This is a modern-English version of Porneiopathology: A Popular Treatise on Venereal and Other Diseases of the Male and Female Genital System; With Remarks on Impotence, Onanism, Sterility, Piles, and Gravel, and Prescriptions for Their Treatment, originally written by Culverwell, Robert James.
It has been thoroughly updated, including changes to sentence structure, words, spelling,
and grammar—to ensure clarity for contemporary readers, while preserving the original spirit and nuance. If
you click on a paragraph, you will see the original text that we modified, and you can toggle between the two versions.
Scroll to the bottom of this page and you will find a free ePUB download link for this book.

Transcriber’s Note
Transcription Note
See the end of this document for details of corrections and other changes.
See the end of this document for details on corrections and other updates.
PORNEIOPATHOLOGY.
A
A
POPULAR TREATISE ON
WELL-KNOWN GUIDE ON
VENEREAL AND OTHER DISEASES
STDs AND OTHER DISEASES
OF THE
OF THE
MALE AND FEMALE GENITAL SYSTEM;
Male and female reproductive system;
WITH REMARKS ON
WITH COMMENTS ON
IMPOTENCE, ONANISM, STERILITY, PILES, AND GRAVEL,
AND PRESCRIPTIONS FOR THEIR TREATMENT.
IMPOTENCE, MASTURBATION, INFERTILITY, HEMORRHOIDS, AND KIDNEY STONES,
AND PRESCRIPTIONS FOR THEIR TREATMENT.
BY R. J. CULVERWELL, M. D.,
Member of the Royal College of Surgeons, Fellow of many
Learned Societies.
BY R. J. CULVERWELL, M.D.,
Member of the Royal College of Surgeons and Fellow of multiple scholarly societies.
WITH ONE HUNDRED PLATES.
WITH 100 PLATES.
NEW YORK:
J. S. REDFIELD, CLINTON HALL.
NEW YORK:
J. S. REDFIELD, CLINTON HALL.
1844.
1844.
Every medical man who will study to investigate as far as possible, in every case, the original channel through which disease or constitutional disorder first found its entry into the system, will be astonished at the mass of human suffering which may be traced up to a venereal origin, although its primary symptoms may have been for years apparently eradicated from the frame. The malady generally commences its attack in early life, before experience has overcome the short-sighted heedlessness of youth, and taught it to look beyond the pains and pleasures of the passing moment. Delicacy or shame will not allow him to seek assistance, until the poison has acquired strength and virulence too alarming to be neglected; and the patient then, instead of applying to his usual professional friends, flies to some empirical practitioner, who temporarily arrests the external symptoms, and discharges him as cured. Thus matters go on, until the malady becomes constitutional; and the patient is at last compelled to place himself under the treatment of those who, at an earlier period, might have preserved his constitution untainted, and his body comparatively uninjured by the ravages of this insidious disease.
Every medical professional who takes the time to thoroughly investigate the initial pathway through which a disease or constitutional disorder enters the body will be shocked by the amount of human suffering that can be traced back to a sexually transmitted origin, even if its early symptoms seem to have been eliminated for years. The illness usually begins its attack in early life, before experience has taught the youthful recklessness to consider more than the immediate joys and pains of the moment. Feelings of embarrassment or shame prevent individuals from seeking help until the infection has grown strong and dangerous enough to become unignorable; at that point, instead of going to their usual doctors, they turn to some unqualified practitioner, who may temporarily alleviate the visible symptoms and then tells them they are cured. This cycle continues until the illness becomes systemic, and the patient is ultimately forced to seek treatment from professionals who, if consulted earlier, might have spared their body from the harm caused by this stealthy disease.
Some years ago the idea first occurred to me that a popular treatise, divested as much as possible of technical phraseology, explaining to the non-medical reader the structure and anatomy of the parts primarily affected by the venereal disease, and describing its first as well as its subsequent and aggravated symptoms, and pointing out the safest treatment of it in inexperienced hands, while in its simple form, would be of much avail in counteracting the effects of the complaint resulting from mal-treatment or neglect among the young and thoughtless. This work is intended to teach him where serious danger exists, or may be apprehended; for the treatment in a great degree, and under any circumstances, must fall upon the patient himself: and every medical man knows that, in very many instances,[4] those who are fully alive to the injury that may arise from such self-management, are yet reduced, by considerations of delicacy and secrecy, to practise it; and it is hoped that a perusal will contribute to give him a knowledge and confidence which he never could acquire from the uneducated empiric. Under these impressions have I ventured to submit the following pages; and while I hope their utility may be acknowledged, I would remark, that they are not intended to supersede medical aid in any stage of the disorder, but that, on the contrary, I would impress upon the reader, if he need it, the prudence of having immediate recourse to a well-educated physician in the earliest stages of the disease, and to beware of advertising quacks. But where, from circumstances which, in venereal complaints, very frequently occur, the party can not have recourse to professional aid, the next best step is certainly to place in his hands a formula of that treatment which is most likely to be successful with himself.
A few years ago, I had the idea to create a popular guide that strips away as much technical jargon as possible. This guide would explain the structure and anatomy of the parts mainly affected by venereal diseases, describe their initial and worse symptoms, and recommend the safest way to treat these issues for those who lack experience. It aims to help young and careless individuals counteract the negative effects of mismanagement or neglect. This work is designed to inform them about serious risks that may exist or be anticipated, since, in many cases, the responsibility for treatment largely falls on the patient. Every medical professional knows that often those who are fully aware of the potential harm from self-treatment still resort to it because of feelings of embarrassment and the need for secrecy. It is hoped that reading this will give them the knowledge and confidence they might not get from an untrained practitioner. Based on this understanding, I have dared to present the following pages, and while I hope their usefulness will be recognized, I want to emphasize that they are not meant to replace professional medical help at any stage of the condition. Instead, I urge readers to seek out a qualified physician as soon as possible if they need it and to be wary of unqualified practitioners. However, if circumstances arise where someone cannot access professional help, the next best option is to provide them with a treatment plan that is most likely to be effective for their situation.
In thus publicly unfolding the mysteries of this department of the profession, I expect some reprehension from those who assume that all medical knowledge should be limited to the regular practisers of the science; but I would fain remind all parties that, although this branch of medical writing has hitherto been in the hands of mercenary empirics, it is equally conducive to the honor of the profession, and the interest of the patient, that these pretenders should be driven from the field. Conscious of my integrity as a regularly educated surgeon, and not altogether destitute of successful practice to rest my claim upon, it is with less hesitation I depart from professional ceremony; and whatever opinion may be pronounced, as to my success in performing the task I have undertaken, I may be allowed to hope, without arrogance, that I am at least entitled to the praise of industry and humanity.
In publicly revealing the mysteries of this part of the profession, I anticipate some criticism from those who believe that all medical knowledge should be restricted to licensed practitioners. However, I want to remind everyone that, even though this area of medical writing has mostly been managed by profit-driven charlatans, it is equally beneficial for the integrity of the profession and the well-being of the patients that these impostors be pushed out. Confident in my integrity as a formally trained surgeon, and backed by a track record of successful practice, I feel less hesitant to move away from professional formalities. Whatever opinions may be expressed about my success in taking on this task, I hope, without appearing arrogant, that I can at least earn recognition for my hard work and compassion.
R. J. CULVERWELL, M. D.
R. J. CULVERWELL, M.D.
1843.
1843.
|
Page. |
General Remarks General Comments |
7 |
Anatomical and Physiological Review of the Male Organs of Generation, with eight engravings Anatomical and Physiological Review of the Male Reproductive Organs, with eight illustrations |
7 |
Of the Testicles, their Structure and Functions, with seven engravings Of the Testicles, their Structure and Functions, with seven illustrations |
14 |
On Gonorrhœa, or Morbid Secretion and Irritability of the Urethra, with five engravings On Gonorrhea, or Abnormal Discharge and Sensitivity of the Urethra, with five illustrations |
20 |
The Surgical Treatment of Gonorrhœa, with prescriptions The Surgical Treatment of Gonorrhea, with prescriptions |
26 |
Medical Treatment of Gonorrhœa and its Consequences, with engravings, prescriptions, and specific remedies Medical Treatment of Gonorrhea and its Consequences, with images, prescriptions, and specific remedies |
29 |
On Gleet On Gleet |
41 |
Morbid Irritability of the Urethra Urethral Irritability |
44 |
Stricture of the Urethra, with fifteen anatomical engravings and diagrams, illustrative of the nature of the disease Stricture of the Urethra, with fifteen anatomical illustrations and diagrams that show the nature of the condition. |
45 |
Treatment of Stricture, with thirty engravings, explanatory of the mode of treatment, prescriptions, &c. Treatment of Stricture, with thirty illustrations that explain the treatment methods, prescriptions, etc. |
58 |
Diseases of the Testicles, with three engravings Diseases of the Testicles, with three illustrations |
68 |
Hydrocele Hydrocele |
69 |
Radical Cure of Hydrocele Radical Treatment for Hydrocele |
71 |
Hydrocele Cured by Acupuncturation Hydrocele Treated by Acupuncture |
71 |
Diseases of the Bladder Bladder Diseases |
73 |
Irritability of the Bladder Bladder Irritability |
74 |
Paralysis of the Bladder Bladder Paralysis |
75 |
Inflammation of the Bladder, with prescriptions Inflammation of the Bladder, with prescriptions |
75 |
Origin of the Venereal Disease Origin of STDs |
79 |
On the Character of the Syphilitic Poison On the Nature of the Syphilitic Poison |
84 |
Of Syphilis, with fifteen engravings Of Syphilis, with 15 engravings |
86 |
Of Buboes, with two engravings Of Buboes, with 2 engravings |
93 |
Of Lues Venerea, or Secondary Symptoms Of Lues Venerea, or Secondary Symptoms |
96 |
Of the Symptoms of the First Stage of Lues, with eight engravings Of the Symptoms of the First Stage of Syphilis, with eight illustrations |
98 |
On the Treatment of Syphilis On Treating Syphilis |
104 |
Treatment of Chancre, with prescriptions Chancre treatment with prescriptions |
106[6] |
Bubo, with engravings and prescriptions Bubo, with carvings and instructions |
112 |
Secondary Symptoms Additional Symptoms |
117 |
Syphilitic Eruption, with an engraving Syphilis outbreak, with an engraving |
117 |
Sore Throat, with prescription Sore throat, with prescription |
121 |
Venereal Affections of the Bones, Joints Venereal Diseases of the Bones and Joints |
122 |
Secondary Symptoms Additional Symptoms |
123 |
Treatment of Ditto, with prescriptions Ditto treatment with prescriptions |
125 |
Syphilitic Lepra Syphilis and Leprosy |
127 |
Nodes and Pains in the Bones Nodes and Pain in the Bones |
128 |
Syphilitic Sore Throat, with prescriptions Syphilis throat infection, with prescriptions |
130 |
Advice to Invalids Advice for the Disabled |
133 |
The Female Organs of Generation—their Structure, Purposes, and Diseases, with thirteen engravings The Female Reproductive Organs—their Structure, Functions, and Disorders, with thirteen illustrations |
136 |
On the use of the Speculum, with an engraving On using the Speculum, with an engraving |
150 |
Gonorrhœa in the Female Gonorrhea in Women |
151 |
Syphilis in Females, with five engravings Syphilis in Women, with five illustrations |
152 |
Leucorrhœa, or the Whites Leucorrhea, or the Whites |
154 |
Treatment of Ditto, with numerous prescriptions Treatment of Ditto, with numerous prescriptions |
155 |
Effects of Incontinence, Celibacy, and Marriage Effects of Incontinence, Celibacy, and Marriage |
162 |
On the Hereditary Transmission of Disease On the Hereditary Transmission of Disease |
169 |
On Impuissance, or Impotence On Impotence |
173 |
Impotence and Sterility of the Male—four engravings Erectile Dysfunction and Male Infertility—four illustrations |
174 |
Impotence and Sterility of the Female—five engravings Impotence and Sterility of Women—five engravings |
180 |
Treatment of Impotence Erectile Dysfunction Treatment |
184 |
Sexual Debility Sexual Dysfunction |
188 |
On Piles, internal and external, with prescriptions and four engravings On Piles, internal and external, with instructions and four engravings |
191 |
Prolapsus of the Rectum, with an engraving Prolapse of the Rectum, with an illustration |
196 |
Stricture of the Rectum, with an engraving Stricture of the Rectum, with an engraving |
197 |
Diseases of the Urine, with three engravings Diseases of the Urine, with three illustrations |
200 |
On Incontinence of the Urine On Urinary Incontinence |
204 |
The Gravel The Gravel |
212 |
Cause of Gravel Reason for Gravel |
213 |
Treatment of Gravel Gravel Treatment |
213 |
The diseases known by the general term of syphilis or venereal disease, and arising from impure coition, appear generally in three forms, gonorrhœa, chancres, and bubo. These sometimes exist alone, and sometimes together. As they affect the genital organs and their appendages, a description of these organs is necessary to a full understanding of the subject.
The diseases commonly referred to as syphilis or venereal disease, resulting from unprotected sexual intercourse, typically manifest in three forms: gonorrhea, chancres, and bubo. These can occur individually or together. Since they impact the genital organs and their related structures, understanding these organs is essential for a complete grasp of the topic.
Genital organs and appendages in the male.—This term embraces the penis, testicles, bladder, and kidneys. The form of the penis is familiar to every one. It commences at the bladder, is of a spongy nature, and is composed of three different parts; the two upper and larger are called the cavernous bodies, and the lower the spongy body; these bodies are covered by the skin which comes over the head of the penis, and forms the prepuce. When this skin is drawn back, the head of the penis, or the glans penis is seen, which is a development of the spongy body, and is extremely sensitive. A whitish secretion, with a peculiar odor, forms at the end of the glans, where the prepuce seems to join it. The object of this secretion is to preserve the sensitiveness of the glans, and to facilitate the withdrawal of the prepuce in coition and in urinating. This material sometimes collects, irritates, hardens, and causes much inconvenience. This can be done away with by circumcision, which is performed as follows:—draw an inked line on the skin of the prepuce, corresponding to the base of the glans penis; draw the prepuce forward, and have the inked part held firmly by an assistant with a pair of forceps. Then the surgeon takes that part of the prepuce projecting beyond the forceps with his left hand,[8] and with a bistoury cuts the prepuce at the inked line with his right. When this is done, the lining skin of the prepuce, which cannot be drawn forward, remains entire, and covers the glans; this lining is divided by a single cut with the scissors: then the flaps are removed round to the frenum, and then the two flaps are held together and removed, with the frenum, at one cut. The mode of holding the prepuce, &c. is seen in the cut.
Male genital organs and appendages.—This term includes the penis, testicles, bladder, and kidneys. The shape of the penis is known to everyone. It starts at the bladder, is spongy in nature, and is made up of three different parts: the two upper and larger parts are called the cavernous bodies, and the lower part is the spongy body; these structures are covered by skin that extends over the tip of the penis and forms the foreskin. When this skin is pulled back, the tip of the penis, or the glans penis, is revealed, which is an extension of the spongy body and is very sensitive. A whitish secretion with a distinct odor forms at the tip of the glans, where the foreskin seems to meet it. The purpose of this secretion is to maintain the sensitivity of the glans and to help in retracting the foreskin during intercourse and urination. This material can sometimes build up, irritate, harden, and cause discomfort. This can be addressed by circumcision, which is done as follows: draw an ink line on the skin of the foreskin corresponding to the base of the glans penis; pull the foreskin forward and have someone firmly hold the inked part with forceps. Then the surgeon grabs the foreskin that extends beyond the forceps with their left hand, and with a bistoury, they cut the foreskin along the inked line with their right. After this, the inner lining of the foreskin, which can’t be pulled forward, remains intact and covers the glans; this lining is divided with one cut using scissors. Then the flaps are cut away up to the frenulum, and finally, the two flaps are brought together and removed along with the frenulum in one cut. The method of holding the foreskin, etc., is illustrated in the image.

On the under side of the glans, near the mouth of the water passage, or urethra, the prepuce is attached by a fold called the frenum, or bridle, or martingale of the penis. The use of this frenum is to confine the movements of the prepuce, and to draw down the mouth of the water passage to direct the flow of the urine. Sometimes the frenum is too short, and confines the prepuce too much; it may be slit down with a pair of scissors as far as is considered expedient. The frenum is frequently ruptured in a first coition. The frenum is very elastic, and protects the sensitive surface beneath it as the eyelid does the eye. Sometimes, however, it becomes permanently contracted;—the glans is then denuded, but soon loses its sensibility. The person is sometimes born with this formation.
On the underside of the glans, near the opening of the urethra, the foreskin is attached by a fold called the frenum, or bridle, of the penis. The purpose of this frenum is to limit the movement of the foreskin and to help guide the flow of urine. Sometimes the frenum is too short and restricts the foreskin too much; it can be snipped with scissors as needed. The frenum often tears during first sexual intercourse. It is very elastic and protects the sensitive area underneath it, like the eyelid protects the eye. However, it can sometimes become permanently tightened; when this happens, the glans is exposed but quickly loses its sensitivity. Some people are born with this condition.
The cavernous bodies form two tubes, united in most of the length of the penis, separated only by a thin partition, and enveloped in a firm sheath; they are composed of an immense number of cells, principally formed by dilated veins, which communicate with each other; these, when the penis is erected, become filled and even distended with blood. The cavernous bodies terminate abruptly and form rounded points under the glans penis. At the other extremity they separate, and form the crura or legs of the penis.
The cavernous bodies create two tubes that run the length of the penis, only separated by a thin wall and covered by a tough sheath. They consist of a vast number of cells primarily made up of enlarged veins that connect with one another. When the penis is erect, these veins fill with blood and stretch. The cavernous bodies end sharply and create rounded tips beneath the glans penis. At the opposite end, they split to form the crura or legs of the penis.
The spongy body forms the lower and under body of the penis, terminates at one end at the point in the glans, whilst it extends the whole length of the penis, again becomes enlarged, and forms the bulb. The urethra or water passage extends through the spongy body, and connects the penis with the bladder. This cut is a section of the penis showing the three bodies:
The spongy body makes up the lower part of the penis and ends at the tip of the glans. It runs the entire length of the penis, where it widens and forms the bulb. The urethra, or urine passage, runs through the spongy body, linking the penis to the bladder. This cut shows a section of the penis displaying the three bodies:

|
a. Corpora Cavernosa. a. Corpora Cavernosa. b. The division or Septum. b. The division or septum. c. Corpus Spongiosum. c. Corpus Spongiosum. d. Urethra. Urethra. e. The great vein of the Penis. e. The main blood vessel of the penis. |
The cut below shows a section of the cavernous body, showing the blood vessels that go to it and cause a distension or erection of the penis:
The cut below shows a section of the cavernous body, showing the blood vessels that lead to it and cause swelling or an erection of the penis:

|
a. Urethric part. Urethra. b. Glans. b. Head of the penis. c. Dorsal Artery serving the Glans. Dorsal artery for the glans. d. Dorsal Artery serving the interior of the Corpus Cavernosum. d. Dorsal artery supplying the inside of the corpus cavernosum. e, f. Deep-seated Arteries. Deep Arteries. |

|
a. Urethra. a. Urethra. b. Glans. b. Head of the penis. c. Dorsal Vein. Dorsal Vein. d. Septum. Septum. e. Vessels. e. Ships. |
In the cut above we see the septum or division of the cavernous bodies, in which are seen the vessels by which, when the erection of the penis subsides, the blood passes into the dorsal vein of the penis.
In the cut above, we see the septum or division of the cavernous bodies, where the vessels are visible that allow blood to flow into the dorsal vein of the penis once an erection subsides.
The Urethra, or water passage, is the canal that passes through the spongy body to the bladder. The urine and[11] semen pass through it. It is very elastic, and may be dilated so as to admit a large instrument to be passed into the bladder, and it contracts on the smallest. It is supported in its course by the spongy body and the prostate gland, between which is a portion unprotected, called the membranous portion. The passage varies in its size in different parts: thus it is rather contracted at the orifice, enlarges within, and for an inch again contracts, dilates nearer the bulb, diminishes at the membranous portion and near the prostate gland, and finally enlarges into the bladder. The cut opposite will show these parts.
The Urethra, or water passage, is the tube that goes through the spongy tissue to the bladder. Urine and[11] semen flow through it. It is very stretchy and can expand enough to allow large instruments to be inserted into the bladder, while it can also constrict with the slightest touch. It is supported along its length by the spongy tissue and the prostate gland, with a section in between that is not protected, known as the membranous portion. The width of the passage varies in different areas: it is narrower at the opening, widens inside, narrows again for an inch, expands closer to the bulb, diminishes at the membranous portion and near the prostate gland, and finally opens up into the bladder. The illustration opposite will show these parts.

|
a. Bladder, or receptacle of urine. Bladder, or urine storage pouch. b. Ureters, or passages through which the urine comes from the kidneys, where it is formed, to the bladder. b. Ureters are the tubes that carry urine from the kidneys, where it’s produced, to the bladder. c. Vas Deferens, through which the semen passes from the testicle, where it is formed, to the seminal vesicles, where it is matured. c. Vas Deferens, through which semen travels from the testicle, where it is produced, to the seminal vesicles, where it is matured. d, d. Openings of Ureters into the bladder. d, d. Openings of ureters into the bladder. e. Prostate Gland. Prostate Gland. f. Orifices of excretory ducts. f. Openings of excretory ducts. g. Openings of the seminal ducts. Openings of the main ducts. h. Ischio-cavernous muscles. Ischiocavernous muscles. i. Bulb of Urethra divided. Urethra bulb divided. k. Cowpers Glands. k. Cowper's Glands. l. Wide part of Urethra. Wide part of urethra. m. Narrow part. Narrow section. n. Fossa Navicularis, usually affected in gonorrhœa. n. Navicular Fossa, usually affected in gonorrhea. o, p. Prepuce. o, p. Foreskin. |
The urethra is constantly moistened with a mucous secretion,—from the membrane itself, the glands, and the folds which yield to the pressure of the urine as it flows, or from other altered conditions of the urethra pour out their contents. The inner surface of the urethra is very vascular and sensitive, as is shown by the slightest laceration by the bougie or by chordee, when considerable bleeding often takes place. Its sensitiveness is well known in the first passing of the bougie, or in inflammation, when the pain of the former and the act of urinating in the latter, often causes fainting.
The urethra is constantly kept moist by mucus secretions from the membrane itself, nearby glands, and the folds that give way to the pressure of urine as it flows. Under different altered conditions, the urethra may release various fluids. The inner surface of the urethra is highly vascular and sensitive, which is evident from even minor injuries caused by a bougie or chordee, leading to significant bleeding. This sensitivity is well recognized during the initial insertion of a bougie or during inflammation, as the pain from the former and urination discomfort in the latter can often lead to fainting.
The bladder is the reservoir of the urine, which is formed in the kidneys, comes into the ureters, passages leading from the kidneys to the bladder, and thence flows, drop by drop, into the bladder. The bladder is shaped somewhat like a pear, but this shape is varied by its contents, and the relative condition of its adjacent parts. Thus, when the bladder is full, its upper part may be felt rising above the pubis, that portion of the lower part of the belly that is covered with hair. In very fat persons the bladder is flattened by the weight of the intestines, and obliged to find room where it can, as in pregnant women. Anatomists, when describing the bladder, speak of its body, base, or upper part, sides and neck, where the urethra or water passage begins, and which is surrounded by the prostate gland. These parts are seen in the first engraving on the opposite page.
The bladder is the container for urine, which is made in the kidneys, travels down the ureters—tubes that lead from the kidneys to the bladder—and then drips into the bladder. The bladder is somewhat pear-shaped, but this shape changes depending on how full it is and the condition of nearby areas. When the bladder is full, its top part can be felt rising above the pubic area, the part of the lower belly that is covered with hair. In very overweight people, the bladder can be squashed by the weight of the intestines and has to adjust its position, similar to what happens in pregnant women. When anatomists describe the bladder, they refer to its body, base, or upper part, sides, and neck, where the urethra or urinary passage begins, surrounded by the prostate gland. These parts are shown in the first engraving on the opposite page.
The bladder is composed of several coats. There is a peculiar membrane investing the important structures in the abdomen called the peritonœum. The base and back part of the bladder is covered by a portion of this peritonœum, which in a measure supports the bladder in its position,[12] and also exercises certain properties which may hereafter be alluded to.
The bladder is made up of several layers. There's a unique membrane that covers the important structures in the abdomen called the peritoneum. The base and back part of the bladder is covered by a section of this peritoneum, which helps support the bladder in its position,[12] and also has certain properties that will be discussed later.

|
a. The inner surface of the Bladder, showing the direction of the Muscular Fibres. a. The inside of the bladder, showing the direction of the muscle fibers. b. The opening of the right Ureter into the Bladder, whence the urine issues. b. The right ureter opens into the bladder, where urine comes out. c, c. The Prostate Gland cut through, and its sides exhibited. c, c. The prostate gland was cut open, and its sides were displayed. d. The Urethra. d. The Urethra. e. Verumontanum. e. Verumontanum. f, f. Orifices of the Seminal Ducts, marked by twigs inserted therein; the other points mark the orifices from the Prostate and other Glands. f, f. Openings of the Seminal Ducts, indicated by twigs inserted there; the other points indicate the openings from the Prostate and other Glands. |
The position of the perineum is seen in the following cuts in which the skin has been removed, disclosing—
The location of the perineum is shown in the following cuts where the skin has been removed, unveiling—

|
1. The superficial fascia of the Perinœum. 1. The outer layer of tissue in the perineum. 2. The fascia lata, or shiny covering of the muscles of the thighs. 2. The fascia lata, or the smooth layer that covers the thigh muscles. 3. The tuberosity of the ischia, or part whereupon we sit. 3. The ischial tuberosity, or the part we sit on. 4. The last portion of the spine, called the Coccyx, easily to be felt posteriorly to the rectum. 4. The last part of the spine, known as the Coccyx, can be easily felt behind the rectum. a. The Sphincter muscle of the Anus. The anal sphincter muscle. b. The inferior border of the great muscles of the buttock, called the Gluteal. b. The bottom edge of the large muscles of the buttock, known as the Gluteal. c. The Levator Ani, or muscles which elevate the rectum. c. The Levator Ani, or the muscles that lift the rectum. |
The following cut represents the muscles of the perinœum exposed, the superficial fascia having been removed.
The following cut shows the muscles of the perineum exposed, with the superficial fascia removed.

|
1. Point in the Perinœum where the principal muscles arise or meet. 1. The area in the perineum where the main muscles originate or come together. 2. Covering of the Thigh. Thigh Coverage. 3. Seat. Seat. 4. Corpora Cavernosa of the Penis. 4. Corpora Cavernosa of the Penis. 5. Corpus Spongiosum. 5. Corpus spongiosum. 6. Coccyx. 6. Tailbone. 7. Great Sacro Sciatic ligament. 7. Great Sacro Sciatic ligament. a, a. Erector Muscles of the Penis. a, a. Erector Muscles of the Penis. b, b. Accelerator Urinæ Muscles. b, b. Urinary Bladder Muscles. c. Line whence the above Muscles take their origin. c. Line from which the above muscles originate. d. Transverse Muscles of the Perinœum. Transverse Muscles of the Perineum. e, e. Sphincter Muscle of the Anus, supposed to be distended with tow or wool. e, e. Sphincter muscle of the anus, thought to be stretched with fiber or wool. f, f. Levatores Ani. f, f. Levator ani. g, g. Great Gluteal Muscles. Great Glute Muscles. |
A brief description of the structures displayed in the two preceding and the following drawing (p. 14) will render this part of our subject perfect.
A short description of the structures shown in the two previous drawings and the following one (p. 14) will complete this part of our topic.
The Fasciæ means the coverings of muscles, such as is seen in cutting a domestic joint—a leg of mutton, for instance—a shiny surface; their use is to strengthen the action of the muscles, to bind them well together, and they mostly exist about the buttocks, back, &c.
The Fasciæ refers to the coverings of muscles, like what you see when you cut into a piece of meat—such as a leg of mutton—where there's a shiny surface. Their purpose is to enhance muscle function, hold them tightly together, and they are generally found around the buttocks, back, etc.
The office of a Sphincter Muscle, of which we have several, as that of the bladder and anus, is to keep closed the aperture they surround. The sphincter ani closes the rectum, and pulls down the bulb of the urethra, by which it assists in ejecting the urine and semen.
The job of a sphincter muscle, of which we have several, like those in the bladder and anus, is to keep the openings they surround closed. The anal sphincter closes the rectum and helps pull down the bulb of the urethra, assisting in the expulsion of urine and semen.
The Levator Muscles lift up the part they are connected with. The levator ani muscles form the funnel appearance of the rectum, and help to draw it up after the fæces or stools are evacuated. They also assist in sustaining the contents of the pelvis, and help to eject the semen and[14] urine, and contents of the rectum, and, perhaps, by pressing upon the veins, contribute to the erection of the penis.
The levator muscles raise the areas they're attached to. The levator ani muscles create the funnel shape of the rectum and help pull it upward after feces or stools are expelled. They also support the contents of the pelvis, aid in expelling semen and urine, and contents of the rectum, and possibly assist in the erection of the penis by compressing the veins.[14]

|
1. Coccyx. Tailbone. 2. Semen. Sperm. 3. Covering of the Thigh. Thigh Covering. 4. Great Sacro Sciatic Ligament. 4. Greater Sacro Sciatic Ligament. a. Bulb of the Urethra. Bulb of the urethra. b. Corpus Spongiosum. b. Corpus Spongiosum. c. Crura of the Penis, being the conclusion of— c. Crura of the Penis, being the conclusion of— d. Corpora Cavernosa Penis. d. Corpus Cavernosum Penis. e. Sphincter of the Anus. e. Anal Sphincter. f. Levatores Ani, covered by a fascia or prolongation of the triangular ligament of the Urethra. f. Levatores Ani, covered by a layer of tissue or extension of the triangular ligament of the Urethra. g. Great Gluteal Muscles. g. Strong Glute Muscles. h, h. Triangular Ligament of the Urethra. The artery of the bulb is seen on the left as it runs between the Crus Penis and bulb of the Urethra. h, h. Triangular Ligament of the Urethra. The artery of the bulb is visible on the left as it runs between the Crus Penis and the bulb of the Urethra. |
The Gluteal Muscles help the rotatory motion of the thigh, and give support generally to the buttocks.
The gluteal muscles aid in the rotational movement of the thigh and provide overall support to the buttocks.
The Sacro-Sciatic Ligaments assist in the firm union of the bones of the pelvis.
The Sacro-Sciatic Ligaments help keep the bones of the pelvis securely connected.
The Erector Muscles of the penis propel the urine and semen forward; and, by grasping the bulb of the urethra, push the blood toward the corpus cavernosum and the glans, and thus distend them.
The erect muscles of the penis push urine and semen forward; by gripping the bulb of the urethra, they push blood toward the corpus cavernosum and the glans, causing them to swell.
The Accelerator Urinæ Muscles, as their name implies, help to eject the urine and semen.
The Accelerator Urinæ Muscles, as their name suggests, assist in pushing out urine and semen.
The Triangular Ligament of the urethra assists the preceding purposes.
The triangular ligament of the urethra helps with the purposes mentioned above.
———<>———
Please provide the text you would like me to modernize.
Testicles.—The testicles are two glandular oval bodies suspended in the scrotum. They furnish the male seed. They are supported by what is called the Spermatic Chord, which consists of the spermatic artery that supplies the testicle with arterial blood, whence the semen is concocted; the veins that return the superfluous blood, and the tube that conveys the semen to the urethra. The testicles are[15] very liable to inflammation, and particularly to changes resulting from the wear and tear of human life—changes that not simply produce pain or inconvenience, but those whereby the power of the organs becomes partially if not wholly lost. A rather ample description of their complicated structure will show the necessity of attending to the earliest symptoms of disturbance. The testicles, in embryo, are lodged in the belly, but they gradually descend, and usually are found in the scrotum at birth. There are occasional exceptions, when one or even both testicles do not descend, but are retained in the groin. Mr. Hunter considered that their virility was thereby impaired, although such an opinion is negatived by numerous illustrations. The non-descent of the testicle, necessarily from its confined situation when in the groin, can not be so fully developed as where it is allowed to range in the scrotum. It is also exposed to accidents when retained, and cases have occurred where Hydrocele, a disease to be noticed hereafter, has ensued, producing much inconvenience, and occasionally the same has been mistaken for rupture. The testicles have several coats. The Scrotum should be considered as one, which is merely a continuation of the common integuments, exceedingly elastic, nearly destitute of fat, and possessing a peculiar contractile power of its own, whereby it can closely embrace the testicles, and at other times yield or become distended, as in hernia or hydrocele, to the size of a melon. The contractile powers of the scrotum have been assigned to the supposed presence of a muscle, which is merely a thickened cellular membrane, and called Dartos. It was stated that the testicles were suspended by their spermatic chords—their support is rendered more perfect by the presence of a muscle to each, that descends into the scrotum, and which is called the Cremaster—it is an expansion of one of the muscles of the abdomen, called the internal oblique, and it spreads itself umbrella fashion around the chord, over the upper part of the testicle, and its fibres extend ray-like over the other coats of the testicle—its office is to draw up the seminal organs during procreation.
Testicles.—The testicles are two oval-shaped glands located in the scrotum. They produce male semen. They are supported by what is known as the Spermatic Cord, which includes the spermatic artery that delivers blood to the testicle, where semen is created; the veins that return excess blood; and the tube that carries the semen to the urethra. The testicles are[15] prone to inflammation and changes caused by the stresses of life—changes that can lead to pain and discomfort, as well as a partial or complete loss of function. A thorough description of their complex structure will highlight the importance of addressing any early signs of problems. In embryos, the testicles are located in the abdomen, but they gradually descend and are usually found in the scrotum at birth. There are occasional exceptions where one or both testicles do not descend and remain in the groin. Mr. Hunter believed that this could impair their virility, although this view has been contradicted by many examples. A testicle that doesn’t descend cannot develop as fully when it is confined to the groin compared to when it is free to move in the scrotum. It is also at risk for injury when it remains in the groin, and there have been instances where Hydrocele, a condition that will be discussed later, has developed, causing significant discomfort, and sometimes this has been confused with a hernia. The testicles have several protective layers. The Scrotum should be regarded as one of these layers; it is essentially an extension of the skin, very elastic, almost fat-free, and it has a unique ability to contract, allowing it to tightly hold the testicles or expand significantly in cases like hernia or hydrocele, reaching the size of a melon. The scrotum's ability to contract is attributed to a presumed muscle, which is actually a thickened layer of tissue called Dartos. It was mentioned that the testicles are suspended by their spermatic cords—this support is enhanced by the presence of a muscle for each testicle, known as the Cremaster, which descends into the scrotum. This muscle is an extension of one of the abdominal muscles, called the internal oblique, and it spreads out like an umbrella over the cord and around the upper part of the testicle, with fibers extending outwards over the other layers of the testicle—its role is to lift the reproductive organs during sexual activity.
The testicles, thus suspended, have two coats, one adhering closely, and the other loosely surrounding the former—between the two, a lubricating fluid is secreted, whereby the various movements of the body are permitted[16] without injury; it is between these coats that water is secreted occasionally, constituting the disease known as hydrocele. The closely fitting coat is termed from its whiteness and density Tunica Albuginea—the other Tunica Vaginalis. These coverings are formed of that extensive membrane in the abdomen called the Peritonœum. The Tunica Albuginea which surrounds the testicle previous to its descent, accompanies it into the scrotum, propelling, as it were, the Tunica Vaginalis before it. On the descent of the testicles into the scrotum, the opening through which they passed becomes impermeably closed.
The testicles, suspended as they are, have two layers: one that fits tightly and another that loosely surrounds it. Between these layers, a lubricating fluid is produced, allowing for various body movements without causing harm. Occasionally, water is also secreted between these layers, leading to a condition known as hydrocele. The tight-fitting layer is called the Tunica Albuginea, named for its white color and density, while the loose layer is the Tunica Vaginalis. These coverings are made from the extensive membrane in the abdomen known as the Peritoneum. The Tunica Albuginea that surrounds the testicle before it descends goes along with it into the scrotum, essentially pushing the Tunica Vaginalis ahead of it. When the testicles descend into the scrotum, the opening through which they passed closes up tightly.[16]
The annexed diagram will explain the coats and facilitate the understanding of subsequent descriptions.
The attached diagram will clarify the coats and help make sense of the following descriptions.

|
1. Body of the Testicle. Testicle Body. 2. Epididymis. 2. Epididymis. 3. Vas Deferens. 3. Vas deferens. 4. Spermatic Artery. Spermatic Artery. 5. Veins. Veins. 6. Cremaster Muscle Cremaster Muscle 7. Tunica Albuginea. 7. Tunica Albuginea. 8. Tunica Vaginalis. 8. Tunica vaginalis. 9. Scrotum. Scrotum. 3, 4, 5, 6, and 8 constituting the Spermatic Chord. 3, 4, 5, 6, and 8 make up the Spermatic Chord. |
When the coats of the testicle are taken off, it is found to consist of innumerable delicate white tubes, which when disengaged from the cellular membrane that connects them together, and steeped in water, exhibit a most astonishing length of convoluted vessels; they appear to consist of one continuous tube, convoluted in partitions of the cellular membrane. When the Tubuli come out from the body of the testicle, they run along the back of it and form a net work of vessels called Rete Testis; it is supposed that by the net work the semen is conveyed from the testicle. The continuations of this Rete Testis have been denominated Vasa Deferentia, which, ending in a number of Vascular Cones, constitute what is called the[17] Epididymis. The Vasa Deferentia, after forming three conical convolutions, unite and form larger tubes, which ultimately end in one large excretory duct, called the Vas Deferens. The following description relates to the accompanying sketch.
When the coverings of the testicle are removed, it reveals countless delicate white tubes. When these tubes are separated from the surrounding tissue that holds them together and soaked in water, they show an impressive length of twisted vessels; they seem to form one continuous tube, twisted in sections by the cellular membrane. When the Tubuli emerge from the testicle, they travel along its back and create a network of vessels known as the Rete Testis; it's believed that this network transports sperm from the testicle. The extensions of this Rete Testis are called Vasa Deferentia, which, ending in several Vascular Cones, form what is known as the [17] Epididymis. The Vasa Deferentia, after creating three conical twists, merge to form larger tubes that ultimately lead to one large excretory duct called the Vas Deferens. The following description corresponds to the accompanying sketch.

|
a. Body of the Testicle. Testicle Body. b. Tubuli Testis. b. Testicular Tubules. c, c. Rete Testis. Rete testis. d. Vasa Deferentia. Vas Deferens. e. Vascular Cones. Vascular Cones. f. Epididymis. f. Epididymis. g. Vas Deferens. g. Vas Deferens. |
The preceding completes the anatomical description of the Testicle. The semen is supposed to be secreted by the arteries that ramify among the seminal tubes; the last drawing exhibits the testicle as from the hand of the dissector. In life and in health the epididymis is attached to the testicle—the vas deferens passes up the chord, enters the abdomen, and, passing down into the pelvis, terminates in the vesiculæ seminales as already, but to be again, alluded to. The two subjoined drawings illustrate the testicles in their natural situation.
The previous section finishes the anatomical description of the testicle. The semen is believed to be produced by the arteries that branch out among the seminal tubes; the last illustration shows the testicle as seen by the dissector. In a living and healthy state, the epididymis is connected to the testicle—the vas deferens travels up the cord, enters the abdomen, and then goes down into the pelvis, ending in the seminal vesicles as mentioned before and will be referenced again. The two accompanying illustrations show the testicles in their natural position.

|
a. Body of the Testicle. Testicular Body. b. Commencement of the Epididymis. b. Start of the Epididymis. c. End of ditto. c. End of same. d. Vas Deferens. d. Vas deferens. |
We now come to speak of the Vesiculæ Seminales. It was just observed, that the Vasa Deferentia terminated in these structures. They are attached to the lowest and back part of the bladder, behind the Prostate Gland. The following drawing is the prelude to the description—It represents the Prostate Gland, the Vesiculæ Seminales and the Bladder.
We now turn to the seminal vesicles. It was noted that the vas deferens end in these structures. They are located at the lower back part of the bladder, behind the prostate gland. The following drawing serves as an introduction to the description—it shows the prostate gland, the seminal vesicles, and the bladder.

|
a, a. Prostate Gland. Prostate Gland. b. Gland cut away to show the Ducts of the Vesiculæ. b. Gland removed to reveal the Ducts of the Vesiculæ. c. Ends of the Ducts. c. Duct Ends. d, d. Cells of the Vesiculæ. d, d. Vesicular cells. e. Left Vas Deferens, also cut open to show its connexion with the Vesiculæ. e. Left Vas Deferens, also opened up to show how it connects with the Vesiculæ. f. Right Vas Deferens. Right Vas Deferens. g, g. Openings of the Vas Deferens and Vesiculæ into the Urethra. g, g. Openings of the Vas Deferens and Seminal Vesicles into the Urethra. h. Bladder. Bladder. i. Ureter. Ureter. |
The Vesiculæ Seminales appear like two cellular bags. They have two coats, the one called nervous, and the inner the cellular, a membrane divided into folds or ridges. The use of the vesiculæ is supposed to be, to act as reservoirs for the semen; but there are different opinions upon the subject, some contending that they furnish a fluid, not spermatic, but merely as an addenda to the seminal secretion; whereas others, who have examined the vesiculæ of persons who have suddenly died, have discovered all the essential qualities of the male seed therein; and, in fact, physiologists, who direct researches in these matters, advise such examinations as the surest means of obtaining, in a state of purity, the seminal fluid.
The seminal vesicles look like two bag-like structures. They have two layers: the outer one is called the nervous layer, and the inner one is a cellular membrane that is folded or ridged. The purpose of the seminal vesicles is believed to be storing semen; however, there are differing opinions on the matter. Some argue that they provide a fluid that isn’t sperm but rather an additive to the seminal fluid. Others, who have studied the seminal vesicles of people who passed away suddenly, have found all the essential characteristics of male sperm in them. In fact, physiologists researching these topics recommend such examinations as the best way to obtain pure seminal fluid.
The Male Semen is a fluid of a starch-ish consistency and of a whitish color. It has a peculiar odor, “like that[19] of a bone while being filed—of a styptic and rather acrid taste,” (for physiologists use more senses than one in these researches), “and of greater specific gravity than any other fluid of the body.” Shortly after its escape, “it becomes liquid and translucent;” if suffered to evaporate, it dries into scurfy-looking substance. By being examined through a powerful microscope it is ascertained to be animated by an infinite number of animalcules; but they are only present in healthy semen, and consequently that fact is taken as a criterion of the virility of the secretion.
The male semen is a fluid with a somewhat starchy consistency and a whitish color. It has a distinct smell, “similar to that[19] of a bone being filed—having a somewhat bitter and sharp taste,” (since physiologists use multiple senses in these studies), “and it has a higher specific gravity than any other fluid in the body.” Shortly after it is released, “it becomes liquid and clear;” if allowed to evaporate, it dries into a scabby-looking substance. When examined under a powerful microscope, it is found to be filled with countless tiny organisms; however, these are only present in healthy semen, and this fact is considered an indicator of the vitality of the secretion.
President Wagner thus describes the germe of future animal life: “The seminal granules are colorless bodies with dark outlines, round and somewhat flattened in shape, and measuring from 1-300 to 1-500th of a line in diameter.” “The animalcules exist in the semen of all animals capable of procreation. They are diversified in form in all animals according to their species, but in man they are extremely small, scarcely surpassing the 1-50th, or almost the 1-40th of a line in breadth. This transparent and flattened body seldom exceeds from the 1-6th to the 1-800th of a line in length.”
President Wagner describes the beginnings of future animal life: “The seminal granules are colorless bodies with dark outlines, round and slightly flattened in shape, measuring between 1/300th and 1/500th of a line in diameter.” “The animalcules are present in the semen of all animals capable of reproduction. They vary in shape across species, but in humans, they are extremely small, barely exceeding 1/50th or nearly 1/40th of a line in width. This transparent and flattened body rarely exceeds 1/6th to 1/800th of a line in length.”
The annexed drawing exhibits the granules and animalcules of a human male being magnified from 900 to 1,000 times:—
The attached drawing shows the granules and tiny organisms of a human male, magnified from 900 to 1,000 times:—

|
1. Animalcules of a man, taken from the Vas Deferens, immediately after death. 1. Tiny living organisms from a man, collected from the Vas Deferens right after death. 2. Seminal Granules. 2. Sperm Granules. 3. A bundle of Animalcules, as grouped together in the Testicle. 3. A collection of tiny organisms, as grouped together in the testicle. 4. Seminal Globule. 4. Seminal Cell. 5. Same surrounded by a cyst or bag. 5. Same enclosed by a cyst or pouch. |
The semen is never discharged pure; it is always diluted with the secretion from the prostate and other glands, and also the mucus of the urethra. A chymical analysis is thus given of 100 parts:
The semen is never released in its pure form; it is always mixed with secretions from the prostate and other glands, as well as mucus from the urethra. A chemical analysis is provided for 100 parts:
| Water | 90 |
| Mucilage | 6 |
| Phosphate of Lime | 3 |
| Soda | 1 |
| —— | |
| 100 |
The semen may certainly be vitiated and diseased: the odor and color assume all the gradations of other secretions when in a morbid condition.
The semen can definitely be damaged and unhealthy: the smell and color take on all the variations of other bodily fluids when in a sick state.
Semen not discharged is supposed to be absorbed, thereby adding to the strength and nutriment of the economy; but as it is furnished for a specific purpose, and its secretion depends much upon the play of our animal passions, and as they are rarely permanently idle, there is not only the inducement that the fluid be furnished, but also emitted, and hence we have nocturnal emissions. These, to a degree, are salutary; but they may happen so frequently that the function becomes disordered and perverted, and in some individuals the semen (unconsciously to them) escapes during sleep, or on the slightest local excitement of riding, walking, or on the action of the bladder or rectum.
Semen that isn’t released is believed to be absorbed, which adds to the body's strength and nutrition. However, since it’s produced for a specific purpose and its secretion is heavily influenced by our animal instincts—which are rarely inactive—there’s not only the motivation for the fluid to be produced but also for it to be released, leading to nocturnal emissions. These emissions can be beneficial to some extent, but they may occur so often that the process becomes disordered and dysfunctional. In some individuals, semen can escape during sleep or with minimal physical stimulation from activities like riding, walking, or even the action of the bladder or rectum.
The prostate gland, as has been stated, contributes much to the dilution of the semen; it may empty itself independently of it. The gland is composed of numerous cells, from which proceed some twenty or thirty pipes or passages that open in the urethra by the sides of the verumontanum, as shown in the drawing.
The prostate gland, as mentioned, plays a significant role in thinning out the semen; it can empty on its own. The gland is made up of many cells, which give rise to about twenty or thirty ducts or passages that open into the urethra on either side of the verumontanum, as illustrated in the drawing.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ———<>———
Morbid Secretions and Irritability of the Urethra.—I have stated that clap or gonorrhœa is one of the first and most frequent complaints of the generative apparatus. There are many secretions common to the urethra, such as those afforded by the various glands for the purpose of lubrication, &c.; and the lining membrane of the passage yields a moisture for its own protection, like the membrane of many other organs, such as the eyes, nose, mouth, and so forth, and these secretions may become unhealthy or vitiated, and give rise to symptoms that lead on to confirmed disease; and, what is still more remarkable, may assume many of the characters and appearances of gonorrhœa, but they rarely induce such constitutional disturbances as clap. The symptoms, consequences, and duration of clap, form its distinguishing features from any other discharge of the urethra: it is very important that such distinction should be understood, for the treatment[21] of the two affections differs most materially; the one is an affection of weakness, and the other of an inflammatory and pestilential nature. The symptoms of clap are as follow: there is usually first felt an uneasy sensation at the mouth of the passage or urethra. The patient is frequently called upon to arrange his person; that uneasy sensation sometimes amounts to an itching (occasionally of a pleasurable kind) the feeling extends a little way up the penis; there is oftentimes an erection and a desire for intercourse, which, if indulged in, the sooner develops the disease. The itching alone will not convey the disease from one person to another; but if intercourse be held, the action of the inflamed vessels is accelerated, and a purulent secretion which is infectious is urged forth and emitted with the semen: therefore the very symptom of the tingling or itching, for it rarely exists in healthy urethræ, should be noticed, and intercourse be avoided until it shall have ceased.
Morbid Secretions and Irritability of the Urethra.—I have mentioned that gonorrhea, commonly referred to as clap, is one of the most common issues affecting the reproductive system. There are various secretions from the urethra, produced by different glands for lubrication and other purposes. The lining of the urethra also produces moisture for its own protection, similar to many other organs like the eyes, nose, and mouth. However, these secretions can become unhealthy or abnormal, leading to symptoms that may develop into serious diseases. Interestingly, they can mimic the signs and characteristics of gonorrhea, but they rarely cause the same systemic reactions as clap. The symptoms, effects, and duration of gonorrhea distinguish it from other urethral discharges. It is crucial to recognize this distinction, as the treatments for the two conditions differ significantly; one involves weakness while the other is inflammatory and dangerous. The symptoms of gonorrhea include an uncomfortable sensation at the opening of the urethra. The patient often feels the need to adjust himself; this discomfort may sometimes feel itchy (occasionally even pleasurable) and can extend slightly up the penis. There is often an erection and a desire for sexual activity, which if acted upon, can worsen the condition. The itching alone does not spread the disease from one person to another, but if sexual intercourse occurs, the inflamed blood vessels become more active, leading to a purulent, infectious discharge that is released with semen. Therefore, the symptom of tingling or itching, which is rarely present in healthy urethras, should be noted, and sexual intercourse should be avoided until it subsides.
About this time is perceived a slight heat on passing water, or at the conclusion of the act; and shortly after, or may be before, a yellowish discharge is observed oozing from the mouth of the glans or nut of the penis; the symptoms then rapidly advance, unless timely and judicious means be adopted to palliate them or effect a cure; the scalding becomes intense, and the pain and smarting continue some time after each operation of passing water: the discharge becomes profuse and clots on the linen, and continues to ooze out with little intermission: the orifice of the urethra looks red and inflamed, and the glans itself swells and is occasionally extremely tender: the foreskin or prepuce sometimes, but fortunately not always, becomes swollen, and tightened over the nut of the penis, from which it can not be drawn back, constituting that form of the disease known by the name of phymosis. See drawing annexed.
At this time, you may notice a slight burning sensation when you urinate or at the end of the process; shortly after, or possibly before, a yellowish discharge begins to ooze from the tip of the penis. The symptoms will quickly worsen unless timely and effective measures are taken to ease them or cure the issue. The burning sensation increases, and the pain persists for a while after each urination. The discharge becomes heavy and stains the fabric, oozing out with little pause. The opening of the urethra appears red and inflamed, and the glans may swell and sometimes be very sensitive. The foreskin can become swollen and tight over the glans, making it difficult to pull back, a condition known as phimosis. See the attached drawing.

When that is the case, other annoyances ensue; the purulent matter collects around the glans; excoriations, ulcerations, and sometimes warts, are the consequence; the whole symptoms become thereby much aggravated. It also happens that the[22] prepuce from inflammation assumes a dropsical appearance, that is to say, the edges or point swell, and appear like a bladder filled with water; thus, the size which the penis then arrives at is enormous, and to the patient very alarming; it usually, however, subsides in a day or two, if rest and proper measures be employed.
When that happens, other irritations follow; pus gathers around the glans; abrasions, ulcers, and sometimes warts are the result; all the symptoms get much worse. It can also occur that the [22] foreskin becomes swollen due to inflammation, meaning the edges or tip puff up and look like a water-filled balloon; this makes the penis appear enormous and can be quite alarming for the patient; however, it usually goes down in a day or two if rest and appropriate treatment are taken.

The glans with some people, is always bare, and the foreskin drawn up around it. Such a state may be induced also by disease: in either case, it may become so inflamed as to resist any efforts to draw it over the glans and, from the swelling and consequent pressure on the penis, a kind of ligature is created; and instances have been known where the most disastrous results have ensued. The circulation of the blood in the glans is checked; the nut puts on a black appearance, and if the ligature be not removed or divided, mortification takes place, and the tip or more of the penis sloughs off or dies away. This state of the prepuce is called paraphymosis: it sometimes happens to young lads, who, having an indicated opening of the foreskin, endeavor to uncover the glans: they succeed, but are unable to pull the prepuce back again. They either take no further notice of it, or else become frightened, but conceal the accident they have committed: in a few hours, the parts become painful, swell, and all the phenomena above detailed ensue.
The glans for some people is always exposed, with the foreskin pulled back around it. This condition can also be triggered by disease: in either case, it may become so inflamed that it resists any attempts to pull it back over the glans. The swelling and pressure on the penis create a kind of constriction; there have been cases where this led to serious complications. The blood flow in the glans is restricted, causing it to appear black, and if the constriction is not removed or cut, tissue death occurs, resulting in the tip or more of the penis dying off. This condition of the foreskin is called paraphimosis: it sometimes happens to young boys who, having an opening in the foreskin, try to uncover the glans. They succeed but can't pull the foreskin back down again. They either ignore the problem or become scared but hide the accident they've caused: within a few hours, the area becomes painful, swells, and all the issues mentioned arise.
The annexed diagram exhibits the foreskin in a state of paraphymosis.
The attached diagram shows the foreskin in a state of paraphimosis.

The next proceeding which will probably be induced, will be an extension of the inflammation to the bladder: the symptoms are a frequent desire to make water, and occasionally ulceration of the membrane lining the bladder follows, when a quantity of muco-purulent matter is discharged, which, mingling with the urine gives it the[23] appearance of whey. Now and then the bladder takes on another form of disordered function: the patient will be seized with retention of urine, that is, a total inability to discharge his water, except by the aid of the catheter. A new and most perplexing feature about this stage of the proceeding is perceived: it is what is called chordee. The existing irritation excites the penis to frequent erections, which are of the most painful nature. The penis is bent downward; the occasion is, the temporary agglutinization of some of the cells of the corpora cavernosa through inflammation, and the distension of the open ones by the arterial blood, thereby putting the adherent cells on the stretch, and so constituting the curve, and giving rise to the pain. This symptom is frequently a very long and troublesome attendant upon a severe clap; it is more annoying, however, than absolutely painful, as it prevents sleep, it being present chiefly at night-time when warm in bed.
The next development that will likely occur is an extension of the inflammation to the bladder. The symptoms include a frequent urge to urinate, and sometimes there’s ulceration of the bladder lining, resulting in a discharge of thick, pus-like material that mixes with the urine, giving it the[23]appearance of whey. Occasionally, the bladder may exhibit another disorder: the patient may experience retention of urine, which means a complete inability to urinate without using a catheter. A new and particularly confusing aspect of this stage is known as chordee. The ongoing irritation causes the penis to have frequent, painful erections. The penis is bent downward due to temporary sticking together of some cells in the corpora cavernosa due to inflammation, while the open cells are filled with arterial blood, stretching the attached cells, creating the curve, and leading to discomfort. This symptom can often linger on for a long time after a severe infection; it tends to be more bothersome than painful, as it disrupts sleep, especially at night when warm in bed.
Occasionally the glands in the groin enlarge and are somewhat painful; they sometimes, but very rarely swell and break; they more frequently sympathise with the adjacent irritation, and may be viewed as indications of the amount of general disturbance present; as the patient gets better the glands go down, leaving a slight or scarcely perceptible hardness as it were to mark where they had been. The most painful of all the attendant phenomenon of clap is swelled testicle, or, as in medical phraseology it is called, Hernia humoralis.
Sometimes the glands in the groin can get swollen and hurt a bit; they can occasionally, but very rarely, swell up and burst. More often, they react to nearby irritation and can be seen as signs of how much overall disturbance is happening. As the patient improves, the glands shrink down, leaving a slight or barely noticeable hardness to mark where they used to be. The most painful symptom associated with gonorrhea is swelled testicle, or, as it's known in medical terms, Hernia humoralis.
The first indication of the approach of the last-named affection is a slight sense of fulness in the testicle, generally the left first, although occasionally in the right, sometimes one after the other, but rarely both together: a smart twinge is now and then felt in the back upon making any particular movement: the testicle becomes sensibly larger and more painful, the chord swells also and feels like a hardened cord in the groin: the patient is soon incapacitated from walking, or walks very lame; if the inflammation be not subdued by some means, and if the patient be of a “burning temperament,” that is, of a very inflammatory constitution, fever is soon set up, and the patient is laid upon a “sick bed.” There is no form of the complaint so dangerous to neglect as swelled testicles; they have sometimes been known to burst or become permanently callous and hardened, and ever after wholly unfit[24] for procreative purposes: in other instances, they have entirely disappeared by absorption: in fact, all diseases of the testicles interfere with the generative power. At the onset of inflammation there may be a brief increase of sexual appetite, but when the structure of the testicle becomes altered or impaired, that appetite is subdued or wholly lost; there is such a wonderful sympathy betwixt all parts of the generative economy of man, that if one portion only be injured, the ordinary end of sexual union is frustrated.
The first sign of the last-mentioned condition is a slight feeling of fullness in the testicle, usually starting with the left, although sometimes it can occur in the right, and occasionally one after the other, but rarely both at the same time. A sharp twinge may be felt in the back during certain movements: the testicle becomes noticeably larger and more painful, the cord swells and feels like a hardened rope in the groin: the patient quickly becomes unable to walk or limps severely; if the inflammation isn't reduced somehow, and if the patient has a "burning temperament," meaning a very inflammatory constitution, a fever will soon develop, and the patient will end up on a "sick bed." There is no form of this condition more dangerous to ignore than swollen testicles; they have been known to burst or become permanently hard and calloused, rendering them completely unfit for procreation: in other cases, they can completely disappear through absorption: in fact, all diseases of the testicles affect reproductive capability. At the beginning of inflammation, there may be a temporary increase in sexual desire, but when the structure of the testicle changes or is damaged, that desire diminishes or is completely lost; there is such a remarkable connection between all parts of the male reproductive system that if even one part is harmed, the typical outcome of sexual union is hindered.[24]
The gonorrhœal poison is capable of producing a similar discharge from other parts to which it may be applied besides the urethra. It has been conveyed by means of the finger or towel to the eyes and nose; and a purulent secretion (attended with much pain and inconvenience, indeed with great danger, when the eye becomes so attacked), has oozed plentifully therefrom. Gonorrhœa is an infectious disorder, and consequently is communicable by whatever means the virus be applied. It certainly is possible, and (if we are to believe the assertions of patients, who are often met with, declaring they have not held female intercourse, and yet have contracted the disease), it certainly is not improbable that it may be taken up from using a water-closet that has been visited by an infectious person just before. It may also be contracted by using a foul bougie.
The gonorrhea bacteria can cause a similar discharge from other areas where it is applied, not just the urethra. It can be transferred through a finger or towel to the eyes and nose, leading to a painful and bothersome discharge (which can be very dangerous if it infects the eye). Gonorrhea is an infectious disease, so it can spread in any way the bacteria are transferred. It’s definitely possible, and (if we’re to believe some patients who claim they haven't had sexual contact with women yet still contracted the disease), it's not unlikely that it can be picked up from using a toilet that was just used by someone who is infected. It can also be contracted through the use of contaminated medical instruments.

If the gonorrhœal discharge be suffered to remain on particular parts of the person, such as around the glans of the penis, or on the outside of the foreskin, excoriations, chaps, and warts, spring up speedily and plentifully, and protrude before the prepuce, or sometimes become adherent to it, as here drawn: it therefore only shows how necessary cleanliness is in these disagreeable complaints, to escape the vexations alluded to. A species of insect also is apt to appear about the hairy part of the genital organs, and indeed extend all over the body, particularly in those parts where hair grows, such as under the armpits, chest, head, &c., if cleanliness be not observed. They are called crabs. The itching they give rise to is very harassing, and the patient, unable to withstand scratching, rubs the parts unto[25] sores, which, in healing, exude little crusts that break off and bleed.
If gonorrheal discharge is allowed to stay on certain areas of the body, like around the tip of the penis or on the outside of the foreskin, sores, chapping, and warts can quickly appear and stick out from under the foreskin or sometimes stick to it, as illustrated here. This highlights how essential cleanliness is when dealing with these unpleasant issues to avoid the mentioned irritations. A type of insect can also show up around the hairy areas of the genital region and can spread all over the body, especially in hairy areas like under the armpits, on the chest, and on the head, if proper hygiene isn't maintained. They are called crabs. The itching they cause can be very bothersome, and the person, unable to resist scratching, rubs the area until it becomes [25] sore, which, while healing, can ooze little crusts that fall off and bleed.

|
A. The Pubis studded with these insects. A. The Pubis filled with these insects. B. The Crabs, or Pediculi Pubis, as they are called, about their natural size, as picked from the skin. B. The Crabs, or Pediculi Pubis, as they are called, about their natural size, as picked from the skin. |
When the gonorrhœa has been severe and there has been much constitutional disturbance, there frequently hang about what are called flying rheumatic pains; and sometimes, if the patient’s health be much broken up, confirmed rheumatism seizes hold of him, and wearies him out of several months of his existence. I have seen many a fine constitution, by a tedious ill-treated or neglected gonorrhœa, much injured, that, had the sufferer consulted a medical man of even ordinary talent, in the first instance, instead of foolishly leaving the disease to wear itself out with the help of this recommended by one, and that by the other, he might have shaken off the hydra, and have averted the hundred vexations that follow.
When gonorrhea has been severe and there has been a lot of overall disturbance, there often linger what are called flying rheumatic pains. Sometimes, if the patient's health is significantly compromised, chronic rheumatism takes hold and drains several months from their life. I've seen many strong individuals suffer greatly due to a poorly managed or neglected gonorrhea. If the person had consulted a doctor of even average skill early on, instead of foolishly allowing the disease to run its course with the help of this remedy recommended by one person and that remedy by another, they might have been able to overcome the infection and avoid the numerous complications that follow.
I come now to add to the list of calamitous consequences, stricture, which, in my opinion, prevails to an enormous extent; however, its consideration will be reserved, as well as the affections of the bladder, and prostate gland, for their proper places. I will simply repeat my impression that a stricture, or narrowing of the urethra, or some organic changes, invariably ensue when the gonorrhœa has been mismanaged, or its cure unfortunately protracted.
I now want to add to the list of disastrous outcomes, stricture, which I believe occurs widely. However, I'll save the discussion of it, as well as the issues related to the bladder and prostate gland, for their appropriate sections. I will just restate my belief that a stricture, or narrowing of the urethra, or some kind of physical changes, always follows when gonorrhea has been poorly treated or its recovery unnecessarily delayed.
It is the opinion of many medical men, and it can, no doubt, be borne out by many patients, that a gonorrhœa if unattended by any untoward circumstance, will wear itself out, and that the duration of such a proceeding is from one to two months; there is no disputing but such has been, and is now and then the case, but such rarely stand even so fair a chance of recovery as to be left entirely alone: even if medicine be not taken, rest, abstemiousness, and such like means, are seldom followed up; either the patient lives gloriously free, or else goes to the opposite extreme.
It is the view of many doctors, and many patients can confirm this, that a gonorrhea, if not complicated by any serious issues, will eventually resolve itself, typically over a period of one to two months. There is certainly truth to this, and it has happened and continues to happen occasionally. However, such cases rarely have a good chance of recovering without any intervention at all. Even when medication is not used, rest, moderation, and similar methods are rarely adhered to; either the patient lives completely carefree or goes to the other extreme.
The cases of gleet which seek medical relief are more numerous, as most professional men must be aware, than those of gonorrhœa, for the reasons so frequently alluded to; the fair inference would be, that a gonorrhœa seldom escapes the terminus of a gleet.
The cases of gleet that seek medical help are more common, as most professionals are likely aware, than those of gonorrhea, for the reasons often mentioned; it would be reasonable to conclude that a gonorrhea rarely ends without developing into a gleet.
The distinguishing feature of gleet from gonorrhœa is that it is not considered infectious: it consists of a discharge ever varying in color and consistence; it is the most troublesome of all urethric derangements, and doubtlessly helps more to disorganize the delicate mucous membrane lining the urinary passage than even the severest clap. Its action is constant though slow; and subject as we are to alternations of health, of which even the urinary apparatus partakes, it is not to be wondered at that a part of our system which is so frequently being employed, should become disturbed at last, and that stricture and all its horrors should form a finale; but as gleet and stricture form in themselves such important diseases, I shall devote a chapter to the consideration of each separately.
The main difference between gleet and gonorrhea is that gleet is not considered contagious. It results in a discharge that constantly changes in color and consistency. It is the most bothersome of all urethral issues and definitely contributes to more damage to the sensitive mucous membrane lining the urinary tract than even the worst case of gonorrhea. Its effects are persistent, though gradual; and given that we experience varying states of health, including the urinary system, it’s no surprise that a part of our body that is constantly in use can become problematic over time, leading to strictures and all their associated issues. However, since gleet and strictures are significant conditions on their own, I will dedicate a chapter to exploring each of them in detail.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ———<>———
The Surgical Treatment of Gonorrhœa.—The principal symptoms indicative of the outbreak of a gonorrhœa are a scalding burning sensation along the urethra as the urine passes through it, and also the pouring forth of a profuse discharge of yellow matter from the same passage. The urethra is lined with a very sensitive membrane, fashioned, however, to be insensible to the urine in its natural state; but if the character of the urine or the membrane itself be altered, the most exquisite misery is produced. Now in gonorrhœa, when it is a first attack, the initiatory sensation is invariably heat, itching, or pain in the urethra; the seat of this suffering is in the mucous membrane. On separating the lips of the orifice of the urethra, the passage appears highly vascular, very red, and looks, according to the popular notion, very sore. On examining it with a powerful glass, little streaks or surfaces of a yellow and tenacious matter are perceived, which, upon being removed, are soon replaced by others. When the patient attempts to urinate, this purulent exudation becomes washed off. By this time, the system is somewhat excited, and the urine is consequently more deeply impregnated with uric acid, which renders it more acrid and pungent to the delicate and now tender outlet through which it flows: the sensation is faint at first, but is rendered very acute by the combined worry inflicted upon the urethra, by its muscular contraction to eject every drop of urine, the denuded state of the membrane itself, and the irritating quality of the water. Such, however, is the habit of action, that the urethra in course of time becomes[27] indifferent to the annoyance of the flow of urine. The nervous sensibility is much diminished, and the urethra is further protected by an abundance of the venereal secretion. There are numerous contingencies that prevent the changes ensuing in such order, and, consequently, the scalding, and the amount of discharge, are seldom two days alike. Were there to be no interruption, the inflammation, for such is the whole process in obedience to the animal law, would fulfil its intention and retire; but molested as it is by diet, exercise, the varied states of health, and numerous other fortuitous circumstances, as we well know, it exists indefinitely. It would be next to an impossibility to explain the process whereby the character of a secretion becomes altered, or to describe the exact changes which the structure or vessels undergo when furnishing the discharge; but we well know that some such changes do take place, and that a cause must precede an effect. In like manner we can ascertain the result of certain experiments, although the modus operandi may baffle our penetration. Gonorrhœa is originally a local complaint, but if not arrested, it involves not only the neighboring parts, but it compromises the general health. Now if the same ends can be brought about by artificial means in a few days, that it takes weeks to effect in the ordinary routine, all the intermediate suffering may be avoided, and all the inconvenience of confinement and physic-taking spared.
The Surgical Treatment of Gonorrhea.—The main symptoms that indicate the onset of gonorrhea are a burning sensation in the urethra when urinating and a heavy, yellow discharge from the same area. The urethra has a very sensitive lining that normally doesn’t react to urine, but if the urine or the lining changes, it can cause intense pain. During the initial stages of gonorrhea, the first sensations are usually heat, itching, or pain in the urethra; this discomfort comes from the mucous membrane. When examining the urethral opening, it appears swollen, very red, and, as people commonly say, quite painful. Under a magnifying glass, you can see small streaks or patches of thick yellow discharge, which are quickly replaced after being wiped away. When the patient tries to urinate, this pus is washed away. By this point, the body is somewhat stirred up, and the urine contains more uric acid, making it more irritating to the sensitive and now tender urethra through which it passes: the initial sensation is mild, but becomes very sharp due to the combined strain from the muscles contracting to push out each drop of urine, the exposed state of the membrane, and the irritating nature of the urine itself. However, over time, the urethra gets used to the discomfort of urinating. The nerve sensitivity decreases, and the urethra is additionally protected by an increase in the venereal discharge. Many factors can disrupt this process and prevent it from following a consistent pattern, meaning the burning sensation and the amount of discharge can vary daily. If there were no interruptions, the inflammation would eventually resolve on its own, but due to diet, exercise, changes in health, and many other unpredictable factors, it can persist indefinitely. It is nearly impossible to explain how the nature of a discharge changes or to detail the specific alterations that the structures or vessels undergo during this process, but we know that some changes do happen and that every effect has a cause. Similarly, we can observe the outcomes of certain experiments, even if the exact mechanism behind them remains unclear. Gonorrhea starts as a local issue but can, if not treated, spread to nearby areas and affect overall health. If the same results can be achieved in a few days through medical intervention rather than weeks of natural progression, it can help avoid unnecessary suffering and the inconveniences of being confined and taking medication.
To cure this disease I find that in many cases, if the parties apply at the very onset of the disease, before the discharge and scalding have set in with anything like severity, and they themselves be not of a very inflammatory temperament, that a sharp stimulating injection will at once subdue the sensitiveness of the urethra and alter the action, and, at the cost of very little, and that only temporary suffering, effect a speedy cure: the mode, except it be by stimulating the relaxed vessels, or owing to the specific action of the injection, is, like all other medical operations, a mystery. A favorite prescription is the nitrate of silver, say one scruple of the nitrate to the ounce of water, but the disease must be thus treated at the very first symptom: the patient must be otherwise in comparatively good health, and his occupation must not expose him to much bodily fatigue. He must not be given to intemperance, nor should those instances be selected where[28] the sufferer is of a very inflammatory constitution. Experience begets confidence, and confidence begets experience. In cautious hands I am satisfied of its usefulness; but there are cases that turn out failures. I have used the injection when the disease itself was a week old, and with like success; but I am ready to confess I have known cases, the cure of which were retarded by its employment. The inflammation has been temporarily aggravated, but they were cases where the treatment was not appropriate; the disease was far advanced, there was much heat and swelling, and the patient’s health was in most instances considerably affected; but yet beyond the few hours’ of suffering merely, no extraordinary symptoms were produced. The cure was very shortly after effected by means which I shall presently allude to.
To treat this condition, I've found that in many cases, if patients seek help right at the start, before severe discharge and burning sensations have begun, and if they aren’t particularly prone to inflammation, a strong stimulating injection can quickly reduce sensitivity in the urethra and change its function, resulting in a fast cure with minimal, temporary discomfort. The method—except for stimulating the relaxed blood vessels or due to the specific effects of the injection—is, like all medical procedures, somewhat of a mystery. A common prescription is silver nitrate, typically one scruple of nitrate to an ounce of water, but this treatment must be started at the very first sign of the condition. The patient should otherwise be in fairly good health and not engage in activities that would cause significant physical strain. They should avoid excessive drinking, and those who are highly inflamed shouldn’t be chosen for this treatment. Experience builds confidence, and confidence builds experience. In careful hands, I'm convinced of its effectiveness; however, there are instances where it doesn't work. I've used the injection even when the disease was a week old and with similar success, but I admit I've seen cases where its use delayed healing. The inflammation may have temporarily worsened, but these were situations where the treatment didn't fit; the disease was too advanced, there was considerable heat and swelling, and the patient's health was often quite affected. Still, aside from a few hours of discomfort, no significant symptoms arose. The cure was achieved shortly afterward through methods I’ll mention shortly.
In all cases of suspicious connexion I recommend copious ablution as soon as possible.[1] The syringes I would advise to be used should have their points conically shelved off pear fashion; they fill up the urethra like a wedge, and prevent the immediate escape of the injection: all injections should be retained a few seconds, and then be allowed to flow out. It is seldom worth while to repeat the operation more than twice on an occasion; but that occasion may be resorted to two or three times a day.
In any case of suspicious connection, I recommend washing thoroughly as soon as possible.[1] The syringes I suggest using should have their tips shaped like a pear; they fit into the urethra like a wedge, preventing the injection from escaping right away. All injections should be held in for a few seconds before they are allowed to flow out. It's rarely necessary to repeat the procedure more than twice in one session, but you can do it two or three times a day.
When the nitrate of silver is used, the syringe had better be made of glass. The nitrate of silver discolors the skin, linen, &c.; therefore gloves should be worn, and care taken that the fluid be not spilt over the person or dress, but should the skin be stained, it can be removed by a strong solution of hydriodate of potash.
When using silver nitrate, it’s best to use a glass syringe. Silver nitrate can stain the skin, linen, etc.; so gloves should be worn, and care should be taken to avoid spilling the fluid on yourself or your clothing. If the skin does get stained, it can be cleaned off with a strong solution of potassium hydriodide.
The plan of injection, I must remind the reader, is only applicable in early and old cases. The recent cases, as I have before stated, are less frequently before the medical man than what we may call a “ripe” gonorrhœa. The old cases present also some difference as to the cause of their continuance, and require also some difference in their treatment, and they will be introduced under the chapter headed “Gleet.”
The injection plan, I must remind the reader, is only suitable for early and chronic cases. Recent cases, as I mentioned before, occur less often for doctors than what we can refer to as “ripe” gonorrhea. The chronic cases also differ in terms of what causes them to persist and need different treatment, which will be covered in the chapter titled “Gleet.”
But all cases of gonorrhœa are not ushered in with such severity; nor do many, if common cleanliness and quiet only be maintained, experience even the various accompaniments just described, and still fewer would if the following precautions and measures were used.
But not all cases of gonorrhea start off so severely; many people, if they just keep clean and stay calm, won’t even experience the symptoms just mentioned, and even fewer would if the following precautions and measures were taken.
The plan just laid down, may be called the surgical treatment of gonorrhœa; the following may be designated the Medical. This is divided into two methods—the one denominated the Antiphlogistic, the other Specific. The Antiphlogistic is a term applied to medicines, plans of diet, and other circumstances, that tend to oppose inflammation by a diminution of the activity of the vital powers, whereby the inflammation is subdued, and nature rights herself again of her own accord. The Specific implies a reliance upon a particular remedy, which is supposed at once to set about curing the disease, as, for instance, by giving Bark in Ague—Colchicum in Rheumatism—Cubebs or Copaiba in Gonorrhœa.
The plan we've just outlined can be called the surgical treatment of gonorrhea; the next part can be termed the Medical. This is divided into two methods: one called Antiphlogistic and the other Specific. The Antiphlogistic refers to medications, dietary plans, and other factors that aim to reduce inflammation by lowering the activity of the vital powers, allowing the inflammation to subside, and letting nature restore itself. The Specific refers to the use of a particular remedy believed to directly cure the disease, such as using Bark for Ague, Colchicum for Rheumatism, or Cubebs or Copaiba for Gonorrhea.
Now, both these plans are successful in curing gonorrhœa; but the majority of medical men adopt the former method, inasmuch as although it but quietly conducts the case to a successful termination, still it does so, whereas the specific, in unskilful hands, is often productive of many annoyances, much delay, and not always a cure.
Now, both these methods successfully treat gonorrhea; however, most doctors prefer the first method because, even though it simply leads to a successful outcome, it actually achieves that. On the other hand, the specific treatment, when administered by inexperienced hands, often results in many complications, delays, and doesn’t always guarantee a cure.
Our plan, however, is as follows: in the first place, I take into consideration the appearance of the patient; if he be strong, robust, sanguine, or of full habit, and youthful—if it be his first attack, and if the symptoms be ushered in with any degree of severity, I invariably and rigidly (where I choose not the surgical) pursue the antiphlogistic course of treatment; if the case be in a person of phlegmatic temperament, of mature age, and the disease be but a repetition of the past, and there be no evidence of physical excitement, I fearlessly adopt the specific. Where, in the third place, I encounter a patient with no very prominent peculiarity, nor with symptoms demanding extraordinarily active measures, experience has taught me the propriety of cautiously combining the two methods—a mild aperient had best always a precede a tonic or a stimulant, in cases where there is a doubt of inflammation lurking in the system; and, recollecting the tendency our complicated organization has, when assailed by a distemper,[30] to become irritable, it is always as important to know when to withhold a remedy as when to prescribe one.
Our plan, however, is as follows: first, I consider the patient's appearance; if they are strong, healthy, energetic, or robust, and young—if this is their first attack, and if the symptoms present themselves with any severity, I consistently and strictly (when I don't opt for surgery) follow the anti-inflammatory treatment approach; if the case is in someone with a calm temperament, of older age, and the condition is just a recurrence of the past, with no signs of physical distress, I confidently use the specific treatment. When I encounter a patient with no significant distinguishing features or symptoms that require highly active measures, experience has taught me it’s appropriate to carefully combine both methods—a mild laxative should always be given before a tonic or stimulant in cases where there might be hidden inflammation in the body; and, remembering the tendency of our complex system, when faced with an illness,[30] to become irritable, it’s just as important to know when to hold back a remedy as it is to know when to prescribe one.
The three following imaginary cases will serve as no inapt illustration of the principles laid down:—
The three imaginary cases that follow will effectively illustrate the principles outlined:—
A. B. A man twenty-six years of age, five feet six inches in height, weighing eleven stone six pounds, of a full rounded form—florid complexion, of what is termed a sanguine temperament, and harassed with the following symptoms: profuse discharge in large yellow clotted lumps of gonorrhœal virus—intolerable scalding on passing water—great pain at the rectum at the close of micturition—redness and swelling of the orifice of the glans penis, puffiness of the prepuce, a vicious chordee—inclination to headache—a bounding pulse—hot skin, and an anxious mind. Treatment: say first bleeding, then purging; warm bath, saline powders or mixtures, cold lotions to the part, rest, abstinence; the following eve, symptoms will be less severe. Continue the powders, temperance and quiet. In a few days, the discharge will be lessened, the scalding mitigated, the chordee gone, and the fever exchanged for the cool skin of health. The resuscitative powers of nature await only the fillip of some gentle stimulant, and the sick man throws off his mantle for the coronal of health.
A. B. A twenty-six-year-old man, five feet six inches tall, weighing eleven stone six pounds, with a full rounded body—flushed complexion, described as having a sanguine temperament, and experiencing the following symptoms: heavy discharge in large yellow clots of gonorrheal virus—intense burning when urinating—severe pain in the rectum at the end of urination—redness and swelling at the opening of the glans penis, swelling of the foreskin, a vicious chordee—tendency to headaches—a strong pulse—hot skin, and an anxious mind. Treatment: start with bleeding, then move on to purging; warm baths, saline powders or mixtures, cold lotions for the affected area, rest, and abstinence; by the next evening, symptoms will be less severe. Continue the powders, maintain moderation and calmness. In a few days, the discharge will decrease, the burning will ease, the chordee will resolve, and the fever will give way to the cool skin of health. The healing power of nature just needs a little boost from some gentle stimulant, and the sick man will cast off his struggles for the crown of health.
B. C. At twenty-three, dark countenance, marked features, well developed muscular form, pulse 66, bilious temperament, accustomed to late hours, hard drinking, and seldom still, and subject to clap. Symptoms: plenteous discharge with but little scalding, and no inconvenience beyond the suspension of ordinary sensualities. Treatment: cleanliness, cubebs or copaiba, injections, a black draught, and half a dozen days’ rest, release him from his quarantine.
B. C. At twenty-three, dark complexion, defined features, well-developed muscular build, pulse 66, irritable temperament, used to staying up late, heavy drinking, and rarely resting, and subject to gonorrhea. Symptoms: abundant discharge with minimal burning, and no discomfort beyond the interruption of regular sexual activities. Treatment: cleanliness, cubebs or copaiba, injections, a laxative, and a week of rest to be freed from his quarantine.
C. D. At nineteen, a timid bashful youth, for the first time infected with gonorrhœa, which he had enduringly borne for the last fortnight, having neglected until now to seek professional aid, although cajoled into the purchase and imbibing of some popular “never-failing antidote” for a “certain disease.” Symptoms: discharge cured? right testicle swollen, and treble the size of the other, and excruciatingly painful; frequent desire to pass water, pain in the groin and back, general lassitude, and a feeling of illness all over. Treatment: leeches, warm bath, bed, purging, fever medicines, cold lotions, hot fomentations, low diet and patience, a month’s imprisonment, and a slow recovery. Had the treatment of the first two cases been reversed, the results would have been very different: and had the last sought timely and efficient aid, he would have been spared much that he endured.
C. D. At nineteen, a shy and introverted young man, he was experiencing gonorrhea for the first time, which he had been dealing with for the past two weeks. He had put off seeking medical help until now, despite being persuaded to buy and try some popular “surefire cure” for a “specific disease.” Symptoms: discharge cured? Right testicle swollen, three times the size of the other, and extremely painful; frequent urge to urinate, pain in the groin and back, overall fatigue, and a general feeling of illness. Treatment: leeches, warm baths, rest, laxatives, fever medication, cold compresses, hot packs, a bland diet, patience, a month’s confinement, and a slow recovery. If the treatments for the first two cases had been swapped, the outcomes would have been much different; and if the last one had sought prompt and effective treatment, he would have avoided much of what he suffered.
However, to particularize the treatment for each symptom; to commence, I will request the reader to remember that on the first appearance of gonorrhœa, attended with an unusual inflammatory aspect, I practise, where permissible, venesection; if the case demand it not, at least there should be administered an aperient; let, therefore, a dose of opening medicine be taken immediately (Form 1). This is the first step toward reducing inflammatory[31] action—the next should be directed toward allaying the local symptoms, by diminishing the nervous irritability of the urethric passage.
However, to focus on the treatment for each symptom; to start, I ask the reader to remember that when gonorrhea first appears, with an unusual inflammatory appearance, I perform bloodletting if it's appropriate; if that's not necessary, at least a laxative should be administered. Therefore, a dose of a laxative should be taken right away (Form 1). This is the first step toward reducing inflammatory[31] action—the next step should be aimed at soothing the local symptoms by reducing the nervous irritation in the urethra.
With this view, no plan surpasses that of bathing the penis in warm water, or immersing the entire body in a warm bath. The former should be repeated several times in the day; the latter daily, or certainly on alternate days, so long as the severity lasts.
With this in mind, nothing beats soaking the penis in warm water or taking a warm bath. You should do the first one several times a day; the second one daily or at least every other day while the issue persists.
By these means, the parts will be preserved clean, and will derive benefit from the soothing influence of warmth; and, in many cases, this will be the means of averting chordee or swelled testicle.
By doing this, the parts will stay clean and benefit from the soothing effect of warmth; in many cases, this will help prevent chordee or swollen testicle.
Where, however, from peculiar circumstances, warm water and warm baths are not to be had, the penis should be bathed in cold water, or encircled with pledgets of rags or lint, moistened with cold goulard or rose-water. Warm, however, is to be preferred, although cold water seldom fails of affording relief.
Where, however, due to specific circumstances, warm water and warm baths are unavailable, the penis should be washed in cold water or wrapped with pieces of cloth or lint, dampened with cold goulard or rose water. Warm water is preferred, but cold water often provides relief.
To lessen the acrimony of the urine, which keeps up the irritability, and somewhat to lower the system, all strong drinks, such as ale, beer, wine, and spirits, should be avoided, and milk, tea, barley-water, toast and water, linseed tea, gum arabic in solution, and other such mucilaginous diluting liquors taken instead. The diet should be lowered: in fact, a spare regimen should be adopted, not wholly abstaining from animal food, but partaking of it only once in the day, and carefully excluding all salted meats, rich dishes, soups, gravies, &c. The usual employment should be suspended, and rest should be taken as much as possible in a recumbent posture.
To reduce the acidity of the urine, which causes irritation, and to slightly lower the body's overall activity, all strong drinks like ale, beer, wine, and spirits should be avoided. Instead, drink alternatives like milk, tea, barley water, toast and water, linseed tea, gum arabic in solution, and other similar soothing drinks should be consumed. The diet should be lighter: essentially, a simple diet should be adopted, not completely cutting out animal products, but limiting them to once a day and carefully avoiding all salted meats, rich dishes, soups, gravies, etc. Regular activities should be paused, and as much rest as possible should be taken while lying down.
Of course the preceding remarks apply only to cases of severity; I mean such cases as first attacks ordinarily prove; and which remarks, if attended to, will greatly mitigate the violence of the disease.
Of course, the comments above only apply to severe cases; I’m talking about first attacks, which are usually what we see; and if these points are taken into consideration, they will significantly reduce the intensity of the illness.
To assist the foregoing treatment, the aperient medicine, which should be repeated, at least, on alternate days, until the inflammation is ameliorated, should be followed by some saline or demulcent medicine to allay the general disturbance. Several formulæ are suggested for that purpose, suitable to various temperaments and conditions—[See Forms 2, 3, 4, 5 in Formulæ annex.]
To support the previous treatment, the laxative medication should be taken again at least every other day until the inflammation improves, followed by some saline or soothing medication to relieve the overall discomfort. Several formulas are recommended for this purpose, tailored to different temperaments and conditions—[See Forms 2, 3, 4, 5 in Formulæ annex.]
By these means, the disease, if not aggravated by intemperance of living, or otherwise, will gradually subside, and in the course of a fortnight or three weeks, cease entirely, without the aid of any other remedy whatever.
By these methods, the disease, as long as it's not made worse by unhealthy living or other factors, will gradually go away, and in about two weeks to three weeks, it will completely stop without needing any other treatment at all.
But we need not rest satisfied with merely “showing” the disease through its stages; we can expedite it, and many of its steps we can skip over, and here it is we may call to our aid the specific method of treatment alluded to. This specific method consists of the suspension of a vitiated secretion, and a restoration of a healthy one. Now how this is effected we know not; we only know that it can be done—and experience has taught us that it may be done safer at one time than another. During the existence of a fevered state of the circulation, it would be highly impolitic suddenly to check a discharge from any surface, much less one situated like the mucous membrane of the urethra, in the immediate connexion, as it is, of important nerves and glandular structures—a metastasis[33] of the inflammation will almost invariably ensue; and hence we account for swollen testicles, buboes, painful affections of the bladder, &c. Whereas, on the subsidence of inflammation, the revulsion is borne; and to our satisfaction, the disease disappears. A constitution in a state of excitement is like a fretted child—it will have its “will” out, and the rod is not always the safest corrective.
But we shouldn't be satisfied with just “showing” the disease through its stages; we can speed up the process and skip some steps. This is where we can use the specific method of treatment mentioned earlier. This specific method involves stopping an unhealthy secretion and restoring a healthy one. We don’t know exactly how this happens; we just know it can be done—and experience has shown us that it can be done more safely at certain times than others. When there's a feverish state in the circulation, it would be very unwise to suddenly stop a discharge from any surface, especially one like the mucous membrane of the urethra, which is closely connected to important nerves and glands—this almost always leads to a spread of inflammation. That’s why we see swollen testicles, buboes, painful bladder issues, etc. However, once the inflammation decreases, the body can handle the change, and thankfully, the disease goes away. A body that’s worked up is like a restless child—it needs to have its “say,” and punishment isn’t always the best solution.
On the subsidence, therefore, of the scalding, and a lessening of the general fever, the specific plan of treatment may be commenced. Upon the same principle that the surgical treatment is selected according to the symptoms, so also are the just-named preliminaries in many cases dispensable, and hence, as hereafter detailed, it will be found that the antiphlogistic and specific do not go always hand in hand. However, to explain the latter:—
On the decrease of the fever and a reduction of the burning sensations, the specific treatment plan can begin. Just like the choice of surgical treatment is based on the symptoms, the aforementioned preliminaries are often unnecessary in many cases. As will be explained later, it's important to understand that the antiphlogistic and specific treatments do not always occur together. However, to clarify the latter:—
For instance, cubebs may be taken alone, in water, in doses of a tablespoonful twice or thrice daily. If cubebs produce no good effect in four or five days, it had better be discontinued, and other means sought after.
For example, cubebs can be taken by themselves or in water, in doses of one tablespoon two or three times a day. If cubebs don’t show any improvement within four or five days, it’s best to stop using them and look for other options.
These proceedings usually carry the disease to a close, and, if no adventitious circumstances occur, successfully and speedily. It is well to deserve success, but it can not be always commanded.
These processes usually bring the illness to an end, and, if no unexpected events happen, effectively and quickly. It's good to earn success, but it can't always be guaranteed.
The business engagements of young men render it almost impossible for them to devote that care and attention so importantly requisite; and few, consequently, will be found who will be fortunate enough to escape the usual concomitants of a gonorrhœa.
The business commitments of young men make it nearly impossible for them to give the necessary care and attention that are so important; as a result, few will be fortunate enough to avoid the typical consequences of gonorrhea.
The inflammation extends in general not more than two inches down that passage, so that much force is not required to inject the intended fluid, nor should an unnecessary quantity be used.
The inflammation usually extends no more than two inches down that passage, so it doesn't require much force to inject the intended fluid, and you shouldn't use an unnecessary amount.
When the inflammation reaches the bladder—which is indicated by pain in that viscus and the perinœum, with a constant desire to pass water—the taking of a warm bath at a temperature of 100°, and remaining therein for a quarter of an hour, will afford essential relief.
When inflammation affects the bladder—shown by pain in that area and the perineum, along with a constant urge to urinate—taking a warm bath at about 100°F and staying in it for fifteen minutes will provide significant relief.
When a chordee is attendant on a gonorrhœa, and the patient can not sleep, the draught (Form 13) may be taken on going to bed, or the powder (Form 14) in some gruel. The embrocation (Form 15) rubbed on the parts affected, however, will instantly remove both the pain and the spasmodic contraction, and not unfrequently prevent their recurrence. Care must be taken that the embrocation be only used for its specific purpose, and not swallowed by mistake, as it is poisonous.
When a chordee accompanies gonorrhea and the patient can't sleep, the drink (Form 13) can be taken before bed, or the powder (Form 14) mixed into some gruel. The lotion (Form 15) applied to the affected area will immediately relieve both the pain and muscle spasms, and often prevent them from returning. It is important to ensure that the lotion is used strictly for its intended purpose and not accidentally ingested, as it is toxic.
In the event of the patient being obliged to follow his ordinary occupation, or to go about, the use of a suspensory bandage will be found of great benefit; indeed it is indispensable, and the neglect of it has often brought on swelled testicle, or most excruciating chordee.
In case the patient needs to continue with their regular job or activities, using a suspensory bandage will be very helpful; in fact, it's essential, and failing to use it has often led to swollen testicles or severe pain.
By way of recapitulation, the treatment of gonorrhœa thus far consists: in severe cases, of bleeding; in ordinary ones, and in both, of warm bathing, local or general—where impracticable, cold—attention to diet, the taking of aperient, soothing and astringent medicines, rest as much as possible, and the use of the suspensory bandage.[36] These remarks are equally applicable, then, through every stage of this complaint that is accompanied by inflammation, and may be relied upon as the most effectual to avert all the consequences I now proceed to detail.
To summarize, the treatment for gonorrhea so far includes: for severe cases, bleeding; for regular cases, and in both types, warm baths, whether local or full-body—if not possible, then cold baths—focus on diet, taking laxatives, soothing and astringent medicines, getting as much rest as possible, and using a support bandage.[36] These suggestions apply to every stage of this condition that's accompanied by inflammation and can be trusted as the most effective way to prevent all the complications I’m about to describe.
The consideration of the symptoms here following is not in the order in which they always occur; for swelled testicle may ensue without phymosis or paraphymosis preceding, or even being present; and the converse holds equally good with regard to every other.
The symptoms listed here do not always appear in a specific order; for example, a swollen testicle can occur without phimosis or paraphimosis happening beforehand or at all; and the opposite is true for every other symptom as well.
The successful treatment of phymosis (that condition of the foreskin in which it can not be drawn back over the glans) depends very much upon local management. Bathing the part frequently in warm water, the daily use of the warm bath, and the frequent injection, by means of a syringe, of warm milk and water, are generally all that is required to reduce phymosis; but where it is attended with much inflammation, where the glans is excoriated, probably by the discharge from the urethra accumulating between it and the prepuce, and thereby inducing irritation, bleeding is even sometimes necessary, the strictest antiphlogistic regimen should be preserved, and the treatment advised in the early stages of gonorrhœa scrupulously followed.
The successful treatment of phimosis (the condition where the foreskin can't be pulled back over the glans) relies heavily on local care. Regularly bathing the area in warm water, taking warm baths daily, and frequently injecting a mix of warm milk and water using a syringe are usually all that's needed to reduce phimosis. However, if there’s significant inflammation or if the glans is irritated, possibly due to discharge from the urethra building up between it and the foreskin, bleeding may sometimes be necessary. It's crucial to maintain a strict anti-inflammatory regimen and to carefully follow the treatment recommended for the early stages of gonorrhea.
Sometimes the prepuce becomes so swollen as to assume an œdematous or dropsical appearance; in which case it may be scarified with a lancet, or several leeches applied. With the exception of concealing the state of the glans, phymosis is less dangerous than paraphymosis, and is most usually produced by the patient worrying the part, by frequently uncovering the glans to observe its condition. Where a discharge is perceived oozing from beneath the prepuce, which is not urethral, and the glans does not feel sore or tender, the injection (Form 16) syringed up five or six times a day, will prove very efficacious in healing the ulceration.
Sometimes the foreskin becomes so swollen that it looks puffy or swollen with fluid; in this case, it can be sliced open with a small knife, or several leeches can be applied. Besides hiding the condition of the head of the penis, phimosis is less dangerous than paraphimosis and is usually caused by the patient frequently exposing the head to check its condition. If there’s a discharge coming from under the foreskin that isn’t from the urethra, and the head doesn’t feel sore or tender, injecting (Form 16) five or six times a day will be very effective in healing the ulceration.
Where there is an unnatural elongation of the prepuce, it will be constantly subject to phymosis, not only from gonorrhœal inflammation, but from the accumulation of[37] the natural secretions of the part. In that case, cleanliness is the only remedy the patient can employ of himself. Occasionally it is necessary to have recourse to the surgeon’s knife.
Where there is an unnatural stretching of the foreskin, it will often be prone to phimosis, not just from gonorrheal inflammation, but also from the buildup of[37] natural secretions in the area. In that situation, maintaining cleanliness is the only remedy the patient can manage on their own. Sometimes, it may be necessary to resort to surgery.
Paraphymosis is the opposite to phymosis, and usually arises in this way: the orifice of the prepuce, being contracted by the inflammation, is drawn back for the purpose of washing or examination, and is allowed to remain, or, as frequently happens, it can not be redrawn. When this continues some time, considerable inflammation, both of the glans and prepuce, arises. The contracted orifice pressing more tightly, it will often happen that a sloughing of both it and the glans will take place; but this occurs only in consequence of neglect, or in constitutions injured by intemperance.
Paraphimosis is the opposite of phimosis and usually happens like this: the opening of the foreskin becomes tight due to inflammation, gets pulled back for cleaning or examination, and then either stays there or, as often occurs, can't be pulled back. If this lasts for some time, significant inflammation of both the glans and the foreskin can occur. As the tight opening squeezes more, it can lead to tissue death of both it and the glans; however, this only happens due to neglect or in individuals with weakened constitutions from unhealthy habits.
If seen and attended to early, this state may be removed very easily. The penis should be immersed in a basin of cold water, or sponged, so as to cool it as much as possible; or it may be well oiled. In either case there will not be much difficulty in pressing up the glans and drawing up the prepuce over it; but where adhesion has taken place, or ulceration exists, it will be harder to accomplish: the adhesions must be separated, or the stricture divided with the scalpel.
If caught and addressed early, this issue can be resolved quite easily. The penis should be soaked in a bowl of cold water, or wiped down, to cool it as much as possible; or it can be well-lubricated. In either situation, it won't be too difficult to push back the glans and pull the foreskin over it; but if there is adhesion or ulceration, it will be tougher to manage: the adhesions need to be separated, or the stricture must be cut with a scalpel.
I need scarcely observe, that such an operation is out of the province of the non-professional person, who should lose no time in consulting his surgeon.
I hardly need to point out that this kind of procedure is beyond the skills of someone who isn't a professional and should waste no time in consulting their surgeon.
I omitted to mention, in the description of the symptoms of gonorrhœa, that occasionally, in very severe cases, a tumor forms in the perinœum, which, if neglected, proceeds to suppuration, and establishes a fistulous communication with the urethra. On the instant of such a swelling appearing, leeches, fomentations, and poultices, should be applied with a view to disperse it; but the management of such a case had better be intrusted to the surgeon.
I forgot to mention, in describing the symptoms of gonorrhea, that sometimes, in very severe cases, a lump can form in the perineum, which, if ignored, can lead to pus formation and create a fistula connecting to the urethra. As soon as such a swelling appears, leeches, warm compresses, and poultices should be applied to try to reduce it; however, it's best to leave the management of such a case to the surgeon.
Excoriation of the membrane of the glans or prepuce requires for its treatment frequent ablution with warm water until the redness and discharge somewhat diminish, when Form 16 may be resorted to, and applied, if practicable, by a moistened layer of lint; but if accompanied by phymosis, the syringe must be used.
Excoriation of the membrane of the glans or prepuce requires frequent washing with warm water for treatment until the redness and discharge decrease somewhat. At that point, Form 16 may be used and applied, if possible, with a damp layer of lint; however, if it is accompanied by phimosis, a syringe should be used.
Warts, if not large, are easily removed, by brushing[38] them with the muriated tincture of iron, or the application of a lotion of lunar caustic (Form 17).
Warts, if they aren't too large, can be easily removed by brushing them with muriated tincture of iron or by applying a lotion of lunar caustic (Form 17).
Where they are numerous and large, and resist the remedies just recommended, the nitric acid is an excellent escharotic; it gives little or no pain, and is rarely productive of inflammation. The glans, if not naturally denuded (in which instance, by the way, warts seldom accrue), should be kept so for a time; and the nitric acid, after a few moments, washed off with cold water. Notwithstanding, excision is sometimes necessary to their complete removal.
Where they are abundant and significant, and don’t respond to the previously mentioned treatments, nitric acid is an effective caustic agent; it causes minimal pain and rarely leads to inflammation. The glans, if not naturally exposed (in which case, by the way, warts usually don't appear), should be kept exposed for a while; and the nitric acid should be rinsed off with cold water after a few moments. However, surgical removal is sometimes required for complete elimination.
When the organs of generation are infested by pediculi, or crab-lice, the most efficacious and agreeable remedy is the sulphur-bath; one bath generally effecting an extinction of every one of them, even though they be all over the body.
When the reproductive organs are infested by pubic lice, the best and most effective treatment is a sulfur bath; usually, one bath is enough to eliminate all of them, even if they are spread throughout the body.
Some recommend shaving the hair off the pubis, the locality in which the vermin are most usually engendered, and applying blue ointment or the black wash. Such a practice is seldom ineffectual, but the irritation attendant upon the reproduction of hair is absolutely intolerable. The hair need not be removed, as the above remedies will be all-sufficient without it. Rubbing the parts well with strong mercurial (or blue) ointment, or the black wash (Form 18), or even powdering them with calomel, will at once destroy the insects, and thereby remove the itching.
Some suggest shaving off the pubic hair, where the pests are most often found, and using blue ointment or the black wash. This method is usually effective, but the irritation that comes with hair regrowth is really unbearable. The hair doesn’t have to be removed, as the remedies mentioned will work just fine without it. Rubbing the area well with strong mercurial (or blue) ointment, or the black wash (Form 18), or even dusting it with calomel, will quickly eliminate the insects and alleviate the itching.
Swelled testicle, or hernia humoralis, more especially that proceeding from gonorrhœal irritation, is ushered in and discovered in the following manner: The patient, on some sudden movement of the body, experiences a pain, darting from one of the testes (both being rarely affected at the same time) to the loins—the left testicle is the one generally attacked. On examination, he finds that the testicle is rather swollen and full, and very painful on being handled; the swelling quickly increases and becomes[39] hard, which hardness extends to the spermatic chord, presenting the feel of a rope, passing from the scrotum to the groin.
Swollen testicle, or hernia humoralis, especially that resulting from gonorrheal irritation, is indicated and identified in the following way: The patient, upon a sudden movement, feels a sharp pain shooting from one of the testes (both are rarely affected at the same time) to the lower back—the left testicle is typically the one that gets affected. Upon examination, the patient finds that the testicle is somewhat swollen and full, and very painful to touch; the swelling quickly increases and becomes[39] hard, with this hardness extending to the spermatic cord, which feels like a rope running from the scrotum to the groin.
It is remarkable that when swelled testicle occurs, the discharge from the urethra, which, from previously being very profuse, and the scalding on making water, which was very severe, both suddenly diminish, or cease entirely, until the inflammation of the testis declines; hence, it has been supposed by some, that the disease is translated from the urethra to the testicle.
It’s interesting that when a swollen testicle happens, the discharge from the urethra, which used to be very heavy, and the burning sensation when urinating, which was quite intense, both suddenly decrease or stop completely until the inflammation of the testis goes down; therefore, some people believe that the disease moves from the urethra to the testicle.
It is more probably however, derived from the sympathy between the two; the irritation of the one affecting the other, and the preponderance of inflammation in the testicle acting on the principle of counter-irritation to the urethra, and, for a time, thereby lessening the disease in it: for it is observed that, as soon as one improves, the disease returns in the other. The treatment of hernia humoralis must be strictly antiphlogistic. In no form of gonorrhœal disease is bleeding more absolutely necessary.
It’s more likely, however, that it comes from the sympathy between the two; the irritation in one affects the other, and the increased inflammation in the testicle operates on the principle of counter-irritation to the urethra, temporarily reducing the disease in it: it’s noticed that as soon as one improves, the disease comes back in the other. The treatment for hernia humoralis must be strictly anti-inflammatory. In no case of gonorrheal disease is bleeding more absolutely necessary.
The timely and prompt loss of twelve or sixteen ounces of blood from the arm will often cut short the complaint, and render other remedies almost unnecessary; while the temporising delay, under the vain hope of the inflammation subsiding, will allow the disease to make rapid progress, and impose a necessity of several weeks’ rest and absence from business, before a cure can be effected.
Losing twelve or sixteen ounces of blood from the arm promptly can often resolve the issue and make other treatments nearly unnecessary. However, waiting too long in the false hope that the inflammation will go down can let the illness progress quickly, requiring several weeks of rest and time away from work before a cure can be achieved.
Immediately, then, on the occurrence of swelled testicle, I would recommend the patient to be bled—to take some aperient medicine, and, if the inflammation continues, to apply from twelve to eighteen leeches, and afterward suffer the wounds to bleed for twenty minutes in a warm bath; to retire to bed or to the sofa, and to maintain a horizontal posture. If he be strong, young, and robust, an emetic (Form 19) may be given previous to the aperient, which has been known to remove the swelling almost instantaneously.
As soon as the patient has a swollen testicle, I would suggest they get some blood drawn, take a laxative, and if the inflammation doesn’t go down, apply between twelve to eighteen leeches. After that, let the wounds bleed for twenty minutes in a warm bath. The patient should then lie down either in bed or on the sofa, keeping a horizontal position. If the patient is strong, young, and healthy, they can take an emetic (Form 19) before the laxative, which is known to reduce the swelling almost immediately.
With regard to local applications, the repeated employment of leeches, fomentations, and poultices, with the frequent use of the warm bath, and, above all, keeping the testicle constantly supported by means of a bag, truss, or suspensory bandage, will subdue the disease in a very short time, without impairing the functions of the important organ concerned.
With local treatments, consistently using leeches, warm compresses, and poultices, along with frequent warm baths, and especially keeping the testicle supported with a bag, truss, or suspensory bandage, will effectively treat the condition in a very short time without harming the functions of the important organ involved.

A hardness, however, of the epididymis commonly remains and continues during life, but rarely gives rise to any inconvenience, although this may often be remedied by compressing the testicles with strips of adhesive plaster, as seen in the cut.
A hardness in the epididymis often persists throughout life, but it usually doesn't cause any problems. However, this can often be fixed by wrapping the testicles with adhesive strips, as shown in the image.
Almost every case of inflamed testicle will terminate favorably by strictly pursuing the plan proposed; but when, from any untoward circumstance, the inflammation proceeds to suppuration, the case must be treated like one of common abscess, in which event professional aid should be sought for without delay.
Almost every case of inflamed testicle will end positively by closely following the suggested plan; however, if, due to any unfortunate circumstances, the inflammation leads to pus formation, the case must be handled like a regular abscess, in which case professional help should be sought immediately.
Other diseases of the testicle will be treated upon under a specific head.
Other testicular diseases will be covered under a specific category.
To return to the treatment of Gonorrhœa:—On the abatement of all or any of the enumerated symptoms, such as the diminution of the scalding upon making water, the subsidence of chordee, the escape from, or cure of, swelled testicle, phymosis and paraphymosis, warts, crabs, excoriations, &c., the discharge may still continue, though thicker in consistence, and deeper in color: and it is at this period, which I will call chronic gonorrhœa, when all inflammatory symptoms have left, that stimulants may be judiciously given; but it must be borne in mind that relapses often occur from imprudence: and this chronic form requires as much attention as the acute or early stage. (See article Gleet.)
To go back to treating gonorrhea:—When all or some of the mentioned symptoms decrease, like the burning sensation while urinating, the easing of chordee, the resolution or healing of swollen testicles, phimosis and paraphimosis, warts, crabs, and abrasions, the discharge might still persist, although it may become thicker and darker. At this stage, which I’ll refer to as chronic gonorrhea, when all inflammatory symptoms have disappeared, stimulants can be appropriately administered; however, it’s important to remember that relapses can often happen due to carelessness: this chronic form needs just as much attention as the acute or earlier stage. (See article Gleet.)
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ———<>———
Gleet.—Gleet is certainly, as its name implies, a discharge of thin ichor from a sore. Patients usually understand, and medical men usually allow, a gleet to be a discharge from the urethra, which has existed some time, of a whitish color, unattended with pain, and that is not infectious, by which is meant is incapable of producing gonorrhœa. There are several kinds of morbid secretions, the successful treatment of which depends upon a knowledge of their differences. They may be divided into two principal orders—those secreted from the mucous surface of the urethra or bladder, and those which proceed from the various glands-leading into one or the other. Gleet is a term popularly applied to both, but more strictly relates to that which proceeds from the membrane lining the urinary canal. There is great analogy in inflammatory affections between the mucous membrane of the digestive and pulmonary, as well as urinary passages. In inflammatory sore throat, the secretions assume various appearances; there is a discharge of viscid mucus, of purulent matter, or of a thin watery nature; these secretions are dependant upon the amount and duration of the inflammation present. Exactly in like manner may be explained those issuing from the urethra. They are consequently alike modified by treatment, by diet, by rest, and aggravated by a departure from constant care. It is the nature of all membranes, lining canals that have external outlets, to attempt the reparative process by pouring forth discharges, while those which line the structures that have not, effect their cure by union with the opposite[42] surface. It is an admirable provision, else important passages might become closed, and so put a stop to vital processes; and in the other case, accumulations ensue that could not escape without occasioning serious mischief. When, however, disease has existed a long time, the operation of the two kinds of membranes is reversed. The serous,[2] through inflammation, take on the character of abscess, dropsy, or other secretions, and the mucous ulcerate or form adhesions, as evidenced in stricture, or ulceration of the throat or urethra. Gleet may be a spontaneous disease, that is to say, may arise from other causes than infection. It may exist independently of gonorrhœa, and be the result of cold, of intemperance, and of general or of local excess. Its long continuance and neglect, however, renders it infectious, and it also gives rise to ulceration, excrescences, and stricture: and when, from other causes, ulceration, or excrescences, or stricture, are set up, gleet is in return generally one of their consequences. Gleet, despite these various occasions, is, after all, most frequently a remnant of gonorrhœa; and it is very difficult to define the time or point where the one ends and the other commences. Pathologists draw this distinction between the two:—they say that gonorrhœal discharge consists of globules, mixed with a serous fluid, while gleet is merely a mucous secretion. I confess it difficult for a non-professional person to decide which is which, the resemblance, in fact, being so great—a gonorrhœal discharge being one day thick and yellow, a few days afterward thin and whitish, and at one time in quantity scanty, and the next profuse. Gleet assumes nearly the same changes. The best test for distinguishing them is, by regarding the accompanying symptoms. Where there is pain on passing water, bladder-irritability, tenderness in the perinœum or neighboring parts, and the discharge plentiful and offensive, staining the linen with a “foul spot,” it may, without much fear, be decided to be clap; but where the discharge is next to colorless, like gum-water, for instance, and where there is no other local uneasiness than a feeling of relaxation, and where it has existed for a long period, and was, or was not, preceded by a gonorrhœa, it may fairly be called a gleet. Now where[43] does the discharge of gleet come from? Let us recapitulate its causes; first from clap, which is a specific inflammatory affection. It may therefore be a chronic inflammatory state of the lining membrane of the urethra, of greater or less extent; in which case we would call it chronic gonorrhœa, and which would be owing to a relaxed state of the secretive vessels. We know that when a disease exists for a long while, and is one not positively destructive to life, a habit of action is acquired that renders its continuation in that state as natural as its healthy condition. This is the state of the secretive vessels in gleet, arising from gonorrhœa; and hence the discharge is poured forth, instead of the secretion natural to the urethral passage in its healthy order. Secondly, such may have been the severity of a clap, that ulceration of some portion of the urethra may have taken place. The disease may have got well except in that identical spot which, owing to the constant irritation occasioned by the urine passing over it, struggles with the reparative intention and effort of nature, and exists even for years. Thirdly, when stricture is brewing, which will be explained in an appropriate chapter, the alteration going on gives forth a discharge, and, as I have stated in another part of this work, I here repeat, that a long and obstinate gleet, as the slightest examination would testify, rarely fails to indicate the presence of a stricture. Lastly, gleet may be produced by loss of tone in some or the whole portion of the secretive vessels, induced by one or many of the accidents of life, or the various kinds of physical intemperance when they not only weep forth various kinds of fluids, at irregular intervals, which impair the muscular and nervous energy of the generative organ, but render persons laboring under this description of weakness very susceptible of infection, if they hold sexual contact with those but slightly diseased. Hence persons laboring under this form of debility incur what others escape. An individual so circumstanced would receive a taint from a female having leucorrhœa. Very many inconveniences have arisen from this infirmity, giving birth occasionally to unjust suspicions, and creating alarms of the most distressing nature.
Gleet.—Gleet is definitely, as the name suggests, a discharge of thin fluid from a sore. Patients generally understand, and doctors typically agree, that a gleet is a discharge from the urethra that lasts for some time, has a whitish color, is painless, and is not infectious, meaning it cannot cause gonorrhea. There are several types of abnormal secretions, and successful treatment relies on understanding their differences. They can be divided into two main categories—those secreted from the mucous surfaces of the urethra or bladder and those that come from the various glands leading to either. Gleet is a term commonly used for both, but it more specifically refers to the discharge from the membrane lining the urinary canal. There is a strong similarity between inflammatory conditions affecting the mucous membranes of the digestive, respiratory, and urinary systems. In cases of inflammatory sore throat, the secretions can appear in various forms; there can be a discharge of thick mucus, pus, or thin watery fluid; these secretions depend on the severity and duration of the inflammation present. Similarly, those from the urethra can also vary. They are therefore influenced by treatment, diet, rest, and worsened by a lack of consistent care. It is the nature of all membranes lining canals that have external openings to try to heal by producing discharges, while those lining structures without such openings heal by fusing with the opposite surface. This is a marvelous system; otherwise, important passages could block and stop vital functions, and in the other case, fluids could accumulate, causing serious harm. However, when a disease persists for a long time, the functioning of these two types of membranes can reverse. The serous membranes, through inflammation, can develop abscesses, swelling, or other secretions, and the mucous membranes can ulcerate or form adhesions, as seen in strictures or ulcers of the throat or urethra. Gleet can be a spontaneous condition, meaning it may arise from causes other than infection. It can exist independently of gonorrhea and result from factors like cold, excessive drinking, or both general and local overindulgence. However, if it lasts long enough and is neglected, it can become infectious, leading to ulceration, growths, and strictures; and when other causes create ulceration, growths, or strictures, gleet is often one of their outcomes. Despite these various causes, gleet is most frequently a residue of gonorrhea, and it is quite challenging to determine when one ends and the other begins. Pathologists make a distinction between the two: they state that gonorrheal discharge contains globules mixed with a serous fluid, while gleet consists solely of mucous secretion. I find it difficult for an average person to tell them apart, as their similarities are so great—a gonorrheal discharge may be thick and yellow one day, thin and whitish a few days later, and sometimes scarce in quantity and other times excessive. Gleet undergoes nearly the same variations. The best way to distinguish them is by looking at the accompanying symptoms. If there is pain while urinating, bladder irritation, tenderness in the perineum or nearby areas, and the discharge is plentiful and foul-smelling, staining linen with a “dirty spot,” it can likely be diagnosed as clap (gonorrhea); but if the discharge is nearly colorless, like gum-water, and if there's no significant local discomfort other than a feeling of relaxation, particularly if it has persisted for a long time, and was preceded by gonorrhea or not, it can reasonably be labeled as gleet. Now, where does the discharge of gleet originate? Let's recap its causes; first, from clap, which is a specific inflammatory condition. It may therefore indicate a chronic inflammatory state of the lining membrane of the urethra, varying in extent; in which case we would refer to it as chronic gonorrhea, due to a relaxed condition of the secretive vessels. We know that when a disease lasts for a long period and is not fatal, a pattern of action is established that makes its continuation in that state feel as natural as a healthy condition. This is the condition of the secretive vessels in gleet resulting from gonorrhea; thus, the discharge occurs instead of the normal secretion of the urethra when it is healthy. Secondly, the severity of a clap might have caused ulceration in some part of the urethra. The disease might have healed except for that specific spot, which, due to continuous irritation from urine passing over it, struggles with the body's natural healing efforts and can persist for years. Thirdly, when a stricture is developing—explained further in a designated chapter—the changes taking place lead to a discharge, and, as I noted elsewhere in this work, a prolonged and stubborn gleet, upon the slightest examination, typically indicates the presence of a stricture. Finally, gleet can arise from a loss of tone in some or all of the secretive vessels, triggered by various life events or forms of physical overindulgence that cause them to release different fluids at irregular times, undermining the muscular and nervous strength of the reproductive organ, making individuals with this form of weakness very vulnerable to infections, especially if they engage in sexual contact with only slightly diseased individuals. Consequently, individuals experiencing this weakness may catch things that others can avoid. A person in such a situation could contract something from a woman with leucorrhea. Many issues have stemmed from this condition, sometimes leading to unfair suspicions and causing significant distress.
Thus, then, we may have gleet from gonorrhœa, gleet from ulceration, gleet from stricture, gleet from debility and discharges, popularly understood to be gleet, but in[44] reality glandular secretions, which will be considered shortly and separately. Gleet is a tiresome and troublesome disorder. So difficult, occasionally, is its management, that oftentimes the more regularly a patient lives, and the more strictly he conforms to medical regimen, the more deceptive is his disorder. He will apparently be fast approaching to, as he conceives, a recovery, when, without “rhyme or reason,” the complaint recurs, and hints that his past forbearance has been thrown away. It would be dispiriting, indeed, were every case of gleet to realize this description; but it is well known that many do, either from neglect or mismanagement. Now it must be evident that the treatment of gleet depends upon what may happen to be the occasion of it. Where the membrane of the urethra is entire, internal remedies may, and do avail. Copaiba will achieve wonders; the use also of a mild injection, perseveringly employed (as a solution of iodide of iron, or citrate of iron, ten grains to the ounce of water), will give tone and stringency to the weakened vessels, and so correct the quantity, at least, of the secretion. In very obstinate cases, stronger injections, as of the nitrate of silver, twenty grains to the ounce of water, are serviceable; and we are not without many useful internal medical combinations, which, properly administered, conquer this troublesome complaint. In ulceration and stricture, these two causes must be removed, else all efforts are unavailing. In general and local debility, the attention must be devoted to the constitution. Common sense and common reading must give to persons, possessing both, every necessary information. The community are beginning to appreciate the advantages of temperance, air, and exercise, too highly, to need instructions how much of the one or either of the other two are essential to the preservation or recovery of health.
So, we can have discharge from gonorrhea, discharge from ulceration, discharge from stricture, discharge from weakness and discharges, often understood as discharge, but in[44] reality, glandular secretions, which will be discussed shortly and separately. Discharge is a bothersome and annoying disorder. Its management can be so challenging that sometimes the more carefully a patient follows instructions and adheres to medical advice, the more misleading their condition becomes. They might seem to be getting closer to what they think is recovery, only for the issue to unexpectedly return, suggesting that their previous patience was wasted. It would be discouraging if every case of discharge fit this description; however, it’s well known that many do, either due to neglect or poor management. Now, it’s clear that the treatment for discharge depends on the underlying cause. When the membrane of the urethra is intact, internal treatments can be effective. Copaiba can work wonders; using a mild injection consistently (like a solution of iodide of iron or citrate of iron, ten grains to an ounce of water) will help tone and tighten the weakened vessels, thus at least regulating the amount of secretion. In very stubborn cases, stronger injections, such as a nitrate of silver solution with twenty grains to an ounce of water, can be helpful; and we have many effective internal medical combinations that, when properly used, can overcome this troublesome issue. In cases of ulceration and stricture, those two factors must be addressed; otherwise, all efforts will be futile. In general and local weakness, attention should focus on overall health. Common sense and basic knowledge will provide individuals with all the necessary information. People are beginning to recognize the benefits of moderation, fresh air, and exercise enough that they don’t need guidance on how much of each is vital for maintaining or regaining health.
Morbid Irritability of the Urethra.—Of the varied symptomatic sensations, few are more provoking and fretting than some continued troublesome itching or pain that frequently attends the passing of water. There may be no discharge of any kind, but there is either a constant tingling, partially pleasurable sensation, drawing the attention perpetually to the urethra, or there is felt some particular heat or pain during the act of micturition. These feelings do not always indicate a venereal affection; they appear to depend upon local irritation, perhaps induced by a[45] morbid condition of the urine. The treatment consists in temperate diet, moderatively laxative medicines, and now and then local applications. Some cases yield to sedatives topically applied, and alkalies given internally, while others need local stimulants and specific tonics. At all events, whenever there is an unhealthy feeling in those parts, it points out some altered action is going on, which, if not arrested, is likely to end in stricture or gleet, and therefore attention had better be bestowed upon it as soon as possible.
Morbid Irritability of the Urethra.—Among the various uncomfortable sensations, few are more annoying and frustrating than persistent itching or pain that often comes with urination. There might not be any discharge, but there is either a constant tingling sensation that draws attention to the urethra or a specific heat or pain during urination. These sensations do not always indicate a sexually transmitted infection; they seem to result from local irritation, possibly caused by a[45] unhealthy condition of the urine. Treatment includes a moderate diet, moderately laxative medications, and occasional local treatments. Some cases respond to sedatives applied topically and alkalies taken internally, while others require local stimulants and specific tonics. In any case, if there is an unhealthy feeling in that area, it indicates that some abnormal process is taking place, which, if not addressed, could lead to stricture or gleet, so it's best to pay attention to it as soon as possible.
On Stricture of the Urethra.—Of all diseases of the genito-urinary system, stricture must be allowed to be the most formidable. It is not the most difficult to cure; but it involves, when neglected, more serious disturbances—disturbances which frequently compromise only with loss of life. Stricture is a disease unfortunately of extensive prevalence; and in nine cases out of ten is the sequence of a gonorrhœa; and, what is still more comforting, few persons who become the prey to the latter infliction escape scot-free from the former; not because a clap must necessarily be succeeded by a stricture, but simply because it is, and all owing to the carelessness and inattention manifested by most young men in the observances so necessary for the perfect cure of the primary disease. One very prevalent notion, and which explains a principal cause of the extension of the venereal disease, is entertained, that the way to give the finishing coup to an expiring clap, is to repeat the act that gave rise to it: the disease becomes temporarily aggravated, and the impatient invalid probably flies, from an unwillingness to confess his new error, from his own tried medical friend to some professional stranger. From a desire to earn fame as well as profit, the newly consulted prescribes some more powerful means; the discharge is arrested for a while, but returns after the next sexual intercourse; a strong injection subdues the recurrent symptom, which only awaits a fresh excitement for its reappearance. Thus a gleet is established. The patient finding little or no inconvenience from the slight oozing, which, as he observes, is sometimes better and occasionally worse, according to his mode of living, determines to let nature achieve her own cure, and for months he drags with him a distemper that, despite all his philosophy, he can not reflect on without an humiliating diminution of self-approval. So insidiously, however, does the[46] complaint worm its progress, that the patient, considering his present state the worst that can befall him, resolves to endure it, since it appears his own constitutional powers are incapable of throwing it off.
On Stricture of the Urethra.—Of all diseases of the genito-urinary system, stricture is definitely the most serious. It's not the hardest to treat, but if left untreated, it can lead to much more serious issues—issues that can often result in death. Stricture sadly is quite common; in nine out of ten cases, it follows a gonorrhea infection. What's even more concerning is that few people who suffer from gonorrhea manage to avoid stricture; not because a gonorrhea infection has to lead to stricture, but simply because it does, primarily due to the negligence and lack of proper care exhibited by most young men in the necessary steps for fully curing the initial disease. One widely held belief, which explains a major reason for the spread of venereal disease, is that to completely finish off a gonorrhea infection, you should engage in the act that caused it. This leads to a temporary worsening of the condition, and the frustrated patient, not wanting to admit to a new mistake, often seeks help from an unfamiliar professional instead of their trusted medical friend. Eager to gain both recognition and financial reward, the new doctor prescribes more potent treatments; the discharge might stop for a bit, but it comes back after the next sexual encounter. A strong injection suppresses the recurring symptoms, which only wait for another trigger to reappear. In this way, a persistent discharge, or gleet, is created. The patient, noticing little to no trouble from the slight dripping—which he finds varies based on his lifestyle—decides to let nature take its course. For months, he carries a condition that, despite his attempts to rationalize, makes him feel humiliated. So insidiously does the[46] complaint progress that the patient thinks his current situation is the worst it can get and resolves to endure it, believing that his body simply can't shake it off.
In the midst of this contentment, the invalid finds that the process of urinating engages more time than formerly, the urine appears to flow in a smaller stream, and is accompanied by a sensation as though there were some pressure “behind it.” The act of making water is not performed so cleanly as it used to be; the stream differs in its flow, seldom coming out full and free, but generally split into three or four fountain-like spirts, as the annexed drawing displays.
In the midst of this contentment, the person with the illness notices that urinating takes longer than it used to, the urine flows in a smaller stream, and there's a feeling as if there's pressure "behind it." The act of urinating isn't as clean as it once was; the stream varies in its flow, rarely coming out strong and steady, but usually breaks into three or four fountain-like spurts, as shown in the attached drawing.
At other times it twists into a spiral form, and then suddenly splits into two or more streams, while at the same moment the urine drops over the person or clothes, unless great care be observed, as witness diagram.
At other times it twists into a spiral shape, and then suddenly splits into two or more streams, while at the same moment the urine drips onto the person or clothes, unless great care is taken, as shown in the diagram.
In advanced cases, the urethra becoming so narrow the bladder has not power to expel the urine forward, and it then falls upon the shoes or trowsers, or between them, as observe illustration.
In advanced cases, the urethra becomes so narrow that the bladder lacks the ability to push the urine out, and it then dribbles onto the shoes or pants, or between them, as shown in the illustration.



Persons afflicted with stricture, and urinating in the streets, may almost be detected from the singular attitude they are obliged to assume to prevent the urine from inconveniencing them, and also from the time occupied in discharging it. Some few minutes after making water, when dressed and proceeding on his way, the patient finds his shirt become moist by some drops of urine that continue to ooze from the penis; and it is only as these annoyances accumulate, he begins to think he is laboring under some other disease than the gleet. The next symptom he will experience will be a positive but temporary difficulty in passing his water—perhaps a total inability to do so; it will, however, subside in a few minutes. This will lead him to reflect, and[47] he will even appease his fears by inclining to think it may be the consequence of his last night’s excess: he resolves to be more careful for the future, and he gets better; his contemplated visit to his usual professional adviser, if he have one, is postponed, and a few more weeks go by without a return of the last symptom. The next attack, which it is very difficult to avert, and which is sure to accompany the succeeding debauch, or to follow a cold or fatigue, does not so speedily subside; the patient finds that he can not complete the act of making water without several interruptions, and each attended with a painful desire resembling that induced by too long a retention of that fluid. In that state he eagerly seeks medical assistance; the treatment generally adopted consisting of some sedative, immersion in a hot bath, or the passage of a bougie. Relief being thus easily obtained, professional advice is thus thrown up, and the symptoms are again soon forgotten. Before proceeding further with the more severe forms and consequences of stricture, which may now be fairly said to have commenced in earnest, a brief anatomical description of the urethra may enable the reader to understand how the constriction or narrowing of that canal takes place.
People dealing with a stricture who urinate in public can often be recognized by the awkward position they have to adopt to avoid discomfort, as well as the length of time it takes them to relieve themselves. A few minutes after urinating, once they’re dressed and on their way, the patient may find their shirt damp from drops of urine that continue to leak from the penis. Only as these annoyances build up do they start to think they might be suffering from something other than a discharge. The next symptom they will notice is a clear but temporary difficulty in urinating—possibly even an inability to do so; however, this will ease after a few minutes. This leads them to contemplate the situation, and they might even calm their fears by considering that it could be due to last night’s drinking. They decide to be more cautious moving forward, and they begin to feel better; the planned visit to their usual doctor, if they have one, gets delayed, and weeks pass without the return of the last symptom. The next episode, which is hard to prevent and will certainly happen after another binge or due to a cold or fatigue, doesn’t go away as quickly; the patient finds they cannot finish urination without several interruptions, each accompanied by a painful urge similar to that felt during prolonged retention of urine. In this condition, they eagerly seek medical help; the common treatment involves some sedatives, a hot bath, or the use of a catheter. Since relief is easily achieved, they often abandon professional guidance, and the symptoms are soon forgotten. Before delving deeper into the more serious forms and repercussions of stricture, which can now be said to have truly begun, a brief anatomical overview of the urethra will help the reader understand how the narrowing of this canal occurs.
I have elsewhere stated the urethra to be a membranous canal, running from the orifice of the penis to the bladder, and situated in the lower groove formed by the corpus spongiosum.
I have mentioned before that the urethra is a membranous tube that runs from the opening of the penis to the bladder and is located in the lower groove created by the corpus spongiosum.
The difference of opinion entertained by some of our first anatomists, on the structure of the urethra, is deserving of notice; for only in proportion to the correctness of our knowledge of it, can we arrive at a just definition of its diseases.
The disagreement among some of our earliest anatomists regarding the structure of the urethra is worth mentioning; because only to the extent that we accurately understand it can we reach a proper definition of its diseases.
One party assert it to be an elastic canal—whether membranous or muscular they do not say—endowed with similar properties of elasticity to India rubber, or to a common spring. That it is elastic, is beyond doubt; but the mere assertion is no explanation of its mode of action.
One side claims it’s an elastic tube—whether it’s made of membrane or muscle, they don’t specify—possessing similar elastic qualities to rubber or a typical spring. That it is elastic is definitely true; however, just stating that doesn’t explain how it works.
Others, from microscopical observations, declare it to consist of two coats—a fine internal membrane, which, when the urethra is collapsed, lies in longitudinal folds—and an external muscular one, composed of very short fasciculi of longitudinal fibres, interwoven together, and connected by their origins and insertions with each other,[48] and united by an elastic substance of the consistence of mucus. This is the more satisfactory of the two.
Others, based on microscopic observations, claim it has two layers—a thin inner membrane that, when the urethra is collapsed, folds lengthwise—and an outer muscular layer made up of very short bundles of longitudinal fibers that are interwoven and connected at their beginnings and ends, [48] and joined by an elastic substance with a slimy consistency. This is the more convincing of the two.
They account for the occurrence of stricture in this way. They say that “a permanent stricture is that contraction of the canal which takes place in consequence of coagulable lymph being exuded between the fasciculi of muscular fibres and the internal membrane, in different quantities, according to circumstances.”
They explain the occurrence of stricture like this. They say that “a permanent stricture is the narrowing of the canal that happens because coagulable lymph seeps between the fasciculi of muscle fibers and the internal membrane, in varying amounts depending on the situation.”
A spasmodic stricture they define to be “a contraction of a small portion of longitudinal muscular fibres, while the rest are relaxed; and as this may take place, either all round, or upon any side, it explains what is met with in practice—the marked impression of a stricture sometimes a circular depression upon the bougie, at others only on one side.”
A spasmodic stricture is defined as “a contraction of a small area of longitudinal muscle fibers while the rest are relaxed. Since this can happen all around or on one side, it explains what is encountered in practice—the noticeable mark of a stricture sometimes shows as a circular indentation on the bougie, and at other times only on one side.”
With respect to the change consequent upon permanent stricture, dissection enables us, in some degree, to arrive at the truth. Excrescences and tubercles have been found growing from the wall of the urethra; but in the majority of instances, the only perceptible change is a thickening of the canal here and there, of indefinite length; but whether it be occasioned by the exudation of coagulable lymph, or whether it be the adhesion of ulcerated surfaces, which I contend are more or less present in gleet, is not so easy to determine; at all events, it is undoubtedly the result of inflammation.
With regard to the changes caused by permanent stricture, dissection allows us to get closer to the truth. Growths and lumps have been discovered on the wall of the urethra; however, in most cases, the only noticeable change is a thickening of the canal at various points, of unclear length. It's not easy to determine whether this is caused by the outpouring of clotted lymph or by the sticking together of ulcerated surfaces, which I argue are often present in gleet. Regardless, it is certainly a result of inflammation.
With regard to the action of spasm, all we know of it is theoretical; but experience every day furnishes instances of its occurrence.
With respect to the action of spasm, all we know about it is theoretical; however, our daily experiences provide examples of its occurrence.
Spasmodic stricture is generally seated at the neck of the bladder, and may occur to persons in good health, from exposure to wet or cold; from some digestive derangement; from long retention of the urine, particularly while walking, owing to the absence of public urinals; or to violent horse exercise; but more frequently does it happen to those young men who, when suffering from gleet or gonorrhœa, imperfectly or only partially cured, are tempted to commit an excess in wine, spirits, or other strong drinks. Surrounded by jovial society, glassful after glassful is swallowed, each one to be the last. The patient, with his bladder full to repletion, scarcely able to retain his water, yet probably “going” every moment, represses his desire until the party breaks up, when, on encountering the cold air, he finds himself unable to void[49] even a drop, or if so, but with extreme difficulty. The greater the effort, and the more determined the straining, the greater is the impossibility, and unless relief should be afforded, the most alarming consequences may ensue.
Spasmodic stricture usually occurs at the neck of the bladder and can affect healthy individuals due to exposure to wet or cold conditions, digestive issues, prolonged urine retention—especially while walking because of the lack of public restrooms—or intense horse riding. However, it is more common in young men who, when dealing with lingering effects of conditions like gleet or gonorrhea that are not fully treated, are tempted to indulge excessively in wine, spirits, or other strong drinks. In lively company, they drink glass after glass, each promising it will be the last. The person, with a painfully full bladder, struggles to hold in their urine, often feeling the urge to go every moment, until the gathering ends. When they step into the cold air, they find it nearly impossible to relieve themselves, and if they do manage to, it's with severe difficulty. The more they try and strain, the harder it becomes, and unless they find relief, serious complications may arise.[49]
The rationale is this: the patient, opposing the action of the muscles of the bladder, by contracting those of the urethra, they (the latter), from irritation, become spasmodically contracted.
The reasoning is this: the patient, by contracting the muscles of the urethra against the action of the bladder muscles, causes the urethral muscles to become spasmodically contracted due to irritation.
The urine, by the powerful action of the muscles of the bladder, is forced against the contracted portion of the urethra; and by its irritation increases the mischief. Where neglected, or unless the spasms yield, extravasation will take place, mortification ensue, and death follow.
The urine, through the strong contractions of the bladder muscles, pushes against the tightened section of the urethra; and this irritation worsens the problem. If left untreated, or unless the spasms subside, leakage will occur, leading to tissue death and ultimately death.
The urethra is situated at the under part of the penis, and is embraced by a substance called the corpus spongiosum; it (the urethra) consists of several different layers or coats—the inner, the one continuous with that lining the bladder, which possesses the power of secreting a mucous fluid, and the other made up of muscular fibres, which give to the urethra the power of contracting and dilating, that regulates the flowing or jetting of the fluid which has to pass through it. The mucous membrane of the urethra is of a highly sensitive nature, and more so in some parts than in others, as, for instance, in the membranous and bulbous portion of the canal; and hence it will be found, that those are the parts most liable to disease. The mucous membrane has several openings called lacunæ, for the furnishing a particular fluid to moisten and lubricate the urinary tube: these also are frequently the seat of disease. These are seen in the drawing on page 50.
The urethra is located underneath the penis and is surrounded by a tissue called the corpus spongiosum. It (the urethra) has several different layers or coats—the inner layer, which is continuous with the lining of the bladder, has the ability to secrete a mucous fluid, and the outer layer is made up of muscle fibers that allow the urethra to contract and expand, controlling the flow or spray of the fluid that passes through it. The mucous membrane of the urethra is highly sensitive, with some areas being more sensitive than others, such as the membranous and bulbous sections of the canal; this makes these areas more prone to disease. The mucous membrane has several openings called lacunæ, which provide a specific fluid to moisten and lubricate the urinary tube; these openings are also often sites of disease. These can be seen in the drawing on page 50.
In passing a bougie in contracted and irritable urethra, it sometimes enters the opening marked B, and if violence be used in propelling the instrument, false passages are made.
Inserting a bougie into a narrowed and sensitive urethra can sometimes lead it to enter the opening labeled B, and if force is used to push the instrument, false passages can occur.
Independently of the function of the urethra being to discharge the urine, it has also to convey the semen to the orifice of the glans; and here in this act is to be observed the wonderful adaptation of means to an end. During the excitement attendant upon venereal commerce, the seminal fluid accumulates, prior to emission, in the bulbous portion, and when the fitting moment arrives for its ejection, the membranous portion spasmodically contracts, thereby preventing the regurgitation of the semen into the [50] bladder, while the muscles surrounding the bulbous portion contract with energetic force, and so complete the transmission of the generative fluid. Such are the functions of the urethra in health.
Regardless of the urethra's primary role in expelling urine, it also serves to carry semen to the opening of the glans. This process showcases the remarkable alignment of methods with purpose. During the arousal associated with sexual activity, semen builds up in the bulbous part of the urethra, and when the moment is right for ejaculation, the membranous part contracts spasmodically. This contraction prevents semen from flowing back into the bladder, while the muscles around the bulbous section vigorously contract to ensure the successful release of the reproductive fluid. These are the functions of the urethra when it's functioning properly.

|
A—Signifying the urethra cut open. A—Indicating the urethra incision.
B—The lacunæ and the cut end of bougie, to show the continuation of the urethra. B—The gaps and the cut end of the bougie, to indicate the continuation of the urethra. |
Now, this canal being extensively supplied with nerves, that have more extensive communication with others than any particular ones have in the whole body, and made up, as before stated, of surficial and muscular membranes, and exposed to the performance of several duties which are often unduly called into exercise, can not be supposed to be exempt from the consequences of such misappropriation; and therefore it is very liable to inflammation. From the sensitive nature of the tube, it is very obnoxious to spasm, which may be partial, general, temporary, or continuous: hence spasmodic stricture. This condition is of course dependent upon many causes, excess of diet, fatigue, cold, &c., irritating the general system; when from the local irritation previously set up in the urethra by the forenamed causes—a neglected gleet or clap—the urethra is not long in participating in it: the phenomena are the symptoms recently narrated. Highly restorative as the powers of nature may be to remove disease, she does not appear readily disposed[51] to interfere with the processes set up in the machine she inhabits, for self-defence, to protect itself from the constant irritation produced by the daily flow of acrid urine, which in several cases often produces ulceration; coagulable lymph is thrown out in the cellular structure of the particular diseased part, thereby thickening the walls thereof, and constituting permanent stricture, it appearing preferable to impede a function which a narrowing of the urethric canal does, namely, that of urinating, than of allowing ulceration to ensue, whereby the urine would escape into the neighboring parts, and occasion great devastation, and probably death. Permanent stricture, as its name implies, outlives the patient; it never yields, unassisted by art. I have described the ordinary symptoms of stricture, especially that form induced by gonorrhœa. Stricture may arise from other causes. Inflammation, in whatever way set up, if allowed to go on or remain, will give rise to stricture, and the celerity or tardiness with which it takes place depends upon circumstance. An injury from falling astride any hard substance, blows, wounds, contusions occasioned by riding, the presence of foreign substances, the injudicious use of injections, and lastly, which is as frequent a cause as any one of those heretofore enumerated, masturbation. The violent manual efforts made by a young sensualist to procure the sexual orgasm for the third or fourth time continuously, I have known to be of that degree that irritation has been communicated to the whole length of the urethra, extending even to the bladder; and retention of urine, in the instance I allude to, ensued, and required much attention before it could be subdued. Excessive intercourse with females will give rise to the same effects; not so likely as in the case preceding, inasmuch as the former can be practised whenever desired, while the latter needs a participator. The act of masturbation repeated, as it is, by many youths and others, day after day, and frequently several times within each twenty-four hours, must necessarily establish a sensitiveness or irritability in the parts, and alteration of structure is sure to follow.
Now, this canal is heavily supplied with nerves that have more extensive connections with others than any specific ones throughout the body. It's made up of surface and muscle membranes and is often pushed to perform various duties that can unnecessarily be called into action. So, it’s very likely to experience inflammation. Due to the sensitive nature of the tube, it is also prone to spasms, which can be partial, general, temporary, or continuous—leading to spasmodic stricture. This condition depends on many factors like overeating, fatigue, cold, etc., which irritate the overall system. When local irritation is triggered in the urethra by these causes—such as a neglected discharge or infection—the urethra quickly gets involved: the symptoms have been recently described. While nature has great powers to heal, it doesn’t readily intervene in the processes set in motion to defend itself against the constant irritation from the daily flow of acidic urine, which can sometimes lead to ulceration. Coagulable lymph is generated in the affected area, thickening the walls and creating a permanent stricture. It seems better to hinder a function like urination caused by a narrowed urethra than to allow ulceration, which could let urine escape into surrounding areas, causing severe damage and possibly death. Permanent stricture, as the name suggests, outlives the patient; it never yields, unassisted by medical intervention. I’ve listed the typical symptoms of stricture, especially those caused by gonorrhea. Stricture can come from other sources too. Inflammation, no matter how it starts, if left unchecked, will lead to stricture, and how quickly it occurs depends on circumstances. An injury from falling onto something hard, blows, wounds, or impact from riding, presence of foreign materials, improper use of treatments, and lastly, a common cause among those listed is masturbation. The intense manual efforts of a young person trying to achieve orgasm repeatedly can cause irritation throughout the entire urethra, even reaching the bladder, leading to urinary retention that requires significant attention to resolve. Excessive sexual activity with women can produce similar effects, but it’s less likely than in the previous case, as the former can happen anytime while the latter requires a partner. The act of masturbation, often repeated by many young people multiple times each day, inevitably creates sensitivity or irritability in the areas involved, and structural changes are sure to follow.
The positive changes which take place in stricture in the urethral passage are these: there ensues a thickening and condensation of the delicate membrane and the cellular tissue underneath, which may possibly unite it to the muscular coat. This thickening or condensation is the[52] result of what we call effusion of coagulable lymph. It will be rather difficult to explain the process; but lymph is that fluid understood to be the nutritious portion of our sustenance or system, and which is here yielded up by the vessels which absorb it, and which vessels abound, with few exceptions, in every tissue of our body. However, it will suffice to say, that where inflammation takes place, there is an alteration of structure, and that alteration is generally an increase. In stricture, this increase or thickening takes place, as I observed before, in particular parts of the urethra, but where the inflammation is severe, no part is exempt, and whole lengths of the passage become occasionally involved. It is true, certain parts are more predisposed than others, as, for instance, the membranous, bulbous, and prostatic portions of the canal; but there are oftentimes cases to be met with where these parts are free, and the remainder blocked up. This effusion or thickening assumes various shapes, and selects various parts of the urethra. The subjoined diagram will convey a tolerably perfect idea of the malady in question; indeed it is a beautiful specimen of simple stricture.
The positive changes that occur in the urethral passage with stricture are these: there’s a thickening and hardening of the delicate membrane and the cellular tissue beneath it, which may even fuse with the muscular layer. This thickening or hardening is the[52] result of what we refer to as the effusion of coagulable lymph. It’s a bit tricky to explain the process, but lymph is the fluid regarded as the nutritious component of our sustenance or body, and it’s released by the vessels that absorb it, which are present in almost every tissue of our body. Nonetheless, it’s enough to say that where inflammation occurs, there’s a change in structure, and that change usually involves an increase. In stricture, this increase or thickening happens, as I mentioned before, in specific parts of the urethra, but when the inflammation is severe, no area is immune, and entire sections of the passage can be affected. It’s true that certain areas are more prone to this, such as the membranous, bulbous, and prostatic parts of the canal, but there are often cases where these areas are unaffected and the rest are blocked. This effusion or thickening takes on various forms and targets different parts of the urethra. The diagram below will give a reasonably clear idea of the condition in question; it’s actually a striking example of simple stricture.

|
A—The cut edges of the corpus spongiosum. A—The cut edges of the spongy tissue.
B—The urethra. B—The urethra.
C—The stricture. C—The limitation. |
To continue the description of the formidable consequences of neglected stricture.
To keep describing the serious consequences of ignored stricture.
In protracted and neglected cases, that part of the urethra[53] between the stricture and bladder becomes dilated, from the frequent pressure of the urine upon it, induced by irritability of the bladder, which has an increasing desire to empty itself. In process of time, complete retention of urine will ensue, ulceration will take place at the irritable spot, and effusion of urine into the surrounding parts will follow; and the consequences will be, as in the instance of the spasmodic affection, fatal, unless controlled by the skilful interference of the surgeon.
In long-term and neglected cases, the section of the urethra[53] between the stricture and the bladder expands due to the constant pressure of urine, caused by the bladder's increased urge to empty itself. Over time, complete urinary retention will occur, leading to ulceration at the irritated site, and urine will leak into the surrounding areas; the results will be, similar to the case of the spasmodic condition, fatal, unless properly addressed by a skilled surgeon.
The symptoms of permanent stricture are often as slow in their progress, and as insidious in their nature, as they are appalling in their results, and are seldom distinctly observed by the patient, until firmly established.
The symptoms of permanent stricture often develop slowly and insidiously, as well as being alarming in their consequences, and are rarely clearly noticed by the patient until they are firmly established.
He is suffering from a long-continued gleet, and is first alarmed by a partial retention of urine—it passes by drops, or by great straining, or not at all. This usually occurs after intemperance, and is relieved by the warm bath, fomentations, and laxative medicines. This is the first stage, and is attributed to the debauch solely; whereas, at this time an alteration of structure is going on in the urethra. Its calibre is becoming diminished, which necessarily causes the urine to flow in a smaller stream. This is not observed at first; and it is only after a long period that the patient becomes aware of the fact.
He has been dealing with a long-lasting discharge, and becomes worried when he starts having trouble urinating—it's either a trickle, requires a lot of effort, or doesn’t happen at all. This usually follows excessive drinking and is eased by warm baths, compresses, and laxatives. This is the initial stage, which is blamed only on the partying; however, at the same time, changes are happening in the urethra. Its diameter is shrinking, which naturally results in a weaker stream of urine. This isn’t noticed right away, and it takes a long time for the patient to realize it.
The disease proceeds. In the morning, from the gluing together of the sides of the urethra, by the discharge from its diseased surface, the urine flows in a forked or double stream; and then, as this agglutinution is dissolved, it become natural.
The disease progresses. In the morning, due to the sticking together of the urethra's sides from the discharge coming from its affected surface, the urine flows in a forked or double stream; then, as this adhesion dissolves, it returns to normal.
There is a greater and more frequent desire to make water, disturbing sleep many times during the night, but unattended with pain, unless the neck of the bladder be affected.
There’s a stronger and more frequent need to urinate, which disrupts sleep many times throughout the night, but it's not accompanied by pain unless the bladder neck is affected.
There are also uneasy sensations in the perinœum, a sense of weight in the pelvis, with flying pains in the hips; and in the permanent stricture there is a remarkable symptom frequently prevailing—that is, a pain extending down the left thigh from the perinœum.
There are also uncomfortable feelings in the perineum, a sense of heaviness in the pelvis, along with sharp pains in the hips; and in the case of a lasting stricture, there is a notable symptom that often occurs—that is, pain radiating down the left thigh from the perineum.
As the disease advances, the urine flows in only a very small stream, or forked, twisted, double, or broken, or in drops; and the patient solicits the flow by pressing with his finger on the perinœum, and elongating the canal, somewhat after the manner in which a dairy-maid milks a cow.
As the disease progresses, the urine flows in a very small stream, or it comes out forked, twisted, double, or in drops; the patient tries to encourage the flow by pressing on the perineum and stretching the canal, similar to how a dairy maid milks a cow.
The dilatation of the urethra between the stricture and the bladder already alluded to, now takes place; and some urine remains in the dilated part, which oozes through the stricture, making the patient wet and uncomfortable.
The widening of the urethra between the blockage and the bladder that was mentioned earlier is now happening; some urine is left in the expanded area, which leaks through the blockage, making the patient feel wet and uncomfortable.
There is great difficulty felt, and more time is occupied in getting rid of the last drop of water, than formerly. This sensation continues all along; and the cure is never accomplished until this is finally removed.
There is a significant struggle, and it takes more time to get rid of the last drop of water than before. This feeling persists throughout, and the treatment is never considered complete until this is finally taken care of.
If the stricture is still neglected, more severe symptoms come on, and the neighboring parts become affected also.
If the issue is still ignored, more serious symptoms emerge, and the surrounding areas get affected too.
The sphincter ani, or the muscles of the anus, are relaxed, from the excessive action of the abdominal muscles; and the fæces pass in small quantities involuntarily. There is a protrusion of the bowel, which adds to the distress, and, by its irritation, brings on a looseness or diarrhœa.
The sphincter ani, or the muscles around the anus, are relaxed due to the excessive action of the abdominal muscles, causing small amounts of stool to pass involuntarily. There's a bulging of the bowel, which increases discomfort and, through its irritation, leads to looseness or diarrhea.
The prostate gland, which is seated near the neck of the bladder, suffers inflammation and enlarges, beginning at the orifice of the ducts, which open into the urethra.
The prostate gland, located near the neck of the bladder, becomes inflamed and enlarges, starting at the opening of the ducts that lead into the urethra.
The emission of semen, which often happens involuntarily, is attended with agonizing pain, producing cold shiverings, followed by heat; and fever soon becomes fairly established.
The release of semen, which often occurs involuntarily, comes with excruciating pain, causing chills that are then followed by feverish heat, and soon a fever becomes quite pronounced.
The liver and its secretions become diseased, discharging in the intestines large quantities of vitiated bile. The fever assumes the intermittent character. The discharge from the urethra is greatly increased in quantity, showing the formation and bursting of an abscess of the prostrate gland into it.
The liver and its secretions become unhealthy, releasing large amounts of contaminated bile into the intestines. The fever has an intermittent pattern. The discharge from the urethra significantly increases, indicating the formation and rupture of an abscess in the prostate gland.
The bladder is much thickened and diminished in size, and acutely or chronically inflamed. The desire to make water is continual, allowing hardly a moment of rest; and the patient, in the agony of despair, prays to be relieved from his sufferings.
The bladder is significantly thickened and smaller than normal, and is either intensely or chronically inflamed. The urge to urinate is constant, leaving hardly any time for relief; and the patient, in deep despair, prays for relief from their suffering.
Soon succeeding the irritation of the prostate, the testicles become involved, the disease being propagated by means of their ducts, which open into the urethra. The testicles swell a little, become uneasy and painful, and a dropsical or hardened enlargement ensues.
Soon after the irritation of the prostate, the testicles become affected, with the disease spreading through their ducts, which connect to the urethra. The testicles swell slightly, become uncomfortable and painful, and a fluid-filled or hardened enlargement occurs.
The scrotum and neighboring parts become distended, erysipelas supervenes, black patches of mortification break out in different places, the febrile symptoms are augmented, and the patient at last irrecoverably sinks into a state of coma or muttering delirium, and death closes the scene. Such is the progress and termination of stricture when neglected.
The scrotum and surrounding areas become swollen, erysipelas sets in, black spots of tissue death appear in various locations, the fever symptoms worsen, and the patient ultimately falls into an irreversible state of coma or incoherent delirium, leading to death. This is the progression and outcome of stricture when left untreated.
The reader, if he be an afflicted one, will eagerly turn to the page wherein the treatment of this formidable and distressing malady is considered; and great will be his satisfaction and delight, on finding it remediable by such simple means, and entirely within his own control; more especially if he direct his attention to the disease in its earlier stages.
The reader, if they are struggling, will eagerly turn to the page where the treatment of this serious and troubling condition is discussed; and they will be very satisfied and pleased to find that it can be treated with such simple methods, all of which are completely within their control, especially if they focus on the disease in its early stages.
He must by no means, however, be too sanguine, from these remarks, or indulge in the idea that as stricture is remediable, it is unimportant when the cure be attempted; the longer the delay, the greater will be the cost to the patient; and, furthermore, the slightest deviation from the instructions laid down, will surely aggravate the disease, and increase the embarrassment of the sufferer.
He should not be overly optimistic based on these comments, nor should he think that, since stricture can be treated, it doesn’t matter when the treatment begins. The longer the wait, the higher the cost to the patient; additionally, even a small deviation from the provided instructions will definitely worsen the condition and increase the patient’s distress.
The following diagrams are further explanatory of the stricture in its amplified forms.
The following diagrams provide additional explanations of the stricture in its expanded forms.

The dark marginal line denote the calibre of the urethra, and the inner lines the actual diameter of the obstructed passage. Figure 1 shows the stricture to be on the lower part of the urethra. Figure 2 the upper part. Figure 3 exhibits a stricture of some length, and a somewhat contracted state of the whole canal. Figure 4 denotes a very common form of stricture, which resembles a flour-bag tied in the middle; it is the least difficult to cure of any, because it signifies that the seat of irritation is limited; but these cases are generally precursory to severer forms, if not promptly attended to. Figure 5 represents a stricture of considerable length, and of course very difficult of removal.
The dark outer line shows the size of the urethra, and the inner lines indicate the actual width of the blocked area. Figure 1 illustrates that the stricture is located in the lower part of the urethra. Figure 2 shows the upper part. Figure 3 displays a longer stricture and a somewhat narrowed condition of the entire canal. Figure 4 represents a very common type of stricture, which looks like a flour bag tied in the middle; it is the easiest to treat because it means the area causing irritation is limited. However, these cases often lead to more severe forms if not addressed quickly. Figure 5 depicts a stricture of significant length, making it very challenging to remove.
There are many provocatives to stricture, and when once mischief is progressing, it makes up for its slow initiation by giant strides. A patient may have a trifling stricture for years without experiencing much inconvenience. He takes cold, fatigues himself, commits some stomachic or other excess, may possibly have fever, all of[56] which more or less disturb the general economy, alter the character of the urine, and in that manner doubly accelerate the disorganization going on in the urethra. A small abscess may spring up in the urethra, or below it among the cellular membranes and integuments. In either case, it chances now and then to burst an opening and create a communication externally with the urinary passage, constituting what is called fistula. A person laboring under stricture is always liable to these occurrences. As much mischief is done oftentimes by mismanagement as by neglect. The clumsy introduction of a bougie, or, in other instances, the unjustifiable introduction of one, is likely to, and very frequently does, lacerate the delicate and irritable membrane, and make a false[57] passage. Figure 6 exhibits an instance at Nos. 1 and 2; the upper numerical shows a false passage made by a bougie, and an obliteration of the ordinary passage of the urethra, the result of inflammation, constituting an impassable stricture; the lower figure exhibits a false opening made, in the first instance, by a fruitless effort at passing an instrument, when inflammation completed the process. No urine escaped from it of course, because communication was cut off from the bladder by the impassable stricture; the outlet for the discharge of that fluid being through a sinuous opening marked No. 2, the No. 3 denoting the closed end of the urethra. The case happened to a man in very ill health, who was prone to ulceration, and he gradually sunk under exhaustion from debility and premature old age. Figure 7 exhibits a stricture where the posterior part was enlarged by the constant pressure of the urine to escape through the narrowed part of the urethra; ulceration ensued, and a fistulous opening was the consequence; the stricture was seated high up, and the fistulous canal was several inches long, terminating in the upper and posterior part of the thigh; the urine used to dribble through it as well as through the urethra. The patient had been a seafaring man; he was in exhausted health from hot climates and intemperate living, and he died at last of consumption. I have the parts showing the stricture and the fistulous opening by me, in a state of good preservation. In Figure 8 is presented an illustration of extensive ulceration producing two fistulous openings; the state of the urethra was only discovered after death, the patient having concealed his infirmity for many years; he died suddenly from apoplexy, being found dead in his bed by the people of the house where he lodged. Figure 9 portrays irregular and extensive ulceration. The patient died from syphilis, having gonorrhœa at the same time. I have the preparation. Figure 10 shows an impervious urethra, and a fistulous opening through which the urine flowed. The urinary passage was blocked up within two inches from the orifice, and the length of the obstruction was perhaps a quarter of an inch. It was perforated successfully by the lanceted stilette, and the passage thereby rendered continuous; the catheter was worn for several days, and the false opening soon healed after a slight application or two of nitric acid. Numerous other illustrations[58] might have been given, but the preceding convey a passable notion of the simplest, and most confirmed, and most severe forms, of the malady in question.
There are many causes of stricture, and once serious damage starts, it quickly escalates despite its slow beginning. A patient might have a minor stricture for years without much trouble. They might catch a cold, overexert themselves, eat poorly, or possibly develop a fever, all of which can disturb their overall health, change their urine, and thereby speed up the damage happening in the urethra. A small abscess can form in the urethra or just below it in the surrounding tissues. In either case, it can sometimes burst and create an opening that connects externally with the urinary tract, resulting in what's called a fistula. A person with a stricture is always at risk of these issues. Often, as much harm comes from poor management as from neglect. Carelessly inserting a bougie, or even unjustifiably doing so, can tear the sensitive and irritated tissue, creating a false passage. Figure 6 shows an example at Nos. 1 and 2; the upper number indicates a false passage made by a bougie and a blockage of the normal urethra due to inflammation, resulting in an impassable stricture; the lower figure shows a false opening initially created by an unsuccessful attempt to insert an instrument, which inflammation then completed. No urine escaped from this opening, of course, because the connection to the bladder was blocked by the impassable stricture, with the discharge being allowed only through a winding opening marked No. 2, while No. 3 indicates the closed end of the urethra. This case involved a man in very poor health, who was prone to ulceration, and he gradually succumbed to exhaustion from weakness and premature aging. Figure 7 illustrates a stricture where the back part was enlarged due to constant pressure from urine trying to pass through the narrowed section of the urethra; ulceration followed, leading to a fistulous opening; the stricture was located high up, and the fistulous canal was several inches long, ending in the upper and back part of the thigh; urine dribbled through this as well as through the urethra. The patient had been a sailor; he was in poor health from hot climates and excessive drinking, and ultimately died from consumption. I have the affected parts showing the stricture and the fistulous opening, preserved well. Figure 8 presents a case of extensive ulceration resulting in two fistulous openings; the condition of the urethra was only discovered after the patient’s death, having hidden his illness for many years; he died suddenly from a stroke and was found dead in bed by his roommates. Figure 9 depicts irregular and extensive ulceration. The patient died from syphilis while also having gonorrhea at the same time. I have this preparation. Figure 10 shows an obstructed urethra and a fistulous opening through which urine flowed. The urinary passage was blocked within two inches from the opening, with the obstruction being about a quarter of an inch long. It was successfully punctured with a lanceted stiletto, restoring continuity, and a catheter was used for several days, with the false opening healing shortly after a couple of applications of nitric acid. Many other examples could have been given, but the previous ones provide a fair idea of the simplest, most common, and most severe forms of this condition.
It is melancholy, notwithstanding the resisting and reparative power of nature to avoid so saddening a disease as stricture, that it is so very prevalent, and that it is occasioned by so many causes. Where it is not destructive to life, it is very injurious. It involves, where it is severe, other important organs beside the seat of its abiding; the repeated calls upon the bladder, through sympathy of the irritation, created so near to that viscus, the efforts which at all times it is obliged to make, although assisted by the muscles of the abdomen and contiguous parts to void its contents, at last, and very frequently end in paralysis, and total inability to pass water ensues, except through the aid of the catheter. Independently of which, where so much disease exists as in the urethra, the urine also constantly pressing against ulcerating and irritable surfaces, extravasation of that secretion takes place, and the most formidable and alarming consequences ensue. In the simplest form of stricture, many important functions are disturbed. A very frequent consequence is permanent irritability of the bladder, so that the patient is obliged, ten or twelve times a day, to micturate, and is unable to pass through the night without suffering nearly the same inconvenience. Besides which, the natural sensitiveness of the genital organs becomes speedily and much impaired. I am satisfied that where disorganization of the testicles does not exist, and where the patient is young, or even middle-aged, if he be impotent, he will in nine cases out of ten be found to have stricture. There are exceptions, which shall be named when speaking on the infirmities of the genital system, but in nearly all cases of impuissance there will be found, if not stricture, at least some morbid irritability of the urethra. During the existence of stricture, there is generally a vitiated secretion from the seat of mischief, constituting a gleet; therefore a gleet at all times should be regarded, lest it be an indication of something more than a mere weeping from enfeebled vessels.
It’s sad, even with nature’s ability to heal, that such a distressing condition as stricture is so common and caused by so many factors. Where it doesn’t threaten life, it’s still very harmful. When severe, it affects other important organs in addition to the area of its origin; the repeated urges on the bladder, due to irritation from the nearby area, along with its continuous efforts to release its contents—though supported by abdominal muscles—often result in paralysis, leading to a complete inability to urinate without a catheter. Furthermore, when there’s so much illness in the urethra, constant pressure from urine against irritated and ulcerated surfaces can occur, leading to serious and alarming complications. Even in the simplest cases of stricture, many essential functions are disrupted. A common result is constant bladder irritability, forcing the patient to urinate ten to twelve times a day and making it difficult to get through the night without similar issues. Additionally, the natural sensitivity of the genital organs quickly diminishes. I am convinced that, unless there is damage to the testicles and if the patient is young or in middle age, impotence will often be associated with stricture in nine out of ten cases. There are exceptions, which will be discussed when addressing weaknesses in the genital system; however, in nearly all cases of impotence, if there isn't stricture, there is likely some abnormal irritation in the urethra. While stricture exists, there is usually an abnormal secretion from the affected area, resulting in a gleet; therefore, any gleet should always be taken seriously, as it might indicate more than just minor leaking from weakened vessels.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ———<>———
On the Treatment of Stricture.—Having fully described the symptoms and progress of stricture, I proceed to the more pleasing part of treatment. Stricture, if early attended to, is a disease easy remediable: if neglected, its[59] horrors accumulate, and sufferings the most acute close the scene. Such, however, is the progress of science, that it is almost possible to cure the most inveterate case, at all events to relieve it; but that is no reason why the initiatory notices should be disregarded. Stricture, as must be perceived, is of two kinds, spasmodic and permanent: the treatment of the first is chiefly medical, the treatment of the latter chiefly mechanical. The principal agents I rely upon in the cure of the former, are the warm bath, rest, sedatives, and certain dietetic restrictions; for the removal of the latter, I place unbounded confidence in the practice of dilatation; and I am of opinion that the other methods, namely, the application of caustic or the scalpel, might be dispensed with altogether, if the dilating method be not delayed too long.
On the Treatment of Stricture.—Having fully described the symptoms and progression of stricture, I now move on to the more pleasant part: treatment. Stricture, if addressed early, is a condition that can be easily treated; if ignored, its[59] horrors accumulate, leading to intense suffering. However, due to advancements in science, it is now almost possible to cure even the most stubborn cases, or at least provide relief. But that doesn’t mean we should ignore the initial signs. Stricture, as you may notice, comes in two forms: spasmodic and permanent. The treatment for the first is mostly medical, while the second is primarily mechanical. The main methods I depend on for treating the former are warm baths, rest, sedatives, and specific dietary restrictions. For the removal of the latter, I have complete confidence in the practice of dilatation; I believe that other methods, such as using caustic agents or surgery, could be entirely avoided if the dilating technique is not postponed too long.
Before commencing the cure of stricture, I need hardly observe, that we ought to be fully satisfied of its existence. Symptoms are not always unerring guides; and, therefore, our reliance should not wholly depend on them.
Before starting the treatment for stricture, I should hardly need to point out that we must be completely sure it exists. Symptoms aren’t always reliable indicators, so we shouldn’t rely solely on them.
The only mode of ascertaining the precise condition of the urethra, is by an examination of it, which should not be delayed a moment after suspicion is entertained of the impending evil.
The only way to accurately determine the state of the urethra is through an examination, which should be done immediately after any suspicion of a problem arises.
For this purpose, it is recommended that a solid silver sound should be used as the best instrument; because it will pass with much less pain or inconvenience. It should be made conical, that is, smaller at the point than at the shaft, and of a size to pass very readily into the orifice; the shaft or body of the sound should not exceed two thirds of the size of the canal. The sound should be warmed, and afterward it should be well oiled. The directions for examining the urethra pertain to the passage of a bougie or catheter; and as it often falls to the lot of a patient, that he is beyond medical assistance, it behooves him to learn how an instrument should be passed, in order that in emergencies he may officiate himself; besides, it often happens, in cases of diseased bladder, and in those cases where retention of urine frequently occurs, that an invalid can not command the necessary constant attendance of his professional man; and therefore such knowledge will well repay any little time or trouble bestowed in the acquisition. The two annexed drawings will render[60] the commonest observer a proficient. The first shows the manner in which the bougie is to be introduced. Where the instrument can be passed thus far, without the assistance of the other hand than that which holds the bougie, it is better, as it keeps the penis and the muscles which influence it in a passive state. When the instrument has passed as far as it will, in the direction the dotted lines denote, it is to be turned gently round, raising the handle toward the abdomen. A slight pressure is then to be made downward, and the handle of the catheter or bougie at the same time to be borne away from the body. See diagram. The instrument will, if there be no impediment, gradually slip into the bladder. A trial or two will perfect and surprise the novice. The same directions apply to the introduction and use of all other instruments into the urethra. The sensation experienced on having a bougie passed, partakes more of a strange tickling feeling than absolute pain, except there exist stricture, and even then the urethra, on a subsequent trial, is almost insensible to it.
For this purpose, it's recommended to use a solid silver sound as the best instrument because it will pass with much less pain or inconvenience. It should be conical, meaning it should be smaller at the tip than at the shaft, and sized to easily fit into the opening; the shaft or body of the sound should not be more than two-thirds the size of the canal. The sound should be warmed and then well oiled. The instructions for examining the urethra relate to the use of a bougie or catheter; since patients may sometimes be beyond medical assistance, it’s important for them to learn how to use an instrument themselves for emergencies. Additionally, in cases of bladder issues and frequent urine retention, a patient may not be able to get regular professional help; therefore, having this knowledge can be very valuable. The two drawings attached will help anyone understand. The first illustrates how to introduce the bougie. If the instrument can be passed this far without needing the other hand, aside from the one holding the bougie, it's better because it keeps the penis and the muscles that affect it relaxed. Once the instrument has been inserted as far as it can go in the direction indicated by the dotted lines, it should be gently turned, lifting the handle toward the abdomen. A slight downward pressure should be applied while the handle of the catheter or bougie is moved away from the body. See diagram. If there are no blockages, the instrument will gradually slide into the bladder. With a couple of tries, beginners will get the hang of it and be surprised by their progress. The same instructions apply to the use of all other instruments for the urethra. The sensation of having a bougie inserted feels more like a strange tickling than real pain, unless there is a stricture, but even then, the urethra becomes almost numb on subsequent attempts.


If soreness or pain is felt, on the sound passing over the affected part, we may presume there is chronic inflammation of the urethra, or that the surface is ulcerated, as in long standing gleet. If the sound meet with an impediment, but proceeds after a little pressure, it indicates a thickening of the mucous membrane, the forerunner of stricture.
If soreness or pain is experienced when the sound passes over the affected area, we can assume there is chronic inflammation of the urethra or that the surface is ulcerated, as seen in long-term gleet. If the sound encounters a blockage but continues after some pressure, it indicates thickening of the mucous membrane, which is a precursor to stricture.
If the sound passes, without hinderance, the last situation, but with increased pain, the membrane of that part is diseased, and may extend to the bladder; which will be indicated by the frequent desire to micturate during the night, owing to the irritable state of that organ.
If the sound passes through without any issues, but with more pain, the membrane in that area is unhealthy and might reach the bladder. This will be shown by the frequent urge to urinate at night, due to the sensitive condition of that organ.
If the instrument be arrested at about six inches and a half, the complaint, in all probability, is seated in the transverse portion of the prostate, and requires very cautious treatment.
If the device is stopped at around six and a half inches, the issue is likely located in the transverse section of the prostate and needs very careful handling.
When the obstruction is at the very entrance of the bladder, a resistance will be perceived, which, on yielding, will impart a peculiar sensation as the sound enters the bladder. When stricture is thus situated, there is a frequent desire, with almost total inability, to micturate; and when once formed, it is productive of the most serious mischief, unless relieved.
When there's a blockage right at the entrance of the bladder, you'll feel a resistance that, when it gives way, creates a distinct sensation as the catheter moves into the bladder. When a stricture is located in this way, there's a frequent urge to urinate but almost no ability to do so; once this situation develops, it can lead to very serious complications if not treated.
In cases of permanent stricture, the passing of the sound conveys the sensation of going over a ridge. Where it meets with a temporary stoppage, and then passes on, it has probably hitched to a fold of the urethra. Sometimes it will enter the orifice of a dilated follicle; and if much pressure is used, it will occasion considerable bleeding.
In cases of permanent stricture, passing the sound feels like going over a bump. When it encounters a temporary blockage and then continues, it has likely caught on a fold of the urethra. Sometimes, it will enter the opening of a dilated follicle, and if too much pressure is applied, it can cause significant bleeding.
The nature and situation of the disease being ascertained, the cure may now be proceeded in, recollecting that no force is to be used, and that too much be not attempted at one essay. Now without entering into an inquiry as to the laws on which contraction and elasticity of certain animal structures depend, it is enough for our purpose to know, that the urethra possesses both properties; it may contract so as to oppose the exit or entrance of the smallest stream, and it may be dilated to admit the introduction of an instrument an inch in circumference. The urethra maintains these properties in disease as well as in health, and upon the strength of this fact, is the practice of dilatation in the cure of permanent stricture founded, permanent stricture, it will be recollected, is a positive narrowing of the urethric canal; and as it is the nature of all organic diseases to progress, unless prevented by art, it needs no stronger argument than necessity to show how imperative it is to set about their removal.
The nature and condition of the disease determined, we can now proceed with the treatment, keeping in mind that no force should be used and that we shouldn’t try to do too much at once. Without diving into the details of the laws governing the contraction and elasticity of certain animal structures, it suffices for our purposes to know that the urethra has both properties; it can contract enough to block even the smallest stream and can expand to allow for the insertion of an instrument with a circumference of an inch. The urethra retains these properties whether in disease or in health, and this fact is the basis for the practice of dilation in treating permanent stricture. It's important to remember that permanent stricture is a significant narrowing of the urethral canal, and since all organic diseases tend to progress unless addressed, it’s clear that necessity makes it crucial to begin their treatment.
The cure by dilatation is as follows:—the seat and size of the stricture being ascertained (both of which can be easily done by the passing of the sound as directed, and the observance of the stream of urine), a bougie in circumference somewhat larger than the calibre of the urinary current, warmed and dipped in an oleaginous mixture combined with some sedative (Forms 22, 23, 24) or stimulant (Form 25) according to circumstances, is to be passed to the stricture, and the gentlest pressure is to be employed for the space of five, ten, or twelve minutes, according to the irritation it produces, removing it as soon as any uneasiness is felt.
The treatment by dilation is as follows: once the location and size of the stricture are determined (which can easily be done by passing a sound as instructed and observing the urine stream), a bougie that is slightly larger in circumference than the urinary flow should be warmed and dipped in an oily mixture combined with a sedative (Forms 22, 23, 24) or a stimulant (Form 25) depending on the situation. It should then be gently passed to the stricture, applying the lightest pressure for five, ten, or twelve minutes, based on the irritation it causes, and removing it as soon as any discomfort is felt.
Even in this very simple operation, a certain dexterity is requisite; for the direction of all urethræ is not alike, and the mere pushing a bougie against a contracted part is not the only likely method of effecting a free passage. Much also depends upon the nature of the bougie—the elastic ones, although assisted in their attempted passage to the bladder, by the smooth and well lubricated sides of the urethra, have a tendency to straighten; and unless considerable rotatory motion be observed, are apt to hitch in a fold of the urethra, especially if the case befall a person of relaxed fibre, and he be much worn down by suffering. The bougies that I employ are constructed upon[63] an improved plan to those in general use, being prepared of a material that will preserve the shape I adapt them to, previously to introducing them, but at the same time sufficiently soft to yield to any accidental tortuosity of the tube they are intended to explore. The bougie then is to be pressed softly, but steadily, against the obstruction, now and then withholding for a minute the bearing, so as to allow a respite to the stretched membrane; then renewing by, what is better done than expressed, an “insinuating” pressure for the space of the time advised above. The patient should not be dispirited, even if the bougie do not perforate the stricture at the first trial; it would doubtless do so, if longer time were employed, but that is rarely advisable, except in cases where the urine can scarcely escape, or much expedition be requisite. Should the operation even be unsuccessful in this first attempt, the patient will find his ability to micturate much greater than before the introduction; but, save in long-standing and obstinate strictures, I rarely find myself foiled, nor do those who practise the same method, if they have patience and skill enough, in overcoming the difficulty at the first interview. A great advantage of the cure by dilatation, independently of its safety and efficacy, is the insignificant pain it occasions; the sensation produced being only like a pressing desire to make water, which immediately subsides on withdrawing the bougie.
Even in this very simple procedure, some skill is necessary; not all urethras are the same, and simply pushing a bougie against a narrow area isn’t the only effective way to create a clear passage. Much also depends on the type of bougie used—the elastic ones, even when helped by the smooth and well-lubricated walls of the urethra, tend to straighten out; if considerable rotational movement isn't applied, they can get stuck in a fold of the urethra, especially if the patient has weak tissues and is already exhausted from discomfort. The bougies I use are made based on[63] an improved design compared to what is generally available; they’re made from a material that retains the shape I set them to before insertion, yet remains soft enough to adapt to any twists in the tube they’re meant to explore. The bougie should then be pressed gently but firmly against the blockage, occasionally letting up for a minute to give the stretched membrane a break; then, it should be reintroduced with a subtle pressure for the recommended duration. The patient shouldn’t be discouraged if the bougie doesn’t penetrate the stricture on the first try; it would likely succeed with more time, but that's rarely advisable unless the urine can barely pass or speed is crucial. If the procedure isn't successful initially, the patient will notice an improved ability to urinate compared to before the introduction; however, except in cases of long-lasting and stubborn strictures, I rarely encounter failure, and neither do others who use the same technique, provided they have enough patience and skill to tackle the challenge on the first attempt. A significant benefit of dilatation treatment, aside from its safety and effectiveness, is the minimal pain it causes; the sensation felt is similar to a strong urge to urinate, which fades away as soon as the bougie is taken out.
Another method of dilating a stricture, where it happens to be of chronic existence, is the passing a plastic catheter into the bladder, and suffering it to remain all night, or even for several nights, stopping up the handle end with a cork or wooden peg, which the patient can remove when he desires to urinate. The urethra, by this means, becomes quickly dilated, and much beyond the size of the instrument. It necessarily confines the patient to his room and couch; but where an expeditious cure is the object, as much may be effected in this manner in six days, as by the ordinary method in as many weeks. Time, however, it must be remembered, is the working material of nine tenths of strictured invalids, and a week’s lay-up may cost a twelve-month’s salary—a purchase too dear to be generally incurred.
Another way to treat a long-term stricture is to insert a plastic catheter into the bladder and let it stay there overnight, or even for several nights, sealing the end with a cork or wooden peg that the patient can remove when they need to urinate. This method quickly dilates the urethra, often beyond the size of the instrument. It does require the patient to stay in their room and rest, but if a quick recovery is the goal, you can achieve in six days what would normally take six weeks with the traditional method. However, it's important to remember that time is the most valuable resource for many people suffering from strictures, and a week of recovery could cost them a year’s worth of salary—a price that is generally too high to pay.
Several other plausible methods have been suggested for the cure of stricture—one by means of an instrument, that the operator could enlarge when it was passed into the[64] urethra, through turning a screw; another, which was to introduce a tube made of some thin skin, and then to distend it with wind or water; a third, and oftentimes, in reality, a very useful and available one, is to compress the penis around the glans, and suffer the urine, as it accumulated, to distend the anterior part of the urethra before the bandage was removed and the urine suffered to escape. But they have their several disadvantages: the processes, with the exception of the last, are complicated and uncertain in their result; the instrument is not so manageable, or so useful, as an ordinary sound; and the gut, instead of distending the strictured part, enlarges the healthy portions of the urethra. The bougie, in proper hands, notwithstanding it is a simple instrument, is the most positive and effectual method of curing stricture as yet, or likely to be, discovered. An entrance, then, having by this means been gained, a bougie of a larger size is to be selected on the next occasion, and the same process repeated. It is never advisable to repeat the operation oftener than once in two days, and when the urethra is irritable, only every three or four days.
Several other feasible methods have been proposed for treating stricture—one involving an instrument that could be expanded by turning a screw once it was inserted into the[64] urethra; another, which involves introducing a tube made from a thin material and then inflating it with air or water; a third, which is often very practical and effective, is to apply pressure around the penis at the glans and allow the accumulating urine to stretch the front part of the urethra before removing the bandage and letting the urine flow out. However, each of these methods has its drawbacks: the processes, except for the last one, are complex and their outcomes are unpredictable; the instrument is not as easy to handle or as useful as a regular sound; and instead of stretching the strictured area, the gut tends to enlarge the healthy parts of the urethra. The bougie, when used by a skilled practitioner, remains the most reliable and effective method for curing stricture discovered to date. Once access has been achieved through this method, a larger bougie should be chosen for the next treatment, and the same process repeated. It’s not advisable to repeat the procedure more than once every two days, and if the urethra is sensitive, only every three or four days.
By continuing in this manner, the stricture gradually yields, and a bougie as large as the orifice will permit to enter will at last proceed through the whole passage without meeting any obstacle. The operation, notwithstanding this apparent success, should not be wholly laid aside, but continued until the disposition for contraction is entirely removed; and the patient should never rest without occasionally examining his urethra, say once a month (at least once a quarter), lest he encounter a relapse.
By continuing this way, the narrowing slowly lessens, and a catheter as large as the opening allows will eventually pass through the entire passage without any issues. The procedure, despite this apparent success, shouldn’t be completely abandoned, but should continue until the tendency to narrow is fully resolved; and the patient should regularly check their urethra, at least once a month (or at least once every three months), to avoid a relapse.
Having disposed of the treatment of stricture in its fortunately most usual—namely, the mildest—form, I proceed to consider the treatment of severe kinds—previously to which, a few remarks upon the various kinds of instruments, their structure, shape, and size, will render any subsequent allusion more intelligible.
Having addressed the treatment of stricture in its most common and mild form, I will now discuss the treatment of more severe cases. Before doing that, a few comments on the different types of instruments, their design, shape, and size will help make any further references clearer.
The diagram here introduced represents the calibre of the various bougies in general use, and the observer will perceive, that as they are made to accommodate themselves to the passage they have to pass, how varied must be the changes which the urethra undergoes. The last outline indicates the natural and healthy bore of the urethra. Bougies are manufactured of different materials: waxen cloth rolled together, elastic and yielding; flexible metal, [65] silver, and gold. The bougies which I employ are constructed upon an improved plan to those in general use: the elastic, as they are termed, although assisted in their attempted passage to the bladder by the smooth and well-lubricated sides of the urethra, have a constant tendency to straighten, and consequently are liable to hitch in all the folds they may encounter, which, in relaxed habits, are very numerous in the membranous portion of the urethra. To obviate such a possibility, I prefer that the bougie should be of such a consistence and manufacture as will admit of its preserving the shape I adapt it to previously to introducing it; at the same time the material to be sufficiently soft to enable it to accommodate itself to any accidental tortuosity of the tube it is exploring.
The diagram shown here illustrates the size of the different types of bougies commonly used, and you will notice that as they are designed to fit the passage they need to go through, the urethra must undergo various changes. The last outline shows the normal and healthy width of the urethra. Bougies are made from different materials: waxed cloth rolled together, flexible and elastic; flexible metal, silver, and gold. The bougies I use are based on an improved design compared to the ones generally available. The elastic ones, as they are called, even with the smooth and well-lubricated sides of the urethra aiding their movement towards the bladder, tend to straighten out and can get caught on the many folds they encounter, which are quite numerous in the relaxed membranous section of the urethra. To avoid this issue, I prefer bougies made from a consistency and material that allows them to maintain the shape I set before inserting them; at the same time, they need to be soft enough to adapt to any unexpected bends in the tube they are navigating.

Catheters are instruments for the purposes of withdrawing the urine; they are consequently hollow, and are made of the same materials as bougies; but the most useful and to be depended upon are composed of silver. Surgeons, like other men, have their fancies: a catheter, when made of silver, has very little flexibility; accordingly it must be shaped beforehand. Some medical men prefer them quite straight, others with an immense curve. A surgeon should possess many forms, as the direction of the urethra differs almost in all men. The subjoined exhibits not the size, but the shape of the more useful and those most generally used. Figures 1, 2, and 3, suffice in most instances, whereas figure 4 is necessary in cases of enlargement[66] of the prostate gland, which presses up the bladder, and renders the urethral passage consequently longer.
Catheters are tools used to drain urine; they are therefore hollow and made from the same materials as bougies. However, the most reliable ones are made of silver. Surgeons, like anyone else, have their preferences: a silver catheter lacks flexibility, so it needs to be shaped in advance. Some medical professionals prefer them completely straight, while others like a significant curve. A surgeon should have various shapes available because the angle of the urethra can vary quite a bit among individuals. The following shows not the sizes but the shapes of the more useful types that are most commonly used. Figures 1, 2, and 3 are sufficient in most cases, whereas figure 4 is needed for cases of prostate gland enlargement, which pushes up the bladder and makes the urethra longer.[66]

The French employ not only variously curved instruments, but variously shaped. In peculiar cases they are doubtlessly useful; but they require to be used only by persons of skill and judgment. In the next three kinds are views of such; they are called conical bougies—the first curved, the second straight. They are made of silver, waxen cloth, or India-rubber. The third exhibits a sound, employed to ascertain the seat of the stricture.
The French use not just different curved tools, but also variously shaped ones. In specific situations, they can be very useful, but they should only be used by skilled and knowledgeable individuals. The next three types show examples of these; they’re called conical bougies— the first one is curved, and the second is straight. They can be made from silver, wax cloth, or rubber. The third type is a sound, which is used to determine the location of a stricture.
I have already alluded to the improved method I employ on finding it necessary to use escharotics. I can not better explain the process than by submitting a sketch of the[67] instruments, whereby the mode of application will be instantly perceived. The instruments are made of silver. The figures represent No. 8 a curved, No. 9 a straightened, No. 10 ditto, with enlarged head, which puts the areola of the stricture on the stretch, and secures the central part for the application of the caustic, or whatever substance may be employed.
I have already mentioned the improved method I use when I find it necessary to apply escharotics. I can explain the process better by providing a sketch of the [67] instruments, which will clearly show how to apply them. The instruments are made of silver. The figures show No. 8 as a curved instrument, No. 9 as a straight one, and No. 10 as a straight instrument with an enlarged head, which stretches the area around the stricture and secures the central part for applying the caustic or any substance being used.
The next kind of instruments are for the purposes of dividing or piercing hardened obstructions—one or two applications creating a passage which a hundred cauterizings would not effect. When any styptic is applied to a morbid growth, its tendency is to create a slough, or to destroy the part whereto it is applied. In some instances a styptic actually promotes increased action: it may temporarily destroy the part; but the moment the effect is over, a reaction follows, and the excrescence is increased. Such is the case in many long-standing, obstinate strictures; and their removal by perforation or division is rendered indispensable. The practice requires the most careful attention and anatomical knowledge; and no one but a professional man would attempt its employment.
The next type of instruments are designed for breaking through or piercing hardened blockages—just one or two uses can create a passage that a hundred cauterizations would not achieve. When a styptic is applied to an unhealthy growth, it tends to cause the tissue to die off or destroy the area where it’s applied. In some cases, a styptic actually stimulates more activity: it may temporarily damage the area, but as soon as the effect wears off, a reaction occurs, and the growth becomes larger. This is often seen in many long-standing, stubborn strictures; therefore, their removal through perforation or division becomes essential. This practice demands meticulous attention and a solid understanding of anatomy, and only a trained professional should attempt to employ it.
No. 11 sketch exhibits a curved instrument, with the pointed lancet projecting as when applied. No. 12 exhibits ditto, but with a differently formed instrument, consisting of two portions separated, so as to allow a director, in the form of a thin silver wire with a silver knob, to pass for the purpose of exploring the passage which the instrument is to follow and enlarge. It is indispensable in strictures seated upon the soft and deep parts, lest a false passage should be made. No. 13 represents a straight instrument; No. 14 ditto, but with the lancet in reserve—the last a perforator.
No. 11 sketch shows a curved instrument, with the pointed lancet sticking out as it would be when used. No. 12 shows a similar instrument, but it has a different design, featuring two parts that are separated to allow a guide, in the form of a thin silver wire with a silver knob, to pass through for exploring the pathway that the instrument is meant to follow and widen. This is essential for strictures located in soft and deep areas, to avoid creating a false passage. No. 13 illustrates a straight instrument; No. 14 is similar, but with the lancet held back—the last one is a perforator.
The reader has now been made acquainted with the various resources the surgeon has at his command. A few words on their employment will complete the necessary amount of information to render the one as wise as the other. By way of recapitulation, the treatment of stricture is by dilatation, cauterization, and division. They are to be estimated in the order of their arrangement. By dilatation is meant the enlarging of the urethral passage through the frequent introduction of bougies of graduated sizes. It is an operation unattended with any considerable pain; its novelty sometimes renders a patient a little nervous, but a complaint is rarely made after a second or[68] third introduction. Indeed, it is oftentimes courted more frequently than is desirable. The application also of caustic, or even the perforator, produces scarcely the least inconvenience. Hemorrhage, of most things to be dreaded, is less frequent, with cauterizing and cutting instruments (in skilful hands), than the incautious employment of blunt-pointed bougies.
The reader has now been introduced to the different resources available to the surgeon. A few words about how to use them will complete the necessary information to make one as knowledgeable as the other. To summarize, the treatment for stricture involves dilatation, cauterization, and division. They should be considered in the order they are listed. Dilatation refers to widening the urethral passage by frequently using bougies of different sizes. This procedure is not generally painful; its novelty may make a patient a bit anxious, but complaints are rare after the second or [68] third insertion. In fact, it is often requested more frequently than desirable. The use of caustic agents or even the perforator causes very little discomfort. Hemorrhage, which is one of the things to be feared, is less common with cauterizing and cutting instruments (in skilled hands) than with the careless use of blunt-tipped bougies.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links.
Diseases of the Testicles.—The testicles, from their office and connexion with other structures equally as important, are liable to many excitations. In gonorrhœa they are subject to sympathetic inflammation, as in hernia humoralis, which, if neglected or maltreated, gives rise to abscess or chronic hardness. Inflammation also occurs in them as in other structures. Accidents, such as blows or bruises, horse-riding, wearing very tight pantaloons, are all fertile sources of derangement. Scrofulous constitutions are predisposed to have their testicles, like the rest of the glands, diseased. The most frequent disturbance, however, of the testicles, is a dilatation of the veins, constituting what is called varicocele; and generally accompanied by a wasting away of the testicle itself. It is rare, indeed, to find perfectly healthy testicles in an individual who has been exposed to amatory pleasures and sensualities; and as, of course, even amative desire, as well as amative power, depends upon the absolute sound condition of the glands in question, the inference is, that in very numerous persons, the sexual instinct is considerably diminished, and not unfrequently wholly suppressed, before half the natural term of their existence has expired, at which time they ought in reality to be at the climax of their prime and capability.
Diseases of the Testicles.—The testicles, due to their role and connection with other equally important structures, are prone to various irritations. In cases of gonorrhea, they can become inflamed due to sympathetic reactions, similar to hernia humoralis, which, if ignored or poorly treated, can lead to abscesses or chronic hardness. Inflammation can also occur in them, just like in other structures. Injuries, such as hits or bruises, horse riding, and wearing very tight pants, are all common triggers for problems. People with scrofulous constitutions are more likely to have diseased testicles, similar to other glands. However, the most common issue with the testicles is the enlargement of veins, known as varicocele, which is usually accompanied by shrinkage of the testicle itself. It is quite rare to find completely healthy testicles in someone who has engaged in sexual activities and pleasures; consequently, since both sexual desire and ability depend on the healthy condition of these glands, the conclusion is that in many individuals, the sexual instinct is significantly reduced, and often completely suppressed, before they reach half of their natural lifespan, at which point they should actually be at their peak vitality and capability.
It is not so much a painful complaint, as an unpleasant one. There are occasionally pains in the back and loins, and other feelings, creating a sensation of lassitude and weariness; and now and then some local uneasiness is felt.
It’s not really a painful issue, but rather an uncomfortable one. Sometimes there are aches in the back and lower back, along with other sensations that cause a feeling of tiredness and fatigue; and occasionally, there’s some local discomfort experienced.
Varicocele gives to the examiner a sensation as though he were grasping a bundle of soft cords. It sometimes exists to such a degree as to resemble a rupture. In advanced stages of the disease, or disorganization, the epididymis becomes detached from the body of the testicle, and is plainly distinguishable by the finger. The result of all is, that a considerable diminution of sexual power takes place; and if means are not adopted to arrest a further[69] break-up of the structure, the venereal appetite will subside altogether. The annexed drawing exhibits a tolerably faithful portrait of the disease; it represents the varicocele to be on the left side—the side most usually affected.
Varicocele makes the examiner feel like they're holding a bunch of soft cords. It can sometimes be so pronounced that it looks like a rupture. In advanced stages of the condition, or if there’s significant damage, the epididymis becomes separate from the body of the testicle and can easily be felt by touch. As a result, there is a significant decline in sexual function, and if steps aren’t taken to prevent further degradation of the structure, the sexual desire could completely fade away. The illustration attached shows a pretty accurate depiction of the condition, highlighting that the varicocele is on the left side, which is the side that is most commonly affected.

The folds formed by the veins lapping over each other are clearly distinguishable, and the dependent state of the scrotum on the affected side exhibits very well the occasion of it. The treatment consists in giving support by means of a suspensory bandage, which may be worn during the day, and the use of local refrigerants night and morning. The state of health is sometimes mixed up with it; and tonics and generous diet are useful. The cold shower bath helps to brace the system. It is a complaint in which, if it be not of very great severity, nor very long continuance, much good may be done. In some instances the veins may be allowed to empty themselves, which they will do when the body is in a recumbent position, and a coated ivory ring, or a silken band, may be so placed around them as shall prevent their refilling. It is, however, a case fitter for the surgeon’s management.
The folds created by the veins overlapping each other are clearly visible, and the way the scrotum hangs on the affected side shows the reason for it. Treatment involves providing support with a suspensory bandage, which can be worn during the day, and using local cold treatments morning and night. Sometimes, health issues are also involved, so tonics and a nutritious diet are beneficial. A cold shower can help invigorate the body. If the issue isn’t very severe or has lasted a long time, a lot of improvement can be made. In some cases, the veins can be allowed to empty themselves, which they will do when lying down, and a coated ivory ring or a silk band can be placed around them to prevent them from refilling. However, this is generally a situation better suited for a surgeon.
Abscess in the Testicle.—The testicle is subject to inflammation and suppuration like any other structure. A case about three years ago fell under my notice, where a quantity of dark fœtid fluid was released on puncturing a testicle in which the sense of fluctuation was very evident; and the patient stated that it had been five or six years in arriving at that condition. He was wasted considerably from nocturnal perspirations and acute pain, and his sexual desire was much diminished. The case did well, and the latter function was restored without much loss.
Abscess in the Testicle.—The testicle can become inflamed and infected like any other body part. About three years ago, I encountered a case where a significant amount of dark, smelly fluid was released after puncturing a testicle that clearly showed signs of fluctuation. The patient reported that it had taken five or six years to reach that state. He had lost a lot of weight due to night sweats and sharp pain, and his sex drive had decreased significantly. The case had a good outcome, and his sexual function was restored with minimal loss.
Hydrocele.—Hydrocele is an accumulation of yellow serous fluid in the tunica vaginalis testis (refer to the engravings in next page), or peritoneal covering of the testicle. It is a disease incident to every period of life, but more commonly met with in grown persons. The ordinary formation of hydrocele is unattended with pain; and the patient[70] accidentally discovers the existence of the swelling, but oftentimes not until it has attained a considerable magnitude. The tumor, when large, produces an unsightly appearance, and forms a hindrance to sexual intercourse, from the integuments of the penis being involved therein, and thereby preventing a perfect erection of that organ. The disease may appear to originate spontaneously; but it is usually traceable to some bruise, blow, or other external injury to the part.
Hydrocele.—Hydrocele is an accumulation of yellow fluid in the tunica vaginalis testis (see the images on the next page), or the peritoneal covering of the testicle. It can occur at any age but is more commonly seen in adults. Typically, the development of hydrocele isn't painful, and patients often discover the swelling by chance, usually not until it has grown quite large. When the tumor is significant, it can look unsightly and interfere with sexual intercourse, as it can affect the skin of the penis and prevent a proper erection. While the condition may seem to arise on its own, it is usually linked to some kind of bruise, blow, or other external injury to the area.
The two following drawings exhibit the outward and inward appearance of the scrotum in hydrocele:—
The two drawings below show the outer and inner appearance of the scrotum in hydrocele:—


The notion that the cure of hydrocele depends on promoting adhesion to the sides of the tunica vaginalis with the testicle is somewhat upset by several preparations in the London hospitals, exhibiting the tunic taken from persons in whom a radical cure was effected by injection, and in whom no fluid was reproduced; nor were the sides of the said investment at all adherent with the testicle, but apart, as in the healthiest individual. Hitherto surgeons,[71] acting on the aforesaid notion, with a view to obliterate the cavity, adopted various plans of treatment—such as, for instance, laying open the entire cavity, cutting away a portion of the tunica vaginalis, the application of caustic, and, lastly, the seton, as advised by Dr. Pott, which was suffered to liberate itself by ulceration. When, in any of these instances, suppuration was induced, the cavity became in time filled up by the granulating process. The plan of the present day is by perforating the sac with a trocar, suffering the effused fluid to escape, and injecting some stimulating liquid which is allowed to remain until a degree of inflammation is produced, that shall cause an obliteration of the cavity by adhesion, or, as it has also been proved, prevent a reproduction of the fluid, by closing the mouths or altering the diseased action of the exhalent arteries. Whichever be the effect produced thereby, the cure is almost certain, and the principles of the treatment consequently judicious. But, notwithstanding, the operation is not always immediately, nor ultimately successful; the degree of inflammation set up may be insufficient, and the effusion again take place, and the operation may require a second and third repetition; or an excessive degree of inflammation may ensue, that shall occasion serious constitutional disturbance, either by suffering the injected fluid to remain too long, or its being of too stimulative a character, or from its escaping into the cellular membrane of the scrotum, an accident not unfrequent, unless great care be used in the operation.
The idea that the treatment of hydrocele relies on encouraging adhesion between the sides of the tunica vaginalis and the testicle is challenged by various cases in London hospitals. In these cases, the tunic from patients who underwent a successful radical cure through injection showed no fluid was produced, and the sides of the tunica were not adhered to the testicle but remained separate, just like in a healthy individual. So far, surgeons[71] have followed this idea and tried different methods to obliterate the cavity. They have opened the entire cavity, removed parts of the tunica vaginalis, applied caustic substances, and finally used a seton, as suggested by Dr. Pott, which allowed itself to drain through ulceration. In cases where suppuration occurred, the cavity would eventually fill up through granulation. Today's approach involves puncturing the sac with a trocar to let the fluid escape and then injecting a stimulating liquid that stays in place until inflammation occurs, which causes the cavity to close up through adhesion or prevents the fluid from returning by affecting the exhaling arteries. Regardless of the exact outcome, the cure is nearly guaranteed, making the treatment methods sound. However, the operation isn't always immediately or ultimately successful; the inflammation may not be strong enough, leading to a recurrence of fluid, requiring the procedure to be repeated two or three times. Conversely, excessive inflammation can lead to serious systemic issues, either from the injected fluid remaining too long, being too irritating, or leaking into the scrotum's cellular membrane, which is a common risk if precautions are not taken during the operation.
Radical Cure of Hydrocele.—The term radical is applied to the process narrated in the last case; but, as has been observed, the operation is occasionally required to be repeated several times. In the case I am adverting to, after tapping, several injections were thrown in between the tunics, and withdrawn; and on one occasion the morbid fluid was secreted to the greatest possible distension of the scrotum by the following morning. Its subsequent withdrawal, and the injection of a more active stimulant, effected, however, a permanent cure. In the country, surgeons frequently plunge a lancet in the scrotum, suffer the effused liquid to escape, and desire the patient merely to wrap the parts up in a handkerchief, to take no further heed, and to ride home: and these cases generally do well.
Radical Cure of Hydrocele.—The term radical refers to the process described in the last case; however, as noted, the operation sometimes needs to be repeated multiple times. In the case I'm referring to, after draining, several injections were made between the layers and then removed; and on one occasion, the abnormal fluid was secreted to the maximum distension of the scrotum by the next morning. Its subsequent removal and the injection of a stronger stimulant ultimately achieved a permanent cure. In rural areas, surgeons often use a lancet to puncture the scrotum, allow the fluid to drain, and tell the patient to just wrap the area in a handkerchief, not to worry about it, and to ride home: and these cases usually turn out well.
Hydrocele Cured by Acupuncturation.—A new method of[72] treating hydrocele has of late years been introduced, namely, by the insertion of a needle into the sac or bladder of the testicle, which, upon its withdrawal, permits the fluid to escape into the cellular membrane, whence it is rapidly absorbed. A pint of fluid may be got rid of in that way in two or three hours; and, although the disease may not be radically cured, it will occupy several months before a reaccumulation of the fluid takes place. In recent cases, this treatment oftentimes proves permanently successful. Many nervous persons will not submit to anything approaching an operation, not even to the simple one of acupuncturation. In such cases, there is no alternative but counter-irritants, to be applied over the part, such as the tincture of iodine, or the following ointment (Form 26).
Hydrocele Cured by Acupuncture.—A new method of[72] treating hydrocele has recently been introduced, which involves inserting a needle into the sac or bladder of the testicle. When the needle is withdrawn, it allows the fluid to escape into the surrounding tissue, where it is quickly absorbed. You can remove a pint of fluid this way in just two or three hours; and while the condition may not be completely cured, it can take several months for the fluid to build up again. In recent cases, this treatment often leads to permanent results. However, many anxious individuals are reluctant to undergo any kind of procedure, even something as simple as acupuncture. In these situations, there are no other options besides using counter-irritants applied to the area, such as tincture of iodine or the following ointment (Form 26).
It is at all times best to attend early to any disease of the testicles; the progress is so rapid, the mischief so great, and the consequences so deplorable, of uncontrolled disease.
It’s always best to address any testicular issues early on; the progression is so fast, the damage so serious, and the outcomes so unfortunate when the disease goes untreated.
Eruptions incident to the Organs of Generation and the Rectum.—The structures included in the above heading are subject to a variety of eruptions, varying in character, intensity, and duration. Thus we have the papular, a chronic inflammation characterized by papules, or very minute pimples, of nearly the same color as the skin, accompanied by intense itching, and terminating, when broken by scratching, in small circular crusts: this is called, by dermoid pathologists, Prurigo. Another order of eruption is designated the vesicular and pustular, and consists of groups of small pimples of a very bright red color, and containing a serous fluid. They are accompanied by itching, which increases as the contained humor becomes turbid, and assumes the puriform aspect; they then incrustate, and at the end of about a fortnight drop off, leaving the skin healthy underneath. The name given to this variety is Herpes.
Eruptions Related to the Sexual Organs and the Rectum.—The structures mentioned above can experience a range of eruptions that differ in type, severity, and duration. One type is the papular eruption, a chronic inflammation marked by papules, or tiny pimples, that are almost the same color as the skin, accompanied by intense itching. When scratched, they can break and form small circular crusts; this condition is referred to by dermatologists as Prurigo. Another type of eruption is the vesicular and pustular type, which consists of clusters of small, bright red pimples filled with a clear fluid. These pimples cause itching that worsens as the fluid inside becomes cloudy and takes on a pus-like appearance. They then form crusts, and after about two weeks, fall off, leaving the skin healthy underneath. This variety is called Herpes.
The last and most inveterate species is characterized by an itching of the skin, which, on inspection, appears of a[73] diffused redness, and gives off, after a while, a number of thin scales: these reaccumulate, and the entire organs of generation becomes sometimes covered with similar patches: this is denominated Psoriasis. These affections, which are but various degrees of inflammation, modified by idiosyncrasy and habit, arise from local and constitutional causes. Among these are frequent excitation of the organs of generation, the contact of the fluids secreted during sexual intercourse, an unhealthy and relaxed condition of the genitals, and, lastly, a disordered state of the digestive organs. It is astonishing to what an extent these disorders prevail, and more so to find how long the individuals, probably from a sense of diffidence in seeking professional assistance, endure them. I have encountered many patients who have informed me that they have had the complaint upon them from five to ten years, purposing during the whole of that period to consult some medical friend, but postponing it until their interview with myself; and it is the more to be regretted, as the cure may always be effected in a week or two, with moderate attention and perseverance; but if the attempt be neglected, there is no limiting the extent to which the disease may proceed. Local diseases, especially of such a nature as those under consideration can not exist any great length of time without involving the digestive organs, which become sympathetically deranged; and in like manner do local diseases participate with dyspeptic disturbances—each, therefore, goes on aggravating the other.
The last and most persistent type is marked by itchy skin, which, when examined, shows a widespread redness and eventually develops thin scales that accumulate, sometimes covering the entire genital area with similar patches. This is called Psoriasis. These conditions, which are simply different levels of inflammation influenced by individual predisposition and lifestyle, stem from local and systemic causes. These include frequent stimulation of the genital organs, contact with fluids secreted during sex, an unhealthy and lax state of the genitals, and finally, a disordered digestive system. It's surprising how common these issues are, and even more so that individuals often endure them for so long, likely due to embarrassment in seeking medical help. I've met many patients who have had this problem for five to ten years, intending to talk to a doctor during that whole time but only coming to me. It's regrettable because the condition can typically be treated in a week or two with some effort and dedication; however, if left untreated, there's no telling how far the disease can progress. Local diseases, especially of this kind, cannot last long without affecting the digestive organs, which become similarly disturbed; and in turn, local diseases can worsen digestive issues—each one exacerbating the other.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links.
Diseases of the Bladder.—The anatomical description of the bladder will be found in the earlier pages of this work. It may simply be restated:
Diseases of the Bladder.—The anatomical description of the bladder is provided in the earlier pages of this work. It can be restated as follows:
The bladder is a viscus somewhat similar in structure to the stomach. It is composed of several coats—muscular, nervous, and mucous. Each are liable to diseases peculiar to their several structures. The size of the bladder differs in most persons, and in the sexes.
The bladder is an organ that is somewhat similar in structure to the stomach. It consists of several layers—muscular, nervous, and mucous. Each layer can be affected by specific diseases related to their structures. The size of the bladder varies among individuals and between the sexes.
The female bladder is generally the largest; but the largeness is observable more especially in females who have borne children. The proverbial ability of females to retain their urine longer than men is thus accounted for.
The female bladder is usually the largest, and this size is especially noticeable in women who have given birth. This explains the common belief that women can hold their urine longer than men.
Much mischief is often done by both sexes disobeying the particular “call of nature” to urinate; and the younger branches should have that fact impressed upon them. I[74] have known children acquire a severe and obstinate form of irritability of the bladder by retaining their urine too long. Diseases of the bladder are generally the consequences of other complaints, and those complaints have already been enumerated. They may be thus summed up:
Much trouble is often caused by both genders ignoring the natural urge to urinate, and younger kids should be taught about this. I[74] have seen children develop a serious and stubborn form of bladder irritation from holding their urine for too long. Bladder issues usually stem from other health problems, which have already been listed. These can be summed up as follows:
Gonorrhœa extending to the bladder, and producing absolutely a clap of the bladder. If the inflammation is not subdued, or does not subside, probably some permanent mischief ensues; at all events, the inflammation extends, and involves other coats than the interior. Accordingly, we have inflammation of the muscular coat, the nervous coat, and, lastly, the peritoneal coat. These terminations, severally, have certain symptoms, and certain names.
Gonorrhea can spread to the bladder, causing a severe bladder infection. If the inflammation isn’t treated or doesn’t go away, it could lead to lasting damage; in any case, the inflammation spreads and affects other layers besides the inner one. As a result, inflammation may occur in the muscular layer, the nerve layer, and finally, the peritoneal layer. Each of these conditions has specific symptoms and names.
There are others, and among them may be named colds, local injuries, hæmorrhoids, excess in drinking particular fluids, sensual indulgences, diseased condition of the kidneys, or long retention or vitiated states of the urine, nervousness, and, lastly, the formation of stone in the bladder. The most common form of bladder ailment is irritability, which is a milder term for inflammation. Then we have absolutely inflammation, and, lastly, loss of power, or paralysis.
There are other issues to consider, including colds, local injuries, hemorrhoids, excessive consumption of certain drinks, indulgence in sensual pleasures, kidney disease, prolonged retention or poor quality of urine, nervousness, and finally, the formation of stones in the bladder. The most common type of bladder problem is irritability, which is a gentler way to describe inflammation. Then we have true inflammation, and finally, loss of function, or paralysis.
Irritability of the Bladder.[3]—The chief indication of disease affecting the bladder is a frequent desire which the patient experiences to pass his water; but that symptom alone does not determine the nature of the complaint. It may be irritable from sympathy with surrounding irritation, and disappear on the subsidence of that irritation. It may constantly be fretting the patient by its contractions, through the urine (owing to some general derangement in the system, being altered in its chemical qualities) exciting the bladder the moment it is secreted therein; or it may be the result of nervous agitation, with or without any actual diseased state of the bladder. These causes[75] should be understood to regulate the treatment, which of course must be qualified by the provocation, and which the patient, when in doubt, had better leave to the discrimination of his physician.
Irritability of the Bladder.[3]—The main sign of a problem with the bladder is a frequent need to urinate that the patient feels; however, this symptom alone doesn't define the issue. It could be irritated due to surrounding inflammation and may go away once that irritation subsides. It might be causing the patient ongoing discomfort through its contractions, with the urine (due to some general imbalance in the body, changing its chemical properties) irritating the bladder as soon as it’s produced; or it could stem from nervous tension, with or without any actual bladder disease. Understanding these causes[75] is essential for determining treatment, which of course should be adjusted based on the triggering factors, and the patient, when unsure, should rely on their doctor’s judgment.
Paralysis of the Bladder.—The bladder may become, through loss of nervous stimulus, insensible to irritation, and consequently be disobedient to its natural functions. The urine, in these cases, accumulates in large quantities, distends the bladder to its utmost, which it does without pain; and the excess of secretion then dribbles away involuntarily. This state of the bladder is called paralysis, and is an aggravated form of disease, arising from the same causes that establish inflammation, or from some contiguous nervous injury. The treatment of paralysis of the bladder must be intrusted to experienced hands; it consists chiefly of purgatives, stimulative enemata up the rectum, the introduction of the catheter, the cold bath, rest, and general medicinal nervous excitants.
Bladder Paralysis.—The bladder can become unresponsive to irritation due to a loss of nerve signals, leading it to fail in its normal functions. In these cases, urine builds up in large amounts, stretching the bladder to its limit without causing pain, and the excess urine then drips out involuntarily. This condition is known as paralysis and is a serious form of illness caused by the same factors that lead to inflammation or from nearby nerve damage. Treating bladder paralysis should be handled by skilled professionals; treatment mainly involves laxatives, stimulating enemas, catheterization, cold baths, rest, and general medications to stimulate the nervous system.
Inflammation of the Bladder.—Cases of acute inflammation of the bladder are of rare occurrence; but they do occur, occasionally prove fatal, and always are productive of much general disturbance, which yields not without vigorous and active treatment. Gonorrhœa is most usually the exciting cause. On the sudden suppression of the urethral discharge, an inflammation sympathetically seizes the testicle, the glands in the groin, or the bladder; and when the latter is the seat of the transference, it may be held as the ratio of the severity of the disease. In inflammation of the bladder, there is a constant desire to pass water, which, when made, is usually in very small quantities, and leaves a sediment. The patient often experiences an insupportable inclination to urinate, with a sensation as though the bladder were ready to burst—whereas there may be little or no urine in it. There is much pain at the root of the penis, and it extends along the perinœum to the rectum, which latter is assailed with almost constant spasms resembling straining. There is considerable thirst, fever, and anxiety; the pulse is full and quick, the tongue furred, and all those symptoms are present that prevail during severe constitutional excitement. The treatment consists of bleeding, leeching, or cupping; relieving the bowels by castor oil and injections; giving mucilaginous drinks, administering opiates, preserving rest, and total abstinence from stimulating[76] diet. If these means fail in subduing the inflammation it runs on to ulceration, permitting extravasation of urine occasioning mortification and death; but where they are effectual, the patient is soon left free from complaint. It often happens that the inflammation is not so vigorously treated, or it may be wholly neglected, and yet it may happily resolve itself without proceeding to the extremity narrated; but, unfortunately, it may degenerate into a minor but not less troublesome form, denominated chronic, and which, in fact, is the disease christened “irritability,” and the one, for obvious reasons, as above stated, for which relief is most usually sought, the patient having in vain daily looked for the subsidence of his malady. Having stated that irritability of the bladder must be treated with reference to its cause, it is obvious that more than non-medical discrimination is required. Where it depends upon stricture, the stricture must be first cured; where upon stone in the bladder, the stone must be removed; where upon sympathetic inflammation, the source must be attacked, and so on.
Inflammation of the Bladder.—Cases of acute bladder inflammation are rare, but they do happen, can sometimes be fatal, and always cause significant discomfort, which doesn't resolve without vigorous and active treatment. Gonorrhea is the most common trigger. When the urethral discharge suddenly stops, inflammation can sympathetically affect the testicle, the lymph nodes in the groin, or the bladder; and if the bladder is affected, it often indicates the severity of the condition. With bladder inflammation, there's a constant urge to urinate, but when the urge is fulfilled, it's usually only a small amount and may leave a sediment. The patient often feels an unbearable need to urinate, with a sensation that the bladder is about to burst, even when there’s little or no urine in it. There's significant pain at the base of the penis, which radiates along the perineum to the rectum, causing almost constant spasms that feel like straining. The patient experiences considerable thirst, fever, and anxiety; the pulse is rapid and strong, the tongue is coated, and all the symptoms associated with severe constitutional distress are present. Treatment includes bleeding, leeching, or cupping; relieving the bowels with castor oil and enemas; providing soothing drinks, administering opiates, ensuring rest, and complete avoidance of stimulating foods and beverages.[76] If these methods fail to reduce the inflammation, it can progress to ulceration, leading to urine leakage, tissue death, and death; however, if effective, the patient may quickly recover. Sometimes, the inflammation isn't treated aggressively, or it might be neglected entirely, yet it may resolve on its own without leading to severe outcomes; unfortunately, it can also develop into a less intense but still bothersome condition called chronic inflammation, which is referred to as "irritability." This is the condition for which relief is most often sought, as patients futilely hope for their symptoms to subside. It’s important to treat bladder irritability based on its underlying cause, meaning that more than just basic observational skills are needed. If it’s due to a stricture, that must be addressed first; if it's caused by a bladder stone, the stone needs to be removed; if it arises from sympathetic inflammation, the original source must be treated, and so on.
However, it has been stated that other causes may exist—that it may even be a primary disease in itself; and as this treatise professes to be a private mentor to the invalid, I will detail such measures as may be safely adopted for the cure of a complaint as often borne from being trusted to unskilful hands, as from a morbid delicacy in seeking proper and legitimate relief. The ordinary symptoms are, first, an inordinate desire to make water; it flows in small quantities, with pain before, during, and after. The urine has an offensive ammoniacal odor; it deposites a thick, adhesive mucus, of a gray or brown color, sometimes streaked with blood, and of an alkaline character.
However, it has been mentioned that there may be other causes—that it could even be a primary condition on its own; and since this guide aims to be a personal advisor to the person suffering, I will outline some safe approaches for addressing a problem that often arises from being placed in the hands of inexperienced practitioners, as much as from an excessive sensitivity in seeking proper and legitimate treatment. The typical symptoms are, first, an intense urge to urinate; it comes in small amounts, with pain before, during, and after. The urine has a strong ammonia-like smell; it contains a thick, sticky mucus, which can be gray or brown in color, sometimes with blood streaks, and has an alkaline nature.
In this stage of affairs, rest is indispensable; sedatives and opiates may be given; but alkalies (rarely omitted in prescriptions for incontinence of urine) should not be indiscriminately given, for they only render the urine more alkaline, which occasions it to deposite calcareous flakes, that, if not passed off, accumulate, unite, and lay the foundation of that frightful disease, stone in the bladder. The extract of conium, or henbane, combined with mucilage, may be given in doses of three to five grains every six hours. The tincture of henbane, in doses of a fluid-drachm, or the tincture of opium, not exceeding ten or fifteen[77] drops at a time, may be given in like manner, and continued for several days, keeping the bowels open with castor oil. The daily or alternate daily use of the hot, general, or hip bath, will afford immense relief. The various preparations of morphine, aconitine, and of hops, possess great power in small and frequent doses. The uva ursi is a remedy of ancient note, and is often prescribed with advantage; the dose is one scruple to a drachm in milk, or any bland fluid, three times a day, or it may be taken in infusion or decoction, one ounce to a pint of water—that quantity to be drank during the day. The pareira brava, exhibited in a decoction (by simmering three pints of water, containing half an ounce of the root, down to a pint), may be taken in divided doses of eight or twelve ounces during the day, or in the form of extract, in quantity of a scruple, which equals the above amount of decoction.
In this situation, rest is essential; sedatives and painkillers can be given, but alkalies (which are usually included in prescriptions for urinary incontinence) shouldn't be given indiscriminately, as they just make the urine more alkaline, leading to the formation of calcareous flakes that can accumulate, combine, and cause the severe condition of bladder stones. The extract of conium or henbane, mixed with mucilage, can be administered in doses of three to five grains every six hours. The tincture of henbane, in doses of a fluid-drachm, or the tincture of opium, not exceeding ten or fifteen[77] drops at a time, can be given similarly and continued for several days, while keeping the bowels regular with castor oil. Using a hot general or hip bath daily or every other day will provide significant relief. Various preparations of morphine, aconitine, and hops are very effective in small, frequent doses. Uva ursi is an old remedy that is often beneficial; the dose is one scruple to a drachm in milk or any mild liquid, three times a day, or it can be taken in infusion or decoction, one ounce to a pint of water, which should be consumed throughout the day. The pareira brava, boiled in a decoction (by simmering three pints of water with half an ounce of the root down to one pint) can be taken in divided doses of eight to twelve ounces during the day, or as an extract, in the amount of a scruple, which is equivalent to the amount of decoction mentioned above.
The achillæ millefoliæ is an excellent plant, and possesses astonishing astringent powers, often restoring the tone of the bladder to a healthy condition, when all other remedies have failed. A handful of the leaves are to be infused in a pint of boiling water, which, when cool, may be poured off, and given in doses of a cupful three times a day. Any of the preceding sedatives may be given in conjunction with these preparations.
The achillæ millefoliæ is a fantastic plant and has amazing astringent properties, often bringing the bladder back to a healthy state when every other remedy has failed. A handful of leaves should be steeped in a pint of boiling water, which, once cool, can be strained and taken in cupful doses three times a day. Any of the previously mentioned sedatives can be taken along with these preparations.
Lime-water taken with milk, as an ordinary drink, is a useful corrective.
Lime water mixed with milk, when consumed as a regular drink, is a helpful remedy.
The buchu (the diosma crenata)—an ounce infused for several hours in a pint of boiling water, and a wineglassful of the cooled liquid administered three or four times a day—has justly obtained some notoriety.
The buchu (the diosma crenata)—an ounce steeped for several hours in a pint of boiling water, with a wineglass of the cooled liquid given three or four times a day—has rightly gained some notoriety.
Where all these means prove ineffectual, the injection of sedative and astringent applications often answers the most sanguine expectations; but they should be employed only by professional persons, and even then with great care; as when the disease has been at its height, and they have been used, much inconvenience, and even mischief, has been occasioned. A mild infusion of poppies, or weak gruel, may be thrown in, once or twice a day, in quantities not exceeding two or three ounces at a time, and withdrawn after being suffered to remain thirty or forty seconds. A catheter, with elastic bag, should be the instrument used.
Where all these methods don’t work, using sedatives and astringents often meets the highest expectations; however, they should only be used by professionals and with great caution. When the disease is at its peak, using them can cause a lot of discomfort and even harm. A mild infusion of poppies or weak gruel may be given once or twice a day, in amounts not exceeding two or three ounces at a time, and should be removed after staying in for thirty or forty seconds. A catheter with an elastic bag should be the tool used.
In the more chronic forms, where the urine does not[78] deposite much mucus, or is tinged with blood, the addition of ten drops (very gradually increasing the quantity) of the diluted nitric acid may be made to the fluid injected, repeating or declining the operation, as the effects are discovered to be advantageous or prejudicial.
In an irritable state of the bladder depending on some disease of the kidney, there is a frequent desire to void the urine without there being any, or but very little, urine in the bladder. There is also a severe cutting pain felt about the neck of the bladder, especially after each effort to make water, followed or attended by a “languid” pain in the loins. The urine is often the color of whey, at other times tinged with blood, and deposites, when suffered to remain a while, a purulent sediment. The severe symptoms should be allayed by the same remedies as prescribed in irritable bladder arising from other causes; but the original seat of the disease in this instance demands energetic attention. The various counter-irritants are in great requisition; leeches, blisters, setons, &c.
In an irritated bladder due to a kidney issue, there's a frequent urge to urinate even when there's little to no urine in the bladder. There's also a sharp pain around the neck of the bladder, especially after trying to urinate, which is followed by a dull ache in the lower back. The urine often looks like whey, and at times, it may be tinged with blood; if left to sit, it develops a purulent sediment. The severe symptoms should be treated with the same remedies used for an irritated bladder from other causes, but the original source of the problem in this case needs thorough attention. Different counter-irritants are heavily used, including leeches, blisters, setons, etc.
In addition to the tonics and astringents already advised, an infusion of the wild-carrot seed, made by macerating for a couple of hours one ounce of the seeds bruised in a pint of boiling water (drinking, when cool and strained, the whole of the liquid in divided doses during the day), may be taken with every chance of relief. As in the other infusions, the patient must persevere in the use of this for some time.
In addition to the tonics and astringents already suggested, an infusion of the wild-carrot seed can be made by soaking one ounce of bruised seeds in a pint of boiling water for a couple of hours (drink the entire liquid in divided doses throughout the day when it's cool and strained). This may provide a good chance of relief. Like the other infusions, the patient should continue using this for a while.
The reader will allow that it can not be for want of materials to produce a book, that this subject is introduced, as the multifarious nature of this work’s contents will readily testify; but it is briefly to explain certain probabilities and conjectures which the afflicted curious are generally desirous of being satisfied upon. Who ever suffered under syphilis but was solicitous to know how such a plague came into the world? Many moralists believe and insist that it is a specific punishment, sent for our physical transgressions. Philosophically speaking, such it is; because the infringement of any natural law always incurs a penalty. However, if it be a manifestation of divine displeasure, it certainly is most unequally apportioned; for it generally happens to the least licentious, instead of the most depraved—the timid, scrupulous, and nervous man, contracting it on the first loose intercourse, whereas the man of the town revels almost with impunity; and, lastly, he who exercises the greatest caution and cleanliness escapes it altogether, although he may be the most deserving of the infliction. In a state of timorous excitement, we are more apt to catch the latent mischief. The careless, thoughtless libertine, hardened against infection by indifference, free living, and probably strong health, often escapes scot-free; and the cool and calculating pleasure-hunter, who exercises those useful antagonists to disease, namely, ablution and selection, comes off triumphant with still greater certainty.
The reader will agree that it's not for lack of material that this topic is being addressed; the diverse range of this work's content proves that. This is meant to briefly clarify certain possibilities and theories that the curious, who are suffering, often want to be informed about. Who hasn't wondered how such a terrible thing as syphilis came to exist? Many moralists believe and assert that it’s a distinct punishment for our physical wrongdoings. Philosophically speaking, it is, since breaking any natural law always comes with consequences. However, if it is a sign of divine anger, it's certainly distributed very unfairly; it usually afflicts those who are the least immoral, rather than the most wicked—the shy, careful, and anxious person who contracts it after the first risky encounter, while the city dweller seems to enjoy himself with little consequence; and, finally, the one who is the most cautious and clean often stays unaffected, even though they might be the most deserving of the affliction. In a state of nervous excitement, we're more likely to catch the hidden dangers. The careless, reckless libertine, shielded from infection by apathy, indulgent habits, and likely good health, often escapes without issue; and the calm, strategic pleasure-seeker, who practices those helpful defenses against disease, like cleanliness and careful choice, comes out ahead with even more certainty.
The point at issue is, when the disease first arose, and where. Medical historians give credit to America, Spain, and France, for its propagation; and controversies have been carried on by various parties, each disclaiming the honor. Now, as I do not propose to analyze the authorities, but simply to venture my own opinion, with the reasons for the same, I have no alternative but to refer the reader, if he be dissatisfied with my attempted exposition, to more comprehensive and elaborate conjectures than my own. Starting upon the proposition that nature’s laws[80] are unalterable, and believing that fever is, and has been fever since the creation of the world; that a cut finger has healed by the first intention, or has festered, and ever may do so—each condition being modified by the state of health of the party, and the nature of the wound; that a broken limb was attended with the same consequences in the year 1 as it will be in the year 1900; and that dirtiness generated itch, and does so still: I can not reconcile myself to any other belief, but that any violation of the laws whereupon sexual intercourse has been permitted, has been, is, and will be, attended with corresponding results; and as such violations most likely exist where numbers cohered together, I consider both gonorrhœa and syphilis to have been coeval with the origin of mankind. They both doubtlessly are much modified by climate, habits, and constitution; and therefrom ensue the many modifications we see in Europe, and the other large portions of the globe. The proofs that can be adduced in favor of this hypothesis are interminable.
The main issue is, when and where the disease first appeared. Medical historians credit America, Spain, and France for its spread, and various groups have argued over who should take the blame, each denying any responsibility. Now, since I don't intend to analyze the experts but simply share my own opinion along with my reasoning, I can only suggest that readers, if they are unsatisfied with my explanation, look to more extensive and detailed theories than my own. Starting with the idea that the laws of nature are unchangeable, and believing that fever has always been fever since the beginning of time; that a cut finger has either healed quickly or has festered, and can do so at any time—each situation being affected by the person's health and the type of injury; that a broken bone had the same implications in the year 1 as it will in the year 1900; and that dirtiness causes itch, and still does: I can't accept any other belief than that any breach of the natural laws governing sexual intercourse has been, is, and will be followed by similar outcomes; and since these breaches likely occur where large groups gather, I believe that both gonorrhea and syphilis have existed since humanity began. They are both certainly influenced by climate, habits, and genetics, leading to the various forms we see in Europe and elsewhere around the world. The evidence supporting this hypothesis is endless.
It is said that, until the arrival of some British sailors at Otaheite, the disease was unknown in that territory. Possibly, in its present modification; but previously to this new intercourse, it is most probable that the sexual cohabitation was not so promiscuous or frequent, and that that very infringement entailed a new form of irritation. In married persons, of even temperate passions, and of most careful habits, local sexual disorders are of frequent occurrence, the slightest derangement of female health giving rise to vaginal disturbance, that unsuspectingly is increased by the marital embrace, and communicated to the husband; and only from its presence does it occur, that the coitus may have been the cause of it. By attending to the simple suggestion of nature, namely, abstinence, cleanliness, and rest, a cure is effected; but where neglected, or should either party be unfaithful to the marriage vow, the disease becomes magnified, and extended to, mayhap, innocent parties.
It’s said that until some British sailors arrived at Otaheite, the disease was unknown in that area. It’s possible that in its current form it wasn’t there before; however, before this new contact, it’s likely that sexual relationships were not as casual or frequent, and that violation of these norms led to a new kind of irritation. In married couples, even those with moderate desires and careful lifestyles, localized sexual disorders are quite common. The slightest disruption in a woman’s health can lead to vaginal issues that are unknowingly worsened by sexual intercourse, which can then be transmitted to the husband. This can lead one to think that it’s the act of intimacy that caused the issue. By following the basic advice of nature, which includes abstinence, cleanliness, and rest, a cure can be attained; but when these are ignored, or if either partner is unfaithful to their marriage vows, the disease can become more severe and spread to possibly innocent parties.
The next question is, are gonorrhœa and syphilis identical? Certainly not, any more than the very many modifications of generative sores. It is absolutely, now-a-days, a difficult question to solve, whether this or that be syphilis; so numerous and yet so closely in resemblance are the ulcers that ensue after sexual cohabitation. The eye is not to be trusted, because so different is real from[81] spurious syphilis that the French surgeons decide the point by inoculating a healthy portion of the body with the matter or discharge from what they suppose to be a syphilitic ulcer. If a corresponding ulcer be produced, the disease is decided to be syphilis. If, on the other hand, no result follow, the patient is proclaimed free from that malady, and stated to be laboring under merely common local irritation. What is still more curious is this: a patient will have ulcers, which every medical man will pronounce, on beholding, to be chancres; yet, upon this trial, the inoculation will not evince them to be so. A while after, supposing the chancres to be healed, secondary or other symptoms will show themselves—sore throat, spotted skin, glandular enlargements, or painful joints, follow. The same consequences oftentimes ensue after gonorrhœa. The primary diseases can not be identical, because the symptoms are vastly different, and the parts attacked are also unlike; and yet there is this anomaly, that the after-consequences frequently closely resemble each other.
The next question is, are gonorrhea and syphilis the same? Definitely not, any more than the many variations of genital sores. Nowadays, it's pretty challenging to determine what is or isn’t syphilis; the ulcers that occur after sexual contact are so numerous and similar to each other. The eye can't be trusted, because real syphilis is so different from fake syphilis that French surgeons settle the matter by inoculating a healthy part of the body with the discharge from what they think is a syphilitic ulcer. If a matching ulcer appears, they confirm it's syphilis. If nothing happens, the patient is declared free of that disease and said to have just a common local irritation. What’s even more interesting is this: a patient might have ulcers that every doctor would immediately identify as chancres, yet this test won't show them to be so. Later on, assuming the chancres have healed, secondary or other symptoms will appear—such as a sore throat, a spotted skin rash, swollen glands, or painful joints. The same thing often happens after gonorrhea. The primary diseases can’t be the same because the symptoms are vastly different, and the affected areas are also different; and yet there’s this oddity that the later consequences often resemble each other closely.
Another surprising result from loose intercourse is, that one female will convey to this individual gonorrhœa, to another syphilis; a third will escape scatheless, and a fourth will have a modifiable affection of both diseases. A satisfactory exposition of the why and wherefore such things should be, or are, is I fancy beyond the skill of pathologists. It is enough to know that they happen; and it is better to use those means which past and daily experience furnishes to get rid of them, than to ponder and wonder in the vain endeavor to explore their origin.
Another surprising result from casual sex is that one female can transmit gonorrhea to one individual, while another can pass on syphilis; a third might come through unscathed, and a fourth could experience a mix of both diseases. I think a satisfying explanation for why this happens is beyond the capability of pathologists. It's enough to know that it occurs; and it's better to use the methods that past and daily experience provide to address these issues than to ponder and wonder in a futile attempt to uncover their origins.
In giving an opinion that we have always been liable to fever, to cut fingers, and to syphilis, I am ready to admit that these several conditions depend upon the varied states of health of the parties. The fevers (ensuing upon the ill-ventilated places) of olden times, compared with those of the present day, differ in intensity and frequency, because the causes are neither so numerous nor severe. The cut finger of a drunkard, and one of otherwise feeble health, is more likely to fester, and even mortify, than should the accident befall a temperate and healthy individual; and the syphilis (or diseases simulating it) at the present time is less severe than formerly, owing to greater attention being paid to personal cleanliness, and the simplicity and earliness of the treatment.
In my opinion, we've always been at risk for fever, cuts, and syphilis. I recognize that these conditions depend on the varying health states of individuals. The fevers that used to arise from poorly ventilated areas in the past are different in intensity and frequency from those we see today because the causes are not as numerous or severe. A cut finger from a drunkard or someone in poor health is more likely to get infected or even lead to serious issues than if it happens to a sober and healthy person. Additionally, syphilis (or diseases that resemble it) today is less severe than it used to be because people pay more attention to personal hygiene and receive simpler and earlier treatment.
A question worthy of inquiry is, why gonorrhœa and[82] syphilis should be infectious? Contagion is a word that many medical men would expel from worldly usage, not believing in its existence; that is to say, the extension of a fever or epidemic, for instance, is not traceable to the disease seizing the individual, but to the peculiar aptitude of the party to become the recipient of it. Consumption is of the most extensive prevalence; but it only occurs in the delicate—those peculiarly formed, or rendered apt for it, from the circumstance of their lungs being hereditarily feebly constructed, or disordered through inflammation following a cold, and which effects are traceable to an infraction of some of nature’s laws. Sickly children owe their condition to their sickly parents, or to their physical mal-education, or some other positive violation of nature’s regulations; and in like manner, where the fire rages or the wind blows, the feeblest and least protected become the earliest victims. Both gonorrhœa and syphilis furnish a remarkably irritating purulent fluid, which, applied to delicate surfaces, produces certain effects. Experiments have not been made to multiply these effects, beyond those incurred by sexual freedom; and the one of inoculation by the French surgeons, as quoted; but accident has proved that the eye, for instance, puts on, after contact with the discharge of gonorrhœa, the same kind of inflammation as follows its contact in coition with the antagonist generative organs.
A question worth asking is why gonorrhea and [82] syphilis are infectious. The term contagion is one that many medical professionals would eliminate from common use, as they do not believe it exists; that is to say, the spread of a fever or epidemic, for example, is not linked to the individual being affected by the disease, but rather to that person's specific susceptibility to it. Tuberculosis is widely prevalent, but it mainly affects those who are delicate—those who are either naturally predisposed due to hereditary weak lungs or those whose lungs have become damaged from inflammation after a cold, which results from a violation of certain natural laws. Sickly children are often a result of having sickly parents, or due to poor physical development, or some other infringement of nature's rules; similarly, where there is fire or strong winds, the most vulnerable and least protected individuals become the first victims. Both gonorrhea and syphilis produce a highly irritating pus-like fluid that causes specific effects when applied to sensitive areas. Experiments have not been conducted to increase these effects beyond those caused by sexual activity; and there was one instance of inoculation by French surgeons, as noted; but it has been observed that the eye, for example, develops the same type of inflammation after contact with gonorrheal discharge as it does after contact during sexual intercourse with opposing reproductive organs.
The rectum has also been the seat of venereal affection; and instances have been known of the mouth being also the recipient of disease communicated by a deposition of the poison. If there be such a thing as contagion, it certainly exists in the venereal disease; for, although I admit it (the disease) may occur spontaneously, or be generated by half a dozen of each of the sexes herding and cohabiting together, and neglecting the duties of cleanliness, or committing excesses, those very circumstances imply that the disease can be extended, notwithstanding a majority of the careful and hardy may escape, after a risk of the same. The fact of its contagious properties is not upset, because escape is owing to the non-susceptibility of the parties, and the caution they exercise to prevent a lodgment of, or contact with, the poisonous matter.
The rectum can also be a site of venereal disease; there have been cases where the mouth has also contracted the disease through exposure to the toxin. If contagion exists anywhere, it is definitely in venereal diseases; although I acknowledge that these diseases can occur spontaneously or arise when multiple people of both sexes are living together, neglecting cleanliness or indulging in excess, these situations suggest that the disease can spread, even if most careful and resilient individuals manage to avoid it after taking risks. The existence of its contagious nature is not negated by those who escape it, as their avoidance is due to their lack of susceptibility and the precautions they take to avoid contact with the toxic substance.
John Hunter observes, that it is only the developed disease that is communicable, and for the propagation of venereal affections the poisonous secretion must be deposited.[83] So confident was he of this, that he even permitted married men having gonorrhœa to cohabit with their wives, to save appearances; care being taken first to clear all the parts of any matter, by syringing the urethra, then making water, and, lastly, washing the glans. Such, however, is my belief of the rapidity of the formation of the secretion, that, aided by the excitement of the generative act, the deposite of the same would necessarily take place with the seminal emission, especially in persons of full temperament, and in the plenitude of the sexual appetite, and thereby be liable to communicate the disease.
John Hunter notes that only the fully developed disease can be transmitted, and for sexually transmitted infections, the toxic secretion needs to be transferred.[83] He was so sure of this that he even allowed men with gonorrhea to have sex with their wives to maintain appearances. Before doing so, they would first clear any discharge by flushing the urethra, then urinating, and finally cleaning the head of the penis. However, I believe that the secretion forms so quickly, especially when combined with the excitement of sexual activity, that it would inevitably occur along with the ejaculation, particularly in individuals with a strong sex drive, making it likely to spread the disease.
It is becoming a prevalent fashion to give new names to the several forms of venereal disease, such as substituting “urethritis,” “blenorrhagia,” &c., for gonorrhœa; and even to syphilis are added “tertiary symptoms;” the names quoted being selected to express more symptoms than the old ones conveyed. I consider that this circumstance tends to support my opinion—that gonorrhœa and syphilis are not identical, and that each disease (the former being distinguished by urethral discharges, and the latter by ulcers and other cutaneous disfigurements) has innumerable varieties. I hold them both to be but modifications of inflammation from a poisonous source, and its consequences common to the structures in which they respectively become seated, and differing in degree according to the severity of the attack. Another proof in support of the last assertion is, I think, the time of the appearance of the particular disease. There is certainly a more usual time for a clap to manifest itself, such as from the seventh to the ninth day; but it very often occurs within twenty-four hours after connexion, and syphilis sometimes as early; and instances occur where weeks elapse before either of the forms shows itself.
It’s becoming common to give new names to different types of sexually transmitted diseases, like using “urethritis,” “blenorrhagia,” etc., instead of gonorrhea; and even syphilis now includes terms like “tertiary symptoms.” These names are chosen to describe more symptoms than the older terms did. I believe this fact supports my view that gonorrhea and syphilis are not the same, and that each disease (with gonorrhea marked by urethral discharges and syphilis by sores and other skin issues) has countless variations. I see both as different forms of inflammation from a toxic source, with outcomes that affect the areas where they occur, differing in severity based on how intense the infection is. Another piece of evidence for this perspective, I think, is when the particular disease shows up. There’s generally a typical timeframe for gonorrhea to show up, usually between the seventh and ninth day; however, it often appears within twenty-four hours after sexual contact, and syphilis can show up just as quickly; there are also cases where it takes weeks for either to manifest.
Briefly to recapitulate, I consider, then—1. That the generative organs have ever been liable to disease from misuse; that the disease is variable and modifiable by many circumstances, such as have been before stated—namely, climate, age, constitution, and cause. 2. That it is contagious; mild cases usually producing mild consequences, but those depending much upon the treatment and health. 3. Newly-indisposed and severer cases, establishing a worse form of disease, alike modifiable by circumstances. I am not prepared to insist that the syphilis of the present time assumes the aspect as it did with the[84] ancients, any more than I would affirm that it will be the same centuries hence: but I contend that all abuses of sexual pleasures will be surely followed by sexual disturbances, and that the most likely form of ailment is marked either by discharges or ulceration; that these diseases are simple or complicated, and all are separate in themselves. There is no fixed order in which what are called secondary symptoms occur. It may more usually happen that a sore throat will follow the healing of a bubo, as swelled testicle is more commonly subsequent to the occurrence of a gonorrhœal discharge; but in very many cases neither occur, or not in the succession stated. The anomalies in the disease I shall consider in describing the symptoms and treatment, when the reader will judge how far the view herein entertained, as to the origin and character of the disease, facilitates and simplifies its management and control.
To summarize briefly, I believe that: 1. The reproductive organs have always been prone to disease from misuse; this disease can vary and be influenced by many factors, such as climate, age, constitution, and cause. 2. The disease is contagious; mild cases typically lead to mild outcomes, but this largely depends on treatment and overall health. 3. Newly affected and more severe cases can lead to a worse form of the disease, which can also be modified by circumstances. I’m not claiming that syphilis today looks the same as it did in ancient times, nor can I say it will remain unchanged for centuries. However, I maintain that all abuses of sexual pleasure will inevitably lead to sexual issues, and the most common symptoms are often linked to discharges or ulcerations. These diseases can be simple or complicated, and they are distinct from one another. There is no set order for what are called secondary symptoms to appear. It’s more common for a sore throat to come after a bubo heals, just as a swollen testicle tends to follow a gonorrheal discharge; yet in many cases, neither occurs, or not in the order I mentioned. I will discuss the variations in the disease when describing the symptoms and treatment, allowing the reader to assess how well the perspective shared here regarding the disease's origin and nature aids in its management and control.
In conclusion of this part of our subject, I may state, that I believe the form and severity of any syphilitic disease depend more upon the state of health and other aptitudes of the party receiving, than of the one communicating the disease.
In conclusion of this part of our subject, I believe that the form and severity of any syphilitic disease depend more on the health and other traits of the person receiving it than on the person transmitting the disease.
Of the Character of the Syphilitic Poison.—“The venereal poison is only known by the action which follows its application.” It has been observed, that it is only communicable by deposition; and that certain parts are essentially prone to its reception: these are the generative apparatus of both sexes. The poison is conveyed in the form of a purulent fluid; that of gonorrhœa from inflamed vessels with corresponding morbid action; that of syphilis, also from a purulent fluid emanating from the surface of an ulcer. The disease prevails only in the human race; it is impossible to transfer it to animals of a lower kind. John Hunter soaked lint in matter from a gonorrhœa and chancre, and introduced it into the vaginæ of bitches and asses without producing any effect. The same experiment was tried by interposing the purulent matter within the prepuce of dogs and male asses, and also by inoculation, but with no other effect than that of producing a common sore. The venereal poison attacks the human body in two ways, locally and constitutionally; the latter by absorption of the poison secreted by the patient himself. We can only suppose the local form of the disease to arise from absorption, and so altering the local action of parts[85] as to produce specific results. The constitutional form is generally an after-occurrence, although instances are known where it has not been preceded by any apparent previous form; albeit, no doubt such has existed without exciting observation. Gonorrhœa shows itself without abrasion of surface; but syphilis is marked by another action—an ulceration of the solids whereon it is found.
The Nature of Syphilitic Poison.—“The venereal poison is only identified by the effects that follow its exposure.” It has been noted that it can only be transmitted through direct contact, and that certain areas are particularly susceptible to it: these include the reproductive organs of both males and females. The poison is transmitted as a purulent fluid; gonorrhea comes from inflamed blood vessels with corresponding disease activity, while syphilis also derives from a purulent fluid that comes from the surface of an ulcer. This disease exists only among humans; it cannot be passed on to lower animals. John Hunter soaked lint in pus from gonorrhea and chancres, then introduced it into the vaginas of female dogs and donkeys without any effect. The same experiment was repeated by placing the purulent matter under the skin of male dogs and donkeys, as well as by inoculation, but only resulted in producing a common sore. The venereal poison affects the human body in two ways: locally and systemically; the latter occurs through the absorption of poison secreted by the infected individual. We can only speculate that the local form of the disease arises from absorption, which alters the local activity of tissues[85] to create specific results. The systemic form typically happens afterward, although there are cases known to occur without any obvious prior manifestation; nonetheless, it's likely that such has existed without drawing attention. Gonorrhea can manifest without any surface abrasion; however, syphilis is characterized by another symptom—ulceration of the tissues where it appears.
In Hunter’s Work on the Venereal Disease, there is an interesting chapter respecting the source of the gonorrhœal secretion, in which it appears that it is produced from the vessels investing the mucous membrane of the urethra, by their becoming altered in their action; and that ulceration is seldom found within the urethra, and when so discovered, it is not from the gonorrhœal poison; and that where ulceration occurs, it must be ascribable to an accession of inflammation of a distinct character. Both gonorrhœa and syphilis are conditions assumed by the human frame in self-defence, and are processes set up to cure the previous one; and unless the constitution be much impaired, the disease gets well. Such impediments, however, exist in the form of moral and social arrangements, occupation and variable health, that the end, without assistance, is seldom accomplished. Gonorrhœa may cease of its own accord; but, according to the belief of Hunter, syphilis never; and certainly every day’s experience proves the fact. We see gonorrhœa cured by the most ignorant persons and by the most empirical measures; but syphilis often defies the most skilful treatment. The first attack of venereal affections, especially gonorrhœa, is the most severe; from which it is presumed that a habit of reconciliation takes place between the disease and the generative organs; so that after a recurrence or two of the complaint, the same party may almost bid defiance to a new infection. Yet, if a man lose the habit obtained by frequent intercourse, through abstinence from venereal pleasures, he will be very likely to contract the disease even on the first re-essay, with the very same parties, who may preserve precisely the same condition of health that formerly was innocuous to him. Cases innumerable can be adduced in support of this statement. In the first part of this book, statements have been made, proving that the difference in the symptoms of gonorrhœa are almost endless. The same may be anticipated with regard to syphilis.
In Hunter's work on venereal diseases, there's an interesting chapter about the source of gonorrheal secretion. It explains that this secretion comes from the vessels surrounding the mucous membrane of the urethra, which change their function. It also notes that ulceration is rarely found in the urethra, and when it is present, it's not caused by the gonorrheal poison. If ulceration occurs, it should be attributed to a different type of inflammation. Both gonorrhea and syphilis are responses the human body creates in self-defense and are processes initiated to heal the previous condition. Unless the body is significantly weakened, the disease tends to resolve on its own. However, barriers such as moral and social factors, work and varying health often prevent this resolution without help. Gonorrhea may resolve on its own, but according to Hunter, syphilis never does, and daily experiences confirm this. We often see gonorrhea cured by untrained individuals using the most rudimentary methods; however, syphilis frequently resists even the most skilled treatments. The first instance of venereal infections, particularly gonorrhea, is usually the most intense, suggesting that the body develops a sort of tolerance toward the disease and the reproductive organs. After experiencing the complaint a couple of times, a person might find it much harder to catch a new infection. Yet, if someone loses the immunity gained through frequent sexual activity due to abstinence, they are likely to contract the disease again even after resuming with the same partners, who may be in the exact same state of health that previously posed no risk. Countless cases can support this claim. In the first part of this book, we've provided evidence showing that the variations in gonorrhea symptoms are nearly endless. The same can be expected regarding syphilis.
Syphilis is another and a more violent form of the venereal disease than gonorrhœa. All its effects and symptoms are divided into two conditions, primary and secondary; the former being those which arise either from the direct application of the virus or poison to the part where the ulceration first shows itself, or from the irritative and specific effects of the poison on the absorbent vessels and glands, as it is passing through them on its way to the circulation.
Syphilis is a more severe form of the sexually transmitted disease compared to gonorrhea. Its effects and symptoms are categorized into two stages: primary and secondary; the primary stage includes the reactions that occur either from the direct contact with the virus or toxin at the site where the ulcer appears, or from the irritative and specific effects of the toxin on the lymphatic vessels and glands as it moves through them on its way to the bloodstream.
Hence, among the first—the primary—may be classed the ulcer, or chancre, which in almost every instance is situated on the parts of generation, and may or may not be followed by a swelling in the glands of the groin, constituting that form of the complaint called bubo.
Hence, at the top of the list—the primary one—can be classified the ulcer, or chancre, which in almost every case is located on the genitals, and may or may not be accompanied by swelling in the groin glands, leading to a form of the condition known as bubo.
The secondary symptoms may be defined to be all those effects of the disease which take place subsequently to, and in consequence of, the absorption of the poison into the system: comprising sore throat, cutaneous affections—both eruptions and ulcers, pains in the bones and joints, and swellings thereon, called nodes.
The secondary symptoms can be described as all the effects of the disease that occur after and because of the poison being absorbed into the body. This includes a sore throat, skin issues—both rashes and ulcers, pain in the bones and joints, and swelling in those areas, known as nodes.
I will first consider the symptoms of primary syphilis—chancre and bubo.
I will first look at the symptoms of primary syphilis—chancre and bubo.
The coverings and linings of the body differ according to their situation. The former, the integuments become hardened by exposure and exercise, and preserve their velvety softness where protected by clothing, and where they are subject to less use—instance the hands, feet, face, and abdomen. Certain functions are assigned to each. The covering of the feet takes on a horny hardness, and in like manner the hands of a laborer assume a glove-like protection. The abdomen, by being constantly clothed, preserves its soft texture. The lining membranes of the body have also separate offices to perform—the serous and mucous, as they are called. The serous is a name given to those lining the cavities; the mucous, to those having outlets. From the glans penis being generally covered by the prepuce, the parts in contact are called mucous. It differs, however, in sensitiveness, from the urethra. The entire covering also of the penis is of a very delicate and tender structure; and hence also, from sexual intercourse, these parts become the chief seat of syphilis. Gonorrhœa[87] confines its attacks to mucous membranes, or, in other words, secreting surfaces. In fact, the matter deposited on the common and exposed skin is harmless; so also, but to a less degree, is that of syphilis. Gonorrhœa is frequently seated on and around the glans, and the inner surface of the prepuce; but more frequently, by a hundred fold, within the urethra. The delicate surface, then, of the glans and prepuce, losing some of its sensitiveness by frequent exposure, and losing also the defence of the secretion which mucous membranes pour out, becomes accessible to an occurrence of syphilis—a disease that is readily communicable, by inoculation, to almost any part of the body. To quote Hunter, he says: “It is an invariable effect, that when any part of an animal is irritated to a certain degree, it inflames and forms matter, the intention of which is to remove the irritating cause. This has been before stated; but it is common only to secreting surfaces; and when the same cause is applied to non-secreting surfaces, ulceration is set up. This is not only the case in common irritation, but also in specific cases, as in syphilis, burns,” &c.
The coverings and linings of the body vary based on their location. The outer layer, or integuments, becomes tougher due to exposure and physical activity, while they maintain a soft, velvety feel in areas protected by clothing or used less frequently, like the hands, feet, face, and abdomen. Each area has specific functions. The covering of the feet develops a tough, hardened layer, and similarly, the hands of someone who works with them gain a glove-like protection. The abdomen, being constantly covered, keeps its soft texture. The lining membranes of the body also have distinct roles—the serous and mucous membranes. The serous membranes line the cavities, whereas the mucous membranes have openings. The part of the penis (glans) that is usually covered by the foreskin is considered mucous. However, it differs in sensitivity compared to the urethra. The entire skin covering the penis is delicate and tender, making it a primary site for syphilis during sexual intercourse. Gonorrhea[87] targets mucous membranes, or secreting surfaces. In fact, the substance deposited on regular, exposed skin is harmless; the same is somewhat true for syphilis. Gonorrhea often affects the surface on and around the glans and the inner surface of the foreskin; however, it is much more commonly found within the urethra. The delicate surface of the glans and foreskin loses some sensitivity with frequent exposure and also loses the protective secretion that mucous membranes produce, making it vulnerable to syphilis—a disease that can easily spread through contact to almost any part of the body. To quote Hunter, “It is a constant effect that when any part of an animal is irritated enough, it becomes inflamed and produces pus to eliminate the cause of irritation. This has been previously mentioned; however, it is only typical of secreting surfaces. When the same irritation occurs on non-secreting surfaces, ulceration starts. This happens not just with common irritation but also with specific cases, like syphilis, burns,” etc.
It is somewhat difficult to explain how a chancrous sore is produced. Surmises are at our service, and those which are founded upon certain facts are the more likely to be true. For instance, a person receiving syphilis must contract it from another individual having it. The mere solitary act of coition will not spontaneously produce it, provided the party be clean, for that surely is not an excess; but having connexion with an infected one, and thereby exposing a healthy surface to a diseased one, becomes an infraction of one of nature’s laws. Well, the patient contaminating the other must have a chancre, which giving off, by contact, its morbid secretion, produces a specific result, namely, a small pimple.
It's somewhat challenging to explain how a chancre develops. We have our theories, and those based on certain facts are more likely to be accurate. For example, someone with syphilis must get it from another person who has it. Just a single act of sex won't cause it to develop, provided the person is healthy, as that isn't inherently excessive; however, having intercourse with an infected person and exposing a healthy area to a diseased one violates one of nature's laws. So, the person who spreads the infection must have a chancre, which, through contact, releases its harmful fluid and leads to a specific result: a small pimple.
In men, the disease is generally contracted upon the frænum, glans penis, or prepuce, or upon the common skin of the body of the penis, but most frequently upon the interior. From the peculiar and alterable structure of the penis and its prepuce, the poison, unless well washed off, is apt to lodge in the folds thereof, and sooner or later it manifests its influence, which may occur in twenty-four hours, or may be withheld for months. Generally, however, seven or eight or nine days puts the patient out of suspense. The first symptoms consist in an itching, succeeded[88] by a redness of the part, out of which is soon observed to spring up a small elevation or pimple. In connexions where haste, disproportion of size, or much excitement or excess prevails, an absolute abrasion of the skin often takes place, and the parts where such occur are generally the everted portion of the prepuce, or the frænum of the same.
In men, the disease usually develops on the frænum, glans penis, or prepuce, or on the regular skin of the penis body, but most often on the inside. Because of the unique and changeable structure of the penis and its prepuce, the poison, unless thoroughly washed away, tends to get trapped in its folds, and eventually it shows its effects, which can happen within twenty-four hours or may take months. Generally, though, it takes about seven to nine days for the patient to stop worrying. The initial symptoms include itching, followed by redness in the area, and soon a small bump or pimple appears. In situations where there’s urgency, size differences, or too much excitement or excess, the skin can often get worn away, and the areas where this happens are usually the everted part of the prepuce or the frænum of the same.


The accompanying drawings represent the extent of the redness and the first appearance of the pimple. The upper diagram alludes to the irritation and excoriation around the frænum, and the lower, the first evidence of a chancre. I am describing the most common form of chancre, such as is known in the profession as Mr. Hunter’s chancre. A perceptible hardness next ensues round the pimple, which becomes more elevated when it ulcerates, or, in other words, the head gets broken off and a little hollow is left. The tumor (for such it may be called) is generally of a limited circumference, seldom exceeding the size of a silver penny, unless in an advanced stage of the disease. When a chancre attacks the frænum, and undermines it, as it were, the frænum is often destroyed; and of course, with its destruction, departs its property of controlling or of directing the orifice of the urethra in urinating, or in the emission of the semen.
The accompanying drawings show the extent of redness and the initial appearance of the pimple. The upper diagram refers to the irritation and scratching around the frenum, while the lower one illustrates the first sign of a chancre. I'm describing the most common type of chancre, known in the medical field as Mr. Hunter’s chancre. A noticeable hardness follows around the pimple, which becomes more raised when it ulcerates, meaning the top breaks off and leaves a small cavity. The lump (as it can be called) is usually small, rarely larger than a silver penny, unless the disease has progressed. When a chancre affects the frenum and undermines it, the frenum can often be destroyed; consequently, with its destruction, it loses its ability to help control or direct the opening of the urethra during urination or the emission of semen.

This drawing exhibits three ulcers: one on the prepuce, another under the frænum, having eaten its way through, as marked by the black cross-line, and the third situated on the glans.
This drawing shows three ulcers: one on the foreskin, another beneath the frenulum, which has eroded through, as indicated by the black cross-line, and the third located on the glans.
When the pimple appears on the outside of the prepuce for instance, it assumes generally a larger form, and, as the head is broken off, crust after crust rises up, until the process of ulceration has very far advanced, or the applications that are generally employed prevent its re-formation. In the former instance, the[89] crusts are attributable to evaporation of the discharge; in the latter, their absence is already explained by the prevention of the same. There is such a thing as sympathy in eruptive disorders. In skin affections of the corners of the mouths of children, we often see the inflammation cross from corner to corner. The same is observable where the attacks comprise the angle of an eye. So is it with the penis, a structure equally as delicate; and accordingly the edges of the prepuce often put on a jagged appearance resembling chaps on hands.
When a pimple appears on the outside of the foreskin, it usually forms a larger bump, and as the top breaks off, layer after layer of crust develops until the ulceration process is quite advanced, or the treatments typically used stop it from coming back. In the first case, the crusts are caused by the evaporation of the discharge; in the second case, their absence is explained by the prevention of the discharge itself. There is a phenomenon of sympathy in eruptive disorders. In skin issues at the corners of children's mouths, we often see the inflammation spread from one corner to the other. The same can be seen when the inflammation affects the corner of an eye. The same happens with the penis, which is also a delicate structure; thus, the edges of the foreskin often take on a jagged look similar to chapped hands.

Witness the above wood-cut. It portrays an ulcer somewhat diffused on the prepuce, and the ragged edge of the same structure. The sketch just introduced was taken from a patient perhaps only a fortnight old with the disease. Being a rackety, dissipated young man, and regardless of the treatment suggested, a week’s neglect produced the following alteration:—
Witness the woodcut above. It shows an ulcer that's somewhat spread out on the foreskin, along with its jagged edge. The sketch just shown was taken from a patient who had the disease for maybe only two weeks. As a wild, carefree young man, he ignored the recommended treatment, and a week of neglect resulted in the following change:—

A new ulcer sprung up, the old one increased in size, and the entire edge of the prepuce became involved in the irritation.
A new ulcer appeared, the old one got bigger, and the entire edge of the foreskin became irritated.
Phymosis and paraphymosis occur in syphilis as they do in gonorrhœa. The treatment is the same in both. Warm, soothing applications are indispensable; and occasionally, to prevent adherence between the glans and prepuce, the scalpel must be had recourse to. I have already expressed my conviction that the progress of the disease rests as much or more upon the condition of the party receiving it, than the specific property of the complaint.
Phimosis and paraphimosis occur in syphilis just like they do in gonorrhea. The treatment is the same for both. Warm, soothing applications are essential; and sometimes, to prevent the glans and foreskin from sticking together, a scalpel may be necessary. I have already shared my belief that the progression of the disease depends as much or more on the condition of the individual affected than on the specific nature of the illness.
“If the inflammation spreads fast and considerably, it shows a constitution more disposed to inflammation than natural; if the pain is great, it shows a strong disposition to irritation. It also sometimes happens that they begin very early to form sloughs; when this is the case, they have a strong tendency to mortification. Bleeding is also[90] a consequence owing to exposure of the ulcered corpus cavernosum.”—Hunter.
“If the inflammation spreads quickly and significantly, it indicates a constitution that is more prone to inflammation than normal; if the pain is intense, it shows a strong tendency towards irritation. Sometimes, they may also start to develop sloughs very early; when that happens, they have a strong tendency towards necrosis. Bleeding is also[90] a result of the exposure of the ulcerated corpus cavernosum.”—Hunter.
The reader will recollect that it has been stated that chancres, like the many symptoms of gonorrhœa, differ in their characteristics. Quoting from authorities, and, as will be further illustrated, the following may be taken as the summary of the most prominent appearances:—
The reader will remember that it has been mentioned that chancres, like many symptoms of gonorrhea, vary in their characteristics. Citing from experts, and as will be further demonstrated, the following can be considered a summary of the most notable appearances:
The ordinary chancre is characterized by a hollow centre, a hard and ragged edge, a yellow surface, with a deposite of tenacious matter, and a red and inflammatory margin. There is also a hardness felt at its base on taking the part up between the fingers. This has already been shown; but as illustrations multiply, the possessor of this publication, especially if he be an invalid, will recognise the annexed. It exhibits the ordinary chancre on the inner part of the prepuce, the glans, and the orifice of the urethra—no unfrequent seat of chancre.
The typical chancre has a sunken center, a firm and jagged edge, a yellow surface with a buildup of thick matter, and a red, inflamed border. You can also feel a hardness at its base when you pinch the area between your fingers. This has already been demonstrated; however, as more examples come up, the person who has this publication—especially if they are unwell—will recognize the attached images. They show the typical chancre located on the inner part of the foreskin, the glans, and the opening of the urethra, which are common places for a chancre to occur.

Many ulcers assume a very indolent form, and remain quiescent for a long period. One patient I knew, who consulted me for rheumatism, and who disavowed ever having had syphilis. He took vapor baths, which assuaged the pain, but did not remove it. Accident discovered to me the existence of a sore on the penis, by observing the dressings of the same, carefully placed on the corner of the mantel-piece in the bath-room. The following was the appearance of the sores. He had endured them for nearly three months, nor had he perceived much alteration, either for better or worse. The disease was properly healed, and he soon got well.
Many ulcers can be very slow to develop and stay inactive for a long time. One patient I saw for rheumatism insisted he had never had syphilis. He took vapor baths that eased the pain but didn't get rid of it. By chance, I found out about a sore on his penis when I noticed the dressings for it carefully placed on the corner of the mantelpiece in the bathroom. This is what the sores looked like. He had been dealing with them for almost three months and hadn't noticed much change, either for better or worse. The disease was properly treated, and he recovered quickly.

Another kind is one denominated the superficial, with raised edges. It is more frequently seated at the upper part of the prepuce, and creating a thickening of it, ending in phymosis, which lasts a long time after the cure of the ulcers. This kind of chancre is sometimes very obstinate, and continues many weeks. The following[91] illustration portrays its presence near the edge of the corona glandis.
Another type is known as the superficial chancre, which has raised edges. It often appears at the upper part of the foreskin, causing a thickening that can lead to phimosis, which lasts for a long time even after the ulcers heal. This type of chancre can be quite stubborn and may persist for several weeks. The following [91] illustration shows its location near the edge of the corona glandis.

There are two other kinds of sores called the phagedenic and sloughing ulcers and chancres.
There are two other types of sores called the phagedenic and sloughing ulcers and chancres.
The phagedenic is a corroding ulcer without granulations. It is also destitute of any surrounding induration, but frequently its circumference is of a livid red color. When the disease is injudiciously treated, the whole of the penis will be destroyed in a very short time. The absence of coloring detracts from a faithful representation of the kind of sore just alluded to. The drawing is sketched from Mr. Skey’s work on Syphilis.
The phagedenic is a deteriorating ulcer without granulations. It also lacks any surrounding hardening, but often its edges are a dark red color. When the disease is improperly treated, the entire penis can be destroyed in a very short time. The lack of color makes it hard to accurately represent the type of sore just mentioned. The drawing is based on Mr. Skey’s work on Syphilis.

|
a—The ulcer. a—The sore. |
Another and more confirmed specimen from the same authority is presented. It represents the sloughing ulcer.
Another confirmed specimen from the same source is presented. It represents the sloughing ulcer.
|
a—The ulcer on the prepuce. The ulcer on the foreskin.
b—The ulcer on the penis. Penile ulcer. |

|
I have witnessed the sloughing, or, in other words, the loss of the entire top of the glans and prepuce, within half a dozen days. The subjoined drawing (overleaf) represents a tumefied state of the penis, ulceration on the glans surrounding the orifice of the urethra, phymosis of the prepuce,[92] and ulcers in different stages on the outside thereof. The sketch was taken from Wallace’s work. Such are often met with. Chancres, as before stated, often become irritable, spread rapidly, and slough, more particularly in persons of intemperate and dissipated habits, or when the case has been improperly treated; and openings into the urethra are formed to a considerable extent, sometimes to the destruction of the glans, or a portion of the penis.
I have seen the shedding, or in other words, the complete loss of the top of the glans and foreskin, happen in just a few days. The drawing below shows a swollen state of the penis, ulcers on the glans around the urethra opening, phimosis of the foreskin,[92] and ulcers at various stages on its surface. The sketch is from Wallace’s work. Such cases are common. Chancres, as mentioned earlier, often become irritated, spread quickly, and shed tissue, especially in people with excessive or reckless habits, or if the condition has been treated incorrectly; significant openings into the urethra can form, sometimes leading to the destruction of the glans or part of the penis.

The illustrative companion to this paragraph exhibits an ulcer that has wormed its way through the prepuce, as marked by the black line.
The accompanying illustration for this paragraph shows an ulcer that has burrowed through the foreskin, as indicated by the black line.

Warts are often met with, as in gonorrhœa, and, like those, will arise from simple local irritation, from the accumulation of the natural secretions, or want of cleanliness. They are hard and soft, and require different treatment accordingly. They are not contagious; that is, they do not communicate a venereal affection, but they very readily produce a similar disease in parts they come in contact with. The story is here well told by the engraver’s aid.
Warts are commonly seen, like in gonorrhea, and can develop from simple local irritation, the buildup of natural secretions, or lack of cleanliness. They can be hard or soft, and each type requires different treatment. They aren't contagious; they don't transmit a sexually transmitted infection, but they can easily cause a similar issue on areas they touch. The engraver effectively illustrates this story.

It often happens that the ulceration appears checked. A tumor (see next page) will form, and the surface will look very red and angry—will even yield a moisture, and finally disappear. I say finally, because it frequently proves very obstinate, and trespasses upon the patience and forbearance almost to induce despair. It usually is very irritable, the itching being most troublesome. The illustration was taken from a patient who had been an invalid several months.
It often happens that the ulceration seems to be under control. A tumor (see next page) will develop, and the surface will appear very red and inflamed—it may even produce moisture, and eventually vanish. I say "eventually" because it often becomes quite stubborn, testing one's patience and endurance to the point of inducing despair. It is usually very sensitive, with itching that can be quite bothersome. The illustration was taken from a patient who had been an invalid for several months.

|
a—The tumor. The tumor. |
After a certain time, varying in proportion to the virulence of the disease, the poison is conveyed by the numerous absorbents (which run from the penis) to the glands in the groin, one or more of which become inflamed and enlarged, producing that well-known swelling, already alluded to, called bubo. Ulcers, too, are sometimes situated within the urethra, as is seen in the annexed cut.
After some time, depending on how severe the disease is, the poison travels through the various vessels that lead from the penis to the lymph nodes in the groin. One or more of these nodes may become swollen and inflamed, resulting in the familiar swelling known as bubo. There can also be ulcers located in the urethra, as shown in the attached illustration.

OF BUBOES.
Surgeons apply the word bubo to inflamed glands from syphilis, wherever they happen to be. The body abounds with absorbents, which are small delicate vessels that form a net-work over the entire surface, and exist also in every structure. Their purpose is to convey the nutriment to the circulation. They form stations, as it were, or points of assemblage; and these are generally situated in the angles of the body—the groin, the armpits, hams, neck, &c.—parts[94] most protected from injury. When skin inflammation is present, to familiarize the meaning, the nearest glands sympathize and swell; as, for, instance, who has escaped a swelling, at one time or other of his life, in the neck, throat, or armpits? When a sore prevails on the penis, or a gonorrhœa exists, there most frequently ensues an enlargement of the glands of the groin. The result of that enlargement depends upon the nature of the inflammation. In gonorrhœa it is merely temporary, not being sufficient to provoke suppuration, or the formation and discharge of matter, or very rarely so; but in the case of venereal ulcers, where the inflammation is so conveyed, the escape from such consequences is as seldom.
Surgeons use the term bubo to describe inflamed glands caused by syphilis, no matter where they occur in the body. The body is full of absorbents, which are tiny, delicate vessels that create a network across the entire surface and are also found in every structure. Their role is to transport nutrients to the bloodstream. They act as stations or gathering points, typically located in the body's corners—the groin, armpits, back of the knees, neck, etc.—areas that are usually well protected from injury. When there is skin inflammation, to illustrate the concept, the nearest glands react and swell; for example, who hasn’t experienced swelling at some point in their life in the neck, throat, or armpits? When there’s a sore on the penis or a gonorrhea infection, there is often swelling of the glands in the groin. The outcome of that swelling depends on the type of inflammation. In gonorrhea, it is usually temporary and typically doesn’t lead to pus formation or discharge, but in the case of venereal ulcers, where the inflammation occurs, avoiding such consequences is quite rare.
The mode which nature adopts to transfer the poison is as inexplicable in its operation as the production of a swelled testicle. Buboes (herein meant), then, are—or I should say a bubo is—a specific inflammation of the glands of the groin. It usually occurs on the same side of the body as the ulcer is situated; but when the ulcer is seated on or under the frænum, there seems to be no fixed rule which side shall have the honor. Another peculiarity is, that they more readily spring up from ulcers on the prepuce than on the glans, and are more attributable to ulcers than merely inflamed surfaces. They do occur sometimes without either being apparent. To facilitate the clear understanding of what we are talking about, a drawing is presented of the inguinal glands, and the absorbents leading to and from it, which conveys but an imperfect idea of the number of the absorbents; but it serves to show the nature of them, and their mode of communication.
The way nature transfers the poison is as mysterious as how a swollen testicle occurs. Buboes (and by that, I mean a bubo) are a specific inflammation of the groin glands. It usually appears on the same side of the body as the ulcer, but if the ulcer is located on or under the frænum, there doesn't seem to be any set rule for which side is affected. Another interesting point is that they are more likely to develop from ulcers on the foreskin than on the glans and are more linked to ulcers than just inflamed surfaces. They can sometimes appear without either being noticeable. To help clarify what we mean, there is a drawing of the inguinal glands and the lymphatic vessels connected to them, which gives an incomplete idea of the number of vessels, but it helps illustrate their nature and how they communicate.

Glands become inflamed from other causes than syphilis; a scratch, a bruise, or any local irritation, will occasion an enlargement of the nearest set of glands, or at least one of them. Scrofula is a specific cause. As the venereal poison carries with it its morbid nature wherever it happens to be conveyed, the glands become infected with it; and hence it is the more readily transferred to the system at large. Very frequently and fortunately the disease terminates in the glands; that is to say, does not extend[95] to the circulation at large. The time that intervenes after absorption has taken place, before bubo manifests itself, is as uncertain as that of chancre appearing after connexion; but generally the party is safe a fortnight after the entire disappearance of the chancre. Where it is otherwise, some trace of irritation on the glans or prepuce is discoverable upon close investigation, or it will follow great fatigue, venereal excesses, &c. If the disease extend to the constitution, it rarely affects other glands than those primarily attacked; and hence it is rare that more than one gland becomes inflamed. Having given the received notions of the cause, the symptoms should next be described.
Glands can get swollen due to reasons other than syphilis; a scratch, a bruise, or any local irritation can cause enlargement in the nearest glands, or at least one of them. Scrofula is a specific cause. Since the venereal poison carries its harmful characteristics wherever it spreads, the glands become infected with it, making it easier for the infection to spread throughout the body. Fortunately, the disease often stays contained in the glands, meaning it doesn’t usually affect the entire system. The time it takes for a bubo to show up after absorption happens is just as unpredictable as when a chancre appears after sexual contact; however, typically, a person is safe at least two weeks after the chancre has completely disappeared. If it’s not the case, there may be some sign of irritation on the glans or foreskin upon close inspection, or it might occur after significant fatigue or sexual excess. If the disease spreads through the body, it rarely affects other glands beyond the ones that were initially affected; therefore, it’s uncommon for more than one gland to become swollen. Now that the established causes have been presented, we should move on to discussing the symptoms.
No person can be unaware of the approach of a bubo. There is seldom much advance of a swelling without pain, which latter may be said to attract the patient’s attention to the part, when a tumor, possibly the size only of a horse-bean, is discovered. If the swelling be venereal, it rapidly increases in size. It is at first moveable, but soon feels as though firmly fixed. There is next experienced inconvenience in walking. If the disease proceed to suppuration, a continued throbbing is felt in the part, which also swells, assumes a diffused redness, and at last an evident sense of fluctuation is perceived. It may be ushered in with a shivering fit. The skin becomes thin and tender, and a conical point protrudes, which, unless punctured, bursts and emits its contents. It is astonishing what immense destruction of parts takes place in large buboes. The theory how solids become converted into fluids—how muscle, fat, and cellular membrane, become absorbed, and a thick purulent secretion deposited, is fitter for a work addressed exclusively to medical men than to the public; and it therefore must suffice that such happen, and few persons are ignorant of the fact; but the modus operandi may at best be but the subject of conjecture.
No one can ignore the onset of a bubo. Swellings rarely appear without pain, which usually draws the patient's attention to the area when a lump, perhaps only the size of a kidney bean, is noticed. If the swelling is due to a sexually transmitted infection, it quickly grows larger. Initially, it's movable but soon feels firmly attached. Then walking becomes uncomfortable. If the condition progresses to pus formation, a persistent throbbing is felt in the area, which also swells, turns red, and eventually shows a definite sense of fluid movement. It may start with a shivering episode. The skin becomes thin and sensitive, and a pointed area appears, which, if not drained, will burst and release its contents. It's shocking how much tissue can be destroyed in large buboes. The explanation of how solid tissues change into liquids—how muscles, fat, and connective tissue are absorbed, and thick pus is produced—is more suitable for a medical textbook than for the general public; so it’s enough just to know that it happens, and most people are aware of this fact. However, the exact process remains largely a matter of speculation.
The artist’s graver has pencilled a faithful picture (see next page) of the appearance of the disease in question. On the right side is represented a bubo that has broken, or discharged its contents, and which is in a state of healing; on the left side a bubo ready to burst; and, by way of economising space, the left testicle is exhibited in a state of varicocele, by no means an unfrequent accompaniment to the previously narrated condition, but at the same time by no means a necessary attendant, it being a[96] totally distinct affection. Buboes present more varieties in their size, and duration, and consequences, than they do on their initiation. Cases in corroboration will be found in their proper place.
The artist's engraver has drawn an accurate depiction (see next page) of the disease in question. On the right side is shown a bubo that has ruptured or released its contents and is in the process of healing; on the left side is a bubo that is about to burst; and to save space, the left testicle is depicted with varicocele, which is often associated with the previously mentioned condition, but is by no means a necessary occurrence, as it is a[96]completely separate issue. Buboes have more variations in their size, duration, and consequences than they do at their onset. Related cases will be found in their appropriate sections.

ON LUES VENEREA, OR SECONDARY SYMPTOMS.
Secondary symptoms are those changes which occur in consequence of the admission of the venereal poison into the system, or common circulation at large. The introduction to the disease of bubo explains the mode of inlet. Like gonorrhœa and primary syphilis, it is often a very complicated complaint. Secondary symptoms are admitted to occur without being preceded by any primary form, as, for instance, by immediate absorption unattended with the irritation which accompanies chancre, or attendant upon bubo; but where one secondary affection arises without the primary, at least many hundred arise subsequent to it; and unless, in the latter instance, treatment, and vigilant too, is adopted, not one in a hundred escapes them.
Secondary symptoms are the changes that happen after the venereal infection enters the body or the general bloodstream. The onset of the disease of bubo illustrates how this happens. Like gonorrhea and primary syphilis, it can often be a very complicated issue. Secondary symptoms can occur without any primary symptoms appearing first, such as when the infection is absorbed immediately without the irritation that comes with chancre or in connection with bubo. However, while some secondary conditions can develop without a primary one, many others will occur after the primary infection. If treatment isn't pursued diligently in these cases, the chances of avoidable complications are slim, with only about one in a hundred managing to escape them.
Lues venerea (a synonymous term with syphilis) is supposed to be imbibed from a very sensitive glans penis, a simple abrasion of the skin of that organ, an ordinary ulcer, or it may be transferred by inoculation. The late John Hunter is certainly the most eminent authority—the vade mecum of professional men. In these matters he was a man of indefatigable perseverance and untiring observation. Few new lights have been thrown on syphilis since his time, except on the treatment, which has become wonderfully simplified.
Lues venerea (another name for syphilis) is believed to be contracted through a very sensitive glans penis, a minor skin abrasion on that area, a common ulcer, or it can be passed on through inoculation. The late John Hunter is undoubtedly the leading authority—the vade mecum for professionals. In this field, he was a man of relentless determination and constant observation. Since his time, there have been few new insights into syphilis, apart from the treatment, which has become significantly simpler.
In thus again adverting to Mr. Hunter’s name, it is[97] chiefly to observe, that the basis of my own thoughts and practice has been built upon his writings; and therefore, in being thus explicit in describing syphilis and its multitudinous varieties, the reader is assured that what is here written is, at all events, well founded, and not compounded of the many new adventurising propositions of the day. Mr. Hunter considered that contamination took place about the beginning of the local complaints; that no person was safe from lues while the original sore was present, and not under treatment; but that, if the seeds of lues were not already implanted in the constitution, the consequences might be averted by treatment. Children are born infected with lues, which they derive from their parents; for instance, a man laboring under secondary, or primary symptoms, cohabits with a healthy female, the female may escape both diseases, but the child may inherit them.
In referring to Mr. Hunter’s name again, it is[97] mainly to point out that my own thoughts and practices are based on his writings. Therefore, by being clear in describing syphilis and its many forms, I assure the reader that what is written here is well-founded and not based on the numerous new and untested ideas of the day. Mr. Hunter believed that contamination occurred at the onset of local issues, and that no one was safe from syphilis while the original sore was present and untreated. However, if the seeds of syphilis were not already present in the body, treatment could prevent the consequences. Children can be born with syphilis, which they inherit from their parents; for example, if a man with secondary or primary symptoms lives with a healthy woman, she may avoid both diseases, but the child may still inherit them.
Instances have been known of children so infected, conveying the disease to the wet nurse, to whose care they may be removed; and, like other infectious disorders, the complaint may be diffused ad infinitum. There is an impression abroad, that, like consumption, healthy persons are obnoxious to the breath and perspiration of the afflicted; but, as in many other conjectures, corroboration is wanted to prove the fact.
Instances have been recorded of children infected with the disease passing it on to the wet nurse who cares for them; and, like other contagious illnesses, the infection can spread ad infinitum. There’s a common belief that, like tuberculosis, healthy people are susceptible to the breath and sweat of those who are ill; however, as with many other ideas, evidence is needed to confirm this.
Syphilis is divided into primary and secondary; but modern pathologists add a third stage, called tertiary symptoms. Hunter used to divide lues into two orders; the first was the most frequent form of the complaint, after chancre and bubo; the second, the remaining symptoms. The former consisted of the affections of the skin, throat, nose, mouth, and tongue; the latter, the bones and their coverings, called the periosteum and the fasciæ of muscles, as explained in the preliminary part of this publication. Lues does not always exhibit itself according to this arrangement; which circumstance explains that the occurrence is more owing to conditions of health, and peculiar tendencies of the structures involved to receive the contamination, than to any properties of the animal poison.
Syphilis is divided into primary and secondary stages; however, modern pathologists include a third stage called tertiary symptoms. Hunter used to categorize syphilis into two types: the first was the most common form, including chancre and bubo; the second encompassed the remaining symptoms. The first type involved issues with the skin, throat, nose, mouth, and tongue; the second involved the bones and their coverings, known as the periosteum and the fasciæ of muscles, as explained in the preliminary part of this publication. Syphilis doesn't always present itself this way; this variation indicates that its occurrence is more related to health conditions and specific tendencies of the affected structures to acquire the infection rather than any properties of the infectious agent.
He considers, also, that the development of the disease depends much upon the state of weather, and the care the patient may bestow upon himself; cold being a formidable predisposer to the extension of secondary symptoms, and[98] that the parts least protected are generally the first to become diseased. Hence the throat usually exhibits a morbid action before the skin, furthermore, upon the cure of the more superficial parts of the body; and, therefore, suddenly suspending treatment, the symptoms manifest themselves in the deeper seated. The deduction from this statement is, a necessity for especial care in the clothing of the body, and the continuance of the treatment some little while after all external evidences of the complaint have disappeared.
He also believes that the progression of the disease is greatly influenced by the weather and the care the patient takes of themselves. Cold weather is a significant factor that can worsen secondary symptoms, and the areas that are least protected tend to become sick first. This is why the throat often shows signs of illness before the skin does. Additionally, when the more superficial areas of the body heal, if treatment is suddenly stopped, symptoms can appear deeper in the body. The takeaway from this is that it's important to pay special attention to how we dress and to continue treatment for a while even after all visible signs of the illness have gone away.
Mr. Hunter considered that the disease may be engrafted in the constitution, and remain dormant for a considerable period, through the parts not being brought into action by any of the aforementioned causes. Ordinary illness, simple fever, excess, fatigue, and a host of other occasions, may excite a particular structure into a morbid condition, when the hitherto dormant disease will sprout out. His arguments are supported by numerous cases wherein several years elapsed between the primary and secondary symptoms, although no new infection was contracted in the intermediate time.
Mr. Hunter believed that the disease might be ingrained in the body's makeup and stay inactive for a long time, as long as the affected areas weren't triggered by any of the previously mentioned factors. Common illnesses, mild fevers, excesses, fatigue, and many other situations can provoke a certain condition into a harmful state, causing the previously dormant disease to emerge. His claims are backed by many cases where several years passed between the initial and later symptoms, even though no new infection occurred in the meantime.
Mercury was Mr. Hunter’s sheet-anchor; his faith in it was to the effect that it would cure every stage of the disease, but that one course of it, although it might cure chancre, would not prevent secondary symptoms. They might not occur, because the poison may not have been carried into the circulation; and in like manner the second stage of the disease need not be followed by a third. But he considered that, when the several forms of the disease betrayed themselves, their origin must be traced to a general contamination of the system at the same time.
Mercury was Mr. Hunter’s go-to solution; he believed it would cure every stage of the disease. However, he thought that one treatment might cure chancre but wouldn’t stop secondary symptoms from developing. These symptoms might not happen if the poison didn’t enter the bloodstream, and similarly, the second stage of the disease might not lead to a third. But he believed that when the various forms of the disease showed up, their cause should be linked to a general contamination of the system happening all at once.
OF THE SYMPTOMS OF THE FIRST STAGE OF LUES.
Six weeks is the time usually allowed to elapse between primary and secondary symptoms; but it is not invariably the case, instances having occurred where the disease has embraced, and most severely, both stages in a fortnight, and others between which a much longer time has existed. The first symptoms of lues consist either of a sore throat or a spotted skin. When the skin is the seat, a red spot, not unlike a flea-bite, is perceived; the color soon dies[99] into a brownish or copper-colored hue. Occasionally, at the outset, a small pimple is observed, which breaks and scurfs; the coppery-colored spot next feels rough, and a kind of scurf will exude that after a few days falls off to make way for more. The disease being more usually slow than rapid in its progress, weeks may be consumed before ulceration occurs, and merely a discoloration of the skin is seen in spots seldom exceeding the size of a sixpenny or fourpenny piece. Some of these spots will nearly disappear, leaving a faint scar, and new ones will spring up. The entire body may be covered with them, but usually those parts nearer the centre of circulation generally possess the most—such as the chest, neck, shoulders, arms, wrists, hands, and head. As the disease progresses, the scurf on the spots accumulates, falls off, re-forms, getting thicker each time, when upon being detached, for they cling now more closely, a sore and moist state of the skin is observable. This may be covered with a new crust, or may at once proceed to suppuration.
Six weeks is usually the time expected to pass between primary and secondary symptoms; however, that's not always the case. There have been instances where the disease has quickly affected both stages within two weeks, and others where a much longer period has passed. The first signs of lues typically include either a sore throat or a spotted skin. When the skin is involved, a red spot that looks somewhat like a flea bite appears; the color soon fades into a brownish or copper tone. Sometimes, at first, a small pimple can be seen, which breaks and forms a scab; the coppery spot then feels rough, and a kind of scab will ooze which falls off after a few days to make way for more. The disease usually progresses slowly rather than quickly, so weeks can go by before ulceration occurs, and often only discoloration of the skin is visible in spots that are rarely larger than a sixpence or fourpence. Some of these spots will nearly fade away, leaving a faint scar, while new ones appear. The entire body may be covered in them, but typically, the areas closer to the center of circulation have the most—like the chest, neck, shoulders, arms, wrists, hands, and head. As the disease advances, the scabs on the spots build up, fall off, and re-form, getting thicker each time. When they detach, they cling more tightly, revealing a sore and moist area of skin. This may be covered by a new crust or may immediately start to ooze.
When an ulcer is formed, it will sometimes spread rapidly, and embrace a patch the size of a crown-piece, when the process of ulceration will assume the vigor of disease.
When an ulcer forms, it can sometimes spread quickly and cover an area as large as a coin, at which point the process of ulceration takes on the intensity of a disease.

The accompanying sketch portrays, perhaps, more the seat of the disease when attacking the upper part of the body, than the appearance; for to give a true portraiture, the drawing should be the size of life, and colored after nature. It is, however, I doubt not, sufficient to exemplify the site of the disorder. The eruption is smaller on the face, and less vicious, generally, than on the body; but it proves most unsightly, and indicates great advancement of the disease. The legs (see next page), and those parts of the skin least vascular, assume a mottled appearance resembling recent bruises; at other times, clusters of spots like grapes hanging together.
The accompanying sketch shows more about where the disease is located when it affects the upper part of the body, rather than what it actually looks like. To truly capture its appearance, the drawing would need to be life-sized and accurately colored. However, I believe it’s enough to illustrate the area of the disorder. The rash is smaller on the face and generally less severe than on the body, but it can look quite unattractive and indicates significant progression of the disease. The legs (see next page) and parts of the skin that are less vascular take on a mottled look similar to fresh bruises; at other times, they form clusters of spots that resemble grapes hanging together.
The shoulders, arms, and wrists, also present a somewhat similar appearance; though perhaps not to the same extent, owing to being more warmly clad, and less in exercise, than the lower extremity.
The shoulders, arms, and wrists also have a somewhat similar look, though maybe not to the same degree, since they are dressed more warmly and are less active than the lower body.
When the disease extends to the hands, it is marked by exfoliations of the palm, with occasional deep cracks that cause much pain. Nor are the fingers and nails exempt from this encroaching malady, which, during its occupation, shows itself by a redness under the nail, that at last ends in the destruction of the nail.
When the disease spreads to the hands, it’s characterized by peeling skin on the palms, along with occasional deep cracks that cause significant pain. The fingers and nails aren’t spared from this advancing condition, which, while it takes hold, appears as redness under the nail, ultimately leading to the destruction of the nail.



The head, also, is a frequent seat of the disorder. It is generally discovered by running the hands through the[101] hair, when a little crust will be detected by the fingers, or a slight itching will show its position, or the brush may break it off. The top and hind parts of the head are generally the situations selected. Occasionally the hair will fall off, leaving spots of a smooth baldness.
The head is often a common area for the disorder. It's usually found by running your hands through the[101] hair, where you might feel a small crust, notice a bit of itching, or see hair breaking off when you brush it. The top and back of the head are typically the main spots affected. Sometimes, the hair will fall out, leaving behind smooth bald patches.

The vital organs, fortunately, are never subject to syphilitic inflammation—such as the brain, the viscera of the chest, and abdomen; nor is even the mucous membrane of the interior of the body affected, its power being confined solely to those parts or structures subject to the influence of external causes.
The vital organs, luckily, are never affected by syphilitic inflammation—like the brain and the organs in the chest and abdomen; even the mucous membrane inside the body isn't impacted, as its effects are limited to those areas or structures influenced by external factors.
When the venereal virus attacks the throat or palate, the membrane of the roof of the mouth becomes red and inflamed, patches ulcerate, and, if not cured, sooner or later expose the bony palate, which may be felt by the probe. This is the first stage. The exposed bone next exfoliates, and a communication is thereby formed between the mouth and nose, the fluids return through it, the voice is changed into a nasal twang, and a most offensive discharge is secreted.
When the venereal virus attacks the throat or palate, the lining of the roof of the mouth becomes red and swollen, patches develop ulcers, and if it’s not treated, it will eventually expose the hard palate, which can be felt with a probe. This is the first stage. The exposed bone will then slough off, creating an opening between the mouth and nose, fluids flow through it, the voice takes on a nasal quality, and a very unpleasant discharge occurs.

This drawing represents ulceration of the tonsils, uvula, and arch of the palate; also the edges of the tongue. The drawing, p. 102, shows the under surface of the tongue, the inner part of the lower lip, and the lower gums affected with venereal ulcers.
This illustration shows the ulceration of the tonsils, uvula, and palate arch, as well as the edges of the tongue. The illustration on p. 102 displays the underside of the tongue, the inner part of the lower lip, and the lower gums impacted by venereal ulcers.
When the tonsils are attacked, ulcers appear, precisely similar in character to chancres, hollow in the centre, with raised ragged edges, yellow on the surface, with a livid color on the surrounding margin. A sense of dryness is perceived, extending up the eustachian tube to the ear. Sometimes the tongue, gums, and inner part of the lips,[102] are attacked (see representation).
When the tonsils are affected, sores develop that closely resemble chancres, having a hollow center with uneven, raised edges, a yellow surface, and a dark color around the edge. A feeling of dryness is felt, reaching up the eustachian tube to the ear. Sometimes, the tongue, gums, and inner lips are also affected (see representation).[102]

In the progress of the disease, the pharynx, or top of the gullet, is brought under its influence, and the ulceration spreads through it to the vertebræ or back-bone. Extending its course, it next attacks the larynx, or top of the windpipe, when, if not arrested, it will soon destroy life. Attending this affection of the larynx, there is always loss of voice—the patient speaks in a low whisper. It is more fatal than any other form of the venereal disease.
In the course of the disease, the pharynx, or the top of the throat, is affected, and the ulceration spreads through it to the vertebrae or spine. As it continues, it next targets the larynx, or the top of the windpipe, and if it isn't stopped, it will soon lead to death. With this condition of the larynx, there is always a loss of voice—the patient speaks in a low whisper. It is more lethal than any other type of sexually transmitted infection.
The mucous membrane of the nose stands next in order, as subject to the influence of syphilis. The patient’s attention is first directed to it by an incrustation which forms in the nostril. On this being removed, a quantity of blood, mixed with purulent matter, is discharged. In two or three days, similar incrustations are formed, and under them ulceration takes place, which frequently lays bare the bone, and occasions it to exfoliate; and this exfoliating often continues after the venereal action has ceased. The number of bones which come away is often very considerable, and horrible deformity is the result.
The mucous membrane of the nose is also affected by syphilis. The patient first notices this due to a crust that forms in the nostril. When this crust is removed, a mixture of blood and pus is discharged. In two or three days, similar crusts appear, and under them, ulcers develop, often exposing the bone, which may start to come off. This shedding of bone can continue even after the venereal disease has resolved. The amount of bone that is lost can be quite significant, leading to severe deformity.
The periosteum and bones become in their turn affected by swellings called nodes—the periosteum first, and the bones subsequently. Of these, the cylindrical, being most exposed to vicissitudes of temperature, are commonly the first attacked. Those which are much covered by muscle are rarely affected, as, for instance, the back part of the tibia, or large bone of the leg, while nothing is more common than to see nodes on its anterior part, which is only covered with skin and periosteum. They occur on the fibula only when it is slightly covered, and only on the ulna, or elbow-bone, when similarly circumstanced. Nodes on the os humeri, or shoulder-bone, except on the outer side, are of very rare occurrence, but are frequently found on the clavicle, or collar-bone, at its scapular and sternal articulations.
The periosteum and bones are affected by swellings called nodes—the periosteum is affected first, followed by the bones. The cylindrical ones are usually the first to be affected since they are most exposed to changes in temperature. Those that are covered by a lot of muscle, like the back part of the tibia, or the large bone of the leg, are rarely affected, while it's quite common to see nodes on the front part, which is only covered with skin and periosteum. They only appear on the fibula when it’s lightly covered, and on the ulna, or elbow bone, under similar conditions. Nodes on the os humeri, or shoulder bone, are very uncommon except on the outer side, but they are frequently found on the clavicle, or collarbone, at its scapular and sternal joints.
In the following wood-cut is an illustration of the most frequent situation of nodes on the forepart of the tibia, or[103] chief bone of the leg. The swelling is considerable; the upper one proceeding to suppuration, and the lower indicating merely a tumefaction of the lower part of the bone, near the instep.
In the following woodcut, there's an illustration of the most common occurrence of nodes on the front of the tibia, or[103] the main bone of the leg. The swelling is significant; the upper one is starting to suppurate, while the lower one shows only a swelling in the lower part of the bone, near the ankle.

The symptoms which mark the disease are as follow: The patient experiences in the evening a sensation of pain in the bone which is afterward the seat of the node. In the course of a few days, a swelling appears in the evening, which disappears again on the following morning. It is excessively painful and tender at night, but in the morning it is hardly perceptible, and the tenderness is almost gone. At this particular period the periosteum is only affected; but when the inflammation has continued some time longer, the bone is diseased and becomes enlarged. The rationale is this: An inflammation of the periosteum ensues. In a short time a deposite takes place between it and the surface of the bone. This deposite, in the first instance, is only a serous fluid, but a cartilaginous substance is soon secreted, which is gradually converted into bone.
The symptoms of the disease are as follows: The patient feels pain in the bone in the evening, which later becomes the location of the node. After a few days, a swelling appears in the evening and disappears by the next morning. It's extremely painful and tender at night, but by morning, it's barely noticeable, and the tenderness is almost gone. At this stage, only the periosteum is affected; however, if the inflammation persists for a while longer, the bone becomes diseased and enlarges. The explanation is as follows: Inflammation of the periosteum occurs. Soon after, a deposit forms between it and the surface of the bone. Initially, this deposit is just a serous fluid, but shortly after, a cartilaginous substance is secreted, which gradually turns into bone.
When attended to early, their treatment is very simple; but occasionally cases of considerable difficulty will arise.
When addressed early, their treatment is quite straightforward; however, sometimes challenging cases will emerge.
Large quantities of fluid will be found fluctuating between the periosteum and the bone, which, when unaccompanied by redness and inflammation of the skin, may be absorbed by proper treatment, but which more usually is only curable by evacuation; and, unless great care be used, exfoliation of the bone will ensue to a very great, and sometimes fatal extent. The eyebrows, forehead, and temples, are often the seat of fluid tumors varying from the size of peas and beans. Their cure must be effected by absorption, or destruction of the bone is often produced.
Large amounts of fluid can be found shifting between the periosteum and the bone. If there’s no redness or skin inflammation, proper treatment can help the fluid be absorbed, but most of the time, it can only be treated by draining it. If not handled carefully, this can lead to serious bone exfoliation, which can sometimes be fatal. The eyebrows, forehead, and temples often have fluid-filled tumors ranging in size from peas to beans. Their treatment needs to focus on absorption, or else it can lead to damage of the bone.
The flat bones are also subject to syphilis. The one most commonly attacked is the os frontis, the symptoms being just the same as those on the skin. The side bones of the head now and then are affected; the os occipitis, or back-bone of the head, very rarely; and the os temporis, or temporal bone, being well covered with muscles, and[104] exposed to very little change of temperature, is never affected.
The flat bones can also be affected by syphilis. The one that gets hit the most is the os frontis, and the symptoms are the same as those seen on the skin. Occasionally, the side bones of the head are involved; the os occipitis, or the back bone of the head, is very rarely affected; and the os temporis, or temporal bone, is well protected by muscles and is exposed to very little temperature change, so it’s never affected.
The os frontis, being the most exposed, is the most frequently attacked. Suppuration sometimes takes place; and when this has occurred on the front, it has happened that the same suppurative process has occurred interiorly between the dura mater, or the external membrane of the brain, and the internal surface of the bone. The matter presses upon the brain, and death is the consequence, if the pressure be not removed by the use of the trephine or trepanning instrument. This is a degree of severity to which the disease rarely reaches now-a-days, from the more extended knowledge and improved treatment of modern times.
The os frontis, being the most exposed, is the most frequently attacked. Sometimes it gets infected, and when that happens on the front, it can also occur inside between the dura mater, which is the outer membrane of the brain, and the inner surface of the bone. The infection puts pressure on the brain, and if that pressure isn’t relieved using a trephine or trepanning tool, it can result in death. However, this level of severity is rare these days due to the greater knowledge and better treatments available in modern times.
It must be observed, generally, of both these diseases—that of the throat and nose, and this of the bones—that they are oftener the result of improper treatment, such as the excessive use of mercury, and exposure to great vicissitudes of weather while under its influence, inducing what is called the mercurial disease (which in fact is, or was, of more frequent occurrence than the constitutional syphilitic one), than the result of the natural tendency of the disease in an otherwise healthy individual.
It should be noted, in general, about both of these diseases—the throat and nose issues, and the bone problems—that they are more often the result of improper treatment, like excessive use of mercury, and exposure to extreme weather conditions while affected, leading to what is known as mercurial disease (which, in fact, was more common than the constitutional syphilitic type), rather than stemming from the natural course of the disease in a healthy person.
On the treatment of Syphilis.—I consider it a fair presumption that any invalided reader, except he be an accidental one, of this book—by which I mean one, not having sought its possession—must be acquainted with the association of mercury and syphilis. If not, let him be told for the first time, that such association exists as between copaiba and gonorrhœa; or perhaps what may be rendered more familiar to him, namely, as between quinine with ague, or colchicum with rheumatism. That for upward of three hundred years past mercury has been held an antidote to venereal affections; and still is, in many forms of the same, acknowledged indispensable for their removal.
On the treatment of Syphilis. — I think it’s safe to assume that anyone reading this book who isn’t just randomly picking it up—meaning someone who has actually sought it out—knows about the link between mercury and syphilis. If not, let me inform you for the first time that this link exists, just like the connection between copaiba and gonorrhea; or perhaps something more familiar, like quinine with chills, or colchicum with rheumatism. For over three hundred years, mercury has been considered a cure for venereal diseases, and it’s still recognized as essential for treating many forms of these conditions.
From old notions afloat, that syphilitic patients to be cured must be salivated to the extent of furnishing or filling two or three wash-hand basins daily with saliva—that the teeth drop out, that the breath becomes horribly fetid, and that the consumer of the poison sacrifices one third of his probable existence, even though he get well—the greatest possible prejudice exists against mercury, and the generality of uninformed patients have acquired a most uncompromising dread of the remedy. From the frequent[105] difficulty in getting patients to submit knowingly to mercurial treatment, many new means have been caught up, and some judiciously applied.
From old ideas going around that syphilis patients need to be treated by having their saliva produced in huge amounts—enough to fill two or three washbasins a day—that their teeth fall out, that their breath becomes extremely foul, and that anyone taking the treatment sacrifices a third of their lifespan, even if they recover—there’s a strong bias against mercury. Most uninformed patients have developed a deep fear of this remedy. Due to the frequent[105]difficulty in getting patients to agree to mercurial treatment, many alternative methods have been adopted, and some have been successfully applied.
This new method has its advantages; but it does not realize all that is promised. It consists in advising rest, cleanliness, simple soothing applications, and, on the other hand, mild astringent ones, a temperate diet, fresh air, an easy mind, sarsaparilla, and other alterative medicines. There are many believers in the efficacy of simplicity; and the success that follows such treatment of nine tenths of the ailments of humanity, bears out the usefulness of the preceding methods; but the remaining tithe have alike a claim upon our consideration, and of this tithe the syphilitic invalids form a large portion.
This new method has its benefits, but it doesn’t deliver everything it promises. It involves recommending rest, cleanliness, gentle soothing applications, and, on the other hand, mild astringents, a balanced diet, fresh air, a relaxed mind, sarsaparilla, and other alternative medicines. Many people believe in the power of simplicity, and the success that comes from such treatment for the majority of human ailments supports the value of these earlier methods. However, the remaining small percentage also deserves our attention, and a significant part of this group consists of individuals suffering from syphilis.
The anti-mercurial advocates have, however, a salvo, and admit now and then, an exception to exist, that particular cases do require a mercurial course, but then it should only be adopted in its mildest possible form, merely with a view to act on the general health, rather than for any specific property of its own. Again, there are books, which are very elaborate, and what is equally important, modern ones, written by talented men,[4] which still profess faith in the curative powers of mercury, and employ it as the chief agent in the cure of the venereal disease. Instead of administering it to the same extent as formerly—instead of attempting to produce salivation to the flow of quarts—they merely aim at producing an impression on the constitution; they are satisfied with a proof that their patient is under mercurial influence: this is ascertained by a coppery taste in the mouth, a slightly increased secretion of saliva, and the presence of the accompanying, but temporary depression.
The advocates against mercury do have a point and occasionally admit that there are certain cases where a mercurial treatment is necessary. However, it should only be used in the mildest form, primarily to improve overall health rather than for any specific effects of mercury itself. Additionally, there are detailed and importantly, modern books written by skilled authors,[4] that still believe in the healing properties of mercury and use it as the main treatment for venereal diseases. Instead of using it as extensively as in the past—trying to induce heavy salivation—they now focus on making an impression on the body. They’re satisfied with evidence that their patient is under the influence of mercury, which is indicated by a metallic taste in the mouth, a slight increase in saliva production, and the presence of a temporary feeling of depression.
Now the question to be resolved is, which of the two methods is the correct one. The many forms of disease of the sexual structures satisfy me, that their treatment should be modified by circumstances; but I believe I am wise enough to know, and certainly old enough to have observed, that the severer forms of syphilis, and even the milder in some constitutions, require the aid of mercury for their cure; in fact, will yield to no other plan of treatment, thereby admitting the specific virtues of the remedy.
Now the question we need to answer is which of the two methods is the right one. The many types of diseases affecting the sexual organs make me think that their treatment should be adjusted based on the situation; however, I believe I am wise enough to know, and certainly old enough to have seen, that the more severe forms of syphilis, and even the milder ones in certain individuals, need mercury to be cured; in fact, will not respond to any other treatment, thereby confirming the specific benefits of the remedy.
The principles, therefore, which I advocate in the treatment[106] of syphilis, are precisely those I depend upon in gonorrhœa, or, to familiarize the analogy, in a fit of indigestion, or an attack of local or general inflammation. Where the health is disturbed, the first step is to attempt restoration. The fact is almost too familiar to every one to need repetition, that, as is the condition of the health, so is the resistance it is capable of opposing to disease. The next proceeding is, to attempt the subdual of the prevailing symptoms. Syphilis, whether in the form of chancre, bubo, or any of its secondary varieties, induces more or less fever, inflammation, and interruption to the important offices of digestion, and other vital processes, which consequently require the promptest attention. Equally various are the local indications of syphilis—the ulcers may be common, superficial, phagedenic, or sloughing, each requiring various treatment, as hereafter will be specified; but, above all, too much reliance can not be placed on the dietetic and physical regimen—two comprehensive significations, which are, after all, the Alpha and Omega of the Materia Medica. With this declaration, I pass on to the treatment in detail of the more frequent and, I may add, leading features of syphilis.
The principles I support for treating[106] syphilis are the same ones I rely on for gonorrhea, or, to make the analogy relatable, for a case of indigestion, or an episode of local or general inflammation. When health is compromised, the first step is to try to restore it. This fact is so well-known that it hardly needs repeating: the state of health determines how well we can resist disease. The next step is to address the symptoms that are present. Syphilis, whether as a chancre, bubo, or any of its secondary forms, causes varying degrees of fever, inflammation, and disruptions to important processes like digestion, which need immediate attention. The local signs of syphilis are equally diverse—the ulcers can be common, superficial, phagedenic, or sloughing, each requiring different treatments, as will be detailed later; however, we can't overstate the importance of diet and physical care—two broad concepts that, after all, are the beginning and end of medical treatment. With that said, I will now move on to a detailed discussion of the more common and, I might add, key aspects of syphilis.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ———<>———
Treatment of Chancre.—Preliminary remarks.—Chancres are of various kinds. The most remarkable are:—
Treatment of Chancre.—Preliminary remarks.—Chancres come in different types. The most notable are:—
1st. That characterized by its circular form, its excavated surface covered by a layer of tenacious and adherent matter, and its hard cartilaginous base and margin.
1st. That is defined by its round shape, its hollowed-out surface covered by a layer of tough and sticky material, and its firm cartilaginous base and edge.
2d. Another form of chancre, unaccompanied by induration, but with a very high margin, appearing often on the outside of the prepuce, and seldom existing alone, called, from the preceding description, the “superficial chancre, with raised edges.” These kinds of ulcers are sometimes very tedious, neither getting better nor worse, but resisting every plan of treatment for their removal. I have known instances where they have existed for several months.
2d. Another type of sore, not swollen but with a very elevated edge, often appearing on the outside of the foreskin, and rarely existing alone, is referred to, based on the earlier description, as the “superficial sore with raised edges.” These types of ulcers can be quite stubborn, neither improving nor worsening, and resisting all treatment efforts aimed at eliminating them. I have seen cases where they lasted for several months.
3d. The phagedenic chancre, a “corroding ulcer without granulations,” and distinguished by its circumference being of a livid red color. This is the kind of chancre that is invariably rendered worse by mercury: indeed, cases have occurred where, from the injudicious administration of that medicine, the whole of the penis has been destroyed.
3d. The phagedenic chancre, a “corroding ulcer without granulations,” is characterized by its edges being a dark red color. This type of chancre is always worsened by mercury: in fact, there have been cases where improper use of that medication has resulted in the complete destruction of the penis.
4th. A most formidable kind of chancre, denominated the sloughing ulcer. It first appears as a black spot, which[107] spreads and becomes detached, leaving a deepened and unhealthy looking surface. The sore is very painful, and encircled with a dark purple areola. If neglected, or improperly treated, the process of mortification goes on until all the parts of generation are destroyed.
4th. A very serious type of sore called the sloughing ulcer. It starts as a black spot that[107] grows and comes away, leaving behind a deep and unhealthy-looking area. The sore is extremely painful and surrounded by a dark purple ring. If ignored or treated incorrectly, the decay continues until all the reproductive areas are damaged.
The last-named chancre is more often the consequence of neglect on the part of the patient, than the natural progress of the disease.
The last-named chancre is more often the result of the patient's neglect than the natural progression of the disease.
Now the usual method adopted by surgeons to remove chancres, has been to excise them, or to apply caustic; the latter is the plan I adopt, and would recommend; but all chancres are not to be treated alike, some requiring antiphlogistic remedies, others soothing, others stimulant. Some practitioners rely entirely upon constitutional remedies.
Now, the common approach that surgeons use to remove chancres is to cut them out or to use caustic treatments; I prefer the latter and would recommend it. However, not all chancres should be treated the same way; some need anti-inflammatory remedies, while others need soothing treatments, and some require stimulants. Some doctors rely entirely on systemic remedies.
On the first appearance of a chancre, I would enjoin an alteration in the diet, regulating it according to the strength of the patient. Abstemiousness should be the motto, avoiding extremes, however, lest debility should be induced. Quietude and rest, in the recumbent position, are two essential adjuncts in the treatment of primary syphilis throughout.
On the first sign of a chancre, I would recommend a change in diet, adjusting it based on the patient’s strength. Moderation should be the key, avoiding extremes to prevent weakness. Relaxation and rest while lying down are two essential components in the treatment of primary syphilis at all times.
With respect to the treatment of the ulcer, characterized by its circular form, excavated surface, and hardened base, as detailed, the plan I almost invariably adopt is, immediately on its appearance, at least as soon as the pimple has broken or desquamated, to smear it with a hair pencil filled with the solution of caustic, sometimes twice, at least once a day (see Form 27), and to keep it frequently washed in the daytime with a lotion of the chloride of soda (see Form 28), or the black, red, or blue wash (see Forms 29, 30, 31).
With regard to treating the ulcer, which has a circular shape, a hollow surface, and a hardened base, I usually follow this plan: as soon as it appears, or at least once the pimple has ruptured or flaked off, I apply a hair pencil soaked in caustic solution, usually twice a day, but at least once (see Form 27). I also make sure to wash it often during the day with a lotion of sodium chloride (see Form 28), or with black, red, or blue wash (see Forms 29, 30, 31).
If the patient be strong, and otherwise in good health, I simply recommend a dose of purgative medicine, in anticipation of any irritation that may arise. After which, I suggest a middle diet to be adopted for the next few days. From the sedative and salutary effects of the warm bath, I recommend its employment immediately after the operation of the medicine, and its repetition at frequent intervals. Independently of its effect on the system, it is the best general cleanser that can be resorted to. The subsequent treatment is regulated by the result of the above, which can be ascertained about the third day.
If the patient is strong and otherwise healthy, I simply recommend a dose of laxative medicine, anticipating any irritation that might occur. After that, I suggest sticking to a moderate diet for the next few days. Because of the calming and healing effects of a warm bath, I recommend using it right after the medication takes effect and repeating it regularly. Besides its effect on the body, it's the best overall cleanser to use. The next steps in treatment depend on the results from the above, which can be observed around the third day.
In numberless instances, and where the disease is thus early detected and similarly treated, the mere continuance of either the chloride lotion, or black wash, the middle diet, an occasional aperient, the bath, with as much rest as possible, are all that will be found needful to cure the disease, which generally is effected in about a week or ten days at farthest. From the universal dread that so sudden a disappearance of the sore occasions, lest it should “be driven into the system,” and from the apprehension that it is incurable without taking mercury, I verily believe that, in many cases, the practitioner, participating in the fears of his patient, and anxious to allay them, reluctantly administers[109] that mineral; and to such weak judgment may be traced the relapses, or the occurrence of other symptoms sometimes mistaken for secondary. Even when the case terminates favorably, and within the space of time alluded to, I would not be considered as recommending a sudden return to free living; on the contrary, I would not release the patient from the restrictions imposed upon his diet, exercise, and regimen, for at least the same time as was occupied in the cure, nor would I predict that, in every instance, secondary symptoms should not ensue. Mercury was supposed to possess some antisyphilitic property, inasmuch that, when chancre healed during its exhibition, secondary symptoms were averted. Facts, however, have been wanting to corroborate that supposition; for secondary symptoms have appeared despite the external and internal employment of mercury, even to the extent of salivation. Authors there are who attach similar properties to other medicines, such as nitric acid, sarsaparilla, and such like. Now, how do these medicines act upon the system? Or what is their tendency of action? Why, by increasing some particular function, such as the secretive process of the salivary and other glands; by increasing perspiration or absorption, &c. The remedies whereby these changes are induced are termed alteratives. I am not going to deny that these, or some such changes in the system, are unessential for the eradication, particularly of morbid conditions of structure and function, dependent[110] probably upon altered condition and diminished action in others. On the contrary, they are the only antagonists to disease which we possess.
In many cases, when the disease is detected early and treated appropriately, simply continuing either the chloride lotion or black wash, maintaining a moderate diet, taking an occasional laxative, having baths, and getting as much rest as possible are all that's needed to cure the disease, which typically resolves in about a week to ten days at most. Due to the widespread fear that such a sudden healing of the sore might lead to it "being driven into the system," and the concern that it's untreatable without using mercury, I genuinely believe that, in many instances, a doctor, sharing in the patient's fears and wanting to ease them, reluctantly gives that mineral. This hesitant judgment can often lead to relapses or to symptoms that are sometimes misidentified as secondary. Even when a case ends positively and within the timeframe mentioned, I wouldn't advocate for an immediate return to unrestricted living; rather, I wouldn't lift the patient's dietary, exercise, and regimen restrictions for at least the same duration as the treatment took, nor would I guarantee that secondary symptoms won't occur in every case. Mercury was thought to have some anti-syphilitic properties because when a chancre heals during treatment, it seems to prevent secondary symptoms. However, there hasn’t been enough evidence to support that belief; secondary symptoms can show up even with the external and internal use of mercury, sometimes to the point of salivation. Some writers attribute similar properties to other medicines like nitric acid and sarsaparilla. So, how do these medicines influence the body? What is their effect? They operate by increasing certain functions, such as the secretory processes of the salivary and other glands, or by boosting sweating and absorption, etc. The treatments that bring about these changes are called alteratives. I'm not denying that these or similar changes in the body are essential for eliminating certain unhealthy structural and functional conditions, which likely depend on changes in state and reduced activity elsewhere. In fact, they are the only true counters to disease that we have.
But what I contend is, that, in our selection, we should prefer those which produce most speedily and effectively the desired change, with the least detriment to the general health. And to this end, I invariably enjoin, where practicable, warm or vapor bathing. I have elsewhere considered this subject at length, to which I refer the reader; but I will fearlessly assert that no one, or any plan of treatment, will be found so effectual toward increasing physical power to repel disease, or so permanently preservative of health, as the modified employment of the warm or vapor bath; and, therefore, in all cases of doubt and apprehension, or independent of either, the use of the warm or tepid, plain, or salt-water bath, two or three times a week for a month, or the vapor bath about every fourth or fifth day for the same period, is the best preventive that can be adopted to avert secondary symptoms. Where bathing of every kind is impracticable, as is the case in some country places, and the same necessity exists, I advocate the administration of alterative medicines; nor do I object to the employment of mercury, where, under other circumstances, without reference to its imaginary efficacy in syphilis, it would be prescribed. But of this as we proceed.
But what I argue is that when making our choices, we should prefer options that quickly and effectively bring about the desired change, with the least harm to overall health. To this end, I always recommend, when possible, warm or steam bathing. I've discussed this topic in detail elsewhere, which I point the reader to; however, I will boldly state that no one method of treatment is as effective at boosting physical strength to fight off disease or as lasting in its preservation of health as the careful use of warm or steam baths. Therefore, in any situation of uncertainty or concern, or regardless of those feelings, using a warm or tepid bath, whether plain or salt water, two or three times a week for a month, or a steam bath every four or five days during the same period, is the best preventive measure to avoid secondary symptoms. Where bathing in any form is not possible, as it might be in some rural areas, and the need still exists, I recommend the use of alternative medicines; I also do not oppose the use of mercury where, under other circumstances, it would be prescribed without considering its supposed effectiveness in treating syphilis. But more on that as we go on.
Where, at the expiration of a week, the chancre neither[111] recedes nor advances, and is the only symptom present, it is to be presumed that the condition of the patient’s health has something to do with it, and that condition should be minutely inquired into. There may be diminished or increased appetite, with imperfect digestion; there may be fever, with restlessness at night; there may be torpor or irritation of the bowels; or the patient may consider his only ailment to be the chancre, the irritation of which may be found to arise from too active exertion. To whichever cause it may be ascribed, the treatment should be directed. In conjunction with local remedies, which may be varied, alteratives may be given—five grains of the blue pill twice a day; for instance, the Plummer’s pill in doses of five grains every night, the occasional application of an active aperient (see Forms 33, 34), the decoction of sarsaparilla (see Forms 49, 50, 51). This plan, carefully pursued, seldom fails in setting up a permanent cure. The patient should be apprized of the vast importance of quiet, rest, and abstemiousness; for, where they can be attended to, the duration of the disease will be diminished one half; whereas, he who is continually in the erect posture, and subject to much walking about, who is indifferent to his diet, and lives as free as formerly, incurs the risk of bubo, and all its alarming consequences. Now, in no case or description of chancre, do these remarks apply so aptly as to the phagedenic and sloughing ulcer; in fact, they are applicable to all, but more particularly the two latter, as they are[112] the result of already increased action. Mercury, violent aperients, and other active remedies, should also be avoided in these two forms of chancre; the local appliances should be poultices of bread and water, linseed meal, and a solution of opium, or poppy water; the sloughs or mortified portions we should endeavor to detach, by the application of a smear of nitric acid, or the chloride lotion (Form 28), or stimulative ointment (Form 38). The superficial sore usually gets well by the same means as the ordinary chancre.
Where, after a week, the sore hasn't improved or worsened, and is the only symptom present, it's likely that the patient's overall health is a factor, and this should be looked into closely. The patient might experience changes in appetite, whether decreased or increased, along with poor digestion; fever and restlessness at night might be an issue; there could be sluggishness or irritation in the bowels; or the patient might think the only problem is the sore, which might actually be aggravated by too much activity. Regardless of the cause, treatment should be tailored accordingly. Along with local treatments, which can vary, alternatives might be prescribed—like five grains of blue pill twice daily; for example, Plummer's pill at five grains every night, the occasional use of an active laxative (see Forms 33, 34), and a decoction of sarsaparilla (see Forms 49, 50, 51). This approach, if diligently followed, rarely fails to achieve a lasting cure. The patient should be made aware of the great importance of rest and moderation; when these can be prioritized, the duration of the condition may be cut by half; however, if the patient stays active, walks a lot, pays little attention to diet, and lives as they normally would, they risk developing bubo, along with all its serious consequences. These observations are especially relevant to phagedenic and sloughing ulcers; in fact, they apply to all types, but particularly the latter two, as they stem from already heightened activity. Mercury, strong laxatives, and other aggressive treatments should be avoided in these two types of sores; local treatment should involve poultices made of bread and water, linseed meal, and a solution of opium or poppy water; we should try to remove dead tissue with a smear of nitric acid, or a chloride lotion (Form 28), or stimulating ointment (Form 38). The superficial sore typically heals through the same methods as an ordinary sore.
Where the chancre is situated under the prepuce, and the latter covering is so inflamed and swollen as to prevent its being drawn back to exhibit the sore, the discharge should be carefully washed out by any of the lotions already recommended, by means of a syringe, several times in the twenty-four hours. Much good is often done by varying the local remedies, occasionally flouring or filling up the ulcer with calomel, tutty powder, blue ointment, or in fact any substance which alters the morbid action of the part; but, as a general rule, the lotions of soda, lime, zinc, or oxymuriate of mercury, will be found sufficient, if persevered in.
Where the chancre is located under the foreskin, and the foreskin is so inflamed and swollen that it can't be retracted to show the sore, the discharge should be carefully rinsed out using any of the previously mentioned lotions, with a syringe, several times a day. Changing up the local treatments often helps; you can occasionally sprinkle or fill the ulcer with calomel, tutty powder, blue ointment, or any substance that modifies the unhealthy condition of the area. However, as a general guideline, the lotions containing soda, lime, zinc, or mercuric chloride will usually be sufficient if you stick with them.
Treatment of Bubo.—Bubo I have already stated to be an inflamed and enlarged condition of the inguinal (as its name implies, signifying the groin), or, in fact, any other gland, occasioned by the passage of the venereal poison from the adjacent ulcer through it, preparatory to its contaminating the constitution. But it is as well to know that the system may become affected, or, in other words, the poison may pass through the glands without involving them in the disease, or that the poison may there stop, and be[113] expelled as the bubo is cured. It is also observed, that buboes are more frequently consequent upon an ulcer seated on the prepuce than on the glans. Buboes are not always, however, a sure criterion of the venereal disease, for they will occur wherever irritation is superficial and adjacent. Leeches applied to the temples will affect the cervical glands, a graze or wound in the leg enlarge the inguinal, and a whitlow on the finger, or any inflammation of the hand or arm, will very often irritate the glands in the axilla. In gonorrhœa, the glands in the groin become swollen and painful, from sympathizing with the sensibility of the urethra; but these and the preceding may, in general, be distinguished from true venereal buboes by their disinclination to proceed to suppuration; whereas, in syphilis, that process runs through its several stages with remarkable celerity, unless timely prevented. Buboes in the groin are much more troublesome, and more likely to betray the disease, than chancres, because they constitute an augmentation to the patient’s suffering, seldom occurring, unless preceded by a chancre, and because they occasion a visible and necessary lameness. They also produce more general disturbance of the patient’s health.
Treatment of Bubo.—A bubo is an inflamed and enlarged condition of the groin glands, as the name suggests, but it can affect any other gland as well. This condition results from the venereal poison moving from a nearby ulcer through the glands, preparing to contaminate the entire system. However, it's important to note that the body can be affected without these glands being involved in the disease. The poison may stop there and be expelled as the bubo heals. It's also observed that buboes are more commonly linked to an ulcer on the foreskin than on the glans. However, buboes are not always a definitive sign of venereal disease, as they can occur wherever there is superficial irritation nearby. For example, leeches applied to the temples can impact the neck glands, a scrape or wound on the leg can cause swelling in the groin, and a whitlow on the finger or any inflammation of the hand or arm can irritate the glands in the armpit. In cases of gonorrhea, the groin glands can become swollen and painful due to the sensitivity of the urethra; however, these and the previous examples can generally be distinguished from true venereal buboes by their tendency not to go to suppuration. In syphilis, that process progresses through its stages quickly, unless addressed in time. Buboes in the groin are often more problematic and more likely to reveal the disease than chancres, as they increase the patient's discomfort, typically occur after a chancre, and can cause noticeable limping. They also cause more overall disruption to the patient's health.
In the treatment of a bubo, venereal or not, the same principles recommended in the section devoted to the cure of chancre, should be followed in this instance—comprising attention to the general health, and a subdual of the prevailing symptoms.
In treating a bubo, whether it’s venereal or not, the same principles outlined in the section on curing chancre should be applied here—focusing on overall health and reducing the main symptoms.
In no form of syphilis is rest more essential than in bubo. The patient will be apt to plead the necessity of following his business, and the utter impossibility of staying at home; that is his affair, mine is only to protest against exercise, and urge the importance of rest, and even the recumbent posture, and I can assure him, that alone will strip the disease of three fourths of its terrors.
In no type of syphilis is rest more crucial than in bubo. The patient will likely argue that they need to keep working and that staying at home is completely impossible; that’s their issue. My job is simply to warn against physical activity and stress the importance of rest, even lying down. I can assure them that doing so alone will remove about three-quarters of the disease's horror.
Certain local diseases produce more constitutional disturbance[114] than others—among them may be classed buboes; it would, therefore, be as impolitic suddenly and violently to repel an inflammation of a gland or glands, without establishing some outlet for the increased action to vent itself, as it would be to check a flux or suppress an exanthematous eruption, like measles or scarlatina.
Certain local diseases cause more overall disruption[114] than others—buboes can be included in this group; therefore, it would be just as unwise to suddenly and forcefully stop an inflammation of a gland or glands, without providing a way for the increased activity to release itself, as it would be to stop a flow or suppress a rash, like measles or scarlet fever.
If the bubo is, therefore, painful and inflamed, my advice is as follows: Stay at home, and rest; descend to middle diet; take some aperient; and should chancres alone be present, and a treatment going on for their extinction, continue the same; or, as bubo often immediately succeeds the ulcer, and probably may be the first symptom noticed, adopt, in addition to that recommended above the treatment as advised for chancre, namely, the administration of some alterative—for instance, five grains of blue pill every night—or the Plummer’s pill every night—the aperient powder every other day; and let the local treatment be directed to remove the prevailing symptom, to subdue the inflammation, and, if possible, thereby prevent suppuration. It was formerly supposed that, unless buboes were allowed to suppurate, the system could not escape the venereal taint. Lower somewhat the vital powers, or, what may be more intelligible, diminish the general inflammatory action, establish some slight drain, by determining the secretions to the intestines or skin: and buboes, even when matter has absolutely formed, may be fearlessly absorbed, which judicious treatment will effect, in nine cases out of ten, without at all impregnating the constitution. To attain this object, warm fomentations constantly applied, and if possible the warm (hip or full length) bath every night. When rest is determined upon, if the swelling is great, red, and painful, leeches are eminently serviceable, but they must be applied in numbers of at least a dozen at a time, and repeated twice or thrice if necessary. Three or four, by the irritation of the bites when healing, and especially[115] if the patient will not or can not remain quiet, only worry and aggravate the disease. Where the inflammatory symptoms are great, where there is fever and much heat of skin, bleeding is the speediest and most effectual plan to subdue them; and, in my opinion, it is to be preferred before the trouble and bother of leeches. Where, however, there is no remarkable excitement, local or universal, the topical application of any of the ointments suggested will often promote absorption (see Forms 35, 36, 37).
If the bubo is painful and inflamed, my advice is as follows: Stay home and rest; stick to a light diet; take some laxatives; and if there are only chancres present with ongoing treatment, continue with that. Since a bubo often follows an ulcer and might be the first symptom noticed, in addition to the above advice, follow the treatment suggested for chancre. This means taking an alterative, such as five grains of blue pill every night, or Plummer’s pill every night, and using the aperient powder every other day. The local treatment should focus on alleviating the main symptom, reducing inflammation, and, if possible, preventing pus from forming. It used to be believed that if buboes didn’t form pus, the body couldn't rid itself of the venereal infection. Lower the vital powers a bit, or, to put it simply, reduce the overall inflammatory response, and create a slight drainage by encouraging secretions to the intestines or skin: even if pus has formed, buboes can still be absorbed safely with careful treatment in nine out of ten cases, without impacting the body's constitution. To achieve this, apply warm compresses regularly, and if possible, take a warm bath (either hip or full length) every night. If you decide to rest, and if the swelling is significant, red, and painful, leeches are very effective. However, they should be applied in groups of at least a dozen at a time, and repeated two or three times if necessary. Using only three or four can irritate the bites during healing, especially if the patient can't stay still, which only exacerbates the condition. When the inflammatory symptoms are severe, with fever and lots of heat in the skin, bleeding is the quickest and most effective way to reduce them, and I believe it’s preferable to the hassle of using leeches. However, if there’s no significant excitement locally or generally, applying any of the recommended ointments often helps promote absorption (see Forms 35, 36, 37).
Blisters applied over the bubo, very often disperse the swelling. Pressure also, made by means of a pad covered with tin foil (as seen in the subjoined cut), and continued for several days, frequently urges the absorption of the accumulated deposition in the gland.
Blisters placed over the bubo often reduce the swelling. Pressure applied with a pad covered in tin foil (as shown in the image below) and maintained for several days often encourages the absorption of the buildup in the gland.

Where bubo has been suffered to proceed, and the suppuration appears inevitable, it would be highly improper[116] to retard it: poultices and warm fomentations should be applied, and when fit, an opening should be made to permit the exit from, and prevent the extension of, the matter in the surrounding cellular membrane; the operation should not, however, be prematurely performed; the skin should be permitted to become thin before an opening is made, and that opening should be made in the most dependent position, in order to allow complete escape of the matter, lest fistulæ and sinuses should form. When an abscess is thus established, its healing must be promoted with all expedition, and care taken to preserve the strength of the patient. For the former purpose, poultices, mild healing ointments, or strapping plaster applied near the edges of the wound, should be used. Poultices may be applied with a bandage, as seen in the subjoined cut.
Where bubo has been allowed to develop, and the formation of pus seems unavoidable, it's very unwise[116] to delay it: poultices and warm compresses should be used, and when appropriate, an incision should be made to allow the pus to drain out and prevent it from spreading into the surrounding tissue; however, this procedure shouldn't be done too early; the skin should be allowed to thin out before making an incision, and that incision should be in the lowest position to ensure the complete drainage of the pus, to avoid the formation of fistulas and sinuses. Once an abscess has formed, its healing should be expedited, and care taken to keep the patient strong. For that purpose, poultices, gentle healing ointments, or adhesive plaster applied near the wound edges should be used. Poultices can be secured with a bandage, as illustrated in the accompanying image.

When the abscess appears indolent and not disposed to heal, carrot and linseed-meal poultices may be substituted. Astringent ointments should also be employed (see Forms 38, 39, 40), or lotions (see Forms 41, 42), and the topical[117] application of caustic to the edges of the wounds, or even paring them with a scalpel. The occasional use of the warm or vapor bath will give a healthy tone to the frame, invigorate the depressed powers, and promote recovery. The strength should be supported by more generous diet, and any of the formulæ comprised under the head of tonics, may be taken internally (see Forms 43, 44, 45, 46, 47, 48). As the patient becomes convalescent, change of air, gradual exercise, the cold shower bath, or sea bathing, will be of essential service.
When the abscess looks lazy and isn't healing, you can use carrot and linseed meal poultices instead. Astringent ointments should also be applied (see Forms 38, 39, 40), or lotions (see Forms 41, 42), and you can apply caustic to the edges of the wounds or even trim them with a scalpel. Occasionally using a warm or steam bath will help improve overall health, boost energy, and speed up recovery. The patient should have a more generous diet to maintain strength, and any of the tonics listed can be taken internally (see Forms 43, 44, 45, 46, 47, 48). As the patient starts to recover, getting fresh air, slowly increasing physical activity, taking cold showers, or swimming in the sea will be very helpful.
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links.
Treatment of secondary symptoms.—Secondary symptoms usually appear from the sixth to the sixteenth week, but are not unfrequently protracted beyond that period; they are commonly ushered in with fever—a general sense of being ill—a quickened pulse, headache, loss of appetite, pains in various parts of the body, and restlessness at night; in short, there is disturbance of all the vital functions, until it is determined which structures are to be the retreat of the common enemy. Some authors assign the skin and throat as more liable to attack than others; but I think the distinction dependant mainly upon the natural or morbid idiosyncrasy of the invalid. At all events, the inquiry here would be foreign to the design of this work, and less useful than the advice, how best to combat the evils when and wherever they occur. I have already stated secondary symptoms to consist of eruptions, ulcerations, and disfigurations of the skin, ulcerations of the mucous membranes of the mouth, throat, and nose, pains in the joints, swellings of the bones and their coverings, and inflammation of the various fibrous textures of the body.
Treatment of secondary symptoms.—Secondary symptoms usually show up between the sixth and sixteenth week, but they can sometimes last longer. They often start with a fever, a general feeling of illness, a faster heartbeat, headache, loss of appetite, body aches, and restlessness at night. In short, there’s a disturbance in all the vital functions until it’s clear which parts of the body are affected by the illness. Some authors say that the skin and throat are more likely to be affected than other areas, but I believe this mainly depends on the individual’s natural or pre-existing conditions. Regardless, discussing that here wouldn’t fit the purpose of this work and would be less helpful than giving advice on how to best address these problems as they arise. I’ve already mentioned that secondary symptoms include rashes, sores, and changes in the skin; sores in the mucous membranes of the mouth, throat, and nose; joint pain; swelling in the bones and their coverings; and inflammation of various fibrous tissues in the body.
Treatment of syphilitic eruptions.—The cutaneous eruptions of syphilis present considerable varieties, assuming a scaly, papular, tubercular, or pustular appearance. Formerly it was the opinion that no eruption was venereal, unless characterized by a scurfy exfoliation, and teinted of a copper color. This test is not now relied on. In the[118] simpler forms, we find that the skin becomes mottled at first, which appearance may partially die away and reappear, deeper in color, and the spots become more numerous in extent. The patient should be apprized that, when the disease has progressed thus far, it is not in its nature to depart unbidden; but it advances usually from bad to worse.
Treatment of syphilitic eruptions.—The skin eruptions of syphilis vary greatly, taking on a scaly, bump-like, tuber-like, or pus-filled appearance. In the past, it was believed that no eruption was considered venereal unless it had a scaly peeling and was tinted a copper color. This test is no longer trusted. In the[118] simpler forms, the skin first becomes blotchy, which can partially fade and then reappear, deeper in color, with more spots appearing over time. The patient should be made aware that once the disease has progressed this far, it does not go away on its own; it typically worsens over time.
The mottled dots enlarge, exfoliate, or scurf, or desquamate, as it is called, leaving the subjacent circle thicker and thicker, and of the same color as the cuticle which peels off. In the ordinary uninterrupted progression, scabs form, suppurate, and constitute an ulcer, like a chancre, which ulcer assumes all the varieties of chancre. In other cases, the eruption, instead of being scaly, “has a raised surface, from which a whitish matter usually oozes.”
The spotted dots grow larger, flake off, or peel, which is known as desquamation, leaving the underlying area thicker and the same color as the skin that is shedding. In the usual continuous progression, scabs form, become infected, and turn into an ulcer, similar to a chancre, which ulcer can take on all the different forms of a chancre. In other cases, the rash, instead of being scaly, has a raised surface, from which a whitish substance typically seeps.

The scaly copper-colored eruption, denominated, according to its severity and appearance, syphilitic lepra or psoriasis, is regarded as most characteristic of true syphilis, and is the most frequent. The annexed is a drawing copied from nature; it is alluded to a few pages further on: its pattern is frequently to be met with. A celebrated writer, Mr. Carmichael, attaches considerable importance to the character and appearance of the eruptions. He divides the venereal disease into four species or varieties: 1st, the scaly venereal disease, which he considers consequent upon the ordinary chancre; 2d, the papular, consequent upon gonorrhœal[119] ulceration; 3d, the tubercular; and 4th, the pustular, he names from its appearance. These distinctions, if correct, must be more interesting to the surgeon, than serviceable to the patient, for the principles of treatment must be alike in all. Now, although mercury may be denied to possess any specific influence over the syphilitic poison, either by its chemical action or neutralizing power, except as a counter-irritant to the system, yet the inability of nature to shake off the pestilential hydra, unassisted by the weapons of the physician, is most apparent; and the most powerful of which is, that class of medicines called alteratives, none of which are more deserving, none more manageable, if the least judgment be displayed, than mercury.
The scaly, copper-colored rash, referred to as syphilitic lepra or psoriasis based on its severity and appearance, is considered the most characteristic of true syphilis and is the most common. The drawing attached is a reproduction from nature; it is mentioned a few pages ahead: its pattern often appears. A well-known writer, Mr. Carmichael, places significant importance on the character and look of the rashes. He categorizes the venereal disease into four types: 1st, the scaly venereal disease, which he believes follows the ordinary chancre; 2nd, the papular, resulting from gonorrheal ulceration; 3rd, the tubercular; and 4th, the pustular, named for its appearance. These distinctions, if accurate, might be more intriguing to the surgeon than helpful to the patient, since the treatment principles should be similar across the board. Now, while it's argued that mercury doesn’t have any specific effect on the syphilitic poison, whether through chemical action or neutralizing capability, except as a counter-irritant to the body, it’s clear that nature struggles to rid itself of the harmful “hydra” without the physician's help; the most effective aid being the class of medications known as alteratives, with none being more deserving or easier to manage, if some judgment is applied, than mercury.
The constitution, when under the influence of syphilitic poison, is being led like a willing horse to its own destruction; and unless the system be entirely revolutionized, that event is not likely to be retarded. Here mercury[5] may[120] lend its powerful aid, and may be carried even so far as to produce mild ptyalism or salivation. But there are instances where mercury is inadmissible. The patient, however, need not despair; extensive resources are still open for him—the preparations of antimony,[6] the mineral acids, sarsaparilla (Forms 49, 50, 51), iodine (Form 52), and a host of others may be resorted to; and last, though not least in importance, is the medicated vapor and fumigating bath. From my connexion with an establishment of that kind, my disinterestedness might be questioned in advising the employment of bathing. As well might the apothecary who deals in his own drugs, or the tradesman who vends his own wares, be suspected of disingenuousness; the reply I would offer should be, that the reader or invalid need not pin his faith on my assertion, unless it so please him; or if he does, may the onus lie at my door. But for his sake, and to bear out my own assertion, I offer this declaration, that, for the last twenty years, in conducting my establishment[121] (wherein more cases of syphilitic eruption have presented themselves, than probably have fallen under the notice of any other medical man in London within the same period), no case, of which I have had the management, has failed of being cured.
The body, when affected by syphilitic poison, is being driven like a willing horse to its own demise; and unless the system is completely overhauled, that outcome isn’t likely to be delayed. Here, mercury[5] may[120] provide significant help and can even go so far as to cause mild ptyalism or salivation. But there are cases where mercury is not appropriate. The patient, however, shouldn’t lose hope; there are still plenty of options available to him—the preparations of antimony,[6] the mineral acids, sarsaparilla (Forms 49, 50, 51), iodine (Form 52), and many more can be used; and lastly, though not less important, is the medicated vapor and fumigating bath. Given my connection with an establishment of that kind, one might question my impartiality in suggesting the use of baths. Just as one might suspect the druggist who sells his own medicines, or the merchant who offers his own products, of being insincere; my response would be that the reader or patient doesn’t have to believe my statement unless he chooses to; or if he does, may the responsibility rest with me. But for his benefit, and to support my claim, I declare that for the past twenty years, while running my establishment[121] (where I’ve treated more cases of syphilitic eruptions than probably any other doctor in London during that time), not a single case under my care has failed to be cured.
Where syphilitic eruptions terminate in ulceration, the same local treatment should be used as advised for chancres. Among the prescriptions will be found formulæ for many useful topical applications, such as ointments, lotions, and fumigations, for all the external developments of syphilitic disease, with appropriate observations appended to each.
Where syphilitic sores lead to ulceration, the same local treatment should be applied as recommended for chancres. The prescriptions include formulas for various effective topical treatments, such as ointments, lotions, and fumigations, for all external manifestations of syphilitic disease, with relevant notes added to each.
Treatment of syphilitic sore throat.—It has already been mentioned, that the order of appearance of secondary symptoms depends more upon the modified state of health than any fixed law of disease. Syphilitic sore throat may precede or follow the cutaneous eruptions; and it not unfrequently happens, that all forms of the disease are present at the same time: therefore, although they are here separately considered, it will be found that the treatment corresponds nearly in all, the only difference being in the local applications.
Treatment of syphilitic sore throat.—It has already been noted that the sequence of secondary symptoms depends more on the individual's health condition than on any strict disease pattern. Syphilitic sore throat can come before or after skin rashes, and it's not uncommon for all forms of the disease to be present simultaneously. Therefore, even though they are discussed separately here, the treatment for each is quite similar, with the main difference being the local treatments used.
Syphilitic sore throat consists of ulcerations of the fauces, tonsils, and soft palate. The inflammation begins in the part affected. There is a redness, and sensation of dryness. A small white spot is perceptible, which rapidly spreads, is detached, reappears, and in four-and-twenty hours, if seated on the tonsils, a cavity, as if a portion of[122] them had been scooped out, is observable. The ulcer has a sharp margin, and its excavated surface is covered by a whitish or yellowish adhesive matter. At other times, the ulceration will be more superficial, but not less rapid in its progress, extending over the upper part of the palate, and back part of the throat. Here the general treatment is precisely the same as in the other forms of the disease, viz., rest, abstemiousness, low diet, aperient, saline, and alterative medicines, the blue pill, preparation of antimony, the bath, and total exclusion from all excitement. The topical treatment consists of fumigations, gargles, styptic lotions, nitrous acid gas, blisters over the larynx, rubbing in of any counter-irritating ointment; the object being throughout to watch, and endeavor to improve the patient’s health, support the strength, and mitigate and remove the local symptoms.
Syphilitic sore throat involves ulcers in the throat, tonsils, and soft palate. The inflammation starts in the affected area. There is redness and a feeling of dryness. A small white spot can be seen, which quickly spreads, falls off, comes back, and within twenty-four hours, if it's on the tonsils, you can see a cavity that looks as if a piece of[122] it has been scooped out. The ulcer has a sharp edge, and its hollow surface is covered with a whitish or yellowish sticky substance. Sometimes, the ulceration is more superficial, but it progresses just as quickly, spreading over the upper palate and back of the throat. Here, the general treatment is exactly the same as in other forms of the disease, which includes rest, moderation, a low diet, laxatives, saline, and altering medicines, blue pills, antimony preparations, baths, and complete avoidance of any excitement. The local treatment involves fumigations, gargles, astringent lotions, nitrous acid gas, blisters on the larynx, and applying any counter-irritating ointment; the goal is to monitor and work on improving the patient’s health, maintaining strength, and alleviating or removing local symptoms.
In the affections of the nose and palate, the fumigations are indispensable; injections must also be used, and styptic lotions applied with a camel’s-hair brush. These cases are very tedious, and, fortunately, in the present day, of rarer occurrence than formerly; and the patient, thus severely attacked, would be more prudent to rely upon some confidential medical adviser, than to trust in his own management.
In dealing with issues of the nose and palate, fumigations are essential; injections should also be used, and styptic lotions applied with a camel’s-hair brush. These cases can be quite tedious, and fortunately, they're less common these days than they used to be; a patient facing such a serious situation would be wiser to rely on a trusted medical professional rather than trying to manage it on their own.
Treatment of venereal affections of the bones and joints.—Nodes are alleged, by medical men of great authority, to be of rare occurrence, except the patient has been taking mercury; but the observation is not always correct.
Treatment of venereal diseases of the bones and joints.—According to highly regarded medical professionals, nodes are said to be uncommon unless the patient has been using mercury; however, this observation isn't always accurate.
Their treatment, of course, must be regulated by various circumstances. When the pain and inflammation are severe, leeches, bleeding, warm fomentations, or cold evaporating lotions composed of vinegar and water, must be resorted to. When they are chronic and painful, without redness and inflammation, the greatest relief will be experienced by the application of the ointment of iodine and morphine (see Form 53), also by the internal employment of iodine in doses of five to ten drops twice or three times a day. Where they are very obstinate, blisters will be often useful in promoting absorption. When they ulcerate, the treatment for chancres must be had recourse to. But the most invaluable remedy, alone or in conjunction with any of the preceding, is the vapor bath; it seldom fails to give instantaneous relief. I have seen patients, who were rendered almost insensible by the pain of nodes in the head, chest, and other parts of the body, experience an entire remission of the pain, and a diminution of the swelling, by the application of one bath; and a course of six or a dozen is rarely inefficient in effecting permanent recovery.
Their treatment, of course, must be guided by various circumstances. When the pain and inflammation are severe, you should use leeches, bloodletting, warm compresses, or cold evaporating lotions made of vinegar and water. When the issues are chronic and painful, without redness and inflammation, the best relief comes from applying iodine and morphine ointment (see Form 53), along with taking iodine internally in doses of five to ten drops two to three times a day. If the condition is very stubborn, blisters can often help promote absorption. When ulcers develop, treatment for chancres should be implemented. However, the most invaluable remedy, either alone or alongside any of the previous treatments, is the vapor bath; it rarely fails to provide instant relief. I have seen patients who were nearly insensible from the pain of nodes in their head, chest, and other areas experience complete relief from pain and a reduction in swelling after just one bath; a series of six to twelve baths is rarely ineffective for achieving lasting recovery.
It has already been mentioned that rheumatism of the bones and joints, and in fact of various parts of the body, is unfortunately but too frequently an accompaniment or a consequence of syphilitic disease: and an observer will discover that nodes rarely exist without rheumatic inflammation (of which by-the-by they are a species) being more or less present.
It has already been mentioned that arthritis affecting the bones and joints, and in fact various parts of the body, is unfortunately a common occurrence or a result of syphilis: and a person observing this will find that nodes rarely exist without some level of rheumatic inflammation (which, by the way, they are a type of) being more or less present.
SECONDARY SYMPTOMS.
In the same manner as bubo, which is more usually preceded by ulceration, but which may occur without it, secondary symptoms, or that form of the disease wherein the constitution is involved, may be carried into the circulation without any local effect on the part to which the poison was first applied being produced; or, in other words, secondary symptoms need not necessarily be preceded by primary. I have already stated that secondary symptoms are also much modified, both as to the time, form, and severity of their appearance, by the state of health of the patient affecting and affected; and hence the varied degrees of syphilitic maladies. By referring to past pages, it will be seen that the mucous membrane of the throat and nose,[124] the skin or surface of the body, and the periosteum and bones, are the structures in which secondary symptoms develop themselves, and accordingly I now proceed to their several consideration in detail. To illustrate each of them practically, I will first select diseases of the skin. They consist of four marked species, distinguished as the scaly, papular, pustular, and tubercular.
In the same way as bubo, which is usually preceded by ulceration but can occur without it, secondary symptoms, or the type of the disease that impacts the overall health, can enter the bloodstream without any local effects at the initial site where the poison was applied; in other words, secondary symptoms don’t have to be preceded by primary ones. I have already mentioned that secondary symptoms are also significantly influenced by the health status of the patient, both in terms of their onset time, form, and severity, leading to the various degrees of syphilitic diseases. By looking back at earlier pages, you’ll see that the mucous membranes of the throat and nose,[124] the skin or body surface, and the periosteum and bones are the areas where secondary symptoms manifest, and so I will now discuss each of these in detail. To illustrate them practically, I will first focus on skin diseases. They consist of four distinct types: scaly, papular, pustular, and tubercular.
The most frequent form of eruption is the scaly, and called syphilitic lepra. It is characterized by dry, flat, and round patches, of different sizes, and of a coppery-red color. Each spot is ushered in by a minute but hard elevation of a purplish hue, that gradually radiates in size until it acquires its limit. It then puts on a scaly appearance, and, as it desquamates, with the exception of the centre, which is sometimes left white, maintains its copper color. These patches may be distinguished from ordinary leprosy by their color, and their running on to ulceration, if uncontrolled by medicine, and again by their more speedily yielding to judicious treatment; when they become paler in appearance, cease to exfoliate, and die away, leaving, however, a coppery stain. Syphilitic eruptions occur in all parts of the body, and are to be observed on the head, face, back, legs, feet, hands, scrotum, &c. (see wood-cut, page 118), but they are much modified in their external characters by the region they affect.
The most common type of eruption is scaly and is known as syphilitic lepra. It features dry, flat, round patches of various sizes that have a coppery-red color. Each spot starts with a small but firm elevation that has a purplish hue, which gradually expands until it reaches its full size. Then, it takes on a scaly look, and as it sheds, except for the center—which can sometimes remain white—it keeps its copper color. These patches can be distinguished from regular leprosy by their color and the way they can ulcerate if left untreated, as well as by how they respond more quickly to proper treatment. They become paler, stop flaking, and eventually fade away, but they leave behind a coppery stain. Syphilitic eruptions can appear on all parts of the body and are seen on the head, face, back, legs, feet, hands, scrotum, etc. (see wood-cut, page 118), but their external characteristics can greatly vary based on the region they affect.
The pustular form of syphilitic eruption is also illimitable as to situation and extent. The pustules, at the onset, are scarcely to be distinguished from the patches of lepra, being of similar color. They differ in size, some being very large, and others very small. When they have existed about a week, a purulent fluid escapes, which hardens and crusts, constituting a conoid tumor, and surrounded by a copper-colored areola. This crust after a while drops off, leaving the under surface of the same teint as the margin. The pustular form of the disease is mostly consecutive to primary infection of the genital organs, and is often complicated with affections of the throat, nose, &c.
The pustular form of syphilitic eruption can appear anywhere on the body and can vary greatly in size. At first, the pustules are hard to distinguish from leprosy patches because they are similar in color. They vary in size, with some being very large and others quite small. After about a week, a purulent fluid oozes out, which then hardens and forms a crust, creating a cone-shaped bump surrounded by a copper-colored ring. Eventually, this crust falls off, revealing skin underneath that has the same color as the surrounding area. This pustular form of the disease usually follows a primary infection of the genital area and is often complicated by issues in the throat, nose, etc.
Syphiloid tubercles ordinarily attack the face, more particularly the nose, angles of the lips, ears, &c. They vary in size, are dispersed or grouped together, and are of a purplish copper color. Like the pustular, they terminate in ulceration, which on healing leaves an indelible scar. This and other forms of syphilitic disease are very irregular[125] in their attacks, first selecting one spot, then another, then several together, so that the body presents often at the same time many stages of the eruption. The papular form of eruption is generally intermixed with the pustular and tubercular. It is less strongly marked, but, like the others, successive in its development, and usually complicated with primary symptoms.
Syphiloid tubercles usually appear on the face, especially on the nose, the corners of the lips, ears, etc. They come in different sizes, can be dispersed or grouped together, and have a purplish copper color. Like pustules, they lead to ulceration, which, when healed, leaves a permanent scar. This and other types of syphilitic disease are very unpredictable in their appearance, initially affecting one area, then another, and sometimes multiple areas at once, so the body often shows many stages of the eruption simultaneously. The papular type of eruption typically mixes with the pustular and tubercular forms. It is less pronounced, but like the others, it develops in stages and is usually linked with primary symptoms.[125]
There is a form of cutaneous disfigurement, entitled syphilitic exanthema, in which the skin is discolored by coppery-red blushes that disappear under pressure of the finger. There are also deep and painful fissures and excrescences, called vegetations, from their resemblance to raspberries, strawberries, cauliflowers, and leeks, observed in syphilis, and most commonly they are to be found about the lips, nose, eyebrows, chin, genitals, &c.
There is a type of skin condition called syphilitic exanthema, where the skin shows coppery-red discolorations that fade when you press on them. There are also deep and painful cracks and growths, known as vegetations, because they look like raspberries, strawberries, cauliflowers, and leeks, which are seen in syphilis, typically around the lips, nose, eyebrows, chin, genitals, etc.
It may not be unimportant to know that syphilitic eruptions are contagious by inoculation, and that secondary symptoms may be transmitted from one individual to another.
It might be worth noting that syphilitic rashes are contagious through inoculation, and that secondary symptoms can be passed from one person to another.
When I was a pupil of the London hospital, a woman and her child presented themselves for treatment. The mother was completely covered with copper-colored scaly eruptions, obviously and unequivocally syphilitic. The child also had venereal sore throat, and ulceration of the mouth. The account which the mother gave of herself was, that the eruption appeared a few weeks after her confinement; and, upon further inquiry, it was discovered that the husband had had a chancre of the penis: that was cured, but secondary symptoms showed themselves upon him. It was during the presence of the latter that he had intercourse with his wife, at about the sixth month of her pregnancy. The surgeon of the week gave it as his opinion, that the disease was conveyed by the male semen being absorbed by the mother, which was sufficient to occasion the disease. The mother, husband, and child, all submitted to mercurial treatment and fumigations, and in a few weeks entirely recovered.
When I was a student at the London hospital, a woman and her child came in for treatment. The mother was completely covered in copper-colored scaly rashes, clearly indicative of syphilis. The child also had a venereal sore throat and mouth ulcers. The mother explained that the rash appeared a few weeks after she gave birth; upon further questioning, it was found that the husband had a penile chancre, which had been treated but secondary symptoms emerged later. It was during this time that he had sexual relations with his wife, about six months into her pregnancy. The surgeon on duty stated that the disease was transferred through the male semen being absorbed by the mother, which was enough to cause the illness. The mother, father, and child all underwent mercurial treatment and fumigations, and within a few weeks, they fully recovered.
Treatment of Secondary Symptoms.—Now in the treatment of these cases, all of which are more than skin deep, it is evident that, unless the cause which produces them be expelled, all local repellants only exhaust the physical energies of the patient; for the cure by such means but provokes a speedier reproduction of the disease, and hence the necessity of constitutional as well as topical remedies.[126] I have fully explained my views regarding the employment of mercury; and every day’s experience convinces me that, where the constitution is imbued with the venereal virus, there is no alternative but to employ the most active alteratives, to effect a decisive and speedy change in the state of the patient’s health. Various habits require various preparations; the blue pill, the oxymuriate, calomel, and the external application of the unguentum hydrargyri fortius, are highly useful. I have, however, of late, been in the habit of employing the proto-ioduret of mercury, with unqualified success; nor do I limit its administration to internal exhibition; it may be used externally. The advantage of this preparation over others is, that it rarely, if ever, produces ptyalism.
Treatment of Secondary Symptoms.—In treating these cases, which go deeper than just skin deep, it’s clear that unless the underlying cause is addressed, all local treatments will only drain the patient’s physical energy; because such remedies often lead to a quicker return of the disease, there’s a need for both systemic and topical treatments.[126] I have thoroughly outlined my perspective on the use of mercury, and every day’s experience shows me that when the body is infected with the venereal virus, the only option is to use the most effective remedies to bring about a quick and substantial improvement in the patient’s health. Different circumstances require different preparations; the blue pill, oxymuriate, calomel, and the external application of unguentum hydrargyri fortius are all highly effective. Recently, I’ve been using proto-iodide of mercury with great success; I do not restrict its use to internal treatment; it can also be applied externally. The benefit of this preparation compared to others is that it hardly ever causes ptyalism.
In old and inveterate cases, combined with the use of the warm and vapor bath, both of which may be impregnated with it, it has wrought wonders; and in cases that had proved rebellious to every other means, although sedulously employed, it had effected a speedy and decisive cure. In the cure of an elderly person, covered almost from head to foot with syphilitic ulceration, the internal and external application of the proto-ioduret occasioned, at the end of a few weeks, the entire disappearance of the sores, leaving only a slight livid trace. In ulceration of the throat, nose, and in fissures of the genitals, indolent buboes, &c., the success is no less remarkable than effectual.
In long-standing and stubborn cases, along with the use of warm and steam baths, both of which can be infused with it, it has done amazing things; and in cases that were resistant to all other treatments, even those used carefully, it achieved a quick and definite cure. In the treatment of an elderly person who was almost entirely covered in syphilitic ulcers, the internal and external use of the proto-iodide led, after a few weeks, to the complete disappearance of the sores, leaving only a faint dark mark. The results are just as impressive and effective in cases of throat and nose ulcers, as well as in genital fissures and swollen lymph nodes, etc.
The following is the formula, which may of course be altered according to circumstances:—
The following is the formula, which can obviously be adjusted based on circumstances:—
| Take of the— | |||
| Proto-ioduret of mercury | 20 | grains. | |
| Gum guaiacum, in powder | 1 | drachm. | |
| Confection of roses, as much as is sufficient. | |||
| Mix to form 36 pills—one to be taken twice or thrice a day. | |||
| For external use, take of the— | |||
| Proto-ioduret of mercury | 1 | drachm. | |
| Lard | 2 | oz. | |
| Mix. | |||
| A portion to be rubbed over, or to dress the affected parts twice a day. If the ulceration be seated in the throat, honey of roses may be substituted for the lard. [127] | |||
| The decoction, or any other preparation of sarsaparilla, may be taken also in conjunction with the treatment just suggested. | |||
| An ounce of the sarsaparilla root infused in one pint of lime-water (cold) for twenty-four hours, and a wineglassful taken three times a day, is a very eligible mode of taking it. Or— | |||
| The compound extract of sarsaparilla, dissolved in lime or soft water, one ounce to the pint, and taken in similar doses to the last, is a very good mode of exhibition. | |||
| Bathing is indispensable. | |||
SYPHILITIC LEPRA.
A person aged about 29 years suffered under the above disease, and presented the following appearances and symptoms: He was covered nearly all over with copper-colored spots, the margins of which were both elevated and red. The voice of the patient was rather hoarse, and he complained also of a tenderness on swallowing: the pain extended to the windpipe and tonsils (or almonds) of the ear, as they are called. He experienced pain in his limbs, which he described to be worse at night when in bed. The spots on the skin every now and then desquamated, or peeled, or scurfed off, leaving the cuticle red and shiny underneath, and here and there the cutis was ulcerated. On examining the throat, the swallow appeared very inflamed, and the “pap” very pendulous. He was hot and feverish, and acknowledged that he had had the venereal disease about nine weeks ago, and for which he had taken some medicines that he bought, and which had cured him. When in bed, he complained of a burning, tingling, and itching of the body, wherever it was covered with the eruption.
Someone around 29 years old was suffering from the aforementioned disease and showed the following signs and symptoms: He was almost completely covered with copper-colored spots that had raised, red edges. His voice was somewhat hoarse, and he also reported pain when swallowing; the pain extended to his windpipe and tonsils (or almonds, as they are sometimes referred to). He felt pain in his limbs, which he said was worse at night while he was in bed. The spots on his skin occasionally peeled off, leaving the surface underneath red and shiny, and in some areas, the skin was ulcerated. Upon examining his throat, it appeared very inflamed, and the “pap” was very droopy. He was hot and feverish and admitted that he had had a sexually transmitted infection about nine weeks ago, for which he had taken some over-the-counter medications that he bought, and which had cured him. When in bed, he complained of a burning, tingling, and itching sensation on his body wherever the rash was present.
The treatment was as follows: I bled him to the amount of twelve ounces, and prescribed a strong aperient powder. On the second day there was less irritation, and the spots appeared less red. I advised him forthwith to take a vapor bath, and repeat the same on alternate days for a fortnight. I prescribed the pills as subjoined, and directed one to be taken twice a day, to be succeeded by a dose of the decoction of woods, as directed already.
The treatment was as follows: I drew twelve ounces of blood and prescribed a strong laxative powder. On the second day, there was less irritation, and the spots looked less red. I advised him to take a steam bath immediately and to continue this every other day for two weeks. I prescribed the pills listed below and instructed him to take one twice a day, followed by a dose of the herbal decoction, as previously directed.
| Take of— | |||
| Proto-ioduret of mercury | 20 | grains. | |
| Gum guaiacum, in powder | 1 | drachm. | |
| To be well mixed together, and made into a mass with syrup, and then divided into 24 pills. | |||
| The body, on coming out of the vapor bath, or while in it, to be sponged over with the following wash made warm | |||
| Take of the— | |||
| Deuto-chloruret of mercury | 1 | drachm. | |
| Eau de Cologne | 1 | oz. | |
| Water | 1 | pint. | |
| Mix. | |||
Occasionally I order the patient to be placed in a mercurial bath, of which there are several kinds, and which can be administered either in the form of the fumigation or in a fluid state.
Occasionally, I instruct that the patient be put in a mercury bath, of which there are several types, and which can be given either through fumigation or in liquid form.
After taking the bath, he could breathe with freedom and comfort; he could also swallow without difficulty, and he expressed himself much refreshed and invigorated. Many of the eruptive spots on the body had exfoliated; and he said he felt a conviction that he should soon get well.
After taking a bath, he could breathe freely and comfortably; he could also swallow without any issues, and he said he felt much more refreshed and energetic. Many of the spots on his body had healed; and he felt certain that he would be better soon.
At the expiration of a week, when he had taken but three baths, the soreness of the throat had left, the pains in his limbs were all gone, and he slept well; the ulcers had healed, and the eruption had nearly died away. I advised a continuation of all the remedies; and after three weeks of such perseverance, he was rewarded by an entire recovery. The only alteration I directed to be made in his diet was an abandonment of stimulants, such as wine, spirits, or porter.
After a week had passed, during which he only took three baths, the sore throat was gone, the aches in his limbs had disappeared, and he was sleeping well; the ulcers had healed, and the rash had almost faded away. I recommended continuing all the treatments, and after three weeks of sticking to it, he fully recovered. The only change I advised for his diet was to stop consuming stimulants like wine, spirits, or beer.
NODES AND PAINS IN THE BONES.
In long-standing cases of syphilis, where either much mercury has been taken, or the constitution weakened by low living or careless treatment, a painful affection of the bones, periosteum, tendons, and ligaments, frequently arises. Where the inflammation attacks the bone or periosteum, it usually exhibits itself in the form of a tumor, that is at first hard and acutely painful, then becomes soft, and does not always subside without ulcerating, and occasioning[129] a tedious and unhealthy sore. These tumors are called nodes, and are extremely rapid in growth, very uncertain in their duration, and sometimes disappear as quickly as they come. When the inflammation is seated in the ligament and tendons, rheumatism is established. Both these affections are very harassing to the patient; the pains are severest at night, and wholly prevent sleep, the countenance becomes sallow, appetite, strength, and flesh fail, and hectic fever completes the list of troubles consequent upon these forms of the disease. Nodes and rheumatic pains may exist independently of, or in connexion with, other syphilitic symptoms. Cases having already been related of gonorrhœal rheumatism, which are analogous to those proceeding from venereal absorption, any further detail of such would be superfluous. The treatment should also be conducted on the same principles in the one as in the other.
In long-term cases of syphilis, where a lot of mercury has been used, or the body's condition has been weakened by poor living or careless treatment, a painful issue involving the bones, periosteum, tendons, and ligaments often develops. When inflammation affects the bone or periosteum, it usually shows up as a tumor that starts off hard and very painful, then becomes soft, and often does not go away without ulcerating, leading to[129] a long-lasting and unhealthy sore. These tumors are called nodes, and they grow extremely quickly, can be unpredictable in how long they last, and sometimes vanish as fast as they appear. When inflammation occurs in the ligaments and tendons, rheumatism sets in. Both conditions are very distressing for the patient; the pain is at its worst at night and completely prevents sleep, the face turns sallow, and appetite, strength, and weight diminish, with hectic fever adding to the list of complications from these types of the disease. Nodes and rheumatic pains can exist on their own or together with other syphilitic symptoms. Cases of gonorrheal rheumatism have already been mentioned, which are similar to those arising from venereal absorption, so further details on that would be unnecessary. The treatment should also follow the same principles in both cases.
The specific virtues of the vapor bath will be attested by one trial. I have seen innumerable instances of immediate relief from a single application. There are few forms of syphiloid disease more distressing than these pains in the bones; the patient is all but distracted with the agony he endures. The relief he experiences from the vapor bath surpasses belief; it verily appears to be magical. It constitutes the best opiate we have.
The benefits of the vapor bath will be confirmed by just one try. I’ve seen countless cases of instant relief from a single use. There are few types of syphilitic disease more agonizing than these bone pains; the patient is nearly driven insane by the suffering they go through. The relief they feel from the vapor bath is unbelievable; it truly seems magical. It serves as the best painkiller we have.
Temporary relief, however, is not all that we want. It is no use to remove the effect, and leave the cause behind. The aid of medicine is indispensable. Formulæ of the most appropriate remedies will be found among the prescriptions. The general directions as to diet, regimen, and clothing, dispersed throughout these pages, must be strictly attended to. The stomach must not be at any time overloaded with indigestible food. Milk diet is the best; milk thickened with farinaceous food, mild tonics to restore the tone of the stomach and impart strength, alteratives, sarsaparilla (Form 58), the old Lisbon diet drink, and all the suggestions[130] hitherto offered with a view of improving the constitution, should be carried into effect.
Temporary relief, however, isn’t all we want. It’s pointless to remove the symptoms while leaving the cause. Medical help is essential. You’ll find the most suitable remedies listed among the prescriptions. The general guidelines about diet, exercise, and clothing throughout these pages must be followed carefully. The stomach should never be overloaded with hard-to-digest food. A milk-based diet is best; milk combined with starchy foods, gentle tonics to restore stomach function and provide strength, alternatives, sarsaparilla (Form 58), the traditional Lisbon diet drink, and all the suggestions[130] made so far to improve overall health should be implemented.
SYPHILITIC SORE THROAT.
The period that elapses between the appearance of the primary and secondary symptoms has already been stated to vary from six weeks to six months; and some medical writers assert that, if months may elapse, upon the same principle years may, and therefore the patient who has once been afflicted with the primary form of the disease is never exempt from the liability of the secondary. That syphilis, and diseases resembling it, do occur at every period of life, is a fact of daily observation; and it is a matter of less moment to know whether the invalid has ever had chancre or bubo than is generally supposed, for the treatment of every form of syphilis, and complaints putting on like appearances, should be conducted on similar principles. If mercury do possess anti-venereal properties, it will be found no less obnoxious to ordinary sore throats, ordinary ulceration, and cutaneous disfigurement. The presence of any of the abovenamed diseases indicates a habit predisposed to their occurrence; and that susceptibility may be induced by a variety of causes, the most prominent of which are those that debilitate the constitution, such as syphilis itself, or the remedies exhibited for its extermination, cold, fever, intemperate or impoverished diet—all of which more or less abstract from, or derange the distribution of, nervous energy. As in the cure of these diseases, their removal depends upon an entire alteration of the system, upon that principle alone should mercury, or any other remedy be administered, not upon its supposed specific neutralizing or annihilating antisyphilitic power.
The time between the onset of primary and secondary symptoms can range from six weeks to six months, and some medical writers argue that if months can pass, then years can also. Therefore, a patient who has experienced the primary form of the disease is never completely free from the risk of the secondary. It is a well-known fact that syphilis and similar diseases can occur at any age; it matters less whether the patient has ever had a chancre or bubo than is commonly believed. The treatment for all forms of syphilis and related conditions should follow similar principles. If mercury has anti-venereal properties, it can also cause issues with regular sore throats, standard ulceration, and skin disorders. The presence of any of these diseases shows a tendency for them to occur, and this susceptibility can be triggered by various factors, especially those that weaken the body, such as syphilis itself, the treatments used against it, cold, fever, or an unbalanced diet—all of which can disrupt the flow of nervous energy. In treating these diseases, their elimination relies on a complete change in the system; thus, mercury or any other remedy should be given based on this principle, not on a presumed ability to specifically neutralize or eliminate syphilis.
All this, of course, is a question of experience; and as I profess that this work should convey the result of mine, I do not hesitate to express my conviction that secondary symptoms do present themselves years after a primary affection; but at the same time I admit their more frequent occurrence to be within three months; and, with regard to diseases resembling the above, they are entirely independent of such influences, and are the result of circumstances from which no man is free. Of syphilitic ulcerations of the throat, which are rarely solitary symptoms of[131] the disease, being usually accompaniments to articular eruptions or rheumatic pains, there are several forms. They are ushered in by feverishness, languor, and a peculiar contour of the countenance, particularly expressive of anxiety and debility. Of the first form of ulcerated throat, and which is perhaps the least frequent, is an excavation of the tonsil, with a tumid and red margin, accompanied by a stiffness and uneasiness in swallowing. A more common form, and which, from its occasioning little or no inconvenience, is seldom discovered by the patient until it degenerates into a worse state, is that where the ulceration is more superficial, resembling fissures rather than ulcers, and being situated at the back part and edges of the tonsils, and low down the throat. From the absence of pain and difficulty in swallowing, the medical man is usually the first to detect it, when, on opening the mouth, the throat—that is, the hinder part of the fauces—will be discovered red and somewhat swollen; and on pressing down the tongue with a spoon or spatula, the ulceration will be apparent.
All this is really about experience; since I believe this work should reflect my own, I’m confident that secondary symptoms can show up years after a primary condition. However, I also acknowledge that they more commonly appear within three months. As for diseases that are similar, they are completely independent of such factors and arise from circumstances that affect everyone. Regarding syphilitic ulcers in the throat, which are rarely the only symptoms of the disease and usually occur alongside joint eruptions or rheumatic pain, there are several types. They often start with fever, fatigue, and a distinctive look on the face, which shows signs of anxiety and weakness. The first type of ulcerated throat, which is perhaps the least common, involves a cavity in the tonsil, with a swollen and red edge, along with stiffness and discomfort when swallowing. A more common type, which usually causes little or no trouble, is often unnoticed by the patient until it worsens; this type has more superficial ulcers that resemble cracks rather than full-blown ulcers, located at the back and sides of the tonsils and lower down the throat. Because there’s little pain and no difficulty swallowing, doctors typically are the first to spot it. When they open the mouth, they’ll see that the throat, or back part of the fauces, is red and somewhat swollen; pressing down the tongue with a spoon or spatula will reveal the ulceration.
The last form—the phagedenic—is the most formidable, both in symptoms and effects. It is characterized by fever, and great pain and difficulty in swallowing, from the beginning; all denoting acute inflammation of the throat. The first appearance of ulceration is on the soft palate, where a small aphthous spot is discovered, surrounded by a deep erysipelatous redness, that proceeds rapidly to involve the neighboring parts, which soon assume the appearance of one extensive slough. This latter disease requires prompt and active treatment, else the bones of the palate and nose become implicated, exfoliate and occasion a permanent deformity.
The last type—the phagedenic—is the most serious, both in symptoms and effects. It starts with fever, along with severe pain and difficulty swallowing, indicating a strong inflammation of the throat. The first sign of ulceration appears on the soft palate, where a small sore is seen, surrounded by a deep, red, inflamed area that quickly spreads to nearby tissues, making them look like one large ulcer. This condition needs fast and effective treatment; otherwise, the bones of the palate and nose can be affected, leading to their removal and causing lasting deformity.
The process of cure in these cases must be regulated by circumstances. In persons of full habit, blood-letting will be requisite to arrest at once the inflammation. An active purgative should also be taken; when, if the ulceration resist these anti-phlegmonous measures, there is no alternative left but to subject the system to the influence of mercury. The proto-ioduret pill will be found the best form, and the diet drink should be taken in conjunction. The vapor bath, which can be medicated with poppies, marsh-mallows, and ivy-leaves, or any other emollient herb, will be found to ease deglutition, promote perspiration, and afford ease. Local applications, such as gargles,[132] styptics, &c., are indispensable. Subjoined are a few formulæ, with remarks:—
The healing process in these cases needs to be adapted based on the situation. For individuals with a strong constitution, bloodletting is necessary to immediately reduce inflammation. An effective laxative should also be used; if the ulceration doesn't respond to these anti-inflammatory treatments, the only option left is to expose the body to mercury. The proto-ioduret pill is considered the best option, and it should be taken along with the dietary drink. The vapor bath, which can be infused with poppies, marshmallows, ivy leaves, or any other soothing herb, will help ease swallowing, encourage sweating, and provide relief. Local treatments, such as gargles, styptics, etc., are essential. Below are a few formulas, along with remarks:—
| Gargle for the milder form of sore throat. |
| Take of— | |||
| Honey of borax | 1 | oz. | |
| Emulsion of bitter almonds | 5 | oz. | |
| Mix. To be used six or seven times a day. | |||
| Or take of— | |||
| Infusion of bark | 6 | oz. | |
| Diluted nitric acid | 40 | drops. | |
| Mix. | |||
| Where the ulcers have an indolent, or present a sloughy appearance, either of the following will prove useful stimuli:— |
| Take of the— | |||
| Oxymel of Verdigris | 1 | oz. | |
| The ulcer to be smeared with this preparation, with a hair pencil, twice or thrice a day. | |||
| Or, take of the muriated tincture of iron a small quantity, to be used in like manner. | |||
| Honey of roses, acidulated with muriatic acid, is a very agreeable astringent. | |||
| In severer cases, such as the phagedenic ulceration, the subjoined prescription will be found worthy of a trial:— | |||
| Take of the— | |||
| Oxymuriate of mercury | 1 | grain. | |
| Mucilage of quince seed | 6 | oz. | |
| To be mixed to form a gargle, to be used frequently. | |||
Ulceration of the larynx is an occasional consequence of syphilis; but fortunately a rare one, as it is generally fatal.
Ulceration of the larynx is a rare complication of syphilis; however, it's fortunately uncommon, as it is usually deadly.
All the symptoms enumerated in this section have been known to succeed gonorrhœa, and demand similar treatment. The advocates for the analogy between gonorrhœa and syphilis herein find a ready explanation for such an[133] occurrence, which those adverse to the above opinion have no other means of controverting than by submitting that its rarity is no very substantial proof. Similar results also transpire from the imprudent, or too free use of mercury. The following case is a prototype of the many:— The patient was a person about thirty years of age, and was thus affected: there was considerable inflammation in the entire back part of the throat; the tonsils were excavated to some depth by ill-looking ulcers, the uvula shared also in partial destruction; the tongue was swollen, the tip and front part of it fissured, and on the left side an irritable ulcer was apparent; the nose discharged a disagreeable fluid, and occasionally gave off crusts of hardened secretion. The body of this person, including the head, was thickly sprinkled with venereal blotches of the usual copper color. His health was much impaired, and he stated the disease to have been of nearly twelve months’ duration from the first to the last.
All the symptoms listed in this section have been known to follow gonorrhea and require similar treatment. Supporters of the comparison between gonorrhea and syphilis provide a clear explanation for this occurrence, while those who disagree with this view argue that its rarity is not strong evidence against it. Similar outcomes can also arise from the careless or excessive use of mercury. The following case is a typical example: the patient was around thirty years old and presented with significant inflammation in the entire back part of the throat; the tonsils were deeply ulcerated, the uvula was partially damaged; the tongue was swollen, with cracks on the tip and front, and there was an annoying ulcer on the left side; the nose discharged an unpleasant fluid and occasionally produced crusts of hardened secretion. The patient's body, including the head, was covered in venereal blemishes of the usual copper color. His health was severely affected, and he reported that the disease had lasted nearly twelve months from beginning to end.
The treatment consisted of the exhibition of mercury in the form of the proto-ioduret, and the sarsaparilla. The ulcers were touched with nitric acid, and submitted to mercurial fumigation. At the end of two months he was convalescent. In cases of ulceration of the throat and nose, I have used the nitrate of silver, both in substance and solution, with good effect.
The treatment involved using mercury in the form of proto-iodide and sarsaparilla. The ulcers were treated with nitric acid and underwent mercurial fumigation. After two months, he was on the mend. In cases of throat and nose ulcers, I've had good results using silver nitrate, both as a solid and in solution.
ADVICE TO INVALIDS.
Having now fully considered every form of syphilitic disease compatible with the design of this work, a few hints relative to the after-management of the patient when relieved from his complaint, to guard against a relapse, and to secure an entire restoration to sound health, may not detract from its utility. There are many patients who, on the disappearance of the more prominent symptoms of their complaint, lose no opportunity of rejoicing in their supposed recovery, and innocently commit sundry inapparent irregularities, that throw them back to their former state of suffering, which a little prudence and attention might have prevented. The more severe the disease has been, the slower, generally, is the recovery, and also less permanent in its result. The mere subsidence of pain, the healing of a wound, the disappearance of a cuticular[134] eruption, or the suppression of a morbid secretion, are not in themselves sufficient indications of substantial recovery. The various physical and mental functions which, during illness, are always more or less involved, have yet to regain their tone. The digestive powers of the stomach are easily deranged, and require watchful management to secure the vantage gained. Equal care is essential, lest the intellectual organs be too prematurely called into active employment. Convalescence is often protracted to an almost indefinite period, frequently from the most trifling errors in diet. The stomach of a person reduced to a low state of debility through a severe inflammatory disorder, remains for a long time exceedingly sensitive, and fails not to evince displeasure when oppressed with indigestible, or too great a quantity of food. No cause predisposes the patient to a relapse, or retards his recovery, so much as inattention to diet. It is a popular error to suppose that the weakness consequent upon severe illness is only to be removed by rich and substantial food and wines, and other stimulating drinks. Such indiscretion often rekindles the disease, or predisposes the system to the supervention of some other complaint. The change from the sick-room to the parlor diet should be gradual and progressive. The milk and farinaceous meal may be varied by degrees to the milder forms and preparations of animal food. Solids should be given at first in small quantities; the diet should be rigidly adhered to, and in the change from low to full diet, the intermediate one should not be skipped over.
Having now fully considered every type of syphilitic disease relevant to this work, a few suggestions for post-treatment management of the patient—once relieved of their illness—to prevent a relapse and ensure a complete return to good health, may be helpful. Many patients, upon the disappearance of the more obvious symptoms, are quick to celebrate what they think is their recovery and unknowingly engage in various subtle irregularities that can lead them back to their previous state of suffering, which could have been avoided with a bit of caution and attention. The more severe the illness has been, generally, the slower the recovery, and the less lasting the results. The simple resolution of pain, the healing of a wound, the vanishing of a skin eruption, or the stopping of an abnormal secretion do not in themselves indicate genuine recovery. The various physical and mental functions, which are usually affected during illness, still need to regain their proper function. The digestive abilities of the stomach can easily be disrupted and need careful management to maintain the progress made. Equal caution is necessary to avoid overworking the mind too soon. Recovery can often take a surprisingly long time, often due to minor mistakes in diet. The stomach of a person weakened by a serious inflammatory illness remains extremely sensitive for a long time and will show discontent when burdened with indigestible food or too much food at once. No factor contributes to a relapse or delays recovery as much as neglecting diet. It's a common misconception that the weakness after severe illness can only be overcome with rich, heavy foods and wines, or other stimulating beverages. Such mistakes often reignite the disease or make the body susceptible to new health issues. The transition from a sickroom diet to a regular diet should be gradual and careful. Milk and light meals can be slowly adjusted to include gentler forms and preparations of animal protein. Solids should be introduced in small amounts at first; the diet should be strictly followed, and the shift from a low to a full diet should not skip any intermediate stages.
With regard to medicines, in no form of disease is it so important, as in venereal affections, that they should be continued for some time after the disappearance of symptoms. Many a relapse of gonorrhœa and secondary symptoms have occurred through the sudden abandonment of the means adopted for their cure.
When it comes to medications, there's no type of illness where it’s more crucial, especially in sexually transmitted infections, to continue treatment for a while even after the symptoms have gone away. Many cases of gonorrhea relapse and secondary symptoms have happened because treatment was abruptly stopped.
Exercise forms another important part of management in convalescence; it should not be suddenly resumed, nor should fatigue by any means be incurred. Early retiring to bed, and early rising in the morning, tend considerably to promote and preserve health. Warm clothing is very essential and necessary for invalids.
Exercise is also a key part of recovery management; it shouldn't be started abruptly, and fatigue should definitely be avoided. Going to bed early and waking up early in the morning greatly helps maintain and enhance health. Warm clothing is very important and necessary for those who are unwell.
The general signs of amendment are as follows: a reduced frequency of the pulse, which is always accelerated in acute diseases, the absence of thirst, a clean tongue, a[135] moist skin, a good appetite, and refreshing sleep; and, lastly, all these are corroborated by an improvement in the looks. The improved aspect of the countenance has always been regarded as a sure criterion of returning health.
The general signs of improvement are as follows: a slower pulse, which is usually fast in acute illnesses, no thirst, a clean tongue, a[135]moist skin, a healthy appetite, and restful sleep; and, finally, all these are supported by a better appearance. A better look on the face has always been seen as a reliable indicator of returning health.
The female genitals occupy the same relative situation in the pelvis as the male, but they are an antithesis to each other. The male are constructed to deposite, and the female to receive; consequently, in the female there is a conduit or passage, in place of the male penis, termed the vagina, leading to the womb—the receptacle for the impregnating fluid. The vagina is placed between the bladder and rectum. Its entrance is marked by doublings, or longitudinal folds of flesh, called labia, between the upper part of which is the opening of the urethra into the bladder, while below is occupied by the aperture, passage, or fissure, as above described. At the roof of the vagina is a fleshy ridge, with a pouting apex or point analogous to the penis in the male, except being impervious, and called the clitoris, which possesses the power of erection, or rather of becoming intumescent when excited, and also of furnishing a peculiar secretion. It is exquisitely sensitive, and believed to be the seat of pleasure in the sexual embrace. The vagina consists of a very soft, vascular, elastic, and contracting structure, constituting, when its sides are collapsed, liliputian rugæ, or ridges, like the impressions left on the sand by a receding sea. Its surface is lined by a delicate mucous membrane, which secretes a lubricating fluid. It is this membrane which is the seat of gonorrhœal discharge, fluor albus, &c.; and it is also subject to ulcerations and other diseases. From the clitoris is suspended an inner fold, like a graceful mantle, called nymphæ, which are also extremely sensitive, and appear to serve, as they surround the urethra, also for the purpose of directing the flow of urine. Under the opening of the urethra, adherent to the external margins of the vagina, is a membranous veil, or curtain, with a small central aperture, called the hymen, the presence of which is looked upon as a test of virginity. After the laceration or dilatation of this membrane, which takes place through other causes than sexual intercourse, the sides of it contract, and form[137] little wing-like slips, to which the fanciful name of carunculæ myrtiformes is applied.
The female genitals are positioned in the pelvis similarly to the male ones, but they have opposite functions. The male anatomy is designed for depositing, while the female is meant for receiving; therefore, the female has a passage called the vagina, which leads to the womb—the place for the sperm. The vagina is situated between the bladder and the rectum. Its entrance is defined by folds of flesh known as labia, with the urethra opening into the bladder at the upper part, and the vaginal opening below. At the top of the vagina is a fleshy ridge with a protruding tip similar to the male penis, known as the clitoris, which can become erect or swollen when stimulated and produces a unique secretion. It is highly sensitive and is thought to be the source of pleasure during sexual activity. The vagina is made up of soft, vascular, elastic, and contracting tissue, creating tiny ridges resembling marks left on sand by a retreating tide when its walls collapse. Its inner surface is covered by a thin mucous membrane that secretes a lubricating fluid. This membrane is where conditions like gonorrheal discharge and leucorrhea occur; it can also suffer from ulcers and other diseases. An inner fold hangs from the clitoris, resembling a delicate mantle, known as nymphæ, which are also very sensitive and help guide the flow of urine as they surround the urethra. Below the urethral opening, attached to the outer edges of the vagina, is a thin membrane called the hymen, which is often viewed as a sign of virginity. When this membrane tears or expands for reasons other than sexual intercourse, its edges can contract and form small wing-like flaps, whimsically named carunculæ myrtiformes.
The subjoined diagram will familiarize the reader with the situations of the female organs thus far given. It exhibits a sectional view of the contents of the pelvis, or lower part of the abdomen:—
The diagram below will help the reader understand the positions of the female organs mentioned so far. It shows a cross-sectional view of the contents of the pelvis, or the lower part of the abdomen:—
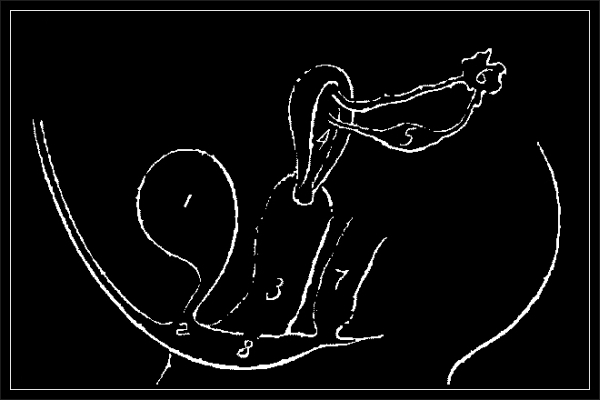
|
1. The bladder. The bladder. 2. The urethra, or entrance to ditto. 2. The urethra, or entrance to it. 3. The vagina. The vagina. 4. The womb. The uterus. 5. The ovary. The ovary. 6. The fimbria, and fallopian tube. 6. The fimbria and fallopian tube. 7. The rectum, or lower extremity of the bowel. 7. The rectum, or the lower end of the bowel. 8. The hymen. The hymen. |
Much has been said regarding the presence of the hymen in its entire state. It has been deemed by many to be there placed as a moral evidence of chastity; but its laceration is by no means an infallible test of dishonor. In females of feeble or consumptive health, and others of delicate constitutions generally, the aperture of the hymen may become dilated from natural causes—from too profuse a flow of the menstrual flux, from local debility of the part itself, such as exist in the disease known by the name of the whites; and it is sometimes to be traced to the habit of personal and solitary excitement, as will be presently alluded to. The membrane is occasionally so dense and hard as to resist sexual cohabitation; and only upon dividing it by the scalpel, can intercourse be sustained. At other times it is so fragile and so vascular as to be torn with the least violence, and profuse hæmorrhage to follow.
Much has been said about the presence of the hymen in its complete form. Many view it as a moral indicator of chastity, but its rupture is by no means a definitive sign of dishonor. In women with weak or compromised health, as well as those with generally delicate constitutions, the opening of the hymen can widen naturally—due to excessive menstrual flow, local weakness in the area, such as seen in the condition known as whites; and it can sometimes be linked to habits of personal and solitary stimulation, which will be discussed shortly. The membrane can sometimes be thick and tough enough to prevent sexual intercourse, requiring surgical division for penetration to occur. At other times, it can be so fragile and filled with blood vessels that even the slightest force can cause it to tear, leading to significant bleeding.
At the end of the vagina is the uterus. It is suspended by what anatomists call its broad ligaments, which have certain local attachments. It resembles in shape a pear. It is of a peculiar structure, capable of great distension, and possessing extraordinary properties. It is divided into a body, neck, and mouth, and when unimpregnated, is very compact, and occupies but little space. The interior is consequently very small, and it secretes and pours forth[138] at certain periods a sanguinous discharge, termed the menstrua. When conception has occurred, the mouth of the womb, which before was open, becomes permanently closed until the period of delivery. Connected with the womb, and constituting a most important part of its machinery, there are discovered in the roof of the interior of the uterus, two openings, which are the ends of two tubes or canals, called the fallopian tubes.
At the end of the vagina is the uterus. It's held in place by what anatomists refer to as its broad ligaments, which have specific local attachments. It looks like a pear in shape. It has a unique structure that can expand significantly and has remarkable properties. It's divided into a body, neck, and mouth, and when not pregnant, it is very compact and takes up little space. The inside is therefore quite small, and it occasionally secretes and releases[138] a blood discharge known as the menstrua. When conception occurs, the mouth of the womb, which was previously open, becomes permanently closed until delivery. Attached to the womb, and playing a crucial role in its function, there are two openings at the top of the interior of the uterus, which are the ends of two tubes or canals called the fallopian tubes.
These tubes have their origin in the ovaria, which are two small bodies encased in the ligamentous band supporting the uterus, and resembling the testicle of the male; hence they have been called the female testes. These ovaria contain a number of little vesicles of the size of mustard-seeds, and some of the size of a pea, in number from twelve to fifteen. These vesicles are denominated the eggs of the human species. Annexed to the ovaria are observed, surrounding the tubes, certain fimbriæ, which grasp the ovaria during the copulative act, when prolific, and squeeze out, as it were, one of these little eggs, and propel it into the uterus.
These tubes originate in the ovaries, which are two small bodies located within the ligamentous band that supports the uterus, resembling male testicles; that's why they are referred to as the female testes. The ovaries contain several tiny sacs, some the size of mustard seeds and others the size of peas, numbering from twelve to fifteen. These sacs are called the eggs of the human species. Attached to the ovaries, surrounding the tubes, are certain fimbriae that grasp the ovaries during the act of copulation when fertile, and essentially squeeze out one of these tiny eggs, pushing it into the uterus.
Still further to facilitate the understanding of the structures described in addition to the preceding diagram, the following drawing is presented. It exhibits a section of the female pelvis, and explains more fully the relative positions of its contents:—
To make it easier to understand the structures described, in addition to the previous diagram, the following drawing is provided. It shows a section of the female pelvis and explains in more detail the relative positions of its contents:—

|
|
|
a—The bony portion of the pelvis separated from its junction with its companion. a—The bony part of the pelvis disconnected from where it joins with its counterpart. b—The spinal column of the back. b—The spine of the back. c—The bladder. Bladder. |
d—The orifice of the urethra. Urethral opening. e—The body of the womb. Womb body. f—The neck of the womb. Cervix. g—The vagina. The vagina. h—The rectum, or end of the intestines. h—The rectum, or the last part of the intestines. |
The subjoined drawing illustrates the shape and appearance of the womb detached from the body:—
The drawing below shows the shape and appearance of the womb removed from the body:—

To particularize: The upper part is called the fundus; the widest part, the body; the neck, the narrow part; and the lower portion the mouth, or the os tincæ. The connexion of the fallopian tubes is well shown.
To be specific: The upper part is called the fundus; the widest part is the body; the narrow part is the neck; and the lower portion is referred to as the mouth, or the os tincæ. The connection of the fallopian tubes is clearly illustrated.
The uterus, or womb, is described by physiologists as being of a spongy structure—a structure that yields with its enlargement—that grows with its growth—that resumes the former size when disburdened of its contents. It is supplied with blood-vessels, is duly supported, has scarcely a cavity when unimpregnated, but is ever in a state of preparation for changes. Of conception we shall presently treat.
The uterus, or womb, is described by physiologists as having a spongy structure—a structure that expands as it grows—that returns to its original size after emptying. It has blood vessels, is properly supported, has almost no cavity when not pregnant, but is always ready for changes. We will discuss conception shortly.
There is one function too important to omit in this place, and this is menstruation—a term indicating a monthly periodical discharge that escapes, or which is given off, from the womb. At the commencement of this function, woman is said to have arrived at puberty; but there are cases of precocity, and others wherein it never occurs, that neutralize this assertion; besides, menstruation, being deferred or protracted, depends frequently upon peculiarities of health. As soon, however, as it occurs, a sensible change takes place in the female economy; and certainly the other developments of womanhood rapidly follow.
There’s one function that’s too important to overlook here, and that’s menstruation—a term for the monthly discharge that comes from the womb. When this function begins, a woman is considered to have reached puberty; however, there are cases of early onset and others where it never happens, which challenges this idea. Additionally, menstruation can be delayed or extended due to specific health issues. However, once it starts, a noticeable change occurs in the female body, and the other developments of womanhood quickly follow.
Menstruation is the monthly discharge of a red fluid, common to females from fifteen or sixteen years of age to between forty and fifty; and it is held that, while a female[140] menstruates, she is apt, and capable also, to conceive. Menstruation is a device of nature to relieve the system, or to preserve the balance of the circulation, from the non-fulfilment of her intentions, by the absence of procreation. It usually continues for four, five, or six days, and seldom exceeds a few ounces. Its suppression is usually attended with marked ill health, and many of the formidable complaints of females are attributable to its irregularities. When anticipated, the female encounters feelings of depression and lassitude, and exhibits an aspect of feeble health. As a physiological fact, women, before and after menstruation, are more desirous of the exercise of sexual privileges, and usually the approach of the menstrual flow is accompanied by a sexual orgasm. It has ever been deemed, by almost universal consent, prudent for married persons and others to abstain from the sexual embrace during that period. If only on the score of cleanliness, it should be observed; besides, the likelihood of establishing irritability, and the probability of interfering with this healthful provision of nature, should deter from the indulgence. In some countries, menstruating women are excluded from associating with the other sex altogether, and are even forbid mingling with household duties. At the close of this article will be found a series of prescriptions and suggestions for the removal of the various disturbances this function is liable to.
Menstruation is the monthly release of a red fluid, common to women from about fifteen or sixteen years old until they are between forty and fifty. It is believed that while a woman is menstruating, she is able to conceive. Menstruation is a natural process that helps the body maintain balance or relieve itself due to the absence of procreation. It usually lasts four to six days and typically involves only a few ounces of fluid. If it doesn't occur, it can lead to significant health problems, and many serious issues that women experience are linked to menstrual irregularities. Before and after menstruation, women often feel depressed and fatigued, showing signs of poor health. Physiologically, women tend to desire sexual activity more before and after their periods, and the approach of menstruation is often accompanied by a sexual response. It's generally considered wise for married couples and others to refrain from sexual activity during menstruation. For one, it's a matter of hygiene, and also, it may lead to irritability and disrupt this natural process. In some cultures, menstruating women are completely kept away from men and prohibited from participating in household duties. At the end of this article, you'll find a list of remedies and suggestions for addressing the various issues that may arise during this process.
The act of connexion is urged by what is called the sexual propensity. It is accompanied by feelings of the intensest kind: the acme of enjoyment is at the moment of seminal ejaculation. The penis is excited to erection by the influx or rush of blood into its cavernous or cellular structure; the scrotum becomes constricted, and compresses the testicles; the vesiculæ seminales, and the prostate gland, are also elevated by the muscles called levatores ani, as shown in the preliminary anatomical drawings, whence their use may now be better understood, as well as those of the perineal muscles, which all more or less assist in causing the prompt and forcible ejaculation of the spermatic fluid.
The act of connection is driven by what we call sexual desire. It comes with intense feelings; the peak of pleasure occurs at the moment of ejaculation. The penis becomes erect due to the rush of blood into its cavernous or sponge-like structure; the scrotum tightens and compresses the testicles; the seminal vesicles and the prostate gland are also lifted by the muscles known as levatores ani, as illustrated in the preliminary anatomical drawings, which help clarify their function, along with the perineal muscles, all of which play a role in enabling rapid and powerful ejaculation of sperm.
“In[7] the female, the sense of enjoyment, sub coitu, appears to be principally excited by the friction of the labia interna and clitoris, which are alike in a state of turgescence or erection. This nervous excitement, as in the[141] male, often reaches such a degree of intensity that a kind of syncoptic state is induced.” A sense of contented lassitude follows, and the mind is permitted to return from the regions of excited imagination to its ordinary quietude.
“In[7] women, the feeling of pleasure during sex mainly comes from the rubbing of the inner labia and clitoris, which are swollen and sensitive. This nervous excitement, like in men, can become so intense that it leads to a sort of brief loss of awareness. Afterwards, a feeling of relaxed satisfaction follows, allowing the mind to return from the heightened state of imagination to its usual calm.”
The due occurrence of the phenomena just detailed does not necessarily secure, although it generally succeeds in producing, a prolific result. Health, aptitude, and one important condition, are indispensable; and the last is—a positive contact between the male sperm and female ovum.
The timely happening of the phenomena just mentioned does not guarantee, although it usually leads to, a fruitful outcome. Health, ability, and one crucial requirement are essential; and that requirement is a direct contact between the male sperm and female ovum.
There are many remarkable eccentricities that embitter married life. A union may exist between two parties who are wholly inapt for mutual enjoyment. The sensations belonging to the sexual act are involuntary, and are provoked independently of the will: hence, in connexion without consent, or under feelings of great repugnance, the orgasm is sometimes aroused; and yet, where the greatest affection and desire prevail, the male oftentimes unseasonably concluding before the female, is a most tantalizing source of disappointment. Further allusions will be found to this subject under the heads of “Sterility,” and “Impuissance.”
There are many striking quirks that can make married life challenging. A couple may find themselves together despite being completely unsuitable for genuine happiness. The physical sensations associated with sex happen involuntarily and can be triggered without one's conscious desire: therefore, in situations lacking consent or filled with strong dislike, orgasm can still occur; yet, even when there is deep affection and desire, it is often frustrating for the male to finish too soon, leaving the female disappointed. More discussions on this topic can be found under the sections “Sterility” and “Impuissance.”
As a preliminary aid to the description of the process of
impregnation, which ensues, the following anatomical draft
is presented:—
As an initial help in describing the process of impregnation that follows, the anatomical outline below is provided:—

|
|
|
1. Section of the womb, upper part. 1. Section of the uterus, upper part. 2. Do. of side. 2. Do. of side. 3. Do. of lateral covering. 3. Perform lateral coverage. 4. Do. of lower part of womb. 4. Do. of lower part of the uterus. 5. Cavity of the womb. Uterine cavity. 6. A prominence leading from the openings of the fallopian tubes. 6. A bump extending from the openings of the fallopian tubes. 7. The vagina. The vulva. 8 and 9. Fallopian tube cut open. 8 and 9. Fallopian tube opened. |
10 and 16. The fimbriated extremity of do. 10 and 16. The fringed end of do. 11. The pavilion. The pavilion. 12. The ovary. The ovary. 13. Vesicles in do. 13. Vesicles in action. 14. Continuation of ovary. 14. Ovary continuation. 15. Ligament of do. 15. Ligament of action. 17. Pavilion of right ovary. 17. Right ovary pavilion. 18. Right ovary. Right ovary. 19. Connecting band. 19. Connection band. |
Man, unlike other animals, is not smitten with desire to propagate only at particular periods. In sentient beings, every season is favorable to the flame of love.
Man, unlike other animals, doesn't only feel the urge to reproduce at specific times. For sentient beings, every season is a good time for love.
When conception takes place, the following phenomena are believed to occur: The womb is supposed to participate in the excitement of the sexual act, and at the moment of the orgasm, to receive the male seed, and to mingle with it a fluid of its own. The whole apparatus of the uterus appears influenced at the same time,[8] by a kind of electric irritability. A vesicle, owing to the ovaria being grasped or embraced by the fimbriæ, escapes from its lodgment and enters the fallopian tube, where it bursts, and its albuminous drop is conveyed into the womb.
When conception happens, the following things are thought to occur: The womb is believed to get involved in the excitement of the sexual act, and at the moment of orgasm, it receives the male sperm and mixes it with a fluid of its own. The entire structure of the uterus seems to be affected at the same time,[8] by a sort of electric sensitivity. A vesicle, due to the ovaries being held by the fimbriae, breaks free from its spot and enters the fallopian tube, where it ruptures, and its protein-rich drop is delivered into the womb.
From the circumstance of the male semen returning from the vagina after copulation, it has been doubted whether it was intended to enter the uterus. It certainly can only enter once,[9] and that when impregnation takes place; and even then a small portion suffices, for immediately after conception the mouth of the womb becomes impermeably closed. The mouth of the womb lies horizontally, like the lips of the face, while that of the orifice of the urethra is arranged perpendicularly: hence the presumption, from this better adaptation to transmit and receive, that the semen to impregnate should enter the uterus.
From the fact that male semen can come back out of the vagina after sex, people have questioned whether it was meant to enter the uterus. It can only enter once,[9] and only when conception happens; even then, just a small amount is enough, because right after conception, the opening of the womb seals shut. The mouth of the womb is positioned horizontally, like the lips of a face, while the opening of the urethra is vertical: this suggests that the structure is better suited to receive and transmit semen, indicating that for impregnation, semen should enter the uterus.
This question is mooted, because it has been supposed by some that impregnation ensues from the vapor or odor of the male seed ascending to the womb. Contending parties admit, while others deny, that the seed may be, and has been, detected in the womb of females and animals having been slain (or who may have died) during or soon after the act of copulation. Impregnation has followed very imperfect penetration, such as in cases of unruptured hymen, or of disproportion of parts, and other causes needless to insert here, by which the supposition is supported that conception takes place from vaginal absorption; but it must be remembered that the seed is projected generally[143] with great force, and that the smallest possible quantity is sufficient for impregnation; also, that the vagina possesses a constrictive movement of its own, whereby the seed is carried into the womb.
This question is raised because some believe that pregnancy happens when the vapor or scent of male semen rises to the womb. Some people agree with this, while others disagree, stating that the semen has been found in the wombs of females and animals that were killed (or died) during or shortly after sexual intercourse. Pregnancy can occur even with very minimal penetration, such as in cases where the hymen is still intact or where there is a size mismatch, among other reasons that don't need to be mentioned here. This supports the idea that conception can happen through vaginal absorption; however, it’s important to note that the semen is usually released with significant force, and even the smallest amount can lead to pregnancy. Additionally, the vagina has its own constrictive movement that helps carry the semen into the womb.
After the escape of the “albuminous drop,” the vascular membrane which contained it is converted into what is called a corpus luteum; denoting thereby—for it assumes the form, after a while, of a fleshy nucleus—that the female has either conceived, or has been under the influence of strong amatory excitement. This salvo must be admitted, for corpora lutea have been discovered in females where intercourse was even impossible; but as this detection of corpora lutea generally corroborates the surmise that so many conceptions have taken place as there are corpora lutea, it is to be presumed that the exception must be owing to some similarly powerful mental, as well as physical excitement.
After the escape of the “albuminous drop,” the vascular membrane that contained it changes into what’s known as a corpus luteum; this indicates—since it eventually takes on the appearance of a fleshy nucleus—that the woman has either conceived or experienced intense sexual excitement. This fact must be acknowledged, as corpora lutea have been found in women where intercourse wasn't even possible; however, since the presence of corpora lutea generally supports the idea that there have been as many conceptions as there are corpora lutea, it's reasonable to assume that the exceptions are due to some similarly strong mental and physical stimulation.
When impregnation has taken place, the womb begins to enlarge, and become more soft, vascular, and turgid—the wonderful process of fluids assuming the form of solids commences, and within a fortnight an investing membrane is formed, called the decidua (I will insert as few names as possible), consisting of two kinds of folds, one lining the womb, and the other containing the ovum which has therein “taken root.” The ovum is now a soft oval mass, fringed with vessels, and composed of membranes containing the early fœtus. See sketch.
When conception occurs, the uterus starts to expand and becomes softer, more vascular, and swollen. The incredible process where fluids turn into solids begins, and within two weeks, a protective membrane called the decidua forms (I'll keep the names to a minimum). This membrane has two types of layers: one that lines the uterus and the other that surrounds the ovum, which has now “taken root.” The ovum is now a soft, oval mass, surrounded by blood vessels, and made up of membranes that contain the early fetus. See sketch.

When opened, the fœtus appears surrounded by three distinct membranes: first, the decidua; secondly, the chorion, the inner fold of the former; thirdly, the amnios. The decidua, as before stated, lines the womb; the two others cover the ovum or fœtus. After a time the amnios and chorion become adherent to each other, and a fluid is interposed betwixt the amnios and fœtus, called the liquor amnii. The fœtus, as it advances, is perceived to be hanging by an organized support, called the umbilical chord, floating in the liquor before named.[10]
When opened, the fetus is surrounded by three distinct membranes: first, the decidua; second, the chorion, which is the inner layer of the former; and third, the amnios. The decidua, as mentioned earlier, lines the womb; the other two cover the ovum or fetus. Over time, the amnios and chorion stick to each other, and a fluid called liquor amnii forms between the amnios and the fetus. As the fetus develops, it is seen hanging by an organized support called the umbilical cord, floating in the aforementioned fluid.[10]
A draft is here presented of an ovum (a section) of a fortnight old; and adjoining is one just double its age, where the chord will be perceived.
A draft is presented here of an egg (a section) that is two weeks old; and next to it is one that is just twice its age, where the chord can be seen.


The following further account may aid the description thus far given. The ovum, protected by a membrane of its own, called the amnios, descends into the uterus, where it takes its hold of the membranes already there—the decidua. It pushes its way before, as exemplified in the subjoined drawing:—
The following additional account may help clarify the description provided so far. The egg, surrounded by its own protective membrane called the amnios, moves down into the uterus, where it attaches to the existing membranes—the decidua. It moves forward, as shown in the attached drawing:—

|
a—The decidua lining the womb. The decidua lining the womb. b—Do. protecting the ovum. b—Do. Protecting the egg. c—The upper part of the womb, where the ovum has become adherent. c—The top part of the uterus, where the egg has attached itself. d—The ovum. d—The egg. |
The next cut shows the advanced condition of the fœtus:—
The next cut shows the advanced condition of the fetus

|
a—The womb. The womb. b—The liquor amnii, with the fœtus. b—The amniotic fluid, along with the fetus. c—The chorion. The chorion. d—The decidua. d—The uterine lining. e—The opening of the fallopian tubes. e—The opening of the fallopian tubes. |
It will answer no practical usefulness to go through the whole minutiæ of the various physiological changes that take place relative to fœtal growth from the hour of impregnation to that of delivery. What has already been detailed, has been offered to unveil a little of that singular ignorance that exists generally among non-medical persons regarding the history of themselves. “Too much learning is a dangerous thing;” and it will readily be allowed, that a sufficient idea that certain things happen is oftentimes as useful as to know how they happen, especially when it belongs to a department requiring much research, time, and ingenuity, thoroughly to understand, and which may chance to be foreign to our ordinary pursuit.
It doesn't really help to go through all the detailed physiological changes that occur during fetal growth from conception to delivery. What I've shared so far aims to shed light on the common lack of knowledge that non-medical people have about their own bodies. “Too much knowledge can be dangerous,” and it’s often enough to just understand that certain things happen without needing to know how they happen, especially when it involves an area that requires a lot of research, time, and creativity to fully grasp, and might not relate to our everyday interests.
The period consumed in gestation is forty weeks, or nine calendar months, and the time is calculated from a fortnight after the suspension of menstruation. Some married ladies pride themselves upon being able to predict to a day—to tell the precise occasion when they conceive, and which they date from some unusual sensation experienced at the particular embrace which effected the important change. Many medical men disallow that such tokens present themselves, and are opposed to the belief which many mothers entertain, that nature is so communicative; and also are skeptical of those extraordinary influences that every day furnish proofs of maternal imagination, occasioning to the burden they carry, sundry marks, malformations, and monstrosities. Examinations have found that the order of fœtal organization is somewhat as follows: the heart and large vessels, the liver and appendages, the brain, stomach, and extremities. The determination of sex and number has hitherto defied exploration. In the early months of pregnancy the womb maintains its natural position; but as it enlarges, it also emerges from the pelvis into the abdomen. The moment of its slipping out of the pelvis is termed quickening, of which most women are sensible—some fainting on the occasion, others being attacked with nausea, hysteria, and palpitation of the heart. Quickening usually occurs between the fourth and fifth month. The fœtus is then called a child—the law ordaining that, if a woman intentionally procure, or such parties as may assist in so doing, abortion or miscarriage before quickening, it is misdemeanor, if after, murder.
The period of pregnancy lasts about forty weeks, or nine months, and it's calculated from two weeks after a woman's period stops. Some married women take pride in being able to predict the exact day they conceive, often linking it to a specific feeling they had during the encounter that caused the significant change. Many medical professionals disagree with the idea that such signs can be recognized and are skeptical of the belief held by some mothers that nature communicates in this way. They also doubt the extraordinary claims that seem to provide evidence of maternal imagination, leading to various marks, deformities, and oddities in the babies they carry. Studies show that fetal development generally follows this order: the heart and major blood vessels, the liver and its parts, the brain, stomach, and limbs. The determination of sex and number of fetuses remains elusive. In the early months of pregnancy, the uterus stays in its normal position, but as it grows, it rises out of the pelvis and into the abdomen. The moment it pops out of the pelvis is called quickening, which most women feel—some may even faint, while others experience nausea, hysteria, or a racing heart. Quickening usually happens between the fourth and fifth month. After this time, the fetus is referred to as a child, and the law states that if a woman intentionally causes an abortion or miscarriage before quickening, it's considered a misdemeanor; if it happens after, it's classified as murder.
The following diagram is presented to show the situation occupied by the womb containing the child just ready to enter the world:—
The following diagram is provided to illustrate the position of the womb holding the child who is about to enter the world:—

|
a—The womb. a—The uterus.
b—The vagina. b—The vulva.
c—The bladder. The bladder.
d—The rectum. d—The anus. |
A full pregnant female, like a very corpulent man, walks very erect: hence the popular notion that ladies in the one condition, and gentlemen in the other, do not think meanly of themselves, but strut along well pleased with their own importance. It is an uncharitable idea; the attitude is unavoidable, the head and shoulders being thrown back to counterbalance the protuberance in front—to preserve, in fact, the centre of gravity, to save themselves from falling.
A fully pregnant woman, like an extremely overweight man, walks very upright: hence the common belief that women in one condition and men in the other take pride in themselves and stride along, pleased with their own importance. It's an unfair assumption; the posture is unavoidable, as the head and shoulders lean back to balance the protrusion in front — to actually maintain their center of gravity and prevent themselves from falling.
Symptoms of Pregnancy.—Mysterious as is the process of impregnation, there are many forewarnings which, being generally found correct, are useful to be known. Great[147] as are the changes that take place in the female economy during child-bearing, and productive as they frequently are of serious disturbances to health, it is benevolently ordained that women who fulfil their destiny of becoming mothers, have better health to sustain them through their travail than the single or unprolific. The signs of pregnancy during the first few weeks are very equivocal. The first probability is the suppression of menstruation, which is accompanied by fulness of the breasts, the nipples of which become surrounded by a dark areola; headache, flushing in the face, and heat in the palms of the hands, ensue; also sickness in the morning, and probably an accession of mental irritability; various longings exist—many very ridiculous, others bordering on insanity, and some indicating great perversion of temper, habits, in hitherto well-conducted inclinations.
Symptoms of Pregnancy.—As mysterious as the process of conception is, there are many signs that are generally accurate and useful to know. Despite the significant changes that happen in a woman’s body during pregnancy, which can often lead to serious health issues, it is thankfully arranged that women who fulfill their role as mothers tend to have better health to support them through childbirth than those who are single or childless. The signs of pregnancy in the first few weeks are often ambiguous. The most likely indicator is the absence of menstruation, which may be accompanied by fullness in the breasts, with the nipples becoming surrounded by a dark areola. Headaches, facial flushing, and warmth in the palms of the hands may follow; there can also be morning sickness and possibly an increase in irritability. Various cravings may arise—some quite silly, others bordering on madness, and some showing a significant change in temper and habits from previously well-behaved inclinations.
There are many phenomena more readily discovered by medical men accustomed to the accoucheur’s employment than describable, that indicate pregnancy; the sinking of the abdomen, the descent and closure of the uterus, the altered facial looks, the state of the pulse, &c., &c.
There are many signs of pregnancy that medical professionals who work with childbirth can identify more easily than describe, such as the dropping of the abdomen, the position and closure of the uterus, changes in facial appearance, the condition of the pulse, etc.
From the fourth month, when the womb ascends into the abdomen, the signs are more positive: the protrusion of the navel, the evident enlargement of the belly, the tenderness and fulness of, and occasional escape of milk from, the breasts, clearly point out the occasion.
From the fourth month, when the uterus rises into the abdomen, the signs become clearer: the navel sticks out, the belly noticeably expands, the breasts feel tender and full, and there may even be some milk leakage, all clearly indicating what's happening.
About the fifth month, the movements of the child are very apparent to the mother, when all doubt is removed.
About the fifth month, the baby's movements become very noticeable to the mother, so there’s no doubt left.
There are some conditions of female life that assimilate to pregnancy, and which have defied the judgment of matrons, and even medical men, but they are rare—such as dropsy of the abdomen, or ovaries, tumors, accumulations of wind, &c. These, with the suspension of menstruation (which last is but an uncertain sign, for it may depend upon cold, fever, or inflammation), have destroyed the anticipations of fond wives, and have alarmed those who desire not to become mothers.
There are certain conditions in women's lives that are similar to pregnancy and have puzzled both experienced women and doctors, but they are uncommon—like abdominal or ovarian swelling, tumors, gas buildup, etc. These, along with missed periods (which is an unreliable sign because it can be caused by cold, fever, or inflammation), have shattered the hopes of eager wives and frightened those who do not wish to become mothers.
Parturition takes place at the end of the ninth month; but children born at the end of seven will live, and examples are related of some that have “gone” ten. In France, legitimacy is allowed to children born on the 299th day of pregnancy.
Childbirth happens at the end of the ninth month; however, babies born at the end of the seventh month can survive, and there are cases of some who have been born at ten months. In France, children born on the 299th day of pregnancy are considered legitimate.
Labor is distinguished by a softening of the soft parts of the female organs of generation, an abundant secretion[148] of mucus, a relaxation of the mouth of the womb, and a forcible contraction of its body. The expulsion of the child is effected by pains of a straining nature. After the birth of the child, the womb contracts to its normal or unimpregnated size, giving forth a discharge, called the lochia, that lasts for several days, and the breasts immediately furnish the secretion of milk.
Labor is marked by the softening of the soft tissues of the female reproductive organs, a heavy discharge[148] of mucus, a loosening of the cervix, and strong contractions of the uterine body. The delivery of the baby occurs through intense straining pains. After the baby is born, the uterus contracts to its normal or non-pregnant size, releasing a discharge known as lochia, which lasts for several days, and the breasts begin producing milk immediately.
Previously to entering upon the consideration of the diseases arising from infection, and for which this book was originally composed, a word or two may be said upon a condition of the womb, unfortunately of frequent prevalence, called prolapsus uteri, or falling of the womb. Such occurrence may take place with single females as well as with married, or those who have borne children. It may be held as the result of debility; and according to the degree of descent is the inconvenience and suffering. The first drawing exhibits the natural position of the uterus:—
Before we dive into the discussion of infectious diseases, which is what this book was originally written for, it's worth mentioning a common condition of the uterus known as prolapsus uteri or falling of the womb. This can affect both single women and those who are married or have had children. It is generally seen as a result of weakness, and the level of discomfort and suffering corresponds to how far the uterus has descended. The first illustration shows the natural position of the uterus:—

|
a—The vagina. a—The vagina.
b—The uterus. The uterus. |
A partial descent of the uterus gives rise to painful dragging sensations about the groins and fundament, and it is usually attended by the “whites,” or leucorrhœa, a disease of which mention is presently made:—
A partial drop of the uterus leads to painful pulling sensations in the groin and lower back, and it is usually accompanied by a discharge known as “the whites” or leucorrhea, a condition that will be discussed shortly:—

|
Partial descent of the uterus. Uterine prolapse.
a, a, a—Vagina. a, a, a—Vulva.
b—Uterus. b—Uterus. |
If prolapsus takes place during pregnancy, the womb impresses upon the bladder and rectum, and occasions irritability of both those structures; but as pregnancy advances, and as the womb ascends into the abdomen, these inconveniences cease, and the womb oftentimes regains its tone and position after child-birth. The womb sometimes protrudes externally, and is a source of great distress. See drawing:—
If prolapsus happens during pregnancy, the uterus puts pressure on the bladder and rectum, causing irritation in both. However, as pregnancy progresses and the uterus moves up into the abdomen, these issues go away, and the uterus often regains its strength and position after childbirth. Sometimes, the uterus protrudes outward, leading to significant discomfort. See drawing:—

|
Prolapsus uteri. Uterine prolapse.
a, a—Vagina. a, a—Vagina.
b—Uterus. b—Womb. |
The treatment in these cases is chiefly mechanical, beside supporting the general health. The first symptoms, however, demand efficient attention, and the medical attendant should be made acquainted with every particular.
The treatment in these cases is mainly mechanical, along with supporting overall health. However, the first symptoms require prompt attention, and the medical provider should be informed of every detail.
It is a question whether the weakened condition of the supports of the womb, and the consequent relaxed state of the vagina, are not owing to the manner in which women clothe themselves. The pelvic part of the female is kept always in a state of unnatural warmth, from the load of petticoats and other unnameable female attire. Contrast but the difference between the simple unlined trowsers of the male and five or six-fold clothing of the other sex: either the one must yield too much warmth, or the other must strike too cold. The sedentary habits of women have of course much influence.
It’s a question of whether the weakened state of the womb’s supports and the resulting relaxed condition of the vagina are due to how women dress. The pelvic area of women is constantly kept in an unnatural state of warmth because of the heavy petticoats and other types of female clothing. Just compare the simple, unlined trousers worn by men to the multiple layers of clothing of women: one must be too warm, or the other must be too cold. Women’s sedentary lifestyles also play a significant role.
When retention of urine follows the falling down or partial descent of the womb, the female should lie on her back, press the uterus into the pelvis, and urinate in that position.
When urine retention happens after the womb has fallen or partially descended, the woman should lie on her back, push the uterus down into the pelvis, and urinate while in that position.
The womb, beside becoming displaced, is subject to an eversion, or a turning inside out. Happily, such cases are unfrequent, but any disturbance of so important an organ demands the promptest attention.
The womb, along with becoming displaced, can undergo an eversion, or a turning inside out. Fortunately, these cases are rare, but any issue with such an important organ requires immediate attention.

The introduction of the stethoscope and the speculum constitute two important epochs in medical science—the former ascertaining, by the conveyance of sound, disease in the most hidden and inaccessible parts of the human frame, and the latter bringing to view structures which, without such aid, are necessarily veiled from our sight. The speculum consists of an instrument formed of silver or steel, that without pain or inconvenience is passed into the vagina, when, by a simple contrivance, it is made to expand[151] and dilate the vaginal passage, and thereby expose to view the entire canal, together with the uterine aperture. The usefulness of such a method, whereby disease can at once be detected, admits of no dispute. It is physically painless; and if opposed to female diffidence and modesty, its importance and serviceableness should be balanced against the mental distress such a procedure may occasion. On the one hand, without its assistance, the treatment of the disease is at best but conjectural; on the other, by its aid, it is safe and sure—much suspense and suffering is at once put an end to. Experience has proved that many local disturbances, that were believed to have been merely vaginal irritation, have been discovered to depend upon absolute disorganization of the neck and mouth of the womb. Deep-seated ulceration has been detected, and cancerous enlargements; the disease thereby having been exposed, has had the necessary and successful treatment. In Paris, it is considered so valuable that a chair, termed a “speculum chair,” has been invented solely for its use. See engraving on previous page.
The introduction of the stethoscope and the speculum marks two significant milestones in medical science—the former allows us to detect disease in the most hidden and hard-to-reach areas of the human body through sound, while the latter reveals structures that, without it, would remain concealed from our view. The speculum is an instrument made of silver or steel that can be inserted into the vagina without causing pain or discomfort; it has a simple mechanism that enables it to expand and widen the vaginal passage, thereby exposing the entire canal along with the uterine opening.[151] Its usefulness in detecting disease is undeniable. It is physically painless; however, if it conflicts with a woman's modesty and shyness, the importance and usefulness should be weighed against the mental discomfort it may cause. On one hand, without this tool, treatments for disease are often just educated guesses; on the other hand, with its help, treatment becomes safe and reliable—eliminating much uncertainty and suffering. Experience has shown that many local issues once thought to be just vaginal irritation have actually turned out to be related to severe damage to the cervix and uterus. Deep ulcers and cancerous growths have been identified, allowing for necessary and effective treatment. In Paris, it is so valued that a special chair, known as a "speculum chair," has been created just for its use. See engraving on previous page.
The speculum is now in the hands of every respectable medical man, and the class of disorders that hold it in requisition are being better understood, and consequently more successfully combated. In no cases is it more useful than in secretive irregularities, such as in leucorrhœa, gonorrhœa, or syphilitic ulceration. Without further comment, these diseases will be considered.
The speculum is now in the hands of every reputable doctor, and the types of conditions that require it are being better understood and, as a result, treated more effectively. It's especially helpful for discreet issues like leucorrhea, gonorrhea, or syphilitic ulcers. Without further discussion, these diseases will be examined.
GONORRHŒA IN THE FEMALE.
This disease is rarely so violent as in man, it being mostly confined to the uterine conduit; in fact, except by the discharge, women are almost unconscious of its existence, mistaking it, when occurring in married life, for leucorrhœa. Occasionally, however, the inflammation is highly acute, and a variety of distressing symptoms ensue. There is considerable excoriation around, and a swelling of the organs, much ardor urinæ, and the same constitutional disturbance as in the other sex.
This disease is rarely as severe in women as it is in men; it mostly affects the uterine canal. In fact, apart from the discharge, women are often unaware of its presence, confusing it with leucorrhea when it happens in married life. However, sometimes the inflammation can be very intense, leading to a range of troubling symptoms. There can be significant irritation around the area, swelling of the organs, a lot of burning sensation during urination, and the same overall health issues as seen in men.
The medical treatment of both sexes is constitutionally alike; but the female has to depend more upon local treatment than the male. Hence the importance of injections. Now here is another source of difficulty: women are as[152] averse to the use of the syringe as they are to the speculum; and the consequence is, vaginal diseases are generally protracted to double as long as they need be. However, as these hints are likely to be seen only by those who doubtlessly have, and who indisputably ought, to exercise it, namely, influence over the sex in persuading them to submit to what common sense bespeaks as most prudent and expedient, appropriate formulæ for the suggestions just recommended will be found a few pages hence. Frequent ablution, rest, temperate diet—the more farinaceous and mucilaginous the better, avoiding entirely wines, fermented and spirituous liquors, together with mild (Form 63) aperients and salines, constitute the chief means of cure. Injections are indispensable.
The medical treatment for both genders is fundamentally the same; however, women tend to rely more on localized treatments than men do. This highlights the importance of injections. Here's another challenge: women are just as reluctant to use a syringe as they are to use a speculum; as a result, vaginal diseases often linger for twice as long as necessary. Nevertheless, since these suggestions are likely to be seen only by those who certainly have, and should definitely exercise, influence over women in encouraging them to follow what common sense suggests is the most sensible and practical approach, suitable recommendations for these suggestions will be found a few pages ahead. Regular washing, rest, and a moderate diet—the more starchy and soothing, the better—should completely avoid wines, fermented and distilled drinks, along with gentle (Form 63) laxatives and saline solutions, are the main methods of treatment. Injections are essential.
I have already alluded to the difficulty of getting female patients to be their own confessors. If they appoint others, every possible information should be furnished, and fastidiousness by no means should supplant the avowal of real facts. Although gonorrhœa in women is generally less severe than in the male, it is vexingly oftentimes more lasting; which is easily accounted for, owing to the extent of surface diseased: whereas in man it is limited to the narrow urethra, and seldom exceeds an inch or two upward, constituting not one tithe part of the space morbidly affected in the former. See, however, the formulæ.
I have already mentioned how challenging it is to get female patients to be their own confessors. If they choose to have someone else do it, all relevant information should be provided, and being overly particular should never replace stating the actual facts. While gonorrhea in women is generally less severe than in men, it often lasts longer, which is easy to understand because of the larger surface area affected. In men, the infection is limited to the narrow urethra and typically extends only an inch or two upward, making it just a fraction of the area negatively impacted in women. See, however, the formulas.
SYPHILIS IN FEMALES.
The principal features of syphilis in women consist of ulcers, excoriations, warts, and buboes. Women, of course, are alike liable to all the forms of secondary symptoms. Chancres usually appear within and on the labiæ. In the [153]drawing here given, the labiæ are drawn aside to expose the ulceration; and they are also found within the vagina and surrounding the mouth or protuberance of the womb. It is in these cases that the speculum is had recourse to; and in the Parisian hospitals every case is subject to such a mode of investigation.
The main signs of syphilis in women include ulcers, scratches, warts, and swollen lymph nodes. Women can experience all the different types of secondary symptoms. Chancres typically show up inside and on the labia. In the [153]illustration provided, the labia are pulled back to show the ulceration; they can also occur inside the vagina and around the mouth or protrusion of the uterus. In these situations, the speculum is used; and in the Parisian hospitals, every case is examined with this method.

The following three illustrations show what a degree of severity ulceration and other changes put on. The first exhibits superficial excoriation extending rapidly, and occasionally a swollen appearance of the os uteri; the second shows extensive chancrous ulceration; and the last of a tuberculous character, like little hardened tumors. But for the speculum, these conditions might have gone on to worse, and led to irremediable mischief: their treatment, independently of local means, such as injections, &c., would have been prolonged to an almost indefinite time. The use of styptics is demanded in female as well as male syphilitic developments, and accordingly the employment of nitrate of silver, copper, &c., is advised, as already explained.
The following three illustrations show the severity of ulceration and other changes. The first depicts superficial excoriation that spreads quickly, sometimes causing swelling of the os uteri; the second shows widespread chancrous ulceration; and the last has a tuberculous appearance, resembling small hardened tumors. Without the speculum, these conditions could have worsened and resulted in irreversible damage: their treatment, aside from local methods like injections, would have taken an almost indefinite amount of time. The use of styptics is necessary for both female and male syphilitic conditions, and as previously explained, the application of nitrate of silver, copper, etc., is recommended.



The following drawing shows the extent of mischief and annoyance to the external organs of female generation consequent upon neglect. The external labiæ are studded with chancres. The thighs, buttocks, and rectum, are dotted and overspread with excoriations. The person[154] from whom this sketch is taken was an unfortunate woman of the town. As it is not my intention to particularize cases, although from my peculiar province I could fill up as many pages as this book contains, with details of such histories, I have only to add, by way of summary, that the topical and constitutional treatment being alike in both sexes, the only modifications required will be the regulating of the doses of the medicines, which must be done with reference to the idiosyncrasy, age, and temperament, of the patient. The frail system of woman is less able to withstand the dire effects of the disease, or the potent means for its extirpation, than her stronger brotherhood, and therefore the abler and more experienced the counsel, the fairer the chance of her recovery; a hint that the writer feels assured will not be received by those to whom his pages are addressed, as a vain appeal to repose confidence in other advice than their own.
The following drawing illustrates the damage and irritation to the external female organs caused by neglect. The outer labia are covered in chancres. The thighs, buttocks, and rectum are marked and covered with sores. The individual[154] from whom this sketch is based was an unfortunate woman from the streets. While I don’t intend to detail specific cases, I could easily fill many pages with such stories from my area of expertise. I will just summarize that the local and overall treatments are similar for both genders; the only changes necessary will involve adjusting the medication doses based on the patient's unique characteristics like their idiosyncrasy, age, and temperament. Women's bodies are generally less capable of handling the severe effects of the disease or the strong treatments used to eliminate it compared to their male counterparts. Therefore, the more skilled and experienced the advice, the better the chance of recovery. I believe this is a point that those reading my work may not take to heart, as they might prefer to trust their own judgment over any other guidance.

LEUCORRHŒA, FLUOR ALBUS, OR THE WHITES
This is the most prevalent of all derangements of the female economy, connected with the uterine system; and from its debilitating effects, induces a train of maladies that tend to embitter personal comfort more than any other human ill. Leucorrhœa consists of a discharge of acrid, or bland, but variously-colored mucus from the vagina, differing in intensity according to the cause and duration. It would be idle to offer the many arguments set up to prove whence it proceeds, or to examine the discussions as to whether it is the produce of the uterine vessels, or the vaginal secretives. That both aid in its formation is doubtless the case (as the employment of the speculum has[155] satisfactorily proved); and equally certain that, according to the amount of irritability existing therein, so depends the quantity and character of the discharge. It exists in the married and single—in the moral and unchaste; and therefore the cause should be cautiously divined, it being evident that other than sexual indulgences establish this annoying and distressing affliction. It may be fairly conceded to be a vitiated secretion, depending upon a weakened state of the local vessels, and, moreover, in particular habits, to be a salutary evacuation. On the other hand, it must not be denied that it is oftentimes, where it occurs to persons living sub judice mariti, the result of sexual intemperance, or disease springing from an indiscriminate indulgence in the same.
This is the most common issue affecting women's reproductive health, linked to the uterine system; and due to its weakening effects, it leads to a range of problems that tend to worsen personal comfort more than any other health issue. Leucorrhea is characterized by a discharge of irritating or mild, but differently colored mucus from the vagina, which varies in intensity based on the cause and duration. It would be pointless to present the numerous arguments regarding its origins or to debate whether it comes from the uterine vessels or the vaginal secretions. It's clear that both contribute to its formation (as the use of the speculum has[155] shown); and it is equally certain that the level of irritation present determines the amount and nature of the discharge. It can occur in both married and single women—in those who are virtuous and those who are not; thus, the cause should be approached with caution, since it is obvious that factors other than sexual activity can lead to this bothersome and distressing condition. It can be reasonably accepted as an abnormal secretion resulting from a weakened state of the local vessels and, in certain habits, can serve as a beneficial discharge. However, it must also be acknowledged that it is often the result, for those living sub judice mariti, of sexual excess or diseases stemming from indiscriminate indulgence in the same.
However, as my purpose is more with the symptoms and treatment, the following may be received as a summary of what occurs, and what should be done for the removal thereof:—
However, since my focus is more on the symptoms and treatment, the following can be taken as a summary of what happens and what should be done to remove them:—
In addition to the discharge, which at one time is scanty, at another profuse, there are usually severe pains in the loins and lower part of the abdomen: there is a sense of bearing down, as though the womb were descending and even protruding. The general health of the patient is disturbed, loss of appetite, excessive languor, a pale and emaciated look, sleepless nights, dark areola around the eyes, various hysterical and other nervous affections, and numerous disturbances indicating a weakened and impaired state of mind and body. Among other causes beside those alluded to, may be enumerated irregular living, late hours, mental and bodily fatigue, deficient exercise, impure air, and neglect of personal ablution. Among the consequences of a long-continued leucorrhœa, an almost certainty of sterility should not be omitted.
In addition to the discharge, which can be sparse at times and heavy at others, there are usually intense pains in the lower back and abdomen: it feels like there's pressure, as if the uterus is dropping or even sticking out. The overall health of the patient suffers, with a loss of appetite, extreme fatigue, a pale and thin appearance, sleepless nights, dark circles under the eyes, various hysterical and other nervous issues, and numerous signs indicating a weakened and troubled state of mind and body. Besides the mentioned causes, other factors can include an irregular lifestyle, staying up late, mental and physical exhaustion, lack of exercise, poor air quality, and neglecting personal hygiene. One consequence of prolonged leucorrhea is a high likelihood of infertility, which should not be overlooked.
Treatment.—In leucorrhœa, where or where not consecutive to gonorrhœa, depending on loss of tone of the secretive vessels of the internal organs of generation, the chief indication is to impart vigor and restore strength, which it is evident depends much upon an avoidance of those causes that first started the disease.
Treatment.—In leucorrhea, whether or not it follows gonorrhea, due to a loss of tone in the secretive vessels of the reproductive organs, the main goal is to boost vitality and restore strength, which clearly depends significantly on avoiding the factors that initially triggered the condition.
Although leucorrhœa bears a strong resemblance to gonorrhœa, there are points by which to distinguish the one from the other. In gonorrhœa, the discharge is unceasing, but small in quantity, and is usually accompanied by inflammatory symptoms; whereas in leucorrhœa, the[156] discharge is irregular and copious, often coming away in large lumps.
The treatment of fluor albus is indicated by the degree of severity present. Where the prominent feature is the discharge, the indication is to increase the action of the absorbents by restoring the tone of the diseased surface, and at the same time to strengthen the system. Where the disease is complicated with weakness and relaxation, astringents should be given by the mouth, and also administered in the form of injections. The alkaline solution of copaiba is a very valuable medicament, and may be taken twice or thrice daily. It may also be employed as an injection, by adding one or two ounces to a pint of water, and a teacupful thrown up several times in the day. There are many domestic remedies, which, from their harmless properties, can at least do no injury, if they are not productive of good; as, for instance, a strong decoction of green tea, an infusion of oak bark, or alum-water; or diluted port wine—all to be used as injections, which, if it shall so please the patient, may be tried prior to the annexed:—
The treatment for fluor albus depends on how severe it is. If the main issue is discharge, the goal is to boost the action of absorbents by restoring the tone of the affected area, while also strengthening the overall system. If the disease comes with weakness and relaxation, astringents should be taken orally and also given as injections. An alkaline solution of copaiba is a very useful medication, which can be taken two to three times a day. It can also be used as an injection by mixing one or two ounces with a pint of water, and a teacupful should be administered several times a day. There are many home remedies that, because they are harmless, can at least do no harm, even if they don’t do much good; for example, a strong brew of green tea, an infusion of oak bark, or alum-water; or diluted port wine—all of these can be used as injections, which, if the patient prefers, may be tried before the annexed:—
| Chalybeate Pills, for Leucorrhœa, or other Female Sexual Weakness. | |||
| Take of— | |||
| Sulphate of iron | 1 | scruple. | |
| Balsam of copaiba and liquorice powder—of each a sufficiency to form the mass, which is to be divided into 40 pills, of which 3 or 4 may be taken three times a day. | |||
| Or, take of— | |||
| Sulphate of zinc | 1 | scruple. | |
| Extract of camomile | 1 | drachm. | |
| ”gentian | 1 | ” | |
| Syrup, a sufficiency. | |||
| Mix, and form 24 pills. Dose—two twice a day. | |||
| Strengthening Mixture. | |||
| Take of— | |||
| Infusion of bark | 7½ | ounces. | |
| Sulphate of quinine | 8 | grains. | |
| Diluted sulphuric acid | ½ | drachm. | |
| Syrup of orange-peel | 2 | drachms. | |
| Mix. Dose—three tablespoonfuls twice or three times a day. | |||
| Astringent Pills for Leucorrhœa. | |||
| Take of— | |||
| Extract of Peruvian bark | 1 | drachm. | |
| Gum kino | 1 | ” | |
| Alum | ½ | ” | |
| Nutmeg | 1 | scruple. | |
| Syrup, sufficient to form the mass. Divide into 36 pills. | |||
| Dose—three pills three times a day, to be followed by a teacupful of lime-water. | |||
| Astringent Pills. | |||
| Take of— | |||
| Alum | 30 | grains. | |
| Catechu | 1 | drachm. | |
| Opium | 5 | grains. | |
| Mix to form 30 pills. Dose—three twice a day. Useful in chronic gonorrhœa and leucorrhœa. | |||
| Astringent Pills for obstinate Gleet, or Leucorrhœa. | |||
| Take of— | |||
| Gum kino | 1 | part. | |
| Canadian turpentine | 4 | parts. | |
| Powder of tormentilla, as much as may be necessary to form a mass. Divide the same into pills of 5 grains each, and take from three to half a dozen of them night and morning. Continue them for a week or fortnight. A very useful remedy. | |||
| Astringent Injections for Leucorrhœa or Gonorrhœa. | |||
| Take of— | |||
| The compound solution of alum | ½ | oz. to 1 oz. | |
| Water | 1 | quart. | |
| Mix. | |||
| Injections may be used two or three times a day. If found to irritate, they should be diluted with water. Appropriate syringes are to be had; but the best are those formed by the Enema apparatus. | |||
| Astringent Injection. | |||
| Take of— | |||
| Sugar of lead | 1 | scruple. | |
| Water | 1 | quart. | |
| Mix. | |||
| Or, take of— | |||
| Catechu | 1 | drachm. | |
| Myrrh | 1 | ” | |
| Lime-water | ½ | pint. | |
| Mix. | |||
| Or, take of— | |||
| Nitrate of silver | 1 | scr. to 1 dr. | |
| Water | 1 | quart. | |
| Mix and strain. This lotion is much, and very effectively, used by the profession. | |||
| Or, take of— | |||
| Sulphate of zinc | ½ | to 1 drachm. | |
| Water | 1 | quart. | |
| Mix. | |||
| See Forms 11 and 12. | |||
The remaining diseases peculiar to the female pelvic viscera and their outlet, are hæmorrhoids, irritability and inflammation of the bladder, disordered uterine functions, urethritis, or inflammation of the urinary passage, and, lastly, internal and external irritation or excoriation. But as these fall within the province of every family practitioner, to the consultation of whom no morbid delicacy should prevent a patient, having such in their confidence, from resorting, I shall conclude this section by appending sundry prescriptions, in order that, should prudence not direct the sick one or her friends to call in the advised assistance, help may not be entirely withheld, and in order that, if the aid offered be not the means of supplying the loss of a more proficient and skilful director, it may at least be found mitigatory of these interruptions of health and comfort:—
The remaining conditions specific to the female pelvic organs and their exits include hemorrhoids, bladder irritation and inflammation, irregular uterine functions, urethritis, which is inflammation of the urinary tract, and finally, both internal and external irritation or chafing. Since these issues fall within the scope of every family doctor, whose help patients should feel comfortable seeking without any embarrassment, I will finish this section by providing several prescriptions. This way, if common sense doesn't guide the sick person or her friends to seek the recommended help, assistance won't be completely unavailable. Additionally, if the help provided isn't as effective as that from a more skilled professional, it may still relieve some of these health issues and discomfort:—
| Pills to promote the flow of the Menstrual Secretion. | |||
| Take of— | |||
| Aloetic pills, with myrrh | 1 | drachm. | |
| Compound iron pill | 1 | ” | |
| Mix to form 24 pills. Take two twice a day. | |||
| Or, take of— | |||
| Compound galbanum pills | 1 | drachm. | |
| Socotrine aloes | 1 | ” | |
| Mix to form 24 pills. Dose—two twice a day. | |||
| Injection for the retention of the Uterine Periodical Secretion. | |||
| Take of— | |||
| Liquor of ammonia | 10 | drops. | |
| Milk | ½ | pint. | |
| To be used morning and evening. This is a remedy that has been used by many medical men with very great success. | |||
| There are no means so importantly serviceable as the frequent use of the warm and vapor bath. |
| Stimulating Drops to restore the Menstrual flow. | |||
| Take of— | |||
| Compound tincture of aloes | 1½ | oz. | |
| Tincture of black hellebore | 1 | drachm. | |
| ”castor | 1 | ” | |
| ”Lyttæ | 30 | drops. | |
| Mix. Dose—a teaspoonful in water three times a day. | |||
| To relieve entire suppression. | |||
| Take of— | |||
| Compound galbanum pills | 1 | drachm. | |
| Sulphate of iron | 1 | ” | |
| Extract of savin | 10 | grains. | |
| Of black hellebore | 20 | ” | |
| Syrup sufficient to form 36 pills. Dose—three twice a day. | |||
| All these medicines must be given with great caution. |
| To check an immoderate flow of the Menstrual secretion. | |||
| Take of— | |||
| Infusion of roses | 8 | oz. | |
| Tincture of opium | 30 | drops. | |
| Mix. Dose—three tablespoonfuls three times a day. | |||
| Or, take of the tincture of ergot of rye, a teaspoonful in water twice a day. |
| Or, take of the sesqui-chloride tincture of iron, 20 to 30 drops in water, three times a day. |
| For painful Menstruation. | |||
| Add to a portion of gruel, upon going to bed, 15 or 20 drops of laudanum. This quantity may also be taken in the morning, and repeated several days; the bowels in the meantime to be relieved by castor oil. | |||
| The warm hip bath, in these cases, is invaluable. | |||
| Or, take of— | |||
| The extract of stramonium | ½ | gr. | |
| Spanish soap | 5 | grs. | |
| Mix to form a pill to be taken twice a day. | |||
| To allay external irritation.—Sedative application. | |||
| Take of— | |||
| Oil of almonds | 6 | ounces. | |
| Spermaceti | ½ | It seems you haven't provided a phrase for me to modernize. Please provide a short piece of text for me to work on! | |
| White wax[11] | ½ | "Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links." | |
| Rose-water | 3 | ” | |
| Orange-flower water | 10 | "” | |
| Dissolve the wax in the oil, then add the waters, and constantly stir till cold. This is an admirable application for irritation or excoriation of the external parts. It is commonly known as “cold cream.” | |||
| To heal Excoriations.—Mild drying ointment.[12] | |||
| Take of— | |||
| The oxide of zinc | 1 | drachm. | |
| Ointment of spermaceti | 1 | ounce. | |
| Mix. | |||
| For obstinate Excoriations. | |||
| Take of— | |||
| Ointment of nitrate of mercury | ½ | ounce. | |
| Superacetate of lead | 1 | scruple. | |
| Spermaceti ointment, or cold cream | 1 | ounce. | |
| Mix. | |||
The past pages relate chiefly to the diseases of the generative system consequent upon contagion, upon accident, and the ordinary wear and tear of human life: the following, to the ills that ensue from the over-indulgence in, and abstinence from, the proper purposes of the reproductive organs, and the benefits derivable from a fulfilment of the intentions of their natural functions.
The previous pages mainly discuss diseases of the reproductive system caused by infection, accidents, and the usual wear and tear of human life. The following sections will focus on the issues that arise from excessive use and neglect of the reproductive organs, as well as the benefits gained from fulfilling their natural functions.
There may be much good policy and correct feeling in objecting to the too public inquiry into these matters. The private closet and the public eye are two very different tribunals, and what may be approved of in the one is very likely to be condemned in the other. The line of deciding what shall be communicated and what should be suppressed may be drawn too closely; and that knowledge which is acquired by stealth is seldom so practical as that obtained by competition. If, therefore, the topics herein embraced were to be expunged, and their discussion prohibited, the afflicted would have no other resource than to apply to the adventuring and ill-educated empiric, instead of confiding his troubles to the legitimate professional man. A study, to become useful, should be general; and it is to be hoped that the prudish reserve which excludes this kind of investigation from our medical schools will be laid aside, and truth be obtained by allowable investigation.
There can be good reasons and valid feelings for objecting to a public examination of these matters. The private space and the public eye are two very different judges, and what might be acceptable in one is often condemned in the other. The balance of deciding what should be shared and what should be hidden can be drawn too tightly; the knowledge gained through secrecy is rarely as useful as that gained through open discussion. Therefore, if the topics discussed here were to be removed and their conversation banned, those in need would have no choice but to turn to rogue and poorly trained individuals, rather than sharing their concerns with qualified professionals. For a study to be effective, it needs to be broad; and we hope that the modesty that keeps this type of inquiry out of our medical schools will be set aside, allowing truth to be discovered through acceptable investigation.
The most moral and chaste, at the age of puberty, are assailed with feelings and desires, that, though new and unanticipated, yet need little interpretation when present, and so urgent and imperious, that if not legitimately satisfied, nature and instinct are not slow in pointing out a means of gratification.
The most virtuous and innocent, when they hit puberty, are overwhelmed with feelings and desires that, although unexpected and surprising, hardly need explanation when they arise. They are so intense and demanding that if not properly fulfilled, nature and instinct quickly find a way to satisfy them.
In the male, imagination commanding a wider range than in the female, and fed by associations with, and the usages of, the world, elicits consequences explanatory of life’s purposes; and the youth having once experienced, perhaps[163] unsolicited, and possibly during sleep, the agony of seminal secretion, can rarely withstand the afterward tempting pleasure of seeking a self-repetition of such solitary indulgence, which the forbidden union of the sexes, at this early period, may urge him to.
In men, imagination has a broader scope than in women, and it draws from their experiences and interactions with the world, leading to insights about life's goals. Once a young man has experienced the intense pleasure of ejaculation—perhaps unexpectedly and possibly while dreaming—he often finds it hard to resist the temptation to seek out that same solitary pleasure again, especially as societal taboos around sexual relationships at this young age can push him towards it.
Setting aside the selfishness and unmanliness of the vice, it is important that the wearer of the cap and bells should know the consequences of abusing a given function by such a means of gratification. There is no mental passion, or physical exertion, that produces such temporary nervous prostration as the completion of the act of sexual intercourse; and it therefore can be easily conceived how debilitating must be the immoderate indulgence of the practice. Health consists in a due performance of all the functions of the organs of the body, and an undue exercise of them is sure to lead to a disturbance of the economy.
Setting aside the selfishness and lack of masculinity of this vice, it's important for someone who wears the cap and bells to understand the consequences of misusing a particular function for personal pleasure. There is no mental passion or physical effort that causes such temporary exhaustion as the act of sexual intercourse; therefore, it's easy to see how harmful excessive indulgence can be. Good health relies on the proper functioning of all body organs, and overdoing it will surely result in a disruption of the body's balance.
In ordinary sexual commerce, particular phenomena ensue, the circulation is powerfully roused, the heart thumps violently, the blood is driven to the brain, and great mental exaltation is induced, and instances have been known of death suddenly crushing the transport. The too frequent repetition of such excitement can not fail to wear out, and disease the overwrought organs, the heart and brain particularly, upon the healthy condition of which the health of the entire frame rests; and hence the diseases of the libertine are usually consumption, physical weakness, and mental imbecility, all the result of disordered circulation and impaired nervous power. If, therefore, such consequences follow a waste of the allotted privileges of man, how much more severe must they be that arise from nervous exhaustion, that which transpires from an absolute stretch of an already overwrought imagination, from, in fact, ideal pleasures, instead of those springing from the instinctive stimulus imparted by the presence of, and cohabitation with, woman. I have elsewhere treated upon the sad and withering effects of self-indulgence in a hygæan point of view. My object here is to portray the consequences of the like, and the more lawful, intemperance of sexual cohabitation in a domestic light, in how far it is destructive to the health and happiness of others, than the party addressed—the partner of our worldly anxieties, and the offspring that issue from our union. How striking is the change of appearance only, much less the positive bodily condition of married persons of both sexes, within one[164] or two years of their union, especially if the match be a youthful one. Let any one, even with a limited acquaintance, recollect such of his former female associates, whom he knew when single, and mayhap may have indulged with in little modest pleasantries; let him recall the gay-lit countenance, the ruddy and prominent cheek, the sparkling and lively eye, the plump and well filled neck—in fact, let him but compare her then and now, and how disheartening the change; the same being may be recognised, but it is the same being only in mind, and not in person. There are exceptions, as I shall presently show, but this is the too frequent portraiture of those who embark in precocious hymeneal contracts, and restrain not the marital privileges. The countenance assumes, when thoughtful, the careworn aspect; the blanched cheek shows here and there a furrowed imprint; the lustre of the eye is dimmed; and, to drop from the figurative to the literal, the collar-bones, hitherto “overlaid with nature’s plastic moulding,” seem appointed only for union’s sake, lest the fabric of neck and shoulders should drop in pieces. Mark also the decayed health and spirits; hear the bitter grief of headaches, sideaches, nerveaches, and behold, perhaps, the puny offspring “mewling and puling in the nurse’s arms.”
In regular sexual relationships, certain things happen: the circulation gets going, the heart races, blood is pumped to the brain, and a heightened mental state occurs. There are even cases where someone dies suddenly in the midst of this excitement. Repeatedly experiencing such intense feelings can wear out and harm the exhausted organs, particularly the heart and brain, which are crucial for the overall health of the body. Therefore, the diseases related to hedonism often include serious conditions like tuberculosis, physical weakness, and mental decline, all stemming from disrupted circulation and weakened nerves. If these effects follow a careless use of one’s natural privileges, imagine how much worse the consequences must be from complete nervous exhaustion—like the overstimulation that occurs from excessive daydreaming about ideal pleasures rather than those arising from genuine face-to-face connections with a woman. I've discussed the negative and draining effects of self-gratification from a health perspective before. Here, I aim to highlight the impact of similar behaviors, especially the more acceptable excesses of sexual relationships, in terms of how destructive they can be to the health and happiness of others involved—especially our partners and the children that come from our union. It’s striking to see how much the appearance, not to mention the actual health, of married individuals of both genders changes within just a year or two of their marriage, especially if the marriage is between young people. Anyone can recall former female friends known when they were single and perhaps enjoyed some light flirtation with. Think back to their bright smiles, flushed cheeks, sparkling eyes, and full necks—now compare that to how they look now, and it's disheartening. While you might recognize the same person, it’s really just in spirit, not in appearance. There are exceptions, which I will mention shortly, but this is often the reality for those who rush into marriage and don't hold back from indulging in their marital rights. When they look pensive, their faces show signs of stress; their once rosy cheeks may now have wrinkles; their eyes lose their sparkle; and physically, their collarbones, once beautifully shaped, seem to lack structure, as if only there for the sake of the marriage. Also, notice how their health and energy decline; listen to their complaints of migraines, side pains, and nerve issues, and you might even see their frail children "crying and fussing in the nurse’s arms."
The bridegroom wears a sorrowful and thoughtful look. He may possess all the comforts which few inherit, but like Pharaoh’s lean kine, as chaff thrown before the wind, their purpose is opposed.
The groom has a sad and pensive expression. He might have all the comforts that few people get, but like Pharaoh’s lean cows, they scatter like chaff in the wind, their purpose is thwarted.
This may be held as a ridiculous picture, but I defy denial of its unhappily too frequent illustration in real life. A word or two on the opposite extreme, continence. The reader will observe, in another page, the remark that every part, be it flesh, bone, or nerve, has its use. The reproductive organs have theirs; but it is not only for the propagation of the species—they afford an outlet for accumulated secretion—they aid in resolving the animal passions—they are the secret incentive to sexual love, and the bond of union between the sexes. They give an appetite that, like hunger, must be appeased, or nature revolts; and the harmony of society falls before the ungovernable fury of maniacal craving. Health, the source of all happiness, without the possession of which the world with its beauties would be, for all we cared, tenantless, materially rests upon a proper and moderate use of the copulative process. Entire continence, a rarity among mankind, establishes in[165] both sexes the most miserable perversions of mind and body. In man, we have instances recorded of mania, melancholy, apoplexy, and foul skin-disorders. Blindness, deafness, and a host of evils, some greater, and few less than these just penned. It is true, continence is, as remarked, but seldom observed, especially in males, who, being denied sexual commerce, are estranged by the distressful habit of onanism; and thereby, in some measure, the enumerated maladies are avoided; but as masturbation, like other vices, grows with unbounded speed, a train of ills, far more distressful, await the sufferer, who, in addition, becomes, in the meridian of life, deprived of the very power he in youth was so improvident of. Continence in females, which all admit to be the brightest ornament a woman possesses, is attended with a poor requital; and its prevalence (to the honor of our countrywomen be it spoken) is truly attested by the miseries of hysteria, and other nervous derangements, that pervade the junior and elderly maiden branches of every family, and constitute so formidable an enemy to domestic felicity. A wide field is open for comment upon this subject, which is better adapted for the moralist than the physician. This manual, professing to be but a vehicle for topics of a professional nature only, the writer apologises for the digression, and can but express his regret, that public opinion is unfavorable to the discussion of such matters, which embrace considerations highly important to a nation, both in a moral and hygæan view. Continent persons but seldom attain old age; whereas, the married females, for instance, although exposed to the dangers of pregnancy and delivery, live generally longer than those who are unmarried or chaste; and provident married men escape the ills and snares that beset single blessedness, as it is called. Libertinism, on the other hand, in whatever way practised, is hurtful and destructive to long life.
This might seem like a ridiculous idea, but I challenge anyone to deny that it happens far too often in real life. A word or two on the other end of the spectrum, continence. You’ll see in another section the observation that every part of the body, whether flesh, bone, or nerve, has its purpose. The reproductive organs serve their purpose, but it's not just about creating new life—they provide an outlet for built-up energy, help manage animal instincts, fuel sexual desire, and create a bond between genders. They create a craving that, like hunger, needs to be satisfied, or else nature reacts, and social harmony suffers under the overwhelming pressure of uncontrollable desire. Health, which is the foundation of happiness, without which the world’s beauty would mean nothing to us, fundamentally relies on the proper and moderate use of sexual activity. Complete continence, which is rare among humans, leads both sexes to suffer from serious mental and physical problems. In men, we see documented cases of mania, depression, strokes, and serious skin issues. Blindness, deafness, and many other problems—some worse, few better than those mentioned—also occur. It's true that continence is rarely seen, especially in males, who, when deprived of sexual activity, often turn to the distressing habit of masturbation; this can partly prevent the aforementioned ailments, but as masturbation, like other vices, escalates quickly, a new set of even more troubling issues arises for the sufferer. By mid-life, they lose the very ability they squandered in their youth. Continence in women, regarded as one of their greatest virtues, often results in low rewards; and its prevalence—honorably acknowledged among our countrywomen—can be seen in the widespread struggles with hysteria and other nervous disorders affecting both young and older single women in every family, which poses a serious threat to domestic happiness. There’s a lot to be said about this topic, which is more suited for moralists than doctors. This manual, which claims to focus solely on professional topics, apologizes for the digression and expresses regret that public opinion is generally against discussing such matters that are critically important to a nation from both moral and health perspectives. Continent individuals rarely reach a ripe old age; however, married women, for example, despite the risks of pregnancy and childbirth, tend to live longer than their unmarried or chaste counterparts; and responsible married men avoid the traps and difficulties that accompany single life. Conversely, libertinism, in whatever form it takes, proves harmful and destructive to longevity.
Continence may be a virtue, but is not imposed where marriage is allowable; and then, if deviated from with moderation only, the greatest amount of health and happiness may be elicited, and the proper end of it obtained. Matrimony, where succeeded by the birth of children, powerfully conduces to the health and happiness of women.
Continence might be seen as a virtue, but it isn't required where marriage is an option. If someone strays from it in moderation, they can achieve a great degree of health and happiness, reaching its true purpose. Marriage, especially when it leads to having children, greatly contributes to the health and happiness of women.
Results should, however, be well weighed, before irrevocable steps are taken. There are many diseases and structural impediments opposed to the matrimonial contract. Malformation and mental imbecility should be held as strong interdicts to the conjugal union. People ought not to marry before manhood is well developed (the male at least 21 to 23 years of age, the female 18 to 21). Precocious or late marriages are injurious to reproduction. The unnatural union of old and young of either sex with the other, entails its own miseries. A curious estimate of salacious appetites and power has been drawn up as pervading the different temperaments. The temperaments, as elsewhere noticed, are four—the Sanguine, Nervous, Bilious, and Phlegmatic. Persons of the sanguine temperament are generally of good health, and vigorous in amorous pleasures. The nervous are extremely susceptible in their sensations, and generally much given to female society. Combined with the sanguine, they are capable of great amorous excesses. The bilious temperament imparts a jealous bearing in all affairs of sexual solicitude, that detracts from the fondness and affection which so entwine a woman to a lover or a husband. The melancholic or phlegmatic person is frigid and apathetic in his amours; and love becomes with him a secondary consideration to advancement in life. These temperaments are frequently intermixed, and are much modified by age and health; and the salacious powers correspond.
Results should, however, be carefully considered before any irreversible actions are taken. There are many illnesses and structural issues that can hinder the marriage contract. Disability and mental incapacity should be viewed as significant barriers to the union. People should not get married before they’ve fully matured (males at least 21 to 23 years old, and females 18 to 21). Marrying too early or too late can negatively affect reproduction. An unnatural pairing of an older person with a younger one, regardless of gender, brings its own hardships. A curious assessment of sexual desires and capabilities has been made based on different temperaments. As previously mentioned, there are four temperaments—the Sanguine, Nervous, Bilious, and Phlegmatic. People with a sanguine temperament are generally healthy and enthusiastic about romantic pursuits. The nervous type is highly sensitive in their feelings and tends to seek female company. When paired with the sanguine temperament, they can engage in intense romantic behaviors. The bilious temperament tends to introduce jealousy into sexual matters, detracting from the affection that binds a woman to her partner or husband. The melancholic or phlegmatic individual is cold and indifferent in love; for them, romance is secondary to achieving success in life. These temperaments often blend together and are significantly influenced by age and health, and the sexual capabilities reflect these changes.
Speculations have arisen among physiologists, as to the effect of climate and season, as well as age and temperament, on the reproductive powers. Temperate and warm climates are more prolific in exciting the copulative desire, than the frigid and uncongenial situations of the northern hemisphere. The seasons bear a somewhat near analogy—spring is supposed to be more potent than summer, autumn, or winter, in arousing the amative propensities, which, like the productions of the earth, come, as it were, at that time into a new existence. This observation is borne out by the statistical fact of there being a greater number of births about Christmas and the new year, than any other period.
Speculations have emerged among physiologists regarding how climate and season, along with age and temperament, affect reproductive abilities. Temperate and warm climates tend to stimulate sexual desire more effectively than the cold and harsh conditions found in the northern hemisphere. The seasons show a similar pattern—spring is believed to be more effective than summer, autumn, or winter in triggering romantic instincts, which, similar to nature's products, seem to come into new existence during that time. This observation is supported by the statistical fact that there are more births around Christmas and the new year than at any other time.
Man, however, is allowed to be omnivorous in all his appetites; and the uniformity of his sexual greediness is[167] preserved by diet corresponding to the season, which renders the whole twelvemonth a perpetual spring. Man, as well as other animals, is, when in a state of health, capable of procreating upon almost any food. But when there is debility of the digestive or generative organs, the injury can be repaired by the use of proper stimulating diet, thereby occasioning due and sufficient secretions.
Man, however, can be greedy in all his desires; and the consistency of his sexual appetites is[167] maintained by a diet that changes with the seasons, making the entire year feel like a continuous spring. Just like other animals, when healthy, man can reproduce on almost any type of food. However, if there is weakness in the digestive or reproductive systems, this can be fixed by having the right stimulating diet, which leads to proper and adequate bodily functions.
Air, exercise, health, and prosperity, are not without considerable influences. If seasons are not positively influential, certain it is, that particular lunar and solar periods are, taken in conjunction with the state of the body.
Air, exercise, health, and prosperity all have significant effects. While the seasons may not always have a positive impact, it's clear that specific lunar and solar phases do, especially when considered alongside the condition of the body.
“Morning,” says a French writer, “is the spring of the journey, when all the functions of the body are renovated.” Others declare, that when night veils the light of the day, the quietude and secresy thereby afforded, offer moments most congenial to the gratification of mutual love. Sexual transports should be avoided after a repast, instances having been known of apoplexy being induced by the excitement of connexion being superadded to the stimulative influence of wine and food.
“Morning,” says a French writer, “is the beginning of the journey, when all the functions of the body are refreshed.” Others claim that when night covers the light of day, the peace and secrecy it brings provide the best moments for enjoying mutual love. Sexual excitement should be avoided after a meal, as there have been cases of apoplexy caused by the excitement of intimacy combined with the stimulating effects of wine and food.
Henry II. consulted one Fernal for the infertility of his queen, Catherine de Medicis. The advice submitted, comprised the following notifications: Abundant and peculiar nourishment; occasional change of residence; the allowing several days to elapse between each conjugal act; and lastly, that the most favorable moment for impregnation was immediately on the cessation of menstruation. It was not until the adoption of these hints, that her majesty conceived.
Henry II consulted a man named Fernal about the infertility of his queen, Catherine de Medici. The advice given included the following suggestions: a rich and unique diet; occasional changes of living arrangements; allowing several days to pass between each sexual encounter; and, finally, that the best time for conception was right after her period ended. It was only after following this advice that her majesty became pregnant.
Professor Dewees, of Philadelphia, enjoins that, for the enjoyment of marriage and the production of children, matrimony should not be engaged in, until the body is healthily and completely developed; until then the most scrupulous continency should be preserved. From the 23d to the 25th year is the suggested period for the male; from the 19th to the 21st, the female. These observations apply to Europeans chiefly; for in India, women become mothers at ten, owing to their early development. Precocious marriages bring premature decay on the father and mother, and entail on their offspring, diminutive stature, debility of body, and imbecility of mind, thus generating consumption, scrofula, insanity, &c. Well-regulated marriages contribute to social and lasting happiness, and the prosperity of the nation at large; but ill-assorted ones, those where the peace[168] of either is infringed by opposing tempers, or by the after-discovery of hitherto concealed physical incapacities, present a scene of wretchedness and disappointment to which death itself were preferable. These remarks might be considerably amplified; but enough has been said, to induce those who approach to manhood, to be provident of that which, once lost, is, under all circumstances, difficult to regain; and those on the eve of embarking in the most binding and solemn obligation of all human contracts, marriage, to ponder well, ere they compromise the happiness of others as well as themselves, by engaging in a compact, they may know themselves incapable of fulfilling or of efficiently performing; one from which they can not with honor retreat, and one that, once sealed, demands a rigid compliance with its recognised duties.
Professor Dewees from Philadelphia advises that for a fulfilling marriage and the creation of children, people shouldn’t get married until their bodies are fully developed and healthy. Until then, it’s essential to practice strict self-restraint. It’s recommended that men wait until they are between 23 and 25 years old, and women until they are between 19 and 21. These suggestions mainly apply to Europeans, as in India, women often become mothers at around ten due to their early development. Early marriages can lead to premature decline in health for both parents, and their children may suffer from short stature, physical weakness, and mental challenges, potentially resulting in conditions like consumption, scrofula, or insanity. Well-planned marriages can lead to social happiness and the overall prosperity of the nation, but poorly matched marriages, where one partner’s peace is disturbed by clashing personalities or the later discovery of hidden health issues, result in misery and disappointment that can sometimes make death seem preferable. These thoughts could be expanded further, but enough has been shared to encourage those approaching adulthood to be mindful of what, once lost, is hard to regain. Those on the brink of entering the most serious and binding commitment of all human agreements, marriage, should carefully consider their actions before putting the happiness of themselves and others at risk by entering into a commitment they may realize they cannot fulfill or perform effectively. Marriage is a bond that, once made, carries responsibilities that must be strictly adhered to.
The gist of the present article may then thus be summed up: That self-indulgence and excessive sexual cohabitation are hurtful in the highest degree; that they induce early impuissance, and bring down a load of menial and corporeal ailments. That premature marriages are destructive to health and long life, and that weak and sickly children are the general result where impregnation of the female follows. That entire continence was never ordained, and is alike productive of disease. That moderate copulation propagates the human kind, preserves health, and promotes longevity, and the sexual capability is thereby retained to the latest verge of senility.
The main point of this article can be summed up as follows: Self-indulgence and excessive sexual activity are very harmful; they lead to early impotence and cause a range of physical and mental health issues. Premature marriages are detrimental to both health and longevity, often resulting in weak and unhealthy children when women become pregnant. Total abstinence was never intended and can also lead to health problems. Moderate sexual activity helps continue the human race, maintains health, and supports a longer life, allowing sexual capability to be preserved well into old age.
That it is unnatural and unjust for impuissant persons to intermarry with those having healthy expectations, and the power of enjoyment; and that it behooves all who have a doubt as to their own capacity, to have that doubt removed; but, if rendered evident, to abstain from shipwrecking their own happiness, or from occasioning disappointment to others.
That it's unnatural and unfair for powerless people to marry those with healthy expectations and the ability to enjoy life; and that anyone who doubts their own ability should get that doubt cleared up; but if it's obvious, they should avoid ruining their own happiness or causing disappointment to others.
The topics of Incontinence, Celibacy, and Marriage, having been severally considered relatively to their effects on society, viewed alike also as to their influence on the health and happiness of the sexes in general, another equally engrossing one naturally presents itself for inquiry to every thinking and sensible person who may contemplate, or be about embarking in what the world deems “a serious speculation,” matrimony, namely, the probability of issue, and how far the health of the progeny may be influenced by that of the parents. That conception requires the necessary aptitudes in both man and wife is indisputable; and that although such capacities are rarely absent, still all unions are not prolific; hence the inference, that some cause must exist to account for such infertility.
The topics of incontinence, celibacy, and marriage have been considered for their effects on society, as well as their influence on the health and happiness of both sexes. Another equally engaging question naturally arises for anyone thinking about or considering what the world calls "a serious commitment," which is marriage: the likelihood of having children and how much the health of the offspring may be affected by the health of the parents. It's clear that conception requires the necessary qualities in both partners; and while these qualities are often present, not all unions result in children. Therefore, it's reasonable to conclude that some other factors must explain such infertility.
It may be local or moral, as elsewhere in this volume explained, which not being the main purport of this paper, needs no other allusion beyond the mere reference. The prevailing resemblance between parents and children in features, form, voice, and even constitutional peculiarities, is sufficiently well known to satisfy any one of the similar possibility of the transmission of disease, or sound health. “It is of great consequence to be well-born; and it were happy for human kind, if only such persons as are sound of body and mind should be allowed to marry.”
It can be local or moral, as explained elsewhere in this book, which, since it's not the main focus of this paper, doesn’t need further detail beyond this brief mention. The strong similarities between parents and children in looks, shape, voice, and even unique traits are widely acknowledged, making it easy to believe in the possibility of passing on both diseases and good health. “It’s very important to be well-born; and it would benefit humanity if only people who are healthy in body and mind were allowed to marry.”
We find in Boethius’s work, “De veterum Scotorum Moribus,” that anciently, in Scotland, if any were visited with the falling sickness, madness, gout, leprosy, or any such dangerous disease, which was likely to be propagated from the father to the son, he was instantly gelded; a woman kept from all company of men; and, if by chance, having some such disease, she were to be found with child, she with her offspring was buried alive. The Spartans destroyed all weakly and deformed children.
We see in Boethius’s work, “De veterum Scotorum Moribus,” that in ancient Scotland, if someone had epilepsy, madness, gout, leprosy, or any serious illness that could be passed down from parent to child, they were immediately castrated; a woman was kept away from all male company; and if she happened to be pregnant while having such a disease, she and her child were buried alive. The Spartans eliminated all sickly and deformed children.
Great as the anxiety may be to perpetuate our identities, to create new objects on whom we may concentrate all our affections and love, and who, when born to us, so instinctively bind us the more to this already attractive world, where is the man who does not feel humbled and mortified at beholding in his anxiously looked-for offspring, the unfolding[170] of infirmity and disease? We are content to encounter the ordinary chances of mortality, let but our children bear the impress of health, and possess the shape of perfect man; but sad and desolating are the reflections that spring from observing in our issue the developments of the evils we have nurtured in ourselves. How many existing beings are there, inhaling the breath of life, in whom every respiration feeds the flame of disease, ignited by those from whose loins they sprung, and is hastening them to a premature tomb. How many are there, secluded from the enjoyment of that, which being deprived of by some scrofulous, pestilential, or other hideous deformity, renders them like isolated wanderers on the earth, and for ever forbids their participation in the main charm of existence—social intercourse. How many living specimens of human prototypes, in whom reason is obliterated, or never dawned, drag on an existence inferior in enjoyment to the forest-hunted beast, or the animal whose life is yielded for the nutriment of man. And are not the diseases that involve so calamitous a result, consumption, scrofula, gout, idiocy, or insanity, traceable in particular families, to the remotest periods of their ancestral records? And should not then a knowledge of cause and effect, like that just detailed, induce individuals about to fulfil one of the purposes to which they were certainly destined, for the perpetuation of their own race, if only from the pride of human nature, well to consider the result of such a consummation? The health of either party is generally omitted among the categories bandied about preliminary to the completion of the other, though decidedly not more important, arrangements of the nuptial contract; or if it should not be, many infirmities, that are well known to descend hereditarily, are (granted in some cases not premeditatedly, but from ignorance of such a result) yet carefully concealed. Cutaneous blemishes, incipient tubercles, or a scrofulous predisposition, which may be likened to the germes of a fruitful plant sown in a torpid soil, lie in ambush, and await some genial transplantation to display their productiveness, which matrimony, by the analogous change which it effects in different constitutions, speedily encourages. In this manner, other morbid phenomena are aroused from their lurking place, whether it be in the brain, the lungs, or the blood, and transferred to those who succeed us.
As much as we might worry about maintaining our identities, about creating new beings to whom we can direct all our love and affection—who, once they come into our lives, instinctively tie us closer to this already captivating world—who here doesn’t feel a mix of humility and disappointment when they see the signs of illness and weakness unfolding in their long-awaited children? We’re generally okay with facing the typical risks of mortality, as long as our children appear healthy and have the form of perfect individuals; but it’s sad and disheartening to recognize the issues we’ve fostered within ourselves reflected in our offspring. How many living people are out there, breathing in life, where every breath fuels the fire of disease ignited by their parents, pushing them toward an early grave? How many are cut off from enjoying life because they’re marked by some debilitating or grotesque condition, making them feel like lonely wanderers on this planet, forever barred from engaging in the greatest joy of life—social interaction? How many living examples of humanity exist where reason is absent or never developed, leading a life less fulfilling than that of a wild animal hunted in the forest, or the creatures that end up as food for humans? And aren’t the diseases that lead to such tragic outcomes—like tuberculosis, scrofula, gout, idiocy, or madness—traceable through specific families, going back to the earliest records of their ancestry? Shouldn’t this understanding of cause and effect prompt individuals about to fulfill their destined role in continuing their lineage—even just for the sake of human dignity—to seriously think about the consequences of such a continuation? The health of either party is usually overlooked among the various details discussed before finalizing the marriage agreement, even though it’s certainly no less important; or even if it’s not, many known hereditary weaknesses are (though sometimes not intentionally, but out of ignorance) deliberately hidden. Skin blemishes, early-stage lumps, or a predisposition to scrofula, which can be compared to the seeds of a thriving plant buried in barren soil, lie in wait, ready for a hospitable environment to show their potential, which marriage, through its transformative effects on different characters, quickly promotes. In this way, other health issues are awakened from their hiding spots—whether in the brain, lungs, or blood—and passed on to those who come after us.
I need not, therefore, waste a line prefatory to, or apologetic of, the following illustrative definition of health, by which any one with tolerable acumen may estimate the probable “worth of a life,” or, at all events, be spared the plea of ignorance, or misplaced confidence, when taking a step of such importance as wedlock. There are numerous means of calculating upon the durability of human life, by an examination of the countenance, the gait, the attitude, the form, the skin, the temperament, the breathing, the speech, the sleep, and in fact, to a practised professional eye, there is not much difficulty in observing some diagnostic mark, if sickness be secreted in the constitution. The countenance in health varies with the age. Health is indicated by a plump, not puffy or bloated state of the face, a fresh complexion, and an absence of that depression around and particularly below the eye, so observable in persons of sick health. The nose should not be “pinched,” as it were, at its junction with the face, nor should there be deep indentations, called furrows, or wrinkles, at the angles of the mouth or eyes, which rarely are manifested in healthy individuals, except they be aged through care or time. Many people part very reluctantly with each succeeding year, and few conform to the outward symbols of age. The era was when age was honorable; now few aspire to it, and such is the deception that would be practised, that the coffin-plate is the only tell-tale.
I don’t need to waste a line explaining or apologizing for the following definition of health, which anyone with reasonable insight can use to assess the potential "value of a life," or at least avoid the excuse of ignorance or misplaced confidence when making an important decision like marriage. There are many ways to gauge the longevity of human life by examining the face, the way someone walks, their posture, body shape, skin condition, temperament, breathing, speech, and sleep. In fact, to a trained professional, it’s not very difficult to spot some signs of illness if it exists within the body. A healthy face varies with age. Health is shown by a full face that isn’t puffy or bloated, a fresh complexion, and no dark circles, especially under the eyes, which are often seen in unhealthy individuals. The nose shouldn’t look “pinched” where it connects to the face, and there shouldn’t be deep lines or wrinkles at the corners of the mouth or eyes, which are rarely seen in healthy people unless they are aged due to stress or time. Many people are reluctant to accept each passing year, and few accept the visible signs of aging. There was a time when aging was respected; now few aim for it, and the only evidence left is what’s on the coffin plate.
If the teeth have dropped out or decayed, the lower jaw will be observed to be more elevated, the lips drawn inward over the gums, and the chin and nose approximating each other; the cheek bones will also be very prominent, and the skin thereon shiny and tightly drawn: these are pretty fair characteristics of disease, or old age. The temperaments modify the complexion. In the sanguine, it is florid and soft; in the bilious, dark and rigid; in the phlegmatic, lax and pallid; and the nervous is modified by its general union with the two former. In health, the countenance is expressive of contentment and gayety, which indicate a happy state of mind, and healthy condition of body. In ill-health, it is pale and expressive of languor and sadness, signifying discontent and nervous debility. Where asthma exists, or other nervous affections of the chest prevail, there is pallidness or lividity, a worn-down and distressing look, and in consumption, in addition to the above, there are alternately, on the slightest exertion,[172] gentle flushings. A bluish tint of the skin denotes some organic affection of the heart. In dropsy, the countenance is bloated, or of a waxy puffiness; and in acute indigestion, there is a lividity of the lips, nose, and cheeks. A slow and cautious step, a bending of the body, a laxity and flabby feel of the muscles of the arms, chest, and lower extremities, a tumid abdomen, or a swelling of the feet and ankles, are no indications of health. Tremulous hands mark age, nervousness, or intemperance. Hurried breathing, palpitation of the heart, frequent attacks of perspiration, sleeplessness, are all symptomatic of weakness, hysteria, or disease. Persons subject to bleedings, are usually of a waxy paleness, and soft fibre. Allowances must be made for females during the menstrual period, whose complexion, at that period, being less clear and fair, is marked by a dark areola around and below the eyes, the breath is slightly tainted, and a languor is evidenced in all their actions. A voracious or scanty appetite, a dry and shrinking skin, a furred and loaded tongue with indented sides, signify the digestive organs to be deranged. In long-standing dyspepsia, the nose, feet, and hands, are generally cold. Emaciation is an infallible diagnostic of disturbed health, and a bloated state equally characteristic. Fits, gout, rheumatic disorders, asthma, occasional brain affections, diseases of the bladder, &c., can not be considered as warranties of health.
If teeth have fallen out or rotted, you’ll notice that the lower jaw appears higher, the lips are drawn in over the gums, and the chin and nose come closer together; the cheekbones will also stand out more, with shiny, tight skin over them. These are pretty good signs of illness or old age. Different temperaments affect the complexion. People with a sanguine temperament have a rosy and soft complexion; bilious individuals tend to have a dark and rigid appearance; phlegmatic types look loose and pale; and the nervous type is influenced by a mix of the previous two. When healthy, a person's face shows contentment and cheerfulness, reflecting a happy mind and a healthy body. When someone is unwell, their face looks pale and expresses fatigue and sadness, indicating dissatisfaction and nervous weakness. In conditions like asthma or other nerve-related chest issues, the person may appear pale or bluish, with a weary and distressed look, and in cases of consumption, they might also experience occasional flushes with even slight exertion.[172] A bluish tint to the skin suggests some heart condition. In cases of dropsy, the face looks swollen or has a waxy puffiness; during acute indigestion, the lips, nose, and cheeks may have a bluish hue. A slow, careful walk, a hunched posture, and loose, flabby muscles in the arms, chest, and legs, along with a swollen abdomen or feet and ankles, are not signs of good health. Shaky hands can indicate age, nervousness, or excess indulgence. Quick breathing, heart fluttering, frequent sweating, and insomnia all signal weakness, anxiety, or illness. People who tend to bleed often have a waxy pallor and soft skin. Special considerations should be made for women during their menstrual period, as their complexion may become less clear and fair, showing dark circles around the eyes, slightly bad breath, and a general lethargy in their movements. A strong or weak appetite, dry and tight skin, and a coated tongue with indentations along the sides indicate digestive issues. In chronic indigestion, the nose, hands, and feet are usually cold. Being very thin is a clear sign of poor health, while bloating can also indicate the same. Conditions like fits, gout, rheumatism, asthma, occasional brain issues, bladder diseases, etc., cannot be considered signs of health.
Lastly, with respect to intemperance, the bloated appearance, the tremulous state of the muscular powers, the fetid breath, and the sunken eye, sufficiently identify the cause, to arrest all doubts on the subject. Where intemperance exists in married life, it is the bane of all comfort and enjoyment; and heaven help the unhappy partner of such a companion. There is but one consolation, that every indulgence of this insane practice tends to sap and break up the powers of the constitution, and hastens the close of such a union. The drunkard should be reminded, that “some leaves fall from the tree every time that its trunk is shaken;” and the dreary nakedness of winter is brought on, long before that season would have commenced in the regular course of nature.
Lastly, regarding excessive drinking, the puffy appearance, the shaky muscles, the bad breath, and the hollow eyes clearly point to the problem, leaving no room for doubt. When excessive drinking is present in a marriage, it ruins all comfort and happiness; and God help the unfortunate spouse of such a partner. There's only one silver lining: every time this reckless behavior is indulged in, it weakens the body and speeds up the end of that relationship. The alcoholic should be reminded that “some leaves fall from the tree every time its trunk is shaken;” and the bleak emptiness of winter arrives long before that season should naturally begin.
Upon pursuing the consideration of the following infirmities of the Reproductive System, a few prefatory observations are requisite. Perhaps of all the physical powers possessed by man, few are subject to so much abuse as the procreative organs—certainly none are more required to be, in a hygiænic point of view, held in a sounder condition of health, for upon their tone and perfect structure hinge the happiness and perpetuation of the human race. In this age of luxury and sensuality, however, the world seems untiringly hunting after, and more or less obtaining, sexual gratification. There can be no doubt, that a greater amount of this species of sensual enjoyment is indulged in before manhood arrives, than can be obtained when man should be in his vigor. The writer is not insensible to the many alluring publications upon this topic, the end and aim of which are not, honestly, to afford relief to the diffident sufferer, but to add to his misery, by draining his pocket. Of legitimate publications, alas! there are but few, for it appears that qualified medical men have, from some prudish or other such notions, kept aloof from entering the lists. Were it otherwise, many an unfortunate victim might be spared from the avaricious clutch of the empiric; but invalids, from such a knowledge of the absence of fair and honorable references, are obliged to seek (or despair of) relief from the unworthy class in question. How far the tendency of the present work may lead to a reformation, is left for the reader to decide. The novelty of the present compendium may subject it to invidious suspicion; the author but invites comparison, feeling convinced that the contents best bespeak its legitimacy and usefulness.
When exploring the issues related to the Reproductive System, a few introductory remarks are necessary. Of all the physical abilities humans possess, few are as commonly misused as the reproductive organs—none are more essential to be kept in a healthy state from a hygiene perspective, since their tone and proper structure are critical for the happiness and continuation of the human race. However, in this age of luxury and indulgence, people seem to relentlessly pursue, and often achieve, sexual pleasure. There's no doubt that more of this type of sensual enjoyment is experienced before reaching adulthood than can be found during a man's peak years. The author is aware of the many tempting publications on this subject, which are not genuinely aimed at helping the hesitant sufferer, but rather at worsening their situation by draining their finances. Unfortunately, there are few credible publications, as it seems qualified medical professionals have refrained from engaging with the topic due to some prudish or similar attitudes. If the situation were different, many unfortunate individuals might be protected from the greedy grasp of unqualified practitioners; however, patients, lacking reliable and honorable references, are forced to seek (or give up on) help from the disreputable individuals in question. Whether this work leads to any change is up to the reader to determine. Its novelty may render it vulnerable to negative scrutiny; the author merely invites comparison, confident that the contents speak for its validity and value.
“Increase and multiply,” is the scriptural text. “Plant trees and beget offspring,” is the apothegm of the Magi. The perpetuation of the species being, with the great Designer of the universe, an object of the first interest, all living beings are mentally and physically formed with a view to this great end.
“Increase and multiply,” is the scriptural text. “Plant trees and have children,” is the saying of the Magi. Since the continuation of the species is a primary concern of the great Designer of the universe, all living beings are shaped both mentally and physically with this important goal in mind.
In the human species, procreation is effected by a congress of the two sexes, and a variety of organs are provided, upon whose condition the due performance of coition mainly depends. The male is destined to furnish a peculiar fecundating secretion, and is accordingly provided with glands to prepare such fluid, and a conduit to convey the same to its proper destination; while the female, being the recipient, possesses an organ capable of effecting a mysterious yet specific change upon the fluid so deposited: a failure, therefore, in any of the structures alluded to, is followed by impotence or sterility.
In humans, reproduction happens through the union of two sexes, and various organs are involved, the function of which is crucial for successful intercourse. The male is designed to produce a specific fertilizing fluid and has glands to create this liquid, along with a passage to deliver it to the right place; while the female, as the receiver, has an organ that can induce a unique yet specific change to the fluid that is deposited. Therefore, any problem with these structures can lead to impotence or infertility.
Impotence implies the incapability of sexual intercourse; sterility, the inability of procreation; the causes of either of which may be deemed organic, functional, or moral. The following section will be devoted, firstly, to its consideration in its relation to the male.
Impotence refers to the inability to have sexual intercourse; sterility means the inability to conceive. The causes of either can be considered organic, functional, or psychological. The next section will focus on this in relation to males.
SECTION I.
IMPOTENCE AND STERILITY OF THE MALE.
IMPOTENCE AND STERILITY OF THE MALE.
Where the hindrance to cohabitation arises from organic defect, congenital malformation, or diseases of some of the organs of generation, the disqualification may generally be considered absolute or irremediable. It is remarkable, however, to what extent mutilation or disease may occur, without total annihilation of the procreative powers; the smallest remnant of the penis, for instance, capable of entering the vagina, provided the testes be sound, being sufficient for impregnation.
Where's the location? the barrier to living together comes from physical defects, congenital issues, or diseases affecting some reproductive organs, the disqualification is usually seen as absolute or unfixable. However, it's interesting to note how much damage or illness can happen without completely destroying reproductive abilities; even a small remnant of the penis that can enter the vagina, as long as the testes are healthy, is enough for conception.
A learned lecturer on medical jurisprudence gives it as his opinion, that the smallest quantity of seminal discharge, deposited in the lower part of the female generative apparatus, provided the female be apt to conceive, is sufficient for impregnation: and it is astonishing how minute a quantity of this plastic agent is necessary for that purpose in some species of creatures. Spallanzani took three grains by weight of the male fluid of the frog, and mixing it with seventeen ounces of water, found that impregnation of the eggs was produced by as much of this exceedingly weak mixture as would adhere to the point of a fine needle.
A knowledgeable lecturer on medical law states that even the smallest amount of semen deposited in the lower part of the female reproductive system, as long as the female is capable of conceiving, is enough for fertilization. It’s incredible how tiny an amount of this essential substance is needed for that purpose in some species. Spallanzani took three grains of male frog fluid and mixed it with seventeen ounces of water, discovering that fertilization of the eggs occurred with just a tiny amount of this extremely diluted mixture that would stick to the tip of a fine needle.
Although, in human formation, it is not essentially necessary that the male material should be deposited in the upper part of the vagina of the female, yet there is little[175] doubt that the deeper entrance of this substance conduces to impregnation.[13]
Although it isn't strictly necessary for the male sperm to be deposited in the upper part of the female's vagina for human reproduction, there’s little doubt that deeper entry of this substance aids in fertilization.[175][13]
Malformation of the genital organs has already been stated as a cause of impotence. Such cases furnish much uneasiness at first, but are easily relievable. I have met with many instances, where consummation has been prolonged from months to years, which a slight knowledge of the functions of the parturient organs might have relieved in a few days; and with respect to the latter, it may be pardonable to mention that, as the husband should be the first to instruct his companion in what is to be expected, but little disappointment will be experienced, except with the vicious and unworthy.
Malformation of the genital organs has already been mentioned as a cause of impotence. Such cases cause a lot of anxiety at first, but they can be easily addressed. I've encountered many situations where the completion of sexual activity has been delayed for months or even years, which understanding the functions of the reproductive organs could have resolved in just a few days. It's worth noting that the husband should be the first to educate his partner on what to expect, so there will be little disappointment, except for those who are dishonest or undeserving.
There is room for much ingenuity in these matters; and as marriages are made for better or worse, there exist powerful inducements to resort to the contrivances of the ingenious and humane.
There is plenty of room for creativity in these situations; and since marriages are made for better or worse, there are strong reasons to turn to the solutions of the clever and compassionate.
The following case of malformation fell under my own observation; the adjoining delineation is a true picture of the circumstance.
The following case of malformation was something I personally observed; the image next to this text is an accurate representation of the situation.

The penis, b, at its under surface, was adherent, from birth, to the scrotum c, consequently, when erection ensued, it presented the form of a half circle; the urine escaped near the root of the penis, a. The penis itself was impervious, but sensible to the amative passion. The gentleman submitted to a division of the fold which united the penis with the scrotum, which former, on being thus released, assumed its proper position; sexual congress was thereby attainable, and during erection the orifice of the urethra was drawn sufficiently up to allow of the ejection of the semen into the vagina. Of the ultimate result I have yet to hear.
The penis, b, on its underside, was attached from birth to the scrotum c, so when an erection occurred, it formed a half-circle. Urine passed out near the base of the penis, a. The penis itself couldn't be penetrated but was responsive to sexual desire. The man agreed to a procedure to sever the connection between the penis and scrotum, and once freed, the penis returned to its proper position; sexual intercourse became possible, and during an erection, the opening of the urethra was pulled up enough to allow semen to be released into the vagina. I have yet to learn about the final outcome.

It may appear almost incredible, that the sketch here presented can be a true one of the penis and testicles of a young man upward of 19 years of age. No less was it a source of wonderment to myself than it may afford a doubt to others. I carefully examined the individual, and saw him urinate; the stream was certainly small, but surprisingly large for so minute an organization.[176] He was quite unconscious of amative feeling; the testicles were distinctly perceptible by the finger, but they certainly were not larger than cherry kernels. The young man, in other respects, preserved the male attributes; he had a slight beard, and his voice, though not powerful, was by no means effeminate. I had several interviews with him, and then lost sight of him.
It might seem unbelievable that the description given here could accurately represent the penis and testicles of a young man over 19 years old. It was just as much a source of curiosity for me as it may raise questions for others. I closely observed the individual and watched him urinate; the stream was definitely small, but surprisingly large for such a small body. [176] He was completely unaware of any sexual feelings; the testicles were clearly noticeable to the touch, but they were definitely no bigger than cherry pits. The young man still showed the characteristics of a male; he had a slight beard, and his voice, while not strong, was by no means feminine. I met with him several times, and then I lost track of him.
I have elsewhere portrayed a relaxed state of the testicle, called varicocele: the accompanying draught exhibits the same in an aggravated form. The patient possessed but little amative power, and had also a thickened condition of the prepuce, which produced a perfect phymosis. The case, however, under treatment became considerably relieved. The phymosis required a division of the prepuce, an operation productive but of little and momentary pain, or rather twinge, and healed in a few days. Children are sometimes not procreated for want of sufficient erectile and consequently penetrative power of the male organ. Much and often needless misery results from this infirmity.
I have previously described a relaxed state of the testicle known as varicocele; the accompanying illustration shows a more severe case. The patient had very little sexual drive and also a thickened condition of the foreskin, which caused a complete phymosis. However, with treatment, the case improved significantly. The phymosis required a circumcision, which caused only minor and temporary discomfort and healed within a few days. Sometimes, children are not conceived due to insufficient erectile and, therefore, penetrative ability of the male organ. This condition leads to much unnecessary suffering.

The loss of erectile power is occasioned through more causes than one. Erection ensues independently of the will or imagination, as instanced on awaking in the morning—the cause is most probably a distended bladder; the phenomena may be a sympathetic irritability of the muscles of the perinœum, especially the erectores; there is a general pelvic disturbance, the nervous excitement is increased, and the rush of blood (obedient to that excitement) is sent to the penis: such, I believe, is the sympathy between all these structures. The will exercises the same, and the results of the imagination do not materially differ; consequently, where the mind fails in producing these effects, local excitants may be found to supply its office hence the usefulness of art in combating the eccentricities of nature. The mere handling of the testicles kindles desire, and in like manner, stimulatives applied over the scrotum generate amative heat.
The loss of erectile power can happen for several reasons. An erection occurs without the influence of will or imagination, as seen when waking up in the morning—the likely cause is a full bladder; this may lead to a sympathetic reaction in the muscles of the perineum, especially the erectors; there’s a general pelvic disturbance, nervous excitement increases, and blood flow (responsive to that excitement) is directed to the penis: such is the connection between all these structures. The will has a similar influence, and the effects of imagination don’t differ significantly; therefore, when the mind fails to trigger these effects, certain local stimulants can take its place, highlighting the role of medical interventions in addressing the unpredictabilities of nature. Simply touching the testicles can spark desire, and similarly, applying stimulants to the scrotum can generate sexual arousal.
A curve of the penis is sometimes an obstruction to connubial intercourse; this arises from adhesion or obliteration of the cells of the Corpora Cavernosa on one side only,[177] preventing the uniform flow of blood into those structures, and consequently the equal distention of the penis. The curve is of course laterally, and occasions in the act of coition pain to both parties, or the power of penetration is insufficient. Occasionally this malformation is only temporary, and consequently remediable.
A curve in the penis can sometimes interfere with sexual intercourse; this happens when there are adhesions or blockages in the cells of the Corpora Cavernosa on one side only,[177] which stops blood from flowing evenly into those structures, leading to uneven expansion of the penis. The curve is usually to the side, causing pain for both partners during sex, or making penetration difficult. Sometimes this condition is only temporary and can be fixed.
Franck gives an instance in which so considerable a portion of the penis had been carried away by a musket-shot, that when the wound healed, the organ remained curved, and yet proved adequate to the performance of its functions.
Franck gives an example where such a large part of the penis was removed by a musket shot that, when the wound healed, the organ was left curved, yet it was still able to perform its functions adequately.
An opinion formerly prevailed, that the existence of the testes was unnecessary for effective copulation; but that is no longer a point of dispute: their absence, whether natural or artificial, invariably rendering the invalid unfruitful. It is not, however, to be inferred, that a person is impotent in whom no testicles are discovered in the scrotum, instances occurring where they do not descend from the abdomen (their embryotic abode) through the whole period of life. One testicle, provided it be sound, is sufficient for procreation. Complete extirpation of the testes, although destructive of procreative powers, does not extinguish venereal desire. Where the genital organs exist, but are malformed, or pathologically altered, their virility may be nullified.
A past belief was that having testicles wasn't necessary for successful copulation; however, that's no longer debated: their absence, whether due to natural causes or surgical removal, always leaves the individual infertile. It shouldn't be assumed that a person is impotent just because no testicles are found in the scrotum—there are cases where they don't descend from the abdomen (their place in embryo development) throughout a person's life. One healthy testicle is enough for reproduction. Complete removal of the testicles, while it eliminates the ability to procreate, doesn't take away sexual desire. If the genital organs are present but malformed or affected by disease, their ability to function may be compromised.
The most frequent malformation is in the urethra, which sometimes opens in the perinœum—the part marked a in the annexed cut; at others, on the dorsum of the penis, and not unfrequently under its surface: so long, however, as the orifice opens in that portion of the penis which enters the vagina, so that the emissio seminis may be therein deposited, impregnation may and will take place; and even in cases where artificial means have been employed to convey the fluid.
The most common malformation occurs in the urethra, which sometimes opens in the perineum—the area marked a in the attached illustration; at other times, it opens on the top of the penis, and often underneath its surface. However, as long as the opening is located in the part of the penis that enters the vagina, allowing for the emissio seminis to be deposited there, pregnancy can and will occur; this includes situations where artificial methods have been used to deliver the fluid.

A contracted state of the prepuce, its adherence to the glans, or that condition of it termed phymosis, form impediments to the emission of the semen which can only be removed by an operation; and if that be neglected, the evil continues through life.
A tight foreskin, its sticking to the head of the penis, or a condition called phimosis can block the release of semen, which can only be corrected through surgery; if ignored, the problem will persist for life.
Among the diseases which occasion sterility in the male, those affecting the penis and those incident to the testicles[178] may be enumerated. With regard to the former, there often exists an excess or deficiency of muscular or nervous energy, inducing priapism or permanent erection in some instances, or paralysis or permanent flaccidity in others. In priapism, the erection is so vigorous, and all the parts so distended, that the semen can not pass into the urethra; while in paralysis, from some inaptitude of nervous or muscular powers of the genital organs, the corpora cavernosa receive but a limited supply of blood, insufficient to create erection, or provoke a seminal discharge.
Among the diseases that cause male infertility, those affecting the penis and those related to the testicles[178] can be listed. For the penis, there is often either too much or too little muscular or nerve energy, leading to priapism or prolonged erection in some cases, and paralysis or permanent limpness in others. In priapism, the erection is so intense and all the parts so swollen that semen cannot move into the urethra; whereas in paralysis, due to some lack of nerve or muscle function in the genital organs, the corpora cavernosa receive only a limited amount of blood, which is inadequate for achieving an erection or triggering a seminal release.
Strictures of the urethra are among the barriers to sexual intercourse; but happily, only in extreme cases, where the urethra is all but closed, so as to oppose the passing of the finest bougie.
Strictures of the urethra are one of the obstacles to sexual intercourse; however, fortunately, this only occurs in severe cases, where the urethra is nearly closed, making it difficult for even the thinnest bougie to pass through.
The testicle is subject to a variety of diseases, wherein such a relaxation or obliteration of its structure ensues, that the seminal fluid is no longer formed: and where both testicles are alike affected, sexual desire is most usually wholly extinguished—the smallest portion, however, of either gland remaining uninjured, may still be capable of secreting semen sufficient for impregnation.
The testicle can experience various diseases that disrupt its structure, preventing the production of seminal fluid. When both testicles are equally affected, sexual desire is usually completely gone. However, if even a small part of either gland remains unharmed, it may still be able to produce enough semen for impregnation.
Impotence may follow accidents to the testicles, such as produced by a bruise; or even a testicle, which shall have become inflamed from clap, shall become so chronically hardened as to be useless. Bruising the testicles was the mode adopted by the oriental courts for destroying masculine efficiency in the attendants of the harem.
Impotence can occur after injuries to the testicles, like from a bruise; or even if a testicle becomes inflamed due to gonorrhea, it might harden over time and become useless. Bruising the testicles was a method used by eastern courts to eliminate masculine ability in the attendants of the harem.
There are certain conditions of health in which, although the genital organs may be perfect, yet, owing to some constitutional frigidity, there is an incapability of erection. The offspring of too young, or very aged, infirm persons, or of those worn down by debauchery, are but too common instances.
There are certain health conditions where, even though the reproductive organs may be functioning properly, a person might struggle with erectile issues due to some underlying lack of sexual desire. Children born to very young or very old, unhealthy individuals, or those who are exhausted from excessive indulgence, are unfortunately common examples.
The appearance of persons of this temperament is thus described by a French writer: “The hair is white, fair, and thin; no beard, and countenance pale; flesh soft and without hair; voice clear, sharp, and piercing; the eyes sorrowful and dull; the form round, shoulders narrow; perspiration acid; testicle small, withered, pendulous, and soft; the spermatic chords small; the scrotum flaccid; the gland of the testicle insensible; no capillary growth on the pubis; a moral apathy; pusillanimity and fear on the least occasion.”
The appearance of people with this temperament is described by a French writer: “The hair is white, light, and thin; no beard, and the face is pale; skin soft and hairless; voice clear, sharp, and piercing; the eyes are sad and dull; the body is round with narrow shoulders; sweating is acidic; the testicles are small, shriveled, hanging, and soft; the spermatic cords are small; the scrotum is loose; the testicle gland is insensitive; no hair growth in the pubic area; a lack of moral engagement; timidity and fear at the slightest provocation.”
The most frequent cause of impotence, at that period[179] of existence when man should be in the zenith of his procreative power, is in a general weakness of the generative organs, induced by too early an indulgence in coition, the pernicious and demoralizing crime of masturbation, or the abuse of venereal pleasures. In these cases, erection will not take place, or but feebly, although the mind be highly excited by lascivious ideas. The erector muscles are paralysed from over-use, and the semen, if any is secreted, from the lax and withered state of the testes, is clear, serous, without consistence, and consequently deficient of prolific virtue. Sometimes there is a want of consent between the immediate and secondary organs of generation; thus, the penis acts without the testicles, and becomes erected when there is no semen to be evacuated; while the testicles secrete too quickly, and an evacuation takes place without any erection of the penis; the latter disappointment is of extensive prevalence.
The most common cause of impotence at that time[179] in a man's life, when he should be at the peak of his reproductive ability, is a general weakness of the reproductive organs. This weakness can be caused by indulging in sex too early, the harmful and degrading act of masturbation, or the misuse of sexual pleasures. In these situations, an erection either won't happen or will be weak, even if the mind is highly aroused by sexual thoughts. The muscles responsible for erections are weakened from overuse, and any semen produced, if at all, is clear and watery due to the weakened and shriveled state of the testes, lacking the strength to be productive. Sometimes, there is a disconnect between the primary and secondary reproductive organs; for instance, the penis becomes erect without the testicles functioning properly, leading to an erection without any semen being released, while conversely, the testicles may produce semen too quickly, resulting in ejaculation without an erection of the penis. This latter situation is quite common.
Impotence is sometimes occasioned by particular diseases during their continuance, such as nervous and malignant fevers; while, strange to relate, an opposite effect is sometimes produced by other diseases, such as gout and rheumatism, hæmorrhoids, &c.; and instances are on record, that others produce such a change in the constitution, that an impotent man may find himself cured of his impotency on their cessation.
Impotence can sometimes be caused by specific illnesses while they last, like nerve-related and severe fevers. Interestingly, the opposite effect can sometimes occur with other conditions, such as gout, rheumatism, hemorrhoids, etc. There are recorded cases where other diseases create such a change in the body that a man who was impotent may find himself cured once those diseases are gone.
Of all the functions of the animal economy, none are so subservient to nervous influence as those of generation, which, when the organs are perfect, and respond not to the natural application of them, the cause may be classed among those impediments termed moral.
Of all the functions of the animal body, none are as influenced by the nervous system as those of reproduction, which, when the organs are functioning properly and do not respond to their natural use, can be categorized among the obstacles referred to as moral.
As the parts of generation are not necessary for the existence or support of the individual, but have a reference to something else in which the mind has a principal concern; so a complete action in those parts can not take place without a perfect harmony of body and mind, that is, there must be both a power of body and disposition of mind; for the mind is subject to a thousand caprices which affect the action of these parts.
As the components of growth aren't essential for a person's existence or well-being but relate to other things that the mind cares about; a complete action in those areas can't happen without a perfect balance of body and mind. In other words, there needs to be both physical ability and mental attitude because the mind is influenced by countless whims that impact these actions.
As these cases do not arise from real inability, they are to be carefully distinguished from such as do; and, perhaps, the only way to distinguish them, is to examine into the state of mind respecting this act. So trifling often is the circumstance which shall produce this inability depending on the mind, that the very desire to please shall[180] have that effect, as in making the woman the sole object to be gratified.
As these cases don’t come from actual inability, they need to be clearly distinguished from those that do; and maybe the only way to tell them apart is to look at the mindset regarding this action. Often, the trigger for this mental inability can be something very trivial, so much so that the mere desire to please can have that effect, especially when it makes the woman the only one to be satisfied.
SECTION II.
IMPOTENCE AND STERILITY OF THE FEMALE.
IMPOTENCE AND STERILITY OF THE FEMALE.
A female may be impotent, and not sterile; and sterile, but not impotent. Impotence can only exist in the female, when there is an impervious vagina; but even this condition does not necessarily infer sterility, many cases being recorded, where the semen, by some means or another, through an aperture that would not admit a fine probe, has found entrance to the vagina and occasioned impregnation.
A woman may be unable to have an orgasm but still be able to conceive; and she might be infertile, yet still able to experience sexual arousal. A woman can only be incapable of sexual activity if her vagina is blocked; however, this blockage doesn’t always mean she’s infertile. There are many documented cases where sperm has managed to enter the vagina through a tiny opening, even smaller than a fine probe, and has led to conception.
Impotence may arise from a malformed pelvis, the absence of a vagina, adhesion of its labia, unruptured hymen, or one of such strength as to resist intromission. In the two former instances, sterility is irremediable; but art, and indeed nature, may overcome the latter impediments.
Impotence can occur due to a misshapen pelvis, the lack of a vagina, fused labia, an intact hymen, or a hymen that is too strong to allow penetration. In the first two cases, infertility is permanent; however, both medical interventions and natural processes can address the latter issues.
Were these pages intended only for the surgery, instead of the public, the annexed wood cuts would be unnecessary, medical men being conversant with the inconvenience in question; but all the world not being blessed with similar anatomical information, the sketches are presented. The upper one represents the relative situation of the female urethra (1), and the contracted orifice of the hymen (2). In the cases of hardened obstruction, where the hymen assumes an almost cartilaginous texture, the attempts at marital consummation are fruitless, and often give rise to severe local inflammation. The infirmity, on the other hand, is easily and painlessly removable by surgical skill. The lower drawing represents a hymen with two apertures (2), which, if broken down by violence, leaves a troublesome lacerated wound. The surgeon’s assistance is indispensable.
Were these pages meant just for the surgery instead of the general public, the added illustrations wouldn't be necessary, as medical professionals already understand the relevant issues. However, since not everyone has the same anatomical knowledge, the sketches are included. The upper illustration shows the position of the female urethra (1) and the narrowed opening of the hymen (2). In cases of severe obstruction, where the hymen becomes almost cartilaginous, attempts at sexual intercourse can be unsuccessful and often lead to intense local inflammation. Fortunately, this condition can be easily and painlessly treated by a surgeon. The lower drawing depicts a hymen with two openings (2), which, if torn violently, can result in a troublesome lacerated wound that requires the surgeon's help.


Where hermaphroditism exists, the sex is usually more masculine; it is a vulgar error to suppose that the two sexes exist entire, and that they[181] are capable of giving and receiving the offices of married life. The present sketch is merely introduced to show the more frequent malformation. The penis exists, but has no urethra: below is an opening resembling the vagina of the female, which is but of short length, at the bottom of which (in fact, the perineum) the urethra opens. The testicles are entire, and the individual from whom the draft was taken possessed somewhat the desire of the male, without the capability of penetration: the penis, when excited, from its attachment to the lips of the imaginary vagina, and also from its contracted form, presenting merely a kind of bulbous tumor. Even where hermaphroditism more closely partakes of the female, conception never takes place; hence all such parties are sterile.
Where hermaphroditism occurs, the characteristics are typically more masculine. It's a common misconception to think that both sexes exist fully and can participate in the roles of married life. This overview is just to highlight the more common forms of malformation. The penis is present but lacks a urethra; instead, there is an opening that looks like a woman's vagina, which is quite short, and at its base (essentially the perineum) is where the urethra opens. The testicles are intact, and the person from whom this description is derived had some male sexual desire, but without the ability to penetrate. When aroused, the penis, due to its attachment to the lips of the imaginary vagina and its contracted shape, appears more like a bulbous swelling. Even when hermaphroditism leans more towards female characteristics, conception never occurs; therefore, all such individuals are sterile.

Nature, as if to atone for denying to some the delights of maternity, has been occasionally doubly bountiful to others. The annexed drawing exhibits a section of a double uterus. Cases are on record, where both have been impregnated.
Nature, as if to make up for not providing the joys of motherhood to some, has sometimes been especially generous to others. The attached drawing shows a section of a double uterus. There are documented cases where both have been impregnated.

In the instance of a deceased married female, that fell under my observation, the uterus or womb presented the following appearances: The usual cavity was discoverable, but it was filled with a cheesy-like substance, and also there were some ulcered-looking caverns filled with the same material. This female, while living, endured continued pains in the uterine region, was insensible to marital physical enjoyments, sterile, although a wife several years, and the constant sufferer from a vaginal discharge. Her death was consequent upon a severe cold that ended in consumption.
In the case of a deceased married woman that I observed, the uterus showed the following characteristics: The usual cavity was present, but it was filled with a cheesy-like substance, and there were also some ulcerated areas filled with the same material. This woman, while she was alive, experienced ongoing pain in her uterine area, was unable to enjoy physical intimacy, remained infertile despite being a wife for several years, and constantly suffered from vaginal discharge. Her death was the result of a severe cold that led to tuberculosis.

Leucorrhœa is often attended with barrenness; at all events, it is very debilitating, and thus impedes conception. A notion once prevailed, that women who did not menstruate could not conceive; it has since been disproved, except in those instances where menstruation never occurred: a single monthly discharge indicates an aptitude for conception. It is observed that barren women have very small breasts. Women who are very fat are often barren, for their corpulence either exists as a mark of weakness of the system, or it depends upon a want of activity in the ovaria: thus spayed or castrated animals generally become fat. The same remarks apply to the male kind, who are outrageously corpulent. There are many other peculiarities in matrimonial life, fertile subjects for speculation; such as, for instance, the lapse of time that often occurs after marriage before conception takes place, and the space between each act of gestation; the solution of which may be, that these occurrences are modified by certain aptitudes, dispositions, state of health, &c.; the same may explain why persons have lived together for years in unfruitful matrimony, and who yet, after being divorced, and marrying others, have both had children.
Leucorrhea often comes with infertility; in any case, it is very draining and can affect the chance of getting pregnant. There was a belief that women who didn't menstruate couldn't conceive; this has since been proven wrong, except in cases where menstruation never happened: having a single monthly period suggests the ability to conceive. It's noted that infertile women have very small breasts. Women who are very overweight are often infertile, as their excess fat could signal weakness in the body or a lack of activity in the ovaries: similarly, spayed or castrated animals usually become overweight. The same observations apply to overweight men. There are many other unique aspects of married life that invite speculation, like the often long wait after marriage before conception happens and the time between pregnancies; these could be influenced by specific traits, dispositions, health conditions, etc.; this may also explain why some couples have lived together for years without having children but then go on to have kids after getting divorced and marrying someone else.
It is not always that the most healthy women are more favorable to conception than the spare and feeble. High feeding and starvation are alike occasionally inimical to breeding. The regularity of the “courses” appears principally essential to secure impregnation; and the intercourse is generally held likely to be the more fruitful that takes place early after that customary relief.
It isn't always true that the healthiest women are more likely to conceive than those who are thin and weak. Both overeating and starvation can sometimes be detrimental to fertility. The regularity of menstrual cycles seems to be crucial for successful conception; generally, it's believed that intercourse is more likely to result in pregnancy if it happens soon after the end of the menstrual period.
Women in health are capable of bearing children, on an average, for a period of thirty years, from the age of fifteen to forty-five; but their incapacity to procreate does not deny them the sexual gratification, it being well accredited, that women upward of seventy years of age have been known, who have lost but little of the amative inclination and enjoyment which they possessed in their early days. Men certainly possess their procreative power to a longer period, it being common for men to become fathers at eighty, ninety, and one hundred—old Parr becoming a parent at the age of one hundred and thirty. Women rarely fall pregnant beyond fifty.
Women can typically bear children for about thirty years, from the age of fifteen to forty-five. However, even if they can’t conceive, it doesn’t mean they aren’t capable of experiencing sexual pleasure. It’s been well documented that women over seventy have lost little of their desire and enjoyment compared to their younger days. Men, on the other hand, tend to maintain their ability to father children for a longer time; it's not uncommon for men to become fathers at eighty, ninety, or even one hundred—like Old Parr, who became a parent at the age of one hundred and thirty. Women usually do not get pregnant after fifty.
Some females endure intense pain during coition, so as to occasion fainting or great exhaustion. Such suffering is usually traceable to internal ailments—such as piles, fistulous[183] openings between the rectum and vagina, ulcerated wombs, vaginal tumors or abscesses. Cases continually present themselves, where, on the removal of the cause, the effect is cured.
Some women experience intense pain during intercourse, to the point of fainting or severe exhaustion. This suffering is usually linked to internal issues—such as hemorrhoids, fistulous[183] openings between the rectum and vagina, ulcerated uteruses, vaginal tumors or abscesses. There are many cases where, once the cause is addressed, the pain resolves.
The number of children that women have individually given birth to is very variable. It is attested, among a collection of facts of this nature, that one female gave birth to eighteen children at six births; another, forty-four children in all, thirty in the first marriage and fourteen in the second; and in a still more extraordinary case, fifty-three children in all, in one marriage, eighteen times single births, five times twins, four times triplets, once six, and once seven.[14] Men have been known to beget seventy or eighty children in two or more marriages. With regard to the average proportion of male and female births, it appears that the males predominate about four or five only in one hundred. The average number of children in each marriage is, in England, from five to seven.
The number of children that women have individually given birth to can vary widely. It's documented that one woman had eighteen children from six births; another had a total of forty-four children, with thirty from her first marriage and fourteen from her second. In an even more extraordinary case, one woman had fifty-three children in total from one marriage, including eighteen single births, five times twins, four times triplets, once six at once, and once seven.[14] Men have been known to father seventy or eighty children across two or more marriages. As for the average ratio of male to female births, it seems that males outnumber females by about four or five in one hundred. In England, the average number of children per marriage ranges from five to seven.
To a continual irritability of temper among females may be ascribed infertility. Independently of ever fostering domestic disquietude, it produces thinness and feeble health; and, where pregnancy does ensue, it most frequently provokes miscarriages, or leads to the birth of ill-conditioned and puny offspring.
To a constant irritability of mood among women can be attributed infertility. Besides causing ongoing domestic unrest, it results in weight loss and poor health; and when pregnancy does occur, it often leads to miscarriages or the birth of unhealthy and weak children.
Perhaps one of the most indispensable and endearing qualifications of the feminine character is an amiable temper. Cold and callous must be the man who does not prize the meek and gentle spirit of a confiding woman. Her lips may not be sculptured in the line of perfect beauty, her eye may not roll in dazzling splendor, but if the native smile be ever ready to welcome, and the glance fraught with clinging devotion, or shrinking sensibility, she must be prized far above gold or rubies. A few moments of enduring silence would often prevent years of discord and unhappiness; but the keen retort and waspish argument too often break the chain of affection, link by link, and leave the heart with no tie to hold it but a cold and frigid duty.
Perhaps one of the most essential and charming qualities of a woman is her friendly demeanor. A cold and unfeeling man must be one who doesn't value the gentle and trusting nature of a sincere woman. Her lips might not be perfectly shaped, and her eyes may not shine bright, but if her smile is always ready to greet and her gaze is full of devoted affection or sensitive shyness, she should be valued far above gold or rubies. A few moments of quiet reflection could often stop years of conflict and unhappiness; however, sharp replies and biting arguments often break the bonds of love, one link at a time, leaving the heart tied only to a cold and distant obligation.
SECTION III.
TREATMENT OF IMPOTENCE.
IMPotence Treatment.
In venturing upon this part of the subject, it will be as well, first, to distinguish those cases that are curable from those that admit of no relief. Among the latter may be enumerated all those arising from an original or accidental defect in the organs of generation. Where, also, old age is the cause, little is to be done: medicines are of no avail, and temporary stimuli not unfrequently worse.
In discussing this part of the topic, it’s important to first differentiate between cases that can be treated and those that cannot be helped. The latter includes all instances caused by a pre-existing or accidental problem with the reproductive organs. Additionally, when old age is the cause, there’s not much that can be done: medications are ineffective, and temporary stimulants often do more harm than good.
That certain medicaments, aliments, and so forth, do possess an aphrodisiac power, is not to be denied; but when adopted by those weak beings, whose bodies are either worn out by age or excess, and who pin their faith to such restoratives, the little remaining sensibility in their frames, the source of life and energy, can not sustain the shock of reaction; and the result is, total annihilation or death.
It's undeniable that some medications, foods, and similar items have an aphrodisiac effect; however, when taken by individuals whose bodies are either worn out by age or overindulgence, and who rely on these restorative substances, the little sensitivity left in their bodies—the source of life and energy—cannot handle the shock of the reaction, resulting in total destruction or death.
From what has already been stated, it will be perceived, that the mind exercises no inconsiderable influence over the functions of the organs of generation: and as the state of the mind depends upon the particular circumstances under which it may be placed, any attempt to establish a code of instructions, applicable to every instance in which a sportive fancy, or disturbed imagination, constituted the prevailing cause, would be abortive, and might be considered as pandering to a vicious and depraved appetite, whereas the object of this treatise is only to encourage the diffident, to assist the afflicted, and render a service to those legitimately deserving it.
From what has already been mentioned, it's clear that the mind has a significant impact on the functioning of the reproductive organs. Since the state of the mind is influenced by the specific situations it finds itself in, any effort to create a set of instructions that applies to every case where playful thoughts or a disturbed imagination are the main issues would be ineffective and might be seen as catering to a negative and unhealthy desire. The aim of this writing is simply to support those who are unsure of themselves, help those in distress, and provide assistance to those who genuinely deserve it.
As excess in sexual indulgence impairs the generative power, no less injurious may entire abstinence be considered. The due exercise of an organ tends to its perfection, as the neglect or misuse of it, to its impairment. Besides, there is not any wonderful virtue in abstaining from the proper use of the sexes. Why, in the name of morality, were such powerful impulses and desires bestowed upon us? Why were such wonderful organizations[185] given to us, if they were not originally designed to be used by every one who is possessed of them? Society, in its present form, is not perhaps constructed with a philosophical regard to our own natural instincts, and our own original rights.
As overindulgence in sex harms our ability to reproduce, complete abstinence can also be harmful. Proper use of an organ leads to its development, while neglect or misuse leads to its deterioration. Moreover, there's no real virtue in avoiding the appropriate use of our sexual nature. Why, in the name of morality, were we given such strong impulses and desires? Why were we endowed with such marvelous bodies[185] if they weren't meant to be used by everyone who has them? Society, as it exists today, may not be built with a thoughtful consideration of our natural instincts and inherent rights.
Among the causes that induce impuissance, or that distressing condition known under the cognomen of nervous debility, there is not one more reprehensive than the unworthy and pernicious practice of self-abuse. It is much to be regretted, that some medical writer, of talent and estimation in society, has not turned his attention to the subject, and given the influence of his name in denouncing to the world the misery and devastation which are the unerring consequences of this sordid and solitary vice. It is indeed an unpleasant and thankless task; and there probably exists in most minds, an unwillingness to enter upon a subject in which there is so much difficulty in selecting language sufficiently appropriate to exhibit the folly in its true colors, without offending the ears of the chaste and virtuous.
Among the causes that lead to impuissance, or the distressing condition commonly known as nervous debility, there’s nothing more reprehensible than the harmful and shameful practice of self-abuse. It’s unfortunate that no talented and respected medical writer has focused on this issue and used their influence to expose the misery and devastation that are the unavoidable results of this sordid and solitary habit. Indeed, it’s an unpleasant and thankless task, and most people likely hesitate to discuss a topic that’s so challenging to express in a way that accurately portrays the foolishness without offending the ears of those who are virtuous and modest.
But a question of such paramount importance should not be sacrificed to any false and prudish notions of delicacy; I shall therefore offer such observations, as I may think calculated to check the progress of a vice, that has done more to demoralize the human mind than the whole catalogue of existing causes besides. It may be deemed an exaggeration, when it is stated that full three fourths of the insane owe their malady to the effects of masturbation: but the assertion is corroborated by one of the first writers on medical jurisprudence, and is fully borne out by the daily experience of proprietors of lunatic asylums. The practice of self-abuse usually has its origin in boarding-schools, and other places where young persons congregate in numbers; and there are few of us who may have observed the vice practised, although it may be unpleasant to avow as much, that could resist the contamination.
But a question this important shouldn’t be sacrificed to any false and overly modest ideas of delicacy. I will therefore share my observations that I believe could help slow the spread of a vice that has done more to corrupt the human mind than all other existing causes combined. It might seem like an exaggeration to say that three-quarters of those who are insane owe their condition to the effects of masturbation, but this claim is supported by one of the leading writers on medical law and is confirmed by the daily experiences of owners of mental health facilities. The habit of self-abuse often starts in boarding schools and other places where young people gather in large groups; and there are few of us who may have noticed the practice of this vice, even though it might be uncomfortable to admit, that could resist its influence.
And thus it is, though ninety-and-nine be pure and spotless as the driven snow, if the hundredth be immoral, the poison is soon disseminated, and the whole flock become initiated into a vice, which, if indulged in, will blast their[186] intellectual faculties, and probably consign them as outcasts of society; rendering them slavering idiots, or the inmates of a lunatic asylum. It is not only in private schools that this sin rages, our public foundations and colleges are not exempt from it. The heads of our universities are particularly scrupulous in driving from their neighborhood the frail fair, lest they should contaminate the votaries of learning; while a vice far more degrading in its practice, and infinitely more baneful in its effects, rages within the very sanctuaries of classic lore. Many a brilliant genius has sunk into fatuity beneath its degrading influence. Loss of memory, idiocy, blindness,[15] total impotence, nervous debility, paralysis, strangury, &c., are among the unerring consequences of an indulgence in this criminal passion. I need not bring a greater proof of the dire effects of an indulgence in the practice of masturbation, than the deplorable state of mind to which it reduced one of our greatest poets.
And so it is, that although ninety-nine may be pure and innocent like fresh snow, if the hundredth is immoral, the toxicity quickly spreads, and the whole group gets caught up in a vice that, if indulged, will ruin their thinking abilities and likely cast them out of society; turning them into drooling idiots or patients in a mental asylum. This isn’t just a problem in private schools; our public institutions and colleges are not immune to it either. The leaders of our universities are particularly careful to keep vulnerable individuals away, fearing they might corrupt the students; yet a vice that is much more degrading and far more harmful rages within the very halls of classical education. Many brilliant minds have fallen into foolishness because of its degrading influence. Memory loss, idiocy, blindness, total impotence, nervous weakness, paralysis, painful urination, etc., are among the certain consequences of indulging in this harmful desire. I need not present a stronger example of the terrible effects of engaging in masturbation than the sad state of mind it brought upon one of our greatest poets.
The treatment of this delusive and mentally annihilating propensity, falls equally within the province of the philosopher and the physician. Without a total abandonment of the practice, the case is hopeless; and he to whom the consequences shall have been portrayed and heeds them not, is unworthy of our sympathy, but deserves the evils he entails upon himself.
The way to deal with this misleading and mentally devastating tendency involves both the philosopher and the doctor. Without completely giving up the behavior, the situation is hopeless; and anyone who has been shown the consequences and still ignores them is not deserving of our sympathy and deserves the negative outcomes they bring upon themselves.
Now, as the consequences of all criminalities continue to ensue so long as the provocative be kept up, it is very evident that, as a first step toward the restoration of order and health, the cause must be removed or withheld. The mere will or resolution is seldom sufficient: virtue, like vice, has its allurements, and those belonging to the former must be called into requisition as antagonists to the snares of the latter. Physic can not check bad principles, or bad indulgences. No method is or can be superior to that full employment of the mental faculties on noble and intellectual subjects, on objects worthy the high ends for[187] which Nature has adapted them. And though the difficulty will be great in inducing new and good habits, to the exclusion of such as are unworthy and degrading, yet the effectual accomplishment of such a resolution is not of uncommon occurrence; and the sufferer may be placed under circumstances where good habits may be more frequently called into action naturally, to the exclusion of vicious propensities. The time should be well filled, so as to leave no room for flying to the various usual sources of amusement that fill up the life of the thoughtless and gay. Every hour and every minute should be provided for, so as to exclude the admission of idleness and sloth, the forerunners of mental and bodily disease. Studies connected with education should be encouraged. Modern languages have a great claim on the consideration of all who are engaged in business to any extent, and are of incalculable use after they have fulfilled the immediate end for which their culture is here recommended. The various sciences bearing more or less on the pursuits and employments of every man, are earnestly recommended to the choice of the unfortunate victim of sensuality. Geology and botany would call him into the healthful fields, or fill up his time by his fireside, in studying the many excellent works on those subjects: the still higher utility of chemistry, as being made of practical use in almost every business, and demonstrating the else unintelligible phenomena of a multitude of natural processes and changes, may be held up as another inducement to call forth his best energies.
Now, as the consequences of criminal behavior continue as long as the provocations persist, it's clear that the first step toward restoring order and well-being is to remove or control the cause. Just wanting to change is rarely enough; virtue, like vice, has its temptations, and we need to actively engage with the virtues to counteract the traps set by vices. Simple remedies can't fix bad principles or unhealthy indulgences. There is no better method than fully engaging our minds with noble and intellectual topics that are worthy of the high purposes for which we are inherently designed. While it may be challenging to develop new, good habits and replace unworthy and degrading ones, successfully doing so is not uncommon. The individual may find themselves in situations where positive habits can more naturally take precedence over harmful tendencies. Every moment should be occupied to prevent drifting into the usual distractions that occupy the lives of the carefree and thoughtless. Every hour and minute should be scheduled to eliminate the space for idleness and laziness, which lead to both mental and physical illness. Educational studies should be encouraged. Modern languages are especially important for anyone involved in business and are incredibly useful even after achieving the immediate goals of their study. Various sciences that relate to everyone's pursuits and occupations are strongly recommended to those struggling with indulgence. Geology and botany can lead one into healthy outdoor activities or provide engaging study materials at home. The practical usefulness of chemistry in almost every field and its ability to explain the otherwise confusing phenomena of many natural processes and changes should also inspire one to tap into their best potential.
Travelling, to those who can afford the expense or the time, is one of the best means of conquering this baneful habit. The numerous objects thereby presented to the eye of the invalid in the manners, government, and productions of art and nature, of the countries he visits, are an incessant source of pleasing and useful excitement, and can not fail, especially if the traveller be accompanied by an intelligent and moral friend, to weaken and eradicate the bad impressions of the past.
Traveling, for those who can afford it, is one of the best ways to overcome this harmful habit. The many sights that an unwell person sees in the customs, governance, and creations of art and nature in the places they visit provide a constant source of enjoyment and valuable stimulation. This experience cannot help but, especially if the traveler is with a thoughtful and ethical friend, diminish and eliminate negative impressions from the past.
To diverge, and at the same time to conclude this part of the subject, I have only to offer a few remarks relative to the medical and therapeutic treatment of those cases of impuissance, that age, disorganization, and total incapacity, do not exclude from consideration. I have already expressed my belief that generative imbecility is consecutive[188] to general debility; hence, whatever tends to improve the latter, tends also to remove the former. The diet, therefore, should be full and generous, with a liberal proportion of spices; but all stimulating liquids, such as wine, brandy, and the rest, should be avoided.
To shift gears and wrap up this section, I just want to share a few thoughts about the medical and therapeutic treatment of cases of impotence that age, disorganization, and total incapacity don’t rule out. I've already mentioned that I believe generative weakness follows from overall debility; therefore, anything that helps improve the latter will also help eliminate the former. The diet should be rich and generous, with a good amount of spices; however, all stimulating drinks like wine, brandy, and the like should be avoided.
Bathing, in its various forms, constitutes no unimportant feature in the treatment; the cold plunging, the tepid shower, the douche, the warm and the vapor baths, possess their several influences. The various medicines that come under the denomination of aphrodisiacs, are not wholly uninfluential, such as stomachics, aromatics, gums and balsams, oils, musk, opium, cantharides, strychnine, and others; but as their administration can only be permitted under professional direction, no real utility can follow any specification or formulary of their proportions.
Bathing, in its many forms, plays an important role in treatment; cold plunges, tepid showers, douches, warm baths, and steam baths all have their unique effects. Various medications classified as aphrodisiacs can also have an impact, including stomachics, aromatics, gums and balsams, oils, musk, opium, cantharides, strychnine, and others. However, since these should only be taken under professional supervision, providing a specific list or formula for their dosages wouldn't be helpful.
OTHER FORMS OF SEXUAL DEBILITY.
Involuntary seminal emissions are oftentimes very serious, distressing, and intractable. They may be produced in two ways—from continence, or by a high degree of morbid irritability or weakness. The latter is by far the more frequent; for the treatment of the former is obvious, and generally effectual. The difference between seminal discharges in persons of full health, and those morbidly weak, is very opposite: in the former it is consequent upon an erection, followed by an act of coitus; while in the latter both are absent. The general debility in the generative system, inseparable from morbid irritability, occasions both a failure in the erection of the penis, and an inability to retain the fluid in the secreting organs. There is no doubt that this disposition to seminal emissions, conjoined as it generally is with more or less deficiency of the vis virilis, is too often owing to the habit of self-abuse in early age. The testes usually wither in these cases, and the patient becomes nearly, if not entirely, impuissant. Sometimes these cases are attended by an excessive irritability of the bladder, accompanied by pains in the loins, kidneys, &c. Their treatment consists in taking nutritious and digestible food, to impart strength and invigorate the constitution. Stimulants are at the same time to be carefully avoided, except where great languor and lassitude prevail. Abstemiousness in liquids is to be[189] enjoined. Habits of a relaxing nature should be avoided; the patient, instead of sleeping on a soft, downy bed, should lie on a firm mattress; the air of the room should be preserved at a moderate temperature, and but few hours should be allotted to sleep; he should pass much of his time in the open air in a cool atmosphere; taking frequent and moderate exercise, so that it does not occasion fatigue. Cold bathing is a very important and essential part of the treatment to be observed; the daily use of the bidet, or the frequent application of a towel, dipped in cold water, to the testes, applied twice or thrice a day, or the douche bath, will be found of much service. To prescribe formulæ for the various temperaments subject to this affection would be to transcribe all the tonics from the pharmacopœia: they are severally useful, but the various preparations of iron surpass all others. During this treatment the state of the mind should not be neglected: no lascivious idea should be for a moment encouraged, nor should the imagination be permitted to wander over the works of fiction or romance in any way connected with matters of love.
Unintentional seminal emissions can be quite serious, distressing, and difficult to manage. They can occur in two ways—due to lack of control or from a high level of abnormal irritability or weakness. The latter is by far the more common cause; the treatment for the former is clear and usually effective. The difference between seminal discharges in healthy individuals and those who are weak is significant: in healthy people, it follows an erection and sexual intercourse, while in weaker individuals, both are absent. General weakness in the reproductive system, which comes with abnormal irritability, leads to both a failure to achieve an erection and an inability to retain the fluid in the glands. It’s clear that this tendency for seminal emissions, often associated with some level of deficiency in the vis virilis, is frequently the result of self-abuse during early years. In these cases, the testes typically shrink, and the individual becomes nearly, if not completely, impotent. Sometimes, these cases are also accompanied by excessive irritability of the bladder, along with pain in the lower back, kidneys, etc. Treatment includes consuming nutritious and easily digestible foods to boost strength and overall health. Stimulants should generally be avoided, except in cases of severe weakness and fatigue. Limiting liquid intake is recommended. Relaxing habits should be avoided; instead of sleeping on a soft, plush bed, the patient should lie on a firm mattress. The room should be kept at a moderate temperature, and sleep hours should be kept to a minimum; the patient should spend a lot of time outdoors in a cool atmosphere, engaging in moderate exercise that doesn’t lead to fatigue. Cold bathing is a crucial and essential part of the treatment plan; daily use of the bidet, or frequent applications of a cold, wet towel to the testes two or three times a day, or using a douche bath, can be very helpful. Writing out specific formulas for the various temperaments affected by this condition would mean listing all the tonics from the pharmacopoeia: each one is somewhat effective, but various preparations of iron are the most beneficial. During this treatment, the state of the mind should not be overlooked: no lascivious thoughts should be entertained, nor should the imagination be allowed to wander through works of fiction or romance related to love.
It not unfrequently happens that patients affected with these complaints are apt to despond, and become miserably depressed in spirits; to remove which, every recreation should be encouraged to prevent them pondering over their own situation, and, if possible, to divert the mind from gloomy ideas: lively and agreeable company should be courted; theatres, concerts, or any other rational amusement consonant with the principles of the patient, should be visited or pursued, and by an uninterrupted perseverance in this mode of treatment for a sufficient length of time, I have seen the most beneficial results arise. The great art and difficulty in treating these cases consist in giving tonics to a certain extent and no further—avoiding excess, whereby we stimulate and produce fever; or depletion, and induce debility. Early hours, fresh air, exercise, attention to diet, the shower bath, topical application of cold, with properly regulated sexual intercourse, are rarely ineffectual in curing the disease.
It often happens that patients with these issues tend to feel hopeless and become deeply depressed. To help lift their spirits, it's important to encourage all kinds of activities to distract them from overthinking their situation and, if possible, to take their minds off gloomy thoughts. They should seek out lively and pleasant company; attend theaters, concerts, or any other reasonable forms of entertainment that align with their values. By sticking to this approach for a considerable time, I've witnessed significant improvements. The key challenge in treating these cases is finding the right balance with tonics—administering them to a certain extent without going overboard. Excess can lead to stimulation and fever, while too little can cause weakness. Keeping a routine with early mornings, fresh air, exercise, careful diet, shower baths, cold applications, and appropriately managed sexual activity is usually effective in treating the condition.
I could narrate many instances wherein the sexual desire declined on the intervention of ordinary illness; any powerful mental solicitude will suffice, but such a cause[190] is commonly remediable. Where the cause is traceable to excesses and pernicious indulgences, if not accompanied by disorganization, hope should not be abandoned; but the patient should not cling to, or hang his reliance upon, hole-and-corner speculators, or their advertised specifics. He should consult men legitimately engaged in the profession, in which, perhaps, more talent and honor are concentrated, than in any other department of science.
I could share many examples where sexual desire decreases due to common illnesses; any strong mental worry can cause this, but such issues are usually fixable. If the cause relates to excesses and harmful indulgences, and there’s no serious damage, there’s still hope. However, the patient shouldn’t rely on shady speculators or their marketed cures. They should consult professionals who are genuinely committed to their field, where perhaps more skill and integrity are found than in any other area of science.
As this disease is generally considered to be of a delicate nature, and one about which the afflicted are unwilling to speak, we shall say a few words on them. Piles constitute a disease that may be very slow or very rapid in its progress. The patient complains of an occasional itching or soreness at the rectum after an evacuation, more particularly if subject to constipation, or if he be an irregular liver: when, after a while, he will be surprised on discovering, subsequent to some straining effort, a knot of elastic but irregularly formed tumors, of a size varying from a hazel-nut to a horse-bean, springing out apparently from the rectum, that in a few days, if they continue, will become sore, and probably be attended with a discharge of blood.
Since this condition is generally seen as sensitive and something people prefer not to discuss, we’ll share a few thoughts on it. Hemorrhoids are a condition that can progress slowly or quickly. The person affected might experience occasional itching or discomfort in the rectal area after a bowel movement, especially if they tend to be constipated or have irregular liver function. After some time, they may be startled to find, following a bout of straining, a lump of elastic, irregularly shaped growths, ranging in size from a hazelnut to a horse bean, emerging from the rectum. If these persist for a few days, they can become painful and may likely lead to bleeding.
|
1. Rectum. Rectum.
2. Hœmorrhoids. 2. Hemorrhoids.
3. Perineum. Perineum. |

|
Another patient will experience similar symptoms, as regards the pain, swelling, and discharge of blood, except that they will be increased in severity, and be more transitory in their appearance and stay. Upon examination, a perceptible difference will be discovered. In the former instance the tumors will be seen to proceed from the outer edge of the rectum, and will be found to be covered with[192] the common skin. Professional men designate this form of the disease “External Piles.”
Another patient will have similar symptoms, including pain, swelling, and blood discharge, but these will be more intense and appear and disappear more quickly. Upon examination, a noticeable difference will be found. In the previous case, the tumors will be seen to come from the outer edge of the rectum and will be covered with[192] regular skin. Medical professionals refer to this type of condition as “External Piles.”

|
1. Inner part of Rectum. Rectal interior.
2. Orifice of Rectum. Rectal opening.
3. External Piles. 3. External Collections.
4. Internal Piles. 4. Internal Hemorrhoids. |
In the latter, the tumors are, as it were, squeezed out of the rectum, and swell in a very short space of time to an enormous size. They are of a much more vivid blood-red color, and will be found to be covered only by the lining membrane of the lower gut. These are called “Internal Piles.”
In the latter case, the tumors are essentially pushed out of the rectum, and within a very short time, they grow to an enormous size. They have a much brighter blood-red color, and will be found to be covered only by the lining membrane of the lower intestine. These are referred to as “Internal Piles.”

|
1. Inner part of Rectum. Inner part of the rectum.
2. Orifice of Rectum. Rectal opening.
3. Internal Piles. Hemorrhoids. |
Now piles are nothing more nor less than dilated veins, like varicose veins in the leg or any other part. The office of veins is to receive the surplus blood of the arteries, after having parted with that necessary supply for the nourishment of every structure they are severally distributed to, and to convey it back to the circulating organ, the heart—and the mesenteric hœmorrhoidal veins, from their dependant and confined position, the circulation in and above them being liable to so many interruptions from the frequent hardened state of the fæces in the rectum, become distended with blood, which acting really like a wedge, dilates them in time to the size we meet them. On the removal of the cause, the blood flows on, and the swelling subsides, and the patient feels no further inconvenience until a recurrence of the pressure. After repeated attacks, the veins become inflamed, and lymph, a sort of defensive[193] mucus, is “thrown out” on the cellular membrane covering the veins, and becomes organized into an indurated texture, which increases with each attack of inflammation, and at last gives them that fleshy appearance which resembles a specific growth (see annexed cut).
Now, piles are just enlarged veins, similar to varicose veins in the leg or anywhere else. The role of veins is to collect the excess blood from the arteries after they have supplied necessary nutrients to the tissues they serve, and to transport it back to the heart. The mesenteric hemorrhoidal veins, due to their dependent and restricted location, are easily affected by frequent hard stools in the rectum, causing them to become swollen with blood, which acts like a wedge and gradually expands them to the size we see. Once the cause is removed, blood circulation resumes, and the swelling goes down, allowing the patient to feel fine until the pressure happens again. After several episodes, the veins can become inflamed, and lymph— a type of protective mucus— is “released” onto the surrounding tissue covering the veins, which becomes organized into a hardened texture that grows with each inflammation episode, eventually giving them a fleshy look that resembles a specific growth (see attached illustration).

The distinction between External and Internal Piles is as follows: In both instances the same veins are diseased. In external piles, the lowermost portion of the hœmorrhoidal veins are dilated, and are thrust by the outer side of the rectum, carrying before them the common skin, which dilates and constitutes the external coat of the piles. The rectum is a portion of gut of four or five inches in length, and of nearly a uniform width; the lower end, constituting the orifice, is, as it were, tied round with a contracting and yielding band of muscular fibres, forming a muscle called the Sphincter Ani. It is a muscle of great power, and, from its connexion with the neighboring muscles of similar strength, helps to afford that support to the contents of the pelvis, that otherwise would descend, and be always forming a projecting tumor. External piles consist, then, of a protrusion of the hœmorrhoidal vein or veins between the cellular union of the sphincter with other muscles, constituting, in fact, a hernia or rupture in the perinœum. Internal piles is that condition of the hœmorrhoidal veins, where, from their dilatation, they become protruded with the fæces, when, from the contraction of the sphincter acting like a ligature, they can not regain their situation until emptied of their contents. Inflammation soon ensues, and the various changes I have and shall hereafter consider take place.
The difference between External and Internal Piles is as follows: In both cases, the same veins are affected. In external piles, the lower part of the hemorrhoidal veins becomes swollen and pushes through the outer side of the rectum, carrying the surrounding skin with it, which stretches and forms the outer layer of the piles. The rectum is a section of the intestines that is about four to five inches long and nearly uniform in width; the lower end, which is the opening, is somewhat constricted by a flexible band of muscle fibers called the Sphincter Ani. This muscle is very strong and, along with nearby muscles of similar strength, helps support the contents of the pelvis to prevent them from descending and forming a protruding tumor. External piles are essentially a bulging of the hemorrhoidal vein or veins through the connective tissue where the sphincter joins other muscles, effectively creating a hernia or rupture in the perineum. Internal piles occur when the hemorrhoidal veins dilate and protrude along with the feces; when the sphincter tightens around them like a ligature, they can’t return to their original position until they've been emptied. Inflammation quickly follows, leading to various changes that I have discussed and will continue to discuss.
Having stated the cause of piles, namely, pressure on, and thereby prevention of, the circulation of the blood through the hœmorrhoidal veins, it follows that persons mostly annoyed with constipation must be the most likely to be afflicted with piles; hence, free and intemperate livers, great wine-bibbers, feeble and relaxed constitutions, those, again, who take little exercise, and pregnant women, and women who have borne many children, seldom escape them. It is rarely that piles attack people in the[194] lower class of life, and those who have to work hard for their livelihood and are much in the open air, which accounts for the prevalence of this disease in the upper ranks of society. The treatment of piles is very simple, if proceeded with at the commencement of the complaint, the grand object being to prevent constipation. An excellent adjunct to the cure of incipient piles, is the warm bath. Its tendency to overcome local congestions, and thereby equalize the circulation of the blood, is well known. The best medicine a hœmorrhoidal patient can take is Turkey rhubarb, to be chewed freely, or castor oil, in doses of one or two teaspoonfuls every morning, or some mild electuary, which should be continued until the piles subside.
Having explained the cause of hemorrhoids, which is pressure that prevents proper blood circulation through the hemorrhoidal veins, it follows that individuals who often struggle with constipation are the most likely to suffer from hemorrhoids. Therefore, those who indulge excessively, heavy drinkers, people with weak and relaxed bodies, those who exercise little, pregnant women, and women who have had multiple children often experience this issue. It's rare for hemorrhoids to affect people in the lower socioeconomic classes or those who work hard outdoors, which explains why this condition is more common among the wealthy. Treating hemorrhoids is quite straightforward if started early, with the main goal being to prevent constipation. A great complement to the treatment of early hemorrhoids is a warm bath, as it helps relieve local congestion and balance blood circulation. The best medicine for someone with hemorrhoids is chewing Turkey rhubarb thoroughly, taking castor oil in doses of one or two teaspoons each morning, or some mild medicinal concoction, which should be taken until the hemorrhoids go away.
The diet during this treatment should be temperate and laxative. Fruits should be used freely, and also coarse bread, rye and Indian mush and molasses; wine and exhilarating stimulants being avoided, and, where admissible, as much out-door exercise taken as possible. An excellent plan is also to inject half a pint or more of cold pump or spring water up the rectum every morning, and suffer it to remain for twenty or thirty minutes, if possible. Where the piles have been of several days’ continuance, and are very much swollen, puncturing them with a needle, and so relieving the tension by evacuating, or at least diminishing their contents, that the obstruction shall be overcome, is serviceable. After this, pledgets of lint dipped in cold water, the patient preserving the horizontal posture, may be applied, or an astringent lotion may be used.
The diet during this treatment should be moderate and laxative. Fruits should be consumed freely, along with whole grain bread, rye, Indian corn mush, and molasses; avoid wine and stimulating drinks, and get as much outdoor exercise as possible. A great idea is to inject half a pint or more of cold pump or spring water into the rectum every morning and let it sit for twenty or thirty minutes, if you can. If the hemorrhoids have lasted several days and are very swollen, puncturing them with a needle to relieve the pressure by releasing, or at least reducing, their contents can be helpful. After that, apply cold water-soaked gauze while keeping the patient lying down, or use an astringent lotion.
Where there is much swelling and inflammation, leeches applied to the neighboring parts will afford relief. It is impolitic, although some surgeons recommend it, to apply leeches on the tumor, as the bites are oftentimes very difficult to heal. Where the piles will admit of it, attempts should be made to empty them, and press them to their places, after which a pad may be worn to prevent their descent. In the commencement of the disease, where there is much heat and itching, a mild and astringent ointment will prove of considerable utility, and a wash of powdered opium, dissolved in flaxseed tea, will relieve pain and soreness.
Where there is a lot of swelling and inflammation, using leeches on the surrounding areas can provide relief. It’s not a good idea, even though some surgeons suggest it, to apply leeches directly on the tumor, as the bites can be very hard to heal. If possible, attempts should be made to drain the piles and push them back into place, after which a pad can be worn to keep them from coming back down. In the early stages of the condition, when there's a lot of heat and itching, a mild and astringent ointment can be very helpful, and a wash made from powdered opium dissolved in flaxseed tea will help relieve pain and soreness.
A very excellent and practical method in the treatment of piles (the internal I am now speaking of) is to deposite a pear-shaped bougie or pessary in the rectum, and suffer it to remain as long as possible. The wearing of bougies[195] gives no pain or even uneasiness, and the patient may pursue his or her ordinary occupation without hinderance: the bougie should be worn from one to several weeks. It affords constant pressure against and support to the dilated veins, and enables them to regain their tone and strength; and I have known numerous instances where a lasting cure has been effected. One of the most alarming consequences of piles is hœmorrhage or bleeding; and it is really wonderful what an extensive loss of that fluid a patient can sustain. Day after day, and week after week, have I known instances of constant bleeding from internal piles, by which the constitution of the patient has been almost broken up. This symptom mostly prevails with females, nor is it limited, although more prevalent, to those who are pregnant. There is naturally a strong objection on the part of a delicate and susceptible female to submit to a professional examination, and consequently it is rarely done, until the urgent necessity of the case, lest death should ensue, induces the patient to consult her medical adviser, that he becomes acquainted with the real nature of the case. Where there is ulceration of the piles, and they are very numerous, and the bleeding frequent and profuse, the only effectual cure is their removal. Where the operation is objected to, the next method is to employ astringent enemata, which must be regulated by the medical attendant.
A very effective and practical method for treating piles (specifically internal ones) is to place a pear-shaped bougie or pessary in the rectum and let it stay in as long as possible. Wearing bougies[195] causes no pain or discomfort, allowing the patient to continue with their daily activities without interruption: the bougie should be worn for anywhere from one to several weeks. It provides constant pressure and support to the swollen veins, helping them regain their tone and strength; I have seen many cases where this has resulted in a lasting cure. One of the most concerning consequences of piles is hemorrhaging or bleeding, and it's truly surprising how much blood a patient can lose. Day after day, and week after week, I have witnessed cases of continuous bleeding from internal piles, which has nearly drained the patient's constitution. This symptom is most common among women, although it is not exclusively found in those who are pregnant. Naturally, there is a significant reluctance among delicate and sensitive women to undergo a professional examination, so it is rarely performed until the urgency of the situation forces the patient to consult a doctor, allowing them to understand the true nature of the condition. When there is ulceration of the piles, and they are numerous with frequent and heavy bleeding, the only effective cure is to remove them. If the operation is declined, the next option is to use astringent enemas, which should be managed by the medical professional.
The celebrated Weir’s balsam (248½ Grand Street) has the credit of effecting miraculous cures. It is a medicine of deserved repute, and ranks high with professional men. Pitch pills have been extolled.
The famous Weir’s balsam (248½ Grand Street) is known for bringing about miraculous cures. It has a well-earned reputation as a medicine and is highly regarded by professionals. Pitch pills have been praised.
Now, where piles, both external and internal, do not yield to the means suggested, or the patient may not think proper to avail himself of them, the next best step is their removal; and this is done either by excision or by ligature. Both processes are safe in the hands of a medical man, and are neither attended with any pain nor suffering worth notice.
Now, if hemorrhoids, both external and internal, don’t respond to the suggested treatments, or if the patient prefers not to use them, the next best option is to remove them. This can be done either by cutting them out or by tying them off. Both methods are safe when performed by a medical professional and don't cause any significant pain or discomfort.
Among the annoyances incident to the rectum, is an occasional preternatural contraction of the sphincter muscle. It is generally the consequence of local irritation set up by purgatives, by which the orifice becomes sore and excoriated, which, if not timely relieved, ulcerates, constituting cracks also, and in process of time a portion sloughs away, and the adjacent edges unite, and thereby diminish the calibre of the opening. This disease may be congenital,[196] that is, the individual may be born with a contracted or narrow sphincter. The treatment, naturally enough, is to dilate the orifice, which is to be attempted by the introduction of bougies, after the mode advised for the cure of stricture, of which this in reality is a form. The cracks of the sphincter are occasionally obstinate to heal; and the ulceration will spread within the rectum. When that is the case, the application of any stimulative ointment will promote a healthy action.
One of the issues related to the rectum is an occasional abnormal tightening of the sphincter muscle. This usually happens due to local irritation caused by laxatives, which can make the opening sore and raw. If not treated promptly, it can lead to ulceration, resulting in cracks, and over time, a part may slough off, causing the nearby edges to come together and reduce the size of the opening. This condition may be congenital, meaning a person might be born with a contracted or narrow sphincter. The obvious treatment is to enlarge the opening, which can be done by inserting bougies, following the method recommended for treating strictures, of which this is essentially a form. The cracks in the sphincter can sometimes be tough to heal, and the ulceration can spread inside the rectum. When that happens, applying any stimulating ointment can help encourage healthy healing.
In inveterate cases division of the sphincter is necessary, which is to be done with a scalpel, and the incision should be made from within laterally, by which injury to the perineum is avoided. The operation is very simple, and by no means painful or dangerous: the cure is perfect. Appropriate medical treatment must not be neglected.
In severe cases, cutting the sphincter is necessary. This should be done with a scalpel, making the incision from the inside toward the side to avoid injuring the perineum. The procedure is very straightforward and isn’t painful or risky: the recovery is complete. It's important not to overlook the right medical treatment.
PROLAPSUS OF THE RECTUM.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
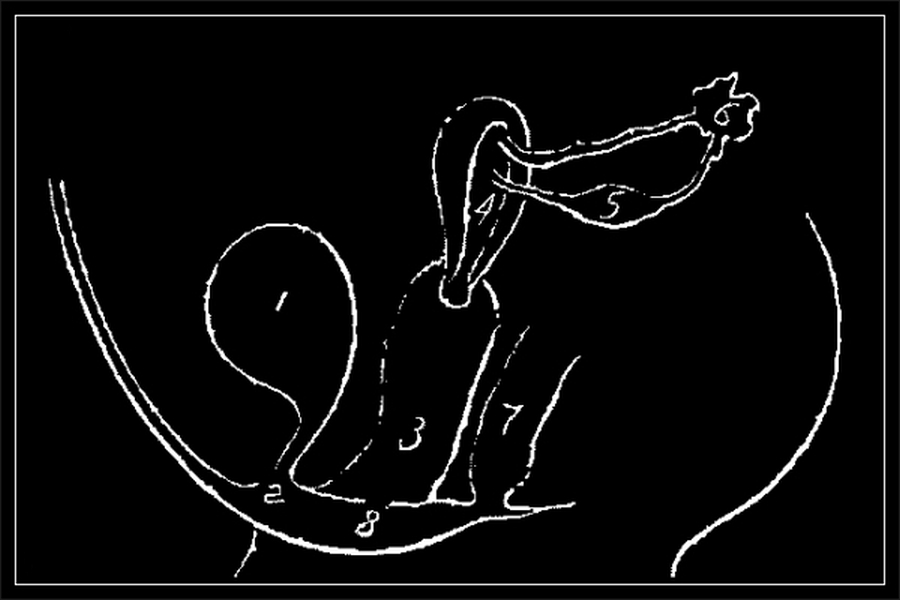{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This disease is often confounded with piles; and as patients are generally diffident in submitting to an examination, any extraordinary protrusion of piles they denominate a falling of the gut. Prolapsus Ani is distinguished from piles by the muscular coats of the intestine descending with the mucous membrane, and forming a bag, like a pendulum, to the length of many inches; the rectum, in fact, becomes everted, as we see the finger part of gloves when turned inside out; and the inner membrane being highly vascular, and the vessels in a congested state, it assumes a blood-red appearance. The case is here well portrayed. Of course the disease occasions much inconvenience and if not abated by appropriate treatment, serious consequences ensue. Piles are most commonly the cause of prolapsus, when, from the frequent and hard straining, the gut at last descends, bringing the piles with it, which will be seen winding around the upper part. When that is the case, the best treatment is first to apply a ligature round the hœmorrhoids, and then return them [197] and the rectum together. Where the gut protrudes from relaxation of the sphincter, the treatment depends upon local support, for which there are many contrivances.[16] Astringent injections should also be used to give tone to the parts, and medicines given to render the alvine evacuations less hurtful. Children are very liable to prolapsus, but with them a return of the fallen gut, and a brisk purgative is all that is needed to prevent a repetition, provided proper attention be paid to the bowels afterward—a disturbance of the latter being, in most instances, the cause. Where a rectum has been for a long time the seat of disease, excrescences are apt to arise, resembling warts: they may be removed without much pain, and with perfect safety.
This disease is often confused with hemorrhoids; and since patients are usually hesitant to undergo an examination, any unusual protrusion of hemorrhoids is referred to as a falling of the gut. Prolapsus Ani is differentiated from hemorrhoids by the intestinal muscle layers descending along with the mucous membrane, creating a bag, similar to a pendulum, extending several inches; the rectum actually turns inside out, much like how the finger part of gloves looks when turned inside out; and the inner membrane, being highly vascular and congested, takes on a bright red color. This condition is well depicted here. Naturally, the disease causes significant discomfort, and if not treated appropriately, serious complications can arise. Hemorrhoids are most commonly the factor leading to prolapse, as repeated and hard straining eventually causes the gut to descend, taking the hemorrhoids with it, which will be seen wrapping around the upper part. In such cases, the best approach is to first place a ligature around the hemorrhoids, then return both them and the rectum together. When the gut protrudes due to relaxation of the sphincter, the treatment focuses on providing local support, for which there are numerous devices available.[16] Astringent injections should also be applied to provide tone to the affected areas, and medications should be given to make bowel movements less painful. Children are particularly prone to prolapse, but for them, simply returning the fallen gut and administering a strong laxative will generally suffice to prevent recurrence, as long as proper attention is given to the bowels afterward—a disturbance in this area is usually the cause. When a rectum has been the site of disease for an extended period, growths resembling warts can develop: they can be removed with minimal pain and complete safety.
STRICTURE OF THE RECTUM.
The rectum, it is presumed, is known to be the lower portion of the intestines that leads to the outlet called, in domestic language, the fundament. Now some writers assert that the rectum answers the same purpose to the bowels generally, as the urethra does to the bladder, while others contend that it is a receptacle for the fæces previous to their expulsion. We are all sensible, I think, that it must answer both purposes; but it is also evident that it is employed more for the former than the latter purpose. The moment the rectum is full, there is a desire to empty it, which is the best proof of its office; but circumstances oftentimes forbid us, for even hours, obeying the summons, which establishes its capability as a recipient. Well, the rectum, consisting of muscular and membranous coats, similar to the urethra, is alike subject to irritation, inflammation,[198] and ulceration, and imitatively gives forth morbid and other secretions. The rectum, from its situation and office, is very obnoxious to disease; and in addition to those already enumerated, it is extremely liable to become strictured.
The rectum is considered to be the lower part of the intestines that leads to the outlet commonly referred to as the anus. Some writers claim that the rectum serves a function for the bowels similar to what the urethra does for the bladder, while others argue that it acts as a storage area for waste before it's expelled. I think we all understand that it actually fulfills both roles; however, it’s clear that it’s used more for the first purpose than the second. As soon as the rectum is full, there’s a urge to empty it, which is the best indication of its function; but circumstances often prevent us from answering that urge for hours, highlighting its role as a storage space. The rectum, made up of muscular and membrane layers like the urethra, can also be affected by irritation, inflammation,[198] and ulceration, and can produce abnormal and other secretions. Because of its location and function, the rectum is very susceptible to disease; in addition to those mentioned, it is also prone to developing strictures.
Neither age nor sex are exempt from this strictural change, although it more usually selects the grown up and female portion of society. It is, generally speaking, the consequence of constipation, or the reverse—diarrhœa or dysentery—or it may follow in the wake of child-bearing. Piles are a frequent precursor. The ordinary symptoms are at first a slight difficulty in voiding the fæces, which assume the form of the passage through which they have to pass, presenting at one time a flattened tape-like shape, at others a spiral appearance, and again the natural form, but of very small diameter.
Neither age nor sex is exempt from this structural change, although it usually affects adults and women more. Generally speaking, it's a result of constipation or the opposite—diarrhea or dysentery—or it can follow childbirth. Hemorrhoids are a common precursor. The usual symptoms start with a slight difficulty in passing stool, which takes on the shape of the passage it goes through, sometimes appearing flattened like a tape, other times spiraled, and at other times retaining a natural shape but with a very small diameter.
As the disease advances, the pain increases, upon going to the water-closet, and after the act may be observed a small or copious discharge of mucus, or blood, from the anus. If the bowels be constipated, there is necessarily a great deal of straining during fæcation, that soon establishes spots of inflammation that rarely resolve, but run on to ulceration; small lodgments then of fæcal matter take place in the cellular membrane; and without detailing the pathological phenomena, it may suffice to say, that sooner or later the whole rectum becomes diseased, and fistula, with its attendant miseries, lends a speedy help to close life’s brief pilgrimage.
As the disease progresses, the pain intensifies, especially when going to the bathroom, and afterward there may be a small or large discharge of mucus or blood from the anus. If the bowels are constipated, there's a lot of straining during bowel movements, which quickly leads to areas of inflammation that rarely heal and can progress to ulceration. Small pieces of stool can then get trapped in the tissue, and without going into all the medical details, it’s enough to say that eventually, the entire rectum becomes diseased, and fistula, along with its associated pain, helps to hasten the end of life’s short journey.
Patients afflicted with rectal diseases lose flesh rapidly. From the constant pain and annoyance they endure, their general health gets undermined, the digestion becomes faulty, the countenance flags and looks care-worn, hectic fever awaits the break-up of functional regularity, and a lingering exhaustion closes the scene.
Patients suffering from rectal diseases lose weight quickly. The constant pain and discomfort they experience undermine their overall health, disrupt their digestion, their appearance becomes tired and worn, they face fever due to the breakdown of regular bodily functions, and a lingering fatigue ultimately takes over.
Stricture of the rectum is a curable disease; but the less complicated, the greater are the chances of recovery. The principles of treatment bear a near resemblance to those for stricture of the urethra. After having ascertained the situation and size of the contraction, a proper-sized bougie may be introduced, and suffered to remain as long as it occasions no inconvenience. The introduction should be repeated every or every other day, increasing the size of the bougie until the dilatation be fully perfected. After vigilance is necessary to prevent a recurrence, and the[199] bougie can not with propriety be entirely laid aside, or the disease will return with increased violence. There are, however, cases that require more imperative means, such as the use of the bistouri, an instrument for the division of stricture of the rectum, which, if the resort be objected to, it behooves persons with the premonitory symptoms to attend to them, that the operation may be rendered unnecessary. There are many excellent palliative medicines that the invalid will derive much comfort from in diseases of the rectum; and enemata constitute a powerful means of relief. The title of stricture of the rectum is fortunately more familiar than the disease is frequent; and what is more consolatory to persons of feeble health, the complaint seldom extends beyond two or three inches from the orifice, so that it need not be feared beyond the reach of relief. See annexed drawing:—
Stricture of the rectum is a treatable condition; however, the less complicated it is, the better the chances of recovery. The treatment principles are quite similar to those for stricture of the urethra. After determining the location and size of the contraction, a properly-sized bougie can be introduced and left in place as long as it causes no discomfort. This should be repeated every day or every other day, gradually increasing the size of the bougie until the expansion is fully achieved. Ongoing vigilance is essential to prevent a recurrence, and the bougie cannot be completely disregarded; otherwise, the condition will return with greater severity. There are, however, cases that need more urgent measures, such as using a bistouri, a tool for cutting the stricture of the rectum. If surgery is not an option, it’s important for individuals with early symptoms to address them so that the operation can be avoided. There are many excellent palliative medications that can provide significant relief to those suffering from rectal issues, and enemas are also an effective means of relief. Fortunately, stricture of the rectum is more well-known than it occurs frequently; and what’s more reassuring for those in poor health is that the issue rarely extends more than two or three inches from the opening, so it shouldn't be feared beyond the reach of treatment. See attached drawing:—
|
1. Rectum. Rectum.
2. Orifice of Rectum. Anus.
3. Stricture of the Rectum, with internal hæmorrhoids in the lower portion. 3. Stricture of the rectum, with internal hemorrhoids in the lower section. |

|
{kind=link}
There are some surgeons who state all diseases to emanate from a disordered liver, a weak stomach, or a “broken wind;” and there are others in this town who are never consulted but they deem the use of the rectum bougie indispensable. The limit to structural disorganization of the bowel is not afforded by stricture; there are, unfortunately, many diseases springing therefrom, and many totally independent of such; but their detail here would exceed the titular object of the book. Enough has been stated to convince any person teased with any of the enumerated symptoms, that however simple may be his malady in his own opinion, it is impolitic to overlook or neglect it.
There are some surgeons who believe all diseases come from a dysfunctional liver, a weak stomach, or a “bad stomach gas;” and there are others in this town who, whenever consulted, insist that using a rectal bougie is essential. The extent of bowel structural issues isn’t limited to strictures; unfortunately, there are many problems that arise from it, as well as many that are completely unrelated; however, going into detail about them would take this book beyond its intended purpose. It’s enough to say that anyone dealing with any of the mentioned symptoms should realize that, no matter how simple they think their condition is, it’s unwise to ignore or dismiss it.
We shall conclude our treatise by a few remarks on diseases of the urine, to which many are subject. Before proceeding to speak of them, it is necessary, for a full understanding of the subject, to state, that the urine is secreted by two bodies called kidneys, placed one on each side of the back-bone, as is shown in the cut. After being formed, the urine passes through the ureters into the bladder whence it is voided, as every one knows, occasionally.
We will wrap up our discussion with a few comments on urinary diseases, which many people experience. Before we dive into those, it's important to clarify that urine is produced by two organs called kidneys, located on either side of the spine, as illustrated in the image. Once formed, urine travels through the ureters into the bladder, from which it is occasionally expelled, as everyone is aware.

|
1—1. The Lungs. 1—1. The Lungs.
2. The Stomach. 2. The Stomach.
3—3. The Kidneys. 3—3. The Kidneys.
4—4. The Ureters. 4—4. The Ureters.
5. The Bladder. The Bladder. |
{kind=link}
The following diagram shows the bladder and its muscular coats, and also its neck imbedded in the prostate gland. The bladder is seen distended, and, of course, as detached from the body. The kidneys are also seen—one in its natural state, the other divided to show its inner structure: the kidneys and their ureters are crossed to save space in the sketch.
The following diagram shows the bladder and its muscle layers, as well as its neck embedded in the prostate gland. The bladder is shown expanded and, of course, detached from the body. The kidneys are also visible—one in its natural state and the other cut open to display its inner structure: the kidneys and their ureters are crossed to save space in the sketch.
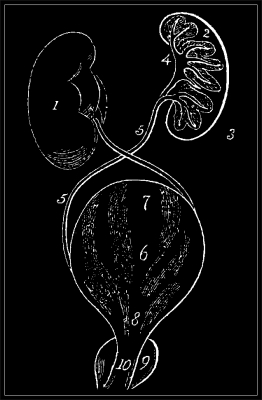
1. The entire kidney. 2. Its cortical, or secreting part. 3. The papilla. 4. The pelvis. 5. The ureter. 6. The bladder. 7. The detrusor muscle. 8. The sphincter muscle. 9. Prostate gland. 10. Neck of the bladder.
(There is no text provided to modernize.) The whole kidney. 2. Its cortex, or secreting part. 3. The papilla. 4. The pelvis. 5. The ureter. 6. The bladder. 7. The detrusor muscle. 8. The sphincter muscle. 9. Prostate gland. 10. Neck of the bladder.
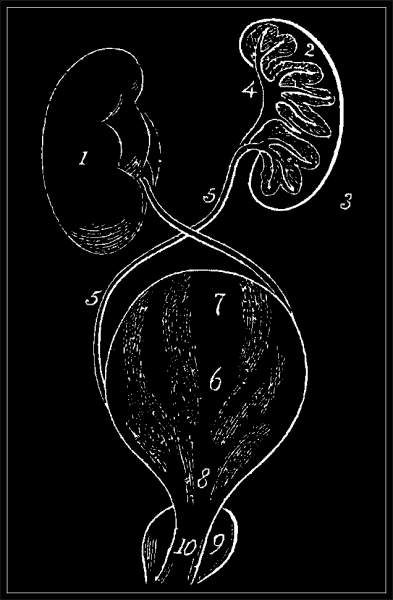{kind=link}
The bladder and adjacent parts are seen more fully in the diagram at the top of the succeeding page.
The bladder and nearby areas are shown in detail in the diagram at the top of the next page.

|
1. Corpus cavernosum. Corpus cavernosum. 2. Bulb of urethra. Bulbourethral gland. 3. Membranous portion of ditto. 3. Membranous part of that. 4. Prostate gland surrounding urethra. Prostate gland encircling urethra. 5. Seminal vesicles. 5. Seminal vesicles. 6. The two vasa deferentia. The two vas deferens. 7. The ureters. The ureters. 8. The bladder. The bladder. |
{kind=link}
It is a very common observation with patients, that they never were in better health in their lives than at the moment of consulting their medical adviser, except in the very particular malady, such as an ulcered limb, a teazing cough, a gleety discharge, or an irritable bladder, that they are seeking relief for; “they are quite well,” they say, “in every other respect.” When illness attacks an individual, it does not always announce its arrival by sound of trumpet. It does not always come on like an apoplectic shock: some minor organization is generally the first to indicate disturbance in the healthy economy by even so simple a presage (I will take for example, more especially as the ensuing remarks bear upon the subject) as excretion of disordered urine. To resume; the patient will content himself, that the only fault in his system is the disordered condition of his urine, and he earnestly seeks for something to touch that particular symptom, forgetting that trifling as he may fancy it, it is not merely owing to the office of the kidneys and bladder, but to the blood itself, whence the urine is formed, and to other circumstances in the economy that influence it. Therefore, it is not merely the urine which is at fault, but the state of it is a pretty good indication of the general state of health; and when it becomes vitiated, the urine is generally, unless restored to a healthy condition, a forerunner of some more serious evil. Still there are many variations in the character and quality of the urine, and each depending upon different causes—some upon a disordered state of the fluids of the body, some upon one remote cause or another, deranging the balance of the circulation, and inducing excessive[203] perspiration, and the like; and certainly not the least important, nor the least influential, exist in the very structures that make (as it were) and receive the urine, namely, the kidneys and bladder. I may observe here, that chymists have detected upward of twenty different substances, animal and saline, in its composition, but in a state of complete solution. Of all these component parts, the most important is an animal product named urea, which exists in about the proportion of one in thirty to the water containing it, while the other materials taken collectively, water excepted, yield only about double the quantity of the urea: hence, when the urine is disordered, its specific gravity[17] is increased or diminished, as the case may be; according to the abundance of the urea, and the various proportions of the saline ingredients of the urine, so is the urine thick, thin, acid, or alkaline, pale, or what is called high colored. The various conditions of the urine are ascertained by producing chymically certain decompositions, or by suffering the urine to effect its own changes, which, on being suffered to “stand,” sooner or later it will.
It’s a common observation among patients that they have never felt better in their lives than at the moment they consult their doctor, except for the specific issue they seek help for—like an ulcerated leg, a bothersome cough, a persistent discharge, or an irritated bladder. They often say, “I’m perfectly fine in every other way.” When someone gets sick, it doesn’t always announce itself dramatically. It doesn’t always come on like a sudden stroke; usually, a minor issue is the first sign of trouble in the body’s healthy functioning. For instance, the early warning can be something as simple as unusual urine. To continue, the patient may assure themselves that the only problem with their health is the abnormal urine, focusing solely on that symptom and overlooking the fact that, as trivial as they might consider it, the issue isn’t solely related to the kidneys and bladder. It’s also tied to the blood that creates the urine and various conditions in the body that affect it. So, the problem isn’t just with the urine; its condition is a good indicator of overall health. When urine quality deteriorates, unless it returns to normal, it usually signals a more serious problem ahead. However, there are many variations in the characteristics and quality of urine, each resulting from different causes—some from imbalances in the body’s fluids, others from various distant factors affecting circulation, leading to excessive sweating, among other things. An important influence comes from the very structures that produce and store urine: the kidneys and bladder. Chemists have identified over twenty different substances, both animal and saline, in urine, all in complete solution. Of these, the most significant is an animal compound called urea, which makes up about one part in thirty compared to the water it’s mixed with. The other substances, excluding water, together make up only about double the amount of urea. Thus, when urine is abnormal, its specific gravity increases or decreases, depending on the urea content and the various proportions of saline elements, making the urine thick, thin, acidic, or alkaline, pale, or darkly colored. The different conditions of urine can be determined by triggering certain chemical reactions or by allowing the urine to naturally change over time, which it will do if left to “stand.”
Healthy urine is perfectly transparent and of a light amber color; it yields an odor when warm resembling violets. Its taste (for pathologists trust not only to sight and smell) is saltish and offensive. As the urine cools, it throws up what may be said to be a “urinous smell.” As decomposition proceeds, the urine becomes cloudy, thick, with shining floating patches on the surface; and lastly, a thick deposite coats the bottom and sides of the vessel, the whole giving forth at the same time a fetid ammoniacal exhalation, as is perceived on entering public urinals.
Healthy urine is completely clear and light amber in color; when warm, it has a scent like violets. Its taste (since pathologists rely not just on sight and smell) is salty and unpleasant. As the urine cools, it develops what might be described as a “urine smell.” As decomposition continues, the urine becomes cloudy and thick, with shiny floating spots on the surface; eventually, a thick deposit gathers at the bottom and sides of the container, all while releasing a foul ammoniac smell, similar to what you notice in public restrooms.
The rapidity with which these several mutations occur, affords some criterion of the healthy or disordered state of the excretion we are talking about, and hence the usefulness of examining especially the urine of persons laboring under any disorder of the urinary system and functions connected therewith. A patient will complain, for instance, of irritable bladder. The symptoms of that complaint, as far as pain and frequent desire to micturate exist, very closely resemble those affections known by the name of “Diabetes,” but which is distinguished from the bladder affection in question by the quantity and character of the urine. I purpose herein to enumerate, in as familiar a manner as is possible, the various disordered states of the urine which my experience has rendered me familiar with, and to present the same as heretofore, in the form of cases that have fallen under my notice.
The speed at which these various changes happen provides a way to determine whether the excretion we’re discussing is healthy or disordered. This is why it’s important to examine the urine of people dealing with any issues related to the urinary system and its functions. For example, a patient might complain of an irritable bladder. The symptoms of that issue, such as pain and the frequent urge to urinate, are very similar to those associated with “Diabetes,” but can be distinguished from bladder problems by the volume and characteristics of the urine. In this piece, I plan to list the different disordered states of urine that I’ve encountered in my experience, and present them as I have in the past, through case studies that I’ve observed.
Now, the urinary disorders that I purpose to collect a description of, and exemplify, may be thus enumerated:—
Now, the urinary disorders that I aim to describe and illustrate can be listed as follows:
First, where too great a quantity of urine is voided.
First, where an excessive amount of urine is passed.
Secondly, where too little is discharged; and also, where suppression of it entirely occurs.
Secondly, where too little is released; and also, where it is completely suppressed.
Thirdly, those states where the urine deposites a sediment, of which two kinds are mostly prevalent, namely, the Lithates or Acid, and the Earthy or Alkaline.
Thirdly, in those cases where urine forms a sediment, there are two main types that are most common: the Lithates or Acid and the Earthy or Alkaline.
Fourthly, a brief exposition of the many but less frequent morbid changes of the urine, in which certain salts and substances, not existing in healthy urine, are precipitated or held in solution.
Fourthly, a quick overview of the various but less common unhealthy changes in urine, where certain salts and substances, not found in healthy urine, are either precipitated or dissolved.
And lastly, to add a few to the number of those already presented herein, of the infirmities of those organs which excrete the fluid under consideration, namely, the kidneys and bladder.
And finally, to add a few more to the list of those already mentioned here, regarding the issues related to the organs that process the fluid in question, specifically the kidneys and bladder.
ON INCONTINENCE OF URINE.
Although this is not the professional term for the disease I am principally about to speak of, yet under this head will the reader, if he be an invalid laboring under a complaint of this character, seek for a description of his own case. Incontinence of urine implies a loss of the retentive faculty of the bladder; but there is a species of disease where micturition is carried to such an extent, that a patient will attribute his leaky condition to the above cause. Not so, however, is the case; the urine, in the[205] disease alluded to, is generated or excreted in great quantity, and the bladder merely fulfils its ordinary duty. Of the affection known under the title of incontinence of urine, most persons are aware that it is one of more frequent occurrence in infancy than in adolescence; but the latter is by no means exempt. In childhood it arises, in all probability, from drinking too much, and the bladder becomes, during sleep, overloaded, and runs over; or, perhaps, from the irritability induced by its distension, becomes excited to action, and so empties itself, the drowsy state of the child rendering it insensible to the passing circumstances.
Even though this isn't the official term for the condition I'm mainly about to discuss, readers who are dealing with this kind of issue will search for a description of their own situation. Incontinence of urine means the bladder can't hold urine anymore; however, there is a type of condition where urination occurs so frequently that a person might think their leakage is due to this. That's not the case, though; in the[205] condition being referenced, urine is produced or expelled in large amounts, and the bladder is simply doing its normal job. Most people know that incontinence of urine is more commonly seen in infants than in teenagers, but teens are not completely immune. In children, it likely happens because they drink too much, causing the bladder to become full during sleep and overflow; or maybe the bladder, being overstretched, becomes so irritated that it triggers action and empties itself, while the child's sleepy state makes them unaware of what's happening.
The infirmity soon becomes a habit, which is often rendered worse by the means taken to check it, namely, chastisement, which is highly reprehensible. It is fortunately, however, a disease that wears itself out as the child grows up; and it may at all times be materially mitigated by a little care and attention, such as inducing the child to micturate before going to bed, and even awakening it before the anticipated time when it usually is attacked with the incontinence. The last fluid meal, which should be a spare one, should be taken some hours before retiring to rest; and if the complaint has gained much ascendency, medicines which give tone to the bladder should be taken. I have known the malady successfully removed, in a very short time, by a combination of the sulphate of iron and quinine, and any sedative extract, such as henbane or hops, given in small doses in the form of pills. Female children are more susceptible of the annoyance than males, probably owing to the shortness of the urethra. Every measure tending to give strength to the child should be used, such as cold bathing, fresh air, or a change of the same, especially if residing in the city, to the country. Mechanical contrivances are to be had to collect the escape of urine, whereby the offensive odor arising from the continually soiled bed-linen may be avoided, and oftentimes the fretting consequences of the urine passing over the person, which induce excoriations and troublesome sores. There are contrivances for both sexes. Where the disease prevails in mid-life, it is generally traceable to early improvident habits, and of course is the result of irritability and debility of the bladder. There are many patients who can somewhat control the functions of that organ while awake, but have no power over it when asleep. The treatment[206] depends a great deal upon the observance of abstemiousness both in eating and drinking: a perseverance in chalybeate remedies, both taken and administered internally (I have injected the bladder of a person subject to nightly incontinence of urine with various tonic preparations, with very great and permanent relief); the use of the warm bath, whereby the skin is brought into healthier action (for it is generally arid, and parched when much urine is voided), which tends to lessen the duty of the kidneys and urinary system, should be adopted; nor should exercise, that pabulum vitæ of even all feeble persons, be disregarded. It is of the utmost importance for the preservation of health, under all the circumstances in which we may be placed. Escaping from this digression, I now proceed to follow out the idea of the first paragraph of this chapter, to treat of those complaints wherein the urine is voided in excess. There is a disease commonly known by the name of diabetes, wherein the prominent symptom is a continual aptitude to pass urine, and in much greater quantities than the fluid consumed as ordinary drink could supply. This is one form of ailment of this class; but there is another, happily less inimical to life, and which, in the order of its frequency and simplicity, should take precedence. It is that state of health, where the patient is of that leaky habit, that whatever he takes runs through him, and that very quickly too. Of course, such a condition must depend upon a seriously-deranged constitution: hence there is present a perpetual thirst, an entire perversion of the perspiratory function, and a morbid condition of many of the phenomena of life. Where this disease springs up in early years, it becomes a habit proper to existence; and although it may not seriously disturb the economy of the being so as to lessen the duration of one’s stay here, yet it furnishes a source of much solicitude, by depriving us of rest, and shutting us out from society.
The problem quickly turns into a habit, often made worse by attempts to control it, like punishment, which is completely wrong. Thankfully, though, it's a condition that usually fades as the child grows older. It can always be significantly improved with some care and attention, like encouraging the child to use the bathroom before bed and even waking them up before they typically have an accident. The last meal, which should be light, should be eaten a few hours before going to sleep. If the issue has become serious, medications that strengthen the bladder should be considered. I've seen this issue successfully resolved in a very short time using a mix of iron sulfate and quinine, along with any calming extracts, such as henbane or hops, given in small pill doses. Female children are generally more affected than males, likely due to their shorter urethra. Any measures to increase the child’s strength should be taken, such as cold baths, fresh air, or a change of scenery, especially for those living in the city who could benefit from moving to the countryside. There are mechanical aids available to catch urine, helping to avoid the unpleasant smell from constantly soiled bed linens and the annoying effects of urine on the skin, which can lead to irritation and sores. There are devices for both boys and girls. When this issue occurs in middle age, it often stems from poor habits in early life, resulting in bladder irritability and weakness. Many patients can control bladder function while awake but struggle with it during sleep. Treatment[206] relies heavily on moderation in both diet and hydration: consistent use of iron remedies, both orally and through injection (I've injected tonic solutions into the bladder of someone who experiences nighttime incontinence with significant and lasting success); warm baths can help activate the skin healthily (since the skin is usually dry and parched when urine output is high), which reduces the burden on the kidneys and urinary system. Regular exercise, essential for the health of even the weakest individuals, should not be overlooked. It's crucial for maintaining health in any situation. Returning to the main topic, I will now address conditions involving excessive urine output. A common illness known as diabetes is characterized by a constant urge to urinate, with amounts exceeding what is typically consumed in fluids. This is one form of this issue; however, there is another, fortunately less life-threatening condition, which should be addressed first due to its frequency and simplicity. It describes a state of health where the person is so leaky that whatever they consume quickly passes through them. Naturally, this condition indicates a serious underlying problem: thus, there is continual thirst, a complete dysfunction of sweating, and an unhealthy state of various bodily functions. When this issue arises in younger years, it tends to become a habitual part of life; although it may not dramatically disrupt the body's overall functioning or shorten one’s life, it causes significant concern by robbing us of rest and isolating us from social interactions.
The patient (for such he or she may be truly called, and the complaint invades both sexes) appears to have a perpetual fever. Such is the desire for drink, that attested cases record the circumstance of individuals consuming from one to two pailfuls of water in twenty-four hours! and I positively know an instance, at the moment of writing this, of a child, fifteen years of age, consuming during the night, notwithstanding a plentiful supply of liquids during the day, a large jugful (two quarts) of water: the[207] quantity of urine excreted is nearly equivalent. In this case, the perspiration is profuse, and the child enjoys tolerably good health, with the exception of being occasionally nervous and hysterical. The case is under treatment, and the quantity of fluid allowed is being daily diminished. The urine on these occasions is aqueous, very pale, and of little specific gravity; the properties of the urine otherwise are not altered. These cases sometimes exist through life; and if they do not terminate fatally, they ultimately enfeeble the health, and predispose the patient, or, in other words, render him less able to combat with ordinary complaints common to us all, and thereby tend to the break-up of his constitution.
The patient (as he or she can truly be called, and this issue affects both genders) seems to have a constant fever. The thirst is so intense that reported cases show some individuals drinking between one and two pailfuls of water in a day! I personally know of a case, while writing this, of a fifteen-year-old child who, despite having plenty of liquids during the day, drank a large jug (two quarts) of water at night: the[207] amount of urine produced is nearly the same. In this case, the sweating is excessive, and the child is generally in decent health, apart from being occasionally anxious and hysterical. The case is being treated, and the amount of fluid allowed is being reduced daily. The urine during these times is watery, very light in color, and has low specific gravity; otherwise, the urine’s properties remain unchanged. These cases can sometimes last a lifetime; and if they don't end in death, they ultimately weaken the person's health, making them less able to fight off common ailments we all face, which can lead to the deterioration of their overall condition.
There are many persons tipplers, not for the love of the specific liquor, but from being always thirsty; and if we reflect a little, we shall soon find how inclined we are to encourage the habit. Since the introduction of tea into this country, what inordinate quantities of that fluid are consumed by individuals. They must, of course, dispose of it, after having drunk it: the stomach can not retain it, and it escapes either by the skin or kidneys, more usually the latter. It is no uncommon thing for nurses, washerwomen, and other females too, to swallow nine or a dozen cups of tea at a sitting: they declare it is their best meal.
There are many drinkers who don't love the specific liquor but are always thirsty. If we think about it for a moment, we’ll see how much we tend to support this habit. Since tea was introduced in this country, people have consumed it in massive amounts. Of course, they have to get rid of it after drinking; the stomach can't hold it all, so it leaves the body through the skin or kidneys, usually the latter. It's quite common for caregivers, laundresses, and other women to drink nine or twelve cups of tea in one sitting; they say it's their best meal.
Man is a great deal more careful of the quadruped world than the class he belongs to himself. He will stint his horse drink, who works as much beyond his strength as man does under his own, while he, the driver, will swill till his mouth can scarcely receive another drop. The moral of a volume might doubtlessly be expressed in very few words, but then it would not be a volume, and, consequently, would not be purchased or read; therefore, the proposition herein intended to be presented to the reader would exist unheeded. It is one thing to observe, that we all drink too much, or that too much fluids are hurtful to digestion and other functions, the public require some illustration (which their own reflection would furnish, if they used it), and hence this expense of verbosity to prove the fact. As one of the consequences, then, of too great an indulgence in fluids (I am here speaking of quantity rather than quality), this form of complaint, wherein the patient is perpetually desiring to urinate, is decidedly the result; and, as all complaints have a beginning, this may be considered as the first step toward setting up the several[208] affections of the kidneys and bladder hereafter treated upon. How important, then, is the arrest of this practice. Where the inconvenience thus detailed is present, the quantity of fluids must by degrees be diminished, the general state of health must be studied. Dieting and warm-bathing are two sheet-anchors, if properly applied. All remedies tending to afford strength to the urinary system must be had recourse to; and where the bladder loses any of its retentive power, I entertain the greatest benefit from an injection.
Humans are much more careful about the animal world than about their own kind. People will limit their horse's water intake, even though the horse works harder than they do, while they themselves will drink until they can hardly fit in another drop. The lesson of a whole book could probably be summed up in just a few words, but then it wouldn't be a book, and therefore wouldn’t be bought or read; as a result, the message intended for the reader would go unnoticed. It’s one thing to note that we all drink too much or that excessive fluids are bad for digestion and other bodily functions; the public needs some examples (which their own thinking could provide if they actually reflected), and that’s why we end up with this lengthy explanation to prove the point. One consequence of drinking too much (I’m talking about the amount rather than the quality) is a condition where the person constantly feels the need to urinate, which clearly results from this overindulgence; and since all health issues have a starting point, this can be seen as the initial step toward various kidney and bladder problems that will be discussed later. This underscores the importance of stopping this habit. When the issues described arise, the amount of fluids consumed needs to be gradually reduced and overall health needs to be examined. Dieting and warm baths can be two solid solutions if used correctly. All treatments aimed at strengthening the urinary system should be considered, and if the bladder loses any of its ability to hold urine, I find that injections can be very helpful.
The next form of urinary disturbance of a proximate nature to the one just described, is also where the urine is discharged in large quantities; but, unlike the former, excreted in greater abundance than the supply. The character of the fluid is also different; it assumes two appearances, modifications doubtlessly owing to the constitution of the patient and the severity and length of the disease. It is known by the name of diabetes: it is happily a complaint the least frequent of urinary derangements, else, from its obstinacy and difficult management, the slightest urinary disorder would excite much just dread and apprehension.
The next type of urinary issue that’s similar to the one just discussed involves urine being expelled in large amounts; however, unlike the previous case, the urine is produced in greater quantities than what the body takes in. The nature of the fluid also differs; it can appear in two forms, which are likely influenced by the patient’s health and the severity and duration of the illness. This condition is known as diabetes. Fortunately, it’s one of the rarer urinary disorders, or else, due to its stubbornness and challenging treatment, even minor urinary problems would cause significant fear and concern.
The forms of the complaint thus vary: In the one instance, there is a deficiency of the animal matter of the urine, namely, the urea, and in the other, a superabundance of it. In the former instance the urine is of a pale color, and transparent, and sometimes like clear water, with a very faint slight odor; whereas, in the latter it is generally of a higher color, and now and then so thick as to resemble brewer’s porter: it is decidedly a disease of great debility. The symptoms are, a wearisomeness and languor of the whole frame, a dry and crimpled state of the skin, a sinking, gnawing pain at the pit of the stomach, the bowels are obstinately bound, while a great thirst always prevails. The body wastes to a mere skeleton, the discharge of urine being almost constant, at least every hour, accompanied with a call that must be immediately obeyed: the leading feature in the composition of the urine, in addition to the varied presence of the urea, is the saccharine matter contained therein. It rarely attacks others than those who have led an irregular life, or else have suffered much from other kinds of sickness.
The types of complaints vary: In one case, there's a lack of animal matter in the urine, specifically urea, and in the other, there's an excess of it. In the first case, the urine is pale, clear, and sometimes as transparent as water, with a very faint odor; while in the latter, it's usually darker and can be thick like beer, indicating a serious health issue. The symptoms include overall fatigue and weakness, dry and wrinkled skin, a gnawing pain in the stomach, constipation, and constant thirst. The body loses weight drastically, and the urge to urinate is frequent, often every hour, requiring immediate attention. Besides the varying levels of urea, the urine also contains sugary substances. It typically affects those who have lived an irregular lifestyle or have been ill with other diseases.
Diabetes is supposed to depend upon a perverted action of the kidneys; but there is little dispute of its being a[209] malady involving the whole process of animal economization. The quantity of urine got rid of in a day has been known to amount to ten quarts; as the disease continues, the patient becomes much emaciated, the feet swell, and he sinks into a state of low hectic fever; the urine discharged continuing all this time to exceed nearly double the amount of nourishment, liquid or solid, that is taken, has given rise to the idea, that water is absorbed from the atmosphere through the body. The disorder is generally lingering, and, unless conquered, at last fatal. The treatment embraces many remedies—bleeding, emetics, diaphoretics, and sedatives, are mostly employed. It being a complaint involving the necessity of constant professional watchfulness, a more lengthened dissertation upon its peculiarities will but little serve the patient. My own opinion is, that the invalid must look for recovery—presuming the initiatory symptoms have been duly attacked and subdued—to careful diet, fresh air, varied scenery, and cheerful society. Bathing, either vapor or warm, is immensely useful; and, among the cases that have travelled across my path (for patients laboring under diabetes, like any other chronic ailment, generally take the round of the profession), I have seen much and great good achieved by the frequent employment of the bath.
Diabetes is believed to be caused by an abnormal functioning of the kidneys; however, there’s little disagreement that it’s a[209] condition that affects the entire process of the body's metabolism. The amount of urine produced in a day can reach ten quarts; as the disease progresses, the patient becomes significantly thinner, their feet swell, and they enter a state of low-grade fever; throughout this time, the urine produced often exceeds nearly double the amount of food and drink consumed, leading to the notion that water is absorbed from the atmosphere through the body. The condition is typically chronic, and unless it is effectively treated, it can ultimately be fatal. Treatment includes a variety of remedies—bleeding, emetics, diaphoretics, and sedatives are commonly used. Since this is an issue that requires constant medical oversight, a more detailed discussion of its specific characteristics would offer little benefit to the patient. I believe that for recovery—assuming the initial symptoms have been properly addressed—the patient should focus on a careful diet, fresh air, changing scenery, and positive interactions with others. Bathing, whether steam or warm, is extremely beneficial; in my experience with diabetes patients (like others with chronic conditions, they often seek various medical opinions), I've witnessed significant improvements achieved through regular use of baths.
As diabetes is mostly a sequence of some previous disturbance of the urinary system, it the more behooves the afflicted to heed the first noticial summons of attack: a handful of water will sometimes quench a mouldering ember that, suffered to rise into a flame, an engineful can not extinguish. I may add, there is no cause so destructive to virility as these drainages from the system through the urethra—an additional reason why they should be attended to upon their first appearance.
As diabetes is usually a result of some prior issue with the urinary system, it's even more important for those affected to pay attention to the first signs of an attack: a small amount of water can sometimes snuff out a smoldering ember that, if allowed to flare up into a full-blown fire, would require a lot of resources to put out. Additionally, there’s no factor more harmful to virility than these discharges from the body through the urethra—another reason why they should be addressed as soon as they show up.
Cases where but a small quantity of urine is voided, terminating in suppression, of urine.—The most popular scientific synonymes for complaints are but little understood by men really of education; for, as yet, medical knowledge forms not one of the items of collegiate lore, and few anticipate sickness to render such acumen necessary. The term “Strangury,” from the frequency of its occurrence, is uppermost in most men’s minds; and they use it on all occasions when there happens an interruption to the process of making water. It is oftentimes misapplied. Strangury implies a difficulty in voiding the urine, but it does not include[210] those cases wherein little is voided, because there is little to void. The affection I am now about to make mention of, is of the latter description. I have stated that the urine is subject to a multitude of changes, that the human frame is constituted to exist under a variety of circumstances, and that occurrences are daily happening, wherein its integrity is put to the test. Excesses, termed sensual, and others, which in themselves might destroy life, are counterbalanced by what may be styled the safety-valves of the system. A violent fit of purging, perspiration, or micturition, is often the means of warding off an otherwise fatal blow. The skin, the bowels, and the kidneys, are severally to be acted upon as emergencies demand: instance the specific operations of diet and medicines. The color of the urine is altered by (to give a popular illustration) rhubarb; its odor, by turpentine (taken internally, or from an inhalation of the vapor of them), and by the well-known vegetable asparagus; and its composition by alkaline and other chymicals. The function of cutaneous exhalation is augmented or diminished by warmth or cold; and the action of the bowels is suspended or increased by innumerable substances, forming portions of our daily food.
Cases where only a small amount of urine is passed, leading to urine retention.—The most common scientific terms for these issues are not well understood by educated individuals; medical knowledge is not yet a standard part of higher education, and few people expect illness to make that knowledge necessary. The term “Strangury,” due to its frequent occurrence, is what most people think of first; they use it whenever there is a disruption in urination. It is often misused. Strangury means having trouble passing urine, but it doesn't account for those situations where little urine is passed simply because there's not much to pass.[210] The condition I’m about to discuss falls into the latter category. I have noted that urine is subject to many changes and that the human body is designed to function under varying conditions, with daily events testing its balance. Excesses, often called sensual, along with others that could potentially harm life, are balanced by what we might consider the system's safety-valves. A sudden episode of diarrhea, sweating, or urination can sometimes prevent what could be a life-threatening situation. The skin, bowels, and kidneys must each respond to emergencies as they arise: take into account the specific effects of diet and medications. The color of urine can change due to (to provide a common example) rhubarb; its smell can be affected by turpentine (used internally or from inhaling its vapor), and the well-known vegetable asparagus; its composition can be altered by alkaline and other chemicals. The process of skin excretion is increased or decreased by heat or cold; and bowel activity can be heightened or slowed by numerous substances present in our daily diet.
Analogous to these effects, is the result of certain conditions of ill-health. A patient, laboring under fever or inflammation of any important organ, will scarcely rid himself of a wineglassful of blood-colored urine in the twenty-four hours; and there are many forms of ailments, where the function of separating the urine from the blood, or even the function of supplying the kidneys with that vital fluid, are suspended, partially or entirely. Few of us have escaped attacks of this kind; they are sure to follow long-pursued habits of dissipation, or even occasional displays of it; and they are often the result of accidents over which we have but little control. A patient will complain of a frequent desire to make water; each effort so to do, will be accompanied with excruciating pain. A small quantity, or a few drops only, will dribble away, excoriating the passage as though vinegar was passing over it, and putting on an appearance almost resembling muddy port wine, or a thick solution or suspension of brick dust: there will be present much fever and constitutional disturbance. The patient may have shivering fits, pain round the loins, down the thighs, and over the lower part of the[211] abdomen. He will betray a readiness to submit to anything, although conscious that his bladder is empty, notwithstanding the violent and urgent efforts at straining, which he is continually being called upon to make, as though his bladder were distended, and ready to burst. On passing the catheter (I am supposing a severe case, where retention of urine has at last occurred), not a drop will flow, and the danger of the disease is thereby made apparent. Except very severe measures be adopted, which it would be idle here to lay down, the case is sure to terminate fatally. Instances are recorded, where that event has been retarded upward of a week, during which time the patient voided not one drop of urine.
Similar to these effects is the outcome of certain health issues. A patient suffering from fever or inflammation of any major organ will barely manage to pass a wineglassful of blood-colored urine in twenty-four hours; and there are many types of illnesses where the ability to separate urine from blood, or even to supply the kidneys with that essential fluid, is completely or partially halted. Few of us have escaped these kinds of issues; they often follow long-term habits of excess, or even occasional indulgence, and can frequently result from accidents beyond our control. A patient might experience a constant urge to urinate; each attempt to do so brings excruciating pain. Only a small amount, or a few drops, will escape, burning the passage as if vinegar were flowing through it, appearing almost like muddy port wine or a thick mixture of brick dust. There will also be a lot of fever and overall discomfort. The patient may have chills, pain in the lower back, down the thighs, and in the lower abdomen. He will show a willingness to submit to anything, even though he knows his bladder is empty, despite the intense and desperate straining he feels compelled to do, as if his bladder is full and about to burst. When using a catheter (assuming this is a severe case where urine retention has finally occurred), not even a drop will flow, making the seriousness of the condition clear. Unless very severe measures are taken, which it would be pointless to detail here, the case is likely to end in death. There are documented cases where this outcome has been delayed for over a week, during which time the patient did not pass a single drop of urine.
The absolute cause of the disease is very obscure; but it has a beginning, and to those only who suffer from a long-continued diminution in this natural excretion, and who disregard it, is this picture presented.
The exact cause of the disease is quite unclear; however, it does have a starting point, and this scenario is only seen in those who experience a prolonged reduction in this natural excretion and who ignore it.
The treatment, in advanced stages of the disease, is strictly professional; but the warning of the altered character of a customary evacuation, should not for a moment be disregarded.
The treatment, in advanced stages of the disease, is strictly professional; however, the warning about the unusual nature of a regular evacuation should not be ignored for even a moment.
Suppression of urine is very different from retention: in the former, there is none to excrete; in the latter, its escape is impeded. In the chapter on stricture, the cause and manner of retention is explained, and the mode of relief laid down, whereby the invalid himself has a remedy at hand; but, in suppression, the resource is neither so ready nor so effectual. It is, therefore, much wiser to notice the first alteration, and to be prompt in seeking the nearest aid. Every practitioner is acquainted with such. Although such are not ever present, even in the most extensive practice, still they do occur; and much as this mode of frightening a patient may be condemned, knowing the frequently existing disinclination toward “laying up,” yet, if it only induce a fellow-mortal to take the tenth instead of the eleventh hour, one life may be saved, and the writer can well submit to the disapproval and contempt of the thoughtless and indifferent.
Suppression of urine is very different from retention: in suppression, there's nothing to excrete; in retention, the release is blocked. In the section on stricture, the causes and methods of retention are explained, along with ways to find relief, so the patient has a solution at hand. However, in cases of suppression, the options aren't as readily available or effective. Therefore, it's much smarter to notice the first signs of trouble and to seek help quickly. Every practitioner knows this. Although these situations don’t happen all the time, even in the busiest practices, they do occur; and even though using fear to motivate a patient may be criticized, considering the common reluctance to take time off for health issues, if it encourages someone to seek help sooner rather than later, it could save a life. The writer is willing to face the disapproval and scorn of those who are careless and indifferent.
Under the head of this disease may be classed all those urinary affections, wherein a sandy deposite is observed, after the urine has stood some time. This sandy excretion varies in its composition, in the quantity voided, and in its continuance: and it is also often separated, for it is held generally in solution in the urine as it comes from the bladder, while in the bladder or in the kidneys; and hence we find gravel in the kidneys, in the bladder, and in the urine. Where it is precipitated, or formed in the kidneys or bladder, it is apt to accumulate, and constitute what is called “Stone” in those organs. As I have just observed, the composition of this gravel differs, and differs also at different times in the same individual, according to circumstances. Stones have been detected that, like the rolling snowball, gather up, as they increase in size, whatever comes in their way; and, accordingly, as the deposites are principally composed of concretions, termed, in chymical phraseology, “Lithates” and “Phosphates,” stones are frequently found to be formed, first of a layer of one covering, then of another, and so on.
Under this condition, we can group all urinary issues where a sandy deposit appears after the urine has been sitting for a while. This sandy substance varies in its composition, the amount produced, and how long it lasts. It is usually dissolved in the urine as it exits the bladder, while in the bladder or kidneys; therefore, we can find gravel in the kidneys, bladder, and urine. When it settles or forms in the kidneys or bladder, it tends to accumulate, leading to what is known as "Stone" in those organs. As I mentioned, the composition of this gravel changes, and can also vary at different times in the same person based on different factors. Stones have been observed that, similar to a rolling snowball, pick up whatever they encounter as they grow larger; thus, since the deposits are mainly made up of substances called "Lithates" and "Phosphates," stones are often found to form layers of one type on top of another, and so forth.
Gravel may exist for years without inducing much disturbance of health, or it may produce serious inconvenience in a very short time. The urine being acid, holds the salts which it contains in solution; and, therefore, if the acid predominate, it becomes, through its own excess, thrown down, when it is detected in the form of red sand; but if there be an insufficiency of acid, the earths and salts of the urine are thrown down, and they exhibit their existence in the form of white gravel. Hence the two names “Red” and “White Gravel.” Acidulated urine is looked upon as certainly indicative of health, and when in excess, of a high tone of health; which, as the degree ascends, is marked by inflammation and fever. Alkaline urine betokens feebleness of constitution, or interrupted health. High living and an excited life induce red gravel; irregular, or an impoverished living, with much mental inquietude and physical exhaustion, establish white gravel. The fact of gravel being known to exist without forming stone, is no justification to suffer it to incur even the chance of such a finale. There is no class of diseases so painful and distressing as those wherein the function of[213] the kidneys or bladder is interrupted, and the majority of these affections are ushered in by a derangement of the urinary fluid.
Gravel can persist for years without causing much health trouble, or it can lead to serious issues very quickly. When urine is acidic, it keeps the salts dissolved; if the acidity is too high, it can settle out, appearing as red sand. Conversely, if there isn’t enough acid, the earths and salts from the urine settle out, showing up as white gravel. That’s why we have the terms “Red” and “White Gravel.” Acidic urine is generally seen as a sign of good health, and when it’s excessive, it suggests a state of high health, which can lead to inflammation and fever as the condition worsens. Alkaline urine indicates weak constitution or poor health. A rich lifestyle and excitement can lead to red gravel; meanwhile, irregular or poor living, along with significant mental stress and physical exhaustion, can cause white gravel. Just because gravel can exist without forming stones doesn’t mean we should ignore the possibility of that happening. Few health issues are as painful and troubling as those affecting the kidneys or bladder, and most of these conditions start with a disruption in the urinary fluid.
Cause of Gravel.—The cause of gravel is owing to chymical affinities. The urine, among its other constituents, contains lithic acid and ammonia, which two, in healthy urine, are combined and held in solution. If any other acid, as may be instanced in expelled urine, possessing a greater affinity for the ammonia than the lithic acid, be added, the lithic will be thrown down. The same process takes place when effected in the system, the source of which new acid is the stomach, which, when in an irritable and feeble state, as in indigestion, furnishes or abounds with muriatic acid. In like manner, the urine containing salts, called phosphate of lime, ammonia, and magnesia, on receiving an additional quantity of ammonia,[18] the lime, for the less affinity to phosphoric acid than the ammonia, is thrown down; and hence a salt, bearing its name, is generated, either to be expelled like gravel, or to feed a nucleus already existing in the bladder. These chymical changes are produced by the causes before enumerated. We are subject to an infinitude of laws: we are perpetually changing, and these changes may fairly be stated as chymical affinities: it is owing to such, that the absorption of fluids, and the deposition of substances, which exist more or less in all derangements of health, ensue—to such, that we resist death, and to such that we become its prey. Gravel is a disease not so productive of fear or suffering, so long as it escapes when formed; but there are so many circumstances that may give rise to the formation of stone, that sandy urine should always command notice and treatment. A clot or point of blood, that may have been discharged from irritation of the kidney or bladder, is often found to form the nucleus of a stone: the slightest substance, once in the bladder, is apt to form a basis for accumulation: a pin, a fragment of a bougie, or any instrument, hair, wood, and numberless other things that have found their way into the bladder, have given rise to the formidable and distressing complaint of stone.
Cause of Gravel.—The cause of gravel is due to chemical affinities. Urine, along with other substances, contains lithic acid and ammonia, which in healthy urine are combined and kept in solution. If any other acid, as seen in expelled urine, has a stronger affinity for ammonia than lithic acid, it will cause the lithic to precipitate. The same process happens within the body, where the source of this new acid is the stomach, which, when irritated and weak, as in indigestion, produces or has an excess of hydrochloric acid. Similarly, when urine containing salts like phosphate of lime, ammonia, and magnesia receives more ammonia,[18] the lime precipitates because it has a weaker affinity for phosphoric acid than ammonia does; thus, a salt, named after it, is created, either to be expelled like gravel or to contribute to an already existing core in the bladder. These chemical changes are caused by the factors mentioned earlier. We are governed by countless laws: we are constantly changing, and these changes can be reasonably described as chemical affinities. It is because of these that fluid absorption and the deposition of substances, which are present to varying degrees in all health disruptions, occur; it is due to these that we resist death, and it is because of these that we sometimes become its victims. Gravel is a condition that does not usually lead to fear or suffering, as long as it passes when formed; however, many circumstances can lead to the formation of stones, so sandy urine should always be noticed and treated. A clot or speck of blood, which may have been discharged due to irritation of the kidney or bladder, often becomes the core of a stone: the tiniest object, once in the bladder, can serve as a base for accumulation: a pin, a piece of a bougie, or any tool, hair, wood, and countless other items that have ended up in the bladder can lead to the severe and distressing problem of stones.
Treatment of Gravel.—It is not to be anticipated that every person is prone to excrete gravelly urine, else certain[214] dietetics, that evidently give rise to the same in particular instances, had better at once be removed from the list of articles of food, and their use prohibited altogether; but there are instances where a constitutional disposition exists in particular families, that is even transmitted from generation to generation, to calculous diseases, and in those cases, every precaution should be taken to avoid even their development.
Treatment of Gravel.—Not everyone is likely to have gravelly urine; otherwise, certain[214] foods that are known to cause this in some cases would need to be completely removed from our diet and banned altogether. However, there are families with a hereditary tendency towards kidney stones, and in those cases, every effort should be made to prevent even the onset of such conditions.
The antidotes to the disposition to gravelly urine are, exercise, temperance, and the adoption of all those means that tend to promote a healthy action of the skin and kidneys, namely, the warm bath—it is a perfect talisman in these affections—it needs but little eulogy; the comfort and relief, where relief is sought, afforded on the first experiment, best bespeak its praise. It is decidedly one of the most useful adjunctive prophylactic measures we have.
The solutions for dealing with gritty urine are exercise, moderation, and all the methods that help keep the skin and kidneys working well. The warm bath is especially effective for these issues—it really doesn’t need much praise; the comfort and relief it provides right from the first use speak for itself. It’s definitely one of the most helpful preventative measures we have.
I have already stated, that disorders of the urine arrange themselves under two great heads—the acid and the alkaline prevalence. The treatment is to neutralize the excess of either: the acid diathesis, as it is called, is considered a less healthy deviation than the alkaline, and is looked upon as indicative of greater constitutional break-up. The medicines most in vogue in gravelly disorders are, turpentine (to increase the formation of lithic acid), sulphuric, nitric, and muriatic acids; while the antagonists to that form of the disease, wherein the above are given, consist of ammonia, potass, and soda. The great object, however, is to balance the health, to allay irritation, and tranquillize the morbid uproar of the system. Here we have an extensive field to select from in the class of sedatives. Opium, perhaps, is the best—the most to be depended upon, its properties being best known; the warm bath comes next; and lastly, the various tonics and astringents of our pharmacopœia, of which quinine, uva ursi, pareira brava, achillæ millefoliæ, buchu, &c., &c., stand foremost.
I’ve already mentioned that urine disorders fall into two main categories—the acidic and alkaline types. The treatment aims to neutralize the excess of either. The acidic condition, known as acid diathesis, is seen as a less healthy variation than the alkaline condition and is thought to indicate more significant constitutional breakdown. The most common medications used for gravelly disorders include turpentine (to boost the production of uric acid), as well as sulfuric, nitric, and hydrochloric acids. The counteragents for the type of disease where the above are prescribed include ammonia, potassium, and sodium. The main goal, however, is to restore balance to health, reduce irritation, and calm the body's distress. There’s a wide range of sedatives to choose from. Opium is probably the best option—it’s the most reliable since its properties are well-known; the warm bath is the next choice; and finally, various tonics and astringents from our pharmacopoeia, with quinine, uva ursi, pareira brava, Achillea millefolium, buchu, etc., being the most prominent.
Although the lithic acid deposition is the most frequent, still, as the disease advances, there is a strong tendency to the formation of the alkaline; and as the remedies for the former are apt to accelerate the latter disorder, it is most important that the urine should undergo frequent examination to regulate the treatment. To recapitulate the substance of this article, it may be stated, that gravel is a disease, not dangerous in itself, but that it is always the forerunner, although not always productive, of stone;[215] stone being formed by the collection and chymical union of the sand itself. This collection takes place in the kidney, the ureters (the vessels that convey the urine to the bladder), the bladder, and sometimes in the urethra. The stone so formed varies in its composition and size, and is one of the saddest ills that can befall human nature. Hence the importance of watching, and attending to every urinary disturbance, of which gravel forms a prominent feature, the treatment of which has been already stated; but which, as it involves more practised judgment than a non-professional invalid can be supposed to possess, had better be intrusted only to professional hands.
Although the buildup of lithic acid is the most common, as the disease progresses, there’s a strong tendency for alkaline formation. Since treatments for the former can worsen the latter, it’s crucial to frequently check the urine to manage the treatment. To sum up this article, it can be said that gravel is a condition that isn’t dangerous on its own, but it often signals the potential for kidney stones, although not always leading to them; stones form from the accumulation and chemical bonding of the sand itself. This buildup can occur in the kidneys, ureters (the tubes that carry urine to the bladder), the bladder, and sometimes in the urethra. The resulting stone can vary in composition and size and is one of the most distressing afflictions that a person can face. Therefore, it’s important to monitor and address any urinary issues, of which gravel is a key symptom. The treatment has already been described, but since it requires more experienced judgment than what a non-professional might have, it’s best handled by a qualified professional. [215]
THE END.
THE END.
FORMULÆ
| Four to six drachms of castor oil, the ordinary black draught, a dose of salts, or a dose of Weir’s Compound Pills. |
| The following mixtures lessens the acrimony in making water, abdues the irritability, and tends to diminish the discharge:— | |||
| Take of— | |||
| Carbonate of potass | 1 | drachm. | |
| Nitrate of ditto | 1 | drachm. | |
| Mucilage of acacia | 5½ | oz. | |
| Hydrocyanic acid | 10 | drops. | |
| Syrup of Tolu | 2 | drachms. | |
| Mix. Take a tablespoonful in a wineglassful of water twice daily. | |||
| Take of— | |||
| Linseed tea | ½ | pint. | |
| Spirits of Sweet Nitre | 2 | drachms. | |
| Battley’s Sedative | 60 | drops. | |
| Mix. Take three tablespoonfuls, twice or thrice daily. | |||
| Where it is inconvenient for a patient to carry a bottle about his person, the following electuary, combining the essential ingredients of the former two, may be substituted:— | |||
| Take of— | |||
| Lenitive electuary | 2 | oz. | |
| Conserve of roses | 2 | oz. | |
| Strong mucilage of acacia | 2 | oz. | |
| Nitrate of potass | 2 | drachms. | |
| Mix. Dose—Two teaspoonfuls twice or thrice a day. | |||
| A good combination, that may be taken even in the inflammatory stage. | |||
| Take of— | |||
| Cubebs | 2 | oz. | |
| Carbonate of magnesia | 1 | drachm. | |
| Mix. Dose—A dessert- or tablespoonful twice or thrice daily. | |||
| Take of— | |||
| Balsam of copaiba | 1 | oz. | |
| Powder of cubebs | ½ | oz. | |
| Mucilage of acacia | 6½ | oz. | |
| Spirits of sweet nitre | 2 | drachms. | |
| Battley’s sedative | 30 | drops. | |
| Or— | |||
| Hydrocyanic acid (Scheele’s strength) | 8 | drops. | |
| Syrup of orange-peel | 2 | drachms. | |
| Mix. Dose—Two tablespoonfuls, once or twice daily, in water. | |||
| Turpentine Pills. |
| Take of Venice turpentine 1 drachm, form it into pills by adding as much rhubarb as is necessary, and take two, three times a day. |
| Turpentine Mixture. | |||
| Take of— | |||
| Venice turpentine | 1 | scruple. | |
| Mucilage of gum arabic | 2 | oz. | |
| Emulsion of bitter almonds | 4 | oz. | |
| Syrup of orange-peel | ½ | oz. | |
| Mix. Dose—Two tablespoonfuls three times a day. Sedatives may be conjoined with the above preparations, if they produce too much action of the bowels. To the pills may be added one scruple of Dover’s powder to the drachm of turpentine. To the mixture, thirty drops of laudanum. | |||
| Take of— | |||
| Terebinthin chiœ | 1 | oz. | |
| Extract of rhubarb | 1½ | drachms. | |
| Camphor | 1 | drachm. | |
| Mix and divide into pills of 5 grains each. Dose—Three, three times a day. | |||
| Take of— | |||
| Cahio turpentine |
|
Of each, equal parts. | |
| Balsam of copaiba | |||
| Oil of amber | |||
| Mix, according to art. The turpentine must be dissolved by warmth. The dose is 30 or 40 drops three or four times a day. This medicine is very nauseous, but very serviceable in long standing gleets and obstinate claps. The best way to remove the flavor left in the mouth after taking turpentine, copaiba, and other filthy medicines, is to chew a piece of gingerbread or cheese, or suck a lemon, or put some salt upon the tongue. | |||
| Take of— | |||
| Cahio turpentine | } | ||
| Balsam of copaiba | } | Of each, equal parts. | |
| Oil of amber | } | ||
| Mix, according to art. The turpentine must be dissolved by warmth. The dose is 30 or 40 drops three or four times a day. This medicine is very nauseous, but very serviceable in long standing gleets and obstinate claps. The best way to remove the flavor left in the mouth after taking turpentine, copaiba, and other filthy medicines, is to chew a piece of gingerbread or cheese, or suck a lemon, or put some salt upon the tongue. | |||
| Injections to diminish the pain on making water. | |||
| Take of— | |||
| Rose-water | 3 | oz. | |
| Solution of the acetate of morphine | 2 | drachms. | |
| Mix. | |||
| Take of— | |||
| Goulard water | 3 | oz. | |
| Mucilage | 4 | oz. | |
| Solution of the acetate of morphine | 2 | drachms. | |
| Mix. | |||
| Sedative draught to be taken at bed-time when annoyed with chordee. | |||
| Take of— | |||
| Acetated liquor of ammonia | ½ | oz. | |
| Camphor julep | 1 | oz. | |
| Solution of the acetate of morphine | 20 | to 25 drops. | |
| Mix. | |||
| Take of— | |||
| Dover’s powder | 12 | grains. | |
| James’s powder | 5 | grains. | |
| Mix. | |||
| Take of— | |||
| Compound camphor liniment | ½ | oz. | |
| Laudanum | ½ | oz. | |
| Mix, to form a liniment. | |||
| Injection for the ulceration of the glans penis. | |||
| Take of— | |||
| Chloride of soda | 1 | oz. | |
| Rose-water | 5 | oz. | |
| Mix. | |||
| Take of— | |||
| Nitrate of silver | 1 | scruple. | |
| Distilled water | 1 | oz. | |
| Mix. | |||
| Take of— | |||
| Calomel | ½ | drachm. | |
| Lime-water | 4 | oz. | |
| Mix. | |||
| Emetic Powder. | |||
| Take of— | |||
| Ipecacuanha powder | 1 | scruple. | |
| Emetic tartar | 1 | grain. | |
| Mix. To be taken in a glassful of warm water, and repeated in twenty minutes, if it do not produce vomiting. | |||
| Iodine. |
| Take of tincture of iodine twenty drops twice or thrice a day in a little water. |
| Take of— | |||
| Hydriodate of potass | ½ | drachm. | |
| Mucilage of acacia | ½ | oz. | |
| Camphor julep | 5½ | oz. | |
| Mix. Dose—three tablespoonfuls three times a day. | |||
| Take of— | |||
| Extract of Aconitine | 1 | grain. | |
| Oil of Olives | 1 | drachm. | |
| Mix. | |||
| Or take of— | |||
| Extract of Henbane | 5 | grains. | |
| Lard or Olive Oil | 1 | drachm. | |
| Mix. | |||
| Or take of— | |||
| Acetate of Morphine | 3 | grains. | |
| Simple Cerate or Oil | 2 | drachms. | |
| Mix. | |||
| Take of powder of calcined alum, and dust the end of a bougie previously oiled, and introduce it to the stricture in the usual manner, and suffer it to remain until the obstacle be overcome. Occasionally the bougie may be smeared with the balsam copaiba, where the case is chronic, and there happens to be much secretion from the part. |
| Take of— | |||
| Iodide of potass | 1 | drachm. | |
| Mercurial ointment | 1 | do. | |
| Simple cerate | 4 | do. | |
| Mix. A portion to be rubbed over the scrotum night and morning, as long as it can be borne. | |||
| Strong caustic solution of Dr. Doane. | |||
| Take of— | |||
| Caustic | ⅓ | drachm. | |
| Distilled water | 1 | oz. | |
| Mix. | |||
| Wash for Chancres. | |||
| Take of— | |||
| The solution of chloride of soda | 2 | oz. | |
| Rose-water | 4 | oz. | |
| Mix. | |||
| Black wash for Chancres. | |||
| Take of— | |||
| Calomel | 1 | scruple. | |
| Lime-water | 3 | ounces. | |
| Mix. | |||
| Red wash for Chancres. | |||
| Take of— | |||
| Bi-chloride of mercury | 4 | grains. | |
| Lime-water | 4 | oz. | |
| Mix. | |||
| Blue wash for Chancres. | |||
| Take of— | |||
| Sulphate of copper | 5 | grains. | |
| Distilled water | 1 | oz. | |
| Mix and strain. | |||
| For dressing chancres, lotions and washes generally answer better than ointments; but their alternate use is sometimes serviceable. In cracked sores near the prepuce, the blue ointment has wrought a cure when all the lotions devised were ineffectual. | |||
| Take of— | |||
| Red precipitate of mercury | 4 | grains. | |
| Ointment of spermaceti | 1 | oz. | |
| Mix.—A little to be smeared over the ulcer, twice a day. | |||
| Active aperient in indolent Chancres. | |||
| Take of— | |||
| Calomel | 4 | grains. | |
| Powder of jalap | 15 | to 20 grains. | |
| Mix.—To be taken in something thick, as jelly, honey, or tamarinds. | |||
| Active aperient, to be mixed in water and (stirring it) to be drank off quickly. | |||
| Take of— | |||
| Chloride of mercury, or calomel | 5 | grains. | |
| Powder of jalap | 25 | grains. | |
| Mix. | |||
| Ointment to promote absorption of Bubo. | |||
| Take of— | |||
| Iodine of potassium | 1 | drachm. | |
| Tincture of iodine | 1 | drachm. | |
| Acetate of morphine | 10 | grains. | |
| Mix.—Apply constantly a plaister of some of this ointment spread upon rag or lint, over the bubo, and occasionally rub a little of it gently into the skin.—Doane. | |||
| Take of blue ointment a similar quantity, and use it in like manner to the preceding. The reliance to be placed on this ointment is precisely the same as the other, namely, to excite absorption. The following ointment may also be used for the same purpose. |
| Take of— | |||
| Calomel | 2 | drachms. | |
| Simple ointment | 6 | drachms. | |
| Mix. | |||
| Stimulating ointments to promote the healing of indolent ulcerated Buboes. | |||
| Take of— | |||
| Red precipitate of mercury | 5 | grains. | |
| Ointment of spermaceti | 1 | oz. | |
| Mix.—The ulcer to be dressed with a small portion of this ointment spread upon lint. Or the following, which is stronger:— | |||
| Take of— | |||
| Red precipitate of mercury | 5 | grains. | |
| Yellow basilicon | 2 | drachms. | |
| Ointment of spermaceti | 6 | drachms. | |
| Mix.—To be used like the preceding. | |||
| Take of nitrated ointment of mercury, diluted with an equal proportion of simple ointment. |
| Or, the unadulterated strong mercurial ointment. |
| Styptic application for indolent Ulcers. | |||
| Take of— | |||
| Caustic | ½ | drachm. | |
| Or, | Sulphate of copper | ½ | do. |
| Distilled water | 1 | oz. | |
| Mix and strain, and smear the surface of the sore with a hair pencil, impregnated with either of the solutions: simple or astringent dressings may be applied afterward. | |||
| Take of— | |||
| Chloride of soda | 2 | ounces. | |
| Rose-water | 2 | do. | |
| Mix. | |||
| Preparation of Iron. |
| Take two drachms of carbonate of iron three times a day, gradually increasing the dose to half an ounce, or even an ounce; the bowels during the taking of this medicine should be kept open. |
| The following is an excellent combination. |
| Take of compound iron pill two drachms, to be divided into 24 2 pills to be taken three times a day. |
| Quinine. |
| Take three grains of sulphate of quinine three times a day. Or, |
| Take of— | |||
| Compound tincture of bark | 2 | ounces. | |
| Sulphate of quinine | 12 | grains. | |
| Muriatic acid | 20 | drops. | |
| Mix.—Dose, a teaspoonful three times a day, in water. | |||
| Strengthening Pills. | |||
| Take of— | |||
| Ioduret of iron | ½ | drachm. | |
| Castile soap | ½ | do. | |
| Alkaline extract of gentian | 1 | do. | |
| Mix.—To form 30 pills—take one twice daily. | |||
| Tonic and Alterative Mixture. | |||
| Take of— | |||
| Oxymuriate of mercury | 2 | grains. | |
| Muriatic acid | 60 | drops. | |
| Tincture of bark | 2 | oz. | |
| Mix.—A teaspoonful to be taken twice or three times a day in a little water. | |||
| These drops are highly serviceable to persons of weak constitutions, whom it is desirable to place under the influence of mercury. They form the basis of most of the advertised anti-scorbutic drops of the patent medicine venders. | |||
| Compound decoction of Sarsaparilla. | |||
| Take of— | |||
| Sarsaparilla root, sliced | 4 | ounces. | |
| Boiling water | 4 | pints. | |
| Macerate for four hours in a vessel lightly covered, and placed near the fire; then take out the sarsaparilla and bruise it; return it again to the liquor, and macerate in a similar manner for two hours; boil it down to two pints, strain it, and then add— | |||
| Sassafras root, sliced | ¼ | ounce. | |
| Guaiacum root, rasped | ¼ | do. | |
| Liquorice root, bruised | ¼ | do. | |
| Bark of mezeroon root | 1½ | drachm. | |
| Boil the whole together for a quarter of an hour, and strain. | |||
| Dose, from a quarter to half a pint, three times a day. | |||
| To avoid the tediousness of daily preparing the above, many manufacturing chemists evaporate a large quantity, and preserve the extract, which retains all the virtues of the decoction, and is at all times ready for immediate use. Or, | |||
| Take of— | |||
| Bruised root of Jamaica sarsaparilla | 4 | ounces. | |
| Liquorice root, sliced | ½ | ounce. | |
| Lime-water | 1 | quart. | |
| Macerate for 24 hours in a dark and cool place—tension and bottle it, and take a pint daily in divided doses. This is a very superior form of administering sarsaparilla. Or, | |||
| Take of— | |||
| Oxymuriate of mercury | 2 | grains. | |
| Muriatic acid | 5 | drops. | |
| Compound extract of sarsaparilla | 2 | oz. | |
| Dissolve the same in one quart of water, and take a wineglassful twice a day. | |||
| The Iodide of Potass Mixture. | |||
| Take of— | |||
| Iodide of potassium | 1 | drachm. | |
| Iodine | 2 | grains. | |
| Mucilage of acacia | 3 | ounces. | |
| Hydrocyanic acid | 12 | drops. | |
| Pure water | 5 | ounces. | |
| White sugar | ½ | ounce. | |
| Mix. Take a dessert- or tablespoonful twice or thrice daily in a wineglassful of water. | |||
| Take of— | |||
| Iodide of potassium | 1 | drachm. | |
| Acetate of morphine | 10 | grains. | |
| Spermaceti ointment | 1 | oz. | |
| Mix. Rub a portion, the size of a nut, over the affected part night and morning. If much irritation be produced, it must be disused for a time. | |||
| Forms 54, 55, 56, 57 see pages 126–128. |
| Take of— | |||
| Sarsaparilla sliced | 1 | oz. | |
| China root | 1 | oz. | |
| Dry rind of 20 walnuts. | |||
| Antimony | 2 | oz. | |
| Pumice stone | 1 | oz. | |
| (Tied in separate bags, and boiled with the other ingredients.) | |||
| Distilled water | 10 | pints. | |
| Boil to one half, and strain. | |||
| Dose—An aleglassful twice or thrice daily. | |||
| Forms 59, 60, 61, 62 see page 132. |
| The best aperient for females is certainly a combination of castor oil. The following form is a very good one:— |
| Take of— | |||
| Castor oil | 1 | oz. | |
| Mucilage of acacia | 2 | oz. | |
| Spirits of sweet nitre | 1 | drachm. | |
| Syrup of orange-peel | ½ | oz. | |
| Water | 1 | oz. | |
| Mix. Take half for a dose. | |||
| Forms 64, 65, 66, 67, 68, 69, 70 see pages 156–158. |
| Forms 71, 72, 73, 74, 75, 76, 77, 78, 79 see pages 158–161. |
FOOTNOTES
[3] To enter into a description of the pathological condition of the bladder in the several states of irritability, paralysis, and inflammation, would be to swell this article to an inordinate length, and serve no useful purpose—the symptoms and treatment comprising the most essential knowledge for the patient to possess. It may be briefly stated, that the bladder is less subject to become disorganized (the function being chiefly the disordered symptom), and sooner even regains its tone than other organs not less important to life.
[3] Describing the issues with the bladder in various states of irritability, paralysis, and inflammation would make this article unnecessarily long and wouldn't be helpful—the symptoms and treatment are the most important information for the patient to know. In short, the bladder is less likely to become disorganized (the problem mainly being the disrupted function) and it often recovers its normal function faster than other vital organs.
[5] Mercury.
The preparations of mercury are various: but those chiefly employed in the treatment of syphilis are the oxymuriate, or bi-chloride, the submuriate, or chloride, the red precipitate, or the hydrargyri nitrico-oxydum, the blue pill, the red sulphate for fumigations, and the blue ointment.
The preparations of mercury vary, but the main ones used for treating syphilis are the oxymuriate, or bichloride, the submuriate, or chloride, the red precipitate, the hydrargyri nitrico-oxydum, the blue pill, the red sulfate for fumigations, and the blue ointment.
Ptyalism or salivation, which implies an extraordinary secretion of the salivary and other glands, occasioned by the taking of mercury, inasmuch that when carried to an unwarrantable extent, ulceration is the consequence, may be produced by the internal exhibition or external application of almost any of its preparations. With this view, however, the blue pill is usually administered in doses of five grains twice a day, or the blue ointment is directed to be rubbed in on the inner part of the legs and thighs, in quantities varying from one to two drachms night and morning. Mercury, when given to excite ptyalism, is generally taken in conjunction with sarsaparilla (see Form 51, or the fluid extract). The symptoms whereby the effects of mercury are ascertained, are a coppery taste in the mouth, followed by a tenderness of the gums on mastication, an increased flow of the saliva, and a peculiar fœtor of the breath. It is usual, on the tainted taste being perceptible, to diminish or discontinue the further use of the medicine, unless the case be very severe, or merely to keep up the effect produced. But it can not be denied that, although sufficiently manageable in scientific hands, mercury, or any one of its preparations, is too powerful to be taken indiscriminately.
Ptyalism, or excessive salivation, refers to an unusually high secretion from the salivary and other glands caused by taking mercury. If this condition becomes too severe, it can lead to ulceration. This can happen from either internal use or external application of almost any mercury preparation. Typically, the blue pill is given in doses of five grains twice daily, or blue ointment is applied to the inner thighs and legs in amounts ranging from one to two drachms, both morning and night. Mercury is usually taken with sarsaparilla to stimulate ptyalism (see Form 51, or the fluid extract). Symptoms indicating the effects of mercury include a metallic taste in the mouth, tenderness of the gums when chewing, increased saliva production, and a distinctive bad breath. When the metallic taste is noticed, it is common to reduce or stop the medication unless the case is very serious or to maintain the treatment's effects. However, it cannot be overlooked that, while manageable in professional hands, mercury and any of its forms are too potent to be used carelessly.
[6] Antimony.
Antimony.
The preparations of antimony consist of the precipitated sulphuret, called now the oxysulphuret of antimony, and the powder, as directed to be made in the Pharmacopœia, or its secret modification, known by the name of “Dr. James’s Powder.” The sulphuret enters into the composition of the red or Plummer’s pills, which is an admirable alterative, given in conjunction with sarsaparilla, in doses of five grains, once or twice a day. The James’s powder, with the like intention, may be taken in two or three grain doses twice or thrice a day.
The preparations of antimony include the precipitated sulfide, now called the oxysulfide of antimony, and the powder, as outlined in the Pharmacopoeia, or its secret version known as “Dr. James’s Powder.” The sulfide is part of the composition of the red or Plummer’s pills, which is an excellent alternative treatment, usually given with sarsaparilla, in doses of five grains once or twice a day. James’s powder, with a similar purpose, can be taken in two or three grain doses two or three times a day.
[7] Wagner, translated by Dr. Willis.
[8] Some say eight days after.
Some say it happens eight days later.
[9] Instances of different conceptions following connexion at brief intervals are of occasional occurrence.
[9] Sometimes, there are different ideas appearing after a brief connection.
A case is recorded of a negress having brought forth a negro and a mulatto child, and who confessed having received the embraces of a white and a negro the same evening. Drs. Dewees of Philadelphia, and Francis of New York, adduce similar instances.
A case is documented of a Black woman giving birth to both a Black child and a mixed-race child, and she admitted to being with a white man and a Black man on the same evening. Drs. Dewees from Philadelphia and Francis from New York present similar cases.
[10] The membrane containing the liquid comes away with the after-birth or placenta; but when it is brought away with the child’s head, it is named a “caul,” to which the ignorant attach a superstitious belief that it saves the possessor from drowning, and hence it has been a source of traffic between the cunning and the weak-minded. Cauls are made by detaching the membrane from the placenta.
[10] The membrane holding the fluid comes away with the afterbirth or placenta; however, when it’s delivered along with the baby’s head, it’s called a “caul.” Some people, lacking knowledge, believe superstitiously that it protects the owner from drowning, which has made it a target for exploitation by the clever and the gullible. Cauls are created by separating the membrane from the placenta.
[13] Blundell.
Blundell.
[14] Dr. A. Sidney Doane has recorded a case, in his edition of “Good’s Study of Medicine,” where a woman brought forth fifty-seven children.—Vol. ii., p. 503.
[14] Dr. A. Sidney Doane documented a case in his edition of “Good’s Study of Medicine” where a woman gave birth to fifty-seven children.—Vol. ii., p. 503.
[15] A patient was admitted into the ophthalmic wards of the Hotel Dieu, Paris, with great weakness of sight, amounting almost to amaurosis. He confessed that he was in the habit of polluting himself, and that he was immediately seized with complete blindness whenever he addicted himself to the practice. Cases very similar to the above have been noticed by Dr. Doane, of New York, who has paid great attention to diseases of this character.
[15] A patient was admitted to the eye care ward at Hotel Dieu in Paris, suffering from severe vision loss, nearly leading to total blindness. He admitted that he frequently engaged in self-destructive behavior, and that he experienced total blindness immediately after indulging in this habit. Similar cases have been observed by Dr. Doane from New York, who has focused extensively on conditions of this kind.
[16] The convertibility of India-rubber to so many useful purposes has not escaped the attention of surgeons, and it is found to be an excellent material for trusses, pessaries, bougies, &c., and consequently much used for them. I find them in my own practice far preferable to metallic or any other description. Many cases of hæmorrhoids, as well as of prolapsus, that have been given up as incurable, on account of the parties objecting to wear metallic instruments, or submit to the operation of excision or ligature, have speedily yielded to the application of the same manufactured of India-rubber; indeed, every day’s experience so convinces me of their superiority and efficacy as a remedy in these disorders, that a patient afflicted with the most formidable form of either disease need not despair of a prompt and certain recovery.
[16] The ability of India-rubber to be used for so many helpful purposes has caught the attention of surgeons, and it has proven to be an excellent material for trusses, pessaries, bougies, etc., and is therefore widely used for these applications. In my own practice, I find them far better than metallic or any other types. Many cases of hemorrhoids, as well as prolapse, which were considered incurable because the patients refused to use metallic instruments or undergo excision or ligature, have quickly responded to the use of those made from India-rubber. In fact, my daily experience continuously confirms their superiority and effectiveness as a treatment for these conditions, so a patient suffering from the most severe form of either illness need not lose hope for a quick and certain recovery.
[17] The specific gravity of the urine materially depends upon those causes which act diuretically, and upon the quantity of fluids swallowed, which, if taken in excess, of course increases the watery portion of the urine, and vice versa. The density of the urine is ascertained by an instrument called an “Hydrometer,” which, upon being immersed in the urine, indicates its specific gravity. The usual specific gravity of healthy human urine varies from 1.010 to 1.015, while the temperature ranges from 75 degrees of Fahrenheit to 120. The quantity averages from two to three pints per diem, but depends not only upon the quantity of fluids consumed, but also upon the nature of the food, vegetables generating more urine than animal substances. In infancy and old age, the temperature of the urine is below this standard, but nearly equivalent to each other; whereas it is only at the period of puberty that the temperature noted exists.
[17] The specific gravity of urine is significantly influenced by factors that cause increased urination and the amount of fluids consumed. When people drink a lot, it increases the water content of the urine, and the opposite is also true. The density of urine is measured using an instrument called a “Hydrometer,” which shows its specific gravity when placed in the urine. The typical specific gravity of healthy urine ranges from 1.010 to 1.015, while the temperature varies from 75 degrees to 120 degrees Fahrenheit. The average amount of urine produced is about two to three pints a day, but this depends not just on fluid intake but also on the type of food consumed, with vegetables leading to more urine production than animal products. In infants and the elderly, urine temperature is below this standard but is relatively similar; this typical temperature is generally reached only during puberty.
Obvious punctuation errors in the transcribed text have been repaired.
Obvious punctuation errors in the transcribed text have been corrected.
Variations in spelling are common in this book. In the case of medical terms in which the ligatures ‘æ’ and ‘œ’ could be used, the variations are numerous and noticeable. Thus we find the terms “hemorrhage”, “hæmorrhage” and “hœmorrhage” being used interchangeably. Similarly for “hæmorrhoids” and “hœmorrhoids” and all the words derived from the foregoing terms.
Variations in spelling are common in this book. For medical terms that use the ligatures ‘æ’ and ‘œ’, there are many noticeable variations. For example, we see the terms “hemorrhage”, “hæmorrhage”, and “hœmorrhage” used interchangeably. The same applies to “hæmorrhoids” and “hœmorrhoids”, along with all the words derived from these terms.
Except as noted below, unusual or variable spelling and hyphenation as published in the original book have been retained.
Except as noted below, any unusual or variable spelling and hyphenation found in the original book have been kept.
Page 11 — “membraneous” changed to “membranous” (diminishes at the membranous portion)
Page 11 — “membraneous” changed to “membranous” (diminishes at the membranous portion)
Page 16 — “then,” changed to “them” (that connects them together)
Page 16 — “then,” changed to “them” (that connects them together)
Page 21 — “developes” changed to “develops” (the sooner develops the disease)
Page 21 — “developes” changed to “develops” (the sooner develops the disease)
Page 22 — “ay” changed to “any” (to resist any efforts)
Page 22 — “ay” changed to “any” (to resist any efforts)
Page 24 — “arm-pits” changed to “armpits” (under the armpits)
Page 24 — “armpits” changed to “armpits” (under the armpits)
Page 29 — “gonorrhæa” changed to “gonorrhœa” (in curing gonorrhœa;)
Page 29 — “gonorrhœa” changed to “gonorrhea” (in curing gonorrhea;)
Page 30 — “head-ache” changed to “headache” (inclination to headache)
Page 30 — “head-ache” changed to “headache” (tendency to headache)
Page 50 — “surfacial” changed to “surficial” (surficial and muscular membranes)
Page 50 — “surfacial” changed to “surficial” (surficial and muscular membranes)
Page 54 — “fœces” changed to “fæces” (the fœces pass in small quantities)
Page 54 — “fæces” changed to “fæces” (the fæces pass in small quantities)
Page 58 — “permaneut” changed to “permanent” (permanent irritability of the bladder)
Page 58 — “permaneut” changed to “permanent” (permanent irritability of the bladder)
Page 62 — “now” changed to “how” (to show how imperative it is)
Page 62 — “how” changed to “how” (to show how imperative it is)
Page 80 — “coherd” changed to “cohered” (where numbers cohered together)
Page 80 — “coherd” changed to “cohered” (where numbers came together)
Page 85 — “empyrical” changed to “empirical” (by the most empyrical measures)
Page 85 — “empirical” changed to “empirical” (by the most empirical measures)
Page 87 — “chancerous” changed to “chancrous” (a chancrous sore)
Page 87 — “chancerous” changed to “chancrous” (a chancrous sore)
Page 89 — “accompanying” changed to “above” (Witness the above wood-cut.)
Page 89 — “accompanying” changed to “above” (See the woodcut above.)
Page 102 — “incrustrations” changed to “incrustations” (similar incrustations are formed)
Page 102 — “incrustrations” changed to “incrustations” (similar incrustations are formed)
Page 107 — “desquemated” changed to “desquamated” (the pimple has broken or desquamated)
Page 107 — “desquemated” changed to “desquamated” (the pimple has burst or desquamated)
Page 109 — “raced” changed to “traced” (to such weknesses may be traced the relapses)
Page 109 — “raced” changed to “traced” (to such weaknesses may be traced the relapses)
Page 118 — “desquemate” changed to “desquamate” (exfoliate, or scurf, or desquamate)
Page 118 — “desquemate” changed to “desquamate” (exfoliate, or flakes of dead skin, or desquamate)
Page 125 — “are are” changed to “are” (There are also deep and painful fissures)
Page 125 — “are” changed to “are” (There are also deep and painful fissures)
Page 131 — “pecuiar” changed to “peculiar” (a peculiar contour of the countenance)
Page 131 — “pecuiar” changed to “peculiar” (a peculiar contour of the face)
Page 134 — “triflind” changed to “trifling” (trifling errors in diet)
Page 134 — “trifling” changed to “trifling” (trifling errors in diet)
Page 137 — “unimpergnated” changed to “unimpregnated” (when unimpregnated, is very compact)
Page 137 — “unimpregnated” changed to “unimpregnated” (when unimpregnated, is very compact)
Page 146 — “corpulant” changed to “corpulent” (like a very corpulent man)
Page 146 — “corpulent” changed to “corpulent” (like a very corpulent man)
Page 149 — “ipresses” changed to “impresses” (the womb impresses upon the bladder)
Page 149 — “impresses” changed to “impresses” (the womb impresses upon the bladder)
Page 167 — “Henry III.” changed to “Henry II.” (Henry II. consulted one Fernal for the infertility of his queen, Catherine de Medicis)
Page 167 — “Henry III.” changed to “Henry II.” (Henry II consulted a man named Fernal about the infertility of his queen, Catherine de Medicis)
Page 196 — “protusion” changed to “protrusion” (extraordinary protrusion of piles)
Page 196 — “protusion” changed to “protrusion” (extraordinary protrusion of piles)
Page 200 — “bladders” changed to “bladder” (into the bladder whence it is voided)
Page 200 — “bladders” changed to “bladder” (into the bladder from which it is expelled)
Page 214 — “pharmacopœa” changed to “pharmacopœia” (of our pharmacopœia)
Page 214 — “pharmacopœa” changed to “pharmacopœia” (of our pharmacopoeia)
In anatomical references, the book uses “chord” throughout in place of “cord” — see for example “umbilical chord” and “spermatic chord”.
In anatomical references, the book uses “chord” throughout instead of “cord” — see, for example, “umbilical chord” and “spermatic chord.”
There are seventy-nine treatment recipes/formulæ (“Forms”) in the book. All are printed in a similar style. However fifty-five appear as footnotes while the rest appear in page text. For ease of reference in the transcription, all the footnoted Forms have been gathered together and moved to a new FORMULÆ annex at the end of the book. Minor changes to the page text consequent on the new arrangement are as follows:
There are seventy-nine treatment recipes/formulas (“Forms”) in the book. All are printed in a similar style. However, fifty-five are shown as footnotes while the rest are in the main text. To make it easier to reference in the transcription, all the footnoted Forms have been collected and moved to a new FORMULÆ annex at the end of the book. Minor changes to the main text due to the new arrangement are as follows:
Page 31 — “[See annexed Formulæ 2, 3, 4, 5.]” changed to “[See Forms 2, 3, 4, 5 in Formulæ annex.]”
Page 31 — “[See annexed Formulæ 2, 3, 4, 5.]” changed to “[See Forms 2, 3, 4, 5 in Formulæ annex.]”
Page 33 — “Subjoined are” changed to “See Formulæ annex for”
Page 33 — “See Formulæ annex for”
Page 34 — “(see note)” changed to “(see Formulæ annex)”
Page 34 — “(see note)” changed to “(see Formulæ annex)”
While the original style and content of the seventy-nine Forms has been carefully preserved, minor corrections to the layout of some have been made so that all are displayed to the reader in a consistent format. This avoids small but distracting variations on a page that look like errors in transcription. For the same reason, variations in the spelling of dosage measures in the Forms have been regularised. Thus “table spoonful”, “table-spoonful” and “tablespoonful” all appear as “tablespoonful”. Similarly for “teaspoonful” and “wineglassful”. Plural forms have been changed in the same way. For consistency, the regularising of these words has also been applied to their appearance elsewhere in the body text.
While the original style and content of the seventy-nine Forms have been carefully preserved, minor layout corrections have been made to ensure that all are presented to the reader in a uniform format. This prevents small but distracting variations on a page that may appear as transcription errors. For the same reason, inconsistencies in the spelling of dosage measures in the Forms have been standardized. Thus “table spoonful,” “table-spoonful,” and “tablespoonful” all appear as “tablespoonful.” The same goes for “teaspoonful” and “wineglassful.” Plural forms have been adjusted in the same manner. For the sake of consistency, this standardization has also been applied to these words throughout the main text.
Ordinary footnotes have been re-indexed using numbers and moved to a FOOTNOTES section placed after the FORMULÆ annex.
Ordinary footnotes have been renumbered and moved to a FOOTNOTES section located after the FORMULÆ annex.
References on a page to originally footnoted Forms are now clickable links to their text in the new FORMULÆ annex. Ordinary footnote references on a page are now clickable links to their text in the FOOTNOTES section.
References on a page that were originally footnoted are now clickable links to their text in the new FORMULÆ annex. Regular footnote references on a page are now clickable links to their text in the FOOTNOTES section.
For technical reasons beyond the control of the transcriber, long chapters in this EPUB version have had to be partitioned into smaller segments of text and illustrations. The reader will see the break between each segment represented as a ‘thought break’. They appear at places in the chapter where the author has started a new subject for discussion. These are easily recognised because the author features the subject title in italic font as the first sentence of a new paragraph. The following extract is an example:
For technical reasons beyond the transcriber's control, long chapters in this EPUB version have been divided into smaller sections of text and illustrations. The reader will notice the break between each section marked as a 'thought break.' These occur at points in the chapter where the author introduces a new topic for discussion. They are easily identified because the author presents the topic title in italic font as the first sentence of a new paragraph. The following extract is an example:
The Surgical Treatment of Gonorrhœa.—The principal symptoms ....
The Surgical Treatment of Gonorrhea.—The main symptoms ....
When a thought break occurs before such a paragraph, it is displayed to the reader as a short, centered, rule thus:
When a thought break happens before a paragraph, it appears to the reader as a short, centered line like this:
———<>———
Below is a short piece of text (5 words or fewer). Modernize it into contemporary English if there's enough context, but do not add or omit any information. If context is insufficient, return it unchanged. Do not add commentary, and do not modify any placeholders. If you see placeholders of the form __A_TAG_PLACEHOLDER_x__, you must keep them exactly as-is so they can be replaced with links. ———<>———
The original chapter text around a thought break is not altered in any way.
The original chapter text around a thought break is not altered in any way.
Download ePUB
If you like this ebook, consider a donation!