss, Cases 455, 457, 569.
- Vulpian, 608.
- Wagner v. Jauregg, 348.
- Walshe, 828.
- Walther, Case 404.
- War and Neurology, Bib. 915, 922, 928, 934, 938, 946, 950, 951, 952, 953, 954, 956, 957, 967, 968, 971, 973, 974, 977, 981.
- War Neurosis (see Shell-shock, Hysteria, etc.).
- War and Psychiatry (see also Recruits, Hospital Organization), Bib. 920, 921, 922, 925, 926, 928, 930, 931, 932, 933, 935, 938, 940, 943, 944, 946, 953, 954, 956, 960, 962, 963, 965, 969, 971, 973, 974, 977, 979, 980, 981.
- [21]War stress, 226, 227, 289.
- Wassermann reaction in suspected Shell-shock, 12. Bib. 927.
- Wassermann reaction in epileptiform seizures, 65.
- Weichardt, 689.
- Wernicke, 161, 409.
- Westphal, 348, Case 435.
- Westphal and Hübner, Cases 73, 290.
- Weygandt, 863, Cases 3, 160, 165, 416.
- White hair (see canities).
- Will therapy, 322.
- Wilmanns, 228.
- Wilson, Gordon, 812.
- Wiltshire, 404, 519, 675, Cases 216, 324, 325, 337, 338, 345, 357.
- Windage, 185, 275, 276, 289, 317, 378, 550.
- Wish-fulfillment, 361.
- Wollenberg, 348, 447.
- Women, Syphilis in, 16 (see Civilians).
- Wound shock, Bib. 909, 927, 961.
- Wounds (brain), 914, 917, 918, 923, 924, 926, 929, 931, 932, 934, 935, 943, 946, 947, 950, 953, 958, 959, 968, 977, 980.
- Wounds (skull, head), 914, 915, 916, 917, 918, 920, 922, 923, 924, 925, 926, 932, 934, 935, 936, 939, 941, 943, 944, 945, 946, 949, 953, 954, 960, 962, 974, 965, 967, 968, 969, 970, 971, 972, 974, 975, 977, 978, 980, 981.
- Wright, H. P., 589.
- Xanthochromia, spinal fluid, 282.
- X-Ray, 354, 480, 529, 531, 534, 559, 561, 565, 566, 594, 596, 602, especially 606-608; 648, 725, 789, 798. Bib. 913.
- Yealland, 723, 753, 786, 900.
- Yealland’s treatment (see Treatment, Shell-shock neuroses, Psychoelectric).
- Yes-no test, 651, 770.
- Zange, 815.
- Zanger, Cases 294, 482.
- Zeehandelaar, 348, 674, 790.
- Zoopsia, 164.
- Zum Busch, 228.
Transcriber’s Note
Transcription Note
In the references (Page 952), the first part of the citation (preceding “med. Wchnschr., 1916, No. 44, p. 1558.”) of a publication by E. Meyer is missing in the original printing.
In the references (Page 952), the first part of the citation (before “med. Wchnschr., 1916, No. 44, p. 1558.”) for a publication by E. Meyer is missing in the original printing.
The index entry on Babinski refers, possibly erroneously, to case numbers not in this book.
The index entry on Babinski refers, maybe incorrectly, to case numbers not included in this book.
Spelling, hyphenation, abbreviations and accents were inconsistent and have been left that way.
Spelling, hyphenation, abbreviations, and accents were inconsistent and have been kept that way.
Download ePUB
If you like this ebook, consider a donation!